BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] E-mail: MarcinkoAdvisors1738@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
An Internet Protocol (IP) address is a numerical identifier assigned to network interfaces participating in an IP‑based network. It functions as the cornerstone of packet‑switched communication, enabling devices to locate, identify, and exchange data across interconnected networks. At a technical level, an IP address encodes both host identity and network topology, allowing routers to forward packets efficiently through hierarchical addressing structures.
IP Address Structure and Protocol Versions
The two dominant versions of the Internet Protocol—IPv4 and IPv6—define the format and semantics of IP addressing.
IPv4, defined in RFC 791, uses a 32‑bit address space. These 32 bits are typically represented in dotted‑decimal notation, divided into four octets. The address space provides possible addresses, roughly 4.3 billion. IPv4 addresses are logically divided into network and host portions, historically using classful addressing (Classes A, B, C), though modern networks rely on Classless Inter‑Domain Routing (CIDR). CIDR allows arbitrary prefix lengths, expressed as a suffix such as /24, enabling more efficient allocation and route aggregation.
IPv6, defined in RFC 8200, expands the address space to 128 bits, represented in eight groups of hexadecimal values separated by colons. The enormous address space— possible addresses—supports hierarchical routing, stateless address autoconfiguration (SLAAC), and built‑in support for multicast and anycast addressing. IPv6 eliminates broadcast traffic entirely, replacing it with more efficient multicast mechanisms.
Address Types and Scopes
IP addresses can be categorized by scope and function:
Unicast: Identifies a single network interface. Most traffic on the internet is unicast.
Multicast: Identifies a group of interfaces; packets are delivered to all group members.
Broadcast (IPv4 only): Targets all hosts on a local network segment.
Anycast (primarily IPv6): Assigned to multiple interfaces; packets are routed to the nearest instance based on routing metrics.
Additionally, addresses can be public (globally routable) or private (RFC 1918 for IPv4, Unique Local Addresses for IPv6). Private addresses require Network Address Translation (NAT) to communicate with the public internet, a workaround that became essential due to IPv4 exhaustion.
Static vs. Dynamic Assignment
IP addresses may be assigned statically or dynamically:
Static addressing involves manual configuration and is common for servers, routers, and infrastructure requiring predictable reachability.
Dynamic addressing uses the Dynamic Host Configuration Protocol (DHCP). DHCP automates address assignment, lease renewal, and configuration of parameters such as default gateways and DNS servers.
In IPv6 networks, dynamic assignment may use DHCPv6 or SLAAC. SLAAC allows hosts to generate their own addresses using router advertisements and interface identifiers, reducing administrative overhead.
Routing and Packet Delivery
IP addresses are integral to routing—the process by which packets traverse networks. When a host sends a packet, it encapsulates data in an IP header containing source and destination addresses. Routers examine the destination address and consult their routing tables to determine the next hop. Routing protocols such as OSPF, BGP, and IS‑IS maintain these tables by exchanging topology information.
The hierarchical nature of IP addressing enables route aggregation, reducing the size of global routing tables. For example, a provider may advertise a single /16 prefix representing thousands of customer networks.
DNS and Address Resolution
Human‑readable domain names must be translated into IP addresses before communication can occur. The Domain Name System (DNS) performs this translation. When a user enters a URL, the system queries DNS resolvers, which return the corresponding A (IPv4) or AAAA (IPv6) records.
On local networks, the Address Resolution Protocol (ARP) maps IPv4 addresses to MAC addresses. IPv6 uses Neighbor Discovery Protocol (NDP) for similar functionality, leveraging ICMPv6 messages.
Security and Privacy Considerations
IP addresses reveal network topology and can expose approximate geographic location. Attackers may use them for reconnaissance, scanning, or targeted attacks. Techniques such as NAT, VPNs, and IPv6 privacy extensions help mitigate exposure by masking or rotating interface identifiers.
Conclusion
An IP address is far more than a simple identifier; it is a fundamental component of the Internet Protocol suite, enabling routing, addressing, and communication across global networks. Its structure, allocation mechanisms, and interaction with routing and resolution protocols form the backbone of modern digital infrastructure. As the internet continues to scale and diversify, the role of IP addressing—particularly IPv6—remains central to the performance, security, and scalability of global communication systems.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on December 31, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
A Comparative Essay
Retirement planning is a cornerstone of financial security, and employers often provide structured plans to help employees prepare for the future. Two prominent options are Defined Benefit (DB) Plans and Cash Balance Plans. While both fall under the umbrella of employer-sponsored retirement programs, they differ significantly in design, funding, and how benefits are communicated to participants. Understanding these distinctions is essential for employers deciding which plan to offer and for employees evaluating their retirement prospects.
Defined Benefit Plans
A Defined Benefit Plan is the traditional pension model. It promises employees a specific retirement benefit, usually calculated based on a formula that considers salary history, years of service, and age at retirement. For example, a plan might provide 2% of the employee’s final average salary multiplied by years of service.
Key Features:
Employer Responsibility: The employer bears the investment risk and is obligated to deliver the promised benefit regardless of market performance.
Predictable Income: Employees receive a guaranteed monthly payment for life, often with survivor benefits.
Funding Requirements: Employers must contribute enough to meet actuarial obligations, which can be costly and complex.
Decline in Popularity: Due to high costs and liabilities, DB plans have become less common in the private sector, though they remain prevalent in government and unionized workplaces.
Advantages for Employees:
Security of lifetime income.
No need to manage investments directly.
Often includes inflation adjustments or survivor benefits.
Challenges for Employers:
Heavy funding obligations.
Sensitivity to interest rates and market fluctuations.
Long-term liabilities that can strain balance sheets.
Cash Balance Plans
***
***
A Cash Balance Plan is technically a type of Defined Benefit Plan but operates more like a hybrid between DB and Defined Contribution (DC) plans. Instead of promising a monthly pension, the plan defines benefits in terms of a hypothetical account balance. Each year, the employer credits the account with a “pay credit” (a percentage of salary or a flat dollar amount) and an “interest credit” (either a fixed rate or tied to an index).
Key Features:
Account-Based Presentation: Employees see a notional account balance that grows annually, making benefits easier to understand.
Employer Responsibility: The employer still manages investments and guarantees the interest credit, meaning the investment risk remains with the employer.
Portability: Benefits can often be rolled into an IRA or another retirement plan if the employee leaves the company.
Popularity Among Professionals: Cash Balance Plans are increasingly used by small businesses and professional practices (like medical or law firms) to allow higher contributions and tax deferrals.
Advantages for Employees:
Transparent account balance that feels similar to a 401(k).
Portability of benefits upon job change.
Potential for larger accumulations, especially for high earners.
Challenges for Employers:
Still responsible for funding and guaranteeing returns.
Requires actuarial oversight and compliance with pension regulations.
Can be complex to administer compared to pure DC plans.
Comparison
While both plans are employer-funded and fall under defined benefit rules, their differences are notable:
Aspect
Defined Benefit Plan
Cash Balance Plan
Benefit Format
Lifetime monthly pension
Hypothetical account balance
Risk
Employer bears investment risk
Employer bears investment risk
Employee Perception
Complex, formula-based
Simple, account-based
Portability
Limited
High (can roll over)
Popularity
Declining in private sector
Growing among small businesses/professionals
Conclusion
Defined Benefit Plans and Cash Balance Plans represent two approaches to retirement security. The former emphasizes guaranteed lifetime income, offering stability but imposing heavy obligations on employers. The latter modernizes the pension concept by presenting benefits as account balances, improving transparency and portability while still requiring employer guarantees. For employees, Cash Balance Plans often feel more tangible and flexible, while Defined Benefit Plans provide unmatched security. For employers, the choice depends on balancing cost, risk, and workforce needs. Ultimately, both plans underscore the importance of structured retirement savings and highlight the evolving landscape of employer-sponsored benefits.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Retirement planning has evolved significantly over the past several decades, with employers and employees seeking solutions that balance security, flexibility, and predictability. Among the various retirement plan options available today, cash balance plans stand out as a hybrid design that combines features of both traditional defined benefit pensions and defined contribution plans. Their unique structure makes them an attractive choice for employers aiming to provide meaningful retirement benefits while maintaining financial predictability.
At their core, cash balance plans are a type of defined benefit plan. Unlike traditional pensions, which promise retirees a monthly income based on years of service and final salary, cash balance plans define the benefit in terms of a hypothetical account balance. Each participant’s account grows annually through two components: a “pay credit” and an “interest credit.” The pay credit is typically a percentage of the employee’s salary or a flat dollar amount, while the interest credit is either a fixed rate or tied to an index such as U.S. Treasury yields. Although the account is hypothetical—meaning the funds are not actually segregated for each employee—the structure provides participants with a clear, understandable statement of their retirement benefit.
One of the primary advantages of cash balance plans is their transparency. Employees can easily track the growth of their account balance, much like they would with a 401(k). This clarity helps workers better understand the value of their retirement benefits and fosters a sense of ownership. Additionally, cash balance plans are portable: when employees leave a company, they can roll over the vested balance into an IRA or another qualified plan, ensuring continuity in retirement savings.
***
***
From the employer’s perspective, cash balance plans offer several benefits as well. Traditional pensions often create unpredictable liabilities, as they depend on factors such as longevity and investment performance. Cash balance plans, by contrast, provide more predictable costs because the employer commits to specific pay and interest credits. This predictability makes them easier to manage and budget for, particularly in industries where workforce mobility is high. Moreover, cash balance plans can be designed to reward long-term employees while still appealing to younger workers who value portability.
Despite these advantages, cash balance plans are not without challenges. Because they are defined benefit plans, employers bear the investment risk and must ensure the plan is adequately funded. Regulatory requirements, including nondiscrimination testing and funding rules, add complexity and administrative costs. Additionally, while cash balance plans are generally more equitable across generations of workers, transitions from traditional pensions to cash balance designs have sometimes sparked controversy, particularly among older employees who may perceive a reduction in benefits.
In recent years, cash balance plans have gained popularity among professional firms, such as law practices and medical groups, as well as small businesses seeking tax-efficient retirement solutions. These plans allow owners and highly compensated employees to accumulate larger retirement savings than would be possible under defined contribution limits, while still providing benefits to rank-and-file workers. As such, they serve as a valuable tool for both talent retention and financial planning.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
For generations, the prevailing belief in healthcare has been that physicians [MD, DO and DPM], with their high salaries and prestige, inevitably retire wealthier than nurses. Yet this assumption overlooks the financial realities of different nursing specialties and the long‑term impact of debt, lifestyle, and retirement planning. In fact, some Registered Nurses (RNs)—particularly Certified Registered Nurse Anesthetists (CRNAs), visiting nurses, and those who participate in structured pay programs like the Baylor plan—can retire richer than physicians. The reasons lie in the interplay of education costs, career flexibility, income potential, and disciplined financial planning.
Education Costs and Debt Burden
One of the most decisive factors shaping retirement wealth is the cost of education. Physicians often spend over a decade in training, including undergraduate studies, medical school, and residency. This path not only delays their earning years but also saddles them with substantial student debt. The median medical school debt in the United States exceeds $200,000, and many physicians spend years paying it down.
By contrast, RNs typically complete their training in two to four years, with advanced practice nurses such as CRNAs requiring graduate‑level education. Even so, their debt burden is far lighter, often less than half of what physicians carry. This difference means nurses can begin earning earlier, save for retirement sooner, and avoid the crushing interest payments that erode physicians’ wealth. A CRNA who starts practicing in their late twenties may already be investing in retirement accounts while a physician is still in residency earning a modest stipend.
Income Potential of Specialized Nurses
While physicians generally earn more annually than nurses, the gap is narrower in certain specialties. CRNAs, for example, are among the highest‑paid nursing professionals, with average salaries often exceeding $200,000 per year. This places them in direct competition with some physician specialties, especially primary care doctors, who may earn similar or even lower salaries.
Visiting nurses also benefit from unique financial advantages. Many work on flexible schedules, contract arrangements, or per‑visit compensation models. This allows them to maximize income while minimizing burnout. By avoiding the overhead costs of private practice and the administrative burdens physicians face, visiting nurses can channel more of their earnings directly into savings and investments.
When combined with lower debt and earlier career starts, these income streams can compound into significant retirement wealth.
The Baylor plan, a structured pay program used by some hospitals, allows nurses to work full‑time hours compressed into fewer days—often weekends—while still receiving full‑time pay and benefits. This arrangement provides several financial advantages. First, it enables nurses to earn competitive wages while freeing up weekdays for additional work, education, or entrepreneurial ventures. Second, it reduces commuting and childcare costs, allowing more income to be saved. Third, the plan often includes robust retirement benefits, such as employer‑matched contributions to 401(k) or pension programs.
Nurses who consistently participate in such structured pay plans can accumulate substantial nest eggs, often surpassing physicians who delay retirement savings due to debt repayment or lifestyle inflation. The Baylor plan highlights the importance of systematic investing: by automating contributions and focusing on long‑term growth, nurses can harness the power of compound interest. A nurse who invests steadily for 35 years may accumulate more wealth than a physician who begins saving late and inconsistently, despite earning a higher salary.
Lifestyle and Work‑Life Balance
Another overlooked factor is lifestyle. Physicians often face grueling schedules, high stress, and the temptation to maintain expensive lifestyles commensurate with their social status. Luxury homes, cars, and vacations can erode their financial base. Nurses, while not immune to lifestyle inflation, often maintain more modest spending habits.
Visiting nurses, in particular, enjoy flexibility that allows them to balance work with personal life. This reduces burnout and healthcare costs while enabling consistent employment into later years. By living within their means and prioritizing savings, nurses can accumulate wealth steadily without the financial pitfalls that sometimes accompany physician lifestyles.
Retirement Wealth Beyond Salary
Retirement wealth is not solely determined by annual income. It is shaped by debt management, savings discipline, investment strategies, and lifestyle choices. Nurses who leverage high‑paying specialties like anesthesia, flexible arrangements like visiting nursing, and structured programs like the Baylor plan can outperform physicians in these areas.
Consider two professionals: a physician earning $250,000 annually but burdened by $200,000 in debt and high living expenses, and a CRNA earning $200,000 with minimal debt and disciplined savings. Over decades, the CRNA may accumulate more net wealth, retire earlier, and enjoy greater financial security.
Conclusion
The assumption that physicians always retire richer than nurses is outdated. While physicians command higher salaries, their delayed earnings, heavy debt, and lifestyle pressures often undermine long‑term wealth. Nurses, particularly CRNAs, visiting nurses, and those who participate in structured pay programs like the Baylor plan, can retire wealthier by combining lower debt, earlier savings, competitive incomes, and disciplined financial planning.
Ultimately, retirement wealth is not about prestige but about strategy. Nurses who recognize this truth and act accordingly may find themselves enjoying more financial freedom than the very physicians they once assisted.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd and Copilot A.I.
***
***
The Baylor method of nurse payments is a scheduling and compensation model that allows nurses to work weekend shifts while receiving full-time pay and benefits, offering flexibility and helping healthcare facilities address staffing shortages.
The Baylor method, also known as the Baylor Plan or Baylor Shift, originated at Baylor University Medical Center in Dallas, Texas, as a strategic response to nurse shortages and burnout. It was designed to retain experienced nurses by offering a more flexible work schedule that still met the demands of patient care. Under this model, nurses typically work two 12-hour shifts on the weekend—Saturday and Sunday—and receive compensation equivalent to a full 40-hour workweek.
This approach has become increasingly popular in hospitals, long-term care facilities, and other healthcare settings. The core idea is simple: by concentrating work hours into the weekend, nurses gain more time off during the week while employers maintain adequate staffing during traditionally hard-to-fill shifts. For many nurses, this arrangement provides a better work-life balance, allowing them to pursue education, spend time with family, or take on additional employment during the week.
***
***
Financially, the Baylor method is attractive to both nurses and employers. Nurses benefit from full-time pay and benefits—including health insurance, retirement contributions, and paid time off—while only working two days per week. Employers, on the other hand, can reduce turnover and improve weekend staffing without increasing overall labor costs. Some facilities even offer Baylor shifts with added incentives, such as shift differentials or bonuses, to further encourage weekend coverage.
However, the Baylor method is not without its challenges. Working two consecutive 12-hour shifts can be physically and emotionally demanding, especially in high-acuity units. Nurses may experience fatigue or burnout if they are not adequately supported. Additionally, because Baylor nurses are paid for 40 hours while only working 24, scheduling extra shifts during the week can complicate overtime calculations. Typically, overtime pay only kicks in after 40 actual hours worked, not hours paid, which can lead to confusion or dissatisfaction if not clearly communicated.
From an operational standpoint, the Baylor method helps facilities maintain consistent staffing levels during weekends, which are often underserved due to lower availability of part-time or weekday-only staff. It also allows for more predictable scheduling and can improve patient outcomes by ensuring continuity of care. Facilities that adopt the Baylor model often report higher nurse satisfaction and retention rates.
In conclusion, the Baylor method of nurse payments is a creative and effective solution to some of the most persistent challenges in healthcare staffing. By offering full-time compensation for weekend work, it provides nurses with flexibility and financial stability while helping facilities maintain high-quality care. As healthcare continues to evolve, models like the Baylor shift demonstrate the importance of innovative scheduling strategies that support both caregivers and patients.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
What Medical School Didn’t Teach Doctors About Money
Medical school is designed to mold students into competent, compassionate physicians. It teaches anatomy, pathology, pharmacology, and clinical skills with precision and rigor. Yet, despite the depth of medical knowledge imparted, one critical area is often overlooked: financial literacy. For many doctors, the transition from student to professional comes with a steep learning curve—not in medicine, but in money. From managing debt to understanding taxes, investing, and retirement planning, medical school leaves a financial education gap that can have long-term consequences.
The Debt Dilemma
One of the most glaring omissions in medical education is how to manage student loan debt. The average medical student graduates with over $200,000 in debt, yet few are taught how to navigate repayment options, interest accrual, or loan forgiveness programs. Many doctors enter residency with little understanding of income-driven repayment plans or Public Service Loan Forgiveness (PSLF), missing opportunities to reduce their financial burden. Without guidance, some make costly mistakes—such as refinancing federal loans prematurely or choosing repayment plans that don’t align with their career trajectory.
Income ≠ Wealth
Medical students often assume that a high salary will automatically lead to financial security. While physicians do earn more than most professionals, income alone doesn’t guarantee wealth. Medical school rarely addresses the importance of budgeting, saving, and investing. As a result, many doctors fall into the “HENRY” trap—High Earner, Not Rich Yet. They spend lavishly, assuming their income will always cover expenses, only to find themselves living paycheck to paycheck. Without a solid financial foundation, even high earners can struggle to build net worth.
***
***
Taxes and Business Skills
Doctors are also unprepared for the complexities of taxes. Whether employed by a hospital or running a private practice, physicians face unique tax challenges. Medical school doesn’t teach how to track deductible expenses, optimize retirement contributions, or navigate self-employment taxes. For those who open their own clinics, the lack of business education is even more pronounced. Understanding profit margins, payroll, insurance billing, and compliance regulations is essential—but rarely covered in medical training.
Investing and Retirement Planning
Another blind spot is investing. Medical students are rarely taught the basics of compound interest, asset allocation, or retirement accounts. Many don’t know the difference between a Roth IRA and a traditional 401(k), or how to evaluate mutual funds and index funds. This lack of knowledge delays retirement planning and can lead to missed opportunities for long-term growth. Some doctors rely on financial advisors without understanding the fees or conflicts of interest involved, putting their wealth at risk.
Insurance and Risk Management
Medical school also fails to educate students on insurance—life, disability, malpractice, and health. Doctors need robust coverage to protect their income and assets, but many don’t know how to evaluate policies or understand terms like “own occupation” or “elimination period.” Inadequate coverage can leave physicians vulnerable to financial disaster in the event of illness, injury, or litigation.
Emotional and Behavioral Finance
Beyond technical knowledge, medical school overlooks the emotional side of money. Physicians often face pressure to maintain a certain lifestyle, especially after years of sacrifice. The desire to “catch up” can lead to impulsive spending, luxury purchases, and financial stress. Without tools to manage money mindset and behavioral habits, doctors may struggle with guilt, anxiety, or burnout related to finances.
The Case for Financial Education
Fortunately, awareness of this gap is growing. Organizations like Medics’ Money and podcasts such as “Docs Outside the Box” are working to fill the void by offering financial education tailored to physicians.
These resources cover everything from budgeting and debt management to investing and entrepreneurship. Some medical schools are beginning to incorporate financial literacy into their curricula, but progress is slow and inconsistent.
Conclusion
Medical school equips doctors to save lives, but it doesn’t prepare them to secure their own financial future. The lack of financial education leaves many physicians vulnerable to debt, poor investment decisions, and lifestyle inflation. To thrive both professionally and personally, doctors must seek out financial knowledge beyond the classroom. Whether through self-study, mentorship, or professional guidance, understanding money is as essential as understanding medicine. After all, financial health is a cornerstone of overall well-being—and every doctor deserves to master both.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 27, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
A paradox is a statement that appears at first to be contradictory, but upon reflection then makes sense. This literary device is commonly used to engage a reader to discover an underlying logic in a seemingly self-contradictory statement or phrase. As a result, paradox allows readers to understand concepts in a different and even non-traditional
***
***
GOVERNMENT HEALTH INFORMATION IS TRUSTED?
Classic Definition: Despite the PP-ACA, there is ambivalence about the role of the US Government as a source of quality healthcare information.
Modern Circumstance: Of brands presented to respondents in a Consumer Reports (50 percent), and AARP (37 percent) survey, they outpolled the “US Government Healthcare Quality Reporting Website” (36 percent) and Medicare Website (32 percent).
Paradox Example: The focus groups expressed “mixed reactions and raised doubts about government involvement in quality ratings information. At least one participant in each group expressed skepticism about trusting ‘the government’ to compile information.”
Younger consumers especially questioned the relevance of Medicare measures to the non-elderly population. Yet participants gravitated to “.gov” websites over “.org” websites as a more authoritative source.
CITE: Williams, Jason: Health Affairs, December 28, 2016
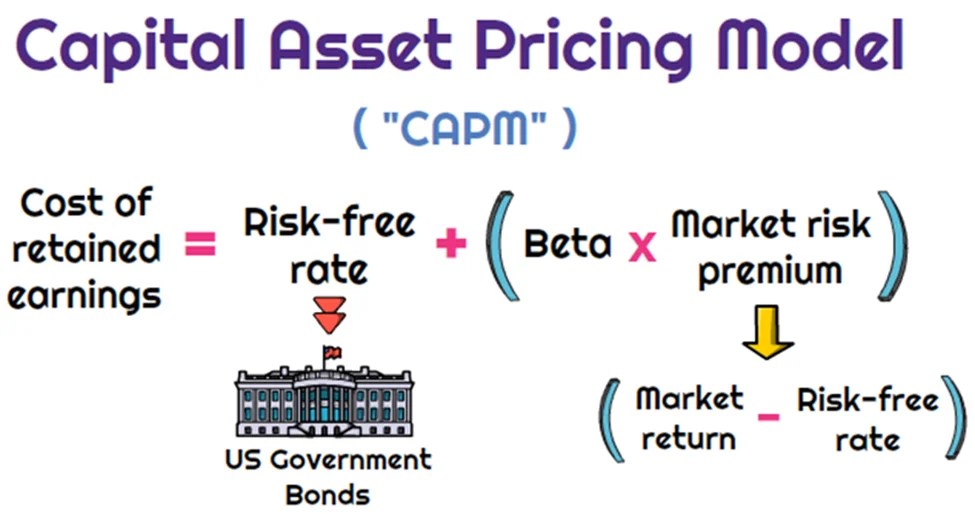
Dr. Harry Markowitz is credited with developing the framework for constructing investment portfolios based on the risk-return tradeoff. William Sharpe, John Lintner, and Jan Mossin are credited with developing the Capital Asset Pricing Model (CAPM).
CAPM is an economic model based upon the idea that there is a single portfolio representing all investments (i.e., the market portfolio) at the point of the optimal portfolio on the Capital Market Line (CML) and a single source of systematic risk, beta, to that market portfolio. The resulting conclusion is that there should be a “fair” return investors should expect to receive given the level of risk (beta) they are willing to assume.
The excess return, or return above the risk-free rate, that may be expected from an asset is equal to the risk-free return plus the excess return of the market portfolio times the sensitivity of the asset’s excess return to the market portfolio excess return. Beta, then, is a measure of the sensitivity of an asset’s returns to the market as a whole. A particular security’s beta depends on the volatility of the individual security’s returns relative to the volatility of the market’s returns, as well as the correlation between the security’s returns and the markets returns.
While a stock may have significantly greater volatility than the market, if that stock’s returns are not highly correlated with the returns of the overall market (i.e., the stock’s returns are independent of the overall market’s returns), then the stock’s beta would be relatively low. A beta in excess of 1.0 implies that the security is more exposed to systematic risk than the overall market portfolio, and likewise, a beta of less 1.0 means that the security has less exposure to systematic risk than the overall market.
MPT has helped focus investors on two extremely critical elements of investing that are central to successful investment strategies.
First, MPT offers the first framework for investors to build a diversified portfolio. Furthermore, an important conclusion that can be drawn from MPT is that diversification does in fact help reduce portfolio risk.
Thus, MPT approaches are generally consistent with the first investment rule of thumb, “understand and diversify risk to the extent possible.”
Additionally, the risk/return tradeoff (i.e., higher returns are generally consistent with higher risk) central to MPT based strategies has helped investors recognize that if it looks too good to be true, it probably is.
Passive Investing
Passive investing is a monetary plan in which an investor invests in accordance with a pre-determined strategy that doesn’t necessitate any forecasting of the economy or an individual company’s prospects. The primary premise is to minimize investing fees and to avoid the unpleasant consequences of failing to correctly predict the future. The most accepted method to invest passively is to mimic the performance of a particular index. Investors typically do this today by purchasing one or more ‘index funds’. By tracking an index, an investor will achieve solid diversification with low expenses.
An ivestor could potentially earn a higher rate of return than an investor paying higher management fees. Passive management is most widespread in the stock markets. But with the explosion of exchange traded funds on the major exchanges, index investing has become more popular in other categories of investing. There are now literally hundreds of different index funds.
Passive management is based upon the Efficient Market Hypothesis theory. The Efficient Market Hypothesis (EMH) states that securities are fairly priced based on information regarding their underlying cash flows and that investors should not anticipate to consistently out-perform the market over the long-term.
The Efficient Market Hypothesis evolved in the 1960s from the Ph.D. dissertation of Eugene Fama. Fama persuasively made the case that in an active market that includes many well-informed and intelligent investors, securities will be appropriately priced and reflect all available information. If a market is efficient, no information or analysis can be expected to result in out-performance of an appropriate benchmark. There are three distinct forms of EMH that vary by the type of information that is reflected in a security’s price:
Weak Form
This form holds that investors will not be able to use historical data to earn superior returns on a consistent basis. In other words, the financial markets price securities in a manner that fully reflects all information contained in past prices.
Semi-Strong Form
This form asserts that security prices fully reflect all publicly available information. Therefore, investors cannot consistently earn above normal returns based solely on publicly available information, such as earnings, dividend, and sales data.
Strong Form
This form states that the financial markets price securities such that, all information (public and non-public) is fully reflected in the securities price; investors should not expect to earn superior returns on a consistent basis, no matter what insight or research they may bring to the table.
While a rich literature has been established regarding whether EMH actually applies in any of its three forms in real world markets, probably the most difficult evidence to overcome for backers of EMH is the existence of a vibrant money management and mutual fund industry charging value-added fees for their services.
The notion of passive management is counterintuitive to many investors. Passive investing proponents follow the strong market theory of EMH. These proponents argue several points including;
In the long term, the average investor will have a typical before-costs performance equal to the market average. Therefore the standard investor will gain more from reducing investment costs than from attempting to beat the market over time.
The efficient-market hypothesis argues that equilibrium market prices fully reflect all existing market information. Even in the case where some of the market information is not currently reflected in the price level, EMH indicates that an individual investor still cannot make use of that information. It is widely interpreted by many academics that to try and systematically “beat the market” through active management is a fools game.
Not everyone believes in the efficient market. Numerous researchers over the previous decades have found stock market anomalies that indicate a contradiction with the hypothesis. The search for anomalies is effectively the hunt for market patterns that can be utilized to outperform passive strategies. Such stock market anomalies that have been proven to go against the findings of the EMH theory include;
Low Price to Book Effect
January Effect
The Size Effect
Insider Transaction Effect
The Value Line Effect
All the above anomalies have been proven over time to outperform the market. For example, the first anomaly listed above is the Low Price to Book Effect. The first and most discussed study on the performance of low price to book value stocks was by Dr. Eugene Fama and Dr. Kenneth R. French. The study covered the time period from 1963-1990 and included nearly all the stocks on the NYSE, AMEX and NASDAQ. The stocks were divided into ten subgroups by book/market and were re-ranked annually. In the study, Fama and French found that the lowest book/market stocks outperformed the highest book/market stocks by a substantial margin (21.4 percent vs. 8 percent). Remarkably, as they examined each upward decile, performance for that decile was below that of the higher book value decile. Fama and French also ordered the deciles by beta (measure of systematic risk) and found that the stocks with the lowest book value also had the lowest risk.
Today, most researchers now deem that “value” represents a hazard feature that investors are compensated for over time. The theory being that value stocks trading at very low price book ratios are inherently risky, thus investors are simply compensated with higher returns in exchange for taking the risk of investing in these value stocks. The Fama and French research has been confirmed through several additional studies. In a Forbes Magazine 5/6/96 column titled “Ben Graham was right–again,” author David Dreman published his data from the largest 1500 stocks on Compustat for the 25 years ending 1994. He found that the lowest 20 percent of price/book stocks appreciably outperformed the market.
One item a medical professional should be aware of is the strong paradox of the efficient market theory. If each investor believes the stock market were efficient, then all investors would give up analyzing and forecasting. All investors would then accept passive management and invest in index funds. But if this were to happen, the market would no longer be efficient because no one would be scrutinizing the markets. In actuality, the efficient market hypothesis actually depends on active investors attempting to outperform the market through diligent research.
The case for passive investing and in favor of the EMH is that a preponderance of active managers do actually underperform the markets over time. The latest study by Standard and Poor’s (S&P) confirms this fact. S&P recently compared the performance of actively-managed mutual funds to passive market indexes twice per year. The 2012 S&P study indicated that indexes were once again outperforming actively-managed funds in nearly every asset class, style and fund category. The lone exception in the 2012 report was international equity, where active outperformed the index that S&P chose. The study examined one-year, three-year and five-year time periods. Within the U.S. equity space, active equity managers in all the categories failed to outperform the corresponding benchmarks in the past five year period. More than 65 percent of the large-cap active managers lagged behind the S&P 500 stock index. More than 81 percent of mid-cap mutual funds were outperformed by the S&P MidCap 400 index.
Lastly, 77 percent of the small-cap mutual funds were outperformed by the S&P SmallCap 600 index. U.S. bond active managers fared no better that equity managers over a five year period. More than 83 percent of general municipal mutual funds under-performed the S&P National AMT-Free Municipal Bond index, 93 percent of government long-term funds under-performed the Barclays Long Government index, nearly 95 percent of high yield corporate bond funds under-performed the Barclays High Yield index. Although the performance measurements for index investing are very strong, many analysts find three negative elements of passive investing;
Downside Protection: When the stock market collapses like in 2008, an index investor will assume the same loss as the market. In the case of 2008, the S&P 500 stock index fell by more than 50 percent, offering index investors no downside protection.
Portfolio Control: An index investor has no control over the holdings in the fund. In the event that a certain sector becomes over-owned (i.e. technology stocks in 2000), an index investor maintains the same weight as the index.
Average Returns: An index investor will never have the opportunity to outperform the market, but will always follow. Although the markets are very efficient, an investor can perhaps take advantage of market anomalies and invest with those managers who have maintained a long-term performance edge over the respective index.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
If you’re looking at this tab, chances are you are fed up with your financial brokerage accounts, thinking of finances, investing, retirement or all of the above.
And so, we can help
An investment portfolio second opinion, also called a “ portfolio review,” is an analysis of your financial holdings and associated strategies, allocations, fees and performance to determine whether the most effective instruments and methodologies are being utilized to reach your goals.
No Worries! You may have come to the right place.
E-Mail Ann Miller RN MHA CPHQ for an Initial Appointment: MarcinkoAdvisors@outlook.com
The purpose of this initial appointment is for you to ask a lot of questions to make sure you are comfortable with potentially working with us. It also helps if you are prepared to provide a verbal summary of your current situation.
Here are some questions to consider asking us during your first meeting:
1) Can you tell us about your financial qualifications, experience, education and training; if any?
2) Can you provide some information about your current financial advisory team?
3) On what type of investments do you typically purchase and own?
5) How much do pay your financial management firm?
6) How long have you been working with your current financial management firm?
8) What other services does your financial team provide?
An investment advisor (sometimes spelled “investment adviser”) is defined as a company or person who has a government registration allowing them to choose, manage and recommend investments for clients. Investment advisors are also sometimes referred to as stock brokers. They are not fiduciaries.
Unlike other financial advisors who may not be regulated, investment advisors are regulated by their state or the Securities Exchange Commission depending on how much money they manage. Investment advisors may also offer services like retirement planning.
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
A hedge fund is a limited partnership of private investors whose money is pooled and managed by professional fund managers. These managers use a wide range of strategies, including leverage (borrowed money) and the trading of nontraditional assets, to earn above-average investment returns. A hedge fund investment is often considered a risky, alternative investment choice and usually requires a high minimum investment or net worth. Hedge funds typically target wealthy investors.
My medical practice has a small self-directed pension plan with profit sharing features.
QUESTION: Can my medical practice’s retirement plan invest in a hedge fund?
Such a pension fund falls under a category called self-directed “plan” assets.
Among the rules are that each participant in the plan counts toward the 100 investor maximum under which most hedge funds operate, that each plan participant be a fully accredited investor, and that the hedge fund keep investments such as pension plans and other funds covered under ERISA to less than 25 percent of total assets under management.
Some retired people live on a fixed income and many of them live right on the edge of their financial capability. At some time in their life, they may have to make a choice regarding many purchases.
In this case, we will illustrate “choice” using a couple’s purchase of Long-Term-Care Insurance [LTCI]. Of course, economics is the study of choice; wants, needs and scarcity, etc. In our case, if they decide to make the purchase they commit to a lifetime of premium payments. The financial tradeoff is this; if they make the commitment to purchase LTCI, they must give up something else.
EXAMPLE: In order to maintain a monthly premium of $100 ($1,200per year), an elderly patient, retired layman or couple must essentially relegate about $30,000 of financial assets to generate the $100 necessary to make an average premium payment (assumes a 7% rate of return with 4% withdrawal rate) or [4% X $30,000 = $1,200 year]. Thus, if the monthly premium cost is $500 per month, the elder must give up the use of $150,000 of retirement asset just to generate enough cash flow to pay for the LTC insurance.
***
***
The married elder couple has to make the Hobson’s Choice decision among lifestyle (dinners, vacations, gifts to children, prescription drugs, medical care or food and shelter) versus paying an insurance premium to provide for nursing home coverage for a need, which may be very real, but will not occur until sometime in the ambiguous future.
And so, when faced with such a tough economics Hobson’s Medicine Choice, neither of which delivers peace of mind or a respectable solution; many will simply decide that, in either case, they may already end up impoverished. Thus, many will often opt for the better lifestyle now … while they can enjoy it … together.
Cite: Anonymous Health Insurance Agent, Norcross, Georgia
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals.
Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed.
Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Posted on April 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
OVER HEARD IN THE FINANCIAL ADVISOR’S LOUNGE
***
***
By Perry D’Alessio, CPA [D’Alessio Tocci & Pell LLP]
What I see in my accounting practice is that significant accumulation in younger physician portfolio growth is not happening as it once did. This is partially because confidence in the equity markets is still not what it was; but that doctors are also looking for better solutions to support their reduced incomes.
For example, I see older doctors with about 25 percent of their wealth in the market, and even in retirement years, do not rely much on that accumulation to live on. Of this 25 percent, about 80 percent is in their retirement plan, as tax breaks for funding are just too good to ignore.
What I do see is that about 50 percent of senior physician wealth is in rental real estate, both in a private residence that has a rental component, and mixed-use properties. It is this that provides a good portion of income in retirement.
***
***
QUESTION: So, could I add dialog about real estate as a long term solution for retirement?
Yes, as I believe a real estate concentration in the amount of 5 percent is optimal for a diversified portfolio, but in a very passive way through mutual or index funds that are invested in real estate holdings and not directly owning properties.
Today, as an option, we have the ability to take pension plan assets and transfer marketable securities for rental property to be held inside the plan collecting rents instead of dividends.
Real estate holdings never vary very much, tend to go up modestly, and have preferential tax treatment due to depreciation of the property against income.
Posted on April 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Beneficiary designations can provide a relatively easy way to transfer an account or insurance policy upon your death. However, if you’re not careful, missing or outdated beneficiary designations can easily cause your estate plan to go awry.
Where you can find them
Here’s a sampling of where you’ll find beneficiary designations:
In several states, so-called “lady bird” deeds for real estate
***
***
10 tips about beneficiary designations
Because beneficiary designations are so important, keep these things in mind in your estate planning:
Remember to name beneficiaries. If you don’t name a beneficiary, one of the following could occur:
The account or policy may have to go through probate. This process often results in unnecessary delays, additional costs, and unfavorable income tax treatment.
The agreement that controls the account or policy may provide for “default” beneficiaries. This could be helpful, but it’s possible the default beneficiaries may not be whom you intended.
Name both primary and contingent beneficiaries. It’s a good practice to name a “back up” or contingent beneficiary in case the primary beneficiary dies before you. Depending on your situation, you may have only a primary beneficiary. In that case, consider whether it may make sense to name a charity (or charities) as the contingent beneficiary.
Update for life events. Review your beneficiary designations regularly and update them as needed based on major life events, such as births, deaths, marriages, and divorces.
Read the instructions. Beneficiary designation forms are not all alike. Don’t just fill in names — be sure to read the form carefully. If necessary, you can draft your own customized beneficiary designation, but you should do this only with the guidance of an experienced attorney or tax advisor.
Coordinate with your will and trust. Whenever you change your will or trust, be sure to talk with your attorney about your beneficiary designations. Because these designations operate independently of your other estate planning documents, it’s important to understand how the different parts of your plan work as a whole.
Think twice before naming individual beneficiaries for particular assets. For example, you may establish three accounts of equal value initially and name a different child as beneficiary of each account. Over the years, the accounts may grow or be depleted unevenly, so the three children end up receiving different amounts — which is not what you originally intended.
Avoid naming your estate as beneficiary. If you designate a beneficiary on your 401(k), for example, it won’t have to go through probate court to be distributed to the beneficiary. If you name your estate as beneficiary, the account will have to go through probate. For IRAs and qualified retirement plans, there may also be unfavorable income tax consequences.
Use caution when naming a trust as beneficiary. Consult your attorney or CPA before naming a trust as beneficiary for IRAs, qualified retirement plans, or annuities. There are situations where it makes sense to name a trust — for example if:
Your beneficiaries are minor children
You’re in a second marriage
You want to control access to funds
Be aware of tax consequences. Many assets that transfer by beneficiary designation come with special tax consequences. It’s helpful to work with an experienced tax advisor to help provide planning ideas for your particular situation.
Use disclaimers when necessary — but be careful. Sometimes a beneficiary may actually want to decline (disclaim) assets on which they’re designated as beneficiary. Keep in mind that disclaimers involve complex legal and tax issues and require careful consultation with your attorney and CPA.
Posted on April 11, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Why would a doctor consider a Roth IRA conversion?
By Staff Reporters
***
***
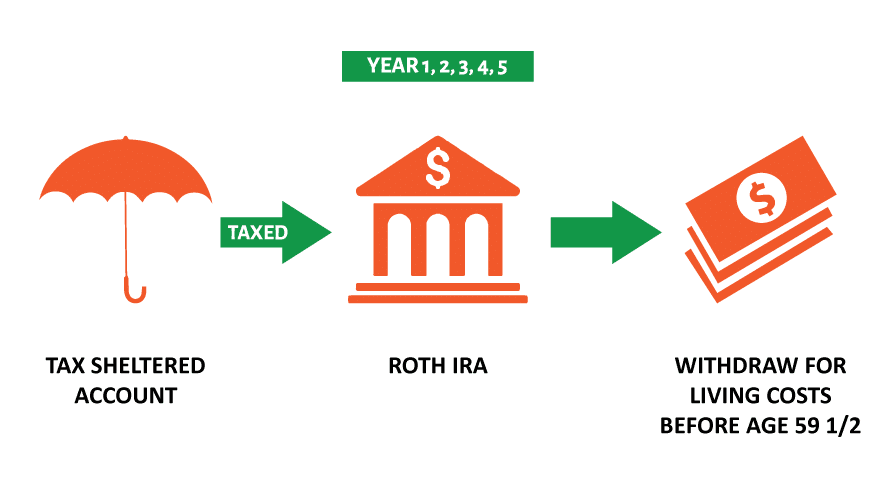
A Roth conversion involves transferring funds from a traditional retirement account—such as a 401(k), 403(b), or individual retirement account (IRA) funded with pre-tax dollars—into a Roth IRA.
The biggest benefit lies in the tax treatment of the converted funds. Once the funds are in the Roth IRA, future growth of those assets is tax-free. Withdrawals in retirement are also tax-free, assuming they meet certain criteria. As with any strategy, there are important considerations to keep in mind.
When you convert funds to a Roth IRA, the amount converted is taxable income in that tax year. For example, if you convert $100,000 from a traditional IRA to a Roth IRA, that $100,000 will be added to your taxable income in the conversion year.
Converting large amounts can result in a significant tax bill and may push you into a higher tax bracket. Even so, using retirement funds to pay taxes may make sense for those looking to convert large IRAs to reduce their future required minimum distributions (RMDs).
The timing of your Roth conversion matters too. Generally, it’s a good idea to convert when your income is lower—for example, after you’ve retired and before you begin drawing Social Security. You may also choose to convert over the course of several years to spread out the tax impacts. But if you can get comfortable with these considerations, a Roth conversion can provide you with benefits beyond tax-free growth and withdrawals.
Some of these benefits are:
Tax diversification. Having both traditional and Roth accounts allows you to manage your tax liability in retirement. For example, if your income in a given year is higher than expected, you can withdraw from the Roth IRA without increasing your taxable income.
No RMDs. Traditional IRAs and 401(k)s require you to begin taking RMDs at age 73. Roth IRAs have no RMD requirement during your lifetime. With a Roth account, you have more control over your retirement withdrawals and can leave the funds to grow for your heirs.
Benefits for heirs. Roth IRAs can be passed on to beneficiaries, who can inherit the account income tax-free. This means your heirs can enjoy the tax-free growth and withdrawals if the Roth IRA has been held for five years or more—a significant advantage, especially if your beneficiaries are in a higher tax bracket.
Posted on April 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Ann Miller RN MHA CPHQ CMP™
***
***
Finally … Fiduciary second investing and financial planning opinions right here!
Telephonic or electronic advice for medical professionals that is:
Objective, affordable, medically focused and financially personalized
Rendered by a pre-screened financial consultant for doctors and medical professionals
Offered on a pay-as-you-go basis, by phone or secure e-mail transmission
The iMBA Discussion Forum™ is a physician-to-financial advisor telephone or e-mail portal that connects independent financial professionals to doctors, nurses or healthcare executives desiring affordable and unbiased financial planning advice.
Medical professionals and healthcare executives can now receive direct access to pre-screened iMBA professionals in the areas of Investing, Financial Planning, Asset Allocation, Portfolio Management, Insurance, Mortgage and Lending, Human Resources, Retirement Planning and Employee Benefits. To assist our medical professional and healthcare executive members, we can be contracted with per-minute or per-project fees, and contacted by client phone, email or secure instant messaging.
Posted on March 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEdCMP®
***
***
Your Executor or personal representative is named in your Will and is responsible for management of assets subject to probate. A basic checklist of the duties of the personal representative looks like this:
Gather all estate assets;
Collect all amounts owed the decedent;
Notify creditors and paying all valid debts;
Selling assets as needed to pay expenses or as directed by the Will;
Distribute assets to beneficiaries;
File decedents final federal income tax return;
File an estate tax return if the estate is large enough; and
File inventories and annual returns with the probate court, if required.
The position requires a lot of responsibility and involves many duties and a considerable commitment of time. The personal representative must petition the probate court for formal appointment.
Selection of your personal representative should not be made lightly, or as a favor to a friend. It requires a lot of work and very often for little or no pay. Friends and family typically will not charge the estate for their time and work. Outside advisers like attorneys and accountants will not hesitate to bill for their work effort. A few items for your selection criteria should be:
Longevity – the person should have a likelihood of being able to serve after your death;
Skill in managing legal and financial affairs;
Familiarity with your estate and wishes;
Integrity and loyalty; and
Impartiality and absence of conflicts of interest.
Alternatives to family or friends might be a corporate executor, such as a bank, an attorney, or other adviser. Similar criteria should be used in the selection of a trustee.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
9. We act with honesty, integrity and are always straightforward. 8. We strive to be innovative, creative, iconoclastic, and flexible. 7. We admit and learn from mistakes and don’t repeat them. 6. We work hard always as competitors are trying to catch up. 5. We treat others with dignity and respect. 4. We are the onus of consulting advice for the well being of others. 3. We fight complacency as former success is in the past. 2. The best management styles are timeless, not timely. 1. Our clients are colleagues and always come first.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
In retirement, according to Josephine Nesbit, your economic class can be broadly categorized into four distinct groups, each defined by their net worth and financial capabilities, ranging from retirees with limited resources to the wealthy. And, according to Moneywise, here are the net worth categories of the poor, middle class (and upper-middle class) and rich:
Poor retirees: Poor retirees are in the lower 20th percentile, and may have a net worth of around $10,000. This is often without property ownership, forcing many to rely mainly on Social Security or minimal pensions.
Middle-class retirees: Making up the 50th percentile, with a median net worth of approximately $281,000, this group usually includes home equity, retirement savings and a 401(k) plan.
Upper-middle-class retirees: These retirees possess a net worth between $201,800 and $608,900. They have diversified assets and enjoy a comfortable retirement cushion.
Rich retirees: In the 90th percentile, with net worth starting at $1.9 million, this group has much more financial freedom and is able to afford luxuries and legacy planning.
Posted on February 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The U.S. added 143,000 jobs in January, fewer than economists expected, but the unemployment rate inched down to 4% from 4.1%, beating forecasts. Forecasters surveyed by Dow Jones had anticipated 169,000 payroll gains in January, after a surprisingly large 256,000 jump in December.
Last month, the Securities and Exchange Commission said Vanguard would pay more than $100 million to settle charges for misleading statements related to capital gains distributions and tax consequences for retail investors who held Vanguard Investor Target Retirement Funds in taxable accounts.
Major U.S. equities indexes moved lower to close out the trading week as the January jobs report showed slower-than-expected hiring but a down tick in the unemployment rate. Despite the slump in job additions, the overall resilience in the labor market could encourage the Federal Reserve to hold off on additional interest-rate cuts. The S&P 500 and the Dow ended Friday’s session with daily losses of roughly 1.0%. The tech-heavy NASDAQ fell 1.4%.
Most notable this month is the appointment of Tim Noel as the new CEO of UnitedHealthcare after former CEO Brian Thompson was fatally shot in New York City in December.
Visualize: How private equity tangled banks in a web of debt, from the Financial Times.
(“Informed Voice of a New Generation of Fiduciary Advisors for Healthcare”)
For most lay folks, personal financial planning typically involves creating a personal budget, planning for taxes, setting up a savings account and developing a debt management, retirement and insurance recovery plan. Medicare, Social Security and Required Minimal Distribution [RMD] analysis is typical for lay retirement. Of course, we can assist in all of these activities, but lay individuals can also create and establish their own financial plan to reach short and long-term savings and investment goals.
But, as fellow doctors, we understand better than most the more complex financial challenges doctors can face when it comes to their financial planning. Of course, most physicians ultimately make a good income, but it is the saving, asset and risk management tolerance and investing part that many of our colleagues’ struggle with. Far too often physicians receive terrible guidance, have no time to properly manage their own investments and set goals for that day when they no longer wish to practice medicine.
For the average doctor or healthcare professional, the feelings of pride and achievement at finally graduating are typically paired with the heavy burden of hundreds of thousands of dollars in student loan debt.
You dedicated countless hours to learning, studying, and training in your field. You missed birthdays and holidays, time with your families, and sacrificed vacations to provide compassionate and excellent care for your patients. Amidst all of that, there was no time to give your finances even a second thought.
Between undergraduate, medical school, and then internship and residency, most young physicians do not begin saving for retirement until late into their 20s, if not their 30s. You’ve missed an entire decade or more of allowing your money and investments to compound and work for you. When it comes to addressing your financial health and security, there’s no time to waste.
Academic Team of Internationally Known Contributors
D. E. Marcinko & Associates is one of the most academically published authorities on the topic of financial planning and private wealth management for physicians, nurses and medical professionals. We have published 33 major peer reviewed textbooks redacted in the Library of Medicine, Institute of Health and the Library of Congress, in four languages, with over 5,025 online white papers, web-posts and related publications. These cover a range of financial planning topics from medical malpractice, risk management and insurance, to investment policy statement analysis and endowment funding management, and to taxation, retirement, estate and legacy planning.
Financial planning, business and strategic management, FMV for practice and clinics and related “hard” topics are included.
***
We also include “soft” subjects from investor psychology, ethics and lost fortunes to luxury spending, from understanding the middle-class millionaire to the political philosophies of physicians and the affluent. Our corpus of work is regularly consulted by doctors, medical, business, graduate and nursing schools, to elite advisors, private and investment bankers, wealth managers, venture capitalists, academics and the press.
Posted on December 21, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Ann Miller RN MHACMP™
INTRODUCING OUR NEXT GENERATION e-BOOK LIBRARYFROM iMBA, Inc.
An e-book is an electronic or digital book that can be read on a computer or a handheld device.
Our new e-books consists of text, images, and are fixed to a specific spot on the page.
And, our e-books are a data files similar in content and structure to a word-processing document that comes in a PDF format. To use our e-books, you need to purchase and download it to a device that has a .pdf file reader app, such as ADOBE® or similar on a smartphone, tablet or computer. A PDF, also known as a portable document format, is the format most people are familiar with and used in our e-books. PDFs are known for their ease of use and ability to hold custom layouts. They are the most commonly used e-Book formats, especially by professionals and adult-learners.
You can then access the e-book and read it, or highlight pages and even take side notes.
e-Books Save Money
With no manufacturing, printing, binding or shipping costs, e-Books are cheaper than traditional hard or paper back books.The price of each specialized and highly niche focused e-Book [50-100 pages] is only $25, whereas similar paperback printed books of this type generally cost $145, or more!
With the PP-ACA, increased compliance regulations and higher tax rates impending from the Biden administration – not to mention the corona pandemic, venture capital based healthcare corporations and telehealth – physicians are more concerned about their retirement and retirement planning than ever before; and with good reason. After payroll taxes, dividend taxes, limited itemized deductions, the new 3.8% surtax on net investment income and an extra 0.9% Medicare tax, for every dollar earned by a high earning physician, almost 50 cents can go to taxes!
Introduction
Retirement planning is not about cherry picking the best stocks, ETFs or mutual funds or how to beat the short term fluctuations in the market. It’s a disciplined long term strategy based on scientific evidence and a prudent process. You increase the probability of success by following this process and monitoring on a regular basis to make sure you are on track.
General Surveys
According to a survey from the Employee Benefit Research Institute [EBRI] and Greenwald & Associates; nearly half of workers without a retirement plan were not at all confident in their financial security, compared to 11 percent for those who participated in a plan, according to the 2014 Retirement Confidence Survey (RCS).
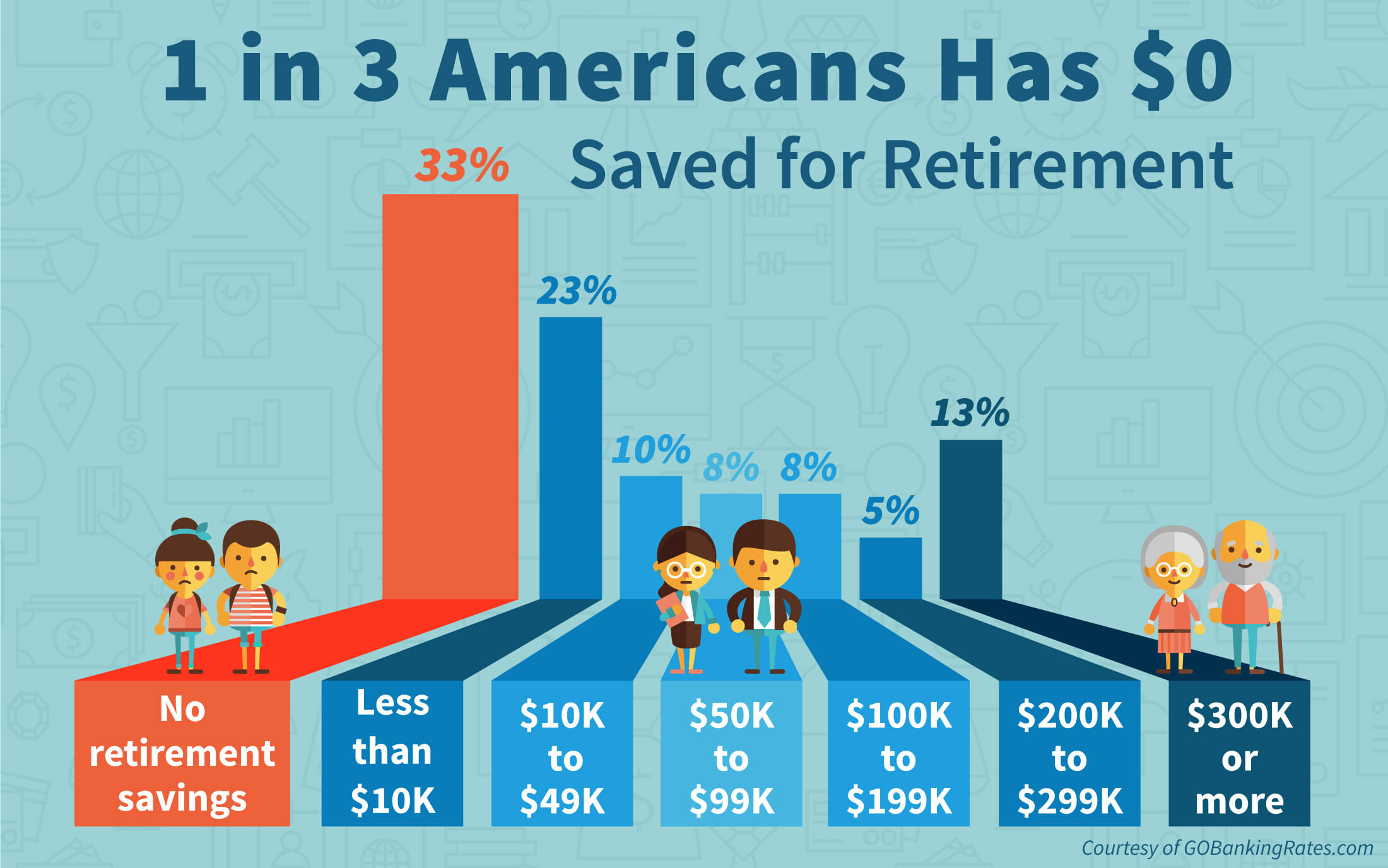
In addition, 35 percent of workers have not saved any money for retirement, while only 57 percent are actively saving for retirement. Thirty-six percent of workers said the total value of their savings and investments—not including the value of their home and defined benefit plan—was less than $1,000, up from 29 percent in the 2013 survey. But, when adjusted for those without a formal retirement plan, 73 percent have saved less than $1,000.
Debt is also a concern, with 20 percent of workers saying they have a major problem with debt. Thirty-eight percent indicate they have a minor problem with debt. And, only 44 percent of workers said they or their spouse have tried to calculate how much money they’ll need to save for retirement. But, those who have done the calculation tend to save more.
The biggest shift in the 24 years has been the number of workers who plan to work later in life. In 1991, 84 percent of workers indicated they plan to retire by age 65, versus only 9 percent who planned to work until at least age 70. In 2014, 50 percent plan on retiring by age 65; with 22 percent planning to work until they reach 70.
Physician Statistics
Now, compare and contrast the above to these statistics according to a 2018 survey of physicians on financial preparedness by American Medical Association [AMA] Insurance. The statistics are still alarming:
The top personal financial concern for all physicians is having enough money to retire.
Only 6% of physicians consider themselves ahead of schedule in retirement preparedness.
Nearly half feel they were behind
41% of physicians average less than $500,000 in retirement savings.
Nearly 70% of physicians don’t have a long term care plan.
Only half of US physicians have a completed estate plan including an updated will and Medical directives.
Thoughts to Ponder
And so, to help make your golden years comfortable and worry free, here are ten important retirement questions for all physicians to consider:
How much money do you need to retire?
What is your retirement cash flow?
What is your retirement vision?
How to stay on retirement track?
How to maximize retirement plan contributions such as 401(k) or 403(b)?
How to maximize retirement income from retirement plans?
What are some other retirement plan savings options?
What is your retirement plan and investing style?
What is the role of social security in retirement planning?
How to integrate retirement with estate planning?
The opinion of a competent Certified Medical Planner® can assist.
ASSESSMENT: Your thoughts, comments and input are appreciated.
Posted on November 17, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
The number of people living with Alzheimer’s disease is growing. The ripple effect is straining families, communities, and the healthcare system, yet talking about the disease on a personal level can be difficult.
November is Alzheimer’s Awareness Month because it can happen in any family, and because it’s worth talking about the challenges of living with or caring for someone with this disease.
You may notice splashes of teal and purple sprouting up this November, as both colors are associated with Alzheimer’s awareness. Teal is the color of the Alzheimer’s Foundation of America, chosen for its calming effect. Purple is the signature color of the Alzheimer’s Foundation, which stands for strength in the fight against Alzheimer’s disease.
Posted on November 16, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The Internal Revenue Service (IRS) ruled that employees at an unnamed company can designate a portion of their employer match to student debt repayments or health reimbursement accounts, in addition to their traditional 401(k).
Warren Buffett’s Midas touch gave a boost to Domino’sPizza and PoolCorp. after Berkshire Hathaway announced it has bought shares of both companies. Domino’s popped to start the day but dropped 1.27%, while Pool climbed just 0.54%.
Palantir is jumping ship, moving from the NYSE to the Nasdaq. Shareholders liked the move, pushing the stock up 11.14%.
Bloom Energy…bloomed 59.19% on the news that the renewable energy company reached an agreement to provide utility company American Electric Power with 1 gigawatt worth of fuel cells.
STOCKS DOWN
What Buffett giveth, Buffett taketh away: Apple sank on the news that Berkshire Hathaway has sold shares of the company, and almost completely eliminated its position in UltaBeauty. Apple fell 1.41%, while Ulta Beauty dropped 4.60%.
Shareholders were expecting the worst from Chinese online retailer Alibaba, and although the company actually beat earnings forecasts, it wasn’t enough—shares still sank 2.20%.
Applied Materials tumbled 9.20% after beating both top and bottom line expectations, but shareholders balked at the slowdown in several key businesses.
Here’s where the major stock market benchmarks ended:
The SPX fell 78.55 points (–1.32%) to 5,870.62 to end the week down 2.08%; the Dow Jones Industrial Average® ($DJI) lost 305.87 points (–0.70%) to 43,444.99 to end the week down 1.24%; and the NASDAQ Composite®($COMP) decreased 427.52 points (–2.24%) to 18,680.12 to end the week down 3.15%.
The 10-year Treasury note yield rose one basis point to 4.43% but added 12 basis points for the week. Shorter-term yields rose less.
The CBOE Volatility Index® (VIX) climbed sharply to 16.11 as stocks fell.
The problems at storied bond manager Western Asset Management keep growing. Clients have pulled about $55 billion from Wamco, as the division is known, since mid-August, representing about 15% of its assets. Franklin Templeton, its 77-year-old parent company and one of the largest asset managers in the U.S., recently reported its steepest quarterly outflows on record.
Visualize: How private equity tangled banks in a web of debt, from the Financial Times.
A defined benefit (DB) pension plan is a type of pension plan in which an employer/sponsor promises a specified pension payment, lump-sum or combination thereof on retirement that is predetermined by a formula based on the employee’s earnings history, tenure of service and age, rather than depending directly on individual investment returns.
Traditionally, many governmental and public entities, as well as a large number of corporations, provide defined benefit plans, sometimes as a means of compensating workers in lieu of increased pay.
CITE: Wikipedia
Defined Contribution Pension Plan
A defined contribution (DC) plan is a type of retirement plan in which the employer, employee or both make contributions on a regular basis. Individual accounts are set up for participants and benefits are based on the amounts credited to these accounts (through employee contributions and, if applicable, employer contributions) plus any investment earnings on the money in the account. In defined contribution plans, future benefits fluctuate on the basis of investment earnings.
The most common type of defined contribution plan is a savings and thrift plan. Under this type of plan, the employee contributes a predetermined portion of his or her earnings (usually pretax) to an individual account, all or part of which is matched by the employer.
Although some might view a budget as unnecessarily restrictive, sticking to a spending plan can be a useful tool in enhancing the wealth of a medical practice. So, I will emphasize keys to smart budgeting and how to track spending and savings in these tough economic times.
There is an aphorism that suggests, “Money cannot buy happiness.” Well, this may be true enough but there is also a corollary that states, “Having a little sure reduces the unhappiness.”
Unfortunately, today there is more than a little financial unhappiness in all medical specialties. The challenges range from the commoditization of medicine, aging demographics, Medicare reimbursement cutbacks and increased competition to floundering equity markets, the home mortgage crisis, the squeeze on credit and declines in the value of a practice. Few doctors seem immune to this “perfect storm” of economic woes.
Far too many physicians are hurting and it is not limited to above-average earning professionals. However, one can strive to reduce the pain by following some basic budgeting principles. By adhering to these principles, physicians can eliminate the “too many days at the end of the month” syndrome and instead develop a foundation for building real wealth and security, even in difficult economic climates like we face today.
There are three major budget types. A flexible budget is an expenditure cap that adjusts for changes in the volume of expense items. A fixed budget does not. Advancing to the next level of rigor, a zero-based budget starts with essential expenses and adds items until the money is gone. Regardless of type, budgets can be extremely effective if one uses them at home or the office in order to spot money troubles before they develop.
For the purpose of wealth building, doctors may think of this budget as a quantitative expression of an action plan. It is an integral part of the overall cost-control process for the individual, his or her family unit or one’s medical practice.
Preparing a net income statement (lifestyle cash flow budget) is often difficult because many doctors perceive it as punitive. Most doctors do not live a disciplined spending lifestyle and they view a budget as a compromise to it. However, a cash flow budget is designed to provide comfort when there is surplus income that can be diverted for other future needs. For example, if you treat retirement savings as just another periodic bill, you are more likely to save for it.
You may construct a personal cash budget by recording each cash receipt and cash disbursement on a spreadsheet. Only the date, amount and a brief description of the transaction are necessary. The cash budget is a simple tool that even doctors who lack accounting acumen can use. Since it is possible to track the cash-in and cash-out in the same format used for a standard check register, most doctors find that the process takes very little time. Such a budget will provide a helpful look at how well you are staying within available resources for a given period.
We then continue with an analysis of your operating checkbook and a review of various source documents such as one’s tax return, credit card statements, pay stubs and insurance policies. A typical statement will show all cash transactions that occur within one year. It is helpful to establish a monthly equivalent to all items of income and expense. For the purposes of getting started, note items of income and expense by the frequency you are accustomed to receiving or spending them.
What You Should Know About The ‘Action Plan’ Cash Budget
For a medical office, the first operations budget item might be salary for the doctor and staff. Operating assets and other big ticket items come next. Some of our doctors/clients review their office P&L statements monthly, line by line, in an effort to reduce expenses. Then they add back those discretionary business expenses they have some control over.
Now, do you still run out of money before the end of the month? If so, you had better cut back on entertainment, eating dinner out or that fancy, new but unproven piece of medical equipment. This sounds draconian until you remind yourself that your choice is either: live frugally later or live a simpler lifestyle now and invest the difference.
As a young doctor, it may be a difficult trade-off. By mid-life, however, you are staring retirement in the face. That is why the action plan depends on your actions concerning monetary scarcity, a plan that one can implement and measure using simple benchmarks or budgeting ratios. By using these statistics, perhaps on an annual basis, the doctor can spot problems, correct them and continue planning actively toward stated goals like building long-term wealth.
Useful Calculations To Assess Your Budgeting Success
In the past, generic budgeting ratios would emphasize not spending more than 15 to 20 percent of your net salary on food or 8 percent on medical care. Now these estimates have given way to more rigorous numbers. Personal budget ratios, much like medical practice financial ratios, represent comparable benchmarks for parameters such as debt, income growth and net worth. Although these ratios are still broad, the following represent some useful personal budgeting ratios for physicians.
• Basic liquidity ratio = liquid assets / average monthly expenses. Cash-on-hand should approach 12 to 24 months or more in the case of a doctor employed by a financially insecure HMO or fragile medical group practice. Yes, chances are you have heard of the standard notion of setting enough cash aside to cover three months in a rainy day scenario. However, we have decried this older laymen standard for many years in our textbooks, white papers and speaking engagements as being wholly insufficient for the competitively unstable environment of modern healthcare.
• Debt to assets ratio = total debt / total assets. This percentage is high initially but should decrease with age as the doctor approaches a debt-free existence
• Debt to gross income ratio = annual debt repayments / annual gross income. This represents the adequacy of current income for existing debt repayments. Doctors should try to keep this below 20 to 25 percent.
• Debt service ratio = annual debt repayment / annual take-home pay. Physicians should aim to keep this ratio below 25 to 30 percent or face difficulty paying down debt.
• Investment assets to net worth ratio = investment assets / net worth. This budget ratio should increase over time as retirement approaches.
• Savings to income ratio = savings / annual income. This ratio should also increase over time as one retires major obligations like medical school debt, a practice loan or a home mortgage.
• Real growth ratio = (income this year – income last year) / (income last year – inflation rate). This budget ratio should grow faster than the core rate of inflation.
• Growth of net worth ratio = (net worth this year – net worth last year) / net worth last year – inflation rate). Again, this budgeting ratio should stay ahead of inflation.
In other words, these ratios will help answer the question: “How am I doing?”
Pearls For Sticking To A Budget
Far from the burden that most doctors consider it to be, budgeting in one form or another is probably one of the greatest tools for building wealth. However, it is also one of the greatest weaknesses among physicians who tend to live a certain lifestyle.
In fact, we have found that less than one in 10 medical professionals have a personal budget. Fear, or a lack of knowledge, is a major cause of procrastination. Fortunately, the following guidelines assist in reversing this microeconomic disaster.
1. Set reasonable goals and estimate annual income. Do not keep large amounts of cash at home or office. Deposit it in an FDIC insured money-market account for safety. Do not deposit it in a money market mutual fund with net asset value (NAV) that may “break the buck” and fall below the one-dollar level. Track actual bills and expenses.
2. Do not pay bills early, do not have more taxes withheld from your salary than needed and develop spending estimates to pay fixed expenses first. Fixed expenses are usually contractual and usually include housing, utilities, food, Social Security, medical, debt repayments, homeowner’s or renter’s insurance, auto, life and disability insurance, etc. Reduce fixed expenses when possible. Ultimately, all expenses get paid and become variable in the long run.
3. Make it a priority to reduce variable expenses. Variable expenses are not contractual and may include clothing, education, recreational, travel, vacation, gas, cable TV, entertainment, gifts, furnishings, savings, investments, etc. Trim variable expenses by 5 to 20 percent.
4. Use “carve-outs or “set-asides” for big ticket items and differentiate true wants from frivolous needs.
5. Calculate both income and expenses as a percentage of your total budget. Determine if there is a better way to allocate resources. Review the budget on a monthly basis to notice any variance. Determine if the variance was avoidable, unavoidable or a result of inaccurate assumptions. Take corrective action as needed.
6. Know the difference between saving and investing. Savers tend to be risk adverse while investors understand risk and take steps to mitigate it. Watch mutual fund commissions and investment advisory fees, which cut into return-rates. Keep investments simple and diversified (stocks, bonds, cash, index, no-load mutual and exchange traded funds, etc.).
Sooner or later, despite the best of budgeting intentions, something will go awry. A doctor will be terminated or may be the victim of a reduction-in-force (RIF) because of cost containment initiatives.4 A medical practice partnership may dissolve or a local hospital or surgery center may close, hurting your practice and livelihood. Someone may file a malpractice lawsuit against you, a working spouse may be laid off or you may get divorced. Regardless of the cause, budgeting crisis management encompasses two different perspectives: awareness and execution.
First, if you become aware that you may lose your job, the following proactive steps will be helpful to your budget and overall financial condition.
• Decrease retirement contributions to the required minimum for company/practice match. • Place retirement contribution differences in an after-tax emergency fund. • Eliminate unnecessary payroll deductions and deposit the difference to cash. • Replace group term life insurance with personal term or universal life insurance. • Take your old group term life insurance policy with you if possible. • Establish a home equity line of credit to verify employment. • Borrow against your pension plan only as a last resort.
If you have lost your job or your salary has been depressed, negotiate your departure and get an attorney if you believe you lost your position through breach of contract or discrimination. Then execute the following steps to recalculate your budget and boost your wealth rebuilding activities.
• Prioritize fixed monthly bills in the following order: rent or mortgage; car payments; utility bills; minimum credit card payments; and restructured long-term debt.
• Consider liquidating assets to pay off debts in this order: emergency fund, checking accounts, investment accounts or assets held in your children’s names.
• Review insurance coverage and increase deductibles on homeowner’s and automobile insurance for needed cash.
• Then sell appreciated stocks or mutual funds; personal valuables such as furnishings, jewelry and real estate; and finally, assets not in pension or annuities if necessary.
• Keep or rollover any lump sum pension or savings plan distribution directly to a similar savings plan at your new employer, if possible, when you get rehired.
• Apply for unemployment insurance.
• Review your medical insurance and COBRA coverage after a “qualifying event” such as job loss, firing or even after quitting. It is a bit expensive due to a 2 percent administrative fee surcharge but this may be well worth it for those with preexisting conditions or who are otherwise difficult to insure. One may continue COBRA for up to 18 months.
• Consider a high deductible Health Savings Account (HSA), which allows tax-deferred dollars like a medical IRA, for a variety of costs not normally covered under traditional heath insurance plans. Self-employed doctors deduct both the cost of the premiums and the amount contributed to the HSA. Unused funds roll over until the age of 59½, when one can use the money as a supplemental retirement benefit.
• Eliminate unnecessary variable, charitable and/or discretionary expenses, and become very frugal.
Final Notes
The behavioral psychologist, Gene Schmuckler, PhD, MBA, sometimes asks exasperated doctors to recall the story of the old man who spent a day watching his physician son treating HMO patients in the office. The doctor had been working at his usual feverish pace all morning. Although he was working hard, he bitterly complained to his dad that he was not making as much money as he used to make. Finally, the old man interrupted him and said, “Son, why don’t you just treat the sick patients?” The doctor-son looked at his father with an annoyed expression and responded, “Dad, can’t you see, I do not have time to treat just the sick ones.”
Always remember to add a bit of emotional sanity into your budgeting and economic endeavors.
Regardless of one’s age or lifestyle, the insightful doctor realizes that it is never too late to take control of a lost financial destiny through prudent wealth building activities. Personal and practice budgeting is always a good way to start the journey.
NOTE: Dr. Marcinko is a former Certified Financial Planner and current Certified Medical Planner™. He has been a medical management advisor for more than a decade. He is the CEO of http://www.MarcinkoAssociates.com
The authors acknowledge the assistance of Mackenzie H. Marcinko PhD in the preparation of this article.
According to the National Institute on Retirement Security, almost 40 million households have no retirement savings at all. The Employee Benefit Research Institute (EBRI) estimates in its 2019 Retirement Security Projection Model that America’s current retirement savings deficit is $3.8 trillion.
What does that mean? Well, the EBRI report aggregates the savings deficit of all U.S. households headed by someone between the ages of 35 and 64, inclusive. In total, those households have $3.8 trillion fewer dollars in savings than they should have for retirement.
For more recent data, Fidelity Investments reported that in the third quarter of 2022 the average account balance for an IRA was $101,900. Employees with a 401(k) averaged $97,200, while those with a 403(b) had $87,400.
Fidelity also estimated that “an average retired couple age 65 in 2022 may need approximately $315,000 saved (after tax) to cover health care expenses in retirement.” Keeping in mind that more Americans are also living longer than ever before, they will face more challenges to cover medical expenses in retirement.
Medical Executive-Post Publisher-in-Chief, Dr. David Edward Marcinko MBA CMP™, and financial planner Paul Larson CFP™, were interviewed by Sharon Fitzgerald for Medical News, Inc. Here is a reprint of that interview.
Doctors Squeezed from both Ends
Physicians today “are getting squeezed from both ends” when it comes to their finances, according Paul Larson, president of Larson Financial Group. On one end, collections and reimbursements are down; on the other end, taxes are up. That’s why financial planning, including a far-sighted strategy for retirement, is a necessity.
Larson Speaks
“We help these doctors function like a CEO and help them quarterback their plan,” said Larson, a Certified Financial Planner™ whose company serves thousands of physicians and dentists exclusively. Headquartered in St. Louis, Larson Financial boasts 19 locations.
Larson launched his company after working with a few physicians and recognizing that these clients face unique financial challenges and yet have exceptional opportunities, as well.
What makes medical practitioners unique? One thing, Larson said, is because they start their jobs much later in life than most people. Physicians wrap up residency or fellowship, on average, at the age of 32 or even older. “The delayed start really changes how much money they need to be saving to accomplish these goals like retirement or college for their kids,” he said.
Another thing that puts physicians in a unique category is that most begin their careers with a student-loan debt of $175,000 or more. Larson said that there’s “an emotional component” to debt, and many physicians want to wipe that slate clean before they begin retirement saving.
Larson also said doctors are unique because they are a lawsuit target – and he wasn’t talking about medical malpractice suits. “You can amass wealth as a doctor, get sued in five years and then lose everything that you worked so hard to save,” he said. He shared the story of a client who was in a fender-bender and got out of his car wearing his white lab coat. “It was bad,” Larson said, and the suit has dogged the client for years.
The Three Mistake of Retirement Planning
Larson said he consistently sees physicians making three mistakes that may put a comfortable retirement at risk.
The first is assuming that funding a retirement plan, such as a 401(k), is sufficient. It’s not. “There’s no way possible for you to save enough money that way to get to that goal,” he said. That’s primarily due to limits imposed by the Internal Revenue Service, which allows a maximum contribution of $49,000 annually if self-employed and just $16,500 annually until the age of 50. He recommends that physicians throughout their career sock away 20 percent of gross income in vehicles outside of their retirement plan.
The second common mistake is making investments that are inefficient from a tax perspective. In particular, real estate or bond investments in a taxable account prompt capital gains with each dividend, and that’s no way to make money, he said.
The third mistake, and it’s a big one, is paying too much to have their money managed. A stockbroker, for example, takes a fee for buying mutual funds and then the likes of Fidelity or Janus tacks on an internal fee as well. “It’s like driving a boat with an anchor hanging off the back,” Larson said.
Marcinko Speaks
Dr. David E. Marcinko MBA MEd CPHQ, a physician and [former] certified financial planner] and founder of the more specific program for physician-focused fiduciary financial advisors and consultants www.CertifiedMedicalPlanner.org, sees another common mistake that wreaks havoc with a physician’s retirement plans – divorce.
He said clients come to him “looking to invest in the next Google or Facebook, and yet they will get divorced two or three times, and they’ll be whacked 50 percent of their net income each time. It just doesn’t make sense.”
Marcinko practiced medicine for 16 years until about 10 years ago, when he sold his practice and ambulatory surgical center to a public company, re-schooled and retired. Then, his second career in financial planning and investment advising began. “I’m a doctor who went to business school about 20 years ago, before it was in fashion. Much to my mother’s chagrin, by the way,” he quipped. Marcinko has written 27 books about practice management, hospital administration and business, physician finances, risk management, retirement planning and practice succession. He’s the founder of the Georgia-based Institute of Medical Business Advisors Inc.
Succession Planning for Doctors
Succession planning, Marcinko said, ideally should begin five years before retirement – and even earlier if possible. When assisting a client with succession, Marcinko examines two to three years of financial statements, balance sheets, cash-flow statements, statements of earnings, and profit and loss statements, yet he said “the $50,000 question” remains: How does a doctor find someone suited to take over his or her life’s work? “We are pretty much dead-set against the practice broker, the third-party intermediary, and are highly in favor of the one-on-one mentor philosophy,” Marcinko explained.
“There is more than enough opportunity to befriend or mentor several medical students or interns or residents or fellows that you might feel akin to, and then develop that relationship over the years.” He said third-party brokers “are like real-estate agents, they want to make the sale”; thus, they aren’t as concerned with finding a match that will ensure a smooth transition.
The only problem with the mentoring strategy, Marcinko acknowledged, is that mentoring takes time, and that’s a commodity most physicians have too little of. Nonetheless, succession is too important not to invest the time necessary to ensure it goes off without a hitch.
Times are different today because the economy doesn’t allow physicians to gradually bow out of a practice. “My overhead doesn’t go down if I go part-time. SO, if I want to sell my practice for a premium price, I need to keep the numbers up,” he noted.
Assessment
Dr. Marcinko’s retirement investment advice – and it’s the advice he gives to anyone – is to invest 15-20 percent of your income in an Vanguard indexed mutual fund or diversified ETF for the next 30-50 years. “We all want to make it more complicated than it really is, don’t we?” he said.
QUESTION: What makes a physician moving toward retirement different from most others employees or professionals? Marcinko’s answer was simple: “They probably had a better shot in life to have a successful retirement, and if they don’t make it, shame on them. That’s the difference.”
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on August 10, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
HEALTH SAVINGS ACCOUNT
***
***
DEFINITION: According to Wikipedia, a health savings account (HSA) is a tax advantaged account available to taxpayers in the USA who are enrolled in a high-deductible health plan (HDHP). The funds contributed to an account are not subject to federal income tax at the time of deposit.
Unlike a flexible spending account (FSA), HSA funds roll over and accumulate year to year if they are not spent. HSAs are owned by the individual, which differentiates them from company-owned Health Reimbursement Arrangements (HRA) that are an alternate tax-deductible source of funds paired with either high-deductible health plans or standard health plans. CITE: https://www.r2library.com/Resource
How to avoid losing out on your HSA funds
The last thing you want is to risk losing out on the money you’ve socked away in an HSA. If you make a point to keep contributing to your account, however, then that alone should be enough to keep it active.
EXAMPLE: So let’s say your goal is to reserve all of your HSA funds for retirement, and you’re only in your 40s. If you make an HSA contribution every year, that should do the trick in keeping your account active. Making investment changes in your account might do the same.
If you have an old HSA you know you haven’t put money into for quite some time and you don’t plan to make a contribution or withdrawal anytime soon, then it could pay to contact the bank holding your HSA and confirm that you wish to keep your account active. At that point, your bank should be able to tell you what steps, if any, you need to take to make sure you don’t end up forfeiting any funds.
Posted on July 15, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Understanding the Impending Retirement-Planning Crisis
[By Somnath Basu PhD, MBA]
A serious retirement-planning crisis is looming in the US with many Baby Boomer physicians, and others, having already spent a portion of their nest egg and undermining any hope for a comfortable lifestyle unless they continue to work. Notwithstanding medical professionals, look no further than an annual “retirement confidence” survey conducted by the Employee Benefit Research Institute and Mathew Greenwald & Associates in each of the past 17 years. Nearly two in five of working Americans responding to the latest survey indicated that they have taken no action in the face of reductions in their employer-provided retirement benefits.
Consumption Equals Happiness?
The population is constantly told that consumption equals happiness. At the same time they are not being asked to understand about the implications of borrowing to fund for such consumption. Before we can expect to effect a change in the ensuing pattern of a vicious cycle, the population mass must have a clear understanding of the difference between needs (e.g., retiring with peace of mind) and desires (e.g., cruises or living the high life).
Negative Savings Rate
When savings first dipped into negative territory during the Great Depression in 1932 and 1933, people didn’t have enough to eat, whereas there has been no such urgency to raid nest eggs since the repeat of this performance in 2005 when the rate fell to minus 0.5 percent. Our grandparents were shining stars in the way they worked hard to build this country’s infrastructure and manufacturing sector, saved every red cent they could get their hands on and created affluence on a mass scale. Today we’re able to enjoy the fruit of their labor. But, somehow their values were lost on future generations.
Changing American Culture
Many of the nation’s top engineers and scientists now hail from China, India and other Asian countries as American culture has undergone a dramatic change to the point where jocks and cheerleaders are more valued than computer geeks and science nerds in our schools. We inherited so much affluence that it made us lazy as a society. The seeds of our destruction have been sown, but it’s up to our politicians, educators and other leaders, including financial advisors, to help reverse this disturbing pattern before it’s too late.
Many people fall into the trap of rushing through dinner and unwinding in front of the TV where a big part of the problem lies in slick and subtle, and hard to resist, primetime advertising and marketing messages (prime time for subtle messages) that seduce viewers into purchasing luxury cars or flying to far-flung resorts where they can sip umbrella-clad cocktails alongside affluent vacationers.
Americans in Debt
A recent wave of foreclosures has put Americans deeper in debt, with the sub-prime crisis exposing despicable predatory lending practices. But, research has shown the wreckage also could be found strewn across in the mid-prime and prime markets as middle-class borrowers struggled to pay adjustable rate mortgages. High hopes have been pinned on the stock market helping people crawl out from this crisis just like when the real estate market had softened the blow when the tech-bubble burst at the turn of this century. So far, this has happened, to an extent. But, if the stock market starts reeling again, then it will spell even bigger trouble. Add to this the international trade imbalance, which implies foreign governmental funding of our conspicuous consumption, and which comes with high interest rates that need to be paid to the lenders, again to such countries as China, India and other emerging economies, and a bigger, worse picture emerges.
Personal Bankruptcies
Personal bankruptcies have an even more devastating effect on an individual’s ability to plan for the future, particularly since the laws pertaining to this area were toughened to a point where reckless spenders will need to muster fiscal and financial discipline as never before. The doomsday scenario is that children now run the risk of inheriting debt instead of wealth, and it’s unconscionable to think future generations would have a standard of living that’s worse than their parents or grandparents.
Assessment
The true grit associated with being an American is to rise up in the face of adversity – a frontier spirit that drew me this remarkable country. We’ve weathered numerous storms and can do it again. But, it requires a serious commitment to stopping mindless consumption of goods and services, as well as understanding there’s a difference between basic needs and pie-in-the-sky desires.
NOTE: Dr. Somnath Basu is a Professor of Finance at California Lutheran University and the Director of its California Institute of Finance. He is also the creator of the innovative AgeBander technology www.agebander.com for planning retirement needs.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Instead, physician assistants (PAs) and nurse practitioners (NPs) will increasingly provide primary care services, according to a report from consulting firm Mercer.
Posted on July 11, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Setty Gundanna Viralam et ux. v. Commissioner
[A Case Model]
By Children’s Home Society of Florida Foundation
In Setty Gundanna Viralam et ux. v. Commissioner; 136 T.C. No. 8; No. 21355-03 (13 Feb 2011), the Tax Court denied a deduction for a charitable gift to an organization maintaining donor advised funds for doctors. In addition to not receiving the charitable deduction, the doctor was subject to capital gains tax on sale of the stock and an accuracy-related penalty.
Physician Example
Dr. Viralam is a medical practitioner. In 1998, Dr. Viralam sold his 50% interest in a medical practice for $2,262,500, producing a taxable gain of $2,261,750. Dr. Viralam had joined a membership organization of doctors named Xelan. He paid a $975 membership fee for the “Xelan tax reduction plan.”
Xelan Foundation
Based upon promotional materials that promised “a tax reduction” program, Dr. Viralam transferred appreciated stock to the Xelan Foundation (“Foundation”) in 1998. The Foundation indicated that Dr. Viralam could create an account described variously as a “donor advised fund” or “family public charity.” The fund was available for “charitable giving, income tax reduction planning, estate tax reduction, educational funding and future retirement planning.”
The Xelan Foundation had been recognized by the IRS as a public charity and was included in IRS Publication 78. In addition, the Foundation had obtained an opinion letter from the Conner & Winters law firm on deductibility of gifts. In their opinion letter, Conner & Winters suggested that gifts to the Foundation were more likely than not to be deductible. However, the opinion letter declined to issue an opinion on the specific grants or educational programs of the Foundation donor advised funds.
The Gifting Mechanism
Following Dr. Viralam’s gift of stock with fair market value of $262,433 and cost basis of $131,360, the Foundation sold the gifted stock and provided him with a receipt. The receipt included the Sec. 170(f)(8) statement that “no goods or services” were transferred in exchange for the gift.
At the recommendation of Dr. Viralam, the Foundation accountant distributed $15,500 to religious organizations for the next two years. However, his Foundation account also made distributions to the University of Pennsylvania of $70,299. Dr. Viralam’s son Vinay was at that time a student at that university. The IRS audited Dr. Viralam and issued a notice of deficiency for 1998. The IRS denied the charitable deduction, assessed a tax on the sale of the appreciated stock by Xelan Corporation and also accessed an accuracy-related penalty under Sec. 6662.
The Court and IRS Opines
The court noted that under Sec. 170(c)(2), a charitable contribution is permitted if it is given to “a foundation organized and operated exclusively for charitable or educational purposes.”
The IRS claimed that the supposed “student loan” to Vinay showed that Dr. Viralam had “never surrendered dominion and control” over the fund. When Dr. Viralam created the fund in 1998, he anticipated that his three children would receive most of the fund for their college expenses. The initial distributions for the benefit of Vinay were made and “the Foundation’s approval of petitioner’s son as a student loan beneficiary was perfunctory.”
While it was true that the Foundation had been granted exempt status and was listed in Publication 78, the issue of the operation exclusively for the benefit of charitable purposes remained. Even though the purported donor advised fund was supposedly for charitable purposes, the facts indicated that Dr. Viralam had retained dominion and control.
The Sec. 170(f)(8)(A) receipt issued by Xelan Foundation indicated that there were no “goods or services” provided in consideration of the gift. However, the “student loans” were clearly within the regulatory definition of “cash, property, services, benefits and privileges.” Because the student loans were contemplated as part of the fund benefits, the gift failed the “no goods or services” test. Under Sec. 170(f)(8), there is “no deduction” if that test is failed.
Assessment
Because there was no charitable deduction, Dr. Viralam is also taxable on the long-term capital gain produced by sale of the stock in 1998. In addition, the penalty under Sec. 6662 applied. Dr. Viralam pointed to the legal opinion by the law firm Connor & Winters. However, that legal opinion explicitly excepted a potential student loan program. In the view of the court, the arrangement fails the “too good to be true” test. In the view of a reasonable person, a taxpayer should realize that this gift to provide university-level educations for children would not be deductible.
Conclusion
And so, your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe. You can unsubscribe at any time. Security is assured.
Sponsors Welcomed: And, credible sponsors and like-minded advertisers are always welcomed.
Posted on June 28, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
An Easy Answer to Retirement Planning -or- MisStep?
By David Wallace [Search and social media marketer from Anthem, Arizona]
Investing in a target date mutual fund seems like the easy answer to retirement planning.
But, how can a single fund be appropriate for thousands of investors, doctors and medical professionals?
Assessment
Check out the above infographic to see the limitations of target date funds.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Posted on June 15, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Spending Money for Comfort and Safety
By Rick Kahler MS CFP®
Want to increase your independence in retirement? Save money? Live safely in your own home? Then buy a new car. No, this isn’t a scam or a seedy sales pitch. In certain cases, a new car can be a wise use of your retirement dollars.
Introduction
As regular readers of the ME-P know, I’m a big fan of frugality. Spending less than you earn is a crucial strategy for building wealth. Continuing this frugal lifestyle in retirement can also be a good way to be sure of having enough money to last for the rest of your life.
Some retirees, though, take it too far. Under-spending can be a threat to retirement as much as overspending, especially when it affects your comfort and safety.
As more of my retired clients move into their later years, I am becoming increasingly aware of one kind of retirement spending that can actually be considered more of an investment than an expense. This, for elderly people or adult children caring for elderly parents, is spending money to make their homes and activities safer.
Safer Spending
One immediate benefit of this kind of spending is being able to live more comfortably and with less anxiety. A second benefit is financial. Helping elderly parents stay in their homes and live independently for as long as possible can save money in the long term by reducing medical costs and long-term care expenses. It’s especially important to invest in this type of spending if you live too far away from your parents to provide regular help yourself.
Some of the ways to invest relatively small amounts to provide more comfort, safety, and independence for elderly parents are obvious. Or, carpet slick tile or hardwood floors to reduce the risk of falls. Upgrade older appliances to newer ones with safety features like automatic shutoffs or warning signals. Add basic safety aids like stair railings and shower bars. Repair hazards like worn carpets, uneven steps, or broken sidewalks. Provide emergency alert buttons. Install phones in several rooms.
Other Considerations
Some less obvious ways to foster safety and extend independent living might require a bit more spending. Such expenditures can be a good use of retirement income if they extend parents’ ability to live independently. Here are a few possibilities to consider:
1. Buying that new car. Safety features like GPS navigation systems and backup cameras can allow elderly people to hold onto their drivers’ licenses longer without putting themselves or others at risk.
2. Paying for gym memberships or exercise classes. Increasing strength, balance, and flexibility can help prevent falls and possibly even help stave off dementia.
3. Taking care of ears and eyes. Hearing aids and corrective lenses may not be cheap, but good hearing and eyesight can help people drive more safely, avoid falls, and take care of themselves and their homes.
4. Remodeling. Moving the laundry room to the main floor or replacing bathtubs with walk-in showers can make homes safer and more comfortable.
5. Hiring help. Many of us equate in-home help for the elderly with home health care. Certainly, hiring aides to help with cooking, bathing, and other needs as people become frail is an important option. But well before that time, it makes sense to get help with a host of other services that become harder or even dangerous to do as we grow older. Hire a house cleaner. Find someone to do yard work, home maintenance, and heavy cleaning jobs (especially if they involve ladders) like window washing.
***
***
Assessment
Spending that creates safety belongs in any retirement budget. It’s a good way to use your financial independence to help maintain your physical and mental independence.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
A retirement nest egg of $2.5 million can likely produce an annual income of $100,000 for as long as you are likely to live. This is using the 4% withdrawal rate many financial advisors consider standard. After starting with the first withdrawal of 4% of the total, the annual withdrawal will adjust for inflation. For example, if inflation runs at the target 2% rate of federal policymakers, during retirement the retiree will withdraw:
$100,000
in the first year
$102,000
in the second year
$104,040
in the third year and so on …
According to this model and conventional wisdom, a 4% withdrawal rate will allow a portfolio to last for at least 30 years. This would permit a 65-year-old retiree to maintain consistent purchasing power until age 95 and beyond.
For most retirees, this will likely be adequate to maintain a satisfying standard of living. Only about 3% of 2,000 retirees surveyed by the Employee Benefit Research Institute in 2022 spent $7,000 or more per month, equivalent to $84,000 in annual spending.
This model does not include a number of other factors. For instance, nearly all retirees are eligible for Social Security. For 2023, the maximum monthly Social Security benefit for people who claim benefits at full retirement age is $3,627. That’s equal to more than half the spending of the top 3% of retirees surveyed by EBRI. And, like the standard withdrawal rate, Social Security benefits are indexed to inflation.
5 Variables for Retiring With $2.5 Million at Age 65
While $2.5 million could seem like enough to retire at 65, many factors could change the outlook.
1. Unexpected Healthcare Costs
The Fidelity Retiree Health Care Cost Estimate suggests an average 65-year-old couple could need (approximate, after taxes):
This assumes both spouses are enrolled in traditional Medicare, which between Medicare Part A and Part B covers expenses such as hospital stays, doctor visits and services, physical therapy, lab tests and more, and in Medicare Part D, which covers prescription drugs.
This figure does not include long-term care (“custodial care”), most dental care, eye exams and more, so your estimated healthcare costs in retirement could be considerably more.
2. Inflation
Inflation can powerfully influence retirees’ financial well-being. When inflation occurs, it reduces the purchasing power of money withdrawn from your retirement account. You can increase withdrawals to maintain purchasing power, but this risks more quickly depleting your savings.
3. Market Downturns
Inflation isn’t the only cause of market downturns. Business cycles and financial crises can exaggerate normal fluctuations in stock market valuations. If you’re selling investments to generate income for living expenses, you may want to sell more if valuations are down.
4. Longevity
While living a long life is positive, you could outlive the money you’ve saved for retirement. Many financial planners use life expectancy to age 95 or 100 when developing plans for funding retirement.
The Social Security Administration says an average 65-year-old male can live to age 83, while the average woman can live to age 86. However, people in their 80s and 90s also generally reduce their spending, with the exception of healthcare costs.
5. Estate Planning
Retiring at 65 with $2.5 million likely involved generating high income and savings, so there’s a chance you could have assets to pass on. With estate planning, adding members of your family as beneficiaries for homes you paid off with a mortgage may have long-term positives.
You may also want to think about any additional income streams. For example, if you own a medical practice or business, you may want to add your family as a beneficiary so they can decide to keep the business running or sell it.
While financial planning rules of thumbs are useful to people as general guidelines, they may be too oversimplified in many situations, leading to underestimating or overestimating an individual’s needs. This may be especially true for physicians and many medical professionals. Rules of thumb do not account for specific circumstances or factors occurring at a particular time, or that could change over time, which should be considered for making sound financial decisions.
For example, in a tight job market, an emergency fund amounting to six months of household expenses does not consider the possibility of extended unemployment. I’ve always suggested 2-3 years for doctors. Venture capitalist lay-offs of physicians during the pandemic confirm this often criticized benchmark opinion of mine.
As another example, buying life insurance based on a multiple of income does not account for the specific needs of the surviving family, which include a mortgage, the need for college funding and an extended survivor income for a non-working spouse. Again a huge home mortgage, or several children or dependents, may be the financial bane of physician colleaguesand life insurance.
A home purchase should cost less than an amount equal to two and a half years of your annual income. I think physicians in practice for 3-5 years might go up to 3.5X annual income; ceteras paribus.
Save at least 10-15% of your take-home income for retirement. Seek to save 20% or more.
Have at least five times your gross salary in life insurance death benefit. Consider 10X this amount in term insurance if young, and/or with several children or other special circumstances.
Pay off your highest-interest credit cards first. Agreed.
The stock market has a long-term average return of 10%. Agreed, but appreciated risk adjusted rates of return..
You should have an emergency fund equal to six months’ worth of household expenses. Doctors should seek 2-3 years.
Your age represents the percentage of bonds you should have in your portfolio. Risk tolerance and assets may be more vital.
Your age subtracted from 100 represents the percentage of stocks you should have in your portfolio. Risk tolerance and assets may still be more vital.
A balanced portfolio is 60% stocks, 40% bonds. With historic low interest rates, cash may be a more flexible alternative than bonds; also avoid most bond mutual funds as they usually never mature.
There are also rules of thumb for determining how much net worth you will need to retire comfortably at a normal retirement age. Here is the calculation that Investopedia uses to determine your net worth:
If you are employed and earning income: ((your age) x (annual household income)) / 10.
If you are not earning income or you are a student: ((your age – 27) x (annual household income)) / 10.
Posted on May 13, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
The High Deductible Insurance Competition Heats Up
By Dr. David Edward Marcinko; MBA MEd CMP
[Editor-in-Chief]
As ME-P readers are aware, I’ve had a High Deductible Healthcare Plan [HDHP] coupled with a Health Savings Account [HSA] for my family, and consulting firm, for more than a decade. We’ve been very pleased with it thus far. No significant health problems along the way; just a few scares that proved costly, but benign, because of physician over-protection, over-reaction, or liability phobia; i.e., its better to be safe, than sorry!.
Still, having some economic skin in the insurance game because of the high-deductible feature, makes one an informed consumer. It also provides a sense of empowerment which, while ultimately illusionary for mortals, does offer a bit of self-control. After all, while we can’t mitigate against drunk-drivers and catastrophic diseases, we can live a healthy lifestyle and pay out of pocket for true health “maintenance” … much as we self-pay to maintain our cars and homes, etc. We can do our best … and hope for the rest.
Of course, the savings portion [HSA] has always been a secondary after-thought relative to the actual re-insurance coverage terms, exclusions and conditions. I personally remain focused on the indemnity or PPO type with full coverage, no co-payments and few restrictions. After all, if I use up my high-deductible for an adverse health incident, I figure I have far more problems to worry about than economic. My health, well-being and probably life are significantly in peril.
Nevertheless, as a health economist, I have always appreciated the above market rates given to my cash HSA account; 5% to 4.0% historically; and now 7.0%. Compared to the paltry 0.29% in my FDIC protected bank money market deposit account, or the 0.8% in my non-FDIC protected money market mutual fund [brokerage] account; this is a great deal.
Oh the Irony!
So, it comes as some surprise that after more than a decade, and the recent health insurance reform political re-debacle, that there is a surge of interest in the HSA companion. This time however, interest comes not from the insured’s – but the insurers. And, not from the health insurance industry, but rather from the affiliated [and desperate] banking industry.
How so – and why?
Well, it now seems some insurance companies actually desire the business of folks like me who are willing to bear a higher deductible in return for lower premiums, or who are willing to research CPT® code prices and question the efficacy of the procedures they negotiate with physicians in a collaborative fashion; or who are willing to watch their weights and abstain from over-indulgences for their own good. How novel; and again, why?
It’s the HSA pot-o-gold; Duh!
The Proof
Below, is a copy of an email I personally received from eHealthInsurance soliciting my separate health savings account [HSA] business; not my health insurance coverage business:
Dear David,
Did you know that your health insurance plan can be complemented by a Health Savings Account (HSA)? If you haven’t opened an HSA yet, it’s not too late! An HSA allows you to:
Use funds to pay for copays, deductibles, prescription drugs, dental services, vision care and more
Save money by deducting 100% of your HSA contributions from your taxable income
Earn tax-free interest on the funds that accrue in your account over time
Grow your account from year to year – the money you contribute won’t expire; you can even use an HSA as a secondary retirement savings account
There are no penalties or taxes when you use your HSA funds to pay for qualified medical expenses. Take advantage of your health plan’s benefits and open an HSA today! eHealthInsurance has partnered with nationally recognized, highly-rated HSA banks to offer you industry leading choices:
The Bancorp Bank
HSA Bank
JPMorgan Chase Bank
OptumHealth Bank
Sovereign Bank
Wells Fargo Bank
We’re with you every step of the way
Our representatives are also available for online chat 24 hours day.
Gary Matalucci
Vice President of Customer Care
The Question Is?
Such the deal; NOT!
So, any thinking HDHP participant [like me] must logically ask why such “nationally recognized, highly-rated HSA banks” would offer above market rates during these times of essentially high interest rate levels. Why the interest at all? Are they trying to loose money; or are they just befriending me?
As tennis player John McEnroe might say: are you serious!
Assessment
Yes John, the high rates are a serious loss-leader for more expensive products.
These banks want to make money; not from the interest rate spread on your HSA cash, but by enticing us to place this growing cash horde into their “investment vehicles.” In the recent past, some of us mortgaged our homes chasing the stock market or were goaded into flipping houses. And now, these same bankers are encouraging us to mortgage our health insurance on whatever high-priced, low-quality, fee-ridden, load bearing, snarky “investment vehicles” they can pawn off on us.
Of course, the health insurance companies get a fat sales commission or percentage cut, as well. A win-win situation for all but us – the insured.
Think AARP.
My Personal Advice
Do not do it. Do not take the bait.
The HSA portion of your HDHP is for paying premiums and future medical care in the event of a health catastrophe. It is for savings, not for investing in a risk-bearing vehicle. Far too many of us realized too late that a home is a place to live – not an investment. Likewise, a health savings account is for your health, and health insurance – not risky investing.
Assessment
Well, that’s my opinion as a retired surgeon, former insurance agent and financial advisor. Your own thoughts are appreciated.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, urls and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Modern Portfolio Theory approaches investing by examining the complete market and the full economy. MPT places a great emphasis on the correlation between investments.
DEFINITION:
Correlation is a measure of how frequently one event tends to happen when another event happens. High positive correlation means two events usually happen together – high SAT scores and getting through college for instance. High negative correlation means two events tend not to happen together – high SATs and a poor grade record.
No correlation means the two events are independent of one another. In statistical terms two events that are perfectly correlated have a “correlation coefficient” of 1; two events that are perfectly negatively correlated have a correlation coefficient of -1; and two events that have zero correlation have a coefficient of 0.
Correlation has been used over the past twenty years by institutions and financial advisors to assemble portfolios of moderate risk. In calculating correlation, a statistician would examine the possibility of two events happening together, namely:
If the probability of A happening is 1/X;
And the probability of B happening is 1/Y; then
The probability of A and B happening together is (1/X) times (1/Y), or 1/(X times Y).
There are several laws of correlation including;
Combining assets with a perfect positive correlation offers no reduction in portfolio risk. These two assets will simply move in tandem with each other.
Combining assets with zero correlation (statistically independent) reduces the risk of the portfolio. If more assets with uncorrelated returns are added to the portfolio, significant risk reduction can be achieved.
Combing assets with a perfect negative correlation could eliminate risk entirely. This is the principle with “hedging strategies”. These strategies are discussed later in the book.
In the real world, negative correlations are very rare
Most assets maintain a positive correlation with each other. The goal of a prudent investor is to assemble a portfolio that contains uncorrelated assets. When a portfolio contains assets that possess low correlations, the upward movement of one asset class will help offset the downward movement of another. This is especially important when economic and market conditions change.
As a result, including assets in your portfolio that are not highly correlated will reduce the overall volatility (as measured by standard deviation) and may also increase long-term investment returns. This is the primary argument for including dissimilar asset classes in your portfolio. Keep in mind that this type of diversification does not guarantee you will avoid a loss. It simply minimizes the chance of loss.
In the table provided by Ibbotson, the average correlation between the five major asset classes is displayed. The lowest correlation is between the U.S. Treasury Bonds and the EAFE (international stocks). The highest correlation is between the S&P 500 and the EAFE; 0.77 or 77 percent. This signifies a prominent level of correlation that has grown even larger during this decade. Low correlations within the table appear most with U.S. Treasury Bills.
Some of the pioneers of behavioral finance are Drs. Kahneman, Twersky and Thaler. This short introduction to the subject is based on John Nofsinger’s little book entitled “Psychology of Investing” an excellent quick read for all medical professionals or anyone who is interested in learning more about behavioral finance.
Rational Decisions?
Much of modern finance is built on the assumption that investors “make rational decisions” and “are unbiased in their predictions about the future”, however this is not always the case.
Cognitive errors come from (1) prospect theory (people feel good/bad about gain/loss of $500, but not twice as good/bad about a gain/loss of $1,000; they feel worse about a $500 loss than feel good about a $500 gain); (2) mental accounting (meaning that people tend to create separate buckets which they examine individually), (3) Self-deception (e.g. overconfidence), (4) heuristic simplification (shortcuts) and (4) mood can affect ability to reach a logical conclusion.
John Nofsinger’s Book
The following are some of the major chapter headings in Nofsinger’s book, and represent some of the key behavioral finance concepts.
Overconfidence leads to: (1) excessive trading (which in turn results in lower returns due to costs incurred), (2) underestimation of risk (portfolios of decreasing risk were found for single men, married men, married women, and single women), (3) illusion of knowledge (you can get a lot more data nowadays on the internet) and (4) illusion of control (on-line trading).
Pride and Regret leads to: (1) disposition effect (not only selling winners and holding on to the losers, but selling winners too soon- confirming how smart I was, and losers to late- not admitting a bad call, even though selling losers increases one’s wealth due to the tax benefits), (2) reference points (the point from where one measures gains or losses is not necessarily the purchase price, but may perhaps be the most recent 52 week high and it is most likely changing continuously- clearly such a reference point will affect investor’s judgment by perhaps holding on to “loser” too long when in fact it was a winner.)
Considering the Past in decisions about the future, when future outcomes are independent of the past lead to a whole slew of more bad decisions, such as: (1) house money effect (willing to increase the level of risk taken after recent winnings- i.e. playing with house’s money), (2) risk aversion or snake-bite effect (becoming more risk averse after losing money), (3) trying to break-even (at times people will increase their willing to take higher risk to try to recover their losses- e.g. double or nothing), (4) endowment or status quo effect (often people are only prepared to sell something they own for more than they would be willing to buy it- i.e. for investments people tend to do nothing, just hold on to investments they already have) (5) memory and decision making ( decisions are affected by how long ago did the pain/pleasure occur or what was the sequence of pain and pleasure), (6) cognitive dissonance (people avoid important decisions or ignore negative information because of pain associated with circumstances).
Mental Accounting is the act of bucketizing investments and then reviewing the performance of the individual buckets separately (e.g. investing at low savings rate while paying high credit card interest rates).
Examples of mental accounting are: (1) matching costs to benefits (wanting to pay for vacation before taking it and getting paid for work after it was done, even though from perspective of time value of money the opposite should be preferred0, (2) aversion to debt (don’t like long-term debt for short-term benefit), (3) sunk-cost effect (illogically considering non-recoverable costs when making forward-going decisions). In investing, treating buckets separately and ignoring interaction (correlations) induces people not to sell losers (even though they get tax benefits), prevent them from investing in the stock market because it is too risky in isolation (however much less so when looked at as part of the complete portfolio including other asset classes and labor income and occupied real estate), thus they “do not maximize the return for a given level of risk taken).
In building portfolios, assets included should not be chosen on basis of risk and return only, but also correlation; even otherwise well educated individuals make the mistake of assuming that adding a risky asset to a portfolio will increase the overall risk, when in fact the opposite will occur depending on the correlation of the asset to be added with the portfolio (i.e. people misjudge or disregard interactions between buckets, which are key determinants of risk).
This can lead to: (1) building behavioral portfolios (i.e. safety, income, get rich, etc type sub-portfolios, resulting in goal diversification rather than asset diversification), (2) naïve diversification (when aiming for 50:50 stock:bond allocation implementing this as 50:50 in both tax-deferred (401(k)/RRSP) accounts and taxable accounts, rather than placing the bonds in the tax-deferred and stocks in taxable accounts respectively for tax advantages), (3) naïve diversification in retirement accounts (if five investment options are offered then investing 1/5th in each, thus getting an inappropriate level of diversification or no diversification depending on the available choices; or being too heavily invested in one’s employer’s stock).
Representativenes may lead investors to confusing a good company with a good investment (good company may already be overpriced in the market; extrapolating past returns or momentum investing), and familiarity to over-investment in one’s own employer (perhaps inappropriate as when stock tanks one’s job may also be at risk) or industry or country thus not having a properly diversified portfolio.
Emotions can affect investment decisions: mood/feelings/optimism will affect decision to buy or sell risky or conservative assets, even though the mood resulted from matters unrelated to investment. Social interactions such as friends/coworkers/clubs and the media (e.g. CNBC) can lead to herding effects like over (under) valuation.
Financial Strategies
Nofsinger finishes with a final chapter which includes strategies for:
(i) beating the biases: (1) Understand the biases, (2) define your investment objectives, (3) have quantitative investment criteria, i.e. understand why you are buying a specific investor (or even better invest in a passive fashion), (4) diversify among asset classes and within asset classes (and don’t over invest in your employer’s stock), and (5) control your investment environment (check on stock monthly, trade only monthly and review progress toward goals annually).
(ii) using biases for the good: (1) set new employee defaults for retirement plans to being enrolled, (2) get employees to commit some percent of future raises to automatically go toward retirement (save-more-tomorrow).
Assessment
Buy the book (you can get used copies through Amazon). As indicated it is a quick read and occasionally you may even want to re-read it to insure you avoid the biases or use them for the good. Also, the book has long list of references for those inclined to delve into the subject more deeply.
You might even ask “How does all this Behavioral Finance coexist with Efficient Market theory?” and that’s a great question that I’ll leave for another time.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on April 25, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Otherwise known as “National Prescription Drug Take Back Day,” National Drug Take Back Day on April 25th is sponsored by the Drug Enforcement Agency. Its goal is to keep the public aware of the dangers of prescription drug use and misuse. Many Americans don’t know how to safely dispose of the prescription drugs that have been sitting in the medicine cabinet past their prime. Using these expired drugs, or using someone else’s, is dangerous and puts both the public and the environment at risk.
Spotify made money in Q1. According to Morning Brew, the streaming music giant grew its revenue last quarter by 20% to $3.8 billion on a record $180 million in profit, it announced yesterday. The smash report comes after Spotify cut costs last year, which included laying off more than a quarter of its workforce. The company also raised prices in 2023 for the first time in a decade as it further expanded beyond music into audio books and other categories. Spotify shares soared ~11% following the news.
***
Here’s where the major benchmarks ended:
The S&P 500 index® (SPX) rose 1.08 points (0.02%) to 5,071.63; the Dow Jones Industrial Average® ($DJI) fell 42.77 points (0.1%) to 38,460.92; the NASDAQ Composite® ($COMP) added 16.11 points (0.1%) to 15,712.75.
The 10-year Treasury note yield rose more than 4 basis points to 4.644%.
The CBOE Volatility Index® (VIX) rose 0.28 to 15.97.
Transportation shares were among the market’s weakest performers Wednesday behind a drop of more than 10% in Old Dominion Freight Line (ODFL), which reported lighter-than-expected quarterly revenue. The shipper’s nosedive helped send the Dow Jones Transportation Average ($DJT) down 2.3%. Consumer staples, semiconductors, and utilities posted moderate advances. The Dow Jones Utility Index ($DJU) gained for the sixth straight day and ended at a three-and-a-half-month high.
***
The National Association of Realtors’ $418 million settlement over an alleged conspiracy to inflate commissions received preliminary approval yesterday. It’s a new world order: Sellers won’t have to pay buyers’ agents anymore. There’s been talk of a metaphorical death of real estate agents, or a mass extinction; the jury is still out, but RE/MAX cofounder and chairman Dave Liniger doesn’t seem too concerned.
The Labor Department announced it has finalized its Retirement Security Rule, which aims to protect American workers who are saving for retirement and relying on advice from fiduciaries for it. The new rule will update the definition of an investment advice fiduciary under the Employee Retirement Income Security Act and the Internal Revenue Code.
Clinicians don’t always get it right, and their mistakes can be costly: Studies show misdiagnoses lead to roughly 800,000 patient deaths or permanent disabilities each year in the US and cost the healthcare system an estimated $20 billion annually. Cleveland Clinic is using telehealth to try to combat misdiagnoses via its virtual second opinions program, which has saved an average of $8,705 per patient by avoiding unnecessary treatments, according to an analysis released in March.
Posted on April 24, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Stat: 740. That’s how many employees Nike will lay off at its Oregon HQ before the end of June. In February, Nike CEO John Donahoe informed employees of the company’s plan to reduce 2% of its workforce, which would mean around 1,600 employees in total. (USA Today)
Let’s say you leave your job at any time during or after the calendar year you turn 55 (or age 50 if you’re a public safety employee with a government defined-benefit plan). Under a little-known separation-of-service provision, often referred to as the “rule of 55,” you may be able take distributions (though some plans may allow only one lump-sum withdrawal) from your 401(k), 403(b), or other qualified retirement planfree of the usual 10% early-withdrawal penalties. However, be aware that you’ll still owe ordinary income taxes on the amount distributed. This exception applies only to the plan (including any consolidated accounts) that you were contributing to when you separated from service. It does not extend to IRAs.
The S&P 500 index rose 59.95 points (1.2%) to 5,070.55; the Dow Jones Industrial Average gained 263.71 points (0.7%) to 38,503.69; the NASDAQ Composite® ($COMP) surged 245.33 points (1.6%) to 15,696.64.
The 10-year Treasury note yield (TNX) decreased about 2 basis points to 4.602%.
The CBOE Volatility Index® (VIX) fell 1.25 to 15.69.
Similar to Monday, chipmakers were among the market’s strongest areas, carrying the Philadelphia Semiconductor Index (SOX) to a 2.2% advance. Retailers and communication services shares were also strong. The Dow Jones Utility Index ($DJU) gained for the fifth straight day and ended at its highest level in over three months. The Russell 2000® Index (RUT) surged nearly 2%.
You’ve got a sense of your ideal retirement age. And you’ve probably made certain plans based on that timeline. But what if you’re forced to retire sooner than you expect? Aging baby-boomers, corporate medicine, the medical practice great resignation and/or the pandemic, etc?
Early retirement is nothing new, but it’s clear how much the COVID-19 pandemic has affected an aging workforce. Whether due to downsizing, objections to vaccine mandates, concerns about exposure risks, other health issues, or the desire for more leisure time, the retired general population grew by 3.5 million over the past two years—compared to an annual average of 1 million between 2008 and 2019—according to the Pew Research Center.1 At the same time, a survey conducted by the National Institute on Retirement Security revealed that more than half of Americans are concerned that the COVID-19 pandemic has impacted their ability to achieve a secure retirement.2
***
***
There’s no need to panic, but those numbers make one thing clear, says Rob Williams, managing director of financial planning, retirement income, and wealth management for the Schwab Center for Financial Research. Flexible and personalized financial planning that addresses how you’d cope if you had to retire early can help you make the best use of all your resources.
So – Here are six steps to follow. We’ll use as an example a person who’s seeing if they could retire five years early, but the steps remain the same regardless of your individual time frame.
Step 1: Think strategically about pension and Social Security benefits
For most retirees, Social Security and (to a lesser degree) pensions are the two primary sources of regular income in retirement. You usually can collect these payments early—at age 62 for Social Security and sometimes as early as age 55 with a pension. However, taking benefits early will mean that you get smaller monthly benefits for the rest of your life. That can matter to your bottom line, even if you expect Social Security to be merely the icing on your retirement cake.
On the Social Security website, you can find a projection of what your benefits would be if you were pushed to claim them several years early. But if you’re part of a two-income couple, you may want to make an appointment at a Social Security office or with a financial professional to weigh the potential options.
For example, when you die, your spouse is eligible to receive your monthly benefit if it’s higher than his or her own. But if you claim your benefits early, thus receiving a reduced amount, you’re likewise limiting your spouse’s potential survivor benefit.
If you have a pension, your employer’s pension administrator can help estimate your monthly pension payments at various ages. Once you have these estimates, you’ll have a good idea of how much monthly income you can count on at any given point in time.
***
Step 2: Pressure-test your 401(k)
In addition to weighing different strategies to maximize your Social Security and/or pension, evaluate how much income you could potentially derive from your personal retirement savings—and there’s a silver lining here if you’re forced to retire early.
Rule of 55
Let’s say you leave your job at any time during or after the calendar year you turn 55 (or age 50 if you’re a public safety employee with a government defined-benefit plan). Under a little-known separation-of-service provision, often referred to as the “rule of 55,” you may be able take distributions (though some plans may allow only one lump-sum withdrawal) from your 401(k), 403(b), or other qualified retirement plan free of the usual 10% early-withdrawal penalties. However, be aware that you’ll still owe ordinary income taxes on the amount distributed.
This exception applies only to the plan (including any consolidated accounts) that you were contributing to when you separated from service. It does not extend to IRAs.
4% rule
There’s also a simple rule of thumb suggesting that if you spend 4% or less of your savings in your first year of retirement and then adjust for inflation each year following, your savings are likely to last for at least 30 years—given that you make no other changes to your withdrawals, such as a lump sum withdrawal for a one-time expense or a slight reduction in withdrawals during a down market.
To see how much monthly income you could count on if you retired as expected in five years, multiply your current savings by 4% and divide by 12. For example, $1 million x .04 = $40,000. Divide that by 12 to get $3,333 per month in year one of retirement. (Again, you could increase that amount with inflation each year thereafter.) Then do the same calculation based on your current savings to see how much you’d have to live on if you retired today. Keep in mind that your money will have to last five years longer in this instance.
Knowing the monthly amount your current savings can generate will give you a clearer sense of whether you’ll have a shortfall—and how large or small it might be. Use our retirement savings calculator to test different saving amounts and time frames.
Step 3: Don’t forget about health insurance, doctor!
Nobody wants to spend down a big chunk of their retirement savings on unanticipated healthcare costs in the years between early retirement and Medicare eligibility at age 65. If you lose your employer-sponsored health insurance, you’ll want to find some coverage until you can apply for Medicare.
Your options may include continuing employer-sponsored coverage through COBRA, insurance enrollment through the Health Insurance Marketplace at HealthCare.gov, or joining your spouse’s health insurance plan. You may also find discounted coverage through organizations you belong to—for example, the AARP.
Step 4: Create a post-retirement budget
To make sure your retirement savings will cover your expenses, add up the monthly income you could get from pensions, Social Security, and your savings. Then, compare the total to your anticipated monthly expenses (including income taxes) if you were to retire five years early and are eligible, and choose to file, for Social Security and pension benefits earlier.
Take into account various life events and expenditures you may encounter. You may not pay off your mortgage by the date you’d planned. Your spouse might still be working (which can add income but also prolong certain expenses). Or your children might not be out of college yet.
You’re probably fine if you anticipate that your monthly expenses will be lower than your income. But if you think your expenses would be higher than your early-retirement income, some suggest that you take one or more of these measures:
Retire later; practice longer.
Save more now to fill some of the potential gap.
Trim your budget so there’s less of a gap down the road.
Consider options for medical consulting or part-time work—and begin to explore some of those opportunities now.
To the last point, finding a physician job later in life can be challenging, but certain employment agencies specialize in this area. If you can find work you like that covers a portion of your expenses, you’ll have the option of delaying Social Security and your company pension to get higher payments later—and you can avoid dipping into your retirement savings prematurely.
When you retire early, you have to walk a fine line with your portfolio’s asset allocation—investing aggressively enough that your money has the potential to grow over a long retirement, but also conservatively enough to minimize the chance of big losses, particularly at the outset.
“Risk management is especially important during the first few years of retirement or if you retire early,” Rob notes, because it can be difficult to bounce back from a loss when you’re drawing down income from your portfolio and reducing the overall number of shares you own.
To strike a balance between growth and security, start by making sure you have enough money stashed in relatively liquid, relatively stable investments—such as money market accounts, CDs, or high-quality short-term bonds—to cover at least a year or two of living expenses. Divide the rest of your portfolio among stocks, bonds, and other fixed-income investments. And don’t hesitate to seek professional help to arrive at the right mix.
Many people are unaccustomed to thinking about their expenses because they simply spend what they make when working, Rob says. But one of the most valuable decisions you can make about your life in retirement is to reevaluate where your money is going now.
This serves two aims. First, it’s a reality check on the spending plan you’ve envisioned for retirement, which may be idealized (e.g., “I’ll do all the home maintenance and repairs!”). Second, it enables you to adjust your spending habits ahead of schedule—whichever schedule you end up following. This gives you more control and potentially more income.
Step 6: Reevaluate your current spending
For example, if you’re not averse to downsizing, moving to a less expensive home could reduce your monthly mortgage, property tax, and insurance payments while freeing up equity that could also be invested to provide additional monthly income.
“When you are saving for retirement, time is on your side”. You lose that advantage when you’re forced to retire early, but having a backup plan that anticipates the possibility of an early retirement can make the unknowns you face a lot less daunting.
The fact that every physician in private medical practice, without a business education, leaves approximately a million dollars on the table and is unaware of it is well known to business experts who work with medical doctors experiencing financial difficulties.
Business experts such as Dan S. Kennedy, Peter Drucker, Michael Gerber, Maxwell Maltz, Neil Baum, William Hanson,Huss and Coleman, Steven Hacker, Thomas Stanley, Chris Hurn, Napoleon Hill, and Dave Ramsey, among others, understand the financial problems faced by medical practices and how to solve them.
Posted on March 2, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
RETIREMENT PLANNING
By Staff Reporters
***
***
A PEP is a defined contribution plan, such as a 401(k), in which multiple employers can participate. When employers join a PEP, they delegate their named fiduciary role to a third-party pooled plan provider (PPP). PEP fiduciary oversight falls on the PPP rather than the employer. And although each PPP may set its own eligibility requirements, businesses joining a PEP benefit plan needn’t operate in the same industry or geographical area.
PEP plans provide viable 401(k) alternatives for small business owners who may otherwise struggle to compete for talent against large organizations with comprehensive benefits packages.
Other advantages include: Less in-house administration: The PPP assumes responsibility for much of the plan administration, handling all plan documentation, governmental filings and ongoing compliance. Employee payroll deductions are left to the employer, but these can be efficiently managed with the help of a payroll service provider that integrates payroll and benefits.
Tax credits can help offset PEP start-up costs. For the first three years of participation, employers may be eligible for a tax credit of $5,000 annually, with an additional $500 available to those who set up automatic enrollment. Under Secure Act 2.0, an additional credit of up to $1,000 per employee for eligible employer contributions may apply to employers with up to 50 employees for the preceding taxable year. This credit phases out from 51 to 100 employees.
Businesses participating in single-employer retirement plans (SEP) must independently communicate and coordinate with their record-keeper, custodian, investment advisor, trustee and auditor. With PEP, all these tasks and services are bundled into one, saving employers time and money.
Despite its advantages, a PEP does have some drawbacks, particularly when compared to an SEP. Unlike a PEP, an SEP gives employers more of the following:
Flexibility: Employers can customize the design of their plan to meet their retirement goals and the needs of their employees.
Control: Employers are not dependent on the actions or decisions of others and can access information and resolve problems directly without the need of a third party.
Choice: Employers have the unilateral freedom to choose a different service provider, move their plan or negotiate better pricing if they are unsatisfied with the cost or quality of service.
Bank of America just acknowledged that the personal information of 57,028 of its customers has been compromised. This breach, attributed to a failure at Infosys McCamish Systems (IMS), a provider of insurance business process solutions engaged by the bank, poses a substantial risk of identity theft to the affected individuals.
The data breach notification, filed in Maine, reveals that sensitive information related to Bank of America’s deferred compensation plans was inadvertently accessed. IMS, in a notification letter to customers, disclosed that the compromised data encompasses a range of critical personal details. The accessed information includes customers’ names, addresses, business email addresses, dates of birth, Social Security numbers, and other account specifics. Such data is typically all required for an identity thief to execute fraudulent activities under another person’s name.
IMS’s admission that it might never be able to precisely identify what information was accessed underscores the severity and potential long-term consequences of the breach. This uncertainty adds an additional layer of anxiety for customers, highlighting the challenges in mitigating the aftermath of such security failures.
Finally, Walmart and Home Depot will be the star of the show this week they report their earnings for the holiday quarter. Nvidia will also try to keep its historic hot streak going when it reports on Wednesday—expectations are through the roof.
For many physicians it’s about demographics. Just like the rest of us, doctors are aging too. Already the average physician age is about 53 years old. The Association of American Medical Colleges reports that about half of doctors are over the age of 55. Over the next decade, an estimated 40% of physicians will be over 65 years old. This means more than two of every five active physicians will reach age 65 within the next 10 years.
***
***
Moreover, compared with their boomer colleagues who were more likely to work past retirement, a robust 60% of younger Generation X doctors are reporting that they plan to retire by age 60.
Doctors cite poor quality of life and stress as reasons for their early departure. The pandemic certainly crushed many providers and has led to burnout. Generation X physicians in their 40s and early 50s were more likely than boomers to report that their current work life was not making the grade. In short, 43% of middle-aged doctors, compared with 31% of doctors over age 55, were reporting lower levels of professional fulfillment. Moreover, 47% of mostly Gen X doctors indicated dissatisfaction with their level of personal fulfillment compared with 36% of practicing boomer physicians.
That dissatisfaction is translating into action and the pandemic is not the only reason for discontent. One survey of physicians in Massachusetts indicated that one in four doctors plans to leave medicine in the next two years and that staffing shortages and related administrative demands, e.g., hospital system metrics, paperwork, eMRs and meeting insurance requirements, were the most cited source of workplace stress.