BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
The idea of a physician who is also an accountant might sound unusual at first, almost like two worlds that rarely intersect. One is rooted in diagnosing illnesses, understanding human physiology, and providing compassionate care. The other revolves around financial statements, regulatory compliance, and strategic fiscal planning. Yet when these two disciplines come together in a single professional, the result is a uniquely capable individual who can navigate both the complexities of modern healthcare and the equally intricate world of financial management. As healthcare systems grow more complicated and financially pressured, the combination of medical expertise and accounting acumen becomes not only valuable but transformative.
Physicians traditionally focus on clinical decision‑making, patient outcomes, and the ethical dimensions of care. Their training emphasizes scientific reasoning, empathy, and the ability to make high‑stakes decisions under uncertainty. Accountants, on the other hand, are trained to think in terms of precision, structure, and long‑term financial sustainability. They understand how organizations allocate resources, manage risk, and maintain compliance with regulatory frameworks. When one person embodies both sets of skills, they gain a rare vantage point: the ability to see how clinical decisions ripple through the financial health of a practice, hospital, or healthcare system.
One of the most significant advantages of this dual expertise is the ability to bridge the communication gap between clinicians and administrators. In many healthcare organizations, physicians and financial officers often struggle to fully understand each other’s priorities. Physicians may feel that financial constraints undermine their ability to provide optimal care, while administrators may worry that clinical decisions are made without regard for cost efficiency or long‑term sustainability. A physician‑accountant can translate between these two perspectives, helping each side understand the other’s reasoning. This can lead to more balanced decision‑making, where patient care remains central but financial realities are acknowledged and managed responsibly.
Another area where this combination shines is in private practice management. Running a medical practice is, at its core, running a business. Physicians who lack financial training often find themselves overwhelmed by budgeting, billing systems, tax obligations, and regulatory compliance. Mistakes in these areas can be costly, both financially and legally. A physician who is also an accountant is far better equipped to manage these responsibilities. They can design efficient billing workflows, interpret financial reports, and make informed decisions about staffing, equipment purchases, and long‑term investments. This not only strengthens the practice but also allows the physician to maintain greater autonomy and stability in an increasingly competitive healthcare landscape.
***
***
Beyond individual practices, physician‑accountants can play influential roles in healthcare policy and leadership. Healthcare spending is a major concern in many countries, and policymakers often struggle to balance cost control with quality of care. Professionals who understand both the clinical and financial dimensions of healthcare are uniquely positioned to contribute to policy development, hospital administration, and health‑system reform. They can evaluate the economic impact of clinical guidelines, assess the cost‑effectiveness of new technologies, and design reimbursement models that incentivize high‑quality care without creating unnecessary financial burdens.
The dual training also enhances ethical decision‑making. Financial pressures in healthcare can sometimes lead to conflicts of interest or difficult trade‑offs. A physician‑accountant is better prepared to navigate these dilemmas because they understand the financial implications without losing sight of the ethical obligations inherent in medical practice. They can advocate for solutions that protect patient welfare while ensuring that resources are used responsibly. This balanced perspective can help organizations avoid short‑sighted decisions that might compromise care or create long‑term financial instability.
Of course, becoming both a physician and an accountant requires an extraordinary level of dedication. Medical training alone demands years of study, residency, and ongoing professional development. Adding accounting education—whether through a degree, certification, or extensive coursework—requires additional time and effort. Yet for those who pursue this path, the rewards can be substantial. They gain a level of professional versatility that few others possess, and they can shape healthcare environments in ways that purely clinical or purely financial professionals cannot.
In a rapidly evolving healthcare landscape, the intersection of medicine and accounting is becoming increasingly relevant. Rising costs, complex insurance systems, and the growing emphasis on value‑based care all demand professionals who can think across traditional disciplinary boundaries. Physicians who are also accountants embody this interdisciplinary approach. They bring clarity to financial decisions, insight to clinical operations, and a holistic understanding of how healthcare systems function. Their unique skill set positions them as leaders who can help shape a more efficient, ethical, and sustainable future for healthcare.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on January 7, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Tariffs on medicines and healthcare products increase costs, disrupt supply chains, and ultimately harm patient access and public health. They raise prices for essential drugs and medical devices, create shortages, and undermine innovation in the healthcare sector.
The Economic Burden of Tariffs
Tariffs are taxes imposed on imported goods. In healthcare, this means pharmaceuticals, medical devices, and raw materials like active pharmaceutical ingredients (APIs) become more expensive. Since the United States imports a significant share of these products from countries such as China, India, and the European Union, tariffs directly raise costs for hospitals, clinics, and patients.
Drug prices rise because manufacturers pass on higher import costs to consumers.
Medical devices such as surgical instruments, diagnostic equipment, and imaging technology become more expensive, straining hospital budgets.
Insurance premiums may increase as healthcare providers face higher operating costs.
This economic burden is not abstract—it translates into higher bills for patients and reduced affordability of care.
Supply Chain Disruptions
Healthcare supply chains are highly globalized. APIs, raw materials, and specialized equipment often come from multiple countries. Tariffs disrupt this delicate balance by:
Creating shortages when suppliers cannot afford to export to tariff-heavy markets.
Delaying shipments as companies seek alternative routes or suppliers.
Reducing resilience by concentrating production in fewer regions, making systems more vulnerable to shocks.
For example, if tariffs make APIs prohibitively expensive, pharmaceutical companies must scramble to find new suppliers, often at higher cost and with longer lead times. This can delay drug availability and compromise patient care.
***
***
Impact on Public Health
The consequences of tariffs extend beyond economics into public health outcomes.
Patients face reduced access to life-saving medicines and devices.
Hospitals may ration supplies, prioritizing urgent cases while delaying elective procedures.
Preventive care suffers, as higher costs discourage investment in vaccines, diagnostic tools, and routine screenings.
In the long run, tariffs can exacerbate health inequities, disproportionately affecting low-income populations who are least able to absorb rising costs.
Innovation and Research Setbacks
Healthcare innovation relies on global collaboration. Tariffs discourage cross-border partnerships by raising costs and creating uncertainty.
Research institutions may struggle to import specialized lab equipment.
Pharmaceutical companies face higher costs for clinical trials and drug development.
Digital health technologies that depend on imported components (like sensors and chips) become more expensive, slowing adoption.
This stifles progress in areas such as cancer treatment, biotechnology, and precision medicine.
Conclusion
Tariffs in healthcare are a blunt economic tool with unintended consequences. While they aim to protect domestic industries, they increase costs, disrupt supply chains, reduce access to care, and hinder innovation. In medicine and healthcare, where lives depend on timely and affordable access to products, tariffs are particularly damaging. Policymakers must weigh these human costs carefully before imposing trade barriers on essential goods.
Posted on January 6, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
Professor Eugene Schmuckler PhD MBA MEd CTS
***
***
Navigating the Challenges of Passive-Aggressive Patients in Healthcare
In the complex landscape of healthcare, effective communication between providers and patients is essential for accurate diagnosis, treatment adherence, and overall patient satisfaction. However, passive-aggressive behavior—characterized by indirect resistance, subtle obstruction, and veiled hostility—can significantly hinder this process. Passive-aggressive patients present unique challenges that require emotional intelligence, patience, and strategic communication skills from healthcare professionals.
Passive-aggressive behavior often stems from underlying feelings of fear, resentment, or a perceived lack of control. Patients may feel overwhelmed by their diagnosis, skeptical of medical advice, or frustrated by systemic issues such as long wait times or insurance complications. Rather than expressing these concerns openly, they may resort to behaviors such as missed appointments, vague complaints, sarcasm, or noncompliance with treatment plans. These actions, though subtle, can disrupt care continuity and erode trust between patient and provider.
One of the most difficult aspects of managing passive-aggressive patients is identifying the behavior early. Unlike overt aggression, passive-aggression is cloaked in ambiguity. A patient might nod in agreement during a consultation but later ignore medical instructions. They may offer compliments laced with sarcasm or express dissatisfaction through third parties rather than directly. These indirect signals can leave providers confused and uncertain about the patient’s true feelings or intentions.
***
***
Addressing passive-aggressive behavior requires a nuanced approach. First, providers must cultivate a nonjudgmental environment where patients feel safe expressing concerns. Active listening, empathy, and validation can encourage more direct communication. For example, acknowledging a patient’s frustration with wait times or side effects can open the door to honest dialogue. Providers should also be mindful of their own reactions, avoiding defensiveness or dismissiveness, which can exacerbate the behavior.
Setting clear boundaries and expectations is another key strategy. Passive-aggressive patients often test limits subtly, so it’s important to reinforce the importance of mutual respect and accountability. Documenting interactions, treatment plans, and patient responses can help track patterns and ensure consistency. In some cases, involving mental health professionals may be beneficial, especially if the behavior is rooted in deeper psychological issues.
Ultimately, the goal is to transform passive-aggressive dynamics into constructive partnerships. This requires time, effort, and a willingness to engage with patients beyond surface-level interactions. When successful, it can lead to improved outcomes, greater patient satisfaction, and a more harmonious clinical environment.
In conclusion, passive-aggressive patients pose a unique challenge in healthcare, but they also offer an opportunity for providers to refine their communication skills and deepen their understanding of patient psychology. By fostering openness, setting boundaries, and responding with empathy, healthcare professionals can navigate these interactions effectively and promote better health outcomes for all.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on November 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Retirement planning has evolved significantly over the past several decades, with employers and employees seeking solutions that balance security, flexibility, and predictability. Among the various retirement plan options available today, cash balance plans stand out as a hybrid design that combines features of both traditional defined benefit pensions and defined contribution plans. Their unique structure makes them an attractive choice for employers aiming to provide meaningful retirement benefits while maintaining financial predictability.
At their core, cash balance plans are a type of defined benefit plan. Unlike traditional pensions, which promise retirees a monthly income based on years of service and final salary, cash balance plans define the benefit in terms of a hypothetical account balance. Each participant’s account grows annually through two components: a “pay credit” and an “interest credit.” The pay credit is typically a percentage of the employee’s salary or a flat dollar amount, while the interest credit is either a fixed rate or tied to an index such as U.S. Treasury yields. Although the account is hypothetical—meaning the funds are not actually segregated for each employee—the structure provides participants with a clear, understandable statement of their retirement benefit.
One of the primary advantages of cash balance plans is their transparency. Employees can easily track the growth of their account balance, much like they would with a 401(k). This clarity helps workers better understand the value of their retirement benefits and fosters a sense of ownership. Additionally, cash balance plans are portable: when employees leave a company, they can roll over the vested balance into an IRA or another qualified plan, ensuring continuity in retirement savings.
***
***
From the employer’s perspective, cash balance plans offer several benefits as well. Traditional pensions often create unpredictable liabilities, as they depend on factors such as longevity and investment performance. Cash balance plans, by contrast, provide more predictable costs because the employer commits to specific pay and interest credits. This predictability makes them easier to manage and budget for, particularly in industries where workforce mobility is high. Moreover, cash balance plans can be designed to reward long-term employees while still appealing to younger workers who value portability.
Despite these advantages, cash balance plans are not without challenges. Because they are defined benefit plans, employers bear the investment risk and must ensure the plan is adequately funded. Regulatory requirements, including nondiscrimination testing and funding rules, add complexity and administrative costs. Additionally, while cash balance plans are generally more equitable across generations of workers, transitions from traditional pensions to cash balance designs have sometimes sparked controversy, particularly among older employees who may perceive a reduction in benefits.
In recent years, cash balance plans have gained popularity among professional firms, such as law practices and medical groups, as well as small businesses seeking tax-efficient retirement solutions. These plans allow owners and highly compensated employees to accumulate larger retirement savings than would be possible under defined contribution limits, while still providing benefits to rank-and-file workers. As such, they serve as a valuable tool for both talent retention and financial planning.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 15, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
For centuries, doctors have occupied one of the highest earning and most respected positions in society. Their extensive education, specialized knowledge, and critical role in preserving human life have traditionally guaranteed them financial security and social prestige. Yet in recent years, a growing conversation has emerged: could skilled tradesmen—electricians, plumbers, welders, carpenters, and other hands‑on professionals—eventually out‑earn doctors in the future? While the answer is complex, shifting economic dynamics suggest that the gap between these professions may narrow, and in certain contexts, tradesmen could indeed surpass doctors in earnings.
One of the most significant factors driving this possibility is supply and demand. The medical profession requires years of schooling, residency, and licensing, which creates a steady pipeline of doctors but also limits entry. By contrast, skilled trades have suffered from declining interest among younger generations, many of whom were encouraged to pursue college degrees instead of vocational training. As a result, there is now a shortage of tradesmen in many regions. When demand for services like plumbing or electrical work rises but supply remains low, wages naturally increase. Already, some master tradesmen charge hourly rates that rival or exceed those of general practitioners.
Another consideration is student debt and overhead costs. Doctors often graduate with hundreds of thousands of dollars in debt, and many must work in hospital systems or private practices with high administrative expenses. Tradesmen, on the other hand, typically face lower educational costs and can enter the workforce much earlier. Many start their own businesses with relatively modest investments, allowing them to keep a larger share of their earnings. In an era where entrepreneurship and independence are highly valued, tradesmen may find themselves financially freer than doctors burdened by debt and bureaucracy.
***
***
The changing economy also plays a role. Automation and artificial intelligence are beginning to reshape medicine, with diagnostic tools, telehealth, and robotic surgery reducing the need for certain human tasks. While doctors will always be essential, parts of their work may become less lucrative as technology takes over. Skilled trades, however, are far harder to automate. Repairing a leaking pipe, rewiring a house, or welding a custom structure requires physical presence, adaptability, and problem‑solving in unpredictable environments—skills machines struggle to replicate. This resilience against automation could make tradesmen’s work increasingly valuable.
That said, doctors will likely continue to command high salaries in specialized fields such as surgery, cardiology, or oncology. The prestige and necessity of medical expertise ensure that society will always reward them. Yet the notion that tradesmen are “lesser” careers is fading. In fact, many tradesmen already earn six‑figure incomes, particularly those who own successful businesses or operate in regions with acute labor shortages.
Ultimately, whether tradesmen will out‑earn doctors depends on how society values different forms of expertise. If current trends continue—rising demand for trades, shortages of skilled labor, resistance to automation, and lower educational barriers—it is plausible that many tradesmen will match or surpass doctors in income. The future may not be defined by one profession dominating the other, but by a more balanced recognition that both healers and builders are indispensable to modern life. In that sense, the financial gap may close, reflecting a broader cultural shift toward valuing practical skills as highly as academic ones.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
BASIC DEFINITIONS
***
***
The Direct Reimbursement Payment Model allows physicians to receive payment directly from patients or employers, bypassing traditional insurance systems. This model emphasizes transparency, autonomy, and personalized care, offering an alternative to fee-for-service and managed care structures.
The Direct Reimbursement Payment Model is a healthcare financing approach in which physicians are paid directly by patients or sponsoring entities—such as employers—rather than through insurance companies or government programs. This model is gaining traction as a response to the administrative burdens, opaque billing practices, and fragmented care often associated with traditional insurance-based systems.
One prominent example of direct reimbursement is Direct Primary Care (DPC). In DPC, patients pay a recurring fee—monthly, quarterly, or annually—that covers a broad range of primary care services. These include routine checkups, preventive screenings, chronic disease management, and basic lab work. By eliminating third-party billing, DPC practices reduce overhead costs and administrative complexity, allowing physicians to spend more time with patients and focus on quality care.
***
***
Employers have also embraced direct reimbursement models to manage healthcare costs and improve employee wellness. In such arrangements, employers reimburse physicians or clinics directly for services rendered to their employees, often through a defined benefit structure. This can be part of a self-funded health plan or a supplemental offering alongside high-deductible insurance policies. The goal is to provide accessible, cost-effective care while avoiding the inefficiencies of traditional insurance networks.
Key advantages of the direct reimbursement model include:
Price transparency: Patients know upfront what services cost, reducing surprise billing and financial stress.
Improved access: Physicians often offer same-day or next-day appointments, extended visits, and direct communication via phone or email.
Lower administrative burden: Without insurance paperwork, practices can operate more efficiently and focus on patient care.
Stronger patient-physician relationships: More time per visit fosters trust, continuity, and better health outcomes.
However, the model is not without limitations. Direct reimbursement may not cover specialist care, hospitalization, or emergency services, requiring patients to maintain supplemental insurance. Additionally, the model may be less accessible to low-income populations who cannot afford recurring fees or out-of-pocket payments. Critics also argue that widespread adoption could fragment care and reduce risk pooling, undermining the broader goals of universal coverage.
Despite these concerns, the direct reimbursement model aligns with broader trends in healthcare reform, including value-based care, consumer empowerment, and decentralized service delivery. It offers a viable path for physicians seeking autonomy and for patients desiring personalized, transparent care. As healthcare continues to evolve, hybrid models that combine direct reimbursement with traditional insurance may emerge, offering flexibility and choice across diverse patient populations.
In conclusion, the Direct Reimbursement Payment Model represents a meaningful shift in how healthcare services are financed and delivered.
By prioritizing simplicity, transparency, and patient-centered care, it challenges the status quo and opens new possibilities for sustainable, high-quality medical practice.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
For generations, the prevailing belief in healthcare has been that physicians [MD, DO and DPM], with their high salaries and prestige, inevitably retire wealthier than nurses. Yet this assumption overlooks the financial realities of different nursing specialties and the long‑term impact of debt, lifestyle, and retirement planning. In fact, some Registered Nurses (RNs)—particularly Certified Registered Nurse Anesthetists (CRNAs), visiting nurses, and those who participate in structured pay programs like the Baylor plan—can retire richer than physicians. The reasons lie in the interplay of education costs, career flexibility, income potential, and disciplined financial planning.
Education Costs and Debt Burden
One of the most decisive factors shaping retirement wealth is the cost of education. Physicians often spend over a decade in training, including undergraduate studies, medical school, and residency. This path not only delays their earning years but also saddles them with substantial student debt. The median medical school debt in the United States exceeds $200,000, and many physicians spend years paying it down.
By contrast, RNs typically complete their training in two to four years, with advanced practice nurses such as CRNAs requiring graduate‑level education. Even so, their debt burden is far lighter, often less than half of what physicians carry. This difference means nurses can begin earning earlier, save for retirement sooner, and avoid the crushing interest payments that erode physicians’ wealth. A CRNA who starts practicing in their late twenties may already be investing in retirement accounts while a physician is still in residency earning a modest stipend.
Income Potential of Specialized Nurses
While physicians generally earn more annually than nurses, the gap is narrower in certain specialties. CRNAs, for example, are among the highest‑paid nursing professionals, with average salaries often exceeding $200,000 per year. This places them in direct competition with some physician specialties, especially primary care doctors, who may earn similar or even lower salaries.
Visiting nurses also benefit from unique financial advantages. Many work on flexible schedules, contract arrangements, or per‑visit compensation models. This allows them to maximize income while minimizing burnout. By avoiding the overhead costs of private practice and the administrative burdens physicians face, visiting nurses can channel more of their earnings directly into savings and investments.
When combined with lower debt and earlier career starts, these income streams can compound into significant retirement wealth.
The Baylor plan, a structured pay program used by some hospitals, allows nurses to work full‑time hours compressed into fewer days—often weekends—while still receiving full‑time pay and benefits. This arrangement provides several financial advantages. First, it enables nurses to earn competitive wages while freeing up weekdays for additional work, education, or entrepreneurial ventures. Second, it reduces commuting and childcare costs, allowing more income to be saved. Third, the plan often includes robust retirement benefits, such as employer‑matched contributions to 401(k) or pension programs.
Nurses who consistently participate in such structured pay plans can accumulate substantial nest eggs, often surpassing physicians who delay retirement savings due to debt repayment or lifestyle inflation. The Baylor plan highlights the importance of systematic investing: by automating contributions and focusing on long‑term growth, nurses can harness the power of compound interest. A nurse who invests steadily for 35 years may accumulate more wealth than a physician who begins saving late and inconsistently, despite earning a higher salary.
Lifestyle and Work‑Life Balance
Another overlooked factor is lifestyle. Physicians often face grueling schedules, high stress, and the temptation to maintain expensive lifestyles commensurate with their social status. Luxury homes, cars, and vacations can erode their financial base. Nurses, while not immune to lifestyle inflation, often maintain more modest spending habits.
Visiting nurses, in particular, enjoy flexibility that allows them to balance work with personal life. This reduces burnout and healthcare costs while enabling consistent employment into later years. By living within their means and prioritizing savings, nurses can accumulate wealth steadily without the financial pitfalls that sometimes accompany physician lifestyles.
Retirement Wealth Beyond Salary
Retirement wealth is not solely determined by annual income. It is shaped by debt management, savings discipline, investment strategies, and lifestyle choices. Nurses who leverage high‑paying specialties like anesthesia, flexible arrangements like visiting nursing, and structured programs like the Baylor plan can outperform physicians in these areas.
Consider two professionals: a physician earning $250,000 annually but burdened by $200,000 in debt and high living expenses, and a CRNA earning $200,000 with minimal debt and disciplined savings. Over decades, the CRNA may accumulate more net wealth, retire earlier, and enjoy greater financial security.
Conclusion
The assumption that physicians always retire richer than nurses is outdated. While physicians command higher salaries, their delayed earnings, heavy debt, and lifestyle pressures often undermine long‑term wealth. Nurses, particularly CRNAs, visiting nurses, and those who participate in structured pay programs like the Baylor plan, can retire wealthier by combining lower debt, earlier savings, competitive incomes, and disciplined financial planning.
Ultimately, retirement wealth is not about prestige but about strategy. Nurses who recognize this truth and act accordingly may find themselves enjoying more financial freedom than the very physicians they once assisted.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A.I.
***
***
The Pitfalls of Capitation in Medicine
Capitation, a payment model in healthcare where providers receive a fixed amount per patient regardless of the services rendered, has been promoted as a way to control costs and incentivize efficiency. However, despite its theoretical appeal, capitation medicine presents significant drawbacks that can compromise patient care, distort provider incentives, and exacerbate systemic inequities.
One of the most concerning aspects of capitation is the potential for under-treatment. Since providers are paid a set fee per patient, regardless of how much care that patient requires, there is a financial incentive to minimize services. This can lead to situations where necessary tests, referrals, or treatments are delayed or denied in order to preserve profit margins. Patients with complex or chronic conditions—who require more frequent and intensive care—may be especially vulnerable under this model. The risk is that medical decisions become driven by cost containment rather than clinical need, undermining the ethical foundation of healthcare.
Capitation also introduces challenges in maintaining quality standards. Unlike value-based care, which ties reimbursement to outcomes, capitation focuses solely on cost predictability. Without robust oversight and accountability mechanisms, providers may cut corners or avoid high-risk patients altogether. This can result in cherry-picking, where healthier individuals are favored, and sicker patients are subtly discouraged from enrolling. Such practices not only distort the patient pool but also deepen health disparities, particularly among marginalized populations who already face barriers to care.
Furthermore, capitation can strain the provider-patient relationship. Physicians may feel pressured to limit time spent with each patient or avoid costly interventions, leading to a sense of transactional care rather than personalized attention. This erosion of trust can diminish patient satisfaction and reduce adherence to treatment plans. In a system where providers are rewarded for doing less, the intrinsic motivation to go above and beyond for patients may be compromised.
Operationally, capitation demands sophisticated infrastructure to manage risk, track utilization, and ensure compliance. Smaller practices or those serving underserved communities may lack the resources to implement such systems effectively. This can create a two-tiered system where well-funded organizations thrive while others struggle to deliver basic care. Additionally, the administrative burden of managing capitation contracts, monitoring performance metrics, and navigating complex reimbursement rules can divert attention from clinical priorities.
Critics also argue that capitation may stifle innovation. When providers are locked into fixed budgets, there is little room to experiment with new technologies, therapies, or care models that might improve outcomes but carry upfront costs. This conservative approach can hinder progress and limit access to cutting-edge treatments.
In conclusion, while capitation medicine aims to control costs and streamline care, its inherent risks—under-treatment, inequity, and diminished quality—make it a problematic model when not carefully regulated. To truly reform healthcare, payment systems must balance financial sustainability with ethical responsibility, ensuring that every patient receives the care they need, not just the care that fits a budget.
What Medical School Didn’t Teach Doctors About Money
Medical school is designed to mold students into competent, compassionate physicians. It teaches anatomy, pathology, pharmacology, and clinical skills with precision and rigor. Yet, despite the depth of medical knowledge imparted, one critical area is often overlooked: financial literacy. For many doctors, the transition from student to professional comes with a steep learning curve—not in medicine, but in money. From managing debt to understanding taxes, investing, and retirement planning, medical school leaves a financial education gap that can have long-term consequences.
The Debt Dilemma
One of the most glaring omissions in medical education is how to manage student loan debt. The average medical student graduates with over $200,000 in debt, yet few are taught how to navigate repayment options, interest accrual, or loan forgiveness programs. Many doctors enter residency with little understanding of income-driven repayment plans or Public Service Loan Forgiveness (PSLF), missing opportunities to reduce their financial burden. Without guidance, some make costly mistakes—such as refinancing federal loans prematurely or choosing repayment plans that don’t align with their career trajectory.
Income ≠ Wealth
Medical students often assume that a high salary will automatically lead to financial security. While physicians do earn more than most professionals, income alone doesn’t guarantee wealth. Medical school rarely addresses the importance of budgeting, saving, and investing. As a result, many doctors fall into the “HENRY” trap—High Earner, Not Rich Yet. They spend lavishly, assuming their income will always cover expenses, only to find themselves living paycheck to paycheck. Without a solid financial foundation, even high earners can struggle to build net worth.
***
***
Taxes and Business Skills
Doctors are also unprepared for the complexities of taxes. Whether employed by a hospital or running a private practice, physicians face unique tax challenges. Medical school doesn’t teach how to track deductible expenses, optimize retirement contributions, or navigate self-employment taxes. For those who open their own clinics, the lack of business education is even more pronounced. Understanding profit margins, payroll, insurance billing, and compliance regulations is essential—but rarely covered in medical training.
Investing and Retirement Planning
Another blind spot is investing. Medical students are rarely taught the basics of compound interest, asset allocation, or retirement accounts. Many don’t know the difference between a Roth IRA and a traditional 401(k), or how to evaluate mutual funds and index funds. This lack of knowledge delays retirement planning and can lead to missed opportunities for long-term growth. Some doctors rely on financial advisors without understanding the fees or conflicts of interest involved, putting their wealth at risk.
Insurance and Risk Management
Medical school also fails to educate students on insurance—life, disability, malpractice, and health. Doctors need robust coverage to protect their income and assets, but many don’t know how to evaluate policies or understand terms like “own occupation” or “elimination period.” Inadequate coverage can leave physicians vulnerable to financial disaster in the event of illness, injury, or litigation.
Emotional and Behavioral Finance
Beyond technical knowledge, medical school overlooks the emotional side of money. Physicians often face pressure to maintain a certain lifestyle, especially after years of sacrifice. The desire to “catch up” can lead to impulsive spending, luxury purchases, and financial stress. Without tools to manage money mindset and behavioral habits, doctors may struggle with guilt, anxiety, or burnout related to finances.
The Case for Financial Education
Fortunately, awareness of this gap is growing. Organizations like Medics’ Money and podcasts such as “Docs Outside the Box” are working to fill the void by offering financial education tailored to physicians.
These resources cover everything from budgeting and debt management to investing and entrepreneurship. Some medical schools are beginning to incorporate financial literacy into their curricula, but progress is slow and inconsistent.
Conclusion
Medical school equips doctors to save lives, but it doesn’t prepare them to secure their own financial future. The lack of financial education leaves many physicians vulnerable to debt, poor investment decisions, and lifestyle inflation. To thrive both professionally and personally, doctors must seek out financial knowledge beyond the classroom. Whether through self-study, mentorship, or professional guidance, understanding money is as essential as understanding medicine. After all, financial health is a cornerstone of overall well-being—and every doctor deserves to master both.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Why It Is Difficult to Practice Medicine Part-Time Today?
In the past, part-time medical practice offered physicians a flexible way to balance professional responsibilities with personal or family commitments. Today, however, the healthcare environment has evolved in ways that make part-time medicine increasingly challenging. From administrative burdens to economic pressures and patient expectations, the obstacles are both systemic and personal.
One of the most significant barriers is the rise in administrative complexity. Physicians are now required to navigate electronic health records (EHRs), comply with insurance documentation, and meet regulatory standards such as HIPAA and MACRA. These tasks consume hours of non-clinical time, which is difficult to compress into a part-time schedule. Even seeing fewer patients doesn’t exempt part-time doctors from the same documentation and compliance requirements as their full-time counterparts.
***
***
Another challenge is financial viability. Many physicians are paid based on productivity metrics, such as Relative Value Units (RVUs), which reward volume over quality. Part-time practitioners often struggle to meet these benchmarks, resulting in lower compensation and reduced benefits. Additionally, malpractice insurance premiums and licensing fees remain fixed regardless of hours worked, further eroding the financial appeal of part-time practice.
Continuity of care is also a concern. Patients increasingly expect immediate access to their providers, especially in primary care and specialties like psychiatry or pediatrics. Part-time physicians may not be available for urgent issues, leading to fragmented care and dissatisfaction. This can strain relationships with patients and colleagues who must cover gaps in availability.
From a professional standpoint, part-time physicians may face limited career advancement. Leadership roles, academic appointments, and research opportunities often favor full-time commitment. There’s also a perception—sometimes unfair—that part-time doctors are less dedicated or less competent, which can affect peer respect and influence within medical institutions.
Technology, while beneficial, adds another layer of complexity. Telemedicine, remote monitoring, and digital communication tools have expanded access but also increased the expectation for constant availability. Part-time physicians may find it difficult to manage asynchronous messages, follow-ups, and virtual visits without extending their work hours beyond what they intended.
***
***
Lastly, burnout and work-life balance—ironically one of the reasons doctors seek part-time roles—can still be elusive. The pressure to maintain clinical excellence, stay updated with medical advancements, and meet patient needs doesn’t diminish with reduced hours. In fact, squeezing these responsibilities into fewer days can intensify stress rather than alleviate it.
In conclusion, while part-time medical practice may seem like a solution to modern work-life challenges, the reality is far more complex. The structure of today’s healthcare system, combined with economic, technological, and cultural pressures, makes it difficult for physicians to thrive in part-time roles. Addressing these challenges will require systemic reform, flexible compensation models, and a cultural shift in how we value and support diverse medical careers.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Hobson’s choice is a free choice in which only one thing is actually offered. The term is often used to describe an illusion that choices are available. The best known example is “I’ll give you a choice: Take it or leave it”, wherein “leaving it” is strongly undesirable.
The phrase is said to have originated with Thomas Hobson (1544–1631), a livery stable owner in Cambridge, England, who offered customers the choice of either taking the horse in the stall nearest to the door or taking none at all.
A CASE MODEL
Half of Physicians Plan to Change Career Paths
The Physicians Foundation recently conducted a survey on physician practice patterns and perspectives. Here are some key findings from the report:
• 31% of physicians identify as independent practice owners or partners. • Almost half (47%) of physicians plan to change career paths. • 78% of physicians sometimes, often or always experience feelings of burnout. • Nearly a quarter of physician time is spent on non-clinical paperwork.
This result is not a good Hobson’s Choice in Medicine.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
A Financial Self Discovery Questionnairefor Medical Professionals
For understanding your relationship with money, it is important to be aware of yourself in the contexts of culture, family, value systems and experience. These questions will help you. This is a process of self-discovery. To fully benefit from this exploration, please address them in writing. You will simply not get the full value from it if you just breeze through and give mental answers. While it is recommended that you first answer these questions by yourself, many people relate that they have enjoyed the experience of sharing them with others who are important to them.
As you answer these questions, be conscious of your feelings, actually describing them in writing as part of your process.
Childhood
What is your first memory of money?
What is your happiest moment with Money? Your most unhappy?
Name the miscellaneous money messages you received as a child.
How were you confronted with the knowledge of differing economic circumstances among people, that there were people “richer” than you and people “poorer” than you?
Cultural heritage
What is your cultural heritage and how has it interfaced with money?
To the best of your knowledge, how has it been impacted by the money forces? Be specific.
To the best of your knowledge, does this circumstance have any motive related to Money?
Speculate about the manners in which your forebears’ money decisions continue to affect you today?
Family
How is/was the subject of money addressed by your church or the religious traditions of your forebears?
What happened to your parents or grandparents during the Depression?
How did your family communicate about money?
How? Be as specific as you can be, but remember that we are more concerned about impacts upon you than historical veracity.
When did your family migrate to America (or its current location)?
What else do you know about your family’s economic circumstances historically?
Your parents
How did your mother and father address money?
How did they differ in their money attitudes?
How did they address money in their relationship?
Did they argue or maintain strict silence?
How do you feel about that today?
Please do your best to answer the same questions regarding your life or business partner(s) and their parents.
Childhood: Revisited
How did you relate to money as a child? Did you feel “poor” or “rich”? Relatively? Or, absolutely? Why?
Were you anxious about money? Did you receive an allowance? If so, describe amounts and responsibilities.
Did you have household responsibilities?
Did you get paid regardless of performance?
Did you work for money?
If not, please describe your thoughts and feelings about that.
***
***
Same questions, as a teenager, young adult, older adult.
Credit
When did you first acquire something on credit?
When did you first acquire a credit card?
What did it represent to you when you first held it in your hands?
Describe your feelings about credit.
Do you have trouble living within your means?
Do you have debt?
Adulthood
Have your attitudes shifted during your adult life? Describe.
Why did you choose your personal path? a) Would you do it again? b) Describe your feelings about credit.
Adult attitudes
Are you money motivated? If so, please explain why? If not, why not? How do you feel about your present financial situation? Are you financially fearful or resentful? How do you feel about that?
Will you inherit money? How does that make you feel?
If you are well off today, how do you feel about the money situations of others? If you feel poor, same question.
How do you feel about begging? Welfare? If you are well off today, why are you working?
Do you worry about your financial future?
Are you generous or stingy? Do you treat? Do you tip?
Do you give more than you receive or the reverse? Would others agree?
Could you ask a close relative for a business loan? For rent/grocery money?
Could you subsidize a non-related friend? How would you feel if that friend bought something you deemed frivolous?
Do you judge others by how you perceive they deal with their Money? Do you feel guilty about your prosperity? Are your siblings prosperous?
What part does money play in your spiritual life?
Do you “live” your Money values?
Conclusion
There may be other questions that would be useful to you. Others may occur to you as you progress in your life’s journey. The point is to know your personal money issues and their ramifications for your life, work, and personal mission.
This will be a “work-in-process” with answers both complex and incomplete. Don’t worry.
Just incorporate fine-tuning into your life’s process.
Despite their high salaries, not all doctors are wealthy, and some live paycheck to paycheck. Here are 5 reasons why many doctors today are broke, according to https://medschoolinsiders.com
1 | Believing They Are Universally Smart
The first reason so many doctors are broke is that many doctors believe they are universally smart. While most doctors have deep specialized knowledge, there’s a big difference between being smart in your profession and being smart with money. A physician’s schooling is quite thorough when it comes to the human body, but med school doesn’t include a prerequisite class on how to handle finances.
Graduating medical school is a major feat and certainly demonstrates superior work ethic and cognitive abilities. But many new doctors believe these accomplishments transcend all aspects of life. If you’re smart enough to earn an MD, you’re certainly smart enough to handle your finances, but only once you properly and intentionally educate yourself.
The truth is doctors, especially traditional graduates, haven’t had an opportunity to manage large sums of money until they become fully trained attending physicians and start pulling in low to mid six figures in income. Prior to that, there was very little of it to manage.
Far too many aspiring doctors, and students in general, don’t take the time to learn financial basics, in part because it’s uncomfortable and seems like something they can figure out “later”, whenever that may be. Their poor spending habits and lack of investment knowledge carry over into their careers, causing many to make irresponsible decisions.
The second factor is overspending too soon, and this comes up at two points in training.
First, it’s natural to want to start spending more as soon as you get into residency and start making a little more money. After all, you’ve been a broke student for 8 or more years, and now you’re finally making a reasonable and reliable wage. But that’s where young doctors get into trouble. Residency pays, but not nearly as much as you will be making once you become an attending physician. The average resident makes about $60K a year, and if you begin spending all of that money right away, thinking you’ll handle your loans once you become an attending, you delay paying off your medical school debt, which means the compounding effect through your student loan interest rate works against you.
Now that $250,000 in student loans has ballooned to over $350,000 by the time you finish residency. The compounding effect, which can be one of your greatest allies in your financial life, becomes an equally powerful enemy when working against you through debt. But of course, pinching pennies is easier said than done, especially when you’re in residency and are surrounded by peers in different professions. They’ve been earning good money much longer than you have, and they can afford more luxurious lifestyles.
They may not be worried about indulging in fine dining or how much a hotel costs when traveling. Students in college and medical school are often confident they will resist the temptations, but the desire to keep up with your friends and family can be difficult to ignore, which causes many to overspend before they technically have the money to do so.
The same is true of attending physicians. As soon as those six-figure salaries come rolling in, many physicians go overboard with spending, trying to make up for lost time and to treat yourself.
Now, we are not suggesting you shouldn’t reward yourself for completing residency, but that reward shouldn’t be a Lamborghini. It’s best to continue living like a resident in your first few years after becoming an attending to pay off loans, put a down payment on a home, and get your financial foundation built before loosening the purse strings.
3 | Decreasing Salaries
Third, doctors continue to make less money than they did before. And this includes nearly all 44 medical specialties. For example, while physician compensation technically rose from $343k to $391k between 2017 and 2022, this rise does not keep up with inflation. The real average compensation in 2022 was less than $325k—a $20k decrease in purchasing power in only six years.
For doctors who are already spending to the limits of their salaries with huge mortgages, car payments, business costs, and other luxuries, a decreased salary can have a huge impact. You might be able to cut back by going on fewer vacations or eating out less frequently, but many accrued costs are locked in, such as a mortgage payment, car loan, or leased rental space for your practice.
4 | Increasing Costs of Private Practice
In the past, running a private practice was much simpler, but recent stricter guidelines and regulations have made it difficult for solo practices to keep up. While regulations like the Health Insurance Privacy and Portability Act, or HIPAA, and mandatory Electronic Medical Records, or EMRs, are necessary to protect patients, they make costs higher for physicians who run their own private practice. These physicians need to spend their own money to set up and maintain EMRs as well as invest in security to ensure patient data is protected.
With the steep rise of inflation we’ve seen over the past couple of years, everything is more expensive, which means costs, such as business space, equipment, and even office supplies, have gone up for private practice physicians while salaries have not. 2013 to 2020 saw an annual inflation rate of anywhere from 0.7% to 2.3%. This skyrocketed to an annual inflation rate of 7.0% in 2021 and another 6.5% in 2022. In fact, the cost of running a private practice has increased by almost 40% between 2001 and 2021.
These increased costs are exacerbated by another problem plaguing private practices; decreased reimbursement. While costs increased by almost 40%, Medicare reimbursement only increased by 11%. When doctors see patients who are insured, the insurance companies pay the physicians for their time. For Medicare, the new proposed rules for 2023 would cut reimbursement by around 5%. When adjusting for inflation, Medicare reimbursement decreased by 20% in the last 20 years.
These costs add up, making it extremely difficult for physicians to thrive financially while running a private practice.
5 | Tuition Debt
Lastly, we can’t talk about a doctor’s finances without mentioning the exorbitant debt so many graduating physicians are left with. It won’t shock you to hear that med school is expensive. Extremely expensive. The average cost of tuition for a single year is nearly $60k, with significant variance from school to school, and that’s before accounting for living expenses.
In-state applicants pay less than out-of-state applicants, and students at private schools typically pay more than students at public medical schools. The astronomical costs mean the vast majority of students can’t pay for medical school out of their own pockets. And unless your family is part of the 1%, even with your parents footing the bill, it’s difficult to cover tuition, let alone rent, groceries, transportation, tech, social activities, exam fees, and application costs.
The average total student debt after college and med school is over $250k. But keep in mind that’s the average, which includes 27% of students who graduate with no debt at all. This means the vast majority of students leave medical school owing much more than $250k.
For some perspective, in 1978, the average debt for graduating MDs was $13,500, which, when adjusted for inflation, is a little over $60,000. There are multiple ways to eventually repay these loans, but time and discipline are essential to ensure this money is paid off as quickly as possible.
According to financial advisor Dr. David Edward Marcinko MEd MBA CMP™; consider the following:
Place a portion of your salary (15-20% or more) into a savings account, and another portion (10-20% or more) into wise investments [stocks, bonds, mutual funds, and/or ETFs].
Pay off your bills each month, and then use leftover spending money to purchase fun things like vacations and fancy dinners, within your means. Shop sales, buy used clothes, and use credit card points for travel.
Hire an excellent tax professional and meet with an investment advisor once or twice a year about your investment status and strategy. http://www.MarcinkoAssociates.com
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
BREAKING NEWS
Law enforcement officials in Utah released a video of the suspected shooter in the assassination of Turning Point USA co-founder and CEO Charlie Kirk, saying that the person wore Converse tennis shoes and left a hand print and a shoe print at the scene.
The suspect in Charlie Kirk’s assassination has been identified as Tyler Robinson, a 22-year-old Utah resident. Law enforcement sources told the Daily Mail that Robinson was taken into custody as the alleged assassin who killed Kirk at a rally at Utah Valley University on Wednesday.
Before today, forensic podiatry has even made it into the public zeitgeist with the hit TV show “Bones” which premiered on September 13, 2005, and concluded on March 28, 2017, airing for 246 episodes over 12 seasons. The show was based on forensic anthropology and forensic archaeology, with each episode focusing on the mystery behind human body remains brought in for examination and identification.
In one show, eight pairs of dismembered feet washed ashore after a flood on the U.S.-Canada border, but things didn’t add up when only seven pairs of feet were identified as research corpses from a nearby university body farm.
When the fictional Canadian forensic podiatrist Dr. Douglas Filmore took the remains back to Canada, he had to form a jurisdictional alliance with the United States to match the pairs of feet and identify the victims. A rare and expensive pair of sneakers led the team to the victim’s murderer.
In 2016, an actual forensic podiatry club was started at the Barry University School of Podiatric Medicine. And, a formal class covering aspects of forensic podiatry is held at the New York College of Podiatric Medicine. Students exit the class with an in depth knowledge of forensic podiatry and other legal knowledge applicable to current cases.
More expertly, real-life colleague Michael Steven Nirenberg DPMactually testified in the murder trial of defendants Kailie Brackett and Donnell Dana with the state calling three witnesses to testify, including the podiatrist who claimed Brackett’s footprints match the ones found in blood at the apartment of the victim, Kimberly Neptune. The forensic podiatrist focused on the footprints discovered at Neptune’s apartment, using prints and images of the defendant’s feet taken by law enforcement. After study, he claimed the prints at the scene bore a resemblance to Kailie Brackett’s in the width of the foot. The defense questioned the field of forensic podiatry and pressed Dr. Nirenberg on whether the measurements would be altered depending on how thick the sock covering the foot was woven.
Dr. Nirenberg was also interviewed on National Public Radio’s Morning Edition on April 14th 2023 about the gait of the bombing suspect associated with the capital riot on Wednesday January 6th, 2021. Dr. Nirenberg is president of the American Society of Forensic Podiatry and co-editor of the textbook: “Forensic Gait Analysis: Principles and Practice”. The bombing suspect had placed bombs at the DNC and RNC headquarters in Washington, DC on the night before. NPR asked Dr. Nirenberg to comment on the features of the person’s gait.
Additionally, Nirenberg was interviewed by Nancy Grace on her TV show Crime Stories. Grace interviewed Nirenberg about his forensic podiatry work in helping to solve the murder of a mother of 3 who was killed in a church. The case remains unsolved. The episode, “Fitness-Mom Missy Bevers Bludgeoned Dead in Creekside Church” aired June 6th, 2024 and is available online at Merit+ TV.
And, Netflix’s 2023 docu-series, “Till Murder Do Us Part”, recounts the killings of Derek and Nancy Haysom by including a series of interviews with a cast of real people. The four-part docu-series revolves around the unpacking of how a wealthy couple was murdered in Virginia in 1985. It also focuses on how the suspects, Elizabeth Haysom, and her boyfriend, Jens Soehring, betrayed each other during the trial. Dr. Sarah Reel DPM was the forensic podiatrist who was involved with Jens’ and Elizabeth’s footprint examination. Dr. Reel pointed out that, statistically, there was no difference “between a bare footprint and a socked footprint.” The doctor suggested that Jens’ reference footprint matched closely with the crime scene footprint.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The so-called money factor (abbreviated as MF on invoices) is a number in a decimal form that dealers use to calculate the APR of a car lease. It’s a major part of your monthly payment and dealers are known to jack up the money factor to pad their profits.
Most doctors don’t ask to see it because they’re not aware of it or don’t know how to calculate it. Ask to see the money factor, then multiply it by 2,400.
For example, if the money factor is .00150, you multiply it by 2,400 to get 3.6%. If that’s higher than the prevailing rate, you have room to talk them down.
How to reduce it
So how do you get a good interest rate when you lease a vehicle? The same way you do when borrowing for any other reason, whether it’s buying a home or applying for a personal loan: by having good credit. This may reduce your interest rate because you’ll represent a lower risk to a lender.
A high residual value on the car could also help you get a better interest rate. A higher residual value means you’d have lower monthly payments because there would be less depreciation on the vehicle. Since interest is applied to your monthly payment, a lower monthly payment would equate to reduced interest charges.
The money factor is one of the many numbers you may want to learn about when leasing a car. It’s one of the transactional costs that come with leasing, and allows dealers and finance companies to make a profit on every lease they execute. As a consumer, it’s a smart idea to learn the financial implications of this number and how it’ll affect your overall costs over the course of a multi-year lease.
***
***
If the interest rate is too high, you may need to shop around for a better rate, negotiate with the dealer or lender to lower the money factor, or consider leasing another vehicle that’s more in line with your budget. Either way, make sure you explore all your financial options before taking a car off the lot.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 24, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
Dr. David Edward Marcinko with non-VIP patients
***
The House Committee on Oversight and Government Reform expanded its investigation of the cover-up of former President Joe Biden’s health, prostate cancer, and mental decline.
On June 4th, Chairman James Comer subpoenaed five former senior White House aides to appear for transcribed interviews in addition to Biden’s physician, Kevin O’Connor, M.D. In May, Biden revealed he was diagnosed with advanced prostate cancer. The announcement left the public dumbfounded.
At 82, having spent more than five decades as a president, vice president and senator, Biden had access to world-class medical care. Donald Trump Jr. was one of many political observers who speculated the diagnosis might have been covered up to win the 2020 election. And, Biden’s doctors may have followed standard medical guidelines, and the recommendations about screenings for people of different ages can be controversial, writes health care economist Devon Herrick at the Goodman Institute Health Care Blog.
“Experts often say that men are more apt to die with prostate cancer than from prostate cancer,” wrote Herrick. “There is even some disagreement about whether doctors should treat most occurrences of prostate cancer in older men. That partly explains why Biden had not been screened in a decade.”
Screenings can be costly, time-consuming and uncomfortable, and false positive results can lead to invasive procedures that do not markedly extend life or health. Biden made his first public remarks about his cancer after a Memorial Day event. Biden said he was “feeling good” and expected to “be able to beat this.”
QUESTION: So, was this a case of VIP Patient Paradox?
***
DEFINITION: “VIP medical patient paradox syndrome” is a term coined in 1964 by the psychiatrist Walter Weintraub to describe an intriguing paradox: Throughout history, the rich and famous, with all their resources and fancy doctors, have often received worse medical treatment, and suffered from worse health outcomes, than the average person.
Example: When physicians afford “special privileges” to their powerful patients, from “Mad King” George III to Michael Jackson, they seem to get sicker and even die.
While Weintraub, a psychoanalyst, attributed the problem in part to doctors unconsciously resenting their influential patients, it seems doctors simply get starstruck around famous people and high-ranking figures. Despite their medical expertise, these physicians find themselves opting out of basic tests for “privacy” or prescribing dangerous medications for “comfort.”
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Medicine today is vastly different than a generation ago, and all health care professionals need new skills to be successful and reduce the emerging risks outlined in this textbook, as well as the “unknown-unknowns” elsewhere. Traditionally, the physician was viewed as the “captain of the ship”. Today, their role may be more akin to a ship’s navigator, using clinical, teaching skills and knowledge to chart the patient’s course through a confusing morass of insurance requirements, fees, choices, rules and regulations to achieve the best attainable clinical outcomes.
This new leadership paradigm includes many classic business school principles, now modified to fit the decade long PP-ACA, the era of health reform, and modern technical connectivity and EMRs.
Thus, the physician must be a subtle guide on the side; not bombastic sage on the stage. These, newer health 3.0 leadership philosophies might include:
•Negotiation – working to optimize appropriate treatment plans; ie., quality of life versus quantity of life, •Team play – working in concert with other allied healthcare professionals to coordinate care delivery ,ithin a clinically appropriate and cost-effective framework; •Working within the limits of competence – avoiding the pitfalls of the medical generalist versus the specialist that may restrict access to treatment, medications, physicians and facilities by clearly acknowledging when a higher degree of service is needed on behalf of the patient – all while embracing holistic primary care; •Respecting different cultures and values – inherent in the support of the medical Principle of Autonomy is the acceptance of values that may differ from one’s own. As the US becomes more culturally hetero geneous, medical providers are called upon to work within, and respect, the socio-cultural and/or spiritual framework of patients, students and their families; •Seeking clarity on what constitutes marginal care – within a system of finite resources; providers are called upon to openly communicate with patients regarding access to marginal medical information and/or treatments. •Supporting evidence-based practice – healthcare providers, should utilize outcomes data to reduce variation in treatments to achieve higher efficiencies and improved care delivery thru evidence based medicine [EBM]; •Fostering transparency and openness in communications – healthcare professionals should be willing, and prepared, to discuss all aspects of care, especially when discussing end-of-life issues or when problems arise; •Exercising decision-making flexibility – treatment algorithms, templates and clinical pathways are useful tools when used within their scope; but providers must have the authority to adjust the plan if circumstances warrant.
Becoming skilled in the art of listening and interpreting — In her ground-breaking book, Narrative Ethics: Honoring the Stories of Illness, Rita Charon, MD PhD, a professor at Columbia University, writes of the extraordinary value of using the patient’s personal story in the treatment plan. She notes that, “medicine practiced with narrative competence will more ably recognize patients and diseases; convey knowledge and regard, join humbly with colleagues, and accompany patients and their families through ordeals of illness.” In many ways, attention to narrative returns medicine full circle to the compassionate and caring foundations of the patient-physician relationship.
These thoughts represent only a handful of examples to illustrate the myriad of new skills that tomorrows’ healthcare professionals must master in order to meet their timeless professional obligations of compassionate care and contemporary treatment effectiveness; all within the context modern risk management principles.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on July 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A.I.
***
***
Medical doctors, dentists, and podiatrists have to undergo extensive training before they can practice medicine independently. Once they receive training, there are opportunities to increase pay and prestige in the medical field through a series of promotions. As a doctor, how much training, experience and skills you have can determine your ability to move upward in these levels. But, personal branding strategies may even be more vital in today’s social media age?
***
Physician, medical and healthcare branding is more than just the creation of logos, taglines, or specific brand messaging. It’s about creating a meaningful connection between your mission, vision and values and the people served – from patients and their families to local and global communities.
While there are many different types of branding strategies in marketing science, they all share key elements that serve as the foundation for the strategy. These 9 elements for all physicians and medical professionals include the following:
Brand purpose: The reason the physician is in practice and what he/she is trying to achieve.
Brand vision: The ideas and goals behind the dentist which serve as inspiration for practice growth.
Brand values: The osteopaths beliefs and what they stand for.
Target audience: The demographic(s) and patient targets that the podiatrist is aiming to reach.
Market analysis: An analysis of the marketplace that identifies gaps where the chiropractor has an opportunity to position him/her self based on a unique value proposition.
Awareness goals: The initiatives the doctor will take in order to reach a target market patient demographic.
Brand personality: The human-like attributes of the physician that will help build relationships with patients, consumers and other physicians and practitioners.
Brand voice: The language and tone the doctor uses to communicate with patients, physicians and consumers.
Brand tagline: A memorable slogan that sums up the physician and their medical offering in a few choice words.
And so, physician branding is the development of a easily recognizable identity for a medical practice, clinic or healthcare organization that helps to shape perception by current and prospective patients and the wider world.
We make second investment portfolio opinions affordable
Approximately 1 million allopathic physicians, 150,000 dentists, 200,000 osteopaths, 15,000 podiatrists and 6 million nurses often find it difficult to get an unbiased and fiduciary second opinion on their retirement or brokerage accounts. By offering second opinions for a flat fee, the monetary barriers that prevented colleagues from receiving a second opinion in the past have been removed.
We make second investment portfolio opinions convenient
Here’s how we work: you book an initial appointment with us, answer a few preliminary questions and email us your portfolio information. We then provide a second opinion. It is then up to you to incorporate or not.
We make second investment portfolio opinions timely
Financial markets, jobs and colleague age change like the weather. It is not always okay to wait a week, year or more, to seek a professional second financial portfolio opinion. You need to receive an opinion now. That’s where we come in. We are standing by, ready to take your email [MarcinkoAdvisors@outlook.com] and schedule a free initial consultation within two or three days, or less.
We make second investment portfolio opinions accurate
Fiduciary and non-sales orientated second opinions have the power to change financial lives in the long term. We’ve seen it happen many times. What characterizes a good second opinion? Three things: the opinion must be individualized to your investment portfolio[s], informed and results-oriented. That’s the informed fiduciary approach we take. We are colleagues and look forward to working with you.
Many doctors are surprised to learn of an alternative investment known as a hedge fund, pooled investment vehicle or private investment fund. Unlike mutual funds, they can be structured in many ways. However, these funds cannot be marketed or advertised, but they are far from illegal or illicit.
In fact, physicians were among the early investors in one the most successful hedge funds. Warren Buffett got his start in 1957 running the Buffett Partnership, a hedge fund not open to the public. His first appearance as a money manager was before a group of physicians in Omaha, Nebraska. Eleven decided to invest some money with him. A few then followed into Berkshire Hathaway Inc, now among the most highly valued companies in the world.
And, more recently, Scion Asset Management® LLC, is a private investment firm founded and led by my eloquent colleague Michael J. Burry, MD and featured in the movie, The Big Short. Other hedge fund mangers of note include: George Soros, Carl Icahn, Ken Griffin, David Tepper, John Paulson and Bill Ackman.
A hedge fund is a limited partnership of private investors whose money is managed by professional fund managers who use a wide range of strategies; including leveraging [debt] or trading of non-traditional assets [real-estate, collectible, commodities, cyrpto-currency, etc] to earn above-average returns. Hedge funds are considered a risky alternative investment and usually require a high minimum investment or net worth. This person is known as an “accredited investor” or “Regulation D” investor by the US Securities Exchange Commission and must have the following attributes:
A net worth, combined with spouse, of over $1 million, not including primary residence
An income of over $200,000 individually, or $300,000 with a spouse, in each of the past two years
The hurdle rate is part of the fund manager’s performance incentive compensation. Also known as a “benchmark,” it is the amount, expressed in percentage points an investor’s capital must appreciate before it becomes subject to a performance incentive fee. Podiatrists should view the hurdle rate as a form of protection or the fee arrangement.
The hurdle rate benchmarks a single year’s performance and may be considered mutually exclusive of any other year, or the hurdle rate may compound each year. The former case is more common. In the latter case, a portfolio manager failing to attain a hurdle rate in the first year will find the effective hurdle rate considerably higher during the second year.
Once a fund manager attains the hurdle rate, the investor’s capital account may be charged a performance incentive fee only on the performance above and beyond the hurdle rate. Alternatively, the account may be charged a performance fee for the entire level of performance, including the performance required to attain the hurdle rate. Other variations on the use of the hurdle rate exist, and are limited only by the contract signed between the fund manager and the investor. The hurdle rate is not generally a negotiating point, however.
Example: A fund charges a performance fee with a 6 percent hurdle rate, calculated in mutually exclusive manner. A podiatrist places $100,000 with the fund. The first year’s performance is 5 percent. The doctor therefore owes no performance fee during the first year because the portfolio manager did not attain the hurdle rate. During year two, the portfolio manager guides the fund to a 7 percent return. Because the hurdle rate is mutually exclusive of any other year, the portfolio manager has attained the 6 percent hurdle rate and is entitled to a performance fee.
High Water Mark
Some hedge funds feature a “high water mark” provision known as a ”loss-carry forward.” As with the hurdle rate, the high water mark is a form of protection. It is an amount equal to the greatest value of an investor’s capital account, adjusted for contributions and withdrawals. The high water mark ensures that the manager charges a performance incentive fee only on the amount of appreciation over and above the high water mark set at the time the performance fee was last charged. The current trend is for newer funds to feature this high water mark, while older, larger funds may not feature it.
Example: A fund charges a 20 percent performance fee with a high water mark but no hurdle rate. A podiatrist contributes $100,000 to the fund. During the first year, the hedge fund manager grows that capital account to $110,000 and charges a 20 percent performance fee, or $2,000. The ending capital account balance and high water mark is therefore $108,000. During year two, the account falls back to $100,000, but the high water mark remains $108,000. During year three, in order for the manager to charge a performance fee, the manager must grow the capital account to a level above $108,000.
Claw Back Provision
Rarely, a hedge fund may provide investors with a “claw back” provision. This term results in a refund to the investor of all or part of a previously charged performance fee if a certain level of performance is not attained in subsequent years. Such refunds in the face of poor or inadequate performance may not be legal in some states or under certain authorities.
ASSESSMENT
Managers of hedge funds, like colleague Dimitri Sogoloff MBA who is the CEO of Horton Point investment-technology firm, often aim to produce returns that are relatively uncorrelated with market indices and are consistent with investors’ desired level of risk.
While hedging may reduce some risks overall, they cannot all be eliminated. According to a report by the Hennessee Group, hedge funds were approximately one-third less volatile between 1993 and 2010.
For a podiatrist who already holds mutual funds and/or individual stocks and bonds, a hedge fund may provide diversification and reduce overall portfolio risk. Consider investing in them with care.
2. Burry, Michael, J: Hedge Funds [Wall Street Personified]. In, Marcinko, DE and Hetico, HR: Comprehensive Financial Planning Strategies for Doctors and Advisors [Best Practices from Leading Consultants and Certified Medical Planners™] Productivity Press, New York, 2017.
3. Marcinko, DE and Hetico, HR: Risk Management, Liability Insurance, and Asset Protection Strategies for Doctors and Advisors [Best Practices from Leading Consultants and Certified Medical Planners™]. Productivity Press, New York, 2015.
4. Marcinko, DE: Dictionary of Health Economics and Finance. Springer Publishing Company, NY 2006
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
A hedge fund is a limited partnership of private investors whose money is pooled and managed by professional fund managers. These managers use a wide range of strategies, including leverage (borrowed money) and the trading of nontraditional assets, to earn above-average investment returns. A hedge fund investment is often considered a risky, alternative investment choice and usually requires a high minimum investment or net worth. Hedge funds typically target wealthy investors.
My medical practice has a small self-directed pension plan with profit sharing features.
QUESTION: Can my medical practice’s retirement plan invest in a hedge fund?
Such a pension fund falls under a category called self-directed “plan” assets.
Among the rules are that each participant in the plan counts toward the 100 investor maximum under which most hedge funds operate, that each plan participant be a fully accredited investor, and that the hedge fund keep investments such as pension plans and other funds covered under ERISA to less than 25 percent of total assets under management.
Posted on April 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Classic Definition: Suppose someone tells you “I am lying.” If what he/she tells you is true, then he/she is lying, in which case what he/she tells you are false. On the other hand, if what he/she tells you is false, then he/she is not lying, in which case what he/she tells you is true.
Modern Circumstance: In short: if “I am lying” is true then it is false, and if it is false then it is true.
Paradox Example: The paradox arises for any sentence that says or implies of itself that it is false (the simplest example being “This sentence is false”). It is attributed to the ancient Greek seer Epimenides (fl. c. 6th century BCE), an inhabitant of Crete, who famously declared that “All Cretans are liars” (consider what follows if the declaration is true). The paradox is important in part because it creates severe difficulties for logically rigorous theories of truth; it was not adequately addressed (which is not to say solved) until the 20th century.
Paradox Example: Doctors lie because, as caretakers, our role isto improve the lives of their patients. Re-assuring patients during some of the most difficult times of their lives counts as improving their well being! This is an acceptable practice because it does not cause harm.
Paradox Example: Cultural differences may make a lie of omission or the practice of withholding information from the patient, prudent. For instance, some cultures and religions dictate that the husband or head male family members make all medical decisions for women.
Paradox Example: Many physicians don’t report “near misses” to their patients. But, concealing serious medical errors is something we recommend against.
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals.
Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed.
Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Posted on April 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
OVER HEARD IN THE FINANCIAL ADVISOR’S LOUNGE
***
***
By Perry D’Alessio, CPA [D’Alessio Tocci & Pell LLP]
What I see in my accounting practice is that significant accumulation in younger physician portfolio growth is not happening as it once did. This is partially because confidence in the equity markets is still not what it was; but that doctors are also looking for better solutions to support their reduced incomes.
For example, I see older doctors with about 25 percent of their wealth in the market, and even in retirement years, do not rely much on that accumulation to live on. Of this 25 percent, about 80 percent is in their retirement plan, as tax breaks for funding are just too good to ignore.
What I do see is that about 50 percent of senior physician wealth is in rental real estate, both in a private residence that has a rental component, and mixed-use properties. It is this that provides a good portion of income in retirement.
***
***
QUESTION: So, could I add dialog about real estate as a long term solution for retirement?
Yes, as I believe a real estate concentration in the amount of 5 percent is optimal for a diversified portfolio, but in a very passive way through mutual or index funds that are invested in real estate holdings and not directly owning properties.
Today, as an option, we have the ability to take pension plan assets and transfer marketable securities for rental property to be held inside the plan collecting rents instead of dividends.
Real estate holdings never vary very much, tend to go up modestly, and have preferential tax treatment due to depreciation of the property against income.
Financial Modeling is one of the most highly valued, but thinly understood, skills in financial analysis. The objective of financial modeling is to combine accounting, finance, and business metrics to create a forecast of a company’s future results.
According to Jeff Schmidt, a financial model is simply a spreadsheet, usually built in Microsoft Excel, that forecasts a business’s financial performance into the future. The forecast is typically based on the company’s historical performance and assumptions about the future and requires preparing an income statement, balance sheet, cash flow statement, and supporting schedules (known as a three-statement model, one of many types of approaches to financial statement modeling). From there, more advanced types of models can be built such as discounted cash flow analysis (DCF model), leveraged buyout (LBO), mergers and acquisitions (M&A), and sensitivity analysis
***
DEFINED TERMS
Discounted Cash Flow (DCF): A valuation method used to estimate the value of an investment based on its expected future cash flows, adjusted for the time value of money. It’s like deciding whether a treasure chest is worth diving for now, based on the gold coins you’ll be able to cash in later.
Sensitivity Analysis: This involves changing one variable at a time to see how it affects an outcome. Imagine tweaking your coffee-to-water ratio each morning to achieve the perfect brew strength.
Budget – A budget is the amount of money a department, function, or business can spend in a given period of time. Usually, but not always, finance does this annually for the upcoming year.
Rolling Forecast – A rolling forecast maintains a consistent view over a period of time (often 12 months). When one period closes, finance adds one more period to the forecast.
Topside – A topside adjustment is an overlay to a forecast. This is typically completed by the corporate or headquarter team. As individual teams submit a forecast, the consolidated result might not make sense or align with expectations. When this occurs, the high-level teams use a topside adjustment to streamline or adjust the consolidated view.
Monte Carlo Simulation: Picture yourself at the casino, but instead of gambling your savings away, you’re using this technique to predict different outcomes of your business decisions based on random variables. It’s like playing financial roulette with the odds in your favor.
What-If Analysis: Ever daydream about what would happen if you took that leap of faith with your business? This tool allows you to explore various scenarios without risking a dime. It’s like trying on outfits in a virtual dressing room before making a purchase.
Leveraged Buyout (LBO) Model: This is a bit like orchestrating a heist, but legally. It’s about acquiring a company using borrowed money, with plans to pay off the debts with the company’s own cash flows. High stakes, high rewards.
Mergers and Acquisitions (M&A) Model: Picture two puzzle pieces coming together. This model evaluates how combining companies can create a new, more valuable entity. It’s the corporate version of a matchmaker.
Three Statement Model: The holy trinity of financial modeling, linking the income statement, balance sheet, and cash flow statement. It’s like weaving a tapestry where each thread is crucial to the overall picture.
Capital Asset Pricing Model (CAPM): A formula that calculates the expected return on an investment, considering its risk compared to the market. It’s like choosing the best roller coaster in the park, balancing thrill and safety.
Cash Flow Forecasting: This is your financial weather forecast, predicting the cash flow climate of your business. It helps you plan for sunny days and save for the rainy ones.
Cost of Capital: The price of financing your business, whether through debt or equity. It’s like the interest rate on your growth engine, pushing you to maximize every dollar invested.
Debt Schedule: A timeline of your business’s debts, showing when and how much you owe. It’s your roadmap to becoming debt-free, one milestone at a time.
Equity Valuation: Determining the value of a company’s shares. It’s like assessing the worth of a rare gemstone, ensuring investors pay a fair price for a piece of the treasure.
Financial Leverage: Using debt to amplify returns on investment. It’s like using a lever to lift a heavy object, increasing force but also risk.
Forecast Model: A crystal ball for your finances, projecting future performance based on past and present data. It’s your guide through the financial wilderness, helping you navigate with confidence.
Operating Model: A detailed blueprint of how a business generates value, mapping out operational activities and their financial impact. It’s like laying out the inner workings of a clock, ensuring every gear turns smoothly.
Revenue Growth Model: This tracks potential increases in sales over time, charting a course for expansion. It’s like plotting your ascent up a mountain, anticipating the effort required to reach the summit.
Posted on April 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
WARNING – WARNING
By Dr. DavidEdwardMarcinko; MBA MEd
***
***
According to www.NPR.org, there are more than120,000 health care forums on the Internet with opinions ranging from pharmaceuticals, to sexual dysfunction, to acne. The same goes for commercial doctor blogs that promote lotions, balms and potions, diets and vitamins, minerals, herbs, drinks and elixirs, or various other ingest-ants, digest-ants or pharmaceuticals, etc.
And, to other doctors, the blogging craze is a new novelty where there are no rules, protocols, standards or precise figures on how many “medical-doctor” or related physician-blogs are “out there.” Unfortunately, too many recount gory ER scenes, or pictorially illustrate horrific medical conditions, or serious and traumatic injuries. Of course, others simply are medical practice websites, or those that entice patients into more lucrative plastic surgery or concierge medical practices. Some are from self-serving/credible plaintiff-seeking attorneys wishing to assist patients.
Not all physician blogs are geared toward practice information, marketing or medical sensationalism. In fact, just the opposite seems to be the case in extremely candid blogs, like “Ranting Docs”, “White Coat Rants,” “Grunt Docs”, “Cancer Doc,” “The Happy Hospitalist,” “Mom MD”, “Cross-Over Health”, “Angry Docs” and “M.D.O.D.,” which bills itself as “Random Thoughts from a Few Cantankerous American Physicians.”
According to some of these, they are more like personal journals, or public diaries, where doctors vent about reimbursement rates, difficult cases, medical mistakes, declining medical prestige and control, and/or what a “bummer” it is to have so many patients die; not pay, or who are indigent, noncompliant. We call these the “disgruntled doctor sites.” Some even talk about their own patients, coding issues, or various doctor-patient shenanigans.
But, according to psychiatrist and blogger Dr. Deborah Peel and others, the problem with blogging about patients is the danger that one will be able to identify themselves – the doctor – or that others who know them will be able to identify them.” Her affiliation, Patient Privacy Rights, rightly worries that patients might track back to the individual, and adversely affect their employment, health insurance or other aspects of life.
***
***
And, according to Dr. Jay S. Grife; MA Esq., it is certainly true that if a doctor violates a patient’s privacy there could be legal consequences. Under HIPAA, physicians could face fines or even jail time. In some states, patients can file a civil lawsuit if they believe a doctor has violated their privacy. Still, internet privacy issues are an evolving gray-area that if not wrong, may still be morally and ethically questionable [personal communication].
Our colleague Robert Wachter MD, author of the blog called “Wachter’s World,” says it’s important for doctors to be able to share cases, as long as they change the facts substantially. On the other hand, the author of “Wachter’s World” and a leading expert on patient safety alternately suggests “You might say we as doctors should never be talking about experiences with our patients online or in books or in articles.” But, he says that “patients shouldn’t take all the information on blogs at face value. Taken for what they are — unedited opinions, and in some cases entertainment — blogs can give readers some useful insight into the good, the bad and the ugly of the medical profession”. Link: http://www.the-hospitalist.org/blogs
Well, fair enough! But, doctors unhappy with their current medical career choice, or its modern evolution, should probably consider counseling or even career change guidance, re-education and re-engineering. It is very inappropriate to vent career frustrations in a public venue. It’s far better for the blog to be private and/or by invitation only; if at all [Personal communication].
We believe that a hybrid mash-up of both views can be wholly appropriate, or grossly inappropriate in some cases. Of course the devil is in the details; linguistics and semantics aside. Nevertheless; what is not addressed in electronic physician “mea-culpas” are the professional liability risks and concerns that are evolving in this quasi-professional, quasi-lay, communication forum.
***
***
Example: We have seen medical mistakes, and liability admissions of all sorts, freely and glibly presented. In fact,
“Some physicians find that the act of liability blogging as a professional confession that is useful in moving past their malpractice mistakes. And, it is also a useful way to begin a commitment to a better professional life of caring in the future. It helps eliminate the toxic residue and angst of professional liability and guilt. Moreover, as they are unburdened of past acts of omission or commission, doctors should remember to also forgive those who have wronged them. This helps greatly with the process and brings additional peace.”
However, although some may say that this electronic confession is good for the soul, it may not be good for your professional liability carrier, or you, when plaintiff’s attorneys release a legion of IT focused interns, or automated bots, searching online for your self-admissions and scouring for your self-incriminations. Of course, a direct connection to a specific patient may still not be made and no HIPAA violation is involved. But, a vivid imagination is not need needed to envision this type of blind medical malpractice discovery deposition query even now.
QUESTION:“Doctor Smith, I noted all the medical errors admitted on your blog. What other mistakes did you make in the care and treatment of my client?”
And so, the question of plausible deniability, or culpability, is easily raised. If you must journalize your thoughts for sanity or stress release; do it in print. And, don’t tell anyone about it so the diary won’t be subpoenaed. Then tear it up and throw it away. Remember, with risk management, “It is all about credibility.” Don’t trash yours! These thoughts may be especially important if you covet a medical career as a researcher, editor, educator, medical expert or something other than a working-class or employed physician.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Patient satisfaction occurs when patient perceptions exceed their expectations. They get an intangible “something extra” from their visit, above what they paid for. When patient expectations match their perceptions, mutual obligations are fulfilled, making both practitioner and patient “break-even”.
The clinical result, within a relevant range, is only part of the patient’s perceptions. Numerous sub-conscious impressions comprise the remainder. We’ve all had patients love us despite a less than optimal result. We’ve all had patients angrily leave the practice over some non-clinical matter like a trivial billing dispute. A patient’s perception of any health care service is colored by a vast array of prior experiences that set up current expectations. The patient is pleased to the extent that his current perceptions exceed his/her pre existing expectations. This encompasses far more than the clinical result (within a relevant range), and includes such non-treatment issues as the demeanor of the staff, condition of the physical premises, psychological comfort during the visit, etc.
Remember, all patients talk about you anyway. In the past, a happy patient told four others about what a nice doctor you are. Today, patients post website comments or blogs immediately after their visits. They are more likely to complete treatment and follow instructions, thus obtaining a better medical outcome, and, generating additional fees for the practice. They pay quicker, cause less bad-debt and help create a pleasant environment for us to work in.
An unhappy patient vehemently tells nine others, onground or online, what a nasty greedy rip-off artist you are. Sad, but true! They are not as likely to complete treatment, thus incurring a less than optimal result, and generate fewer fees. They pay slower, if at all, create a stressed environment and detrimentally affect the attitude of other patients in the office.
Try to eliminate problems that might cause negative perceptions (i.e., a filthy restroom) and implement controls that help assure positive perceptions. Patient satisfaction is a soft managerial science. It is a numbers game. Most patients don’t pre-define what would be “acceptable” from this encounter, but have vaguely defined ranges of prior expectations anyway, gleaned from a lifetime of health care related experience. Any variance between these this “acceptable” range of expectations and each trivial encounter invokes some degree positive or negative feeling in the patient.
***
***
The total perception of the office experience is an aggregate of multiple trivial, often subliminal, observations. Patient satisfaction is an intangible and amorphous process complicated by:
Inter patient variables: Significant differences between patients in their “expectations”. Intra patient variables: A single patient can perceive the same thing or situation differently at different times, depending on uncontrollable variables like mood, or, context of occurrence which may (sometimes and/or partially) be controllable by the practice. Luck of the draw” in physical variables: Does Sally or Mary escort the patient to the exam room? Was it the blue or green exam room? Did the last patient to use the rest room, five minutes ago, leave a disgusting mess? Heterogeneous staff variables: Even with appropriate training, people are not machines and have their own quirks.
ASSESSMENT
By proactively anticipating the entire visit, from the patient’s perspective, the practitioner can structure and arrange things such that most patients have, mostly positive perceptions, most of the time. This can be done despite all the potential hetero-genicity of the above factors. Patient satisfaction can be improved in any office, and can be done by anyone.
CONCLUSION
Because patient satisfaction is a multi-faceted amorphous subject, there are multiple correct approaches to the subject and no “cook book” recipe on how to proceed. Try and get the big picture. Identify the worst areas and fix them. Identify the best areas and reinforce them. Proceed slowly. It can be done one facet at a time. Adapt things to your own managerial style and personality. Be completely open to suggestion and change.
Finally, be aware that patient relationship and satisfaction implementation strategies frequently overlap.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on March 29, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
EDITOR-IN-CHIEF
By Dr. David Edward Marcinko; FACFAS MBA MEd
***
***
NATIONAL PHYSICIANS WEEK
National Physicians Week sets out March 25-31 to honor the healers dedicated to the art of medicine. In 2017, National Physicians Week highlighted the shortage of physicians in the United States against a growing landscape of minorities joining the ranks.
#NationalPhysiciansWeek
“In hindsight, I am proud of what we have accomplished in a short period of time, including raising the recognition of our group and spotlighting the years of sacrifice by those in our profession to serve our patients. We are poised to initiate actionable efforts to engage and educate our physician community.”
Cite: Dr. Kimberly Funches Jackson, President
Today in 2025, let’s explore the invaluable contributions of physicians, celebrate their hard work during National Physicians Week, and highlight the essential role that locum doctors play in enhancing healthcare delivery.
A Week to Honor All Physicians
National Physicians Week is a celebration of the remarkable work that doctors do every single day. From diagnosing complex conditions to providing life-saving treatments, physicians dedicate themselves to improving the health and well-being of their patients. It’s a week for healthcare professionals, patients, and communities to come together and show appreciation for the doctors who make a difference in our lives.
Physicians work long hours, face immense pressure, and make critical decisions daily. Their contributions go beyond the walls of the hospital, as many are also involved in research, teaching, and community outreach.
So, this week, it’s important to acknowledge not only their professional expertise but also the compassion and resilience they exhibit in their work.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Without proper internal accounting controls, a medical practice [MD, DO, DPM, DDS, DMD] might never reach peak profitability. Internal controls designed and implemented by the physician-owner help prevent bad things from happening.
Embezzlement protection is the classic example. However, internal controls also help ensure good things happen most of the time; according to colleague Dr. Gary Bode; MSA, CPA.
Some Common Embezzlement “Old School” Schemes
Here are some ‘old-school” embezzlement schemes to avoid; however the list is imaginative and endless.
The physician-owner pocketing cash “off the books”. To the IRS, this is like embezzlement to intentionally defraud it out of tax money.
Employee’s pocketing cash from cash transactions. This is why you see cashiers following protocol that seems to take forever when you’re in the grocery check out line. This is also why you see signs offering a reward if he/she is not offered a receipt. This is partly why security cameras are installed.
Bookkeepers writing checks to themselves. This is easiest to do in flexible software programs like QuickBooks, Peachtree Accounting and related financial software. It is one of the hardest schemes to detect. The bookkeeper self-writes and cashes the check to their own name; and then the name on the check is changed in the software program to a vendor’s name. So a real check exists which looks legitimate on checking statements unless a picture of it is available.
Employees ordering personal items on practice credit cards.
Bookkeepers receiving patient checks and illegally depositing them in an unauthorized, pseudo practice checking account, set up by themselves in a bank different from yours. They then withdraw funds at will. If this scheme uses only a few patients, who are billed outside of the practice’s accounting software it is hard to detect. The doctor must have a good knowledge of existing patients to catch the ones “missing” from practice records. Monitoring the bookkeeper’s lifestyle might raise suspicion, but this scheme is generally low profile and protracted. Checking the accounting software “audit trail” shows the required original invoice deletions or credit memos in a less sophisticated version of this scheme.
Bookkeepers writing payroll checks to non-existent employees. This scheme works well in larger practices and medical clinics with high seasonal turnover of employees, and practices with multiple locations the podiatrist-owner doesn’t visit often.
Bookkeepers writing inflated checks to existing employees, vendors or subcontractors. Physician-owners should beware if romantic relationships between the bookkeeper and other practice related parties.
Bookkeepers writing checks to false vendors. This is another low profile, protracted scheme that exploits the podiatrists-owner’s indifference to accounts payable.
Assessment
Operating efficiency, safeguarding assets, compliance with existing laws and accuracy of financial transactions are common goals of internal managerial and cost accounting in medical practice.
CONCLUSION
Hopefully, the above is a good review to prevent common practice embezzlement schemes. Unfortunately, it is a never-ending endeavor.
References: Marcinko, DE: Dictionary of Health Economics and Finance. Springer Publishing Company, NY 2007.
Some Stupid Things Financial Advisors Say to Physician Clients
A few years ago and just for giggles, colleague Lon Jefferies MBA CFP® and I collected a list of dumb-stupid things said by some Financial Advisors to their doctor, dentist, nurse and and other medical professional clients, along with some recommended under-breath rejoinders:
“They don’t have any debt except for a mortgage and student loans.” OK. And I’m vegan except for bacon-wrapped steak.
“Earnings were positive before one-time charges.” This is Wall Street’s equivalent of, “Other than that Mrs. Lincoln; how was the play?”
“Earnings missed estimates.” No. Earnings don’t miss estimates; estimates miss earnings. No one ever says “the weather missed estimates.” They blame the weatherman for getting it wrong. Finance is the only industry where people blame their poor forecasting skills on reality.
“Earnings met expectations, but analysts were looking for a beat.” If you’re expecting earnings to beat expectations, you don’t know what the word “expectations” means.
“It’s a Ponzi scheme.” The number of things called Ponzi schemes that are actually Ponzi schemes rounds to zero. It’s become a synonym for “thing I disagree with.”
“The [thing not going perfectly] crisis.” Boy who cried wolf, meet analyst who called crisis.
“He predicted the market crash in 2008.” He also predicted a crash in 2006, 2004, 2003, 2001, 1998, 1997, 1995, 1992, 1989, 1984, 1971…
“More buyers than sellers.” This is the equivalent of saying someone has more mothers than fathers. There’s one buyer and one seller for every trade. Every single one.
“Stocks suffer their biggest drop since September.” You know September was only six weeks ago, right?
“We’re cautiously optimistic.” You’re also an oxymoron.
[Guy on TV]: “It’s time to [buy/sell] stocks.” Who is this advice for? A 20-year-old with 60 years of investing in front of him, or a 82-year-old widow who needs money for a nursing home? Doesn’t that make a difference?
“We’re neutral on this stock.” Stop it. You don’t deserve a paycheck for that.
“There’s minimal downside on this stock.” Some lessons have to be learned the hard way.
“We’re trying to maximize returns and minimize risks.” Unlike everyone else, who are just dying to set their money ablaze!
“Shares fell after the company lowered guidance.” Guys, they just proved their guidance can be wrong. Why are you taking this new one seriously?
“Our bullish case is conservative.” Then it’s not a bullish case. It’s a conservative case. Those words mean opposite things.
“We look where others don’t.” This is said by so many investors that it has to be untrue most of the time.
“Is [X] the next black swan?” Nassim Taleb’s blood pressure rises every time someone says this. You can’t predict black swans. That’s what makes them dangerous.
“We’re waiting for more certainty.” Good call. Like in 1929, 1999 and 2007, when everyone knew exactly what the future looked like. Can’t wait!
“The Dow is down 50 points as investors react to news of [X].” Stop it – you’re just making stuff up. “Stocks are down and no one knows why” is the only honest headline in this category.
“Investment guru [insert name] says stocks are [insert forecast].” Go to Morningstar.com. Look up that guru’s track record against their benchmark. More often than not, their career performance lags an index fund. Stop calling them gurus.
“We’re constructive on the market.” I have no idea what that means. I don’t think you do, either.
“[Noun] [verb] bubble.” (That’s a sarcastic observation from investor Eddy Elfenbein.)
“Investors are fleeing the market.” Every stock is owned by someone all the time.
“We expect more volatility.” There has never been a time when this was not the case. Let me guess, you also expect more winters?
“This is a strong buy.” What do I do with this? Click the mouse harder when placing the order in my brokerage account?
“He was tired of throwing his money away renting, so he bought a house.” He knows a mortgage is renting money from a bank, right?
“This is a cyclical bull market in a secular bear.” Vapid nonsense.
“Will Obamacare ruin the economy?” No. And get a grip.
So, don’t let these aphorisms blind you to the critical thinking skills you learned in college, honed in medical school and apply every day in life.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
RISK MANAGEMENT, LIABILITY INSURANCE AND ASSET PROTECTION ABBREVIATIONS
[Glossary of Important Acronyms]
Much has been written and much has been opined on the topic of medical risk management, insurance, asset protection and professional liability for physicians and healthcare providers in this textbook; and elsewhere.
But occasionally, we all still get lost in a wide array of abbreviations, acronyms, and initialisms that are constantly changing in this ecosystem.
And so, this glossary serves as a ready reference for those who want to know about these medical risk management definitions in a quick and ready fashion.
Acronyms and Abbreviations
AAASC American Association of Ambulatory Surgery Centers
AAHP American Association of Health Plans
ABN advance beneficiary notice
ABQAUR American Board of Quality Assurance and Utilization Review
ACE acute care episode
ACHCE American College of Health Care Executives
ACS American College of Surgeons
ADA Americans with Disabilities Act
ADC average daily census
ADL activities of daily living
ADT Admission/Discharge/Transfer
AHA American Hospital Association
AHIMA American Health Information Management Association
AHRQ Agency for Healthcare Research and Quality
AI average inventory
AIMR Association for Investment Management and Research
AIR assumed interest rate
ALE annualized loss expectancy
ALF assisted living facility
ALOS average length of stay
AMA American Medical Association
AMBAC AMBAC Indemnity Corporation
AMGA American Medical Group Association
ANSI American National Standards Institute
AP accounts payable
APA American Psychiatric Association
APC ambulatory payment classification
APG ambulatory payment group
APR annual percentage rate
AR accounts receivable
ASA American Society of Appraisers
ASC ambulatory surgery centers; also Accredited Standards Committee
ASHA American Surgical Hospital Association
ASO administrative services only
ASTC ancillary service technical component
ATM asynchronous transfer mode
AVG ambulatory visit group
BANTA best alternative to negotiated agreement
BBA Balanced Budget Act of 1997
BBRA Balanced Budget Refinement Act [1999]
BCP business continuity planning
BEA break-even analysis
BEP break-even point
BIPA Benefits Improvement and Protection Act [2000]
BLS Bureau of Labor Statistics
BPD border protection device
BS balance sheet
BSA Bank Secrecy Act
BVS business valuation standard
CA certificate authority
CAC Carrier Advisory Committee
CAS cost accounting standards
CASB Cost Accounting Standards Board
CC common criteria [for IT Security Evaluation —ISO/IEC 15408]; complication or comorbidity [for MS-DRGs]
CCA certified cost accountant
CCC cash conversion cycle
CCEVS common criteria evaluation and validation scheme
CCHIT Certification Commission for Healthcare Information Technology
CCU critical care unit
CDC Centers for Disease Control and Prevention
CDH consumer-directed healthcare
CDHP consumer-directed healthcare plan
CDPM Clinical Data Project Manager
CDSS clinical decision support system
CEO Chief Executive Officer
CF conversion factor
CFA Chartered Financial Analyst
CFO Chief Financial Officer
CFR Code of Federal Regulations
CHAMP Children’s Health and Medicare Protection Act of 2007
CHAMPUS Civilian Health and Medical Program of the Uniformed Services
CHE Certified Healthcare Executive
CHIPS Center for Healthcare Industry Performance Studies
CIA Corporate Integrity Agreement
CIO Chief Information Officer
CIP Customer Identification Program
CIS computer information systems
CLIA Clinical Laboratory Improvement Act
CLT capitation liability theory
CME continuing medical education
CMI case mix index
CMIO Chief Medical Information Officer
CMIS contribution margin income statement
CMN Certificate of Medical Necessity
CMP Certified Medical Planner ™
CMS Centers for Medicare and Medicaid Services [formerly HCFA]
COD cash on delivery
COGME Council of Graduate Medical Education
COH cash on hand
COLA cost of living allowance
CON Certificate of Need
COO Chief Operating Officer
COSO Committee of Sponsoring Organizations
COTS commercial off-the-shelf
CPHQ Certified Physician in Healthcare Quality
CPIM Certificate in Production and Inventory Management
CPI-U Consumer Price Index—urban
CPM critical (clinical) path method
CPOE computerized physician order entry [system]
CPR computer-based patient record
CPT current procedural terminology
CQI continuous quality improvement
CRL Certification Revocation List
CRM customer relationship management
CRVS California Relative Value Studies
CSO Chief Security Officer
CT scan computed tomography scan [also called CAT scan]
CUSIP Committee on Uniform Security Identification Procedures
Candid CIO: Will Weider, CIO of Ministry Health Care and Affinity Health System, offers his perspectives on administration issues in this blog.
Christina’s Considerations: Christina Thielst is a hospital and healthcare administrator and entrepreneur with a deep desire for continually improving the health of the community being served. This is her blog.
Healing Hospitals — Formerly Ask a Hospital President: F. Nicholas “Nick” Jacobs has more than 20 years experience in hospital management, with an acknowledged reputation for innovation and consumer-centered leadership.
Hospital Impact: Part of the Fierce network of health sites, this site is becoming popular among healthcare administrators for its news updates, tips and opinions on health care matters.
Leading the Way to Medical Excellence: the president of McLeod Health non-profit institutions provides weekly insights into his facilities and health care in general.
Let’s Talk Health Care: Bruce Bullen, Interim Chief Executive Officer at Harvard Pilgrim in Massachusetts, provides and open and ongoing conversation about health care administration.
Life as a Healthcare CIO: Dr. John Halamka records his experiences with infrastructure, applications, policies, management, and governance as he supports 3,000 doctors, 18,000 faculty and about three million patients.
Managed Care Matters: Joe Paduda shares his knowledge on managed care for group health, health policy, health research, and medical news for insurers, employers, and healthcare providers.
More than Medicine: Tom Quinn, president and CEO of Community General Hospital in Syracuse, New York, began his career as a hospital kitchen worker. His perspective on administration reflects his knowledge on how hospitals work from every angle.
Running a Hospital: A CEO of a large Boston hospital shares thoughts on hospitals, medicine and health care issues.
St. Joseph Medical Center: Chief Executive Officer at St. Joseph Medical Center in Missouri, Mr. Kashman, provides personal insight into administrative matters and general topics.
Todd’s Perspective: Todd Linden, president and CEO of Grinnell Regional Medical Center, offers insights into medical administration and guest bloggers provide insight into various departments.
Wachter’s World: This blog focuses on hospitals, hospitalists, quality, safety, policy and much more from Robert M. Wachter, MD, Professor and Associate Chairman of the Department of Medicine at the University of California, San Francisco.
Legal Matters
Drug and Device Law: This blog contains an attorney’s personal views (and those of several other Dechert attorneys) on topics that arise in the defense of pharmaceutical and medical device product liability litigation.
Drug Injury Watch: Learn more about drug injury lawsuits from an attorney who represents patients and their families.
FDA Law Blog: Hyman, Phelps & McNamara, P.C. is the largest dedicated food and drug law firm in the country. Their knowledge about laws and regulations governing drugs, medical devices, foods, dietary supplements, and cosmetics is helpful to anyone interested in these topics.
Health Care Law Blog: Bob Coffield’s expertise lies in helping businesses and health care providers weave through a variety of state and federal health care regulations and assisting them in business transactions.
Health Plan Law: This site contains information about group health plans, claims administration and related ERISA fiduciary issues. This site also contains tutorials.
HealthBlawg: this is David Harlow’s popular health care law blog, offering expert insights and easy-to-understand analysis.
Healthcare Law Blog: Holland & Hart’s healthcare practice provides insight into this arena, including HIPAA, Stark law, the Anti-kickback Statute and more.
HIPAA Blog: Join in on this discussion of medical privacy issues often buried in “political arcana.”
HIPAA, HiTech & HIT: This updated blog brings insight into legal issues, developments and other pertinent information that relates to the creation, use and exchange of electronic health records.
HIT Blawg: This blog is focused on national health information technology legal trends and current news on this topic.
Home Care Law Blog: Learn more about legal and policy issues in the home health care, private duty and hospice industries from Gilliland & Markette LLP.
Med Law Blog: This law blog focuses on topics that range from compliance to contracts and from employee benefits to HIPAA and HIT.
Physician Law: This blog provides and easy way to stay on top of current news, updates and useful tips relating to legal issues that affect physicians and non-institutional providers.
eHealth and Health IT
Chilmark Research: This blog provides perspectives on key IT trends in the healthcare sector.
davidrothman.net: David is the Information Services Specialist at the Community General Hospital Medical Library, but he also provides great ideas for 2.0 tools and tips for healthcare industry professionals on this blog.
e-CareManagement blog: Vince Kuraitis, owner of Better Health Technologies, LLC, has a passion for disease management and care coordination that dates back to 1995.
e-HealthExpert: A non-profit organization provides a free and open forum to support the development of expertise in the field of eHealth, Healthcare Information Systems, and Health IT (Clinical IT).
eHealth: John Sharp is an IT Manager for a major medical center in Northeast Ohio, with a focus on ehealth, personal health records, Web 2.0 technologies, Windows Sharepoint Services and project management.
Found In Cache: If you would prefer a professional’s take on social media matters, Web sites and all things technological, then follow Ed Bennett, a technology expert for a Maryland medical care system.
Future Health IT: A health IT and EPR advocate from the UK provides a format to discuss the future of health care and IT.
Informaticopia: This UK blogger provides eclectic news and views on health informatics and elearning.
MedGadget: Stay ahead of the gadget curve with this site, which offers information about the newest health care gadgets on the market as well as emerging medical technologies.
Neil Versel’s Healthcare IT Blog: A healthcare journalist’s provides his views on the major segment of the industry he covers — and, he provides a ton of links to other sites as well.
Schwartz Healthcare IT Blog: A variety of authors from Schwartz Communications provide insights into ways to use IT effectively within healthcare facilities.
The Health IT Channel: For a different perspective on IT and EHR as well as other health care issues, watch a few videos at this site.
The Healthcare IT Guy: The CEO of Netspective, a Java/.NET consultancy that specializes in healthcare IT with an emphasis on e-health, EMRs, data integration, and legacy modernization, supplies tips and information for physicians and healthcare administration.
ACKNOWLEDGEMENTS: To Mackenzie H. Marcinko PhD of iMBA Inc., Perry D’Alessio CPA CMP™ [Hon] New York, NY; and Daniel B. Moisand CFP®, Principal for Moisand Fitzgerald Tamayo, Melbourne, FL.
Posted on March 3, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Suppose, as a medical or nursing school student, or new practitioner, you want to invest in a company, but its stock price may be higher than what you want, or can afford, to pay.
Instead of buying a whole share of stock, you can buy a fractional share, which is a “slice” of stock that represents a partial share, for very little money (ie., $5 at Charles Schwab).
***
***
Example: If a company’s stock is selling at $1,000 a share and you were buying $200 worth of it, you would own 0.2 (20%) of a share. With stock slices, investing has never been more accessible.
In 1972, Nobel Laureate Kenneth J. Arrow, PhD shocked academe’ by identifying health economics as a separate and distinct field. Yet, the seemingly disparate insurance, tax, risk management and financial planning principles that he also studied are just now becoming transparent to some medical professionals and their financial advisors. Despite the fact that a basic, but hardly promoted premise of this new wave financial planning era, is imprecision.
Nevertheless, to informed cognoscenti like Certified Medical Planners™, the principles served as predecessors to the modern physician-focused financial advisory niche sector. In 2004, Arrow was selected as one of eight recipients of the National Medal of Science for his innovative views.
And now, as a long bull market may be over, and if the current “new-normal” prevails – meaning a 4.5% real annualized rate of return on equities and a 1.5% real rate on bonds – wealth accumulation for all may be reduced.
An Imprecise Science
There is a major variable, dominant in any marketplace that pushes an economy in a forward direction. It is called consumerism. This became apparent while waiting in a doctor’s office one recent afternoon.
Scenario:
The front office receptionist, who appeared to be about 21 years old, was breaking for lunch and her replacement, who appeared not much older, came over to assist. Realizing the propensity for a long wait, one was taken by the size of waiting room and the number of patients coming in and out of the office. [Americans consume healthcare and a lot of it]. There was another notable peculiarity. The sample prescription bags being carried out the door were no match for the bags under everyone’s eyes, including the doctor’s. The office staff was probably working overtime, if not two jobs, and the doctor was working harder and faster in a managed care system.
Assessment
Why? So they all could afford to buy and voraciously consume for their children and themselves. Americans indeed work longer hours than any other industrialized nation.
Conclusion
Finally, as women medical professionals entered the workforce in unprecedented numbers, the stock markets reached an all time high in 2025, even as money was spent at a feverish pace as the Federal Reserve pumped out money in inflammatory fashion.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
9. We act with honesty, integrity and are always straightforward. 8. We strive to be innovative, creative, iconoclastic, and flexible. 7. We admit and learn from mistakes and don’t repeat them. 6. We work hard always as competitors are trying to catch up. 5. We treat others with dignity and respect. 4. We are the onus of consulting advice for the well being of others. 3. We fight complacency as former success is in the past. 2. The best management styles are timeless, not timely. 1. Our clients are colleagues and always come first.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on November 29, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Is it Good for Retailers … but Bad for Doctors and Consumers?
***
If Black Friday 2024 is anything like 2023, retailers may not be swimming in cash while shoppers bathe in savings. Black Friday deals drew 212 million shoppers to stores in fabulous 2010 and collectively spent $39 billion on products and services.
And, the average amount spent by a Black Friday shopper in 2010 was a whopping $365.34.
***
***
Assessment
We predict Black Friday 2024 sales surpass 2023 with a slight increase over 20222 because of fewer shopping days; and the COVID pandemic explosion..
QUESTION: But, is Black Friday good for the [healthcare] economics sector post [thu] the pandemic? Do patients go shopping rather than to the doctor? What about inflation?
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
If you’ve found yourself worrying about the stock market or money lately, you definitely have company. Money anxiety, also called financial anxiety, has become more common than ever after the presidential election of November 2024.
In fact, the American Psychological Association’s 2022 Stress in America Survey, 87 percent of people who responded listed inflation as a source of significant stress. The rise in prices for everything from fuel to food has people from all backgrounds worried, today. The researchers say, in fact, that no other issue has caused this much stress since the survey began in 2007.
When money and financial concerns cause ongoing stress in your life, you could eventually begin to experience some feelings of anxiety as a result. This anxiety can, in turn, have a negative impact on your quality of life.
***
Chrometophobia, commonly known as fear of money, is a psychological condition characterized by overwhelming anxiety and avoidance of currency; according to colleague Dan Ariely PhD.
Physician Financial Fear is probably the most common emotion among physicians. The fear of being wrong – as well as the fear of being correct! It can be debilitating, as in the corollary expression on fear: the paralysis of analysis.
According to Paul Karasik, there are four common investor and physician fears, which can be addressed by financial advisors and psychologists in the following manner:
Fear of making the wrong decision: ameliorated by being a teacher and educator.
Fear of change: ameliorated by providing an agenda, outline and/or plan.
Fear of giving up control: ameliorated by asking for permission and agreement.
Fear of losing self-esteem: ameliorated by serving the client first and communicating that sentiment in a positive manner.
The Physicians Foundation conducted a survey on physician practice patterns and perspectives a few years ago. Here are some key findings from the report:
• 31% of physicians identify as independent practice owners or partners. • Almost half (47%) of physicians plan to change career paths. • 78% of physicians sometimes, often or always experience feelings of burnout. • Nearly a quarter of physician time is spent on non-clinical paperwork.
The Society of Physician Entrepreneurs (SoPE) was established as a community of interest in 2008 by several members of the American Academy of Otolaryngology – Head and Neck Surgery (AAO-HNS), including Dr. Arlen Meyers, the founding past President & CEO. SoPE became a separate and independent legal entity; incorporating in Washington, D.C. in January 2011. It is a 501 (c) 6 member organization with the stated purpose of providing support; idea stage through funding, for physician entrepreneurs with ideas on how to improve healthcare.
SoPE’s vision is to accelerate physician originated biomedical innovation.
The mission of SoPE is to foster scholarship in biomedical entrepreneurship and provide education, training and support; idea stage through funding, to primarily community-based physician entrepreneurs in the interest of better healthcare.
SoPE membership is open to all physicians and also accepts individuals as associate members; representatives of medical device, legal, venture capital, and other firms with an interest in serving and/or supporting physician entrepreneurs.
Did you know that at MARCINKO & Associates, all medical colleagues throughout the United States may contact us when they are considering the sale, purchase, strategic operating improvement, merger, acquisition and/or other financial business or related personal financial planning transaction?
Our difference is “hard” knowledge and insider financial guidance that helps medical colleagues, nurses, private practitioners, clinics, ambulatory surgery, radiology and outpatient wound care centers realize their ultimate economic goals. This typically includes managerial and cost accounting, financial ratio analysis, fair market valuation business appraisals, business plan creation and personal financial planning.
Our “expert witness” business litigation support service and divorce mediation, arbitration, asset division, settlement and second opinion offerings are always available, as well.
And, our “soft” skill professional career guidance and mentoring center includes executive coaching, consulting and mentoring advisory programs for stressed, conflicted or burned-out physicians and medical practitioners.
Most importantly, our professional fees are reasonable and always transparent.
MARCINKO & Associates also serves universities, medical, business, graduate and nursing schools; physicians, dentists, podiatrists, optometrists and legal societies. This includes accountants, financial service providers, wealth and hedge fund managers, emerging entities, hospitals, CEOs and their BODs, the press, media and related organizations.
Posted on July 18, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd CMP
I grew up in SE inner city Baltimore, Maryland and played stick ball in the parking lot of JHU medical school. And so, I was gratified to learn that it is about to get a lot cheaper—for many students at Johns Hopkins University, at least.
Thanks Mike Bloomberg. Be like Mike!
***
***
The former New York mayor, entrepreneur, and 1964 John Hopkins alum Michael Bloomberg donated $1 billion to the university, according to Bloomberg Philanthropies and the university in a recent announcement. Starting this fall, tuition will be free for students coming from households that earn less than $300,000 annually, and the gift will also cover living expenses and other fees for students from families with less than $175,000 in annual income.
Financial access to medical school is a challenge for many students: The median debt for the class of 2023 is $200,000, according to the Association of American Medical Colleges. This cost can discourage students from attending medical school at a time when the US needs more physicians; the association predicted that there will be a physician shortage of up to 86,000 doctors nationwide by 2036.
Check back periodically for practical updates. Our catalogue library of major books, texts, case models and dictionaries is suggested for additional financial, economic, business and medical practice management information and education.
(“Informed Voice of a New Generation of Fiduciary Advisors for Healthcare”)
For most lay folks, personal financial planning typically involves creating a personal budget, planning for taxes, setting up a savings account and developing a debt management, retirement and insurance recovery plan. Medicare, Social Security and Required Minimal Distribution [RMD] analysis is typical for lay retirement. Of course, we can assist in all of these activities, but lay individuals can also create and establish their own financial plan to reach short and long-term savings and investment goals.
But, as fellow doctors, we understand better than most the more complex financial challenges doctors can face when it comes to their financial planning. Of course, most physicians ultimately make a good income, but it is the saving, asset and risk management tolerance and investing part that many of our colleagues’ struggle with. Far too often physicians receive terrible guidance, have no time to properly manage their own investments and set goals for that day when they no longer wish to practice medicine.
For the average doctor or healthcare professional, the feelings of pride and achievement at finally graduating are typically paired with the heavy burden of hundreds of thousands of dollars in student loan debt.
You dedicated countless hours to learning, studying, and training in your field. You missed birthdays and holidays, time with your families, and sacrificed vacations to provide compassionate and excellent care for your patients. Amidst all of that, there was no time to give your finances even a second thought.
Between undergraduate, medical school, and then internship and residency, most young physicians do not begin saving for retirement until late into their 20s, if not their 30s. You’ve missed an entire decade or more of allowing your money and investments to compound and work for you. When it comes to addressing your financial health and security, there’s no time to waste.
Informational essays of most current interest to healthcare professionals. Check back periodically for practical updates. Our catalogue library of major books, texts, case models and dictionaries is suggested for additional financial, economic, business and medical practice management information and education.
At D.E.Marcinko & Associates our clients traditionally are medical entrepreneurs that include physicians [MD, MBBS, DPM and DO], dentists [DDS and DMD], Registered Nurses [RNs], Certified Registered Nurse Anesthetists [CRNA], Physician Assistants [PA] and Nurse Practitioners [NP]. A growing cohort of clients include medical technologists, physical, speech and occupational therapists, etc.
The above healthcare providers are naturally segregated into three career tranches: 1. New practitioners, 2] Mid-Career practitioners and 3] Mature practitioners. We serve them all and are fully prepared for any special needs situation that may arise in any tranche [death, divorce, adverse risk event and/or bankruptcy, reorganization, etc].
At D. E. Marcinko & Associates, our colleagues are located throughout the United States. They are considering the sale, purchase, strategic or operational improvement, merger, acquisition and/or other business or personal financial planning transaction. Our guidance helps doctors, nurses, practices, clinics, ambulatory surgery centers, outpatient wound care facilities realize their ultimate goals.
We can do it all for you, or educate and guide do it yourself colleagues to reach the best possible outcomes.
Posted on December 13, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
QUESTION: Why are doctors leaving their practices?
For many it’s about demographics. Just like the rest of us, doctors are aging too. Already the average physician age is about 53 years old. The Association of American Medical Colleges reports that about half of doctors are over the age of 55. Over the next decade, an estimated 40% of physicians will be over 65 years old. This means more than two of every five active physicians will reach age 65 within the next 10 years.
Moreover, compared with their boomer colleagues who were more likely to work past retirement, a robust 60% of younger Generation X doctors are reporting that they plan to retire by age 60.
***
***
Doctors cite poor quality of life and stress as reasons for their early departure. The pandemic certainly crushed many providers and has led to burnout. Generation X physicians in their 40s and early 50s were more likely than boomers to report that their current work life was not making the grade. In short, 43% of middle-aged doctors, compared with 31% of doctors over age 55, were reporting lower levels of professional fulfillment. Moreover, 47% of mostly Gen X doctors indicated dissatisfaction with their level of personal fulfillment compared with 36% of practicing boomer physicians.

























































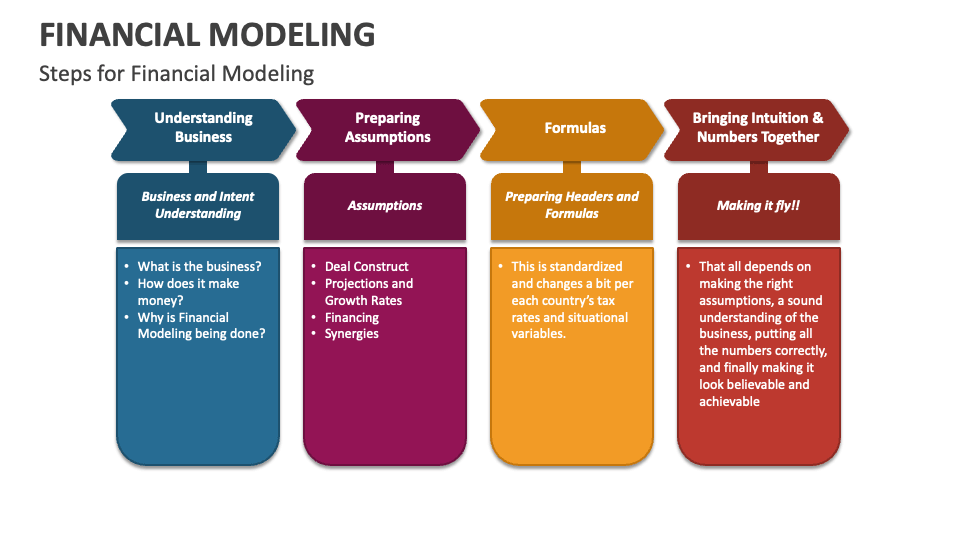








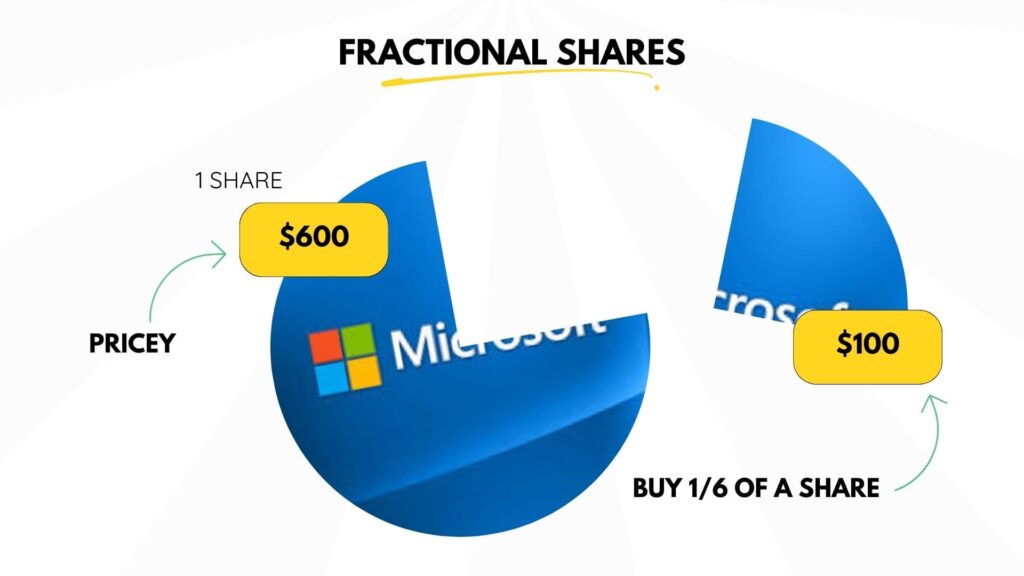



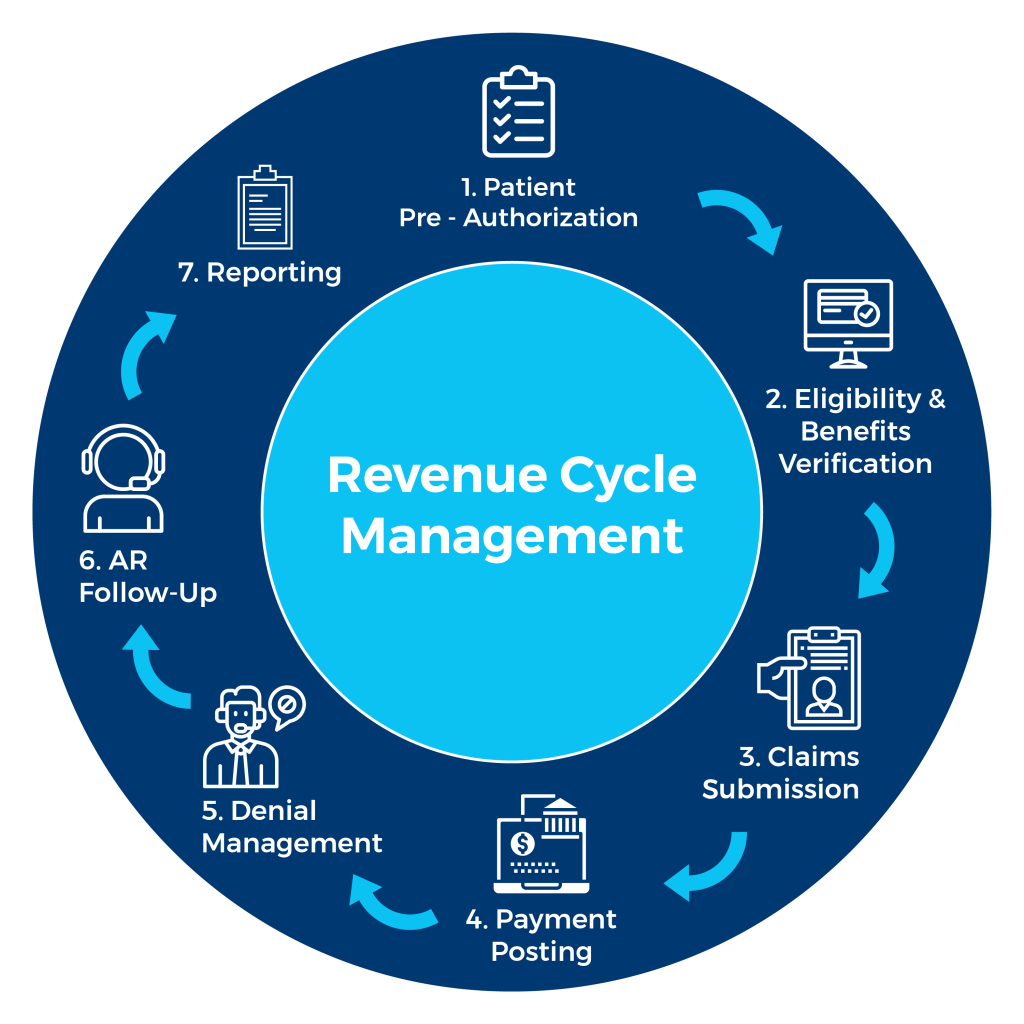























STUPID COMMENTS: Financial Advisors Say to Physician Clients
BY DR. DAVID EDWARD MARCINKO; MBA MEd CMP®
***
***
SPONSOR: http://www.MarcinkoAssociates.com
***
Some Stupid Things Financial Advisors Say to Physician Clients
A few years ago and just for giggles, colleague Lon Jefferies MBA CFP® and I collected a list of dumb-stupid things said by some Financial Advisors to their doctor, dentist, nurse and and other medical professional clients, along with some recommended under-breath rejoinders:
So, don’t let these aphorisms blind you to the critical thinking skills you learned in college, honed in medical school and apply every day in life.
COMMENTS APPRECIATED
Refer, Like and Subscribe
***
EDUCATION: Books
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
***
***
Share this:
Filed under: "Advisors Only", "Doctors Only", Ethics, Jokes and Puns, LifeStyle | Tagged: bears, bulls, crypto, DO, doctor clients, DPM, dumb comments, finance, financial advisors, financial planners, Investing, Lon Jefferies, Marcinko, MD, personal-finance, Physician Clients, physicians, Ponzi, stocks, stupid comments, Wall Street | Leave a comment »