BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] E-mail: MarcinkoAdvisors1738@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
A medical economic white elephant is a healthcare-related investment—such as a hospital, device, or system—that consumes vast resources but fails to deliver proportional value, often becoming a financial burden rather than a benefit to public health.
In economic terms, a white elephant refers to an asset whose cost of upkeep far exceeds its utility. In the medical field, this concept manifests in projects or technologies that are expensive to build, maintain, or operate, yet offer limited practical use, accessibility, or return on investment. These ventures often begin with noble intentions—improving care, advancing technology, or expanding access—but end up draining resources due to poor planning, misaligned incentives, or lack of demand.
One prominent example is the construction of underutilized hospitals or specialty centers in regions with low patient volume. Governments or private entities may invest heavily in state-of-the-art facilities without conducting thorough needs assessments. The result: gleaming buildings with advanced equipment but few patients, high operating costs, and staff shortages. These facilities often struggle to stay open, becoming financial sinkholes that divert funds from more pressing healthcare needs.
Medical devices and technologies can also become white elephants. For instance, robotic surgical systems or high-end imaging machines are sometimes purchased by hospitals to boost prestige or attract patients, despite limited clinical necessity or trained personnel. These devices require costly maintenance, specialized training, and may not significantly improve outcomes compared to traditional methods. When reimbursement rates don’t justify their use, they become liabilities.
***
***
Electronic health record (EHR) systems offer another cautionary tale. While digitizing patient records is essential, some EHR implementations have ballooned into multi-million-dollar projects plagued by inefficiencies, poor interoperability, and user dissatisfaction. Hospitals may invest in proprietary systems that are difficult to integrate with others, leading to fragmented care and wasted resources. In extreme cases, these systems are abandoned or replaced, compounding the financial loss.
The consequences of medical white elephants are far-reaching. They can strain public budgets, increase healthcare costs, and erode trust in institutions. In developing countries, such projects may be funded by international aid or loans, saddling governments with debt while failing to improve population health. Even in wealthier nations, misallocated resources can mean fewer funds for primary care, preventive services, or community health initiatives.
***
***
Avoiding medical white elephants requires rigorous planning, stakeholder engagement, and evidence-based decision-making. Health systems must assess actual needs, forecast demand, and consider long-term sustainability. Cost-benefit analyses should include not only financial metrics but also health outcomes, equity, and accessibility. Transparency and accountability are key to ensuring that investments serve the public good.
In conclusion, the concept of a medical economic white elephant highlights the importance of aligning healthcare investments with real-world needs and outcomes. While innovation and expansion are vital, they must be grounded in practicality and sustainability.
By learning from past missteps, health systems can prioritize value-driven care and avoid the costly pitfalls of overambitious or poorly conceived projects.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Why It Is Difficult to Practice Medicine Part-Time Today?
In the past, part-time medical practice offered physicians a flexible way to balance professional responsibilities with personal or family commitments. Today, however, the healthcare environment has evolved in ways that make part-time medicine increasingly challenging. From administrative burdens to economic pressures and patient expectations, the obstacles are both systemic and personal.
One of the most significant barriers is the rise in administrative complexity. Physicians are now required to navigate electronic health records (EHRs), comply with insurance documentation, and meet regulatory standards such as HIPAA and MACRA. These tasks consume hours of non-clinical time, which is difficult to compress into a part-time schedule. Even seeing fewer patients doesn’t exempt part-time doctors from the same documentation and compliance requirements as their full-time counterparts.
***
***
Another challenge is financial viability. Many physicians are paid based on productivity metrics, such as Relative Value Units (RVUs), which reward volume over quality. Part-time practitioners often struggle to meet these benchmarks, resulting in lower compensation and reduced benefits. Additionally, malpractice insurance premiums and licensing fees remain fixed regardless of hours worked, further eroding the financial appeal of part-time practice.
Continuity of care is also a concern. Patients increasingly expect immediate access to their providers, especially in primary care and specialties like psychiatry or pediatrics. Part-time physicians may not be available for urgent issues, leading to fragmented care and dissatisfaction. This can strain relationships with patients and colleagues who must cover gaps in availability.
From a professional standpoint, part-time physicians may face limited career advancement. Leadership roles, academic appointments, and research opportunities often favor full-time commitment. There’s also a perception—sometimes unfair—that part-time doctors are less dedicated or less competent, which can affect peer respect and influence within medical institutions.
Technology, while beneficial, adds another layer of complexity. Telemedicine, remote monitoring, and digital communication tools have expanded access but also increased the expectation for constant availability. Part-time physicians may find it difficult to manage asynchronous messages, follow-ups, and virtual visits without extending their work hours beyond what they intended.
***
***
Lastly, burnout and work-life balance—ironically one of the reasons doctors seek part-time roles—can still be elusive. The pressure to maintain clinical excellence, stay updated with medical advancements, and meet patient needs doesn’t diminish with reduced hours. In fact, squeezing these responsibilities into fewer days can intensify stress rather than alleviate it.
In conclusion, while part-time medical practice may seem like a solution to modern work-life challenges, the reality is far more complex. The structure of today’s healthcare system, combined with economic, technological, and cultural pressures, makes it difficult for physicians to thrive in part-time roles. Addressing these challenges will require systemic reform, flexible compensation models, and a cultural shift in how we value and support diverse medical careers.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Despite their high salaries, not all doctors are wealthy, and some live paycheck to paycheck. Here are 5 reasons why many doctors today are broke, according to https://medschoolinsiders.com
1 | Believing They Are Universally Smart
The first reason so many doctors are broke is that many doctors believe they are universally smart. While most doctors have deep specialized knowledge, there’s a big difference between being smart in your profession and being smart with money. A physician’s schooling is quite thorough when it comes to the human body, but med school doesn’t include a prerequisite class on how to handle finances.
Graduating medical school is a major feat and certainly demonstrates superior work ethic and cognitive abilities. But many new doctors believe these accomplishments transcend all aspects of life. If you’re smart enough to earn an MD, you’re certainly smart enough to handle your finances, but only once you properly and intentionally educate yourself.
The truth is doctors, especially traditional graduates, haven’t had an opportunity to manage large sums of money until they become fully trained attending physicians and start pulling in low to mid six figures in income. Prior to that, there was very little of it to manage.
Far too many aspiring doctors, and students in general, don’t take the time to learn financial basics, in part because it’s uncomfortable and seems like something they can figure out “later”, whenever that may be. Their poor spending habits and lack of investment knowledge carry over into their careers, causing many to make irresponsible decisions.
The second factor is overspending too soon, and this comes up at two points in training.
First, it’s natural to want to start spending more as soon as you get into residency and start making a little more money. After all, you’ve been a broke student for 8 or more years, and now you’re finally making a reasonable and reliable wage. But that’s where young doctors get into trouble. Residency pays, but not nearly as much as you will be making once you become an attending physician. The average resident makes about $60K a year, and if you begin spending all of that money right away, thinking you’ll handle your loans once you become an attending, you delay paying off your medical school debt, which means the compounding effect through your student loan interest rate works against you.
Now that $250,000 in student loans has ballooned to over $350,000 by the time you finish residency. The compounding effect, which can be one of your greatest allies in your financial life, becomes an equally powerful enemy when working against you through debt. But of course, pinching pennies is easier said than done, especially when you’re in residency and are surrounded by peers in different professions. They’ve been earning good money much longer than you have, and they can afford more luxurious lifestyles.
They may not be worried about indulging in fine dining or how much a hotel costs when traveling. Students in college and medical school are often confident they will resist the temptations, but the desire to keep up with your friends and family can be difficult to ignore, which causes many to overspend before they technically have the money to do so.
The same is true of attending physicians. As soon as those six-figure salaries come rolling in, many physicians go overboard with spending, trying to make up for lost time and to treat yourself.
Now, we are not suggesting you shouldn’t reward yourself for completing residency, but that reward shouldn’t be a Lamborghini. It’s best to continue living like a resident in your first few years after becoming an attending to pay off loans, put a down payment on a home, and get your financial foundation built before loosening the purse strings.
3 | Decreasing Salaries
Third, doctors continue to make less money than they did before. And this includes nearly all 44 medical specialties. For example, while physician compensation technically rose from $343k to $391k between 2017 and 2022, this rise does not keep up with inflation. The real average compensation in 2022 was less than $325k—a $20k decrease in purchasing power in only six years.
For doctors who are already spending to the limits of their salaries with huge mortgages, car payments, business costs, and other luxuries, a decreased salary can have a huge impact. You might be able to cut back by going on fewer vacations or eating out less frequently, but many accrued costs are locked in, such as a mortgage payment, car loan, or leased rental space for your practice.
4 | Increasing Costs of Private Practice
In the past, running a private practice was much simpler, but recent stricter guidelines and regulations have made it difficult for solo practices to keep up. While regulations like the Health Insurance Privacy and Portability Act, or HIPAA, and mandatory Electronic Medical Records, or EMRs, are necessary to protect patients, they make costs higher for physicians who run their own private practice. These physicians need to spend their own money to set up and maintain EMRs as well as invest in security to ensure patient data is protected.
With the steep rise of inflation we’ve seen over the past couple of years, everything is more expensive, which means costs, such as business space, equipment, and even office supplies, have gone up for private practice physicians while salaries have not. 2013 to 2020 saw an annual inflation rate of anywhere from 0.7% to 2.3%. This skyrocketed to an annual inflation rate of 7.0% in 2021 and another 6.5% in 2022. In fact, the cost of running a private practice has increased by almost 40% between 2001 and 2021.
These increased costs are exacerbated by another problem plaguing private practices; decreased reimbursement. While costs increased by almost 40%, Medicare reimbursement only increased by 11%. When doctors see patients who are insured, the insurance companies pay the physicians for their time. For Medicare, the new proposed rules for 2023 would cut reimbursement by around 5%. When adjusting for inflation, Medicare reimbursement decreased by 20% in the last 20 years.
These costs add up, making it extremely difficult for physicians to thrive financially while running a private practice.
5 | Tuition Debt
Lastly, we can’t talk about a doctor’s finances without mentioning the exorbitant debt so many graduating physicians are left with. It won’t shock you to hear that med school is expensive. Extremely expensive. The average cost of tuition for a single year is nearly $60k, with significant variance from school to school, and that’s before accounting for living expenses.
In-state applicants pay less than out-of-state applicants, and students at private schools typically pay more than students at public medical schools. The astronomical costs mean the vast majority of students can’t pay for medical school out of their own pockets. And unless your family is part of the 1%, even with your parents footing the bill, it’s difficult to cover tuition, let alone rent, groceries, transportation, tech, social activities, exam fees, and application costs.
The average total student debt after college and med school is over $250k. But keep in mind that’s the average, which includes 27% of students who graduate with no debt at all. This means the vast majority of students leave medical school owing much more than $250k.
For some perspective, in 1978, the average debt for graduating MDs was $13,500, which, when adjusted for inflation, is a little over $60,000. There are multiple ways to eventually repay these loans, but time and discipline are essential to ensure this money is paid off as quickly as possible.
According to financial advisor Dr. David Edward Marcinko MEd MBA CMP™; consider the following:
Place a portion of your salary (15-20% or more) into a savings account, and another portion (10-20% or more) into wise investments [stocks, bonds, mutual funds, and/or ETFs].
Pay off your bills each month, and then use leftover spending money to purchase fun things like vacations and fancy dinners, within your means. Shop sales, buy used clothes, and use credit card points for travel.
Hire an excellent tax professional and meet with an investment advisor once or twice a year about your investment status and strategy. http://www.MarcinkoAssociates.com
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Medicine today is vastly different than a generation ago, and all health care professionals need new skills to be successful and reduce the emerging risks outlined in this textbook, as well as the “unknown-unknowns” elsewhere. Traditionally, the physician was viewed as the “captain of the ship”. Today, their role may be more akin to a ship’s navigator, using clinical, teaching skills and knowledge to chart the patient’s course through a confusing morass of insurance requirements, fees, choices, rules and regulations to achieve the best attainable clinical outcomes.
This new leadership paradigm includes many classic business school principles, now modified to fit the decade long PP-ACA, the era of health reform, and modern technical connectivity and EMRs.
Thus, the physician must be a subtle guide on the side; not bombastic sage on the stage. These, newer health 3.0 leadership philosophies might include:
•Negotiation – working to optimize appropriate treatment plans; ie., quality of life versus quantity of life, •Team play – working in concert with other allied healthcare professionals to coordinate care delivery ,ithin a clinically appropriate and cost-effective framework; •Working within the limits of competence – avoiding the pitfalls of the medical generalist versus the specialist that may restrict access to treatment, medications, physicians and facilities by clearly acknowledging when a higher degree of service is needed on behalf of the patient – all while embracing holistic primary care; •Respecting different cultures and values – inherent in the support of the medical Principle of Autonomy is the acceptance of values that may differ from one’s own. As the US becomes more culturally hetero geneous, medical providers are called upon to work within, and respect, the socio-cultural and/or spiritual framework of patients, students and their families; •Seeking clarity on what constitutes marginal care – within a system of finite resources; providers are called upon to openly communicate with patients regarding access to marginal medical information and/or treatments. •Supporting evidence-based practice – healthcare providers, should utilize outcomes data to reduce variation in treatments to achieve higher efficiencies and improved care delivery thru evidence based medicine [EBM]; •Fostering transparency and openness in communications – healthcare professionals should be willing, and prepared, to discuss all aspects of care, especially when discussing end-of-life issues or when problems arise; •Exercising decision-making flexibility – treatment algorithms, templates and clinical pathways are useful tools when used within their scope; but providers must have the authority to adjust the plan if circumstances warrant.
Becoming skilled in the art of listening and interpreting — In her ground-breaking book, Narrative Ethics: Honoring the Stories of Illness, Rita Charon, MD PhD, a professor at Columbia University, writes of the extraordinary value of using the patient’s personal story in the treatment plan. She notes that, “medicine practiced with narrative competence will more ably recognize patients and diseases; convey knowledge and regard, join humbly with colleagues, and accompany patients and their families through ordeals of illness.” In many ways, attention to narrative returns medicine full circle to the compassionate and caring foundations of the patient-physician relationship.
These thoughts represent only a handful of examples to illustrate the myriad of new skills that tomorrows’ healthcare professionals must master in order to meet their timeless professional obligations of compassionate care and contemporary treatment effectiveness; all within the context modern risk management principles.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on April 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
e Department of Veterans Affairs announced plans last week to accelerate the rollout of its embattled electronic health records system. Lawmakers, meanwhile, continue to call for oversight despite concerns over the future of the modernization program. The VA added nine new medical facilities in Ohio, Kentucky, Indiana, and Alaska to the deployment schedule, along with four sites in Michigan that will launch in 2026 after the program expansion has largely been on hold since April 2023, when the agency acknowledged glitches in the system had contributed to at least four veterans’ deaths and “catastrophic harm” to others.
After a roller coaster day, the Dow closed lower by 349 points, or 0.91%. The broader S&P 500 fell 0.23%. The NASDAQ Composite was 0.1% higher after fluctuating between gains and losses. Wall Street’s fear gauge, the CBOE Volatility Index, or VIX, on Monday closed at the highest level since the Covid pandemic as investors fretted over the market’s next move. The VIX surpassed an intraday level of 50 points midday Monday, a rare level associated with extreme volatility.
Posted on July 8, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Bad things can happen in paperless practices, Doc
By Darrell Pruitt DDS
***
***
“Illinois Hospital First To Shut Down Completely After Ransomware Attack”
-By Karl Bode for Techdirt, Jun 16th 2023.
“Such attacks can have a chain reaction on already broken hospitals and health care systems. Health care workers are sometimes forced to resort to pen and paper for patient charts and prescriptions, increasing the risk of potentially fatal error. Delays in care can also prove fatal. And ransomware is only one of the problems that plague dated medical IT systems whose repair is being made increasingly costly and difficult by medical health care system manufacturers keen on monopolizing repair.”
Remember the MCNA (Managed Care of North America) data breach that was reported by Bill Toulas in Bleeping Computer on May 29th? There have been new developments.
“Patients of a Florida-based dental insurance provider brought a proposed class action lawsuit alleging negligence over a ransomware data breach that leaked the private information of more than 8.9 million people on the dark web, saying they face a lifetime risk of having their identities stolen.”
–David Minsky for Law 360
[June 16th, 2023]
If you are still using paper records, don’t change now.
Today’s electronic media makes physician-patient communication possible; yet there is another kind of intimacy. ICTs—information and communication technologies—enable 24/7 monitoring of basic information such as blood pressure, glucose levels, pulse, and respiration, etc.
Example:
In one study, an ICT not only made it easier for patients to stay in touch with their doctors, the outcomes were also significantly better.[i] Today, Hippocrates is no longer trailing patients around the house to keep track of their snacks and moods. But Hippocrates has gone digital in the form of a wearable device that records subtle changes in biological markers and communicates them instantaneously to a health provider.
While this is obviously a great advance, we suggest you pause for a moment before plugging in.
Why?
ICTs and social media tools can make a difference to one of the most important dimensions—physiological outcomes. But you can have the latest interactive technology at your disposal and still fail to be connected.
Example:
A story that a friend told me shows how.
***
One morning, her elderly father was touching up the paint on his sailboat. Nearby, another boat-owner, who happened to be an emergency medical technician, noticed her father was struggling to breathe and that his lips had turned purple. A trip to the local community hospital led to a barrage of high-tech tests and procedures, a diagnosis of emphysema, later complications with cerebral hematomas, and hospitalizations and re-hospitalizations that brought him into contact with a neurologist, a neurosurgeon, a cardiologist, and a pulmonologist.
Throughout her father’s medical ordeal, the team of specialists stayed in touch with each other and the primary care physician via various electronic media. But one person remained out of the loop—her father. One day, six months into the experience, the primary care physician phoned our friend’s mother to check on his patient. Her father recalls thinking, “Why was he calling her?”
The physician was communicating, but he was emotionally disconnected.
***
The Moral
The moral of the story: communication needs to be patient-centered in both electronic and psychological terms. That means understanding how someone likes to communicate and making sure the medium fits the message. Electronic media are just part of the equation. The other is the doctor-patient relationship. Once a relationship is established, it may be fine to use e-mail to send information about dosage.
But, delivering a new diagnosis may require the extra effort of scheduling a phone call or a face-to-face visit. Today, since you have so many Health 2.0 choices, it takes some effort to select the right way to communicate in a particular situation.
Use the Right Relationship Strategy
A colleague recently shared another story about an encounter with a specialist.
Example:
***
After an examination for a minor ailment, he was told that there might be a medicated lotion that could ameliorate his condition. The doctor thought for a moment, then swiveled around to the computer on his desk. As our colleague watched the screen, his physician typed a few words into a search engine. Up popped a list and he wrote out a script. “Try this,” his doctor concluded. “I think it will help.”
It did, almost overnight.
***
The Moral
Even though his physical problem had disappeared completely, our colleague felt there was something missing in the interaction. “It bothered me that my doctor turned to the Web for help at that moment. He found a cure, but I felt he wasn’t paying attention to me.”
The physician is supposed to be an authority who has a special relationship to the patient. “Anybody can Google,” our colleague complained. Was he being unreasonable? Maybe.
But; this story tells us something important about technology—it cuts both ways.
***
***
Assessment
Everyone has their own preferences when it comes to how they want to interact with each other and with technology. If these preferences are explicit and aligned, the chances for a productive partnership are high. The preferences, however, are many and complex. You can easily get lost in the tangled thicket of interpersonal styles and virtual mediums.
In the Web 2.0 environment, it helps to narrow down the endless choices to just a few options.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
DEFINITION: According to the Food and Drug Administration [FDA], the broad scope of digital health includes categories such as mobile health (mHealth), health information technology (IT), wearable devices, tele-health and tele-medicine, and personalized medicine. From mobile medical apps and software that support the clinical decisions doctors make every day to artificial intelligence and machine learning, digital technology has been driving a revolution in health care. Digital health tools have the vast potential to improve our ability to accurately diagnose and treat disease and to enhance the delivery of health care for the individual. Digital health technologies use computing platforms, connectivity, software, and sensors for health care and related uses. These technologies span a wide range of uses, from applications in general wellness to applications as a medical device. They include technologies intended for use as a medical product, in a medical product, as companion diagnostics, or as an adjunct to other medical products (devices, drugs, and biologics). They may also be used to develop or study medical products.
As many investors predicted, digital health funding took a dive in 2023, according to Rock Health’s year-end funding report. Startups got creative to stay afloat but many digital health founders will have to “face the music” in 2024, the VC firm’s analysts say.
Editor’s Note: I am on the Advisory Board of Medblob™a start-up based in Boston, MA. The digital mission of Medblob™ is to improve community and national health by allowing patients to better manage their health, providers to better treat their patients, and researchers to have the best information to discover cures to the most prevalent and pernicious diseases.
Kentucky-based healthcare provider NortonHealthcare has confirmed that it has suffered a significant ransomware attack that may have put the data of millions of its patients at risk. In a filing to the Maine Attorney General on December 8th, the healthcare giant said that 2.5 million individuals had been affected by the breach.
***
***
Meanwhile, the nation’s largest pharmacy chains have handed over Americans’ prescription records to police and government investigators without a warrant, a congressional investigation found, raising concerns about threats to medical privacy. Though some of the chains require their lawyers to review law enforcement requests, three of the largest — CVS Health, Kroger and Rite Aid, with a combined 60,000 locations nationwide — said they allow pharmacy staff members to hand over customers’ medical records in the store.
The policy was revealed in a letter sent to Xavier Becerra, the secretary of the Department of Health and Human Services, by Sen. Ron Wyden (D-Ore.) and Reps. Pramila Jayapal (D-Wash.) and Sara Jacobs (D-Calif.).
HIPAA anyone?
***
Here’s where the major benchmarks ended:
The S&P 500 index was up 21.26 points (0.5%) at 4,643.70; the Dow Jones Industrial Average®(DJI) was up 173.01 points (0.5%) at 36,577.94; the NASDAQ Composite® (COMP) was up 100.91 points (0.7%) at 14,533.40.
The 10-year Treasury note yield (TNX) was down about 3 basis points at 4.206%.
The CBOE® Volatility Index (VIX) was down 0.56 at 12.07.
Technology shares were among Tuesday’s strongest performers despite a 12% drop in Oracle (ORCL), which plunged after reporting lighter-than-expected quarterly revenue late Monday. The Philadelphia Semiconductor Index (SOX) posted its highest close since January 2022.
Financial shares were also firm. Energy shares were under pressure because WTI Crude Oil futures (/CL) extended a slump below $70 per barrel and settled at its lowest price since late June.
Posted on October 12, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
By Darrell Pruitt DDS
***
***
Even though the American Dental Association officially disagrees, if you haven’t adopted electronic dental records, now is not the time.
“Ransomware attack threatens to expose McLaren Health patient data” – Michigan Attorney General Dana Nessel notes: “This attack shows, once again, how susceptible our information infrastructure may be”. Organizations that handle our most personal data have a responsibility to implement safety measures that can withstand cyber-attacks and ensure that a patient’s private health information remains private.”
I’d give it a few more years. Otherwise, your digital records could be the cause of your bankruptcy.
***
Ransomware hits small businesses too
Business Tips from SCORE: Hackers focusing on small businesses. Here’s how to protect yourself, by Marc L. Goldberg for Cape Cod Times, October 8, 2023.
“Ransomware is the type of malware that has been on the rise over the last couple of years. After the ransomware infects the device, you’ll know right away. It encrypts files (or parts of the infrastructure) and displays the ransom message on the screen of the victim. Some strains can steal data making the organization vulnerable. Those that are most vulnerable gather and store lots of data — health care, insurance, banking and credit card providers.”
If a dental office is hacked, and it becomes known in the community that patients’ identities are appearing on the dark web, it is likely to cause bankruptcy.
Costly problem. Cybersecurity is the ultimate risk factor: In 2023, the average cost of a data breach worldwide was $4.45 million, marking a 15% increase in the last three years, according to a 2023 IBM report.
EDITOR’SNOTE: Dr. Zubin Damania, MD is a UCSF/Stanford-trained hospital doctor and host of The ZDoggMD Show, dedicated to Alt-Middle sense-making in healthcare and beyond. Videos are informational and are not medical advice, more info: https://zdoggmd.com/terms
Posted on July 31, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
By Darrell Pruitt DDS
***
***
“Regardless whether you are a physician, dentist or optometrist, they are coming for your patients’ records, Doc.” Family Vision of Anderson Data Breach Leaks Social Security Numbers of Up to 62,631 Patients
On July 26, 2023, Family Vision of Anderson filed a notice of data breach with the Attorney General of Maine after a ransomware attack exposed confidential patient information to unauthorized access. In this notice, Family Vision explains that the incident resulted in an unauthorized party being able to access patients’ sensitive information, which includes their first and last names, dates of birth, Social Security numbers, driver’s license numbers, addresses, telephone numbers, email addresses, genders, health insurance information, and protected health information.
Upon completing its investigation, Family Vision began sending out data breach notification letters to all individuals whose information was affected by the recent data security incident.
“Twenty-one percent of organizations stated that ransomware is now specifically excluded from their policies, and those with cyber insurance saw changes in their last policy renewals: 74% saw increased premiums, 43% saw increased deductibles, 10% saw coverage benefits reduced.” From “Ransomware is being excluded from cyber insurance policies”
Posted on June 5, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
WHAT IT IS?
By Staff Reporters
***
***
FORMAL DEFINITION:
According to Wikipedia, Health informatics is the field of science and engineering that aims at developing methods and technologies for the acquisition, processing, and study of patient data, which can come from different sources and modalities, such as electronic health records, diagnostic test results, medical scans. The health domain provides an extremely wide variety of problems that can be tackled using computational techniques.
‘Clinical informaticians’ are qualified health and social care professionals and ‘clinical informatics’ is a subspecialty within several medical specialties.
What does it mean to be a medical or healthcare informaticist practitioner?
A medical or healthcare informaticist works to improve how we use information to improve health and healthcare. You can have medical informaticists who are of various specialties, like a nurse informaticist, dentist informaticist. There is even a board certification level in clinical informatics. Improving healthcare also means improving the work of healthcare professionals—not just improving patients’ health, but making things easier for physicians, nurses, and all the various healthcare workers.
What kind of information do MI and HI clinicians deal with?
Patient information that’s stored in our electronic health record (EHR). A lot of the work we do is just making sure that information is showing up in the right places and that it’s flowing from other sources—whether through referrals or the lab system or radiology—then making sure it’s easy to find and easy to use by treating clinicians.
Posted on October 4, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Darrell Pruitt DDS
***
***
“Small- and medium-sized businesses with two to 200 employees suffered the most attacks during the period, accounting for 46%, or 2,300 ransomware attacks total, according to the report.” That’s us, Doc. Patterson and Schein won’t admit it, but if you don’t put patients’ information on a computer, you and your patients are completely safe from ransomware.
“US organizations hit by almost half of all ransomware since 2020 – American exceptionalism extends to ransomware as organizations based in the U.S. suffered the greatest number of attacks, ahead of Canada and the U.K.”
By Matt Kapko: Cybersecurity Dive, Sept. 28, 2022.
Paper’s security – “Report: 90% of companies affected by ransomware in 2022 – An annual SpyCloud survey found that 90% of organizations were impacted by ransomware over the past twelve months, an alarming increase from last year’s 72.5%.”
Posted on October 2, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
ADVERTISEMENT
Whither the “Dictionary of Health Information Technology and Security?”
A simple query that demands a cogent answer!
There is a myth that all stakeholders in the healthcare space understand the meaning of basic information technology jargon. In truth, the vernacular of contemporary medical information systems is unique, and often misused or misunderstood. It is sometimes altogether confounding.
Terms such as, “RSS”, “eHRs”, “DRAM”, “ROM”, “USB”, “PDA”, “NPI”, “CCHIT”, and “DNS” are common acronyms, but is their meaning AND functionality truly understood?
We appreciate the support of our sponsors. So, click-on on the links below and review all dictionary products.
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on June 26, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Darrell K. Pruitt DDS
***
***
“We’re now truly in the era of ransomware as pure extortion without the encryption – Why screw around with cryptography and keys when just stealing the info is good enough”
Posted on June 17, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Darrell K. Pruitt DDS
***
***
Some say e-prescriptions are a swell idea for dentists!
“Over 70% of organizations suffered two or more ransomware attacks in the past 12 months – According to the data presented by the Atlas VPN team based on a Veeam 2022 Ransomware Trends Report, 73% of organizations suffered two or more ransomware attacks in the past 12 months. The majority — 44% of ransomware infections entered through phishing emails, links, and websites. In total, 35% of organizations experienced two ransomware attacks, nearly a quarter (24%) endured three, close to a fifth (9%) of companies had four, and 4% went through five. Meanwhile, 1% of organizations suffered six or more ransomware attacks in the past 12 months. The remaining 27% of organizations faced only one ransomware attack.” By Acrofan, June 15, 2022. https://us.acrofan.com/detail.php?number=679260
“Why Ransomware Extortion is a Threat – In a typical ransomware extortion scheme, files are not only encrypted, but are also copied and exfiltrated from the network. Then, when the time comes to demand payment, hackers also say that if the business doesn’t meet their ransom demands within a given timeframe, they will publish the stolen files, or undertake some other activity to harm the business, such as a DDoS attack. This is known as double, or even triple extortion, with threats to release confidential information to the public, disrupt internet access or inform customers, shareholders or other partners about the incident unless they pay the ransom. It puts more pressure on businesses to make a quick decision, boosts the odds of criminals getting a big payout and increases the number of risks firms are exposed to, so this type of ransomware is something every firm should be concerned about.” By Brenda Robb for Security Boulevard on June 15, 2022. https://securityboulevard.com/2022/06/why-ransomware-extortion-is-a-threat/
It is also worth noting that if a dentist suffers a ransomware attack, HIPAA demands that all affected patients be notified that their identities might have been breached and might show up on the internet. If the breach involves 500 or more records, a description of the incident must be reported in the local media. This could easily bankrupt a practice even before the ransom is paid. What’s more, from the increasing numbers of data breaches that are occurring, one can surmise that dentists are not obeying the law … not yet.
Posted on May 17, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Staff Reporters
***
***
4 Takeaways from HIMSS
• 84% of respondents say their organizations require them to use digital health tools and most clinicians see the value in digital transformation. • 99% of leaders in U.S.-based health systems say it is important for their organizations to invest in digital transformation and 95% of international health system leaders agree. • 93% of international payer respondents and 74% of U.S. payers say their organizations have a team focused on digital transformation. • 80% of health system leader respondents in the U.S. think that a physician visit deserves to be reimbursed at the same or higher levels than an in-person visit.
NOTE: The Healthcare Information and Management Systems Society is an American not-for-profit organization dedicated to improving health care in quality, safety, cost-effectiveness and access through the best use of information technology and management systems.
Posted on May 6, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Advancing Medical Practice Success with Strategic Relationships
By Staff Reporters
To be efficient in healthcare delivery today, doctors must partner and understand the resources and affiliations that are available to them. Here is a brief list of several healthcare trade associations and leading industry vendors submitted for your review.
AHIMA
The American Health Information Management Association (AHIMA) is the premier association of health information management professionals. AHIMA’s 51,000 members are dedicated to the effective management of personal health information needed to deliver quality healthcare to the public. Founded in 1928 to improve the quality of medical records, AHIMA is committed to advancing the health information management profession in an increasingly electronic and global environment through leadership in advocacy, education, certification, and lifelong learning.
EHRA
HIMSS EHRA is a trade association of Electronic Health Record (EHR) vendors that addresses national efforts to create interoperable EHRs in hospital and ambulatory care settings. HIMSS EHRA operates on the premise that the rapid, widespread adoption of EHRs will help improve the quality of patient care and the productivity of the healthcare system. The primary mission of the association is to provide a forum for the EHR vendor community relative to standards development, the EHR certification process, interoperability, performance and quality measures, and other EHR issues that may become the subject of increasing government, insurance and physician association initiatives and requests.
HIMSS
HIMSS (Healthcare Information and Management Systems Society) is the healthcare industry’s membership organization exclusively focused on providing leadership for the optimal use of healthcare information technology and management systems for the betterment of human health. Founded in 1961 with offices in Chicago, Washington D.C., and other locations across the country, HIMSS represents approximately 17,000 individual members and some 275 member corporations that employ more than 1 million people. HIMSS frames and leads healthcare public policy and industry practices through its advocacy, educational and professional development initiatives designed to promote information and management systems’ contributions to ensuring quality patient care.
HITSP
The Healthcare Information Technology Standards Panel serves as a cooperative partnership between the public and private sectors for achieving a widely accepted and useful set of standards specifically to enable and support widespread interoperability among healthcare software applications, as they will interact in a local, regional, and national health information network for the United States. Comprised of a wide range of stakeholders, the Panel will assist in the development of the U.S. Nationwide Health Information Network (NHIN) by addressing issues such as privacy and security within a shared healthcare information system. The Panel is sponsored by the American National Standards Institute (ANSI) in cooperation with strategic partners such as the Healthcare Information and Management Systems Society (HIMSS), the Advanced Technology Institute (ATI), and Booz Allen Hamilton. Funding for the Panel is being provided via the ONCHIT contract award from the U.S. Department of Health and Human Services.
HL7
Health Level Seven is an American National Standards Institute (ANSI)-accredited Standards Developing Organization (SDO) operating in the healthcare clinical and administrative data arena. It is a not-for-profit volunteer organization made up of providers, vendors, payers, consultants, government groups, and others who develop clinical and administrative data standards for healthcare. Health Level Seven develops specifications; the most widely used being a messaging standard that enables disparate healthcare applications to exchange keys sets of clinical and administrative data.
MSHUG
Microsoft Healthcare Users Group (MS-HUG) unified with the Healthcare Information and Management Systems Society (HIMSS) as part of the HIMSS Users Group Alliance Program in October 2003. The unification strengthens the commitment of HIMSS and MS-HUG to better serve their members and the industry through a shared strategic vision to provide leadership and healthcare information technology solutions that improve the delivery of patient care.
WEDI
The Workgroup for Electronic Data Interchange [WEDI’s] goal is to improve the quality of healthcare through effective and efficient information exchange and management. They aim to provide leadership and guidance to the healthcare industry on how to use and leverage the industry’s collective knowledge, expertise, and information resources to improve the quality, affordability, and availability of healthcare.
Assessment
As the health information technology industry evolves, we will continue to contribute our expertise to foster ideas that shape the future of healthcare by offering more examples similar to the above.
Conclusion
And so, your thoughts and comments on this Medical Executive-Post are appreciated. Who did we miss? Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on March 28, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
SAD
[By staff reporters]
***
***
***
***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
Recent advances in biomedical and health sciences—from immunotherapy to treat cancer, to the highly effective COVID-19 vaccines—demonstrate the strengths and successes of the U.S. biomedical enterprise. Such advances present an opportunity to revolutionize how to prevent, treat, and even cure a range of diseases including cancer, infectious diseases, Alzheimer’s disease, and many others that together affect a significant number of Americans.
To improve the U.S. government’s capabilities to speed research that can improve the health of all Americans, President Biden is proposing the establishment of the Advanced Research Projects Agency for Health (ARPA-H). Included in the President’s FY2022 budget as a component of the National Institutes of Health (NIH) with a requested funding level of $6.5B available for three years, ARPA-H will be tasked with building high-risk, high-reward capabilities (or platforms) to drive biomedical breakthroughs—ranging from molecular to societal—that would provide transformative solutions for all patients.
Posted on January 28, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
According to reporter Neal Freyman, Tech giant Oracle said it’s paying $28.3 billion to buy electronic medical records company Cerner, because anything that makes paperwork less excruciating seems like a savvy business play.
Oracle is known for being aggressive with acquisitions (it even rallied a group to try and buy TikTok last year), but Cerner is Oracle’s biggest purchase in its history. The deal is further evidence that health care is “on par with banking in terms of the importance to our future,” as cofounder Larry Ellison told analysts earlier this month.
In Cerner, Oracle will get the Klay Thompson of the electronic medical records market—a very influential player, but in second place behind Epic, which owns a 31% market share.
Bottom line: Big tech companies see a golden opportunity in bringing the health care industry to the cloud, given its size (health care spending accounts for almost 20% of US GDP), and its old-school record-keeping process. A Mayo Clinic study cited by Oracle showed that doctors and nurses spend an average of 1–2 hours on desk work for every hour they take to see patients.
Posted on December 15, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
What to do to mitigate risk
[By Shahid N. Shah MS]
It is a common scenario that the hardware and electronic media are re-used instead of being simply disposed. They can be reused either internally within the healthcare organization or they can be resold or donated to other organizations/individuals.
Whatever may be the nature of reuse, it is important that all ePHI are completely erased using official government approved wiping methods, before it is given out for re-use. If this is not done, there are fairly high chances of the data being exposed and there by compromising ePHI.
Major Mitigation
Specific policies and procedures needs to be defined which clearly provides guidelines on the measures to be adopted when hardware or electronic media are reused. Often the risks associated with internal reuse of these media are overlooked, and as such there are no guidelines. Even if it is internal reuse, the same level of risks associated with unauthorized access exists here.
Secondary Mitigation
Policies and procedures which advocates the use of logs and book keeping for these reuse would help to track these media in a better way.
Success criteria
Audit of the logs and book keeping records will provide the information on whether the policies are being followed. And, the risk assessment report will give a clearer picture whether this risk has been mitigated or not.
***
***
ABOUT
Mr. Shahid N. Shah is an internationally recognized healthcare thought-leader across the Internet. He is a consultant to various federal agencies on technology matters and winner of Federal Computer Week’s coveted “Fed 100″ Award, in 2009. Over a twenty year career, he built multiple clinical solutions and helped design-deploy an electronic health record solution for the American Red Cross and two web-based eMRs used by hundreds of physicians with many large groupware and collaboration sites. As ex-CTO for a billion dollar division of CardinalHealth, he helped design advanced clinical interfaces for medical devices and hospitals. Mr. Shah is senior technology strategy advisor to NIH’s SBIR/STTR program helping small businesses commercialize healthcare applications. He runs four successful blogs: At http://shahid.shah.org he writes about architecture issues; at http://www.healthcareguy.com he provides valuable insights on applying technology in health care; at http://www.federalarchitect.com he advises senior federal technologists; and at http://www.hitsphere.com he gives a glimpse of HIT as an aggregator. Mr. Shah is a Microsoft MVP (Solutions Architect) Award Winner for 2007, and a Microsoft MVP (Solutions Architect) Award Winner for 2006. He also served as a HIMSS Enterprise IT Committee Member. Mr. Shah received a BS in computer science from the Pennsylvania State University and MS in Technology Management from the University of Maryland.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on August 29, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
EMR OVERVIEW
BY ERIC BRICKER MD
Electronic Medical Records (EMRs) are Used by 80-90% of Hospitals and Physician Practices. One Study Found that EMRs Have Lowered Patient Mortality by 0.09%.
Posted on July 2, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
ELECTRIC HEALTH RECORDS
By White Hat Anonymous
Epic Systems, the country’s leading e-health record company, says an algorithm it developed can accurately flag sepsis in patients 76% of the time. The life-threatening disease, which arises from infections, is a major concern for hospitals: One-third of patients who die in hospitals have sepsis, per the CDC.
Generally, the earlier sepsis is diagnosed and treated, the better a patient’s chances of survival—and hundreds of hospitals use Epic Systems’s sepsis prediction model, The Verge reports.
The problem: According to a study published this week in JAMA Internal Medicine, Epic Systems may have gotten the success rate wrong: The model is only correct 63% of the time—“substantially worse than the performance reported by its developer,” the researchers wrote.
Part of the issue can be traced to the algorithm’s development, Stat News reports. It was trained to flag when doctors would submit bills for sepsis treatment—which doesn’t always line up with patients’ first signs of symptoms.
“It’s essentially trying to predict what physicians are already doing,” Dr. Karandeep Singh, study author.
When reached for comment, Epic Systems told us the researchers’ hypothetical scenario lacked “the required validation, analysis, and tuning that organizations need to do before deployment,” adding that the JAMA study’s findings differed from other research.
Posted on March 7, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
LAUGHTER
By staff reporters
Laughter is a physical reaction in humans consisting usually of rhythmical, often audible contractions of the diaphragm and other parts of the respiratory system resulting most commonly in forms of “hee-hee” or “ha-ha”.
Posted on February 1, 2019 by Dr. David Edward Marcinko MBA MEd CMP™
OR … Not!
[By staff reporters]
A Medical Office Exam – FROM THIS EMR VISIT!
Your privacy is not protected.
We use Electronic Health Records.
[Courtesy Dr. DK Pruitt]
A Medical Office Exam – TO THIS PMR VISIT!
***
Assessment
Beware – No medical specialty is immune! Which office visit style do you prefer? Are we “Back to the Future?”
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
Posted on January 2, 2018 by Dr. David Edward Marcinko MBA MEd CMP™
EMRs – Providers Need to Prepare for Virulent Ransomware in 2018
[By staff reporters]
Ransomware emerged as a significant threat on the worldwide stage in 2017, but new variants will challenge healthcare providers well into 2018, with some versions of new malware not even needing a network to distribute themselves throughout an organization. Previous variants of ransomware, particularly the WannaCry attack in May, showed the ability to self-propagate and spread across a network and onto other networks via the Internet.
Educating a healthcare’s organization workforce on cyberattacks is necessary, but it’s not enough to bring them up to speed on phishing and other threats. Practices need to harden their own email systems; for example, Matt Sherman, a malware outbreak specialist at Symantec, advises using secure email systems as a best practice along with two-factor authentication software. Email systems should scan links contained in incoming messages, and they should enable automatic image loading in messages.
Source: Joseph Goedert, adapted from Health Data Management [12/28/17]
***Courtesy: FunnyBones
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
Posted on June 25, 2017 by Dr. David Edward Marcinko MBA MEd CMP™
2015 … Really?
By Darrell K. Pruitt DDS
***
“By 2015, health care is scheduled to be chartless. The federal National Health Information Infrastructure (NHII) is already formulating the parameters for this future. Chartless records are not a choice. The year 2015 is less than seven years away. We have seen hospitals, physicians’ offices, and other health-care providers moving in this direction.
In dentistry, only about 25% of practices are using computers chairside and only 1% is chartless. The American Dental Association is taking a proactive role in NHII. Individual dentists must also take part in the coming changes or once again be victims to others’ choices.”
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on August 11, 2016 by Dr. David Edward Marcinko MBA MEd CMP™
Paper is Safer!
[By Darrell K. Puitt DDS]
“Ransomware Attacks Can’t Hide from HIPAA Anymore – Hospital and health system executives are on notice: Come clean about ransomware attacks as early as possible or be prepared to face sanctions.”
By Scott Mace, for HealthLeaders Media, July 19, 2016.
Dean Sittig, a clinical informatics professor at University of Texas Health Science Center and the Houston UT-Memorial Hermann Center for Health Care Quality and Safety, tells HealthLeaders,
“The new HHS guidance is going to really ratchet up people’s attention, because now you’re also talking about big fines from the government, as well as the effects of the ransomware.”
***
***
Show Me the Money?
“Survey: Nearly Three Quarters of Physicians Say They Haven’t Seen ROI From Electronic Records.”
By Matt Goodman: [Dallas/Fort Worth Healthcare Daily, July 21, 2016]
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on March 30, 2016 by Dr. David Edward Marcinko MBA MEd CMP™
OCR pays its own way
Submitted By Darrell Pruitt DDS
“OCR unleashes second wave of HIPAA audits, but will it diminish patients’ privacy and security expectations?
Healthcare entities should expect the Office for Civil Rights to levy fines that help fund the program. And until OCR delivers a draft audit protocol breaches will continue at patients’ expense.”
Sullivan: “Here come the HIPAA audits. And even though OCR has yet to clearly outline what healthcare providers should expect exactly, one thing to anticipate is plenty of financial penalties.”
And David Harlow, a health lawyer, consultant and founder of The Harlow Group, tells HealthcareIT News,
“Who loses out as a result? Patients. The breaches continue, free credit monitoring services are offered, and we all move forward with a diminished expectation of privacy and security.”
***
***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
The best defense against any medical malpractice liability claim is a complete and accurate written or electronic record of the facts. In particular, medical malpractice claims will frequently be stalled or thwarted by a consistent written description of the symptoms you observe and the treatments you prescribe.
Extensive record keeping will not only help formulate a defense against a claim, but it will also (and perhaps more importantly) create the appearance that you are careful and highly competent in all of your affairs. Members of a jury may not be able to discern whether the medical judgments you made in a particular case were good or bad, as they do not have the years of education and training that you do.
***
***
Jurors can, however, sense whether your practice is organized and professional. If your records are thorough and consistent, jurors will assume that you dedicate as much attention to the substantive aspects of your work as you do to the tedium of recordkeeping. If you are active in the management of your office, you should keep track of its operations and establish logs for your employees to complete as they perform their daily tasks.
Assessment
Not all information, however, ought to be written down. Keep your written records to the facts you have observed and leave your speculations for department meetings.
And, is there an emerging movement back to paper medical records?
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
To understand the MR revolution that has occurred the past decade , place yourself for a moment in the position of third-party payer.
You want to know if Dr. Brown actually gave the care for which he is submitting a bill. You want to know if that care was needed. You want to know that the care was given to benefit the patient, rather than to provide financial benefit to the provider beyond the value of the services rendered.
Can you send one of your employees to follow Dr. Brown around on his or her office hours and hospital visits?
Of course not! You cannot see what actually happened in Dr. Brown’s office that day or why Dr. Black ordered a CAT scan on the patient at the imaging center. What you can do is review the medical record that underlies the bill for services rendered from Dr. Blue.
Most of all, you can require the doctor to certify that the care was actually rendered and was indicated. You can punish Dr. White severely if an element of a referral of a patient to another health care provider was to obtain a benefit in cash or in kind from the health care provider to whom the referral had been made [Stark Laws]. You can destroy Dr. Rose financially and put him in jail if his medical records do not document the bases for the bills he submitted for payment.
This nearly complete change in function of the medical record has precious little to do with the quality of patient care. To illustrate that point, consider only an office visit in which the care was exactly correct, properly indicated and flawlessly delivered, but not recorded in the office chart. As far as the patient was concerned, everything was correct and beneficial to the patient. As far as the third-party payer is concerned, the bill for those services is completely unsupported by required documentation and could be the basis for a False Claims Act [FCA] charge, a Medicare audit, or a criminal indictment. We have left the realm of quality of patient care far behind. Shall we change it back to the way it was? That is not going to happen.
***
***
Instead, practitioners must adjust their attitudes to the present function of patient records. They must document as required under pain of punishment for failure to do so. That reality is infuriating to many since they still cling to the ideal of providing good quality care to their patients and disdain such requirements as hindrances to reaching that goal. They are also aware of the fact that full documentation can be provided without a reality underlying it.
“Fine, you want documentation? I’ll give you documentation!”
Some have given in to the temptation of “cookbook” entries in their charts, or canned computer software programs, EHR [electronic medical record] templates, listing all the examinations they should have done, all the findings which should be there to justify further treatment; embedded “billing engines” not with-standing. We have personally seen records of physical examinations which record a patient’s ankle pulses as “equal and bounding bilaterally” when the patient had only one leg; hospital chart notes which describe extensive discussion with the patient of risks, alternatives and benefits in obtaining informed consent when the remainder of the record demonstrates the patient’s complaint that the surgeon has never told her what he planned to do; operative reports of procedures done and findings made in detail which, unfortunately, bear no correlation with the surgery which was actually performed.
***
***
Whether electronic medical records (EMR) will really be helpful, in the future, is still not known.
In fact, according to Ed Pullen MD, a board certified family physician practicing in Puyallup WA, electronic health records are defined primarily as repositories of patient data [much like paper records].
But, in the era of meaningful use [MU], patient-centered medical homes, and Accountable Care Organizations [ACOs], mere patient data repositories are not sufficient to meet the complex care support needs of clinical professionals. These complaints arise because EHR systems are being used as clinical care support systems, which means they should enhance the productivity of clinical professionals and support their information needs, not hinder them [personal communication, and DrPullen.com].
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
In the event of an emergency [likes now storm Jonas last week], a well defined contingency plan helps the team to allow for data restoration in addition to providing physical security. A contingency plan is usually used when there is an emergency, for example when there is an outage. During the crisis it is important that the doctors still have access to EMRs/ePHI so that the quality of care is not compromised.
Major Mitigation:
Based on the size of the physician’s practice, the contingency plans in place may vary. For small doctor’s offices, the whole staff may need to be involved in restoration. In the case of large physician practices, authorized personnel may need to be accompanied into the buildings by guards.
A contingency plan should be in place that ensures the right people have access to where the PHI is physically housed. This would mean that there needs to be procedures and processes that are well established so that in the case of an emergency, authorized people that have access can retrieve the PHI or even make a back up copy of the PHI data.
For example, this can mean bringing up the application in another data center if the primary data center housing the application becomes inaccessible. This should be done so that the physician’s have uninterrupted access to their patient’s PHI even in the event of an emergency.
Periodic third party audits of contingency plans and mock emergency drills can help ensure that this risk has been taken care of and mitigated.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on December 31, 2015 by Dr. David Edward Marcinko MBA MEd CMP™
An iMBA Inc., Review
***
[By Dr. David Edward Marcinko CMP®MBA]
***
As little as a hundred years ago, detailed medical records were likely to have been compiled by medical researchers such as Charcot and Hughlings-Jackson. The medical record was an aide memoire for detecting changes in patients’ conditions over time, solely for the benefit of the physician in treating the patient.
As health care became more institutionalized, medical records became a communications device among health care providers. Doctors made progress notes and gave orders. Nurses carried them out and kept a record of patient responses. A centralized record, theoretically, allowed all to know what each was doing. The ideal was that if the doctor were unable to care for the patient, another physician could stand in his or her shoes and assume the patient’s care.
***
***
Enter Third Parties
Then pressures from third party payers occurred. As insurance and then government programs became larger players in the compensation game, they wanted to know if the care they were paying for was being delivered efficiently.
Why were these tests ordered?
Why weren’t these studies done?
Why had the patient remained hospitalized after his temperature had returned to normal for so many hours and no pain medications had been required?
Why couldn’t this pre-operative work be done on an outpatient basis?
Though the real push behind these questions was the desire to save money, utilization review also directly contributed to better patient care. A patient who was being given inefficient care was getting substandard care as well. Utilization review was mainly retrospective; denial of compensation was rarely imposed, and suasion by peers was the main effector of change. Though “economic credentialing” was shouted about, it rarely showed itself in public.
PP-ACA
Even health reform which openly admitted economic incentives as one of its motivators preferred to find some other reason for deciding not to reimburse, or admit Dr. Jones to its narrow panel of ACA, or other “skinny” network providers, or not renewing Dr. Smith’s contract an HMO. The medical record remained essentially a record of patient care which was good or not, efficient or not. If the record wasn’t complete, the doctor could always supplement it with an affidavit, use information from somewhere else, or provide explanations.
***
***
Socio Economic Status
Today, the concept known as Socio Economic Status [S.E.S.] is conceptualized as the social standing, or class of an individual or group. It is often measured as a combination of education, income and occupation. Examinations of socioeconomic status often reveal inequities in access to medical resources, plus issues related to privilege, power and control. SES is increasingly being considered as another payment component [CPT® codes] to medical providers, as reflected in the paper medical record, EMR and elsewhere.
Assessment
Have you encountered any Socio Economic Status initiative in your clinic, hospital or other medical institution?
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on June 5, 2015 by Dr. David Edward Marcinko MBA MEd CMP™
Used by 91% of doctors according to research2guidance
By Ralf Jahns
Denmark emerges as the number one country to start an mHealth business according to a survey conducted by research2guidance in partnership with HIMSS Europe. Over 5000 app developers, healthcare professionals and mHealth practitioners took part in the “European mHealth App Market Ranking” survey, where participants were asked to rank the mHealth App market readiness of the 28 EU member states. The results were recently revealed by Ralf Jahns, Managing Director at research2guidance, during the HIMSS Europe event in Riga, the mHealth Summit, on 12th May 2015.
The results, which establish Denmark as having the best market pre-requisites needed for an mHealth business, are based on the average of the scores in five categories: eHealth adoption, level of digitalisation, market potential, ease of starting an mHealth business and mHealth regulatory framework. Hans Erik Henriksen, CEO of Healthcare Denmark commented on the survey findings: “Denmark has a very digitalised society and is familiar with using technology in healthcare, supported by a regulatory framework. The research2gudiance and HIMSS Europe survey confirms the progress we are making. I sincerely hope that this will inspire the European countries and mHealth community in their efforts to progress mobile solutions, which will make a big difference for our citizens”. Denmark ranked top country for eHealth adoption being the only country where exchanging patients’ medical data electronically is used amongst 91% of doctors, whereas the average of other covered countries is only 34%
In terms of market attractiveness and healthcare investments, Denmark is at the top in the mHealth market potential category, together with Austria which also has one of the highest expenditures for health. The ease of starting mHealth business category describes how easy it is to start and maintain a new business based on the number of days needed to start business, the number of necessary start-up procedures to register a business and the level of tax and, in this case, Denmark also ranked extremely high, as the smaller countries – Ireland was also top in this category – tend to support new businesses better compared to larger countries. Rainer Herzog, General Manager at HIMSS Europe, added: “This year’s survey has revealed that the market conditions for mHealth which Denmark offers are truly remarkable. This has been the largest global mHealth research study to date and there are different learnings that could be drawn from the EU countries’ mHealth App Market Ranking. Ultimately though, although mHealth is still it is an emerging market, and a number of countries in Europe are currently in the process of defining their mHealth roadmaps, Denmark leads the way in all aspects”.
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on May 31, 2015 by Dr. David Edward Marcinko MBA MEd CMP™
About OpenNotes
[By Staff Reporters]
In an OpenNotes study, researchers examined the impact on patients and doctors when patients were allowed access to their doctors’ notes via a secure EHR Internet portal. Through the use of surveys, patients’ benefits, concerns, and behaviors, as well as physicians workload, were measured.
***
***
The Players
Beth Israel Deaconess Medical Center (BIDMC) in Boston, Geisinger Health System (GHS) in Pennsylvania, and Harborview Medical Center (HMC) in Seattle were selected for this quasi-experimental year-long study.
The Study
The study included 105 physicians and 13,564 of their patients. Patients were notified when their notes were available, but whether or not to open the note was at their own discretion. The authors analyzed both pre- and post-intervention surveys from the physicians who completed the study; 99 physicians submitted both pre- and post-intervention surveys. Of the patients who viewed at least one note, 41 percent completed post-intervention surveys.
***
***
The Results
Almost 99 percent of patients at BIDMC, GHS, and HMC wanted to have continued access to their visit notes at the completion of the study; no physician elected to end this practice. Although a limited geographic area was represented, the positive feedback and clinically relevant benefits demonstrate the potential for a widespread adoption of OpenNotes. Moreover, it may be a powerful tool in helping improve the lives of patients.
Citation: Inviting Patients to Read Their Doctors’ Notes: Author(s): Delbanco, T; Walker, J; Bell, SK and Darrer, JD et; al: American College of Physicians, Annals of Internal Medicine, October 2012.
***
***
Assessment
Open Notes, a grantee of the Robert Wood Johnson Foundation, was developed to demonstrate and evaluate the impact on both patients and clinicians of fully sharing (through an electronic patient portal) all encounter notes between patients and their primary care providers.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on April 28, 2015 by Dr. David Edward Marcinko MBA MEd CMP™
Tips on using strong passwords
[Securing yourself from a world of hackers]
By Shahid N. Shah MS
What is at Risk?
Here are some specific tools, gadgets, cloud servers, EHRs and other reasons you should secure your PWs:
Fax Server – a fax server allows you to centrally manage all incoming and outgoing faxes. Since most medical practices live on fax, this is one of the fastest investments you can recoup.
Shared drives – start using shared drives either using your existing software or you can purchase inexpensive “network disks” for a few hundred dollars to share business forms, online directories, reports, scanned charts, and many other files.
Online backups and Internet PACSstorage – there are online tools like JungleDisk.com that allow you to store gigabytes of encrypted data into the Internet “cloud” for just a few dollars a month.
E-mail (beware of HIPAA, though) – internal office messaging and email is a great place to start. If you haven’t started your office automation journey here you should. If you’re going to use it for patient communications you’ll need to make sure you have patient approvals and appropriate encryption. If you’re on Gmail today and you want to have customers immediately be able to communicate with you on Gmail, that’s generally HIPAA compliant because communications between two Gmail accounts stays within the Google data center and is not sent unencrypted over the Internet.
E-Prescribing – e-prescribing is a great place to start your automation journey because it’s a fast way to realize how much slower the digital process is in capturing clinical data. If e-prescribing alone makes you slower in your job, EMRs will likely affect you even more. If you’re productive with e-prescribing then EMRs in general will make you more productive too.
Office Online and Google Apps (scheduling, document sharing) – Google and Microsoft® have some very nice online tools for managing contacts (your patients are contacts), scheduling (appointments), dirt simple document management, and getting everyone in the office “on the same page”. Before you jump into full-fledged EMRs see if these basic free tools can do the job for you.
Modular clinical groupware – this is a new category of software that allows you to collaborate with colleagues on your most time-consuming or most-needy patients and leave the remainder of them as-is. By automating what’s taking the most of your time you don’t worry about the majority of patients who aren’t.
Patient registry and CCR bulletin boards – if you’re just looking for basic patient population management and not detailed office automation then patient registries and CCR databases are a great start. These don’t help with workflow but they do manage patient summaries.
Document imaging – scanning and storing your paper documents is something that affects everyone; all scanners come with some basic imaging software that you can use for free. Once you’re good at scanning and paper digitization you can move to “medical grade” document managements that can improve productivity even more.
Clinical content repository (CMS) – open source systems like DrupalModules.com and Joomla.org do a great job of content management and they can be adapted to do clinical content management.
Electronic lab reporting – if labs are taking up most of your time, you can automate that pretty easily with web-based lab reporting systems.
Electronic transcription – if clinical note taking is taking most of your time, you can automate that by using electronic transcribing.
Speech recognition – another “point solution” to helping with capturing clinical notes; you can get a system up and running for under $250.
Instant Messaging (IM) – IM gives you the ability to connect directly with multiple rooms within your office using free software; if you want, you can also connect with patients and other physicians during work hours.
How to avoid the most common and dangerous passwords?
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on April 5, 2015 by Dr. David Edward Marcinko MBA MEd CMP™
Taking Cloud Computing to a New Level
[By GE Healthcare IT]
American healthcare has by far the most expensive system in the world, but few would argue that it’s also the most efficient. A study published in the Journal of American Medical Association found that almost 40 percent of patients are misdiagnosed in primary care1. Another report by the American College of Physicians discovered that unnecessary testing and medical procedures, and extra days in the hospital caused by wrong diagnosis could add up to $800 billion per year2.
That’s close to a third of all U.S. healthcare costs. “There is a lot of waste in the system,” says Jeanine Banks, general manager of marketing at GE Healthcare IT. “We want to help rein in the costs and make the system far more efficient.”
That’s not just talk. Engineers at GE Healthcare IT are developing a new “cloud imaging” solution that will allow doctors to create a professional profile, store patient images and data together in one place, view 3D images from anywhere, and access intuitive analytics. “It’s like LinkedIn professional networking meets diagnostic imaging,” Banks says. “It’s all about virtually limitless computing, storage and collaboration on tough cases to help healthcare teams make more informed decisions.”
***
***
Banks says that the information physicians need to make diagnoses is often fragmented and sits in siloes. The new platform, GE’s Cloud Imaging solution, allows doctors to exchange images and use social digital tools to share cases with each other over a network instead of distributing CDs, as common practice now. “They can open their browser, click on a link and share quickly,” she says.
Banks says that GE intends to give hospitals the flexibility to host the system on their own servers, as a private cloud, or through GE’s public cloud environment. “We are committed to using industry standards to make it easy to connect medical devices, link with existing PACS (picture archiving and communication systems) and EMR (electronic medical records environments), and enable consistent access to a flourishing ecosystem of apps,” she says. “Providers don’t need more silos of data.” GE’s first Cloud Imaging pilot site is the Kadlec Health System in Washington State. Kadlec is helping evaluate the platform ahead of plans to demonstrate the new solution during the annual meeting of the Radiological Society of North America in December. “It’s an opportunity for them to use it inside their health system and give us feedback,” Banks says.
***
***
For Banks, this is the beginning of a new healthcare revolution. “What if together with industry we could help physicians reduce waste?” she asks. “We could process that information, learn from past diagnostic decisions and store the data all in the cloud to inform future decisions. One day, we could tap into knowledge based on cases from around the world.”
Assessment
That’s just brilliant.
Citations:
1 Journal of American Medical Association 2012
2 Reuter’s, citing study by American College of Physicians
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:

















































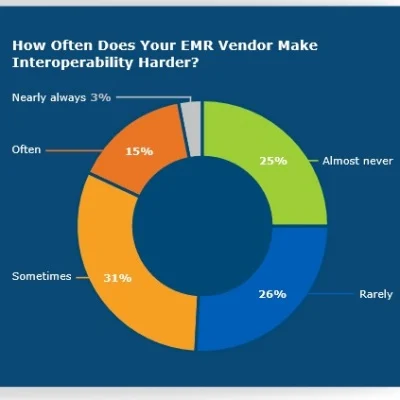











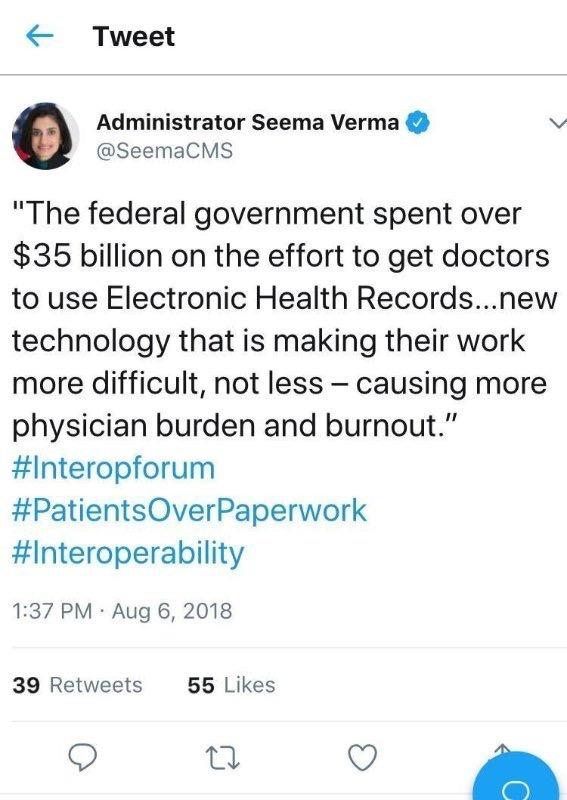
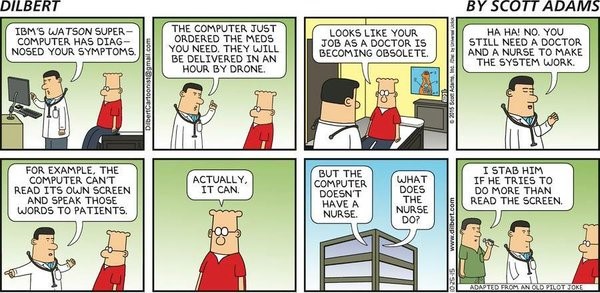














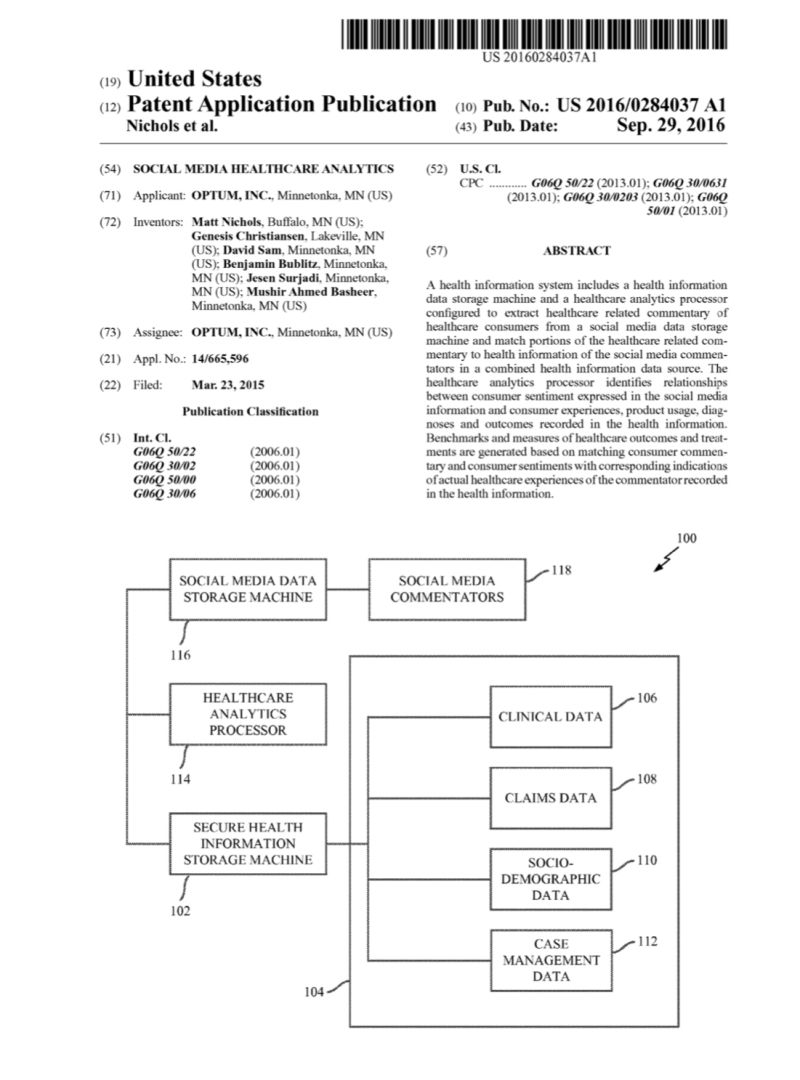 ***
***