BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on June 29, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A.I.
***
***
Markets: That feeling when you have a $10 trillion rally. To wit:
The S&P 500 closed at a record high this week despite a brief dip as trade tensions with Canada ratcheted up. That puts the index about 20% up from its April low, when the broad tariff announcement sent it spiraling, and up ~5% for the year.
NVIDIA also hit an all-time high, and it keeps edging closer to becoming the first company to hit a $4 trillion valuation.
If you are just starting out managing your finances and don’t know where to begin, a financial coach may be a good option for you. They are helpful for someone who wants to become proficient in the basics of finance, from learning how to budget or save money to building an emergency fund or creating a plan for paying off debt. If you have short-term money goals, like saving for a big purchase or just practicing better money habits, a financial coach can help you reach them by working with you to create a plan and holding you accountable. Even more for physicians and most all medical professionals.
Pros and Cons of Working with a Financial Coach A financial coach can have a positive impact on your financial well–being and your life in a number of ways:
Financial coaches see the bigger picture of how you relate to money. They can help you develop better habits, resulting in positive personal growth.
By providing education and encouragement, they can reduce financial stress, confusion, and what it is about money that overwhelms you.
Through accountability and support, they can help you accomplish your goals and help you feel more confident in your finances.
Available 24/7/365.
Modest fees.
At you service. Dr. David Edward Marcinko MBA MEd CMP
Posted on June 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A.I.
***
***
Deals: The US and China revealed the details of their trade deal framework, easing restrictions on rare earth metals and semiconductor chips. Commerce Secretary Howard Lutnick promised up to 10 more deals are on their way ahead of the July 9th tariff-pause deadline, but that probably won’t include Canada: President Trump ended all trade discussions with the country thanks to a dispute over the digital services tax.
Stocks: Indexes climbed at the open thanks to the deal with China, but they tumbled on news of a fallout with Canada. Still, the S&P 500 managed to post its 1,245th new all-time high, while the NASDAQ booked its own record close. The Dow trundled higher as well, though it’s still about 1,600 points below its previous record.
Posted on June 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
A June 11th report from global professional services firm Alvarez & Marsal (A&M) predicts that more beneficiaries might soon ditch insurance coverage for options like short-term, limited duration plans or healthcare sharing ministries (HCSMs), which aren’t regulated like health insurance and aren’t required to comply with ACA protections like covering maternity care or pre-existing conditions.
Nvidia extended its winning streak to five days, rising another 1.73% as the AI trade continues to recover.
EchoStar climbed 13.16% after the parent company of Dish TV disclosed that President Trump did in fact prod the FCC to make a deal.
Cyngn soared another 20.07% following a big day of gains after the company that makes self-driving tech for industrial vehicles announced a partnership with Nvidia.
Strong earnings from Nike (more on that later) propelled sporting goods stocks higher today. ONHoldings rose 1.74%, while Dick’s Sporting Goods climbed 3.59%.
Domestic power producers popped on reports that Trump is planning to issue an executive order increasing energy production to meet AI demand. Vistra gained 2.44%, GE Vernova climbed 2.54%, and Vertiv added 2.71%.
What’s down
Coinbase Global ended its winning streak, tumbling 5.77% after GENIUS Act hype propelled the crypto stock skyward all week long. Traders took profits in Circle as well, pushing the stablecoin stock down 15.54%.
Chinese EV maker LiAuto fell 1.93% on its weaker-than-expected deliveries forecast for the second quarter.
Fellow Chinese EV maker Xiaomi stunned markets with reports that it received 240,000 orders for its new SUV within 18 hours of its debut, but shares still sank 4%.
Pony.ai lost 6.31% on a report that Uber is considering helping its founder Travis Kalanick fund his acquisition of the US subsidiary of the Chinese autonomous vehicle company.
Gold miners tumbled while the price of the precious metal fell as investors took a risk-on stance. Newmont lost 4.11%, BarrickMining fell 3.44%, and KinrossGold shed 6.18%.
Today’s trade deal reopens the door for Chinese rare earth imports, bad news for US producers like MPMaterials (down 8.59%) and USA Rare Earth (down 12.14%).
Posted on June 27, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
NEWS UPDATE!
***
***
On June 10th, Bobby Mukkamala was inaugurated as the 180th president of the American Medical Association (AMA).
An otolaryngologist from Flint, Michigan, Mukkamal chairs the organization’s substance use and pain care task force, won the AMA Foundation’s Excellence in Medicine Leadership Award last June, and served on the AMA board of trustees in 2017 and 2021.
Much has been written and much has been opined on the topic of health information technology, electronic health records and medical security liability for physicians and healthcare providers in this textbook. But occasionally, we all still get lost in a wide array of acronyms, jargon and terms that are constantly changing in this ecosystem. And so, this brief glossary serves as a ready reference for those who want to know about these definitions in a quick and ready fashion.
Access control: The process of controlling the access of a user
Access security: To allow computer or healthcare network entry using ID / password / secure socket layer (SSL) encryption / biometrics, etc; unique identification and password assignments are usually made to medical staff members for access to medical information on a need-to-know basis, and only upon written authority of the owner of the data.
Access level authorization: Establishes a procedure to determine the computer or network access level granted to individuals working on or near protected health information, medical data or secure health data.
Accredited standards committee: Organization that helps develop American National Standards (ANS) for computer and health information technology; accredited by ANSI for the development of American National Standards; ASC X12N develops medical electronic business exchange controls like 835-Health Care Claim Payment/Advice and 837-Health Care Claim.
Accountability: The security goal that generates the requirement for actions of an entity to be traced uniquely to that entity. This supports nonrepudiation, deterrence, fault isolation, intrusion detection and prevention, and after-action recovery and legal action.
Accounting: Creating an historical record of who was authenticated, at what time, and how long they accessed the computer system.
Administrative simplification: The use of electronic standard code sets for health information exchange; Title II, Subtitle F of HIPAA gives HHS the authority to mandate the use of standards for the electronic exchange of health care data; to specify what medical and administrative code sets should be used within those standards; to require the use of national identification systems for health care patients, providers, payers (or plans), and employers (or sponsors); and to specify the types of measures required to protect the security and privacy of personally identifiable health care and medical information.
Alternative backup sites: Off-site locations that are used for transferring computer operations in the event of an emergency.
American Health Information Management Association: A large trade association of health information and medical data management professionals.
American Medical Informatics Association: An organization that promotes the use of electronic medical management and healthcare informatics for clinical and administrative endeavors.
American Telemedicine Association: Established in 1993 as a leading resource and advocate promoting access to medical care for patients and health professionals via telecommunications technology; membership open to individuals, companies, and other organizations with an interest in promoting the deployment of telemedicine throughout the world.
Anti-virus software: A software package or subscription service used to thwart malicious computer or network attacks, such as: Symantec®, McAfee®, Trend Micro®, Panda Software®, Sunbelt Software®, Computer Associates®, AVG® or MS-FF ®, etc.
ASC X12N: HIPAA transmission standards, specifications and implementation guides from the Washington Publishing Company; or the National Council of Prescription Drug Programs.
Assurance: Grounds for confidence that the other four security goals (integrity, availability, confidentiality, and accountability) have been adequately met by a specific implementation. “Adequately met” includes (1) functionality that performs correctly, (2) sufficient protection against unintentional errors (by users or software), and (3) sufficient resistance to intentional penetration or bypass.
Asymmetric cryptology: The use of two different but mathematically related electronic keys for secure health data and medical information storage, transmission and manipulation.
Asymmetric encryption: Encryption and decryption performed using two different keys, one of which is referred to as the public key and one of which is referred to as the private key; also known as public-key encryption.
Asymmetric key: A half of a key pair used in an asymmetric “public-key” encryption system with two important properties: (1) the key used for encryption is different from the one used for decryption, (2) neither key can feasibly be derived from the other.
Attack tree: An inverted tree diagram that provides a visual image of the attacks that may occur against an asset.
Audio teleconferencing: A multi-simultaneous dual voice communications between two parties at remote locations; two way communications between physician and patient at various locations.
Authentication: The process of verifying and confirming the identity of a user.
Availability: The security goal that generates the requirement for protection against – Intentional or accidental attempts to (1) perform unauthorized deletion of data or (2) otherwise cause a denial of service or data.
Back door: A means to access to a computer program that bypasses security mechanisms, sometimes installed by a programmer so that the program can be accessed for troubleshooting or other purposes.
Back door trojans or bots: Currently, the biggest threat to healthcare and all PC users worldwide according to the MSFT Corporation.®
Bandwidth: The amount of information that can be carried over a communications link.
Bar coding systems: Final FDA ruling issued in February 2004 that required bar codes on most prescription and non-prescription medications used in hospitals and dispensed based on a physician’s order; the bar code must contain at least the National Drug Code (NDC) number, which specifically identifies the drug; although hospitals are not required at this time to have a bar code reading system on the wards, this ruling has heightened the priority of implementing hospital-wide systems for patient-drug matching using bar codes.
Baud: A unit of digital transmission that indicates the speed of information flow. The rate indicates the number of events able to be processed in one second and is expressed as bits per second (bps). The baud rate is the standard unit of measure for data transmission capability; typical older rates were 1200, 2400, 9600, and 14,400 baud; the signaling rate of a telephone line in the number of transitions made in a second; 1/300 sec = 300 baud.
Beta test: The secondary or final stress examination of newly developed computer hardware, software or peripheral devices; site, etc.
Bibliographic database: Indexed computer or printed source of citations of journal articles and other reports in the literature; typically include author, title, source, abstract, and/or related information; MEDLINE® and EMBASE®.
Bioinformatics: The application of medical and biological science to the health information management field.
Biological Information technology: Cross industry alliance of the Microsoft Corporation to enhance the ability to use and share digital health and biomedical data.
Biometric: Personal security identity characteristics, such as a signature, fingerprints, voice, iris or retinal scan, hand or foot vein geometry, facial characteristics, hair analysis, eye, blood vessel or DNA; uses the unique human characteristics of a person as a means of authenticating.
Biometric identification: Secure identification using biometrics that identifies a human from a measurement of a physical feature or repeatable action of the individual (for example, hand geometry, retinal scan, iris scan, fingerprint patterns, facial characteristics, DNA sequence characteristics, voice prints, and hand written signature).
Biopassword: Start-up healthcare IT security pioneer of keyboarding patterns to boost online security through neural network patterns.
Bluetooth® device: Machines, like cell phone with headset, transmitting across communications channels 1 to 14, over time.
Bluetooth® technology: Wireless mobile technology standard built into millions of mobile phones, headsets, portable computers, desktops and notebooks; named after Harold Bluetooth, a 10th century Viking king; healthcare telemetry and rural data transmissions; the Bluetooth Special Interest Group (BSIG) advocates measures aimed at pushing healthcare interoperability for wireless devices and other computers designed for use in the medical field; other wireless stands include: Wi-Fi, ZigBe®, IrDA and RFID.
Buffer: A temporary storage area.
Buffer overflow: A security breach that occurs when a computer program attempts to stuff more data into a temporary storage area than it can hold
Business continuity plan: A plan that outlines the procedures to follow after a business experiences an attack on its security.
California Database Security Breach Act: A state act that requires disclosure to California residents if a breach of personal information has or is believed to have occurred.
Certification authority: An independent third-party organization that assigns digital certificates.
Chain of custody: A process that documents everyone who has had contact with or direct possession of the evidence.
Chain of trust: Suggestion that each and every covered entity and business associate share responsibility and accountability for confidential PHI.
Chain of trust agreement: Contract entered into by two business partners in which it is agreed to exchange data and that the first party will transmit information to the second party, where the data transmitted is agreed to be protected between the partners; sender and receiver depend upon each other to maintain the integrity and confidentiality of the transmitted information; multiple two-party contracts may be involved in moving information from the originator to the ultimate recipient; for example, a provider may contract with a clearing house to transmit claims to the clearing house; the clearing house, in turn, may contract with another clearing house or with a payer for the further transmittal of those same claims.
Children’s Online Privacy Protection Act: A federal act that requires operators of online services or Web sites directed at children under the age of 13 to obtain parental consent prior to the collection, use, disclosure, or display of a child’s personal information.
Cipher lock: A combination lock that uses buttons that must be pushed in the proper sequence in order to open the door.
Clearing house: HIPAA medical invoice, healthcare data transaction exchange and medical data implementation service center that that meets or exceeds Federally-mandated standardized Electronic Data Interchange (EDI) transaction requirements.
Clinger-Cohen Act: Public Law 104-106; Information Technology Management Reform Act (ITMRA) of 1996.
Clinical data: Protected Health Information (PHI) from patient, physician, laboratory, clinic, hospital and/or payer, etc; identifiable patient medical information.
Clinical data information systems: Automatic and securely connected system of integrated computers, central severs and the Internet that transmits Protected Health Information (PHI) from patient, physician, laboratory, clinic, hospital and/or payer, etc.
Clinical data repository: Electronic storehouse of encrypted patient medical information; clinical data storage.
Clinical informatics: The management of medical and clinical data; the use of computers, networks and IT for patient care and health administration.
Clinical information: All the related medical information about a patient; Protected Health Information (PHI) from patients, providers, laboratories, clinics, hospitals and/or payers or other stakeholders, etc.
Clinical information system: A computer network systems that supports patient care; relating exclusively to the information regarding the care of a patient, rather than administrative data, this hospital-based information system is designed to collect and organize data.
Clinical regional health information system: Electronic entity committed to securely share private patient health information among entities like medical providers, clinics, laboratories, hospitals, outpatient centers, hospice and other healthcare facilities; Community Health Management Information Systems (CHMIS), Enterprise Information Networks (EINs), Regional Health Information Networks (RHINs) and Health Information Networks (HINs).
Cold site: An alternative backup site that provides the basic computing infrastructure, such as wiring and ventilation, but very little equipment.
Compact disc – read only memory (CD-ROM): A computer drive that can read CD-R and CD-RW discs.
Compact disc – recordable (CD-R): An optical disc that contains up to 650 megabytes of data and cannot be changed once recorded.
Compact disc – rewriteable (CD-RW): An optical disc that can be used to record data, erase it, and re-record again.
Computer security: A computer or network that is free from threats against it.
Computerized Physician Order Entry System: Automatic medical provider electronic medical chart ordering system that usually includes seven features: medication analysis, system order clarity, increased work efficiency, point of care utilization, benchmarking and performance tracking, on-line alerts and regulatory reporting.
Confidential health information: Protected Health Information (PHI) that is prohibited from free-use and secured from unauthorized dissemination or use; patient specific medical data.
Counter signature: The ability to prove the order of application of signatures; analogous to the normal business practice of signing a document which has already been signed by another party (ASTM E 1762 -95); part of a digital signature.
Covered entity: 42 CFR § 164.504(e)(2)(i)(B). Any of three broadly defined entities that deal with protected health information (PHI): providers, individuals or group health plans, and clearinghouses.
Cracker: A person who breaks into or otherwise violates the system security with a malicious intent.
Cryptography: The science of transforming information so that it is secure while it is being transmitted or stored.
Cyber-terrorism: Attacks by a terrorist group using computer technology and the Internet to cripple or disable a nation’s electronic infrastructure.
Data backup: The process of copying data to another media and storing it in a secure location.
Data encryption standard: An older health or medical data private key cryptology federal protocol for secure information exchange; replaced by AES.
Data interchange standard: X12 HIPAA health data transmission standard format.
Data interchange standard association: The organization that provides X12 HIPAA transmission standards and formats.
Deadbolt lock: A lock that extends a solid metal bar into the door frame for extra security.
Decision support system: Computer tools or applications to assist physicians in clinical decisions by providing evidence-based knowledge in the context of patient-specific data; examples include drug interaction alerts at the time medication is prescribed and reminders for specific guideline-based interventions during the care of patients with chronic disease; information should be presented in a patient-centric view of individual care and also in a population or aggregate view to support population management and quality improvement.
Decryption: Changing an encrypted message back to its original form.
Definition files: Files that contain updated antivirus information.
De-identified health information: Protected health information that is no longer individually identifiable health information; a covered entity may determine that health information is not individually identifiable health information only if: (1) a person with appropriate knowledge of and experience with generally accepted statistical and scientific principles and methods for rendering information not individually identifiable determines that the risk is very small that the information could be used, alone or in combination with other available information, to identify an individual, and documents the methods and results of the analysis; or (2) the following identifiers of the individual, relatives, employers or household members of the individual are removed.
Denial of service: The prevention of authorized access to resources or the delaying of time critical operations.
Designated record set: Contains medical and billing records and any other records that a physician and/or medical practice utilizes for making decisions about a patient; a hospital, emerging healthcare organization, or other healthcare organization is to define which set of information comprises “protected health information” and which set does not; contains medical or mixed billing records, and any other information that a physician and/or medical practice utilizes for making decisions about a patient. It is up to the hospital, EHO, or healthcare organization to define which set of information comprises “protected health information” and which does not though logically this should not differ from locale to locale. The patient has the right to know who in the lengthy data chain has seen their PHI. This sets up an audit challenge for the medical organization, especially if the accountability is programmed, and other examiners view the document without cause.
Designated standard: HIPAA standard as assigned by the department of HHS
Device lock: A steel cable and a lock used to secure a notebook computer.
Digital certificate: A certificate that binds a specific person to a public key.
Digital imaging and communications in medicine: Technology broadband transmission imaging standards for X-rays, MRIs, CT and PET scans, etc; health IT standard transmissions platform aimed at enabling different computing platforms to share image data without compatibility problems; a set of protocols describing how radiology images are identified and formatted that is vendor-independent and developed by the American College of Radiology and the National Electronic Manufacturers Association.
Digital radiology: Medical digital imaging applied to x-rays, CT, PET scans and related non-invasive and invasive technology; broadband intensive imaging telemedicine.
Digital rights management: The control and protection of digital intellectual property.
Digital signature: Encrypted electronic authorization with verification and security protection; private and public key infrastructure; based upon cryptographic methods of originator authentication, computed by using a set of rules and a set of parameters so that the identity of the signer and the integrity of medical or other data can be verified.
Digital signature standard: Encryption technology to ensure electronic medical data transmission integrity and authentication of both sender and receiver; date and time stamps; public and private key infrastructure.
Digital versatile disc – recordable (DVD-R): An optical disc technology that can record once up to 3.95 gigabytes of data on a single-sided disc and 7.9 GB on a double-sided disc.
Digital versatile disc – rewriteable (DVD-RAM): An optical disc technology that can record, erase, and re-record data and has a capacity of 2.6 GB (single side) or 5.2 GB (double side).
Digital versatile disc (DVD): A technology that permits large amounts of data to be stored on an optical disc.
Disaster recovery plan: A process to restore vital health and/or critical healthcare technology systems in the event of a medical practice, clinic, hospital or healthcare business interruption from human, technical or natural causes; focuses mainly on technology systems, encompassing critical hardware, operating and application software, and any tertiary elements required to support the operating environment; must support the process requirements to restore vital company data inside the defined business requirements; does not take into consideration the overall operating environment; an emergency mode operation plan is still necessary.
Disclosure: Release of PHI outside a covered entity or business agreement space, under HIPAA; the release, transfer, provision of access to or divulging of medical information outside the entity holding the information.
Disc – rewriteable (DVD-RW): An optical disc technology that allows data to be recorded, erased, and re-recorded.
Due care: Managers and their organizations have a duty to provide for information security to ensure that the type of control, the cost of control, and the deployment of control are appropriate for the system being managed.
e-health: Emerging field in the intersection of medical informatics, public health and business, referring to health services and information delivered or enhanced through the Internet and related technologies; characterizes not only a technical development, but also a state-of-mind, attitude, and a commitment for networked, global thinking, to improve health care worldwide by using information and communication technology.
Electronic data interchange: Inter healthcare organization computer-to-computer transmission of business or health information in a standard format; direct transmission from the originating application program to the receiving, or processing, application program; an EDI transmission consists only of business or health data, not any accompanying verbiage or free-form messages; a standard format is one that is approved by a national or international standards organization, as opposed to formats developed by health industry groups, medical practices, clinics or companies; the electronic transmission of secure medical and financial data in the healthcare industrial complex; X12 and similar variable-length formats for the electronic exchange of structured health data. The Centers for Medicare and Medicaid Services (CMS) regulates security and Electronic Data Interchange (EDI).
Electronic data interchange standards: The American National Standards Institute (ANSI) set of EDI standards known as the X12 standards. These standards have been developed by private sector standards development organizations (SDOs) and are maintained by the Accredited Standards Committee (ASC) X12. ANSI ASC X12N standards, Version 4010, were chosen for all of the transactions except retail pharmacy transactions, which continue to use the standard maintained by the National Council for Prescription Drug Programs (NCPDP) because it is already in widespread use. The NCPDP Telecommunications Standard Format Version 5.1 and equivalent NCPDP Batch Standard Version 1.0 have been adopted in this rule (health plans will be required to support one of these two NCPDP formats). The standards are designed to work across industry and company boundaries. Changes and updates to the standards are made by consensus, reflecting the needs of the entire base of standards users, rather than those of a single organization or business sector. Specifically, the following nine healthcare transactions were required to use X12N standard electronic claim formats by October 16, 2003.
Electronic health record: A real-time patient health record with access to evidence-based decision support tools that can be used to aid clinicians in decision-making; the EHR can automate and streamline a clinician’s workflow, ensuring that all clinical information is communicated; prevents delays in response that result in gaps in care; can also support the collection of data for uses other than clinical care, such as billing, quality management, outcome reporting, and public health disease surveillance and reporting; electronic medical record.
Electronic medication administrative record: Electrical file keeping computerized system for tracking clinical medication dispensation and use; integrated with TPAs, PBMs, robotic dispensing devices and CPOEs, etc.
Electronic medical (media) claims: Usually refers to a flat file format used to transmit or transport medical claims, such as the 192-byte UB-92 Institutional EMC format and the 320-byte Professional EMC-NSF.
Electronic prescribing: A type of computer technology whereby physicians use handheld or personal computer devices to review drug and formulary coverage and to transmit prescriptions to a printer or to a local pharmacy; e-prescribing software can be integrated into existing clinical information systems to allow physician access to patient-specific information to screen for drug interactions and allergies.
Electronic preventive services selector: A digital tool for primary care clinicians to use when recommending preventive services for their patients unveiled by the Department of Health and Human Services’ Agency for Healthcare Research and Quality (AHRQ), in November 2006; designed for use on a personal digital assistant (PDA) or desktop computer to allow clinicians to access the latest recommendations from the AHRQ-sponsored U.S. Preventive Services Task Force; designed to serve as an aid to clinical decision-making at the point of care and contains 110 recommendations for specific populations covering 59 separate preventive services topics; a real time search function allows a clinician to input a patient’s age, gender, and selected behavioral risk factors, such as whether or not they smoke, in the appropriate fields, while the software cross-references the patient characteristics entered with the applicable Task Force recommendations and generates a report specifically tailored for that patient.
Electronic signature: Various date and time stamped electronic security verification systems, such as passwords, encryption, ID numbers, biometrics identifiers, etc; electrical transmission and authentication of real signatories; signatory attribute that is affixed to an electronic health document to bind it to a particular entity; an electronic signature process secures the user authentication (proof of claimed health identity, such as by biometrics (fingerprints, retinal scans, hand written signature verification, etc.), tokens or passwords) at the time the signature is generated; creates the logical manifestation of signature (including the possibility for multiple parties to sign a medical document and have the order of application recognized and proven) and supplies additional information such as time stamp and signature purpose specific to that user; and ensures the integrity of the signed document to enable transportability, interoperability, independent verifiability, and continuity of signature capability; verifying a signature on a document verifies the integrity of the document and associated attributes and verifies the identity of the signer; there are several technologies available for user authentication, including passwords, cryptography, and biometrics (ASTM 1762-95).
Encryption: Changing the original text to a secret message.
Gigabytes (GB): Billions of bytes of data.
Gramm-Leach-Bliley Act: A federal act that requires private data be protected by banks and financial institutions.
Hacker: A person who possesses advanced computer skills and is adept at exploring computers and networks in order to break into them.
HEALTH 1.0: This is the dying healthcare system of yesterday and today. Information is communicated from doctors to patients. It is a basic B2C [business-to-consumer] website as the internet became one big encyclopedia by aggregating knowledge silos. Some doctors maintain websites, others do not. Nevertheless, Health 1.0 has a command and control hierarchy; doctors on top of the pyramid, patients on the bottom.
HEALTH 2.0:According to Matthew Holt [personal communication] Healthcare 2.0 may be defined as: “The foundation of healthcare 2.0 is information exchange plus technology. It employs user-generated content, social networks and decision support tools to address the problems of inaccessible, fragmentary or unusable health care information. Healthcare 2.0 connects users to new kinds of information, fundamentally changing the consumer experience (e.g., buying insurance or deciding on/managing treatment), clinical decision-making (e.g., risk identification or use of best practices) and business processes (e.g., supply-chain management or business analytics)”.
And so, if Health 1.0 was a static book, Health 2.0 is a dynamic discussion
Example: The power of the internet is illustrated in the phenomenon of “crowd-sourcing.” In this context, the term means to harvest the reach of social networking [wisdom of crowds] to solve a problem. A knowledge seeker asks a question and participants respond. For example, readers can participate on the www.MedicalExecutivePost.com or www.BusinessofMedicalPractice.com sites to improve the administration of any medical practice. And, www.PodiatryPrep.com is an example of how podiatrists connect for global board certification assistance.
***
***
HEALTH 2.0 Plus:The Dictionary of Health Insurance and Managed Care defines this emerging hybrid as a bridge uniting the philosophy of contemporary Health 2.0 with futuristic Health 3.0 technologies. Cisco System’s HealthPresence is one example developed in 2010, by Dr. T. Warner Hudson. Using the network as a platform, HealthPresence combines video, audio and information to create an environment similar to what patients experience when they visit their own doctor.
HEALTH 3.0: Soon, patients will not only be seeking information; but actionable intelligence – whether it is artificial or real. Patients will communicate almost as with another patient or doctor. The internet won’t just blindly do what we tell it to do – it will think and represent some amazing opportunities. For example, imagine your toilet running a SMAC 20 and then being instantly notified of the results by your smart phone? Or; use your iPhone to send pictures and streaming videos of conditions for a second opinion www.KnockingLive.com
Health information technology: The application of information processing involving both computer hardware and software that deals with the storage, retrieval, sharing, and use of health care information, medical data, and knowledge for communication and decision making.
Health information technology auditor: An expert who evaluate a health organization’s computer systems to ensure the proper safeguards are in place to protect and maintain the integrity of the firm’s data; While the position has existed since the mid-1960s, companies that previously employed just a handful of HIT auditors are now significantly adding to their ranks, sometimes doubling, tripling or quadrupling current staff levels; much current demand is due to the Sarbanes-Oxley Act and other legislation aimed at improving corporate governance in the wake of major accounting scandals earlier in the decade; publicly traded hospital systems require the expertise of HIT auditors to meet ongoing compliance requirements; the Gramm-Leach-Bliley Act and the Health Insurance Portability and Accountability Act (HIPAA), among other regulations, also are fueling the need for HIT auditors. Health IT auditors must have a general understanding of accounting principles and the strategic vision to ensure a health organization’s HIT systems allow it to achieve its short- and long-term objectives. Many hospitals promote from within for this role. Health facilities who look outside the organization for these professionals usually seek candidates with experience, knowledge of healthcare of emerging technologies and issues, and increasingly, certifications such as the certified information systems auditor (CISA) designation.
Health information technology promotion act: Legislation to accelerate the adoption of interoperable electronic health records by ensuring uniform standards, championed by Rep. Nancy Johnson, R-Conn, (H.R. 4157) which would: codify the Office of the National Coordinator for Health Information Technology in statute and delineate its ongoing responsibilities; create exceptions to the fraud and abuse statutes to allow certain providers to fund health information technology equipment and services for other providers; and provide for a study of federal and state health privacy policies.
Health Insurance Portability and Accountability Act (HIPAA): A federal act that requires enterprises in the health sector to guard protected health information and implement policies and procedures to safeguard it.
Health level seven: An international community of healthcare subject matter experts and information technology physicians and scientists collaborating to create standards for the exchange, management and integration of protected electronic healthcare information; the Ann Arbor, Mich.-based Health Level Seven (HL7) standards developing organization has evolved Version 3 of its standard, which includes the Reference Information Model (RIM) and Data Type Specification (both ANSI standards); HL7 Version 3 is the only standard that specifically deals with creation of semantically interoperable healthcare information, essential to building the national infrastructure; HL7 promotes the use of standards within and among healthcare organizations to increase the effectiveness and efficiency of healthcare delivery for the benefit of all patient, payers, and third parties; uses an Open System Interconnection (OSI) and high level seven healthcare electronic communication protocol that is unique in the medical information management technology space and modeled after the International Standards Organization (ISO) and American National Standards Institute (ANSI); each has a particular healthcare domain such as pharmacy, medical devices, imaging or insurance (claims processing) transactions. Health Level Seven’s domain is clinical and administrative data.
Hot site: An alternative backup site that contains the same equipment as found in the organization’s actual IT center.
Human firewall: An employee who practices good security techniques to prevent any security attacks from passing through them.
Incident response team: An employee team charged with gathering and handling the digital evidence of an attack.
Individually identifiable health information: Medical information that is created or received by a covered entity; relates to the physical or mental health condition of an individual, provision of health care or the payment for the provision of health care; identifies the individual or there is reasonable belief that the information can be used to identify the individual.
Information security: A computer or network that is free from threats against it.
Integrity: The security goal that generates the requirement for protection against either intentional or accidental attempts to violate data integrity (the property that data has when it has not been altered in an unauthorized manner) or system integrity (the quality that a system has when it performs its intended function in an unimpaired manner, free from unauthorized manipulation).
Intellectual property: Works created by others such as books, music, plays, paintings, and photographs.
IT-related risk: The net mission impact considering (1) the probability that a particular threat-source will exercise (accidentally trigger or intentionally exploit) system vulnerability and (2) the resulting impact if this should occur. IT-related risks arise from legal liability or mission loss due to:
* Unauthorized (malicious or accidental) disclosure, modification, or destruction of information
* Unintentional errors and omissions
* IT disruptions due to natural or man-made disasters
* Failure to exercise due care and diligence in the implementation and operation of the IT system.
Key-in-knob lock: A basic lock that has the lock mechanism embedded in the knob or handle.
Keystroke logger: A type of hardware spyware that captures keystrokes as they are typed.
Logic bombs: A computer program that lies dormant until it is triggered by a specific event.
Lossless: To compress electronic digital data.
Malicious code: Programs that are intentionally created to break into secure computers or to create havoc after the computers are accessed.
Master patient index: Healthcare facility composite that links and assists in tracking patient, person, or member activity within an organization (or health enterprise) and across patient care settings; hardcopy or electronic identification of all patients treated in a facility or enterprise and lists the medical record or identification number associated with the name; can be maintained manually or as part of a computerized system; typically, those for healthcare facilities are retained permanently, while those for insurers, registries, or others may have different retention periods; a database of all the patients ever registered (within reason) at a facility; name, demographics, insurance, next of kin, spouse, etc.
Medically unbelievablE event: Implemented on Jan. 1, 2007, the CMS blockage of payments for medical services that make no sense based on “anatomic considerations” or medical reasonableness when the same patient, date of service, HCPCS code or provider is involved; unlike other National Correct Coding Initiative (NCCI) edits, MUEs can’t be overridden by a modifier because there will never be a scenario where the physician had a good reason to submit a claim for removing a second appendix from the same person; etc.
Megabytes (MB): Millions of bytes of storage.
Memory stick: USB flash or non-volatile storage device; Sony CompactFlash®, pen or mini-drive; flash card, smart media, slang terms.
Mesh: Medical Subject Headings, the controlled vocabulary of about 16,000 terms used for MEDLINE and certain other MEDLARS databases.
Minimum necessary: The amount of protected health information shared among internal or external parties determined to me the smallest amount needed to accomplish its purpose for Use or Disclosure; the amount of health information or medical data needed to accomplish a purpose varies by job title, CE or job classification.
Minimum necessary rule: HIPAA regulation that suggests any PHI used to identify a patient, such as a social security number, home address or phone number; divulge only essential elements for use in transferring information from patient record to anyone else that requires the information; especially important with financial information; changes the way software is written and vendor access is provided. The “Minimum Necessary” Rule states the minimum use of PHI that can be used to identify a person, such as a social security number, home address or phone number. Only the essential elements are to be used in transferring information from the patient record to anyone else that needs this information. This is especially important when financial information is being addressed. Only the minimum codes necessary to determine the cost should be provided to the financial department. No other information should be accessed by that department. Many institutions have systems where a registration or accounting clerk can pull up as much information as a doctor or nurse, but this is now against HIPAA policy and subject to penalties. The “minimum necessary” rule is also changing the way software is set up and vendor access is provided.
Mirror site: A secondary location identical to the primary IT site that constantly receives a copy of data from the primary site.
National health information network: The technologies, standards, laws, policies, programs and practices that enable health information to be shared among health decision makers, including consumers and patients, to promote improvements in health and healthcare; vision for the NHII began more than a decade ago with publication of an Institute of Medicine report, The Computer-Based Patient Record. The path to a national network of healthcare information is through the successful establishment of Regional Health Information Organizations (RHIO).
National provider identifier: Originally was an eight-digit alphanumeric identifier. However, the healthcare industry widely criticized this format, claiming that major information systems incompatibilities would make it too expensive and difficult to implement. DHHS therefore revised its recommendation, instead specifying a 10-position numeric identifier with a check digit in the last position to help detect keying errors. The NPI carries no intelligence; in other words, its characters will not in themselves provide information about the provider. More recently, CMS announced that HIPAA-covered entities such as providers completing electronic transactions, healthcare clearinghouses, and large health plans, must use only the NPI to identify covered healthcare providers in standard transactions by May 23, 2007. Small health plans must use only the NPI by May 23, 2008. The proposal for a Standard Unique National Health Plan (Payer) Identifier was withdrawn on February, 2006. (According to CMS, “withdrawn” simply means that there is not a specific publication date at this time. Development of the rule has been delayed; however, when the exact date is determined, the rule will be put back on the agenda.)
Network: A group of interconnected computers.
Notebook safe: A special safe secured to a wall or the trunk of a car used for storing a notebook computer.
Operating system hardening: Steps that can be taken to make a personal computer operating system more secure.
Optical disc: A disc that uses laser technology to record data.
Password: A secret combination of words or numbers that authenticates or identifies the user.
Patch: A software update to correct a problem.
Patch management: Tools, utilities, and processes for keeping computers up to date with new software updates that are developed after a software product is released.
Pharmacy information system: Drug tracking and dispensation related health management information system for hospitals and healthcare organizations.
PhisHing: An attempt to fraudulent gather confidential information by masquerading as a trustworthy entity, person or business in an apparently official email, text message or website; carding or spoofing; video vishing; phish-tank; vish-tank; slang terms.
Physical security: The process of protecting the computer itself.
Port scanning: Sending a flood of information to all of the possible network connections on a computer.
Ports: The network connections on a computer.
Preset lock: A basic lock that has the lock mechanism embedded in the knob or handle.
Privacy: The quality or state of being hidden, encrypted, obscure, or undisclosed; especially medical data or PHI.
Privacy act: Federal legislature of 1974 which required giving patient some control over their PHI.
Privacy enhanced mail: Email message standard protocol for enhanced medical, health data or other security.
Privacy officer: A medical entity’s protected client information and security officer; required by each covered entity, to be responsible for “the development and implementation of the policies and procedures” necessary for compliance.
Privacy rule: The Federal privacy regulations promulgated under the Health Insurance Portability and Accountability Act (HIPAA) of 1996 that created national standards to protect medical records and other protected health information. The Office of Civil Rights (OCR) within the Department of Health and Human Services (DHHS) regulates the privacy rules.
Privacy standards: Any protocol to ensure the confidentiality of PHI.
Private key system: A means of cryptography where the same key is used to both encrypt and decrypt a message.
Public key system: A means of cryptography where two keys are used.
* Psychotherapy notes recorded (in any medium) by a health care provider who is a mental health professional documenting or analyzing the contents of conversation during a private counseling session or a group, joint, or family counseling session and that are separated from the rest of the individual’s medical record; excludes medication prescription and monitoring, counseling session start and stop times, the modalities and frequencies of treatment furnished, results of clinical tests, and any summary of the following items: diagnosis, functional status, the treatment plan, symptoms, prognosis, and progress to date.
* Public health authority means an agency or authority of the United States, a State, a territory, a political subdivision of a State or territory, or an Indian tribe, or a person or entity acting under a grant of authority from or contract with such public agency, including the employees or agents of such public agency or its contractors or persons or entities to whom it has granted authority, that is responsible for public health matters as part of its official mandate.
* Required by law means a mandate contained in law that compels a covered entity to make a use or disclosure of protected health information and that is enforceable in a court of law; includes but is not limited to, court orders and court-ordered warrants; subpoenas or summons issued by a court, grand jury, a governmental or tribal inspector general, or an administrative body authorized to require the production of information; a civil or an authorized investigative demand; Medicare conditions of participation with respect to health care providers participating in the program; and statutes or regulations that require the production of information, including statutes or regulations that require such information if payment is sought under a government program providing public benefits.
Regional health information organization: A multi-stakeholder organization that enables the exchange and use of health information, in a secure manner, for the purpose of promoting the improvement of health quality, safety and efficiency; the U.S. Department of Health and Human Services see RHIOs as the building blocks for the national health information network (NHIN) that will provide universal access to electronic health records; other experts maintain that RHIOs will help eliminate some administrative costs associated with paper-based patient records, provide quick access to automated test results and offer a consolidated view of a patient’s history.
Risk assessment: The process of identifying the risks to system security and determining the probability of occurrence, the resulting impact, and additional safeguards that would mitigate this impact.
Risk management: The total process of identifying, controlling, and mitigating information system–related risks. It includes risk assessment; cost-benefit analysis; and the selection, implementation, test, and security evaluation of safeguards. This overall system security review considers both effectiveness and efficiency, including impact on the mission and constraints due to policy, regulations, and laws.
Royalties: Payment to the owner or creator of intellectual property for their work.
Sarbanes-Oxley Act (Sarbox): A federal act that enforces reporting requirements and internal controls on electronic financial reporting systems.
Scanning: Locating a computer that can be broken into.
Script kiddies: Younger and less sophisticated users who break into a computer with malicious intent.
Secure virtual private network: Cryptographic tunneling protocols to provide the necessary health data confidentiality (preventing snooping), sender authentication (preventing identity spoofing), and message integrity (preventing message alteration) to achieve the medical privacy intended. When properly chosen, implemented, and used, such techniques can provide secure communications over unsecured networks.
Security: A set of healthcare information technology system characteristic and mechanisms which span the system both logically and physically; electronic access control against unauthorized intervention, both friendly or malicious; encompasses all of the safeguards in an information system, including hardware, software, personnel policies, information practice policies, disaster preparedness, and the oversight of all these areas; the purpose of health information security is to protect both the system and the information it contains from unauthorized access from without and from misuse from within; through various security measures, a health information system can shield confidential information from unauthorized access, disclosure and misuse, thus protecting privacy of the individuals who are the subjects of the stored data; security life cycle.
Security administration: The physical and electrical protection features of an IT health system needed to be managed in order to meet the needs of a specific installation and to account for changes in the healthcare entities operational environment.
Security compromise: Physical or electronic data, file, program or transmission error due to malicious miscreants or software interventions; health data confidentiality breach.
Security configuration: Measures, practices, and procedures for the safety of information systems that must be coordinated and integrated with each other and other methods, practices, and procedures of the organization established in order to credential safekeeping policy; provides written security plans, rules, procedures, and instructions concerning all components of a healthcare entity’s security; procedures must give instructions on how to report breaches and how those breaches are to be handled within the organization.
Security configuration management: The measurement of practices and procedures for the security of information systems that is coordinated and integrated with each other and other measures, practices and procedures of the organization so as to create a coherent system of health data security (NIST Pub 800-14).
Security domain: A set of subjects, their information objects, and a common security policy; foundation for IT security is the concept of security domains and enforcement of data and process flow restrictions within and between these domains.
Security goals: The five security goals are integrity, availability, confidentiality, accountability, and assurance.
Security information system: security is a system characteristic and a set of mechanisms that span the system both logically and physically.
Security policy: A formal written policy that outlines the importance of security to the organization and establishes how the security program is organized.
Share: An object that is shared with others over a computer network.
Signature files: Files that contain updated antivirus information.
Smart card: A device that contains a chip that stores the user’s private key, login information, and public key digital certificate.
Sniffing: Listening to the traffic on a computer network and then analyzing it.
Social engineering: Relying on trickery and deceit to break security and gain access to computers.
Spam: Unsolicited e-mail messages.
Spy: A person who has been hired to break into a computer and steal data.
Spyware: Hardware or software that “spies” on what the user is doing and captures that activity without their knowledge.
Stealth signal transmitter: Software installed on a notebook computer that sends a signal that can be traced.
Threat analysis: The examination of threat-sources against system vulnerabilities to determine the threats for a particular system in a particular operational environment.
Threat modeling: A process of constructing scenarios of the types of threats that assets face.
Threat: The potential for a threat-source to exercise (accidentally trigger or intentionally exploit) a specific vulnerability.
Threat-source: Either (1) intent and method targeted at the intentional exploitation of a vulnerability or (2) a situation and method that may accidentally trigger a vulnerability.
Token: A security device used to authenticate the user by having the appropriate permission (like a password) embedded into the device.
USA Patriot Act: A federal act designed to broaden the surveillance of law enforcement agencies to enhance the detection and suppression of terrorism.
Username: A unique identifier of a person used to access a computer system.
Virus: A program that secretly attaches itself to other programs and when executed causes harm to a computer.
Vulnerability: A flaw or weakness in system security procedures, design, implementation, or internal controls that could be exercised (accidentally triggered or intentionally exploited) and result in a security breach or a violation of the system’s security policy.
Vulnerability assessment: A process to determine what vulnerabilities exist in the current system against these attacks.
Vulnerability assessment managed services: Agencies that use scanning devices connected to probe an organization’s security to look for vulnerabilities.
War driving: A technique used to locate wireless local area networks (WLANs).
WiMax: A more powerful version of Wi-Fi that can provide wireless Internet access over wider geographic location such as a city; an acronym that stands for Worldwide Interoperability for Microwave Access, and is a certification mark for products that pass conformity and interoperability tests for the IEEE 802.16 standards. IEEE 802.16 is working group number 16 of IEEE 802, specializing in point-to-multipoint broadband wireless access.
Wireless hot spot: Specific geographic location in which an access point provides public wireless broadband network services; security is risky for PHI; hotspot.
Wireless local area networks: A computer network that uses radio waves instead of wires to connect computers.
Worm: A program that does not attach itself to other programs or need user intervention to execute.
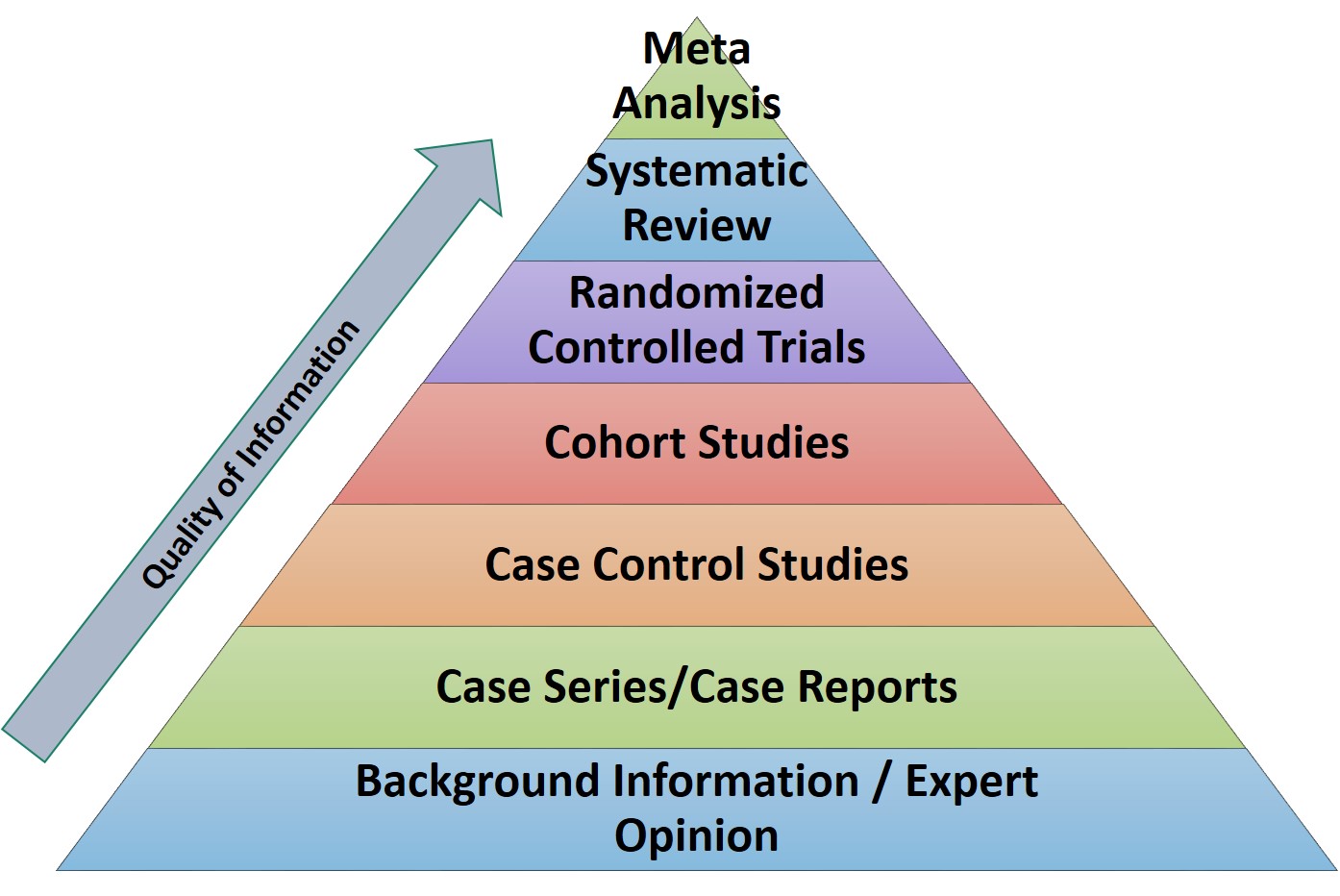
The average directional movement index (ADX) was developed in 1978 by J. Welles Wilder as a technical indicator of trend strength in a series of prices of a financial instrument. ADX has become a widely used indicator for technical analysts, and is provided as a standard in collections of indicators offered by various trading platforms.
The ADX is a combination of two other indicators developed by Wilder, the positive directional indicator (abbreviated +DI) and negative directional indicator (-DI). The ADX combines them and smooths the result with a smoothed moving average.
The average directional index (ADX) is a technical indicator used by traders to determine the strength of a financial security’s price trend. It helps them reduce risk and increase profit potential by trading in the direction of a strong trend. Many traders consider the ADX to be the ultimate trend gauge because it is so reliable.
ADX quantifies trend strength by measuring the degree of directional movement in price. ADX calculations are based on a moving average of price range expansion or contraction over a given period. The default setting is 14 periods, although other settings can be used.
ADX can be used with any financial security, including stocks, exchange-traded funds, and futures.
We make second investment portfolio opinions affordable
Approximately 1 million allopathic physicians, 150,000 dentists, 200,000 osteopaths, 15,000 podiatrists and 6 million nurses often find it difficult to get an unbiased and fiduciary second opinion on their retirement or brokerage accounts. By offering second opinions for a flat fee, the monetary barriers that prevented colleagues from receiving a second opinion in the past have been removed.
We make second investment portfolio opinions convenient
Here’s how we work: you book an initial appointment with us, answer a few preliminary questions and email us your portfolio information. We then provide a second opinion. It is then up to you to incorporate or not.
We make second investment portfolio opinions timely
Financial markets, jobs and colleague age change like the weather. It is not always okay to wait a week, year or more, to seek a professional second financial portfolio opinion. You need to receive an opinion now. That’s where we come in. We are standing by, ready to take your email [MarcinkoAdvisors@outlook.com] and schedule a free initial consultation within two or three days, or less.
We make second investment portfolio opinions accurate
Fiduciary and non-sales orientated second opinions have the power to change financial lives in the long term. We’ve seen it happen many times. What characterizes a good second opinion? Three things: the opinion must be individualized to your investment portfolio[s], informed and results-oriented. That’s the informed fiduciary approach we take. We are colleagues and look forward to working with you.
FIVE INVESTING MISTAKES OF DOCTORS; PLUS 1 VITAL TIP
As a former US Securities and Exchange Commission [SEC] Registered Investment Advisor [RIA] and business school professor of economics and finance, I’ve seen many mistakes that doctors must be aware of, and most importantly, avoid. So, here are the top 5 investing mistakes along with suggested guideline solutions.
Mistake 1: Failing to Diversify Investment but Beware Di-Worsification
A single investment may become a large portion of your portfolio as a result of solid returns lulling you into a false sense of security. The Magnificent Seven stocks are a current example:
Apple, up +5,064%% since 1/18/2008
Amazon, up +30,328% since 9/6/2002
Alphabet, up +1,200% since 7/20/2012
Tesla, up +21,713% since 11/16/2012
Meta, up +684% since 2/20/2015
Microsoft, up +22% since 12/21/2023
Nvidia, up +80,797% since 4/15/2005
Guideline: The Magnificent Seven [7] has grown from 9% of the S&P 500 at the end of 2013 to 31% at the end of 2024! That means even if you don’t own them, you’re still very exposed if you have an Index Fund [IF] or Exchange Traded Fund [ETF] that tracks the market. Accordingly, diversification is the only free lunch in investing which can reduce portfolio risk. But, remember the Wall Street insider aphorism that states: “Di-Versification Means Always Having to Say Your Sorry.”
The term “Di-Worsification” was coined by legendary investor Peter Lynch in his book, One Up On Wall Street to refer to over-diversifying an investment portfolio in such a way that it reduces your overall risk-return characteristics. In other words, the potential return rises with an increase in risk and invested money can render higher profits only if willing to accept a higher possibility of losses [1].
A podiatrist can easily fall into the trap of chasing securities or mutual funds showing the highest return. It is almost an article of faith that they should only purchase mutual funds sporting the best recent performance. But in fact, it may actually pay to shun mutual funds with strong recent performance. Unfortunately, many struggle to appreciate the benefits of their investment strategy because in jaunty markets, people tend to run after strong performance and purchase last year’s winners.
Similarly, in a market downturn, investors tend to move to lower-risk investment options, which can lead to missed opportunities during subsequent market recoveries. The extent of underperformance by individual investors has often been the most awful during bear markets. Academic studies have consistently shown that the returns achieved by the typical stock or bond fund investors have lagged substantially.
Guideline: Understand chasing performance does not work.Continually monitor your investments and don’t feel the need to invest in the hottest fund or asset category. In fact, it is much better to increase investments in poor performing categories (i.e. buy low). Also keep in remind rebalancing of assets each year is key. If stocks perform poorly and bonds do exceptionally well, then rebalance at the end of the year. In following this strategy, this will force a doctor into buying low and selling high each year.
Often doctors make their investment decisions under the belief that stocks will consistently give them solid double-digit returns. But the stock markets go through extended long-term cycles.
In examining stock market history, there have been 6 secular bull markets (market goes up for an extended period) and 5 secular bear markets (market goes down) since 1900. There have been five distinct secular bull markets in the past 100+ years. Each bull market lasted for an extended period and rewarded investors.
For example, if an investor had started investing in stocks either at the top of the markets in 1966 or 2000, future stock market returns would have been exceptionally below average for the proceeding decade. On the other hand, those investors fortunate enough to start building wealth in 1982 would have enjoyed a near two-decade period of well above average stock market returns. They key element to remember is that future historical returns in stocks are not guaranteed. If stock market returns are poor, one must consider that he or she will have to accept lower projected returns and ultimately save more money to make up for the shortfall. For example,
The May 6th, 2010, flash crash, also known as the crash of 2:45, was a United States trillion-dollar stock market plunge which started at 2:32 pm EST and lasted for approximately 36 minutes.
And, investors who have embraced the “buy the dip” strategy in 2025 have been handsomely rewarded, with the S&P 500 delivering its strongest post-pull back returns in over three decades.
According to research from Bespoke Investment Group, the S&P 500 has gained an average of 0.36% in the trading session following a down day so far in 2025. The only year with a comparable performance was 2020, which saw a 0.32% average post-dip gain [2].
The most recent example came on May 27, 2025 when the S&P 500 surged more than 2% after falling 0.7% in the final session before the holiday weekend. The rally was sparked by President Trump’s decision to scale back huge previously threatened tariffs on EU —a recurring catalyst behind many of 2025’s rebound.
Guideline: Beware of projecting forward historical returns. Doctors should realize that the stock markets are inherently volatile and that, while it is easy to rely on past historical averages, there are long periods of time where returns and risk deviate meaningfully from historical averages.
Some doctors believe they are “smarter than the market” and can time when to jump in and buy stocks or sell everything and go to cash. Wouldn’t it be nice to have the clairvoyance to be out of stocks on the market’s worst days and in on the best days?
Using the S&P 500 Index, our agile imaginary doctor-investor managed to steer clear of the worst market day each year from January 1st, 1992 to March 31st, 2012. The outcome: s/he compiled a 12.42% annualized return (including reinvestment of dividends and capital gains) during the 20+ years, sufficient to compound a $10,000 investment into $107,100.
But what about another unfortunate doctor-investor that had the mistiming to be out of the market on the best day of each year. This ill-fated investor’s portfolio returned only 4.31% annualized from January 1992 – March 2012, increasing the $10,000 portfolio value to just $23,500 during the 20 years. The design of timing markets may sound easy, but for most all investors it is a losing strategy.
More contemporaneously on December 18th 2024, the DJIA plummeted 2.5%, while the S&P 500 declined 3% and the NASDAQ tumbled 3.5%
Guideline: If it looks too good to be true, it probably is. While jumping into the market at its low and selling right at the high is appealing in theory, we should recognize the difficulties and potential opportunity and trading costs associated with trying to time the stock market in practice. In general, colleagues are be best served by matching their investment with their time horizon and looking past the peaks / valleys along the way.
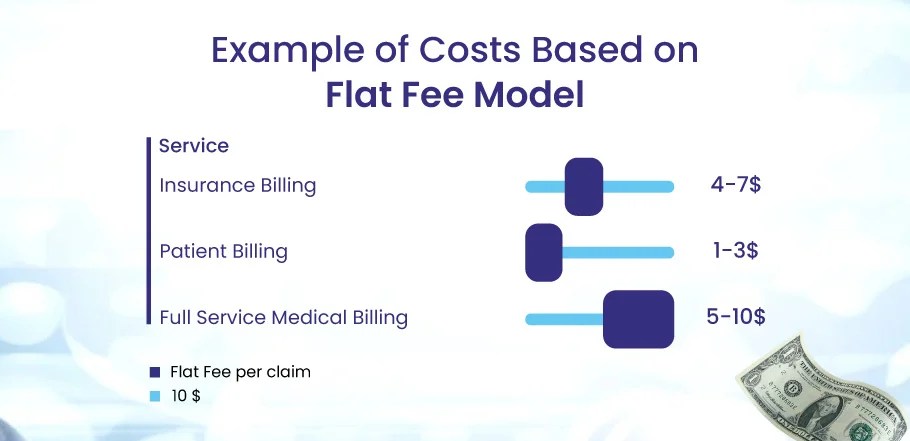
Mistake 5: Failing to Recognize the Impact of Fees and Expenses
A free dinner seminar or a polished stock-broker sales pitch may hide the total underlying costs of an investment. So, fees absolutely matter.
The first costing step is determining what the fees actually are. In a mutual fund, these costs are found in the company’s obligatory “Fund Facts”. This manuscript clearly outlines all the fees paid–including up front fees (commissions and loads), deferred sales charges and any switching fees. Fund management expense ratios are also part of the overall cost. Trading costs within the fund can also impact performance.
Here is a list of the traditional mutual fund fees:
Front End Load: The commission charged to purchase a fund through a stock broker or financial advisor. The commission reduces the amount you have available to invest. Thus, if you start with $100,000 to invest, and the advisor charges up to an 8 percent front end load, you end up actually investing $92,000.
Deferred Sales Charge (DSC) or Back End Load: Imposed if you sell your position in the mutual fund within a pre-specified period of time (normally one – five years). It is initiated at a higher start percentage (i.e. as high as 10 percent) and declines over a specific period of time.
Operating Fees: Costs of the mutual fund including the management fee rewarded to the manager for investment services. It also includes legal, custodial, auditing and marketing fees.
Annual Administration Fee: Many mutual fund companies also charge a fee just for administering the account – usually under $100-150 per year.
Guideline: Know and understand all fees.
For example: A 1 percent disparity in fees may not seem like much but it makes a considerable impact over a long time period.
Consider a $100,000 portfolio that earns 8 percent before fees, grows to $320,714 after 20 years if the investor pays a 2 percent operating fee. In comparison, if s/he opted for a fund that charged a more reasonable 1 percent fee, after 20 years, the portfolio grows to be $386,968 – a divergence of over $66,000!
This is the value of passive or index investing. In the case of an index fund, fees are generally under 0.5 percent, thus offering even more savings over a long period of time.
One Vital Tip: Investing Time is on Your Side
Despite thousands of TV shows, podcasts, textbooks, opinions and university studies on investing, it really only has three simple components. Amount invested, rate of return and time. By far, the most important item is time! For example:
Nvidia: if you invested $1,000 in 2009, you’d have $338,103 today.
Apple: if you invested $1,000 in 2008, you’d have $48,005 today.
Netflix: if you invested $1,000 in 2004, you’d have $495,679 today.
Unfortunately, this list of investing mistakes is still being made by many doctors. Fortunately, by recognizing and acting to mitigate them, your results may be more financially fruitful and mentally quieting.
REFERENCES:
1. Lynch, Peter: One Up on Wall Street [How to Use What You Already Know to Make Money in the Market]: Simon and Shuster (2nd edition) New York, 2000.
1. Marcinko, DE; Comprehensive Financial Planning Strategies for Doctors and Advisors [Best Practices from Leading Consultants and Certified Medical Planners™] Productivity Press, New York, 2017.
2. Marcinko, DE: Dictionary of Health Economics and Finance. Springer Publishing Company, New York, 2006.
3. Marcinko, DE; Risk Management, Liability Insurance, and Asset Protection Strategies for Doctors and Advisors [Best Practices from Leading Consultants and Certified Medical Planners™] CRC Press, New York, 2015.
BIO: As a former university Professor and Endowed Department Chair in Austrian Economics, Finance and Entrepreneurship, the author was a NYSE Registered Investment Advisor and Certified Financial Planner for a decade. Later, he was a private equity and wealth manager
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on June 10, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
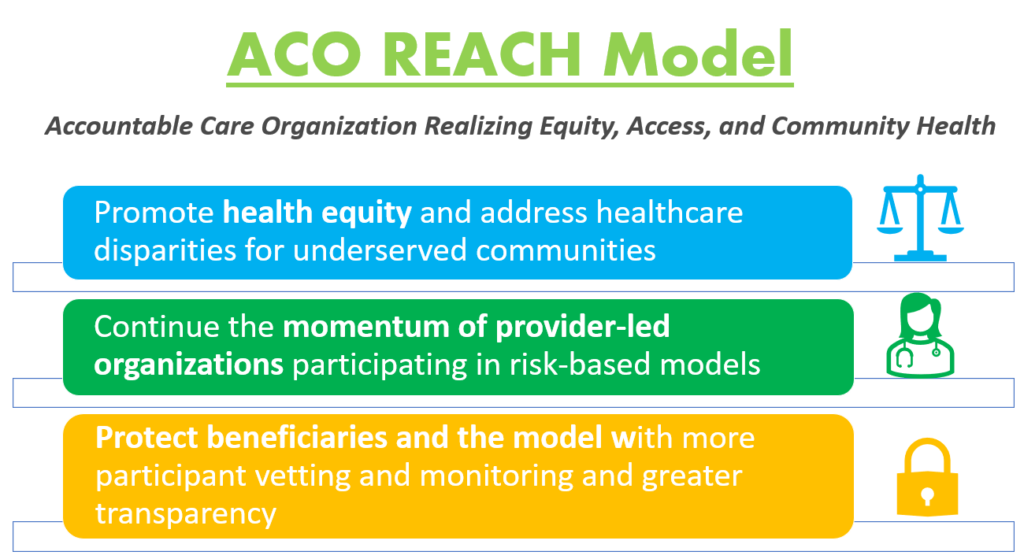
On May 13th, 2025, the CMS Center for Medicare & Medicaid Innovation (CMMI) introduced a new strategic plan for its models going forward. After ending four payment models early and canceling two not-yet-implemented models in March 2025, the agency had promised to release a new strategy. Nearly two weeks later, CMMI released that strategy, as well as a preliminary evaluation of, and changes to, one of its core payment models.
This Health Capital Topics article will review CMMI’s recent actions and what initial indications these actions provide. (Read more…)
Posted on June 9, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By AI
***
***
A POD (Payable on Death) or TOD (Transfer on Death) account is a type of bank account where the account owner names a beneficiary to receive the account assets when the owner dies.
Key points about these accounts include:
Beneficiaries can be anyone, including minors, non-U.S. citizens, and organizations.
The beneficiary needs to provide a certified copy of the deceased’s death certificate to the bank or brokerage firm.
The assets are transferred immediately upon the account owner’s death.
Probate avoidance: By sidestepping probate, POD and TOD accounts streamline the distribution of assets post-death, allowing beneficiaries to gain access to these funds with greater speed.
Simplicity: Setting up these accounts is generally straightforward, often requiring just the completion of a form at the bank or brokerage firm.
No additional cost: There’s usually no cost to establish these accounts, aligning with the needs of individuals seeking a cost-effective method of transferring assets.
Cons
Joint ownership complexity. When an account is jointly owned, the beneficiary of the account won’t receive the assets until the surviving owner(s) die. The same applies to accounts owned in states with tenancy by the entirety for married couples.
Naming alternative beneficiaries: These accounts do not allow for the nomination of alternative beneficiaries if the primary beneficiary or beneficiaries predecease the account owner. This could lead to the assets being subjected to probate if the primary beneficiary is no longer alive at the time of the account holder’s death.
Transfers only happen after death: These accounts stipulate that the person must pass away before the beneficiary can access the funds – a restriction that could prove troublesome if the beneficiary requires access to these assets during the account holder’s life or if the account owner becomes incapacitated during their lifetime.
Posted on June 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
On April 11th, 2025, the Centers for Medicare & Medicaid Services (CMS) released its proposed rules for the payment and policy updates for the Medicare inpatient prospective payment system (IPPS) and long-term care hospital prospective payment system (LTCH PPS) for fiscal year (FY) 2026.
This Health Capital Topics article will discuss the proposed rule and the implications for stakeholders. (Read more…)
Posted on June 3, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
A recent joint report by the National Association of Accountable Care Organizations (NAACOS) and Innovaccer Inc., a healthcare artificial intelligence (AI) company, found tangible evidence that the U.S. healthcare delivery system is indeed moving toward value-based care (VBC).
Fifteen years after the passage of the Patient Protection and Affordable Care Act (ACA), which promoted VBC through the advent of ACOs and other alternative payment models, there is finally evidence that providers are actually moving in that direction.
This Health Capital Topics article reviews the joint report on “The State and Science of Value-based Care 2025.”(Read more…)
Posted on June 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
BREAKING NEWS
By Staff Reporters
***
***
Stanley Fischer, one of the most influential economists of recent decades, has died. He was 81. His death was confirmed by the WSJ and Bank of Israel, where he served as governor from 2005 to 2013.
Fischer served as vice chairman of the Federal Reserve from 2014 to 2017. He left his biggest mark in prior decades, as professor of economics at the Massachusetts Institute of Technology, second in command at the International Monetary Fund, and at the Bank of Israel. In those roles, Fischer helped shape how an entire generation of central bankers and economic policymakers do their jobs.
Fischer was born in 1943 in Northern Rhodesia (now the independent country of Zambia) and first came to the U.S. in 1966 to get a Ph.D. at MIT.
After several years at the University of Chicago, he joined the faculty of MIT.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Life planning and behavioral finance as proposed for physicians and integrated by the Institute of Medical Business Advisors Inc., is unique in that it emanates from a holistic union of personal financial planning, human physiology and medical practice management, solely for the healthcare space. Unlike pure life planning, pure financial planning, or pure management theory, it is both a quantitative and qualitative “hard and soft” science, with an ambitious economic, psychological and managerial niche value proposition never before proposed and codified, while still representing an evolving philosophy. Its’ first-mover practitioners are called Certified Medical Planners™.
Financial Life Planning is an approach to financial planning that places the history, transitions, goals, and principles of the client at the center of the planning process. For the financial advisor or planner, the life of the client becomes the axis around which financial planning develops and evolves.
Financial Life Planning is about coming to the right answers by asking the right questions. This involves broadening the conversation beyond investment selection and asset management to exploring life issues as they relate to money.
Financial Life Planning is a process that helps advisors move their practice from financial transaction thinking, to life transition thinking. The first step is aimed to help clients “see” the connection between their financial lives and the challenges and opportunities inherent in each life transition.
But, for informed physicians, life planning’s quasi-professional and informal approach to the largely isolate disciplines of financial planning and medical practice management is inadequate. Today’s practice environment is incredibly complex, as compressed economic stress from HMOs managed care, financial insecurity from insurance companies, ACOs and VBC, Washington DC and Wall Street; liability fears from attorneys, criminal scrutiny from government agencies, and IT mischief from malicious electronic medical record [eMR] hackers. And economic bench marking from hospital employers; lost confidence from patients; and the Patient Protection and Affordable Care Act [PP-ACA] more than a decade ago. All promote “burnout” and converge to inspire a robust new financial planning approach for physicians and most all medical professionals.
The iMBA Inc., approach to financial planning, as championed by the Certified Medical Planner™ professional certification designation program, integrates the traditional concepts of financial life planning, with the increasing complex business concepts of medical practice management. The former topics are presented in this textbook, the later in our recent companion text: The Business of Medical Practice [Transformational Health 2.0 Skills for Doctors].
***
***
For example, views of medical practice, personal lifestyle, investing and retirement, both what they are and how they may look in the future, are rapidly changing as the retail mentality of medicine is replaced with a wholesale and governmental philosophy. Or, how views on maximizing current practice income might be more profitably sacrificed for the potential of greater wealth upon eventual practice sale and disposition.
Or, how the ultimate fear represented by Yale University economist Robert J. Shiller, in The New Financial Order: Risk in the 21st Century, warns that the risk for choosing the wrong profession or specialty, might render physicians obsolete by technological changes, managed care systems or fiscally unsound demographics. OR, if a medical degree is even needed for future physicians?
Say, what medical license?
Dr. Shirley Svorny, chair of the economics department at California State University, Northridge, holds a PhD in economics from UCLA. She is an expert on the regulation of health care professionals who participated in health policy summits organized by Cato and the Texas Public Policy Foundation. She argues that medical licensure not only fails to protect patients from incompetent physicians, but, by raising barriers to entry, makes health care more expensive and less accessible. Institutional oversight and a sophisticated network of private accrediting and certification organizations, all motivated by the need to protect reputations and avoid legal liability, offer whatever consumer protections exist today.
Yet, the opportunity to revise the future at any age through personal re-engineering, exists for all of us, and allows a joint exploration of the meaning and purpose in life. To allow this deeper and more realistic approach, the informed transformation advisor and the doctor client, must build relationships based on trust, greater self-knowledge and true medical business management and personal financial planning acumen.
[A] The iMBA Philosophy
As you read this ME-P website, we hope you will embrace the opportunity to receive the focused and best thinking of some very smart people. Hopefully, along the way you will self-saturate with concrete information that proves valuable in your own medical practice and personal money journey. Maybe, you will even learn something that is so valuable and so powerful, that future reflection will reveal it to be of critical importance to your life. The contributing authors certainly hope so.
At the Institute of Medical Business Advisors, and thru the Certified Medical Planner™ program, we suggest that such an epiphany can be realized only if you have extraordinary clarity regarding your personal, economic and [financial advisory or medical] practice goals, your money, and your relationship with it. Money is, after only, no more or less than what we make of it.
Ultimately, your relationship with it, and to others, is the most important component of how well it will serve you.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Classic: Flat fee paid for a patient’s treatment based on their diagnosis and/or presenting problem. For this fee the provider covers all of the services required for a specific period of time.
Modern: Often characterizes “second generation” managed care systems. After a Managed Care Organization squeezes out costs by discounting fees, they often come to this method. If provider is still standing after discount blitz, this approach can be good for provider and clients, since it permits a lot of flexibility for provider in meeting client needs.
Posted on May 25, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITION
By Staff Reporters
***
***
Meta-analysis is a quantitative, formal, epidemiological study design used to systematically assess previous research studies to derive conclusions about that body of research. Outcomes from a meta-analysis may include a more precise estimate of the effect of treatment or risk factor for disease, or other outcomes, than any individual study contributing to the pooled analysis. The examination of variability or heterogeneity in study results is also a critical outcome.
The benefits of meta-analysis include a consolidated and quantitative review of a large, and often complex, sometimes apparently conflicting, body of literature. The specification of the outcome and hypotheses that are tested is critical to the conduct of meta-analyses, as is a sensitive literature search. A failure to identify the majority of existing studies can lead to erroneous conclusions; however, there are methods of examining data to identify the potential for studies to be missing; for example, by the use of funnel plots.
Rigorously conducted meta-analyses are useful tools in evidence-based medicine. The need to integrate findings from many studies ensures that meta-analytic research is desirable and the large body of research now generated makes the conduct of this research feasible.
Classic Definition: Although the human body can develop a low-grade fever, muscular aches and pains in response to any vaccine, rumors that a flu shot can cause the flu are not true.
Modern Circumstance: Flu shots do contain dead flu viruses, but they are indeed dead. As for vaccines causing autism, this myth was started in 1998 with an article in the journal The Lancet.
Paradox Examples: In the study, the parents of eight children with autism said they believed their children acquired the condition after they received a vaccination against measles, mumps and rubella (the MMR vaccine). Since then, rumors have run rampant despite the results of many studies.
And, a 2002 study in The New England Journal of Medicine of 530,000 children found no link between vaccinations and the risk of a child developing autism.
Unfortunately, the endurance of this paradoxical myth continues to eat up time and funding dollars that could be used to make advances in autism, rather than proving, over and over again, that vaccinations do not cause the condition.
Cite: Dr. Rachel Vreeman, St. Martin’s Griffin 2009.
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
When you visit health clinic or hospital for a medical appointment, you’ll be seen by a doctor, healthcare provider and/or medical prescriber. But what do these words really mean?
***
***
Doctors / Physicians
Doctor of Medicine (MD), Doctor of Podiatric Medicine (DPM), Doctor of Osteopathy (DO, or Doctor of Dental Surgery (DDS/DMD). Doctors, also known as physicians, have extensive prescription privileges across various specialties. They can diagnose medical conditions, prescribe medication, and oversee the overall management of patient care. Doctors include general practitioners, specialists such as cardiologists or dermatologists, and surgeons. Their prescription authority encompasses a wide range of medications to address acute and chronic health conditions, ranging from antibiotics to specialized treatments for complex diseases.
A medical provider is a general term that encompasses a wide range of education levels, skill-sets, and specializations. A provider could be a Physician Assistant (PA), Nurse Practitioner (NP), Clinical Nurse Specialist (CNS), Doctor of Medicine (MD), Doctor of Podiatric Medicine (DPM), Dentist (DDSDMD) or Doctor of Osteopathy (DO).
***
Medical Drug Prescribers
Generally, psychologists and therapists do not have prescription privileges. They focus on psychotherapy and counseling rather than medication management. However, some jurisdictions may grant limited prescription rights to psychologists who undergo additional training and certification. Like psychologists, therapists typically do not have prescription privileges. They focus on providing counseling and psychotherapy to address mental health issues and emotional concerns.
Psychiatrists are medical doctors (MD/DO) who specialize in the diagnosis and treatment of mental health disorders. They have full prescription privileges and can prescribe a wide range of medications to manage psychiatric conditions.
In most cases, physical therapistsdo not have the authority to prescribe medication. They primarily focus on rehabilitation and physical interventions to improve mobility and function.
Nurse practitioners are advanced practice nurses with the authority to diagnose, treat, and prescribe medication independently in many states and countries. They undergo extensive education and training, which allows them to provide a wide range of healthcare services, including medication management.
Similar to nurse practitioners, psychiatric nurse practitioners have the authority to prescribe medication for mental health conditions. They specialize in psychiatric and mental health care, offering comprehensive treatment that may include medication management.
Chiropractors primarily focus on diagnosing and treating musculoskeletal disorders through manual adjustments and therapies. They do not have surgical or prescription privileges in most jurisdictions.
Optometrists are trained to diagnose and treat vision problems, including prescribing corrective lenses and medications for certain eye conditions such as infections or inflammation.
Registered nursestypically do not have prescription privileges. They work under the direction of physicians and nurse practitioners, assisting with patient care but not prescribing medication themselves.
Dentists have limited prescription privileges related to dental care, such as antibiotics or pain medications for dental procedures. However, they do not have the authority to prescribe general medications outside of their scope of practice.
Nutritionists typically do not have prescription privileges. They specialize in providing dietary advice and counseling to promote health and well-being through nutrition but do not prescribe medication.
Depending on their scope of practice and legal regulations in their jurisdiction, nurse midwives may have limited prescription privileges for certain medications related to prenatal care, childbirth, and postpartum care.
According to Baumol’s Cost Disease, in theory, workers should get higher pay because they get more productive. But an economist named William J. Baumol PhD noticed this isn’t always true; as in a paradox.
For example, musicians take the same time to play a string quartet as they did in Mozart’s day, but are paid more nevertheless. The reason is competition for labor; musicians can take other jobs. So rising wages in productive parts of the economy (eg, manufacturing) lead to higher wages in less productive sectors.
MORE: For more on the paradoxical disease, read this article; and for more on Baumol, read this one.
Free-market economists are those who believe that the market is better at allocating resources than governments and that excessive regulation and high public spending tend to diminish growth in the long run.
“Medical economics and finance is an integral component of the health care industrial complex. Its language is a diverse and broad-based concept covering many other industries: accounting, insurance, mathematics and statistics, public health, provider recruitment and retention, Medicare, health policy, forecasting, aging and long-term care, are all commingled arenas …. The Dictionary of Health Economics and Finance will be an essential tool for doctors, nurses and clinicians, benefits managers, executives and health care administrators, as well as graduate students and patients. With more than 5,000 definitions, 3,000 abbreviations and acronyms, and a 2,000 item oeuvre of resources, readings, and nomenclature derivatives, it covers the financial and economics language of every health care industry sector.”
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on May 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Health Insurance Co-Payments Upfront or Lose Your Appointment
Definition: A co-payment is a fixed amount you pay each time you get a particular type of healthcare service, and co-pays will generally be quite a bit smaller than deductibles. However, deductibles and co–pays are both fixed amounts, as opposed to coinsurance, which is a percentage of the claim.
On some health plans, certain services are covered with a co-pay before you’ve met the deductible, while other health insurance plans have co-pays only after you’ve met your deductible. And, the pre-deductible versus post-deductible co-pay rules often vary based on the type of medical service you’re receiving.
Starting in June 2025, Cleveland Clinic patients who can’t pay their co-pay on the spot will have non-emergency appointments rescheduled or cancelled. This new policy could make it harder for low-income people who prefer to be billed to see a clinic doctor, and create delays that could lead to medical emergencies down the road.
For example, a delay in care can mean six to eight more weeks of a tumor growing or a blood clot developing or an infection brewing.
Posted on May 16, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Oak Street Health, headquartered in Chicago and a wholly-owned subsidiary of CVS Health since 2023, has agreed to pay $60 million to resolve allegations that it violated the False Claims Act by paying kickbacks to third-party insurance agents in exchange for recruiting seniors to Oak Street Health’s primary care clinics.
The Anti-Kickback Statute prohibits anyone from offering or paying, directly or indirectly, any remuneration — which includes money or any other thing of value — to induce referrals of patients or to provide recommendations of items or services covered by Medicare, Medicaid and other federally funded programs. Under the Medicare Advantage (MA) Program, also known as Part C, Medicare beneficiaries have the option to obtain their health care through privately-operated insurance plans known as MA plans. Some MA Plans contract with health care providers, including Oak Street Health, to provide their plan members with primary care services.
The United States alleged that, in 2020, Oak Street Health developed a program to increase patient membership called the Client Awareness Program. Under the Program, third-party insurance agents contacted seniors eligible for or enrolled in Medicare Advantage and delivered marketing messages designed to generate interest in Oak Street Health. Agents then referred interested seniors to an Oak Street Health employee via a three-way phone call, otherwise known as a “warm transfer,” and/or an electronic submission.
In exchange, Oak Street Health paid agents typically $200 per beneficiary referred or recommended. These payments incentivized agents to base their referrals and recommendations on the financial motivations of Oak Street Health rather than the best interests of seniors. The settlement resolves allegations that, from September 2020 through December 2022, Oak Street Health knowingly submitted, and caused the submission of, false claims to Medicare arising from kickbacks to agents that violated the Anti-Kickback Statute.
Posted on May 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
History of Spinal Cord Injury Awareness Day
The first mention of spinal cord injuries was in the ancient Egyptian Edwin Smith’s papyrus from 2,500 B.C. The ancient Egyptian physicians described the injury as “untreatable.”
The first treatment for spinal cord injuries occurred in ancient India, where Hindu doctors used traction techniques to straighten the spine. The Greeks also employed the same technique as the Hindus. For example, Hippocrates — born in the 5th century B.C. — developed traction devices that helped straighten patients’ spines. It wasn’t until the second century A.D. that Galen, a Greek physician, discovered the relation between spinal cord injuries and loss of autonomic function and sensation.
Paul of Aegina, born in 625 A.D., became the first physician to pioneer surgical techniques for spinal cord injuries. He employed laminectomy to relieve pressure on the spine and recommended using a windlass to reduce the dislocation. The notion and treatment remained the same until the latter half of the 20th century; physicians continued to believe that spinal cord injuries were incurable. Although during the Renaissance, Leonardo da Vinci and Andreas Vesalius, made contributions to S.C.I. through their accurate depiction of the human spine and nerves.
In 1981, the Canadians Albert Aguayo and Sam David ended the millennia-long belief that S.C.I. is incurable. Through experiments on rats, they showed that axons could regenerate in the central nervous system in the right environment. The introduction of imaging, surgery, medical care, and rehabilitation medicine in the mid-20th century helped improve the care for spinal cord injuries and increased the life expectancy of those living with the condition.
Posted on May 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Classic Definition: In our hemisphere, there is the mystery of the Cuban health care paradox.
Modern Circumstance: This small island country whose economy produces about $6,000 in goods and services per person annually, a mere fraction of U.S. economic activity, lacks access to many commonly used drugs. Specialty medical care is scarce, and obesity rates are high and growing.
Paradox Example: Yet Cuba paradoxically boasts a life expectancy that surpasses the U.S. by six months. So, could this finding be explained by their diet, too, one that is rich in fresh produce, but low in saturated fats?
Question: Or, might it be related to their accessibility to primary care services and high compliance rates of childhood vaccination?
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Posted on May 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
BREAKING NEWS
***
***
UnitedHealth Group just announced the exit of CEO Andrew Witty and suspended its 2025 forecast due to surging medical costs, sending its shares down more than 10%. Chairman Stephen Hemsley will become CEO, effective immediately.
The fourth-largest U.S company big revenue in 2024, Minnetonka-based UnitedHealth has experienced a turbulent year that saw the shock killing of United Healthcare CEO Brian Thompson in New York City, and a cyberattack that affecting an estimated 190 million people and cost the company an estimated $3.1 billion dollars.
Virtual chronic care provider Omada Health has filed to go public in the United States, the latest in a string of healthcare listings expected this year. Omada did not disclose the details as to how much it plans to raise from its IPO.
The San Francisco, California-based company, which last raised $192 million in a Series E funding round in 2022, reported a 38% increase in revenue to $169.8 million for 2024, according to its IPO paperwork. For the first quarter of 2025, the company posted a 56.6% year-on-year jump in revenue to $55 million. Omada has applied to list its common stock on the NASDAQ under the symbol “OMDA”.
Healthcare IPOs on U.S. exchanges have fetched $7.1 billion in 2024, compared with $2.8 billion a year earlier, according to data compiled by LSEG.
Posted on May 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters and ChatGPT
***
***
President Trump to bring down prescription costs
In a Sunday post to Truth Social, President Trump signed an executive order at 9 am today to institute a most-favored-nation policy with pharmaceutical companies that he predicted could lower drug prices by 30% to 80%.
“The United States will pay the same price as the Nation that pays the lowest price anywhere in the World,”
While Americans pay more for pharmaceuticals than any other country, Bloomberg reported that the American market fuels innovation and drives growth in the industry. Drug makers have pushed back on previous efforts to revamp the system in the US, saying it would make revenue evaporate and hinder the development of potentially lifesaving drugs.
Financial Advisor, Planner and Insurance Agent Information
By Staff Reporters
***
***
Ostrich Bias is a behavioral phenomenon describing the tendency of individuals to avoid or ignore information that they perceive as negative or threatening. This term is derived from the popular but inaccurate belief that ostriches bury their heads in the sand when faced with danger, even though they do not exhibit such behavior.
Evidence: There is neuro-scientific evidence of the ostrich effect. Sharot et al. (2012) investigated the differences in positive and negative information when updating existing beliefs. Consistent with the ostrich effect, participants presented with negative information were more likely to avoid updating their beliefs; wills, estate plans, investment portfolios, and insurance policies, etc..
Moreover, they found that the part of the brain responsible for this cognitive bias was the left IFG – inferior frontal gyrus – by disrupting this part of the brain with TMS – transcranial magnetic stimulation – participants were more likely to accept the negative information provided.
EXAMPLE: The Ostrich Bias can cause someone to avoid looking at their bills, because they’re worried about seeing how far behind they are on home mortgage payments, credit cards, education or auto loans, etc.
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals.
Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed.
Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Posted on May 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITION
By Staff Reporters
***
***
Classic: Despite a wide variety of empirical methods and data sources, the demand for health care is consistently found to be price inelastic
Modern: If you are sick, you will not be very price sensitive. There are exceptions to this rule (e.g., elective surgery such as plastic surgery, purchases of eyeglasses) but most studies find that patients are fairly insensitive to changes in health care prices.
Examples: For instance, the RAND Health Insurance Experiment found that the price elasticity of medical expenditures is -0.2.
***
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Posted on May 4, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants LLC
***
***
During the first 90 days of the Republican Party’s government trifecta (controlling the White House, Senate, and House of Representatives), both the Trump Administration and Congress have laid the groundwork for seismic change to the U.S. healthcare industry.
In an attempt to track the latest actions of the federal government’s legislative and executive branches affecting the healthcare industry since the first installment in our February issue, this Health Capital Topics article summarizes recent events in Washington and the impact of these changes on providers and patients. (Read more…)
An emergency medicine physician is a medical doctor who specializes in the diagnosis, treatment, and management of acute and life-threatening medical conditions that require immediate intervention. These physicians work in hospital emergency departments, urgent care centers, and other acute care settings, where they provide rapid assessment, stabilization, and treatment to patients of all ages with a wide range of medical emergencies.
Emergency medicine physicians are trained to handle diverse medical emergencies, including trauma, cardiac emergencies, respiratory distress, severe infections, neurological emergencies, and obstetric emergencies, among others. They play a vital role in the front line management of medical emergencies, ensuring that patients receive prompt and appropriate care to improve outcomes and save lives.
***
Classic: Emergent Room or Emergency Department care is the provision of immediate medical service offering outpatient care for the treatment of acute and chronic illness and injury. It requires a broad and comprehensive fund of knowledge to provide such care. Excellence in care for patients with complex and or unusual conditions is founded on the close communication and collaboration between the urgent care medicine physician, the specialists and the primary physicians.
Modern: Urgent care does not replace your primary care physician. An urgent care center is a convenient option when someone’s regular physician is on vacation or unable to offer a timely appointment. Or, when illness strikes outside of regular office hours, urgent care offers an alternative to waiting for hours in a hospital Emergency Room.
Examples: Chest pain, bleeding that cannot be stopped and loss of consciousness; etc.
***
***
SOME ER DOCTORS WORK FOR FREE
The new president of emergency medicine for the Alberta Medical Association says Emergency Room physicians already coping with long hours, staff shortages and jammed waiting rooms are also being obligated, in some cases, to work for free. Dr. Warren Thirsk says the government has yet to follow through on a promise to reimburse emergency room doctors for so-called “good faith” payments.
“There’s been lots of excuses, but the bottom line is no one has actually received a penny for those suspended good-faith payments,” Thirsk said in an interview. “On average, every emergency physician in this province is out thousands of dollars for free work.” Good-faith payments reimburse ER doctors when they see patients who don’t have identification and can’t prove an Alberta Health Care Insurance Plan billing number.
Thirsk said the United Conservative government stopped those payments when it ripped up the master agreement with the AMA in early 2020. He said it promised to bring back those payments when the two sides agreed to a new deal in September 2022. But to date that hasn’t happened, he said.
“I’m legally and morally bound to look after you [if] you’re unidentified [as a patient],” said Thirsk, an emergency room doctor at Edmonton’s Royal Alexandra Hospital.
“I’m going to look after you because it’s the right thing to do no matter what the problem is.”
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Some retired people live on a fixed income and many of them live right on the edge of their financial capability. At some time in their life, they may have to make a choice regarding many purchases.
In this case, we will illustrate “choice” using a couple’s purchase of Long-Term-Care Insurance [LTCI]. Of course, economics is the study of choice; wants, needs and scarcity, etc. In our case, if they decide to make the purchase they commit to a lifetime of premium payments. The financial tradeoff is this; if they make the commitment to purchase LTCI, they must give up something else.
EXAMPLE: In order to maintain a monthly premium of $100 ($1,200per year), an elderly patient, retired layman or couple must essentially relegate about $30,000 of financial assets to generate the $100 necessary to make an average premium payment (assumes a 7% rate of return with 4% withdrawal rate) or [4% X $30,000 = $1,200 year]. Thus, if the monthly premium cost is $500 per month, the elder must give up the use of $150,000 of retirement asset just to generate enough cash flow to pay for the LTC insurance.
***
***
The married elder couple has to make the Hobson’s Choice decision among lifestyle (dinners, vacations, gifts to children, prescription drugs, medical care or food and shelter) versus paying an insurance premium to provide for nursing home coverage for a need, which may be very real, but will not occur until sometime in the ambiguous future.
And so, when faced with such a tough economics Hobson’s Medicine Choice, neither of which delivers peace of mind or a respectable solution; many will simply decide that, in either case, they may already end up impoverished. Thus, many will often opt for the better lifestyle now … while they can enjoy it … together.
Cite: Anonymous Health Insurance Agent, Norcross, Georgia
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals.
Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed.
Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Posted on May 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Meta Platforms jumped 4.23% after the big tech giant reported that its advertising revenue came in at $41.39 billion, beating analyst projections of $40.44 billion, thanks to higher ad price growth than expected. Daily active users rose to 3.43 billion, up from 3.35 billion last quarter, while nearly 1 billion people use its digital AI assistant every month. Management expects Q2 sales to come in between $42.5 billion and $45.5 billion, in-line with analyst forecasts of $44.03 billion.
EPS: $6.43 per share, crushing estimates of $5.28
Revenue: $42.31 billion, above the $41.10 expected
Microsoft leaped 7.63% after reporting its profit jumped a staggering 18% from a year earlier. That wasn’t the only good news: Revenue from Microsoft’s Azure cloud software grew 33% year over year, higher than the 31% expected by analysts. But perhaps the best news of all was management’s upbeat guidance—Microsoft projected revenue between $73.15 billion and $74.25 billion for the current quarter, well above expectations of $72.26 billion.
EPS: $3.46 per share, beating forecasts of $3.22
Revenue: $70.07 billion, above the $68.42 billion projected
Eli Lilly dropped 11.66% today, despite the fact that the pharmaceutical giant reported that sales skyrocketed 45% year over year thanks to its lucrative GLP-1 drugs, Zepbound and Mounjaro. Two things spooked investors today: The company lowered its profit outlook well below its preview estimate due its acquisition of a cancer drug from Scorpion Therapeutics, and CVS Health dropped Zepbound from its preferred drug list in lieu of arch-rival Novo Nordisk’s Wegovy this morning.—LB
EPS: $3.34 adjusted, beating the $3.02 expected
Revenue: $12.73 billion, compared to the $12.67 projected
Carrier Global climbed 11.61% after the air conditioning company boosted its fiscal forecast. Turns out everyone needs AC regardless of economic uncertainty.
People also need straight teeth: Dental products manufacturer Align Technology rose 1.98% on solid earnings.
Quanta Services gained 9.99% after the construction engineering company beat Wall Street estimates on both the top and bottom line.
What’s down
Qualcomm may have beaten earnings expectations, but shares fell 8.92% after investors were disappointed by the chipmaker’s lower guidance.
GM was in the same boat: Earnings beat forecasts, but poor guidance and warnings that tariffs could cost the company up to $5 billion this year pushed shares 0.42% lower.
Robinhood Markets enjoyed a 50% increase in revenue last quarter as traders played the volatile market, but the stock still sank 5.07%.
Moderna fell 5.29% after the vaccine maker missed revenue expectations and said it’s planning another $1.5 billion in cost cuts.
Church & Dwight, maker of household goods like Arm & Hammer Baking Soda, missed revenue forecasts last quarter and sank 6.87%.
Becton Dickinson & Co. lost 18.13% after the medical device maker warned of the adverse effects of, what else, tariffs.
Posted on May 1, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants LLC
***
***
While the healthcare industry has been dealing with high employee turnover since the start of the COVID-19 pandemic, that turnover was largely among clinical staff.
However, a recent survey found that significant healthcare leadership turnover may also be on the horizon. AMN Healthcare subsidiary B.E. Smith found that nearly half of healthcare executives plan to leave their organization in the next year.
This Health Capital Topics article reviews the survey and the reasons behind the intended exits. (Read more…)
Posted on April 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants LLC
***
***
On April 7, 2025, the Centers for Medicare & Medicaid Services (CMS) published their 2026 Rate Announcement for Medicare Advantage (MA) and Medicare Part D Prescription Drug Plans.
For 2026, the payment rate to MA plans will increase 5.06%, the largest increase in the past ten years, and up significantly from the 2.2% rate increase proposed by the Biden Administration.
This Health Capital Topics article will review the Rate Announcement.(Read more…)
In a discussion of competitive healthcare economic models, assumptions must include normal demand quantities, many fully informed patients and the fact that physicians cannot directly influence demand for medical care. These assumptions, although fluid, also preclude that patient buyers are large enough to have any influence over price and result in the following”:
In a “pure monopoly”, there is only one provider with a unique service. The doctor is a “price maker” and charges whatever s/he wishes.
In an “oligopoly”, there are a few physicians who provide similar services. For example, when it becomes clear to Dr. Smith and Dr. Jones that neither can win their price war, oli-gopolists return prices to prior, but still inflated levels!
In “monopolistic competition”, there are many providers with differentiated services. For example, should Dr. Jones decide to have evening hours, she may charge a premium for her fees if Dr. Jones doe not follow suit.
Finally, when “pure competition” occurs, there are many physicians, providing providing similar and substitutable services. Marketing and advertising does not affect fees, and prices are determined by supply and demand. The doctors become “price takers” by accepting fees arrived at by practicing competitively.
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals.
Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed.
Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Posted on April 24, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
OpenAI would be open to buying Chrome if Google is forced by a federal court to sell the web browser, the company’s ChatGPT head said yesterday.
The FDA suspended milk quality tests in some dairy products due to reduced capacity stemming from federal workforce cuts, Reuters reported.
Roche, the Swiss pharmaceutical giant, is investing $50 billion in US manufacturing to circumvent President Trump’s tariffs, the company said yesterday.
Rite Aid is preparing to sell itself in pieces ahead of a possible second bankruptcy, Bloomberg reported.
Oklo gained 8.60% after OpenAI CEO Sam Altman announced he’s stepping down as chairman of the board of the nuclear power startup.
Duolingo popped 10.01% after Morgan Stanley initiated coverage of the language learning company, calling it a “best-in-class consumer internet asset.”
Cava climbed 6.29% due to an upgrade from analysts at Bernstein, who think the bowl slop stock will not only survive but thrive in an economic downturn.
Amphenol rose 8.21% thanks to impressive earnings for the high-speed cable company, coupled with a solid fiscal outlook.
Vertiv Holdings jumped 8.60% after the data center company posted an impressive quarterly profit and raised its fiscal forecast.
Stocks surged first thing this morning after President Trump said the media blew things out of proportion and that he has “no intention” of firing Jerome Powell. He also said he would be “very nice” to China in tariff negotiations.
Treasury Secretary Scott Bessent also did some damage control, touting the opportunity for a “big deal” between the US and China.
The combination sent a relief rally sweeping through markets, and while the euphoria faded by mid-afternoon, all three indexes ended the day in the green.
Gold fell and bitcoin rose as investors took on more risk (see below), while oil dropped on reports that OPEC+ may hike its crude output after its meeting next month.
Classic: An arrangement by which a patient requests that their health benefit payments be made directly to a designated person or facility, such as a physician or hospital. It is a legally binding agreement between patient and Insurance company asking them to send your reimbursement checks directly to your doctor.
Modern: To accept assignment means that the provider agrees to accept what ever the insurance company allows or approves as payment in full for the claim. The patient signs paperwork requiring his health insurance provider to pay his physician or hospital directly. EXAMPLES:
CMS: The approved amount, also known as the Medicare-approved amount, is the fee that Medicare sets as how much a provider or supplier should be paid for a particular service or item. Original Medicare calls this “assignment.”
Tardiness: When a medical office accepts an assignment of benefits, the insured patients may have to wait several months for their insurance reimbursement to arrive.
Classic: It’s no surprise that people are more honest when they know that they’re being watched. But what about just reminding them of the idea of being watched, without them actually being watched?
Modern: Researchers at the University of Newcastle’s Division of Psychology have an honor (or trust) system where they are requested to deposit payment for coffee in an “honesty box.” There was a note saying how much they should pay.
In 2006, Dr. Melissa Bateson and colleagues decided to do a little experiment: they placed an image above the note. They alternate between two pictures: one week they would use a picture of alleged human eyes and the other week, flowers. After 10 weeks, they plotted the amount of money received versus drinks consumed and found that people paid nearly three times as much for their drinks when eyes were displayed.
“There’s an argument that if nobody is watching us it is in our interests to behave selfishly. But when we think we’re being watched we should behave better, so people see us as co-operative and behave the same way towards us,” — Dr Bateson said
EXAMPLE:
Tax: This has great exemplar potential in things like federal, state and local income tax preparation, etc.
Insight: “It’s a definite that you’re all going to screw up, but it’s not a definite that any of you will learn from that,” declared one of our medical school instructors, years ago. “Cultivate the attitude that allows you to own your mistakes, and then, not repeat them” — reported Monique Tello MD MPH.
Posted on April 15, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Stocks kept the good vibes going for a second trading day yesterday with tech companies like Apple rising as investors reacted to the weekend’s news that smartphones and computers would be temporarily exempt from “reciprocal” tariffs—at least until new semiconductor tariffs are imposed.
Car companies also jumped after President Trump suggested he wanted to “help” as automakers try to transition their production to the US in the face of 25% auto tariffs.
Posted on April 15, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
A recent study published in the Annals of Internal Medicine found that in 2021, UnitedHealth Group received just under $14 billion in extra Medicare Advantage payments after using a code that made its members appear sicker. It’s another tough break for the plan and provider that has faced allegations of illegally taking additional money from patients and taxpayers, especially after its CEO was fatally shot in early December.
US stocks edged higher on Monday as investors focused on tech’s temporary reprieve from President Trump’s tariffs.
The S&P 500 (^GSPC) trimmed bigger gains to rise a healthy 0.8%. The tech-heavy NASDAQ (^IXIC) also closed off its session high, up 0.6%. The Dow Jones Industrial Average (^DJI) was up around 0.7%, or more than 300 points.
Posted on April 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
🟢 What’s up
Auto stocks soared on comments from President Trump that car companies “need a little bit of time.” GM rose 3.48%, Ford climbed 4.13%, and Stellantis gained 5.64%.
Investors are bullish: WeBull exploded 374.72% after the online investment platform went public via SPAC merger last Friday.
Goldman Sachs rose 1.87% after the Wall Street titan announced record revenue in its equities-trading business thanks to stock market volatility in the first quarter.
Palantir gained 4.60% after it sealed a deal with NATO to provide the organization with its advanced AI-powered warfighting system.
Intel climbed 2.89% on news that it will sell a 51% stake in its programmable chips unit Altera to Silver Lake Management.
Pfizer somehow rose 0.96% despite announcing that it is discontinuing the development of a once-daily weight-loss pill after a patient experienced a liver injury. That’s great news for Viking Therapeutics, which has its own oral weight-loss pill in the pipeline. Shares of Viking rose 10.58%.
Speaking of biotech stocks, Verve Therapeutics soared 26.38% after the company reported no issues with patients trialing its new gene-editing technology.
What’s down
Meta Platforms fell 2.22% as its antitrust trial began today. If it loses its case against the FTC, it may be forced to sell off Instagram.
DaVita sank 3.03% after the kidney disease treatment company announced it was the victim of a ransomware attack.
Hilton Worldwide Holdings fell 1.10% on a downgrade from Goldman Sachs analysts, who believe the vacation club company will struggle as fewer people splurge on travel. Marriott International received the same treatment, and also dropped 0.77%.
LVMH Moet Hennessy Louis Vuitton (really rolls off the tongue) tumbled 6.39% after the luxury goods retailer missed analyst expectations, reporting a 3% decline in sales compared to forecasts of 2% growth.
It’s a bit broad, but Citi analysts downgraded all US stocks to “neutral” this morning. The analysts argued that US stocks are too exposed to President Trump’s policies and are expensive compared to international peers, and endorsed investing in Japanese, European, and UK equities instead.
An alternative investment is a financial asset that does not fall into one of the conventional investment categories. Conventional categories include stocks, bonds, and cash. Alternative investments can include private equity or venture capital, hedge funds, managed futures, art and antiques, commodities, and derivatives contracts. Real estate is also often classified as an alternative investment.
QUESTION: But what about a medical, podiatric or dental practice?
***
***
AnAlternate Asset Class Surrogate?
A medical practice is much like an alternative investment [AI], or alternate asset class in, two respects.
First, it provides the work environment that generates personal income which has been considered generous, to date.
Second, it has inherent appreciation and sales value that can be part of an exit (retirement) or succession planning transfer strategy.
Conclusion
So, unlike the emerging thought that offers Social Security payments as a surrogate for an asset classes; or a federally insured AAA bond – a medical practice might also be considered by some folks as an asset class within a well diversified modern investment portfolio.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Financial Modeling is one of the most highly valued, but thinly understood, skills in financial analysis. The objective of financial modeling is to combine accounting, finance, and business metrics to create a forecast of a company’s future results.
According to Jeff Schmidt, a financial model is simply a spreadsheet, usually built in Microsoft Excel, that forecasts a business’s financial performance into the future. The forecast is typically based on the company’s historical performance and assumptions about the future and requires preparing an income statement, balance sheet, cash flow statement, and supporting schedules (known as a three-statement model, one of many types of approaches to financial statement modeling). From there, more advanced types of models can be built such as discounted cash flow analysis (DCF model), leveraged buyout (LBO), mergers and acquisitions (M&A), and sensitivity analysis
***
DEFINED TERMS
Discounted Cash Flow (DCF): A valuation method used to estimate the value of an investment based on its expected future cash flows, adjusted for the time value of money. It’s like deciding whether a treasure chest is worth diving for now, based on the gold coins you’ll be able to cash in later.
Sensitivity Analysis: This involves changing one variable at a time to see how it affects an outcome. Imagine tweaking your coffee-to-water ratio each morning to achieve the perfect brew strength.
Budget – A budget is the amount of money a department, function, or business can spend in a given period of time. Usually, but not always, finance does this annually for the upcoming year.
Rolling Forecast – A rolling forecast maintains a consistent view over a period of time (often 12 months). When one period closes, finance adds one more period to the forecast.
Topside – A topside adjustment is an overlay to a forecast. This is typically completed by the corporate or headquarter team. As individual teams submit a forecast, the consolidated result might not make sense or align with expectations. When this occurs, the high-level teams use a topside adjustment to streamline or adjust the consolidated view.
Monte Carlo Simulation: Picture yourself at the casino, but instead of gambling your savings away, you’re using this technique to predict different outcomes of your business decisions based on random variables. It’s like playing financial roulette with the odds in your favor.
What-If Analysis: Ever daydream about what would happen if you took that leap of faith with your business? This tool allows you to explore various scenarios without risking a dime. It’s like trying on outfits in a virtual dressing room before making a purchase.
Leveraged Buyout (LBO) Model: This is a bit like orchestrating a heist, but legally. It’s about acquiring a company using borrowed money, with plans to pay off the debts with the company’s own cash flows. High stakes, high rewards.
Mergers and Acquisitions (M&A) Model: Picture two puzzle pieces coming together. This model evaluates how combining companies can create a new, more valuable entity. It’s the corporate version of a matchmaker.
Three Statement Model: The holy trinity of financial modeling, linking the income statement, balance sheet, and cash flow statement. It’s like weaving a tapestry where each thread is crucial to the overall picture.
Capital Asset Pricing Model (CAPM): A formula that calculates the expected return on an investment, considering its risk compared to the market. It’s like choosing the best roller coaster in the park, balancing thrill and safety.
Cash Flow Forecasting: This is your financial weather forecast, predicting the cash flow climate of your business. It helps you plan for sunny days and save for the rainy ones.
Cost of Capital: The price of financing your business, whether through debt or equity. It’s like the interest rate on your growth engine, pushing you to maximize every dollar invested.
Debt Schedule: A timeline of your business’s debts, showing when and how much you owe. It’s your roadmap to becoming debt-free, one milestone at a time.
Equity Valuation: Determining the value of a company’s shares. It’s like assessing the worth of a rare gemstone, ensuring investors pay a fair price for a piece of the treasure.
Financial Leverage: Using debt to amplify returns on investment. It’s like using a lever to lift a heavy object, increasing force but also risk.
Forecast Model: A crystal ball for your finances, projecting future performance based on past and present data. It’s your guide through the financial wilderness, helping you navigate with confidence.
Operating Model: A detailed blueprint of how a business generates value, mapping out operational activities and their financial impact. It’s like laying out the inner workings of a clock, ensuring every gear turns smoothly.
Revenue Growth Model: This tracks potential increases in sales over time, charting a course for expansion. It’s like plotting your ascent up a mountain, anticipating the effort required to reach the summit.
Posted on April 9, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Just after midnight, President Trump’s “reciprocal” tariffs went into effect against 86 countries. Analysts have estimated that the new US average effective tariff rate is north of 20%, the highest in more than 100 years. Ahead of the tariff deadline, markets swung violently, mostly way down: According to Bloomberg’s Cameron Crise, yesterday was the fourth straight trading day when the S&P 500’s trading range was 5% or more. That’s only happened in 1987, 2008, and 2020.
***
***
The Apple A18 and Apple A18 Pro are a pair of 64-bit ARM-based system on a chip (SoC) designed by Apple Inc., part of the Apple silicon series. They are used in the iPhone 16 and iPhone 16 Pro lineups and the iPhone 16e, and built on a second generation 3 nm process by TSMC.
***
Yesterday, for several hours on Tuesday, it looked like stocks were going to regain some of the ground lost during the market’s very bad week. But after the Trump administration made it clear that its increased tariffs on China would go into effect, all three indexes plunged. Apple, which makes most of its iPhones in China, was hit harder than many of its Big Tech peers.
So shoppers are thinking it’s better to have an Apple A18 processor and not need it, than to need it and not have it. Apple customers are scrambling to buy new iPhones out of fear that the company could raise prices to offset President Trump’s tariffs.
Employees at locations throughout the US said they’re being bombarded with questions about potential price hikes and have witnessed customers panic-buying phones. Though Apple declined to comment to Bloomberg, its retail stores reportedly saw higher sales over the last weekend than in previous years.
Posted on April 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
ACCOUNTABLE CARE ORGANIZATIONS
Realizing Equity, Access, and Community Health
By Staff Reporters
***
***
Model Overview
The ACO REACH Model provides novel tools and resources for health care providers to work together in an ACO to improve the quality of care for people with Traditional Medicare. REACH ACOs are comprised of different types of providers, including primary and specialty care physicians.
The ACO REACH Model makes important changes to the previous Global and Professional Direct Contracting (GPDC) Model which include:
***
***
Promote Provider Leadership and Governance. The ACO REACH Model includes policies to ensure doctors and other health care providers continue to play a primary role in accountable care. At least 75% control of each ACO’s governing body generally must be held by participating providers or their designated representatives, compared to 25% during the first two Performance Years of the GPDC Model. In addition, the ACO REACH Model goes beyond prior ACO initiatives by requiring at least two beneficiary advocates on the governing board (at least one Medicare beneficiary and at least one consumer advocate), both of whom must hold voting rights.
Protect Beneficiaries and the Model with More Participant Vetting, Monitoring and Greater Transparency. CMS will ask for additional information on applicants’ ownership, leadership, and governing board to gain better visibility into ownership interests and affiliations to ensure participants’ interests align with CMS’s vision. We will employ increased up-front screening of applicants, robust monitoring of participants, and greater transparency into the model’s progress during implementation, even before final evaluation results, and will share more information on the participants and their work to improve care. Last, CMS will also explore stronger protections against inappropriate coding and risk score growth.
Stocks were decimated yesterday in the first full trading day following President Trump’s tariff announcement. It was the biggest single-day decline since the start of the Covid-19 pandemic in March 2020. Every Magnificent Seven stock was battered—Apple worst of all. And so perhaps it is a good time to discuss the concept of “Money Scripts”.
***
Money Scripts are unconscious beliefs about money that are typically only partially true, are developed in childhood, and drive adult financial behaviors. Money scripts may be the result of “financial flashpoints,” which are salient early experiences around money that have a lasting impact in adulthood. Money scripts are often passed down through the generations and social groups often share similar money scripts. And so, we argue that Money scripts are at the root of all illogical, ill-advised, self-destructive, or self-limiting financial behaviors.
In research at Kansas State University [KSU], researchers identified four distinct Money script patterns, which are associated with financial health and predict financial behaviors. These include: (a) money avoidance, (b) money worship, (c) money status, and (d) money vigilance [personal communication Brad Klontz, PsyD, CFP®, Kenneth Shubin-Stein, MD, MPH, MS, CFA and Sonya Britt, PhD, CFP®].
And so, we all like to think our financial decisions are fully rational, but the truth is that our subconscious beliefs have a dramatic impact on our money and financial decisions. These money scripts are important to know and understand. A summary is below:
Money Avoidance
Money avoidance scripts are illustrated by beliefs such as “Rich people are greedy,”“It is not okay to have more than you need,” and “I do not deserve a lot of money when others have less than me.” Money avoiders believe that money is bad or that they do not deserve money. They believe that wealthy people are corrupt and there is virtue in living with less money. They may sabotage their financial success or give money away even though they cannot afford to do so. Money avoidance scripts may be associated with lower income and lower net worth and predict financial behaviors including ignoring bank statements, overspending, financial dependence on others, financial enabling of others, and having trouble sticking to a budget.
Money Worship
Money worship is typified by beliefs such as “More money will make you happier,” “You can never have enough money,” and “Money would solve all my problems.” Money worshipers are convinced that money is the key to happiness. At the same time, they believe that one can never have enough. Money worships have lower income, lower net worth, and higher credit card debt. They are more likely to be hoarders, spend compulsively, and put work ahead of family.
Money Status
Money status scripts include “I will not buy something unless it is new,” “Your self-worth equals you net worth,” and “If something isn’t considered the ‘best’ it is not worth buying.” Money status seekers see net worth and self-worth as being synonymous. They pretend to have more money than they do and tend to overspend as a result. They often grew up in poorer families and believe that the universe should take care of their financial needs if they live a virtuous life. Money status scripts are associated with compulsive gambling, overspending, being financially dependent on others, and lying to one’s spouse about spending.
Money Vigilance
Money vigilant beliefs include “It is important to save for a rainy day,” “You should always look for the best deal, even if it takes more time,” and “I would be a nervous wreck if I did not have an emergency fund.” The money vigilants are alert, watchful and concerned about their financial welfare. They are more likely to save and less likely to buy on credit. As a result, they tend to have higher income and higher net worth. They also have a tendency to be anxious about money and are secretive about their financial status outside of their household. While money vigilance is associated with frugality and saving, excessive anxiety can keep someone from enjoying the benefits that money can provide.
Identification
When money scripts are identified, it is helpful to examine where they came from. A simple behavioral finance technique involves reflecting on the following questions:
What three lessons did you learn about money from your mother?
What three lessons did you learn about money from your father?
What is your first memory around money?
What is your most painful money memory?
What is your most joyful money memory?
What money scripts emerged for you from this experience?
How have they helped you?
How have they hurt you?
What money scripts do you need to change?
Conclusion
Ideally, from a balanced middle ground, we can see past the limitations of money scripts, our self and others who are polarized. Those who believe “Money is meant to be spent” or “Money is meant to be saved” have a world view that results in extreme positions. Labeling them as “correct” or “wrong” is not a useful way to try to shift anyone’s polarized money script beliefs.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com