BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
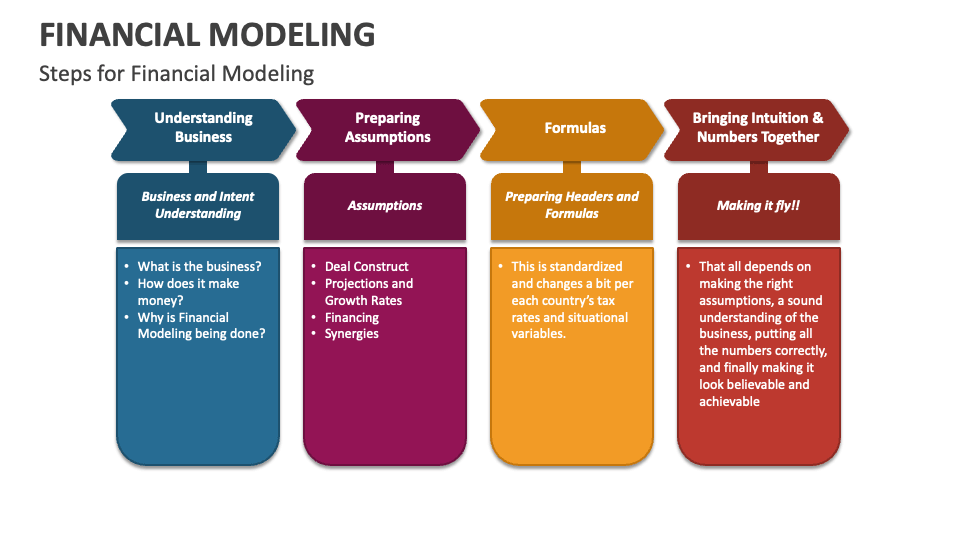
Financial Modeling is one of the most highly valued, but thinly understood, skills in financial analysis. The objective of financial modeling is to combine accounting, finance, and business metrics to create a forecast of a company’s future results.
According to Jeff Schmidt, a financial model is simply a spreadsheet, usually built in Microsoft Excel, that forecasts a business’s financial performance into the future. The forecast is typically based on the company’s historical performance and assumptions about the future and requires preparing an income statement, balance sheet, cash flow statement, and supporting schedules (known as a three-statement model, one of many types of approaches to financial statement modeling). From there, more advanced types of models can be built such as discounted cash flow analysis (DCF model), leveraged buyout (LBO), mergers and acquisitions (M&A), and sensitivity analysis
***
DEFINED TERMS
Discounted Cash Flow (DCF): A valuation method used to estimate the value of an investment based on its expected future cash flows, adjusted for the time value of money. It’s like deciding whether a treasure chest is worth diving for now, based on the gold coins you’ll be able to cash in later.
Sensitivity Analysis: This involves changing one variable at a time to see how it affects an outcome. Imagine tweaking your coffee-to-water ratio each morning to achieve the perfect brew strength.
Budget – A budget is the amount of money a department, function, or business can spend in a given period of time. Usually, but not always, finance does this annually for the upcoming year.
Rolling Forecast – A rolling forecast maintains a consistent view over a period of time (often 12 months). When one period closes, finance adds one more period to the forecast.
Topside – A topside adjustment is an overlay to a forecast. This is typically completed by the corporate or headquarter team. As individual teams submit a forecast, the consolidated result might not make sense or align with expectations. When this occurs, the high-level teams use a topside adjustment to streamline or adjust the consolidated view.
Monte Carlo Simulation: Picture yourself at the casino, but instead of gambling your savings away, you’re using this technique to predict different outcomes of your business decisions based on random variables. It’s like playing financial roulette with the odds in your favor.
What-If Analysis: Ever daydream about what would happen if you took that leap of faith with your business? This tool allows you to explore various scenarios without risking a dime. It’s like trying on outfits in a virtual dressing room before making a purchase.
Leveraged Buyout (LBO) Model: This is a bit like orchestrating a heist, but legally. It’s about acquiring a company using borrowed money, with plans to pay off the debts with the company’s own cash flows. High stakes, high rewards.
Mergers and Acquisitions (M&A) Model: Picture two puzzle pieces coming together. This model evaluates how combining companies can create a new, more valuable entity. It’s the corporate version of a matchmaker.
Three Statement Model: The holy trinity of financial modeling, linking the income statement, balance sheet, and cash flow statement. It’s like weaving a tapestry where each thread is crucial to the overall picture.
Capital Asset Pricing Model (CAPM): A formula that calculates the expected return on an investment, considering its risk compared to the market. It’s like choosing the best roller coaster in the park, balancing thrill and safety.
Cash Flow Forecasting: This is your financial weather forecast, predicting the cash flow climate of your business. It helps you plan for sunny days and save for the rainy ones.
Cost of Capital: The price of financing your business, whether through debt or equity. It’s like the interest rate on your growth engine, pushing you to maximize every dollar invested.
Debt Schedule: A timeline of your business’s debts, showing when and how much you owe. It’s your roadmap to becoming debt-free, one milestone at a time.
Equity Valuation: Determining the value of a company’s shares. It’s like assessing the worth of a rare gemstone, ensuring investors pay a fair price for a piece of the treasure.
Financial Leverage: Using debt to amplify returns on investment. It’s like using a lever to lift a heavy object, increasing force but also risk.
Forecast Model: A crystal ball for your finances, projecting future performance based on past and present data. It’s your guide through the financial wilderness, helping you navigate with confidence.
Operating Model: A detailed blueprint of how a business generates value, mapping out operational activities and their financial impact. It’s like laying out the inner workings of a clock, ensuring every gear turns smoothly.
Revenue Growth Model: This tracks potential increases in sales over time, charting a course for expansion. It’s like plotting your ascent up a mountain, anticipating the effort required to reach the summit.
Posted on April 10, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Stat: 5.06%. That’s how much Medicare payment rates will increase for 2026, doubling what was previously proposed. (the Wall Street Journal)
Quote: “The move displays the utmost disrespect for public service. It is clearly designed to force talented scientists and health experts to leave government. It is also an insult to those healthcare professionals in the Indian Health Service who dedicate their lives to providing healthcare services on tribal lands.”—Richard Besser, CEO of the nonprofit Robert Wood Johnson Foundation, on offers to reassign HHS workers on administrative leave to the Indian Health Service (NPR)
Read: Some psychologists are offering free or low-cost therapy for federal healthcare workers. (Stat)
US stocks rocketed higher on Wednesday as President Trump announced a 90-day pause on tariffs for most countries, yet at the same time upped increasingly ballooning levies on China.
The benchmark S&P 500 (^GSPC) roared up over 9.5%, posting its best day since 2008. The tech-heavy NASDAQ Composite (^IXIC) rallied a whopping 12% for its second-best day on record and its biggest gain since 2001. The Dow Jones Industrial Average (^DJI) was up over 7.8%, or roughly 3,000 points.
Posted on April 9, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Stat: 11%. That’s the share of US residents who said they couldn’t afford medical care or medication over a three-month period, according to a new Gallup survey. (the New York Times)
An epic stock-market bounce turned into a historic fizzle, extending the bruising selloff sparked by President Donald Trump’s sweeping tariff measures to a fourth straight session.
SPX-1.57% saw an intra-day gain of 4.05% evaporate to end with a loss of 1.6%, marking its biggest blown percentage gain since Oct. 14th, 2008, during the darkest days of the 2007-09 financial crisis. And it’s the first time the S&P 500 was up more than 4% at its intra-day high but finished with a loss of more than 1%, based on data going back to 1978, according to Dow Jones Market Data.
DJIA-0.84% rallied 1,461 points, or 3.85%, at its intra-day peak, but ended the day down more than 400 points, its biggest erased percentage gain since April 2020.The tech-heavy NASDAQ Composite.
Posted on April 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
e Department of Veterans Affairs announced plans last week to accelerate the rollout of its embattled electronic health records system. Lawmakers, meanwhile, continue to call for oversight despite concerns over the future of the modernization program. The VA added nine new medical facilities in Ohio, Kentucky, Indiana, and Alaska to the deployment schedule, along with four sites in Michigan that will launch in 2026 after the program expansion has largely been on hold since April 2023, when the agency acknowledged glitches in the system had contributed to at least four veterans’ deaths and “catastrophic harm” to others.
After a roller coaster day, the Dow closed lower by 349 points, or 0.91%. The broader S&P 500 fell 0.23%. The NASDAQ Composite was 0.1% higher after fluctuating between gains and losses. Wall Street’s fear gauge, the CBOE Volatility Index, or VIX, on Monday closed at the highest level since the Covid pandemic as investors fretted over the market’s next move. The VIX surpassed an intraday level of 50 points midday Monday, a rare level associated with extreme volatility.
Posted on April 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
WARNING – WARNING
By Dr. DavidEdwardMarcinko; MBA MEd
***
***
According to www.NPR.org, there are more than120,000 health care forums on the Internet with opinions ranging from pharmaceuticals, to sexual dysfunction, to acne. The same goes for commercial doctor blogs that promote lotions, balms and potions, diets and vitamins, minerals, herbs, drinks and elixirs, or various other ingest-ants, digest-ants or pharmaceuticals, etc.
And, to other doctors, the blogging craze is a new novelty where there are no rules, protocols, standards or precise figures on how many “medical-doctor” or related physician-blogs are “out there.” Unfortunately, too many recount gory ER scenes, or pictorially illustrate horrific medical conditions, or serious and traumatic injuries. Of course, others simply are medical practice websites, or those that entice patients into more lucrative plastic surgery or concierge medical practices. Some are from self-serving/credible plaintiff-seeking attorneys wishing to assist patients.
Not all physician blogs are geared toward practice information, marketing or medical sensationalism. In fact, just the opposite seems to be the case in extremely candid blogs, like “Ranting Docs”, “White Coat Rants,” “Grunt Docs”, “Cancer Doc,” “The Happy Hospitalist,” “Mom MD”, “Cross-Over Health”, “Angry Docs” and “M.D.O.D.,” which bills itself as “Random Thoughts from a Few Cantankerous American Physicians.”
According to some of these, they are more like personal journals, or public diaries, where doctors vent about reimbursement rates, difficult cases, medical mistakes, declining medical prestige and control, and/or what a “bummer” it is to have so many patients die; not pay, or who are indigent, noncompliant. We call these the “disgruntled doctor sites.” Some even talk about their own patients, coding issues, or various doctor-patient shenanigans.
But, according to psychiatrist and blogger Dr. Deborah Peel and others, the problem with blogging about patients is the danger that one will be able to identify themselves – the doctor – or that others who know them will be able to identify them.” Her affiliation, Patient Privacy Rights, rightly worries that patients might track back to the individual, and adversely affect their employment, health insurance or other aspects of life.
***
***
And, according to Dr. Jay S. Grife; MA Esq., it is certainly true that if a doctor violates a patient’s privacy there could be legal consequences. Under HIPAA, physicians could face fines or even jail time. In some states, patients can file a civil lawsuit if they believe a doctor has violated their privacy. Still, internet privacy issues are an evolving gray-area that if not wrong, may still be morally and ethically questionable [personal communication].
Our colleague Robert Wachter MD, author of the blog called “Wachter’s World,” says it’s important for doctors to be able to share cases, as long as they change the facts substantially. On the other hand, the author of “Wachter’s World” and a leading expert on patient safety alternately suggests “You might say we as doctors should never be talking about experiences with our patients online or in books or in articles.” But, he says that “patients shouldn’t take all the information on blogs at face value. Taken for what they are — unedited opinions, and in some cases entertainment — blogs can give readers some useful insight into the good, the bad and the ugly of the medical profession”. Link: http://www.the-hospitalist.org/blogs
Well, fair enough! But, doctors unhappy with their current medical career choice, or its modern evolution, should probably consider counseling or even career change guidance, re-education and re-engineering. It is very inappropriate to vent career frustrations in a public venue. It’s far better for the blog to be private and/or by invitation only; if at all [Personal communication].
We believe that a hybrid mash-up of both views can be wholly appropriate, or grossly inappropriate in some cases. Of course the devil is in the details; linguistics and semantics aside. Nevertheless; what is not addressed in electronic physician “mea-culpas” are the professional liability risks and concerns that are evolving in this quasi-professional, quasi-lay, communication forum.
***
***
Example: We have seen medical mistakes, and liability admissions of all sorts, freely and glibly presented. In fact,
“Some physicians find that the act of liability blogging as a professional confession that is useful in moving past their malpractice mistakes. And, it is also a useful way to begin a commitment to a better professional life of caring in the future. It helps eliminate the toxic residue and angst of professional liability and guilt. Moreover, as they are unburdened of past acts of omission or commission, doctors should remember to also forgive those who have wronged them. This helps greatly with the process and brings additional peace.”
However, although some may say that this electronic confession is good for the soul, it may not be good for your professional liability carrier, or you, when plaintiff’s attorneys release a legion of IT focused interns, or automated bots, searching online for your self-admissions and scouring for your self-incriminations. Of course, a direct connection to a specific patient may still not be made and no HIPAA violation is involved. But, a vivid imagination is not need needed to envision this type of blind medical malpractice discovery deposition query even now.
QUESTION:“Doctor Smith, I noted all the medical errors admitted on your blog. What other mistakes did you make in the care and treatment of my client?”
And so, the question of plausible deniability, or culpability, is easily raised. If you must journalize your thoughts for sanity or stress release; do it in print. And, don’t tell anyone about it so the diary won’t be subpoenaed. Then tear it up and throw it away. Remember, with risk management, “It is all about credibility.” Don’t trash yours! These thoughts may be especially important if you covet a medical career as a researcher, editor, educator, medical expert or something other than a working-class or employed physician.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on April 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Microsoft is reportedly pulling back on data center projects around the world as it reexamines its AI plans. Hershey reportedly bought the popcorn brand LesserEvil for $750 million.
US stocks cratered on Friday with the Dow Jones Industrial Average (^DJI) plunging more than 2,200 points after China stoked trade-war fears and Fed Chair Jerome Powell warned of higher inflation and slower growth stemming from tariffs.
The Dow pulled back 5.5% to enter into correction territory. Meanwhile, the S&P 500 (^GSPC) sank nearly 6%, as the broad-based benchmark capped its worst week since 2020. The tech-heavy NASDAQ Composite (^IXIC) dropped 5.8% to close in bear market territory.
Profitability ratios measure a company’s ability to generate income relative to revenue, balance sheet assets, operating costs, and equity. Common profitability financial ratios include the following:
The gross margin ratio compares the gross profit of a company to its net sales to show how much profit a company makes after paying its cost of goods sold:
Gross margin ratio = Gross profit / Net sales
The operating margin ratio, sometimes known as the return on sales ratio, compares the operating income of a company to its net sales to determine operating efficiency:
Operating margin ratio = Operating income / Net sales
The return on assets ratio measures how efficiently a company is using its assets to generate profit:
Return on assets ratio = Net income / Total assets
The return on equity ratio measures how efficiently a company is using its equity to generate profit:
Return on equity ratio = Net income / Shareholder’s equity
Posted on April 4, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
BREAKING US STOCK MARKET NEWS
By ME-P Staff Reporters
***
***
Stocks in the U.S. opened sharply lower on Friday, extending a slide from the previous trading session triggered by President Trump’s announcement of sweeping new tariffs on U.S. imports earlier this week.
The S&P 500 fell 144 points, or 2.5%, to 5,252 as of 9:34 a.m. EST. The Dow Jones Industrial Average tumbled 1,006 points, or 2.5%, and the NASDAQ Composite slid 3.1%.
The indexes’ free-fall Thursday was their biggest one-day drop since 2020, with more than $2 trillion in investor wealth erased from the S&P 500. The S&P 500 and Dow each sank more than 4% yesterday, while the tech-heavy NASDAQ plunged nearly 6%.
NOTE: Drops of this magnitude aren’t unheard of on Wall Street, but they’re rare. Over the last 25 years, the S&P 500 has fallen 4% in a single day 38 times, according to Adam Turnquist, chief technical strategist for brokerage firm LPL Financial.
Posted on April 4, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Roughly $2.5 trillion was erased from the S&P 500 Index on Thursday amid worries that President Donald Trump’s sweeping new round of tariffs could plunge the economy into a recession. The damage was heaviest in companies whose supply chains are most dependent on overseas manufacturing. Apple Inc., which makes the majority of its US-sold devices in China, fell 9.3%. Lululemon Athletica Inc. and Nike Inc., among companies with manufacturing ties to Vietnam, were both down more than 9%. Target Corp. and Dollar Tree Inc., retailers whose stores are filled with products sourced outside of the US, dropped more than 10%.
The tech-heavy NASDAQ Composite (^IXIC) led the sell-off, plummeting 6%. The S&P 500 (^GSPC) sank nearly 5%, while the Dow Jones Industrial Average (^DJI) tumbled 4%. The Dow’s 1,700-point drop was the fifth-worst in its history.
Posted on April 3, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
BREAKING NEWS – MARKET VOLATILITY
By Staff Reporters
***
***
US stocks nosedived on Thursday, with the Dow tumbling more than 1,200 points as President Trump’s surprisingly steep “Liberation Day” tariffs sent shock waves through markets worldwide. The tech-heavy NASDAQ Composite (IXIC) led the sell-off, plummeting over 4%. The S&P 500 (GSPC) dove 3.7%, while the Dow Jones Industrial Average (^DJI) tumbled roughly 3%. [ongoing story].
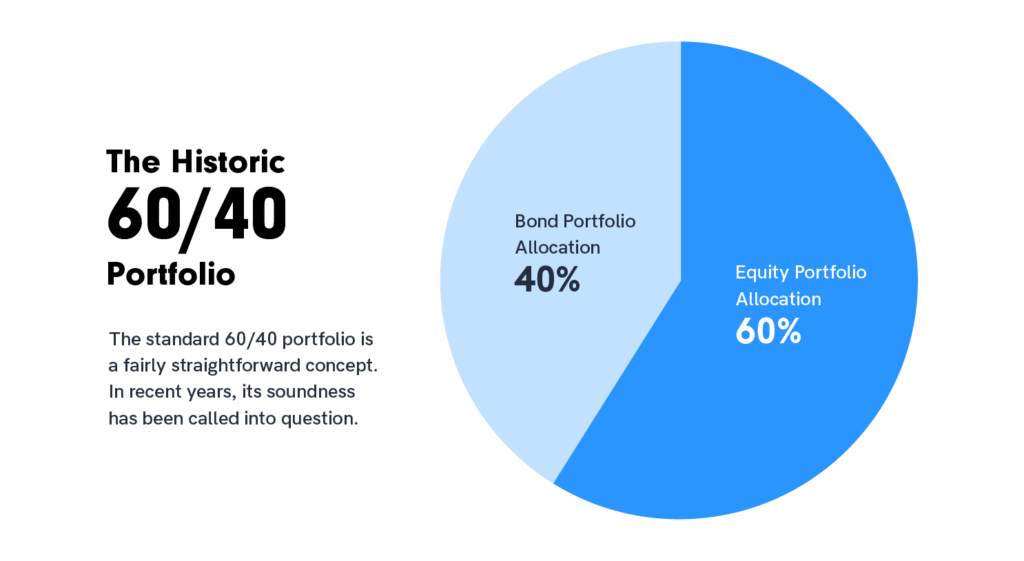
So, does the traditional 60 stock / 40 bond strategy still work or do we need another portfolio model?
***
The 60/40 strategy evolved out of American economist Harry Markowitz’s groundbreaking 1950s work on modern portfolio theory, which holds that investors should diversify their holdings with a mix of high-risk, high-return assets and low-risk, low-return assets based on their individual circumstances.
While a portfolio with a mix of 40% bonds and 60% equities may bring lower returns than all-stock holdings, the diversification generally brings lower variance in the returns—meaning more reliability—as long as there isn’t a strong correlation between stock and bond returns (ideally the correlation is negative, with bond returns rising while stock returns fall).
For 60/40 to work, bonds must be less volatile than stocks and economic growth and inflation have to move up and down in tandem. Typically, the same economic growth that powers rallies in equities also pushes up inflation—and bond returns down. Conversely, in a recession stocks drop and inflation is low, pushing up bond prices.
***
But, the traditional 60/40 portfolio may “no longer fully represent true diversification,” BlackRock CEO Larry Fink writes in a new letter to investors.
Instead, the “future standard portfolio” may move toward 50/30/20 with stocks, bonds and private assets like real estate, infrastructure and private credit, Fink writes.
Here’s what experts say individual investors may want to consider before dabbling in private investments.
It may be time to rethink the traditional 60/40 investment portfolio, according to BlackRock CEO Larry Fink. In a new letter to investors, Fink writes the traditional allocation comprised of 60% stocks and 40% bonds that dates back to the 1950s “may no longer fully represent true diversification.“
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Patient satisfaction occurs when patient perceptions exceed their expectations. They get an intangible “something extra” from their visit, above what they paid for. When patient expectations match their perceptions, mutual obligations are fulfilled, making both practitioner and patient “break-even”.
The clinical result, within a relevant range, is only part of the patient’s perceptions. Numerous sub-conscious impressions comprise the remainder. We’ve all had patients love us despite a less than optimal result. We’ve all had patients angrily leave the practice over some non-clinical matter like a trivial billing dispute. A patient’s perception of any health care service is colored by a vast array of prior experiences that set up current expectations. The patient is pleased to the extent that his current perceptions exceed his/her pre existing expectations. This encompasses far more than the clinical result (within a relevant range), and includes such non-treatment issues as the demeanor of the staff, condition of the physical premises, psychological comfort during the visit, etc.
Remember, all patients talk about you anyway. In the past, a happy patient told four others about what a nice doctor you are. Today, patients post website comments or blogs immediately after their visits. They are more likely to complete treatment and follow instructions, thus obtaining a better medical outcome, and, generating additional fees for the practice. They pay quicker, cause less bad-debt and help create a pleasant environment for us to work in.
An unhappy patient vehemently tells nine others, onground or online, what a nasty greedy rip-off artist you are. Sad, but true! They are not as likely to complete treatment, thus incurring a less than optimal result, and generate fewer fees. They pay slower, if at all, create a stressed environment and detrimentally affect the attitude of other patients in the office.
Try to eliminate problems that might cause negative perceptions (i.e., a filthy restroom) and implement controls that help assure positive perceptions. Patient satisfaction is a soft managerial science. It is a numbers game. Most patients don’t pre-define what would be “acceptable” from this encounter, but have vaguely defined ranges of prior expectations anyway, gleaned from a lifetime of health care related experience. Any variance between these this “acceptable” range of expectations and each trivial encounter invokes some degree positive or negative feeling in the patient.
***
***
The total perception of the office experience is an aggregate of multiple trivial, often subliminal, observations. Patient satisfaction is an intangible and amorphous process complicated by:
Inter patient variables: Significant differences between patients in their “expectations”. Intra patient variables: A single patient can perceive the same thing or situation differently at different times, depending on uncontrollable variables like mood, or, context of occurrence which may (sometimes and/or partially) be controllable by the practice. Luck of the draw” in physical variables: Does Sally or Mary escort the patient to the exam room? Was it the blue or green exam room? Did the last patient to use the rest room, five minutes ago, leave a disgusting mess? Heterogeneous staff variables: Even with appropriate training, people are not machines and have their own quirks.
ASSESSMENT
By proactively anticipating the entire visit, from the patient’s perspective, the practitioner can structure and arrange things such that most patients have, mostly positive perceptions, most of the time. This can be done despite all the potential hetero-genicity of the above factors. Patient satisfaction can be improved in any office, and can be done by anyone.
CONCLUSION
Because patient satisfaction is a multi-faceted amorphous subject, there are multiple correct approaches to the subject and no “cook book” recipe on how to proceed. Try and get the big picture. Identify the worst areas and fix them. Identify the best areas and reinforce them. Proceed slowly. It can be done one facet at a time. Adapt things to your own managerial style and personality. Be completely open to suggestion and change.
Finally, be aware that patient relationship and satisfaction implementation strategies frequently overlap.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on April 3, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Stocks looked like a very concerning EKG recently, fluctuating throughout as investors weighed today’s tariff announcement. The Newsmax meme stock kept on surging, stacking a 180% gain on top of Monday’s 735% spike to skyrocket over 900% since the conservative media outlet went public earlier this week.
U.S. stocks whipped through another dizzying day Wednesday in the final hours before President Donald Trump’s unveiling of the tariffs promised as part of his “Liberation Day,” which could drastically remake the global economy. The S&P 500 rose 0.7%, but only after careening between an earlier loss of 1.1% and a later gain of 1.1%. It’s had a pattern this week of opening with sharp drops only to finish the day higher.
The Dow Jones Industrial Average added 235 points, or 0.6%, and the NASDAQ composite climbed 0.9%. Both also veered from sharply lower in the morning to sharply higher in the afternoon before doubling back.
Mass layoffs at health agencies begin. The purge of thousands of Health and Human Services (HHS) employees announced last week by Secretary Robert F. Kennedy Jr. started yesterday, with senior leaders at the FDA, CDC, and other departments saying they had been pushed out. Among those removed were the FDA’s chief tobacco regulator, its top veterinarian, and medical officers in charge of new drug approvals.
f you like to use Zelle to send money to others, you need to find a new solution. On April 1st, the digital payment app shut down.
Visualize: How private equity tangled banks in a web of debt, from the Financial Times.
A hedge fund is a limited partnership of private investors whose money is pooled and managed by professional fund managers. These managers use a wide range of strategies, including leverage (borrowed money) and the trading of nontraditional assets, to earn above-average investment returns. A hedge fund investment is often considered a risky, alternative investment choice and usually requires a high minimum investment or net worth. Hedge funds typically target wealthy investors.
QUESTION:Can I invest my Individual Retirement Account [IRA] in a Hedge Fund?
This is up to the manager, but there is no legal restriction on a hedge fund accepting individual retirement account (IRA) assets. IRA accounts are not well suited for funds that make extensive use of leverage, however. In such cases, the fund is likely to generate significant amounts of unrelated business taxable income (UBTI) – profits of the fund attributable to the use of leverage. The holder of an IRA account must pay taxes on UBTI, even if the UBTI was generated in an IRA account.
But, today’s hedge funds may or may not use leverage. Many hedge funds are not hedged at all, but rather are just specialized versions of regular long stock portfolios. If such funds do not use much leverage, IRA investors will not encounter much difficulty with UBTI and should not hesitate in considering these funds.
In considering whether to accept IRA money, hedge fund managers must consider several factors. If the only type of retirement money accepted by the hedge funds is IRA money, then the manager has no limit on how much retirement money the fund can accept. If, however, there are other types of retirement money invested in the fund, such as pension funds, IRA money will be counted towards a total of 25 percent of fund assets that can be invested in retirement accounts before the fund becomes subject to the Employment Retirement Income Security Act of 1974 (ERISA). Funds subject to ERISA regulations face a heavy administrative burden and more restrictions than most fund managers like.
Finally, IRA distributions from a hedge fund are subject to the standard 20 percent withholding unless the funds are directly rolled over to other qualified plans.
Posted on April 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The CEO of a Texashealth insurance company was fired after admitting before a DOGE panel of state lawmakers that he hired private investigators to spy on customers and obtain sensitive details about their lives. Mark Sanders was dismissed from his duties as chief executive of Austin-based Superior HealthPlan after he testified before the Texas House Delivery of Government Efficiency Committee in a hearing on Medicaid procurement last week.
US stocks closed mixed on Tuesday as investors cautiously counted down to President Trump’s highly anticipated “Liberation Day” rollout of sweeping new reciprocal tariffs. The S&P 500 (^GSPC) rose about 0.4%, extending the gains the benchmark index secured on Monday, while the Dow Jones Industrial Average (^DJI) fell just below the flatline. The tech-heavy NASDAQ Composite (^IXIC) rebounded to close up around 0.9%.
Suppose that in a new Accountable Care Organization [ACO] contract, a certain medical practice was awarded a new global payment or capitation styled contract that increased revenues by $100,000 for the next fiscal year. The practice had a gross margin of 35% that was not expected to change because of the new business. However, $10,000 was added to medical overhead expenses for another assistant and all Account’s Receivable (AR) are paid at the end of the year, upon completion of the contract.
Cost of Medical Services Provided (COMSP):
The Costs of Medical Services Provided (COMSP) for the ACO business contract represents the amount of money needed to service the patients provided by the contract. Since gross margin is 35% of revenues, the COMSP is 65% or $65,000. Adding the extra overhead results in $75,000 of new spending money (cash flow) needed to treat the patients. Therefore, divide the $75,000 total by the number of days the contract extends (one year) and realize the new contract requires about $ 205.50 per day of free cash flows.
Assumptions
Financial cash flow forecasting from operating activities allows a reasonable projection of future cash needs and enables the doctor to err on the side of fiscal prudence. It is an inexact science, by definition, and entails the following assumptions:
All income tax, salaries and Accounts Payable (AP) are paid at once.
Durable medical equipment inventory and pre-paid advertising remain constant.
Gains/losses on sale of equipment and depreciation expenses remain stable.
Gross margins remain constant.
The office is efficient so major new marginal costs will not be incurred.
***
***
Physician Reactions:
Since many physicians are still not entirely comfortable with global reimbursement, fixed payments, capitation or ACO reimbursement contracts; practices may be loath to turn away short-term business in the ACA era. Physician-executives must then determine other methods to generate the additional cash, which include the following general suggestions:
1. Extend Account’s Payable
Discuss your cash flow difficulties with vendors and emphasize their short-term nature. A doctor and her practice still has considerable cache’ value, especially in local communities, and many vendors are willing to work them to retain their business
2. Reduce Accounts Receivable
According to most cost surveys, about 30% of multi-specialty group’s accounts receivable (ARs) are unpaid at 120 days. In addition, multi-specialty groups are able to collect on only about 69% of charges. The rest was written off as bad debt expenses or as a result of discounted payments from Medicare and other managed care companies. In a study by Wisconsin based Zimmerman and Associates, the percentages of ARs unpaid at more than 90 days is now at an all time high of more than 40%. Therefore, multi-specialty groups should aim to keep the percentage of ARs unpaid for more than 120 days, down to less than 20% of the total practice. The safest place to be for a single specialty physician is probably in the 30-35% range as anything over that is just not affordable.
The slowest paid specialties (ARs greater than 120 days) are: multi-specialty group practices; family practices; cardiology groups; anesthesiology groups; and gastroenterologists, respectively. So work hard to get your money, faster. Factoring, or selling the ARs to a third party for an immediate discounted amount is not usually recommended.
3. Borrow with Short-Term Bridge Loans
Obtain a line of credit from your local bank, credit union or other private sources, if possible in an economically constrained environment. Beware the time value of money, personal loan guarantees, and onerous usury rates. Also, beware that lenders can reduce or eliminate credit lines to a medical practice, often at the most inopportune time.
4. Cut Expenses
While this is often possible, it has to be done without demoralizing the practice’s staff.
5. Reduce Supply Inventories
If prudently possible; remember things like minimal shipping fees, loss of revenue if you run short, etc.
6. Taxes
Do not stop paying withholding taxes in favor of cash flow because it is illegal.
Hyper-Growth Model:
Now, let us again suppose that the practice has attracted nine more similar medical contracts. If we multiple the above example tenfold, the serious nature of potential cash flow problem becomes apparent. In other words, the practice has increased revenues to one million dollars, with the same 35% margin, 65% COMSP and $100,000 increase in operating overhead expenses.
Using identical mathematical calculations, we determine that $750,000 / 365days equals $2,055.00 per day of needed new free cash flows! Hence, indiscriminate growth without careful contract evaluation and cash flow analysis is a prescription for potential financial disaster.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on April 1, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
US stocks rebounded Monday to cap a volatile month and quarter as trade-war worries mount in the run-up to President Trump’s tariff bonanza later in the week.
The tech-heavy NASDAQ Composite (^IXIC) closed down about 0.1%, while the S&P 500 (^GSPC) recuperated losses of as much as 1.7% to close up nearly 0.6%. The Dow Jones Industrial Average (^DJI) erased early morning losses to gain 1%, or about 400 points.
Markets wrapped up March on a woeful note after a rough month and quarter beset by Trump’s fast-evolving tariff policy. Last week was the fifth in six weeks that the NASDQ Composite and S&P 500 ended the week in the red. The benchmark index is down over 4.5% to start the year while the NASDAQ has lost over 10%, finishing with their worst quarters since 2022.
Some of the biggest-name megacaps have led the decline. NVIDIA (NVDA) fell Monday as it has neared a 20% loss so far this year, while TESLA (TSLA) has lost more than 35%.
Posted on March 31, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
[Reviewing Terms, Conditions and Selling Agreements]
By Dr. Charles F. Fenton III JD
***
***
Dealing with many issues concerning the actual contract that affect the purchase or sale of a medical practice can be daunting. For example, this chapter will not deal with issue of determining whether or not a physician should retire. Nor will it determine the proper Fair Market Value [FMV] of the practice. However, physicians may be assisted in both instances by a medically focused financial advisor, or valuation specialist. [AVA, CPA-CVA, Certified Medical Planner™; etc] working in conjunction with an experience health care contract attorney to act as an advocate and determine certain contingencies that might occur, and protect him/her from them.
THE PARTIES
The first determination is whether the party at interest is an individual, group of individuals, or an entity (such as a partnership, limited liability partnership, limited partnership, limited liability company, or corporation – whether an S corporation, C corporation or a professional corporation). In many instances, even if the party at interest is an individual is an entity, the individual or individuals behind the entity should be made parties to the agreement.
From the buyer’s perspective, the purchase of a medical practice is a highly person-oriented business. The practice value depends much upon the personality of the current treating physicians. If the current treating physicians are also the owners of the entity, then binding those individuals (especially as applies to the restrictive covenant) is of primary importance.
If the current treating physicians are not owners of the entity, but rather employees, then a determination of whether they will continue in their same positions or whether the buyer will be taking over the treatment of patients becomes the prime focus. If the current treating physicians will be continuing in their same positions, then their current employment contract must be reviewed to determine whether the rights of the seller will accrue to the buyer.
If the rights of the seller will not accrue to the buyer, then the Purchase and Sale Agreement must have a provision that makes the continued employment of those current-treating physicians a condition to consummation of the sale. In such instances, the new employment agreement might be an exhibit to the main agreement and executed contemporaneously with the main agreement.
If the current treating physicians will not be continuing in their same position and if the purchaser will be assuming treatment of the patients, then the main agreement must provide for the dissolution of the employment agreement and provision must be made for restricting the ability of those physicians from competing with the buyer. If the employment contract with the seller contains a restrictive covenant, then the buyer must ensure that such covenants will accrue to the buyers benefit. Otherwise, the buyer should insist that those physicians sign restrictive covenants. In such an instance, a portion of the purchase price may need to be allocated towards the consideration for those restrictive covenants and paid directly to those physicians.
DATE OF AGREEMENT AND CLOSING DATE
In general, it usually does not matter when the agreement is dated. It should usually be dated once all the terms are agreed to and the parties desire to bind each other and to be bound. In certain instance, the parties may have reached an agreement, but certain issues (such as the obtaining of a state license to practice medicine) may be outstanding. In such a case, then an option can be given by either the seller or the buyer to bind the other to sell or buy the practice upon exercise of the option. Giving an option can also push the agreement date into the future. The option will usually be given with token consideration (e.g., one hundred dollars) and will have a fixed expiration date (e.g., thirty to ninety days).
The determination of the closing date is more important than the date that the agreement is dated. Just like in the purchase of a house where certain issues (such as obtaining a mortgage and home inspection) must occur before closing, in the purchase of a practice, there may be certain issues which require time to undertake before the actual transfer can be consummated. For example, the buyer may still need to obtain financing or the landlord may need to approve the assignment of the lease.
RECITALS
The recitals – or “whereas” clauses – traditionally enunciate the reasons the parties are entering into the agreement. In the sale of the practice the recitals may simply state that the buyer wishes to buy the practice and the seller wishes to sell the practice. Yet, there is a modern growing tendency among contract attorneys to eliminate the “whereas” clauses as some attorneys feel that such language is antiquated. In such instances, the agreement will simply have a paragraph or two delineation of the “Purpose” of the agreement.
ARTICLES, SECTIONS, AND PARAGRAPHS
The agreement will often be divided and numbered in some logical fashion, either into articles, sections, paragraphs, or a combination of these. The reason for doing so is twofold. First, it allows ready reference to the numbered paragraph, and secondly it allows the agreement to be divided and grouped in logical associations.
BINDING THE PARTIES
The first paragraph of the first article will often bind the seller to sell and the buyer to buy the practice under the terms of the agreement. The rest of the agreement simply spells out those terms.
WHAT IS PURCHASED?
The agreement must disclose the items which are being transferred and the items which are not considered part of the agreement. This section should be crystal clear, so that anybody reading the contract (and hence a court which may be called upon to enforce the contract) and not privy to the preliminary negotiations will know what is part of the agreement and what is not part of the agreement.
[1] Sale of Stock vs. Sale of Assets
In most cases, well-informed financial advisors [FAs] will recommend that the buyer solely purchase the assets of the practice and not the stock of the practice. By purchasing selected assets, the buyer is ensured that he will not become responsible for the known or unknown liabilities of the corporation. In prior days, avoiding purchasing the stock of the corporation was a wise recommendation.
However, with the advent of managed care, the purchase of the stock of the corporation can provide the new practitioner with certain competitive advantages. It may take a new practitioner three to nine months to get onto enough managed care panels to make the practice profitable. Purchase of the stock of the corporation ensures the new practitioner of acquiring the Federal Tax Identification Number [TIN], Personal Identification Number [PIN], Drug Enforcement Agency [DEA], Centers for Medicare and Medicaid [CMS], Global Location Number [GLN] , National Provider Identifier [NPI], HIE-Form 834 transmission number, Durable Medical Equipment Number [DME] etc, of the corporate entity. Since most managed care corporations identify providers by the Federal TIN, purchase of the stock of the corporation should allow the new practitioner to be enrolled on managed care panels in a shorter period of time.
[2] Items Purchased
Items purchased often lists the tangible and intangible property of the seller which will be transferred to the buyer. Such items often include:
A detailed inventory of the tangible assets to be purchased;
A detailed listing of the inventory of the practice;
The names and addresses of all of the patients of record treated by the seller;
The patient medical records maintained by seller;
The computer records maintained by seller;
All licenses, permits, accreditation and franchises issued by any federal, state, municipal, or quasi-government authority relating to the use, maintenance or operation of the practice, running to or in favor of seller, but only to the extent that they are accepted by buyer;
All of sellers’ right, title, and interest in and to all real estate and equipment leases, if any, services agreements, employment and professional service contracts relating to the practice but only to the extent that the foregoing are accepted by buyer;
Assignment of lease should be attached and be incorporated to the agreement;
All existing telephone numbers used in connection with the operation of the practice and all yellow page advertising of the practice; and
The goodwill of the practice, which includes seller’s assistance and cooperation in transfer of all sellers’ rights and interests in the practice to buyer and any other intangible assets of the practice not listed in any other category.
Certain items purchased, such as [paper or electronic] medical records, governmental licenses, fax, email, website and telephone numbers have special considerations as discussed below.
[3] Medical Records
The seller should protect its future need to use the transferred patient medical records. In the current managed care environment, providers are subject to strict scrutiny. Even after leaving practice the provider may find himself subject to a government or third party audit or subject to a medical malpractice lawsuit. Therefore, the provider should ensure that the contract allows for him to take future possession of the specific medical record(s) of the practice in order to mount an appropriate defense.
[4] Governmental Licenses
Certain government licenses and permits may be nontransferable. These would include items such as the federal and state employer identification numbers, as these are unique to seller as a corporate entity. Likewise, other items unique to seller include Medicare identification numbers, Medicaid identification numbers, NPIs and UPINs. The buyer would have to purchase the stock of the corporation order to acquire such items, which is another advantage of a stock transaction versus an asset transaction. Likewise, some local business licenses may or may not be transferable.
[5] Telephone and Fax Numbers, Website URLs and Twitter [X] Accounts, etc
Transference of the telephone numbers often requires that a special local telephone company form authorizing transfer of the telephone numbers to the buyer. Often the new owner of the telephone number will also become liable for any current yellow page advertisement monthly fees. It is the same with an URL or website or e-mail address or office Twitter X account, etc.
[6] Items Not Purchased
Items not purchased or “excluded items” often list the personal items of the parties or of the employees of the parties. Such items would often include:
All cash on hand or on deposit;
All accounts receivable generated prior to the closing date;
All prepaid expenses, utility deposits, tax rebates, insurance claims, credits due from suppliers and other allowances after Closing Date;
The personal effects, including but not limited to photographs, diplomas, uniforms, books, mementos, memorabilia, personally owned art and any personal property owned by them;
Life insurance, disability insurance, and disability buy-out insurance on seller;
Motor vehicles used in connection with the practice;
Any or all tangible-intangible assets used in conjunction with another practice of seller; and
All other assets owned by seller other than those specifically described as items purchased.
The exact items transferred will often depend upon the prior negotiations of the parties. For example, the parties may have agreed that the accounts receivable will be transferred with the practice. In such an instance, the accounts receivable will be listed as an item to be purchased.
PURCHASE PRICE AND TERMS
The price of the transaction (or the value of the practice) is often the one item that is aggressively negotiated between the parties. That is because both the buyer and the seller are overly concerned with “how much?” As this chapter demonstrates, there are a lot more details that go into the negotiation and final contract than just the price. The buyer or seller would be doing themselves a disservice to consider the other factors simply “lawyer details.” Many additional terms of the agreement should be considered by one side or the other as “walk-way” conditions. The party that fully adheres to their additional terms is likely to find the other party capitulating to them. This is because the other party will most likely be fixated on the price.
The purchase price should be delineated in the agreement. Furthermore, the method of payment of the purchase price should be delineated. Although the usual method of payment would be cash, there are other methods available as well.
Cash payment can be made by an official bank cashier’s check, by a certified check, by deposit of funds into an escrow account, or by other method agreed upon by the parties.
Non-cash type transactions include loan agreements and exchanges. Exchanges can provide certain tax benefits if the exchange is a “like kind” exchange. A like kind exchange would occur when parties swap practices. For example, a group practice might have several offices. As part of the breakup of the group, the parties might exchange their stock of one office for all of the stock of another office. Like kind exchanges have strict guidelines that must be adhered to or the tax advantages will disappear. The reader is cautioned to get current legal and financial advice prior to the time of exchange.
It is in the seller’s best interest to get all cash at the time of closing. Then the seller can walk away and not worry about the success or failure of his predecessor. The seller will not have to worry about collecting periodic payments. The seller will not have to worry about placing the buyer in default or about eventually having to repossess the practice and begin to practice medicine at that office again. If a seller repossesses a practice, the buyer may have driven the patients away or lost the managed care contracts (why else would the buyer not be able to honor the loan agreement?). So the repossessed practice will have a significantly lower market value – if it is even marketable at that time.
On the opposite end of the spectrum, it is in the buyer’s best interest to get long and lean loan terms. First, by getting loan terms, the buyer will often have to come up with much less initial capital. Second, because of the discussion in the preceding paragraph, the seller has a vested interest in ensuring that the buyer succeeds once the practice changes hands.
If the transaction involves a seller-financed loan, then the agreement should specify the terms. Additionally, a separate loan agreement and security agreement should be attached as exhibits to the agreement. Finally, in order to perfect the security agreement, the lien should be recorded at the local courthouse in accordance to local rules and customs.
***
***
ALLOCATION OF PURCHASE PRICE
The final purchase price will actually be the amalgamation of various assets of the practice. Those assets include the tangible and intangible assets. The tangible assets include the hard assets (such as computers, treatment tables, chairs and furniture, DME and x-ray machines, etc) and the soft assets (such as Q-tips, paper and cotton balls). The intangible assets will include going concern value, goodwill, and the value of any restrictive covenant.
The parties should delineate the allocation of the purchase price amongst those various categories to reach a mutual best fit with the potential tax obligations. The buyer is the one who should strive to make the allocation fit his needs as best as possible.
Generally, the sale of the assets will be ordinary income to the seller and taxed at the seller’s usual rate. The buyer will be able to depreciate the purchased items. However, the characterization of those assets and the allocated portion of the purchase price will determine how much can be depreciated and over what time period the items can be depreciated.
As a general rule, soft assets can be depreciated fully in the year of purchase. Generally, hard assets can be depreciated over a three to seven year time period, depending upon the class of the asset. Also, under Section §179, a certain dollar amount can be “expensed” or deducted in the year of purchase. The sooner and the faster that the assets can be deducted the less current taxes that the buyer will be required to pay. However, intangible assets generally must be deducted over a 15-year period. This prolongs the tax benefits of any payments characterized as such.
Nonetheless, purchase of the assets results in better tax consequences that purchase of the stock of the practice. When stock is purchased, there is no depreciation allowance allocated in the current or subsequent years. Instead, the cost of the stock becomes the “basis” of the buyer in the practice. Any gain or loss from that basis will only have tax benefits or tax consequences in the year that the stock is sold or becomes worthless.
Because of the tax consequences of the characterization of the allocations of the purchase price, it is important that the agreement delineate the portion of the practice price which is allocated to each category. Each party should further agree never to claim a different allocation in any future tax filings. Generally, the soft and hard assets will be valued at their current actual cash value. In no event should the purchase price allocated to the soft and hard assets exceed the actual initial cost that the seller paid for the item. The only exception to the foregoing would be if the sale involved the transfer of an appreciable asset.
LEASE ASSIGNMENT
The agreement should provide that upon closing that the seller will assign the lease to the buyer. The buyer then acquires possession of the premises and assumes responsibility for the lease payments.
Sellers often do not understand that even though they do not practice at the leased premises and even though the buyer is making the lease payments, that the seller still remains liable to the landlord under the original lease. Usually this does not present a problem for the seller. But if the buyer abandons the premises or stops making the lease payments, then the landlord will look to the seller for the lease payments through the expiration of the lease.
If the seller has signed a restrictive covenant, then the seller may find himself in the unenviable position of making lease payments for the premises and prohibited from practicing at the premises. The seller should protect himself from this possibility. Therefore, the seller should ensure that the original agreement contains a provision that if the seller becomes liable under the lease that the seller can enter onto the premises, take possession of the practice and the practice assets and can practice medicine at the location until the seller’s liabilities are extinguished.
INDEMNIFICATION AND EXCLUSION/INCLUSION OF LIABILITIES
During the sale of a medical practice, each party will have certain liabilities that the other party should not assume and should not be required to assume. A mutual indemnification clause will act to ensure that each party remains liable for its own liabilities.
In a medical practice, the most common liability is a claim of medical malpractice against the provider. The seller has an interest in insuring that he is not liable for any claim brought by a patient that resulted after he leaves the practice and the buyer has an interest in insuring that she is not liable for any claim brought by a patient that resulted before she acquired the practice.
There are other areas of liability in the sale of a medical practice that may not be readily apparent. These include premise liability (e.g., slip and fall claims), employment claims (e.g., unemployment liability, sexual harassment, discrimination, and wrongful termination claims), tax claims (e.g., unpaid employment taxes and income or sales tax liabilities), and third party payer claims (e.g., Medicare recoupment claims). Consult your insurance agent to determine whether you can obtain insurance coverage to limit your liability under these clauses.
Medical practitioners should understand the full risk of signing an indemnification or hold harmless clause. If a claim is brought against the other party, then the party giving indemnification can be forced to pay any judgment or settlement incurred by that other party. The party giving indemnification can even be required to pay the other party’s attorney bills. This is an important point that the reader should consider carefully: Even if the other party successfully defends a claim, the indemnifying party can be held liable for the other party’s attorney’s fees. Since attorney fees can mount up rapidly, the indemnifying party can find itself responsible for thousands or even tens or thousands of dollars of attorneys’ fees.
If at all possible, one should never sign an indemnification agreement, whether in the sale of a medical practice, a managed care contract, or even a home security monitoring contract. Sometimes, one has no choice but to assume the risk and sign the contract. If at all possible, one should strive to sign such clauses in a corporate capacity and not in an individual capacity. If that is not possible, then seek insurance to minimize the risk. Indemnification clauses and the potential unlimited risk that they pose is one reason why the professional should undertake a carefully planned asset protection program.
***
***
OTHER FACTORS AND CLAUSES
[A] Integration
As a general rule, once parties have seen fit to put their agreement in writing, then no prior oral agreement regarding the same subject is binding. A paragraph stating that the written agreement contains the entire understanding of the parties simply reflects this rule of contract construction. Such a paragraph also places the parties on notice that any oral representation of the other party that has not been placed in the contract will be worthless.
[B] Construction
At times a court may hold any ambiguities in a contract against the party that prepared the agreement or that had the agreement prepared for them. If the party on the other side of the contract is an individual that was not represented by counsel and especially if that party has had very little business experience (such as a physician or medical provider recently in practice), courts are much more likely to hold ambiguities against the drafter of the agreement.
A paragraph regarding the construction of the agreement and stating that the agreement was formed from negotiation (as opposed to a “take-it-or-leave-it” proposition) can identify for any court constructing the contract that the court should not hold any ambiguities against the drafter. After all, even with negotiated contracts, one party or the other draws up the agreement.
[C] Choice of Law
In the United States today, it is common for parties in different states to have business dealings with each other. Likewise, in the sale of a medical practice, the buyer may begin negotiations in one state and then move to the practice state after consummation of the sale. In a similar vein, following the sale the buyer may move to another state.
In most cases, the various state laws should be similar on the contractual issues involved in the sale of a medical practice. However, a statement in the contract identifying the state whose laws will govern the contract will eliminate one possible source of dispute involving a side issue to the contract. In the vast majority of contracts, the laws of the state where the practice is physically located should be chosen by the parties to govern the contract
[D] Choice of Venue
Just like providing for choice of law, a side issue to the contract can be eliminated by choosing ahead of time the venue to resolve any conflicts that may arise. The venue is simply the place where the conflict will be decided. In most cases, the parties should choose the trial court of the county in which the practice is located.
[E] Survival of Obligations
An agreement to purchase a medical practice contains two aspects. First is the transference of the practice assets in exchange for the purchase price. Second are the various other terms, such as preservation of the medical records. By providing that these obligations survive the closing, each party is assured that the other party will not claim that the actual closing of the agreement extinguished the rights of the parties under the agreement.
[F] No Waiver Clause
A provision providing that a party does not waive its rights unless such a waiver is committed to writing allows a party to be a “nice guy” without risking its future rights. In some instances, if a party does not insist upon full compliance by the other party, then the first party may be considered to have waived its rights and may have no recourse against the other party.
There may be instances when the forbearance to exercise a right under the contract will benefit both parties. For example, if the buyer cannot pay the seller an installment on time, the seller may agree to extend the time for payment of that installment. The no waiver clause allows the seller to refuse to extend the time for payment of a future installment. Without the clause the buyer might be able to argue that the seller had waived its future rights to timely payments.
[G] Notices
There may be various reasons under the contract why one party may need to give a notice to the other party. Most often such notice will be that a party is claiming that the other is in breach of some provision of the agreement.
By specifying the address and method of delivery of any notice, the sending party can be assured that a court will rule that the receiver had actual or constructive notice.
Such a provision should also provide that one type of notice would be a change of address. Such a change of address notification would then supersede the address delineated in the agreement.
In most cases, the agreement should provide that the counsel to the party would receive a copy of any notice. This accomplishes two goals. First, there is a greater likelihood that the receiving party would receive actual notice. If the receiving party had moved and had failed to provide notice of the change of address, then the party’s counsel would have received the notice. Secondly, the party’s counsel would have received the notice in a timely manner and could take any immediate action that may be necessary.
[H] Severability Clause
A severability clause helps to ensure that if one provision is held by a court to be illegal or unenforceable, then the offending clause will be stricken from the agreement and the parties will be held to the agreement without the clause.
Without a severability clause, if a court finds that one provision of the agreement illegal or unenforceable, then the court has the power to strike down the entire agreement. Although even with a severability clause a court could strike down the entire agreement, the severability clause tells the court that the intent of the parties was that only the offending clause be stricken and essentially asks the court to honor the parties’ intent.
[I] Further Assurances Clause
After execution of the agreement, the parties may discover that certain other documents are necessary to complete the transaction. Unless such documents materially change the meaning and purpose of the agreement, a further assurance clause requires the party of parties to execute and deliver the document.
***
***
CLOSING – SETTLEMENT
The closing or settlement date should be chosen for a mutually time and place. Generally the date will be between 30 and 90 days from the execution of the agreement. This will allow the buyer and the seller adequate time to complete any conditions precedent to closing. At closing, the buyer will tender to the seller the agreed upon funds and will execute any loan and security agreements required under the purchase and sale agreement. If the restrictive covenant also contains a buyer’s covenant, then the buyer will execute that document. The seller will deliver to the buyer a bill of sale for the assets of the practice, will execute the restrictive covenant, will deliver the keys to the practice, and will surrender the assets and the premises to the buyer. Both the buyer and the seller will execute the lease assignment.
Many of the provisions of the agreement will survive the closing. This includes any agreement to prorate expenses not allocated in at the closing, the restrictive covenant agreement, the indemnifications, and any seller’s right maintained in the medical records.
TRANSITION
Both the seller and the buyer have certain interests to protect after the closing which would require the seller to stay with the practice for a period of time following the closing. The seller may have ongoing treatment plans with certain patients (such as post-operative follow-up treatment). The agreement should specify that the seller be allowed to continue at the practice location for the purpose of finishing such treatment plans. Although the buyer may be fully capable of completing such treatment plans, both the buyer and seller should be cognizant that the patient may claim abandonment. Allowing the seller to complete treatment plans in progress will mitigate against any perceived or actual claims of abandonment.
The buyer will want to require the seller to stay with the practice for a certain period of time, usually between three to six months. During that time, the seller will act to introduce the buyer to the current patients and the buyer will begin treatment of any new patients to the practice. In this way, the transition will appear smooth and natural to the current patients.
Of course, during the transition period, the seller will have the right to be paid by the buyer. To avoid misunderstanding, the method of payment should be reduced to writing. Usually the rate of compensation will be the profit margin percentage of the practice allocated to all income collected from the seller’s efforts during the time period in question. An astute negotiator might be able to require the seller to function during the transition period as an implicit condition for the payment of the practice price.
RESTRICTIVE COVENANTS
As part of the purchase price the buyer is paying for intangible assets of the practice. A medical practice is a highly individual based business. The practice depends in large part upon the reputation of the selling physician. For that reason, the buyer must ensure that the seller cannot use that highly individualized asset to compete against the practice for which she has just paid a high sum. The restrictive covenant protects this interest of the buyer.
A restrictive covenant actually contains several covenants to protect the buyer’s interests. These include not only the obvious covenant not to compete, but also a covenant regarding financial interests, a covenant regarding solicitations, and a covenant regarding proprietary information.
The first covenant is the covenant not to compete. In this covenant, the seller agrees not to compete with the practice in the geographic area during the time term of the agreement. This covenant prohibits the seller from actually practicing or from practicing indirectly. For example, the seller could not set up a clinic within the geographic area during the time period and employ a nurse practitioner to treat patients under his medical license.
The next covenant would be the covenant regarding financial interests. In this covenant, the seller is prohibited from investing in a competing business (i.e., medical practice), within the geographic area during the time period. This provision prevents the seller from investing in such a medical practice, even if he does not directly treat patients at that location.
The third covenant would be the covenant regarding solicitation. In this covenant the seller agrees not only to refrain from contacting patients of the practice during the time period, but also to refrain from contacting employees of the practice. If the seller maintains another office location which will not be sold, then the seller should ensure that the agreement provides that the seller is allowed to treat patients which find themselves to that practice location. Otherwise, the seller may be liable for patient abandonment and may also violate managed care contracts.
A final covenant would be a covenant regarding proprietary information. Simply by the fact of operating the practice, the seller has obtained certain proprietary information about the practice. This includes patient lists, accounting information, managed care contracts, and forms and handbooks. The seller should be prohibited from using such knowledge to the detriment of the practice.
[A] Time and Distance
The time and distance covered by the restrictive covenants must be reasonable. If either the time or distance is unreasonable, then a court might strike down the entire restrictive covenant.
A reasonable time is usually between two to five years. A two-year time period should be the minimum that the buyer should insist upon. The purpose of the time period is to allow sufficient time for the practice patients to consider the buyer as their “doctor” and to lose confidence in the selling doctor. For that reason, any time period over five years is likely to be considered an unreasonable restraint.
On the other hand, a reasonable distance depends upon many individual factors. A reasonable distance in an urban area like New York City would most likely be completely unreasonable in rural areas, such as rural Iowa. In most metropolitan areas, a five to ten mile radius from the practice location is likely to be considered reasonable. In rural areas, an entire county or even several contiguous counties may be considered reasonable. The main determination of the reasonableness of the distance factor is the total area from which the practice draws its patients.
Most practice management software programs allow for delineation of the practice patient base determined by zip code. That will provide the parties a starting point from which to negotiate the distance factor of the restrictive covenant.
[B] Buyer’s Covenants
The restrictive covenant should also contain buyer’s covenants, although it may seem counterintuitive that the buyer, having paid the seller tens of thousands of dollars for the practice, should be required to sign buyer’s covenants. However, a buyer’s covenant is an important part of the restrictive covenant. Under the purchase agreement, the seller might retain the right to repossess the practice, the practice assets, and the premises. This is most likely to happen when the seller finances the purchase price and the buyer defaults on the payments. It can also happen when the seller assigns the lease to the buyer and the buyer either abandons the premises or otherwise causes a default under the lease. The seller then remains liable as principle under the lease.
For those reasons, the restrictive covenant should provide that if the seller is required to enter onto the premises and take possession of the practice, then the Seller is relieved of his obligations under the restrictive covenants and the buyer now becomes bound by those same obligations. Such buyer’s covenants will prevent the buyer from abandoning the practice and then setting up a nearby competing practice.
CORPORATE RESOLUTION
Most medical practices being sold are corporate entities. If the transaction is a sale for stock, then the transaction is between private parties – the buyer paying cash and the seller transferring the stock.
However, in those cases where the buyer is purchasing the assets of the corporate practice, then the corporation must take certain prerequisite steps. Generally, a corporation, through its officers and directors, is prohibited from selling significant assets without permission of the shareholders.
For that reason, a shareholder meeting must be held and the shareholders at that meeting must approve a resolution allowing the officers and directors to sell significant assets of the corporation.
ASSESSMENT
The contract regarding the sale of a medical practice is the final agreement of the parties. Such a contract should only be executed after sufficient investigation into the practice and upon consultation with proficient professionals, including attorneys, accountants, FAs and practice management consultants. Understanding the basic terms and conditions of a contract regarding the sale of a medical practice is the first step in successfully negotiating the best agreement possible. Before one can negotiate for a certain provision, one must first be aware of the possibility of such a provision and its possible ramifications.
So, what else can FAs and consultants do to help plan properly for the sale of a medical practice, physician succession planning, and this major life liquidity event? Some experience FAs suggest constructing a “dry run template analysis” so the doctor can envision what life will be like after the sale, and what their corresponding financial needs might be. When the practice is sold, life is very different because many expenses that the practice paid become expenses the doctor now must pay. And so, the use of an astute financial advisor, practice valuation specialist, and healthcare contract attorney is highly advised.
CONCLUSION
As we have seen, the purchase price of a medical practice, although am important part of any sale, should only be considered one element of the negotiations. There are many clauses and provisions of a contract regarding the sale of the medical practice, which if not negotiated favorably should be considered factors to initiate the party to walk away from the sale.
Boundy, Charles: Business Contracts Handbook Gower Pub, NY 2010
Fenton, CF: Contracts Regarding the Sales of a Medical Practice. Financial Planning for Physicians and Healthcare Professionals; Aspen Publishers, New York, NY, 2003.
Hekman, K: Buying, Selling & Merging a Medical Practice. Keneth Hekman, New York 2008.
Walker, Lewis: The Ultimate Transition. Financial Advisor, page 33, 2014.
Schatzki, M: Negotiation Speak: Winning Words and Phrases for Sales, Purchasing, Contract and Other Business Negotiations – All the Dialogue and Skills You Need to Come Out Ahead, Dynamic Negotiations, Chicago, IL 2009.
UCC, Commercial Contracts and Business Law Blog: LexisNexis 2010.
Merger risk arbitrage, while a subset of a larger strategy called event-driven arbitrage, represents a sufficient portion of the market-neutral universe to warrant separate discussion.
Merger arbitrage earned a bad reputation in the 1980s when Ivan Boesky and others like him came to regard insider trading as a valid investment strategy. That notwithstanding, merger arbitrage is a respected strategy and when executed properly, can be highly profitable. It bets on the outcomes of mergers, takeovers and other corporate events involving two stocks which may become one.
Example:
A classic example is acquisition of SDL Inc. (SDLI) by JDS Uniphase Corp (JDSU). On July 10, 2010 JDSU announced its intent to acquire SDLI by offering to exchange 3.8 shares of its own shares for one share of SDLI. At that time, the JDSU shares traded at $101 and SDLI at $320.5. It was apparent that there was almost 20 percent profit to be realized if the deal went through (3.8 JDSU shares at $101 are worth $383 while SDLI was worth just $320.5).
This apparent mispricing reflected the market’s expectation about the deal’s outcome. Since the deal was subject to the approval of the U.S. Justice Department and shareholders, there was some doubt about its successful completion.
Risk arbitrageurs who did their homework and properly estimated the probability of success bought shares of SDLI and simultaneously sold short shares of JDSU on a 3.8 to 1 ratio, thus locking in the future profit. Convergence took place about eight months later, in February 2011, when the deal was finally approved and the two stocks began trading at exact parity, eliminating the mis-pricing and allowing arbitrageurs to realize a profit.
***
***
Hedge Fund Research defines the strategy as follows:
Merger Arbitrage,also known as risk arbitrage, involves investing in securities of companies that are the subject of some form of extraordinary corporate transaction, including acquisition or merger proposals, exchange offers, cash tender offers and leveraged buy-outs. These transactions will generally involve the exchange of securities for cash, other securities or a combination of cash and other securities. Typically, a manager purchases the stock of a company being acquired or merging with another company, and sells short the stock of the acquiring company. A manager engaged in merger arbitrage transactions will derive profit (or loss) by realizing the price differential between the price of the securities purchased and the value ultimately realized when the deal is consummated. The success of this strategy usually is dependent upon the proposed merger, tender offer or exchange offer being consummated.
When a tender or exchange offer or a proposal for a merger is publicly announced, the offer price or the value of the securities of the acquiring company to be received is typically greater than the current market price of the securities of the target company. Normally, the stock of an acquisition target appreciates while the acquiring company’s stock decreases in value. If a manager determines that it is probable that the transaction will be consummated, it may purchase shares of the target company and in most instances, sell short the stock of the acquiring company. Managers may employ the use of equity options as a low-risk alternative to the outright purchase or sale of common stock. Many managers will hedge against market risk by purchasing S&P put options or put option spreads.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on March 29, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
What exactly is an Expert Witness?
At D.E.Marcinko & Associates an “expert witness” possesses specialized knowledge in a particular field and is qualified to provide deposition or testimony in court and under oath. This testimony can be based on their personal experience, education, training and/or research. The role of an expert witness is to provide objective and unbiased opinions, analysis, and insights to help a lawyer, judge and/or jury understand technical or complex issues related to the case.
An expert witness can be called by either the prosecution or the defense in a legal case. The expert witness may be required to provide a written report or affidavit detailing their opinions, analyses and conclusions, and they may be asked to testify in court to provide oral testimony and answer questions from the judge and lawyers.
Posted on March 29, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
EDITOR-IN-CHIEF
By Dr. David Edward Marcinko; FACFAS MBA MEd
***
***
NATIONAL PHYSICIANS WEEK
National Physicians Week sets out March 25-31 to honor the healers dedicated to the art of medicine. In 2017, National Physicians Week highlighted the shortage of physicians in the United States against a growing landscape of minorities joining the ranks.
#NationalPhysiciansWeek
“In hindsight, I am proud of what we have accomplished in a short period of time, including raising the recognition of our group and spotlighting the years of sacrifice by those in our profession to serve our patients. We are poised to initiate actionable efforts to engage and educate our physician community.”
Cite: Dr. Kimberly Funches Jackson, President
Today in 2025, let’s explore the invaluable contributions of physicians, celebrate their hard work during National Physicians Week, and highlight the essential role that locum doctors play in enhancing healthcare delivery.
A Week to Honor All Physicians
National Physicians Week is a celebration of the remarkable work that doctors do every single day. From diagnosing complex conditions to providing life-saving treatments, physicians dedicate themselves to improving the health and well-being of their patients. It’s a week for healthcare professionals, patients, and communities to come together and show appreciation for the doctors who make a difference in our lives.
Physicians work long hours, face immense pressure, and make critical decisions daily. Their contributions go beyond the walls of the hospital, as many are also involved in research, teaching, and community outreach.
So, this week, it’s important to acknowledge not only their professional expertise but also the compassion and resilience they exhibit in their work.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on March 29, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Dr. Jay Bhattacharya is officially the new NIH director. The Senate voted to confirm the Stanford University professor’s appointment on March 26 in a 53–47 vote. Marty MakaryMD was also confirmed as FDA commissioner in the same hearing in a 56–44 vote. The appointments come as additional “healthcare disruptors,” alongside Robert F. Kennedy Jr.’s confirmation as HHS secretary and Mehmet Oz’s nomination as head of the Centers for Medicare and Medicaid Services. The nominees have faced backlash from the medical community following their controversial stances on topics like vaccinations and alternative medical practices.
The Dow Jones Industrial Average (^DJI) dropped more than 700 points or nearly 1.7%, while the benchmark S&P 500 (^GSPC) fell almost 2%. The NASDAQ Composite (^IXIC) dropped 2.7% as tech stocks led the declines.
As noted above, the major averages fell on Friday after the release of a hotter-than-expected Personal Consumption Expenditures index reading, which includes the Federal Reserve’s preferred inflation gauge of “core” PCE. The reading showed prices increased more than expected last month, rising 0.4% month over month and 2.8% year over year, continuing a stubborn plateau on the path to the Fed’s 2% target.
Visualize: How private equity tangled banks in a web of debt, from the Financial Times.
Both median and average family net worth surged between 2019 and 2022, according to the U.S. Federal Reserve. Average net worth increased by 23% to $1,063,700, the Fed reported in October 2023, the most recent year it published the data. Median net worth, on the other hand, rose 37% over that same period to $192,900.
You might wonder why the average and median net worth figures are so different. That’s because when you take the average of something, you add together every value in a data set and then divide that figure by the number of individual values.
When calculating a median, you simply look at the middle figure within a data set. That said, an average figure can be significantly higher or lower than a median figure if there are extreme outliers – meaning a group of people with significantly more net worth than the rest of the group can bring the average higher.
Average Net Worth by Age
The average net worth of someone younger than 35 years old is $183,500, as of 2022. From there, average net worth steadily rises within each age bracket. Between 35 to 44, the average net worth is $549,600, while between 45 and 54, that number increases to $975,800. Average net worth surges above the $1 million mark between 55 to 64, reaching $1,566,900.
Average net worth again rises for those ages 65 to 74, to $1,794,600, before falling to $1,624,100 for the 75 and older group. The median net worth within every single age bracket, however, is much lower than the average net worth.
***
***
Physicians [MD/DO]Net Worth by Specialty
A 2023 Medscape report shows the top 10 specialties with the most survey respondents saying they are worth more than $5 million.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on March 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Health and Human Services Secretary Robert F. Kennedy Jr. is expected to announce 10,000 employees will be cut, the Wall Street Journal reported today—the latest round of layoffs in the Trump administration’s push to slash the size of the federal workforce.
US stocks slid lower on Thursday after President Trump pushed ahead with hefty new tariffs on auto imports, stoking concerns about a potential full-on trade war and global economic harm. The S&P 500 (^GSPC) and the Dow Jones Industrial Average (^DJI) fell just over 0.3% on the heels of a losing day for the major gauges. The tech-heavy NASDAQ Composite (^IXIC) led the losses, falling more than 0.5%.
An important concept for all medical professionals to understand is the current rate of return (CCR).
According to this principle, the current rate of a taxable return must be evaluated in reference to a similar non-taxable rate of return. This allows you to focus on your portfolio’s real (after-tax return), rather than its’ nominal, or stated return.
Now, since most medical professionals own a combination of both vehicles, it is important to calculate the average rate of return (ARR), as demonstrated in the following matrix. Usually, this will result in the assumption of more risk, for the possibility of great return.
To compare after tax yields, with taxable yields, use the following formulas:
Tax equivalent yield = yield / (1 – MTB), while taxable yield X (1-tax rate) = tax exempt yield.
Example: if the yield on a tax exempt municipal bond was 6%, and you are in a 28% tax bracket; the equivalent taxable yield (ETY), is 8.3%, calculated in the following manner: 06 / 1.00 – .28 =.083, or, 8.3% ETY. This means that you would need a taxable instrument paying almost 9 % to equal the 6 percent tax exempt bond.
Posted on March 27, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Over the next decade, advances in artificial intelligence will mean that humans will no longer be needed “for most things” in the world, says Bill Gates. That’s what the Microsoft co-founder and billionaire philanthropist told comedian Jimmy Fallon during an interview on NBC’s “The Tonight Show” in February. At the moment, expertise remains “rare,” Gates explained, pointing to human specialists we still rely on in many fields, including “a great doctor” or “a great teacher.”
US stocks closed sharply loser Wednesday as President Trump prepared to unveil new tariffs on US auto imports. The benchmark S&P 500 (^GSPC) was down more than 1.1%, while the Dow Jones Industrial Average (^DJI) fell about 0.4%. The tech-heavy NASDAQ Composite (^IXIC) led the losses, sliding over 2%. Tech leaders Nvidia (NVDA) and Tesla (TSLA) both closed down more than 5%.
It’s a shocking fall for 23andMe that once boasted a $6 billion valuation in 2021—despite never making a profit. As of Friday, it was worth $50 million, and on Monday, shares for the consumer genetic testing pioneer fell 50% to 88 cents, Reuters reported.
Visualize: How private equity tangled banks in a web of debt, from the Financial Times.
*** Several years ago we noted that far too many mid-career, mature and physician clients using traditional stock brokers, management consultants and “financial advisors”, seemed to be less successful than those who went it alone. These Do-it-Yourselfers [DIYs] had setbacks and made mistakes, for sure. But, the ME Inc,. doctors seemed to learn from their mistakes and did not incur the high management and service fees demanded from general or retail one-size-fits-all “advisors.”
In fact, an informal inverse related relationship was noted, and dubbed the “Doctor Effect.” In other words, the more consultants an individual doctor retained; the less well they did in all disciplines of the financial planning, professional portfolio and investing continuum.
Of course, the reason for this discrepancy eluded many of them as Wall Street brokerages and wire-houses flooded the media with messages, infomercials, print, radio, TV, texts, tweets, and internet ads to the contrary. Rather than self-learn the basics, the prevailing sentiment seemed to purse the holy grail of finding the “perfect financial advisor.” This realization was a confirmation of the industry culture which seemed to be: Bread for the advisor – Crumbs for the client!
And so, we at the the Institute of Medical Business Advisors Inc. (iMBA), and this Medical Executive-Post, formed a cadre’ of technology focused and highly educated doctors, financial advisors, attorneys, accountants, psychologists and educational visionaries who decided there must be a better way for their healthcare colleagues to receive financial planning advice, products and related management services within a culture of fiduciary responsibility.
We trust you agree with this ME Inc philosophy as illustrated in this free white paper available upon request.
PROFESSIONAL PORTFOLIO CONSTRUCTION [Investing Assets and their Management] Subscribe, Read, Like and Refer
Email whiote paper request here:MarcinkoAdvisors@outlook.com
Without proper internal accounting controls, a medical practice [MD, DO, DPM, DDS, DMD] might never reach peak profitability. Internal controls designed and implemented by the physician-owner help prevent bad things from happening.
Embezzlement protection is the classic example. However, internal controls also help ensure good things happen most of the time; according to colleague Dr. Gary Bode; MSA, CPA.
Some Common Embezzlement “Old School” Schemes
Here are some ‘old-school” embezzlement schemes to avoid; however the list is imaginative and endless.
The physician-owner pocketing cash “off the books”. To the IRS, this is like embezzlement to intentionally defraud it out of tax money.
Employee’s pocketing cash from cash transactions. This is why you see cashiers following protocol that seems to take forever when you’re in the grocery check out line. This is also why you see signs offering a reward if he/she is not offered a receipt. This is partly why security cameras are installed.
Bookkeepers writing checks to themselves. This is easiest to do in flexible software programs like QuickBooks, Peachtree Accounting and related financial software. It is one of the hardest schemes to detect. The bookkeeper self-writes and cashes the check to their own name; and then the name on the check is changed in the software program to a vendor’s name. So a real check exists which looks legitimate on checking statements unless a picture of it is available.
Employees ordering personal items on practice credit cards.
Bookkeepers receiving patient checks and illegally depositing them in an unauthorized, pseudo practice checking account, set up by themselves in a bank different from yours. They then withdraw funds at will. If this scheme uses only a few patients, who are billed outside of the practice’s accounting software it is hard to detect. The doctor must have a good knowledge of existing patients to catch the ones “missing” from practice records. Monitoring the bookkeeper’s lifestyle might raise suspicion, but this scheme is generally low profile and protracted. Checking the accounting software “audit trail” shows the required original invoice deletions or credit memos in a less sophisticated version of this scheme.
Bookkeepers writing payroll checks to non-existent employees. This scheme works well in larger practices and medical clinics with high seasonal turnover of employees, and practices with multiple locations the podiatrist-owner doesn’t visit often.
Bookkeepers writing inflated checks to existing employees, vendors or subcontractors. Physician-owners should beware if romantic relationships between the bookkeeper and other practice related parties.
Bookkeepers writing checks to false vendors. This is another low profile, protracted scheme that exploits the podiatrists-owner’s indifference to accounts payable.
Assessment
Operating efficiency, safeguarding assets, compliance with existing laws and accuracy of financial transactions are common goals of internal managerial and cost accounting in medical practice.
CONCLUSION
Hopefully, the above is a good review to prevent common practice embezzlement schemes. Unfortunately, it is a never-ending endeavor.
References: Marcinko, DE: Dictionary of Health Economics and Finance. Springer Publishing Company, NY 2007.
Posted on March 26, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Donald Trump has officially dropped a stablecoin. It’s called USD1, and it’s pegged 1:1 with the US dollar, according to a statement from his family company World Liberty Financial Inc, (WLFI) today. The company says the token is fully backed by short-term US government treasuries, USD deposits, and other cash equivalents. Every token equals one dollar, no exceptions. WLFI says it built the whole thing to give people a stablecoin they don’t have to second guess.
US stocks rose for a third day in a row despite souring consumer confidence — and as investors weighed whether President Trump would temper his plans for upcoming tariffs.
The benchmark S&P 500 (^GSPC) rose more than 0.1%, while the Dow Jones Industrial Average (^DJI) ticked just above the flatline. The tech-heavy NASDAQ Composite (^IXIC) rose nearly 0.5%, bolstered by a more than 3% jump from Tesla (TSLA).
Posted on March 25, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
US stocks closed near session highs on Monday as investors welcomed reports that the next wave of President Trump’s tariffs will be narrower than expected.
The S&P 500 (^GSPC) rose almost 1.8% on the heels of the broad benchmark snapping a four-week losing streak. The Dow Jones Industrial Average (^DJI) advanced 1.4%, while contracts on the tech-heavy NASDAQ Composite (^IXIC) led the gains, up 2.3%.
A hostile takeover happens when an entity takes control of a company without the knowledge and against the wishes of the company’s management. A hostile takeover is an acquisition strategy requiring that the entity acquire and control more than 50% of the voting shares issued by the company.
In mergers and acquisitions (M&A), a hostile takeover is the acquisition of a target company by an acquiring company that goes directly to the target company’s shareholders, either by making a tender offer or through a proxy vote.
Ideally, an entity interested in acquiring a company should seek approval from the target company’s Board of Directors. The difference between a hostile and a friendly takeover is that, in a friendly takeover, the target company’s board of directors approve of the transaction and recommend shareholders vote in favor of the deal.
Defenses against a hostile takeover
These defense mechanisms can be preemptive or reactive, depending on how prepared the company is for the possibility of a hostile bid.
Poison pill is one of the most common defenses against a hostile takeover. Officially known as a “shareholder rights plan,” the poison pill allows existing shareholders to purchase additional shares at a discount, diluting the ownership interest of the acquiring company. The goal is to make it prohibitively expensive for the acquirer to complete the takeover.
A golden parachute is another defense strategy, which involves providing lucrative compensation packages (bonuses, severance pay, stock options, etc.) to key executives in the event they are terminated as a result of the takeover. This creates a financial disincentive for the acquiring company, as it would need to pay out these large sums upon completing the takeover.
In a Crown jewel defense, the target company sells or threatens to sell its most valuable assets—its “crown jewels”—if the takeover is completed. This reduces the attractiveness of the company to the acquirer, as the most desirable assets would no longer be part of the deal.
The Pac-Man defenses a more aggressive strategy in which the target company turns the tables by attempting to buy shares of the acquiring company, effectively launching a counter-takeover. While rare, this defense can deter hostile bids by making the takeover battle more costly and complex.
A White-Knight defense involves the target company seeking out a more favorable acquirer, or “white knight,” to make a friendly takeover bid. This allows the target company to avoid the hostile acquirer while still securing the benefits of a merger or acquisition.
The hostile takeover between Sanofi-Aventis and Genzyme Corp. occurred in 2010 when Sanofi, a French pharmaceutical company, wanted to buy Genzyme, a US biotech firm specializing in rare diseases. Genzyme resisted the offer, leading to conflict. Sanofi started a public campaign to pressure Genzyme’s shareholders into selling.
After months of negotiations, the two companies reached a deal in 2011. Sanofi agreed to pay $74 per share, with additional payments tied to Genzyme’s future performance, bringing the total deal value to around $20.1 billion. This acquisition allowed Sanofi to expand into the lucrative market for rare disease treatment.
The genetic testing company 23andMe went from biotech superstar to the brink of collapse. And, its most valuable asset might be its controversial customer DNA data trove.
Now, 23andMe filed for bankruptcy late Sunday night and announced the resignation of its chief executive officer Anne Wojcicki who is stepping down from her position but remains on the board of directors.
Wojcicki has so far tried unsuccessfully to rescue the business by buying it back and capping a precipitous fall for the DNA-testing company.
Posted on March 24, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Futures attached to the benchmark S&P 500 (ES=F) rose 0.6%, with NASDAQ 100 (NQ=F) futures up 0.7%. Futures tied to the Dow Jones Industrial Average (YM=F) advanced around 0.4%.
Absolute Return – the goal is to have a positive return, regardless of market direction. An absolute return strategy is not managed relative to a market index.
Accredited Investor – wealthy individual or well-capitalized institutions covered under Regulation D of the Securities Act of 1933.
Alpha – the return to a portfolio over and above that of an appropriate benchmark portfolio (the manager’s “value added”).
Arbitrage – any strategy that invests long in an asset, and short in a related asset, hoping the prices will converge.
Attribution – the process of “attributing” returns to their sources. For example, did the returns to a portfolio (over and above some benchmark) come from stock selection, industry/sector over- or under-weighting or factor weighting. Software programs are helpful in reporting an attribution.
Beta – a measure of systematic (i.e., non-diversifiable) risk. The goal is to quantify how much systematic risk is being taken by the fund manager vis-à-vis different risk factors, so that one can estimate the alpha or value-added on a risk-adjusted basis.
Correlation – a measure of how strategy returns move with one another, in a range of –1 to +1. A correlation of –1 implies that the strategies move in opposite directions. In constructing a portfolio of hedge funds, one usually wants to combine a number of non-correlated strategies (with decent expected returns) to be well diversified.
Drawdown – the percentage loss from a fund’s highest value to its lowest, over a particular time frame. A fund’s “maximum drawdown” is often looked at as a measure of potential risk.
Hurdle Rate – the return where the manager begins to earn incentive fees. If the hurdle rate is 5% and the fund earns 15% for the year, then incentive fees are applied to the 10% difference.
Leverage – one uses leverage if he borrows money to increase his position in a security. If one uses leverage and makes good investment decisions, leverage can magnify the gain. However, it can also magnify a loss.
Opportunistic – a general term that describes an aggressive strategy with a goal of making money (as opposed to holding on to the money one already has).
***
***
Pairs Trading – usually refers to a long/short strategy where one stock is bought long, and a similar stock is sold short, often within the same industry. Buying the stock of Home Depot and shorting Lowe’s in an equal amount would be an example.
Portfolio Simulation – involves testing an investment strategy by “simulating” it with a database and analytic software. Often referred to as “backtesting” a strategy. The simulated returns of the strategy are compared to those of a benchmark over a specific time frame to see if it can beat that benchmark.
Sharpe Ratio – a measure of risk-adjusted return, computed by dividing a fund’s return over the risk-free rate by the standard deviation of returns. The idea is to understand how much risk was undertaken to generate the alpha.
Short Rebate – if you borrow stock and then sell it short, you have cash in your account. The short rebate is the interest earned on that cash.
R-Squared – a measure of how closely a portfolio’s performance varies with the performance of a benchmark, and thus a measure of what portion of its performance can be explained by the performance of the overall market or index. Hedge fund investors want to know how much performance can be explained by market exposure versus manager skill.
Transportable Alpha – the alpha of one active strategy can be combined with another asset class. For example, an equity market-neutral strategy’s value-added can be “transported” to a fixed income asset class by simply buying a fixed income futures contract. The total return comes from both sources.
Value at Risk – a technique which uses the statistical analysis of historical market trends and volatilities to estimate the likelihood that a specific portfolio’s losses will exceed a certain amount.
Posted on March 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The S&P 500 edged up 0.1%. The index finished with a 0.5% gain for the week. It’s still down 4.8% so far this month. The Dow Jones Industrial Average eked out a 0.1% gain, while the NASDAQ composite rose 0.5%.
It appears Medicare coverage for tele-health is here to stay—at least for the next six months. When the House of Representatives and Senate passed a budget on March 11t and 14th, respectively, they not only avoided a government shutdown, but also extended a resolution for Medicare to cover non-behavioral health tele-health appointments until September 30th.
Visualize: How private equity tangled banks in a web of debt, from the Financial Times.
Posted on March 21, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
U.S. stock indexes edged lower Thursday following another reminder that big, unsettling policy changes are underway because of President Donald Trump, along with more signals suggesting the U.S. economy remains solid for now.
The S&P 500 slipped 0.2% after flipping between modest gains and losses through the day. The Dow Jones Industrial Average dipped by 11 points, or less than 0.1 %, and the NASDAQ composite fell 0.3%.
Tax avoidance—An action taken to lessen tax liability and maximize after-tax income.
Tax evasion—The failure to pay or a deliberate underpayment of taxes.
Underground economy—Money-making activities that people don’t report to the government, including both illegal and legal activities.
Voluntary compliance—A system of compliance that relies on individual citizens to report their income freely and voluntarily, calculate their tax liability correctly, and file a tax return on time.
Posted on March 20, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Stat: $1.2 billion. That’s how much San Diego-based Scripps Health plans to spend building a new hospital in San Marcos, California. (Becker’s Hospital Review)
Read: What WHO Director-General Tedros Adhanom Ghebreyesus said about USAID cuts. (Stat)
Pharm fresh: Check out in-depth strategies designed to help increase engagement between pharma reps and primary care clinicians. It’s all right here in Pri-Med’s research. Read the report.
Shares of Charles Schwab Corp. SCHW+1.51% rallied 1.51% to $78.73 Wednesday, on what proved to be an all-around favorable trading session for the stock market, with the S&P 500 IndexSPX+1.08% rising 1.08% to 5,675.29 and the Dow Jones Industrial AverageDJIA+0.92% rising 0.92% to 41,964.63.
Posted on March 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Split-Dollar Life Insurance: An arrangement under which a life insurance policy’s premium, cash values, and death benefit are split between two parties—usually a corporation and a key employee or executive. Under such an arrangement an employer may own the policy and pay the premiums and give a key employee or executive the right to name the recipient of the death benefit.
***
***
Several factors will affect the cost and availability of life insurance, including age, health, and the type and amount of insurance purchased. Life insurance policies have expenses, including mortality and other charges. If a policy is surrendered prematurely, the policy holder also may pay surrender charges and have income tax implications. You should consider determining whether you are insurable before implementing a strategy involving life insurance.
Any guarantees associated with a policy are dependent on the ability of the issuing insurance company to continue making claim payments.
9. We act with honesty, integrity and are always straightforward. 8. We strive to be innovative, creative, iconoclastic, and flexible. 7. We admit and learn from mistakes and don’t repeat them. 6. We work hard always as competitors are trying to catch up. 5. We treat others with dignity and respect. 4. We are the onus of consulting advice for the well being of others. 3. We fight complacency as former success is in the past. 2. The best management styles are timeless, not timely. 1. Our clients are colleagues and always come first.
SPEAKING: Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements.
***
***
CONTACT: Ann Miller RN MHA at: MarcinkoAdvisors@outlook.com
Posted on March 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
US stocks pulled back on Tuesday, led by a nearly 2% decline in the NASDAQ, following two days of gains as investors concerned about an economic slowdown looked to the Federal Reserve’s policy meeting for insights.
The tech-heavy NASDAQ Composite (^IXIC) plummeted about 1.7% as Nvidia (NVDA) shares fell roughly 3% as its annual GTC event failed to impress investors. Other “Magnificent Seven” names also dragged down the tech-heavy index. Notably, those stocks are having their worst quarter in more than two years.
The Dow Jones Industrial Average (^DJI) and S&P 500 (^GSPC) also moved to the downside on Tuesday, dropping about 0.6% and 1.1%, respectively.
“Malta has quietly leveraged the rising tide of the financial transparency imperative to attract hedge funds.“
There was a time when the quaint island sought to play on the traditional terrain, offering anonymity and a “laissez-faire regulatory regime,” not to mention very low taxes, as in no capital gains taxes and no taxes on dividends; all while English speaking and USD currency denominated.
***
***
While many leading domiciles for offshore hedge funds remain in the Caribbean – notably the Cayman Islands, the British Virgin Islands, Bermuda, and the Bahamas – the island of Malta is drawing attention, especially from European funds.
SO – HOW MUCH IS A “FINANCIAL ADVISOR” REALLY WORTH?
This blog holds a rather uncomplimentary opinion of financial advisors, and the financial services and brokerage industry as a whole; deserved, or not? The entire site hints at this attitude as well, in favor of a going it alone or ME, Inc investing when possible. Nevertheless, it is reasonable to wonder how much boost in net-returns might an educated and informed, fee transparent and honest, fiduciary focused “financial advisor” add to a clients’ investment portfolio; all things being equal [ceteris paribus].
And, can it be quantified?
Well, according to Vanguard Brokerage Services®, perhaps as much as 3%? In a decade long paper from the Valley Forge, PA based mutual fund and ETF giant, Vanguard said financial advisors can generate returns through a framework focused on five wealth management principles:
• Being an effective behavioral coach: Helping clients maintain a long-term perspective and a disciplined approach is arguably one of the most important elements of financial advice. (Potential value added: up to 1.50%).
• Applying an asset location strategy: The allocation of assets between taxable and tax-advantaged accounts is one tool an advisor can employ that can add value each year. (Potential value added: from 0% to 0.75%).
• Employing cost-effective investments: This component of every advisor’s tool kit is based on simple math: Gross return less costs equals net return. (Potential value added: up to 0.45%).
• Maintaining the proper allocation through rebalancing: Over time, as investments produce various returns, a portfolio will likely drift from its target allocation. An advisor can add value by ensuring the portfolio’s risk/return characteristics stay consistent with a client’s preferences. (Potential value added: up to 0.35%).
• Implementing a spending strategy: As the retiree population grows, an advisor can help clients make important decisions about how to spend from their portfolios. (Potential value added: up to 0.70%).
Source: Financial Advisor Magazine, page 20, April 2014.
Assessment
However, Vanguard notes that while it’s possible all of these principles could add up to 3% in net returns for clients, it’s more likely to be an intermittent number than an annual one because some of the best opportunities to add value happen during extreme market lows and highs when angst or giddiness [fear and greed] can cause investors to bail on their well-thought-out investment plans.
And, is the study applicable to doctors and allied healthcare providers? Doe Vanguard have a vested interest in the topic. What about fee based versus fee-only financial advice?
Conclusion
Finally, recognize the plethora of other financial planning life-cycle topics addressed in this ME-P were not included in the Vanguard investment portfolio-only study a decade ago.
And what about today with contemporaneous internet advising, chat-rooms, linkedin, robo-advisors, reddit and the like?
Posted on March 18, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
A group of current and former employees of JPMorgan Chase (NYSE:JPM) has filed a lawsuit alleging that the company, through its prescription drug plan run by CVS Health (NYSE:CVS), overpaid for medicines, resulting in higher expenses for its workers, according to Bloomberg News.
The S&P 500 (^GSPC) gained about 0.6% to rebound for a second day in row, while the Dow Jones Industrial Average (^DJI) gained more than 350 points, or more than 0.8%. The tech-heavy NASDAQ Composite (^IXIC) rose 0.3% as “Magnificent 7” stocks, including Nvidia (NVDA) and Tesla (TSLA), faltered.
Posted on March 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
BANK IDENTIFICATION NUMBER – DEFINED
By Staff Reporters
***
***
What Is a BIN Attack?
The BIN, or the Bank Identification Number, is the first six digits on a credit card. These are always tied to its issuing institution – usually a bank. In a BIN attack, fraudsters use these six numbers to algorithmically try to generate all the other legitimate numbers, in the hopes of generating a usable card number.
How Does a BIN Attack Work?
Fraudsters conduct BIN attacks by generating hundreds of thousands of possible credit card numbers and testing them out.
A fraudster looks up the BIN of the bank they will target. Ranging from four to six digits, this information is in the public domain and is thus easy to source.
Using dedicated software such as an auto-dialer, they generate thousands, often tens of thousands, combinations of possible existing card numbers by this issuer.
At this point, these credentials need to be tested. The fraudster identifies a suitable online shop or donation page.
They start card testing by attempting a small payment with each generated card number.
They keep track of the small percentage of card details that worked, which they are ready to use in earnest for their fraudulent pursuits.
***
***
Remember that the fraudster will start off with only six digits, yet there are many more card details required for a successful transaction. If those are entered erroneously, the transaction will decline. This includes the CVV number, the expiration date, as well as likely address verification service (AVS) failures. Card testing transactions are executed remotely in a fast fashion, so distance checks should also be a hint as well as velocity alerts.
Fraudsters may use bad merchant accounts directly for this purpose, or more frequently involve multiple online stores and services during a BIN attack, as their attempts keep getting blocked at most outlets.
When analyzing a set of financial statements to determine practice value, adjustments (normalizations) generally are needed to produce a clearer picture of likely future income and distributable cash flow. It also allows more of an “apples to apples” line item comparison. This normalization process usually consists of making three main adjustments to a medical practice’s net income (profit and loss) statement.
1. Non-Recurring Items: Estimates of future distributable cash flow should exclude non-recurring items. Proceeds from the settlement of litigation, one-time gains/losses from the selling of assets or equipment, and large write-offs that are not expected to reoccur, each represent potential nonrecurring items. The impact of nonrecurring events should be removed from the practice’s financial statements to produce a clearer picture of likely future income and cash flow.
2. Perquisites: The buyer of a medical practice may plan to spend more or less than the current doctor-owner for physician executive compensation, travel and entertainment expenses, and other perquisites of current management. When determining future distributable cash flow, income adjustments to the current level of expenditures should be made for these items.
3. Non-cash Expenses: Depreciation expense, amortization expense, and bad debt expense are all non-cash items which impact reported profitability. When determining distributable cash flow, you must analyze the link between non-cash expenses and expected cash expenditures.
The annual depreciation expense is a proxy for likely capital expenditures over time. When capital expenditures and depreciation are not similar over time, an adjustment to expected cash flow is necessary. Some practices reduce income through the use of bad debt expense rather than direct write-offs. Bad debt expense is a non-cash expense that represents an estimate of the dollar volume of write-offs that are likely to occur during a year. If bad debt expense is understated, practice profitability will be overstated.
***
***
Balance Sheet Adjustments
Adjustments also can be made to a practice’s balance sheet to remove non-operating assets and liabilities, and to restate asset and liability value at market rates (rather than cost rates). Assets and liabilities that are unrelated to the core practice being valued should be added to or subtracted from the value, depending on whether they are acquired by the buyer.
Examples include the asset value less outstanding debt of a vacant parcel of land, and marketable securities that are not needed to operate the practice. Other non-operating assets, such as the cash surrender value of officer life insurance, generally are liquidated by the seller and are not part of the business transaction.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Health actuaries analyze potential risks, profits and trends that will affect their employers, which are often in the health insurance, government health services and medical provider industries. They advise companies on issuing policies to consumers based on risks, calculated premiums and upcoming changes in health-care costs.
It’s common for an actuary to have a bachelor’s degree or higher in actuary studies, mathematics or statistics. Coursework on medical terminology and hierarchy of the medical field is also beneficial. In addition to academic education, certification is also necessary to reach “professional status,” which is required by most employers.
***
***
The professional organization, Society of Actuaries, certifies actuaries in the health and medical field. Their statistical work is commonly done with predictive tables, probability tables and life tables that are created on customized statistical analysis software such as Stata or XLSTAT.
The actuary field as a whole is growing faster than other fields, according to the Bureau of Labor Statistics [BLS]. In 2020, it expanded by 27 percent. The average annual salary for an actuary in 2010 was $87,650. More specifically, in the health insurance field, the salary was slightly higher at $91,000.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
In the United States, the difference between a Ph.D and a Sc.D is that the former is awarded to most, if not all, disciplines, while a Sc.D is awarded to science or STEM (science, technology, engineering, mathematics) disciplines.
This means that, in the United States at least, a Ph.D and a Sc.D are equal to one another in terms of telling people about an individual’s mastery of a particular skill, training, and prestige. A Ph.D holder and a Sc.D holder are viewed as peers and equals by most, if not all, American universities.
Meanwhile in Europe, according to Emily Summer, the difference between a Ph.D and a Sc.D is that the former is awarded at the start of an academic career, while the Sc.D is awarded much later, after the individual has built up an impressive body of work.
Posted on March 15, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITION
By Staff Reporters and FTC
***
***
Surveillance pricing is a broad term to describe the practice of linking pricing to individualized consumer data.
Companies employing it might use algorithms, personal information, and AI to set a price for their goods based on everything from where you live to your age to your browsing or credit history. The practice, sometimes called dynamic pricing or personalized pricing, is growing increasingly common, but isn’t completely new.
In 2012, the travel website Orbitz began directing people on Macs to higher hotels after realizing they often had more purchasing power. It stopped the practice after the Wall Street Journalreported on it.
Is surveillance pricing the same thing as surge pricing?Yes and no.
You might know about surge pricing from the last time you tried to call an Uber during a rainstorm. As demand skyrockets for a ride share, so does the price. This is one kind of surveillance pricing, but what the FTC is targeting appears more specific. The FTC said its probe concerns “when the pricing is based on surveillance of an individual’s personal characteristics and behavior.”
Is surveillance pricing bad?
The FTC opened its probe into companies using surveillance pricing because it’s worried about the risks it might pose to consumers
“Firms that harvest Americans’ personal data can put people’s privacy at risk. Now firms could be exploiting this vast trove of personal information to charge people higher prices,” FTC Chair Lina M. Khan said in a statement. “Americans deserve to know whether businesses are using detailed consumer data to deploy surveillance pricing, and the FTC’s inquiry will shed light on this shadowy ecosystem of pricing middlemen.”
The FTC is looking into four major areas of the practice: types of products being offered, data collection, customer and sales information, and impacts on consumers and prices.
Many Americans, it fears, don’t know when their data is being harvested and how it is affecting what they pay. “Consumers may now be subjected to surveillance pricing when they shop for anything, big or small, online or in person: a house, a car, even their weekly groceries,” the FTC said.
The FTC sent the orders for more information to Accenture, Bloomreach, Chase, Mastercard, McKinsey & Co., Pros, Revionics, and Task.
“Advancements in machine learning make it cheaper for these systems to collect and process large volumes of personal data, which can open the door for price changes based on information like your precise location, your shopping habits, or your web browsing history,” the FTC wrote.
According to Patricia Salber MD [personal communication], there are a number of reasons why direct patient access to laboratory medical results is a good idea:
Between 8 and 26% of abnormal test results, including those suspicious for cancer, are not followed up in a timely manner. Direct access could help reduce the number of times this occurs
Self-management, particularly of chronic illness has known benefits. Just like the QS people, many folks with chronic illness obtain and manage to self-acquired lab results every day via gluco-meters, home pulmonary function tests, blood pressure measurements, and so forth. Direct access to laboratory-acquired data, one could argue is a continuation of that personal responsibility
Patients want to be notified about their results in what they perceive as a timely fashion. In one study, patients who received direct notification of their bone density tests results were more likely to perceive they had timely notification compared to usual care even though there was no measurable effect on actual treatment received after three months
Being more responsible for test results could encourage consumers to try to learn more about the meaning of the test results, conceivably increasing their health literacy.
But, the arguments against direct access discussed include the following:
Patients prefer their physicians contact them directly when they have abnormal test results, although the major studies published in 2005 and 2009, preceded the extraordinary use of the internet to access health information that exists today.
There is concern over whether patients will know what to do when they receive the results – will they make erroneous interpretations or fail to contact their docs? This could be, but the intent of the proposed rule is shared access to the results. We suspect if the rule become law, docs will develop better notification mechanisms so that they reach the patient before the patient directly accesses the results or lab companies will design better lab test notifications with easy-to-understand interpretations or a whole new industry will appear that can provide instantly available individualized lab interpretation…or maybe all three of these would happen and that would be a very good thing.
Unknown impact of dual notification (doctors and patients) of lab test results on physician behavior…would docs simply shift responsibility for initiating follow-up care from themselves to their patients?
Would direct access of life-changing lab tests, such as HIV or malignancy, lead to unnecessary patient anxiety – or worse? (Conversely, is there less anxiety, desperation, or suicidal ideation if the bad news is delivered face to face?
Individuals likely may contact their physicians immediately after getting the lab results asking for a telephonic or face-to-face interpretation … it is not known how this would impact physician workload and/or potential for reimbursement [personal communication, Richard Hudson DO, Atlanta, GA].
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com