BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] E-mail: MarcinkoAdvisors1738@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
As 2027 approaches, Americans are bracing for a significant spike in health insurance costs. Rising premiums are not new, but the scale and speed of the increases expected in 2027 represent a turning point. Households, employers, and healthcare providers will all feel the impact, and understanding what is driving these changes—and what to expect next—will be essential for navigating the year ahead.
One of the biggest forces behind the 2027 surge is the post‑pandemic cost rebound. Throughout the early 2020s, many insurers saw unusual fluctuations in claims: first a drop in elective care, then a surge as patients returned for delayed procedures. By 2026, insurers were still absorbing the financial consequences of those swings. Now, as utilization stabilizes, insurers are recalibrating premiums to reflect higher baseline costs. More people are seeking care, and they are seeking more expensive care. That alone pushes premiums upward.
Another major driver is the rapid rise in medical inflation. Healthcare costs have been increasing faster than general inflation for decades, but 2027 is expected to bring an acceleration. Hospital labor shortages, higher wages for nurses and technicians, increased pharmaceutical prices, and the growing cost of advanced medical technologies all contribute to a more expensive healthcare ecosystem. Insurers pass those costs along to consumers through higher premiums, deductibles, and out‑of‑pocket maximums.
A third factor is the aging population. As more Americans enter retirement age, demand for chronic disease management, specialty care, and long‑term services rises. Even though Medicare covers older adults, private insurers still bear significant costs through Medicare Advantage plans and supplemental policies. The demographic shift increases overall healthcare spending, and insurers adjust pricing accordingly.
Employers will face their own challenges in 2027. Many companies already struggle with the rising cost of providing health benefits, and the expected spike will force difficult decisions. Some employers may shift more costs to workers through higher payroll deductions or increased deductibles. Others may reduce coverage options, narrow provider networks, or move toward high‑deductible health plans paired with health savings accounts. Smaller businesses, in particular, may find it harder to offer competitive benefits, potentially affecting hiring and retention.
For individuals buying coverage on the marketplace or directly from insurers, the spike will be even more visible. Premiums for Affordable Care Act plans are expected to rise sharply, and while subsidies may soften the blow for some, many middle‑income families will feel the full weight of the increases. The result could be a rise in underinsurance—people technically covered but unable to afford meaningful care due to high deductibles and copays.
Another consequence of rising costs is the continued growth of alternative care models. Telehealth, direct primary care, and concierge medicine have gained traction as consumers seek more predictable costs and better access. In 2027, these models may expand further, especially among younger and tech‑savvy populations. While they do not replace comprehensive insurance, they can reduce reliance on traditional care pathways and help people manage routine health needs more affordably.
The spike in costs will also intensify debates around healthcare policy. Lawmakers, regulators, and industry leaders will face pressure to address affordability, transparency, and competition. Some will push for stronger oversight of insurance pricing, while others will advocate for reforms aimed at reducing underlying medical costs. Regardless of the political direction, the issue will be impossible to ignore as millions of Americans confront higher bills.
Consumers should prepare for 2027 by reviewing their coverage options carefully. Comparing plans, understanding cost‑sharing structures, and evaluating employer benefits will be more important than ever. Families may need to adjust budgets to account for higher premiums or explore supplemental coverage to manage risk. Preventive care, wellness programs, and chronic disease management will also play a larger role in controlling personal healthcare expenses.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors1738@outlook.com -OR-http://www.MarcinkoAssociates.com
The insurance industry is often portrayed as a field of limitless earning potential, where motivated agents can build substantial wealth through commissions, renewals, and long‑term client relationships. Yet behind that glossy promise lies a stark reality: many insurance agents struggle financially, and some end up broke. Understanding why this happens requires looking beyond surface‑level assumptions and examining the structural, behavioral, and psychological factors that shape an agent’s financial trajectory.
One of the most significant reasons some insurance agents end up broke is the commission‑only compensation structure that dominates the industry. New agents frequently enter the business with no salary, no guaranteed income, and no established client base. They must generate revenue entirely through sales, which can take months or even years to build. During this ramp‑up period, many agents face inconsistent income, making it difficult to cover basic expenses, invest in marketing, or maintain financial stability. Without savings or a financial cushion, the pressure of unpredictable earnings can quickly become overwhelming.
Another major factor is high turnover and inadequate training. Insurance companies often recruit aggressively, emphasizing opportunity rather than the realities of the job. Many new agents receive minimal training in sales, product knowledge, compliance, or business management. They are handed a license and a list of prospects and told to “go sell.” Without strong mentorship or structured development, inexperienced agents make avoidable mistakes, fail to close deals, or struggle to retain clients. Poor training leads to poor performance, and poor performance leads to financial hardship.
A related issue is the misalignment between personality and profession. Successful insurance agents must be resilient, self‑motivated, disciplined, and comfortable with rejection. They must prospect constantly, network strategically, and maintain a high level of emotional stamina. Many people enter the industry attracted by the promise of flexible hours or high commissions but lack the temperament required for sustained sales activity. When the reality of cold calling, door knocking, or relentless follow‑up sets in, they lose momentum. Without consistent effort, income dries up.
Marketing is another area where agents often stumble. In today’s competitive environment, insurance agents must invest in branding, advertising, digital presence, and lead generation. Yet many agents operate with no marketing budget or rely solely on outdated methods. They underestimate the cost of acquiring clients and fail to reinvest earnings into growth. As a result, their pipeline remains thin, and their income remains unstable. Agents who treat their work like a job rather than a business often fail to build the infrastructure needed for long‑term financial success.
Financial mismanagement also plays a significant role. When agents do experience a strong month or close a large policy, they may spend impulsively, assuming the momentum will continue. But insurance income is cyclical, and commissions can fluctuate dramatically. Agents who do not budget carefully, save consistently, or plan for slow periods often find themselves in financial trouble. The lack of predictable income requires disciplined money management, yet many agents enter the field without those skills.
Another challenge is overreliance on one product or one carrier. Agents who focus too narrowly—selling only life insurance, only Medicare, or only auto policies—become vulnerable to market shifts, regulatory changes, or carrier adjustments. When commissions drop or underwriting guidelines tighten, their income can collapse. Diversification is essential, but many agents fail to broaden their offerings or adapt to changing conditions.
Finally, some agents struggle because they underestimate the importance of client retention. Selling a policy is only the beginning; maintaining relationships, providing service, and ensuring renewals are what create stable, recurring income. Agents who neglect follow‑up or treat clients as one‑time transactions lose renewals, referrals, and long‑term revenue. Without a strong retention strategy, even agents who sell well can end up broke.
In the end, the reasons some insurance agents struggle financially are not mysterious. They stem from structural challenges, skill gaps, inconsistent habits, and the demanding nature of the profession. The agents who thrive are those who treat their work as a business, invest in their development, manage money wisely, and maintain relentless discipline. The ones who do not often find themselves facing financial instability. The industry offers opportunity, but it does not guarantee success; that part is entirely up to the agent.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors1738@outlook.com -OR-http://www.MarcinkoAssociates.com
The Medicare Part A Trust Fund, formally known as the Hospital Insurance (HI) Trust Fund, occupies a central place in the United States’ health‑care landscape. It finances inpatient hospital services, skilled nursing facility care, hospice services, and some home health care for tens of millions of older adults and people with disabilities. Because it is funded primarily through payroll taxes, its financial health is often viewed as a barometer of the broader relationship between the American workforce, the federal budget, and the aging population. When projections indicate that the trust fund will remain solvent for an additional twelve years, the implications ripple far beyond accounting tables. This extended solvency horizon shapes political debates, influences health‑care planning, and affects the sense of security felt by current and future beneficiaries.
At its core, solvency means that the trust fund can fully pay its obligations without requiring legislative intervention. When analysts project twelve more years of solvency, they are essentially saying that the fund’s income—mainly payroll taxes, taxes on Social Security benefits, and interest—will be sufficient to cover expected expenditures for more than a decade. This is not a trivial achievement. Medicare Part A has long faced pressure from demographic shifts, particularly the retirement of the baby‑boomer generation and the corresponding slowdown in the growth of the working‑age population. As more people draw benefits and fewer workers contribute payroll taxes, the financial balance naturally tightens. Extending solvency by twelve years suggests that recent economic conditions, policy adjustments, or health‑care cost trends have temporarily eased that pressure.
One of the most important consequences of a longer solvency window is the breathing room it provides for policymakers. Medicare reform is notoriously difficult. It requires navigating ideological divides, balancing fiscal responsibility with social commitments, and confronting the political risks of altering a program that millions of Americans rely on. When insolvency looms just a few years away, the pressure to act can lead to rushed or contentious proposals. A twelve‑year buffer, however, allows for a more deliberate and thoughtful approach. Lawmakers can explore structural reforms, evaluate the long‑term effects of payment changes, and consider broader health‑care system improvements without the immediate threat of benefit disruptions.
***
***
For beneficiaries, the extension of solvency carries psychological and practical significance. Medicare is not merely a government program; it is a promise woven into the fabric of American retirement planning. Workers contribute payroll taxes throughout their careers with the expectation that Medicare will be there when they need it. News that the trust fund is projected to remain solvent for twelve more years reinforces that sense of reliability. It reassures current beneficiaries that their hospital coverage is secure and signals to younger workers that the system is not on the brink of collapse. While projections are not guarantees, they shape public confidence in ways that influence everything from personal financial planning to political engagement.
The extended solvency period also reflects underlying trends in health‑care spending and economic performance. When the economy grows, payroll tax revenue increases, strengthening the trust fund. Similarly, when health‑care cost growth slows—whether due to changes in provider behavior, technological improvements, or policy adjustments—Medicare’s expenditures rise more gradually. A twelve‑year solvency projection suggests that, at least for now, these forces are aligned in a favorable direction. It does not mean that long‑term challenges have disappeared, but it does indicate that the system is more resilient than some earlier forecasts suggested.
Still, the projection of twelve more years of solvency should not be interpreted as a signal to relax. The trust fund’s long‑term trajectory remains shaped by structural factors that will not resolve themselves. The aging population will continue to grow, and the ratio of workers to beneficiaries will continue to shrink. Health‑care costs, even when growing more slowly, still tend to outpace general inflation. Moreover, Medicare Part A relies heavily on payroll taxes, which are sensitive to economic cycles. A recession, a shift in employment patterns, or a slowdown in wage growth could quickly erode the projected solvency cushion. In this sense, the twelve‑year projection is both a reassurance and a warning: the system is stable for now, but not indefinitely.
***
***
The extended solvency window also invites a broader conversation about the future of Medicare financing. Some argue that the trust fund’s challenges highlight the need for new revenue sources, such as adjustments to payroll tax rates or expansions of the taxable wage base. Others advocate for reforms on the spending side, including changes to provider payments, incentives for value‑based care, or efforts to reduce unnecessary hospitalizations. Still others propose more sweeping transformations, such as integrating Medicare’s financing streams or rethinking the division between Part A and Part B. A twelve‑year horizon does not dictate which path policymakers should choose, but it does create space for a more comprehensive and less crisis‑driven debate.
Another dimension of the solvency discussion involves the broader health‑care system. Medicare is a major payer, and its policies influence hospitals, physicians, insurers, and state governments. When the trust fund is under severe financial strain, Medicare may adopt more aggressive cost‑control measures, which can ripple through the entire system. A longer solvency period reduces the immediate pressure for abrupt changes, allowing the health‑care sector to adapt more gradually. Hospitals, for example, can plan capital investments with greater confidence, and providers can engage in long‑term quality‑improvement initiatives without fearing sudden reimbursement cuts.
Ultimately, the projection of twelve more years of solvency for the Medicare Part A Trust Fund is a reminder of both the program’s durability and its vulnerability. It underscores the importance of economic growth, prudent policy choices, and ongoing efforts to improve the efficiency of health‑care delivery. It also highlights the need for vigilance. Solvency projections can shift from year to year, and a comfortable cushion today does not eliminate the need for long‑term planning. But for now, the extended horizon offers a measure of stability—an opportunity to strengthen Medicare for future generations while honoring the commitment made to those who depend on it today.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
For many people, renting a home or apartment feels like a temporary or transitional stage, something less permanent than homeownership and therefore less in need of formal protection. Yet this assumption often leads renters to overlook one of the most important safeguards available to them: renter’s insurance. While landlords typically carry insurance for the building itself, that coverage does not extend to a tenant’s personal belongings or liability. Renter’s insurance fills that gap, offering a surprisingly robust layer of protection at a relatively low cost. Understanding what renter’s insurance covers, how it works, and why it matters can help renters make informed decisions that protect their financial stability and peace of mind.
At its core, renter’s insurance is designed to protect personal property. Many renters underestimate the value of their belongings, assuming that they do not own enough to justify insurance. But when you add up the cost of furniture, electronics, clothing, kitchenware, and other essentials, the total value can easily reach several thousands of dollars. A single fire, burst pipe, or break‑in could wipe out years of accumulated possessions. Renter’s insurance provides reimbursement for these losses, allowing tenants to replace what was damaged or stolen without bearing the full financial burden. Policies typically cover a wide range of events, including theft, vandalism, smoke damage, and certain types of water damage. For renters who rely on their belongings for work or daily living, this protection can be invaluable.
Another major component of renter’s insurance is liability coverage. This aspect of the policy protects renters if they are found legally responsible for injuries or property damage that occur within their rented space. For example, if a guest slips on a wet floor and suffers an injury, the renter could be held liable for medical expenses or legal fees. Without insurance, these costs could be financially devastating. Liability coverage also extends to accidental damage caused by the renter to someone else’s property. Even a small mishap—like a kitchen fire that spreads to a neighboring unit—can result in significant costs. Renter’s insurance helps shield tenants from these unexpected financial risks, offering a safety net that many people do not realize they need until it is too late.
A lesser‑known but highly valuable feature of renter’s insurance is coverage for additional living expenses. If a rental unit becomes uninhabitable due to a covered event, such as a fire or severe water damage, the policy can help pay for temporary housing, meals, and other necessary expenses. This benefit ensures that renters are not left scrambling for a place to stay or forced to pay out‑of‑pocket for hotel rooms while repairs are underway. In moments of crisis, having this support can make a significant difference in maintaining stability and reducing stress.
One of the most compelling aspects of renter’s insurance is its affordability. Compared to other types of insurance, premiums for renter’s policies are generally low, often costing less per month than a typical streaming subscription. This affordability makes it accessible to a wide range of renters, including students, young professionals, and families. The relatively small investment can yield substantial financial protection, making renter’s insurance one of the most cost‑effective forms of coverage available. For many renters, the peace of mind alone is worth the modest monthly expense.
***
***
Despite its benefits, renter’s insurance remains underutilized. Some renters assume that their landlord’s insurance will cover their belongings, not realizing that the landlord’s policy only protects the building structure. Others believe that their possessions are not valuable enough to insure, or they simply have not taken the time to explore their options. Education plays a key role in addressing these misconceptions. When renters understand what is at stake and how renter’s insurance works, they are more likely to recognize its importance and take steps to protect themselves.
Choosing the right renter’s insurance policy involves evaluating personal needs and understanding the different types of coverage available. One important decision is whether to select actual cash value coverage or replacement cost coverage. Actual cash value policies reimburse the depreciated value of items, while replacement cost policies cover the cost of buying new items at current prices. Although replacement cost coverage is typically more expensive, it often provides more meaningful protection, especially for essential items like electronics or furniture. Renters should also consider the policy’s deductible, coverage limits, and any optional add‑ons that may be relevant to their situation.
Ultimately, renter’s insurance is about more than protecting belongings; it is about safeguarding financial well‑being and creating a sense of security. Life is unpredictable, and even the most careful renter cannot control every circumstance. Whether it is a break‑in, a kitchen accident, or a burst pipe, unexpected events can disrupt daily life and lead to significant expenses. Renter’s insurance offers a practical, affordable way to prepare for these possibilities. By investing in a policy, renters take an important step toward protecting themselves, their possessions, and their future stability.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Understanding the Foundations of Financial Protection
Insurance plays a quiet but essential role in modern life. It is one of the few tools that helps individuals, families, and businesses manage uncertainty in a world where accidents, illnesses, natural disasters, and unexpected losses can occur at any moment. At its core, insurance is a system of risk transfer: a policyholder pays a relatively small, predictable premium to an insurer, who in turn promises financial protection against specific, larger risks. Over time, different types of insurance have evolved to address different needs. Understanding these categories not only helps people make informed decisions but also highlights how deeply insurance is woven into the structure of society.
Health Insurance
Health insurance is often considered the most essential type because medical care can be extremely expensive. A single hospital stay or emergency procedure can create financial strain for even the most prepared households. Health insurance helps reduce this burden by covering part or all of the cost of doctor visits, hospitalizations, surgeries, medications, and preventive care. Policies vary widely, from employer-sponsored plans to individual policies and government programs. Regardless of the structure, the purpose remains the same: to ensure that people can access medical care without facing overwhelming financial consequences.
Life Insurance
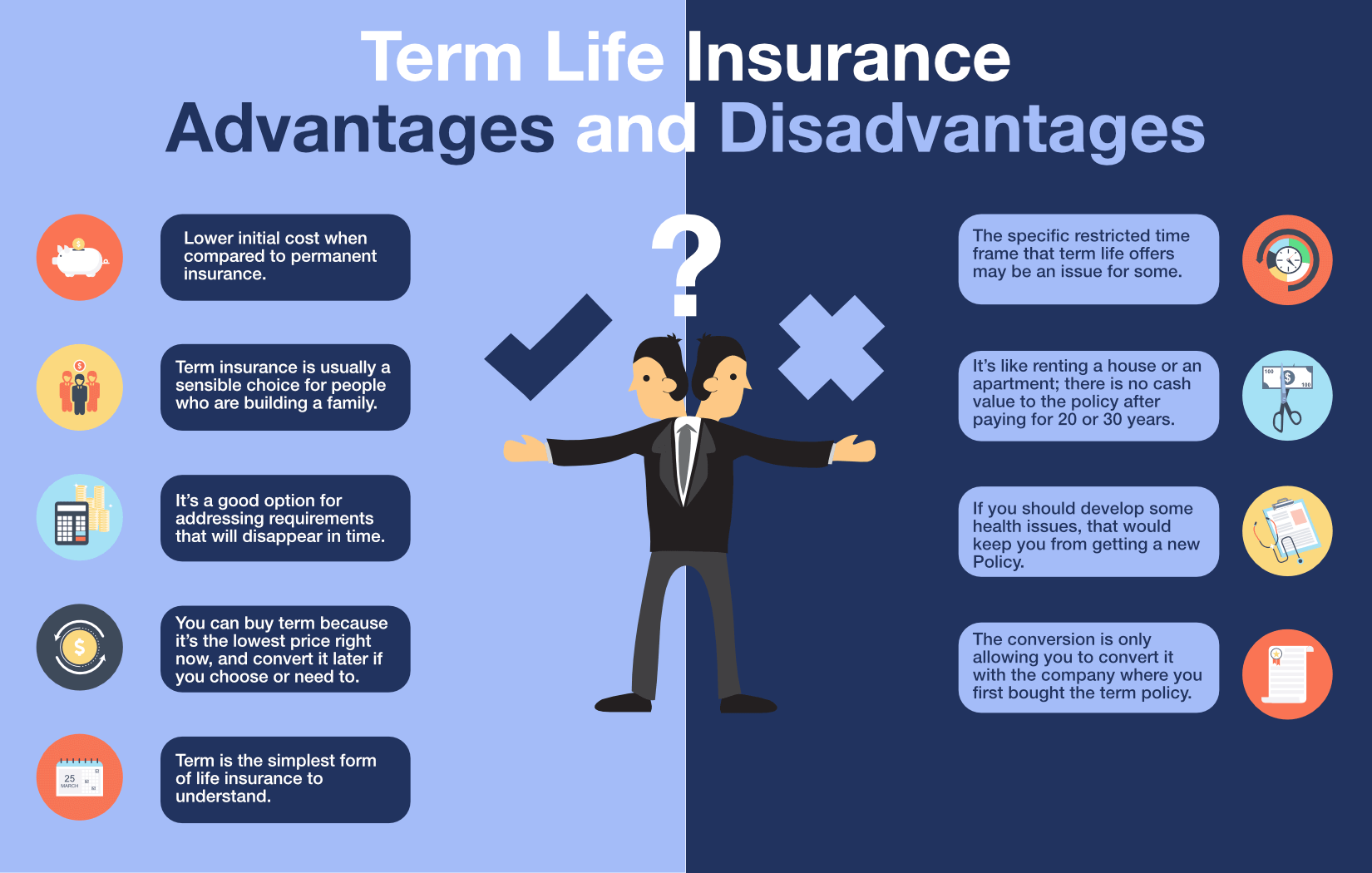
Life insurance addresses a different kind of risk—the financial impact of a person’s death on their dependents. When the insured person passes away, the insurer pays a lump sum to the beneficiaries. This money can replace lost income, cover funeral expenses, pay off debts, or support long-term financial goals such as education. There are two major forms: term life insurance, which provides coverage for a specific period, and whole life insurance, which lasts for the insured’s lifetime and often includes a savings component. Life insurance is especially important for families who rely on one or more income earners.
Auto Insurance
For anyone who owns or drives a vehicle, auto insurance is both a legal requirement in most places and a practical necessity. It protects drivers financially if they cause an accident, damage property, or injure someone. Many policies also cover damage to the insured’s own vehicle from collisions, theft, vandalism, or natural events. Auto insurance is typically divided into components such as liability, collision, and comprehensive coverage. Because driving involves constant exposure to risk, auto insurance is one of the most widely purchased forms of protection.
Homeowners and Renters Insurance
A home is often the largest investment a person makes, and protecting it is crucial. Homeowners insurance covers the structure of the home and the personal belongings inside it against risks like fire, theft, storms, and other hazards. It also includes liability protection if someone is injured on the property. Renters insurance serves a similar purpose for those who do not own their homes, covering personal belongings and liability but not the building itself. These policies provide peace of mind by ensuring that a single disaster does not lead to financial ruin.
Disability Insurance
While many people think about protecting their property, fewer consider protecting their ability to earn an income. Disability insurance fills this gap by providing income replacement if a person becomes unable to work due to illness or injury. Short‑term disability covers temporary conditions, while long‑term disability can provide support for years or even decades. Because the loss of income can be more financially damaging than the loss of property, disability insurance is a critical but often overlooked component of financial planning.
Business Insurance
Businesses face a wide range of risks, from property damage to lawsuits to employee injuries. Business insurance is a broad category that includes many specialized policies. General liability insurance protects against claims of injury or property damage caused by the business. Property insurance covers buildings, equipment, and inventory. Workers’ compensation insurance provides benefits to employees who are injured on the job. More specialized forms, such as cyber insurance or professional liability insurance, address modern risks that have emerged with technological and economic changes. For companies of all sizes, insurance is essential to maintaining stability and continuity.
***
***
Travel Insurance
Travel insurance has grown in popularity as more people explore the world. It typically covers trip cancellations, lost luggage, medical emergencies abroad, and other unexpected events that can disrupt travel plans. While not always necessary, it can be extremely valuable when traveling internationally, where healthcare systems and costs may differ significantly from those at home.
Why Insurance Matters
Across all these categories, the underlying purpose of insurance remains consistent: to reduce the financial impact of unpredictable events. It allows individuals and businesses to plan for the future with greater confidence. Without insurance, many people would be unable to recover from major setbacks, and many businesses would struggle to survive unexpected losses. Insurance also contributes to broader economic stability by spreading risk across large groups of people.
Conclusion
Insurance may not be the most exciting topic, but its importance is undeniable. By understanding the different types of insurance—health, life, auto, homeowners, renters, disability, business, and travel—people can make informed decisions about the protections they need. Each type addresses a specific category of risk, and together they form a comprehensive safety net that supports financial security and resilience. In a world full of uncertainties, insurance remains one of the most reliable tools for safeguarding the future.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on February 2, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
The Role of Artificial Intelligence in Insurance and Risk Management
Artificial Intelligence (AI) is revolutionizing the insurance and risk management industries by enhancing efficiency, accuracy, and customer experience. As data becomes increasingly central to decision-making, AI offers powerful tools to analyze vast datasets, predict outcomes, and automate complex processes. Its integration is reshaping traditional models and enabling insurers to better assess risk, detect fraud, and personalize services.
One of the most transformative applications of AI in insurance is in underwriting. Traditionally, underwriting relied on manual evaluation of risk factors, which was time-consuming and prone to human error. AI algorithms can now process structured and unstructured data—from medical records to social media activity—to assess risk profiles with greater precision. Machine learning models continuously improve as they ingest more data, allowing insurers to refine their risk assessments and pricing strategies dynamically.
Claims processing is another area where AI is making a significant impact. Through natural language processing (NLP) and image recognition, AI can automate the evaluation of claims, reducing the time and cost associated with manual reviews. For example, AI can analyze photos of vehicle damage to estimate repair costs or flag inconsistencies in a claim that may indicate fraud. This not only speeds up the claims cycle but also enhances fraud detection, a critical concern in the industry.
Risk management benefits from AI’s predictive capabilities. By analyzing historical data and identifying patterns, AI can forecast potential risks and suggest mitigation strategies. In property insurance, AI can assess the likelihood of natural disasters by combining satellite imagery with climate data. In health insurance, predictive analytics can identify individuals at higher risk of chronic conditions, enabling early interventions and reducing long-term costs.
***
***
Customer experience is also being transformed by AI. Chatbots and virtual assistants provide 24/7 support, answering queries, guiding users through policy selection, and even initiating claims. These tools improve accessibility and responsiveness, fostering customer satisfaction and loyalty. Moreover, AI-driven personalization allows insurers to tailor products and communications to individual preferences and behaviors, enhancing engagement.
Despite its advantages, the adoption of AI in insurance and risk management raises ethical and regulatory challenges. Data privacy is a major concern, as AI systems require access to sensitive personal information. Ensuring transparency in AI decision-making is also critical, especially when algorithms influence coverage eligibility or claim outcomes. Regulators are increasingly scrutinizing AI applications to ensure fairness, accountability, and compliance with legal standards.
In conclusion, AI is a game-changer for insurance and risk management, offering tools to streamline operations, improve accuracy, and enhance customer service. As the technology evolves, insurers must balance innovation with ethical responsibility, ensuring that A.I. serves both business goals and societal interests. The future of insurance lies in intelligent systems that not only manage risk but also anticipate and prevent it—ushering in a new era of proactive, data-driven protection.
Posted on January 8, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko; MBA MEd
***
***
What Medicare Does Not Cover: Understanding the Gaps in Coverage
Medicare, the federal health insurance program primarily for individuals aged 65 and older, provides essential coverage through its various parts—Part A (hospital insurance), Part B (medical insurance), Part C (Medicare Advantage), and Part D (prescription drug coverage). While it offers substantial support for many healthcare needs, Medicare does not cover everything. Understanding these gaps is crucial for beneficiaries to avoid unexpected expenses and plan for supplemental coverage.
One of the most significant omissions in Original Medicare (Parts A and B) is routine dental care. Services such as cleanings, fillings, tooth extractions, and dentures are generally not covered. Although Medicare began covering limited dental exams related to specific medical procedures in 2023 and 2024, comprehensive dental care remains excluded.
Vision care is another area where Medicare falls short. Routine eye exams, eyeglasses, and contact lenses are not covered unless related to specific medical conditions like cataract surgery. Similarly, hearing services, including exams and hearing aids, are not covered under Original Medicare, despite their importance to seniors’ quality of life.
Long-term care, such as custodial care in nursing homes or assisted living facilities, is also excluded. Medicare may cover short-term stays in skilled nursing facilities following hospitalization, but it does not pay for extended stays or help with daily activities like bathing and dressing.
Alternative therapies such as acupuncture, massage therapy, and chiropractic care are generally not covered unless deemed medically necessary. For example, Medicare may cover limited chiropractic services for spinal subluxation but not for general wellness or pain relief.
Cosmetic surgery is excluded unless it is required for reconstructive purposes following an accident or disease. Similarly, routine foot care and podiatry services are not covered unless related to specific medical conditions like diabetes.
To address these gaps, many beneficiaries turn to Medicare Advantage plans (Part C) or Medigap policies, which may offer additional benefits such as dental, vision, and hearing coverage. However, these plans vary widely, and not all supplemental policies cover every excluded service.
In conclusion, while Medicare provides a strong foundation for healthcare coverage, it leaves out several essential services that can significantly impact seniors’ health and finances. Awareness of these exclusions empowers beneficiaries to seek supplemental insurance, budget for out-of-pocket costs, and make informed decisions about their healthcare needs.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on January 3, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
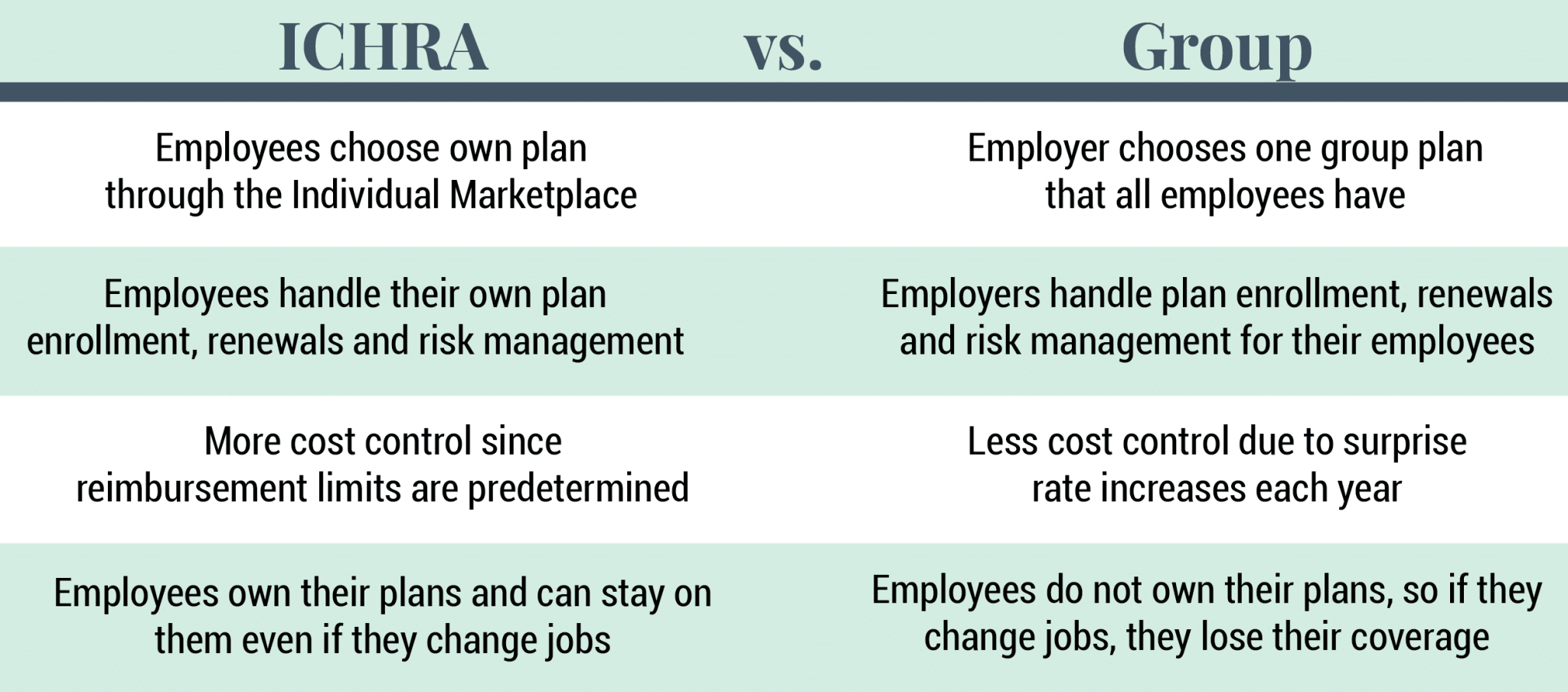
Alternative health coverage models like Short-Term Duration Plans, Health Care Sharing Ministries (HCSMs), and Individual Coverage Health Reimbursement Arrangements (ICHRAs) offer flexible, cost-conscious options for individuals and employers seeking alternatives to traditional insurance.
As the landscape of American healthcare continues to evolve, many consumers and employers are exploring non-traditional coverage models to address rising costs, limited access, and regulatory complexity. Among the most prominent alternatives are Short-Term Duration Plans, Health Care Sharing Ministries (HCSMs), and Individual Coverage Health Reimbursement Arrangements (ICHRAs)—each offering distinct advantages and trade-offs.
Short-Term Duration Plans are designed to provide temporary coverage for individuals experiencing gaps in insurance, such as between jobs or during waiting periods. These plans are typically less expensive than ACA-compliant insurance but come with significant limitations. They often exclude coverage for pre-existing conditions, maternity care, mental health services, and prescription drugs. While they offer affordability and quick enrollment, they lack the comprehensive protections mandated by the Affordable Care Act (ACA), making them a risky choice for those with ongoing health needs.
Health Care Sharing Ministries (HCSMs) represent a faith-based approach to healthcare financing. Members contribute monthly fees into a shared pool used to cover eligible medical expenses for others in the group. These arrangements are not insurance and are not regulated by state insurance departments, meaning they are not required to cover essential health benefits or guarantee payment. However, HCSMs appeal to individuals seeking community-based support and lower costs. They often include moral or religious requirements for membership and may exclude coverage for lifestyle-related conditions or services deemed inconsistent with their beliefs.
***
***
Individual Coverage Health Reimbursement Arrangements (ICHRAs) are employer-sponsored programs that allow businesses to reimburse employees for individual health insurance premiums and qualified medical expenses. Introduced in 2020, ICHRAs offer flexibility for employers to control costs while giving employees the freedom to choose plans that suit their needs. Unlike traditional group health insurance, ICHRAs shift the purchasing power to employees, promoting consumer choice and market competition. However, they require employees to navigate the individual insurance marketplace, which can be complex and variable depending on location and income.
Other emerging models include Direct Primary Care (DPC), where patients pay a monthly fee for unlimited access to a primary care provider, and Health Savings Accounts (HSAs) paired with high-deductible plans, which encourage consumer-driven healthcare spending. These models emphasize affordability, personalization, and preventive care, but may not offer sufficient protection against catastrophic health events.
In conclusion, alternative health coverage models provide valuable options for individuals and employers seeking flexibility and cost savings. However, they often come with trade-offs in coverage, regulation, and consumer protection. As ACA subsidies fluctuate and healthcare costs rise, these models are likely to gain traction—but consumers must carefully assess their health needs, financial risks, and eligibility before choosing a non-traditional path.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on December 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Employer-sponsored healthcare benefit programs have become a cornerstone of modern employment, shaping not only the financial well-being of workers but also the overall health of society. These programs represent a partnership between employers and employees, where organizations provide access to medical coverage as part of compensation packages. While wages remain the most visible form of remuneration, healthcare benefits often carry equal or greater significance, influencing job satisfaction, retention, and productivity.
At their core, employer-sponsored healthcare programs are designed to reduce the financial burden of medical expenses for employees. Healthcare costs can be unpredictable and overwhelming, and insurance coverage provides a safety net against sudden illness or injury. By offering group plans, employers can negotiate better rates with insurers, spreading risk across a larger pool of participants. This collective approach makes healthcare more affordable than if individuals were to purchase coverage independently. For employees, the assurance of medical support fosters peace of mind, allowing them to focus on their work without the constant worry of healthcare expenses.
From the employer’s perspective, healthcare benefits serve as a strategic tool for attracting and retaining talent. In competitive labor markets, robust benefit packages can distinguish one company from another. Workers often weigh healthcare coverage heavily when deciding between job offers, and organizations that provide comprehensive plans are more likely to secure skilled professionals. Moreover, offering healthcare benefits demonstrates a company’s commitment to employee welfare, reinforcing a culture of care and responsibility. This perception can strengthen loyalty and reduce turnover, ultimately saving organizations the costs associated with recruiting and training new staff.
***
***
Beyond recruitment and retention, healthcare benefits contribute directly to workplace productivity. Employees who have access to preventive care and regular medical services are less likely to suffer from untreated conditions that impair performance. Routine checkups, vaccinations, and screenings help identify health issues early, reducing absenteeism and minimizing disruptions to workflow. In addition, healthier employees tend to be more engaged, energetic, and capable of sustaining high levels of output. Employers thus benefit from a workforce that is not only present but also performing at its best.
Employer-sponsored healthcare programs also play a role in shaping organizational culture. When companies invest in employee health, they send a message that well-being is valued. This can foster trust and strengthen relationships between management and staff. In many cases, healthcare benefits are paired with wellness initiatives such as gym memberships, mental health resources, or nutritional counseling. These programs encourage healthier lifestyles, which in turn reduce long-term medical costs and enhance overall morale. The integration of healthcare and wellness initiatives reflects a holistic approach to employee support, extending beyond the workplace into personal lives.
Despite their advantages, employer-sponsored healthcare programs are not without challenges. Rising medical costs place pressure on employers to balance affordability with coverage quality. Smaller businesses may struggle to provide comprehensive plans, limiting their competitiveness in attracting talent. Additionally, employees may face limitations in provider networks or coverage options, leading to dissatisfaction. The complexity of healthcare systems can also create confusion, requiring employers to invest in education and communication to ensure employees understand their benefits. These challenges highlight the need for ongoing innovation and adaptation in benefit design.
Looking ahead, employer-sponsored healthcare programs are likely to evolve in response to changing workforce expectations and healthcare landscapes. Remote work, diverse employee demographics, and advances in medical technology will influence how benefits are structured. Employers may increasingly emphasize flexibility, offering customizable plans that cater to individual needs. Digital health tools, telemedicine, and wellness apps are already becoming integrated into benefit packages, expanding access and convenience. As organizations continue to adapt, the central principle remains the same: supporting employee health is both a moral responsibility and a strategic advantage.
In conclusion, employer-sponsored healthcare benefit programs are more than a financial perk; they are a vital component of modern employment relationships. By reducing medical costs, attracting talent, enhancing productivity, and fostering a culture of care, these programs create value for both employees and employers. While challenges persist, the continued evolution of healthcare benefits promises to strengthen their role in shaping healthier, more resilient workplaces. Ultimately, the success of these programs lies in their ability to balance economic realities with the human need for security and well-being.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Money is a powerful tool. It can provide security, open opportunities, and help build a fulfilling life. Yet, when mismanaged, it can quickly become a source of stress and regret. Understanding the worst ways to use money is essential for anyone who wants to avoid financial pitfalls and build lasting stability.
1. Impulse Spending
One of the most damaging habits is spending without thought. Buying items on impulse—whether it’s clothes, gadgets, or luxury goods—often leads to regret and wasted resources. These purchases rarely align with long‑term goals and can drain savings meant for emergencies or investments.
2. High‑Interest Debt
Credit cards and payday loans can trap people in cycles of debt. Paying 20% or more in interest means that even small purchases balloon into massive financial burdens. Using debt irresponsibly is one of the fastest ways to erode wealth.
3. Ignoring Savings and Investments
Failing to save for the future is another critical mistake. Without an emergency fund, unexpected expenses like medical bills or car repairs can derail financial stability. Similarly, neglecting investments means missing out on compound growth that builds wealth over time.
4. Chasing Get‑Rich‑Quick Schemes
From pyramid schemes to speculative “hot tips,” chasing unrealistic returns is a recipe for disaster. These schemes prey on greed and impatience, often leaving participants with nothing but losses. Sustainable wealth comes from patience and discipline, not shortcuts.
5. Overspending on Status
Many people waste money trying to impress others—buying luxury cars, designer clothes, or extravagant experiences they cannot afford. This pursuit of status often leads to debt and financial insecurity, while providing only fleeting satisfaction.
6. Neglecting Insurance
Skipping health, auto, or home insurance to save money may seem smart in the short term, but it can be catastrophic when disaster strikes. Without protection, one accident or emergency can wipe out years of savings.
7. Failing to Budget
Living without a plan is like sailing without a map. Without a budget, it’s easy to overspend, miss bills, or fail to allocate money toward goals. Budgeting is not restrictive—it’s empowering, because it ensures money is used intentionally.
8. Ignoring Education and Skills
Spending money without investing in personal growth is another hidden mistake. Education, training, and skill development often yield lifelong returns. Neglecting these opportunities can limit earning potential and financial independence.
Conclusion
The worst things to do with money often stem from short‑term thinking, lack of discipline, or the desire for instant gratification. Impulse spending, high‑interest debt, chasing schemes, and neglecting savings all undermine financial health. By avoiding these traps and focusing on budgeting, investing wisely, and protecting against risks, money can serve as a foundation for security and freedom rather than a source of stress.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Insurance agents are primarily paid through commissions, but may also earn salaries, bonuses, and fees depending on their employment model and the types of policies they sell.
Insurance agents play a vital role in helping individuals and businesses navigate the complex world of insurance. Their compensation structures vary widely, influenced by factors such as the type of insurance they sell, whether they work independently or for a company, and the specific agreements they have with insurers. Understanding how insurance agents are paid is essential for consumers who want to make informed decisions and for aspiring agents considering a career in the industry.
The most common form of compensation for insurance agents is commission-based pay. Agents earn a percentage of the premium paid by the customer when they successfully sell a policy. These commissions can vary depending on the type of insurance. For example, first-year commissions for auto and homeowners insurance typically range from 5% to 20%, while commercial property and casualty policies may offer 10% to 15%. Life insurance policies often provide higher initial commissions, sometimes exceeding 50% of the first-year premium, followed by smaller renewal commissions in subsequent years.
There are two main types of insurance agents: captive agents and independent agents. Captive agents work exclusively for one insurance company and usually receive a combination of salary and commissions. Their compensation may also include performance bonuses and incentives tied to sales targets. Independent agents, on the other hand, represent multiple insurers and rely more heavily on commissions. They have the flexibility to offer a wider range of products, but their income is directly tied to their ability to sell policies and maintain client relationships.
***
***
In addition to commissions, some agents earn fees for services such as policy reviews, risk assessments, or consulting. These fees are more common in commercial insurance or financial planning contexts, where agents provide specialized expertise. However, fee-based compensation is less prevalent in personal lines of insurance like auto or home coverage.
Bonuses and incentives are another component of agent compensation. Insurance companies often reward agents for meeting sales quotas, retaining clients, or selling specific types of policies. These bonuses can significantly boost an agent’s income, but they may also create potential conflicts of interest if agents prioritize higher-paying products over client needs.
Some agents, particularly those employed by large firms or call centers, receive a fixed salary. This model provides stability but may limit earning potential compared to commission-based roles. Salaried agents may still receive performance bonuses or profit-sharing depending on company policy.
Ultimately, an insurance agent’s earnings depend on their business model, experience, and ability to build a loyal client base. While commissions remain the cornerstone of insurance compensation, the rise of fee-based services and hybrid models reflects a shift toward more transparent and client-focused practices.
Consumers should feel empowered to ask agents about their compensation structure to ensure they receive unbiased advice tailored to their needs.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on November 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Here’s a risk to your financial health that may surprise you!
By Rick Kahler CFP™
There are two reasons for this.
First, we tend to trust and rely on people we know.
Second, research finds that humans have a deep-seated desire to meet the needs of others, so “helping” a relative or friend get started in their financial sales career is just human nature. Unfortunately, brokerage and insurance companies know this. They train their new agents that the easiest sales to make when getting started are to relatives and friends.
Any time I find an ill-advised financial product a client has purchased from a relative or friend, I cringe, anticipating the client’s resistance to canceling it. Regardless of how bad the advice was or how outrageous the fees of an investment product may be, the deeper the relationship the more difficulty there will be in changing course.
***
***
Here’s a typical example
Jim and Sofia, two young professionals, married at around the same time Jim’s uncle went to work for a financial services company. The uncle sold Jim a $250,000 Variable Universal Life (VUL) policy with a $500 monthly premium. Jim and Sofia were happy, thinking they had made a prudent choice to start saving for retirement and help out a relative at the same time.
When Sofia became pregnant, the couple decided to engage a fee-only financial planner. She found they were under insured to provide for a family and also that the VUL policy was incredibly expensive and ill-advised for their needs. She recommended canceling the VUL policy with its $500 monthly premium, instead paying $300 monthly for two $1 million term life insurance policies and putting $200 a month into a tax-free Roth IRA.
Sofia and Jim told this to their uncle, who was “shocked” at the planner’s “poor advice.”
He contended that any competent financial planner would know a person needs permanent insurance as a foundation to “raise their child in the case of a premature death, fund their retirement, pay estate taxes and just like a Roth, it is tax free.”
Sadly, the uncle was unwilling to admit that $250,000 of insurance wouldn’t be enough to raise their child, fund their retirement, and pay estate taxes; nor was it truly tax free. He also didn’t mention that he had a vested interest in their keeping the policy. While he probably earned 55% to 100% of the first year’s commission, it is common practice that an agent will also receive 10-15% of the annual premium from years 2-10.
***
***
Sofia and Jim agreed with the financial planner’s recommendation. They could see the sense in having $1 million of insurance on each of them instead of $250,000 on just Jim for almost half the price, plus the tax-free growth of $200 a month in the Roth IRA.
Yet they didn’t follow the planner’s advice, because they didn’t want to upset their uncle. They chose to weaken their financial health, plus risk the well-being of their family if one of them died prematurely, in order to enrich their uncle for fear of offending him.
This happens more frequently than you would think. And it isn’t limited to life insurance. I’ve seen clients invest in a variety of “opportunities,” based on advice from a family member, that were not in their best interest.
Assessment
Next time a friend or family member offers to sell you a financial product or give you some great advice, you may want to do yourself a favor and decline. If you really want to help them out, invite them over for dinner.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, urls and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Posted on October 29, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Level-funded health care is an increasingly popular option for small to mid-sized businesses seeking a balance between cost control and comprehensive employee coverage. It blends features of fully insured and self-funded health plans, offering employers greater flexibility and potential savings while minimizing risk.
In a traditional fully insured plan, employers pay a fixed premium to an insurance carrier, which assumes all financial risk for employee claims. In contrast, self-funded plans allow employers to pay for claims out-of-pocket, which can lead to significant savings—but also exposes them to unpredictable costs. Level-funded plans sit between these two models, offering a structured and predictable approach to self-funding.
With level-funded health care, employers pay a fixed monthly amount that covers three components: estimated claims funding, stop-loss insurance, and administrative fees. The estimated claims portion is based on actuarial data and reflects the expected health care usage of the employee group. Stop-loss insurance protects the employer from catastrophic claims by capping their financial exposure. Administrative fees cover third-party services such as claims processing and customer support.
One of the key advantages of level-funded plans is the potential for cost savings. If actual claims fall below the estimated amount, employers may receive a refund or credit at the end of the year. This incentivizes wellness programs and preventive care, as healthier employees lead to lower claims. Additionally, level-funded plans often provide more transparency into claims data, allowing employers to better understand health trends and make informed decisions about benefits.
***
***
Another benefit is flexibility. Level-funded plans can be customized to suit the needs of a specific workforce, offering a range of coverage options and provider networks. This contrasts with the rigid structure of many fully insured plans. Employers also gain more control over plan design, which can help attract and retain talent in competitive job markets.
However, level-funded health care is not without challenges. It requires careful planning and a solid understanding of risk. Employers must be prepared for the possibility that claims may exceed projections, although stop-loss insurance helps mitigate this. Additionally, level-funded plans may not be suitable for very small groups or those with high-risk populations, as the cost of stop-loss coverage can be prohibitive.
Regulatory considerations also play a role. Level-funded plans are typically governed by federal ERISA laws rather than state insurance regulations, which can affect compliance and reporting requirements. Employers should work closely with benefits consultants or brokers to ensure they understand the legal landscape and choose a plan that aligns with their goals.
In conclusion, level-funded health care offers a compelling alternative for businesses seeking to manage costs while providing quality coverage. By combining predictability with the potential for savings and customization, it empowers employers to take a more active role in their health benefits strategy. As the health care landscape continues to evolve, level-funded plans are likely to remain a valuable option for organizations looking to strike the right balance between affordability and employee well-being.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on October 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
In the evolving landscape of digital health care, Amazon Pharmacy and GoodRx have emerged as two leading platforms offering consumers affordable and convenient access to prescription medications. While both aim to simplify the process of obtaining prescriptions, they differ significantly in their approach, pricing models, and user experience.
Amazon Pharmacy, launched in 2020, is a full-service online pharmacy that allows customers to order medications directly through Amazon. It offers fast, free delivery for Prime members and integrates with most insurance plans. One of its standout features is RxPass, a subscription service available to Prime members for $5 per month, which covers unlimited eligible generic medications. This model is particularly attractive to individuals who take multiple generics regularly, as it can significantly reduce out-of-pocket costs.
In contrast, GoodRx, founded in 2011, operates primarily as a price comparison and discount platform. It does not dispense medications itself but partners with local and mail-order pharmacies to help users find the lowest prices. GoodRx provides coupons that can be used at thousands of pharmacies nationwide, often resulting in substantial savings—especially for those without insurance. It also offers GoodRx Gold, a paid membership that unlocks deeper discounts and telehealth services.
***
***
When comparing the two, pricing transparency is a key differentiator. GoodRx excels in showing users a range of prices across different pharmacies, empowering them to choose the most cost-effective option. Amazon Pharmacy, while competitive, typically offers fixed prices and focuses more on convenience and integration with its broader ecosystem.
Convenience is another area where Amazon Pharmacy shines. With its streamlined ordering process, automatic refills, and integration with Amazon’s delivery network, it appeals to users who prioritize ease and speed. GoodRx, while convenient in its own right, requires users to present coupons at the pharmacy or use mail-order services, which may involve more steps.
Insurance compatibility also varies. Amazon Pharmacy accepts most major insurance plans, making it a viable option for insured individuals. GoodRx, on the other hand, is often used by those without insurance or with high deductibles, as its discounts can sometimes beat insurance copays.
However, both platforms have limitations. Amazon Pharmacy’s RxPass is restricted to generic medications and excludes certain states due to regulatory issues. GoodRx’s discounts may not apply to all medications, and prices can fluctuate depending on location and pharmacy.
In terms of user experience, Amazon offers a seamless, tech-driven interface with customer support and medication management tools. GoodRx provides educational resources, price alerts, and a mobile app that helps users track savings and prescriptions.
Ultimately, the choice between Amazon Pharmacy and GoodRx depends on individual needs. For those seeking a one-stop solution with predictable costs and fast delivery, Amazon Pharmacy may be ideal. For users who want to shop around for the best deal or lack insurance, GoodRx offers unmatched flexibility and savings.
As digital health continues to grow, both platforms are reshaping how Americans access medications—making prescriptions more affordable, transparent, and accessible than ever before.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
What Medical School Didn’t Teach Doctors About Money
Medical school is designed to mold students into competent, compassionate physicians. It teaches anatomy, pathology, pharmacology, and clinical skills with precision and rigor. Yet, despite the depth of medical knowledge imparted, one critical area is often overlooked: financial literacy. For many doctors, the transition from student to professional comes with a steep learning curve—not in medicine, but in money. From managing debt to understanding taxes, investing, and retirement planning, medical school leaves a financial education gap that can have long-term consequences.
The Debt Dilemma
One of the most glaring omissions in medical education is how to manage student loan debt. The average medical student graduates with over $200,000 in debt, yet few are taught how to navigate repayment options, interest accrual, or loan forgiveness programs. Many doctors enter residency with little understanding of income-driven repayment plans or Public Service Loan Forgiveness (PSLF), missing opportunities to reduce their financial burden. Without guidance, some make costly mistakes—such as refinancing federal loans prematurely or choosing repayment plans that don’t align with their career trajectory.
Income ≠ Wealth
Medical students often assume that a high salary will automatically lead to financial security. While physicians do earn more than most professionals, income alone doesn’t guarantee wealth. Medical school rarely addresses the importance of budgeting, saving, and investing. As a result, many doctors fall into the “HENRY” trap—High Earner, Not Rich Yet. They spend lavishly, assuming their income will always cover expenses, only to find themselves living paycheck to paycheck. Without a solid financial foundation, even high earners can struggle to build net worth.
***
***
Taxes and Business Skills
Doctors are also unprepared for the complexities of taxes. Whether employed by a hospital or running a private practice, physicians face unique tax challenges. Medical school doesn’t teach how to track deductible expenses, optimize retirement contributions, or navigate self-employment taxes. For those who open their own clinics, the lack of business education is even more pronounced. Understanding profit margins, payroll, insurance billing, and compliance regulations is essential—but rarely covered in medical training.
Investing and Retirement Planning
Another blind spot is investing. Medical students are rarely taught the basics of compound interest, asset allocation, or retirement accounts. Many don’t know the difference between a Roth IRA and a traditional 401(k), or how to evaluate mutual funds and index funds. This lack of knowledge delays retirement planning and can lead to missed opportunities for long-term growth. Some doctors rely on financial advisors without understanding the fees or conflicts of interest involved, putting their wealth at risk.
Insurance and Risk Management
Medical school also fails to educate students on insurance—life, disability, malpractice, and health. Doctors need robust coverage to protect their income and assets, but many don’t know how to evaluate policies or understand terms like “own occupation” or “elimination period.” Inadequate coverage can leave physicians vulnerable to financial disaster in the event of illness, injury, or litigation.
Emotional and Behavioral Finance
Beyond technical knowledge, medical school overlooks the emotional side of money. Physicians often face pressure to maintain a certain lifestyle, especially after years of sacrifice. The desire to “catch up” can lead to impulsive spending, luxury purchases, and financial stress. Without tools to manage money mindset and behavioral habits, doctors may struggle with guilt, anxiety, or burnout related to finances.
The Case for Financial Education
Fortunately, awareness of this gap is growing. Organizations like Medics’ Money and podcasts such as “Docs Outside the Box” are working to fill the void by offering financial education tailored to physicians.
These resources cover everything from budgeting and debt management to investing and entrepreneurship. Some medical schools are beginning to incorporate financial literacy into their curricula, but progress is slow and inconsistent.
Conclusion
Medical school equips doctors to save lives, but it doesn’t prepare them to secure their own financial future. The lack of financial education leaves many physicians vulnerable to debt, poor investment decisions, and lifestyle inflation. To thrive both professionally and personally, doctors must seek out financial knowledge beyond the classroom. Whether through self-study, mentorship, or professional guidance, understanding money is as essential as understanding medicine. After all, financial health is a cornerstone of overall well-being—and every doctor deserves to master both.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 10, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITIONS
By Staff Reporters
***
***
Rate Review & the 80/20 Rule
The health care law provides 2 ways to hold insurance companies accountable and help keep your costs down: Rate Review and the 80/20 rule.
Rate Review
Rate Review helps protect you from unreasonable rate increases. Insurance companies must now publicly explain any rate increase of 15% or more before raising your premium. This does not apply to grandfathered plans.
The 80/20 Rule generally requires insurance companies to spend at least 80% of the money they take in from premiums on health care costs and quality improvement activities. The other 20% can go to administrative, overhead, and marketing costs.
The 80/20 rule is sometimes known as Medical Loss Ratio, or MLR. If an insurance company uses 80 cents out of every premium dollar to pay for your medical claims and activities that improve the quality of care, the company has a Medical Loss Ratio of 80%.
Insurance companies selling to large groups (usually more than 50 employees) must spend at least 85% of premiums on care and quality improvement.
If your insurance company doesn’t meet these requirements, you’ll get a rebate on part of the premium that you paid.
Will I get a rebate check from my insurance company?
If your insurance company doesn’t meet its 80/20 targets for the year, you’ll get back some of the premium that you paid.
You may see the rebate in a number of ways:
A rebate check in the mail
A lump-sum deposit into the same account that was used to pay the premium, if you paid by credit card or debit card
A direct reduction in your future premium
Your employer may also use one of the above rebate methods, or apply the rebate in a way that benefits employees
If you or your employer will get a rebate, your insurance company must notify you by August 1.
If you have an individual insurance policy, you’ll get the rebate directly from your insurance company.
For small group and large group plans, the rebate is usually paid to the employer. It may use one of the above rebate methods, or apply the rebate in a way that benefits employees.
FYI: The 80/20 rebate rules don’t apply when an insurance company has fewer than 1000 enrollees in a particular state or market.
For Rate Review: These requirements don’t apply to grandfathered plans. Check your plan’s materials or ask your employer or your benefits administrator to find out if your health plan is grandfathered.
For the 80/20 Rule: These rights apply to all individual, small group, and large group health plans, whether your plan is grandfathered or not.
Doctors and dentists earn money by treating patients. CPAs and Attorneys have clients, and retail stores buy items low and sell them at higher prices. This is called a business model.
More formally, a business model identifies the products or services the business plans to sell, the target market, and any anticipated expenses, in order to outline how to generate a profit. Business models are important for both new and established businesses. They help companies attract investment, recruit talent, and motivate management and staff.
Businesses should regularly update their business model, or they’ll fail to anticipate trends and challenges ahead. Business models also help investors to evaluate companies that interest them and employees to understand the future of a company they may aspire to join.
***
The Business Model of Pharmacy Benefits Managers
In the United States, health insurance providers often hire a third party to handle price negotiations, insurance claims, and distribution of prescription drugs. Providers that use such pharmacy benefit managers include commercial health plans, self-insured employer plans, Medicare Part D [drug] plans, the Federal Employees Health Benefits Program, and state government employee plans. PBMs are designed to aggregate the collective buying power of en-rollees through their client health plans, enabling plan sponsors and individuals to obtain lower prices for their prescription drugs. PBMs negotiate price discounts from retail pharmacies, rebates from pharmaceutical manufacturers, and mail-service pharmacies which home-deliver prescriptions without consulting face-to-face with a pharmacist.
Pharmacy benefit management companies can make revenue in several ways.
First, they collect administrative and service fees from the original insurance plan.
Then, they can also collect rebates from the manufacturer.
Traditional PBMs do not disclose the negotiated net price of the prescription drugs, allowing them to resell drugs at a public list price (also known as a sticker price), which is higher than the net price they negotiate with the manufacturer. This practice is known as “spread pricing”. The industry argues that savings are trade secrets. Pharmacies and insurance companies are often prohibited by PBMs from discussing costs and reimbursements. This leads to lack of transparency.
***
***
Therefore, states are often unaware of how much money they lose due to spread pricing, and the extent to which drug rebates are passed on to en-rollees of Medicare plans. In response, states like Ohio, West Virginia, and Louisiana have taken action to regulate PBMs within their Medicaid programs.
For instance, they have created new contracts that require all discounts and rebates to be reported to the states. In return, Medicaid pays PBMs a flat administrative fee.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on July 24, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Insurers selling plans on ACA exchanges are expected to hike premiums next year as subsidies on them are set to expire, with the average person expected to be paying 75% more, according to an analysis from the nonpartisan research group KFF.
Posted on June 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
A June 11th report from global professional services firm Alvarez & Marsal (A&M) predicts that more beneficiaries might soon ditch insurance coverage for options like short-term, limited duration plans or healthcare sharing ministries (HCSMs), which aren’t regulated like health insurance and aren’t required to comply with ACA protections like covering maternity care or pre-existing conditions.
Nvidia extended its winning streak to five days, rising another 1.73% as the AI trade continues to recover.
EchoStar climbed 13.16% after the parent company of Dish TV disclosed that President Trump did in fact prod the FCC to make a deal.
Cyngn soared another 20.07% following a big day of gains after the company that makes self-driving tech for industrial vehicles announced a partnership with Nvidia.
Strong earnings from Nike (more on that later) propelled sporting goods stocks higher today. ONHoldings rose 1.74%, while Dick’s Sporting Goods climbed 3.59%.
Domestic power producers popped on reports that Trump is planning to issue an executive order increasing energy production to meet AI demand. Vistra gained 2.44%, GE Vernova climbed 2.54%, and Vertiv added 2.71%.
What’s down
Coinbase Global ended its winning streak, tumbling 5.77% after GENIUS Act hype propelled the crypto stock skyward all week long. Traders took profits in Circle as well, pushing the stablecoin stock down 15.54%.
Chinese EV maker LiAuto fell 1.93% on its weaker-than-expected deliveries forecast for the second quarter.
Fellow Chinese EV maker Xiaomi stunned markets with reports that it received 240,000 orders for its new SUV within 18 hours of its debut, but shares still sank 4%.
Pony.ai lost 6.31% on a report that Uber is considering helping its founder Travis Kalanick fund his acquisition of the US subsidiary of the Chinese autonomous vehicle company.
Gold miners tumbled while the price of the precious metal fell as investors took a risk-on stance. Newmont lost 4.11%, BarrickMining fell 3.44%, and KinrossGold shed 6.18%.
Today’s trade deal reopens the door for Chinese rare earth imports, bad news for US producers like MPMaterials (down 8.59%) and USA Rare Earth (down 12.14%).
Posted on June 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Accidental Death and Dismemberment
By AI
***
***
What is AD&D insurance?
AD&D insurance combines two types of coverage: an accidental death policy that pays out if you die in an accident, and a dismemberment policy that pays out if you have a serious injury such as losing a limb or becoming paralyzed because of an accident. The beneficiary of your AD&D policy (such as your spouse) collects the money in the case of an accidental death, and you collect it if you suffer one of the injuries outlined in the policy.
Here’s the catch: The death or injury must be the direct result of an accident. So, for example, if you have a heart attack while you’re driving and get into a fatal car crash, your beneficiaries probably won’t receive any money.
***
***
While AD&D insurance can offer financial peace of mind to you and your loved ones in the event of an accident, it won’t pay out if you die from natural causes or a terminal illness — so it’s not a replacement for life insurance. And since it doesn’t cover all injuries or disabilities, it isn’t as comprehensive as disability insurance either.
Be aware that insurers often sell accidental death insurance without dismemberment coverage. These policies pay out only if you die and won’t cover an accident that leaves you seriously injured but alive.
Posted on June 10, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
On May 13th, 2025, the CMS Center for Medicare & Medicaid Innovation (CMMI) introduced a new strategic plan for its models going forward. After ending four payment models early and canceling two not-yet-implemented models in March 2025, the agency had promised to release a new strategy. Nearly two weeks later, CMMI released that strategy, as well as a preliminary evaluation of, and changes to, one of its core payment models.
This Health Capital Topics article will review CMMI’s recent actions and what initial indications these actions provide. (Read more…)
Posted on May 16, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Oak Street Health, headquartered in Chicago and a wholly-owned subsidiary of CVS Health since 2023, has agreed to pay $60 million to resolve allegations that it violated the False Claims Act by paying kickbacks to third-party insurance agents in exchange for recruiting seniors to Oak Street Health’s primary care clinics.
The Anti-Kickback Statute prohibits anyone from offering or paying, directly or indirectly, any remuneration — which includes money or any other thing of value — to induce referrals of patients or to provide recommendations of items or services covered by Medicare, Medicaid and other federally funded programs. Under the Medicare Advantage (MA) Program, also known as Part C, Medicare beneficiaries have the option to obtain their health care through privately-operated insurance plans known as MA plans. Some MA Plans contract with health care providers, including Oak Street Health, to provide their plan members with primary care services.
The United States alleged that, in 2020, Oak Street Health developed a program to increase patient membership called the Client Awareness Program. Under the Program, third-party insurance agents contacted seniors eligible for or enrolled in Medicare Advantage and delivered marketing messages designed to generate interest in Oak Street Health. Agents then referred interested seniors to an Oak Street Health employee via a three-way phone call, otherwise known as a “warm transfer,” and/or an electronic submission.
In exchange, Oak Street Health paid agents typically $200 per beneficiary referred or recommended. These payments incentivized agents to base their referrals and recommendations on the financial motivations of Oak Street Health rather than the best interests of seniors. The settlement resolves allegations that, from September 2020 through December 2022, Oak Street Health knowingly submitted, and caused the submission of, false claims to Medicare arising from kickbacks to agents that violated the Anti-Kickback Statute.
Posted on May 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITION
By Staff Reporters
***
***
Classic: Despite a wide variety of empirical methods and data sources, the demand for health care is consistently found to be price inelastic
Modern: If you are sick, you will not be very price sensitive. There are exceptions to this rule (e.g., elective surgery such as plastic surgery, purchases of eyeglasses) but most studies find that patients are fairly insensitive to changes in health care prices.
Examples: For instance, the RAND Health Insurance Experiment found that the price elasticity of medical expenditures is -0.2.
***
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
An emergency medicine physician is a medical doctor who specializes in the diagnosis, treatment, and management of acute and life-threatening medical conditions that require immediate intervention. These physicians work in hospital emergency departments, urgent care centers, and other acute care settings, where they provide rapid assessment, stabilization, and treatment to patients of all ages with a wide range of medical emergencies.
Emergency medicine physicians are trained to handle diverse medical emergencies, including trauma, cardiac emergencies, respiratory distress, severe infections, neurological emergencies, and obstetric emergencies, among others. They play a vital role in the front line management of medical emergencies, ensuring that patients receive prompt and appropriate care to improve outcomes and save lives.
***
Classic: Emergent Room or Emergency Department care is the provision of immediate medical service offering outpatient care for the treatment of acute and chronic illness and injury. It requires a broad and comprehensive fund of knowledge to provide such care. Excellence in care for patients with complex and or unusual conditions is founded on the close communication and collaboration between the urgent care medicine physician, the specialists and the primary physicians.
Modern: Urgent care does not replace your primary care physician. An urgent care center is a convenient option when someone’s regular physician is on vacation or unable to offer a timely appointment. Or, when illness strikes outside of regular office hours, urgent care offers an alternative to waiting for hours in a hospital Emergency Room.
Examples: Chest pain, bleeding that cannot be stopped and loss of consciousness; etc.
***
***
SOME ER DOCTORS WORK FOR FREE
The new president of emergency medicine for the Alberta Medical Association says Emergency Room physicians already coping with long hours, staff shortages and jammed waiting rooms are also being obligated, in some cases, to work for free. Dr. Warren Thirsk says the government has yet to follow through on a promise to reimburse emergency room doctors for so-called “good faith” payments.
“There’s been lots of excuses, but the bottom line is no one has actually received a penny for those suspended good-faith payments,” Thirsk said in an interview. “On average, every emergency physician in this province is out thousands of dollars for free work.” Good-faith payments reimburse ER doctors when they see patients who don’t have identification and can’t prove an Alberta Health Care Insurance Plan billing number.
Thirsk said the United Conservative government stopped those payments when it ripped up the master agreement with the AMA in early 2020. He said it promised to bring back those payments when the two sides agreed to a new deal in September 2022. But to date that hasn’t happened, he said.
“I’m legally and morally bound to look after you [if] you’re unidentified [as a patient],” said Thirsk, an emergency room doctor at Edmonton’s Royal Alexandra Hospital.
“I’m going to look after you because it’s the right thing to do no matter what the problem is.”
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Some retired people live on a fixed income and many of them live right on the edge of their financial capability. At some time in their life, they may have to make a choice regarding many purchases.
In this case, we will illustrate “choice” using a couple’s purchase of Long-Term-Care Insurance [LTCI]. Of course, economics is the study of choice; wants, needs and scarcity, etc. In our case, if they decide to make the purchase they commit to a lifetime of premium payments. The financial tradeoff is this; if they make the commitment to purchase LTCI, they must give up something else.
EXAMPLE: In order to maintain a monthly premium of $100 ($1,200per year), an elderly patient, retired layman or couple must essentially relegate about $30,000 of financial assets to generate the $100 necessary to make an average premium payment (assumes a 7% rate of return with 4% withdrawal rate) or [4% X $30,000 = $1,200 year]. Thus, if the monthly premium cost is $500 per month, the elder must give up the use of $150,000 of retirement asset just to generate enough cash flow to pay for the LTC insurance.
***
***
The married elder couple has to make the Hobson’s Choice decision among lifestyle (dinners, vacations, gifts to children, prescription drugs, medical care or food and shelter) versus paying an insurance premium to provide for nursing home coverage for a need, which may be very real, but will not occur until sometime in the ambiguous future.
And so, when faced with such a tough economics Hobson’s Medicine Choice, neither of which delivers peace of mind or a respectable solution; many will simply decide that, in either case, they may already end up impoverished. Thus, many will often opt for the better lifestyle now … while they can enjoy it … together.
Cite: Anonymous Health Insurance Agent, Norcross, Georgia
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals.
Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed.
Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Phantom equity is an increasingly popular tool within businesses, particularly startups and private companies, for incentivizing employees without diluting ownership. It allows firms to reward key personnel by linking compensation to the company’s performance, aligning employee interests with those of shareholders.
Basic Mechanisms of Phantom Equity
Phantom equity operates as a contractual agreement offering employees a simulated stake in the business without issuing actual stock. This arrangement appeals to companies aiming to maintain control over their equity structure while providing performance-based incentives. The benefits mimic stock ownership, such as dividends and capital appreciation, without the complexities of transferring actual shares.
The company establishes a phantom equity plan that defines terms such as vesting schedules, performance metrics, and payout conditions. Vesting schedules, often ranging from three to five years, encourage employee retention. Performance metrics may include revenue growth, profit margins, or other financial indicators aligned with strategic goals. Once vested, employees receive cash payments based on the value of the phantom shares, determined by the company’s valuation at payout.
Valuations, often conducted through third-party appraisals or internal financial metrics, directly affect payouts. If the company grows significantly, the value of phantom shares increases, resulting in higher payouts. Conversely, if performance declines, the value of these shares decreases, reducing compensation.
Types of Phantom Equity Plans
Phantom equity plans can be customized to suit a company’s goals, with two primary types being most common: appreciation-only arrangements and full-value arrangements.
Appreciation-Only Arrangements
Appreciation-only arrangements reward employees for the increase in the company’s value over a specified period. Employees are granted phantom shares that reflect the appreciation in the company’s valuation from the grant date to the payout date.
For instance, if phantom shares are initially valued at $10 each and the valuation rises to $15, the employee receives a payout of $5 per share. This structure ties employee rewards to company growth without affecting equity. Companies must rely on precise valuation methods, often adhering to GAAP or IFRS, to ensure fairness and compliance.
Full-Value Arrangements
Full-value arrangements provide payouts equivalent to the full value of phantom shares at vesting or payout. This includes both the initial value and any appreciation.
For example, if phantom shares are initially valued at $10 and later rise to $15, the employee receives $15 per share. While offering greater potential rewards, full-value arrangements require a larger financial commitment from the company. Careful financial planning and adherence to standards like ASC 718, which governs share-based compensation, are essential for managing these plans effectively.
Several years ago a group of highly trusted and deeply experienced financial advisors, insurance service professionals and estate planners noted that far too many of their mature retiring physician clients, using traditional stock brokers, management consultants and financial advisors, seemed to be less successful than those who went it alone. These Do-it-Yourselfers [DIYs] had setbacks and made mistakes, for sure. But, the ME Inc doctors seemed to learn from their mistakes and did not incur the high management and service fees demanded from general or retail one-size-fits-all “advisors.”
In fact, an informal inverse related relationship was noted, and dubbed the “Doctor Effect.” In others words, the more consultants an individual doctor retained; the less well they did in all disciplines of the financial planning and medical practice management, continuum.
Of course, the reason for this discrepancy eluded many of them as Wall Street brokerages and wire-houses flooded the media with messages, infomercials, print, radio, TV, texts, tweets, dinners and internet ads to the contrary. Rather than self-learn the basics, the prevailing sentiment seemed to purse the holy grail of finding the “perfect financial advisor.” This realization confirmed the industry culture which seemed to be:
Bread for the advisor – Crumbs for the client!
And so, Marcinko Associates formed a cadre’ of technology focused and highly educated multi-degreed doctors, nurses, financial advisors, attorneys, accountants, psychologists and educational visionaries who decided there must be a better way for their healthcare colleagues to receive financial planning advice, products and related advisory services within a culture of fiduciary responsibility.
We trust you agree with this specific niche knowledge, and collegial consulting philosophy, as illustrated thru our firm and these two books.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Classic: An arrangement by which a patient requests that their health benefit payments be made directly to a designated person or facility, such as a physician or hospital. It is a legally binding agreement between patient and Insurance company asking them to send your reimbursement checks directly to your doctor.
Modern: To accept assignment means that the provider agrees to accept what ever the insurance company allows or approves as payment in full for the claim. The patient signs paperwork requiring his health insurance provider to pay his physician or hospital directly. EXAMPLES:
CMS: The approved amount, also known as the Medicare-approved amount, is the fee that Medicare sets as how much a provider or supplier should be paid for a particular service or item. Original Medicare calls this “assignment.”
Tardiness: When a medical office accepts an assignment of benefits, the insured patients may have to wait several months for their insurance reimbursement to arrive.
Posted on April 15, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Natural Disaster Insurance
Protecting accumulated assets by insuring them against the wrath of Mother Nature
Most homeowners’ insurance policies do not cover damages arising from floods or earthquakes. If a home, or any other real property like a vacation home or beach condo, is in an area subject to floods or earthquakes, consider the value of purchasing insurance that covers such catastrophes.
Take the time to review your homeowners’ policy, making sure that it will repair or replace your roof if damaged by hail, and will apply in the event of high winds, rather than only in tornadoes. The key to the maintenance of any type of insurance is to anticipate all of the possible calamities, and then to decide whether you can afford to lose the assets exposed to those calamities.
Posted on April 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Ann Miller RN MHA CPHQ CMP™
***
***
Finally … Fiduciary second investing and financial planning opinions right here!
Telephonic or electronic advice for medical professionals that is:
Objective, affordable, medically focused and financially personalized
Rendered by a pre-screened financial consultant for doctors and medical professionals
Offered on a pay-as-you-go basis, by phone or secure e-mail transmission
The iMBA Discussion Forum™ is a physician-to-financial advisor telephone or e-mail portal that connects independent financial professionals to doctors, nurses or healthcare executives desiring affordable and unbiased financial planning advice.
Medical professionals and healthcare executives can now receive direct access to pre-screened iMBA professionals in the areas of Investing, Financial Planning, Asset Allocation, Portfolio Management, Insurance, Mortgage and Lending, Human Resources, Retirement Planning and Employee Benefits. To assist our medical professional and healthcare executive members, we can be contracted with per-minute or per-project fees, and contacted by client phone, email or secure instant messaging.
Posted on March 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
While some medical practitioners and facilities can operate without Professional Liability Insurance coverage, one business related insurance that cannot / should not be avoided is Worker’s Compensation. Employers in all but seven states – so-called “monopolistic” states because they have their own state funds, are under statutory obligation to provide coverage for their employees. Historically, Worker’s Compensation pre-dates Social Security entitlements and well before the emergence of employer sponsored group benefits.
The coverage under worker’s compensation provides for lost income due to on-the-job accidents or work-related disability or death and the amount of benefits vary by state. In some instances, the coverage will reimburse the employee for medical expenses incurred with the accident.
The four general benefits covered under Worker’s Compensation are:
Medical Care – for expenses incurred usually without limitations on amount or period of care.
Disability Income – payable for both total and partial disability and is usually based on 66 2/3 percent of their wage base.
Death Benefits – generally fall into two categories; one a flat amount for “burial” insurance; and two, survivor benefits. Though varying by state, these benefits are similar to the disability payment (a percentage of weekly base wages) but may be capped as to total benefit, such as $50,000 or a period, such as 10 years
Rehabilitation Benefits – includes not only medical rehabilitation, but vocational rehabilitation, vocational counseling, retraining or educational benefits, and job placement
Traditionally, the secondary purpose of Worker’s Compensation was to reduce potential litigation because employees accepting the benefits from a Worker’s Compensation claim generally waived their right to sue their employer.
***
***
However, in our litigious society, this “protective shelter” has been severely tested and is crumbling.
Employers may provide their Worker’s Compensation three ways:
Private commercial insurance
State government funds
Self-insurance
Very few factors drive the premium structure – the occupation of the workers is the single most important determinant of premiums. An office worker may have premiums as low as $.10 per hundred of wages and a coal miner may exceed $50.00 per hundred of wages. Generally speaking, however, Worker’s Compensation premiums for the medical profession or healthcare worker are among the lowest available.
Therefore, for the medical practice, some physicians may consider self-insurance because the weekly benefits are typically below $500, thus making this decision attractive.
Alternatively, because officers and owners can elect not to be covered by Worker’s Compensation, the decision to purchase coverage from a private insurance company may afford inexpensive assurance that the benefits will be conveniently provided, and administered, by a private insurance company for their employees.
Posted on March 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Split-Dollar Life Insurance: An arrangement under which a life insurance policy’s premium, cash values, and death benefit are split between two parties—usually a corporation and a key employee or executive. Under such an arrangement an employer may own the policy and pay the premiums and give a key employee or executive the right to name the recipient of the death benefit.
***
***
Several factors will affect the cost and availability of life insurance, including age, health, and the type and amount of insurance purchased. Life insurance policies have expenses, including mortality and other charges. If a policy is surrendered prematurely, the policy holder also may pay surrender charges and have income tax implications. You should consider determining whether you are insurable before implementing a strategy involving life insurance.
Any guarantees associated with a policy are dependent on the ability of the issuing insurance company to continue making claim payments.
Health actuaries analyze potential risks, profits and trends that will affect their employers, which are often in the health insurance, government health services and medical provider industries. They advise companies on issuing policies to consumers based on risks, calculated premiums and upcoming changes in health-care costs.
It’s common for an actuary to have a bachelor’s degree or higher in actuary studies, mathematics or statistics. Coursework on medical terminology and hierarchy of the medical field is also beneficial. In addition to academic education, certification is also necessary to reach “professional status,” which is required by most employers.
***
***
The professional organization, Society of Actuaries, certifies actuaries in the health and medical field. Their statistical work is commonly done with predictive tables, probability tables and life tables that are created on customized statistical analysis software such as Stata or XLSTAT.
The actuary field as a whole is growing faster than other fields, according to the Bureau of Labor Statistics [BLS]. In 2020, it expanded by 27 percent. The average annual salary for an actuary in 2010 was $87,650. More specifically, in the health insurance field, the salary was slightly higher at $91,000.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
According to Patricia Salber MD [personal communication], there are a number of reasons why direct patient access to laboratory medical results is a good idea:
Between 8 and 26% of abnormal test results, including those suspicious for cancer, are not followed up in a timely manner. Direct access could help reduce the number of times this occurs
Self-management, particularly of chronic illness has known benefits. Just like the QS people, many folks with chronic illness obtain and manage to self-acquired lab results every day via gluco-meters, home pulmonary function tests, blood pressure measurements, and so forth. Direct access to laboratory-acquired data, one could argue is a continuation of that personal responsibility
Patients want to be notified about their results in what they perceive as a timely fashion. In one study, patients who received direct notification of their bone density tests results were more likely to perceive they had timely notification compared to usual care even though there was no measurable effect on actual treatment received after three months
Being more responsible for test results could encourage consumers to try to learn more about the meaning of the test results, conceivably increasing their health literacy.
But, the arguments against direct access discussed include the following:
Patients prefer their physicians contact them directly when they have abnormal test results, although the major studies published in 2005 and 2009, preceded the extraordinary use of the internet to access health information that exists today.
There is concern over whether patients will know what to do when they receive the results – will they make erroneous interpretations or fail to contact their docs? This could be, but the intent of the proposed rule is shared access to the results. We suspect if the rule become law, docs will develop better notification mechanisms so that they reach the patient before the patient directly accesses the results or lab companies will design better lab test notifications with easy-to-understand interpretations or a whole new industry will appear that can provide instantly available individualized lab interpretation…or maybe all three of these would happen and that would be a very good thing.
Unknown impact of dual notification (doctors and patients) of lab test results on physician behavior…would docs simply shift responsibility for initiating follow-up care from themselves to their patients?
Would direct access of life-changing lab tests, such as HIV or malignancy, lead to unnecessary patient anxiety – or worse? (Conversely, is there less anxiety, desperation, or suicidal ideation if the bad news is delivered face to face?
Individuals likely may contact their physicians immediately after getting the lab results asking for a telephonic or face-to-face interpretation … it is not known how this would impact physician workload and/or potential for reimbursement [personal communication, Richard Hudson DO, Atlanta, GA].
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on March 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITION
By Staff Reporters
***
***
1035 Exchange
DEFINITION: A method of exchanging insurance-related assets without triggering a taxable event. Cash-value life insurance policies and annuity contracts are two products that may qualify for a 1035 exchange.
***
A 1035 exchange is a feature in the tax code that permits individuals to transfer funds from an existing life insurance endowment, or annuity policy to a new one without tax consequences.
These transactions are not subject to tax deductions or tax credits but rather tax deferrals, meaning that individuals would only pay taxes on any earnings once they receive money from the policy later.
Without this provision, policyholders would have to close their previous accounts and be subjected to both taxes and surrender charges before they could open a new account.
If you have ever filed a homeowners insurance claim, you know it can feel more like an endurance test than a straightforward process. While insurers are legally required to honor valid claims, they have strong financial incentives to delay, underpay, or deny them whenever possible.
Over the years, I’ve learned this the hard way. The most recent lesson started when a hailstorm hit my home in June 2023. I promptly filed an insurance claim. I also made up a story that leaving someone more qualified than me in charge would free me from a part-time job as a contractor, so I relied on a roofing contractor to handle the whole claim, including the gutter and siding damage. That was my first mistake.
About 15 months later, my roof and gutters were replaced, but the siding repairs and painting remained undone. Every time the insurance company reassigned my claim to a new adjuster, I had to start over. When I called the contractor after a period of inactivity, they said the adjuster had ghosted them, so they’d given up—and I still owed them the full roofing bill.
At that point, I had two choices: pay out of pocket for the unfinished work or escalate. I chose the latter. I filed a complaint with the state insurance division, contacted my agent, reached out to the last adjuster, hired my own painter, and withheld final payment to the contractor. I also made it clear that I was prepared to take legal action if necessary. That was not a bluff.
Within a week, things started moving. Seven days later, the insurance company reinspected my home and sent a check covering all but $3,000 of the painting costs. After nearly two years of delays and excuses, progress finally happened when I took matters into my own hands.
Delay is a common insurer tactic. They’ll repeatedly ask for more documentation, take months to respond, or swap adjusters to force you to restart the process—all in hopes that you’ll give up or accept a lower payout.
Another common tactic is the lowball offer. Insurers often rely on software that underestimates damages or send adjusters unfamiliar with actual repair costs. Accepting their first offer without question can be a costly mistake. It’s wise to get independent repair estimates or even hire a public adjuster who works for you rather than the insurance company.
Insurers also deny claims based on fine print, arguing that damage was pre-existing, caused by poor maintenance, or excluded under some obscure clause. Knowing your policy inside out and keeping pre-loss photos can help you counter these claims.
Another trick? Steering homeowners toward “preferred” contractors who work at discounted rates and may prioritize the insurer’s interests over yours. Getting independent estimates ensures repairs are done properly.
For homeowners stuck in an insurance battle, persistence is key. Withholding final payment until work is complete, filing a complaint with the state insurance division, and even considering small claims court can help push a claim forward. If the dispute is within your state’s small claims limit—often between $10,000 and $25,000—filing may push the insurer to settle.
Assuming my contractor would handle everything was my biggest mistake, and it cost me nearly two years of frustration. Even though progress happened quickly once I took control, my claim isn’t over. I suspect I will be filing legal action in small claims court against the insurance company, contractor, and insurance agent.
If you need to navigate an insurance claim, be persistent and attentive. Keeping records, pushing back on delays, and escalating when necessary can mean the difference between being shortchanged and getting the settlement you deserve.
During the January 2025 J.P. Morgan Healthcare Conference, Teladoc’s executives announced the company has partnered with Amazon Health Services, joining its Health Benefits Connector program. The program was rolled out in January 2024 and connects Amazon customers with virtual care benefits covered by their insurance plan or employer; if eligible, customers are able to apply to join the program(s).
Teladoc is the fifth company to join Amazon’s Health Benefits Connector program (formerly known as Health Conditions Programs), along with digital physical therapy company Hinge Health; chronic condition management company Omada; online therapy and mental health firm Rula; and behavioral healthcare provider Talkspace. (Read more…)
RISK MANAGEMENT, LIABILITY INSURANCE AND ASSET PROTECTION ABBREVIATIONS
[Glossary of Important Acronyms]
Much has been written and much has been opined on the topic of medical risk management, insurance, asset protection and professional liability for physicians and healthcare providers in this textbook; and elsewhere.
But occasionally, we all still get lost in a wide array of abbreviations, acronyms, and initialisms that are constantly changing in this ecosystem.
And so, this glossary serves as a ready reference for those who want to know about these medical risk management definitions in a quick and ready fashion.
Acronyms and Abbreviations
AAASC American Association of Ambulatory Surgery Centers
AAHP American Association of Health Plans
ABN advance beneficiary notice
ABQAUR American Board of Quality Assurance and Utilization Review
ACE acute care episode
ACHCE American College of Health Care Executives
ACS American College of Surgeons
ADA Americans with Disabilities Act
ADC average daily census
ADL activities of daily living
ADT Admission/Discharge/Transfer
AHA American Hospital Association
AHIMA American Health Information Management Association
AHRQ Agency for Healthcare Research and Quality
AI average inventory
AIMR Association for Investment Management and Research
AIR assumed interest rate
ALE annualized loss expectancy
ALF assisted living facility
ALOS average length of stay
AMA American Medical Association
AMBAC AMBAC Indemnity Corporation
AMGA American Medical Group Association
ANSI American National Standards Institute
AP accounts payable
APA American Psychiatric Association
APC ambulatory payment classification
APG ambulatory payment group
APR annual percentage rate
AR accounts receivable
ASA American Society of Appraisers
ASC ambulatory surgery centers; also Accredited Standards Committee
ASHA American Surgical Hospital Association
ASO administrative services only
ASTC ancillary service technical component
ATM asynchronous transfer mode
AVG ambulatory visit group
BANTA best alternative to negotiated agreement
BBA Balanced Budget Act of 1997
BBRA Balanced Budget Refinement Act [1999]
BCP business continuity planning
BEA break-even analysis
BEP break-even point
BIPA Benefits Improvement and Protection Act [2000]
BLS Bureau of Labor Statistics
BPD border protection device
BS balance sheet
BSA Bank Secrecy Act
BVS business valuation standard
CA certificate authority
CAC Carrier Advisory Committee
CAS cost accounting standards
CASB Cost Accounting Standards Board
CC common criteria [for IT Security Evaluation —ISO/IEC 15408]; complication or comorbidity [for MS-DRGs]
CCA certified cost accountant
CCC cash conversion cycle
CCEVS common criteria evaluation and validation scheme
CCHIT Certification Commission for Healthcare Information Technology
CCU critical care unit
CDC Centers for Disease Control and Prevention
CDH consumer-directed healthcare
CDHP consumer-directed healthcare plan
CDPM Clinical Data Project Manager
CDSS clinical decision support system
CEO Chief Executive Officer
CF conversion factor
CFA Chartered Financial Analyst
CFO Chief Financial Officer
CFR Code of Federal Regulations
CHAMP Children’s Health and Medicare Protection Act of 2007
CHAMPUS Civilian Health and Medical Program of the Uniformed Services
CHE Certified Healthcare Executive
CHIPS Center for Healthcare Industry Performance Studies
CIA Corporate Integrity Agreement
CIO Chief Information Officer
CIP Customer Identification Program
CIS computer information systems
CLIA Clinical Laboratory Improvement Act
CLT capitation liability theory
CME continuing medical education
CMI case mix index
CMIO Chief Medical Information Officer
CMIS contribution margin income statement
CMN Certificate of Medical Necessity
CMP Certified Medical Planner ™
CMS Centers for Medicare and Medicaid Services [formerly HCFA]
COD cash on delivery
COGME Council of Graduate Medical Education
COH cash on hand
COLA cost of living allowance
CON Certificate of Need
COO Chief Operating Officer
COSO Committee of Sponsoring Organizations
COTS commercial off-the-shelf
CPHQ Certified Physician in Healthcare Quality
CPIM Certificate in Production and Inventory Management
CPI-U Consumer Price Index—urban
CPM critical (clinical) path method
CPOE computerized physician order entry [system]
CPR computer-based patient record
CPT current procedural terminology
CQI continuous quality improvement
CRL Certification Revocation List
CRM customer relationship management
CRVS California Relative Value Studies
CSO Chief Security Officer
CT scan computed tomography scan [also called CAT scan]
CUSIP Committee on Uniform Security Identification Procedures
Candid CIO: Will Weider, CIO of Ministry Health Care and Affinity Health System, offers his perspectives on administration issues in this blog.
Christina’s Considerations: Christina Thielst is a hospital and healthcare administrator and entrepreneur with a deep desire for continually improving the health of the community being served. This is her blog.
Healing Hospitals — Formerly Ask a Hospital President: F. Nicholas “Nick” Jacobs has more than 20 years experience in hospital management, with an acknowledged reputation for innovation and consumer-centered leadership.
Hospital Impact: Part of the Fierce network of health sites, this site is becoming popular among healthcare administrators for its news updates, tips and opinions on health care matters.
Leading the Way to Medical Excellence: the president of McLeod Health non-profit institutions provides weekly insights into his facilities and health care in general.
Let’s Talk Health Care: Bruce Bullen, Interim Chief Executive Officer at Harvard Pilgrim in Massachusetts, provides and open and ongoing conversation about health care administration.
Life as a Healthcare CIO: Dr. John Halamka records his experiences with infrastructure, applications, policies, management, and governance as he supports 3,000 doctors, 18,000 faculty and about three million patients.
Managed Care Matters: Joe Paduda shares his knowledge on managed care for group health, health policy, health research, and medical news for insurers, employers, and healthcare providers.
More than Medicine: Tom Quinn, president and CEO of Community General Hospital in Syracuse, New York, began his career as a hospital kitchen worker. His perspective on administration reflects his knowledge on how hospitals work from every angle.
Running a Hospital: A CEO of a large Boston hospital shares thoughts on hospitals, medicine and health care issues.
St. Joseph Medical Center: Chief Executive Officer at St. Joseph Medical Center in Missouri, Mr. Kashman, provides personal insight into administrative matters and general topics.
Todd’s Perspective: Todd Linden, president and CEO of Grinnell Regional Medical Center, offers insights into medical administration and guest bloggers provide insight into various departments.
Wachter’s World: This blog focuses on hospitals, hospitalists, quality, safety, policy and much more from Robert M. Wachter, MD, Professor and Associate Chairman of the Department of Medicine at the University of California, San Francisco.
Legal Matters
Drug and Device Law: This blog contains an attorney’s personal views (and those of several other Dechert attorneys) on topics that arise in the defense of pharmaceutical and medical device product liability litigation.
Drug Injury Watch: Learn more about drug injury lawsuits from an attorney who represents patients and their families.
FDA Law Blog: Hyman, Phelps & McNamara, P.C. is the largest dedicated food and drug law firm in the country. Their knowledge about laws and regulations governing drugs, medical devices, foods, dietary supplements, and cosmetics is helpful to anyone interested in these topics.
Health Care Law Blog: Bob Coffield’s expertise lies in helping businesses and health care providers weave through a variety of state and federal health care regulations and assisting them in business transactions.
Health Plan Law: This site contains information about group health plans, claims administration and related ERISA fiduciary issues. This site also contains tutorials.
HealthBlawg: this is David Harlow’s popular health care law blog, offering expert insights and easy-to-understand analysis.
Healthcare Law Blog: Holland & Hart’s healthcare practice provides insight into this arena, including HIPAA, Stark law, the Anti-kickback Statute and more.
HIPAA Blog: Join in on this discussion of medical privacy issues often buried in “political arcana.”
HIPAA, HiTech & HIT: This updated blog brings insight into legal issues, developments and other pertinent information that relates to the creation, use and exchange of electronic health records.
HIT Blawg: This blog is focused on national health information technology legal trends and current news on this topic.
Home Care Law Blog: Learn more about legal and policy issues in the home health care, private duty and hospice industries from Gilliland & Markette LLP.
Med Law Blog: This law blog focuses on topics that range from compliance to contracts and from employee benefits to HIPAA and HIT.
Physician Law: This blog provides and easy way to stay on top of current news, updates and useful tips relating to legal issues that affect physicians and non-institutional providers.
eHealth and Health IT
Chilmark Research: This blog provides perspectives on key IT trends in the healthcare sector.
davidrothman.net: David is the Information Services Specialist at the Community General Hospital Medical Library, but he also provides great ideas for 2.0 tools and tips for healthcare industry professionals on this blog.
e-CareManagement blog: Vince Kuraitis, owner of Better Health Technologies, LLC, has a passion for disease management and care coordination that dates back to 1995.
e-HealthExpert: A non-profit organization provides a free and open forum to support the development of expertise in the field of eHealth, Healthcare Information Systems, and Health IT (Clinical IT).
eHealth: John Sharp is an IT Manager for a major medical center in Northeast Ohio, with a focus on ehealth, personal health records, Web 2.0 technologies, Windows Sharepoint Services and project management.
Found In Cache: If you would prefer a professional’s take on social media matters, Web sites and all things technological, then follow Ed Bennett, a technology expert for a Maryland medical care system.
Future Health IT: A health IT and EPR advocate from the UK provides a format to discuss the future of health care and IT.
Informaticopia: This UK blogger provides eclectic news and views on health informatics and elearning.
MedGadget: Stay ahead of the gadget curve with this site, which offers information about the newest health care gadgets on the market as well as emerging medical technologies.
Neil Versel’s Healthcare IT Blog: A healthcare journalist’s provides his views on the major segment of the industry he covers — and, he provides a ton of links to other sites as well.
Schwartz Healthcare IT Blog: A variety of authors from Schwartz Communications provide insights into ways to use IT effectively within healthcare facilities.
The Health IT Channel: For a different perspective on IT and EHR as well as other health care issues, watch a few videos at this site.
The Healthcare IT Guy: The CEO of Netspective, a Java/.NET consultancy that specializes in healthcare IT with an emphasis on e-health, EMRs, data integration, and legacy modernization, supplies tips and information for physicians and healthcare administration.
ACKNOWLEDGEMENTS: To Mackenzie H. Marcinko PhD of iMBA Inc., Perry D’Alessio CPA CMP™ [Hon] New York, NY; and Daniel B. Moisand CFP®, Principal for Moisand Fitzgerald Tamayo, Melbourne, FL.
Posted on February 18, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITION
By Staff Reporters
***
***
Variable Universal Life Insurance: Permanent life insurance that allows the policyholder to vary the amount and timing of premiums and, by extension, the death benefit. Universal life insurance policies accumulate cash value which grows tax deferred. Within certain limits, policyholders can direct how this cash value will be allocated among sub-accounts offered within the policy.
Several factors will affect the cost and availability of life insurance, including age, health, and the type and amount of insurance purchased. Life insurance policies have expenses, including mortality and other charges. If a policy is surrendered prematurely, the policyholder also may pay surrender charges and have income tax implications. You should consider determining whether you are insurable before implementing a strategy involving life insurance.
Any guarantees associated with a policy are dependent on the ability of the issuing insurance company to continue making claim payments.
Posted on February 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
DEFINITION BAR SLIDES LEFT TO RIGHT
Understanding Insurance Jargon
1. Premiums
When you purchase an insurance policy, you'll be required to make regular payments, known as premiums. These payments are typically made monthly or annually and are the cost of maintaining your insurance coverage.
2. Deductible
Think of a deductible as the money you have to shell out from your own pocket before your insurance kicks in to help cover your expenses. It's like the upfront cost you need to cover before your insurance really starts working for you.For example, if you have a $500 deductible and make a claim for $1,000, you'll need to pay $500, and your insurer will cover the remaining $500.
3. Policyholder
The policyholder is the person who owns an insurance policy. This individual is responsible for paying premiums and making claims under the policy.
4. Coverage Limit
Every insurance policy has a coverage limit, which is the maximum amount your insurer will pay out for a covered claim. It's crucial to understand your policy's limits to ensure you have adequate coverage.
5. Underwriting
Underwriting is the process insurers use to assess the risk of providing coverage to an individual or entity. It involves evaluating factors such as age, health, and driving record to determine premium rates and eligibility.
Types of Insurance
6. Auto Insurance
Auto insurance provides financial protection in case of accidents, theft, or damage to your vehicle. It's a legal requirement in many places and typically includes liability, collision, and comprehensive coverage.
7. Health Insurance
Health insurance covers medical expenses, including doctor visits, hospital stays, and prescription medications. It can be provided by employers or purchased individually.
8. Homeowners Insurance
Homeowners insurance is like a safety net for your home and stuff. It steps in to help if your place or belongings get damaged or stolen. Plus, it's got your back with liability coverage in case someone gets hurt while on your property.
9. Life Insurance
Life insurance pays out a death benefit to beneficiaries when the policyholder passes away. It can provide financial security to loved ones and cover funeral expenses.
10. Liability Insurance
Liability insurance covers you in case you're responsible for injuring someone or damaging their property. It's often included in auto and homeowners insurance policies.
Navigating Insurance Policies
11. Exclusions
Exclusions are specific events or circumstances that your insurance policy doesn't cover. It's essential to review these carefully to understand what situations won't be reimbursed.
12. Riders
Riders are add-ons to insurance policies that provide additional coverage for specific situations. For example, you can add a rider to your homeowners policy to cover expensive jewelry.
13. Claim
A claim is a formal request to your insurance company for coverage or reimbursement for a loss or damage. It's essential to follow the claims process outlined in your policy.
14. Grace Period
The grace period is the amount of time you have to pay your premium after the due date without your coverage lapsing. Be aware of your policy's grace period to avoid a lapse in coverage.
15. No-Claims Discount
Many insurance companies offer a no-claims discount to policyholders who haven't filed any claims within a specified period. This can lead to lower premiums over time.
Specialized Insurance Terms
16. Subrogation
Subrogation is the process by which an insurance company seeks reimbursement from a third party for a claim it has already paid out. This often occurs in auto accidents when your insurer goes after the at-fault driver's insurance company.
17. Actuary
An actuary is a professional who uses mathematics and statistics to assess risk and set premium rates for insurance policies. They play a crucial role in the insurance industry's financial stability.
18. Adjuster
An insurance adjuster is responsible for investigating claims, evaluating damage, and determining how much the insurance company should pay. They work to ensure fair settlements for policyholders.
19. Premium Credit
Premium credit is a discount offered by insurers to policyholders who meet specific criteria, such as having a good driving record or installing safety features in their home.
20. Salvage Value
When an insured item is damaged or totaled, it may still have some value. Salvage value refers to the amount the insurer can recover by selling the damaged item.
Protecting Your Financial Future
21. Risk Management
Effective risk management involves identifying potential risks and taking steps to minimize or mitigate them. Insurance is one tool in your risk management toolkit.
22. Beneficiary
A beneficiary is the person or entity designated to receive the proceeds of a life insurance policy when the policyholder passes away. It's essential to keep this information up to date.
23. Policy Term
The policy term is the duration for which your insurance policy is valid. It's crucial to renew your policy before it expires to maintain coverage.
24. Umbrella Policy
An umbrella policy provides additional liability coverage beyond the limits of your primary insurance policies. It can protect your assets in the event of a costly lawsuit.
25. Coinsurance
Coinsurance is the percentage of costs that you and your insurance company share after you've met your deductible. It's often seen in health insurance policies.
Insurance in Practice
26. Premium Increase
Your insurance premium may increase due to factors such as claims history, changes in coverage, or external economic conditions. It's essential to shop around for the best rates.
27. Depreciation
Depreciation is the decrease in the value of an asset over time. Insurance policies may account for depreciation when settling claims for damaged property.
28. Reinstatement
If your insurance policy lapses due to non-payment, you may have the option to reinstate it by paying any outstanding premiums and fees.
29. Excess
Excess, also known as a deductible, is the portion of a claim that you're responsible for paying. It's designed to prevent small, frequent claims.
30. Pre-Existing Condition
In health insurance, a pre-existing condition is a medical condition you had before obtaining coverage. Within the framework of the Affordable Care Act, insurance providers are prohibited from refusing coverage or imposing elevated premiums due to pre-existing medical conditions.
Insurance Regulations
31. State Insurance Department
Each state in the United States has a department or commission responsible for regulating insurance within its borders. They oversee insurers' operations and protect consumers.
32. Consumer Reports
Consumer reports provide information on insurance companies' financial strength, customer satisfaction, and claims-handling. They can help you choose a reputable insurer.
33. Guaranteed Renewal
Guaranteed renewal is a provision in some insurance policies that ensures the insurer cannot refuse to renew your policy as long as you pay your premiums.
34. Non-Cancelable Policy
A non-cancelable policy is one that the insurer cannot cancel or change the terms of as long as you pay your premiums. This provides certainty in coverage.
35. Market Conduct Examination
Insurance regulators conduct market conduct examinations to assess insurers' business practices and ensure they comply with laws and regulations.
Insurance for Businesses
36. Business Interruption Insurance
Business interruption insurance provides coverage for lost income and expenses when a covered event, such as a fire or natural disaster, forces your business to close temporarily.
37. Workers’ Compensation
Workers' compensation insurance covers medical expenses and lost wages for employees who are injured on the job. It's typically required by law for businesses with employees.
38. Professional Liability Insurance
Professional liability insurance, often called errors and omissions insurance, protects professionals from liability claims resulting from errors or negligence in their work.
39. Business Owner’s Policy (BOP)
A business owner's policy bundles essential coverages, such as property and liability insurance, into a single policy designed for small businesses. It's a cost-effective option.
40. D&O Insurance
Directors and officers (D&O) insurance protects the personal assets of company leaders in case they are sued for alleged wrongful acts while managing the business.
Advanced Insurance Concepts
41. Aggregate Limit
The aggregate limit is the maximum amount an insurance policy will pay out during a policy term, regardless of the number of claims made.
42. Risk Pooling
Insurance works on the principle of risk pooling, where policyholders collectively share the financial burden of covered losses.
43. Loss Ratio
The loss ratio is a measure of an insurance company's claims payouts compared to its earned premiums. A high loss ratio may indicate financial instability.
44. Surplus Lines Insurance
Surplus lines insurance covers risks that standard insurers won't or can't cover. It's often used for unique or high-risk situations.
45. Rescission
Rescission is the cancellation of an insurance policy retroactively, often due to misrepresentation or fraud on the policyholder's part.
Future of Insurance
46. Insurtech
Insurtech refers to the use of technology, such as artificial intelligence and data analytics, to streamline and improve the insurance industry's processes.
47. Telematics
Telematics devices track driving behavior and can lead to personalized auto insurance rates based on individual habits.
48. Microinsurance
Microinsurance provides affordable coverage to low-income individuals and communities, helping them mitigate risks and protect their assets.
49. Blockchain in Insurance
Blockchain technology can enhance transparency and security in insurance by creating immutable records of policies and claims.
50. Climate Change and Insurance
Climate change poses significant challenges to the insurance industry as it leads to more frequent and severe weather events. Insurers must adapt to these changing risk landscapes.
Insurance is a complex field with a language of its own, but understanding these 50 common insurance terms can help you navigate the world of insurance with confidence. Whether you're looking for auto, health, home, or any other type of insurance, being informed about these terms and concepts is essential to making informed decisions about your coverage.
Posted on February 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Blue Cross Blue Shield will soon begin paying out $2.67 billion to customers follow a years-long lawsuit alleging that the health insurance giant broke antitrust laws. The litigation began in 2013, when a class-action lawsuit was filed against more than 35 Blue Cross Blue Shield health insurance plans. The lawsuit claims the company broke antitrust laws by limiting market competition, resulting in increased premiums and reduced options for customers.
US stocks closed mixed on Tuesday as investors assessed more tariff policy shifts from President Donald Trump and looked ahead to upcoming inflation data.
Traders also digested the start of Federal Chair Jerome Powell’s two-day testimony in Congress. In his opening remarks, Powell told lawmakers the Fed is not in a rush to adjust interest rates and reiterated the central bank’s stance of not commenting on trade policy.
The Dow Jones Industrial Average (^DJI) edged around 0.3% higher, while the benchmark S&P 500 (^GSPC) closed just above the flatline. The tech-heavy NASDAQ Composite (^IXIC) pulled back about 0.4%.
Posted on February 7, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Permanent Life Insurance: A class of life insurance policies that do not expire—as long as premiums are kept current—and which combine a death benefit with a savings component. This savings portion can accumulate a cash value against which the policy owner may be able to borrow funds.
Several factors will affect the cost and availability of life insurance, including age, health and the type and amount of insurance purchased. Life insurance policies have expenses, including mortality and other charges. If a policy is surrendered prematurely, the policyholder also may pay surrender charges and have income tax implications. So, you should consider determining whether you are insurable before implementing a strategy involving life insurance.
Finally, any guarantees associated with a policy are dependent on the ability of the issuing insurance company to continue making claim payments.
Posted on February 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Term Insurance: Life insurance that provides coverage for a specific period. If the policyholder dies during that time, his or her beneficiaries receive the benefit from the policy. If the policyholder outlives the term of the policy, it is no longer in effect. Several factors will affect the cost and availability of life insurance, including age, health, and the type and amount of insurance purchased.
Life insurance policies have expenses, including mortality and other charges. If a policy is surrendered prematurely, the policyholder also may pay surrender charges and have income tax implications.
And, you should consider determining whether you are insurable before implementing a strategy involving life insurance. Any guarantees associated with a policy are dependent on the ability of the issuing insurance company to continue making claim payments.
Posted on February 1, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
US stocks lost ground on Friday after the White House said tariffs against Mexico, Canada, and China will take effect on Saturday, reigniting fears of a coming trade war with the nation’s closest trading partners. White House Press Secretary Karoline Leavitt said the president would impose 25% tariffs on goods from Mexico and Canada, as well as a 10% tariff on goods from China.
All three major gauges fell into the red Friday. The S&P 500 (^GSPC) lost 0.5% at the closing bell, while the Dow Jones Industrial Average (^DJI) shed 0.8%. The tech-heavy NASDAQ Composite (^IXIC) gave up 0.3%, reversing earlier gains.
The dramatic tariff news pushed aside more optimistic updates from earlier in the day, which had buoyed stocks. Solid earnings from Apple (AAPL) and an inflation reading that matched expectations lifted market sentiment for much of the day.
Finally, the S&P and the Nasdaq posted losses for the week of 1% and 1.6%, respectively. The Dow, meanwhile, recorded a weekly gain of 0.3%.
Posted on January 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Stocks ended firmly higher on Tuesday, with the S&P 500 rising 0.88% and reclaiming the 6,000 point mark amid a pullback in Treasury yields and optimism over Donald Trump’s focus on deregulation, focused tariff strategies and the prospect of solid corporate earnings into the fourth quarter reporting season.
Tech stocks are likely to pace early gains in the Wednesday session, however, following the unveiling of a new AI joint venture called ‘Stargate’ that will include an initial $100 billion investment from SoftBank, Oracle Corp. (ORCL) and OpenAI.
Executive Order 14009, titled “Strengthening Medicaid and the Affordable Care Act,” includes several key components designed to increase access to affordable health care and reduce the number of uninsured Americans:
Reversal of Trump administration policies: The order sought to undo measures that limited ACA provisions or made healthcare less accessible.
Longer enrollment periods: The order encouraged states to lengthen enrollment periods and provided additional federal support. As a result, many states extended their enrollment windows to ensure broader access to affordable healthcare.
Restoration of pre-existing condition protections: Reaffirmed protections for individuals with pre-existing conditions and reinforced nondiscrimination policies in healthcare.
Immediate review of agency actions: The order directed various executive departments and agencies to review existing regulations, orders, and policies to ensure they align with the goal of strengthening Medicaid and the ACA.
xecutive Order 14070, titled “Continuing To Strengthen Americans’ Access to Affordable, Quality Health Coverage,” aimed to maintain and enhance Medicaid and the ACA. Key components included:
Enhanced marketplace subsidies: The order highlights the positive impact of the American Rescue Plan Act on access to coverage, including enhanced marketplace subsidies.
Extended postpartum Medicaid coverage: It provides options for states to extend postpartum Medicaid coverage.
New incentives for Medicaid expansion: The order includes new incentives for states to expand their Medicaid programs.
Posted on January 16, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The U.S. Department of Labor reported a 0.4% increase in the monthly CPI after seasonal adjustment, overshooting the forecast of 0.3% and the previous value of 0.3%. On an annual basis, inflation climbed to 2.9%, up from 2.7% in November, the highest rate since July 2024.
US stocks ripped higher on Wednesday as high hopes for bank earnings paid off and a crucial consumer inflation update showed key prices increased less than expected in December.
The benchmark S&P 500 (^GSPC) popped more than 1.8%, while the Dow Jones Industrial Average (^DJI) rose more than 1.6%, or over 700 points. Meanwhile, the tech-heavy NASDAQ Composite (^IXIC) soared 2.5%.
Stocks took a leg higher after the Consumer Price Index (CPI) showed progress toward the Fed’s 2% inflation target in December. Prices climbed 0.2% month-on-month on a “core” basis, which strips out the more volatile costs of food and gas, an easing from November’s 0.3% gain. Over last year, core CPI rose 3.2%.
Capital One is being sued by the US government’s consumer watchdog agency for “cheating millions of consumers” and not paying more than $2 billion in interest to holders of its high-interest savings accounts.
As of January 1st 2025, beneficiaries enrolled in Part D prescription drug plans will have their out-of-pocket spending capped at $2,000 for the year. This new policy was part of President Joe Biden’s 2022 Inflation Reduction Act (IRA), which included other drug pricing measures such as capping the cost of insulin at $35 per month for seniors.
But only a small share of Medicare enrollees will benefit from the cap, according to an analysis from nonprofit organization AARP’s Public Policy Institute, as most don’t spend more than $2,000 annually on their medications after hitting their deductible (which is up to $590 for standard plans in 2025). Beneficiaries spent an average of $400 to $500 per year as of 2022, the Hill reported, citing data from the US Department of Health and Human Services (HHS).
Posted on January 7, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
US stocks largely rose on Monday as chip names popped and investors awaited the release of key monthly jobs data later this week.
The S&P 500 (^GSPC) was up about 0.5%, while the Dow Jones Industrial Average (^DJI) fell about 0.1% after being higher for most of the session. The tech-heavy NASDAQ Composite (^IXIC) led the gains, adding about 1.2%, after a tech-led rally on Friday.
Posted on December 28, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
US stocks closed the holiday week on a downbeat note as Wall Street slogged to the finish of a largely triumphant year.
The S&P 500 (^GSPC) lost 1.1%, while the tech-heavy NASDAQ Composite (^IXIC) shed 1.5% Friday at the close. The Dow Jones Industrial Average (^DJI) gave up 0.8%. Meanwhile, the 10-year Treasury yield (^TNX) hovered near seven-month highs around 4.6%.
After stacking impressive gains this year, some of the biggest names in tech lost ground as investors took profits, rebalance portfolios, or reassessed their lofty valuations. Tesla (TSLA) lost 5%. Nvidia (NVDA) gave up c2%, while Amazon (AMZN) decreased by 1%.
Wall Street has just three trading days remaining in a 2024 full of big gains, but markets have been unable to mount a “Santa Claus” rally into the end of the year.
Achieving your financial, wealth and medical practice management goals is important, but handling everything on your own can be overwhelming. That’s where we come in. At D. E. Marcinko & Associates, our team of dual degree experienced physician advisors and medical consultants is here to guide you every step of the way. We believe in providing unbiased, high-quality financial and business advice.
For example, we offer a one-time written financial plan with oral evaluation for a flat fee with no ongoing sales or assets under management fees or commissions. Together, we can create a personalized financial plan tailored to your unique goals, empowering you to make confident, informed decisions as you navigate your financial future.
Other Services Include:
Estate Planning We have a network of qualified legal professionals that we can refer you to for state specific estate planning needs.
Tax Strategy We can work alongside your CPA for tax planning purposes. If needed, we can refer you to a qualified tax professional.
Investment Analysis If you have investments, we review your accounts to make sure they are aligned with your long-term goals.
401-k Allocations We evaluate your 401(k) allocations and provide recommendations that align with your goals.
Education Savings We help you explore the various ways to plan and save for education expenses.
Insurance & Risk Management We assess your insurance coverage to ensure it adequately protects you against potential risks; as well as evaluate and provide expert litigation witnesses, as needed.
Medical Practice Management We evaluate your current or potential medical practice to determine value and/or private equity offers or physician practice management formats [PPMC] for new, mid-career or retiring physicians, nurses and dentists.
D. E. Marcinko & Associates is unique and fully committed to all phases of a medical professionals personal and business life cycle. We are at your service 24/7: Email MarcinkoAdvisors@outlook.com
Posted on December 9, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
U.S. stocks closed mostly higher Friday, with the S&P 500 and NASDAQ Composite each notching fresh record peaks after the latest employment report showed jobs growth bounced back in November. The S&P 500 rose 15.16 points, or 0.2%, to end at 6,090.27. The NASDAQ climbed 159.05 points, or 0.8%, to close at 19,859.77. The Dow Jones Industrial Average fell 123.19 points, or 0.3%, to end at 44,642.52.