

Medical Executive-Post Staff
***

Share this:

Filed under: LifeStyle, Op-Editorials | Tagged: 2025, happy thanksgiving, thanksgiving | Leave a comment »
ME-P SYNDICATIONS:
WSJ.com,
CNN.com,
Forbes.com,
WashingtonPost.com,
BusinessWeek.com,
USNews.com, Reuters.com,
TimeWarnerCable.com,
e-How.com,
News Alloy.com,
and Congress.org

![]()
![]()



BOARD CERTIFICATION EXAM STUDY GUIDES
Lower Extremity Trauma
[Click on Image to Enlarge]
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] E-mail: MarcinkoAdvisors1738@outlook.com
![]()


 ePodiatryConsentForms.com
ePodiatryConsentForms.com
 “Providing Management, Financial and Business Solutions for Modernity”
“Providing Management, Financial and Business Solutions for Modernity”


Medical Executive-Post Staff
***
Filed under: LifeStyle, Op-Editorials | Tagged: 2025, happy thanksgiving, thanksgiving | Leave a comment »
Turn Financial A-Ha Moments Into Lasting Change With Memory Re-Consolidation
By Rick Kahler MSFS CFP™
***
***
Have you ever had a light bulb moment about money?
Maybe you leave a workshop, a therapy session, or a conversation with a financial advisor, feeling as if you have finally cracked the code. You understand why you keep overspending. You see the pattern that keeps you procrastinating about saving and investing. You feel the reason you panic about money, even when you know you are okay. In that moment, it all seems so clear.
Yet a week later, you are right back at it. Swiping the credit card. Avoiding the budget. Losing sleep over the same worries you thought you had just solved. What happened to that breakthrough? Why did it not last?
BRAIN ANCHORING: https://medicalexecutivepost.com/2024/10/22/anchoring-initial-mental-brain-trickery/
I’ve experienced this myself, more times than I’d like to admit. Recently, I found a book that explains why: Unlocking the Emotional Brain by Bruce Ecker, Robin Ticic, and Laurel Hulley. The authors explain that lasting change happens through something called “memory re-consolidation.” It is the brain’s way of updating emotional patterns we have carried for years—often since childhood.
Most of us have old money stories tucked away in our emotional memory. Suppose, for example, as a child you were scolded for asking a neighbor how much money they earned. This and other similar experiences that left you feeling shamed or dismissed taught you that it was rude to talk about money.
Such early experiences are filed away as emotional truths. They shape what feels true, even years later as an adult, whether or not that “truth” is still relevant.
NEUROLINK: https://medicalexecutivepost.com/2023/03/07/neurolink-brain-chips-rejected-by-the-fda/
As an adult, you may have come to understand that talking about money is often essential for your emotional and financial well being. But when the moment comes to have a money conversation, your body still freezes up. That is not weakness. That is your brain pulling up the old file.
Here is where memory re-consolidation comes in. The brain does not update the file just because you think new thoughts. It updates when you have a new experience that feels different. Maybe someone listens without judgment, or you realize you are talking about money and still feel safe. That emotional mismatch tells the brain, “Maybe this file is not true anymore.”
But the update is not finished. To make the change stick, you have to hold both the old belief and the new experience together for a little while. It is like showing your brain two pictures: here is how it used to feel, and here is how it feels now. That moment of holding both is when the rewrite happens.
Even more interesting, the brain keeps the file open for several hours after the shift. What you do in that window can help the change settle in—or not. If you rush back into busyness or distractions, you might accidentally let the old version save itself again.
BRAIN HEALTH: https://medicalexecutivepost.com/2025/02/19/brain-health-bilingualism/
So what can we do to give those shifts a better chance of sticking? I have noticed that insights gained during a retreat or workshop, with ample time to focus and reflect, are more likely to last. Even in our everyday lives, we can slow down, even for a few minutes, to write about what we felt, check in with our bodies, or talk with someone who supports us. We can protect a little bit of quiet space before diving back into the noise.
The next time you have a money breakthrough, try giving yourself that space. Consciously notice both the old belief and the new experience. Give the re-consolidation time to settle in.
Then, the next time your brain pulls up that old money story, you’ll have access to the updated, more accurate version.
COMMENTS APPRECIATED
Like and Refer
***
***
Filed under: "Ask-an-Advisor", Ethics, Experts Invited, Financial Planning, Investing, mental health, Op-Editorials, Portfolio Management | Tagged: A-HA moment, brain, brain anchoring, brain health, Bruce Ecker, CFP, emotional brain, Ethics, financial advisor, light bulb moment, Lurel Hulley, mental health, money, money stories, neurolink, old money, rick kahler, Robin Ticic | Leave a comment »
By Brian J. Knabe MD, Certified Medical Planner
Historically, the term “risk management” has brought to mind one subject for the practicing physician – medical malpractice. Unfortunately, physicians today face a multitude of other risks which may be more insidious and daunting than malpractice. It is important to recognize these risks, and to have the appropriate procedures and policies in place to mitigate the risks. These risks come from the federal government, state government, insurance companies, patients, employees, and even prospective employees. Some risks, many unique to small businesses and medical practices, include the following:
The practicing physician should seek the advice of professionals with expertise in these areas. Every practice should have an experienced attorney on retainer. It is very important to seek advice from fiduciaries – experts who have no conflicts of interest and who can therefore act in the best interest of the client. A Certified Medical Planner is such a fiduciary with training and expertise in these areas.
http://www.CertifiedMedicalPlanner.org
It can be particularly challenging to find an insurance advisor with no conflicts of interest, as this industry is built upon product sales and commissions. One such insurance advisor is Scott Witt, a fee-only insurance advisor with Witt Actuarial Services (www.wittactuarialservices.com).
Others can be found with an internet search for “fee only insurance advisor”.
Conclusion
Your comments on this ME-P are appreciated. How do you select an advisor? Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Sponsors Welcomed: And, credible sponsors and like-minded advertisers are always welcomed.
Link: https://healthcarefinancials.wordpress.com/2007/11/11/advertise
![]()
***
Filed under: CMP Program, Experts Invited, Op-Editorials, Practice Management, Risk Management | Tagged: brian knabe, CMS, DOJ, financial advisors, FTC, HHS, HIPAA, insurance agents, Marcinko, medicare, Medicare compliance, National Association of Personal Financial Advisors, OSHA, RICO, www.certifiedmedicalplanner.com | Leave a comment »
Micro-Credentials on the Rise
KNOWLEDGE RICHES IN SPECIALTY NICHES
DR. DAVID EDWARD MARCINKO MBA MEd CMP™
SPONSOR: http://www.CertifiedMedicalPlanner.org
***

***
Do you ever wish you could acquire specific information for your career activities without having to complete a university Master’s Degree or finish our entire Certified Medical Planner™ professional designation program? Well, Micro-Certifications from the Institute of Medical Business Advisors, Inc., might be the answer. Read on to learn how our three Micro-Certifications offer new opportunities for professional growth in the medical practice, business management, health economics and financial planning, investing and advisory space for physicians, nurses and healthcare professionals.
Stock-Brokers, Financial Advisors, Investment Advisors, Accountants, Consultants, Financial Analyists and Financial Planners need to enhance their knowledge skills to better serve the changing and challenging healthcare professional ecosystem. But, it can be difficult to learn and demonstrate mastery of these new skills to employers, clients, physicians or medical prospects. This makes professional advancement difficult. That’s where Micro-Certification and Micro-Credentialing enters the online educational space. It is the process of earning a Micro-Certification, which is like a mini-degree or mini-credential, in a very specific topical area.
Once you’ve completed all of the requirements for our Micro-Certification, you will be awarded proof that you’ve earned it. This might take the form of a paper or digital certificate, which may be a hard document or electronic image, transcript, file, or other official evidence that you’ve completed the necessary work.
Micro-Certifications may be used to demonstrate to physicians prospective medical clients that you’ve mastered a certain knowledge set. Because of this, Micro-Certifications are useful for those financial service professionals seeking medical clients, employment or career advancement opportunities.
Here are the three most popular Micro-Certification course from the Institute of Medical Business Advisors, Inc:
Other Topics include: economics, finance, investing, marketing, advertising, sales, start-ups, business plan creation, financial planning and entrepreneurship, etc.
Now that you’re familiar with Micro-Credentialing, you might consider earning a Micro-Certification with us. We offer 3 official Micro-Certificates by completing a one month online course, with a live instructor consisting of twelve asynchronous lessons/online classes [3/wk X 4/weeks = 12 classes]. The earned official completion certificate can be used to demonstrate mastery of a specific skill set and shared with current or future employers, current clients or medical niche financial advisory prospects.
Mini-Certification Tuition, Books and Related Fees
The tuition for each Mini-Certification live online course is $1,250 with the purchase of one required dictionary handbook. Other additional guides, white-papers, videos, files and e-content are all supplied without charge. Alternative courses may be developed in the future subject to demand and may change without notice.
***
Contact: For more information, or to speak with an academic representative, please contact Ann Miller RN MHA CMP™ at Email: MarcinkoAdvisors@msn.com [24/7].
***

Filed under: "Advisors Only", "Ask-an-Advisor", Book Reviews, Career Development, CMP Program, Experts Invited, Financial Planning, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Information Technology, Investing, Op-Editorials, Touring with Marcinko | Tagged: accountants, certifications, certified medical planner, CMP, financial advisors, financial planners, investment advisors, Marcinko, micro, micro-certifications, micro-credentials | Leave a comment »
By Staff Reporters
Is the Doctor – In?
SPONSOR: http://www.CertifiedMedicalPlanner.org
INFO-GRAPHIC
***

***
Doctorate, or doctoral, is an umbrella term for many degrees — PhD among them — at the height of the academic ladder. Doctorate degrees fall under two categories, and here is where the confusion often lies.
The first category, Research (also referred to as Academic) includes, among others:
The second category, Applied (also referred to as Professional) includes, among others:
As you can see, applied doctorates are generally paired with very specific careers – medical doctors, podiatrists, dentists, optometrists, psychologists, and law professionals.
When it comes to outlining the differences between a PhD and doctorate, the real question should be, “What is the difference between a PhD and an applied doctorate?” The answer, again, can be found in the program outcomes. The online Doctor of Psychology at UAGC, for example, lists outcomes that are heavily focused on the ability to put theory into practice in a professional setting. For example:
Bottom line: As the PhD is more academic, research-focused, and heavy on theory, an applied doctorate degree is intended to master a subject in both theory and practice.
The debate over whether a PhD graduate should be called a doctor has existed for decades, and if you’re a member of this exclusive club, you’ll no doubt hear both sides of the argument during your lifetime. After all, if a PhD is a doctor, can a person with a doctoral degree in music – the Doctor of Musical Arts (DMA) – be called a doctor as well?
Those in favor argue that having “Dr.” attached to your name indicates that you are an expert and should be held in higher regard. For some, the debate is at the heart of modern gender disparity. For example, on social media and in some academic circles, there is an argument that female PhD holders should use the “Dr.” title in order to reject the notion that women are less worthy of adding the title to their name once they have earned a doctoral degree.
The American Psychological Association has, for years, challenged the Associated Press (AP) and other news outlets to broaden its use of “Dr.” beyond those that practice medicine – MDs, podiatrists, dentists, etc. – in its reporting. However, the organization was rebuked, as the AP argued that, “It comes down to a basic distinction. Psychologists earn PhDs, and AP style allows the ‘Dr.’ title only for those with medical degrees.”
The AP has, thus far, refused to change their style guide when it comes to the “doctor question.”
COMMENTS APPRECIATED
Refer and Subscribe
***

***
Filed under: "Doctors Only", Career Development, CMP Program, Experts Invited, Glossary Terms, iMBA, Inc., Op-Editorials, Professional Liability, Quality Initiatives | Tagged: American Psychological Association, AP, APA, Associated Press, CMP, DBA, DCS, DDS, DMA, DMD, DNP, DNSc, DO, doctor, DPM, DSc, EdD, education, EngD, higher-education, JD, MD, MEd, news, OD, PhD, Psy.D, research, ThD, UAGC | Leave a comment »
FOR ETHICAL PHYSICIAN CLIENT ACQUISITION SUCCESS
By Dr. David Edward Marcinko; MBA MEd CMP™
***
***
SPONSOR: http://www.CertifiedMedicalPlanner.org
Critical thinking allows a Financial Advisor [FA] to analyze information and make an objective judgment. By impartially evaluating the facts related to a matter, Financial Planners [FPs] can draw realistic conclusions that will help make a sound decision. The ability of being able to properly analyze a situation and come up with a logical and reasonable conclusion is highly valued by employers, as well as current and potential clients.
Now, according to Indeed, we present the six main critical thinking and examples that will help you evaluate your own thought process as a FA, FP or Wealth Manager, etc.
What is critical thinking?
Critical thinking is the ability to objectively analyze information and draw a rational conclusion. It involves gathering information on a subject and determining which pieces of information apply to the subject and which don’t, based on deductive reasoning. The ability to think critically helps people in both their personal and professional lives and is valued by most clients and employers.
Critical thinking skills are a valuable asset for an employee, as employers, brokerages and Registered Investment Advisors [RIAs] typically appreciate candidates who can correctly assess a situation and come up with a logical resolution. Time is a valuable resource for most managers, and an employee able to make correct decisions without supervision will save both that manager and the whole company much valuable time.
***
***
There are six main critical thinking skills you can develop to successfully analyze facts and situations and come up with logical conclusions:
Being able to properly analyze information is the most important aspect of critical thinking. This implies gathering information and interpreting it, but also skeptically evaluating data. When researching a work topic, analytical thinking helps you separate the information that applies to your situation from that which doesn’t.
Whether you are gathering information or convincing others that your conclusions are correct, good communication is crucial in the process. Asking people to share their ideas and information with you and showing your critical thinking can help step further towards success. If you’re making a work-related decision, proper communication with your coworkers can help you gather the information you need to make the right choice.
Being able to discover certain patterns of information and make abstract connections between seemingly unrelated data helps improve your critical thinking. When analyzing a work procedure or process, you can creatively come up with ways to make it faster and more efficient. Creativity is a skill that can be strengthened over time and is valuable in every position, experience level and industry.
Previous education and life experiences leave their mark on a person’s ability to objectively evaluate certain situations. By acknowledging these biases, you can improve your critical thinking and overall decision process. For example, if you plan to conduct a meeting in a certain way and your firm suggests using a different strategy, you should let them speak and adjust your approach based on their input.
The ability to correctly analyze a problem and work on implementing a solution is another valuable skill.
In both private and professional situations, asking the right questions is a crucial step in formulating correct conclusions. Questions can be categorized in various forms as mentioned below:
***
***
Asking open-ended questions can help the person you’re communicating with provide you with relevant and necessary information. These are questions that don’t allow a simple “yes” or “no” as an answer, requiring the respondent to elaborate on the answer.
When you feel like another person’s experience and skills could help you work more effectively, consider asking outcome-based questions. Asking someone how they would act in a certain hypothetical situation, such as a stock market correction, can give you an insight into their perspective, helping you see things you hadn’t thought about before.
You can gain insight by asking a client to reflect and evaluate an experience and explain their thought processes during that time. This can help you develop your critical thinking by providing you real-world examples.
An easy way to understand something is to ask how something works. Any working system results from a long process of trial and error, and properly understanding the steps that needed to be taken for a positive result could help you be more efficient in your own endeavors.
CONCLUSION
Critical thinking is like a muscle that can be exercised and built over time. It is a skill that can help propel your career to new heights. You’ll be able to solve workplace issues, use trial and error to troubleshoot ideas, and more.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
COMMENTS APPRECIATED
Read, Subscribe, Like and Refer
***
***
Filed under: "Advisors Only", "Ask-an-Advisor", Career Development, CMP Program, Experts Invited, Financial Planning, Investing, Managed Care, Marcinko Associates, Marketing & Advertising, Op-Editorials, Sponsors | Tagged: CFPs, creative thinking, critical thinking skills, decision-making, education, FAs, financial advisors, financial planners, FPs, indeed, learning, life, Marcinko, problems, questions, RIA, thinking, what, when, why | Leave a comment »
 By Dr. David Edward Marcinko MBA MEd CMP®
By Dr. David Edward Marcinko MBA MEd CMP®
SPONSOR: http://www.CertifiedMedicalPlanner.org
Definition
Population health has been defined as “the health outcomes of a group of individuals, including the distribution of such outcomes within the group”. It is an approach to health that aims to improve the health of an entire human population or cohort. http://www.HealthDictionarySeries.org
History
In fact, the nominal “father of population health” is colleague and Dean David B. Nash MD MBA of Jefferson Medical School in Philadelphia. And, although I attended Temple University down the street, David still wrote the Foreword to my textbook years later; Financial Management Strategies for Hospitals and Healthcare Organizations [Tools, Techniques, Checklists and Case Studies].
Factors
Now age, income, location, race, gender and education are just a few characteristics that differentiate the world’s population. These are called ”disparities” and they have a major impact on people’s lives; especially their healthcare. And, I’ve written about them before. Perform a ME-P “search” for more.
So, it’s only natural that we’re keeping an eye on two major demographic trends: aging baby boomers and maturing Millennials [1982-2002 approximately].
Why it’s important
The impact of large population shifts propagate throughout an economy benefitting certain sectors more than others and influencing a country’s growth prospects; tantalizing investing ideas?
Example:
For example, as baby boomers retire, we’ll likely see higher spending on health care, but less on education and raising children. Likewise, tech-savvy Millennials will likely prioritize consumption on experiences over cars and houses [leading economic indicator].
So, can we profit from these trends?

Assessment
Well maybe – maybe not! Overall economic prospects may not be completely affected by these trends. Spending habits on combined goods and services will shift, rather than rise or decline.
So, be careful. What matters most for your investment success is your demographics and investing according to your personal circumstances and goals [paradox-of-thrift].
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
***
Filed under: Glossary Terms, Health Economics, Investing, Op-Editorials, Touring with Marcinko | Tagged: David B. Nash MD, David Edward Marcinko, economic disparities, Healthcare Disparities, Investing, paradox of thrift, Population Health | Leave a comment »
Doctor of Medicine
Doctor of Osteopathic Medicine
Doctor of Podiatric Medicine
By Staff Reporters and APMA
***

***
APMA INFOGRAPHIC: https://www.apma.org/apmamain/document-server/?cfp=/apmamain/assets/file/public/about/physician-education-comparison-fact-sheet.pdf
COMMENTS APPRECIATED
Like, Refer and Subscribe
***
***
Filed under: Ask a Doctor, Experts Invited, Health Economics, Health Insurance, Health Law & Policy, Op-Editorials | Tagged: APMA, DO, do education, doctor education, DPM, dpm education, MD, md education, medical education osteopathic education, osteopath, osteopathic education, physician, podiatrist, podiatry | Leave a comment »
U.S. Department for Health & Human Services & Centers for Medicare & Medicaid Services
By Health Capital Consultants, LLC
***

***
On August 21, 2025, the U.S. Department for Health & Human Services (HHS) and the Centers for Medicare & Medicaid Services (CMS) announced the formation of a new Healthcare Advisory Committee.
The Committee is expected to be comprised of a group of experts who will make strategic recommendations to HHS Secretary Robert F. Kennedy Jr. and CMS Administrator Dr. Mehmet Oz.
This Health Capital Topics article discusses this announcement and potential implications on the healthcare industry. (Read more…)
COMMENTS APPRECIATED
Subscribe, Refer and Like
***
***
Filed under: "Ask-an-Advisor", Experts Invited, Health Economics, Health Law & Policy, Healthcare Finance, Op-Editorials | Tagged: CMS, Health Capital Consultants, Healthcare Advisory Committee., HHS, Jessica Bailey-Wheaton, Mehmet Oz, Robert Kennedy, TODD A. ZIGRANG | Leave a comment »
By Dr. David Edward Marcinko MBA MEd
***
***
Medicine today is vastly different than a generation ago, and all health care professionals need new skills to be successful and reduce the emerging risks outlined in this textbook, as well as the “unknown-unknowns” elsewhere. Traditionally, the physician was viewed as the “captain of the ship”. Today, their role may be more akin to a ship’s navigator, using clinical, teaching skills and knowledge to chart the patient’s course through a confusing morass of insurance requirements, fees, choices, rules and regulations to achieve the best attainable clinical outcomes.
This new leadership paradigm includes many classic business school principles, now modified to fit the decade long PP-ACA, the era of health reform, and modern technical connectivity and EMRs.
LEADERSHIP: https://medicalexecutivepost.com/2023/04/14/what-is-a-leadership-and-can-it-be-defined/
Thus, the physician must be a subtle guide on the side; not bombastic sage on the stage. These, newer health 3.0 leadership philosophies might include:
•Negotiation – working to optimize appropriate treatment plans; ie., quality of life versus quantity of life,
•Team play – working in concert with other allied healthcare professionals to coordinate care delivery ,ithin a clinically appropriate and cost-effective framework;
•Working within the limits of competence – avoiding the pitfalls of the medical generalist versus the specialist that may restrict access to treatment, medications, physicians and facilities by clearly acknowledging when a higher degree of service is needed on behalf of the patient – all while embracing holistic primary care;
•Respecting different cultures and values – inherent in the support of the medical Principle of Autonomy is the acceptance of values that may differ from one’s own. As the US becomes more culturally hetero geneous, medical providers are called upon to work within, and respect, the socio-cultural and/or spiritual framework of patients, students and their families;
•Seeking clarity on what constitutes marginal care – within a system of finite resources; providers are called upon to openly communicate with patients regarding access to marginal medical information and/or treatments.
•Supporting evidence-based practice – healthcare providers, should utilize outcomes data to reduce variation in treatments to achieve higher efficiencies and improved care delivery thru evidence based medicine [EBM];
•Fostering transparency and openness in communications – healthcare professionals should be willing, and prepared, to discuss all aspects of care, especially when discussing end-of-life issues or when problems arise;
•Exercising decision-making flexibility – treatment algorithms, templates and clinical pathways are useful tools when used within their scope; but providers must have the authority to adjust the plan if circumstances warrant.
HEALTHCARE LEADERSHIP: https://medicalexecutivepost.com/2025/05/01/healthcare-leadership-on-the-brink-executives-eyeing-the-exits/
Assessment
Becoming skilled in the art of listening and interpreting — In her ground-breaking book, Narrative Ethics: Honoring the Stories of Illness, Rita Charon, MD PhD, a professor at Columbia University, writes of the extraordinary value of using the patient’s personal story in the treatment plan. She notes that, “medicine practiced with narrative competence will more ably recognize patients and diseases; convey knowledge and regard, join humbly with colleagues, and accompany patients and their families through ordeals of illness.” In many ways, attention to narrative returns medicine full circle to the compassionate and caring foundations of the patient-physician relationship.
These thoughts represent only a handful of examples to illustrate the myriad of new skills that tomorrows’ healthcare professionals must master in order to meet their timeless professional obligations of compassionate care and contemporary treatment effectiveness; all within the context modern risk management principles.
BRAND MANAGEMENT: https://medicalexecutivepost.com/2025/07/07/brand-management-7-approaches-for-doctors-and-financial-advisors/
COMMENTS APPRECIATED
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR- http://www.MarcinkoAssociates.com
Like and Subscribe
***
***
Filed under: Ask a Doctor, Career Development, Health Law & Policy, Managed Care, Management, Marcinko Associates, mental health, Op-Editorials, Practice Management | Tagged: AI, Columbia University, david marcinko, EBM, EHRs, EMRs, health, healthcare, leadership skills, Management, medicine, mental health, physicians, PP-ACA, Rita Charon MD, Technology | Leave a comment »
BY DR. DAVID EDWARD MARCINKO, MBA MEd CMP®
***
SPONSOR: http://www.MarcinkoAssociates.com
ORGANIZATIONAL BEHAVIOR AND CLASSIFICATION OF RISKS
DEFINITION EMOTIONAL INTELLIGENCE: Emotional intelligence [EI] refers to the ability to identify and manage one’s own emotions, as well as the emotions of others. Emotional intelligence is generally said to include a few skills: namely emotional awareness, or the ability to identify and name one’s own emotions; the ability to harness those emotions and apply them to tasks like thinking and problem solving; and the ability to manage emotions, which includes both regulating one’s own emotions when necessary and helping others to do the same.
DEFINITIONAL ORGANIZATIONAL BEHAVIOR: Organizational behavior (OB) is the study of how individuals, groups, and organizations interact and influence one another. Though it is largely used within the field of business management as means to understand–and more effectively manage–groups of people. The reason businesses look to OB is because it can help organizations increase employee performance, while also creating a positive working environment.
CITE: Eugene Schmuckler; PhD MBA MEd CTS®
***
***
And so, as we review the concept of Emotional Intelligence and Organizational Behavior, it is possible to set up five EI/OB risk classes, based on the economic consequences of the occurrence of specific individual risks:
1. Prevented risks: Risks whose cost of occurrence is higher than their cost of management and whose occurrence may invoke additional legal sanctions. This class would include intentional torts and injuries caused by gross negligence.
2. Normally prevented risks: Risks whose cost of occurrence is greater than the cost of their management but whose occurrence will be considered only as negligent. This class includes most negligent injuries
and most types of product liability actions.
3. Managed risks: Risks whose cost of occurrence is only slightly greater than their cost of management. The plaintiff usually has the burden of showing that the defendant owed the plaintiff a special duty to recover for one of these risks.
4. Un-Prevented risks: Risks whose cost of occurrence is less than their cost of management. The classic example of this class is the cost of railroad crossing barriers compared to the cost of people being hit by
trains.
5. Un-Preventable risks: Risks whose occurrence is unmanageable. The assignment of a risk to one of these classes is a major problem in medical and healthcare quality control, because the class of a risk determines how much effort must be expended to prevent the risk. The misclassification of a prevented or normally prevented risk as a managed or un-prevented risk can result in large financial losses.
***

For example: A medical clinic that does not update obsolete equipment, such as inaccurate oxygen monitors, would be liable for any injuries attributable to the obsolete equipment. The classifications of risk must be reviewed periodically to determine if the cost of the risk-taking behavior has changed, thereby altering the classification.
***
***
For example: A small hospital in a rural area would not be expected to have the sophisticated equipment as a major hospital in a city. If an accident victim is brought into the rural facility, the hospital’s duty may be to transfer the patient to a better-equipped facility. The patient will face the risk of dying because of the delay in treatment, but the risk of insufficient treatments outweighs the risk of transfer. If the same victim were brought into a hospital in a major metropolitan center, the duty would be to treat the patient without a transfer. The risk of transfer has not changed, but the risk of insufficient treatment has disappeared.
COMMENTS APPRECIATED
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR- http://www.MarcinkoAssociates.com
Like, Refer and Subscribe
***
***
Filed under: "Ask-an-Advisor", "Doctors Only", Ethics, Experts Invited, mental health, Op-Editorials, Risk Management, Sponsors, Touring with Marcinko | Tagged: books, DO, doctor EQ, DPM, economics, Emotional Intelligence, EQ, intelligence quota, IQ, Marcinko, MD, OB, op-editorial, organizational behavior, physicians IQ, Risk Management, schmuckler, Technology | Leave a comment »
By Health Capital Consultants LLC
***

***
On June 25th, 2025, the Centers for Medicare & Medicaid Services (CMS) released its forecast on U.S. healthcare spending through 2033. The analysis, published in Health Affairs, estimated healthcare spending growth in 2024 and projected the growth into 2033. CMS found that overall healthcare spending growth has decreased slightly but is still elevated compared to pre-pandemic levels, and is expected to continue to moderately grow.
This Health Capital Topics article examines the factors underlying the forecasts. (Read more…)
COMMENTS APPRECIATED
Like and Subscribe
***
***
Filed under: "Ask-an-Advisor", Accounting, Ethics, Funding Basics, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Interviews, Investing, Managed Care, Op-Editorials, Sponsors | Tagged: Centers for Medicare & Medicaid Services, CMS, HCC, Health Capital Consultants, Health Capital Topics, healthcare spending, how much healthcare spending?, Jessica Bailey-Wheaton, TODD A. ZIGRANG, what is CMS | Leave a comment »
MARCINKO ASSOCIATES, Inc.
SPONSOR: http://www.MarcinkoAssociates.com
***
***
Did you Know?
Experts estimate that it can cost more than $1 million to recruit and train a replacement for a doctor who leaves the profession because of burnout. But, as no broad calculation of burnout costs exists, Dr. Tait Shanafelt [Mayo Clinic researcher and Stanford Medicine’s first Chief Physician Wellness Officer] said Stanford, Harvard Business School, Mayo Clinic and the American Medical Association (AMA) are further cost estimating the issue. Nevertheless, Shanafelt and other researchers have shown that burnout erodes job performance, increases medical errors, and leads doctors to leave a profession they once loved.
Fortunately, we can help. From formal coaching to second career opinions, mentoring and advising, we can help with our remediation executive career programs. Regardless of what is happening in your life, it is wonderful to have a non-partial, confidential and informed career coach and sounding board on your side.
CITE: JAMA Internal Medicine [Effect of a Professional Coaching Intervention on the Well-Being and Distress of Physicians].
NCBI: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6686971/
THANK YOU
CONTACT US: https://marcinkoassociates.com/process-what-we-do/
***
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Filed under: "Advisors Only", "Doctors Only", Career Development, Ethics, iMBA, Inc., LifeStyle, Marketing & Advertising, mental health, Op-Editorials, Quality Initiatives, Sponsors, Touring with Marcinko | Tagged: advise, advising, career advice, career advising, career coach, career coaching, coach, coaching, Marcinko, Marcinko Associates, Marcinko coaching, mentor, mentoring | Leave a comment »
By Health Capital Consultants; LLC
***

***
On May 22, 2025, the U.S. House of Representatives moved President Trump’s budget proposal forward, sending to the Senate a budget reconciliation bill (with a one-vote margin) – the One Big Beautiful Bill Act of 2025 – that renews expiring tax cuts and enacts new ones at a cost of almost $4 trillion. These costs would largely be paid for by cuts to other programs, including to federal healthcare programs, which cuts will have significant ramifications for the healthcare industry.
This Health Capital Topics article reviews the current status of the budget bill and healthcare industry implications. (Read more…)
COMMENTS APPRECIATED
Like and Refer
***
***
Filed under: "Ask-an-Advisor", Accounting, Career Development, Drugs and Pharma, Ethics, Funding Basics, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Managed Care, Management, Op-Editorials | Tagged: HCC, Health Capital Topics, Jessica Bailey-Wheaton, One Big Beautiful Bill Act, TODD A. ZIGRANG, Trump | Leave a comment »
BY DR. DAVID EDWARD MARCINKO: MBA MEd CMP™
***
SPONSOR: http://www.MarcinkoAssociates.com
***
Performance of Growth & Value Stocks
Although many academics argue that value stocks outperform growth stocks, the returns for individuals investing through mutual funds demonstrate a near match.
Introduction
A 2005 study Do Investors Capture the Value Premium? written by Todd Houge at The University of Iowa and Tim Loughran at The University of Notre Dame found that large company mutual funds in both the value and growth styles returned just over 11 percent for the period of 1975 to 2002. This paper contradicted many studies that demonstrated owning value stocks offers better long-term performance than growth stocks.
The studies, led by Eugene Fama PhD and Kenneth French PhD, established the current consensus that the value style of investing does indeed offer a return premium. There are several theories as to why this has been the case, among the most persuasive being a series of behavioral arguments put forth by leading researchers. The studies suggest that the out performance of value stocks may result from investors’ tendency toward common behavioral traits, including the belief that the future will be similar to the past, overreaction to unexpected events, “herding” behavior which leads at times to overemphasis of a particular style or sector, overconfidence, and aversion to regret. All of these behaviors can cause price anomalies which create buying opportunities for value investors.
Another key ingredient argued for value out performance is lower business appraisals. Value stocks are plainly confined to a P/E range, whereas growth stocks have an upper limit that is infinite. When growth stocks reach a high plateau in regard to P/E ratios, the ensuing returns are generally much lower than the category average over time.
Moreover, growth stocks tend to lose more in bear markets. In the last two major bear markets, growth stocks fared far worse than value. From January 1973 until late 1974, large growth stocks lost 45 percent of their value, while large value stocks lost 26 percent. Similarly, from April 2000 to September 2002, large growth stocks lost 46 percent versus only 27 percent for large value stocks. These losses, academics insist, dramatically reduce the long-term investment returns of growth stocks.
***

***
However, the study by Houge and Loughran reasoned that although a premium may exist, investors have not been able to capture the excess return through mutual funds. The study also maintained that any potential value premium is generated outside the securities held by most mutual funds. Simply put, being growth or value had no material impact on a mutual fund’s performance.
Listed below in the table are the annualized returns and standard deviations for return data from January 1975 through December 2002.
Index Return SD
S&P 500 11.53% 14.88%
Large Growth Funds 11.30% 16.65%
Large Value Funds 11.41% 15.39%
Source: Hough/Loughran Study
The Hough/Loughran study also found that the returns by style also varied over time. From 1965-1983, a period widely known to favor the value style, large value funds averaged a 9.92 percent annual return, compared to 8.73 percent for large growth funds. This performance differential reverses over 1984-2001, as large growth funds generated a 14.1 percent average return compared to 12.9 percent for large value funds. Thus, one style can outperform in any time period.
However, although the long-term returns are nearly identical, large differences between value and growth returns happen over time. This is especially the case over the last ten years as growth and value have had extraordinary return differences – sometimes over 30 percentage points of under performance.
This table indicates the return differential between the value and growth styles since 1992.
YEARLY RETURNS OF GROWTH/VALUE STOCKS
| Year | Growth | Value |
| 1992 | 5.1% | 10.5% |
| 1993 | 1.7% | 18.6% |
| 1994 | 3.1% | -0.6% |
| 1995 | 38.1% | 37.1% |
| 1996 | 24.0% | 22.0% |
| 1997 | 36.5% | 30.6% |
| 1998 | 42.2% | 14.7% |
| 1999 | 28.2% | 3.2% |
| 2000 | -22.1% | 6.1% |
| 2001 | -26.7% | 7.1% |
| 2002 | -25.2% | -20.5% |
| 2003 | 28.2% | 27.7% |
| 2004 | 6.3% | 16.5% |
| 2005 | 3.6% | 6.1% |
| 2006 | 10.8% | 20.6% |
| 2007 | 8.8% | 1.5% |
| 2008 | -38.43% | -36.84% |
| 2009 | 37.2% | 19.69% |
| 2010 | 16.71% | 15.5% |
| 2011 | 2.64% | 0.39% |
| 2012 | 15.25% | 17.50% |
Source: Ibbottson.
Between the third quarter of 1994 and the second quarter of 2000, the S&P Growth Index produced annualized total returns of 30 percent, versus only about 18 percent for the S&P Value Index. Since 2000, value has turned the tables and dramatically outperformed growth. Growth has only outperformed value in two of the past eight years. Since the two styles are successful at different times, combining them in one portfolio can create a buffer against dramatic swings, reducing volatility and the subsequent drag on returns.
Assessment
In our analysis, the surest way to maximize the benefits of style investing is to combine growth and value in a single portfolio, and maintain the proportions evenly in a 50/50 split through regular rebalancing. Research from Standard & Poor’s showed that since 1980, a 50/50 portfolio of value and growth stocks beats the market 75 percent of the time.
Conclusion
Due to the fact that both styles have near equal performance and either style can outperform for a significant time period, a medical professional might consider a blending of styles. Rather than attempt to second-guess the market by switching in and out of styles as they roll with the cycle, it might be prudent to maintain an equal balance your investment between the two.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
COMMENTS APPRECIATED
Refer, Subscribe and Like
***
***
Filed under: "Ask-an-Advisor", "Doctors Only", Experts Invited, Financial Planning, Funding Basics, Glossary Terms, Investing, Marcinko Associates, Op-Editorials, Risk Management | Tagged: 50/50, bear, bulls, DJIA, Eugene Fama, fama, Fama and French, finance, french, Growth, growth investors, growth stocks, growth stocks value versus growth stocks, herding, Investing, Kenneth French, Loughran, Marcinko, Mutual Funds, NASDAQ, pe, PE ratio, personal-finance, S&P 500, stock market, stocks, Todd Houge, value, value investors, value stocks | Leave a comment »
SPONSOR: http://www.MarcinkoAssociates.com
By Dr. David Edward Marcinko; MBA MEd CMP™
***
***
SPONSOR: http://www.CertifiedMedicalPlanner.org
Life planning and behavioral finance as proposed for physicians and integrated by the Institute of Medical Business Advisors Inc., is unique in that it emanates from a holistic union of personal financial planning, human physiology and medical practice management, solely for the healthcare space. Unlike pure life planning, pure financial planning, or pure management theory, it is both a quantitative and qualitative “hard and soft” science, with an ambitious economic, psychological and managerial niche value proposition never before proposed and codified, while still representing an evolving philosophy. Its’ first-mover practitioners are called Certified Medical Planners™.
Life planning, in general, has many detractors and defenders. Formally, it has been defined by Mitch Anthony, Gene R. Lawrence, AAMS, CFP© and Roy T. Diliberto, ChFC, CFP© of the Financial Life Institute, in the following trinitarian way.
Financial Life Planning is an approach to financial planning that places the history, transitions, goals, and principles of the client at the center of the planning process. For the financial advisor or planner, the life of the client becomes the axis around which financial planning develops and evolves.
Financial Life Planning is about coming to the right answers by asking the right questions. This involves broadening the conversation beyond investment selection and asset management to exploring life issues as they relate to money.
Financial Life Planning is a process that helps advisors move their practice from financial transaction thinking, to life transition thinking. The first step is aimed to help clients “see” the connection between their financial lives and the challenges and opportunities inherent in each life transition.
But, for informed physicians, life planning’s quasi-professional and informal approach to the largely isolate disciplines of financial planning and medical practice management is inadequate. Today’s practice environment is incredibly complex, as compressed economic stress from HMOs managed care, financial insecurity from insurance companies, ACOs and VBC, Washington DC and Wall Street; liability fears from attorneys, criminal scrutiny from government agencies, and IT mischief from malicious electronic medical record [eMR] hackers. And economic bench marking from hospital employers; lost confidence from patients; and the Patient Protection and Affordable Care Act [PP-ACA] more than a decade ago. All promote “burnout” and converge to inspire a robust new financial planning approach for physicians and most all medical professionals.
The iMBA Inc., approach to financial planning, as championed by the Certified Medical Planner™ professional certification designation program, integrates the traditional concepts of financial life planning, with the increasing complex business concepts of medical practice management. The former topics are presented in this textbook, the later in our recent companion text: The Business of Medical Practice [Transformational Health 2.0 Skills for Doctors].
***
***
For example, views of medical practice, personal lifestyle, investing and retirement, both what they are and how they may look in the future, are rapidly changing as the retail mentality of medicine is replaced with a wholesale and governmental philosophy. Or, how views on maximizing current practice income might be more profitably sacrificed for the potential of greater wealth upon eventual practice sale and disposition.
Or, how the ultimate fear represented by Yale University economist Robert J. Shiller, in The New Financial Order: Risk in the 21st Century, warns that the risk for choosing the wrong profession or specialty, might render physicians obsolete by technological changes, managed care systems or fiscally unsound demographics. OR, if a medical degree is even needed for future physicians?
Say, what medical license?
Dr. Shirley Svorny, chair of the economics department at California State University, Northridge, holds a PhD in economics from UCLA. She is an expert on the regulation of health care professionals who participated in health policy summits organized by Cato and the Texas Public Policy Foundation. She argues that medical licensure not only fails to protect patients from incompetent physicians, but, by raising barriers to entry, makes health care more expensive and less accessible. Institutional oversight and a sophisticated network of private accrediting and certification organizations, all motivated by the need to protect reputations and avoid legal liability, offer whatever consumer protections exist today.
Yet, the opportunity to revise the future at any age through personal re-engineering, exists for all of us, and allows a joint exploration of the meaning and purpose in life. To allow this deeper and more realistic approach, the informed transformation advisor and the doctor client, must build relationships based on trust, greater self-knowledge and true medical business management and personal financial planning acumen.
[A] The iMBA Philosophy
As you read this ME-P website, we hope you will embrace the opportunity to receive the focused and best thinking of some very smart people. Hopefully, along the way you will self-saturate with concrete information that proves valuable in your own medical practice and personal money journey. Maybe, you will even learn something that is so valuable and so powerful, that future reflection will reveal it to be of critical importance to your life. The contributing authors certainly hope so.
At the Institute of Medical Business Advisors, and thru the Certified Medical Planner™ program, we suggest that such an epiphany can be realized only if you have extraordinary clarity regarding your personal, economic and [financial advisory or medical] practice goals, your money, and your relationship with it. Money is, after only, no more or less than what we make of it.
Ultimately, your relationship with it, and to others, is the most important component of how well it will serve you.
COMMENTS APPRECIATED
Read, Subscribe, Like and Refer
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
***
Filed under: "Ask-an-Advisor", "Doctors Only", CMP Program, Experts Invited, Financial Planning, Glossary Terms, Health Economics, Healthcare Finance, iMBA, iMBA, Inc., Insurance Matters, Investing, Managed Care, Marcinko Associates, Op-Editorials, Portfolio Management, Practice Management, Practice Worth, Professional Liability, Recommended Books, Touring with Marcinko | Tagged: ACA, ACOs, behavioral finance, certified medical planner, CFP, CMP, DO, doctors practice management, DPM, finance, Financial Planning, HMO, iMBA, Investing, life planning, Marcinko, MBA, MD, medical business advisors, personal-finance, PPACA, PPO, retirement planning, VBC | 1 Comment »
By Rick Kahler MSFP CFP®
***

***
OVER HEARD IN THE FINANCIAl ADVISOR’S LOUNGE
A basic strategy for asset protection is to hold various assets in different entities. Putting real estate, small businesses, and other assets into trusts, corporations, or limited liability companies (LLCs) is effective protection that is relatively easy to put into practice. Not only do I recommend this strategy to clients, I use it myself. Recently, however, I discovered a potential downside.
About 25 years ago, I invested in some rare coins in a corporation I owned and put them into a safe deposit box owned by the corporation. When my business relocated 12 years ago, the safe deposit box billing was not forwarded to the new address and was never paid again. Last year I went to retrieve the coins from the safe deposit box, which I had not visited in 25 years. I discovered the box had been drilled open three years earlier and my collection turned over to the unclaimed property division of the State Treasurer’s office.
I was told getting the coins back would be simple enough. I just needed to verify that I owned the company which owned them by providing the corporation’s tax ID number. However, the corporation no longer existed. I didn’t have a record of its tax ID number. The IRS wouldn’t verify the number without my giving them the address the company had used. That address was a post office box number that I no longer used and couldn’t remember. The state’s position was “no tax ID, no coins.” The only verification of my identity as owner of the corporation was my signature on the bank’s safe deposit box application. Eventually, with the support of bank officers who were willing to swear that I was who I claimed to be, I got my coin collection back. The hassle involved in this process was a reminder of an important component of asset protection. Maintain accurate records so you don’t end up hiding assets from yourself.
***
***
A good start is to create a master file of all the entities that hold your assets. This can be any system that’s easy for you to use: a computer spreadsheet, a set of file folders, or a single paper list. Share it as appropriate with your CPA, attorney, or financial planner. The master list should include the name of each company, its date of incorporation, tax ID number, address, and other relevant information like phone or bank account numbers. Also keep an inventory of the assets each company owns.
Once you’ve created a master list, it’s essential to keep it up to date as you buy or sell assets, close companies, or transfer ownership. Set up a system, as well, to remind yourself of tasks like filing tax returns, completing minutes of annual meetings, and paying the annual safe deposit box rent. Make your record-keeping easier by eliminating unnecessary complications.
For example, you probably don’t need a separate address for each trust, corporation, or LLC. Instead of creating a separate company for each asset, you might consider grouping smaller assets within one entity. I’d suggest first discussing the pros and cons with an attorney or financial planner. For larger assets like real estate, I do recommend holding each one separately.
When I talk to clients about asset protection, I mention that part of the price we pay for it is an increase in paperwork. It’s easy to accept that idea with casual good intentions. The case of my reclaimed coin investment is a good reminder of the importance of keeping up with that paperwork. If we don’t, we might protect ourselves right out of access to our own assets.
COMMENTS APPRECIATED
Subscribe, Refer and Like
***
***
Filed under: "Ask-an-Advisor", Accounting, Experts Invited, Financial Planning, Funding Basics, Op-Editorials, Risk Management, Taxation | Tagged: asset protection, attorney, CFP, CPA, financial advisor, financial planner, IRS, law, lawyer, legal, records verification, rick kahler, tax, Tax ID, taxes | Leave a comment »
By Rick Kahler CFP™
***

***
On January 21, 1980, in what I thought was a brilliant financial move, I bought gold. At what was then an all-time high of $873 an ounce.
Fast forward 45 years, and here we are again. Gold is on a tear, priced just over $3,000 an ounce at the time of this writing. It needs to rise another 16% to reach its inflation-adjusted record and many analysts think it might just get there.
What’s driving this gold rally? The same thing that drove it in 1980—fear.
Back then, the U.S. was grappling with rising inflation, double-digit price increases, and interest rates in the high teens. Investors feared that the dollar and stock market would collapse, that their hard-earned savings would erode into oblivion, and that gold was a safe haven. Sound familiar?
Today, inflation is less dramatic and the stock market would have to go a long way down to even register as a bear market, but it’s still a major concern. Central banks are buying gold at record levels. Gold-backed ETFs, which had been seeing years of outflows, are finally pulling investors back in.
For most, gold isn’t just an investment, it’s an emotional hedge against uncertainty. Back in 1980, I wasn’t thinking about long-term strategy. I was reacting to fear. Inflation had hit 14%, and like many others, I was convinced the dollar would soon be worthless. Gold, I thought, was my best shot at preserving wealth.
The problem? Inflation eventually cooled; it had dropped to an average of 3.5% by the mid-1980s. Gold prices tumbled along with it. Investors who, like me, bought at the peak, 45 years later still haven’t broken even on an inflation-adjusted basis. (My $873 purchase price, adjusted for inflation, equates to $3,580 today.) If I had stuck with a well-diversified portfolio, I likely would have fared much better over time.
Over the years, I’ve come to realize that our financial decisions aren’t just about numbers. They’re deeply influenced by our Internal Financial System™, a framework that helps explain why we handle money the way we do. I now see that my decision to buy gold was a battle between different financial “parts” of myself.
One part panicked, convinced that money was about to become worthless. Another saw gold prices soaring and didn’t want to miss out. Yet another part convinced me that buying at the peak was still a smart move. Had I paused and examined these internal voices, I might have made a different decision.
My gold purchase shows why emotionally driven investment decisions rarely lead to great financial outcomes. Instead of asking, “Is gold a smart long-term investment?” I was asking, “How do I make sure I don’t lose everything?” Those are two very different questions.
If you’re thinking about buying gold, I urge you to consider these questions:
“Am I investing from a place of fear or strategy?” If you’re rushing in because you’re scared of inflation, pause and reassess.
“How does gold fit into my broader financial plan?” Gold can be a great hedge—if held in appropriate amounts in a diversified portfolio. It is best viewed as catastrophic financial insurance, rather than an investment.
“Am I reacting to headlines or making a well-thought-out decision?” The financial media loves a good gold rally. But remember, markets move in cycles. Today’s rally may be history repeating itself.
Back in 1980, fear persuaded me that gold was a sure thing. I forgot an essential caveat—there are no sure things in investing. If bad market timing were an Olympic sport, I’d have taken home the gold (pun intended) for least profitable performance.
COMMENTS APPRECIATED
Refer and Like
***
***
Filed under: "Ask-an-Advisor", Alternative Investments, Experts Invited, Glossary Terms, mental health, Op-Editorials, Portfolio Management | Tagged: diversification, economy, ETFs, finance, FOMA, gold, gold fever, gold prices, inflation, internal financial system, Investing, mental health, rick kahler | Leave a comment »
FRANKLY SPEAKING MY MIND!
By Dr. David Edward Marcinko MBA MEd CMP™
SPONSOR: http://www.CertifiedMedicalPlanner.org
***
SPONSOR: http://www.MarcinkoAssociates.com
***
The vast majority of physicians and medical professionals major in one of the hard science while in college; biology, engineering, chemistry, mathematics, computer science or physics; etc. Few take undergraduate courses in finance, business management, securities analysis, accounting or economics; although this paradigm is changing with modernity. These course are not particularly difficult for the pre-medical baccalaureate major, they are just not on the radar screen for time compressed and highly competitive students; nor are they needed for medical or nursing school admission, or the many related allied health professional schools.
In fact, William C. Roberts MD, originally from Emory University in Atlanta, and former editor for the Baylor University Medical Center Proceedings and The American Journal of Cardiology, opined just a decade ago:
“Of the 125 medical schools in the USA, only one of them to my knowledge offers a class related to saving or investing money.”
And so, it is important to review some basic principles of economics, finance and accounting as they relate to financial planning in thees two textbooks; and this ME-P.
COMMENTS APPRECIATED
Refer and Subscribe
***
***
***
Filed under: "Ask-an-Advisor", "Doctors Only", Accounting, Experts Invited, Financial Planning, Funding Basics, Glossary Terms, Investing, Marcinko Associates, Op-Editorials, Portfolio Management, Practice Worth, Risk Management, Taxation | Tagged: Accounting, CFP, CMP, education, emory, estate, Financial Planning, Investing, Marcinko, medical school, retirement, Risk Management, tax | Leave a comment »
By Vitaliy Katsenelson CFA
***
***
| The Reputational Bankruptcy of the American Dollar |
| I am in an unenviable position. The policy coming out of the White House has a significant impact on economics, more than ever before in my career. If I say anything positive about that policy, I’ll be put in the MAGA camp. If I criticize it, I’ll be accused of suffering from Trump derangement syndrome. I am hired by you to make the best investment decisions possible. Rather than see me as engaged in political commentary, I’d ask that you view my remarks as purely analytical. Let me give you this analogy. I live in Denver. Let’s imagine I am a huge Broncos fan, and the Broncos are playing the Chicago Bears. If I am betting a significant amount of money on this game, I should put my affinity for the Broncos and hatred of the Chicago Bears aside and analyze data and facts. The Broncos are either going to win or lose; my wanting them to win has zero impact on the outcome. The same applies to my analysis here. My motto in life is Seneca’s saying, “Time discovers truth.” I just try to discover it before time does. When it comes to politics, I also have a significant advantage. I was not born in this country. From a young age, I was brainwashed about communism, not about team Republican versus team Democrat. The failure of the Soviet Union de-brainwashed me fast concerning the virtues of communism and converted me into a believer in free markets. As a result, I never bought into either party’s ideology, and thus in the last four presidential elections I voted for a Republican, an independent, a Democrat, and wrote in my youngest daughter, Mia Sarah (not in that order). In my articles I have criticized the policies of both Biden (student loan forgiveness, unions) and Trump (Bitcoin reserve). I remind myself that in times like these you have to be a nuanced thinker. Some of Trump’s policies are terrific, others … not so much (I am being diplomatic here). Scott Fitzgerald once said “The test of a first-rate intelligence is the ability to hold two opposed ideas in mind at the same time, and still retain the ability to function.” In 2025 we are taking this “first-rate intelligence” test daily. What will happen to the US dollar? The US dollar will likely continue to get weaker, which is inflationary for the US. Let me start with some easily identifiable reasons: We have too much debt. We ran 6-7% budget deficits while our economy was growing and unemployment was at record lows. Now we have $36 trillion in debt. Our interest expenses exceed our defense spending, and these costs will continue to climb. If/when we go into recession, we may see something we have not seen in a long time – higher interest rates. Our budget deficits will balloon to between 9–12%, and the debt market, realizing that inflation (i.e., money printing) is inevitable, will say, “Pay up!” New competition from Bitcoin. President Trump’s approval of Bitcoin as a potential reserve currency is one of the most self-serving and anti-American things I’ve seen any president do. The US dollar is the world’s reserve currency. We still have little competition for that title. China could be a contender, but it is not a democracy and has capital controls. This policy has no upside for America, only downside. A stronger Europe. Ironically, we may inadvertently create a stronger Europe by threatening to abandon NATO. I don’t want to insult European clients (or my European friends), but the following analogy describes the US-Europe relationship on some level: Europe gradually evolved into a trust fund kid (when it came to security) and the US turned into its sugar daddy. The trust fund kid was incredibly dependent on the sugar daddy. It criticized its parent for being a barbarian and money-driven, but it relied heavily on that parent to protect it from bullies. President Trump cut off Europe’s allowance by threatening that the US might not protect Europe from Russia. This has forced Europe to spend more money on defense. Outside of Germany (which has little debt), few European economies can afford that. This may force Europe (or at least some European countries) to become more pragmatic – to cut social programs and bureaucracy. If this leads to a stronger Europe both economically and militarily, the euro will be competing with the US dollar. This is a big if. Our new foreign policy. When people describe President Trump’s foreign policy as “transactional,” they’re highlighting a fundamental shift in how America engages with the world – one with profound implications for our global standing, national interests, and the US dollar. The shift affects both types of capital – financial and reputational. Reputational capital isn’t at risk in ‘one-shot’ transactions like house selling. Imagine you’re selling your primary residence and moving elsewhere. Do you disclose every flaw, or let the buyer figure things out? Your incentive is to maximize short-term profits. You’ll likely never meet this buyer again, and therefore there are incentives not to care what they’ll think of you afterward. You’ll be transactional, seeking the highest price possible for your biggest asset. This exemplifies a ‘one-shot’ system where future interactions aren’t expected. Contrast this with a relationship- and trust-based system. Now imagine you are a homebuilder in a small town. Your suppliers only extend credit if you have a reputation for paying on time. Your employees do quality work only if you treat them fairly. Your buyers tell friends about their experience with you. The incentives naturally create a relational approach. In this trust-based system, incentives skew toward maximizing long-term profits, where reputational capital becomes the glue creating continuity. Reputational capital radiates predictability – you know how someone will behave based on their history – but operating with low or negative reputational capital is difficult and expensive. People won’t enter long-term contracts with you or will demand external guarantees. Many potential partners will simply refuse to deal with you. Building reputational capital works like adding pennies to a jar – each good deed incrementally adds to your standing. Yet reputational capital can collapse instantly by removing the jar’s bottom. A single breach of trust doesn’t just remove one penny; it can wipe out your entire balance and plunge you into reputational bankruptcy. The math is brutally asymmetric: good deeds might add a point or two, while bad deeds subtract by factors of 50 or 100. This doesn’t mean transactions shouldn’t be profitable. If you’re accumulating reputational capital while consistently losing money, you’re probably in the wrong business. Each deal should be evaluated considering both long-term financial and reputational capital. Individual transactions can sacrifice some profit but cannot afford to lose reputational capital. A “one-shot” transactional approach used in a trust-system environment may provide greater short-term profitability, but if this success comes at the expense of reputational capital, the long-term consequences for America’s global position could be devastating. This brings us to our current foreign policy. Relationships between nations are a trust-based system. I’d argue it’s a super-relational system because it’s multigenerational, lasting beyond the life of any one human. Reputational capital is paramount here. Part of the US’s strength has been the soft power – the reputational capital – it exerted. We had a lot of friends, which helped us to be more effective in dealing with our foes. We keep telling ourselves that America is an “exceptional” nation. This exceptionalism didn’t just come from our financial and military might – it accumulated based on our reputational capital. Though we don’t always succeed, we are a people who try to do the right thing. Our exceptionalism has been earned through our actions. We are the country that helped rebuild Europe and gave it six decades to repay lend-lease. We toppled communism. I don’t know the nuances of the Ukraine mineral deal, but initially it had the optics of extortion. Though I think the renegotiated and signed version appears to be fair to both sides, forcing repayment while Ukraine is dodging Russian missiles made the US look transactional. Actions by President Trump over the last month have undermined our reputation. We are quickly becoming a “one-shot” transactional player in a trust-based environment. Imposing tariffs on Canada on a whim to try to get it to become the 51st state erodes American reputational capital. So does not ruling out America invading Greenland. This puts us on the same moral plane as Russia invading Ukraine. The conversation about tariffs has many nuances. For instance, I don’t know anyone who opposes reciprocal tariffs – they seem fair and don’t consume any reputational capital. But tariffs that are used as weapons in a trade war in order to annex another country erode reputational capital. Threatening to leave NATO and not protect countries that don’t spend enough on their defense diminishes reputational capital. Maybe the only way to get European countries to spend on defense was to threaten not to defend them – you can agree or disagree with the rationale behind each of Trump’s decisions, but what can’t be argued is that they undermined our reputational capital. As we lose soft power, our influence will diminish, and thus so will perceptions of our power. The world will start looking at us not from the perspective of the continuity of generations but of presidential cycles. The word of the American president will have an expiration date of the next presidential or mid-term election. There are two negotiation styles – Warren Buffett’s and Donald Trump’s. Both have their advantages and disadvantages. Buffett will give you one offer and one offer only. Once the deal is agreed to, even just verbally, that is the deal. Critics would say that there is downside to that predictability, as foes know how you are going to respond. Donald Trump’s style is to be unpredictable, which has its own advantages when you deal with foes – it keeps opponents guessing. But it destroys trust with your allies. In a world of fiat currencies, all currency is a financial and reputational promise. President Trump, with the help of DOGE (and maybe even tariffs) may increase our financial strength. I hope he does, but it will likely come at a very high cost to our reputational capital, and therefore US global influence and the US dollar will continue its decline. How are we positioned for this? About half of our portfolio is foreign companies whose sales are not in dollars. They will benefit from a weaker dollar. We also have exposure to oil, which is priced in the US dollar and usually appreciates when the dollar weakens. A weaker dollar means our imports will become more expensive, which is inflationary. We own many companies with pricing power and also companies that have claims on someone else’s revenues. Take Uber for example: they get about 20% of each ride. If the cost of the ride goes up, so does their dollar take. Why does President Trump keep pushing crypto? In July 2019, Trump said the following: “I am not a fan of Bitcoin and other cryptocurrencies, which are not money, and whose value is highly volatile and based on thin air.” Five years later he promised to establish the US Crypto Reserve, and in 2025 he did. What changed? There is no logical reason for an American president to endorse crypto. None. Here is the honest answer: Crypto bros made mega-contributions to his campaign. To top it off, three days before he took office he issued $TRUMP – a shitcoin. Believe it or not, “shitcoin” is a technical term in the crypto community (any coin other than Bitcoin is called a shitcoin by Bitcoin “maximalists”, folks who believe Bitcoin is the one and only digital currency). The future sitting president literally issued – I don’t want to call it a currency, so I guess shitcoin is the right name – that will at some point decline to zero in value. In other words, he’ll fleece his loyal followers who purchase $TRUMP of billions of dollars. I previously referenced both reputational capital and soft power. These types of acts by a sitting president subtract from both. |
***
***
COMMENTS APPRECIATED
Refer and Subscribe
***
***
***
Filed under: "Ask-an-Advisor", Alternative Investments, Experts Invited, Financial Planning, Funding Basics, Glossary Terms, Investing, LifeStyle, Op-Editorials, Portfolio Management | Tagged: american dollar, bankruptcy american dollar, Bitcoin, blockchain, Buffett, consumers, CPI, crypto, cryptocurrency, debt, DOGE, dollar, Europe, Europe NATO, finance, NATO, reputational bankruptcy, Trump, US Crypto Reserve, US Dollar, Vitaliy Katsenelson | Leave a comment »
BILL ACKMAN versus JIM KRAMER
By Staff Reporters
SPONSOR: http://www.CertifiedMedicalPlanner.org
***
***
Interesting Day?
Markets: Last week’s market bloodbath will go down in the history books. The S&P 500’s 10% plunge on Thursday and Friday, after President Trump announced massive tariffs, ranks among the steepest two-day decline in the last 70 years, on par with Black Monday in 1987, the post-Lehman Brothers rout in 2008, and the Covid plunge in March 2020. More than $6 trillion was wiped out from stocks over two days, and the NASDAQ entered a bear market, down 20% from a previous high.
Trading restarted at 9:30 am ET for what Bill Ackman predicts will be “one of the more interesting days in our country’s economic history.”
***
Monday Crash?
On the other hand, CNBC host and market commentator Jim Cramer just warned that America is in store for another “Black Monday” market crash similar to the record 1987 collapse if President Trump doesn’t curtail his tariff plan.
Cramer — who noted that the 1987 crash saw the Dow Jones Industrial Average fall by 22.6% in a single day — said the bloodbath could be repeated after the brutal two-day sell-off following the announcement of Trump’s sweeping tariffs against nearly 90 countries.
If the president doesn’t try to reach out and reward these countries and companies that play by the rules, then the 1987 scenario … the one where we went down three days and then down 22% on Monday, has the most cogency,” Cramer said on his show Saturday, referencing the worst single-day fall in the history of the Dow.
QUESTION: Who is correct; Ackman or Cramer?
COMMENTS APPRECIATED
Read, Like, Refer and Subscribe
***
***
Filed under: CMP Program, Experts Invited, Financial Planning, Funding Basics, Glossary Terms, Investing, Op-Editorials, Portfolio Management | Tagged: Bill Ackman, black monday, CNBC, DJIA, DOW, finance, financial crisis, jim cramer, Portfolio Management, recession, redeux, stock crisis, stocks, stocks drop, tariffs, Trump | Leave a comment »
WARNING – WARNING
By Dr. DavidEdwardMarcinko; MBA MEd
***
***
According to www.NPR.org, there are more than120,000 health care forums on the Internet with opinions ranging from pharmaceuticals, to sexual dysfunction, to acne. The same goes for commercial doctor blogs that promote lotions, balms and potions, diets and vitamins, minerals, herbs, drinks and elixirs, or various other ingest-ants, digest-ants or pharmaceuticals, etc.
And, to other doctors, the blogging craze is a new novelty where there are no rules, protocols, standards or precise figures on how many “medical-doctor” or related physician-blogs are “out there.” Unfortunately, too many recount gory ER scenes, or pictorially illustrate horrific medical conditions, or serious and traumatic injuries. Of course, others simply are medical practice websites, or those that entice patients into more lucrative plastic surgery or concierge medical practices. Some are from self-serving/credible plaintiff-seeking attorneys wishing to assist patients.
Not all physician blogs are geared toward practice information, marketing or medical sensationalism. In fact, just the opposite seems to be the case in extremely candid blogs, like “Ranting Docs”, “White Coat Rants,” “Grunt Docs”, “Cancer Doc,” “The Happy Hospitalist,” “Mom MD”, “Cross-Over Health”, “Angry Docs” and “M.D.O.D.,” which bills itself as “Random Thoughts from a Few Cantankerous American Physicians.”
According to some of these, they are more like personal journals, or public diaries, where doctors vent about reimbursement rates, difficult cases, medical mistakes, declining medical prestige and control, and/or what a “bummer” it is to have so many patients die; not pay, or who are indigent, noncompliant. We call these the “disgruntled doctor sites.” Some even talk about their own patients, coding issues, or various doctor-patient shenanigans.
But, according to psychiatrist and blogger Dr. Deborah Peel and others, the problem with blogging about patients is the danger that one will be able to identify themselves – the doctor – or that others who know them will be able to identify them.” Her affiliation, Patient Privacy Rights, rightly worries that patients might track back to the individual, and adversely affect their employment, health insurance or other aspects of life.
***

***
And, according to Dr. Jay S. Grife; MA Esq., it is certainly true that if a doctor violates a patient’s privacy there could be legal consequences. Under HIPAA, physicians could face fines or even jail time. In some states, patients can file a civil lawsuit if they believe a doctor has violated their privacy. Still, internet privacy issues are an evolving gray-area that if not wrong, may still be morally and ethically questionable [personal communication].
Our colleague Robert Wachter MD, author of the blog called “Wachter’s World,” says it’s important for doctors to be able to share cases, as long as they change the facts substantially. On the other hand, the author of “Wachter’s World” and a leading expert on patient safety alternately suggests “You might say we as doctors should never be talking about experiences with our patients online or in books or in articles.” But, he says that “patients shouldn’t take all the information on blogs at face value. Taken for what they are — unedited opinions, and in some cases entertainment — blogs can give readers some useful insight into the good, the bad and the ugly of the medical profession”. Link: http://www.the-hospitalist.org/blogs
Well, fair enough! But, doctors unhappy with their current medical career choice, or its modern evolution, should probably consider counseling or even career change guidance, re-education and re-engineering. It is very inappropriate to vent career frustrations in a public venue. It’s far better for the blog to be private and/or by invitation only; if at all [Personal communication].
We believe that a hybrid mash-up of both views can be wholly appropriate, or grossly inappropriate in some cases. Of course the devil is in the details; linguistics and semantics aside. Nevertheless; what is not addressed in electronic physician “mea-culpas” are the professional liability risks and concerns that are evolving in this quasi-professional, quasi-lay, communication forum.
***
***
Example: We have seen medical mistakes, and liability admissions of all sorts, freely and glibly presented. In fact,
“Some physicians find that the act of liability blogging as a professional confession that is useful in moving past their malpractice mistakes. And, it is also a useful way to begin a commitment to a better professional life of caring in the future. It helps eliminate the toxic residue and angst of professional liability and guilt. Moreover, as they are unburdened of past acts of omission or commission, doctors should remember to also forgive those who have wronged them. This helps greatly with the process and brings additional peace.”
However, although some may say that this electronic confession is good for the soul, it may not be good for your professional liability carrier, or you, when plaintiff’s attorneys release a legion of IT focused interns, or automated bots, searching online for your self-admissions and scouring for your self-incriminations. Of course, a direct connection to a specific patient may still not be made and no HIPAA violation is involved. But, a vivid imagination is not need needed to envision this type of blind medical malpractice discovery deposition query even now.
QUESTION: “Doctor Smith, I noted all the medical errors admitted on your blog. What other mistakes did you make in the care and treatment of my client?”
And so, the question of plausible deniability, or culpability, is easily raised. If you must journalize your thoughts for sanity or stress release; do it in print. And, don’t tell anyone about it so the diary won’t be subpoenaed. Then tear it up and throw it away. Remember, with risk management, “It is all about credibility.” Don’t trash yours! These thoughts may be especially important if you covet a medical career as a researcher, editor, educator, medical expert or something other than a working-class or employed physician.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
COMMENTS APPRECIATED
Read, Like Subscribe and Refer
***
***
Filed under: "Doctors Only", Experts Invited, Marcinko Associates, Marketing & Advertising, mental health, Op-Editorials, Risk Management | Tagged: Angry Docs, anxiety, blogging doctors, blogs, Cancer Doc, DO, doctors, Grunt Docs, Happy Hospitalist, health, healthcare, jay grife, Marcinko, MD, mental health, MOM MD, news, NPR, physicians, Risk Management, Robert Wachter | Leave a comment »
By Health Capital Consultants, LLC
***

Continuing Resolution Excludes Physician Payment Increase Again
On March 15th, 2025, President Donald Trump signed a continuing resolution (CR) that avoided a government shutdown and funds the federal government for the rest of the fiscal year, i.e., through September 30th, 2025.
Perhaps more notable than what was included in the spending bill was what was once again excluded. While the COVID-era tele-health waivers were temporarily extended, Medicare physician payment rates were not addressed, meaning physicians will continue experiencing a 2.93% pay cut for 2025.
This Health Capital Topics article discusses the healthcare provisions included in and excluded from the CR, and the impacts on healthcare providers. (Read more…)
COMMENTS APPRECIATED
Like, Refer, Subscribe and Refer
***
***
***
Filed under: "Ask-an-Advisor", "Doctors Only", Accounting, Ethics, Funding Basics, Health Insurance, Health Law & Policy, Healthcare Finance, Op-Editorials | Tagged: continuing resolution, CR, DO, doctor payment, DPM, Jessica Bailey-Wheaton, MD, medicare, physician payment, Tele-Health, Todd Zigrang, Trump | Leave a comment »
SPONSOR: http://www.MarcinkoAssociates.com
By. Dr. David Edward Marcinko; MBA MEd CMP®
***
SPONSOR: http://www.CertifiedMedicalPlanner.org
***
WARNING – DISASTROUS ACO EXAMPLE – WARNING
GIVEN CASH FLOW MODEL
Suppose that in a new Accountable Care Organization [ACO] contract, a certain medical practice was awarded a new global payment or capitation styled contract that increased revenues by $100,000 for the next fiscal year. The practice had a gross margin of 35% that was not expected to change because of the new business. However, $10,000 was added to medical overhead expenses for another assistant and all Account’s Receivable (AR) are paid at the end of the year, upon completion of the contract.
Cost of Medical Services Provided (COMSP):
The Costs of Medical Services Provided (COMSP) for the ACO business contract represents the amount of money needed to service the patients provided by the contract. Since gross margin is 35% of revenues, the COMSP is 65% or $65,000. Adding the extra overhead results in $75,000 of new spending money (cash flow) needed to treat the patients. Therefore, divide the $75,000 total by the number of days the contract extends (one year) and realize the new contract requires about $ 205.50 per day of free cash flows.
Assumptions
Financial cash flow forecasting from operating activities allows a reasonable projection of future cash needs and enables the doctor to err on the side of fiscal prudence. It is an inexact science, by definition, and entails the following assumptions:
***
***
Physician Reactions:
Since many physicians are still not entirely comfortable with global reimbursement, fixed payments, capitation or ACO reimbursement contracts; practices may be loath to turn away short-term business in the ACA era. Physician-executives must then determine other methods to generate the additional cash, which include the following general suggestions:
1. Extend Account’s Payable
Discuss your cash flow difficulties with vendors and emphasize their short-term nature. A doctor and her practice still has considerable cache’ value, especially in local communities, and many vendors are willing to work them to retain their business
2. Reduce Accounts Receivable
According to most cost surveys, about 30% of multi-specialty group’s accounts receivable (ARs) are unpaid at 120 days. In addition, multi-specialty groups are able to collect on only about 69% of charges. The rest was written off as bad debt expenses or as a result of discounted payments from Medicare and other managed care companies. In a study by Wisconsin based Zimmerman and Associates, the percentages of ARs unpaid at more than 90 days is now at an all time high of more than 40%. Therefore, multi-specialty groups should aim to keep the percentage of ARs unpaid for more than 120 days, down to less than 20% of the total practice. The safest place to be for a single specialty physician is probably in the 30-35% range as anything over that is just not affordable.
The slowest paid specialties (ARs greater than 120 days) are: multi-specialty group practices; family practices; cardiology groups; anesthesiology groups; and gastroenterologists, respectively. So work hard to get your money, faster. Factoring, or selling the ARs to a third party for an immediate discounted amount is not usually recommended.
3. Borrow with Short-Term Bridge Loans
Obtain a line of credit from your local bank, credit union or other private sources, if possible in an economically constrained environment. Beware the time value of money, personal loan guarantees, and onerous usury rates. Also, beware that lenders can reduce or eliminate credit lines to a medical practice, often at the most inopportune time.
4. Cut Expenses
While this is often possible, it has to be done without demoralizing the practice’s staff.
5. Reduce Supply Inventories
If prudently possible; remember things like minimal shipping fees, loss of revenue if you run short, etc.
6. Taxes
Do not stop paying withholding taxes in favor of cash flow because it is illegal.
Hyper-Growth Model:
Now, let us again suppose that the practice has attracted nine more similar medical contracts. If we multiple the above example tenfold, the serious nature of potential cash flow problem becomes apparent. In other words, the practice has increased revenues to one million dollars, with the same 35% margin, 65% COMSP and $100,000 increase in operating overhead expenses.
Using identical mathematical calculations, we determine that $750,000 / 365days equals $2,055.00 per day of needed new free cash flows! Hence, indiscriminate growth without careful contract evaluation and cash flow analysis is a prescription for potential financial disaster.
COMMENTS APPRECIATED
Subscribe, Read, Refer and Like
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
***
***
Filed under: "Ask-an-Advisor", "Doctors Only", Accounting, Career Development, CMP Program, Funding Basics, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, iMBA, iMBA, Inc., Marcinko Associates, Op-Editorials, Risk Management, Taxation | Tagged: Accounting, accounts payable, accounts receivable, ACO, APs, ARs, certified medical planner, CMP, COMPS, cost of medical services provided, CPA, DME, HMO, loans, Marcinko, marginal costs, PPO, tax, Technology | Leave a comment »
By Staff Reporters
Sponsor: http://www.MarcinkoAssociates.com
***

***
Avram Noam Chomsky is an American professor known for his traditional work in linguistics and political activism. Sometimes called “the father of modern linguistics”, Chomsky is also one of the founders of the field of cognitive science. He is a laureate professor of linguistics at the University of Arizona and an professor emeritus at MIT.
And so, modern linguists today approach their work with scientific rigor and perspective [STEM], although they use methods that were once thought to be solely an academic discipline of the humanities.
Contrary to this humanitarian belief, according to Professor Mackenzie Hope Marcinko PhD of the University of Delaware, linguistics is now multidisciplinary. It overlaps each of the human sciences including psychology, neurology, anthropology, and sociology. Linguists conduct formal studies of sound structure, grammar and meaning, but also investigate the history of language families, and research language acquisition.
COMMENTS APPRECIATED
Subscribe and Refer
***
***
Filed under: "Doctors Only", Ethics, Experts Invited, Glossary Terms, Interviews, LifeStyle, Op-Editorials, Touring with Marcinko | Tagged: AI, anthropology, artificial intelligence, cognitive science, human sciences, language, linguistics, Mackenzie Marcinko, MIT, modern linguistics, neurology, Noam Chomsky, philosophy, psychology, sociology, STEM | Leave a comment »
By Rick Kahler CFP®
http://www.KahlerFinancial.com
***

***
Is cryptocurrency really money?
For years, I thought of cryptocurrency as a digital replacement for traditional money. After all, Bitcoin has “coin” right in the name. But let’s be honest: if Bitcoin is a currency, then my mother’s old Beanie Baby collection is a retirement fund.
A real currency needs to be stable. It should allow you to buy a coffee today without wondering whether, by tomorrow, that same amount could buy a car—or be worth nothing at all. Bitcoin and its kin like Ethereum and Dogecoin fail this test spectacularly.
Recently I have realized that cryptocurrency might be something even bigger and stranger than currency. It is not just digital money; it’s a bet on the huge global demand for financial autonomy.
In an age where every dollar is tracked, crypto offers an escape from traditional financial oversight. That makes it attractive not just to cybercriminals and tax evaders, but also to privacy advocates, speculators, and people living under restrictive financial policies. It doesn’t replace traditional money, it sidesteps it. It allows people to move, store, create, and destroy wealth outside of conventional banking systems. Some use it for transactions. Others see it as a hedge against inflation or a bet on the future of decentralized finance. Governments and banks don’t quite know what to do with it.
Crypto exists in a financial gray zone. It’s not widely accepted for everyday purchases, yet it can hold immense value. Unlike cash, which is limited by geography, or gold, which requires secure storage, crypto can be transferred globally in seconds. That’s part of its appeal, especially in countries with strict capital controls or volatile economies.
At the heart of cryptocurrency’s identity is the way it is produced. Crypto isn’t just a speculative asset—it’s an industrialized wealth-creation system. Imagine a massive warehouse filled with powerful computers “manufacturing” cryptocurrency. These mining operations exist solely to create new “coins” and process transactions, consuming enormous amounts of electricity in the process. The larger the operation, the more crypto it produces.
This is not how traditional currencies work. Fiat currencies are managed by central banks aiming for economic stability. Crypto, by contrast, is controlled by a decentralized network of miners and participants [block-chain]. Its supply is fixed, immune to government intervention. Some see this as a weakness. Others argue it is crypto’s greatest strength.
As Bitcoin and other major cryptocurrencies become more integrated into mainstream finance, the risks evolve. Even as regulators warn about crypto’s role in illicit activity, major corporations and investment firms are offering crypto-backed products. Some politicians, including President Trump, are discussing national Bitcoin reserves. This growing legitimacy makes crypto harder to ignore. But if crypto-backed funds become widespread, a crash could ripple far beyond crypto traders. That said, crypto remains a small fraction of global finance. Unless institutional adoption grows significantly, even a major downturn likely wouldn’t trigger systemic collapse.
Crypto’s increasing presence in finance does not make it a sound retirement investment. It is still a speculation. And speculations—whether in Bitcoin, meme stocks, or dot-com startups—are high-risk and not suitable for long-term financial security. Retirement portfolios should be built on diversification, stability, and predictable returns. Crypto offers none of these.
For years, I saw crypto as a failed currency. What I now think it to be is a decentralized speculative asset, driven by a growing demand to bypass traditional financial systems. Its future remains uncertain. As regulation increases and mainstream adoption expands, its role will continue to shift. But crypto is no longer just a niche experiment. It has become a financial force that governments, institutions, and individuals must reckon with—whether they embrace it or try to control it.
COMMENTS APPRECIATED
Read, Like, Refer and Subscribe
***
***
Filed under: "Ask-an-Advisor", Experts Invited, Financial Planning, Funding Basics, Glossary Terms, Investing, Op-Editorials | Tagged: bit coin, Bitcoin, block-chain, blockchain, CFP, coin, crypto, cryptocurrency, currency, dodgecoin, economics, fiat, finance, financial, Kahler CFP, kahler financial, money, op-ed, speculation | 1 Comment »
BY DR. DAVID EDWARD MARCINKO; MBA MEd CMP®
***
SPONSOR: http://www.MarcinkoAssociates.com
***
SO – HOW MUCH IS A “FINANCIAL ADVISOR” REALLY WORTH?
This blog holds a rather uncomplimentary opinion of financial advisors, and the financial services and brokerage industry as a whole; deserved, or not? The entire site hints at this attitude as well, in favor of a going it alone or ME, Inc investing when possible. Nevertheless, it is reasonable to wonder how much boost in net-returns might an educated and informed, fee transparent and honest, fiduciary focused “financial advisor” add to a clients’ investment portfolio; all things being equal [ceteris paribus].
And, can it be quantified?
Well, according to Vanguard Brokerage Services®, perhaps as much as 3%? In a decade long paper from the Valley Forge, PA based mutual fund and ETF giant, Vanguard said financial advisors can generate returns through a framework focused on five wealth management principles:
• Being an effective behavioral coach: Helping clients maintain a long-term perspective and a disciplined approach is arguably one of the most important elements of financial advice. (Potential value added: up to 1.50%).
• Applying an asset location strategy: The allocation of assets between taxable and tax-advantaged accounts is one tool an advisor can employ that can add value each year. (Potential value added: from 0% to 0.75%).
• Employing cost-effective investments: This component of every advisor’s tool kit is based on simple math: Gross return less costs equals net return. (Potential value added: up to 0.45%).
• Maintaining the proper allocation through rebalancing: Over time, as investments produce various returns, a portfolio will likely drift from its target allocation. An advisor can add value by ensuring the portfolio’s risk/return characteristics stay consistent with a client’s preferences. (Potential value added: up to 0.35%).
• Implementing a spending strategy: As the retiree population grows, an advisor can help clients make important decisions about how to spend from their portfolios. (Potential value added: up to 0.70%).
Source: Financial Advisor Magazine, page 20, April 2014.
Assessment
However, Vanguard notes that while it’s possible all of these principles could add up to 3% in net returns for clients, it’s more likely to be an intermittent number than an annual one because some of the best opportunities to add value happen during extreme market lows and highs when angst or giddiness [fear and greed] can cause investors to bail on their well-thought-out investment plans.
And, is the study applicable to doctors and allied healthcare providers? Doe Vanguard have a vested interest in the topic. What about fee based versus fee-only financial advice?
Conclusion
Finally, recognize the plethora of other financial planning life-cycle topics addressed in this ME-P were not included in the Vanguard investment portfolio-only study a decade ago.
And what about today with contemporaneous internet advising, chat-rooms, linkedin, robo-advisors, reddit and the like?
COMMENTS APPRECIATED
Read, Subscribe and Like
***
***
Filed under: "Advisors Only", "Ask-an-Advisor", Accounting, Alternative Investments, Career Development, CMP Program, Ethics, Experts Invited, Financial Planning, Funding Basics, Industry Indignation Index, Investing, Marcinko Associates, Op-Editorials, Touring with Marcinko | Tagged: asset allocation, behavioral coach, CFP, CMP, diversification, ETF, ETFs, fee based, fee only, finance, financial advisor, financial advisors, financial planners, internet, Investing, Marcinko, mutual fund, Mutual Funds, personal-finance, Reddit, robo advisors, stocks, Vanguard | Leave a comment »
PROS and CONS
BY DR. DAVID EDWARD MARCINKO MBA MEd CMP®
***
***
SPONSOR: http://www.MarcinkoAssociates.com
§ DIRECT PATIENT ACCESS TO LABORATORY RESULTS
According to Patricia Salber MD [personal communication], there are a number of reasons why direct patient access to laboratory medical results is a good idea:
But, the arguments against direct access discussed include the following:
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
COMMENTS APPRECIATED
Subscribe, Refer and Like
***
***
Filed under: "Doctors Only", Drugs and Pharma, Ethics, Op-Editorials, Risk Management, Sponsors, Touring with Marcinko | Tagged: CMP, finance, insurance, Investing, investment, lab tests, laboratory results, life insurance, Marcinko, medical laboratory medical tests, medical test results, Risk Management | Leave a comment »
By Vitaliy Katsenelson; CFA
***

***
| ENCORE: March 22, 2004 A basic property of religion is that the believer takes a leap of faith: to believe without expecting proof. Often you find this property of religion in other, unexpected places – for example, in the stock market. It takes a while for a company to develop a “religious” following: only a few high-quality, well-respected companies with long track records ever become worshipped by millions of investors. My partner, Michael Conn, calls these “religion stocks.” The stock has to make a lot of shareholders happy for a long period of time to form this psychological link. The stories (which are often true) of relatives or friends buying few hundred shares of the company and becoming millionaires have to fester a while for a stock to become a religion. Little by little, the past success of the company turns into an absolute – and eternal – truth. Investors’ belief becomes set: the past success paints a clear picture of the future. Gradually, investors turn from cautious shareholders into loud cheerleaders. Management is praised as visionary. The stock becomes a one-decision stock: buy. This euphoria is not created overnight. It takes a long time to build it, and a lot of healthy pessimists have to become converted into believers before a stock becomes a “religion.” Once a stock is lifted up to “religion” status, beware: Logic is out the window. Analysts start using T-bills to discount the company’s cash flows in order to justify extraordinary valuations. Why, they ask, would you use any other discount rate if there is no risk? When a T-bill doesn’t do the trick, suddenly new and “more appropriate” valuation metrics are discovered. Other investors don’t even try to justify the valuation – the stock did well for me in the past, why would it stop working in the future? Faith has taken over the stock. Fundamentals became a casualty of “stock religion.” These stocks are widely held. The common perception is that they are not risky. The general public loves these companies because they can relate to the companies’ brands. A dying husband would tell his wife, “Never sell _______ (fill in the blank with the company name).” Whenever a problem surfaces at a “religion stock,” it is brushed away with the comment that “it’s not like the company is going to go out of business.” True, a “religion stock” company is a solid leader in almost every market segment where it competes and the company’s products carry a strong brand name. However, one should always remember to distinguish between good companies and good stocks. Coca-Cola is a classic example of a “religion stock.” There are very few companies that have delivered such consistent performance for so long and have such a strong international brand name as Coca-Cola. It is hard not to admire the company. But admiration of Coca-Cola achieved an unbelievable level in the late nineties. In the ten years leading up to 1999, Coca-Cola grew earnings at 14.5% a year, very impressive for a 103-year-old company. It had very little debt, great cash flow and a top-tier management. This admiration came at a steep price: Coca-Cola commanded a P/E of 47.5. That P/E was 2.7 times the market P/E. Even after T-bills could no longer justify Coke’s valuation, analysts started to price “hidden” assets – Coke’s worldwide brand. No money manager ever got fired for owning Coca-Cola. The company may not have had a lot of business risk. But in 1999, the high valuation was pricing in expectations that were impossible for any mature company to meet. “The future ain’t what it used to be” – Yogi Berra never lets us down. Success over a prolonged period of time brings a problem to any company – the law of large numbers. Enormous domestic and international market share, combined with maturity of the soft drink market, has made it very difficult for Coca-Cola to grow earnings and sales at rates comparable to the pre-1999 years. In the past five years, earnings and sales have grown 2.5% and 1.5% respectively. After Roberto C. Goizueta’s death, Coke struggled to find a good replacement – which it acutely needed. Old age and arthritis eventually catch up with “religion stocks.” No company can grow at a fast pace forever. Growth in earnings and sales eventually decelerates. That leads to a gradual deflation of the “religion” premium. For Coke, the descent from its “religious” status resulted in a drop of nearly 20% in the share price – versus an increase of 65% in the broad market over the same time. And at current prices, the stock still is not cheap by any means. It trades at 25 times December 2004 earnings, despite expectations for sales growth in the mid single digits and EPS growth in the low double digits. It takes a while for the religion premium to be totally deflated because faith is a very strong emotion. A lot of frustration with sub-par performance has to come to the surface. Disappointment chips away at faith one day at a time. “Religion” stocks are not safe stocks. The leap of faith and perception of safety come at a large cost: the hidden risk of reduction in the “religion premium.” The risk is hidden because it never showed itself in the past. “Religion” stocks by definition have had an incredibly consistent track record. Risk was rarely observed. However, this hidden risk is unique because it is not a question of if it will show up but a question of when. It is very hard to predict how far the premium will inflate before it deflates – but it will deflate eventually. When it does, the damage to the portfolio can be huge. Religion stocks generally have a disproportionate weight in portfolios because they are never sold – exposing the trying-to-be-cautious investor to even greater risks. Coca-Cola is not alone in this exclusive club. General Electric, Gillette, Berkshire Hathaway are all proud members of the “religion stock” club as well. Past members would include: Polaroid – bankrupt; Eastman Kodak – in a major restructuring; AT&T – struggling to keep its head above water. That stock is down from over $80 in 1999 to $18 today. Emotions have no place in investing. Faith, love, hate, and disgust should be left for other aspects of our life. More often than not, emotions guide us to do the opposite of what we need to do to be successful. Investors need to be agnostic towards “religion stocks.” The comfort and false sense of certainty that those stocks bring to the portfolio come at a huge cost: prolonged under performance. My thoughts today (20+ years later) This is one of the first investment articles I ever wrote. I had just started writing for TheStreet.com. It’s interesting to read this article more than 20 years later. I am surprised my writing was not as bad as I had feared (though in many cases it was worse than I feared when I read my other early articles). So much has happened since then – I am a different person today than I was back then. I have two more kids; I have written three more books and a thousand articles. The last two decades were my formative years as an investor and adult. The goal of the article was not to make predictions but to warn readers that the long-term success of certain companies creates a cult-like following and deforms thinking. In fact, my original article – the one I submitted to TheStreet.com – did not mention any companies other than Coke. The editors wanted me to include more names so that the article would show up on more pages of Yahoo! Finance. With the exception of Berkshire Hathaway, all of these companies have produced mediocre or horrible returns. In the best case, their fundamental returns in their old age were only a fraction of what they were when these companies were younger and the world was their oyster. To my surprise, Coke’s stock is still trading at a high valuation. Its business has performed like the old-timer it is, with revenue and earnings growing by only 3–4% a year. The days of double-digit revenue and earnings growth were left in the 80s and 90s, though the high valuation remained. |
COMMENTS APPRECIATED
Refer, Like and Subscribe
***
***
Filed under: "Ask-an-Advisor", Experts Invited, Financial Planning, Funding Basics, Investing, Op-Editorials, Risk Management | Tagged: ATT, Berkshire Hathaway, coca cola, coke, finance, GE, Investing, ko, Kodak, Michael Conn, Polaroid, Risk Management, roberto guizueta, stock market, Vitaliy Katsenelson CFA, Warren Buffett | Leave a comment »
By Health Capital Consultants, LLC
***

***
During its January 2025 meeting, the Medicare Payment Advisory Commission (MedPAC) reviewed and endorsed recommendations for Medicare payment reform and updates. Among other decisions, the commission recommended revisions to the annual Medicare Physician Fee Schedule (MPFS) update methodology and increased pay rates to hospitals under the Inpatient Prospective Payment System (IPPS).
This Health Capital Topics article reviews MedPAC’s recommendations, responses from industry stakeholders, and the likelihood that the commission’s recommendations will be enacted by Congress. (Read more…)
COMMENTS APPRECIATED
Refer, Like and Subscribe
***
***
Filed under: Accounting, Experts Invited, Glossary Terms, Health Law & Policy, Healthcare Finance, Op-Editorials | Tagged: Health Capital Consultants, hospital payments, Inpatient Prospective Payment System, IPPS, medicare payment reform, Medicare Physician Fee Schedule, MedPAC, physician payments | Leave a comment »
By Staff Reporters
***
***
Read Across America Day and Week for the year 2025 is celebrated / observed on Monday, March 3rd-7th.
Read Across America Day is held annually on a school day closest to March 2nd each year. The day promotes reading for children. The popular children’s author Dr. Seuss had his birthday on March 2nd thus original planners of the holiday wanted it to be near his birthday.
The National Education Association (NEA) was one of the main backers of this idea to have a special day to promote reading among the population and especially children.
COMMENTS APPRECIATED
Subscribe, Like and Refer
***
Filed under: Alerts Sign-Up, Book Reviews, Career Development, Glossary Terms, LifeStyle, Op-Editorials | Tagged: books, Dr. Seuss, National Education Association, NEA, Read Across America Day, Read Across America Week, read books | Leave a comment »
AMERICAN DENTAL ASSOCIATION
By ADA and Staff Reporters

***
Every day should be about children’s dental health
This is the message behind the ADA’s National Children’s Dental Health Month resources for 2025. Observed nationally each February, the recognition brings together thousands of dedicated professionals, health care providers and educators to promote the benefits of good oral health to children, their caregivers, teachers and many others.
The ADA is offering new materials to celebrate and promote the importance of children’s dental health, not only during the month of February, but all year.
Posters and flyers emphasizing the importance of brushing are available for free download in two kid-friendly, topical designs and two sizes, 8.5″x11″ and 11″x17″. Matching coloring sheets are offered in 8.5″x11″. All materials have instructions for proper brushing and are available in English and Spanish from ADA.org/NCDHM.
***
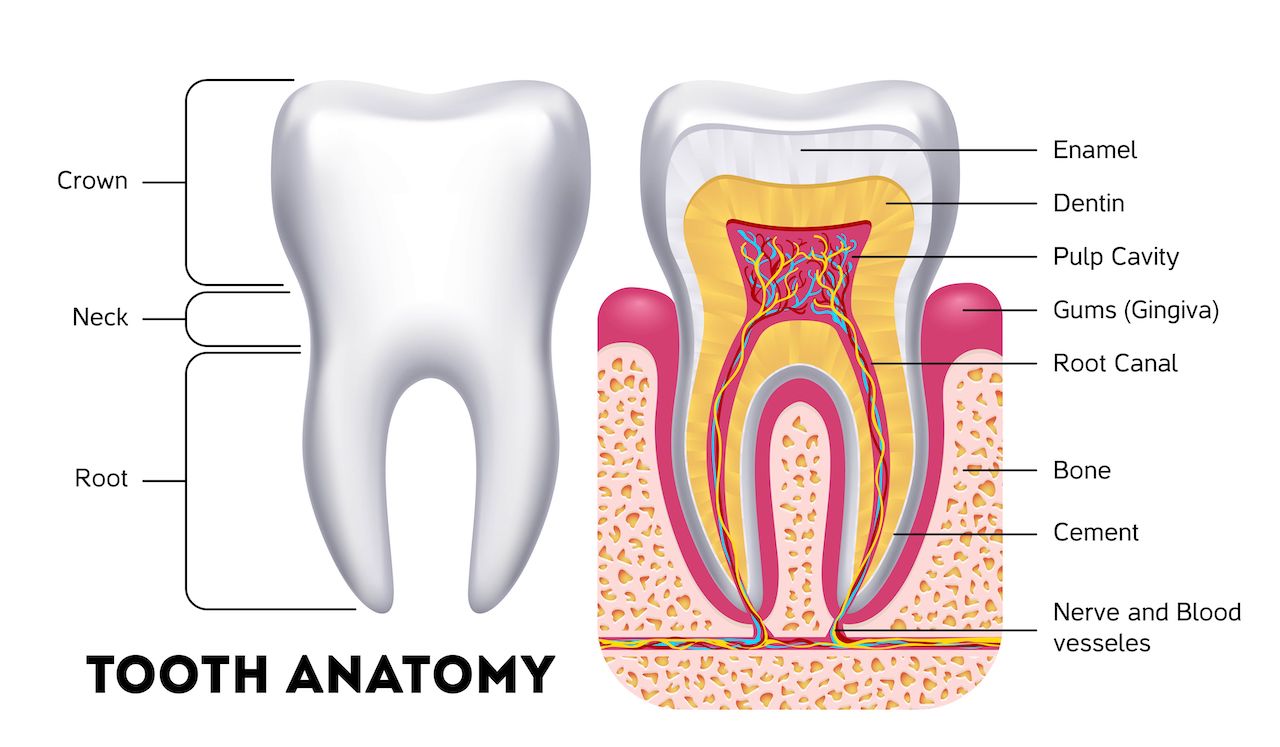
***
In addition, the ADA’s 2025 Brushing Calendar is available for free download. This 12-month calendar is valuable year-round for promoting healthy behaviors like brushing twice a day with a fluoride toothpaste to help prevent dental disease. Kids can track their daily brushing and flossing routines and exercise their creativity by coloring the calendar image for each month.
Another tool, the NCDHM Program Planning Guide, provides resources for program coordinators, dental societies, teachers and parents to promote the benefits of good oral health to children. The guide includes easy-to-do activities, program planning tips, a sample NCDHM proclamation and more.
“The sooner children understand the value of good oral health habits, the more likely they are to continue these habits well into adulthood,” said ADA President Brett Kessler, D.D.S. “The ADA is proud that NCDHM will once again equip some of the most influential figures in kids’ lives — like parents, educators and health care providers — to help set our nation’s kids on the path to a lifetime of healthy smiles and healthier lives.”
National Children’s Dental Health Month observances began with a one-day event in Cleveland and a one-week celebration in Akron, Ohio, in February 1941. Since then, the concept has evolved into a nationwide program.
The ADA held the first national observance of Children’s Dental Health Day on February 8th, 1949. The one-day event became a week long event in 1955, and in 1981 the program was extended to a month long celebration known today as National Children’s Dental Health Month.
For questions about NCDHM resources, please email ncdhm@ada.org. For oral health resources, visit MouthHealthy.org.
COMMENTS APPRECIATED
Refer and Subscribe
***
***
Filed under: "Doctors Only", Career Development, Ethics, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Op-Editorials | Tagged: ADA, ADA February, books, Brett Kessker, cement, crown neck, DDS, dentin pulp, dentist, dentistry, DMD, enamel, food, gums, health-wellness, healthy mouth, mouth, National Children’s Dental Health Month., NCDHM, nerves, oral health, oral hygiene, pediatric dentistry, photography, root canal, teeth, too brushing, tooth brush, tooth past, travel | Leave a comment »
FULL ARTICLE WITH TAKE AWAY POINTS
By Vitaliy Katsenelson CFA
***

***
Key Take Away Points
***

***
Full Article
I wrote this from Las Vegas, where my son Jonah and I were at CES (the Consumer Electronics Show).
In investing and life, it’s very easy to get tunnel vision – doing what works and staying in your comfort zone. I wanted to attend CES to shake myself out of this pattern.
It’s hard to describe how massive this event is. It sprawls through five enormous pavilions at the Las Vegas Convention Center and takes up two floors of the Venetian Hotel. It is attended by over one hundred thousand people.
Here are my initial, off-the-cuff, somewhat random thoughts from CES.
Robotaxis There were several robotaxi companies here, in addition to Alphabet’s Waymo. Multiple robotaxis are going to hit the market over the next few years; it won’t be just Waymo. Most will start geofenced (they’ll work in specific areas), just like Waymo did.
This is good news for Uber: The more fragmented the robotaxi market, the more players are in this market, the more valuable is Uber’s switchboard system (which will bring higher utilization to robotaxi operators).
This will also hugely transform public transportation. Think about school buses – that market is primed for disruption since most buses follow the same route every day in a relatively small area.
Chinese EVs Chinese electric cars are awesome. This reminds me of what happened in Africa. Most of Africa skipped phone landlines completely and went straight to wireless phones. Similarly, Chinese automakers weren’t great at making regular gas-powered cars (everyone else had dominated that space), so they just leapfrogged straight to electric cars. And leapfrog they did – they’ll make even Tesla work hard.
I can’t speak for their reliability, but their designs are fresh; and without labor unions mandating how many workers need to screw in a single lightbulb, they’re much cheaper than Western alternatives.
If they hit the US market without tariffs, they would decimate the incumbents – similar to what Japanese carmakers did in the early 80s to the Big Three.
Machines on Autopilot Autonomous and remote-controlled equipment is going to change construction, mining, and farming completely. Imagine excavators digging dirt on a project in the middle of nowhere, operated remotely from air-conditioned urban offices – maybe even by experienced operators brought out of retirement.
Jobs that were physically demanding and that pulled workers away from their families are going to become regular nine-to-five office jobs. This means workers can have normal family lives and work longer – way past when they’d normally have to retire due to the physical demands of the job.
Or picture a colony of Caterpillar trucks working autonomously 24/7 at a mine site. The efficiency and safety gains would be huge. You’ll still need workers, but different workers, and fewer of them.
Think about agriculture. All those jobs that “Americans don’t want to do” will be done by tractors or other farm equipment going through strawberry fields, using AI to spray pesticides only where needed and collecting apples and oranges.
Here’s an economic observation with slight policy overtones: The nature of the job market will change. This is one of those turning points in history where our immigration policy should be forward-thinking, adjusted for the world where AI will be playing a larger role in it (that is inevitable), not just focused on the past and today’s needs.
***

***
Cracking the US Market China has a significant competitive advantage in manufacturing; it has a very robust ecosystem and well-oiled supply chain – nothing new here. Its labor is no longer the cheapest, but Chinese manufacturing is getting more automated.
We talked to one of the chief designers of Renpho, a Hong Kong company that makes digital scales (among other gadgets) and is the number one seller of those scales on Amazon. They outsource all manufacturing to China, and the factory that manufactures their scales is completely automated.
What’s also interesting is that in the past, to break into the US market, you had to have relationships with Best Buy and Costco. They were the gatekeepers and also the quality-control testers. Today, all you need is a product. You have direct access to the US consumer through Amazon – you just have to be willing to spend on Amazon advertising to promote your product.
Brand or Bust It’s incredible how fast technology gets commoditized. There are literally fifteen (!) companies selling Oura-like rings (sleep-tracking biometric devices worn as a ring; I’ve been wearing one for five years).
In technology, you need to keep moving all the time or you’ll be eaten by the competition (true in life in general), but you also need a strong brand. I couldn’t tell the difference between my Oura ring and the fifteen replicas, most of them sold at a fraction of Oura’s price. But I trust Oura, and that’s the power of the brand.
I remember researching GoPro stock after it got bombed out (down 80%). During our research, I found that GoPro was selling their cameras for $300-400, while Chinese-made, no-name replicas were sold on Amazon for $40. These replicas didn’t have GoPro’s brand, but they had tens of thousands of five-star (hard to fake) reviews on Amazon. GoPro may have been exceptional (loved by pros), and these no-name cameras were just okay, but they were 10 times cheaper.
I put GoPro stock into the “too hard” pile and moved on – thank God I did; after declining 80%, the stock fell another 80%.
This brings me back to the value of a brand. GoPro wasn’t worth 10x more to consumers than Chinese no-name alternatives. Can Oura command 10x pricing over its no-name competitors? I don’t know. That’s the beauty of investing – I don’t have to have an actionable opinion on everything. With time I have become very comfortable saying “I don’t know.” Investing is one of the few professions where you don’t have to have an answer for everything. “I don’t know” should be the default answer, unless you do know. Which isn’t that often.
Global Tech Showdown Korean companies are really dominating screen technology. LG and several other Korean companies showed off transparent, glass-like LCD screens at CES. Imagine sitting in your self-driving car, and your windows are both regular see-through glass and LCD screens at the same time. Our lives are slowly becoming what we used to see in sci-fi movies, and these screens are definitely a leap in that direction.
CES is a truly global show, with technology on display that spans every aspect of our future. There were a lot of companies from Asia (especially China). In certain pavilions focused on consumer or business hardware, China completely dominated the exhibits. There were quite a few large American companies and many American startups, mostly focused on software (though all their hardware was manufactured in Asia). America still dominates in software.
A few, mainly Chinese, companies were showcasing their humanoid robots. One robot was slowly but accurately moving and stacking boxes in a defined area. Others were roaming more freely and were good at avoiding objects. At this point, these robots have the IQ of a smart dog, an average cat (now cat lovers will love me), or Siri. I bet in a few years this will have changed.
I was only mildly surprised by how few European companies were at the show. It’s a very broad generalization, but Europe seems to be running on fumes of past glory. Western Europe has become a pro at regulation and mastered the redistribution of wealth (activities that don’t help innovation or economic growth), and not much else. Yes, there are exceptions, but that’s the point – they are exceptions. If Europe doesn’t change course, eventually it will run out of fumes.
The beauty of learning is that you don’t always know everything you’ve learned at the moment of learning. Often, you’re just depositing data points that will crystallize into insights at a much later date. I don’t know if CES will become an every-year tradition or something I do sporadically, but it’s definitely fertile ground for learning.
COMMENTS APPRECIATED
Like, Refer and Subscribe
***
***
Filed under: "Ask-an-Advisor", Alternative Investments, Experts Invited, Funding Basics, Glossary Terms, Investing, Op-Editorials, Portfolio Management | Tagged: autopilot machines, books, CES, chinease evs, consumer electronics show, EVs, GoPro, robotaxis, sports, Technology, Vitaliy Katsenelson, Waymo | Leave a comment »
LEGIT or NOT?
By Staff Reporters
***
***
A new pathway will result in a degree called the “Doctor of Medical Science” (DMS); this training is designed for someone—not a physician—to practice clinical medicine with all of the privileges afforded to a medical doctor in the discipline of primary care.
Lincoln Memorial University (LMU) recently announced the start of this new program. In a recent press release they stated, “Lincoln Memorial University is pleased to announce a new type of medical training with its launch of the brand new Doctor of Medical Science (DMS) degree. The only one of its kind, this program bridges the gaps between physician and physician assistant (PA) training for the development of a new type of doctoral trained provider to aid Appalacia and other health care shortage areas.”
The DMS will be for Physician Assistants who have at least three years experience in clinical practice. The curriculum will be a two year program and will consist of 50 credits. The first year will have online didactics delivered by clinical and PhD specialists on staff at LMU-DeBusk College of Osteopathic Medicine and other teaching hospitals. The second year will be more online didactics specific to a clinical specialty.
LMU has already received approval for this program from the Southern Association of Colleges and Schools Commission on Colleges.
Cite: https://www.huffpost.com/entry/the-doctor-of-medical-science_b_593ef537e4b094fa859f1af3
COMMENTS APPRECIATED
Refer and Subscribe
***
***
Filed under: "Doctors Only", Career Development, Drugs and Pharma, Ethics, Glossary Terms, Managed Care, Op-Editorials, Quality Initiatives, Risk Management | Tagged: academia, clinical medicine cognate, Darryl S. Weiman, DDS, DeBusk College Osteopathic Medicine, DMS, DMS degree, DO, doctor medical science, DPM, education, J.D., lincoln memorial university, LMU, M.D., news, PhD, research | Leave a comment »
Human life is Inherently Insecure
By Staff Reporters
SPONSOR: http://www.MarcinkoAssociates.com
***
***
The desire for security and feelings of insecurity are the same thing.
The idea of security, financial or otherwise, is an illusion; human life is inherently insecure. But, this doesn’t mean we shouldn’t be prudent with risk and diligent financial planning with strategies like saving and investing.
However, according to colleague Eugene Schmuckler PhD, MBA, MEd seeking security is like many things; the more you try to grasp and obsess about financial security, the more quickly you will reach a point of diminishing returns. You will feel increasingly less secure at a certain point.
COMMENTS APPRECIATED
Refer and Subscribe
***
***
Filed under: Accounting, Career Development, Ethics, Financial Planning, Funding Basics, Insurance Matters, LifeStyle, Marcinko Associates, mental health, Op-Editorials | Tagged: budgeting, finance, financial insecurity, financial planner, Financial Planning, financial security, insecurity, Investing, Marcinko, mental health, money, obsessions, personal-finance, schmuckler, security | Leave a comment »
SPONSOR: http://www.MarcinkoAssociates.com

Book Dr. David E. Marcinko MBA MEd CMP for your Next Medical, Pharma or Financial Services Seminar or Personal and Corporate Coaching Sessions
Dr. Marcinko enjoys personal coaching and public speaking and gives as many talks each year as possible, at a variety of medical society and financial services conferences around the country and world. These have included lectures and visiting professorships at major academic centers, keynote lectures for hospitals, economic seminars and health systems, keynote lectures at city and statewide financial coalitions, and annual keynote lectures for a variety of internal yearly meetings.
His talks tend to be engaging, iconoclastic, and humorous. His most popular presentations include a diverse variety of topics and typically include those in all iMBA, Inc’s textbooks, handbooks, white-papers and most topics covered on this blog.
MORE: https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
CONTACT: Ann Miller RN MHA
Email: MarcinkoAdvisors@outlook.com
***
***
Filed under: Career Development, Ethics, Financial Planning, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Investing, LifeStyle, Marcinko Associates, Media Mentions and PR, Op-Editorials, Practice Management, Practice Worth, Sponsors, Touring with Marcinko | Tagged: business, career, Career Development, career developments, careers, david marcinko, education, Invite Marcinko, Marcinko, marcinko invitations, marcinko seminars, marcinko speakings, Marcinko Speaks, MBA, news | Leave a comment »
By Health Capital Consultants, LLC
***

***
HCC recently authored the article “Generative AI in Healthcare – Valuation Considerations” published by the National Association of Certified Valuators and Analysts in the November/December issue of The Value Examiner.
Generative artificial intelligence (AI) is the utilization of algorithms to create content—such as text, code, imagery, videos, and even simulations—in mere seconds. The goal of AI in general is to mimic the intelligence of humans to perform tasks. “Generative” AI aims to learn from data without the assistance of humans. While today’s generative AI bots are not yet prepared for widespread utilization in patient care settings, AI is garnering significant interest in the healthcare industry as providers begin to test its capabilities in clinics and offices.
This article reviews the role that generative AI is beginning to play in the U.S. healthcare system, the potential of AI in healthcare, and concerns related to the technology.
COMMENTS APPRECIATED
Refer and Subscribe
***
***
Filed under: "Ask-an-Advisor", Accounting, Book Reviews, Health Economics, Health Insurance, Healthcare Finance, Investing, Op-Editorials, Taxation | Tagged: AI patient care, AI valuations, Generative AI in Healthcare, HCC, Health Capital Consultants, healthcare valuations, NACVA, US healthcare | Leave a comment »
MISSION STATEMENT
Open Letter from the CEO

Dr. David Edward Marcinko MBA CMP™
http://www.MarcinkoAssociates.com
ALL MEDICAL AND HEALTHCARE COLLEAGUES
Did you know that at MARCINKO & Associates, all medical colleagues throughout the United States may contact us when they are considering the sale, purchase, strategic operating improvement, merger, acquisition and/or other financial business or related personal financial planning transaction?
MORE: https://marcinkoassociates.com/welcome-medical-colleagues/
***
Our difference is “hard” knowledge and insider financial guidance that helps medical colleagues, nurses, private practitioners, clinics, ambulatory surgery, radiology and outpatient wound care centers realize their ultimate economic goals. This typically includes managerial and cost accounting, financial ratio analysis, fair market valuation business appraisals, business plan creation and personal financial planning.
MORE: https://marcinkoassociates.com/fmv-appraisals/
Our “expert witness” business litigation support service and divorce mediation, arbitration, asset division, settlement and second opinion offerings are always available, as well.
MORE: https://marcinkoassociates.com/expert-witness/
And, our “soft” skill professional career guidance and mentoring center includes executive coaching, consulting and mentoring advisory programs for stressed, conflicted or burned-out physicians and medical practitioners.
Most importantly, our professional fees are reasonable and always transparent.
MARCINKO & Associates also serves universities, medical, business, graduate and nursing schools; physicians, dentists, podiatrists, optometrists and legal societies. This includes accountants, financial service providers, wealth and hedge fund managers, emerging entities, hospitals, CEOs and their BODs, the press, media and related organizations.
MORE: https://marcinkoassociates.com/speaking-seminars/
Contact us for an educational white-paper on most any topic.
MORE: https://marcinkoassociates.com/case-studies/
***
Now, please review our website to learn more.
And, always retain us when needed.
How May We Serve You?
DAVID EDWARD MARCINKO
email: MarcinkoAdvisors@msn.com

© Copyright: Institute of Medical Business Advisors, Inc. All rights reserved, USA. Present to 2024.
Filed under: "Advisors Only", "Doctors Only", Career Development, Experts Invited, Financial Advisor Listings, Financial Planning, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Insurance Matters, Investing, Marcinko Associates, Media Mentions and PR, Nominations Sought, Op-Editorials, Portfolio Management, Practice Management, Practice Worth, Recommended Books, Research & Development, Risk Management, Touring with Marcinko | Tagged: david marcinko, Dr. David Edward Marcinko, Dr. David Marcinko, Dr. Marcinko, economics, estate, finance, Investing, INVESTMENT BANKING, Marcinko, Marcinko Associates, retirement, Venture Capital | Leave a comment »
 To Our ME-P Subscribers, iMBA Inc., Clients and Friends
To Our ME-P Subscribers, iMBA Inc., Clients and Friends
As we look forward to sharing the holidays with family and friends, we also remember those less fortunate.
And, as has been our practice in recent years, rather than sending holiday greeting cards, the iMBA Inc will provide support to several charities dedicated to helping those in need.
We hope this gesture provides happier holidays for others and serves to express our gratitude to you, in the spirit of the season, for your continued support and loyalty to this ME-P.
Happy New Year 2024
We also extend our hope that the New Year 2022 brings you and your loved ones good health, happiness and a world that comes to know peace and understanding.
***

***
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
MORE: Shopping Trends and Physicians
A New Christmas Tradition: Take a Walk?
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Filed under: Ethics, Experts Invited, iMBA, Inc., LifeStyle, Marcinko Associates, Op-Editorials, Videos | Tagged: Christmas Eve, Dr. David Marcinko, Hampden, Happy New Year, Merry Christmas, tour | 4 Comments »
By Dr. Bertalan Meskó, MD PhD
***
Regarding AI, the emphasis will shift away from the regulatory environment towards technology companies making their own decisions. Trump also promised to repeal Biden’s executive order on AI because it “hinders AI Innovation”.
Regarding health care, Trump said he would let Robert F. Kennedy “go wild” on health. Being a vaccine doubter and having made many unscientific claims about health, this could be a huge risk to digital health and the FDA’s job on regulating technologies. READ MORE
COMMENTS APPRECIATED
Subscribe Today!
***
***
Filed under: Breaking News, Drugs and Pharma, Ethics, Experts Invited, Health Economics, Health Insurance, Information Technology, Op-Editorials | Tagged: AI, Biden, Dr. Bertalan Meskó, FDA, health care, Kennedy, Robert F. Kennedy, Trump | Leave a comment »
***
***
Our guest on this episode is Dr. Farzad Mostashari. Farzad is the co-founder and CEO of Aledade, a primary care enablement company that partners with independent PCPs to transition to value-based care and, as a result, maintain their independence.
Founded in 2014, Aledade works with 11,000 physicians across 40 states and DC, accounting for 1.7M patients under management in Medicare, Medicare Advantage, Commercial and Medicaid contracts. Farzad previously served as the National Coordinator for Health IT in the Department of Health and Human Services, he completed medical school at the Yale School of Medicine and a Master’s in Population Health from Harvard’s T.H. Chan School of Public Health. Earlier this year, Aledade raised a $123M Series E round of funding led by OMERS Growth Equity.
***
In this episode, colleague Shahid N. Shah will discuss with Farzad about (1) his journey to starting Aledade and the role policy expertise and evidence have played in the company’s success (2) why he and the company are betting on independent physicians as the drivers of change in value-based care and (3) how Aledade became the rare profitable health tech company.
-Dr. David Edward Marcinko MBA MEd
PODCAST: https://soundcloud.com/wharton-pulse-podcast/mostashari-aledade
***
***

COMMENTS APPRECIATED
Thank You
***
Filed under: "Advisors Only", "Doctors Only", Alternative Investments, Career Development, Experts Invited, Health Economics, Healthcare Finance, Information Technology, Interviews, Op-Editorials, Practice Management, Research & Development, Videos | Tagged: aledade, Farzad Mostashari, medicare, OMERS Growth Equuity, PCPs, primary care, Shahid N. Shah | 1 Comment »
SPONSORED BY: http://www.MarcinkoAssociates.com
***

***
Most doctors report feeling overworked and are considering a change in career, according to a new poll.
Doximity, a virtual network for physicians, found that 81% doctors surveyed last fall said they felt overworked—a slight decline from 86% who reported burnout in 2022 but still up from 73% in 2021. Meanwhile, about three in five doctors said they were considering early retirement (30%), looking for another employer (15%), or leaving the profession altogether (14%), the poll found.
The findings, released last year, come amid reports of rising rates of physician burnout and dissatisfaction since after the Covid-19 pandemic.
LEARN MORE: https://tinyurl.com/y3j2t3ab
COMMENTS APPRECIATED
Thank You
***
***
Filed under: "Doctors Only", Career Development, Ethics, Experts Invited, Financial Planning, Interviews, Investing, LifeStyle, Managed Care, Marcinko Associates, Op-Editorials, Touring with Marcinko | Tagged: AMA, career coaching, doctor burnout, doctor stress, Doximetry, Marcinko, overworked doctors, overworked physicians, physician coaching, physician stress | Leave a comment »

By Rick Kahler CFP®
There is an old adage that says, “What is good for the goose is good for the gander.”
In today’s urbanized world, most of us probably wouldn’t have the slightest idea what’s good for geese. Yet we still know that this saying reminds us to be cautious about anyone who makes recommendations they don’t follow themselves.
This is especially important when it comes to investment advice.
Duopoly
Have you ever wondered how your investment advisor invests their money? Have you wondered if the agent selling you cash value life insurance as a retirement investment is investing their retirement in the same? Or whether an advisor recommending a specific mutual fund, stock investment, or bond issue buys the same for their own portfolio?
Ask
My suggestion is to stop wondering and ask. I rarely have a client or prospective client ask me whether I invest my own money in the same way I invest the funds of clients. Most people think it is just too personal to ask how an advisor is investing their own funds and that the advisor may take offense.
Yet knowing how anyone offering investment advice to you invests their own funds is highly relevant. It’s especially wise to ask this if someone is trying to sell you on an “exciting opportunity” that sounds too good to be true. An evasive or vague answer is an obvious red flag. But even with a fiduciary advisor, I believe asking how they invest their own money is a legitimate question. I for one am happy to answer it. Yes, the investment vehicles and strategies I recommend for clients are the same ones I use for myself.
If an advisor is recommending a strategy or investment for you that they don’t subscribe to or invest in themselves, then it’s a good idea to ask another question.
Why not?
Certainly, there are good reasons why an advisor would not have the same asset allocation that they recommend for you. They may be significantly younger or older, or they may have a significantly more aggressive or adverse tolerance for risk. But if your advisor outsources your investments to SEI but uses Vanguard for themselves, I would want to explore that. Or if your advisor is about the same age as you are, but has a significantly different asset allocation and uses none of the investments she recommends that you invest in, I would want to know why.
If an advisor suggests that you put 35% of your investment funds into a private REIT but they don’t own a private REIT, what’s the reason? Or if they are recommending you own a managed futures limited partnership but they don’t own that same partnership or any managed futures funds. Or, maybe they are recommending the A shares of an actively managed mutual fund but themselves purchase passively managed institutional shares.
If you don’t feel comfortable or knowledgeable enough to ask questions like these about specific investments, it’s still important to find out about an advisor’s broader approach to investing. Do they recommend that you “buy and hold,” yet they actively time the market with their own portfolio? Or maybe they actively trade your portfolio while following a “buy and hold” strategy themselves.
Assessment
While portfolio specifics might vary, I want any investment advisor to buy into the same investment philosophy they are recommending to me. If they are going to be timing the market with my funds, I want them to be making the same market moves with their own funds.
If a “sauce” isn’t good enough for the advisor personally, it isn’t good enough to recommend to clients.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Book Marcinko: https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
***
Filed under: "Ask-an-Advisor", Ethics, Experts Invited, Financial Planning, Investing, Op-Editorials, Point-Counter Point | Tagged: financial advice, iMBA, institute medical advisors, Investment Advice, medicaol executive post, Rick Kahler CFP® | Leave a comment »
By Marybeth Gasman, Tiffany Smith, Carmen Ye, and Thai-Huy Nguyen
An important issue facing the world of medicine and health care is the field’s lack of diversity, especially regarding African American doctors. African Americans made up 6% of all physicians in the U.S. in 2008, 6.9% of enrolled medical students in 2013 and 7.3% of all medical school applicants.
The existing literature on the lack of diversity within the medical field emphasizes the role that inclusion would play in closing the health disparities among racial groups and the benefits acquired by African Americans through better patient-doctor interactions and further respect for cultural sensitivity. A large portion of current research regarding Black medical students and education focuses on why minority students do not go into medical school or complete their intended pre-med degrees.
Common notions and conclusions are that many institutions do not properly prepare and support students, who despite drive and desire, may lack adequate high school preparation and may go through additional stress unlike their other peers. Historically Black Colleges and Universities (HBCUs) are institutions that were designed to support African American students by providing an educational learning environment that caters to their unique challenges and cultural understandings. Given that HBCUs have had much success in preparing minority students for STEM fields, and for medical school success more specifically, this article looks at the history of such universities in the context of medical education, their effective practices, the challenges faced by African Americans pursing medical education, and what they can do in the future to produce more Black doctors.
We also highlight the work of Xavier University and Prairie View A&M University, institutions that regularly rank among the top two and top ten producers, respectively, of future African American doctors among colleges and universities.
***

****
READ: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6111265/
YOUR THOUGHTS AND COMMENTS ARE APPRECIATED.
Dr. Marcinko at Tuskegee University
Thank You
INVITE DR. MARCINKO: https://medicalexecutivepost.com/dr-david-marcinkos-
***
***
Filed under: Career Development, Ethics, Experts Invited, Op-Editorials, Research & Development | Tagged: Carmen Ye, David Edward Marcinko, HBCUs, HBCUs produce Doctors, Marybeth Gasman, Tiffany Smith, tuskegee university | Leave a comment »
http://www.CertifiedMedicalPlanner.org
Frequently, we hear the axiom that asset allocation is the most important investment decision, explaining 93.6% of portfolio returns. The presumption has been that once the risk tolerance and time horizon have been established, investing is simply a matter of implementing a fixed mix of stocks, bonds, and cash using mutual funds selected for this purpose. This axiom is based on a famous study by Brinson, Hood, and Beebower (BHB) published in the Financial Analysts Journal in July/August 1986. It is the stuff of most modern business school and graduate students in economics and finance.
Enter the Critics
One critic claims that BHB’s conclusions and the interpretation of their conclusions are wrong, stating that because of several methodological problems, BHB needed to make certain assumptions for their analysis to go forward. They assumed that the average asset-class weights for the 10-year period studied are the same as the actual normal policy weights; that investments in foreign stocks, real estate, private placements, and venture capital can be proxied by a mix of stocks, bonds, and cash; and that the benchmarks for stocks, bonds, and cash against which fund performance was measured are appropriate. The author believes that each of these assumptions can lead to a faulty measurement of success or failure at market timing and stock selection.
The Jahnke Study
William Jahnke claims that BHB erred in their focus on explaining the variation of quarterly portfolio returns rather than portfolio returns over the 10-year period studied. According to the study, asset allocation policy explains only a small fraction of the range of 10-year portfolio returns earned by the pension funds reported in the study. The author concluded that this discrepancy is caused by the effect of compounding returns. He adds that BHB were wrong to use variance of quarterly returns rather than the standard deviation. Use of standard deviation would reduce the often cited 93.6% to about 79%. Moreover, BHB did not consider the cost of investing, such as operating expenses, management fees, brokerage commissions, and other trading costs, which are more significant for individual investors than for the pension plans studied. Jahnke claims that excessive costs can reduce wealth accumulation by 50%.
Note: (“The Asset Allocation Hoax,” William W. Jahnke, Journal of Financial Planning, February 1997, Institute of Certified Financial Planners [303] 759-4900).
Assessment
Finally, the author takes issue with establishing long-term fixed asset class weights. Asset allocation should be a dynamic process. Higher equity return expectations should in turn produce larger equity allocations, other things being equal.
Conclusion
Are doctors different than the average investor noted in this essay?
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
 8
8
***
Filed under: CMP Program, Experts Invited, Investing, Marcinko Associates, Op-Editorials, Portfolio Management, Touring with Marcinko | Tagged: asset allocation, Brinson, CMP, david marcinko, Hood Beebower, The Asset Allocation Hoax, William Jahnke, www.certifiedmedicalplanner.com | Leave a comment »
ACCORDING TO AUSTRIAN ECONOMISTS
BY PER BYLUND
Colleague Peter R. Quinones and Per Bylund return to the show to talk about the role of the entrepreneur not only in society, but according to the Austrian School of Economics. Medical perspectives are implied.
PODCAST: https://freemanbeyondthewall.libsyn.com/episode-312
YOUR THOUGHTS AND COMMENTS ARE APPRECIATED.
Thank You
***
***
Filed under: "Advisors Only", "Doctors Only", Experts Invited, Health Economics, Op-Editorials, Videos | Tagged: Austrian Economics, Entrepreneurs, Free Man Beyond the Wall, Mises, Per Byland, Peter Quinones | Leave a comment »
By Dr. David Edward Marcinko MBA MEd CMP
SPONSOR: http://www.MarcinkoAssociates.com
The Society of Physician Entrepreneurs (SoPE) was established as a community of interest in 2008 by several members of the American Academy of Otolaryngology – Head and Neck Surgery (AAO-HNS), including Dr. Arlen Meyers, the founding past President & CEO. SoPE became a separate and independent legal entity; incorporating in Washington, D.C. in January 2011. It is a 501 (c) 6 member organization with the stated purpose of providing support; idea stage through funding, for physician entrepreneurs with ideas on how to improve healthcare.
SoPE’s vision is to accelerate physician originated biomedical innovation.
The mission of SoPE is to foster scholarship in biomedical entrepreneurship and provide education, training and support; idea stage through funding, to primarily community-based physician entrepreneurs in the interest of better healthcare.
SoPE membership is open to all physicians and also accepts individuals as associate members; representatives of medical device, legal, venture capital, and other firms with an interest in serving and/or supporting physician entrepreneurs.
Website: www.sopenet.org
MORE: https://sopenet.org/wp/wp-content/uploads/2019/09/aug-2014.pdf
COMMENTS APPRECIATED
Thank You.
***
***
Filed under: "Doctors Only", Career Development, CMP Program, Health Insurance, Healthcare Finance, iMBA, Inc., Op-Editorials | Tagged: david marcinko, Entrepreneurs, physicians, soceity physicien entreprenerus, Sope | Leave a comment »

By Dr. David Edward Marcinko MBA MEd CMP™
CONSULTING ADVICE – NOT SALES
“AT YOUR SERVICE”
E-mail: MarcinkoAdvisors1738@outlook.com
SPONSOR: http://www.MarcinkoAssociates.com
Marcinko & Associates is financial guide. We help answer your questions in an empowering way. We educate and guide medical colleagues to understand their financial picture and to make better financial decisions. We strive to simplify everything, clear up confusion, and address specific needs and goals.
Simply put, we’re a financial services company on a mission to empower financial freedom for all healthcare professionals; only. We work with doctors, nurses, medical providers, individuals and all sizes of organizations to offer investment, wealth management and retirement solutions so everyone can have a clear and simple understanding of where their finances and career is today and where it is headed tomorrow.

Whatever your financial situation, we do not shame, criticize, or sell. We enrich, educate and empower. We work only with medical colleagues at every stage of their financial journey [students, interns, residents, practitioners, mid-career and mature physicians], through big life personal changes to annual employment reviews, in order to help them understand, invest, and protect their money and lifestyle.
CITE: https://www.r2library.com/Resource
For example, the following are current issues of review need for each Fall and Winter:
***
***
At Marcinko & Associates we discuss specific needs and answer specific questions. We educate and make personalized recommendations that you are free to use, incorporate or disregard. Referrals to trusted specialists and strategic alliance partners then occur if – and as – needed [pro re nata].
SPONSOR: http://www.CertifiedMedicalPlanner.org
***
Filed under: "Doctors Only", Career Development, Experts Invited, Financial Planning, Investing, Marcinko Associates, Op-Editorials, Portfolio Management, Practice Management, Recommended Books, Research & Development, Risk Management, Touring with Marcinko | Tagged: business, business education, business medicine, david marcinko, financial education, Financial Planning, Management, management educati9on, Marcinko, Marcinko Associates | Leave a comment »
By Free Man Beyond the Wall
***

***
We welcomes Senior Mises Institute Fellow Dr. Mark Thornton to the show. Dr. Thornton recently gave a talk at the Mises Institute Supporters Summit on the opioid crisis that is plaguing the United States. Dr. Thornton lays out a short history of this tragic epidemic that is taking lives every day.
CITE: https://www.r2library.com/Resource/Title/0826102549
He addresses how doctors prescribe these drugs, how government regulates them and explains what happens when people are forced into the “black market” to sustain their addiction.
PODCAST HERE: https://freemanbeyondthewall.libsyn.com/episode-169-the-opioid-crisis
***
COMMENTS APPRECIATED
Thank You
***
Filed under: "Doctors Only", Career Development, Drugs and Pharma, Ethics, Experts Invited, LifeStyle, Op-Editorials, Videos | Tagged: Austrian Economics, Capitalism, Dr. Mark Thornton, Free Markets, Ludwig Von Mises Institute, Mises, Peter Quinones, The Free Man Beyond the Wall | Leave a comment »
“MAKING CARE PRIMARY”
By Health Capital Consultants, LLC
***
***
| CMS Announces New Primary Care Model On June 8, 2023, the Centers for Medicare and Medicaid Services (CMS) announced the establishment of Making Care Primary (MCP) Model, a voluntary primary care model that will be tested in Colorado, Massachusetts, Minnesota, New Mexico, North Carolina, New York, New Jersey, and Washington. Launched on July 1, 2024, the 10 ½ year model will seek to improve the coordination and management of care, enable primary care clinicians to form relationships with healthcare specialists, and form community-based connections to address the health needs of patients, as well as health-related social needs such as nutrition and housing. CITE: https://www.r2library.com/Resource This Health Capital Topics article will discuss the new MCP Model and its implications for the healthcare industry. (Read more...) |
***
***
COMMENTS APPRECIATED
Thank You
***
Filed under: "Advisors Only", "Doctors Only", Career Development, Drugs and Pharma, Ethics, Events-Planner, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Managed Care, Op-Editorials, Quality Initiatives, Taxation | Tagged: CDC, CMS, Health Capital Consultants LLC, Making Care Primary, MCP, medical care, primary care, primary medicine | Leave a comment »
















































