By A.I. and Dr. David Edward Marcinko MBA MEd CMP™
SPONSOR: http://www.CertifiedMedicalPlanner.org
***

***
Business Model Defined
Doctors and dentists earn money by treating patients. CPAs and Attorneys have clients, and retail stores buy items low and sell them at higher prices. This is called a business model.
More formally, a business model identifies the products or services the business plans to sell, the target market, and any anticipated expenses, in order to outline how to generate a profit. Business models are important for both new and established businesses. They help companies attract investment, recruit talent, and motivate management and staff.
Businesses should regularly update their business model, or they’ll fail to anticipate trends and challenges ahead. Business models also help investors to evaluate companies that interest them and employees to understand the future of a company they may aspire to join.
***
The Business Model of Pharmacy Benefits Managers
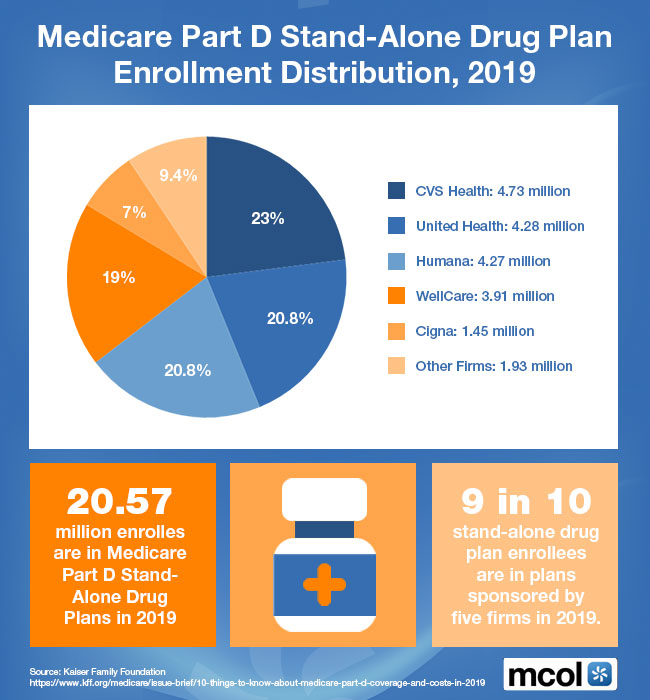
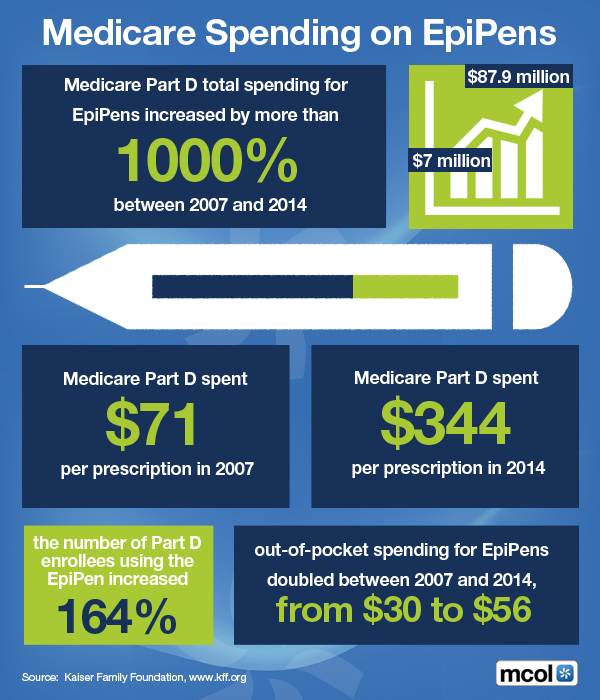
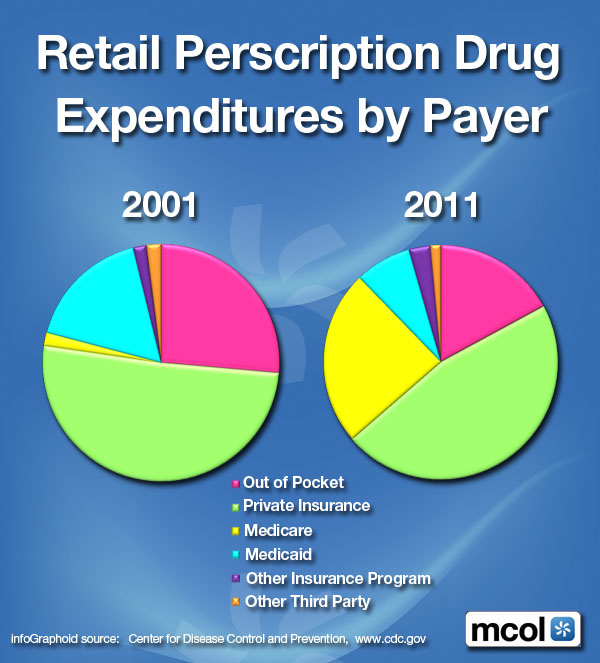
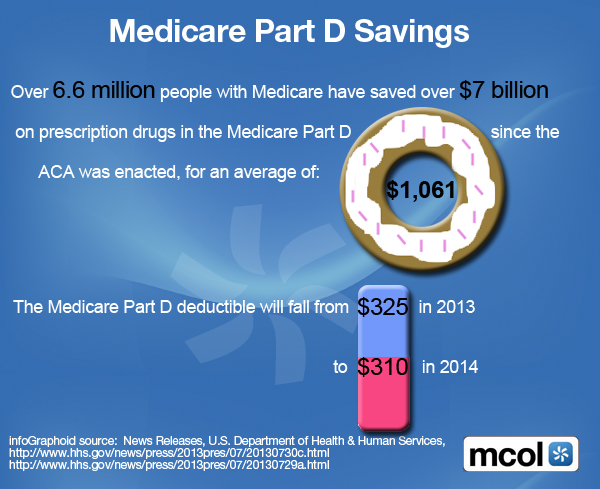
In the United States, health insurance providers often hire a third party to handle price negotiations, insurance claims, and distribution of prescription drugs. Providers that use such pharmacy benefit managers include commercial health plans, self-insured employer plans, Medicare Part D [drug] plans, the Federal Employees Health Benefits Program, and state government employee plans. PBMs are designed to aggregate the collective buying power of en-rollees through their client health plans, enabling plan sponsors and individuals to obtain lower prices for their prescription drugs. PBMs negotiate price discounts from retail pharmacies, rebates from pharmaceutical manufacturers, and mail-service pharmacies which home-deliver prescriptions without consulting face-to-face with a pharmacist.
PBMs DEFINED: https://medicalexecutivepost.com/2019/01/18/on-pbms-pharmacy-benefits-management/
Pharmacy benefit management companies can make revenue in several ways.
First, they collect administrative and service fees from the original insurance plan.
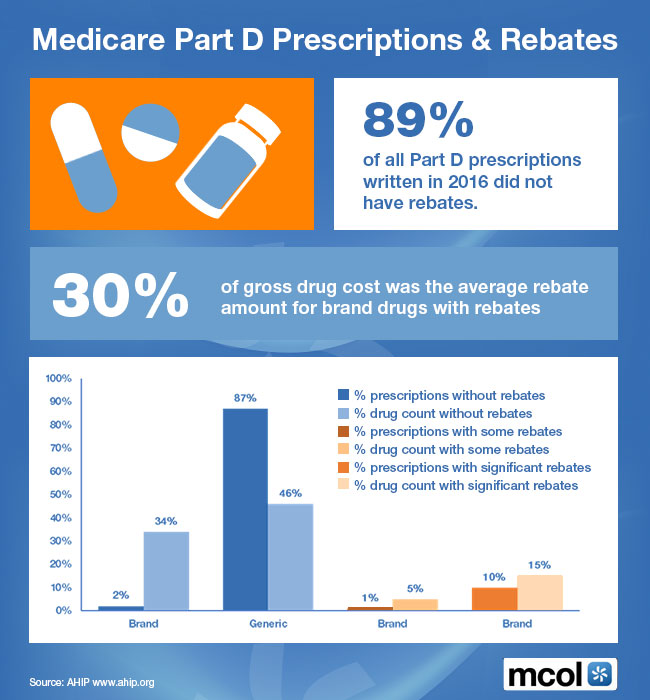
Then, they can also collect rebates from the manufacturer.
Traditional PBMs do not disclose the negotiated net price of the prescription drugs, allowing them to resell drugs at a public list price (also known as a sticker price), which is higher than the net price they negotiate with the manufacturer. This practice is known as “spread pricing”. The industry argues that savings are trade secrets. Pharmacies and insurance companies are often prohibited by PBMs from discussing costs and reimbursements. This leads to lack of transparency.
***
***
Therefore, states are often unaware of how much money they lose due to spread pricing, and the extent to which drug rebates are passed on to en-rollees of Medicare plans. In response, states like Ohio, West Virginia, and Louisiana have taken action to regulate PBMs within their Medicaid programs.
For instance, they have created new contracts that require all discounts and rebates to be reported to the states. In return, Medicaid pays PBMs a flat administrative fee.
PBM PODCAST: https://medicalexecutivepost.com/2023/08/26/podcast-cvs-replaces-its-pbm/
COMMENTS APPRECIATED
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR- http://www.MarcinkoAssociates.com
Like and Subscribe
***
***
Share this:

Filed under: Accounting, Ask a Doctor, business, CMP Program, curated experts,, Drugs and Pharma, finance, Funding Basics, Health Economics, Healthcare Finance, Managed Care, Videos | Tagged: business modelk, CMP, CMP pricing, CMP Program, david marcinko, drug plans, drug rebates, Drugs, health, Health Insurance, healthcare, insurance, medicare, Medicare Part D, PBMs, pharmacy benefits manager, retail pharmacies, spread pricing | Leave a comment »