BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] E-mail: MarcinkoAdvisors1738@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on April 11, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
On March 18, 2026, the House Energy and Commerce Committee’s Subcommittee on Health held its third hearing in an ongoing series on healthcare affordability, titled “Lowering Health Care Costs for All Americans: An Examination of the U.S. Provider Landscape.”
This Health Capital Topics article examines the key themes that emerged from the hearing, including the ongoing decline of independent physician practice, legislative approaches to Medicare physician payment reform, and the intensifying bipartisan scrutiny of hospital consolidation. (Read more…)
The phrase “Make America Healthy Again” captures a national aspiration that goes far beyond physical wellness. It speaks to a collective desire for strength, resilience, and unity at a time when the country faces complex challenges that touch every aspect of life. Health is not merely the absence of illness; it is the foundation of a thriving society. When people are healthy, communities flourish, economies grow, and the nation as a whole becomes more capable of meeting the demands of the future. Reimagining what it means to make America healthy again requires looking at health in its broadest sense—physical, mental, social, and environmental—and understanding how each dimension shapes the country’s long‑term vitality.
At the most basic level, physical health remains a central pillar of national well‑being. Chronic diseases, preventable conditions, and unequal access to care continue to affect millions of Americans. These issues are not just medical; they influence productivity, family stability, and economic opportunity. A healthier America begins with empowering individuals to take control of their well‑being through education, access to nutritious food, and environments that support active living. But personal responsibility alone is not enough. A society that values health must ensure that every person—regardless of income, geography, or background—has the tools and support needed to live a healthy life. This includes reliable healthcare, preventive services, and communities designed to promote wellness rather than hinder it.
Mental health is another essential component of a healthy nation. In recent years, conversations about stress, anxiety, depression, and burnout have become more open, reflecting a growing recognition that mental well‑being is inseparable from physical health. A country cannot thrive when large portions of its population feel overwhelmed, isolated, or unsupported. Making America healthy again means reducing stigma, expanding access to mental health resources, and fostering environments—schools, workplaces, and neighborhoods—where people feel safe, connected, and valued. When mental health is prioritized, individuals are better able to contribute to their families, communities, and the broader society.
Social health, though less frequently discussed, plays a powerful role in shaping national wellness. Strong communities are built on trust, cooperation, and shared purpose. Yet many Americans feel disconnected from one another, divided by political tensions, economic disparities, and cultural differences. Rebuilding social health requires creating spaces where people can come together, listen to one another, and work toward common goals. It means strengthening local institutions, supporting families, and encouraging civic engagement. When people feel connected, they are more likely to support one another, make healthier choices, and contribute to a more stable and compassionate society.
Environmental health is equally important. Clean air, safe water, and healthy ecosystems are not luxuries; they are prerequisites for human well‑being. Communities exposed to pollution or environmental hazards often experience higher rates of illness and reduced quality of life. Making America healthy again involves protecting natural resources, promoting sustainable practices, and ensuring that all communities—especially those historically overlooked—have access to safe, healthy environments. A nation that cares for its environment is ultimately caring for its people.
***
***
Economic health also intersects with personal and national wellness. When individuals struggle to afford housing, food, or medical care, their health inevitably suffers. A strong economy provides stability, opportunity, and the resources needed to invest in public health, education, and infrastructure. But economic health is not just about growth; it is about fairness and access. Ensuring that all Americans have the chance to succeed strengthens the entire nation and reduces the long‑term costs associated with poor health outcomes.
Ultimately, making America healthy again is not a single policy, program, or slogan. It is a mindset—a commitment to valuing human well‑being as the foundation of national strength. It requires collaboration across political lines, sectors, and communities. It asks individuals to take responsibility for their own health while also recognizing the importance of collective action. It challenges leaders to think long‑term and prioritize investments that support the physical, mental, social, and environmental health of the nation.
A healthy America is a more resilient America. It is a country where children grow up with opportunities, where adults can pursue meaningful lives, and where communities are strong enough to face challenges together. The path forward may be complex, but the goal is simple: a nation where every person has the chance to live a healthy, fulfilling life. That vision—rooted in dignity, opportunity, and shared purpose—is what it truly means to make America healthy again.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Redefining Access, Value and the Patient Experience
Concierge medicine has gained steady traction across many medical specialties, but its relevance to podiatry is especially compelling. Podiatrists sit at the intersection of primary care, chronic disease management, biomechanics, and minor surgical intervention. They often treat conditions that profoundly affect mobility, independence, and quality of life. Yet podiatry practices face the same pressures that challenge the broader healthcare system: shrinking reimbursements, rising administrative burdens, and patient panels that grow faster than the time available to serve them. Concierge medicine offers podiatrists a model that can restore time, autonomy, and depth to the patient relationship while elevating the standard of care.
At its core, concierge medicine replaces the high‑volume, insurance‑driven model with a membership‑based structure that allows clinicians to limit their patient load and provide more personalized, accessible care. For podiatrists, this shift can be transformative. Foot and ankle issues often require ongoing monitoring, detailed biomechanical assessments, and frequent follow‑ups. In a traditional practice, these needs can be difficult to meet when appointment slots are compressed into ten‑ or fifteen‑minute increments. Concierge podiatry, by contrast, allows for extended visits, same‑day access, and direct communication between patient and provider. This creates space for deeper evaluation, more thoughtful treatment planning, and a more collaborative approach to long‑term foot health.
One of the strongest arguments for concierge podiatry is the nature of the conditions podiatrists treat. Many patients struggle with chronic issues such as diabetic neuropathy, peripheral vascular disease, recurrent wounds, or structural deformities that require ongoing attention. These conditions do not resolve with a single visit; they evolve, fluctuate, and often require proactive management. In a concierge model, podiatrists can monitor these patients more closely, intervene earlier, and spend the time necessary to educate them about prevention and self‑care. This can reduce complications, improve outcomes, and foster a sense of partnership that is difficult to achieve in a high‑volume setting.
Concierge podiatry also aligns well with the growing emphasis on preventive care. Many foot and ankle problems—such as tendon injuries, stress fractures, or progressive deformities—develop gradually and can be mitigated with early intervention. A concierge structure allows podiatrists to conduct more comprehensive biomechanical evaluations, gait analyses, and footwear consultations. It also gives them the freedom to integrate services that are often squeezed out of traditional practice models, such as personalized orthotic management, fall‑risk assessments, or long‑term monitoring for athletes. Patients benefit from a more holistic approach that prioritizes prevention rather than simply reacting to acute problems.
***
***
Another advantage of concierge podiatry is accessibility. Foot pain can be debilitating, and delays in care often worsen the underlying condition. Concierge patients typically enjoy same‑day or next‑day appointments, direct messaging with their podiatrist, and the ability to address concerns quickly before they escalate. For individuals with diabetes, mobility limitations, or demanding schedules, this level of access can be invaluable. It also reduces reliance on urgent care centers or emergency departments, where foot issues may not receive specialized attention.
From the podiatrist’s perspective, concierge medicine offers a path to greater professional satisfaction. Many podiatrists enter the field because they enjoy building long‑term relationships and helping patients maintain mobility and independence. Yet the realities of insurance‑based practice—documentation requirements, declining reimbursements, and the pressure to see more patients in less time—can erode that sense of purpose. A concierge model restores control over scheduling, reduces administrative strain, and allows podiatrists to practice in a way that reflects their values. This can help prevent burnout and create a more sustainable career.
Of course, concierge podiatry is not without challenges. The most common criticism of concierge medicine in general is that it may limit access for patients who cannot afford membership fees. When a podiatrist transitions to a concierge model and reduces their patient panel, some individuals may need to seek care elsewhere. In communities with limited access to foot and ankle specialists, this can create gaps in care. Podiatrists considering this model must weigh the benefits of improved care for a smaller group of patients against the potential impact on the broader community.
Another challenge is determining which services are included in the membership fee and which remain billable through insurance. Podiatry encompasses a wide range of procedures—from routine nail care to surgical interventions—and patients may misunderstand what their membership covers. Clear communication is essential to avoid confusion and maintain trust. Some concierge podiatrists choose a hybrid model, where the membership fee covers enhanced access and preventive services, while procedures and surgeries are billed separately. Others opt for a fully cash‑based practice. Each approach has advantages, but all require transparency.
***
***
Despite these complexities, the potential for concierge medicine to elevate podiatric care is significant. As patients increasingly seek personalized, relationship‑driven healthcare, podiatrists are well positioned to offer a concierge experience that feels both meaningful and practical. Foot and ankle health is foundational to overall well‑being, and many patients are willing to invest in a model that prioritizes mobility, comfort, and long‑term function.
Looking ahead, concierge podiatry may continue to evolve in creative ways. Some practices may integrate wellness services such as physical therapy, nutrition counseling, or sports performance programs. Others may develop specialized concierge offerings for athletes, older adults, or individuals with diabetes. Technology may also play a role, enabling remote monitoring of gait, pressure distribution, or wound healing. The flexibility of the concierge model allows podiatrists to tailor their services to the unique needs of their patient population.
Ultimately, concierge medicine offers podiatrists an opportunity to reimagine how they deliver care. It provides a framework that values time, expertise, and human connection—elements that are often lost in traditional practice. While it may not be the right fit for every clinician or every community, it represents a powerful alternative for podiatrists who want to deepen their relationships with patients, enhance the quality of their care, and build a practice that reflects the true spirit of their profession.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The medical bundled payment system has emerged as one of the most significant shifts in modern healthcare financing, aiming to balance cost control with improved patient outcomes. Unlike the traditional fee‑for‑service model—where providers are paid for each individual test, visit, or procedure—bundled payments offer a single, predetermined payment for all services related to a specific episode of care. This episode might include a surgery, a chronic condition flare‑up, or a defined period of treatment. By restructuring financial incentives, bundled payments encourage coordination, efficiency, and quality in ways that fee‑for‑service simply does not.
At its core, the bundled payment system is designed to align the interests of patients, providers, and payers. Under fee‑for‑service, providers are rewarded for volume: more procedures generate more revenue. This can unintentionally promote unnecessary services and fragmented care. Bundled payments flip that logic. Providers receive a fixed amount for the entire episode, regardless of how many services are delivered. This encourages them to focus on what truly matters—delivering the right care at the right time, avoiding complications, and preventing avoidable re-admissions.
***
***
One of the most powerful effects of bundled payments is the incentive for care coordination. When multiple providers—surgeons, hospitals, rehabilitation centers, primary care physicians—share a single payment, they must work together to manage the patient’s journey. This collaboration can reduce duplication of services, streamline communication, and create a more seamless experience for patients. For example, in a joint replacement bundle, the orthopedic surgeon and hospital have a shared interest in ensuring that the patient receives appropriate pre‑operative education, avoids infections, and transitions smoothly to rehabilitation. If complications arise, the cost of addressing them comes out of the same fixed payment, motivating providers to prevent problems before they occur.
Bundled payments also encourage providers to adopt evidence‑based practices. Because the financial risk shifts partially to the provider, there is a strong incentive to use interventions that are proven to work and avoid those that add cost without improving outcomes. This can accelerate the adoption of clinical guidelines, standardized care pathways, and quality improvement initiatives. Over time, these changes can lead to more predictable outcomes and reduced variability in care—two hallmarks of a high‑performing healthcare system.
***
***
However, the bundled payment system is not without challenges. One concern is the potential for providers to avoid high‑risk patients who might require more resources than the bundled payment covers. To address this, many programs incorporate risk adjustment, ensuring that payments reflect the complexity of the patient population. Another challenge is the administrative burden of implementing bundled payments. Providers must invest in data analytics, care coordination infrastructure, and new management processes to track costs and outcomes across an entire episode of care. Smaller practices may struggle with these demands, potentially widening gaps between large, well‑resourced systems and smaller providers.
Despite these challenges, bundled payments represent a meaningful step toward value‑based care. They encourage a shift from reactive, fragmented treatment to proactive, coordinated management. Patients benefit from smoother care transitions, fewer complications, and a clearer understanding of their treatment plan. Payers benefit from more predictable costs and reduced waste. Providers benefit from the opportunity to innovate and redesign care delivery in ways that improve both quality and efficiency.
In many ways, the bundled payment system reflects a broader transformation in healthcare: a move away from paying for services and toward paying for outcomes. While not a perfect solution, it offers a compelling framework for aligning incentives and improving the overall value of care. As healthcare systems continue to evolve, bundled payments are likely to remain a central strategy in the pursuit of high‑quality, cost‑effective care.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The breakup of the Medical Act represents one of the most significant turning points in the evolution of modern healthcare governance. For decades, the Act served as a foundational framework that regulated medical practice, established professional standards, and defined the relationship between the state, medical institutions, and practitioners. Its dissolution did not occur suddenly; rather, it emerged from a complex interplay of political pressures, professional disputes, and shifting societal expectations. Understanding the breakup requires examining both the structural weaknesses within the Act itself and the broader forces that made its continuation untenable.
At its core, the Medical Act was designed to centralize authority over medical licensing and professional conduct. When it was first introduced, this centralization was seen as a necessary step toward ensuring uniform standards and protecting the public from unqualified practitioners. Over time, however, the rigidity of the Act became a source of tension. Medical knowledge expanded rapidly, new specialties emerged, and healthcare delivery became increasingly complex. Yet the Act remained anchored in assumptions that no longer reflected the realities of modern medicine. Many practitioners argued that the Act constrained innovation, limited professional autonomy, and failed to adapt to new models of care.
One of the major catalysts for the breakup was the growing dissatisfaction among medical professionals who felt that the Act imposed excessive bureaucratic oversight. Licensing procedures, disciplinary mechanisms, and continuing education requirements were often criticized as outdated or overly punitive. Younger practitioners, in particular, viewed the Act as an obstacle to entering the profession, citing long delays, inconsistent evaluation standards, and a lack of transparency. These frustrations fueled calls for reform, but attempts to revise the Act repeatedly stalled due to political disagreements and resistance from established institutions that benefited from the status quo.
Another factor contributing to the breakup was the increasing involvement of non‑physician healthcare providers in delivering essential services. Nurses, physician assistants, pharmacists, and other allied health professionals sought expanded scopes of practice to meet rising patient demand. However, the Medical Act was built around a physician‑centric model that did not easily accommodate these shifts. As collaborative care models became more common, the Act’s limitations became more apparent. Conflicts emerged over authority, responsibility, and professional boundaries, creating friction within the healthcare system. The inability of the Act to adapt to these new dynamics weakened its legitimacy and fueled arguments for its dissolution.
Public expectations also played a significant role. Patients became more informed, more vocal, and more demanding of accountability. They expected transparency in medical decision‑making, greater access to care, and more equitable treatment across communities. Yet the Medical Act was often criticized for protecting professional interests rather than prioritizing patient welfare. High‑profile cases involving malpractice, discrimination, or regulatory failures eroded public trust. Advocacy groups argued that the Act lacked sufficient mechanisms for patient representation and that its disciplinary processes were opaque and slow. As public pressure mounted, political leaders found it increasingly difficult to defend the existing framework.
***
***
The breakup of the Medical Act was ultimately driven by a convergence of these pressures. When reform efforts repeatedly failed, stakeholders began to explore alternative regulatory models. Some advocated for decentralization, arguing that regional or specialty‑specific bodies could respond more effectively to local needs. Others pushed for a more integrated system that would regulate all healthcare professionals under a unified framework, promoting collaboration and reducing duplication. The eventual dissolution of the Act opened the door to these new possibilities, though not without controversy.
The consequences of the breakup have been far‑reaching. On one hand, it created opportunities for modernization. New regulatory structures have been more flexible, more responsive to emerging trends, and more inclusive of diverse healthcare professions. Licensing processes have been streamlined, interdisciplinary collaboration has improved, and patient advocacy has gained a stronger voice in governance. Many practitioners feel that the new system better reflects the realities of contemporary healthcare and supports innovation rather than hindering it.
On the other hand, the transition has not been without challenges. The breakup initially created uncertainty, as practitioners and institutions navigated shifting rules and responsibilities. Some critics argue that decentralization has led to inconsistencies in standards, making it harder to ensure uniform quality of care. Others worry that the new system may lack the strong oversight mechanisms that once protected the public. Balancing flexibility with accountability remains an ongoing struggle, and debates continue over how best to regulate a rapidly evolving healthcare landscape.
In many ways, the breakup of the Medical Act symbolizes a broader transformation in society’s understanding of healthcare. It reflects a shift away from rigid, hierarchical models toward more dynamic, collaborative, and patient‑centered approaches. While the dissolution of such a longstanding framework inevitably brought disruption, it also created space for innovation and reform. The legacy of the Medical Act lives on in the structures that replaced it, shaped by the lessons learned from its strengths and its shortcomings.
Ultimately, the breakup was not merely a legal or administrative event; it was a reflection of changing values, expectations, and realities. As healthcare continues to evolve, the story of the Medical Act serves as a reminder that regulatory systems must remain adaptable, transparent, and responsive to the needs of both practitioners and the public.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Blinded medical payments have emerged as a compelling approach to addressing some of the most persistent challenges in modern healthcare systems. At their core, these payment structures are designed to separate the financial aspects of care from the clinical decision‑making process. By obscuring or “blinding” the cost of specific services from either the patient, the provider, or both, the model aims to reduce conflicts of interest, encourage unbiased medical judgment, and create a more equitable healthcare experience. Although the concept may seem counterintuitive in a system where transparency is often championed, blinded payments offer a nuanced strategy for improving trust, fairness, and outcomes.
One of the primary motivations behind blinded medical payments is the desire to minimize the influence of financial incentives on clinical decisions. In many traditional payment models, providers are acutely aware of the reimbursement rates associated with different procedures. This awareness can unintentionally shape treatment recommendations, even when clinicians strive to act solely in the patient’s best interest. Blinded payment systems attempt to remove this pressure by ensuring that providers do not know the exact compensation tied to each service. Without this knowledge, the theory goes, decisions are more likely to be guided by clinical need rather than financial reward. This can be particularly valuable in specialties where high‑cost procedures are common and where the potential for overuse is well documented.
Patients, too, can benefit from a degree of blinding. When individuals are confronted with detailed cost information at the point of care, they may feel compelled to make decisions based on price rather than medical necessity. This dynamic can lead to underuse of essential services, delayed treatment, or heightened anxiety during an already stressful moment. By shielding patients from granular cost details until after care is delivered, blinded payment systems aim to preserve the integrity of the clinical encounter. The patient can focus on understanding their condition and the recommended treatment, rather than navigating a complex and often confusing financial landscape.
Another important dimension of blinded medical payments is their potential to reduce disparities. In many healthcare systems, providers may unconsciously adjust their recommendations based on assumptions about a patient’s ability to pay. Even well‑intentioned clinicians can fall into patterns of offering different options to different socioeconomic groups. Blinding payment information helps counteract this tendency by ensuring that all patients are presented with the same range of medically appropriate choices. This can contribute to more consistent care across populations and help narrow gaps in outcomes that have persisted for decades.
***
***
However, blinded medical payments are not without challenges. Critics argue that withholding cost information from patients undermines their autonomy. In an era where consumer‑driven healthcare is increasingly emphasized, some believe that individuals should have full access to pricing details so they can make informed decisions about their care. Others worry that blinding providers to reimbursement rates may reduce accountability or make it more difficult to evaluate the cost‑effectiveness of different treatments. These concerns highlight the delicate balance between transparency and impartiality, and they underscore the need for thoughtful implementation.
Operationally, blinded payment systems require sophisticated administrative structures. Healthcare organizations must develop mechanisms to process claims, allocate funds, and track utilization without revealing sensitive financial details to clinicians or patients. This can be resource‑intensive, especially for smaller practices or systems with limited technological infrastructure. Additionally, the success of blinded payments depends on trust—trust that the system is fair, that reimbursement is adequate, and that no party is being disadvantaged by the lack of visibility.
Despite these complexities, blinded medical payments represent a meaningful attempt to address the misaligned incentives that often distort healthcare delivery. They challenge the assumption that more information is always better and instead propose that strategic withholding of information can sometimes lead to more ethical and equitable outcomes. As healthcare systems continue to evolve, blinded payments may serve as one of several innovative tools aimed at creating a more patient‑centered and value‑driven environment.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Risk‑based medical payment models have become one of the most significant shifts in modern health‑care financing. They move providers away from the traditional fee‑for‑service structure, where every test, visit, or procedure generates a separate payment, and toward arrangements that reward value, outcomes, and cost‑conscious care. This shift reflects a broader recognition that paying for volume alone can unintentionally encourage overuse, fragmentation, and rising costs. Risk‑based models attempt to realign incentives so that providers are financially accountable for the quality and efficiency of the care they deliver.
At the core of these models is the idea of financial risk transfer. Instead of insurers or government programs bearing the full cost of patient care, providers accept some degree of responsibility for spending that exceeds predetermined benchmarks. The level of risk can vary widely. Upside‑only arrangements allow providers to share in savings if they keep costs below expectations, while downside risk requires them to repay losses if spending surpasses targets. Full‑risk or global‑capitation models go even further, giving providers a fixed per‑patient payment to cover all necessary services. The more risk a provider assumes, the greater the potential reward—but also the greater the potential financial exposure.
***
***
One of the most widely used risk‑based models is the accountable care organization, or ACO. In an ACO, groups of physicians, hospitals, and other clinicians coordinate care for a defined population. They are measured on quality metrics such as preventive care, chronic disease management, and patient experience. If they meet quality standards while keeping total spending below a benchmark, they share in the savings. If they take on two‑sided risk, they may also owe money back when costs exceed expectations. The structure encourages collaboration, data sharing, and proactive management of high‑risk patients, all of which are difficult to achieve in a purely fee‑for‑service environment.
Bundled payments represent another important risk‑based approach. Instead of paying separately for each component of a treatment episode, such as a surgery and its follow‑up care, a bundled payment provides a single, predetermined amount for the entire episode. Providers must work together to deliver care efficiently within that budget. If they can do so while maintaining quality, they keep the difference as savings. If complications or inefficiencies drive costs above the bundle price, they absorb the loss. Bundled payments are particularly effective for procedures with predictable care pathways, such as joint replacements or cardiac interventions, and they encourage standardization and reduction of unnecessary variation.
Capitation, one of the oldest risk‑based models, assigns providers a fixed per‑member, per‑month payment to cover all or most services. This model creates strong incentives for preventive care, early intervention, and careful resource management. When implemented well, capitation can support integrated care delivery and long‑term population health strategies. However, it also requires robust infrastructure, accurate risk adjustment, and safeguards to ensure that cost control does not come at the expense of necessary care. Providers must be able to manage complex patients effectively, and payment rates must reflect the true needs of the population.
Risk adjustment is a critical component across all risk‑based models. Without it, providers who care for sicker or more socially complex patients could be unfairly penalized. Risk adjustment uses demographic and clinical data to estimate expected costs for each patient, ensuring that benchmarks and payments reflect the underlying health status of the population. Accurate risk adjustment protects against adverse selection and supports fairness, but it also requires sophisticated data systems and careful oversight to prevent gaming or upcoding.
Despite their promise, risk‑based payment models face challenges. Providers must invest in care‑management teams, data analytics, and interoperable technology to succeed. Smaller practices may struggle with the administrative and financial demands of taking on risk. Patients may also experience confusion if networks narrow or if care pathways become more structured. Policymakers and payers must balance incentives for efficiency with protections that ensure access and quality.
***
***
Even with these complexities, risk‑based models continue to expand because they offer a path toward a more sustainable and patient‑centered health‑care system. By rewarding outcomes rather than volume, they encourage providers to focus on prevention, coordination, and long‑term health. They also create opportunities for innovation in care delivery, from telehealth to home‑based services to integrated behavioral health. As health‑care costs continue to rise, risk‑based payment models represent a strategic attempt to align financial incentives with the goals of better care, healthier populations, and more efficient use of resources.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Financial fraud has long been woven into the fabric of American economic history. From Ponzi schemes to corporate deception, the United States has witnessed a series of high‑profile scandals that not only devastated investors but also reshaped regulatory frameworks. While the methods evolve with technology and time, the underlying motivations—greed, power, and the illusion of success—remain constant. This essay explores ten of the most notorious U.S. financial scammers whose actions left lasting scars on markets, institutions, and public trust.
1. Kenneth Lay & Jeffrey Skilling (Enron)
Few scandals loom as large as Enron, a company once hailed as an innovative energy titan before collapsing under the weight of its own deception. Enron executives Kenneth Lay and Jeffrey Skilling engineered an elaborate system of off‑balance‑sheet entities to hide debt and inflate earnings. The fraud, involving an estimated $74 billion, shattered investor confidence and triggered the Sarbanes‑Oxley Act, one of the most sweeping corporate governance reforms in U.S. history.
Their scheme demonstrated how corporate culture—when driven by unchecked ambition—can incentivize fraud at scale. Enron’s downfall remains a cautionary tale about transparency, oversight, and the dangers of financial engineering gone awry.
2. Bernie Madoff (Madoff Investment Securities)
Bernie Madoff orchestrated the largest Ponzi scheme in world history, defrauding investors of an estimated $65 billion. His reputation as a respected financier and former NASDAQ chairman allowed him to operate undetected for decades. Madoff’s scam unraveled during the 2008 financial crisis, exposing how trust, prestige, and secrecy can mask catastrophic fraud.
Though not directly cited in the retrieved sources, Madoff’s case is widely recognized as one of the most consequential financial crimes in U.S. history.
3. Andrew Fastow (Enron CFO)
While Lay and Skilling were the public faces of Enron, CFO Andrew Fastow was the architect behind the company’s labyrinth of special‑purpose vehicles (SPVs). These entities allowed Enron to hide massive liabilities while presenting a façade of profitability. Fastow personally profited from managing these off‑books partnerships, blurring the line between corporate officer and self‑interested operator. His actions exemplify how technical accounting knowledge can be weaponized to deceive investors.
4. Elizabeth Holmes (Theranos)
Elizabeth Holmes captivated Silicon Valley and Wall Street with promises of revolutionary blood‑testing technology. Theranos, valued at $9 billion at its peak, claimed it could run hundreds of tests from a single drop of blood. Investigations later revealed that the technology did not work, and the company relied on traditional machines while misleading investors, regulators, and patients.
Holmes’ downfall highlighted the dangers of hype‑driven investment culture and the need for scientific validation in health‑tech ventures.
5. Allen Stanford (Stanford Financial Group)
Allen Stanford ran a massive Ponzi scheme disguised as a global banking empire. Through fraudulent certificates of deposit issued by his Antigua‑based bank, Stanford defrauded investors of more than $7 billion. His charisma and lavish lifestyle helped him cultivate an image of legitimacy, masking the underlying fraud for years.
Stanford’s case underscored the vulnerabilities in cross‑border financial regulation and the risks of opaque offshore banking structures.
***
***
6. Jordan Belfort (Stratton Oakmont)
Popularized by The Wolf of Wall Street, Jordan Belfort’s pump‑and‑dump schemes in the 1990s defrauded investors through aggressive sales tactics and artificially inflated stock prices. While his crimes were smaller in scale than others on this list, Belfort’s cultural impact is enormous. His story illustrates how manipulation, high‑pressure sales, and market hype can devastate unsuspecting investors.
7. Charles Ponzi (The Original Ponzi Scheme)
Although his scheme dates back to the early 20th century, Charles Ponzi’s name remains synonymous with financial fraud. His promise of extraordinary returns through international postal coupon arbitrage attracted thousands of investors. When the scheme collapsed, it revealed the classic structure of a fraud model still used today: paying old investors with new investors’ money.
Ponzi’s legacy endures as a blueprint for countless modern scams.
8. Martin Shkreli (Turing Pharmaceuticals)
Martin Shkreli, often dubbed “Pharma Bro,” became infamous for dramatically raising the price of a life‑saving drug. While his price‑gouging was legal, Shkreli was later convicted of securities fraud unrelated to the drug scandal. His case illustrates how unethical behavior in one domain can draw scrutiny that uncovers deeper financial misconduct.
***
***
9. Sam Bankman‑Fried (FTX)
Sam Bankman‑Fried’s cryptocurrency exchange FTX collapsed in 2022 amid revelations of misused customer funds, lack of internal controls, and deceptive financial practices. Although crypto is a new frontier, the underlying fraud echoed classic themes: commingled funds, misleading investors, and unchecked executive power.
Bankman‑Fried’s downfall signaled a turning point in calls for crypto regulation and transparency.
10. Modern Imposter & Digital Scammers
While not tied to a single individual, modern imposter scams represent one of the fastest‑growing categories of financial fraud in the U.S. According to the Federal Trade Commission, Americans lost $5.8 billion to fraud in a single reporting year, with imposter scams leading the list. These schemes often involve criminals posing as government officials, financial advisors, or tech support agents to extract money or personal information.
Digital fraudsters exploit urgency, fear, and technological sophistication to deceive victims. As noted in recent analyses, imposter scams remain among the most prevalent and damaging forms of financial deception today.
Conclusion
The stories of these ten financial scammers reveal recurring themes: the power of perceived legitimacy, the exploitation of trust, and the persistent evolution of fraudulent tactics. From Enron’s corporate labyrinth to Madoff’s quiet betrayal, from Silicon Valley hype to digital‑age imposters, financial fraud continues to adapt to new technologies and cultural shifts.
Yet each scandal also brings progress. Regulatory reforms, improved oversight, and increased public awareness have emerged from the wreckage of these schemes. Understanding the methods and motivations of past scammers is essential to preventing future ones. As long as financial systems exist, so too will those who seek to exploit them—but informed vigilance remains society’s strongest defense.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Pay‑for‑performance (P4P) has become one of the most widely discussed strategies for improving healthcare quality in modern health systems. At its core, P4P links financial incentives to specific measures of performance, such as patient outcomes, adherence to clinical guidelines, or efficiency metrics. The idea is straightforward: reward providers for delivering high‑quality care, and they will be more motivated to improve their practices. Yet the simplicity of the concept masks a complex set of challenges, trade‑offs, and ethical considerations that shape how P4P functions in real‑world healthcare environments.
One of the primary arguments in favor of P4P is that it attempts to shift healthcare away from volume‑based reimbursement. Traditional fee‑for‑service models reward providers for doing more—more tests, more procedures, more visits—regardless of whether those services improve patient health. P4P, in contrast, aims to reward value rather than volume. By tying payment to outcomes or evidence‑based processes, the model encourages clinicians to focus on preventive care, chronic disease management, and coordination across the continuum of care. In theory, this alignment of financial incentives with patient well‑being should lead to better outcomes and more efficient use of resources.
***
***
Another potential benefit of P4P is its ability to promote transparency and accountability. When performance metrics are clearly defined and publicly reported, providers have a clearer understanding of expectations and benchmarks. This can foster a culture of continuous improvement, where clinicians and organizations regularly evaluate their performance and identify opportunities for better care. For patients, transparency can empower more informed decision‑making and build trust in the healthcare system.
Despite these advantages, P4P is far from a perfect solution. One of the most persistent criticisms is that performance metrics often fail to capture the full complexity of patient care. Healthcare outcomes are influenced by a wide range of factors, many of which lie outside a provider’s control, such as socioeconomic conditions, patient adherence, and comorbidities. When incentives are tied to outcomes without adequate risk adjustment, providers may be unfairly penalized for caring for more complex or disadvantaged populations. This can inadvertently discourage clinicians from accepting high‑risk patients, undermining equity in access to care.
Another challenge is the potential for P4P to encourage “teaching to the test.” When financial rewards depend on specific metrics, providers may focus narrowly on those measures at the expense of other important aspects of care that are harder to quantify. This can lead to a checkbox mentality, where meeting the metric becomes more important than understanding the patient’s broader needs. In extreme cases, P4P can even incentivize gaming the system, such as upcoding diagnoses to make patient populations appear sicker and performance outcomes appear better.
Implementation complexity also poses a barrier. Designing fair, meaningful, and comprehensive performance measures requires significant administrative effort. Providers must invest time and resources into documentation, data reporting, and quality improvement initiatives. Smaller practices, which often lack the infrastructure of large health systems, may struggle to keep up with these demands. If the administrative burden outweighs the financial incentives, P4P can become more of a bureaucratic hurdle than a driver of improvement.
***
***
Ultimately, the effectiveness of pay‑for‑performance depends on thoughtful design and careful balancing of incentives. When metrics are clinically meaningful, risk‑adjusted, and aligned with broader goals of patient‑centered care, P4P can encourage positive change. When poorly designed, it risks distorting provider behavior and exacerbating inequities. As healthcare systems continue to evolve, P4P will likely remain part of the conversation, but it must be integrated with other reforms—such as care coordination models, population health strategies, and patient engagement efforts—to truly enhance quality and value.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Podiatry, a specialized branch of medicine focused on diagnosing and treating conditions of the foot, ankle, and lower extremities, is often perceived as a stable and rewarding career. However, beneath the surface of clinical success and professional prestige lies a growing concern: the emotional and psychological toll of the profession. Stress, burnout, divorce, and practice turmoil are increasingly common among podiatrists, threatening not only their personal well-being but also the sustainability of their practices and the quality of patient care.
The Nature of Stress in Podiatry
Stress in podiatry arises from multiple sources. Clinical responsibilities, administrative burdens, patient expectations, and financial pressures converge to create a high-stakes environment. Podiatrists often work long hours, manage complex cases, and juggle the demands of running a business. The pressure to maintain high standards of care while navigating insurance reimbursements, staffing issues, and regulatory compliance can be overwhelming.
Moreover, podiatrists frequently deal with chronic conditions that require ongoing management rather than quick resolution. This can lead to emotional fatigue, especially when patients experience limited improvement or express dissatisfaction. The cumulative effect of these stressors can erode a podiatrist’s sense of purpose and satisfaction, leading to burnout.
Burnout: A Silent Epidemic
Burnout is characterized by emotional exhaustion, depersonalization, and a reduced sense of personal accomplishment. In podiatry, it manifests as fatigue, irritability, cynicism, and a decline in empathy toward patients. Burnout not only affects the practitioner’s mental health but also compromises patient safety, increases the risk of medical errors, and contributes to staff turnover.
Studies have shown that healthcare professionals, including podiatrists, are at a higher risk of burnout compared to other professions. The isolation of solo practice, lack of peer support, and limited access to mental health resources exacerbate the problem. Without intervention, burnout can progress to depression, substance abuse, and even suicidal ideation.
The personal lives of podiatrists are not immune to the pressures of the profession. Divorce rates among physicians, including podiatrists, are notably high. The demands of the job often leave little time for family, leading to strained relationships and emotional disconnect. The stress of managing a practice can spill over into home life, creating tension and conflict.
Divorce, in turn, can intensify professional stress. Legal proceedings, financial settlements, and emotional upheaval can distract from clinical duties and disrupt practice operations. The dual burden of personal and professional turmoil can be devastating, leading to a downward spiral that affects every aspect of life.
Practice Turmoil: The Business of Healing
Running a podiatry practice is akin to managing a small business. Beyond clinical expertise, podiatrists must master marketing, human resources, billing, and compliance. Practice turmoil can arise from staff conflicts, financial mismanagement, poor patient retention, or changes in healthcare regulations.
For example, a sudden drop in reimbursements or a lawsuit can destabilize a practice. Staff turnover, especially among key personnel like office managers or billing specialists, can disrupt workflow and erode morale. Inadequate leadership or poor communication can lead to a toxic work environment, further fueling stress and burnout.
Addressing the Crisis
To combat these challenges, podiatrists must prioritize self-care, seek support, and implement systemic changes. Here are several strategies:
Mental Health Support: Regular counseling, peer support groups, and wellness programs can help podiatrists process stress and prevent burnout.
Work-Life Balance: Setting boundaries, delegating tasks, and scheduling personal time are essential for maintaining emotional health.
Practice Management Training: Investing in leadership and business education can improve operational efficiency and reduce turmoil.
Staff Engagement: Creating a positive work culture, recognizing achievements, and fostering open communication can enhance team cohesion.
Technology Integration: Utilizing electronic health records, telemedicine, and automation can streamline administrative tasks and reduce workload.
Professional organizations also play a vital role. The American Podiatric Medical Association (APMA) and similar bodies can offer resources, advocacy, and continuing education to support practitioners. Medical schools and residency programs should incorporate wellness training and stress management into their curricula to prepare future podiatrists for the realities of the profession.
Podiatry is a noble and essential field, but it is not without its challenges. Stress, burnout, divorce, and practice turmoil are real and pressing issues that demand attention. By acknowledging these problems and taking proactive steps, podiatrists can safeguard their well-being, strengthen their practices, and continue to provide compassionate care to their patients. The path to healing begins not just with treating others, but with caring for oneself.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The Net Investment Income Tax (NIIT) occupies a distinctive place in the modern U.S. tax landscape. Introduced as part of the Affordable Care Act, it was designed to generate revenue from higher‑income households by taxing certain forms of unearned income. Although it affects a relatively small portion of taxpayers, its implications reach into investment strategy, tax planning, and broader debates about fairness and economic policy. Understanding how the NIIT works—and why it exists—offers insight into the evolving relationship between tax policy and wealth in the United States.
At its core, the NIIT is a 3.8 percent surtax applied to specific types of investment income for individuals whose modified adjusted gross income exceeds statutory thresholds. These thresholds—$200,000 for single filers and $250,000 for married couples filing jointly—are not indexed for inflation. As a result, over time, more taxpayers may find themselves subject to the tax even if their real purchasing power has not increased. This “bracket creep” is one of the subtle but important features of the NIIT, shaping its long‑term reach.
The tax applies only to “net investment income,” a term that includes interest, dividends, capital gains, rental income, royalties, and passive business income. It does not apply to wages, self‑employment earnings, or distributions from qualified retirement plans. The logic behind this distinction is straightforward: the NIIT targets income derived from wealth rather than labor. In practice, this means that two taxpayers with identical total income may face different NIIT liabilities depending on how much of their income comes from investments versus work.
The mechanics of the NIIT involve a comparison between two amounts: net investment income and the excess of modified adjusted gross income over the applicable threshold. The tax is applied to whichever of these two figures is smaller. This structure ensures that the NIIT functions as a surtax on high‑income households without taxing investment income for those below the threshold. It also means that taxpayers with large investment portfolios but modest overall income may avoid the tax entirely, while those with high wages and relatively small investment income may still owe it.
One of the most significant effects of the NIIT is its influence on investment behavior. Because the tax applies to capital gains, it can affect decisions about when to sell appreciated assets. Taxpayers may choose to time sales to avoid pushing their income above the threshold in a given year. Others may shift toward tax‑exempt investments, such as municipal bonds, or toward assets that generate unrealized rather than realized gains. The NIIT therefore becomes not just a revenue tool but a factor shaping the broader investment landscape.
The tax also interacts with other parts of the tax code in ways that can be complex. For example, rental real estate income is generally subject to the NIIT unless the taxpayer qualifies as a real estate professional and materially participates in the activity. Trusts and estates face their own NIIT rules, often reaching the surtax threshold at much lower income levels than individuals. These layers of complexity mean that the NIIT is often a central topic in tax planning for high‑income households, especially those with diverse investment portfolios.
Beyond its technical features, the NIIT reflects broader policy debates about equity and the distribution of tax burdens. Supporters argue that it helps ensure that high‑income individuals contribute a fair share to the cost of public programs, particularly those related to health care. Because investment income is disproportionately concentrated among wealthier households, the NIIT is seen as a way to align tax policy with ability to pay. Critics, however, contend that the tax discourages investment, adds unnecessary complexity, and imposes an additional layer of taxation on income that may already be subject to corporate taxes or other levies.
Despite these debates, the NIIT has become a stable part of the federal tax system. It raises billions of dollars annually and plays a role in funding health‑related initiatives. As discussions about tax reform continue, the NIIT often resurfaces as policymakers consider how best to balance revenue needs with economic incentives. Whether it remains unchanged, is expanded, or is modified in future legislation, the NIIT will continue to shape the financial decisions of high‑income taxpayers and contribute to the ongoing conversation about how the United States taxes wealth.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Austrian economics stands out in the landscape of economic thought because it places human decision‑making, uncertainty, and the dynamic nature of markets at the center of its analysis. Rather than relying heavily on mathematical models or large datasets, it emphasizes the subjective experiences of individuals and the ways in which real people navigate a world of incomplete information. This school of thought emerged in the late nineteenth century and has continued to influence debates about markets, government intervention, and the nature of economic knowledge.
At the heart of Austrian economics is the idea that value is subjective. Instead of assuming that goods possess inherent worth, Austrian thinkers argue that value arises from the preferences and priorities of individuals. A glass of water might be priceless to someone stranded in a desert but nearly worthless to someone standing next to a full pitcher. This simple insight leads to a broader understanding of how prices emerge in a market economy. Prices are not arbitrary numbers; they are signals that reflect countless individual judgments about scarcity, usefulness, and opportunity cost. Because these judgments vary from person to person, Austrian economists see markets as constantly shifting processes rather than static systems.
Another defining feature of Austrian economics is its focus on the entrepreneur. In this view, entrepreneurs are not just business owners but the driving force behind economic progress. They notice opportunities that others overlook, take risks in the face of uncertainty, and coordinate resources in new and productive ways. This entrepreneurial role cannot be captured fully by equations or statistical averages because it depends on creativity, intuition, and the ability to interpret subtle changes in consumer preferences. Austrian economists argue that entrepreneurship is the mechanism through which economies grow and adapt, and that attempts to centrally plan or regulate markets often stifle this essential process.
***
***
Austrian economics also places great importance on the concept of spontaneous order. This is the idea that complex and beneficial social arrangements can arise without central direction. Just as language evolves naturally through countless interactions rather than through a committee’s design, markets develop through the decentralized decisions of individuals pursuing their own goals. Prices, competition, and patterns of production emerge from this interplay. Austrian thinkers argue that this spontaneous order is far more flexible and efficient than any system imposed from above, because no central authority can ever possess the vast amount of dispersed knowledge held by millions of individuals.
This emphasis on dispersed knowledge leads to one of the school’s most influential arguments: the critique of central planning. Austrian economists contend that even well‑intentioned planners cannot gather or process the information needed to allocate resources effectively. The knowledge required to make economic decisions is scattered across society, embedded in local conditions, personal experiences, and constantly changing circumstances. Markets, through the price system, coordinate this information in a way that no planner could replicate. When governments attempt to override or replace market signals, they risk creating shortages, surpluses, and distortions that ripple through the economy.
Austrian economics is also known for its distinctive perspective on business cycles. Instead of attributing booms and busts to inherent flaws in capitalism, Austrian theorists argue that cycles often originate from distortions in the money and credit system. When interest rates are artificially lowered, for example, businesses may undertake long‑term investments that do not align with actual consumer preferences or available resources. These misalignments eventually become unsustainable, leading to a correction or recession. In this view, economic downturns are not random shocks but the result of earlier imbalances created by misguided monetary policy.
One of the strengths of Austrian economics is its insistence on methodological individualism—the idea that economic phenomena must be understood by examining the choices and motivations of individuals. This approach resists the temptation to treat “the economy” as a single entity with unified goals. Instead, it highlights the diversity of human aims and the ways in which people adapt to changing circumstances. By grounding economic analysis in human action, Austrian economics offers a framework that is both philosophically coherent and attentive to the complexity of real‑world behavior.
Critics sometimes argue that Austrian economics relies too heavily on theory and not enough on empirical testing. Supporters counter that many aspects of economic life—especially those involving creativity, uncertainty, and subjective value—cannot be captured adequately by statistical methods. Whether one agrees with its conclusions or not, Austrian economics challenges conventional assumptions and encourages a deeper examination of how markets function.
Ultimately, Austrian economics presents a vision of the economy as a dynamic, evolving process shaped by individual choices, entrepreneurial discovery, and the constant flow of information. It emphasizes the limits of centralized control and the power of decentralized decision‑making. By focusing on human action rather than abstract models, it offers a distinctive and thought‑provoking perspective on how societies organize production, exchange, and innovation.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on February 16, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
Dr. David Edward Marcinko MBA MEd
***
***
Why podiatry surgery volume matters so much?
Podiatry Management Service Organizations typically rely on three revenue pillars:
Office visits (high volume, low margin)
Ancillaries (DME, orthotics, imaging)
Surgery (low volume, high margin)
Surgery is the only pillar that reliably moves EBITDA in a meaningful way. Buyers know this, so they scrutinize surgical volume harder than anything else.
***
***
🔍 What “surgery volume” really means in podiatry
It’s not just the number of cases. Buyers look at:
Case mix (forefoot vs. rearfoot vs. trauma)
Site of service (ASC vs. hospital vs. office)
Provider concentration (is one surgeon doing 40% of cases?)
Payer mix (Medicare vs. commercial)
Seasonality (podiatry has real seasonal swings)
Referral stability (orthopedics, PCPs, wound care centers)
If any of these look unstable, the MSO’s valuation drops fast.
🚧 What happens to surgery volume when an MSO misses its exit window
1. Surgeons become less motivated
When the exit stalls:
Equity feels less valuable
Surgeons may slow down elective cases
Some shift cases back to hospitals
Others reduce ASC utilization
A few may even explore leaving the MSO
This is one of the biggest hidden risks.
2. Case mix often deteriorates
High‑value cases (rearfoot, reconstructive, trauma) may decline, while:
Nail procedures
Callus debridements
Routine diabetic care
…take up more of the schedule. This drags down EBITDA even if total visit volume stays stable.
3. Referral patterns weaken
If the MSO is perceived as unstable:
Orthopedic groups may stop referring
PCPs may shift to independent podiatrists
Wound care centers may diversify referrals
Referral leakage is subtle but devastating.
4. ASC strategy becomes strained
Many podiatry MSOs depend on:
Owning ASCs
Leasing block time
Negotiating better payer rates
If surgery volume softens:
ASC utilization drops
Fixed costs become painful
Lenders get nervous
Buyers discount the valuation
ASC underperformance is one of the top reasons podiatry MSOs fail to exit.
5. Productivity gaps widen between providers
Podiatry MSOs often have:
A few high‑volume surgeons
Many low‑volume generalists
When the exit stalls:
High performers may feel under‑rewarded
Low performers may drag down averages
Buyers see concentration risk
If one surgeon leaves, the MSO’s EBITDA can collapse.
6. Compliance scrutiny increases
Surgical coding in podiatry is a known risk area. When an MSO can’t sell, buyers often dig deeper into:
Modifier usage
Global period billing
Site‑of‑service documentation
Medical necessity for certain procedures
If anything looks aggressive, the deal dies.
***
***
🎯 The bottom line
Podiatry surgery volume is the core value driver of a podiatry MSO. When an MSO fails to sell at its vintage year, surgery volume usually:
Softens
Becomes more concentrated
Shifts toward lower‑margin cases
Shows referral instability
Raises compliance questions
Buyers interpret this as EBITDA fragility, which is why podiatry MSOs often end up in continuation funds or sell at discounted multiples.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The idea of a physician who is also an accountant might sound unusual at first, almost like two worlds that rarely intersect. One is rooted in diagnosing illnesses, understanding human physiology, and providing compassionate care. The other revolves around financial statements, regulatory compliance, and strategic fiscal planning. Yet when these two disciplines come together in a single professional, the result is a uniquely capable individual who can navigate both the complexities of modern healthcare and the equally intricate world of financial management. As healthcare systems grow more complicated and financially pressured, the combination of medical expertise and accounting acumen becomes not only valuable but transformative.
Physicians traditionally focus on clinical decision‑making, patient outcomes, and the ethical dimensions of care. Their training emphasizes scientific reasoning, empathy, and the ability to make high‑stakes decisions under uncertainty. Accountants, on the other hand, are trained to think in terms of precision, structure, and long‑term financial sustainability. They understand how organizations allocate resources, manage risk, and maintain compliance with regulatory frameworks. When one person embodies both sets of skills, they gain a rare vantage point: the ability to see how clinical decisions ripple through the financial health of a practice, hospital, or healthcare system.
One of the most significant advantages of this dual expertise is the ability to bridge the communication gap between clinicians and administrators. In many healthcare organizations, physicians and financial officers often struggle to fully understand each other’s priorities. Physicians may feel that financial constraints undermine their ability to provide optimal care, while administrators may worry that clinical decisions are made without regard for cost efficiency or long‑term sustainability. A physician‑accountant can translate between these two perspectives, helping each side understand the other’s reasoning. This can lead to more balanced decision‑making, where patient care remains central but financial realities are acknowledged and managed responsibly.
Another area where this combination shines is in private practice management. Running a medical practice is, at its core, running a business. Physicians who lack financial training often find themselves overwhelmed by budgeting, billing systems, tax obligations, and regulatory compliance. Mistakes in these areas can be costly, both financially and legally. A physician who is also an accountant is far better equipped to manage these responsibilities. They can design efficient billing workflows, interpret financial reports, and make informed decisions about staffing, equipment purchases, and long‑term investments. This not only strengthens the practice but also allows the physician to maintain greater autonomy and stability in an increasingly competitive healthcare landscape.
***
***
Beyond individual practices, physician‑accountants can play influential roles in healthcare policy and leadership. Healthcare spending is a major concern in many countries, and policymakers often struggle to balance cost control with quality of care. Professionals who understand both the clinical and financial dimensions of healthcare are uniquely positioned to contribute to policy development, hospital administration, and health‑system reform. They can evaluate the economic impact of clinical guidelines, assess the cost‑effectiveness of new technologies, and design reimbursement models that incentivize high‑quality care without creating unnecessary financial burdens.
The dual training also enhances ethical decision‑making. Financial pressures in healthcare can sometimes lead to conflicts of interest or difficult trade‑offs. A physician‑accountant is better prepared to navigate these dilemmas because they understand the financial implications without losing sight of the ethical obligations inherent in medical practice. They can advocate for solutions that protect patient welfare while ensuring that resources are used responsibly. This balanced perspective can help organizations avoid short‑sighted decisions that might compromise care or create long‑term financial instability.
Of course, becoming both a physician and an accountant requires an extraordinary level of dedication. Medical training alone demands years of study, residency, and ongoing professional development. Adding accounting education—whether through a degree, certification, or extensive coursework—requires additional time and effort. Yet for those who pursue this path, the rewards can be substantial. They gain a level of professional versatility that few others possess, and they can shape healthcare environments in ways that purely clinical or purely financial professionals cannot.
In a rapidly evolving healthcare landscape, the intersection of medicine and accounting is becoming increasingly relevant. Rising costs, complex insurance systems, and the growing emphasis on value‑based care all demand professionals who can think across traditional disciplinary boundaries. Physicians who are also accountants embody this interdisciplinary approach. They bring clarity to financial decisions, insight to clinical operations, and a holistic understanding of how healthcare systems function. Their unique skill set positions them as leaders who can help shape a more efficient, ethical, and sustainable future for healthcare.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on February 15, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
Dr. David Edward Marcinko MBA MEdCMP
Eugene Schmuckler PhD MBA MEd CTS
***
***
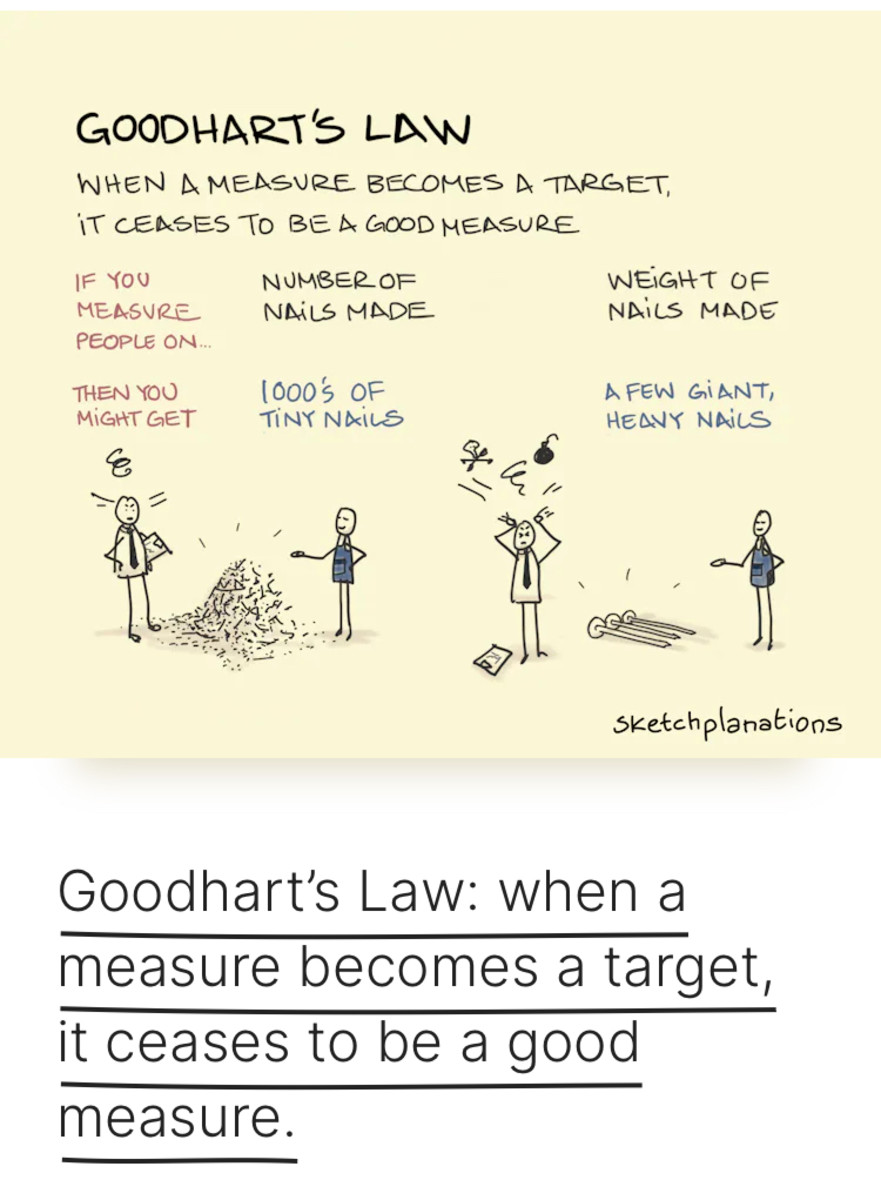
A paradox is a logically self-contradictory statement or a statement that runs contrary to one’s expectation. It is a statement that, despite apparently valid reasoning from true or apparently true premises, leads to a seemingly self-contradictory or a logically unacceptable conclusion. A paradox usually involves contradictory-yet-interrelated elements that exist simultaneously and persist over time. They result in “persistent contradiction between interdependent elements” leading to a lasting “unity of opposites”.
***
1. The Paradox of Skill
As more investors become skilled, skill matters less.
When everyone is highly skilled, outperformance becomes mostly luck because the competition is too tight.
2. The Market Efficiency Paradox
Markets are efficient because people believe they are not.
If everyone believed markets were efficient, no one would try to exploit mispricings—and markets would become inefficient.
3. The Liquidity Paradox
Liquidity is abundant until you need it most.
In crises, assets that were easy to trade suddenly become impossible to sell at a fair price.
4. The Volatility Paradox
Strategies that appear safe (low volatility) can be the most dangerous.
Strategies that look risky (high volatility) can be safer long-term.
Example: selling insurance-like options feels safe—until it blows up.
5. The Risk Paradox
Taking more risk can lead to lower returns if the risks are poorly compensated.
Taking less risk can lead to higher returns if it keeps you invested through downturns.
6. The Diversification Paradox
Diversification always feels unnecessary before a crisis and always feels insufficient during one.
7. The Time Paradox
The longer your time horizon, the less risky stocks become.
But the longer your time horizon, the harder it is to stay disciplined.
8. The Cash Paradox
Holding cash feels safe, but over long periods it’s one of the riskiest assets because inflation quietly destroys it.
9. The Contrarian Paradox
Being contrarian works only when you’re right.
Most of the time, the crowd is correct—so being contrarian for its own sake is a losing strategy.
10. The Information Paradox
More information doesn’t always lead to better decisions.
Sometimes it leads to overconfidence, noise-chasing, and worse outcomes.
11. The Performance Paradox
The best-performing funds are often the worst-performing funds right before and after their peak.
Investors chase past returns and end up buying high and selling low.
12. The Leverage Paradox
Leverage boosts returns—until it destroys them.
The more leverage you use, the more fragile your portfolio becomes.
13. The Behavioral Paradox
You can know all the right investing principles and still fail because behavior > knowledge.
14. The “Do Nothing” Paradox
Doing nothing is often the most profitable strategy.
But doing nothing is psychologically the hardest thing to do.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
A growing number of surveys measure physician compensation, encompassing a varying depth of analysis. Physician compensation data, divided by specialty and subspecialty, is central to a range of consulting activities including practice assessments and valuations of healthcare enterprises. The AMA maintains the most comprehensive database of information on physicians in the U.S., with information on over 940,000 physicians and residents, and 77,000 medical students. Started in 1906, the AMA “Physician Masterfile,” which contains information on physician education, training, and professional certification information, is updated annually through the Physicians’ Professional Activities questionnaire and the collection and validation efforts of AMA’s Division of Survey and Data Resources (SDR).A selection of other sources of healthcare related compensation and cost data is set forth below.
“Physician Characteristics and Distribution in the U.S.” is an annual survey based on a variety of demographic information from the Physician Masterfile dating back to 1963. It includes detailed information regarding trends, distribution, and professional and individual characteristics of the physician workforce.
“Physician Socioeconomic Statistics”, published from 2000 to 2003, was a result of the merger between two prior AMA annuals: (1) “Socioeconomic Characteristics of Medical Practice”; and, (2) “Physician Marketplace Statistics.” Data has compiled from a random sampling of physicians from the Physician Masterfile into what is known as the Socioeconomic Monitoring System, which includes physician age profiles, practice statistics, utilization, physician fees, professional expenses, physician compensation, revenue distribution by payor, and managed care contracts, among other categories.
The Medical Group Management Association’s (MGMA) “Physician Compensation and Production Survey” is one of the largest in the U.S. with approximately 3,000 group practices responding as of the 2023 edition publication. Data is provided on compensation and production for 125 specialties. The survey data are also published on CD by John Wiley & Sons ValueSource; the additional details available in this media provide better bench marking capabilities.
The MGMA’s “Cost Survey” is one of the best known surveys of group practice income and expense data, having been published in some form since 1955, and obtaining over 1,600 respondents, combined, for the 2008 surveys: “Cost Survey for Single Specialty Practices” and “Cost Survey for Multispecialty Practices.” Data is provided for a detailed listing of expense categories and is also calculated as a percentage of revenue and per FTE physician, FTE provider, patient, square foot, and Relative Value Unit (RVU). The survey provides information on multispecialty practices by performance ranking, geographic region, legal organization, size of practice, and percent of capitated revenue. Detailed income and expense data is provided for single specialty practice in over 50 different specialties and subspecialties.
The “Medical Group Financial Operations Survey” was created through a partnership between RSM McGladrey and the American Medical Group Association (AMGA), and provides benchmark data on support staff and physician salaries, physician salaries, staffing profiles and benefits, and other financial indicators. Data is reported as a percent of managed care revenues, per full-time physician, and per square foot, and is subdivided by specialty mix, capitation level, and geographic region with detailed summaries of single specialty practices in several specialties.
“Statistics: Medical and Dental Income and Expense Averages” is an annual survey produced by the National Society of Certified Healthcare Business Consultants (NSCHBC), formerly known as the National Association of Healthcare Consultants (NAHC), and the Academy of Dental CPAs. It has been published annually for a number of years and the “2023 Report Based on 2022 Data” included detailed income and expense data from over 2,700 practices and 4,900 physicians in 62 specialties.
***
***
Medical Specialty Trends
The characteristics of both the practice and the profitability of different physician specialties vary greatly. Information on trends affecting specific specialties should further refine the types of industry information gathered including changes in treatment, technology, competition, reimbursement, and the regulatory environment. For many of the subspecialties, oversupply and under supply issues and the corresponding demand and compensation trends are central to the analysis of potential future earnings and the value of established medical entities. Information that is available and that may be gathered can range from broad practice overviews to, for example, specific procedural utilization demand and forecasts for a precise local geographic area.
A large number of national and state medical associations and organizations gather and produce information on these various aspects of the practice of different individual physician specialties and subspecialties. Information may be found in trade press articles, medical specialty associations and their publications, national surveys, specialty accreditation bodies, governmental reports and studies, and elsewhere. The American Medical Association’s (AMA) as well as the MGMA both publish comprehensive physician practice survey information.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on January 26, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
***
***
By Dr. David Edward Marcinko MBA MEd
***
Milton Friedman: Champion of Free Markets
Milton Friedman was a towering figure in the field of economics, renowned for his unwavering advocacy of free-market capitalism and limited government intervention. Born in 1912 in New York City and raised in Rahway, New Jersey, Friedman rose from modest beginnings to become a Nobel laureate and a leading voice of the Chicago School of Economics.
Friedman’s academic journey began at Rutgers University, where he earned a degree in mathematics and economics. He later pursued graduate studies at the University of Chicago and Columbia University, where he was mentored by prominent economists like Simon Kuznets. His intellectual foundation laid the groundwork for a career that would challenge prevailing economic thought and reshape public policy.
One of Friedman’s most significant contributions was his development of monetarism, a theory emphasizing the role of governments in controlling the money supply to manage inflation and economic stability. In contrast to Keynesian economics, which advocated for active fiscal policy and government spending, Friedman argued that excessive government intervention often led to inefficiencies and inflation. His research demonstrated that inflation is “always and everywhere a monetary phenomenon,” a principle that became central to modern macroeconomic policy.
Friedman’s influence extended beyond academia. His 1962 book, Capitalism and Freedom, articulated a powerful case for economic liberty as a foundation for political freedom. He argued that voluntary exchange and competitive markets were essential for individual choice and prosperity. The book also introduced the Friedman Doctrine, which posited that the primary responsibility of business is to increase its profits, a view that sparked ongoing debates about corporate social responsibility.
In 1976, Friedman was awarded the Nobel Memorial Prize in Economic Sciences for his work on consumption analysis, monetary history, and stabilization policy. His Permanent Income Hypothesis, which suggests that people base their consumption on expected long-term income rather than current income, revolutionized understanding of consumer behavior.
Friedman’s ideas had profound policy implications. He was a vocal critic of the draft and successfully advocated for an all-volunteer military. He also proposed the concept of school vouchers, allowing parents to choose schools for their children, which laid the foundation for modern school choice movements. His work influenced leaders like Ronald Reagan and Margaret Thatcher, who embraced free-market reforms during their administrations.
Despite his acclaim, Friedman’s views were not without controversy. Critics argued that his emphasis on deregulation and privatization sometimes overlooked social equity and environmental concerns. Nonetheless, his legacy remains deeply embedded in economic thought and public discourse.
Milton Friedman passed away in 2006, but his ideas continue to shape debates on economic policy, freedom, and the role of government. His belief in the power of markets and individual choice remains a cornerstone of classical liberalism and a guiding light for economists and policymakers around the world.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on January 25, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
***
***
A paradox is a logically self-contradictory statement or a statement that runs contrary to one’s expectation. It is a statement that, despite apparently valid reasoning from true or apparently true premises, leads to a seemingly self-contradictory or a logically unacceptable conclusion. A paradox usually involves contradictory-yet-interrelated elements that exist simultaneously and persist over time. They result in “persistent contradiction between interdependent elements” leading to a lasting “unity of opposites”.
Classic Definition: Artificial intelligence (AI) refers to computer systems capable of performing complex tasks that historically only a human could do, such as reasoning, making decisions, or solving problems. The term “AI” describes a wide range of technologies that power many of the services and goods we use every day – from apps that recommend TV shows to chat-bots that provide customer support in real time.
Modern Circumstance: The role of artificial intelligence in health care is becoming an increasingly topical and controversial discussion. There remains uncertainty about what is achievable regarding ongoing medical artificial intelligence research. Although there are some people who believe that artificial intelligence will be used, at best, as a tool to assist clinicians in their day-to-day activities, there are others who believe that job automation and replacement is a looming threat.
Paradox Example: Moravec’s paradox is a phenomenon observed by robotics researcher Hans Moravec, in which tasks that are easy for humans to perform (eg, motor or social skills) are difficult for machines to replicate, whereas tasks that are difficult for humans (eg, performing mathematical calculations or large-scale data analysis) are relatively easy for machines to accomplish.
***
***
For example, a computer-aided diagnostic system might be able to analyze large volumes of images quickly and accurately but might struggle to recognize clinical context or technical limitations that a human radiologist would easily identify.
Similarly, a machine learning algorithm might be able to predict a patient’s risk of a specific condition on the basis of their medical history and laboratory results but might not be able to account for the nuances of the patient’s individual case or consider the effect of social and environmental factors that a human physician would consider.
In surgery, there has been great progress in the field of robotics in health care when robotic elements are controlled by humans, but artificial intelligence-driven robotic technology has been much slower to develop.Thus far, research into clinical artificial intelligence has focused on improving diagnosis and predictive medicine.
Assessment
Moravec’s paradox also highlights the importance of maintaining a human element in the health-care system, and the need for collaboration between humans and technology to achieve the best possible outcomes.
Conclusion
In the field of medicine, it is becoming indisputable that artificial intelligence will have a role in population health analysis, predictive medicine, and personalized care.
However, for now, the job of doctors seems safe from automation.
Cite: Shuaib A: The increasing role of artificial intelligence in health care: will robots replace doctors in the future? Int J Gen Med. 2020; 13: 891-896
The economics of information explores how knowledge—or the lack of it—affects decision-making, market behavior, and resource allocation. It reveals why perfect competition rarely exists and why information itself can be a powerful economic asset.
Economics of Information: Understanding the Value and Impact of Knowledge
In traditional economic models, markets are often assumed to operate under perfect information—where all participants have equal access to relevant data. However, in reality, information is often incomplete, asymmetric, or costly to obtain. The field known as economics of information emerged to address these discrepancies, fundamentally reshaping how economists understand markets, incentives, and efficiency.
One of the core concepts in this field is information asymmetry, where one party in a transaction possesses more or better information than the other. This imbalance can lead to adverse selection and moral hazard. For example, in the insurance market, individuals who know they are high-risk are more likely to seek coverage, while insurers may struggle to differentiate between high- and low-risk clients. Similarly, in lending, borrowers may have private knowledge about their ability to repay, which lenders cannot easily verify.
To mitigate these problems, economists have developed mechanisms such as signaling and screening. Signaling occurs when the informed party takes action to reveal their type—like a job applicant earning a degree to signal competence. Screening, on the other hand, involves the uninformed party designing tests or contracts to elicit information—such as offering different insurance packages to separate risk levels.
Another important area is the cost of acquiring information. Gathering data, analyzing trends, or verifying facts requires time and resources. This leads to decisions being made under uncertainty, where individuals rely on heuristics or limited data. The economics of information examines how these costs influence behavior, pricing, and market structure. For instance, consumers may not compare every available product due to search costs, allowing firms to maintain price dispersion.
The rise of digital technology has intensified the relevance of this field. In the age of big data, companies like Google and Amazon thrive by collecting and analyzing vast amounts of user information. This data allows them to personalize services, predict behavior, and gain competitive advantages. However, it also raises concerns about privacy, market power, and inequality—issues that economists of information are increasingly addressing.
Moreover, information goods—such as software, media, and research—have unique economic properties. They are often non-rivalrous and can be reproduced at near-zero marginal cost. This challenges traditional pricing models and calls for innovative approaches like freemium strategies, bundling, and subscription services.
In public policy, the economics of information plays a crucial role in designing regulations, transparency standards, and consumer protections. Governments must balance the need for open access to information with incentives for innovation and investment. For example, patent laws aim to encourage research by granting temporary monopolies, while disclosure requirements in finance promote market integrity.
In conclusion, the economics of information reveals that knowledge is not just a passive input but a dynamic force shaping economic outcomes. By understanding how information is produced, distributed, and used, economists can better explain real-world phenomena and design systems that promote fairness, efficiency, and innovation.
The Impact of Medical Equipment Tariffs on Healthcare Systems
Tariffs on medical equipment have become a contentious issue in global trade and healthcare policy, particularly in the United States. These import taxes, designed to protect domestic industries and generate government revenue, can have unintended consequences when applied to essential healthcare supplies. As the U.S. healthcare system relies heavily on imported medical devices, consumables, and components, tariffs can significantly affect costs, accessibility, and innovation.
One of the most immediate impacts of medical equipment tariffs is the increase in operational costs for hospitals and healthcare providers. According to the American Hospital Association, the U.S. imported nearly $15 billion in medical equipment in 2024, much of it from countries like China. Recent tariff hikes on items such as syringes, respirators, gloves, and medical masks have raised concerns about affordability and supply chain stability. These cost increases are particularly burdensome for rural hospitals and smaller health systems, which operate on tighter budgets and have less flexibility to absorb price shocks.
Tariffs also disrupt supply chains by introducing unpredictability into procurement strategies. Unlike market-driven price changes, tariffs are policy-based and often implemented with little warning. This volatility can affect everything from disposable supplies to high-tech imaging equipment. Long-term contracts may temporarily shield hospitals from tariff impacts, but as these agreements expire, renegotiations often reflect the new cost realities. Manufacturers, in turn, may respond by relocating production, adding surcharges, or reducing product lines to manage tariff-related risks.
Beyond cost and logistics, tariffs can hinder innovation in the medical field. Many U.S.-based manufacturers rely on imported components to build advanced medical devices. When these parts become more expensive due to tariffs, companies may scale back research and development or pass costs onto consumers. This can slow the adoption of cutting-edge technologies and reduce the competitiveness of domestic firms in the global market.
***
***
From a policy perspective, the rationale for imposing tariffs on medical equipment is often rooted in national security and economic protectionism. However, critics argue that such measures may weaken health security by limiting access to critical supplies during emergencies, such as pandemics or natural disasters. The National Taxpayers Union has emphasized that tariffs on personal protective equipment and other medical goods can undermine preparedness and increase vulnerability.
To mitigate these challenges, healthcare systems and policymakers must explore strategic solutions. These include advocating for tariff exemptions on essential medical supplies, diversifying sourcing strategies, and investing in domestic manufacturing capabilities. Additionally, standardizing procurement practices and implementing cost-saving measures can help health systems navigate tariff-related pressures more effectively.
In conclusion, while tariffs may serve broader economic goals, their application to medical equipment demands careful consideration. The stakes are high—not just in terms of dollars, but in the quality and accessibility of patient care. A balanced approach that protects domestic interests without compromising health outcomes is essential for a resilient and equitable healthcare system.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The contrasting economic philosophies of John Maynard Keynes and Friedrich Hayek have shaped not only macroeconomic policy but also approaches to investing. While both thinkers sought to understand and improve economic systems, their views diverge sharply on the role of government, market behavior, and investor decision-making.
Keynesian economics emphasizes the importance of aggregate demand in driving economic growth. Keynes argued that markets are not always self-correcting and that government intervention is necessary during downturns to stimulate demand. In the context of investing, Keynesian theory supports counter-cyclical strategies. Investors following this approach might increase exposure to equities during recessions, anticipating that fiscal stimulus will boost corporate earnings and market performance. Keynes himself was a successful investor, known for his contrarian style and long-term focus. He advocated for active portfolio management, believing that markets are driven by psychological factors and herd behavior, which create mispricings that savvy investors can exploit.
In contrast, Hayekian economics is rooted in classical liberalism and the belief in spontaneous order. Hayek argued that markets are efficient information processors and that decentralized decision-making leads to better outcomes than centralized planning. From an investment standpoint, Hayekian theory favors passive strategies and minimal interference. Investors aligned with Hayek’s philosophy might prefer index funds or diversified portfolios that reflect market signals rather than attempting to time the market or predict government actions. Hayek was skeptical of the ability of any individual or institution to possess enough knowledge to outsmart the market consistently.
The Keynesian approach tends to be more optimistic about the power of policy to influence markets. For example, during economic crises, Keynesians may expect stimulus packages to revive demand and thus invest in sectors likely to benefit from increased government spending. Hayekians, on the other hand, may view such interventions as distortions that lead to malinvestment and eventual corrections. They might invest more cautiously during periods of heavy government involvement, anticipating inflation, asset bubbles, or regulatory overreach.
Risk perception also differs between the two schools. Keynesians may see risk as cyclical and manageable through diversification and active management. Hayekians view risk as inherent and unpredictable, best mitigated through adherence to market fundamentals and long-term discipline.
In practice, modern investors often blend elements of both approaches. For instance, they may use Keynesian insights to anticipate short-term market movements while relying on Hayekian principles for long-term portfolio construction. The rise of behavioral finance has also added nuance, validating Keynes’s view of irrational market behavior while reinforcing Hayek’s skepticism of centralized forecasting.
Ultimately, the choice between Keynesian and Hayekian investing reflects deeper beliefs about how economies function and how much control investors—or governments—really have. Keynesians embrace adaptability and intervention, while Hayekians champion restraint and trust in the market’s invisible hand. Both offer valuable lessons, and understanding their differences can help investors navigate complex financial landscapes with greater clarity.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
A medical economic white elephant is a healthcare-related investment—such as a hospital, device, or system—that consumes vast resources but fails to deliver proportional value, often becoming a financial burden rather than a benefit to public health.
In economic terms, a white elephant refers to an asset whose cost of upkeep far exceeds its utility. In the medical field, this concept manifests in projects or technologies that are expensive to build, maintain, or operate, yet offer limited practical use, accessibility, or return on investment. These ventures often begin with noble intentions—improving care, advancing technology, or expanding access—but end up draining resources due to poor planning, misaligned incentives, or lack of demand.
One prominent example is the construction of underutilized hospitals or specialty centers in regions with low patient volume. Governments or private entities may invest heavily in state-of-the-art facilities without conducting thorough needs assessments. The result: gleaming buildings with advanced equipment but few patients, high operating costs, and staff shortages. These facilities often struggle to stay open, becoming financial sinkholes that divert funds from more pressing healthcare needs.
Medical devices and technologies can also become white elephants. For instance, robotic surgical systems or high-end imaging machines are sometimes purchased by hospitals to boost prestige or attract patients, despite limited clinical necessity or trained personnel. These devices require costly maintenance, specialized training, and may not significantly improve outcomes compared to traditional methods. When reimbursement rates don’t justify their use, they become liabilities.
***
***
Electronic health record (EHR) systems offer another cautionary tale. While digitizing patient records is essential, some EHR implementations have ballooned into multi-million-dollar projects plagued by inefficiencies, poor interoperability, and user dissatisfaction. Hospitals may invest in proprietary systems that are difficult to integrate with others, leading to fragmented care and wasted resources. In extreme cases, these systems are abandoned or replaced, compounding the financial loss.
The consequences of medical white elephants are far-reaching. They can strain public budgets, increase healthcare costs, and erode trust in institutions. In developing countries, such projects may be funded by international aid or loans, saddling governments with debt while failing to improve population health. Even in wealthier nations, misallocated resources can mean fewer funds for primary care, preventive services, or community health initiatives.
***
***
Avoiding medical white elephants requires rigorous planning, stakeholder engagement, and evidence-based decision-making. Health systems must assess actual needs, forecast demand, and consider long-term sustainability. Cost-benefit analyses should include not only financial metrics but also health outcomes, equity, and accessibility. Transparency and accountability are key to ensuring that investments serve the public good.
In conclusion, the concept of a medical economic white elephant highlights the importance of aligning healthcare investments with real-world needs and outcomes. While innovation and expansion are vital, they must be grounded in practicality and sustainability.
By learning from past missteps, health systems can prioritize value-driven care and avoid the costly pitfalls of overambitious or poorly conceived projects.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on January 7, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Tariffs on medicines and healthcare products increase costs, disrupt supply chains, and ultimately harm patient access and public health. They raise prices for essential drugs and medical devices, create shortages, and undermine innovation in the healthcare sector.
The Economic Burden of Tariffs
Tariffs are taxes imposed on imported goods. In healthcare, this means pharmaceuticals, medical devices, and raw materials like active pharmaceutical ingredients (APIs) become more expensive. Since the United States imports a significant share of these products from countries such as China, India, and the European Union, tariffs directly raise costs for hospitals, clinics, and patients.
Drug prices rise because manufacturers pass on higher import costs to consumers.
Medical devices such as surgical instruments, diagnostic equipment, and imaging technology become more expensive, straining hospital budgets.
Insurance premiums may increase as healthcare providers face higher operating costs.
This economic burden is not abstract—it translates into higher bills for patients and reduced affordability of care.
Supply Chain Disruptions
Healthcare supply chains are highly globalized. APIs, raw materials, and specialized equipment often come from multiple countries. Tariffs disrupt this delicate balance by:
Creating shortages when suppliers cannot afford to export to tariff-heavy markets.
Delaying shipments as companies seek alternative routes or suppliers.
Reducing resilience by concentrating production in fewer regions, making systems more vulnerable to shocks.
For example, if tariffs make APIs prohibitively expensive, pharmaceutical companies must scramble to find new suppliers, often at higher cost and with longer lead times. This can delay drug availability and compromise patient care.
***
***
Impact on Public Health
The consequences of tariffs extend beyond economics into public health outcomes.
Patients face reduced access to life-saving medicines and devices.
Hospitals may ration supplies, prioritizing urgent cases while delaying elective procedures.
Preventive care suffers, as higher costs discourage investment in vaccines, diagnostic tools, and routine screenings.
In the long run, tariffs can exacerbate health inequities, disproportionately affecting low-income populations who are least able to absorb rising costs.
Innovation and Research Setbacks
Healthcare innovation relies on global collaboration. Tariffs discourage cross-border partnerships by raising costs and creating uncertainty.
Research institutions may struggle to import specialized lab equipment.
Pharmaceutical companies face higher costs for clinical trials and drug development.
Digital health technologies that depend on imported components (like sensors and chips) become more expensive, slowing adoption.
This stifles progress in areas such as cancer treatment, biotechnology, and precision medicine.
Conclusion
Tariffs in healthcare are a blunt economic tool with unintended consequences. While they aim to protect domestic industries, they increase costs, disrupt supply chains, reduce access to care, and hinder innovation. In medicine and healthcare, where lives depend on timely and affordable access to products, tariffs are particularly damaging. Policymakers must weigh these human costs carefully before imposing trade barriers on essential goods.
Posted on January 5, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
In today’s healthcare landscape, small medical practices face a dual threat: the emotional toll of provider burnout and the growing risk of cyberattacks. While these challenges may seem unrelated, both can have devastating financial and operational consequences. Fortunately, the right insurance coverage can serve as a critical safety net, helping practices stay resilient in the face of adversity.
1. Prioritize Cyber Liability Insurance
Cyberattacks on healthcare providers are on the rise, with small practices often being prime targets due to limited IT resources. A single ransomware attack or data breach can lead to HIPAA violations, patient trust erosion, and costly legal battles. Cyber liability insurance is no longer optional—it’s essential. This coverage typically includes data breach response, legal fees, notification costs, and even ransom payments. When selecting a policy, ensure it covers both first-party (your practice’s losses) and third-party (claims from affected patients or partners) liabilities.
Burnout can lead to high staff turnover, workplace tension, and even wrongful termination claims. EPLI protects your practice from lawsuits related to employment issues such as discrimination, harassment, and retaliation. As burnout increases the likelihood of HR-related disputes, having EPLI in place can prevent a bad situation from becoming financially catastrophic.
3. Review Malpractice and Professional Liability Policies
While malpractice insurance is a given, it’s crucial to review your policy regularly. Burnout can increase the risk of medical errors, and some policies may have exclusions or limitations that leave your practice vulnerable. Ensure your coverage limits are adequate and that your policy includes tail coverage if you’re planning to retire or close your practice.
4. Invest in Business Interruption Insurance
Cyberattacks and burnout-related staffing shortages can disrupt operations. Business interruption insurance helps cover lost income and operating expenses during downtime. This can be a lifeline if your electronic health records system is compromised or if you need to temporarily close due to staff burnout or illness.
***
***
5. Bundle Policies for Better Rates and Coverage
Many insurers offer bundled packages tailored to healthcare providers. These may include general liability, property, malpractice, and cyber coverage under one umbrella. Bundling not only simplifies management but can also lead to cost savings and fewer coverage gaps.
6. Work with a Healthcare-Savvy Insurance Broker
Navigating the insurance landscape can be complex. Partnering with a broker who specializes in healthcare ensures your policy is tailored to your unique risks. They can help you identify coverage gaps, negotiate better terms, and stay compliant with evolving regulations.
Conclusion
Small practices are the backbone of community healthcare, but they face mounting pressures from both internal and external threats. By proactively investing in comprehensive insurance coverage—especially cyber liability and employment practices liability—practices can protect their financial health and focus on what matters most: delivering quality patient care. In an era where burnout and cybercrime are increasingly common, insurance isn’t just a safety net—it’s a strategic asset.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Required Minimum Distributions (RMDs) are mandatory withdrawals from certain retirement accounts that begin at age 73, designed to ensure the IRS collects taxes on previously tax-deferred savings.
Required Minimum Distributions (RMDs) are a critical component of retirement planning in the United States. They represent the minimum amount that retirees must withdraw annually from specific tax-deferred retirement accounts, such as traditional IRAs, 401(k)s, and other qualified plans, once they reach a certain age. As of 2025, individuals must begin taking RMDs at age 73, a change implemented by the SECURE 2.0 Act for those born between 1951 and 1959.
The rationale behind RMDs is rooted in tax policy. Contributions to tax-deferred accounts are made with pre-tax dollars, allowing investments to grow without immediate tax consequences. However, the IRS eventually wants its share. RMDs ensure that retirees begin paying taxes on these funds, preventing indefinite tax deferral. The amount of each RMD is calculated using the account balance at the end of the previous year and a life expectancy factor provided by IRS tables.
Failing to take an RMD can result in steep penalties. Historically, the penalty was 50% of the amount not withdrawn, but recent changes have reduced this to 25%, and potentially 10% if corrected promptly. These penalties underscore the importance of understanding and complying with RMD rules.
Not all retirement accounts are subject to RMDs. Roth IRAs are exempt during the original account holder’s lifetime, and under the SECURE 2.0 Act, Roth 401(k) and Roth 403(b) accounts are also exempt from RMDs while the original owner is alive. However, beneficiaries of these accounts may still face RMD requirements.
***
***
Strategically managing RMDs can help retirees minimize tax impacts and optimize their retirement income. For example, retirees might consider withdrawing more than the minimum in years with lower income to reduce future RMD amounts. Others may choose to convert traditional IRA funds to Roth IRAs before reaching RMD age, thereby reducing future taxable distributions. Additionally, using RMDs to fund charitable donations through Qualified Charitable Distributions (QCDs) can satisfy the RMD requirement while excluding the amount from taxable income.
Timing is also crucial. The first RMD must be taken by April 1 of the year following the year the individual turns 73. Subsequent RMDs must be taken by December 31 each year. Delaying the first RMD can result in two withdrawals in one year, potentially increasing taxable income and affecting Medicare premiums or tax brackets.
In conclusion, RMDs are more than just a tax obligation—they are a planning opportunity. Understanding the rules, calculating the correct amount, and integrating RMDs into a broader retirement strategy can help retirees maintain financial stability and reduce unnecessary tax burdens.
As regulations evolve, staying informed and consulting with financial professionals is essential to make the most of retirement savings.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on January 3, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Alternative health coverage models like Short-Term Duration Plans, Health Care Sharing Ministries (HCSMs), and Individual Coverage Health Reimbursement Arrangements (ICHRAs) offer flexible, cost-conscious options for individuals and employers seeking alternatives to traditional insurance.
As the landscape of American healthcare continues to evolve, many consumers and employers are exploring non-traditional coverage models to address rising costs, limited access, and regulatory complexity. Among the most prominent alternatives are Short-Term Duration Plans, Health Care Sharing Ministries (HCSMs), and Individual Coverage Health Reimbursement Arrangements (ICHRAs)—each offering distinct advantages and trade-offs.
Short-Term Duration Plans are designed to provide temporary coverage for individuals experiencing gaps in insurance, such as between jobs or during waiting periods. These plans are typically less expensive than ACA-compliant insurance but come with significant limitations. They often exclude coverage for pre-existing conditions, maternity care, mental health services, and prescription drugs. While they offer affordability and quick enrollment, they lack the comprehensive protections mandated by the Affordable Care Act (ACA), making them a risky choice for those with ongoing health needs.
Health Care Sharing Ministries (HCSMs) represent a faith-based approach to healthcare financing. Members contribute monthly fees into a shared pool used to cover eligible medical expenses for others in the group. These arrangements are not insurance and are not regulated by state insurance departments, meaning they are not required to cover essential health benefits or guarantee payment. However, HCSMs appeal to individuals seeking community-based support and lower costs. They often include moral or religious requirements for membership and may exclude coverage for lifestyle-related conditions or services deemed inconsistent with their beliefs.
***
***
Individual Coverage Health Reimbursement Arrangements (ICHRAs) are employer-sponsored programs that allow businesses to reimburse employees for individual health insurance premiums and qualified medical expenses. Introduced in 2020, ICHRAs offer flexibility for employers to control costs while giving employees the freedom to choose plans that suit their needs. Unlike traditional group health insurance, ICHRAs shift the purchasing power to employees, promoting consumer choice and market competition. However, they require employees to navigate the individual insurance marketplace, which can be complex and variable depending on location and income.
Other emerging models include Direct Primary Care (DPC), where patients pay a monthly fee for unlimited access to a primary care provider, and Health Savings Accounts (HSAs) paired with high-deductible plans, which encourage consumer-driven healthcare spending. These models emphasize affordability, personalization, and preventive care, but may not offer sufficient protection against catastrophic health events.
In conclusion, alternative health coverage models provide valuable options for individuals and employers seeking flexibility and cost savings. However, they often come with trade-offs in coverage, regulation, and consumer protection. As ACA subsidies fluctuate and healthcare costs rise, these models are likely to gain traction—but consumers must carefully assess their health needs, financial risks, and eligibility before choosing a non-traditional path.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on November 20, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Shaping Well-being Beyond Medicine
Health is often thought of as the result of medical care, but in reality, it is deeply influenced by the conditions in which people are born, grow, live, work, and age. These conditions, known as social determinants of health, include a wide range of social, economic, and environmental factors that shape health outcomes. They are responsible for many of the differences in health status between individuals and communities. Understanding these determinants is essential for promoting fairness in health and designing policies that reduce disparities.
Economic Stability
Economic stability is one of the most powerful determinants of health. Individuals with steady income can afford nutritious food, safe housing, and preventive healthcare. Conversely, poverty increases vulnerability to chronic diseases, mental health challenges, and limited access to medical services. Families with fewer financial resources may struggle to afford medications or healthy diets, leading to higher rates of obesity, diabetes, and cardiovascular disease. Unemployment or unstable work further exacerbates stress, which itself is linked to poor health outcomes. Economic inequality directly translates into health inequality.
Education
Education shapes health both directly and indirectly. Higher educational attainment is associated with better employment opportunities, higher income, and improved health literacy. People with more education are more likely to understand medical information, adopt healthy behaviors, and navigate healthcare systems effectively. Limited education can perpetuate cycles of poverty and poor health. For instance, children who grow up in underfunded schools may face restricted opportunities, leading to lower lifetime earnings and poorer health outcomes. Education is therefore a critical lever for breaking intergenerational cycles of disadvantage.
***
***
Neighborhood and Physical Environment
The environment in which individuals live plays a crucial role in determining health. Safe neighborhoods with clean air, accessible parks, and reliable transportation promote physical activity and reduce exposure to pollutants. In contrast, communities with high crime rates, poor housing, and environmental hazards contribute to stress, injury, and illness. Food deserts—areas with limited access to affordable, healthy food—are a striking example of how environment shapes health. Residents in these areas often rely on processed foods, increasing risks of obesity and related diseases. Housing quality also matters: overcrowding, mold, or lead exposure can lead to respiratory illnesses and developmental delays.
Healthcare Access and Quality
Access to healthcare is a fundamental determinant, but it is shaped by social and economic factors. Insurance coverage, affordability, and cultural competence of providers influence whether individuals receive timely and effective care. Marginalized groups often face barriers such as discrimination, language differences, or lack of nearby facilities. Even when healthcare is available, disparities in quality persist. For example, minority populations may receive less aggressive treatment for certain conditions compared to others. Addressing these inequities requires systemic reforms that prioritize inclusivity and affordability.
Social and Community Context
Social relationships and community support networks significantly affect health. Strong social ties provide emotional support, reduce stress, and encourage healthy behaviors. Communities with high levels of trust and civic engagement often experience better health outcomes. Conversely, discrimination, racism, and social exclusion undermine health by increasing stress and limiting opportunities. Social cohesion and equity are therefore vital for fostering healthier societies.
Conclusion
The social determinants of health highlight that medicine alone cannot ensure well-being. Economic stability, education, environment, healthcare access, and social context collectively shape health outcomes and drive disparities. Addressing these determinants requires a holistic approach that integrates public health, social policy, and community action. By investing in education, reducing poverty, improving neighborhoods, and ensuring equitable healthcare, societies can move closer to achieving health equity. Ultimately, health is not just about treating illness—it is about creating conditions in which everyone has the opportunity to thrive.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Doctors use loss leader tactics—offering discounted or free services—to attract new patients and build long-term loyalty. These strategies are increasingly common in competitive healthcare markets.
In today’s healthcare landscape, physicians and clinics face intense competition for patient attention. Traditional referral systems are no longer sufficient, as patients increasingly rely on online reviews, social media, and digital advertising to choose providers. To stand out, many doctors have adopted loss leader marketing tactics—a strategy borrowed from retail where a business offers a product or service at a loss to attract customers and stimulate future sales.
A loss leader in healthcare typically involves offering free consultations, discounted exams, or low-cost procedures. For example, aesthetic clinics might advertise free skin evaluations or reduced-price Botox sessions. Primary care practices may offer complimentary wellness screenings or discounted flu shots. These services are not intended to generate immediate profit but to introduce patients to the practice, build trust, and encourage them to return for more comprehensive—and profitable—care.
This tactic works particularly well in specialties where patients have discretionary choice, such as dermatology, dentistry, chiropractic care, and cosmetic surgery. By lowering the barrier to entry, doctors can attract hesitant or price-sensitive patients who might otherwise delay care. Once inside the practice, patients experience the quality of service firsthand, increasing the likelihood of repeat visits and word-of-mouth referrals.
***
***
Digital marketing amplifies the effectiveness of loss leader strategies. Physicians use platforms like Google Ads, Facebook, and Instagram to promote their offers to targeted demographics. A well-designed landing page might advertise a “$49 New Patient Exam” with a clear call to action and online booking. These campaigns often include retargeting ads and email follow-ups to nurture leads into loyal patients.
However, loss leader tactics must be carefully managed. Offering services below cost can strain resources if not paired with a clear conversion strategy. Doctors must ensure that the initial offer leads to higher-value services, such as diagnostic testing, treatment plans, or elective procedures. Additionally, practices must maintain ethical standards and avoid misleading promotions that could erode patient trust.
Reputation management plays a crucial role in sustaining the benefits of loss leader marketing. Positive patient experiences from initial discounted visits often translate into glowing online reviews, which further attract new patients. Conversely, poor execution—such as rushed appointments or upselling pressure—can backfire and damage the practice’s credibility.
Ultimately, loss leader marketing is not about giving away services indefinitely. It’s a strategic investment in patient acquisition, brand building, and long-term growth. When executed thoughtfully, it allows doctors to showcase their expertise, differentiate their practice, and foster lasting relationships with patients.
In conclusion, loss leader tactics have become a powerful tool in the modern physician’s marketing arsenal. By offering low-cost entry points to care, doctors can attract new patients, build trust, and grow their practice sustainably.
As competition intensifies, those who master this strategy—while maintaining quality and transparency—will be best positioned to thrive in the evolving healthcare marketplace.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 15, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
For centuries, doctors have occupied one of the highest earning and most respected positions in society. Their extensive education, specialized knowledge, and critical role in preserving human life have traditionally guaranteed them financial security and social prestige. Yet in recent years, a growing conversation has emerged: could skilled tradesmen—electricians, plumbers, welders, carpenters, and other hands‑on professionals—eventually out‑earn doctors in the future? While the answer is complex, shifting economic dynamics suggest that the gap between these professions may narrow, and in certain contexts, tradesmen could indeed surpass doctors in earnings.
One of the most significant factors driving this possibility is supply and demand. The medical profession requires years of schooling, residency, and licensing, which creates a steady pipeline of doctors but also limits entry. By contrast, skilled trades have suffered from declining interest among younger generations, many of whom were encouraged to pursue college degrees instead of vocational training. As a result, there is now a shortage of tradesmen in many regions. When demand for services like plumbing or electrical work rises but supply remains low, wages naturally increase. Already, some master tradesmen charge hourly rates that rival or exceed those of general practitioners.
Another consideration is student debt and overhead costs. Doctors often graduate with hundreds of thousands of dollars in debt, and many must work in hospital systems or private practices with high administrative expenses. Tradesmen, on the other hand, typically face lower educational costs and can enter the workforce much earlier. Many start their own businesses with relatively modest investments, allowing them to keep a larger share of their earnings. In an era where entrepreneurship and independence are highly valued, tradesmen may find themselves financially freer than doctors burdened by debt and bureaucracy.
***
***
The changing economy also plays a role. Automation and artificial intelligence are beginning to reshape medicine, with diagnostic tools, telehealth, and robotic surgery reducing the need for certain human tasks. While doctors will always be essential, parts of their work may become less lucrative as technology takes over. Skilled trades, however, are far harder to automate. Repairing a leaking pipe, rewiring a house, or welding a custom structure requires physical presence, adaptability, and problem‑solving in unpredictable environments—skills machines struggle to replicate. This resilience against automation could make tradesmen’s work increasingly valuable.
That said, doctors will likely continue to command high salaries in specialized fields such as surgery, cardiology, or oncology. The prestige and necessity of medical expertise ensure that society will always reward them. Yet the notion that tradesmen are “lesser” careers is fading. In fact, many tradesmen already earn six‑figure incomes, particularly those who own successful businesses or operate in regions with acute labor shortages.
Ultimately, whether tradesmen will out‑earn doctors depends on how society values different forms of expertise. If current trends continue—rising demand for trades, shortages of skilled labor, resistance to automation, and lower educational barriers—it is plausible that many tradesmen will match or surpass doctors in income. The future may not be defined by one profession dominating the other, but by a more balanced recognition that both healers and builders are indispensable to modern life. In that sense, the financial gap may close, reflecting a broader cultural shift toward valuing practical skills as highly as academic ones.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
BASIC DEFINITIONS
***
***
The Direct Reimbursement Payment Model allows physicians to receive payment directly from patients or employers, bypassing traditional insurance systems. This model emphasizes transparency, autonomy, and personalized care, offering an alternative to fee-for-service and managed care structures.
The Direct Reimbursement Payment Model is a healthcare financing approach in which physicians are paid directly by patients or sponsoring entities—such as employers—rather than through insurance companies or government programs. This model is gaining traction as a response to the administrative burdens, opaque billing practices, and fragmented care often associated with traditional insurance-based systems.
One prominent example of direct reimbursement is Direct Primary Care (DPC). In DPC, patients pay a recurring fee—monthly, quarterly, or annually—that covers a broad range of primary care services. These include routine checkups, preventive screenings, chronic disease management, and basic lab work. By eliminating third-party billing, DPC practices reduce overhead costs and administrative complexity, allowing physicians to spend more time with patients and focus on quality care.
***
***
Employers have also embraced direct reimbursement models to manage healthcare costs and improve employee wellness. In such arrangements, employers reimburse physicians or clinics directly for services rendered to their employees, often through a defined benefit structure. This can be part of a self-funded health plan or a supplemental offering alongside high-deductible insurance policies. The goal is to provide accessible, cost-effective care while avoiding the inefficiencies of traditional insurance networks.
Key advantages of the direct reimbursement model include:
Price transparency: Patients know upfront what services cost, reducing surprise billing and financial stress.
Improved access: Physicians often offer same-day or next-day appointments, extended visits, and direct communication via phone or email.
Lower administrative burden: Without insurance paperwork, practices can operate more efficiently and focus on patient care.
Stronger patient-physician relationships: More time per visit fosters trust, continuity, and better health outcomes.
However, the model is not without limitations. Direct reimbursement may not cover specialist care, hospitalization, or emergency services, requiring patients to maintain supplemental insurance. Additionally, the model may be less accessible to low-income populations who cannot afford recurring fees or out-of-pocket payments. Critics also argue that widespread adoption could fragment care and reduce risk pooling, undermining the broader goals of universal coverage.
Despite these concerns, the direct reimbursement model aligns with broader trends in healthcare reform, including value-based care, consumer empowerment, and decentralized service delivery. It offers a viable path for physicians seeking autonomy and for patients desiring personalized, transparent care. As healthcare continues to evolve, hybrid models that combine direct reimbursement with traditional insurance may emerge, offering flexibility and choice across diverse patient populations.
In conclusion, the Direct Reimbursement Payment Model represents a meaningful shift in how healthcare services are financed and delivered.
By prioritizing simplicity, transparency, and patient-centered care, it challenges the status quo and opens new possibilities for sustainable, high-quality medical practice.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Say’s Law, named after the French economist Jean‑Baptiste Say, is a foundational idea in classical economics. Often summarized as “supply creates its own demand,” the law suggests that the act of producing goods and services inherently generates the income necessary to purchase them. This principle shaped economic thought throughout the 19th century and continues to influence debates about markets, government intervention, and the causes of economic crises.
Origins and Meaning Jean‑Baptiste Say introduced his law in the early 1800s in his Treatise on Political Economy. He argued that production is the source of demand: when producers create goods, they pay wages, rents, and profits, which in turn become purchasing power. In this view, general overproduction is impossible because every supply of goods corresponds to an equivalent demand. If imbalances occur, they are temporary and limited to specific sectors, not the economy as a whole.
Core Principles Say’s Law rests on several assumptions:
Markets are self‑correcting: Any surplus in one area leads to adjustments in prices and production.
Money is neutral: It serves only as a medium of exchange, not as a driver of demand.
Production drives prosperity: Economic growth depends on increasing output, not stimulating consumption.
No long‑term unemployment: Since supply creates demand, workers displaced in one industry will eventually find employment elsewhere.
These ideas aligned with classical economists’ belief in minimal government intervention and the efficiency of free markets.
Influence on Classical Economics Say’s Law became a cornerstone of classical economics, reinforcing the belief that recessions or depressions were temporary and self‑correcting. Economists like David Ricardo and John Stuart Mill adopted versions of the law, using it to argue against policies aimed at stimulating demand. The law supported laissez‑faire approaches, suggesting that governments should avoid interfering with markets, as production itself would ensure economic balance.
Criticism and Keynesian Revolution Say’s Law faced its greatest challenge during the Great Depression of the 1930s. Widespread unemployment and idle factories contradicted the idea that supply automatically generates demand. John Maynard Keynes famously rejected Say’s Law in his General Theory of Employment, Interest, and Money (1936). Keynes argued that demand, not supply, drives economic activity. He showed that insufficient aggregate demand could lead to prolonged recessions, requiring government intervention through fiscal and monetary policies.
Keynes’s critique marked a turning point in economics. While Say’s Law emphasized production, Keynesian economics highlighted consumption and demand management. This shift reshaped economic policy, leading to active government roles in stabilizing economies.
Modern Perspectives Today, Say’s Law is not accepted in its original form, but elements of it remain relevant. Supply‑side economists, for example, argue that policies encouraging production—such as tax cuts and deregulation—can stimulate growth. In contrast, Keynesians stress the importance of demand management. The debate reflects a broader tension in economics: whether prosperity depends more on producing goods or ensuring people have the means and willingness to buy them.
Conclusion: Say’s Law was a bold attempt to explain the self‑sustaining nature of markets. While its claim that “supply creates its own demand” proved too simplistic in the face of modern economic realities, it remains a vital part of the history of economic thought. The controversy surrounding Say’s Law highlights the evolving nature of economics, where theories are tested against real‑world crises and adapted to new circumstances. Even today, discussions of supply‑side versus demand‑side policies echo the enduring influence of Say’s original insight.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 10, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Ricardian economics, rooted in the theories of 19th-century economist David Ricardo, emphasizes comparative advantage, free trade, and the neutrality of government debt—most notably through the concept of Ricardian equivalence. While these ideas have shaped macroeconomic thought, their relevance to medicine and healthcare policy is less direct. Still, exploring Ricardian principles offers a provocative lens through which to examine the fiscal sustainability and efficiency of modern healthcare systems.
At the heart of Ricardian equivalence is the idea that consumers are forward-looking and internalize government budget constraints. If a government finances healthcare through debt rather than taxes, rational agents will anticipate future tax burdens and adjust their behavior accordingly. In theory, this undermines the effectiveness of deficit-financed healthcare spending as a stimulus. Applied to medicine, this suggests that long-term fiscal responsibility is crucial: expanding healthcare access through borrowing may not yield the intended economic or health benefits if citizens expect future costs to rise.
This insight could inform debates on healthcare reform, especially in countries grappling with ballooning medical expenditures. Ricardian economics warns against short-term fixes that ignore long-term fiscal implications. For example, expanding public insurance programs without sustainable funding mechanisms could lead to intergenerational inequities and economic distortions. Policymakers might instead focus on reforms that align incentives, reduce waste, and promote cost-effective care—principles that resonate with Ricardo’s emphasis on efficiency and comparative advantage.
***
***
However, Ricardian economics offers limited guidance on the unique moral and practical dimensions of medicine. Healthcare is not a typical market good. Patients often lack the information or autonomy to make rational choices, especially in emergencies. Moreover, the sector is rife with externalities: one person’s vaccination benefits the broader community, and untreated illness can strain public resources. These complexities challenge the assumption of rational, forward-looking behavior central to Ricardian equivalence.
Additionally, Ricardo’s theory of comparative advantage—where nations benefit by specializing in goods they produce most efficiently—has implications for global health. It supports international collaboration in pharmaceutical production, medical research, and telemedicine. Yet, over-reliance on global supply chains can expose vulnerabilities, as seen during the COVID-19 pandemic when countries faced shortages of critical medical supplies.
In conclusion, Ricardian economics provides valuable fiscal insights that can inform healthcare policy, particularly regarding debt sustainability and efficient resource allocation. Its emphasis on long-term planning and comparative advantage can guide reforms that make medicine more resilient and cost-effective. However, the theory’s assumptions about rational behavior and market dynamics limit its applicability to the nuanced realities of healthcare. Medicine requires not just economic efficiency but ethical considerations, equity, and compassion—areas where Ricardian economics falls short. Thus, while it can contribute to the conversation, it cannot “save” medicine alone.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on November 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A.I.
***
***
The Pitfalls of Capitation in Medicine
Capitation, a payment model in healthcare where providers receive a fixed amount per patient regardless of the services rendered, has been promoted as a way to control costs and incentivize efficiency. However, despite its theoretical appeal, capitation medicine presents significant drawbacks that can compromise patient care, distort provider incentives, and exacerbate systemic inequities.
One of the most concerning aspects of capitation is the potential for under-treatment. Since providers are paid a set fee per patient, regardless of how much care that patient requires, there is a financial incentive to minimize services. This can lead to situations where necessary tests, referrals, or treatments are delayed or denied in order to preserve profit margins. Patients with complex or chronic conditions—who require more frequent and intensive care—may be especially vulnerable under this model. The risk is that medical decisions become driven by cost containment rather than clinical need, undermining the ethical foundation of healthcare.
Capitation also introduces challenges in maintaining quality standards. Unlike value-based care, which ties reimbursement to outcomes, capitation focuses solely on cost predictability. Without robust oversight and accountability mechanisms, providers may cut corners or avoid high-risk patients altogether. This can result in cherry-picking, where healthier individuals are favored, and sicker patients are subtly discouraged from enrolling. Such practices not only distort the patient pool but also deepen health disparities, particularly among marginalized populations who already face barriers to care.
Furthermore, capitation can strain the provider-patient relationship. Physicians may feel pressured to limit time spent with each patient or avoid costly interventions, leading to a sense of transactional care rather than personalized attention. This erosion of trust can diminish patient satisfaction and reduce adherence to treatment plans. In a system where providers are rewarded for doing less, the intrinsic motivation to go above and beyond for patients may be compromised.
Operationally, capitation demands sophisticated infrastructure to manage risk, track utilization, and ensure compliance. Smaller practices or those serving underserved communities may lack the resources to implement such systems effectively. This can create a two-tiered system where well-funded organizations thrive while others struggle to deliver basic care. Additionally, the administrative burden of managing capitation contracts, monitoring performance metrics, and navigating complex reimbursement rules can divert attention from clinical priorities.
Critics also argue that capitation may stifle innovation. When providers are locked into fixed budgets, there is little room to experiment with new technologies, therapies, or care models that might improve outcomes but carry upfront costs. This conservative approach can hinder progress and limit access to cutting-edge treatments.
In conclusion, while capitation medicine aims to control costs and streamline care, its inherent risks—under-treatment, inequity, and diminished quality—make it a problematic model when not carefully regulated. To truly reform healthcare, payment systems must balance financial sustainability with ethical responsibility, ensuring that every patient receives the care they need, not just the care that fits a budget.
Posted on November 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd and Copilot A.I.
***
***
The Baylor method of nurse payments is a scheduling and compensation model that allows nurses to work weekend shifts while receiving full-time pay and benefits, offering flexibility and helping healthcare facilities address staffing shortages.
The Baylor method, also known as the Baylor Plan or Baylor Shift, originated at Baylor University Medical Center in Dallas, Texas, as a strategic response to nurse shortages and burnout. It was designed to retain experienced nurses by offering a more flexible work schedule that still met the demands of patient care. Under this model, nurses typically work two 12-hour shifts on the weekend—Saturday and Sunday—and receive compensation equivalent to a full 40-hour workweek.
This approach has become increasingly popular in hospitals, long-term care facilities, and other healthcare settings. The core idea is simple: by concentrating work hours into the weekend, nurses gain more time off during the week while employers maintain adequate staffing during traditionally hard-to-fill shifts. For many nurses, this arrangement provides a better work-life balance, allowing them to pursue education, spend time with family, or take on additional employment during the week.
***
***
Financially, the Baylor method is attractive to both nurses and employers. Nurses benefit from full-time pay and benefits—including health insurance, retirement contributions, and paid time off—while only working two days per week. Employers, on the other hand, can reduce turnover and improve weekend staffing without increasing overall labor costs. Some facilities even offer Baylor shifts with added incentives, such as shift differentials or bonuses, to further encourage weekend coverage.
However, the Baylor method is not without its challenges. Working two consecutive 12-hour shifts can be physically and emotionally demanding, especially in high-acuity units. Nurses may experience fatigue or burnout if they are not adequately supported. Additionally, because Baylor nurses are paid for 40 hours while only working 24, scheduling extra shifts during the week can complicate overtime calculations. Typically, overtime pay only kicks in after 40 actual hours worked, not hours paid, which can lead to confusion or dissatisfaction if not clearly communicated.
From an operational standpoint, the Baylor method helps facilities maintain consistent staffing levels during weekends, which are often underserved due to lower availability of part-time or weekday-only staff. It also allows for more predictable scheduling and can improve patient outcomes by ensuring continuity of care. Facilities that adopt the Baylor model often report higher nurse satisfaction and retention rates.
In conclusion, the Baylor method of nurse payments is a creative and effective solution to some of the most persistent challenges in healthcare staffing. By offering full-time compensation for weekend work, it provides nurses with flexibility and financial stability while helping facilities maintain high-quality care. As healthcare continues to evolve, models like the Baylor shift demonstrate the importance of innovative scheduling strategies that support both caregivers and patients.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 7, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
An October 2025 Health Affairs study found that payment equity between facilities owned by hospitals, known as hospital outpatient departments (HOPDs), and independent outpatient facilities such as ambulatory surgery centers (ASCs), is still far from reality. Comparing payments for common procedures, researchers found commercial prices were 78% higher in HOPDs compared to ASCs, although payment differentials varied considerably.
This Health Capital Topics article reviews the article and potential policy implications. (Read more…)
Posted on November 6, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters and Copilot A.I.
***
***
Goodhart’s law is an adage often stated as, “When a measure becomes a target, it ceases to be a good measure”. It is named after British economistCharles Goodhart, who is credited with expressing the core idea of the adage in a 1975 article on monetary policy in the United Kingdom:
Any observed statistical regularity will tend to collapse once pressure is placed upon it for control purposes.
It was used to criticize the British Margaret Thatcher Government for trying to conduct monetary policy on the basis of targets for broad and narrow money, but the law reflects a much more general phenomenon.
And so, aother famous Goodhart’s Law example is the cobra effect, where well-intentioned government policies inadvertently worsened the problem they were designed to solve.
For example, the British colonial government in India, concerned about the increasing number of venomous cobras in Delhi, began offering a bounty for each dead cobra that was delivered. Initially, this strategy was successful as locals brought in large numbers of slaughtered snakes. Over time, however, enterprising individuals started breeding cobras to kill them for supplemental income. When the government abandoned the bounty, the cobra breeders released their cobras into the wild, leading to a surge in Delhi’s snake population.
The cobra effect, where efforts to control a problem lead to unintended and often worse outcomes, serves as a cautionary tale for health care AI. If developers or health care institutions focus too narrowly on specific performance AI metrics, they risk undermining the system’s overall effectiveness, leading to suboptimal patient outcomes. Physicians must be vigilant in ensuring that health care AI systems are not only optimized for performance metrics but are also truly beneficial in practical, clinical applications.
Posted on November 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
According to colleague Dan Ariely PhD, the Scitovsky Paradox and using the Kaldor–Hicks criterion, allocation A may be more efficient than allocation B, while at the same time B is more efficient than A.
Moreover, the Scitovsky paradox in welfare economics which is resolved by stating that there is no increase in social welfare by a return to the original part of the losers. It is named after the Hungarian born American economist, Tibor Scitovsky. According to Scitovsky, ther Kaldor-Hicks criterion involves contradictory and inconsistent results.
What Scitovsky demonstrated was it is possible that if an allocation A is deemed superior to another allocation B by the Kaldor compensation criteria, then by a subsequent set of moves by the same criteria, we can prove that B is also superior to A.
Posted on November 3, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
***
***
By Health Capital Consultants, LLC
On October 23, 2025, both Democratic and Republican lawmakers expressed support during a Senate Health, Education, Labor, and Pensions (HELP) Committee hearing for reforming the 340B Drug Discount Program. Although senators acknowledged that any reform would necessitate an intentional, considered approach to mitigate unintended consequences, the bipartisan agreement (particularly during a government shutdown deadlocked on healthcare) indicates that changes to the program may be on the horizon.
This Health Capital Topics article outlines the 340B program, discusses issues that have made the program controversial, and discusses potential reform options. (Read more…)
Posted on November 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
Since lawmakers failed to pass a bill to fund the federal government before the September 30, 2025 deadline, lawmakers have remained deadlocked over the spending bill. The deadlock is centered on the continuation of health insurance exchange subsidies, but the shutdown has broader implications on the healthcare industry.
This Health Capital Topics article provides an update on the continuing saga. (Read more…)
Posted on October 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
In the evolving landscape of digital health care, Amazon Pharmacy and GoodRx have emerged as two leading platforms offering consumers affordable and convenient access to prescription medications. While both aim to simplify the process of obtaining prescriptions, they differ significantly in their approach, pricing models, and user experience.
Amazon Pharmacy, launched in 2020, is a full-service online pharmacy that allows customers to order medications directly through Amazon. It offers fast, free delivery for Prime members and integrates with most insurance plans. One of its standout features is RxPass, a subscription service available to Prime members for $5 per month, which covers unlimited eligible generic medications. This model is particularly attractive to individuals who take multiple generics regularly, as it can significantly reduce out-of-pocket costs.
In contrast, GoodRx, founded in 2011, operates primarily as a price comparison and discount platform. It does not dispense medications itself but partners with local and mail-order pharmacies to help users find the lowest prices. GoodRx provides coupons that can be used at thousands of pharmacies nationwide, often resulting in substantial savings—especially for those without insurance. It also offers GoodRx Gold, a paid membership that unlocks deeper discounts and telehealth services.
***
***
When comparing the two, pricing transparency is a key differentiator. GoodRx excels in showing users a range of prices across different pharmacies, empowering them to choose the most cost-effective option. Amazon Pharmacy, while competitive, typically offers fixed prices and focuses more on convenience and integration with its broader ecosystem.
Convenience is another area where Amazon Pharmacy shines. With its streamlined ordering process, automatic refills, and integration with Amazon’s delivery network, it appeals to users who prioritize ease and speed. GoodRx, while convenient in its own right, requires users to present coupons at the pharmacy or use mail-order services, which may involve more steps.
Insurance compatibility also varies. Amazon Pharmacy accepts most major insurance plans, making it a viable option for insured individuals. GoodRx, on the other hand, is often used by those without insurance or with high deductibles, as its discounts can sometimes beat insurance copays.
However, both platforms have limitations. Amazon Pharmacy’s RxPass is restricted to generic medications and excludes certain states due to regulatory issues. GoodRx’s discounts may not apply to all medications, and prices can fluctuate depending on location and pharmacy.
In terms of user experience, Amazon offers a seamless, tech-driven interface with customer support and medication management tools. GoodRx provides educational resources, price alerts, and a mobile app that helps users track savings and prescriptions.
Ultimately, the choice between Amazon Pharmacy and GoodRx depends on individual needs. For those seeking a one-stop solution with predictable costs and fast delivery, Amazon Pharmacy may be ideal. For users who want to shop around for the best deal or lack insurance, GoodRx offers unmatched flexibility and savings.
As digital health continues to grow, both platforms are reshaping how Americans access medications—making prescriptions more affordable, transparent, and accessible than ever before.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
The global healthcare sector faces mounting challenges: rising costs, inefficiencies, limited access, and bureaucratic entanglements. In response, some economists and policymakers have turned to Austrian Economics for answers. Rooted in the works of Ludwig von Mises and Friedrich Hayek, Austrian Economics emphasizes individual choice, market-driven solutions, and skepticism toward centralized planning. But can this school of thought truly “save” healthcare?
At its core, Austrian Economics champions the idea that decentralized decision-making and free-market mechanisms lead to more efficient and responsive systems. In healthcare, this would mean reducing government control and allowing competition to drive innovation, lower costs, and improve quality. Proponents argue that when patients act as consumers and providers compete for their business, the system becomes more accountable and efficient. For example, direct primary care models—where patients pay physicians directly without insurance intermediaries—reflect Austrian principles and have shown promise in improving care and reducing administrative overhead.
Austrian theorists also critique the price distortions caused by third-party payers like insurance companies and government programs. According to them, when consumers are insulated from the true cost of care, demand becomes artificially inflated, leading to overutilization and waste. By restoring price signals—where patients see and respond to the actual cost of services—Austrian economists believe the market can better allocate resources and curb unnecessary spending.
However, critics argue that healthcare is not a typical market. Patients often lack the information, time, or capacity to make rational choices, especially in emergencies. Moreover, healthcare involves significant externalities and moral considerations that pure market logic may overlook. For instance, should access to life-saving treatment depend solely on one’s ability to pay? Austrian Economics offers little guidance on equity or universal access, which are central concerns in modern healthcare debates.
Austria itself provides an interesting case study. Despite the name, Austrian Economics is not the guiding philosophy behind Austria’s healthcare system. Instead, Austria operates a social insurance model with near-universal coverage, funded through mandatory contributions and managed by a mix of public and private actors. While recent reforms have aimed to streamline administration and reduce fragmentation he system remains largely collectivist—contrary to Austrian ideals.
In conclusion, Austrian Economics offers valuable insights into the inefficiencies of centralized healthcare systems and the potential benefits of market-based reforms. Its emphasis on individual choice, price transparency, and entrepreneurial innovation can inspire meaningful improvements. However, its limitations in addressing equity, access, and the unique nature of healthcare suggest that it cannot “save” the system on its own. A hybrid approach—blending market mechanisms with safeguards for universal access—may offer a more balanced path forward.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Valuing a medical practice involves assessing its financial performance, assets, and intangible factors like goodwill and patient loyalty to determine its fair market worth.
Determining the value of a medical practice is a nuanced process that blends financial analysis with strategic insight. Whether you’re preparing to sell, merge, or bring in a partner, understanding how to value your practice ensures informed decision-making and fair negotiations.
There are several recognized methods for valuing a medical practice, each suited to different scenarios. The most common include the income approach, market approach, asset-based approach, and the rule-of-thumb method.
The income approach focuses on the practice’s ability to generate future earnings. This method involves analyzing historical financial statements, projecting future cash flows, and discounting them to present value using a risk-adjusted rate. It’s particularly useful when the practice has stable revenue and predictable expenses. Key metrics include net income, physician productivity, and reimbursement rates.
The market approach compares the practice to similar ones that have recently sold. It relies on data from comparable transactions, adjusted for differences in size, specialty, location, and profitability. This method is ideal when reliable market data is available, though such data can be scarce for niche specialties or rural practices.
The asset-based approach calculates the value of tangible and intangible assets. Tangible assets include medical equipment, office furniture, and real estate. Intangible assets—like patient records, brand reputation, and goodwill—are harder to quantify but can significantly impact value. Goodwill, for instance, reflects the practice’s reputation, patient loyalty, and referral networks.
The rule-of-thumb method uses industry benchmarks, such as a multiple of annual revenue or earnings. For example, a general practice might be valued at 60–80% of annual gross revenue. While quick and easy, this method oversimplifies and may not reflect the unique strengths or weaknesses of a specific practice.https:/https://medicalexecutivepost.com/2025/03/17/medial-practice-valuation-adjustments//medicalexecutivepost.com/2025/03/17/medial-practice-valuation-adjustments/
Beyond these methods, several qualitative factors influence valuation. These include the size and diversity of the patient base, the practice’s specialty, use of technology (like EHR systems or telemedicine), and whether key physicians will remain post-sale. A practice heavily reliant on one provider may be less valuable than one with a strong team and succession plan.
Timing also matters. Economic conditions, regulatory changes, and shifts in healthcare reimbursement can affect practice value. Tax implications and deal structure—such as asset sale vs. stock sale—should also be considered during negotiations.
Ultimately, valuing a medical practice is both art and science. Engaging a professional appraiser or valuation expert can help ensure accuracy and objectivity. They bring experience, access to market data, and the ability to tailor valuation methods to your specific situation.
In summary, a comprehensive valuation considers financial performance, assets, market trends, and intangible factors. By understanding these elements, practice owners can make strategic decisions that reflect the true worth of their medical enterprise.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
What Medical School Didn’t Teach Doctors About Money
Medical school is designed to mold students into competent, compassionate physicians. It teaches anatomy, pathology, pharmacology, and clinical skills with precision and rigor. Yet, despite the depth of medical knowledge imparted, one critical area is often overlooked: financial literacy. For many doctors, the transition from student to professional comes with a steep learning curve—not in medicine, but in money. From managing debt to understanding taxes, investing, and retirement planning, medical school leaves a financial education gap that can have long-term consequences.
The Debt Dilemma
One of the most glaring omissions in medical education is how to manage student loan debt. The average medical student graduates with over $200,000 in debt, yet few are taught how to navigate repayment options, interest accrual, or loan forgiveness programs. Many doctors enter residency with little understanding of income-driven repayment plans or Public Service Loan Forgiveness (PSLF), missing opportunities to reduce their financial burden. Without guidance, some make costly mistakes—such as refinancing federal loans prematurely or choosing repayment plans that don’t align with their career trajectory.
Income ≠ Wealth
Medical students often assume that a high salary will automatically lead to financial security. While physicians do earn more than most professionals, income alone doesn’t guarantee wealth. Medical school rarely addresses the importance of budgeting, saving, and investing. As a result, many doctors fall into the “HENRY” trap—High Earner, Not Rich Yet. They spend lavishly, assuming their income will always cover expenses, only to find themselves living paycheck to paycheck. Without a solid financial foundation, even high earners can struggle to build net worth.
***
***
Taxes and Business Skills
Doctors are also unprepared for the complexities of taxes. Whether employed by a hospital or running a private practice, physicians face unique tax challenges. Medical school doesn’t teach how to track deductible expenses, optimize retirement contributions, or navigate self-employment taxes. For those who open their own clinics, the lack of business education is even more pronounced. Understanding profit margins, payroll, insurance billing, and compliance regulations is essential—but rarely covered in medical training.
Investing and Retirement Planning
Another blind spot is investing. Medical students are rarely taught the basics of compound interest, asset allocation, or retirement accounts. Many don’t know the difference between a Roth IRA and a traditional 401(k), or how to evaluate mutual funds and index funds. This lack of knowledge delays retirement planning and can lead to missed opportunities for long-term growth. Some doctors rely on financial advisors without understanding the fees or conflicts of interest involved, putting their wealth at risk.
Insurance and Risk Management
Medical school also fails to educate students on insurance—life, disability, malpractice, and health. Doctors need robust coverage to protect their income and assets, but many don’t know how to evaluate policies or understand terms like “own occupation” or “elimination period.” Inadequate coverage can leave physicians vulnerable to financial disaster in the event of illness, injury, or litigation.
Emotional and Behavioral Finance
Beyond technical knowledge, medical school overlooks the emotional side of money. Physicians often face pressure to maintain a certain lifestyle, especially after years of sacrifice. The desire to “catch up” can lead to impulsive spending, luxury purchases, and financial stress. Without tools to manage money mindset and behavioral habits, doctors may struggle with guilt, anxiety, or burnout related to finances.
The Case for Financial Education
Fortunately, awareness of this gap is growing. Organizations like Medics’ Money and podcasts such as “Docs Outside the Box” are working to fill the void by offering financial education tailored to physicians.
These resources cover everything from budgeting and debt management to investing and entrepreneurship. Some medical schools are beginning to incorporate financial literacy into their curricula, but progress is slow and inconsistent.
Conclusion
Medical school equips doctors to save lives, but it doesn’t prepare them to secure their own financial future. The lack of financial education leaves many physicians vulnerable to debt, poor investment decisions, and lifestyle inflation. To thrive both professionally and personally, doctors must seek out financial knowledge beyond the classroom. Whether through self-study, mentorship, or professional guidance, understanding money is as essential as understanding medicine. After all, financial health is a cornerstone of overall well-being—and every doctor deserves to master both.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Turning 65 is often seen as the gateway to retirement—a time to slow down, reflect, and enjoy the fruits of decades of labor. But for some, including doctors who may have faced financial setbacks, poor planning, or unexpected life events, reaching this milestone without financial security can be deeply unsettling. The image of a broke 65-year-old doctor may seem paradoxical, given the profession’s reputation for high earnings. Yet, reality paints a more nuanced picture. Fortunately, even in the face of financial hardship, retirement is not a closed door—it’s a challenge that can be met with creativity, resilience, and strategic planning.
Understanding the Situation
Before exploring solutions, it’s important to understand how a physician might arrive at retirement age without adequate savings. Medical school debt, late career starts, divorce, health issues, poor investment decisions, or supporting family members can all contribute. Some doctors work in lower-paying specialties or underserved areas, sacrificing income for impact. Others may have lived beyond their means, assuming their high salary would always be enough. Regardless of the cause, the key is to shift focus from regret to action.
Traditional retirement—ceasing work entirely—is not the only option. For a broke 65-year-old doctor, retirement may mean transitioning to a less demanding role, reducing hours, or shifting to a new field. The goal is to create a sustainable lifestyle that balances income, purpose, and well-being.
Leveraging Medical Expertise
Even if full-time clinical practice is no longer viable, a physician’s knowledge remains valuable. Here are several ways to continue earning while easing into retirement:
Telemedicine: Remote consultations are in high demand, especially in primary care, psychiatry, and chronic disease management. Telemedicine offers flexibility, reduced overhead, and the ability to work from home.
Locum Tenens: Temporary assignments can fill staffing gaps in hospitals and clinics. These roles often pay well and allow for travel or seasonal work.
Medical Writing and Reviewing: Physicians can write for journals, websites, or pharmaceutical companies. Peer reviewing, editing, and content creation are viable options.
Teaching and Mentoring: Medical schools, nursing programs, and residency programs need experienced educators. Adjunct teaching or mentoring can be fulfilling and financially helpful.
Consulting: Doctors can advise healthcare startups, legal teams, or insurance companies. Their insights are valuable in product development, litigation, and policy.
Exploring Non-Clinical Opportunities
Some physicians may wish to pivot entirely. Transferable skills—critical thinking, communication, leadership—open doors in other industries:
Health Coaching or Life Coaching: With certification, doctors can guide clients in wellness, stress management, or career transitions.
Entrepreneurship: Starting a small business, such as a tutoring service, online course, or specialty clinic, can generate income and autonomy.
Real Estate or Investing: With careful planning, investing in rental properties or learning about the stock market can create passive income.
Maximizing Government and Community Resources
At 65, individuals become eligible for Medicare, which can significantly reduce healthcare costs. Additionally, Social Security benefits may be available, depending on work history. While delaying benefits until age 70 increases monthly payments, some may need to claim earlier to meet immediate needs.
***
***
Other resources include:
Supplemental Security Income (SSI): For those with limited income and assets.
SNAP (food assistance) and LIHEAP (energy assistance): These programs help cover basic living expenses.
Community Organizations: Nonprofits and religious groups often provide support with housing, transportation, and social engagement.
Downsizing and Budgeting
Reducing expenses is a powerful way to stretch limited resources. Consider:
Relocating: Moving to a lower-cost area or state with favorable tax policies can reduce housing and living expenses.
Selling Assets: A large home, unused vehicle, or collectibles may be converted into cash.
Shared Housing: Living with family, roommates, or in co-housing communities can cut costs and reduce isolation.
Minimalist Living: Prioritizing needs over wants and embracing simplicity can lead to financial and emotional freedom.
Creating a realistic budget is essential. Track income and expenses, eliminate unnecessary costs, and prioritize essentials. Free budgeting tools and financial counseling services can help.
Financial stress can take a toll on mental health. It’s important to cultivate resilience and maintain a sense of purpose. Strategies include:
Staying Active: Physical activity improves mood and health. Walking, yoga, or swimming are low-cost options.
Volunteering: Giving back can provide structure, community, and fulfillment.
Learning New Skills: Online courses, hobbies, or certifications can reignite passion and open new doors.
Building a Support Network: Friends, family, and peer groups offer emotional support and practical advice.
Planning for the Future
Even at 65, it’s not too late to plan. Consider:
Debt Management: Negotiate payment plans, consolidate loans, or seek professional help.
Estate Planning: Create a will, designate healthcare proxies, and organize important documents.
Insurance Review: Ensure adequate coverage for health, life, and long-term care.
Financial Advising: A fee-only advisor can help create a sustainable plan without selling products.
Embracing a New Chapter
Retirement is not a destination—it’s a transition. For a broke 65-year-old doctor, it may not look like the glossy brochures, but it can still be rich in meaning. By leveraging experience, reducing expenses, accessing resources, and nurturing well-being, retirement becomes a journey of reinvention.In many ways, doctors are uniquely equipped for this challenge. They’ve faced long hours, high stakes, and complex problems. That same grit and adaptability can guide them through financial hardship and into a fulfilling retirement.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on October 20, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Understanding the Differences Between Microeconomics and Macroeconomics
Economics is the study of how societies allocate scarce resources to meet the needs and wants of individuals. It is broadly divided into two main branches: microeconomics and macroeconomics. While both aim to understand economic behavior and decision-making, they differ significantly in scope, focus, and application. Understanding these differences is essential for grasping how economies function at both individual and national levels.
Microeconomics focuses on the behavior of individual economic agents—such as consumers, firms, and households—and how they make decisions regarding resource allocation. It examines how these entities interact in specific markets, how prices are determined, and how supply and demand influence economic outcomes.
Key concepts in microeconomics include:
Demand and Supply: Microeconomics analyzes how the quantity of goods demanded by consumers and the quantity supplied by producers interact to determine market prices.
Elasticity: This measures how responsive demand or supply is to changes in price or income.
Consumer Behavior: Microeconomics studies how individuals make choices based on preferences, budget constraints, and utility maximization.
Production and Costs: It explores how firms decide on the optimal level of output and the costs associated with production.
Market Structures: Microeconomics categorizes markets into perfect competition, monopolistic competition, oligopoly, and monopoly, each with distinct characteristics and implications for pricing and output.
Microeconomic analysis is crucial for understanding how specific sectors operate, how businesses strategize, and how consumers respond to changes in prices or income. For example, a company might use microeconomic principles to determine the price point that maximizes profit or to assess the impact of a new competitor entering the market.
Macroeconomics: The Study of the Economy as a Whole
Macroeconomics, on the other hand, deals with the performance, structure, and behavior of an entire economy. It looks at aggregate indicators and phenomena, such as national income, unemployment, inflation, and economic growth. Macroeconomics seeks to understand how the economy functions at a broad level and how government policies can influence economic outcomes.
Key areas of macroeconomics include:
Gross Domestic Product (GDP): This measures the total value of goods and services produced within a country and serves as a key indicator of economic health.
Unemployment: Macroeconomics examines the causes and consequences of unemployment and the effectiveness of policies aimed at reducing it.
Inflation and Deflation: It studies changes in the general price level and their impact on purchasing power and economic stability.
Fiscal and Monetary Policy: Macroeconomics evaluates how government spending, taxation, and central bank actions influence economic activity.
International Trade and Finance: It explores exchange rates, trade balances, and the impact of globalization on national economies.
Macroeconomic analysis is essential for policymakers, economists, and financial institutions. For instance, central banks use macroeconomic data to set interest rates, while governments design fiscal policies to stimulate growth or curb inflation.
Despite their differences, microeconomics and macroeconomics are deeply interconnected. Micro-level decisions collectively shape macroeconomic outcomes. For example, widespread consumer spending boosts aggregate demand, influencing GDP and employment levels. Conversely, macroeconomic conditions—such as inflation or interest rates—affect individual behavior. A rise in interest rates may discourage borrowing and reduce consumer spending, impacting businesses at the micro level.
Economists often use insights from both branches to develop comprehensive models and forecasts. For instance, understanding consumer behavior (micro) helps predict changes in aggregate consumption (macro), which in turn informs policy decisions.
Microeconomics and macroeconomics offer distinct yet complementary perspectives on economic activity. Microeconomics provides a granular view of individual decision-making and market dynamics, while macroeconomics offers a broader understanding of national and global economic trends. Together, they form the foundation of economic theory and practice, guiding businesses, governments, and individuals in making informed decisions.
A well-rounded grasp of both branches is essential for anyone seeking to understand how economies function and evolve in an increasingly complex world.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The U.S. healthcare system is often criticized for its high costs, unequal access, and inconsistent outcomes. With nearly 30 million Americans uninsured and many more underinsured, the question arises: could socialized medicine be the solution to these systemic issues?
Socialized medicine refers to a system where the government owns and operates healthcare facilities and employs medical professionals, funded primarily through taxation. While the term is often used pejoratively in American discourse, countries like the United Kingdom and Sweden have long embraced such models. These systems guarantee universal access to healthcare, regardless of income or employment status.
One of the strongest arguments in favor of socialized medicine is its potential to reduce overall healthcare costs. In the U.S., administrative expenses, profit margins, and fragmented billing systems contribute to exorbitant prices. A centralized system could streamline operations, negotiate better drug prices, and eliminate the need for private insurance middlemen. Countries with socialized systems typically spend less per capita on healthcare while achieving comparable or better health outcomes.
Moreover, socialized medicine could address the issue of healthcare access. In the current U.S. model, losing a job often means losing health insurance. Even with the Affordable Care Act, many Americans face high premiums and deductibles. A government-run system would ensure that healthcare is a right, not a privilege, and that no one is denied care due to financial constraints.
***
***
However, critics argue that socialized medicine could lead to longer wait times, reduced innovation, and lower quality of care. They point to examples in Canada and the U.K. where patients sometimes wait weeks or months for non-emergency procedures. Additionally, skeptics fear that government control could stifle competition and reduce incentives for medical advancement.
Yet, these concerns may be overstated. Many countries with socialized systems still foster innovation through public-private partnerships and maintain high standards of care. France, for example, combines universal coverage with private providers and consistently ranks among the top healthcare systems globally.
Transitioning to socialized medicine in the U.S. would be a monumental task, requiring political will, public support, and a reimagining of healthcare financing. It would disrupt entrenched interests, including insurance companies and pharmaceutical firms. But if the goal is to create a more equitable, efficient, and humane system, socialized medicine deserves serious consideration.
In conclusion, while not a panacea, socialized medicine offers a compelling framework for addressing the deep-rooted problems in U.S. healthcare. By prioritizing access, affordability, and public health over profit, it could pave the way for a healthier and more just society.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Do you ever wish you could acquire specific information for your career activities without having to complete a university Master’s Degree or finish our entire Certified Medical Planner™ professional designation program? Well, Micro-Certifications from the Institute of Medical Business Advisors, Inc., might be the answer. Read on to learn how our three Micro-Certifications offer new opportunities for professional growth in the medical practice, business management, health economics and financial planning, investing and advisory space for physicians, nurses and healthcare professionals.
Micro-Certification Basics
Stock-Brokers, Financial Advisors, Investment Advisors, Accountants, Consultants, Financial Analyists and Financial Planners need to enhance their knowledge skills to better serve the changing and challenging healthcare professional ecosystem. But, it can be difficult to learn and demonstrate mastery of these new skills to employers, clients, physicians or medical prospects. This makes professional advancement difficult. That’s where Micro-Certification and Micro-Credentialing enters the online educational space. It is the process of earning a Micro-Certification, which is like a mini-degree or mini-credential, in a very specific topical area.
Micro-Certification Requirements
Once you’ve completed all of the requirements for our Micro-Certification, you will be awarded proof that you’ve earned it. This might take the form of a paper or digital certificate, which may be a hard document or electronic image, transcript, file, or other official evidence that you’ve completed the necessary work.
Uses of Micro-Certifications
Micro-Certifications may be used to demonstrate to physicians prospective medical clients that you’ve mastered a certain knowledge set. Because of this, Micro-Certifications are useful for those financial service professionals seeking medical clients, employment or career advancement opportunities.
Examples of iMBA, Inc., Micro-Certifications
Here are the three most popular Micro-Certification course from the Institute of Medical Business Advisors, Inc:
1. Health Insurance and Managed Care: To keep up with the ever-changing field of health care physician advice, you must learn new medical practice business models in order to attract and assist physicians and nurse clients. By bringing together the most up-to-date business and medical prctice models [Medicare, Medicaid, PP-ACA, POSs, EPOs, HMOs, PPOs, IPA’s, PPMCs, Accountable Care Organizations, Concierge Medicine, Value Based Care, Physician Pay-for-Performance Initiatives, Hospitalists, Retail and Whole-Sale Medicine, Health Savings Accounts and Medical Unions, etc], this iMBA Inc., Mini-Certification offers a wealth of essential information that will help you understand the ever-changing practices in the next generation of health insurance and managed medical care.
2. Health Economics and Finance: Medical economics, finance, managerial and cost accounting is an integral component of the health care industrial complex. It is broad-based and covers many other industries: insurance, mathematics and statistics, public and population health, provider recruitment and retention, health policy, forecasting, aging and long-term care, and Venture Capital are all commingled arenas. It is essential knowledge that all financial services professionals seeking to serve in the healthcare advisory niche space should possess.
3. Health Information Technology and Security: There is a myth that all physician focused financial advisors understand Health Information Technology [HIT]. In truth, it is often economically misused or financially misunderstood. Moreover, an emerging national HIT architecture often puts the financial advisor or financial planner in a position of maximum uncertainty and minimum productivity regarding issues like: Electronic Medical Records [EMRs] or Electronic Health Records [EHRs], mobile health, tele-health or tele-medicine, Artificial Intelligence [AI], benefits managers and human resource professionals.
Other Topics include: economics, finance, investing, marketing, advertising, sales, start-ups, business plan creation, financial planning and entrepreneurship, etc.
How to Start Learning and Earning Recognition for Your Knowledge
Now that you’re familiar with Micro-Credentialing, you might consider earning a Micro-Certification with us. We offer 3 official Micro-Certificates by completing a one month online course, with a live instructor consisting of twelve asynchronous lessons/online classes [3/wk X 4/weeks = 12 classes]. The earned official completion certificate can be used to demonstrate mastery of a specific skill set and shared with current or future employers, current clients or medical niche financial advisory prospects.
Mini-Certification Tuition, Books and Related Fees
The tuition for each Mini-Certification live online course is $1,250 with the purchase of one required dictionary handbook. Other additional guides, white-papers, videos, files and e-content are all supplied without charge. Alternative courses may be developed in the future subject to demand and may change without notice.
***
Contact: For more information, or to speak with an academic representative, please contact Ann Miller RN MHA CMP™ at Email: MarcinkoAdvisors@msn.com [24/7].