Blurring the Line between Medical Professionalism … and Mercantilism
By Dr. David Edward Marcinko; MBA, CMP™
[Publisher-in-Chief]
Concerns and complaints about pushy dentists are apparently becoming more numerous among consumers, as elective cosmetic treatments and marginally effective tests and modalities are increasingly available from the same providers that patients formerly turned to for unbiased dental advice and oral healthcare. All for a price!
http://www.msnbc.msn.com/id/37198272/ns/health-oral_health
So, enter the cosmetic [rank-and-file] dentists and the elective renaissance of the profession – at least economically. An entire industry has even sprung up teaching dentists how to sell various products, and up-sell related services and procedures.
[picapp align=”none” wrap=”false” link=”term=dentists&iid=166771″ src=”0163/1731b859-b744-4a0e-b055-a9e985ad8673.jpg?adImageId=12959860&imageId=166771″ width=”372″ height=”459″ /]
Root-Cause [pun intended]
Why is this happening? Economics of course! Dental profession success in eradicating cavities, caries and other common mouth disorders – which used to comprise 80% of dental procedures and income – is now a two-edge sword working against their financial self interests … damn!
In fact, I recall about three decades ago when the situation first became acute, as more than a few of our nation’s dental schools closed for lack of interest in matriculation. Right here in Atlanta, the prestigious Emory University School of Dentistry closed its doors while I myself was a patient there; and employed as a surgical resident at a nearby acute care hospital. Contemporaneous cocktail party talk and medical gossip centered on the “death of dentistry” as I exhaled a sigh of relief at my career choice.
Going forward, years later, far too many managed care contracts reimbursed so poorly that they became a loss-leader [access portal to a patient population] for dental practitioners. In other worlds, lose money or break-even on the covered services contract, but profit handsomely by offering [pushing] non-covered services to cohort contract members … and their sphere of influence.
One Word from Mrs. Robinson – Plastics
Plastic surgeons, of course, are still the doctors most commonly associated with non-covered and purely cosmetic and elective treatments such as Botox injections, facelifts and tummy tucks. But, similar elective procedures — which generally aren’t covered by insurance — are being offered by a wide variety of medical specialists.
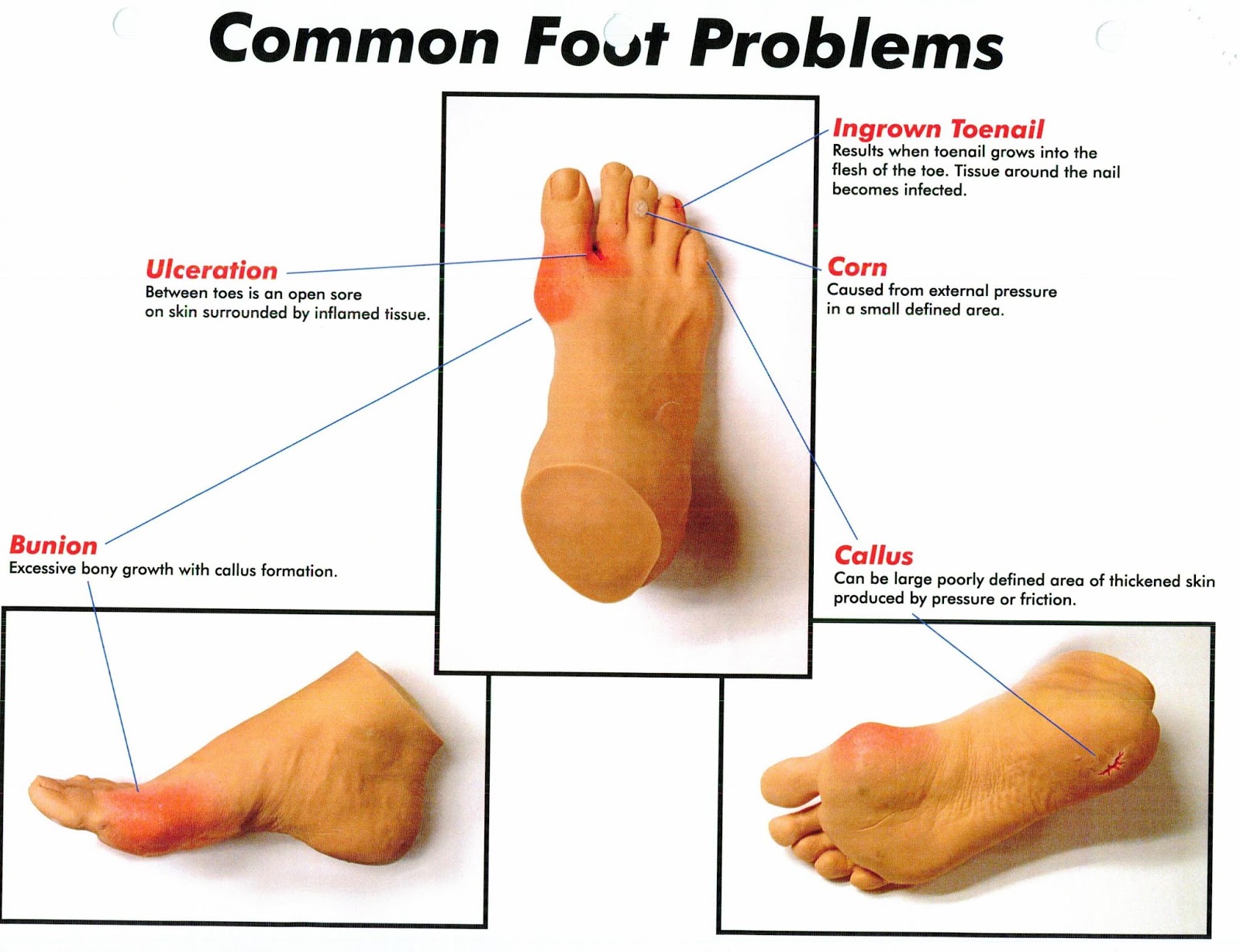
For example, many dermatologists, who treat patients for skin cancer and other diseases, also promote treatments to smooth wrinkles, lighten age spots and remove hair. Otolarnygologists, who care for patients with conditions of the ear, nose and throat, commonly perform nose jobs, brow lifts and eyelid surgery. And, podiatrists, who are often experts at foot reconstructive, diabetic and ankle surgery, sell shoes, shoe-inserts, laser beam treatments for fungus toenails and various cosmetic and prosthetic devices for deformed toenails and crooked digits.
Medicare Limits – Privates Don’t
At least Medicare requires an ABN [advanced beneficiary notice] for non-covered medical services, and limits non-participating doctors to 115% of the Medicare fee schedule for all providers. Increasingly, some private health plans are doing and proposing, same.
Practice Management Guru
Now, I have no issue with efficient medical practice management operations, for any specialty. In this era of managed care and health 2.0, governmental intervention is onerous, competition is fierce and patient empowerment is reversing the aging command-control medical establishment. Nor, do I have a problem with offering the entire range of therapeutic and/or elective options to any patient. This is a “good – better – best” elective marketing concept.
In fact, the third edition of our best-selling book, the Business of Medical Practice [Transformational Health 2.0 Skills for Doctors] will soon be released this autumn www.BusinessofMedicalPractice.com. In it, we seek to educate doctors about modern business, management and economics practices; as well as the emerging participatory health 2.0 philosophy and information technology skills. Our goal is enhancing the survival potential of the independent practicing medical professional.
But, the ever expanding menu of treatment options – promoted by a trusted medical professional – should include procedural risks and complications, period of recovery and alternatives, including benign neglect [watchful waiting], marginal benefit and marginal utility, as well as price transparency.
Call this new-wave litany, a type of “informed patient business consent”.
[picapp align=”none” wrap=”false” link=”term=doctor+money&iid=182012″ src=”0178/66353b45-9776-48b9-9bdd-2993a48f32bf.jpg?adImageId=12959922&imageId=182012″ width=”372″ height=”459″ /]
Aphorisms of the Past
Over the years, we have heard phrases like the following from all sorts of independent specialists. I know I have, and so have you. Many are the butt of “insider” jokes:
MD: I’m sure that appendix is hot – I have a car payment to make
DPM: Even the normal foot can be surgically improved
DO: Now, I can bill like a real MD
DDS: We can straighten out – the straightest teeth
DC: I’ll crack your back in only forty sessions … and I finance
But, these are aphorisms of the last-generation. Today we are responsible adults. Let’s grow up and become medical professionals and “DOCTORS” again … not healthcare merchants, sales sharks or equipment shills that offer strategic competitive advantages; but not real patient benefits.

Assessment
The old practice management business adage of yesteryear – to work longer hours, see more patients quicker, up-sell marginally effective procedures, or do more treatments in order to realize more income – will not necessarily hold true in the modern era.
http://www.washingtonpost.com/wp-dyn/content/article/2010/05/17/AR2010051703034.html
According to colleague, financial advisor and ME-P thought leader Brian J. Knabe MD – a primary care physician and current www.CertifiedMedicalPlanner.com matriculant – and textbook chapter 27 co-author on physician compensation and salary:
In the environment of Healthcare 2.0, those doctors who embrace efficiency, innovation and appropriate business models will be better positioned to optimize their incomes.
http://businessofmedicalpractice.com/chapter-27-salary-compensation-2/
Conclusion
Comments from our dental – and other – physician readers are requested. And, so are your general or specific thoughts on this ME-P. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Get our Widget: Get this widget!
Our Other Print Books and Related Information Sources:
Practice Management: http://www.springerpub.com/prod.aspx?prod_id=23759
Physician Financial Planning: http://www.jbpub.com/catalog/0763745790
Medical Risk Management: http://www.jbpub.com/catalog/9780763733421
Healthcare Organizations: www.HealthcareFinancials.com
Health Administration Terms: www.HealthDictionarySeries.com
Physician Advisors: www.CertifiedMedicalPlanner.com
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Sponsors Welcomed
And, credible sponsors and like-minded advertisers are always welcomed.
Link: https://healthcarefinancials.wordpress.com/2007/11/11/advertise
Filed under: "Doctors Only", CMP Program, Ethics, Op-Editorials, Quality Initiatives | Tagged: ABN, DDS, DMD, DO, DPM, MD, medicare, osteopaths, Otolarnygologists, podiatrists, Practice Management, www.BusinessofMedicalPractice.com, www.certifiedmedicalplanner.com, www.healthcarefinancials.com, www.healthdictionaryseries.com, www.medicalbussinessadvisors.com | 2 Comments »


































































































{kind=link}
{kind=link}
STUPID COMMENTS: Financial Advisors Say to Physician Clients
BY DR. DAVID EDWARD MARCINKO; MBA MEd CMP®
***
***
SPONSOR: http://www.MarcinkoAssociates.com
***
Some Stupid Things Financial Advisors Say to Physician Clients
A few years ago and just for giggles, colleague Lon Jefferies MBA CFP® and I collected a list of dumb-stupid things said by some Financial Advisors to their doctor, dentist, nurse and and other medical professional clients, along with some recommended under-breath rejoinders:
So, don’t let these aphorisms blind you to the critical thinking skills you learned in college, honed in medical school and apply every day in life.
COMMENTS APPRECIATED
Refer, Like and Subscribe
***
EDUCATION: Books
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
***
***
Share this:
Filed under: "Advisors Only", "Doctors Only", Ethics, Jokes and Puns, LifeStyle | Tagged: bears, bulls, crypto, DO, doctor clients, DPM, dumb comments, finance, financial advisors, financial planners, Investing, Lon Jefferies, Marcinko, MD, personal-finance, Physician Clients, physicians, Ponzi, stocks, stupid comments, Wall Street | Leave a comment »