Are Dentists like … Rodney Dangerfield?
By Darrell Kellus Pruitt; DDS

“Let’s face it — in our world dentists do not get the respect they deserve. They are not perceived to be ‘real’ doctors … Perhaps the lack of sex appeal in dentistry is part of why dental coverage for everyone is an afterthought in the national health care conversation.”
Gary Kadi DDS, DentistryiQ
http://www.dentaleconomics.com/index/display/article-display/4196579430/articles/dental-economics/volume-100/issue-5/features/the-cavity_in_the.html
Even if Dr. Kadi is correct, and the barrier between a 12 year old and his toothbrush is a world-wide lack of respect of dentistry, that hardly means that electronic dental records (eDR) are going to make the kid brush any better. Experience tells me that if mom’s nagging won’t motivate the stinker, the computer won’t either.
eDR Rationalization?
For those who read the article, did you notice how Dr. Kadi, a dental practice consultant, attempts to subtly insert a fat rationalization for adopting eDRs into the middle of a comment lamenting dentistry’s lack of respect? Tricks like Kadi’s make stakeholders look silly at times, and it bothers me that hardly anyone notices and appreciates the humor that these pros bring to marketplace conversation. That’s why I like to point out mistakes like Kadi’s when I come across them. It’s getting harder to find these kinds of articles about eDRs. My pleasure!
Working Both Sides of the Consulting Fence
As far as I can tell, all but a few dental consultants work both sides of the fence in order to please vendors who give them good deals, as well as dentists who pay for unbiased help. Sponsorship by vendors is the bottom level of a consultant career if one chooses to make a living at selling advice. In this way, the dental consultant business is a lot like the financial advice business. Some advisors push their favorite investments that serve them well no matter what happens to their clients’ money. If a client wants advice, but prefers not to pay full price, interested vendors can be counted on to quietly chip in on an advisor’s bill. And that is why the customer must always be cynical. What’s more, it is arguably one’s community obligation to publicly challenge such artists by luring them out into the open to explain further what they meant to say to naïve people. Dr. Kadi begins:
“The national health-care debate cannot be complete unless we include dental care as part of the discourse.”
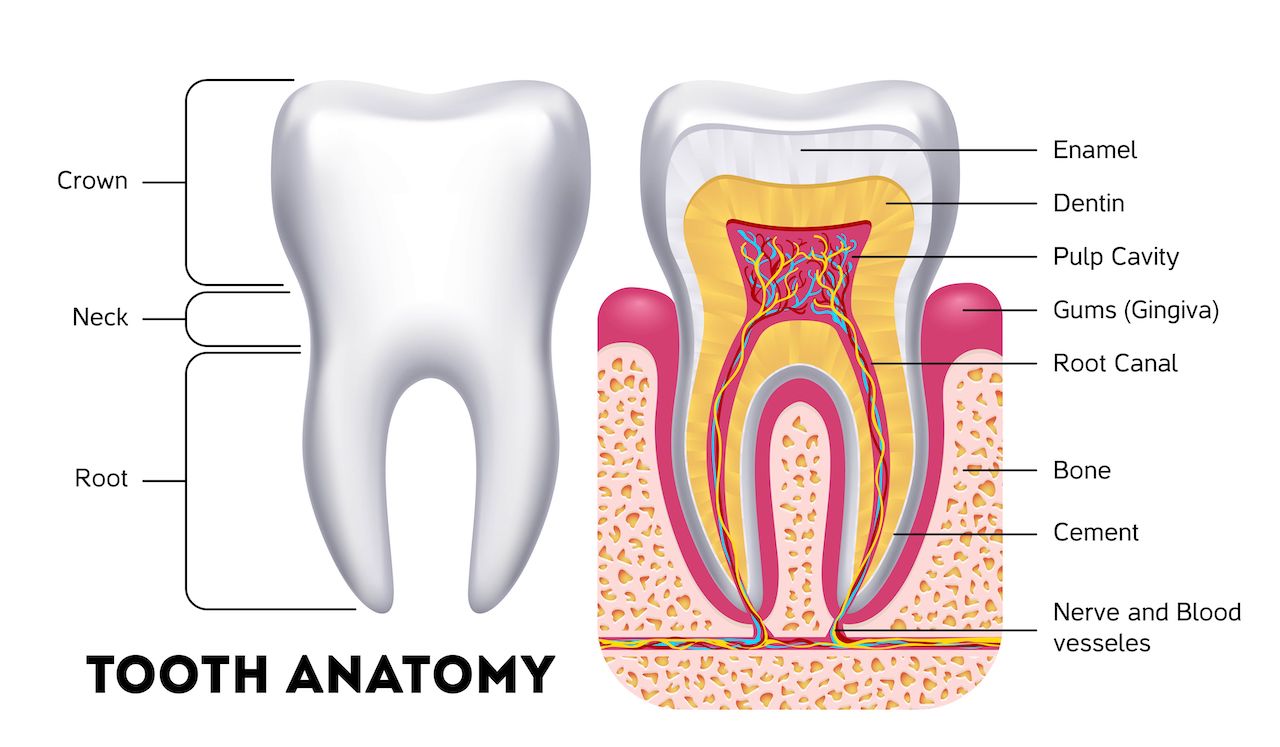
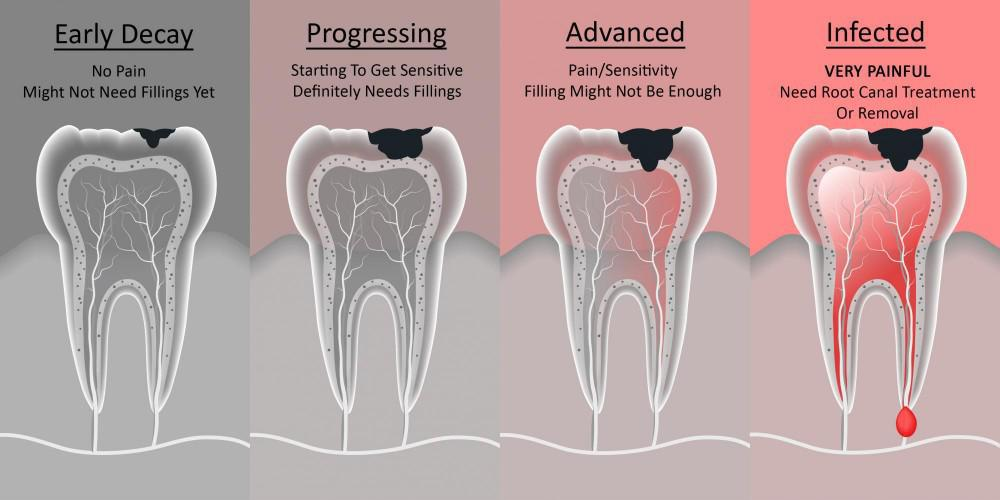
He then presents oft-repeated, convincing findings which support the widely held conclusion that one’s overall health is dependent on one’s oral health. Even though this chunk of common sense has recently been supported with well-respected research, the news isn’t a revelation. Other stakeholders have proclaimed the findings as an example of ultra-modern “Evidence-Based Dentistry,” and proof of the need for thousands of their dental products. However, let’s not kid ourselves. A healthy mouth has less to do with computerization than the proper application of a low-tech toothbrush. 10,000 years ago, even buzzards recognized that bad breath from advanced gum disease smells like imminent death from a long way off if the wind is right. The results Dr. Kadi leans his reasons against only confirm traditional Evidence-Based Superstition.
eDR Lobbying
By half-way through the article Dr. Kadi turned “The cavity in the health-care debate” into a PR piece for eDRs. He’s in so deep that he cannot recognize that his misplaced concerns about image have nothing to do with dental patients’ oral health. Image is only cosmetic.
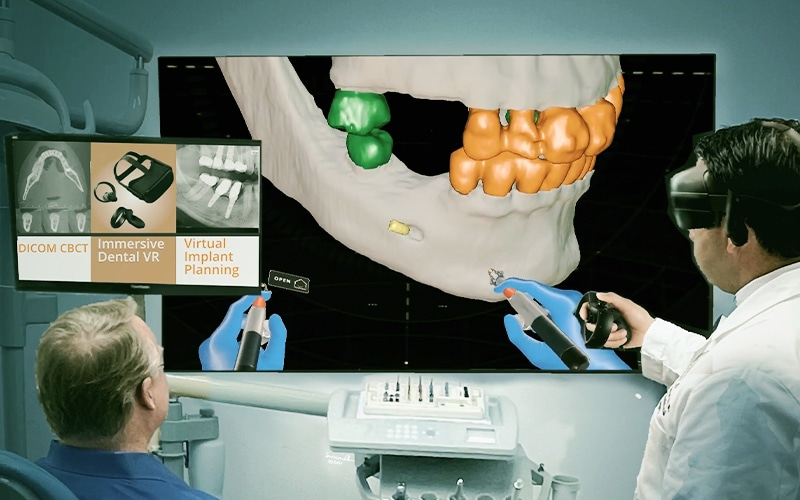
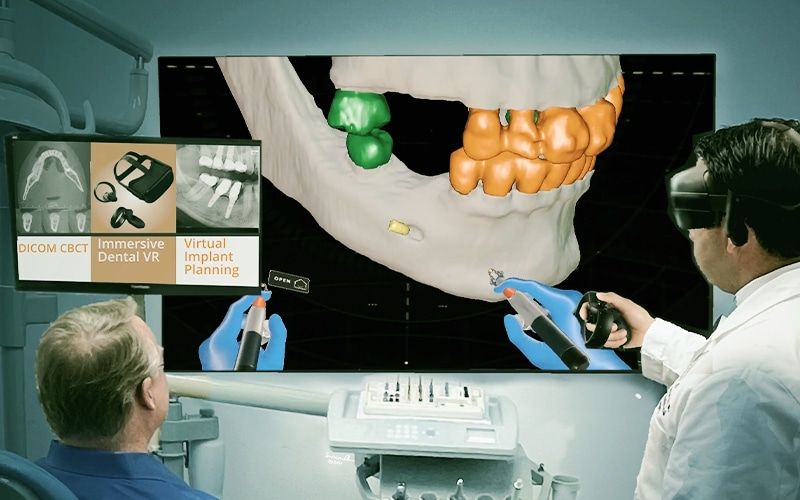
“A validation [of bringing “sex appeal” to the profession] is the inclusion of dentistry in the recently mandated National Healthcare Information Infrastructure (NHII). The purpose of the NHII is to create an information network to facilitate the creation of an electric health record [eHR] for all aspects of health care. The primary impetus is to achieve interoperability of health information technologies used in the mainstream delivery of health care.”
Note: Dr. Kadi admits that the goal is HIT, and sharing health information is the tool – not the other way around. As anyone can see, that kind of nonsense will never work out well in the US. Why that would be as foolish as stuffing a certifying commission for eHRs with industry, government and academic leaders rather than providers – and then tossing billions of dollars that could otherwise be used for treating disease out in the street for the biggest and fastest stakeholders who grab the most. That would be simply ridiculous.
Dr. Kadi bravely continues: “This will enable an individual’s health care information to be shared by all the necessary health care parties in a secure manner, including dentistry. It will improve patient care and reduce the number of patients, currently 100,000 plus, who die each year due to a lack of accurate, complete, or timely information. The federal government estimates a cost savings of $85 billion to $100 billion per year with electronic health records [eHR].”
Is HIT – Or any IT – Really Secure?
In a secure manner – really? There are so many other misleading statements in this paragraph as well. First of all, how can an eDR improve a dentist’s chance of successfully extracting a molar in one piece? It can’t. Secondly, how many of the alleged 100,000 victims died because of lack of electronic DENTAL records? Third, how many patients will die because of faulty information in interoperable records that would not have occurred if the records were paper? Fourth, to insinuate that patient information can only be shared over the Internet is plain silly. Telephone, fax and the US mail have been sufficient for dentistry for decades, and none involve HIPAA. Finally, the $85 to $100 billion in savings Dr. Kadi casually throws out is based on a five year old Rand study that’s been widely trashed for being biased in favor of the stakeholders who funded the research. That happens. It just amazes me that anyone in the healthcare industry who knows anything about HIT is foolish enough to still shop discarded garbage. And once again, regardless of the success of electronic medical records, how will eDRs save even $10 in dentistry? It’s impossible without re-defining “savings.”

Cost Savings
“Dentists and hygienists will play a vital role in this cost savings because people who go for regular cleanings will have their medical history updated in the shared system during each visit. In some cases, dental cleanings may be the only medical attention a person receives yearly.”
“Cost savings”? Where have I heard that term? And why didn’t Dr. Kadi simply say “savings”?
Now I remember. It was Dr. Robert Ahlstrom, the ADA’s eDR expert, who coined the handy buzzword in his testimony describing the benefits of paperless dental practices for the US Department of Health and Human Services in July of 2007. “Cost savings to providers and plans will translate in less costly health care for consumers. Premiums and charges will be lowered.” That would be the seventh of his 11 reasons that are each one so lame that other than Dr. Kadi, stakeholders never borrow them. Although it is undeniable that electronic records benefit insurers and the government more than the patient, if Ahlstrom hadn’t been coy, and had clearly stated that eDRs will save money in dentistry, his testimony would have been false. By calling it a “cost savings,” Ahlstrom technically concedes that using eDRs will indeed require an increase in cost of overhead – which dental patients will ultimately have to pay to obtain dental care. The saving part comes from “what could have been.” Whatever that could possibly mean, HHS Secretary Michael Leavitt bought it.
The PennWell Article
Because of a situation beyond my control, I am unable to provide a link, but to find more of my opinion of Ahlstrom’s testimony that is still used by lawmakers to establish national policy, simply google “Dr. Robert Ahlstrom.” My PennWell article from a year ago or so, “Dr. Robert H. Ahlstrom’s controversial HIPAA testimony,” is probably still his first hit. It could be on his first page the rest of his life.

Assessment
If necessary, I’ll make a few more examples of insensitive HIT stakeholders who know better than to offer such crap to the nation’s lawmakers as well as providers who are too busy to pay attention to the welfare of their profession. The ADA should reassure the nation that there are cheap, effective low-tech ways dental patients can stay healthy that don’t risk their identities and won’t bankrupt a dental practice because of a stolen computer. But; they won’t do it.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
DICTIONARIES: http://www.springerpub.com/Search/marcinko
PHYSICIANS: www.MedicalBusinessAdvisors.com
PRACTICES: www.BusinessofMedicalPractice.com
HOSPITALS: http://www.crcpress.com/product/isbn/9781466558731
CLINICS: http://www.crcpress.com/product/isbn/9781439879900
ADVISORS: www.CertifiedMedicalPlanner.org
PODIATRISTS: www.PodiatryPrep.com
BLOG: www.MedicalExecutivePost.com
FINANCE: Financial Planning for Physicians and Advisors
INSURANCE: Risk Management and Insurance Strategies for Physicians and Advisors



Filed under: Op-Editorials, Practice Management, Pruitt's Platform, Quality Initiatives | Tagged: ADA, Darrell Pruitt, DDS, dental consultants, dental economics, dentistry, DentistryiQ, DMD, Dr. Robert Ahlstrom, eDRs, EHRs, EMRs, Gary Kadi DDS, HIPPA, HIT, NHII, PennWell | 37 Comments »