BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
If you’re looking at this tab, chances are you are fed up, burned out, seeking a better work-life balance, looking for a new non-clinical career, thinking of retirement, or all of the above. Perhaps you are just looking to regain the joy and meaning in your medical career. No worries! You may have come to the right place.
We work only with doctors, dentists, podiatrists, nurses, technicians and healthcare providers who struggle with personal and professional disillusionment, burnout, financial distress and an unbalanced life – all of which can happen at any stage of a medical career.
Through our coaching sessions, medical and healthcare professionals and colleagues can achieve a more meaningful, purposeful, and financially flourishing life.
Life planning and behavioral finance as proposed for physicians and integrated by the Institute of Medical Business Advisors Inc., is unique in that it emanates from a holistic union of personal financial planning, human physiology and medical practice management, solely for the healthcare space. Unlike pure life planning, pure financial planning, or pure management theory, it is both a quantitative and qualitative “hard and soft” science, with an ambitious economic, psychological and managerial niche value proposition never before proposed and codified, while still representing an evolving philosophy. Its’ first-mover practitioners are called Certified Medical Planners™.
Financial Life Planning is an approach to financial planning that places the history, transitions, goals, and principles of the client at the center of the planning process. For the financial advisor or planner, the life of the client becomes the axis around which financial planning develops and evolves.
Financial Life Planning is about coming to the right answers by asking the right questions. This involves broadening the conversation beyond investment selection and asset management to exploring life issues as they relate to money.
Financial Life Planning is a process that helps advisors move their practice from financial transaction thinking, to life transition thinking. The first step is aimed to help clients “see” the connection between their financial lives and the challenges and opportunities inherent in each life transition.
But, for informed physicians, life planning’s quasi-professional and informal approach to the largely isolate disciplines of financial planning and medical practice management is inadequate. Today’s practice environment is incredibly complex, as compressed economic stress from HMOs managed care, financial insecurity from insurance companies, ACOs and VBC, Washington DC and Wall Street; liability fears from attorneys, criminal scrutiny from government agencies, and IT mischief from malicious electronic medical record [eMR] hackers. And economic bench marking from hospital employers; lost confidence from patients; and the Patient Protection and Affordable Care Act [PP-ACA] more than a decade ago. All promote “burnout” and converge to inspire a robust new financial planning approach for physicians and most all medical professionals.
The iMBA Inc., approach to financial planning, as championed by the Certified Medical Planner™ professional certification designation program, integrates the traditional concepts of financial life planning, with the increasing complex business concepts of medical practice management. The former topics are presented in this textbook, the later in our recent companion text: The Business of Medical Practice [Transformational Health 2.0 Skills for Doctors].
***
***
For example, views of medical practice, personal lifestyle, investing and retirement, both what they are and how they may look in the future, are rapidly changing as the retail mentality of medicine is replaced with a wholesale and governmental philosophy. Or, how views on maximizing current practice income might be more profitably sacrificed for the potential of greater wealth upon eventual practice sale and disposition.
Or, how the ultimate fear represented by Yale University economist Robert J. Shiller, in The New Financial Order: Risk in the 21st Century, warns that the risk for choosing the wrong profession or specialty, might render physicians obsolete by technological changes, managed care systems or fiscally unsound demographics. OR, if a medical degree is even needed for future physicians?
Say, what medical license?
Dr. Shirley Svorny, chair of the economics department at California State University, Northridge, holds a PhD in economics from UCLA. She is an expert on the regulation of health care professionals who participated in health policy summits organized by Cato and the Texas Public Policy Foundation. She argues that medical licensure not only fails to protect patients from incompetent physicians, but, by raising barriers to entry, makes health care more expensive and less accessible. Institutional oversight and a sophisticated network of private accrediting and certification organizations, all motivated by the need to protect reputations and avoid legal liability, offer whatever consumer protections exist today.
Yet, the opportunity to revise the future at any age through personal re-engineering, exists for all of us, and allows a joint exploration of the meaning and purpose in life. To allow this deeper and more realistic approach, the informed transformation advisor and the doctor client, must build relationships based on trust, greater self-knowledge and true medical business management and personal financial planning acumen.
[A] The iMBA Philosophy
As you read this ME-P website, we hope you will embrace the opportunity to receive the focused and best thinking of some very smart people. Hopefully, along the way you will self-saturate with concrete information that proves valuable in your own medical practice and personal money journey. Maybe, you will even learn something that is so valuable and so powerful, that future reflection will reveal it to be of critical importance to your life. The contributing authors certainly hope so.
At the Institute of Medical Business Advisors, and thru the Certified Medical Planner™ program, we suggest that such an epiphany can be realized only if you have extraordinary clarity regarding your personal, economic and [financial advisory or medical] practice goals, your money, and your relationship with it. Money is, after only, no more or less than what we make of it.
Ultimately, your relationship with it, and to others, is the most important component of how well it will serve you.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Classic: Flat fee paid for a patient’s treatment based on their diagnosis and/or presenting problem. For this fee the provider covers all of the services required for a specific period of time.
Modern: Often characterizes “second generation” managed care systems. After a Managed Care Organization squeezes out costs by discounting fees, they often come to this method. If provider is still standing after discount blitz, this approach can be good for provider and clients, since it permits a lot of flexibility for provider in meeting client needs.
When New York-based Zocdoc was founded back in 2007, the idea was to help patients get off the phone, founder and CEO Oliver Kharraz told Healthcare Brew. The company created a website that helps patients find clinicians who fit their needs in their area and are under their insurance, and books appointments online.
But on May 1st, Zocdoc launched a new product to get people back on the phone: an artificial intelligence (AI) voice agent called Zo. Zo helps people book doctor appointments 24/7—but instead of speaking with a person, patients speak with an AI voice that is trained to meet their needs.
“Until recently, we didn’t do the phone because the experience on the phone was just so miserable,” Kharraz said. “Now you can actually have a consistent experience, where the AI can pick up after the first ring an unlimited number of times concurrently [and] have a natural conversation with you.”
When you visit health clinic or hospital for a medical appointment, you’ll be seen by a doctor, healthcare provider and/or medical prescriber. But what do these words really mean?
***
***
Doctors / Physicians
Doctor of Medicine (MD), Doctor of Podiatric Medicine (DPM), Doctor of Osteopathy (DO, or Doctor of Dental Surgery (DDS/DMD). Doctors, also known as physicians, have extensive prescription privileges across various specialties. They can diagnose medical conditions, prescribe medication, and oversee the overall management of patient care. Doctors include general practitioners, specialists such as cardiologists or dermatologists, and surgeons. Their prescription authority encompasses a wide range of medications to address acute and chronic health conditions, ranging from antibiotics to specialized treatments for complex diseases.
A medical provider is a general term that encompasses a wide range of education levels, skill-sets, and specializations. A provider could be a Physician Assistant (PA), Nurse Practitioner (NP), Clinical Nurse Specialist (CNS), Doctor of Medicine (MD), Doctor of Podiatric Medicine (DPM), Dentist (DDSDMD) or Doctor of Osteopathy (DO).
***
Medical Drug Prescribers
Generally, psychologists and therapists do not have prescription privileges. They focus on psychotherapy and counseling rather than medication management. However, some jurisdictions may grant limited prescription rights to psychologists who undergo additional training and certification. Like psychologists, therapists typically do not have prescription privileges. They focus on providing counseling and psychotherapy to address mental health issues and emotional concerns.
Psychiatrists are medical doctors (MD/DO) who specialize in the diagnosis and treatment of mental health disorders. They have full prescription privileges and can prescribe a wide range of medications to manage psychiatric conditions.
In most cases, physical therapistsdo not have the authority to prescribe medication. They primarily focus on rehabilitation and physical interventions to improve mobility and function.
Nurse practitioners are advanced practice nurses with the authority to diagnose, treat, and prescribe medication independently in many states and countries. They undergo extensive education and training, which allows them to provide a wide range of healthcare services, including medication management.
Similar to nurse practitioners, psychiatric nurse practitioners have the authority to prescribe medication for mental health conditions. They specialize in psychiatric and mental health care, offering comprehensive treatment that may include medication management.
Chiropractors primarily focus on diagnosing and treating musculoskeletal disorders through manual adjustments and therapies. They do not have surgical or prescription privileges in most jurisdictions.
Optometrists are trained to diagnose and treat vision problems, including prescribing corrective lenses and medications for certain eye conditions such as infections or inflammation.
Registered nursestypically do not have prescription privileges. They work under the direction of physicians and nurse practitioners, assisting with patient care but not prescribing medication themselves.
Dentists have limited prescription privileges related to dental care, such as antibiotics or pain medications for dental procedures. However, they do not have the authority to prescribe general medications outside of their scope of practice.
Nutritionists typically do not have prescription privileges. They specialize in providing dietary advice and counseling to promote health and well-being through nutrition but do not prescribe medication.
Depending on their scope of practice and legal regulations in their jurisdiction, nurse midwives may have limited prescription privileges for certain medications related to prenatal care, childbirth, and postpartum care.
A hedge fund is a limited partnership of private investors whose money is pooled and managed by professional fund managers. These managers use a wide range of strategies, including leverage (borrowed money) and the trading of nontraditional assets, to earn above-average investment returns. A hedge fund investment is often considered a risky, alternative investment choice and usually requires a high minimum investment or net worth. Hedge funds typically target wealthy investors.
My medical practice has a small self-directed pension plan with profit sharing features.
QUESTION: Can my medical practice’s retirement plan invest in a hedge fund?
Such a pension fund falls under a category called self-directed “plan” assets.
Among the rules are that each participant in the plan counts toward the 100 investor maximum under which most hedge funds operate, that each plan participant be a fully accredited investor, and that the hedge fund keep investments such as pension plans and other funds covered under ERISA to less than 25 percent of total assets under management.
An emergency medicine physician is a medical doctor who specializes in the diagnosis, treatment, and management of acute and life-threatening medical conditions that require immediate intervention. These physicians work in hospital emergency departments, urgent care centers, and other acute care settings, where they provide rapid assessment, stabilization, and treatment to patients of all ages with a wide range of medical emergencies.
Emergency medicine physicians are trained to handle diverse medical emergencies, including trauma, cardiac emergencies, respiratory distress, severe infections, neurological emergencies, and obstetric emergencies, among others. They play a vital role in the front line management of medical emergencies, ensuring that patients receive prompt and appropriate care to improve outcomes and save lives.
***
Classic: Emergent Room or Emergency Department care is the provision of immediate medical service offering outpatient care for the treatment of acute and chronic illness and injury. It requires a broad and comprehensive fund of knowledge to provide such care. Excellence in care for patients with complex and or unusual conditions is founded on the close communication and collaboration between the urgent care medicine physician, the specialists and the primary physicians.
Modern: Urgent care does not replace your primary care physician. An urgent care center is a convenient option when someone’s regular physician is on vacation or unable to offer a timely appointment. Or, when illness strikes outside of regular office hours, urgent care offers an alternative to waiting for hours in a hospital Emergency Room.
Examples: Chest pain, bleeding that cannot be stopped and loss of consciousness; etc.
***
***
SOME ER DOCTORS WORK FOR FREE
The new president of emergency medicine for the Alberta Medical Association says Emergency Room physicians already coping with long hours, staff shortages and jammed waiting rooms are also being obligated, in some cases, to work for free. Dr. Warren Thirsk says the government has yet to follow through on a promise to reimburse emergency room doctors for so-called “good faith” payments.
“There’s been lots of excuses, but the bottom line is no one has actually received a penny for those suspended good-faith payments,” Thirsk said in an interview. “On average, every emergency physician in this province is out thousands of dollars for free work.” Good-faith payments reimburse ER doctors when they see patients who don’t have identification and can’t prove an Alberta Health Care Insurance Plan billing number.
Thirsk said the United Conservative government stopped those payments when it ripped up the master agreement with the AMA in early 2020. He said it promised to bring back those payments when the two sides agreed to a new deal in September 2022. But to date that hasn’t happened, he said.
“I’m legally and morally bound to look after you [if] you’re unidentified [as a patient],” said Thirsk, an emergency room doctor at Edmonton’s Royal Alexandra Hospital.
“I’m going to look after you because it’s the right thing to do no matter what the problem is.”
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Posted on April 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Classic Definition: Suppose someone tells you “I am lying.” If what he/she tells you is true, then he/she is lying, in which case what he/she tells you are false. On the other hand, if what he/she tells you is false, then he/she is not lying, in which case what he/she tells you is true.
Modern Circumstance: In short: if “I am lying” is true then it is false, and if it is false then it is true.
Paradox Example: The paradox arises for any sentence that says or implies of itself that it is false (the simplest example being “This sentence is false”). It is attributed to the ancient Greek seer Epimenides (fl. c. 6th century BCE), an inhabitant of Crete, who famously declared that “All Cretans are liars” (consider what follows if the declaration is true). The paradox is important in part because it creates severe difficulties for logically rigorous theories of truth; it was not adequately addressed (which is not to say solved) until the 20th century.
Paradox Example: Doctors lie because, as caretakers, our role isto improve the lives of their patients. Re-assuring patients during some of the most difficult times of their lives counts as improving their well being! This is an acceptable practice because it does not cause harm.
Paradox Example: Cultural differences may make a lie of omission or the practice of withholding information from the patient, prudent. For instance, some cultures and religions dictate that the husband or head male family members make all medical decisions for women.
Paradox Example: Many physicians don’t report “near misses” to their patients. But, concealing serious medical errors is something we recommend against.
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals.
Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed.
Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Several years ago a group of highly trusted and deeply experienced financial advisors, insurance service professionals and estate planners noted that far too many of their mature retiring physician clients, using traditional stock brokers, management consultants and financial advisors, seemed to be less successful than those who went it alone. These Do-it-Yourselfers [DIYs] had setbacks and made mistakes, for sure. But, the ME Inc doctors seemed to learn from their mistakes and did not incur the high management and service fees demanded from general or retail one-size-fits-all “advisors.”
In fact, an informal inverse related relationship was noted, and dubbed the “Doctor Effect.” In others words, the more consultants an individual doctor retained; the less well they did in all disciplines of the financial planning and medical practice management, continuum.
Of course, the reason for this discrepancy eluded many of them as Wall Street brokerages and wire-houses flooded the media with messages, infomercials, print, radio, TV, texts, tweets, dinners and internet ads to the contrary. Rather than self-learn the basics, the prevailing sentiment seemed to purse the holy grail of finding the “perfect financial advisor.” This realization confirmed the industry culture which seemed to be:
Bread for the advisor – Crumbs for the client!
And so, Marcinko Associates formed a cadre’ of technology focused and highly educated multi-degreed doctors, nurses, financial advisors, attorneys, accountants, psychologists and educational visionaries who decided there must be a better way for their healthcare colleagues to receive financial planning advice, products and related advisory services within a culture of fiduciary responsibility.
We trust you agree with this specific niche knowledge, and collegial consulting philosophy, as illustrated thru our firm and these two books.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on April 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
OVER HEARD IN THE FINANCIAL ADVISOR’S LOUNGE
***
***
By Perry D’Alessio, CPA [D’Alessio Tocci & Pell LLP]
What I see in my accounting practice is that significant accumulation in younger physician portfolio growth is not happening as it once did. This is partially because confidence in the equity markets is still not what it was; but that doctors are also looking for better solutions to support their reduced incomes.
For example, I see older doctors with about 25 percent of their wealth in the market, and even in retirement years, do not rely much on that accumulation to live on. Of this 25 percent, about 80 percent is in their retirement plan, as tax breaks for funding are just too good to ignore.
What I do see is that about 50 percent of senior physician wealth is in rental real estate, both in a private residence that has a rental component, and mixed-use properties. It is this that provides a good portion of income in retirement.
***
***
QUESTION: So, could I add dialog about real estate as a long term solution for retirement?
Yes, as I believe a real estate concentration in the amount of 5 percent is optimal for a diversified portfolio, but in a very passive way through mutual or index funds that are invested in real estate holdings and not directly owning properties.
Today, as an option, we have the ability to take pension plan assets and transfer marketable securities for rental property to be held inside the plan collecting rents instead of dividends.
Real estate holdings never vary very much, tend to go up modestly, and have preferential tax treatment due to depreciation of the property against income.
Posted on April 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Credit Card Mistakes to Avoid
No number has as far-reaching an impact on your money as your credit scores. Here are some credit card obstacles all physicians, nurses and medical professionals should dodge on the road to financial security
Posted on April 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
THE “FIVE-FIVE” FINANCIAL RULE
By Staff Reporters
***
***
Many of the pros of home ownership will appeal to medical retirees for whom their home is their castle and who appreciate being settled both financially and geographically:
1. Building equity in your home: Each mortgage payment you make brings you closer to owning your house free and clear with no payments. If you can buy a new home or condo outright by selling your current home, you can still build equity in your new home over time.
2. Predictability: If you have a fixed-rate mortgage, your mortgage payments will remain consistent for years and you don’t have to worry about a landlord ever making you move.
3. Tax benefits: You can deduct mortgage interest and property taxes up to certain limits.
4. Customization: You don’t need a landlord’s permission to alter and improve your home.
5. Home appreciation: Homes generally increase in value, so you can increase your net worth by owning a property.
***
***
Renting also has five significant upsides, particularly for physician retirees who want greater freedom to travel and to make bigger moves — potentially across the country or even abroad:
1. Extreme flexibility: You can leave your property after giving notice and go wherever you want much more easily than with an illiquid home you’d have to sell first.
2. Lower upfront costs: You only have to pay first and last month’s rent and a security deposit to move into a rental, not make a large home down payment.
3. No maintenance concerns: If something breaks, your landlord is responsible for the cost of fixing it and the actual repairs. You don’t have to build up an emergency fund for maintenance.
4. Predictable expenses: For the duration of your lease, your monthly housing costs including utilities will remain consistent, even if the cost of energy goes up, for example.
5. Lack of worry: If you’re in a rental apartment, you won’t have to concern yourself with shoveling snow, mowing grass or other matters of upkeep.
Posted on April 11, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Why would a doctor consider a Roth IRA conversion?
By Staff Reporters
***
***
A Roth conversion involves transferring funds from a traditional retirement account—such as a 401(k), 403(b), or individual retirement account (IRA) funded with pre-tax dollars—into a Roth IRA.
The biggest benefit lies in the tax treatment of the converted funds. Once the funds are in the Roth IRA, future growth of those assets is tax-free. Withdrawals in retirement are also tax-free, assuming they meet certain criteria. As with any strategy, there are important considerations to keep in mind.
When you convert funds to a Roth IRA, the amount converted is taxable income in that tax year. For example, if you convert $100,000 from a traditional IRA to a Roth IRA, that $100,000 will be added to your taxable income in the conversion year.
Converting large amounts can result in a significant tax bill and may push you into a higher tax bracket. Even so, using retirement funds to pay taxes may make sense for those looking to convert large IRAs to reduce their future required minimum distributions (RMDs).
The timing of your Roth conversion matters too. Generally, it’s a good idea to convert when your income is lower—for example, after you’ve retired and before you begin drawing Social Security. You may also choose to convert over the course of several years to spread out the tax impacts. But if you can get comfortable with these considerations, a Roth conversion can provide you with benefits beyond tax-free growth and withdrawals.
Some of these benefits are:
Tax diversification. Having both traditional and Roth accounts allows you to manage your tax liability in retirement. For example, if your income in a given year is higher than expected, you can withdraw from the Roth IRA without increasing your taxable income.
No RMDs. Traditional IRAs and 401(k)s require you to begin taking RMDs at age 73. Roth IRAs have no RMD requirement during your lifetime. With a Roth account, you have more control over your retirement withdrawals and can leave the funds to grow for your heirs.
Benefits for heirs. Roth IRAs can be passed on to beneficiaries, who can inherit the account income tax-free. This means your heirs can enjoy the tax-free growth and withdrawals if the Roth IRA has been held for five years or more—a significant advantage, especially if your beneficiaries are in a higher tax bracket.
Financial Modeling is one of the most highly valued, but thinly understood, skills in financial analysis. The objective of financial modeling is to combine accounting, finance, and business metrics to create a forecast of a company’s future results.
According to Jeff Schmidt, a financial model is simply a spreadsheet, usually built in Microsoft Excel, that forecasts a business’s financial performance into the future. The forecast is typically based on the company’s historical performance and assumptions about the future and requires preparing an income statement, balance sheet, cash flow statement, and supporting schedules (known as a three-statement model, one of many types of approaches to financial statement modeling). From there, more advanced types of models can be built such as discounted cash flow analysis (DCF model), leveraged buyout (LBO), mergers and acquisitions (M&A), and sensitivity analysis
***
DEFINED TERMS
Discounted Cash Flow (DCF): A valuation method used to estimate the value of an investment based on its expected future cash flows, adjusted for the time value of money. It’s like deciding whether a treasure chest is worth diving for now, based on the gold coins you’ll be able to cash in later.
Sensitivity Analysis: This involves changing one variable at a time to see how it affects an outcome. Imagine tweaking your coffee-to-water ratio each morning to achieve the perfect brew strength.
Budget – A budget is the amount of money a department, function, or business can spend in a given period of time. Usually, but not always, finance does this annually for the upcoming year.
Rolling Forecast – A rolling forecast maintains a consistent view over a period of time (often 12 months). When one period closes, finance adds one more period to the forecast.
Topside – A topside adjustment is an overlay to a forecast. This is typically completed by the corporate or headquarter team. As individual teams submit a forecast, the consolidated result might not make sense or align with expectations. When this occurs, the high-level teams use a topside adjustment to streamline or adjust the consolidated view.
Monte Carlo Simulation: Picture yourself at the casino, but instead of gambling your savings away, you’re using this technique to predict different outcomes of your business decisions based on random variables. It’s like playing financial roulette with the odds in your favor.
What-If Analysis: Ever daydream about what would happen if you took that leap of faith with your business? This tool allows you to explore various scenarios without risking a dime. It’s like trying on outfits in a virtual dressing room before making a purchase.
Leveraged Buyout (LBO) Model: This is a bit like orchestrating a heist, but legally. It’s about acquiring a company using borrowed money, with plans to pay off the debts with the company’s own cash flows. High stakes, high rewards.
Mergers and Acquisitions (M&A) Model: Picture two puzzle pieces coming together. This model evaluates how combining companies can create a new, more valuable entity. It’s the corporate version of a matchmaker.
Three Statement Model: The holy trinity of financial modeling, linking the income statement, balance sheet, and cash flow statement. It’s like weaving a tapestry where each thread is crucial to the overall picture.
Capital Asset Pricing Model (CAPM): A formula that calculates the expected return on an investment, considering its risk compared to the market. It’s like choosing the best roller coaster in the park, balancing thrill and safety.
Cash Flow Forecasting: This is your financial weather forecast, predicting the cash flow climate of your business. It helps you plan for sunny days and save for the rainy ones.
Cost of Capital: The price of financing your business, whether through debt or equity. It’s like the interest rate on your growth engine, pushing you to maximize every dollar invested.
Debt Schedule: A timeline of your business’s debts, showing when and how much you owe. It’s your roadmap to becoming debt-free, one milestone at a time.
Equity Valuation: Determining the value of a company’s shares. It’s like assessing the worth of a rare gemstone, ensuring investors pay a fair price for a piece of the treasure.
Financial Leverage: Using debt to amplify returns on investment. It’s like using a lever to lift a heavy object, increasing force but also risk.
Forecast Model: A crystal ball for your finances, projecting future performance based on past and present data. It’s your guide through the financial wilderness, helping you navigate with confidence.
Operating Model: A detailed blueprint of how a business generates value, mapping out operational activities and their financial impact. It’s like laying out the inner workings of a clock, ensuring every gear turns smoothly.
Revenue Growth Model: This tracks potential increases in sales over time, charting a course for expansion. It’s like plotting your ascent up a mountain, anticipating the effort required to reach the summit.
Posted on April 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
ACCOUNTABLE CARE ORGANIZATIONS
Realizing Equity, Access, and Community Health
By Staff Reporters
***
***
Model Overview
The ACO REACH Model provides novel tools and resources for health care providers to work together in an ACO to improve the quality of care for people with Traditional Medicare. REACH ACOs are comprised of different types of providers, including primary and specialty care physicians.
The ACO REACH Model makes important changes to the previous Global and Professional Direct Contracting (GPDC) Model which include:
***
***
Promote Provider Leadership and Governance. The ACO REACH Model includes policies to ensure doctors and other health care providers continue to play a primary role in accountable care. At least 75% control of each ACO’s governing body generally must be held by participating providers or their designated representatives, compared to 25% during the first two Performance Years of the GPDC Model. In addition, the ACO REACH Model goes beyond prior ACO initiatives by requiring at least two beneficiary advocates on the governing board (at least one Medicare beneficiary and at least one consumer advocate), both of whom must hold voting rights.
Protect Beneficiaries and the Model with More Participant Vetting, Monitoring and Greater Transparency. CMS will ask for additional information on applicants’ ownership, leadership, and governing board to gain better visibility into ownership interests and affiliations to ensure participants’ interests align with CMS’s vision. We will employ increased up-front screening of applicants, robust monitoring of participants, and greater transparency into the model’s progress during implementation, even before final evaluation results, and will share more information on the participants and their work to improve care. Last, CMS will also explore stronger protections against inappropriate coding and risk score growth.
Posted on April 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
WARNING – WARNING
By Dr. DavidEdwardMarcinko; MBA MEd
***
***
According to www.NPR.org, there are more than120,000 health care forums on the Internet with opinions ranging from pharmaceuticals, to sexual dysfunction, to acne. The same goes for commercial doctor blogs that promote lotions, balms and potions, diets and vitamins, minerals, herbs, drinks and elixirs, or various other ingest-ants, digest-ants or pharmaceuticals, etc.
And, to other doctors, the blogging craze is a new novelty where there are no rules, protocols, standards or precise figures on how many “medical-doctor” or related physician-blogs are “out there.” Unfortunately, too many recount gory ER scenes, or pictorially illustrate horrific medical conditions, or serious and traumatic injuries. Of course, others simply are medical practice websites, or those that entice patients into more lucrative plastic surgery or concierge medical practices. Some are from self-serving/credible plaintiff-seeking attorneys wishing to assist patients.
Not all physician blogs are geared toward practice information, marketing or medical sensationalism. In fact, just the opposite seems to be the case in extremely candid blogs, like “Ranting Docs”, “White Coat Rants,” “Grunt Docs”, “Cancer Doc,” “The Happy Hospitalist,” “Mom MD”, “Cross-Over Health”, “Angry Docs” and “M.D.O.D.,” which bills itself as “Random Thoughts from a Few Cantankerous American Physicians.”
According to some of these, they are more like personal journals, or public diaries, where doctors vent about reimbursement rates, difficult cases, medical mistakes, declining medical prestige and control, and/or what a “bummer” it is to have so many patients die; not pay, or who are indigent, noncompliant. We call these the “disgruntled doctor sites.” Some even talk about their own patients, coding issues, or various doctor-patient shenanigans.
But, according to psychiatrist and blogger Dr. Deborah Peel and others, the problem with blogging about patients is the danger that one will be able to identify themselves – the doctor – or that others who know them will be able to identify them.” Her affiliation, Patient Privacy Rights, rightly worries that patients might track back to the individual, and adversely affect their employment, health insurance or other aspects of life.
***
***
And, according to Dr. Jay S. Grife; MA Esq., it is certainly true that if a doctor violates a patient’s privacy there could be legal consequences. Under HIPAA, physicians could face fines or even jail time. In some states, patients can file a civil lawsuit if they believe a doctor has violated their privacy. Still, internet privacy issues are an evolving gray-area that if not wrong, may still be morally and ethically questionable [personal communication].
Our colleague Robert Wachter MD, author of the blog called “Wachter’s World,” says it’s important for doctors to be able to share cases, as long as they change the facts substantially. On the other hand, the author of “Wachter’s World” and a leading expert on patient safety alternately suggests “You might say we as doctors should never be talking about experiences with our patients online or in books or in articles.” But, he says that “patients shouldn’t take all the information on blogs at face value. Taken for what they are — unedited opinions, and in some cases entertainment — blogs can give readers some useful insight into the good, the bad and the ugly of the medical profession”. Link: http://www.the-hospitalist.org/blogs
Well, fair enough! But, doctors unhappy with their current medical career choice, or its modern evolution, should probably consider counseling or even career change guidance, re-education and re-engineering. It is very inappropriate to vent career frustrations in a public venue. It’s far better for the blog to be private and/or by invitation only; if at all [Personal communication].
We believe that a hybrid mash-up of both views can be wholly appropriate, or grossly inappropriate in some cases. Of course the devil is in the details; linguistics and semantics aside. Nevertheless; what is not addressed in electronic physician “mea-culpas” are the professional liability risks and concerns that are evolving in this quasi-professional, quasi-lay, communication forum.
***
***
Example: We have seen medical mistakes, and liability admissions of all sorts, freely and glibly presented. In fact,
“Some physicians find that the act of liability blogging as a professional confession that is useful in moving past their malpractice mistakes. And, it is also a useful way to begin a commitment to a better professional life of caring in the future. It helps eliminate the toxic residue and angst of professional liability and guilt. Moreover, as they are unburdened of past acts of omission or commission, doctors should remember to also forgive those who have wronged them. This helps greatly with the process and brings additional peace.”
However, although some may say that this electronic confession is good for the soul, it may not be good for your professional liability carrier, or you, when plaintiff’s attorneys release a legion of IT focused interns, or automated bots, searching online for your self-admissions and scouring for your self-incriminations. Of course, a direct connection to a specific patient may still not be made and no HIPAA violation is involved. But, a vivid imagination is not need needed to envision this type of blind medical malpractice discovery deposition query even now.
QUESTION:“Doctor Smith, I noted all the medical errors admitted on your blog. What other mistakes did you make in the care and treatment of my client?”
And so, the question of plausible deniability, or culpability, is easily raised. If you must journalize your thoughts for sanity or stress release; do it in print. And, don’t tell anyone about it so the diary won’t be subpoenaed. Then tear it up and throw it away. Remember, with risk management, “It is all about credibility.” Don’t trash yours! These thoughts may be especially important if you covet a medical career as a researcher, editor, educator, medical expert or something other than a working-class or employed physician.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
On March 15th, 2025, President Donald Trump signed a continuing resolution (CR) that avoided a government shutdown and funds the federal government for the rest of the fiscal year, i.e., through September 30th, 2025.
Perhaps more notable than what was included in the spending bill was what was once again excluded. While the COVID-era tele-health waivers were temporarily extended, Medicare physician payment rates were not addressed, meaning physicians will continue experiencing a 2.93% pay cut for 2025.
This Health Capital Topics article discusses the healthcare provisions included in and excluded from the CR, and the impacts on healthcare providers. (Read more…)
A hedge fund is a limited partnership of private investors whose money is pooled and managed by professional fund managers. These managers use a wide range of strategies, including leverage (borrowed money) and the trading of nontraditional assets, to earn above-average investment returns. A hedge fund investment is often considered a risky, alternative investment choice and usually requires a high minimum investment or net worth. Hedge funds typically target wealthy investors.
QUESTION:Can I invest my Individual Retirement Account [IRA] in a Hedge Fund?
This is up to the manager, but there is no legal restriction on a hedge fund accepting individual retirement account (IRA) assets. IRA accounts are not well suited for funds that make extensive use of leverage, however. In such cases, the fund is likely to generate significant amounts of unrelated business taxable income (UBTI) – profits of the fund attributable to the use of leverage. The holder of an IRA account must pay taxes on UBTI, even if the UBTI was generated in an IRA account.
But, today’s hedge funds may or may not use leverage. Many hedge funds are not hedged at all, but rather are just specialized versions of regular long stock portfolios. If such funds do not use much leverage, IRA investors will not encounter much difficulty with UBTI and should not hesitate in considering these funds.
In considering whether to accept IRA money, hedge fund managers must consider several factors. If the only type of retirement money accepted by the hedge funds is IRA money, then the manager has no limit on how much retirement money the fund can accept. If, however, there are other types of retirement money invested in the fund, such as pension funds, IRA money will be counted towards a total of 25 percent of fund assets that can be invested in retirement accounts before the fund becomes subject to the Employment Retirement Income Security Act of 1974 (ERISA). Funds subject to ERISA regulations face a heavy administrative burden and more restrictions than most fund managers like.
Finally, IRA distributions from a hedge fund are subject to the standard 20 percent withholding unless the funds are directly rolled over to other qualified plans.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on March 29, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
EDITOR-IN-CHIEF
By Dr. David Edward Marcinko; FACFAS MBA MEd
***
***
NATIONAL PHYSICIANS WEEK
National Physicians Week sets out March 25-31 to honor the healers dedicated to the art of medicine. In 2017, National Physicians Week highlighted the shortage of physicians in the United States against a growing landscape of minorities joining the ranks.
#NationalPhysiciansWeek
“In hindsight, I am proud of what we have accomplished in a short period of time, including raising the recognition of our group and spotlighting the years of sacrifice by those in our profession to serve our patients. We are poised to initiate actionable efforts to engage and educate our physician community.”
Cite: Dr. Kimberly Funches Jackson, President
Today in 2025, let’s explore the invaluable contributions of physicians, celebrate their hard work during National Physicians Week, and highlight the essential role that locum doctors play in enhancing healthcare delivery.
A Week to Honor All Physicians
National Physicians Week is a celebration of the remarkable work that doctors do every single day. From diagnosing complex conditions to providing life-saving treatments, physicians dedicate themselves to improving the health and well-being of their patients. It’s a week for healthcare professionals, patients, and communities to come together and show appreciation for the doctors who make a difference in our lives.
Physicians work long hours, face immense pressure, and make critical decisions daily. Their contributions go beyond the walls of the hospital, as many are also involved in research, teaching, and community outreach.
So, this week, it’s important to acknowledge not only their professional expertise but also the compassion and resilience they exhibit in their work.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Both median and average family net worth surged between 2019 and 2022, according to the U.S. Federal Reserve. Average net worth increased by 23% to $1,063,700, the Fed reported in October 2023, the most recent year it published the data. Median net worth, on the other hand, rose 37% over that same period to $192,900.
You might wonder why the average and median net worth figures are so different. That’s because when you take the average of something, you add together every value in a data set and then divide that figure by the number of individual values.
When calculating a median, you simply look at the middle figure within a data set. That said, an average figure can be significantly higher or lower than a median figure if there are extreme outliers – meaning a group of people with significantly more net worth than the rest of the group can bring the average higher.
Average Net Worth by Age
The average net worth of someone younger than 35 years old is $183,500, as of 2022. From there, average net worth steadily rises within each age bracket. Between 35 to 44, the average net worth is $549,600, while between 45 and 54, that number increases to $975,800. Average net worth surges above the $1 million mark between 55 to 64, reaching $1,566,900.
Average net worth again rises for those ages 65 to 74, to $1,794,600, before falling to $1,624,100 for the 75 and older group. The median net worth within every single age bracket, however, is much lower than the average net worth.
***
***
Physicians [MD/DO]Net Worth by Specialty
A 2023 Medscape report shows the top 10 specialties with the most survey respondents saying they are worth more than $5 million.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Without proper internal accounting controls, a medical practice [MD, DO, DPM, DDS, DMD] might never reach peak profitability. Internal controls designed and implemented by the physician-owner help prevent bad things from happening.
Embezzlement protection is the classic example. However, internal controls also help ensure good things happen most of the time; according to colleague Dr. Gary Bode; MSA, CPA.
Some Common Embezzlement “Old School” Schemes
Here are some ‘old-school” embezzlement schemes to avoid; however the list is imaginative and endless.
The physician-owner pocketing cash “off the books”. To the IRS, this is like embezzlement to intentionally defraud it out of tax money.
Employee’s pocketing cash from cash transactions. This is why you see cashiers following protocol that seems to take forever when you’re in the grocery check out line. This is also why you see signs offering a reward if he/she is not offered a receipt. This is partly why security cameras are installed.
Bookkeepers writing checks to themselves. This is easiest to do in flexible software programs like QuickBooks, Peachtree Accounting and related financial software. It is one of the hardest schemes to detect. The bookkeeper self-writes and cashes the check to their own name; and then the name on the check is changed in the software program to a vendor’s name. So a real check exists which looks legitimate on checking statements unless a picture of it is available.
Employees ordering personal items on practice credit cards.
Bookkeepers receiving patient checks and illegally depositing them in an unauthorized, pseudo practice checking account, set up by themselves in a bank different from yours. They then withdraw funds at will. If this scheme uses only a few patients, who are billed outside of the practice’s accounting software it is hard to detect. The doctor must have a good knowledge of existing patients to catch the ones “missing” from practice records. Monitoring the bookkeeper’s lifestyle might raise suspicion, but this scheme is generally low profile and protracted. Checking the accounting software “audit trail” shows the required original invoice deletions or credit memos in a less sophisticated version of this scheme.
Bookkeepers writing payroll checks to non-existent employees. This scheme works well in larger practices and medical clinics with high seasonal turnover of employees, and practices with multiple locations the podiatrist-owner doesn’t visit often.
Bookkeepers writing inflated checks to existing employees, vendors or subcontractors. Physician-owners should beware if romantic relationships between the bookkeeper and other practice related parties.
Bookkeepers writing checks to false vendors. This is another low profile, protracted scheme that exploits the podiatrists-owner’s indifference to accounts payable.
Assessment
Operating efficiency, safeguarding assets, compliance with existing laws and accuracy of financial transactions are common goals of internal managerial and cost accounting in medical practice.
CONCLUSION
Hopefully, the above is a good review to prevent common practice embezzlement schemes. Unfortunately, it is a never-ending endeavor.
References: Marcinko, DE: Dictionary of Health Economics and Finance. Springer Publishing Company, NY 2007.
Posted on March 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
A CONTROVERSY?
By Staff Reporters
***
***
DEFINITION
State medical boards are the agencies that license medical doctors, investigate complaints, discipline physicians who violate the medical practice act, and refer physicians for evaluation and rehabilitation when appropriate. The overriding mission of medical boards is to serve the public by protecting it from incompetent, unprofessional, and improperly trained physicians. Medical boards accomplish this by striving to ensure that only qualified physicians are licensed to practice medicine and that those physicians provide their patients with a high standard of care.
The right to practice medicine is a privilege granted by the state. Each state has laws and regulations that govern the practice of medicine and specify the responsibilities of the medical board in regulating that practice. These regulations are laid out in a state statute, usually called a medical practice act. State medical boards establish the standards for the profession through their interpretation and enforcement of this act.
Assembling a quality physician population to meet the needs of the public begins with licensure. During the process of evaluating applicants for medical licensure, state medical boards’ primary focus is on a physician’s qualifications, including undergraduate and graduate medical education, work history, and personal character.
Candidates for licensure also must successfully complete a rigorous examination designed to assess their ability to apply knowledge, concepts, and principles of health and disease that constitute the basis for safe and effective patient care.
The Federation of State Medical Boards of the United States, Inc., and the National Board of Medical Examiners (NBME) have collaborated to establish a single, 3-step examination for medical licensure in the United States, known as the United States Medical Licensing Examination (USMLE). The USMLE provides state medical boards with a common evaluation system for all licensure applicants. To assure the continued relevance of the exam, the NBME uses basic science and clinical faculty from the nation’s medical schools as well as practicing physicians, some of whom serve on state medical boards, to generate the examinations.
“… I am persuaded that licensure has reduced both the quantity and quality of medical practice…It has reduced the opportunities for people to become physicians, it has forced the public to pay more for less satisfactory service, and it has retarded technological development…I conclude that licensure should be eliminated as a requirement for the practice of medicine”
-Milton Friedman, Nobel prize-winning economist
“As a rule, regulation is acquired by the industry and is designed and operated primarily for its benefit”
-George J. Stigler Nobel Prize-winning economist
“Licensing has served to channel the development of health care services by granting an exclusive privilege and high status to practitioners relying on a particular approach to health care, a disease-oriented intrusive approach rather than a preventive approach….By granting a monopoly to a particular approach to health care, the licensing laws may serve to assure an ineffective health care system”
-Lori B. Andrews, Professor of Law, Chicago-Kent College
“Let us allow physicians, hospitals and schools to spring up where they’re needed, abolish the restrictive licensure laws, and simply invoke the laws against fraud to insure honesty among all providers of health care …That will make health care affordable for everyone”
9. We act with honesty, integrity and are always straightforward. 8. We strive to be innovative, creative, iconoclastic, and flexible. 7. We admit and learn from mistakes and don’t repeat them. 6. We work hard always as competitors are trying to catch up. 5. We treat others with dignity and respect. 4. We are the onus of consulting advice for the well being of others. 3. We fight complacency as former success is in the past. 2. The best management styles are timeless, not timely. 1. Our clients are colleagues and always come first.
SPEAKING: Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements.
***
***
CONTACT: Ann Miller RN MHA at: MarcinkoAdvisors@outlook.com
Posted on March 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
BEHAVIORAL ECONOMICS
By Staff Reporters
***
***
Prospect theory is a psychological and behavioral economics theory developed by Daniel Kahneman and Amos Tversky in 1979. It explains how people make decisions when faced with alternatives involving risk, probability, and uncertainty. According to this theory, decisions are influenced by perceived losses or gains.
Example:
Amanda, a DO client, was just informed by her financial advisor that she needed to re-launch her 403-b retirement plan. Since she was leery about investing, she quietly wondered why she couldn’t DIY. Little does her FA know that she doesn’t intend to follow his advice, anyway! So, what went wrong?
The answer may be that her advisor didn’t deploy a behavioral economics framework to support her decision-making. One such framework is the “prospect theory” model that boils client decision-making into a “three step heuristic.”
Prospect theory makes the unspoken biases that we all have more explicit. By identifying all the background assumptions and preferences that clients [patients] bring to the office, decision-making can be crafted so that everyone [family, doctor and patient] or [FA, client and spouse] is on the same page. Briefly, the three steps are:
1. Simplify choices by focusing on the key differences between investment [treatment] options such as stock, bonds, cash, and index funds.
2. Understanding that clients [patients] prefer greater certainty when it comes to pursuing financial [health] gains and are willing to accept uncertainty when trying to avoid a loss [illness].
3. Cognitive processes lead clients and patients to overestimate the value of their choices thanks to survivor bias, cognitive dissonance, appeals to authority and hindsight biases.
Assessment
Much like healthcare today, the current mass-customized approaches to the financial services industry falls short of recognizing more personalized advisory approaches like prospect theory and assisted client-centered investment decision-making.
Some Stupid Things Financial Advisors Say to Physician Clients
A few years ago and just for giggles, colleague Lon Jefferies MBA CFP® and I collected a list of dumb-stupid things said by some Financial Advisors to their doctor, dentist, nurse and and other medical professional clients, along with some recommended under-breath rejoinders:
“They don’t have any debt except for a mortgage and student loans.” OK. And I’m vegan except for bacon-wrapped steak.
“Earnings were positive before one-time charges.” This is Wall Street’s equivalent of, “Other than that Mrs. Lincoln; how was the play?”
“Earnings missed estimates.” No. Earnings don’t miss estimates; estimates miss earnings. No one ever says “the weather missed estimates.” They blame the weatherman for getting it wrong. Finance is the only industry where people blame their poor forecasting skills on reality.
“Earnings met expectations, but analysts were looking for a beat.” If you’re expecting earnings to beat expectations, you don’t know what the word “expectations” means.
“It’s a Ponzi scheme.” The number of things called Ponzi schemes that are actually Ponzi schemes rounds to zero. It’s become a synonym for “thing I disagree with.”
“The [thing not going perfectly] crisis.” Boy who cried wolf, meet analyst who called crisis.
“He predicted the market crash in 2008.” He also predicted a crash in 2006, 2004, 2003, 2001, 1998, 1997, 1995, 1992, 1989, 1984, 1971…
“More buyers than sellers.” This is the equivalent of saying someone has more mothers than fathers. There’s one buyer and one seller for every trade. Every single one.
“Stocks suffer their biggest drop since September.” You know September was only six weeks ago, right?
“We’re cautiously optimistic.” You’re also an oxymoron.
[Guy on TV]: “It’s time to [buy/sell] stocks.” Who is this advice for? A 20-year-old with 60 years of investing in front of him, or a 82-year-old widow who needs money for a nursing home? Doesn’t that make a difference?
“We’re neutral on this stock.” Stop it. You don’t deserve a paycheck for that.
“There’s minimal downside on this stock.” Some lessons have to be learned the hard way.
“We’re trying to maximize returns and minimize risks.” Unlike everyone else, who are just dying to set their money ablaze!
“Shares fell after the company lowered guidance.” Guys, they just proved their guidance can be wrong. Why are you taking this new one seriously?
“Our bullish case is conservative.” Then it’s not a bullish case. It’s a conservative case. Those words mean opposite things.
“We look where others don’t.” This is said by so many investors that it has to be untrue most of the time.
“Is [X] the next black swan?” Nassim Taleb’s blood pressure rises every time someone says this. You can’t predict black swans. That’s what makes them dangerous.
“We’re waiting for more certainty.” Good call. Like in 1929, 1999 and 2007, when everyone knew exactly what the future looked like. Can’t wait!
“The Dow is down 50 points as investors react to news of [X].” Stop it – you’re just making stuff up. “Stocks are down and no one knows why” is the only honest headline in this category.
“Investment guru [insert name] says stocks are [insert forecast].” Go to Morningstar.com. Look up that guru’s track record against their benchmark. More often than not, their career performance lags an index fund. Stop calling them gurus.
“We’re constructive on the market.” I have no idea what that means. I don’t think you do, either.
“[Noun] [verb] bubble.” (That’s a sarcastic observation from investor Eddy Elfenbein.)
“Investors are fleeing the market.” Every stock is owned by someone all the time.
“We expect more volatility.” There has never been a time when this was not the case. Let me guess, you also expect more winters?
“This is a strong buy.” What do I do with this? Click the mouse harder when placing the order in my brokerage account?
“He was tired of throwing his money away renting, so he bought a house.” He knows a mortgage is renting money from a bank, right?
“This is a cyclical bull market in a secular bear.” Vapid nonsense.
“Will Obamacare ruin the economy?” No. And get a grip.
So, don’t let these aphorisms blind you to the critical thinking skills you learned in college, honed in medical school and apply every day in life.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
In 1972, Nobel Laureate Kenneth J. Arrow, PhD shocked academe’ by identifying health economics as a separate and distinct field. Yet, the seemingly disparate insurance, tax, risk management and financial planning principles that he also studied are just now becoming transparent to some medical professionals and their financial advisors. Despite the fact that a basic, but hardly promoted premise of this new wave financial planning era, is imprecision.
Nevertheless, to informed cognoscenti like Certified Medical Planners™, the principles served as predecessors to the modern physician-focused financial advisory niche sector. In 2004, Arrow was selected as one of eight recipients of the National Medal of Science for his innovative views.
And now, as a long bull market may be over, and if the current “new-normal” prevails – meaning a 4.5% real annualized rate of return on equities and a 1.5% real rate on bonds – wealth accumulation for all may be reduced.
An Imprecise Science
There is a major variable, dominant in any marketplace that pushes an economy in a forward direction. It is called consumerism. This became apparent while waiting in a doctor’s office one recent afternoon.
Scenario:
The front office receptionist, who appeared to be about 21 years old, was breaking for lunch and her replacement, who appeared not much older, came over to assist. Realizing the propensity for a long wait, one was taken by the size of waiting room and the number of patients coming in and out of the office. [Americans consume healthcare and a lot of it]. There was another notable peculiarity. The sample prescription bags being carried out the door were no match for the bags under everyone’s eyes, including the doctor’s. The office staff was probably working overtime, if not two jobs, and the doctor was working harder and faster in a managed care system.
Assessment
Why? So they all could afford to buy and voraciously consume for their children and themselves. Americans indeed work longer hours than any other industrialized nation.
Conclusion
Finally, as women medical professionals entered the workforce in unprecedented numbers, the stock markets reached an all time high in 2025, even as money was spent at a feverish pace as the Federal Reserve pumped out money in inflammatory fashion.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on February 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
A Doctor of Physical Therapy (DPT) helps people improve their mobility and physical functioning, manage pain, and prevent disability. After earning an undergraduate degree, a person can enroll in a DPT program, which is typically three years. The curriculum includes courses in biology, anatomy, physiology, kinesiology (movement), neurology, cardiopulmonary (heart and lung) rehabilitation, behavioral sciences, and pharmacology.
Clinical rotations are a major component of DPT education. They may perform clinical rotations in various settings including a PT clinic, hospital, nursing care facility, rehabilitation clinic, and school. At the end of their coursework and clinical rotation, a student earns a DPT degree but still must pass a state licensure exam to practice as a physical therapist.2
On average, a DPT in the U.S. makes $105,710 per year, according to 2024 statistics.
While a DPT may use the title “Dr,” they are different from an MD/DO/DPM/DDS. A DPT cannot write prescriptions or perform surgery. A DPT is also different from a PhD (Doctor of Philosophy). DPT is treatment-focused, whereas the PhD is research-focused.
It has been said that most ordinary people should have at least three to six months of living expenses (not including taxes) in a cash-equivalent reserve fund that is easily accessible (i.e., liquid). The amount needed for a one-month reserve is equal to the amount of expenses for the month, rather than the amount of monthly income. This is because during no-income months there is no income tax.
However, the situation might not be the same for physicians in today’s harsh economic climate.
The New Realities
Now, some physician-focused financial advisors, financial planners and Certified Medical Planners™ suggest even more reserve fund savings; up to two years. That’s because many factors come into play when determining how much a particular doctor’s family should have.
For example:
Does the family have one income or two? If the doctor is in a dual-income family with stable incomes and they live on a single income, the need for a liquid reserve is less.
How stable is the doctor’s income source? If a sole provider with an unstable income who spends all of the income each month, the need for a liquid cash reserve is high.
Does the doctor own the practice, work in a clinic, medical group, hospital or healthcare system? In other words – employee (less control) or employer (more control).
What is the doctor’s medical specialty and how has managed care penetrated his locale, or affected her focus? What about a DO, DDS/DMD or DPM, etc.
How does the family use its income each month; does it have a saver, spender, or investor mentality?
Does the family anticipate the possibility of large expenses occurring in the future (medical practice start-up costs or practice purchase; children, medical school student debts; auto or home loans; and/or liability suits, etc)?
Pan physician lifestyle?
The Past
In the ancient past, a doctor may have opted for a nine-twelve month reserve if the need for security was high – and a six-to-nine month reserve if the need for security was low. But today, even more may be needed. How about 15-18 months, or more? Perhaps even 24 months!
So, the following questions may be helpful in determining the amount of reserve needed by the physician:
1. How long would it take you to find another job in your medical specialty if you suddenly found yourself unemployed – same for your spouse?
2. Would you have to relocate – same for your spouse?
3. How much do you spend each month on fixed or discretionary expenses and would you be willing to lower your monthly expenses if you were unemployed?
Assessment
Once the amount of reserve is determined, the doctor should use the appropriate investment vehicles for the funds.
At minimum, the reserve should be invested in a money market fund. For larger reserves, an ultra-short-term bond fund might be appropriate for amounts over three-six months. While even larger reserves might be kept in a short term bond fund depending on interest rates and trends.
So, what do the initials M.D. really mean? … More Dough!
How much reserve do you have and where is it stashed?
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Understanding how economic behavior factors into health and health care decisions can benefit anyone interested in this field. However, the following groups of individuals may benefit most from the study of health economics:
Medical providers: Doctors, nurses, and assistants can evaluate new treatments, technologies, and services to determine ways to deliver value-based care. Medical providers benefit from understanding the economics behind these developments [MD/DO, DPM, DDS/DMD, RN, PA, etc].
Administrators: Health care administrators process insurance co-payments and manage financial metrics for health care providers. Learning the intricacies of health care economics can provide the necessary context as they liaise with insurance providers and use new technologies to process payments.
Policymakers or public health officials: Those who are in charge of policy decisions at the local, state, federal, or international levels benefit from understanding the economic relationship between stakeholders and the general public.
Business leaders: Because many Americans receive private insurance, health care becomes a major expense for employers. Business leaders must understand the health economics outlook to appease their employees, shareholders, and even their customers.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on February 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Optometry Doctor [OD]: An optometrist has an Optometry Doctor (OD) degree and can assess overall eye health and the quality of a person’s vision through a comprehensive examination. They diagnose and treat many eye disorders that do not require surgery or further specialized care. An optometrist can also identify symptoms of other health conditions that may affect the eyes, such as diabetes. Some also specialize in a field like pediatric care.
Optometrists [OD] and ophthalmologists [MD/DO] are both eye doctors, but they have different types of training and areas of expertise. If you need an eye exam—and think you may need glasses or contact lenses—an optometrist is a good first choice. To become an optometrist, a person needs to complete four years of additional education after a bachelor’s degree. Sometimes they complete a residency as well.
Now, ODs are licensed doctors and can prescribe medication. However, optometrists have a defined scope of practice that that revolves largely around the eyes. Optometrists can not prescribe all the same medications that your family doctor or ophthalmologist can.
So, if your eye issue requires surgery, or for specific conditions related to your eyes or overall health, you’ll want to visit an ophthalmologist [MD/DO].
On average, an optometrist in the U.S. makes about $131,860 per year, according to 2023 statistics.
Posted on February 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
PharmD – Doctor of Pharmacy
A Doctor of Pharmacy [ParrmD] is the professional degree required to become a pharmacist in the US. Practicing pharmacists complete an average of six years in school—including their pre-pharmacy education—before passing required exams and completing post-graduate training.
Here’s where things often get confusing. The word “pharmacist” is sometimes used in casual conversation to refer to healthcare professionals who aren’t technically licensed to be pharmacists.
For example, pharmacy technicians assist licensed pharmacists. They work behind the counter among the medications right alongside the pharmacist. However, they don’t need a Doctor of Pharmacy to do their job. A pharmaceutical sales representative typically needs four years of a bachelor’s degree with a foundation in chemistry and biology, though this is not always a requirement. Neither of these professionals is technically a pharmacist, although laypeople may mistakenly describe them that way.
And pursuing a PharmD doesn’t always mean you’ll work in a community pharmacy. In fact, just slightly fewer than half of all PharmD recipients end up in this role. Another 15 percent practice in other healthcare settings—hospitals, nursing homes, and managed care centers, for example. Other pharmacy students pursue research roles, government regulation positions, or work in highly specialized areas like oncology or geriatric pharmacy.
A PharmD or RPH [registered pharmacist] fills the electronic or written prescriptions of a MD/DO/DPM/DDS/DMD. They generally can not prescribe drugs or write prescriptions, however.
As of February 01, 2025, the average annual pay of Doctor of Pharmacy in the United States was $196,904. While Salary.com suggests that a Doctor of Pharmacy salary in the US can go up to $236,908 or down to $149,197, most earn between $171,932 and $217,844.
Posted on February 4, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
According to Wikipedia, the Flexner Report was a book-length landmark report of medical education in the United States and Canada, written by Abraham Flexner and published in 1910 under the aegis of the Carnegie Foundation. Flexner not only described the state of medical education in North America, but he also gave detailed descriptions of the medical schools that were operating at the time. He provided both criticisms and recommendations for improvements of medical education in the United States.
Many aspects of the present-day American medical profession stem from the Flexner Report and its aftermath. While it had many positive impacts on American medical education, the Flexner report has been criticized for introducing policies that encouraged systemic racism and sexism.
The Report, also called Carnegie Foundation Bulletin Number Four, called on American medical schools to enact higher admission and graduation standards, and to adhere strictly to the protocols of mainstream science principles in their teaching and research. The report talked about the need for revamping and centralizing medical institutions. Many American medical schools fell short of the standard advocated in the Flexner Report and, subsequent to its publication, nearly half of such schools merged or were closed outright.
Colleges for the education of the various forms of alternative medicine, such as electro-therapy were closed. Homeopathy, traditional osteopathy, eclectic medicine, and physiomedicalism (botanical therapies that had not been tested scientifically) were derided.
The Report also concluded that there were too many medical schools in the United States, and that too many doctors were being trained. A repercussion of the Flexner Report, resulting from the closure or consolidation of university training, was the closure of all but two black medical schools and the reversion of American universities to male-only admittance programs to accommodate a smaller admission pool.
In Chapter 11, Flexner stressed that the success of medical education reform and the professionalization of medicine relied heavily on the effective legal and ethical functioning of state medical boards. However, he noted that these boards were failing in their mission, stalling progress and allowing substandard medical practices to continue, thereby jeopardizing public health. This problem persists as a significant issue in the current practice of medicine in the United States.
MBBS Degree [Bachelor of Medicine, Bachelor of Surgery]
The MBBS is usually a five-year undergraduate degree that medical students complete when they want to become doctors. However, some programs take six years to complete because the institution expects you to earn a Bachelor of Science (BSc) in your training.
By the time a student applies to a medical program, they have likely taken several foundational science courses as part of their high school (or secondary) education. For example, medical applicants in the United Kingdom are often expected to show high scores on their General Certificate of Secondary Education (GCSE) and A-levels.
Earning an MBBS means that students are certified to care for patients as junior physicians without specialized training. Graduates are expected to complete two years of additional training, which rotates them through different specialties. Once they identify a specialty they like, they can apply for additional training, which can take anywhere between three and eight years.
MD Degree [Doctor of Medicine]
The acronym “MD” stands for the Latin term “Medicinae Doctor,” which translates to “Doctor of Medicine” in English.
It refers to the title that students from the United States of America obtain after finishing medical school. Some countries consider the “MD” title a postgraduate doctoral degree that MBBS graduates can obtain with additional years of training.
Posted on December 14, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Stocks ended the session little changed on Friday despite Broadcom’s (AVGO) jump to all-time highs driven by the chipmaker’s bullish AI-fueled sales forecast.
The S&P 500 (^GSPC) closed flat while the tech-heavy NASDAQ Composite (^IXIC) gained 0.1%. The Dow Jones Industrial Average (^DJI) slipped 0.1%
The fight between payers and anesthesiologists isn’t over, despite Anthem Blue Cross Blue Shield (BCBS) reversing plans for a policy that would put time limits on commercial claims for anesthesia coverage. The policy would have set a time limit for claims by procedure, with the exception of maternity and pediatric care, in New York, Connecticut, and Missouri starting next year. It called for providers “requiring more time than set or recommended by these standards” to undergo the insurance company’s claim dispute process in order to get paid, according to a statement Anthem provided to FOX61 in November.
The plan received backlash from everyone, from anesthesiologists to New York Governor Kathy Hochul.
Posted on September 4, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Fundamentals of Physician Investing
By Daniel B. Moisand CFP®, and ME-P staff
It used to be that the only way to get investments and investment information was through paying commissions to a traditional broker. Then in the 70’s (specifically, May, 1975) the brokerage industry went through significant deregulation allowing for the discounting of commissions. Charles Schwab and Company, among others, was able to eliminate the advice component and offer trades at dramatically reduced rates. The full service brokerage business responded by emphasizing the scope of their services namely research and advice in order to compete. The demand for both has continued to grow, even though research information is now readily available through many sources. These brokerage firms continue to thrive despite their poor performance in analyzing tech stocks and the Enron and Global Grossing debacles. More recent debacles in 2008-09, the flash crash a decade ago and more recent developments are legion, as well.
Fundamental Flaws
The fundamental flaw with these firms is the array of conflicts of interest between the firm and its customers. While the incentive to trade has been well chronicled as a conflict, these firms have not let consumer’s demand for a better-aligned compensation arrangement go unnoticed. Fee-based account relationships have proliferated accordingly. In theory, this type of arrangement, usually a percentage of assets, gives an incentive for performance and service rather than trade activity. This certainly has merit. However, conflicts remain that should be considered.
Pay to Play
The practice of paying brokers, higher levels of compensation for in-house products was commonplace. Today, explicitly higher payouts still exist but are less common. Instead, many firms use the sale of proprietary mutual funds and other products as part of management’s compensation. Other forms of non-monetary compensation such as a better office can be used as incentive for the brokers. The greater profitability of these in-house offerings will keep this conflict around for some time.
Subtle Conflicts of Interest
Less obvious is the conflict between the investment banking arm, the research department, and the retail brokerage operations of a firm. Even firms with no proprietary funds to sell may grapple with this issue. Here, research is pressured to say favorable things about a particular company’s stock by the investment bankers in hopes of obtaining more of that company’s business. When a firm brings a company public odds are great that a “strong buy” rating will come with the IPO. Of course, the lesson remains – consider the source.
Assessment
Traditional brokers have a somewhat higher standard of accountability than the on-line firms as to their accountability. If you buy the stock of a company that goes bankrupt through an on-line broker you have little recourse. After all, that was your choice. If a full-service broker recommended the stock to you, that broker will have to defend the recommendation.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Instead, physician assistants (PAs) and nurse practitioners (NPs) will increasingly provide primary care services, according to a report from consulting firm Mercer.
Almost every medical profession has its fair share of grossness and unbelievable moments. But, when it comes to podiatrists, you could argue that they have it extra bad for the simple reason that they specialize in feet. Most people would probably agree feet can be one of the human body’s most disgusting parts. People often neglect or ignore their feet, which can suffer badly from some common diseases and become a hotbed for unsanitary practices.
But, is a podiatrist really a physician?
You bet! Now, while the American Podiatric Medical Association [APMA] defines Doctor of Podiatric Medicine, or podiatrist, as “a physician and surgeon of the foot and ankle,” the The Social Security Administration’s Program Operations Manual System (POMS) legally defines a podiatrist as the following:
A podiatrist is a “physician” with respect to those functions which the podiatrist is legally authorized to perform in the State in which the individual performs them. Furthermore, the POMS states: A podiatrist is considered a “physician” for any of the following purposes: 1. for making the required physician certification and re-certifications of the medical necessity for Part A and Part B provider services. 2. for the purpose of establishing and periodically reviewing a home health plan of treatment; and for purposes of constituting a member of a Utilization Review (UR) committee but only if: a. the performance of these functions is consistent with the policy of the institution or agency with respect to which the podiatrist performs them; b. the podiatrist is legally authorized by the State to perform such functions; and c. at least two of the physicians on the Utilization Review committee are doctors of medicine or osteopathy.
In the United States, podiatrists are educated and licensed as Doctors of Podiatric Medicine (DPM). After a 4-year bachelor’s degree, the preparatory education of most podiatric physicians — similar to the paths of traditional physicians (MD or DO) — includes four years of undergraduate work, followed by four years in an accredited podiatric medical school, followed by a three or four year hospital-based residency program.
Optional one to two-year fellowships in foot and ankle reconstruction, surgical limb salvage, sports medicine, plastic surgery, pediatric foot and ankle surgery, and wound care is also available. Podiatric medical residencies and/ or fellowships are accredited by the Council on Podiatric Medical Education (CPME). The overall scope of podiatric practice varies from state to state with a common focus on foot and ankle surgery. Podiatrists work in hospitals, private practices and clinics, university medical centers and/or specialized practices.
Generally podiatrists can:
Perform physical examinations and study medical histories
Order and interpret X-rays and also other imaging studies like MRIs, and CAT scans.
Giving podiatric advice, second opinions and diagnosis
Administer drugs, narcotics, anesthetics and also sedation
Perform surgery related to the foot, ankle and legs
Perform plastic, macro and micro-surgeries and reconstructive bone surgeries
Prescribe medications such as narcotic pain killers, sleep aides and antibiotics
Perform certain physical and occupational therapies
Be on hospital staffs and take Emergency Room hospital call
Be on health insurance plans for covered physicians and medical providers
Prescribe, order, and fit prosthetics, casts, insoles, and orthotic devices
Attest to physical disability, write a doctor’s medical, treatment or absentee note, etc
In fact, the American Board of Podiatric Medicine [ABPM] offers a comprehensive qualification and certification process in podiatric medicine and orthopedics. Sub-specialties of podiatry include:
Posted on July 23, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
A report published by Becker’s Hospital Review highlights a large number of job elimination efforts that have been announced or already implemented across 66 hospitals, including the following:
As an organizational redesign measure, Oklahoma University (OU) Health has eliminated around 100 positions.
200 healthcare jobs were cut by Oklahoma City-based Integris Health to curb expenses.
ProMedica in Toledo, Ohio, announced plans to lay off 262 employees in March.
337 employees of New York City-based Memorial Sloan Kettering Cancer Center are likely to be laid off shortly.
112 employees of Pikeville Medical Center in Kentucky were laid-off at the end of 2022.
Desert Springs Hospital Medical Center in Las Vegas has already notified its workers that 970 jobs will be lost as it transitions to an emergency department.
California-based Kaweah Health in Visalia is likely to eliminate 94 positions.
These healthcare worker layoffs only reveal a part of the crisis because the complete closure of numerous hospitals is also on the horizon.
While the closure rate is faster for rural hospitals, urban hospitals are not safe either. In November 2022, Atlanta Medical Center (AMC) in Atlanta Georgia, announced its closure, leaving hundreds of workers jobless. This closure also had a severe adverse impact on the availability of trauma care in Atlanta. In 2019, the city council in Washington D.C. voted in favor of closing United Medical Center prior to COVID, leaving a healthcare gap during the pandemic.
NOTE:The current trend of hospital closures and healthcare job cuts not only affects the healthcare workers and their families but also poses serious questions about the quality of healthcare in the country. Last year, McKinsey & Company predicted that by the end of 2025, the US healthcare system may face a shortage of up to 450,000 registered nurses [RNs].
Posted on June 17, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
Battle of the Allopathic Vs. Osteopathic Physicians
By Dr. David Edward Marcinko MBA
***
***
What’s the difference between an MD and a DO?
An MD is a Doctor of Medicine, while a DO is a Doctor of Osteopathic Medicine. The bottom line? They do the same job, have similar schooling, can prescribe medication and can practice all over the U.S.
“In general, DOs practice a more holistic, whole-person type of care,” explains Dr. Vyas. “MDs take a more allopathic, or illness-based, approach.”
Allopathic and osteopathic medicine differ in several ways:
Allopathic medicine uses medication, surgery and other interventions to treat illnesses.
Osteopathic medicine emphasizes the relationship between the mind, body and spirit. It focuses on treating the person as a whole and improving wellness through education and prevention. DOs also receive extra training in osteopathic manipulative medicine (OMM), a hands-on method for diagnosing and treating patients.
But these philosophical differences don’t necessarily define the way DOs and MDs practice medicine. For example, DOs use all types of modern medical treatments, and MDs provide whole-person and preventive care.
***
***
What’s in a Medical Degree?
Allopathic and Osteopathic medical schools have similar curriculum structures. Students spend 12–24 months of their program in the classroom and then continue training in clinical settings, according to the American Medical Association (AMA).
Posted on March 25, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Eye doctors can track changes in your vision, as well as detect abnormalities in the retinas and lenses of the eyeball. If your eyes are reddened and itchy and the issue is not resolved with over-the-counter eye drops, make sure you see a doctor to eliminate the possibility of an eye infection.
VISION RULE: Here’s your reminder to practice the 20-20-20 rule: Every 20 minutes, take a 20-second break from your screen and look at something 20 feet away.
Posted on March 22, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
According to HealthcareBrew, thousands of doctors are expected to reach retirement age in the next three years, and their replacements won’t be physicians. Instead, physician assistants (PAs) and nurse practitioners (NPs) will increasingly provide primary care services, according to a report from consulting firm Mercer.
By 2026, 21% of family medicine, pediatric, and obstetrics and gynecology physicians—or about 32,000 doctors—will be 65 or older, and Mercer anticipates about 23,000 physicians will leave the profession permanently. At the same time, demand for primary care physicians is expected to grow 4%, the report found.
PAs and NPs—also called advanced practice providers (APPs) or physician extenders—are highly trained medical professionals. To become a PA, you have to have both a bachelor’s and a master’s, some clinical work experience, pass the Physician Assistant National Certifying Exam, and then apply to get licensed in your state (you know, easy peasy). It takes seven to nine years to go through that process, compared to 11+ years to become an MD.
To become an NP, you must have both a bachelor’s and a master’s in nursing, become a registered nurse, and pass a national NP board certification exam. It takes between six to eight years to become an NP.
Compared to physicians, PAs and NPs are “considerably younger professions with less than half the retirement risk,” the Mercer report stated. Roughly 40,000 PAs and NPs join the workforce annually.
“We’re certainly going to see increasing demand for APPs,” David Mitchell, a partner in Mercer’s career consulting business and a specialist in the healthcare industry, told Healthcare Brew.
While most state licensing boards require a physician to oversee APPs, both PAs and NPs have the authority to do many services primary care physicians do, like seeing and diagnosing patients, ordering lab tests, and writing prescriptions, said Mitchell.
Posted on May 13, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Jules Lipoff, MD: Senior fellow at the Leonard Davis Institute of Health Economics and an assistant professor of clinical dermatology at Perelman School of Medicine, both of the University of Pennsylvania. Erica Mark, medical student at the University of Virginia, contributed to this article.The opinions expressed in this article do not necessarily represent those of the University of Pennsylvania Health System or the Perelman School of Medicine.
***
If you follow the news or your social media feed, you know that crowdsourcing medical expenses is increasingly popular for financing health care costs. In fact, you might have contributed to one; 22 percent of American adults report donating to GoFundMe medical campaigns.
As of 2021, approximately $650 million, or about one-third of all funds raised by GoFundMe, went to medical campaigns. That staggering amount of money highlights how dysfunctional our health care system is, forcing people to resort to crowdsourcing to afford their medical care — but it’s not surprising. In the United States, 62 percent of bankruptcies are related to medical costs. This should be a wake-up call to address and reform the system further.
The mission of AJPH is to advance public health research, policy, practice and education. Toward that goal, the journal also produces monthly podcasts available in English, Spanish and Chinese at ajph.org. The monthly podcasts also are on iTunes and Google Play.
The mission of the journal is to advance public health research, policy, practice and education. Toward that goal, the journal also produces monthly podcasts in English, Spanish and Chinese.
















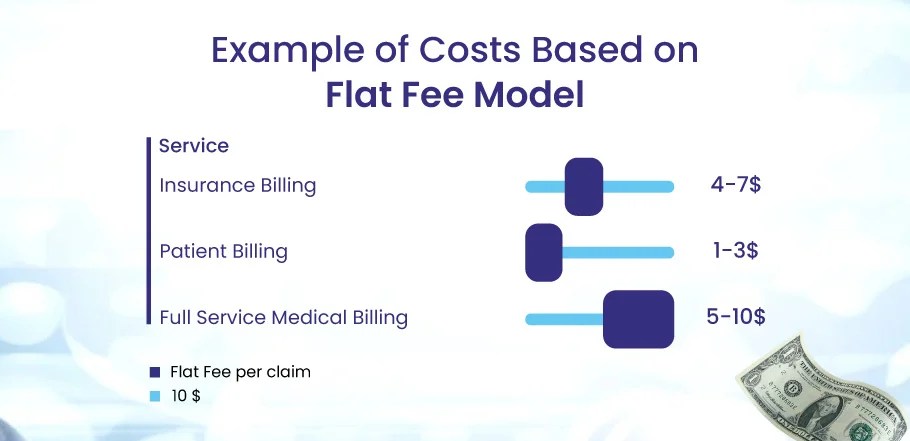

















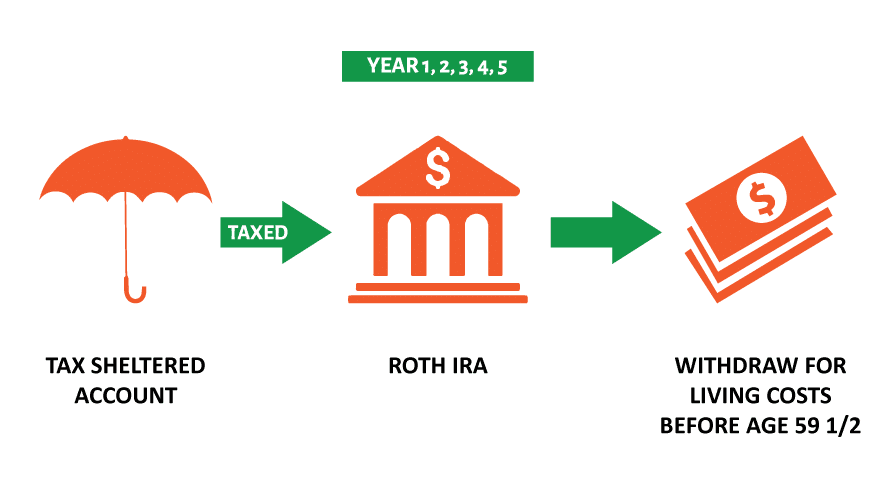

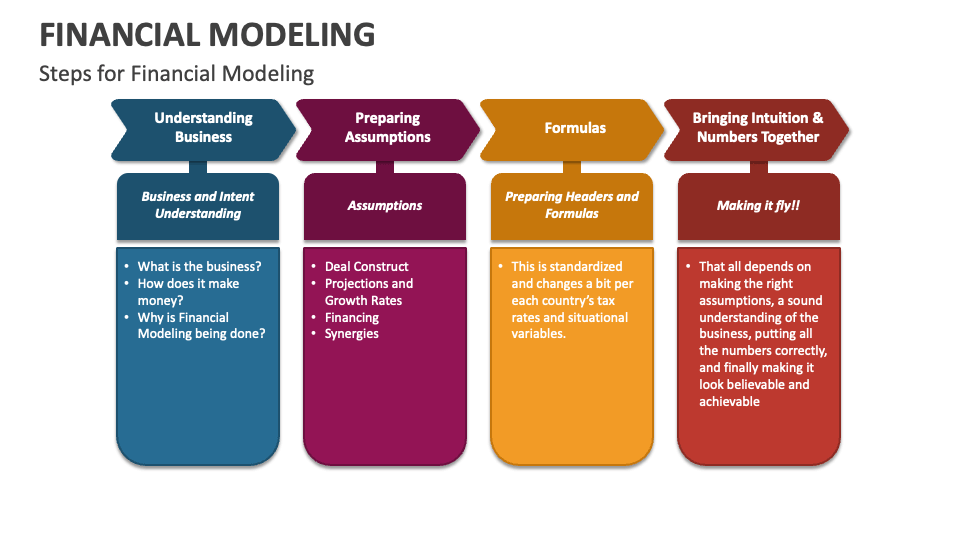

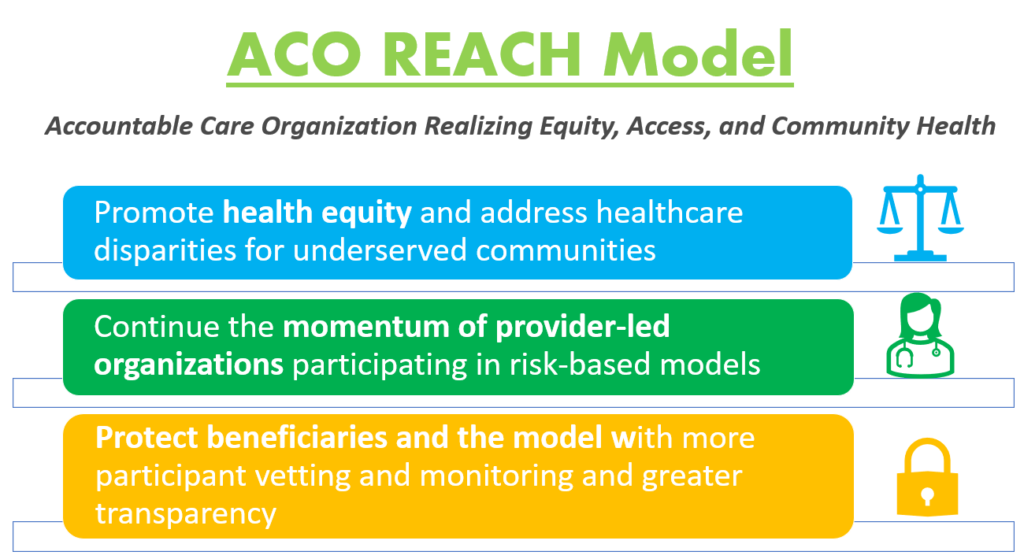












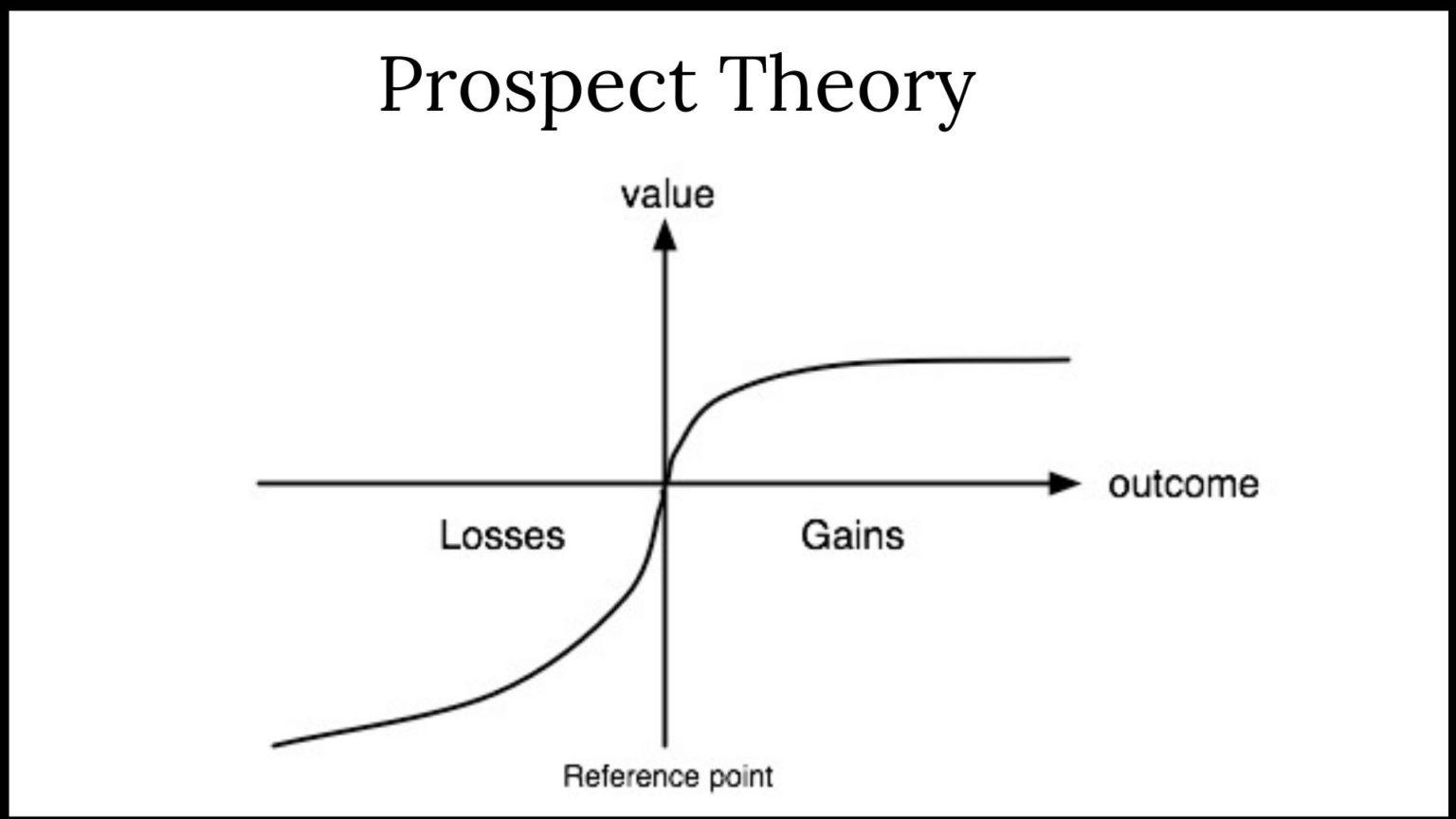






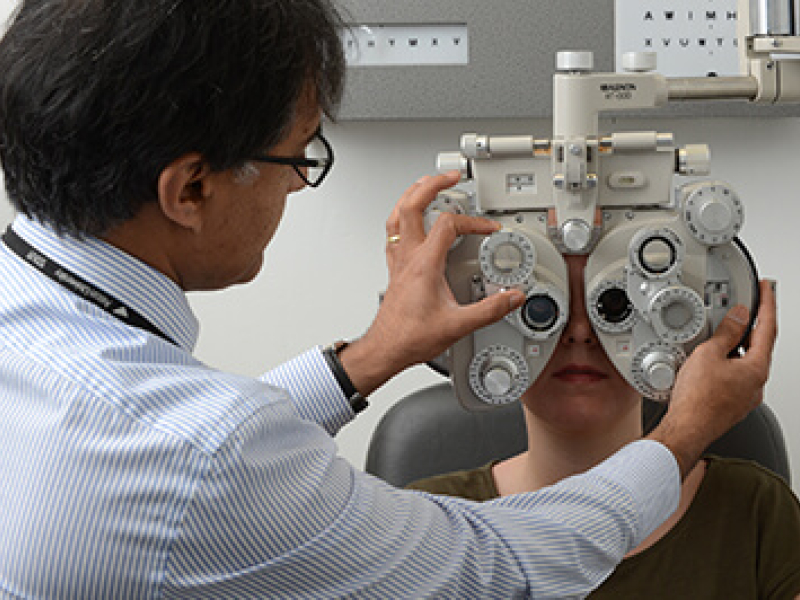







































STUPID COMMENTS: Financial Advisors Say to Physician Clients
BY DR. DAVID EDWARD MARCINKO; MBA MEd CMP®
***
***
SPONSOR: http://www.MarcinkoAssociates.com
***
Some Stupid Things Financial Advisors Say to Physician Clients
A few years ago and just for giggles, colleague Lon Jefferies MBA CFP® and I collected a list of dumb-stupid things said by some Financial Advisors to their doctor, dentist, nurse and and other medical professional clients, along with some recommended under-breath rejoinders:
So, don’t let these aphorisms blind you to the critical thinking skills you learned in college, honed in medical school and apply every day in life.
COMMENTS APPRECIATED
Refer, Like and Subscribe
***
EDUCATION: Books
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
***
***
Share this:
Filed under: "Advisors Only", "Doctors Only", Ethics, Jokes and Puns, LifeStyle | Tagged: bears, bulls, crypto, DO, doctor clients, DPM, dumb comments, finance, financial advisors, financial planners, Investing, Lon Jefferies, Marcinko, MD, personal-finance, Physician Clients, physicians, Ponzi, stocks, stupid comments, Wall Street | Leave a comment »