BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on October 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
A paradox is a logically self-contradictory statement or a statement that runs contrary to one’s expectation. It is a statement that, despite apparently valid reasoning from true or apparently true premises, leads to a seemingly self-contradictory or a logically unacceptable conclusion. A paradox usually involves contradictory-yet-interrelated elements that exist simultaneously and persist over time. They result in “persistent contradiction between interdependent elements” leading to a lasting “unity of opposites”.
THE TELE-MEDICINE PARADOX
Classic Definition: Refers specifically to the treatment of various medical conditions without seeing the patient in person. Healthcare providers may use electronic and internet platforms like live video, audio, PCs, tablets, or instant messaging to address a patient’s concerns and diagnose their condition remotely.
Modern Circumstance: This may include giving medical advice, walking them through at-home exercises, or recommending them to a local provider or facility. Even more exciting is the emergence of telemedicine apps which give patients access to care right from their phones or computer screens.
Paradox Examples: Treating certain conditions remotely can be challenging. Tele-medicine is often used to treat common illnesses, manage chronic conditions, or provide specialist services. If a patient is dealing with an emergent or serious condition, the remote provider suggests they seek in-person medical care.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on October 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
STOCKHOLM (AP) — Three researchers who probed the process of business innovation won the Nobel memorial prize in economics Monday for explaining how new products and inventions promote economic growth and human welfare, even as they leave older companies in the dust.
Their work was credited with helping economists better understand how ideas and technology succeed by disrupting established ways — a process as old as steam locomotives replacing horse-drawn wagons and as contemporary as e-commerce shuttering shopping malls.
The award was shared by Dutch-born Joel Mokyr, 79, who is at Northwestern University; Philippe Aghion, 69, who works at the Collège de France and the London School of Economics; and Canadian-born Peter Howitt, 79, who is at Brown University.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on October 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A. I.
***
***
Value-Based Medical Care: A Paradigm Shift in Healthcare
In recent years, the healthcare industry has undergone a transformative shift from volume-driven services to outcome-focused care. This evolution is embodied in the concept of value-based medical care, a model that emphasizes delivering high-quality healthcare while controlling costs and improving patient outcomes. Unlike traditional fee-for-service systems, which reward providers for the quantity of services rendered, value-based care aligns incentives with the value of care provided—measured by patient health outcomes relative to the cost of achieving them.
Core Principles of Value-Based Care
At its heart, value-based medical care is built on several foundational principles:
Patient-Centeredness: Care is tailored to individual needs, preferences, and values, promoting shared decision-making and holistic treatment.
Quality Over Quantity: Providers are rewarded for improving health outcomes, reducing hospital readmissions, and preventing disease rather than performing more procedures.
Integrated Care Delivery: Coordination among healthcare professionals ensures seamless transitions between services, reducing fragmentation and duplication.
Data-Driven Accountability: Performance metrics and health analytics guide clinical decisions and track progress toward better outcomes.
Cost Efficiency: By focusing on prevention and effective management of chronic conditions, value-based care aims to reduce unnecessary spending.
Benefits for Patients and Providers
For patients, value-based care offers a more personalized and proactive approach to health. It encourages preventive screenings, chronic disease management, and wellness programs that lead to longer, healthier lives. Providers benefit from shared savings programs, performance bonuses, and stronger relationships with their patients. Moreover, healthcare systems can allocate resources more effectively, reducing waste and improving overall population health.
Posted on October 6, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Fierce Healthcare [7/29/25]
***
***
UnitedHealthcare CEO Tim Noel offered investors a deeper look at the medical cost spike that’s plaguing the insurance giant’s finances. He said during the company’s earnings call that pricing assumptions set by the company “were well short of actual medical costs” for 2025. UHC’s current outlook, he said, instead reflects an additional $6.5 billion in medical costs, with more than half, or about $3.6 billion, coming from its Medicare plans.
Noel said that in Medicare Advantage specifically, the team is looking to adjust pricing and benefit designs to account for the cost pressures, which they anticipate will stretch into much of 2026.
It has also decided to exit certain markets largely with plans that are more loosely designed, such as PPOs, in a move that will impact 600,000 beneficiaries.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Population health has been defined as “the health outcomes of a group of individuals, including the distribution of such outcomes within the group”. It is an approach to health that aims to improve the health of an entire human population or cohort. http://www.HealthDictionarySeries.org
History
In fact, the nominal “father of population health” is colleague and Dean David B. Nash MD MBA of Jefferson Medical School in Philadelphia. And, although I attended Temple University down the street, David still wrote the Foreword to my textbook years later; Financial Management Strategies for Hospitals and Healthcare Organizations [Tools, Techniques, Checklists and Case Studies].
Now age, income, location, race, gender and education are just a few characteristics that differentiate the world’s population. These are called ”disparities” and they have a major impact on people’s lives; especially their healthcare. And, I’ve written about them before. Perform a ME-P “search” for more.
So, it’s only natural that we’re keeping an eye on two major demographic trends: aging baby boomers and maturing Millennials [1982-2002 approximately].
Why it’s important
The impact of large population shifts propagate throughout an economy benefitting certain sectors more than others and influencing a country’s growth prospects; tantalizing investing ideas?
Example:
For example, as baby boomers retire, we’ll likely see higher spending on health care, but less on education and raising children. Likewise, tech-savvy Millennials will likely prioritize consumption on experiences over cars and houses [leading economic indicator].
So, can we profit from these trends?
Assessment
Well maybe – maybe not! Overall economic prospects may not be completely affected by these trends. Spending habits on combined goods and services will shift, rather than rise or decline.
So, be careful. What matters most for your investment success is your demographics and investing according to your personal circumstances and goals [paradox-of-thrift].
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
Posted on October 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
On September 22, 2025, the Government Accountability Office (GAO) released a report estimating “the Extent and Effects of Physician Consolidation.” The GAO, the non-partisan audit, evaluation, and investigative arm of Congress, undertook the analysis of physician consolidation in response to lawmakers’ request.
This Health Capital Topics article reviews the GAO report and stakeholder reactions. (Read more…)
Classic: A pre-payment plan refers to health insurance plans that provide medical or hospital benefits in service rather than dollars, such as the plans offered by various Health Maintenance Organizations. A method providing in advance for the cost of predetermined benefits for a population group, through regular periodic payments in the form of premiums, dues, or contributions including those contributions that are made to a health and welfare fund by employers on behalf of their employees!
Modern: A Prepaid Group Practice Plan specifies health services are rendered by participating physicians to an enrolled group of persons, with a fixed periodic payment made in advance by (or on behalf of) each person or family. If a health insurance carrier is involved, a contract to pay in advance for the full range of health services to which the insured is entitled under the terms of the health insurance contract.
Examples:
Pre-Paid Hospital Service Plan: The common name for a health maintenance organization (HMO), a plan that provides comprehensive health care to its members, who pay a flat annual fee for services.
Pre-Paid Premium: An insurance or other premium payment paid prior to the due date. In insurance, payment by the insured of future premiums, through paying the present (discounted) value of the future premiums or having interest paid on the deposit.
Pre-Paid Prescription Plan: A drug reimbursement plan that is paid in advance.
ME-P readers might believe the hedge fund industry is a small, exclusive club of elites, rich investors. But a new count by Preqin shows that it’s actually a large—and growing—sector of investing.
In fact, there may be more hedge funds globally (30,000+) than Burger King locations (18,700), and more more hedge fund managers than Taco Bell managers, per the FTE
Posted on October 1, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
BREAKING NEWS!
UNITED STATES GOVERNMENT SHUTS DOWN
***
By Health Capital Consultants, LLC
***
***
With hours to go until the midnight deadline on September 30th, 2025 to fund the government, lawmakers appear deadlocked over whether certain healthcare provisions should be included in the temporary funding bill.
Should this deadlock continue, the federal government will shut down beginning today October 1st and remain shut down until that deadlock is resolved.
This Health Capital Topics article provides an update on the developing saga. (Read more…)
Hobson’s choice is a free choice in which only one thing is actually offered. The term is often used to describe an illusion that choices are available. The best known example is “I’ll give you a choice: Take it or leave it”, wherein “leaving it” is strongly undesirable.
The phrase is said to have originated with Thomas Hobson (1544–1631), a livery stable owner in Cambridge, England, who offered customers the choice of either taking the horse in the stall nearest to the door or taking none at all.
A CASE MODEL
Half of Physicians Plan to Change Career Paths
The Physicians Foundation recently conducted a survey on physician practice patterns and perspectives. Here are some key findings from the report:
• 31% of physicians identify as independent practice owners or partners. • Almost half (47%) of physicians plan to change career paths. • 78% of physicians sometimes, often or always experience feelings of burnout. • Nearly a quarter of physician time is spent on non-clinical paperwork.
This result is not a good Hobson’s Choice in Medicine.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 27, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
A paradox is a statement that appears at first to be contradictory, but upon reflection then makes sense. This literary device is commonly used to engage a reader to discover an underlying logic in a seemingly self-contradictory statement or phrase. As a result, paradox allows readers to understand concepts in a different and even non-traditional
***
***
GOVERNMENT HEALTH INFORMATION IS TRUSTED?
Classic Definition: Despite the PP-ACA, there is ambivalence about the role of the US Government as a source of quality healthcare information.
Modern Circumstance: Of brands presented to respondents in a Consumer Reports (50 percent), and AARP (37 percent) survey, they outpolled the “US Government Healthcare Quality Reporting Website” (36 percent) and Medicare Website (32 percent).
Paradox Example: The focus groups expressed “mixed reactions and raised doubts about government involvement in quality ratings information. At least one participant in each group expressed skepticism about trusting ‘the government’ to compile information.”
Younger consumers especially questioned the relevance of Medicare measures to the non-elderly population. Yet participants gravitated to “.gov” websites over “.org” websites as a more authoritative source.
CITE: Williams, Jason: Health Affairs, December 28, 2016
[An Internet WIKI CROWD-SOURCED Curation Project]*
To keep up with the ever-changing healthcare industrial complex, we must learn new definitions and re-learn old terminology in order to correctly apply it to practice. By aggregating the most up-to-date abbreviations, acronyms, definitions and terms, the Health DictionarySeries offers a wealth of information to help understand the ever-changing terms-of-art in healthcare today.
Each 10,000 item handbook is essential for doctors, nurses, benefits managers and insurance agents, CPAs, and administrators; as well as graduate and under graduate students and professors. Our goal to for each dictionary to be designated as a Doody’s Core Title.
Dictionary of Health Insurance and Managed Care
With more than 8,000 definitions, 4,000 abbreviations and acronyms, and a 3,000 item oeuvre of resources, readings, and nomenclature derivatives, this dictionary covers the Medicare, managed care and Medicaid, private insurance, Veteran’s Administration and PP-ACA language of the entire health and long-term care insurance sector.
Dictionary of Health Economics and Finance
Health economics and finance is an integral component of the health care industrial complex. Its language is a diverse and broad-based concept covering many other industries: accounting, mathematics, the actuarial sciences, stochastics and statistics, salary reimbursements, physician payments, compensation and forecasting are all commingled arenas.
Dictionary of Health Information Technology Security
There is a myth that all healthcare stakeholders understand the meaning of information technology jargon. In truth, the vernacular of contemporary systems is unique, and often misused or misunderstood. Moreover, emerging Heath Information Technology (HIT) thru the HITECG initiatives; in the guise of terms, definitions, acronyms, abbreviations and standards; often puts the non-expert in a position of maximum uncertainty and minimum productivity.
*NOTE: A wiki website allows users to add or update content using their browser thru a hosted server created by the collaborative effort of site visitors. The Hawaiian term “wiki wiki” means “super fast.”
A Financial Self Discovery Questionnairefor Medical Professionals
For understanding your relationship with money, it is important to be aware of yourself in the contexts of culture, family, value systems and experience. These questions will help you. This is a process of self-discovery. To fully benefit from this exploration, please address them in writing. You will simply not get the full value from it if you just breeze through and give mental answers. While it is recommended that you first answer these questions by yourself, many people relate that they have enjoyed the experience of sharing them with others who are important to them.
As you answer these questions, be conscious of your feelings, actually describing them in writing as part of your process.
Childhood
What is your first memory of money?
What is your happiest moment with Money? Your most unhappy?
Name the miscellaneous money messages you received as a child.
How were you confronted with the knowledge of differing economic circumstances among people, that there were people “richer” than you and people “poorer” than you?
Cultural heritage
What is your cultural heritage and how has it interfaced with money?
To the best of your knowledge, how has it been impacted by the money forces? Be specific.
To the best of your knowledge, does this circumstance have any motive related to Money?
Speculate about the manners in which your forebears’ money decisions continue to affect you today?
Family
How is/was the subject of money addressed by your church or the religious traditions of your forebears?
What happened to your parents or grandparents during the Depression?
How did your family communicate about money?
How? Be as specific as you can be, but remember that we are more concerned about impacts upon you than historical veracity.
When did your family migrate to America (or its current location)?
What else do you know about your family’s economic circumstances historically?
Your parents
How did your mother and father address money?
How did they differ in their money attitudes?
How did they address money in their relationship?
Did they argue or maintain strict silence?
How do you feel about that today?
Please do your best to answer the same questions regarding your life or business partner(s) and their parents.
Childhood: Revisited
How did you relate to money as a child? Did you feel “poor” or “rich”? Relatively? Or, absolutely? Why?
Were you anxious about money? Did you receive an allowance? If so, describe amounts and responsibilities.
Did you have household responsibilities?
Did you get paid regardless of performance?
Did you work for money?
If not, please describe your thoughts and feelings about that.
***
***
Same questions, as a teenager, young adult, older adult.
Credit
When did you first acquire something on credit?
When did you first acquire a credit card?
What did it represent to you when you first held it in your hands?
Describe your feelings about credit.
Do you have trouble living within your means?
Do you have debt?
Adulthood
Have your attitudes shifted during your adult life? Describe.
Why did you choose your personal path? a) Would you do it again? b) Describe your feelings about credit.
Adult attitudes
Are you money motivated? If so, please explain why? If not, why not? How do you feel about your present financial situation? Are you financially fearful or resentful? How do you feel about that?
Will you inherit money? How does that make you feel?
If you are well off today, how do you feel about the money situations of others? If you feel poor, same question.
How do you feel about begging? Welfare? If you are well off today, why are you working?
Do you worry about your financial future?
Are you generous or stingy? Do you treat? Do you tip?
Do you give more than you receive or the reverse? Would others agree?
Could you ask a close relative for a business loan? For rent/grocery money?
Could you subsidize a non-related friend? How would you feel if that friend bought something you deemed frivolous?
Do you judge others by how you perceive they deal with their Money? Do you feel guilty about your prosperity? Are your siblings prosperous?
What part does money play in your spiritual life?
Do you “live” your Money values?
Conclusion
There may be other questions that would be useful to you. Others may occur to you as you progress in your life’s journey. The point is to know your personal money issues and their ramifications for your life, work, and personal mission.
This will be a “work-in-process” with answers both complex and incomplete. Don’t worry.
Just incorporate fine-tuning into your life’s process.
Despite their high salaries, not all doctors are wealthy, and some live paycheck to paycheck. Here are 5 reasons why many doctors today are broke, according to https://medschoolinsiders.com
1 | Believing They Are Universally Smart
The first reason so many doctors are broke is that many doctors believe they are universally smart. While most doctors have deep specialized knowledge, there’s a big difference between being smart in your profession and being smart with money. A physician’s schooling is quite thorough when it comes to the human body, but med school doesn’t include a prerequisite class on how to handle finances.
Graduating medical school is a major feat and certainly demonstrates superior work ethic and cognitive abilities. But many new doctors believe these accomplishments transcend all aspects of life. If you’re smart enough to earn an MD, you’re certainly smart enough to handle your finances, but only once you properly and intentionally educate yourself.
The truth is doctors, especially traditional graduates, haven’t had an opportunity to manage large sums of money until they become fully trained attending physicians and start pulling in low to mid six figures in income. Prior to that, there was very little of it to manage.
Far too many aspiring doctors, and students in general, don’t take the time to learn financial basics, in part because it’s uncomfortable and seems like something they can figure out “later”, whenever that may be. Their poor spending habits and lack of investment knowledge carry over into their careers, causing many to make irresponsible decisions.
The second factor is overspending too soon, and this comes up at two points in training.
First, it’s natural to want to start spending more as soon as you get into residency and start making a little more money. After all, you’ve been a broke student for 8 or more years, and now you’re finally making a reasonable and reliable wage. But that’s where young doctors get into trouble. Residency pays, but not nearly as much as you will be making once you become an attending physician. The average resident makes about $60K a year, and if you begin spending all of that money right away, thinking you’ll handle your loans once you become an attending, you delay paying off your medical school debt, which means the compounding effect through your student loan interest rate works against you.
Now that $250,000 in student loans has ballooned to over $350,000 by the time you finish residency. The compounding effect, which can be one of your greatest allies in your financial life, becomes an equally powerful enemy when working against you through debt. But of course, pinching pennies is easier said than done, especially when you’re in residency and are surrounded by peers in different professions. They’ve been earning good money much longer than you have, and they can afford more luxurious lifestyles.
They may not be worried about indulging in fine dining or how much a hotel costs when traveling. Students in college and medical school are often confident they will resist the temptations, but the desire to keep up with your friends and family can be difficult to ignore, which causes many to overspend before they technically have the money to do so.
The same is true of attending physicians. As soon as those six-figure salaries come rolling in, many physicians go overboard with spending, trying to make up for lost time and to treat yourself.
Now, we are not suggesting you shouldn’t reward yourself for completing residency, but that reward shouldn’t be a Lamborghini. It’s best to continue living like a resident in your first few years after becoming an attending to pay off loans, put a down payment on a home, and get your financial foundation built before loosening the purse strings.
3 | Decreasing Salaries
Third, doctors continue to make less money than they did before. And this includes nearly all 44 medical specialties. For example, while physician compensation technically rose from $343k to $391k between 2017 and 2022, this rise does not keep up with inflation. The real average compensation in 2022 was less than $325k—a $20k decrease in purchasing power in only six years.
For doctors who are already spending to the limits of their salaries with huge mortgages, car payments, business costs, and other luxuries, a decreased salary can have a huge impact. You might be able to cut back by going on fewer vacations or eating out less frequently, but many accrued costs are locked in, such as a mortgage payment, car loan, or leased rental space for your practice.
4 | Increasing Costs of Private Practice
In the past, running a private practice was much simpler, but recent stricter guidelines and regulations have made it difficult for solo practices to keep up. While regulations like the Health Insurance Privacy and Portability Act, or HIPAA, and mandatory Electronic Medical Records, or EMRs, are necessary to protect patients, they make costs higher for physicians who run their own private practice. These physicians need to spend their own money to set up and maintain EMRs as well as invest in security to ensure patient data is protected.
With the steep rise of inflation we’ve seen over the past couple of years, everything is more expensive, which means costs, such as business space, equipment, and even office supplies, have gone up for private practice physicians while salaries have not. 2013 to 2020 saw an annual inflation rate of anywhere from 0.7% to 2.3%. This skyrocketed to an annual inflation rate of 7.0% in 2021 and another 6.5% in 2022. In fact, the cost of running a private practice has increased by almost 40% between 2001 and 2021.
These increased costs are exacerbated by another problem plaguing private practices; decreased reimbursement. While costs increased by almost 40%, Medicare reimbursement only increased by 11%. When doctors see patients who are insured, the insurance companies pay the physicians for their time. For Medicare, the new proposed rules for 2023 would cut reimbursement by around 5%. When adjusting for inflation, Medicare reimbursement decreased by 20% in the last 20 years.
These costs add up, making it extremely difficult for physicians to thrive financially while running a private practice.
5 | Tuition Debt
Lastly, we can’t talk about a doctor’s finances without mentioning the exorbitant debt so many graduating physicians are left with. It won’t shock you to hear that med school is expensive. Extremely expensive. The average cost of tuition for a single year is nearly $60k, with significant variance from school to school, and that’s before accounting for living expenses.
In-state applicants pay less than out-of-state applicants, and students at private schools typically pay more than students at public medical schools. The astronomical costs mean the vast majority of students can’t pay for medical school out of their own pockets. And unless your family is part of the 1%, even with your parents footing the bill, it’s difficult to cover tuition, let alone rent, groceries, transportation, tech, social activities, exam fees, and application costs.
The average total student debt after college and med school is over $250k. But keep in mind that’s the average, which includes 27% of students who graduate with no debt at all. This means the vast majority of students leave medical school owing much more than $250k.
For some perspective, in 1978, the average debt for graduating MDs was $13,500, which, when adjusted for inflation, is a little over $60,000. There are multiple ways to eventually repay these loans, but time and discipline are essential to ensure this money is paid off as quickly as possible.
According to financial advisor Dr. David Edward Marcinko MEd MBA CMP™; consider the following:
Place a portion of your salary (15-20% or more) into a savings account, and another portion (10-20% or more) into wise investments [stocks, bonds, mutual funds, and/or ETFs].
Pay off your bills each month, and then use leftover spending money to purchase fun things like vacations and fancy dinners, within your means. Shop sales, buy used clothes, and use credit card points for travel.
Hire an excellent tax professional and meet with an investment advisor once or twice a year about your investment status and strategy. http://www.MarcinkoAssociates.com
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
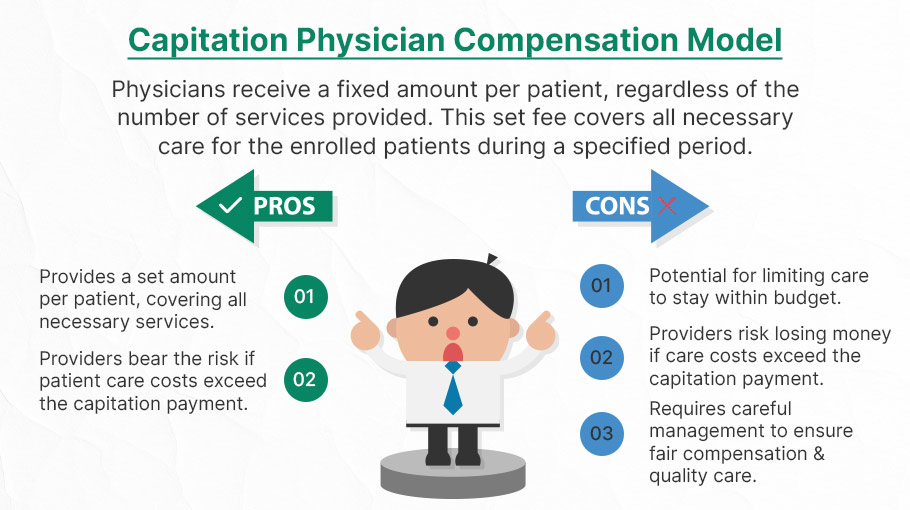
Capitation is a type of healthcare payment system in which a physician or hospital is paid a fixed amount of money per patient for a prescribed period by an insurer or physician association. The cost is based on the expected healthcare utilization costs for a group of patients for that year.
With capitation, the physician—otherwise known as the primary care physician— is paid a set amount for each enrolled patient whether a patient seeks care or not. The PCP is usually contracted with an HMO whose role it is to recruit patients.
According to Richard Eskow, CEO of Health Knowledge Systems of Los Angeles, capitated medical reimbursement has been used in one form or another, in every attempt at healthcare reform since the Norman Conquest. Some even say an earlier variant existed in ancient China [personal communication].
Initially, when Henry I assumed the throne of the newly combined kingdoms of England and Normandy, he initiated a sweeping set of healthcare reforms. Historical documents, though muddled, indicate that soon thereafter at least one “physician,” John of Essex, received a flat payment honorarium of one penny per day for his efforts. Historian Edward J. Kealey opined that sum was roughly equal to that paid to a foot-soldier or a blind person. Clearer historical evidence suggests that American doctors in the mid-19th century were receiving capitation-like payments. No less an authoritative figure than Mark Twain, in fact, is on record as saying that during his boyhood in Hannibal, MO his parents paid the local doctor $25/year for taking care of the entire family regardless of their state of health.
Later, Sidney Garfield MD [1905-1984] is noted as one of the great under-appreciated geniuses of 20th century American medicine stood in the shadow cast by his more celebrated partner, Henry J. Kaiser. Garfield was not the first physician to embrace the notion of prepayment capitation, nor was he the first to understand that physicians working together in multi-specialty groups could, through collaboration and continuity of care, outperform their solo practice colleagues in almost every measure of quality and efficiency. The Mayo brothers, of course, had prior claim to that distinction. What Garfield did, was marry prepayment to group practice, providing aligned financial incentives across every physician and specialty in his medical group, as well as a culture of group accountability for the care of every member of the affiliated health plan. He called it “the new economics of medicine,” and at its heart was a fundamentally new paradigm of care that emphasized – prevention before treatment – and health before sickness. Under his model: the fewer the sick – the greater the remuneration. And: the less serious the illness, the better off the patient and the doctors.
Such ideas were heresy to the reigning fee-for-service, solo practice, ideologues of the mainstream medical establishment of the 1940s and ‘50s, of course. Throughout the period, Garfield and his group physicians were routinely castigated by leaders of the AMA and county medical associations as socialistic and unethical. The local medical associations in Garfield’s expanding service areas – the San Francisco Bay Area, Los Angeles, and Portland, Oregon – blocked group practice physicians from association membership, effectively shutting them out of local hospitals, denying them patient referrals or specialty society accreditation. Twice in the 1940s, formal medical association charges were brought against Garfield personally, at one time temporarily succeeding in suspending his license to practice medicine.
Of course, capitation payments made a comeback in the first cost-cutting managed care era of the 1980-90s because fee-for-service medicine created perverse incentives for physicians by paying more for treating illnesses and injuries than it does for preventing them — or even for diagnosing them early and reducing the need for intensive treatment later. Nevertheless, the modern managed care industry’s experience with capitation wasn’t initially a good one. The 1980-90s saw a number of HMOs attempt to put independent physicians, especially primary care doctors, into a capitation reimbursement model. The result was often negative for patients, who found that their doctors were far less willing to see them — and saw them for briefer visits — when they were receiving no additional income for their effort. Attempts were also made to aggregate various types of health providers — including hospitals and physicians in multiple specialties — into “capitation groups” that were collectively responsible for delivering care to a defined patient group. These included healthcare facilities and medical providers of all types: physicians, osteopaths, podiatrists, dentists, optometrists, pharmacies, physical therapists, hospitals and skilled nursing homes, etc.
However, the healthcare industry isn’t collective by nature, and these efforts tended to be too complicated to succeed. One lesson that these experiments taught is that provider behavior is difficult to change unless the relationship between that behavior and its consequences is fairly direct and easy to understand.
Today, the concept of prepayment and medical capitation is to uncouple compensation from the actual number of patients seen, or treatments and interventions performed. This is akin to a fixed price restaurant menu, as opposed to an àla carte eatery.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
BREAKING NEWS
Law enforcement officials in Utah released a video of the suspected shooter in the assassination of Turning Point USA co-founder and CEO Charlie Kirk, saying that the person wore Converse tennis shoes and left a hand print and a shoe print at the scene.
The suspect in Charlie Kirk’s assassination has been identified as Tyler Robinson, a 22-year-old Utah resident. Law enforcement sources told the Daily Mail that Robinson was taken into custody as the alleged assassin who killed Kirk at a rally at Utah Valley University on Wednesday.
Before today, forensic podiatry has even made it into the public zeitgeist with the hit TV show “Bones” which premiered on September 13, 2005, and concluded on March 28, 2017, airing for 246 episodes over 12 seasons. The show was based on forensic anthropology and forensic archaeology, with each episode focusing on the mystery behind human body remains brought in for examination and identification.
In one show, eight pairs of dismembered feet washed ashore after a flood on the U.S.-Canada border, but things didn’t add up when only seven pairs of feet were identified as research corpses from a nearby university body farm.
When the fictional Canadian forensic podiatrist Dr. Douglas Filmore took the remains back to Canada, he had to form a jurisdictional alliance with the United States to match the pairs of feet and identify the victims. A rare and expensive pair of sneakers led the team to the victim’s murderer.
In 2016, an actual forensic podiatry club was started at the Barry University School of Podiatric Medicine. And, a formal class covering aspects of forensic podiatry is held at the New York College of Podiatric Medicine. Students exit the class with an in depth knowledge of forensic podiatry and other legal knowledge applicable to current cases.
More expertly, real-life colleague Michael Steven Nirenberg DPMactually testified in the murder trial of defendants Kailie Brackett and Donnell Dana with the state calling three witnesses to testify, including the podiatrist who claimed Brackett’s footprints match the ones found in blood at the apartment of the victim, Kimberly Neptune. The forensic podiatrist focused on the footprints discovered at Neptune’s apartment, using prints and images of the defendant’s feet taken by law enforcement. After study, he claimed the prints at the scene bore a resemblance to Kailie Brackett’s in the width of the foot. The defense questioned the field of forensic podiatry and pressed Dr. Nirenberg on whether the measurements would be altered depending on how thick the sock covering the foot was woven.
Dr. Nirenberg was also interviewed on National Public Radio’s Morning Edition on April 14th 2023 about the gait of the bombing suspect associated with the capital riot on Wednesday January 6th, 2021. Dr. Nirenberg is president of the American Society of Forensic Podiatry and co-editor of the textbook: “Forensic Gait Analysis: Principles and Practice”. The bombing suspect had placed bombs at the DNC and RNC headquarters in Washington, DC on the night before. NPR asked Dr. Nirenberg to comment on the features of the person’s gait.
Additionally, Nirenberg was interviewed by Nancy Grace on her TV show Crime Stories. Grace interviewed Nirenberg about his forensic podiatry work in helping to solve the murder of a mother of 3 who was killed in a church. The case remains unsolved. The episode, “Fitness-Mom Missy Bevers Bludgeoned Dead in Creekside Church” aired June 6th, 2024 and is available online at Merit+ TV.
And, Netflix’s 2023 docu-series, “Till Murder Do Us Part”, recounts the killings of Derek and Nancy Haysom by including a series of interviews with a cast of real people. The four-part docu-series revolves around the unpacking of how a wealthy couple was murdered in Virginia in 1985. It also focuses on how the suspects, Elizabeth Haysom, and her boyfriend, Jens Soehring, betrayed each other during the trial. Dr. Sarah Reel DPM was the forensic podiatrist who was involved with Jens’ and Elizabeth’s footprint examination. Dr. Reel pointed out that, statistically, there was no difference “between a bare footprint and a socked footprint.” The doctor suggested that Jens’ reference footprint matched closely with the crime scene footprint.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 10, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITIONS
By Staff Reporters
***
***
Rate Review & the 80/20 Rule
The health care law provides 2 ways to hold insurance companies accountable and help keep your costs down: Rate Review and the 80/20 rule.
Rate Review
Rate Review helps protect you from unreasonable rate increases. Insurance companies must now publicly explain any rate increase of 15% or more before raising your premium. This does not apply to grandfathered plans.
The 80/20 Rule generally requires insurance companies to spend at least 80% of the money they take in from premiums on health care costs and quality improvement activities. The other 20% can go to administrative, overhead, and marketing costs.
The 80/20 rule is sometimes known as Medical Loss Ratio, or MLR. If an insurance company uses 80 cents out of every premium dollar to pay for your medical claims and activities that improve the quality of care, the company has a Medical Loss Ratio of 80%.
Insurance companies selling to large groups (usually more than 50 employees) must spend at least 85% of premiums on care and quality improvement.
If your insurance company doesn’t meet these requirements, you’ll get a rebate on part of the premium that you paid.
Will I get a rebate check from my insurance company?
If your insurance company doesn’t meet its 80/20 targets for the year, you’ll get back some of the premium that you paid.
You may see the rebate in a number of ways:
A rebate check in the mail
A lump-sum deposit into the same account that was used to pay the premium, if you paid by credit card or debit card
A direct reduction in your future premium
Your employer may also use one of the above rebate methods, or apply the rebate in a way that benefits employees
If you or your employer will get a rebate, your insurance company must notify you by August 1.
If you have an individual insurance policy, you’ll get the rebate directly from your insurance company.
For small group and large group plans, the rebate is usually paid to the employer. It may use one of the above rebate methods, or apply the rebate in a way that benefits employees.
FYI: The 80/20 rebate rules don’t apply when an insurance company has fewer than 1000 enrollees in a particular state or market.
For Rate Review: These requirements don’t apply to grandfathered plans. Check your plan’s materials or ask your employer or your benefits administrator to find out if your health plan is grandfathered.
For the 80/20 Rule: These rights apply to all individual, small group, and large group health plans, whether your plan is grandfathered or not.
Classic: The portion of medical expenses a patient is responsible for paying.
Modern: Refers to the maximum you will pay during your policy period, which is typically a year, before your plan starts to pay 100% of your allowed amount. The costs of your deductible, co-pay, and co-insurance are included here, but not your premium.
Classic: “Out-of-network” health care providers do not have an agreement with your insurance company to provide care. While insurance companies may have some out-of-network benefits, medical care from an out-of-network provider will usually cost more out-of-pocket than an in-network provider.
Modern: The amount that a health care insurance plan will contribute toward out-of-network services will vary by your insurance company and is often based on a “reasonable and customary” amount that the service should cost
Example: If you go to an out-of-network dentist and are billed $300 for the service, your insurance company may contribute $200 toward paying this cost because $200 is the amount it has decided is “reasonable and customary” for this service. When out-of-network, any remaining cost above this amount ($100 in this case) may have to be fully covered by the person receiving care. When out-of-network, the usual coinsurance rates that apply in-network may not apply out-of-network. Additionally, out-of-network service costs may not count toward an annual deductible.
According to Medical Economics, there were 10 clinic and physician practices filing bankruptcy in 2024, making it the highest level of the last six years, according to a new analysis of cases with liabilities of at least $10 million.
Meanwhile, the Steward Health Care System bankruptcy, which was based in Massachusetts but making headlines across the nation, has become “the largest hospital sector bankruptcy by far in the last 30 years,” according to a new analysis by Gibbins Advisors, based in Nashville, Tennessee.
Health care bankruptcy filings totaled 57 last year, down from 79 in 2023, said “Healthcare Restructuring: Trends and Outlook.” The report analyzed Chapter 11 health care bankruptcy cases with liabilities of at least $10 million, since 2019.
Last year’s total was down 28% from 2023’s peak, but greater than the 2019 to 2022 average of 42 filings a year, the report said.
Bankruptcy, often considered a last financial resort, is a legal process that can help alleviate outstanding debts for individuals and businesses. Reasons to file for bankruptcy can include divorce, job loss, exorbitant medical bills or credit card debt.
There are several types of bankruptcy — six, as a matter of fact. The two most common types of bankruptcy for individuals are Chapter 7 and Chapter 13.
But there are four other types as well: Chapter 9, Chapter 11, Chapter 12 and Chapter 15. And, the type of bankruptcy filed depends on the situation.
Regardless of which type, the process is typically the same: You’ll usually retain an attorney and make your case before a judge, who will then erase some debts or set up a repayment plan.
Also note that an eligibility requirement — for all bankruptcy chapters — is that you must undergo credit counseling within the 180 days before filing.
Posted on September 7, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
A recent study of hospital physician acquisition and employment found that such acquisitions decrease competition and raise prices. A National Bureau of Economic Research (NBER) working paper, released in July 2025, “empirically analyze[d] the effects of mergers between complementary firms on competition and pricing,” and found hospital prices increased by an average of 3.3%, while physician prices increased by an average of 15.1%.
This Health Capital Topics article reviews the study’s findings and implications for the healthcare industry. (Read more…)
Posted on September 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
U.S. Department for Health & Human Services & Centers for Medicare & Medicaid Services
By Health Capital Consultants, LLC
***
***
On August 21, 2025, the U.S. Department for Health & Human Services (HHS) and the Centers for Medicare & Medicaid Services (CMS) announced the formation of a new Healthcare Advisory Committee.
The Committee is expected to be comprised of a group of experts who will make strategic recommendations to HHS Secretary Robert F. Kennedy Jr. and CMS Administrator Dr. Mehmet Oz.
This Health Capital Topics article discusses this announcement and potential implications on the healthcare industry. (Read more…)
Posted on September 3, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Medicare Inpatient Prospective Payment System
***
***
By Health Capital Consultants, LLC
On July 31, 2025, the Centers for Medicare & Medicaid Services (CMS) released its finalized payment and policy updates for the Medicare Inpatient Prospective Payment System (IPPS) and the Long-Term Care Hospital (LTCH) Prospective Payment System (PPS) for fiscal year (FY) 2026.
The final rule authorized Medicare inpatient reimbursement increases for 2026 and moved forward with improvements to quality measurement, and provided more information on a new value-based payment model.
This Health Capital Topics article will discuss the IPPS final rule and stakeholder reactions. (Read more…)
Posted on August 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL PROVIDER PAYMENTS LOWERED
***
***
Statistic: $2.8+ billion dollars
That’s how much Blue Cross and Blue Shield plans agreed to pay to settle litigation over claims they conspired to lower payments to providers. (Healthcare Dive)
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
It is normal for physician litigants to develop a case of “buyer’s remorse” after any mediation or divorce settlement. They may feel disappointed after entering into a settlement agreement or feel that they received a bad deal.
Mediation: Some advantages of divorce mediation over divorce litigation include:
◊ Mediation is generally faster and less costly.
◊ Mediation is voluntary, private and confidential.
◊ Mediation facilitates creative and realistic solutions.
◊ Mediation allows parties to control their agreements.
◊ Mediation eliminates a win-lose atmosphere and result.
◊ Mediation provides a forum for addressing future disputes.
◊ Mediation fosters communication and helps mend relationships.
***
***
Settlement
And so, in a vast majority of cases, mediation and settlement is probably a good deal. In fact, it is probably a great deal because you are receiving something without having to risk losing. Remember, trial can be a crap-shoot, and nothing is worse than losing it all at the time of trial.
Bench trial verdict by a trial judge.
Jury trial verdict by your “peers.”
Instead, you entered into a settlement agreement and now your divorce case is over.
But beware since trying to get out of a settlement agreement reached at mediation or settlement is virtually impossible.
Why? Well, there is a strong interest by the court to enforce mediation and settlement agreements. The court wants your divorce case to be over and off its docket. There are a few very narrow exceptions; for example, if one party was truly coerced because someone held a gun to their head. But that rarely happens, and it certainly doesn’t happen to most doctors or dentists.
Of course, you can fight against your mediation or settlement agreement if you like, but you won’t get too far. There’s an old adage in the law that a bad settlement is better than a great trial. That’s because no one knows how a judge or jury will rule come time of trial.
***
***
This buyers remorse phenomenon also isn’t uncommon among people who receive sudden wealth, whether through divorce settlements, inheritances, lottery winnings, or other windfalls.
Assessment
Financial advisors often see clients struggle with “sudden wealth syndrome”—the inability to properly manage a large sum of money they’re not accustomed to having.
Common mistakes include:
Lifestyle inflation without sustainable income to support it.
Poor investment decisions or lack of investment planning.
Emotional spending following traumatic life events like divorce.
Failure to set aside money for taxes on the settlement.
Not creating a long-term financial plan for the money.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
A Supply Chain Management Strategy
By Staff Reporters
***
***
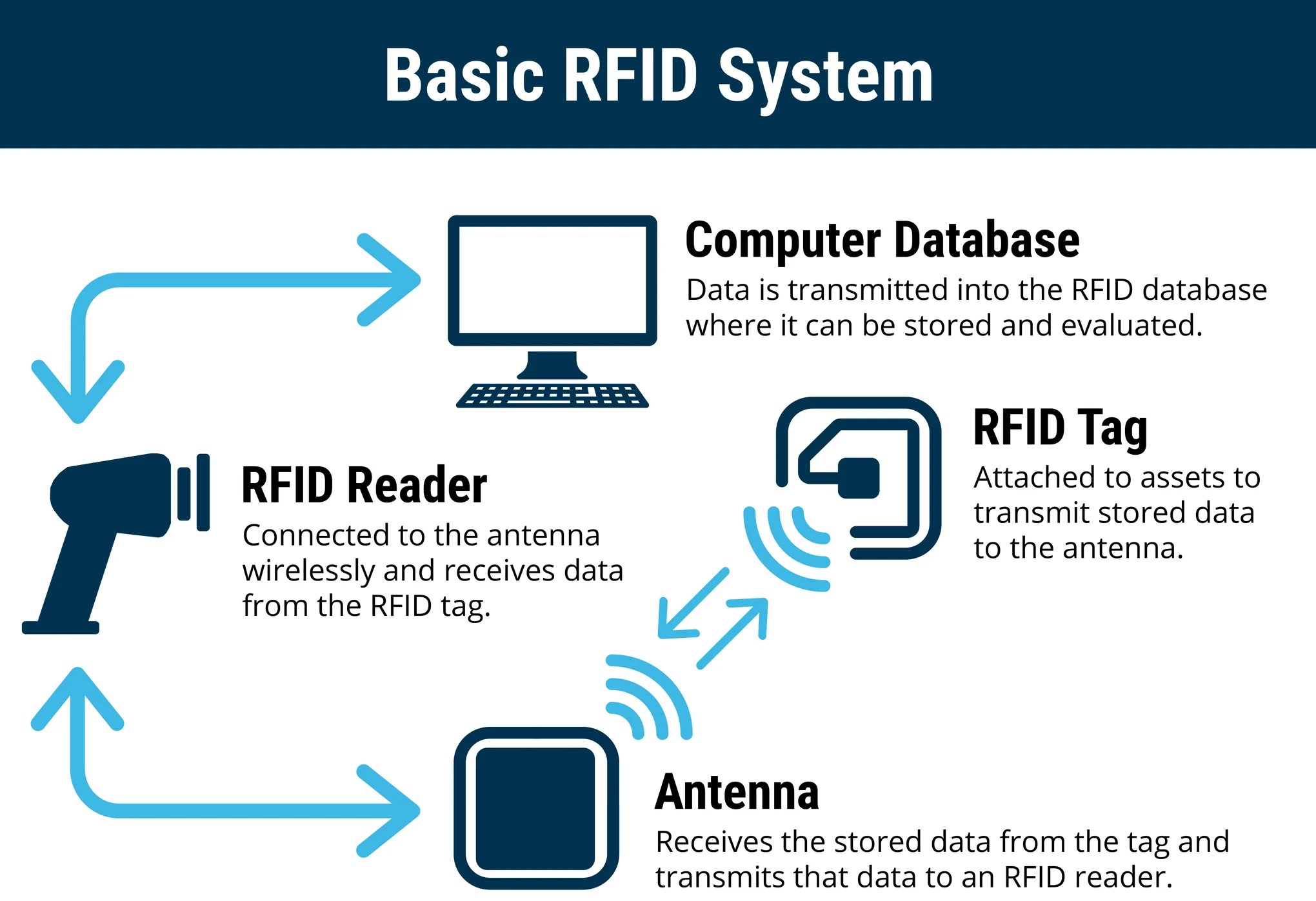
RADIO FREQUENCY IDENTIFICATION
RFID refers to a device attached to an object that transmits data to an RFID receiver. A device can be a large piece of hospital hardware the size of a small book like those attached to ocean containers, or a very small device inserted into a label on a package. RFID has advantages over bar codes such as the ability to hold more data, and to change the stored data as processing occurs. Moreover, it does not require line-of-sight to transfer data, and is very effective in harsh environments where bar-code labels will not work. RFID is not without its own problems, however, as RF signals can be compromised by materials such as metals and liquids.
Although RFID technology is receiving much current attention, it still tends to be cost-prohibitive for some hospital inventory tracking applications. As chip prices go down, there will be continued growth in the application of RFID, but, as in the case of 2D bar codes, many hospital warehouse applications simply do not require this added functionality. The low-cost 1D bar code may continue to be the technology of choice for many hospital inventory tracking applications in the short term.
Smart labels are labels with integrated RFID chips. The idea is to produce labels (probably with bar codes) as well as programming the RFID chips embedded in the label. This would provide all current functionality (human- and machine-readable text and bar codes) as well as adding RFID functionality.
Slap-and-ship describes an approach to complying with vendor requirements for physical identification of shipped goods. More recently, slap-and-ship has been used to describe complying With RFID requirements (such as those from large health care systems); however, it is also applicable to any compliance labeling requirement (such as compliance bar-code labels). Slap-and-ship implies meeting the customer’s requirement by applying the bar-code labels or RFID tags, but not utilizing the technology internally.
Finally, anti-skimming bills were first approved by California and Washington State relative to RFID privacy and are focused on making it illegal for criminals or businesses (or criminal businesses) to read and use personal information from RFID-enabled items such as driver’s licenses and credit cards without the owner’s consent.
An important component of hospital credit analysis is essentiality. Hospitals are unusual businesses that many times possess some form of essentiality to their communities. Health care is important to the economic vitality of every community. Many hospitals have served their communities for many years; it is not uncommon to find hospitals that have been continuously operating for more than 100 years in the same community.
Most hospitals are not-for-profit. In not-for-profit hospitals, no private party actually “owns” the hospital; control is vested in various boards, but no one explicitly owns a not-for-profit hospital. In a broad sense, communities own not-for-profit hospitals. They are considered “charities” with a “charitable purpose.” Though a not-for-profit hospital may not have owners, it has many “stakehold-ers,” parties that have vested interests in the continuing success of the hospital.
Many hospitals have broad and vast webs of stakeholders. Stakeholders are why hospitals rarely close or are shut down. Too many stakeholders have interests in the continuing successful operation of hospitals.
Another dimension of the essentiality analysis is service analysis. How significant are the hospital’s services? If the hospital shuts down, what population segments would suffer? How significant is the population that would suffer? How much would they suffer?
And so, hospital stakeholder relationships need to be considered in the analysis of essentiality. How strong are these relations? How many are there? How important is the continuing success of this hospital to these stakeholders?
Analysis of hospital’s stakeholders and services should provide a credible view of the degree of essentiality associated with a hospital. Higher degrees of essentiality suggest higher likelihoods that hospitals, one way or another, will meet their commitments, particularly their payment commitments.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
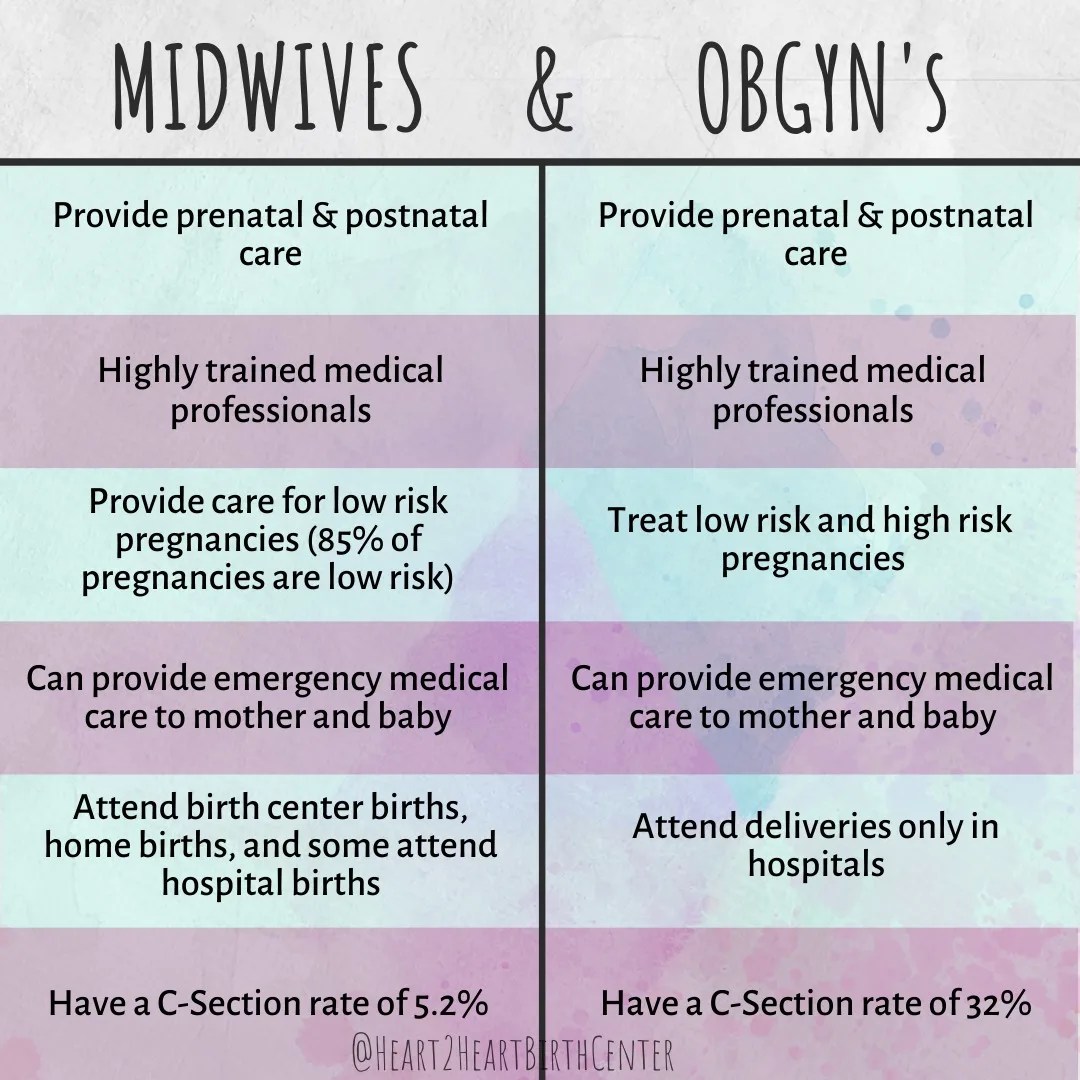
An obstetrician-gynecologist, or OB-GYN, has expertise in female reproductive health, pregnancy, and childbirth. Some OB-GYNs offer a wide range of general health services similar to a primary care doctor. Others focus on the medical care of the female reproductive system. OB-GYNs also provide routine medical services and preventive screenings. This type of doctor has studied obstetrics and gynecology. The term “OB-GYN” can refer to the doctor, an obstetrician-gynecologist, or to the sciences that the doctor specializes in, which are obstetrics and gynecology.
Obstetrician
Obstetrics is the branch of medicine related to medical and surgical care before, during, and after a woman gives birth. Obstetrics focuses on caring for and maintaining a woman’s overall health during maternity. This includes:
pregnancy
labor
childbirth
the postpartum period
OB-GYNs can conduct office visits, perform surgery, and assist with labor and delivery. Some OB-GYNs provide services through a solo or private practice. Others do so as part of a larger medical group or hospital.
***
***
Gynecologist
Gynecology is the branch of medicine that focuses on women’s bodies and their reproductive health. It includes the diagnosis, treatment, and care of women’s reproductive system. This includes the:
vagina
uterus
ovaries
fallopian tubes
This branch of medicine also includes screening for and treating issues associated with women’s breasts. Gynecology is the overarching field of women’s health from puberty through adulthood. It represents most of the reproductive care received during a lifetime. If pregnant, one goes to an obstetrician.
Mid-Wife
Midwives are registered nurses who specialize in midwifery. As such, they’re trained healthcare providers who can oversee low-risk pregnancies, labor, and birth. They can provide other obstetric and gynecological services too. They can do exams and help with basic gynecological concerns like sexually transmitted infections, urinary tract infections, or yeast infections. They help support during labor and in the postpartum period with breastfeeding and birth control.
Doula
Doulas aren’t clinical professionals and can’t give medical advice. They can’t prescribe medicines, and they can’t deliver a baby. But they can offer physical and emotional support during labor—and sometimes during and after pregnancy. Doulas can help with breathing techniques, positional changes, and relaxation strategies during labor. Studies show doulas are associated with fewer C-sections and more vaginal births.
Doctors and dentists earn money by treating patients. CPAs and Attorneys have clients, and retail stores buy items low and sell them at higher prices. This is called a business model.
More formally, a business model identifies the products or services the business plans to sell, the target market, and any anticipated expenses, in order to outline how to generate a profit. Business models are important for both new and established businesses. They help companies attract investment, recruit talent, and motivate management and staff.
Businesses should regularly update their business model, or they’ll fail to anticipate trends and challenges ahead. Business models also help investors to evaluate companies that interest them and employees to understand the future of a company they may aspire to join.
***
The Business Model of Pharmacy Benefits Managers
In the United States, health insurance providers often hire a third party to handle price negotiations, insurance claims, and distribution of prescription drugs. Providers that use such pharmacy benefit managers include commercial health plans, self-insured employer plans, Medicare Part D [drug] plans, the Federal Employees Health Benefits Program, and state government employee plans. PBMs are designed to aggregate the collective buying power of en-rollees through their client health plans, enabling plan sponsors and individuals to obtain lower prices for their prescription drugs. PBMs negotiate price discounts from retail pharmacies, rebates from pharmaceutical manufacturers, and mail-service pharmacies which home-deliver prescriptions without consulting face-to-face with a pharmacist.
Pharmacy benefit management companies can make revenue in several ways.
First, they collect administrative and service fees from the original insurance plan.
Then, they can also collect rebates from the manufacturer.
Traditional PBMs do not disclose the negotiated net price of the prescription drugs, allowing them to resell drugs at a public list price (also known as a sticker price), which is higher than the net price they negotiate with the manufacturer. This practice is known as “spread pricing”. The industry argues that savings are trade secrets. Pharmacies and insurance companies are often prohibited by PBMs from discussing costs and reimbursements. This leads to lack of transparency.
***
***
Therefore, states are often unaware of how much money they lose due to spread pricing, and the extent to which drug rebates are passed on to en-rollees of Medicare plans. In response, states like Ohio, West Virginia, and Louisiana have taken action to regulate PBMs within their Medicaid programs.
For instance, they have created new contracts that require all discounts and rebates to be reported to the states. In return, Medicaid pays PBMs a flat administrative fee.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
An ophthalmologist is a physician [MD, DO] who undergoes sub-specialty training in medical and surgical eye care. Following a medical degree, a doctor specializing in ophthalmology must pursue additional postgraduate residency training specific to that field. In the United States, following graduation from medical school, one must complete a four-year residency in ophthalmology to become an ophthalmologist. Following residency, additional specialty training (or fellowship) may be sought in a particular aspect of eye pathology.
Ophthalmologists prescribe medications to treat ailments, such as eye diseases, implement laser therapy, and perform surgery when needed. Ophthalmologists provide both primary and specialty eye care—medical and surgical. Most ophthalmologists participate in academic research on eye diseases at some point in their training and many include research as part of their career. Ophthalmology has always been at the forefront of medical research with a long history of advancement and innovation in eye care.
Optometrist
Optometrists focus on regular vision care and primary health care for the eye. After college, they spend 4 years in a professional program and get a doctor of optometry degree. But they don’t go to medical school. Some optometrists get additional clinical training or complete a specialty fellowship after optometry school. They:
Monitor eye conditions related to diseases like diabetes
Manage and treat conditions like dry eye and glaucoma
Provide low-vision aids and vision therapy
There are specialties among optometrists. They include:
Pediatric optometry. These providers work with babies, toddlers, and children, using special techniques to test their vision.
Neuro-optometry. If you have vision problems that result from a brain injury, this is the type of optometrist you might visit.
Low-vision optometry. If you have low vision—that means you can’t see well enough to perform your daily activities and your sight can’t be corrected by glasses or contact lenses, medicine, or surgery—low-vision optometrists offer devices and strategies that can improve your quality of life.
***
***
Optician
An optician is an eye care specialist who helps you choose the right eyeglasses, contact lenses or other vision correction devices. They can’t diagnose or treat conditions that affect your eyes or vision. They’ll work with you to get the right corrective lenses after your optometrist or ophthalmologist gives you a prescription.
Ocularist
An ocularist is an eye care specialist who provides care for people needing prosthetic eyes due to injury, infection or congenital disease (present at birth). Losing or damaging an eye can be a traumatic experience, and the need for a prosthetic can be overwhelming. Ocularists offer long-term care. They collaborate with your healthcare team to create or restore a more natural facial appearance with the goal of enhancing your health-related quality of life.
Posted on August 10, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
On July 2, 2025, the Department of Justice (DOJ) and Department of Health & Human Services (HHS) announced during the American Health Law Association (AHLA) Annual Meeting that the agencies have reestablished a Working Group to “strengthen” their ongoing collaboration, specifically as relates to the False Claims Act (FCA).
This Health Capital Topics article discusses the Working Group’s priorities and the implications for providers. (Read more…)
Trump says pharma tariffs could be as high as 250%
The president revealed that he plans to formally announce tariffs on the pharmaceutical industry “within the next week or so” in an attempt to force drug manufacturing to the US, he told CNBC several days ago.
In the early 1980s, Daniel Kahneman and Amos Tverskey proved in numerous experiments that the reality of decision making differed greatly from the assumptions held by economists. They published their findings in Prospect Theory: An analysis of decision making under risk, which quickly became one of the most cited papers in all of economics.
To understand the importance of their breakthrough, we first need to take a step back and explain a few things. Up until that point, economists were working under a normative model of decision making. A normative model is a prescriptive approach that concerns itself with how people should make optimal decisions. Basically, if everyone was rational, this is how they should act.
Amanda, an RN client, was just informed by her financial advisor that she needed to re-launch her 403-b retirement plan. Since she was leery about investing, she quietly wondered why she couldn’t DIY. Little does her Financial Advisor know that she doesn’t intend to follow his advice, anyway! So, what went wrong?
The answer may be that her advisor didn’t deploy a behavioral economics framework to support her decision-making. One such framework is the “prospect theory” model that boils client decision-making into a “three step heuristic.”
According to colleague Eugene Schmuckler PhD MBA MEd CTS, Prospect theory makes the unspoken biases that we all have more explicit. By identifying all the background assumptions and preferences that clients [patients] bring to the office, decision-making can be crafted so that everyone [family, doctor and patient] or [FA, client and spouse] is on the same page.
1. Simplify choices by focusing on the key differences between investment [treatment] options such as stock, bonds, cash, and index funds.
2. Understanding that clients [patients] prefer greater certainty when it comes to pursuing financial [health] gains and are willing to accept uncertainty when trying to avoid a loss [illness].
3. Cognitive processes lead clients and patients to overestimate the value of their choices thanks to survivor bias, cognitive dissonance, appeals to authority and hindsight biases.
CITE: Jaan E. Sidorov MD [Harrisburg, PA]
Assessment
Much like in healthcare today, the current mass-customized approaches to the financial services industry fall short of recognizing more personalized advisory approaches like prospect theory and assisted client-centered investment decision-making.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
An acute care inpatient hospital is a health care organization or “anchor hospital” in which a patient is treated for an acute (immediate and severe) episode of illness or the subsequent treatment of injuries related to an accident or trauma, or during recovery from surgery. Specialized personnel using complex and sophisticated technical equipment and materials usually render acute professional care in a hospital setting. Unlike chronic care, acute care is often necessary for only a short time. Measures of acute health care utilization are represented by three separate rates:
Rate of admissions per 1000 patients.
Average length of stay per admission.
Total days of care per 1000 patients.
***
***
Psychiatric Hospital
A psychiatric hospital (behavioral health, mental hospital, or asylum) specializes in the treatment of patients with mental illness or drug-related illness or dependencies. Psychiatric wards differ only in that they are a unit of a larger hospital.
Specialty Hospital
A specialty hospital is a type of health care organization that has a limited focus to provide treatment for only certain illnesses such as cardiac care, orthopedic or plastic surgery, elder care, radiology / oncology services, neurological care, or pain management cases. These organizations are often owned by doctors who refer patients to them. In recent years, single-specialty hospitals have emerged in various locations in the United States. Instead of offering a full range of inpatient services, these hospitals focus on providing services relating to a single medical specialty or cluster of specialties.
Long-Term Care Hospital
A long-term care hospital is an entity that provides assistance and patient care for the activities of daily living (ADLs), including reminders and standby help for those with physical, mental, or emotional problems. This includes physical disability or other medical problems for 3 months or more (90 days). The criteria of five ADLs may also be used to determine the need for help with the following: meal preparation, shopping, light housework, money management, and telephoning. Other important considerations include taking medications, doing laundry, and getting around outside.
Rural Hospital
The parameters of a rural hospital are determined based on distance. A rural hospital is defined as a hospital serving a geographic area 10 or more miles from the nexus of a population center of 30,000 or more.
More specifically, a rural hospital means an entity characterized by one of the following:
Type A rural hospital—small and remote, has fewer than 50 beds, and is more than 30 miles from the nearest hospital
Type B rural hospital—small and rural, has fewer than 50 beds, and is 30 miles or less from the nearest hospital
Type C rural hospital—considered rural and has 50 or more beds
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on July 31, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
***
On July 14, 2025, the Centers for Medicare & Medicaid Services (CMS) released its proposed Medicare Physician Fee Schedule (MPFS) for calendar year (CY) 2026.
In addition to the agency’s suggested increase to physician payments, the proposed rule also announces a new payment model and more tele-health flexibilities.
According to CMS, the “proposed rule is one of several proposed rules that reflect a broader Administration-wide strategy to create a health care system that results in better quality, efficiency, empowerment, and innovation for all Medicare beneficiaries.” (Read more…)
Posted on July 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
THE FOOT & ANKLE DOCTORS
By A.I.
***
***
Podiatry offers a promising career with a balanced mix of specialization and income. By understanding the factors that influence salaries—such as location, experience, and practice type—a doctor can strategically enhance his/er earning potential. Staying informed about healthcare policies and market trends is crucial for maximizing income.
With an aging population and advancements in technology, the demand for podiatrists is expected to grow, making it a rewarding field both professionally and financially. Investing in specialized training and adapting to policy changes will help doctors remain competitive and successful in the evolving healthcare landscape.
A podiatrist is a healthcare professional specialized in diagnosing and treating conditions related to the feet and ankles. Their responsibilities include performing surgeries, prescribing orthotics, and providing preventive care.
What education is required to become a podiatrist?
To become a podiatrist, one must complete a Doctor of Podiatric Medicine (DPM) degree, which typically takes four years after earning a bachelor’s degree. Following this, a residency program lasting 2-3 years is required for practical training.
What factors influence the salary of a podiatrist?
Geographic location, level of experience, specialization, and type of practice significantly affect a podiatrist’s salary. Areas with a higher cost of living or demand for services usually offer higher salaries.
How does the salary of a podiatrist compare to other medical professions?
Podiatrists generally earn more than general practitioners but less than specialty surgeons. This disparity is due to differences in training length, specialization, and practice complexity among these professions.
Can the salary of a podiatrist increase over time?
Yes, a podiatrist’s salary can increase with additional experience, further specialization, and strategic practice location choices. Continuing education and staying updated on healthcare policies can also enhance earning potential.
What impact do healthcare policies have on podiatrist salaries?
Healthcare policies, including changes in insurance reimbursement rates and government health initiatives, can affect podiatrist salaries. Adapting to these policy shifts is crucial for maximizing earning potential in the field.
What are the future trends in podiatry salaries?
Future trends suggest potential salary growth due to increasing demand from an aging population, technological advancements, and geographic disparities in healthcare access. Keeping informed about these trends can help podiatrists plan their careers strategically.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, hospitals, financial advisory firms, RIAs, or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on July 26, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
On July 15, 2025, the Centers for Medicare & Medicaid Services (CMS) released the proposed rule for the Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical Center (ASC) Payment System for calendar year (CY) 2026.
Among other items, the agency proposes increasing payments to all outpatient providers, eliminating the Inpatient Only (IPO) List, and changing quality reporting programs.
This Health Capital Topics article reviews the proposed updates and changes to outpatient reimbursement. (Read more…)
Stocks: Investors were pleased to hear about the trade deal with Japan yesterday and reports of an agreement with the EU coming soon kept the stock rally alive through market close. The S&P 500 notched its 12th new closing record this year, and the NASDAQ ended the day above 21,000 for the first time.
Bonds: Treasury yields rose a bit after an auction of 20-year notes was met with strong demand, indicating investor appetite for longer-term US debt.
Commodities: Oil inched higher while gold edged lower as investors hedge their bets in anticipation of more trade deals before the August 1st deadline.
Posted on July 24, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Insurers selling plans on ACA exchanges are expected to hike premiums next year as subsidies on them are set to expire, with the average person expected to be paying 75% more, according to an analysis from the nonpartisan research group KFF.
Posted on July 15, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Drug and medical device companies paid at least $13.2 billion to medical professionals in 2024, according to CMS data released June 30th. There’s been steady growth in these payments over the last few years, which include everything from research payments to free meals to promotional or conference fees. Drug and medical device companies paid out $13.1 billion in 2023, $13.1 in 2022, and $12.6 in 2021. If you’re a medical provider, you’ve probably gotten one of those perks from a drug or medical device company and thought it wouldn’t affect your decision-making.
But research suggests physicians are more likely to prescribe drugs from companies that pay them, with some studies specifically associating this with drugs that are costlier to patients. “Really well-trained people who affirm an oath to do no harm can be influenced, and are,” Neil Jay Sehgal, associate professor of health systems and population health at the University of Washington School of Public Health, told Healthcare Brew.
Bitcoin is booming, and crypto stocks climbed along with it. MicroStrategy rose 3.86%, RobinhoodMarkets added 1.67%. and Coinbase gained 1.80%.
Boeing rose 1.64% on preliminary reports that investigators have found no evidence of malfunction in the plane that crashed in India last month. Engine-maker GEAerospace also gained 2.71%.
Warner Bros Discovery climbed 2.39% thanks to a strong opening weekend for the new Superman movie.
Autodesk popped 5.05% on the news that it is not pursuing an acquisition of rival software maker PTC. PTC fell 1.25%.
Kenvue, the company behind Band Aids and Listerine, gained 2.18% after kicking its CEO to the curb.
PayPal climbed 3.55% despite the news that JPMorgan will start charging the fintech fees for access to customer data.
Stocks Down
Starbucks sank 1.60% on news that employees will have to return to the office four days a week. Shareholders were also unimpressed with the coffee giant’s new secret menu.
Synopsys stumbled 1.74% after getting regulatory approval from Chinese authorities to acquire software designer Ansys for $35 billion. Ansys rose 3.03% on the news.
Waters plunged 13.81% on the news that it will merge with Becton Dickinson’s bioscience and diagnostic solutions business in a $17.5 billion deal.
RivianAutomotive lost 2.15% thanks to a downgrade from Guggenheim analysts, who forecast soft sales for the automaker’s latest models.
The terms “psychologist” and “psychiatrist” are often used interchangeably to describe anyone who provides therapy services, but the two professions and the services they provide differ in terms of content and scope. A major difference between the two types of experts is that psychiatrists can prescribe medication [Rx].
As physicians [MD/DO] psychiatrists are trained to recognize the ways biological processes affect mental functioning.
Psychologists are oriented to how thoughts, feelings, and social factors influence mental functioning.
PSYCHIATRIST
Psychiatrists are medical or osteopathic doctors who are able to prescribe psychotropic medications, which they do in conjunction with providing psychotherapy though medical and pharmacological interventions are often their focus.
PSYCHOLOGIST
Though many psychologists hold doctorate degrees, they are not medical doctors, and most cannot prescribe medications. Rather, they solely provide psycho-therapy, which may involve cognitive and behavioral interventions, psycho-dynamic or psycho-analytic approaches.
NOTEPROTECTED TITLE: The title of “psychologist” can only be used by an individual who has completed the required education, training, and state license requirements. Informal titles, such as “counselor” or “therapist,” are often used as well. Other mental health care professionals, such as licensed social workers, can claim those titles, but not the title of “psychologist.”
Posted on July 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants LLC
***
***
On June 25th, 2025, the Centers for Medicare & Medicaid Services (CMS) released its forecast on U.S. healthcare spending through 2033. The analysis, published in Health Affairs, estimated healthcare spending growth in 2024 and projected the growth into 2033. CMS found that overall healthcare spending growth has decreased slightly but is still elevated compared to pre-pandemic levels, and is expected to continue to moderately grow.
This Health Capital Topics article examines the factors underlying the forecasts. (Read more…)
Posted on July 6, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants LLC
***
***
On June 9th, 2025, Oregon’s governor signed into law the country’s strictest corporate practice of medicine (CPOM) prohibition. Senate Bill (SB) 951 will severely curtail the involvement of private equity firms and other corporations in the state’s medical practices.
This Health Capital Topics reviews the bill and discusses the implications on the healthcare industry. (Read more…)
One Big Beautiful Bill Act (OBBBA; OBBB; BBB), or the Big Beautiful Bill, is a budget reconciliation bill in the 119th US Congress.
Hospitals are not happy with the health care provisions of the bill, which would reduce the support they receive from states to care for Medicaid enrollees and leave them with more uncompensated care costs for treating uninsured patients.
“The real-life consequences of these nearly $1 trillion in Medicaid cuts – the largest ever proposed by Congress – will result in irreparable harm to our health care system, reducing access to care for all Americans and severely undermining the ability of hospitals and health systems to care for our most vulnerable patients,” said Rick Pollack, CEO of the American Hospital Association.
The association said it is “deeply disappointed” with the bill, even though it contains a $50 billion fund to help rural hospitals contend with the Medicaid cuts, which hospitals say is not nearly enough to make up for the shortfall.
Posted on June 30, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants; LLC
***
***
On May 22, 2025, the U.S. House of Representatives moved President Trump’s budget proposal forward, sending to the Senate a budget reconciliation bill (with a one-vote margin) – the One Big Beautiful Bill Act of 2025 – that renews expiring tax cuts and enacts new ones at a cost of almost $4 trillion. These costs would largely be paid for by cuts to other programs, including to federal healthcare programs, which cuts will have significant ramifications for the healthcare industry.
This Health Capital Topics article reviews the current status of the budget bill and healthcare industry implications. (Read more…)
Assets under advisement refer to assets on which your firm provides advice or consultation but for which your firm does either does not have discretionary authority or does not arrange or effectuate the transaction. Such services would include financial planning or other consulting services where the assets are used for the informational purpose of gaining a full perspective of the client’s financial situation, but you are not actually placing the trade.
Assets under advisement could also be those which you monitor for a client on a non-discretionary basis, where you may make recommendations but where the client is the party responsible for arranging or effecting the purchase or sale. A common example of this AUM scenario is when an advisor reviews a participant’s 401(k) allocations. If the adviser does not have the authority or ability to effect changes in the portfolio, these assets are likely considered assets under advisement rather than regulatory assets under management.
Assets under advisement are permitted to be disclosed on Form ADV Part 2A as a separate asset figure from the assets under management. There is no requirement to disclose the assets under advisement figure, but some advisors opt to include the figure to give prospective clients a more complete picture of the firm’s responsibilities. If you choose to report your assets under advisement, be sure to make a clear distinction between this figure and your regulatory assets under management.
***
D. E. Marcinko & Associates Core Operating Values
9. We act with honesty, integrity and are always straightforward. 8. We strive to be innovative, creative, iconoclastic, and flexible. 7. We admit and learn from mistakes and don’t repeat them. 6. We work hard always as competitors are trying to catch up. 5. We treat others with dignity and respect. 4. We are the onus of consulting advice for the fiduciary well being of others. 3. We fight complacency as former success is in the past. 2. The best management styles are timeless, not timely. 1. Our clients are colleagues and always come first.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com