BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] E-mail: MarcinkoAdvisors1738@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Did you know that most experts recommend against naming a practice with your own name because it limits future growth and you may lose the benefits that a more descriptive name would bring?
Your business name will likely be incorporated using your practice’s name, although larger (multi-specialty group) practices may use a more general name for the entire enterprise; and then having multiple “dba’s” (”Doing Business As”) for the individual practices under the umbrella. It is important to discuss these options with an attorney if you believe this arrangement has advantage; others find it confusing.
Usually, your medical specialty can be used as a base-name, and then some descriptor to differentiate it from local competing practices. Selecting a name like “The Allegiance Partners” does not indicate that medicine is your service. On the other hand, naming your practice “Podiatry Associates of Your Town” won’t be helpful to patients looking for you in the yellow pages, health insurance provider network list, or internet search engines, and finding your practice listed just before “Your Town Podiatry Partners”. It is therefore good to be cognizant of your competitors’ names when choosing your own. And, you should select a name that will hopefully grow with you into a larger enterprise.
For example, are you a solo doctor, but are pretty sure you’ll take on one or more partners in the future? Then besides not naming your practice after yourself, you may choose to add “Group” or “Partners” to your name initially even if you’re the only doctor. Is there any possibility you’ll open a second office in another town? Naming your medical practice something like the ”Apple Street Internal Medicine Group” may not make sense when your second office is opened on Main Street in a nearby city, in a few years.
Order Forms and Practice Stationary
Orders forms, invoices, purchase and estimate forms, business cards, envelopes, stationary and specialty labels can all be personalized for your medical practice name, script, colors and logo. Often, local or regional printers are the most cost effective and you support another entrepreneur, as well.
The Physician Executive Summary is always included at the beginning of a formal business plan and represents a brief synopsis of the medical prarctice entire plan. Its appearance, grammar and style should be sharp and crisp as it represents an enticement for the reader to maintain interest and contribute intelligent or economic input into the new venture.
It should contain information about the practice, advertising and marketing opportunities, physician management, proposed financing with four Pro Forma financial statements, business operations and exit strategy. This last point, while unpleasant is often overlooked by naive practitioners. Business experts however, look favorably upon an escape plan and view it as the mark of mature professional that realizes the possibility of success as well as failure.
****
***
Ultimately, the plan must explain to potential investors how you will make the practice profitable and produce the required Return on Investment (ROI) for them. It must describe medical services, patient acceptance and benefits, provider qualifications and accomplishments, the amount of capital required, market size, potential practice growth rate, and market niche.
Additional information may include office location, proximity to labor, transportation, license requirements, business entity status, proprietary technology and potential working agreements with various insurance, managed care, ACA and HMO plans. If all of the above seems bewildering to the uninitiated, you are correct.
Remember however, that if you do not have, or can’t borrow the funds to begin a private practice, you will just have to become an employed practitioner until you can. It is therefore imperative to start off on the right foot, with a sound business plan, as you begin your medical career.
Recruitment has become a refined art in recent years as practices and physicians themselves grow increasingly savvy about the finer points of marketing positions and securing employment. It’s more competitive than ever, too. Many organizations are going after the same physicians. Add to that a shortage of doctors in key specialties and certain geographical areas and the pressure becomes that much more intense. Moreover, the aging of the physician workforce, their increased dissatisfaction with managed care, and changes in doctors’ work expectations (they want more free time) have affected the demand and supply.
Additionally, both practicing physicians and residents fresh out of training have become more discerning and skillful in managing the search process. Candidates have learned to be selective based on how they’re treated on the phone, how they’re treated in person during site visits, or how smoothly the negotiations go. One small bump in the road and they could choose to go elsewhere. In truth, they look to rule organizations out, not in.
Even the smallest of practices must have an effective recruitment plan because they compete directly with the big guys — larger practices and hospitals that have polished their efforts and perfected their processes.
Facts about Physician Recruiters and Executive Search Firms
1) If you are job hunting, you should send your resume to recruiters
Different recruiters know about different positions. They do not usually know about the same ones. This is particularly true with retained firms. By sending your resume out widely, you will be placed in many different confidential databases and be alerted of many different positions. If you send your resume to only a few, it may be that none you send to will be working with positions which are suited for you. Throw your net widely.
If you change jobs, it is also wise to send follow-up letters to the recruiters and alert them of your new career move. Many search firms follow people throughout their careers and enjoy being kept up-to-date. It is a good idea to have your resume formatted in plain text so you can copy and paste it into email messages when requested to do so. Then, follow up with a nicely formatted copy on paper by postal mail.
Some estimate that only 1% to 3% of all resumes sent will result in actual job interviews. So, if you only send 50 resumes, you may only have less than 2 interviews, if that many. Send your resume to as many recruiters as you can. It is worth the postage or email time. Generally, recruiters will not share your resume with any employer or give your name to anyone else without obtaining your specific permission to do so. The recruiter will call first, talk to you about a particular position and then ask your permission to share your resume with that employer.
2) Your resume will be kept strictly confidential by the executive search firm.
It is safe to submit your resume to a search firm and not worry that the search firm will let it leak out that you are job hunting. Recruiters will call you each and every time they wish to present you to an employer in order to gain your permission. Only after they have gained your permission will they submit your name or resume to the identified employer. The wonderful aspect of working with search firms is that you can manage your career and your job search in confidence and privacy.
3) Fees are always paid by the employer, not the job candidate.
Recruiters and search firms work for the employer or hiring entity. The employer pays them a fee for locating the right physician for the job opening. This is important to remember, in that when you interact with executive recruiters, you are essentially interacting with an agent or representative of the employer. Recruiters are more loyal to employers than they are to job candidates because they work for the employer. This should not present a problem, but, should cause you to develop your relationship with the recruiter with the same integrity and professionalism that you would with the employer.
Recruiters are paid fees in one of two ways – retainer fees or contingency fees. This is an important distinction and will affect your process with both the employer and the recruiter. Some employers prefer working with contingency firms and some with retained firms. Both are respected by employers and useful in your job search, but, the two types of firms will not be handling the same positions with the same employers simultaneously.
A “retained” recruiter has entered an exclusive contract with an employer to fill a particular position. The retained recruiter, then, is likely to advertise a position, sharing the specifics of the position, location and employer openly. The retained firm feels a great obligation to fulfill the contract by finding the best person for the job.
A “contingency recruiter” on the other hand, usually does not have an exclusive relationship with the employer, and is only paid a fee if the job search is successful. Often, if the employer uses contingency firms, there will be more than one contingency firm competing to fill a certain position. As a job hunter, if you are sent to an interview by a contingency firm, you may find that you are competing with a larger number of applicants for a position. Generally, retained firms only send in from 3 to 5 candidates for a position.
Recruiters will be paid fees equal to about 25% to 35% of the resulting salary of the successful candidate plus expenses. This does not come out of the job candidate’s salary. This is paid to the recruiter through a separate relationship between the employer and the search firm. This may seem like a large fee, but, keep in mind that recruiters incur a great many expenses when searching for successful job candidates. They spend enormous amounts of money on computer systems, long distance calls, mail-outs, travel and interviews. Recruiters work very hard for these fees. Employers recognize the value of using recruiters and are more than willing to pay recruiters the fees. All you have to do is contact the recruiter to get the process moving.
4) Not all medical recruiters work only with physicians.
Some search firms work exclusively with physicians or in healthcare, while others may work in several fields at once. Some of the larger generalist firms will have one or more search consultants that specialize in healthcare. It is important for you, as a job hunter, to assess the recruiters’ knowledge of your field. If you use industry or medical specialty buzz words in describing your skills, experience or career aspirations, you may or may not be talking a language the recruiter understands fully. It is wise to explore fully with the recruiter his understanding of your field and area of specialization.
5) Recruiters and search consultants move around.
Recruiters, like many professionals, move to new firms during their careers. Often you will find that recruiters will work at several firms during their careers. Since it is much more effective to address your letters to a person rather than “to whom it may concern”, it is smart for job hunters to have accurate and up-to-date information about who is who and where, since this can change frequently. Search firms also move their offices, sometimes to another suite, street or state. If you have a list of recruiters that is over one year old, you will certainly waste some postage in mailing your resumes and cover letters. Many of your mail-outs will be returned to you stamped “non-deliverable”, unless you obtain an up-to-date list. A resource, like the Directory of Healthcare Recruiters is updated very frequently, usually monthly [www.pohly.com/dir3.html].
6) Most search firms work with positions all over the country.
If you are from a particular state, and want to remain in that state, don’t make the mistake of only sending your resume to recruiters in your state. Often the recruiters in your state are working on positions in other states, and recruiters in other states are working on positions in your state. This is usually the case. Very few recruiters work only in their local area, most work all around the US and some internationally. Regardless of your geographic preference, you should still send your resume to all the healthcare recruiters. If you really only want to remain in your area, you can specify that preference in your cover letter.
7) Recruiters primarily work with hard to fill positions or executive positions.
Some recruiters specialize in clinical positions for physicians, managed care executive positions, healthcare financial positions or health administration positions. Others may specialize in finding doctors, nurses or physical therapists. Generally, an employer does not engage a recruiter’s assistance in filling a position unless it is hard to fill. Sometimes employers will engage search firms to save them the valuable time of advertising or combing through dozens of resumes.
Contingency recruiters tend to work with more mid-level management and professional positions, but, this is not always the case. Retained firms generally work with the higher level clinical or administrative positions.
One thing you will be assured of is that if a recruiter is working on a position that means that the employer is willing to pay a fee. That usually means that the position is a valued position and one worth closer inspection on your part. Even in healthcare, with certain exceptions, our economy is an “employer’s market”. This means that employers receive a deluge of resumes for their open positions. Increasingly, employers are using recruitment firms to handle their openings and schedule the interviews because employers simply do not have the manpower or time to handle the many resumes they receive. Therefore, if a job hunter is submitted by a recruiter, that job hunter has a great advantage over all other applicants.
Posted on December 25, 2018 by Dr. David Edward Marcinko MBA MEd CMP™
City Lights in Baltimore, Maryland
By Dr. David Edward Marcinko; MBA, CMP™
[Editor-in-Chief]
I stopped off in Baltimore, Maryland during the recent holidays to visit current clients, prospect for new ones, do a little public speaking and promote our book [Business of Medical Practice, third edition].
Of course, we stopped by Johns Hopkins University where my sister worked, and promoted the Medical Executive-Post, as well.
Enter Christmas Street
And so, it was with great anticipation that we agreed with our host to visit Baltimore’s Christmas Street, in a section of the city known as Hampden. For 65 years, the residents of Baltimore’s 34th Street have drawn crowds from all over the world to view their display of Christmas lights.
Assessment
Crowd favorites are the motorized robot, the hubcap “Christmas tree”, and “snowmen” made from bicycle tires. The eaves of houses drip with strings of lights that illuminate Nativity scenes, while glowing candy canes light the sidewalks.
And, the hot chocolate and pizza, down the street at Angelo’s Restaurant, was especially delicious on any cold wintry night.
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Sponsors Welcomed
And, credible sponsors and like-minded advertisers are always welcomed.
The market for medicine is incredibly interesting. Almost every day we learn something new about a treatment that we thought would work but does not, or about a treatment that we didn’t think would work but does.
Beyond the particular fascination, I think that the medicine market can also teach us important lessons about rationality … read more:
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
***
***
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
It is important to develop a general checklist that touches some of the most important issues in launching a traditional medical practice; or an extended medical service line.
Once the checklist or “to-do” list is completed, and practically it never will be, a time-line may be developed, accelerated, decelerated or modified depending on circumstances. Just think of it as an overlapping continuum rather than discrete steps using appropriate elements of the checklist below.
Time-Line Milestones to Office Launch
12 Months Out:
Determine your strategic competitive advantage
Obtain medical license
Craft a business plan
Secure capital funding and living expenses
Secure office location for professional, demographic or lifestyle reasons
Retain a practice management consultant, accountant, banker and attorney.
9-11 Months Out:
Retain and hire contractor, architect or remodeling firm and build out the office space
Obtain certificate of occupancy or appropriate permits
Incorporate the business [S Corp, LLC, PC, etc]
Obtain state and federal tax ID and EIN, DEA number, NPI, Medicare and Medicaid provider numbers, etc
Contact insurance companies for credentialing applications to become a contracted provider
Contact local medical professionals, hospitals and ASCs, etc.
Contact and set up an account with a medical waste company (unless the landlord includes this in the lease or sub-lease)
Secure credit card or similar payment services
Prepare for MCO, HMO, CAQH credentialing and walk-thru’s, etc
Order office stationary, logos, business cards, etc.
Open house parties.
Impending Opening
Commence patient care.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, urls and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
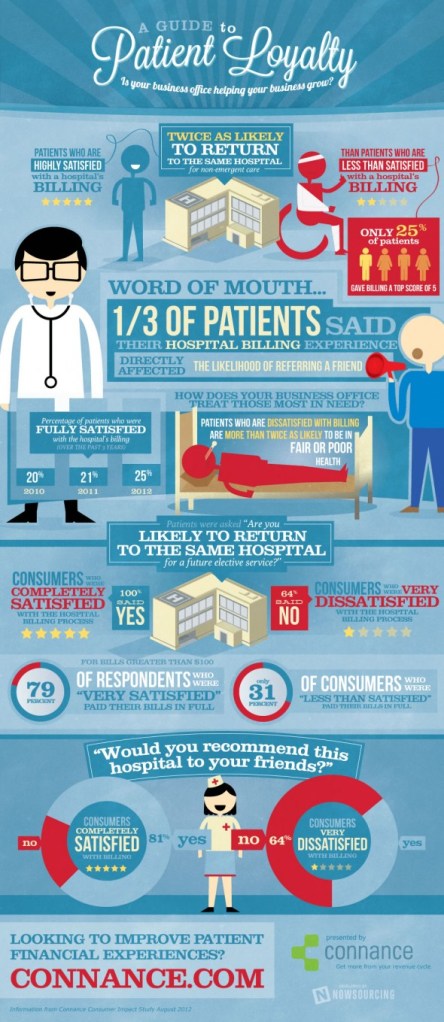
Many factors are involved when a patient has a good experience at a hospital, clinic or medical practice. One huge component in patient loyalty and satisfaction is the billing process.
This infographic colorfully shows what factors to consider in gaining and keeping loyal patients.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Connection Makes the Difference – A Collaborative Shift in Bedside Manner?
Healthcare 2.0 is all about connecting. Take your pick: you can communicate via blogs, tweets, IMs, wikis, or social networks. And then, of course, you can opt for just plain old face-to-face dialogue.
The Communication Explosion
According to ME-P experts and Business of Medical Practice textbook contributors Mario Moussa PhD and Jennifer Tomasik MA, on the face of it, the explosion of communication options seems like a very good thing indeed.
In the most basic ways, human beings need connection. Without the give and take of social interaction, our health suffers. In extreme situations—in solitary confinement or similar conditions—the brain almost completely shuts down.
What We Can Learn from Terry Anderson
The journalist Terry Anderson was held hostage in Lebanon from 1985 to 1992, enduring months at a time of almost complete isolation. In his memoir Den of Lions, Anderson described the catastrophic result: “The mind is a blank…. Where are all the things I learned, the books I read, the poems I memorized? There’s nothing there, just a formless, gray-black misery. My mind’s gone dead.”
The Link Between Social Connection and Good Health
On the positive side, studies have established a link between social connection and good health. (Even contact with people you dislike is better than having no contact at all). The same goes for the relationship between doctor and patient: data show that when the relationship is satisfying, it has tangible health benefits.
For example, when patients have a positive emotional connection with their doctors, they remember a higher percentage of care-related information and even experience significantly better physiological outcomes.
The Conversation
And the way doctors converse with patients—apart from the actual content of the conversations—has an equally powerful effect:
Do you want your patient’s nagging headaches to go away?
Discuss their expectations and feelings, in addition to the neurological facts. This is much more effective than sticking to the facts alone, since a strong psychological bond is strong medicine.
Do you want your medical advice to be followed?
Draw your patient into conversations about treatment. The research shows that engagement makes a difference.
Assessment
Is there an analogy here for financial advisors and medical management consultants?
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
December 23rd, 2011 – The Institute of Medical Business Advisors [iMBA] Inc, in Atlanta, GA www.MedicalBusinessAdvisors.com and Springer Publishing Company of New York, just released the third edition of “The Business of Medical Practice” [Transformational Health 2.0 Skills for Doctors] edited by iMBA founder Dr. David Edward Marcinko MBA, CMP™ and President Hope Rachel Hetico RN, MHA, CPHQ, CMP™
Internal Contents
The 37 chapter, 750 page hard-cover textbook provides a comprehensive resource for those physicians, medical professionals, practice managers, nurse executives, health care administrators and graduate students seeking working knowledge on running a private facility or medical clinic.
Three Major Sections
The BoMP is comprised of three enterprise-wide sections: [1] Qualitative Office Operations, [2] Quantitative Aspects of Medical Practice and [3] Health Policies, Ethics and Leadership. Topics like ARRA, HITECH, ACA and the social networking aspects and ramifications of health 2.0 connectivity for all stakeholders are included for modernity.
Tools and Templates
Tools used throughout the book help readers reference and retain complex information. These tools include:
Sidebars. Key terms, key concepts, key sources, associations, and factoids all serve to enhance and reinforce the core takeaways from each chapter.
Tables. Tables are used to display and reference benchmark data, draw comparisons, and illustrate industry data trends.
Figures. Graphical depictions of concepts help you comprehend the material.
Charts. Charts allow easily referenced standard industry taxonomies alongside comparisons of related topics.
Assessment
For a further description of the Business of Medical Practice, with online “live’ community, please click: www.BusinessofMedicalPractice.com
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on November 19, 2011 by Dr. David Edward Marcinko MBA MEd CMP™
Business Education Needed for Physicians and all Medical Colleagues
By Dr. David Edward Marcinko MBA CMP™
[Publisher-in-Chief]
While the doctors consult, the patient dies
-English Proverb
There are many self-help publications, online resources and management guru’s purporting to impart business information to their physician clients. Within the current managed care climate, economic malaise, and specter of nationalized healthcare following the 2010 health insurance reform legislation, medical business consultants are all the rage.
However, in the same vein, physician bankruptcies are mounting, medical student loan delinquencies are increasing, physician finances are friable and medical and ancillary practices are closing at record numbers. What gives?
Do Doctors Lack Business Knowledge?
Perhaps the answer lies in the lack of real business, accounting, financial and managerial acumen by the average practitioner? This growing concern is prompting more and more doctors to seek the help of a healthcare consultant or financial advisor. But, just what does a practice management consultant do, what credentials are needed to be in the business, and how can a healthcare advisor help you coordinate all aspects of your practice’s life?
Here are two examples of major practice management fiascos.
Corporate Medicine and Doctor Super-Groups
As the managed and healthcare care crisis exacerbates, and Obama Care [Patient Protection and Affordable Care Act] unfolds over the next eight years, there will be many examples of irrational practice management behavior on the part of physicians, and no specialty is immune.
Just collectively reflect a moment on colleagues willing to securitize their practices a decade ago – and currently with so the so called medical super groups – and cash out to Wall Street for riches that were not rightly deserved. Where are firms such as MedPartners, Phycor, FPA and Coastal Healthcare now? A survey of the Cain Brothers Physician Practice Management Corporation Index of publicly traded PPMCs revealed a market capital loss of more than 99%, since inception; despite their various heath 2.0 re-incarnations. And, how will modern financial regulatory reform, Dodd-Frank, the SEC, insurance company and banking controls resulting from Wall Street’s 2008-09 economic debacles, impact physicians?
A Southern Gentleman and Solo Physician
Or, consider the personal situation of a solo Southern primary care physician who learned an accounting lesson the hard way when he asked his CPA to appraise his business. Upon sale, his attorney brother-in-law drew up the contract, as he was pleased the practice quickly sold for its full asking price. What he didn’t know, but would soon discover, is that accounting value or “book” value — the figure his accountant gave him — is far different than the fair-market value that he could have received for his long years of toil. Was the CPA wrong? Not really. Was the gentleman doctor incorrect? No. Both were merely operating under a different set of practice management terms, and accounting definitions, without communication or knowledge of each other’s perspectives.
And so, your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
The conversion to managed healthcare and capitation financing is a significant marketing force and not merely a temporary business trend. More than 60% of all physicians in the country are now employees of a MCO. Those that embrace these forces will thrive, while those opposed will not.
Developing an Attractive Practice
After you have evaluated the HMOs in your geographic area, you must then make your practice more attractive to them, since there are far too many physicians in most regions today. The following issues are considered by most MCO financial managers and business experts, as they decide whether or not to include you in their network:
General Standards
Is there a local or community need for your practice, with a sound patient base that is not too small or large? Remember, practices that already have a significant number of patients have some form of leverage since MCOs know that patients do not like switching their primary care doctors or pediatricians, and women do not want to be forced to change their OB/GYN specialist. If the group leaves the plan, members may complain to their employers and give a negative impression of the plan.
A positive return on investment (ROI) from your economically sound practice is important to MCOs because they wish to continue their relationship with you. Often, this means it is difficult for younger practitioners to enter a plan, since plan actuaries realize that there is a high attrition rate among new practitioners. They also realize that more established practices have high overhead costs and may tend to enter into less lucrative contract offerings just to pay the bills.
A merger or acquisition is a strategy for the MCO internal business plan that affords a seamless union should a practice decide to sell out or consolidate at a later date. Therefore, a strategy should include things such as: strong managerial and cost accounting principles, a group identity rather than individual mindset, profitability, transferable systems and processes, a corporate form of business, and a vertically integrated organization if the practice is a multi-specialty group.
Human resources, capital, and IT service should complement the existing management information system (MIS) framework. This is often difficult for the solo or small group practice and may indicate the need to consolidate with similar groups to achieve needed economies of scale and capital, especially in areas of high MCO penetration.
Consolidated financial statements should conform to Generally Accepted Accounting Principles (GAAP), Internal Revenue Code (IRC), Office of the Inspector General (OIG), and other appraisal standards.
Strong and respected MD leadership in the medical and business community is an asset. MCOs prefer to deal with physician executives with advanced degrees. You may not need a MBA or CPA, but you should be familiar with basic business, managerial, and financial principles. This includes a conceptual understanding of horizontal and vertical integration, cost principles, cost volume analysis, financial ratio analysis, and cost behavior.
The doctors on staff should be willing to treat all conditions and types of patients. The adage “more risk equates to more reward” is still applicable and most groups should take all the full risk contracting they can handle, providing they are not pooled contracts.
Are you a team player or solo act? The former personality type might do better in a group or MCO-driven practice, while a fee-for-service market is still possible and may be better suited to the latter personality type.
Each member of a physician group, or a solo doctor, should have a valid license, DEA narcotics license, continuing medical education, adequate malpractice insurance, board qualification or certification, hospital privileges, agree with the managed care philosophy, and have partners in a group practice that meet all the same participation criteria. Be available for periodic MCO review by a company representative.
Specific Medical Office Standards
MCOs may require that the following standards are maintained in the medical office setting:
It is clean and presentable with a professional appearance.
It is readily accessible and has a barrier-free design (see OSHA requirements).
There is appropriate medical emergency and resuscitation equipment.
The waiting room can accommodate 5 – 7 patients with private changing areas.
There is an adequate capacity (e.g., 5,000 – 10,000 member minimum), business plan, and office assistants for the plan.
There is an office hour minimum (e.g., 20 hours/week).
24/7 on-call coverage is available, with electronic tracking and eMRs.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on March 16, 2011 by Dr. David Edward Marcinko MBA MEd CMP™
Look Before you Leap
By Shahid N. Shah MS
Because of all the talk about electronic medical records [EMRs] and medical records software, doctors have many reasons to start immediately looking for an EMR vendor.
But, try to resist that urge and look at broader non-EMR solutions that can help remove some of the non-clinical burdens from your staff.
Using Microsoft Office Outlook® or an online calendaring system like Google to maintain patient schedules. While most vendors of clinical scheduling will tell you that medical scheduling is too complex to be handled by non-medical scheduling systems, most small and medium sized physician practices can easily get by with free or very inexpensive and non-specialized scheduling tools. By using general-purpose scheduling tools you will find that you can use less expensive consultants or IT help to manage your patient scheduling technology needs.
Using off-the-shelf address book software such as those built into Microsoft Office®, the Windows® and Macintosh® operating systems, or online tools such as Google apps you can maintain complete patient and contact registries for managing your patient lists. While a patient registry may not give you all of the features and functions you need immediately they can grow to a system that will meet your needs over time.
Using physician practice management systems you can remove much of the financial bookkeeping and insurance record-keeping burdens from your staff. Unlike calendaring or address book functionality which can be adapted from non-medical systems, insurance claims and related bookkeeping is an area where you should choose specific software based on how your practice earns its revenue. For example if a majority of your claims are Medicare related, then you should choose software that is specifically geared towards government claims management. If however your revenue comes less from insurance and more from traditional cash or related means you can easily use small business accounting software like Quicken® or Microsoft accounting.
Using computer telephony technology you can integrate automatic call in and call out the services that can be tied to your phone system so that you can track phone calls or send out call reminders.
Using integrated medical devices that can capture, collect, and transmit physiological patient data you can reduce paper capture of vital signs and other clinical data so that your staff are freed to do other work.
Using e-mail, instant messaging, social networking, and other online advanced tools you can reduce the number of phone calls that your practice receives and needs to return and yet continue to improve the patient physician communication process. One of the most time-consuming parts of any office is the back-and-forth phone calls so any reduction in phone calls will yield significant productivity increases.
And so, your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com and http://www.springerpub.com/Search/marcinko
Our Other Print Books and Related Information Sources:
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on February 16, 2011 by Dr. David Edward Marcinko MBA MEd CMP™
Can this Vital Buck be More Efficiently Used?
By Dr. David Edward Marcinko MBA CMP™
[Editor-in-Chief]
Recently, healthcare economist Austin Frakt PhD offered these points about healthcare dollars spent on the margin:
1. Spending on health is not without value. It does improve lives [See Cutler]. Yet, we spend much to get that value.
2. Price per QALY is very high [See Aaron’s series on spending and his other on quality).
3. Just staying within the realm of health, the price per QALY on another “service” might be a lot lower [like nutrition, exercise, and healthy habits, etc].
Note: The quality-adjusted life year (QALY) is a measure of disease burden, including both the quality and the quantity of life lived. It is most often used in assessing the value for money of a medical intervention. The QALY model requires independent utility, neutral risk and constant proportional tradeoff behavior.
Understanding Marginal Profit
Recalling the equation: Profit = (Price x Volume) – Total Costs
We could amend it and say that:
Total Profit = P x V – (FC + VC) or: Total Profit = Price x Volume – (Fixed Costs + Variable Costs)
However, most medical office or clinic contracts today are based not on total profit, but on additional or marginal profit, because overhead costs always remain and clinic fixed costs are not important in contracted medicine.
And, for other pricing decisions, the equation can again be re-written, to emphasize variable costs, as follows: Marginal Profit = (P x V) – VC.
In other words, the marginal benefit must exceed the marginal cost of practice.
Cost-Volume-Profit Analysis
Now, once a basic understanding of marginal profit and medical cost behavior is achieved, the techniques of cost-volume-profit analysis (CVPA) can be used to further refine the managerial cost and profit aspects of the medical office business unit. CVPA is thus concerned with the relationship among prices of medical services, unit volume, per unit variable costs, total fixed costs, and the mix of services provided.
Austin felt that if [*]od were jointly designing all health-related systems and functions of society and government – He’d look at the marginal cost/QALY over all possible ways to spend the next dollar and pick the smallest. How about you?
But, it’s not always going to be on health care services and it probably isn’t given what we’re already spending for those and what we’re getting for that spending.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
As you’ve probably heard – and experienced or know from our books, journal and this ME-P – there’s a primary care medical shortage out-there! Maybe you’ve even read or heard about the Physician’s Foundation study describing the overwhelming number of PCPs who want out of this toxic environment. On one hand, we have patients desperately searching for a PCP, while on the other hand we have good caring doctors being forced out of the profession. Of course, NPs, ANPs, DNPs and other ancillaries are part of the solution; but not entirely.
And humanely, as stated by our medical colleague L. Gordon Moore MD, these statistics miss the very real pain and anguish of people who entered primary care to help patients when they find the environment for primary care toxic to the ethical practice of medicine. Even to the point of suicide!
Assessment
These voices need to be heard. And so, we are asking doctors and providers of all stripes to post in the comments section below personal examples of medical practitioners leaving primary, solo or small group practice because they just can’t stand the toxic environment any longer.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on November 5, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
Part Two
By Dr. David Edward Marcinko MBA
[Publisher-in-Chief]
If you read this ME-P regularly or have read my earlier blogs, you know that I am writing a book on practice management for the private medical practitioner.
A recent story in the Chicago Tribune on the difficult business life of private practitioners today reminds me that I need to keep my nose to the grindstone.
For example, according to the sanofi-aventis Pharmaceutical Company Managed Care Digest Series, for 2008-10, the following patterns and comparative trend information has been empirically determined and may provide a basic starting point for medical practitioners to share business management, facilities, personnel, and records information for enhanced success www.managedcaredigest.com
Mid-Level Provider and Staffing Trends
Mid-level provider use increased among multi-specialty groups, especially in those with more than half of their revenue from capitated contracts. Use also rose with the size of the practice and was highest with OB/GYN groups.
Medical support staff for all multi-specialty groups fell and was lowest in medical groups with less than 10 full-time equivalent (FTE) physicians. However, groups with a large amount of capitated revenue actually added support staff. Smaller groups limited support staff.
Compensation costs of support staff increased and the percentages of total operating costs associated with laboratories, professional liability insurance, IT services, and imaging also increased. Support staff costs increase with capitation levels and more than half of all operating costs are tied to support staff endeavors.
Managed Care Activity and Contracting Trends
More medical group practices are likely to own interests in preferred provider organizations (PPOs) than in HMOs and the percentages of groups with managed care revenue continues to rise. Multi-specialty and large groups also derive more revenue from MCOs than single specialty or smaller groups.
Managed care has little effect on physician payment methods that are still predominantly based on productivity. Physicians were paid differently for at-risk managed care contracts in only a small percentage of cases.
Most medical groups (75%) participating in managed care medicine have PPO contracts. Group practices contract with network HMOs more often than solo practices. Single-specialty groups more often have PPO contracts.
Capitated lives often raise capitation revenues in large group practices. Group practices are more highly capitated than smaller groups or solo practices. Almost 30% of highly capitated medical groups have more than 15 contracts and 22% have globally capitated contracts.
Higher capitation is linked with increased risk contracting. Larger groups have more risk contracting than smaller groups.
Financial Profile Trends
Medicare fee-for-service reimbursement is decreasing. Highly capitated groups incur high consulting fees.
The share of total gross charges for OB/GYN groups associated with managed care at-risk contracts is rising while non-managed care, or not-at-risk charges are declining.
Capitated contracts have little effect on the amount of on-site office non-surgical work. Off-site surgeries are most common for surgery groups, not medical groups.
Half of all charges are for on-site non-surgical procedures.
Highly capitated medical groups have higher operating costs and lower net profits.
Groups without capitation have higher laboratory expenses than those who do.
Physician costs are highest in orthopedic surgery group practices. Generally, median costs at most specialty levels are rising and profits shrinking.
Assessment
Obviously, the above information is only a gauge since regional differences, and certain medical sub-specialty practices and carve-outs, do exist.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on October 27, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
Part One of Two
By Dr. David Edward Marcinko MBA
[Publisher-in-Chief]
If you read this ME-P regularly or have read my earlier blogs, you know that I am writing a book on practice management for the private medical practitioner.
And, a recent story in the Chicago Tribune on the difficult business life of private practitioners today reminds me that I need to keep my nose to the grindstone.
For example, knowing your medical contract negotiation objectives, gathering information on the choices of contracts and discount payment systems, and understanding the pitfalls to watch for when evaluating a contract are the keys to any successful negotiation process.
Reimbursement Contract Negotiations
According to the sanofi-aventis Pharmaceutical Company Managed Care Digest Series, for 2008-10, the following pattern and trend comparative information has been empirically determined and may provide a basic starting point for practitioners to share business management, facilities, personnel, and other records for enhanced contract negotiation success.
Among all physicians in a single-specialty group practice, invasive cardiologists averaged the most encounters with total hospital inpatient admissions down from the prior year. However, encounters rose for cardiologists in multispeciality group practices.
Echocardiography was the most commonly performed procedure on HMO seniors, followed by coronary artery bypass graft surgery. Group practices performed cardiovascular stress tests for circulatory problems most often.
CT studies of the brain and chest were the most common studies for HMO seniors, while MRI head studies were the most common diagnostic test on commercial HMO members.
Colonoscopy was the most common digestive system procedure on senior HMO members, while barium enemas were more common on commercial members.
Hospital admission volume decreased for allergists, family practitioners, internists, OB/GYNs, pediatricians, and general surgeons.
Internists ordered more in-hospital laboratory procedures than any other physicians in single-specialty groups.
Non-hospital MD/DOs used in-hospital radiology services most frequently, continuing a three-year upward trend.
Pediatricians averaged the most ambulatory encounters, down from the prior year.
Non-hospitalist internists ordered a higher number of in-hospital laboratory procedures than any other single medical specialty group, but allergists and immunologists increased their laboratory usage.
The number of ambulatory encounters increased for general surgeons, while group surgeons had the most cases. Capitated surgeons, of all types, had a lower mean number of surgical cases than surgeons in groups without capitation. Surgeons in internal medical groups also had more cases than those in multi-specialty groups.
The average number of total office visits per commercial and senior HMO visits fell, along with the number of institutional visits for both commercial and senior HMO members.
The average length of hospital stay for all commercial HMO members increased to 3.6 days but decreased to 6 days for all HMO members.
The total number of births increased for commercial HMO members served by medical group practices, and decreased for solo practitioners.
More than one-third of all medical groups use treatment protocols, rising from the year before. Multi-specialty groups were more likely to use them than single-specialty groups, who often develop their own protocols. The use of industry benchmarks to judge the quality of healthcare delivery also increased.
Outcome studies are most common at larger medical groups, and multi-specialty groups pursue quality assurance activities more often than single-specialty groups.
Provider interaction during office visits is increasingly coming under scrutiny. Patients approve of cardiologists more frequently than allergists and ophthalmologists.
Assessment
Obviously, the above information is only a gauge since regional differences, and certain medical sub-specialty practices and carve-outs, do exist.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Dr. David Edward Marcinko, a former residency director, department chairman, and hospital vice-president in Atlanta GA, retired from clinical practice at the age of 45 after selling his Ambulatory Surgery Center to a public company. As a fellow and board certified surgeon, he authored more than two dozen medical and business textbooks in three languages, teaching and operating in the EuroZone, co-founding a pre-IPO PPMC, and forming a series of successful internet ventures while still maintaining a 60 hour work week.
His companies have created dozens of cognitive products in the last few years that maintain a comfortable lifestyle that started from his home office after retirement. Dr. Marcinko picked up an MBA degree, became a certified financial planner and insurance agent, and developed a cult following thru collaborative on-ground and online education for physicians, financial advisors and management consultants. A social media pioneer and publisher, this Medical Executive-Post is an influential syndicated blog with thousands of content contributions from nationally know experts.
Dr. Marcinko is a highly sought after futurist and speaker in the areas of health economics, financial planning, medical practice management and related entrepreneurial e-insights for intersecting sectors in the healthcare industrial complex.
Edited with Professor Hope Rachel Hetico of the Institute of Medical Business Advisors [iMBA] Inc www.MedicalBusinessAdvisors.com
Financial Planning and Risk Management Handbooks for Doctors
Posted on October 13, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
It’s Not All about Electronic Records
By Dr. David Edward Marcinko; MBA, CMP™
[Editor-in-Chief]
Introduction
To understand the medical records revolution that has occurred this decade, put your self for a moment in the position of a third-party payer; ie; a private insurance company, Medicare or Medicaid etc.
For example, you want to know if Dr. Joel Brown MD actually gave the care for which he is submitting a [super] bill or invoice. You want to know if that care was needed. You want to know that the care was given to benefit the patient, rather than to provide financial benefit to the provider beyond the value of the services rendered.
Can you send one of your employees to follow Dr. Brown around on his or her office hours and hospital visits? Of course not! You cannot see what actually happened in Dr. Brown’s office that day or why Dr. Black ordered a PET scan on the patient at the imaging center. What you can do however, is review the medical record that underlies the bill for services rendered from Dr. Blue. Most of all, you can require the doctor to certify that the care was actually rendered and was indicated. You can punish Dr. White severely if an element of a referral of a patient to another health care provider was to obtain a benefit in cash or in kind from the health care provider to whom the referral had been made. You can destroy Dr. Rose financially and put him in jail if his medical records do not document the bases for the bills he submitted for payment.
The Payment Paradigm Shift
This nearly complete change in function of the medical record has precious little to do with the quality of patient care. To illustrate this medical records evolution/revolution point, consider only an office visit in which the care was exactly correct, properly indicated and flawlessly delivered, but not recorded in the office chart. As far as the patient was concerned, everything was correct and beneficial to the patient. As far as the third-party payer is concerned, the bill for those services is completely unsupported by required documentation and could be the basis for a False Claims Act [FCA] charge, a Medicare audit, or a criminal indictment. We have left the realm of quality of patient care far behind.
Provider Attitude Adjustments Required
Instead, medical practitioners must adjust their attitudes to the present function of patient records. They must document as required under pain of punishment for failure to do so. That reality is infuriating to many since they still cling to the ideal of providing good quality care to their patients and disdain such requirements as hindrances to reaching that goal. They are also aware of the fact that full documentation can be provided without a reality underlying it. “Fine, you want documentation? I’ll give you documentation!”
Computer Charting and eMRs
Some doctors have given in to the temptation of “cookbook” entries in their charts, canned computer software programs or eMRs listing all the examinations they should have done, all the findings which should be there to justify further treatment. Many have personally seen, for example, hospital chart notes which describe extensive discussion with the patient of risks, alternatives and benefits in obtaining informed consent when the remainder of the record demonstrates the patient’s complaint that the surgeon has never told her what he planned to do; operative reports of procedures done and findings made in detail which, unfortunately, bear no correlation with the surgery which was actually performed.
Assessment
Whether electronic medical records (eMRs) will be helpful regarding fraud prevention, in the future is still not known. But, it is at best naive and more frequently closer to a death wish to think that a practitioner can beat the system, with handwritten notes, computer generated records, or fabricated eMR documentation.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on October 11, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
About the Institute for Clinical Systems Integration [ICSI]
By Brent A. Metfessel MD, CMP™
The Institute for Clinical Systems Integration (ICSI) is a strong proponent of the value of evidence-based clinical guidelines, and cites the following objections that make their implementation and acceptance more difficult.
The Issues
These issues generally apply to technology assessments as well:
Guidelines are a legal hazard: There is a fear that following a guideline that turns out to be wrong increases the risk of litigation. Good guidelines, however, are evidence-based and not opinion-based drivers of care. Furthermore, once a review of the literature takes place and is synthesized into a preliminary guideline, multi-specialty physician focus groups review the guidelines prior to finalization. The strength of evidence supporting each conclusion is usually stated, highlighting areas of remaining scientific uncertainty. “Evidence hierarchies” are often used as aids to grading recommendations, with meta-analysis, systematic reviews, and randomized controlled trials being at or near the top of the hierarchy in strength, with narrative reviews, case reports, and medical opinion pieces being considered the weakest forms of evidence. This provides additional checks and balances to guideline development.
Guidelines are cookbook medicine: Guidelines are just that – guidelines. Each patient should be provided treatment according to his/her individual needs. Evidence-based clinical guidelines are based on extensive reviews of the literature and are applicable to the vast majority of cases for a particular clinical condition but not necessarily all cases. In the case of practice pattern evaluation or profiling, comparisons of such patterns to medical guidelines can help identify overall systematic variations from the norm rather than variations due to particular patients with special needs.
Guidelines do not work: When used as the sole basis for practice improvement, this statement contains some truth. However, when incorporated into a systematic continuous quality improvement approach, they have been shown to improve practice patterns and reduce variation.
Physicians will not use guidelines: Once physicians know that the guidelines are based on a sound review of the medical literature, practitioner buy-in greatly increases. In addition, clinicians need to realize that clinical guidelines are only one part of the total treatment picture since a team approach to patient care is becoming the norm.
Guidelines need validation through actual outcomes data: This is correct when based on a continuous quality improvement approach, but is incorrect if outcomes are based on individual events. Local implementation of guidelines can be compared to outcomes data one or two years after implementation. Depending on the actual level of practice pattern improvement, minor alterations can be made to the guidelines to reflect local needs.
Guideline Adaptation
National guidelines in some cases may need adaptation to local patient needs and concerns. For example, a practice in a major metropolitan area where specialty care is readily available differs in major ways from a rural practice which is based more on primary care. Practices where many patients are poor or on public assistance also differs from practices in affluent areas. When used as basic guides to appropriate practice, however, clinical guidelines can significantly decrease practice variation.
Evidence Based Medicine
With the recent emphasis on evidence-based medicine and on decreasing the time lag between evidence publication and its effect on actual patient care, a number of agencies have added clinical guideline and technology assessment development to their task lists. Such agencies include specialty societies such as the American College of Cardiology (ACC), private companies and non-profit organizations, governmental bodies such as the Agency for Health Care Research and Quality (AHRQ), and MCOs that review the scientific evidence for the purpose of determining coverage policy.
Assessment
MCOs may post medical coverage policies on the Web for physicians to access, and these generally contain narrative justifications (often with evidence grading) in terms of why a particular procedure or diagnostic test may or may not be covered based on level of efficacy shown in scientific studies. It is important to note that for many high-tech or new procedures, different MCOs may have somewhat different coverage policies based on variation in terms of interpreting the evidence, especially in areas where the science is less certain.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
With the passage of healthcare reform legislation, officially known as the Patient Protection and Affordable Care Act of 2010, many questions remain regarding its effect upon physicians’ livelihood.
Undoubtedly this bill moves the healthcare system several steps closer to a socialized model, but the effects on physicians’ salaries and compensation models are far from clear.
Other Countries
One way to see the effect that this shift may have on compensation is to look to other countries, many of which already have a more socialized system in place.
According to the CRS Report for Congress, US Health Care Spending: Comparison with Other OECD Countries http://assets.opencrs.com/rpts/RL34175_20070917.pdf) US specialists rank near the top in compensation compared to these other countries, trailing the Netherlands and Australia. The average specialist in the US made $230,000 in this survey. The comparable salary in Canada is $161,000, $150,000 in the UK, and $253,000 in the Netherlands. Generalists in the US are at the top in terms of compensation with an average of $161,000. This compares to $107,000 in Canada, $118,000 in the UK, and $117,000 in the Netherlands.
Inflation Adjustments
Another indicator of physician salary trends is the change in compensation adjusted for inflation. According to the American Medical Association, the inflation-adjusted income for the average patient care physician declined from $180,930 to $168,122 from 1995 to 2003, a 7% decrease. And, the inflation adjusted decrease is more substantial given the low interest rate environment thru 2010, and going forward.
Given these trends, as well as the fact that an increasing percentage of healthcare payments are coming from dwindling government sources, it is likely that physician salaries will decline as “healthcare reform” legislation is implemented. In fact, it is likely that this trend will accelerate. A 15% to 25% inflation-adjusted decline in salaries over the next decade is a reasonable prediction.
Assessment
It is also important to note that the level of student debt in the US continues to rise, while college and medical education are usually subsidized in other countries. Many foreign physicians graduate with no student loan debt. The ratio of debt level to salary in the US continues to become more onerous for new physicians.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Whether it is an employer interested in the results of an employee’s health screening; an insurer attempting to learn more about an enrollee’s prior health history; the media in search of a story; or health planners examining the potential value of national health databases, the confidential nature of the traditional doctor-patient relationship may be compromised through demands for clinical information by parties other than the patient and treating caregivers.
Impact of eMRs
In addition, without clear safeguards the growth in use of electronic medical records may put personal health information at risk of tampering or unauthorized access. Clearly, employers and insurers are interested in the status of an individual’s health and ability to work; but does this desire to know, combined with their role as payers for health care, constitute a right to know? The patient’s right to privacy remains a volatile and unresolved issue.
Assessment
Counter to this concern is the recognition that electronic records may dramatically improve communications by offering greater accessibility of information to clinicians in the hospital or office potentially reducing medical errors through elimination of handwritten notes, increased use of built in prompts and clinically-derived triggers for orders and treatments, and development of pathways for optimal treatments based on clinically valid and tested best practices.
Conclusion
And so, your thoughts and comments on this ME-P are appreciated. What do you think about this confidentiality conflict and the role of eMRs? Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now:Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on October 5, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
Versus Healthcare Management
[By Eugene Schmuckler PhD, MBA and Dr. David Edward Marcinko MBA]
Many times, individuals or physicians will use the terms management and leadership synonymously. In actuality the terms have significantly different meanings.
For example, Warren Bennis describes the difference between managers and leaders as “Managers do thing right, Leaders the right thing.”
***
***
The Managers
Managers are those individuals who have as their primary function managing a team of people and their activities. In effect, managers are those who have been given their authority by the nature of their role and ensure that the work gets done by focusing on day to day tasks and their activities.
On other hand, a leader’s approach is generally innate in its approach. Good leadership skills are difficult to learn because they are far more behavioral in nature than those skills needed for management. Leaders are also very focused on change recognizing that continual improvement can be achieved in their people and their activities can be a great step towards continued success.
Leadership Development
Perhaps some of the best training grounds for the development of leaders are the military. The Marine Corps slogan is “A Few Good Men” and the military academies at Annapolis (Navy), New London, Connecticut (Coast Guard), Colorado Springs (Air Force), and West Point (Army) all have as their main mission, the development of leaders. This is done by a number of different techniques. At graduation, the new officers, regardless of the branch of service, have been taught, and more importantly, have internalized the following: communicate the missions, sensitivity matters, real respect is earned, trust and challenge your soldiers. It is due to these lessons that many graduates of the military academies go on to positions of leadership in the private sector as well as in government. Communicating the mission refers to conveying to those who work with us what are practice is hoping to accomplish and the role of each employee in achieving that goal. Given an understanding and awareness of the mission, when confronted with a barrier, employees are able to face hard problems when there is no well-defined approach by which to deal with them.
Sensitivity does matter – A leader treats each employee with respect and dignity, regardless of race, gender, cultural background or particular role they actually perform in the practice. Consider how many legal suits are filed against any type of organization, whether it is a medical practice or a large manufacturing facility due to perceived disparate treatment towards the employee based on race, religion, gender sexual preference or other non-work related issues.
Real respect is earned – Having initials after one’s name and the wearing of a lab coat does not automatically entitle an individual to respect. Formal authority has been found to be one of the least effective forms of influence. Only by earning the respect of your staff as well as your patients can you be sure that your intent will be carried out when you are not present. Setting the example in performance and conduct, rather than ‘do as I say, not as I do,” level of activity enables one to exert influence far greater than titles.
Trust and challenge your employees – How many times have practices sought to hire the best and brightest only to second guess the employee. Eric Schmidt, the CEO of Google, describes his management philosophy as having “… an employee base in which everybody is doing exactly what they want every day.” Obviously there are certain policies and procedures, but at the same time, the leader enables decision making to the lowest possible level. This also enables employees to question why certain policies and procedures are still being followed when more effective and efficient methods are available. (How the Army Prepared Me to Work at Google, Doug Raymond, Harvard Business)
Internal Faults
The phrase “Physician, heal thyself” (Luke 4:23, King James Version) means that we have to attend to our own faults, in preference to pointing out the faults of others. The phrase alludes to the readiness of physicians to heal sickness in others while sometimes not being able or will to heal themselves. By the same token, it now is necessary for us to learn how to manage ourselves. It suggests that physicians, while often being able to help the sick, cannot always do so, and when sick themselves are no better placed than anyone else (Gary Martin, phrases.org.uk/meanings/281850.html, 2010).
Self Development
“We will have to learn how to develop ourselves. We will have to place ourselves outside the boundaries where we can make the greatest contribution. And we will have to stay mentally alert and engaged during a 50-year working life, which means knowing how and when to change the work we do” (Managing Oneself, Harvard Business Review – Jan. 2005 – pp 100-109, by Peter Drucker). Although one’s IQ and certain personality characteristics are more or less innate and appear to remain stable over time there are individual capabilities that enable leadership and can be developed. Enhancement of these capabilities can lead to the individual being able to carry out the leadership tasks of setting direction, gaining commitment, and creating alignment. These capabilities include self-management capabilities, social capabilities and work facilitation capabilities.
***
***
Assessment
Without question, while it is possible to cram for at test and graduate at the top of one’s class, that does not assure leadership ability. We all know at least one person who scores at the highest levels on cognitive measures but would be incapable of pouring liquid out of a boot if the instructions were written on the heel.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Dear David and ME-P Subscribers, Readers and Visitors
I hope this finds you well and busy. I am sure you are pleased with the publication of the updated text book. Thank you again for allowing me to participate by authoring Chapter 33: Professional Relations.
I am sending this along to my fellow consultants asking them to seek their client’s participation. I thought you might be able to post or push out to your ME-P readers.
The CHG
Corporate Health Group (CHG) is conducting our third benchmarking study on Physician Sales and Service. The success of this study depends on the survey being distributed to the appropriate people to be completed. Because I know that you have many contacts in physician sales and service, I am hopeful that you would forward the survey to those contacts and encourage them to participate. To show CHG’s appreciation you will receive a complimentary copy of the results including the trended data from the 2005 and 2008 studies.
Viral Contacts Sought
If you, or your subscribers and partners, should also happen to have a contact that is a large system or association we have the ability to set up a unique organization code that those completing the survey would enter in the “organization” section. CHG would in return give them a report that shows the overall trended data (2005, 2008, 2010) – compared to their organization’s data. If you want a code, please contact jstratton@corporatehealthgroup.com or 309-647-5456 for this set-up.
Contact Instructions
Instructions on sending the survey to your contacts:
1. Below you will find a brief description of the survey along with a html message that could be used in your communication to your contacts. In order to use the html embedded in this email you must “forward” the message. It is set-up so that you could “forward” the message and simply delete the top portion of this message.
2. If you are unable to forward this html message, I have created a link to the survey.
The Physician Sales and Service Survey
Physicians still direct the vast majority of inpatient healthcare in the marketplace – as many as 80% of patients enter the doors of hospitals and facilities at the direction of physicians. Notwithstanding he movement toward a consumer-driven market – many hospitals, health systems and large specialty practices have turned to physician sales or referral development programs to grow their business. Unfortunately, motivating physicians to change referral patterns is a daunting task under the best of circumstances and the lack of industry “best practices” complicates the situation even further.
Third Benchmarking Study
September 2010 Corporate Health Group (CHG) launched their third benchmarking study of Physician Sales and Service. The National survey will obtain new trends and craft comparisons and a gap analysis of data captured 2005, 2008 and now 2010. The survey (a mix of open and closed ended questions) is available online and respondents will get a free Executive Summary. The results will provide detailed management and benchmarking data for physician sales managers and healthcare executives to benefit their programs for future success!
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Due to high-profile concerns in terms of the variation in quality of care as well as its affordability, practice pattern measurement is here to stay. And, until further advances in this area are created, physicians with unexpectedly poor performance ratios, especially in the area of cost-efficiency, should review their data to determine if there are opportunities to improve as well as potential outlier cases contributing to an aberrant value, as well as looking at the health plan methodology for statistical analysis and outlier exclusions.
Communication is Key
It is important for the physician or other provider being measured to communicate any issues to health plan personnel where possible. Physicians need to remember that practice pattern analysis is a continually evolving field.
Assessment
Given the state of the art, physicians, specialty societies, and other advocacy groups have a responsibility to work with health plans or other practice measurement agencies to make sure quality improvement is at the forefront, that they are active in giving feedback on health plan practice measurement methods, and that as much as possible a collaborative approach is used in working with health plans and other measurement organizations.
Conclusion
And so, your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Few areas of life are as personal as an individual’s health and people have long relied on a caring and competent physician to be their champion in securing the medical resources needed to retain or restore health and function.
Nevertheless, this philosophy is currently in flux.
Foundation of Medicine
For many physicians, the care of patients was the foundation of their professional calling. However, in the contemporary delivery organization, there may be little opportunity for generalist physician “gatekeepers” or “specialty hospitalists or intensivists” to form a lasting relationship with patients. These institution-based physicians may be called upon to deliver treatments determined by programmatic protocols or algorithm-based practice guidelines that leave little discretion for their professional judgment.
Personal Values
In addition, the physician’s personal values may be impeded by seemingly perverse financial incentives that may directly conflict with their advocacy role, especially if a patient may be in need of expensive services that may not be covered in their insurance plan, or are beyond the resources of a patient’s HSA or savings account.
Assessment
Marcia Angell, MD., noted during a PBS interview that the “financial incentives directly affecting doctors…put them at odds with the best interests of their patients … and it puts ethical doctors in a terrific quandary.”
Conclusion
And so, your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Our Other Print Books and Related Information Sources:
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
One area where technology assessments, clinical guidelines, and EMR data can make a true difference in patient care is in disease management.
DMAA Definition
The Disease Management Association of America (DMAA) defines disease management as “a system of coordinated health care interventions and communications for populations with conditions in which patient self-care efforts are significant”. Disease management supports the physician-patient relationship and places particular significance on the prevention of exacerbations and complications of chronic diseases using evidence-based clinical guidelines and integrating those recommendations into initiatives to empower patients to be active partners with their physicians in managing their conditions.
Usual Conditions
Typically, targets for disease management efforts include chronic conditions such as asthma, diabetes, chronic obstructive pulmonary disease, coronary artery disease, and heart failure, where patients can be active in self-care and where appropriate lifestyle changes can have a significant favorable impact on illness progression.
Outcomes Measurement
The DMAA also emphasizes the importance of process and outcomes measurement and evaluation, along with using the data to influence management of the medical condition.
Assessment
Although claims and administrative data can be used to measure and evaluate selected processes and outcomes, EMRs will be needed to capture the full spectrum of data for analyzing illness response to disease management programs and to support necessary changes in care plans to improve both intermediate outcomes (such as lab values), and long-range goals (such as the prevention of illness exacerbations, managing co-morbidities, and halting the progression of complications).
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on September 7, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
ADVERTISEMENT
Transformational Health 2.0 Skills for Doctors
By Ann Miller; RN MHA
[Executive Director]
Revised and updated to include the most current information on healthcare administration, the Third Edition of The Business of Medical Practice is an essential business tool for doctors, nurses, and healthcare administrators; management and business consultants; accountants; and medical, dental, podiatry, business, and healthcare administration graduates, managers, and doctoral students.
Journalistic Style
Written in plain language using non-technical jargon, the text presents a comprehensive and progressive discussion of management and operation strategies. It integrates various medical practice business disciplines-from finance to marketing to the strategic management sciences-to improve patient outcomes and achieve best practices in the healthcare administration field.
Returning Contributors
Dr. Gary L. Bode; MSA, CPA, CMP™ [Hon]
Render S. Davis; MHA, CHE
Dr. Charles F. Fenton III; FACFAS, Esquire
Eric Galtress
Hope R. Hetico; RN, MHA, CMP™
Carolyn Merriman; FRSA
Dr. Brent A. Metfessel; MS
Rachel Pentin-Maki, RN, MHA, CMP[Hon]
Eugene Schmuckler; PhD, MBA, CTS
Patricia A. Trites; MPA, CHBC, CMP[Hon]
Exciting New Thought-Leaders
And, we seek to breathe additional diversity into this work with these new contributing authors:
Suzanne R. Dewey; MBA
Dr. Brian J. Knabe; CMP™
Parin Kothari; MBA
Mario Moussa; PhD, MBA
Shahid N. Shah; MS
Susan Theuns; PA-C
Jennifer Tomasik; MS
Topic Content and Chapters
With 37 chapters, 512 pages, and contributions by a world-class team of expert authors, this new edition – under the direction of Chief Editor Dr. David Edward Marcinko MBA – covers brand new information such as this partial list demonstrates:
Web 2.0 Technologies Impact on the Healthcare Industry
Office Location, Logistics, Layout and Execution
Internal Office Controls for Preventing Waste, Fraud and Abuse
Direct-Concierge Medicine and Niche Providers
Medical Workplace Violence and Sexual Harassment
Office Financial Statements and Analysis
Human Resources, Hiring, Firing and Office Staffing
Healthcare Marketing, Advertising, and Public Relations
Health Economics, Cost and Practice Managerial Accounting
Mico-Medical Practice Business Models
Incurred but Not Reported [IBNR] Healthcare Claims
Revenue Management, Coding and the Cash Conversion Cycle
Medical Professional Social Media and Collaborative patient care
Healthcare Compliance and Health Law Policies
The USA PATRIOT and SAR-BOX Acts
Physician Leadership, Communication, and Career Development
Patient Service Management and CRM + [plus]
Physician Compensation, Micro-Capitation with P-4-P Trend Analysis
Office Financial Statements and Analysis
Human Resources, Hiring, Firing and Office Staffing
Healthcare Marketing, Advertising, and Public Relations
EHRs, Mobile IT systems, Medical Devices, SaaS and Cloud Computing
Medical Ethics, Participatory Care and Moral Philosophy
Health Macro and Micro Economics and Finance
Medical Practice Sales and Succession Planning
Next-generation Physician Leadership
Obama Care American Recovery and Reinvestment Act [ARRA and HITECH]
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on June 21, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
Challenging Assertions
By Shahid N. Shah MS
As the physician executive of your medical practice, it’s your job to challenge any eMR vendors’ assertions about why you need an eMR, especially during the selection and production demonstration phase.
Information Availability [Anytime – Anywhere]
The most important reason for the digitization of medical records is to make patient information available when the physician needs that information to either care for the patient or supply information to another caregiver.
Electronic medical records are not about the technology but about whether or not information is more readily available at the point of need.
Reasons to Purchase?
In no particular order, the major reasons given for the business case of eMRs by vendors include:
• Increase in staff productivity
• Increase of practice revenue and profit
• Reduce costs outright or control cost increases
• Improve clinical decision making
• Enhance documentation
• Improve patient care
• Reduce medical errors
Assessment
So, doctors beware! Challenge vendor “authority.”
Editor’s Note
Shahid N. Shah is an ME-P thought leader who is writing Chapter 13: “Interoperable e-MRs for the Small-Medium Sized Medical Practice” [On Being the CIO of your Own Office] for the third edition of the best selling book: Business of Medical Practice [Transformational Health 2.0 Skills for Doctors] to be released this fall by Springer Publishers, NY. He is also the CEO of Netspective Communications, LLC.
And so, your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Mr. Shah and Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – are available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now:Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on June 16, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
On “Smart Phones” and Mobiles Devices
By Shahid N. Shah MS
M-Health or “mobile health” is an industry term for collectively defining those tools and technologies that can be used on “smart phones” like iPhone, Blackberry, Android, or on traditional mobile phones from various vendors.
Unlike traditional computers, almost every patient that walks into your medical office, as well as all your own staff, have mobile devices already. If you can find mobile applications that can help your practice you can immediately put to use without large capital expenses, network configuration, and other technical tasks.
According to the mHealth Initiative, there are 12 major “application clusters” in mobile health: patient communication, access to web-based resources, point of care documentation, disease management, education programs, professional communication, administrative applications, financial applications, emergency care, public health, clinical trials, and body area networks.
Almost all of these applications are focused around the patient but most of them will be directly useful to you and your staff as well. Here’s how:
Improving physician-patient communications. You can get your staff to send out text messages, e-mails, photos, and other information about your practice to the patient before their visit. You can remind them about appointments, tell them what to expect, ask them for their insurance and check-in information, or let them send you their personal health record link. During the visit you can send them patient education information directly to their phones instead of handing out paper. After the visit you can send medication reminders, additional educational resources, and update to their personal health record, or ask them to join a Health 2.0 social network. PumpOne, GenerationOne, Intouch Clinical, Life:Wire, and Jitterbug phones all have great patient user experiences and you should tell your patients about them.
Faster access to information for you and your patients. There are countless web-based resources that are now at your fingertips on a phone. Patients can lookup providers, labs, testing services, etc. that you can refer them to; you can help them join clinical trials, and manage their health records online. None of these require a computer either in your office or in their home, it can all be done on the phone. Check out companies like Healthagen and iSeek.
Real-time documentation of office or hospital visits. Most of the things you want to do in your EMR are possible on a smart phone today. You can get your patient profiles, document an encounter with basic order management and lab results review capabilities, and immediate storage into either your own EMR or your hospital’s information system.
Help those patients with the most time-consuming treatments. You already know that disease management is an important part of managing the health of chronic patients; diabetes and hypertension are two perfect examples. Help enroll your patients into Diabetes Connect, MediNet, HealthCentral, and similar applications that can help track compliance with your medical treatment guidance. If they use these applications they can simply give you printouts or login credentials so that you can track their progress without doing any data entry yourself. There are patient tools for most common diseases.
Editor’s Note
Shahid N. Shah is an ME-P thought leader who is writing Chapter 13: “Interoperable e-MRs for the Small-Medium Sized Medical Practice” [On Being the CIO of your Own Office] for the third edition of the best selling book: Business of Medical Practice [Transformational Health 2.0 Skills for Doctors] to be released this fall by Springer Publishing, NY. He is also the CEO of Netspective Communications, LLC.
And so, your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Mr. Shah and Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – are available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
In the piece, she profiles the newly created Society for Participatory Medicine, which “encourages patients to learn as much as they can about their health and also helps doctors support patients on this data-intensive quest,” as well as PatientsLikeMe.com, a free service which makes its money by selling anonymized patient information.
For more information, please visit our new companion blog for the: Business of Medical Practice [Transformational Health 2.0 Profit Maximizing Skills for Savvy Doctors] – third edition.
And so, your comments on this ME-P are appreciated. What are your thoughts on health 2.0? Are doctors worried? Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on January 6, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
And Textbook Contributor, Too!
By Ann Miller; RN, MHA
[Executive Director]
Shahid N. Shah is an internationally recognized healthcare thought-leader across the Internet. He is a consultant to various federal agencies on technology matters and winner of Federal Computer Week’s coveted “Fed 100” Award, in 2009.
Professional Career
Over a twenty year career, Shahid built multiple clinical solutions and helped design-deploy an electronic health record solution for the American Red Cross and two web-based eMRs used by hundreds of physicians with many large groupware and collaboration sites. As ex-CTO for a billion dollar division of CardinalHealth, he helped design advanced clinical interfaces for medical devices and hospitals. Mr. Shah is senior technology strategy advisor to NIH’s SBIR/STTR program helping small businesses commercialize healthcare applications.
Mr. Shah is a Microsoft MVP (Solutions Architect) Award Winner for 2007, and a Microsoft MVP (Solutions Architect) Award Winner for 2006. He also served as a HIMSS Enterprise IT Committee Member. Mr. Shah received a BS in computer science from the Pennsylvania State University and MS in Technology Management from the University of Maryland.
Assessment
Shahid is also contributing the chapter on HIT in the third edition of our book “Business of Medical Practice” [Transformational Health 2.0 Profit Maximization for Savvy Doctors], now in-progress www.BusinessofMedicalPractice.com
Channel Surfing
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on September 23, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
Eying Contemporary Medical Ethics in Healthcare Reform
By Render S. Davis; MSA, CHE
And, Staff Reporters
Not so long ago, a physician’s clinical judgment was virtually unquestioned. Now with the advent of clinical pathways and case management protocols, many aspects of treatment are outlined in algorithm-based plans that allied health professionals may follow with only minimal direct input from a physician. Much about this change has been good. Physicians have been freed from much tedious routine and are better able to watch more closely for unexpected responses to treatments or unusual outcomes and then utilize their knowledge to chart an appropriate response.
Restrictive Protocols
What is of special concern, though, is the restrictive nature of protocols in some managed care plans that may unduly limit a physician’s clinical prerogatives to address a patient’s specific needs. Such managed care plans may prove to be the ultimate bad examples of “cook book” medicine. While some may find health care and the practice of medicine an increasingly stressful and unrewarding field, others are continuing to search for ways to assure that caring, compassionate, and ethically rewarding medicine remain at the heart of our health care system.
And so, your thoughts and comments on this Medical Executive-Post are appreciated. How does the specter of HR 3200-3400 in the healthcare reform debate impact the concept of medical autonomy and professional ethics? Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Posted on July 19, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
And Suggestions for Improvement, Too!
By Ann Miller; RN, MHA
[Executive Director]
We love accolades at the ME-P, but we also love your suggestions for improvement, too. So, talk to us!If you participate, you can win a chance to receive a signed first-edition copy of the best-selling textbook: Business of Medical Practice.
Have you visited our channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on June 10, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
The “Art of the Deal” for Buyers and Sellers
By Dr. David Edward Marcinko; MBA, CMP™
Publisher-in-Chief
Are you considering selling your practice — or merging it with another? Thinking of buying? If you are, you’re hardly alone. Despite the decline of the big physician practice management companies [PPMCs] of the 1990s, the merger-and-acquisition market remains robust for small, private practices, as they respond to the continuing financial squeeze being placed on them, in 2009.
Humana’s YourPractice is a quarterly publication for office staff, physicians and other health care providers within the Humana network, and is produced by Corporate Communications in conjunction with “Physicians Practice”.
Note:David Marcinko is also a writer for Physicians Practice
Conclusion
And so, your thoughts and comments on this Medical Executive-Post are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com or Bio: www.stpub.com/pubs/authors/MARCINKO.htm
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Accordingly, we would be honored for you to consider contributing a new or revised chapter, in your area of expertise, for a low-effort but high-yield contribution. Our goal is to help physician colleagues and management executives benefit from nationally known experts, as an essential platform for their success in the healthcare 2.0 business industry. Many topics are still available: [health accounting and costing; law, policy and administration; Medicare fraud and abuse; coding and insurance; HIT, grid and cloud computing; finance and economics, competitive models, collaboration and leadership, etc].
Support Always Available
Editorial support is available, and you would enjoy increasing subject-matter notoriety, exposure and public relations in an erudite and credible fashion. As a reader, or preferably a subscriber to the ME-P, your synergy in this space may be ideal. Time line for submission of a 5,000-7,500 word chapter is ample, and in a prose writing style that is “wide, not deep.”
A Health 2.0 Initiative
And, be sure to address health 2.0 modernity. Update chapters from the second edition are also available.
Please contact me for more details, if interested. A best selling-book is rare; while a third-edition volume even more so. Join us in this project. Regardless, we trust you will remain apostles of our core ME-P vision, “uniting medical mission and financial profit margin”, promoting it whenever possible.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on February 9, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
An HIT Report from the Inner City Trenches
By Dr. David Edward Marcinko; MBA, CMP™
[Publisher-in-Chief]
While not an IT guru by any means, I am a prudent fan of health IT where appropriate, and have always been a bit on the curious side.
A Bit about Me
OK; I am a member of the American Health Information Management Association (AHIMA) and the Healthcare Information and Management Systems Society (HIMSS). I am also a beta-tester for the Microsoft Corporation, a member of the Microsoft Health User’s Group (MS-HUG) and the Sun Executive Boardroom program sponsored by CEO Jonathan Schwartz; as well as SUNSHINE [Solutions for Healthcare Information, Networking and Education [NASD/FINRA-JAVA]. I also was fortunate to just finish editing the Dictionary of Health Information Technology and Security, with Foreword by Chief Medical Information Officer Richard J. Mata; MD MS MS-CIS of Johns Hopkins University.
And, I was incredibly lucky to have my colleague Ahmad Hashem; MD PhD, who was the Global Productivity Manager for the Microsoft Healthcare Solutions Group at the time, to pen the Foreword to the second edition of my book, the Business of Medical Practice
And so, it was with the pleasure of potential intellectual satiety that goaded me into testing the airwaves, so to speak, on my recent visit to my home town of Bal’more. Thus, this exclusive ME-P report follows.
Location … Location … Location
If you lived in San Francisco a few years ago, during the ill-fated and costly WiFi experiment, you have my sincere condolences. If you live in Baltimore however, and want to have fast, wireless Internet speeds, then congratulations because you’ve chosen your place of residence wisely. Me, I’m an ex-patriot who was ecstatic when Sprint announced in October 2008, that Baltimore would be the first US city to have access to its new Wi-Max mobile data network; known as Xohm. I visit my home town 3-4 times, annually.
About the Wireless Xohm Data Network
Xohm is a wireless data service which, thanks to its WiMax capability, reportedly provides broadband-like speeds on a wireless PC. With this, as long as you have a WiMAX adapter and can pay for the service, the Internet should be available anywhere within the city. For home use, service for WiMAX costs $25 per month for six months, and $35 per month after that. Laptop access was to be $30 per month for the first six months. If you’re just visiting the city, single day access will cost $10, which is a bit steep, but not bad compared to the price of Wi-Fi access in some airports. Or, their unsecure networks were purported free; anywhere in the city. This was the object of my informal beta-testing activities.
City of Baltimore
My neighborhood, in Baltimore, is known as the historic Fell’s Point District. It was founded in 1670 by William Cole who bought 550 acres on the Inner Harbor, downtown. English Quaker, William Fell then bought land he named “Fell’s Prospect”. The land was also known as “Long Island Point” and “Copus Harbor”.
This area was the ideal hostile site for the Wi-Max experiment. The surrounding neighborhoods are composed of many dense, old-brick and stone-masonry buildings, with abundant large expanses of Chesapeake Bay with its related estuaries and inlets. Local gossip about the experiment suggested that if it was successful in this hostile Baltimore environment, it would like be successful in more modern American cities.
I used my daughter’s [age 12, eighth-grade] Dell Latitude D600 laptop PC, running a Windows XP professional downgrade, with an Intel® P4 micro-processor [1.4 GHZ, 512 MB, 30 GIG CD with 24X CD-RW/DVD] for data only. It was originally purchased used – not new – for a few hundred bucks and badly in need of some upgrades. For the test, we added 512 MB LT DDR PC-3200, and a wireless LINKSYS PCMCIA card [WPC54GX].
Network Results
First, set up was a snap. While the network is expansive, it was not exactly blazingly fast, at least not for unsecure roaming access. The network can provide “download speeds of 2 to 4 megabits per second“. While, it is faster than most cellular networks, the service is nothing compared to some home internet connections. Although, the option to use it on a laptop is useful, the 4 Mbps is good enough for checking email or other smaller, lower bandwidth internet surfing usages. It’s hard to say if these estimates actually hold up with a lot of people using the network at once, especially if you are far from a broadcast tower – or in a funky part of the city – which is everywhere. But, they seemed to work quite well. My daughter, wife and I were suitably impressed.
Of Medical PACS
Of course, we also talked to local town folk about their free unsecured use. All were pleased with the Baltimore experience. We found business, law, nursing and graduate school students who were ferocious users. We even found medical students using open network wireless PCAS. To the uninitiated, picture archiving and communication systems (PACS) are computers or networks dedicated to the storage, retrieval, distribution and presentation of digital radiology images. The medical images are stored in an independent format. The most common format for image storage is Digital Imaging and Communications in Medicine [DICOM].
Roll-Put in Other Cities
Apparently, Sprint plans on releasing Xohm WiMAX networks in Chicago and Washington DC, this year. While they are both major cities, it is hard to speak for just how well the WiMAX works when you’re sitting in Atlanta, GA. Should these networks actually get some decent use, perhaps the service will be released in more markets. I just don’t know.
About NETGEAR
Local Baltimore provider NETGEAR has been a worldwide leader of technologically advanced, branded networking products since 1996. Their mission is to be the preferred customer-driven provider of innovative networking solutions for small businesses and homes.
As an old city, Baltimore has a rich medical heritage. There is the University of Maryland School of Medicine, Dentistry, Nursing and Pharmacy. Up the street from the Inner Harbor are the famed Johns Hospital School of Medicine and the Kennedy School of Public Health. It is here where I played stickball, as a child, in the parking lot. Nevertheless, given the high demands of business networking security and emerging network management in the local, State and Federal space today, NETGEAR is reported to have an end-to-end solution to meet most agency needs. This did seem to be the case in my ad-hoc experiment. We always found an open channel, and dropped links were few and far between; usually while mobile or riding in an automobile, bus, train or high-rail transportation system.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES: