Dr. David Edward Marcinko; MBA MEd CMP
SPONSOR: http://www.CertifiedMedicalPlanner.org
***

***
Risk‑based medical payment models have become one of the most significant shifts in modern health‑care financing. They move providers away from the traditional fee‑for‑service structure, where every test, visit, or procedure generates a separate payment, and toward arrangements that reward value, outcomes, and cost‑conscious care. This shift reflects a broader recognition that paying for volume alone can unintentionally encourage overuse, fragmentation, and rising costs. Risk‑based models attempt to realign incentives so that providers are financially accountable for the quality and efficiency of the care they deliver.
At the core of these models is the idea of financial risk transfer. Instead of insurers or government programs bearing the full cost of patient care, providers accept some degree of responsibility for spending that exceeds predetermined benchmarks. The level of risk can vary widely. Upside‑only arrangements allow providers to share in savings if they keep costs below expectations, while downside risk requires them to repay losses if spending surpasses targets. Full‑risk or global‑capitation models go even further, giving providers a fixed per‑patient payment to cover all necessary services. The more risk a provider assumes, the greater the potential reward—but also the greater the potential financial exposure.
***
***
One of the most widely used risk‑based models is the accountable care organization, or ACO. In an ACO, groups of physicians, hospitals, and other clinicians coordinate care for a defined population. They are measured on quality metrics such as preventive care, chronic disease management, and patient experience. If they meet quality standards while keeping total spending below a benchmark, they share in the savings. If they take on two‑sided risk, they may also owe money back when costs exceed expectations. The structure encourages collaboration, data sharing, and proactive management of high‑risk patients, all of which are difficult to achieve in a purely fee‑for‑service environment.
Bundled payments represent another important risk‑based approach. Instead of paying separately for each component of a treatment episode, such as a surgery and its follow‑up care, a bundled payment provides a single, predetermined amount for the entire episode. Providers must work together to deliver care efficiently within that budget. If they can do so while maintaining quality, they keep the difference as savings. If complications or inefficiencies drive costs above the bundle price, they absorb the loss. Bundled payments are particularly effective for procedures with predictable care pathways, such as joint replacements or cardiac interventions, and they encourage standardization and reduction of unnecessary variation.
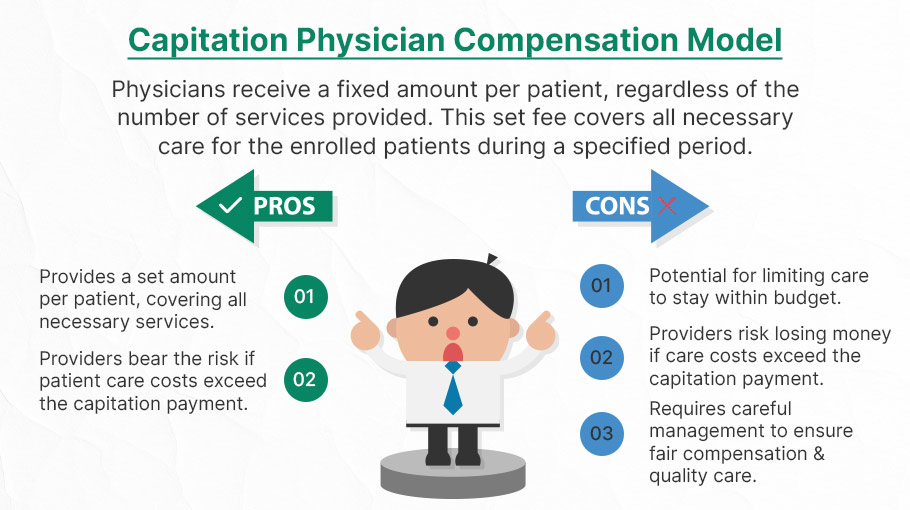
Capitation, one of the oldest risk‑based models, assigns providers a fixed per‑member, per‑month payment to cover all or most services. This model creates strong incentives for preventive care, early intervention, and careful resource management. When implemented well, capitation can support integrated care delivery and long‑term population health strategies. However, it also requires robust infrastructure, accurate risk adjustment, and safeguards to ensure that cost control does not come at the expense of necessary care. Providers must be able to manage complex patients effectively, and payment rates must reflect the true needs of the population.
Risk adjustment is a critical component across all risk‑based models. Without it, providers who care for sicker or more socially complex patients could be unfairly penalized. Risk adjustment uses demographic and clinical data to estimate expected costs for each patient, ensuring that benchmarks and payments reflect the underlying health status of the population. Accurate risk adjustment protects against adverse selection and supports fairness, but it also requires sophisticated data systems and careful oversight to prevent gaming or upcoding.
Despite their promise, risk‑based payment models face challenges. Providers must invest in care‑management teams, data analytics, and interoperable technology to succeed. Smaller practices may struggle with the administrative and financial demands of taking on risk. Patients may also experience confusion if networks narrow or if care pathways become more structured. Policymakers and payers must balance incentives for efficiency with protections that ensure access and quality.
***
***
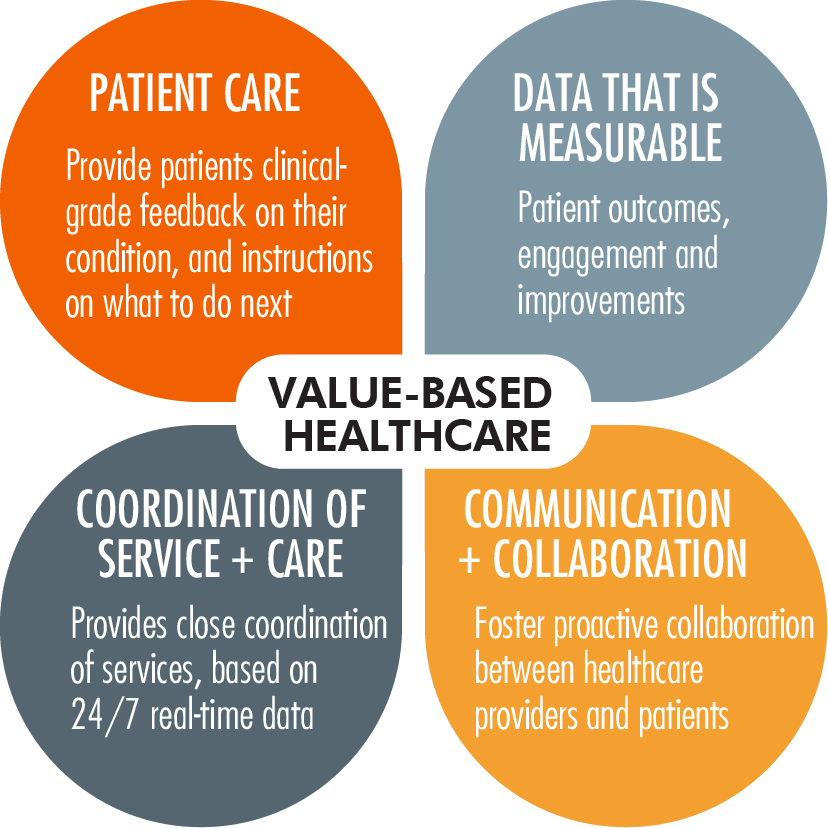
Even with these complexities, risk‑based models continue to expand because they offer a path toward a more sustainable and patient‑centered health‑care system. By rewarding outcomes rather than volume, they encourage providers to focus on prevention, coordination, and long‑term health. They also create opportunities for innovation in care delivery, from telehealth to home‑based services to integrated behavioral health. As health‑care costs continue to rise, risk‑based payment models represent a strategic attempt to align financial incentives with the goals of better care, healthier populations, and more efficient use of resources.
COMMENTS APPRECIATED
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR- http://www.MarcinkoAssociates.com
Like, Refer and Subscribe
***
***
Share this:

Filed under: Accounting, Ask a Doctor, Career Development, CMP Program, finance, Financial Planning, Funding Basics, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Investing, Touring with Marcinko | Tagged: ACAO, capitation, CMP, david marcinko, financial risk, healthcare financing, Risk‑Based Medical Payment Models | Leave a comment »