BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on October 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
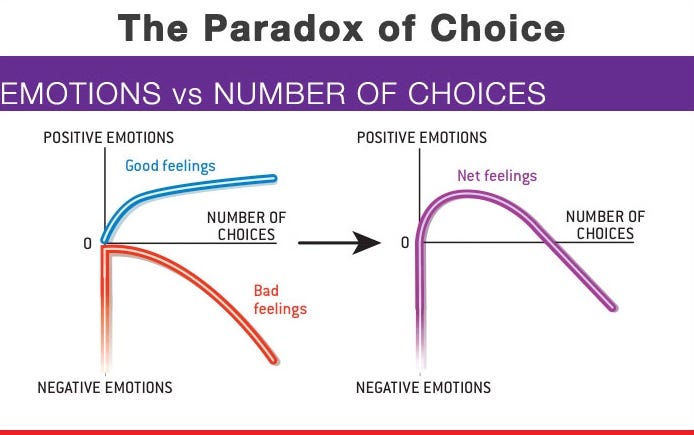
A paradox is a logically self-contradictory statement or a statement that runs contrary to one’s expectation. It is a statement that, despite apparently valid reasoning from true or apparently true premises, leads to a seemingly self-contradictory or a logically unacceptable conclusion. A paradox usually involves contradictory-yet-interrelated elements that exist simultaneously and persist over time. They result in “persistent contradiction between interdependent elements” leading to a lasting “unity of opposites”.
THE TELE-MEDICINE PARADOX
Classic Definition: Refers specifically to the treatment of various medical conditions without seeing the patient in person. Healthcare providers may use electronic and internet platforms like live video, audio, PCs, tablets, or instant messaging to address a patient’s concerns and diagnose their condition remotely.
Modern Circumstance: This may include giving medical advice, walking them through at-home exercises, or recommending them to a local provider or facility. Even more exciting is the emergence of telemedicine apps which give patients access to care right from their phones or computer screens.
Paradox Examples: Treating certain conditions remotely can be challenging. Tele-medicine is often used to treat common illnesses, manage chronic conditions, or provide specialist services. If a patient is dealing with an emergent or serious condition, the remote provider suggests they seek in-person medical care.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Classic: Acute care is a branch of secondary health care where a patient receives active but short-term treatment for a severe injury or episode of illness, an urgent medical condition, or during recovery from surgery. In medical terms, care for acute health conditions is the opposite from chronic care, or longer term care.
Modern: Acute care is active, short-term treatment for a severe injury or episode related to illness, an urgent medical condition or recovery from surgery.
Despite their high salaries, not all doctors are wealthy, and some live paycheck to paycheck. Here are 5 reasons why many doctors today are broke, according to https://medschoolinsiders.com
1 | Believing They Are Universally Smart
The first reason so many doctors are broke is that many doctors believe they are universally smart. While most doctors have deep specialized knowledge, there’s a big difference between being smart in your profession and being smart with money. A physician’s schooling is quite thorough when it comes to the human body, but med school doesn’t include a prerequisite class on how to handle finances.
Graduating medical school is a major feat and certainly demonstrates superior work ethic and cognitive abilities. But many new doctors believe these accomplishments transcend all aspects of life. If you’re smart enough to earn an MD, you’re certainly smart enough to handle your finances, but only once you properly and intentionally educate yourself.
The truth is doctors, especially traditional graduates, haven’t had an opportunity to manage large sums of money until they become fully trained attending physicians and start pulling in low to mid six figures in income. Prior to that, there was very little of it to manage.
Far too many aspiring doctors, and students in general, don’t take the time to learn financial basics, in part because it’s uncomfortable and seems like something they can figure out “later”, whenever that may be. Their poor spending habits and lack of investment knowledge carry over into their careers, causing many to make irresponsible decisions.
The second factor is overspending too soon, and this comes up at two points in training.
First, it’s natural to want to start spending more as soon as you get into residency and start making a little more money. After all, you’ve been a broke student for 8 or more years, and now you’re finally making a reasonable and reliable wage. But that’s where young doctors get into trouble. Residency pays, but not nearly as much as you will be making once you become an attending physician. The average resident makes about $60K a year, and if you begin spending all of that money right away, thinking you’ll handle your loans once you become an attending, you delay paying off your medical school debt, which means the compounding effect through your student loan interest rate works against you.
Now that $250,000 in student loans has ballooned to over $350,000 by the time you finish residency. The compounding effect, which can be one of your greatest allies in your financial life, becomes an equally powerful enemy when working against you through debt. But of course, pinching pennies is easier said than done, especially when you’re in residency and are surrounded by peers in different professions. They’ve been earning good money much longer than you have, and they can afford more luxurious lifestyles.
They may not be worried about indulging in fine dining or how much a hotel costs when traveling. Students in college and medical school are often confident they will resist the temptations, but the desire to keep up with your friends and family can be difficult to ignore, which causes many to overspend before they technically have the money to do so.
The same is true of attending physicians. As soon as those six-figure salaries come rolling in, many physicians go overboard with spending, trying to make up for lost time and to treat yourself.
Now, we are not suggesting you shouldn’t reward yourself for completing residency, but that reward shouldn’t be a Lamborghini. It’s best to continue living like a resident in your first few years after becoming an attending to pay off loans, put a down payment on a home, and get your financial foundation built before loosening the purse strings.
3 | Decreasing Salaries
Third, doctors continue to make less money than they did before. And this includes nearly all 44 medical specialties. For example, while physician compensation technically rose from $343k to $391k between 2017 and 2022, this rise does not keep up with inflation. The real average compensation in 2022 was less than $325k—a $20k decrease in purchasing power in only six years.
For doctors who are already spending to the limits of their salaries with huge mortgages, car payments, business costs, and other luxuries, a decreased salary can have a huge impact. You might be able to cut back by going on fewer vacations or eating out less frequently, but many accrued costs are locked in, such as a mortgage payment, car loan, or leased rental space for your practice.
4 | Increasing Costs of Private Practice
In the past, running a private practice was much simpler, but recent stricter guidelines and regulations have made it difficult for solo practices to keep up. While regulations like the Health Insurance Privacy and Portability Act, or HIPAA, and mandatory Electronic Medical Records, or EMRs, are necessary to protect patients, they make costs higher for physicians who run their own private practice. These physicians need to spend their own money to set up and maintain EMRs as well as invest in security to ensure patient data is protected.
With the steep rise of inflation we’ve seen over the past couple of years, everything is more expensive, which means costs, such as business space, equipment, and even office supplies, have gone up for private practice physicians while salaries have not. 2013 to 2020 saw an annual inflation rate of anywhere from 0.7% to 2.3%. This skyrocketed to an annual inflation rate of 7.0% in 2021 and another 6.5% in 2022. In fact, the cost of running a private practice has increased by almost 40% between 2001 and 2021.
These increased costs are exacerbated by another problem plaguing private practices; decreased reimbursement. While costs increased by almost 40%, Medicare reimbursement only increased by 11%. When doctors see patients who are insured, the insurance companies pay the physicians for their time. For Medicare, the new proposed rules for 2023 would cut reimbursement by around 5%. When adjusting for inflation, Medicare reimbursement decreased by 20% in the last 20 years.
These costs add up, making it extremely difficult for physicians to thrive financially while running a private practice.
5 | Tuition Debt
Lastly, we can’t talk about a doctor’s finances without mentioning the exorbitant debt so many graduating physicians are left with. It won’t shock you to hear that med school is expensive. Extremely expensive. The average cost of tuition for a single year is nearly $60k, with significant variance from school to school, and that’s before accounting for living expenses.
In-state applicants pay less than out-of-state applicants, and students at private schools typically pay more than students at public medical schools. The astronomical costs mean the vast majority of students can’t pay for medical school out of their own pockets. And unless your family is part of the 1%, even with your parents footing the bill, it’s difficult to cover tuition, let alone rent, groceries, transportation, tech, social activities, exam fees, and application costs.
The average total student debt after college and med school is over $250k. But keep in mind that’s the average, which includes 27% of students who graduate with no debt at all. This means the vast majority of students leave medical school owing much more than $250k.
For some perspective, in 1978, the average debt for graduating MDs was $13,500, which, when adjusted for inflation, is a little over $60,000. There are multiple ways to eventually repay these loans, but time and discipline are essential to ensure this money is paid off as quickly as possible.
According to financial advisor Dr. David Edward Marcinko MEd MBA CMP™; consider the following:
Place a portion of your salary (15-20% or more) into a savings account, and another portion (10-20% or more) into wise investments [stocks, bonds, mutual funds, and/or ETFs].
Pay off your bills each month, and then use leftover spending money to purchase fun things like vacations and fancy dinners, within your means. Shop sales, buy used clothes, and use credit card points for travel.
Hire an excellent tax professional and meet with an investment advisor once or twice a year about your investment status and strategy. http://www.MarcinkoAssociates.com
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 10, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITIONS
By Staff Reporters
***
***
Rate Review & the 80/20 Rule
The health care law provides 2 ways to hold insurance companies accountable and help keep your costs down: Rate Review and the 80/20 rule.
Rate Review
Rate Review helps protect you from unreasonable rate increases. Insurance companies must now publicly explain any rate increase of 15% or more before raising your premium. This does not apply to grandfathered plans.
The 80/20 Rule generally requires insurance companies to spend at least 80% of the money they take in from premiums on health care costs and quality improvement activities. The other 20% can go to administrative, overhead, and marketing costs.
The 80/20 rule is sometimes known as Medical Loss Ratio, or MLR. If an insurance company uses 80 cents out of every premium dollar to pay for your medical claims and activities that improve the quality of care, the company has a Medical Loss Ratio of 80%.
Insurance companies selling to large groups (usually more than 50 employees) must spend at least 85% of premiums on care and quality improvement.
If your insurance company doesn’t meet these requirements, you’ll get a rebate on part of the premium that you paid.
Will I get a rebate check from my insurance company?
If your insurance company doesn’t meet its 80/20 targets for the year, you’ll get back some of the premium that you paid.
You may see the rebate in a number of ways:
A rebate check in the mail
A lump-sum deposit into the same account that was used to pay the premium, if you paid by credit card or debit card
A direct reduction in your future premium
Your employer may also use one of the above rebate methods, or apply the rebate in a way that benefits employees
If you or your employer will get a rebate, your insurance company must notify you by August 1.
If you have an individual insurance policy, you’ll get the rebate directly from your insurance company.
For small group and large group plans, the rebate is usually paid to the employer. It may use one of the above rebate methods, or apply the rebate in a way that benefits employees.
FYI: The 80/20 rebate rules don’t apply when an insurance company has fewer than 1000 enrollees in a particular state or market.
For Rate Review: These requirements don’t apply to grandfathered plans. Check your plan’s materials or ask your employer or your benefits administrator to find out if your health plan is grandfathered.
For the 80/20 Rule: These rights apply to all individual, small group, and large group health plans, whether your plan is grandfathered or not.
Posted on August 29, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko; MBA MEd
***
***
Healthcare comes with its share of mental challenges, especially considering that clinicians often care for patients when they’re in difficult and sometimes tragic situations. New research shows that even the path to getting into the workforce can be a challenge, with some physicians burning out before they make it to graduation.
***
American medicine is undergoing vast changes, placing the status of physicians in the medical industrial complex at great risk. Most physicians feel overwhelmed by increasing bureaucratic mandates from insurers, hospitals, and government. At the same time, physicians are the front line employees of healthcare and assume the majority of the risk for patient care. This has left many in the profession with increasing disillusionment.
Samantha Meltzer-Brody a psychiatrist and director of, Taking Care of Our Own, University of North Carolina, Chapel Hill, NC states it best:
“Daily, I am contacted by good doctors who are struggling with symptoms of burnout syndrome and who have become overwhelmed by the challenges of attempting to practice medicine in today’s health care environment. As a psychiatrist who runs a program to address and treat these distressed doctors, I am troubled by the ever-growing number of calls I receive.”
What causes physician burnout?
The “Big 4” factors known to contribute to stress and burnout include:
Time pressure, especially in patient visits or documentation
Lack of control over work environment
Chaotic, fast-paced workplaces
Culture of the organization, specifically a culture that does not emphasize communication, cohesion, trust, and alignment of values between clinicians and their leaders
In addition to burnout rates, these factors can be assessed to help direct interventions toward those drivers that are most likely to be contributing to burnout at your organization.
The burned-out physician is exhausted — mentally and physically — and often no longer able to find empathy or connection with patients. The question of how to escape from what has become a highly unpleasant situation becomes a frequent one. Given the high demands of the profession and serious consequences of mistakes, the burned-out doctor is a potentially impaired one. And the impaired physician is not able to maintain the unflappable, perpetually cool under fire, always objective, professional and yet compassionate demeanor that is expected by society. Worst of all, the impaired physician is at great risk for developing depression, suicidal ideation, or a serious addiction.
The doctors who contact me report feeling beaten down by an increasingly hostile work environment. They say that they don’t have time to take care of patients the way they envisioned when they decided to apply to medical school. Many describe feeling betrayed by a system that they say seems focused on achieving the bottom line with little regard for the impact on both doctors and patients.
Most of these doctors report spending a significant amount of their time dealing with the electronic medical record and documentation. The ratio of time spent on doctor-patient
interactions compared to physician-computer ones appears so horribly skewed that it has reached the point of complete dysmorphia. These good physicians call me when they feel like they can’t continue any longer in the profession. They want to quit medicine. They report a loss of joy and meaning in their work. They describe the toll that the profession has had on their mental health, physical health, and personal lives. And most wrenchingly, they don’t see an end.
What can we do? There are no easy answers to the complex issues that threaten our profession. “The Taking Care of Our Own Program…has had an over 200% rate of growth in the first year, reflecting the enormous need…”
Burned out physicians will eventually be labeled as disruptive, impaired, an outlier or arrogant. There’s a reason it’s difficult and extremely expensive for physicians to find disability insurance; psychiatric claims. Burnout leads to depression, anxiety, PTSD, suicide, divorce, drug abuse, surly behaviors and interactions, etc. It’s nothing new; it’s been occurring for a long time. Go without routine sleep, eat erratically, work long hours, operate under constantly stressful situations and have no time for your family or self and most individuals will de-compensate physically and psychologically within weeks.
Conclusion
Physicians operate within these parameters year after year.
How are they to remain healthy, functional humans? They can’t. Even a superhero couldn’t, yet physicians are expected to endure and thrive under such conditions.
If a physician makes a single mistake, or snaps just one day, their entire career is on the line.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Medicine today is vastly different than a generation ago, and all health care professionals need new skills to be successful and reduce the emerging risks outlined in this textbook, as well as the “unknown-unknowns” elsewhere. Traditionally, the physician was viewed as the “captain of the ship”. Today, their role may be more akin to a ship’s navigator, using clinical, teaching skills and knowledge to chart the patient’s course through a confusing morass of insurance requirements, fees, choices, rules and regulations to achieve the best attainable clinical outcomes.
This new leadership paradigm includes many classic business school principles, now modified to fit the decade long PP-ACA, the era of health reform, and modern technical connectivity and EMRs.
Thus, the physician must be a subtle guide on the side; not bombastic sage on the stage. These, newer health 3.0 leadership philosophies might include:
•Negotiation – working to optimize appropriate treatment plans; ie., quality of life versus quantity of life, •Team play – working in concert with other allied healthcare professionals to coordinate care delivery ,ithin a clinically appropriate and cost-effective framework; •Working within the limits of competence – avoiding the pitfalls of the medical generalist versus the specialist that may restrict access to treatment, medications, physicians and facilities by clearly acknowledging when a higher degree of service is needed on behalf of the patient – all while embracing holistic primary care; •Respecting different cultures and values – inherent in the support of the medical Principle of Autonomy is the acceptance of values that may differ from one’s own. As the US becomes more culturally hetero geneous, medical providers are called upon to work within, and respect, the socio-cultural and/or spiritual framework of patients, students and their families; •Seeking clarity on what constitutes marginal care – within a system of finite resources; providers are called upon to openly communicate with patients regarding access to marginal medical information and/or treatments. •Supporting evidence-based practice – healthcare providers, should utilize outcomes data to reduce variation in treatments to achieve higher efficiencies and improved care delivery thru evidence based medicine [EBM]; •Fostering transparency and openness in communications – healthcare professionals should be willing, and prepared, to discuss all aspects of care, especially when discussing end-of-life issues or when problems arise; •Exercising decision-making flexibility – treatment algorithms, templates and clinical pathways are useful tools when used within their scope; but providers must have the authority to adjust the plan if circumstances warrant.
Becoming skilled in the art of listening and interpreting — In her ground-breaking book, Narrative Ethics: Honoring the Stories of Illness, Rita Charon, MD PhD, a professor at Columbia University, writes of the extraordinary value of using the patient’s personal story in the treatment plan. She notes that, “medicine practiced with narrative competence will more ably recognize patients and diseases; convey knowledge and regard, join humbly with colleagues, and accompany patients and their families through ordeals of illness.” In many ways, attention to narrative returns medicine full circle to the compassionate and caring foundations of the patient-physician relationship.
These thoughts represent only a handful of examples to illustrate the myriad of new skills that tomorrows’ healthcare professionals must master in order to meet their timeless professional obligations of compassionate care and contemporary treatment effectiveness; all within the context modern risk management principles.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
A Johns Hopkins University study, by Michael J. Klag MD in 1997, found that physicians in some specialties — chiefly psychiatry and surgery — are at higher risk for divorce than their medical brethren in other fields. But, the results did not support the common view that job-related anxiety and depression are linked to marital breakup. Alerting medical students to the risks of divorce in some specialties may influence their career choices and strengthen their marriages whatever field they choose. The study, supported by the National Institutes of Health [NIH], was published in the March 13th issue of The New England Journal of Medicine. Results also strongly suggested that the high divorce risk in some specialties may result from the inherent demands of the job as well as the emotional experiences of physicians who enter those fields.
For example, the Hopkins team assessed the specialty choices, marriage histories, psychological characteristics, and other career and personal factors of 1,118 physicians who graduated from The Johns Hopkins University School of Medicine from 1948 through 1964. Over 30 years of follow-up, the divorce rate was 51 percent for psychiatrists, 33 percent for surgeons, 24 percent for internists, 22 percent for pediatricians and pathologists, and 31 percent for other specialties. The overall divorce rate was 29 percent after three decades of follow-up and 32 percent after nearly four decades of follow-up.
Physicians who married before medical school graduation had a higher divorce rate than those who waited until after graduation (33 percent versus 23 percent). The year of first marriage was linked with divorce rates: 11 percent for marriages before 1953, 17 percent for those from 1953 to 1957, 24 percent for those from 1958 to 1962 and 21 percent for those after 1962. Those who had a parent die before medical school graduation had a lower divorce rate.
Female physicians had a higher divorce rate (37 percent) than their male colleagues (28 percent). Physicians who were members of an academic honor society in medical school had a lower divorce rate, although there was no difference in divorce rates according to class rank. Religious affiliation, being an only child, having a parent who was a physician and having a divorced parent were not associated with divorce rates. Physicians who reported themselves to be less emotionally close to their parents and who expressed more anger under stress also had a significantly higher divorce rate, but anxiety and depression levels were not associated with divorce rates.
*Cite: Co-authors of the study, which was part of the Johns Hopkins Precursors Study, an ongoing, prospective study of physicians from the Hopkins medical school graduating classes of 1948 through 1964, were lead author Bruce L. Rollman, M.D., Lucy A. Mead, Sc.M., and Nae-Yuh Wang, M.S.
***
***
The Painful Truth
In their article “The Painful Truth: Physicians Are Not Invincible” [1] Miller and McGowen state that divorce rates among physicians have been reported to be 10% to 20% higher than those in the general population. They explain that for many years in pre-med college, medical school, and residency, physicians focus on getting through the next hurdle. They may postpone the pleasures of life that others enjoy. Compulsive traits that allow them to postpone enjoyment may have the unwanted consequence of leading to more distant relationships., thus placing strain on intimate relationships.
A 2002 study looking at dual physician marriages found they have a relatively low divorce rate of 11%. “They’re a happily married cohort,” says Dr Wayne Sotile of the Sotile Cetner for Resilience (www.sotile.com). “They’re more compassionate about the passion for the career — they understand the calling because they share it.”
A study published in The New England Journal of Medicine in 1997 with Bruce L. Rollman as the lead researcher [2] found that physicians in some specialties — chiefly psychiatry and surgery — are at higher risk for divorce than their medical brethren in other fields. Alerting medical students to the risks of divorce in some specialties may influence their career choices and strengthen their marriages whatever field they choose.
The study suggested that the high divorce risk in some specialties may result from the inherent demands of the job as well as the emotional experiences of physicians who enter those fields. The divorce rate was 51 percent for psychiatrists, 33 percent for surgeons, 24 percent for internists, 22 percent for pediatricians and pathologists, and 31 percent for other specialties.
The overall divorce rate was 29 percent after three decades of follow-up and 32 percent after nearly four decades of follow-up. Physicians who married before medical school graduation had a higher divorce rate than those who waited until after graduation (33 percent versus 23 percent). Female physicians had a higher divorce rate (37 percent) than their male colleagues (28 percent).
***
***
References:
Miller, M. N., McGowen, R., 2000, “The painful truth: Physicians are not invincible,” Southern Medical Journal, 93: 966-973.
Rollman BL, Mead LA, Wan NY, Klag MJ. Medical specialty and the incidence of divorce. N Engl J Med. 1997;336:800–3
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Doctors and dentists earn money by treating patients. CPAs and Attorneys have clients, and retail stores buy items low and sell them at higher prices. This is called a business model.
More formally, a business model identifies the products or services the business plans to sell, the target market, and any anticipated expenses, in order to outline how to generate a profit. Business models are important for both new and established businesses. They help companies attract investment, recruit talent, and motivate management and staff.
Businesses should regularly update their business model, or they’ll fail to anticipate trends and challenges ahead. Business models also help investors to evaluate companies that interest them and employees to understand the future of a company they may aspire to join.
***
The Business Model of Pharmacy Benefits Managers
In the United States, health insurance providers often hire a third party to handle price negotiations, insurance claims, and distribution of prescription drugs. Providers that use such pharmacy benefit managers include commercial health plans, self-insured employer plans, Medicare Part D [drug] plans, the Federal Employees Health Benefits Program, and state government employee plans. PBMs are designed to aggregate the collective buying power of en-rollees through their client health plans, enabling plan sponsors and individuals to obtain lower prices for their prescription drugs. PBMs negotiate price discounts from retail pharmacies, rebates from pharmaceutical manufacturers, and mail-service pharmacies which home-deliver prescriptions without consulting face-to-face with a pharmacist.
Pharmacy benefit management companies can make revenue in several ways.
First, they collect administrative and service fees from the original insurance plan.
Then, they can also collect rebates from the manufacturer.
Traditional PBMs do not disclose the negotiated net price of the prescription drugs, allowing them to resell drugs at a public list price (also known as a sticker price), which is higher than the net price they negotiate with the manufacturer. This practice is known as “spread pricing”. The industry argues that savings are trade secrets. Pharmacies and insurance companies are often prohibited by PBMs from discussing costs and reimbursements. This leads to lack of transparency.
***
***
Therefore, states are often unaware of how much money they lose due to spread pricing, and the extent to which drug rebates are passed on to en-rollees of Medicare plans. In response, states like Ohio, West Virginia, and Louisiana have taken action to regulate PBMs within their Medicaid programs.
For instance, they have created new contracts that require all discounts and rebates to be reported to the states. In return, Medicaid pays PBMs a flat administrative fee.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on July 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
US measles cases have reached a 33-year high. A little more than halfway into 2025, the US has reported 1,288 measles cases, marking the highest yearly total since 1992, according to data from the Centers for Disease Control and Prevention.
VC powerhouse and diehard Tolkien fan Peter Thiel revealed he’s taken a 9% stake in bitcoin miner BitMine Immersion Technologies. Shares popped 12.11%, while fellow miners that have also recently invested in ether soared in tandem: SharpLinkGaming added 29.03%, and BitDigital gained 19.45%.
In fact, most crypto stocks had a good day thanks to renewed optimism that Crypto Week isn’t over in Congress. MicroStrategy climbed 3.07% and MARAHoldings jumped 3.62%.
Johnson & Johnson rose 6.19% after the consumer goods giant reported impressive earnings last quarter and raised its forward guidance.
BrightHouseFinancial popped 6.23% on reports that the insurer may be bought by private equity firm Aquarian Holdings.
Tesla gained 3.50% after the EV maker revealed the new six-seat Model Y it will begin selling in China this fall.
What’s down
ASML dropped 8.33% after the chipmaker warned that growth might be completely flat next year.
Ford fell 2.85% on the news that the automaker is recalling nearly 700,000 crossover SUVs due to fuel leaks.
GrabAGun Digital Holdings, the online gun seller backed by Donald Trump, Jr., made its market debut today. Investor reception was scathing, and the stock slid 24.19%.
Though Medicaid cuts in the Trump administration’s budget bill shocked hospitals, providers may start singing its praises after learning they’re due for a pay bump next year. On Monday, the Centers for Medicare and Medicaid Services (CMS) shared its proposed 2026 physician fee schedule, which determines Medicare payments based on the amount of resources in provider services like office visits, hospice, diagnostic testing, ambulance care, and more.
According to Leslie Kernisan MD MPH, these are the basic self-care tasks that we initially learn as very young children. They are sometimes referred to as “Basic Activities of Daily Living” (BADLs). They include:
Walking, or otherwise getting around the home or outside. The technical term for this is “ambulating.”
Feeding, as in being able to get food from a plate into one’s mouth.
Dressing and grooming, as in selecting clothes, putting them on, and adequately managing one’s personal appearance.
Toileting, which means getting to and from the toilet, using it appropriately, and cleaning oneself.
Bathing, which means washing one’s face and body in the bath or shower.
Transferring, which means being able to move from one body position to another. This includes being able to move from a bed to a chair, or into a wheelchair. This can also include the ability to stand up from a bed or chair in order to grasp a walker or other assistive device.
***
***
If a person is not fully independent with ADLs, then we usually include some information about the amount of assistance they require. ADLs were originally defined in the 1950s by a geriatrician named Sidney Katz, who was trying to define what it might look like for a person to recover to independence after a disabling event such as a stroke or hip fracture. So these measures are sometimes called the “Katz Index of Independence in Activities of Daily Living.”
Posted on July 6, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants LLC
***
***
On June 9th, 2025, Oregon’s governor signed into law the country’s strictest corporate practice of medicine (CPOM) prohibition. Senate Bill (SB) 951 will severely curtail the involvement of private equity firms and other corporations in the state’s medical practices.
This Health Capital Topics reviews the bill and discusses the implications on the healthcare industry. (Read more…)
When you visit health clinic or hospital for a medical appointment, you’ll be seen by a doctor, healthcare provider and/or medical prescriber. But what do these words really mean?
***
***
Doctors / Physicians
Doctor of Medicine (MD), Doctor of Podiatric Medicine (DPM), Doctor of Osteopathy (DO, or Doctor of Dental Surgery (DDS/DMD). Doctors, also known as physicians, have extensive prescription privileges across various specialties. They can diagnose medical conditions, prescribe medication, and oversee the overall management of patient care. Doctors include general practitioners, specialists such as cardiologists or dermatologists, and surgeons. Their prescription authority encompasses a wide range of medications to address acute and chronic health conditions, ranging from antibiotics to specialized treatments for complex diseases.
A medical provider is a general term that encompasses a wide range of education levels, skill-sets, and specializations. A provider could be a Physician Assistant (PA), Nurse Practitioner (NP), Clinical Nurse Specialist (CNS), Doctor of Medicine (MD), Doctor of Podiatric Medicine (DPM), Dentist (DDSDMD) or Doctor of Osteopathy (DO).
***
Medical Drug Prescribers
Generally, psychologists and therapists do not have prescription privileges. They focus on psychotherapy and counseling rather than medication management. However, some jurisdictions may grant limited prescription rights to psychologists who undergo additional training and certification. Like psychologists, therapists typically do not have prescription privileges. They focus on providing counseling and psychotherapy to address mental health issues and emotional concerns.
Psychiatrists are medical doctors (MD/DO) who specialize in the diagnosis and treatment of mental health disorders. They have full prescription privileges and can prescribe a wide range of medications to manage psychiatric conditions.
In most cases, physical therapistsdo not have the authority to prescribe medication. They primarily focus on rehabilitation and physical interventions to improve mobility and function.
Nurse practitioners are advanced practice nurses with the authority to diagnose, treat, and prescribe medication independently in many states and countries. They undergo extensive education and training, which allows them to provide a wide range of healthcare services, including medication management.
Similar to nurse practitioners, psychiatric nurse practitioners have the authority to prescribe medication for mental health conditions. They specialize in psychiatric and mental health care, offering comprehensive treatment that may include medication management.
Chiropractors primarily focus on diagnosing and treating musculoskeletal disorders through manual adjustments and therapies. They do not have surgical or prescription privileges in most jurisdictions.
Optometrists are trained to diagnose and treat vision problems, including prescribing corrective lenses and medications for certain eye conditions such as infections or inflammation.
Registered nursestypically do not have prescription privileges. They work under the direction of physicians and nurse practitioners, assisting with patient care but not prescribing medication themselves.
Dentists have limited prescription privileges related to dental care, such as antibiotics or pain medications for dental procedures. However, they do not have the authority to prescribe general medications outside of their scope of practice.
Nutritionists typically do not have prescription privileges. They specialize in providing dietary advice and counseling to promote health and well-being through nutrition but do not prescribe medication.
Depending on their scope of practice and legal regulations in their jurisdiction, nurse midwives may have limited prescription privileges for certain medications related to prenatal care, childbirth, and postpartum care.
Posted on May 16, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Oak Street Health, headquartered in Chicago and a wholly-owned subsidiary of CVS Health since 2023, has agreed to pay $60 million to resolve allegations that it violated the False Claims Act by paying kickbacks to third-party insurance agents in exchange for recruiting seniors to Oak Street Health’s primary care clinics.
The Anti-Kickback Statute prohibits anyone from offering or paying, directly or indirectly, any remuneration — which includes money or any other thing of value — to induce referrals of patients or to provide recommendations of items or services covered by Medicare, Medicaid and other federally funded programs. Under the Medicare Advantage (MA) Program, also known as Part C, Medicare beneficiaries have the option to obtain their health care through privately-operated insurance plans known as MA plans. Some MA Plans contract with health care providers, including Oak Street Health, to provide their plan members with primary care services.
The United States alleged that, in 2020, Oak Street Health developed a program to increase patient membership called the Client Awareness Program. Under the Program, third-party insurance agents contacted seniors eligible for or enrolled in Medicare Advantage and delivered marketing messages designed to generate interest in Oak Street Health. Agents then referred interested seniors to an Oak Street Health employee via a three-way phone call, otherwise known as a “warm transfer,” and/or an electronic submission.
In exchange, Oak Street Health paid agents typically $200 per beneficiary referred or recommended. These payments incentivized agents to base their referrals and recommendations on the financial motivations of Oak Street Health rather than the best interests of seniors. The settlement resolves allegations that, from September 2020 through December 2022, Oak Street Health knowingly submitted, and caused the submission of, false claims to Medicare arising from kickbacks to agents that violated the Anti-Kickback Statute.
Posted on May 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Classic Definition: In our hemisphere, there is the mystery of the Cuban health care paradox.
Modern Circumstance: This small island country whose economy produces about $6,000 in goods and services per person annually, a mere fraction of U.S. economic activity, lacks access to many commonly used drugs. Specialty medical care is scarce, and obesity rates are high and growing.
Paradox Example: Yet Cuba paradoxically boasts a life expectancy that surpasses the U.S. by six months. So, could this finding be explained by their diet, too, one that is rich in fresh produce, but low in saturated fats?
Question: Or, might it be related to their accessibility to primary care services and high compliance rates of childhood vaccination?
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Virtual chronic care provider Omada Health has filed to go public in the United States, the latest in a string of healthcare listings expected this year. Omada did not disclose the details as to how much it plans to raise from its IPO.
The San Francisco, California-based company, which last raised $192 million in a Series E funding round in 2022, reported a 38% increase in revenue to $169.8 million for 2024, according to its IPO paperwork. For the first quarter of 2025, the company posted a 56.6% year-on-year jump in revenue to $55 million. Omada has applied to list its common stock on the NASDAQ under the symbol “OMDA”.
Healthcare IPOs on U.S. exchanges have fetched $7.1 billion in 2024, compared with $2.8 billion a year earlier, according to data compiled by LSEG.
Posted on May 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITION
By Staff Reporters
***
***
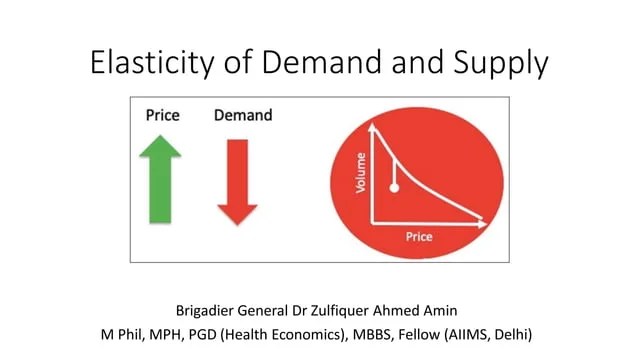
Classic: Despite a wide variety of empirical methods and data sources, the demand for health care is consistently found to be price inelastic
Modern: If you are sick, you will not be very price sensitive. There are exceptions to this rule (e.g., elective surgery such as plastic surgery, purchases of eyeglasses) but most studies find that patients are fairly insensitive to changes in health care prices.
Examples: For instance, the RAND Health Insurance Experiment found that the price elasticity of medical expenditures is -0.2.
***
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
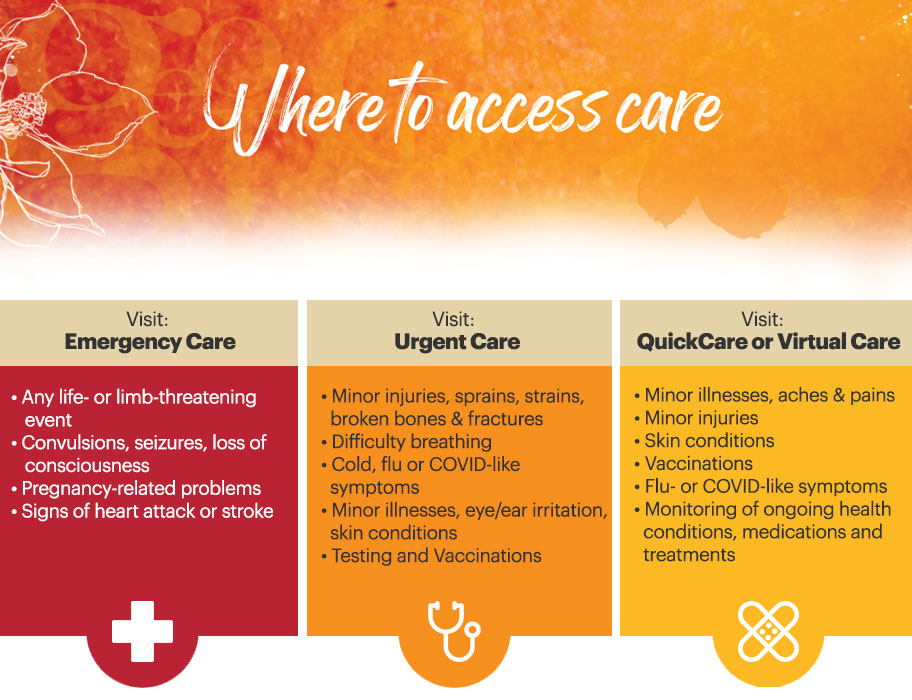
An emergency medicine physician is a medical doctor who specializes in the diagnosis, treatment, and management of acute and life-threatening medical conditions that require immediate intervention. These physicians work in hospital emergency departments, urgent care centers, and other acute care settings, where they provide rapid assessment, stabilization, and treatment to patients of all ages with a wide range of medical emergencies.
Emergency medicine physicians are trained to handle diverse medical emergencies, including trauma, cardiac emergencies, respiratory distress, severe infections, neurological emergencies, and obstetric emergencies, among others. They play a vital role in the front line management of medical emergencies, ensuring that patients receive prompt and appropriate care to improve outcomes and save lives.
***
Classic: Emergent Room or Emergency Department care is the provision of immediate medical service offering outpatient care for the treatment of acute and chronic illness and injury. It requires a broad and comprehensive fund of knowledge to provide such care. Excellence in care for patients with complex and or unusual conditions is founded on the close communication and collaboration between the urgent care medicine physician, the specialists and the primary physicians.
Modern: Urgent care does not replace your primary care physician. An urgent care center is a convenient option when someone’s regular physician is on vacation or unable to offer a timely appointment. Or, when illness strikes outside of regular office hours, urgent care offers an alternative to waiting for hours in a hospital Emergency Room.
Examples: Chest pain, bleeding that cannot be stopped and loss of consciousness; etc.
***
***
SOME ER DOCTORS WORK FOR FREE
The new president of emergency medicine for the Alberta Medical Association says Emergency Room physicians already coping with long hours, staff shortages and jammed waiting rooms are also being obligated, in some cases, to work for free. Dr. Warren Thirsk says the government has yet to follow through on a promise to reimburse emergency room doctors for so-called “good faith” payments.
“There’s been lots of excuses, but the bottom line is no one has actually received a penny for those suspended good-faith payments,” Thirsk said in an interview. “On average, every emergency physician in this province is out thousands of dollars for free work.” Good-faith payments reimburse ER doctors when they see patients who don’t have identification and can’t prove an Alberta Health Care Insurance Plan billing number.
Thirsk said the United Conservative government stopped those payments when it ripped up the master agreement with the AMA in early 2020. He said it promised to bring back those payments when the two sides agreed to a new deal in September 2022. But to date that hasn’t happened, he said.
“I’m legally and morally bound to look after you [if] you’re unidentified [as a patient],” said Thirsk, an emergency room doctor at Edmonton’s Royal Alexandra Hospital.
“I’m going to look after you because it’s the right thing to do no matter what the problem is.”
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Some retired people live on a fixed income and many of them live right on the edge of their financial capability. At some time in their life, they may have to make a choice regarding many purchases.
In this case, we will illustrate “choice” using a couple’s purchase of Long-Term-Care Insurance [LTCI]. Of course, economics is the study of choice; wants, needs and scarcity, etc. In our case, if they decide to make the purchase they commit to a lifetime of premium payments. The financial tradeoff is this; if they make the commitment to purchase LTCI, they must give up something else.
EXAMPLE: In order to maintain a monthly premium of $100 ($1,200per year), an elderly patient, retired layman or couple must essentially relegate about $30,000 of financial assets to generate the $100 necessary to make an average premium payment (assumes a 7% rate of return with 4% withdrawal rate) or [4% X $30,000 = $1,200 year]. Thus, if the monthly premium cost is $500 per month, the elder must give up the use of $150,000 of retirement asset just to generate enough cash flow to pay for the LTC insurance.
***
***
The married elder couple has to make the Hobson’s Choice decision among lifestyle (dinners, vacations, gifts to children, prescription drugs, medical care or food and shelter) versus paying an insurance premium to provide for nursing home coverage for a need, which may be very real, but will not occur until sometime in the ambiguous future.
And so, when faced with such a tough economics Hobson’s Medicine Choice, neither of which delivers peace of mind or a respectable solution; many will simply decide that, in either case, they may already end up impoverished. Thus, many will often opt for the better lifestyle now … while they can enjoy it … together.
Cite: Anonymous Health Insurance Agent, Norcross, Georgia
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals.
Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed.
Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Posted on May 1, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants LLC
***
***
While the healthcare industry has been dealing with high employee turnover since the start of the COVID-19 pandemic, that turnover was largely among clinical staff.
However, a recent survey found that significant healthcare leadership turnover may also be on the horizon. AMN Healthcare subsidiary B.E. Smith found that nearly half of healthcare executives plan to leave their organization in the next year.
This Health Capital Topics article reviews the survey and the reasons behind the intended exits. (Read more…)
Posted on April 30, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
FUNDAMENTAL INDUSTRY CHANGES
By Staff Reporters
***
***
Index Funds
An index mutual fund or ETF (exchange-traded fund) tracks the performance of a specific market benchmark—or “index,” like the popular S&P 500 Index—as closely as possible. That’s why you may hear people refer to indexing as a “passive” investment strategy.
Instead of hand-selecting which stocks or bonds the fund will hold, the fund’s manager buys all (or a representative sample) of the stocks or bonds in the index it tracks.
***
Quantum Computing
Unlike traditional computers that use bits, quantum computers utilize qubits. These qubits are capable of being in a state of superposition, where they can represent both 0 and 1 simultaneously, enabling the processing of multiple calculations at once. This could allow quantum computers to outperform classical computers in solving certain complex problems. However, the field is still overcoming challenges such as qubit stability and decoherence; especially in these three areas:
Quantum computing could fundamentally alter healthcare by accelerating drug discovery and improving individualized medicine. Rapid analysis of enormous volumes of biological data allows quantum computers to find trends that might guide the creation of more potent treatments. In addition to accelerating drug development, this will enable customized treatments tailored to unique genetic profiles.
Faster and more accurate financial models produced by quantum computing will transform the banking sector. Through real-time analysis of intricate financial systems, it can help investors to control risk and make better decisions. More precise market forecasts will help maximize portfolio management and trading strategies.
Through greatly enhanced medical diagnosis and patient care, quantum computing can transform the healthcare industry. Quantum computers can remarkably accurately find trends and possible health hazards by analyzing enormous volumes of medical data in a fraction of the time. Early diagnosis and more customized treatment alternatives follow from this.
B–QTUM Index Fund
Index Description: The BlueStar® Machine Learning and Quantum Computing Index (BQTUM) tracks liquid companies in the global quantum computing and machine learning industries, including products and services related to quantum computing or machine learning, such as the development or use of quantum computers or computing chips, superconducting materials, applications built on quantum computers, embedded artificial intelligence chips, or software specializing in the perception, collection, visualization, or management of big data.
In a discussion of competitive healthcare economic models, assumptions must include normal demand quantities, many fully informed patients and the fact that physicians cannot directly influence demand for medical care. These assumptions, although fluid, also preclude that patient buyers are large enough to have any influence over price and result in the following”:
In a “pure monopoly”, there is only one provider with a unique service. The doctor is a “price maker” and charges whatever s/he wishes.
In an “oligopoly”, there are a few physicians who provide similar services. For example, when it becomes clear to Dr. Smith and Dr. Jones that neither can win their price war, oli-gopolists return prices to prior, but still inflated levels!
In “monopolistic competition”, there are many providers with differentiated services. For example, should Dr. Jones decide to have evening hours, she may charge a premium for her fees if Dr. Jones doe not follow suit.
Finally, when “pure competition” occurs, there are many physicians, providing providing similar and substitutable services. Marketing and advertising does not affect fees, and prices are determined by supply and demand. The doctors become “price takers” by accepting fees arrived at by practicing competitively.
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals.
Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed.
Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Classic: An arrangement by which a patient requests that their health benefit payments be made directly to a designated person or facility, such as a physician or hospital. It is a legally binding agreement between patient and Insurance company asking them to send your reimbursement checks directly to your doctor.
Modern: To accept assignment means that the provider agrees to accept what ever the insurance company allows or approves as payment in full for the claim. The patient signs paperwork requiring his health insurance provider to pay his physician or hospital directly. EXAMPLES:
CMS: The approved amount, also known as the Medicare-approved amount, is the fee that Medicare sets as how much a provider or supplier should be paid for a particular service or item. Original Medicare calls this “assignment.”
Tardiness: When a medical office accepts an assignment of benefits, the insured patients may have to wait several months for their insurance reimbursement to arrive.
Posted on April 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
WARNING – WARNING
By Dr. DavidEdwardMarcinko; MBA MEd
***
***
According to www.NPR.org, there are more than120,000 health care forums on the Internet with opinions ranging from pharmaceuticals, to sexual dysfunction, to acne. The same goes for commercial doctor blogs that promote lotions, balms and potions, diets and vitamins, minerals, herbs, drinks and elixirs, or various other ingest-ants, digest-ants or pharmaceuticals, etc.
And, to other doctors, the blogging craze is a new novelty where there are no rules, protocols, standards or precise figures on how many “medical-doctor” or related physician-blogs are “out there.” Unfortunately, too many recount gory ER scenes, or pictorially illustrate horrific medical conditions, or serious and traumatic injuries. Of course, others simply are medical practice websites, or those that entice patients into more lucrative plastic surgery or concierge medical practices. Some are from self-serving/credible plaintiff-seeking attorneys wishing to assist patients.
Not all physician blogs are geared toward practice information, marketing or medical sensationalism. In fact, just the opposite seems to be the case in extremely candid blogs, like “Ranting Docs”, “White Coat Rants,” “Grunt Docs”, “Cancer Doc,” “The Happy Hospitalist,” “Mom MD”, “Cross-Over Health”, “Angry Docs” and “M.D.O.D.,” which bills itself as “Random Thoughts from a Few Cantankerous American Physicians.”
According to some of these, they are more like personal journals, or public diaries, where doctors vent about reimbursement rates, difficult cases, medical mistakes, declining medical prestige and control, and/or what a “bummer” it is to have so many patients die; not pay, or who are indigent, noncompliant. We call these the “disgruntled doctor sites.” Some even talk about their own patients, coding issues, or various doctor-patient shenanigans.
But, according to psychiatrist and blogger Dr. Deborah Peel and others, the problem with blogging about patients is the danger that one will be able to identify themselves – the doctor – or that others who know them will be able to identify them.” Her affiliation, Patient Privacy Rights, rightly worries that patients might track back to the individual, and adversely affect their employment, health insurance or other aspects of life.
***
***
And, according to Dr. Jay S. Grife; MA Esq., it is certainly true that if a doctor violates a patient’s privacy there could be legal consequences. Under HIPAA, physicians could face fines or even jail time. In some states, patients can file a civil lawsuit if they believe a doctor has violated their privacy. Still, internet privacy issues are an evolving gray-area that if not wrong, may still be morally and ethically questionable [personal communication].
Our colleague Robert Wachter MD, author of the blog called “Wachter’s World,” says it’s important for doctors to be able to share cases, as long as they change the facts substantially. On the other hand, the author of “Wachter’s World” and a leading expert on patient safety alternately suggests “You might say we as doctors should never be talking about experiences with our patients online or in books or in articles.” But, he says that “patients shouldn’t take all the information on blogs at face value. Taken for what they are — unedited opinions, and in some cases entertainment — blogs can give readers some useful insight into the good, the bad and the ugly of the medical profession”. Link: http://www.the-hospitalist.org/blogs
Well, fair enough! But, doctors unhappy with their current medical career choice, or its modern evolution, should probably consider counseling or even career change guidance, re-education and re-engineering. It is very inappropriate to vent career frustrations in a public venue. It’s far better for the blog to be private and/or by invitation only; if at all [Personal communication].
We believe that a hybrid mash-up of both views can be wholly appropriate, or grossly inappropriate in some cases. Of course the devil is in the details; linguistics and semantics aside. Nevertheless; what is not addressed in electronic physician “mea-culpas” are the professional liability risks and concerns that are evolving in this quasi-professional, quasi-lay, communication forum.
***
***
Example: We have seen medical mistakes, and liability admissions of all sorts, freely and glibly presented. In fact,
“Some physicians find that the act of liability blogging as a professional confession that is useful in moving past their malpractice mistakes. And, it is also a useful way to begin a commitment to a better professional life of caring in the future. It helps eliminate the toxic residue and angst of professional liability and guilt. Moreover, as they are unburdened of past acts of omission or commission, doctors should remember to also forgive those who have wronged them. This helps greatly with the process and brings additional peace.”
However, although some may say that this electronic confession is good for the soul, it may not be good for your professional liability carrier, or you, when plaintiff’s attorneys release a legion of IT focused interns, or automated bots, searching online for your self-admissions and scouring for your self-incriminations. Of course, a direct connection to a specific patient may still not be made and no HIPAA violation is involved. But, a vivid imagination is not need needed to envision this type of blind medical malpractice discovery deposition query even now.
QUESTION:“Doctor Smith, I noted all the medical errors admitted on your blog. What other mistakes did you make in the care and treatment of my client?”
And so, the question of plausible deniability, or culpability, is easily raised. If you must journalize your thoughts for sanity or stress release; do it in print. And, don’t tell anyone about it so the diary won’t be subpoenaed. Then tear it up and throw it away. Remember, with risk management, “It is all about credibility.” Don’t trash yours! These thoughts may be especially important if you covet a medical career as a researcher, editor, educator, medical expert or something other than a working-class or employed physician.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on March 25, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
US stocks closed near session highs on Monday as investors welcomed reports that the next wave of President Trump’s tariffs will be narrower than expected.
The S&P 500 (^GSPC) rose almost 1.8% on the heels of the broad benchmark snapping a four-week losing streak. The Dow Jones Industrial Average (^DJI) advanced 1.4%, while contracts on the tech-heavy NASDAQ Composite (^IXIC) led the gains, up 2.3%.
A hostile takeover happens when an entity takes control of a company without the knowledge and against the wishes of the company’s management. A hostile takeover is an acquisition strategy requiring that the entity acquire and control more than 50% of the voting shares issued by the company.
In mergers and acquisitions (M&A), a hostile takeover is the acquisition of a target company by an acquiring company that goes directly to the target company’s shareholders, either by making a tender offer or through a proxy vote.
Ideally, an entity interested in acquiring a company should seek approval from the target company’s Board of Directors. The difference between a hostile and a friendly takeover is that, in a friendly takeover, the target company’s board of directors approve of the transaction and recommend shareholders vote in favor of the deal.
Defenses against a hostile takeover
These defense mechanisms can be preemptive or reactive, depending on how prepared the company is for the possibility of a hostile bid.
Poison pill is one of the most common defenses against a hostile takeover. Officially known as a “shareholder rights plan,” the poison pill allows existing shareholders to purchase additional shares at a discount, diluting the ownership interest of the acquiring company. The goal is to make it prohibitively expensive for the acquirer to complete the takeover.
A golden parachute is another defense strategy, which involves providing lucrative compensation packages (bonuses, severance pay, stock options, etc.) to key executives in the event they are terminated as a result of the takeover. This creates a financial disincentive for the acquiring company, as it would need to pay out these large sums upon completing the takeover.
In a Crown jewel defense, the target company sells or threatens to sell its most valuable assets—its “crown jewels”—if the takeover is completed. This reduces the attractiveness of the company to the acquirer, as the most desirable assets would no longer be part of the deal.
The Pac-Man defenses a more aggressive strategy in which the target company turns the tables by attempting to buy shares of the acquiring company, effectively launching a counter-takeover. While rare, this defense can deter hostile bids by making the takeover battle more costly and complex.
A White-Knight defense involves the target company seeking out a more favorable acquirer, or “white knight,” to make a friendly takeover bid. This allows the target company to avoid the hostile acquirer while still securing the benefits of a merger or acquisition.
The hostile takeover between Sanofi-Aventis and Genzyme Corp. occurred in 2010 when Sanofi, a French pharmaceutical company, wanted to buy Genzyme, a US biotech firm specializing in rare diseases. Genzyme resisted the offer, leading to conflict. Sanofi started a public campaign to pressure Genzyme’s shareholders into selling.
After months of negotiations, the two companies reached a deal in 2011. Sanofi agreed to pay $74 per share, with additional payments tied to Genzyme’s future performance, bringing the total deal value to around $20.1 billion. This acquisition allowed Sanofi to expand into the lucrative market for rare disease treatment.
Posted on March 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
While some medical practitioners and facilities can operate without Professional Liability Insurance coverage, one business related insurance that cannot / should not be avoided is Worker’s Compensation. Employers in all but seven states – so-called “monopolistic” states because they have their own state funds, are under statutory obligation to provide coverage for their employees. Historically, Worker’s Compensation pre-dates Social Security entitlements and well before the emergence of employer sponsored group benefits.
The coverage under worker’s compensation provides for lost income due to on-the-job accidents or work-related disability or death and the amount of benefits vary by state. In some instances, the coverage will reimburse the employee for medical expenses incurred with the accident.
The four general benefits covered under Worker’s Compensation are:
Medical Care – for expenses incurred usually without limitations on amount or period of care.
Disability Income – payable for both total and partial disability and is usually based on 66 2/3 percent of their wage base.
Death Benefits – generally fall into two categories; one a flat amount for “burial” insurance; and two, survivor benefits. Though varying by state, these benefits are similar to the disability payment (a percentage of weekly base wages) but may be capped as to total benefit, such as $50,000 or a period, such as 10 years
Rehabilitation Benefits – includes not only medical rehabilitation, but vocational rehabilitation, vocational counseling, retraining or educational benefits, and job placement
Traditionally, the secondary purpose of Worker’s Compensation was to reduce potential litigation because employees accepting the benefits from a Worker’s Compensation claim generally waived their right to sue their employer.
***
***
However, in our litigious society, this “protective shelter” has been severely tested and is crumbling.
Employers may provide their Worker’s Compensation three ways:
Private commercial insurance
State government funds
Self-insurance
Very few factors drive the premium structure – the occupation of the workers is the single most important determinant of premiums. An office worker may have premiums as low as $.10 per hundred of wages and a coal miner may exceed $50.00 per hundred of wages. Generally speaking, however, Worker’s Compensation premiums for the medical profession or healthcare worker are among the lowest available.
Therefore, for the medical practice, some physicians may consider self-insurance because the weekly benefits are typically below $500, thus making this decision attractive.
Alternatively, because officers and owners can elect not to be covered by Worker’s Compensation, the decision to purchase coverage from a private insurance company may afford inexpensive assurance that the benefits will be conveniently provided, and administered, by a private insurance company for their employees.
9. We act with honesty, integrity and are always straightforward. 8. We strive to be innovative, creative, iconoclastic, and flexible. 7. We admit and learn from mistakes and don’t repeat them. 6. We work hard always as competitors are trying to catch up. 5. We treat others with dignity and respect. 4. We are the onus of consulting advice for the well being of others. 3. We fight complacency as former success is in the past. 2. The best management styles are timeless, not timely. 1. Our clients are colleagues and always come first.
SPEAKING: Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements.
***
***
CONTACT: Ann Miller RN MHA at: MarcinkoAdvisors@outlook.com
Health actuaries analyze potential risks, profits and trends that will affect their employers, which are often in the health insurance, government health services and medical provider industries. They advise companies on issuing policies to consumers based on risks, calculated premiums and upcoming changes in health-care costs.
It’s common for an actuary to have a bachelor’s degree or higher in actuary studies, mathematics or statistics. Coursework on medical terminology and hierarchy of the medical field is also beneficial. In addition to academic education, certification is also necessary to reach “professional status,” which is required by most employers.
***
***
The professional organization, Society of Actuaries, certifies actuaries in the health and medical field. Their statistical work is commonly done with predictive tables, probability tables and life tables that are created on customized statistical analysis software such as Stata or XLSTAT.
The actuary field as a whole is growing faster than other fields, according to the Bureau of Labor Statistics [BLS]. In 2020, it expanded by 27 percent. The average annual salary for an actuary in 2010 was $87,650. More specifically, in the health insurance field, the salary was slightly higher at $91,000.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
RISK MANAGEMENT, LIABILITY INSURANCE AND ASSET PROTECTION ABBREVIATIONS
[Glossary of Important Acronyms]
Much has been written and much has been opined on the topic of medical risk management, insurance, asset protection and professional liability for physicians and healthcare providers in this textbook; and elsewhere.
But occasionally, we all still get lost in a wide array of abbreviations, acronyms, and initialisms that are constantly changing in this ecosystem.
And so, this glossary serves as a ready reference for those who want to know about these medical risk management definitions in a quick and ready fashion.
Acronyms and Abbreviations
AAASC American Association of Ambulatory Surgery Centers
AAHP American Association of Health Plans
ABN advance beneficiary notice
ABQAUR American Board of Quality Assurance and Utilization Review
ACE acute care episode
ACHCE American College of Health Care Executives
ACS American College of Surgeons
ADA Americans with Disabilities Act
ADC average daily census
ADL activities of daily living
ADT Admission/Discharge/Transfer
AHA American Hospital Association
AHIMA American Health Information Management Association
AHRQ Agency for Healthcare Research and Quality
AI average inventory
AIMR Association for Investment Management and Research
AIR assumed interest rate
ALE annualized loss expectancy
ALF assisted living facility
ALOS average length of stay
AMA American Medical Association
AMBAC AMBAC Indemnity Corporation
AMGA American Medical Group Association
ANSI American National Standards Institute
AP accounts payable
APA American Psychiatric Association
APC ambulatory payment classification
APG ambulatory payment group
APR annual percentage rate
AR accounts receivable
ASA American Society of Appraisers
ASC ambulatory surgery centers; also Accredited Standards Committee
ASHA American Surgical Hospital Association
ASO administrative services only
ASTC ancillary service technical component
ATM asynchronous transfer mode
AVG ambulatory visit group
BANTA best alternative to negotiated agreement
BBA Balanced Budget Act of 1997
BBRA Balanced Budget Refinement Act [1999]
BCP business continuity planning
BEA break-even analysis
BEP break-even point
BIPA Benefits Improvement and Protection Act [2000]
BLS Bureau of Labor Statistics
BPD border protection device
BS balance sheet
BSA Bank Secrecy Act
BVS business valuation standard
CA certificate authority
CAC Carrier Advisory Committee
CAS cost accounting standards
CASB Cost Accounting Standards Board
CC common criteria [for IT Security Evaluation —ISO/IEC 15408]; complication or comorbidity [for MS-DRGs]
CCA certified cost accountant
CCC cash conversion cycle
CCEVS common criteria evaluation and validation scheme
CCHIT Certification Commission for Healthcare Information Technology
CCU critical care unit
CDC Centers for Disease Control and Prevention
CDH consumer-directed healthcare
CDHP consumer-directed healthcare plan
CDPM Clinical Data Project Manager
CDSS clinical decision support system
CEO Chief Executive Officer
CF conversion factor
CFA Chartered Financial Analyst
CFO Chief Financial Officer
CFR Code of Federal Regulations
CHAMP Children’s Health and Medicare Protection Act of 2007
CHAMPUS Civilian Health and Medical Program of the Uniformed Services
CHE Certified Healthcare Executive
CHIPS Center for Healthcare Industry Performance Studies
CIA Corporate Integrity Agreement
CIO Chief Information Officer
CIP Customer Identification Program
CIS computer information systems
CLIA Clinical Laboratory Improvement Act
CLT capitation liability theory
CME continuing medical education
CMI case mix index
CMIO Chief Medical Information Officer
CMIS contribution margin income statement
CMN Certificate of Medical Necessity
CMP Certified Medical Planner ™
CMS Centers for Medicare and Medicaid Services [formerly HCFA]
COD cash on delivery
COGME Council of Graduate Medical Education
COH cash on hand
COLA cost of living allowance
CON Certificate of Need
COO Chief Operating Officer
COSO Committee of Sponsoring Organizations
COTS commercial off-the-shelf
CPHQ Certified Physician in Healthcare Quality
CPIM Certificate in Production and Inventory Management
CPI-U Consumer Price Index—urban
CPM critical (clinical) path method
CPOE computerized physician order entry [system]
CPR computer-based patient record
CPT current procedural terminology
CQI continuous quality improvement
CRL Certification Revocation List
CRM customer relationship management
CRVS California Relative Value Studies
CSO Chief Security Officer
CT scan computed tomography scan [also called CAT scan]
CUSIP Committee on Uniform Security Identification Procedures
Candid CIO: Will Weider, CIO of Ministry Health Care and Affinity Health System, offers his perspectives on administration issues in this blog.
Christina’s Considerations: Christina Thielst is a hospital and healthcare administrator and entrepreneur with a deep desire for continually improving the health of the community being served. This is her blog.
Healing Hospitals — Formerly Ask a Hospital President: F. Nicholas “Nick” Jacobs has more than 20 years experience in hospital management, with an acknowledged reputation for innovation and consumer-centered leadership.
Hospital Impact: Part of the Fierce network of health sites, this site is becoming popular among healthcare administrators for its news updates, tips and opinions on health care matters.
Leading the Way to Medical Excellence: the president of McLeod Health non-profit institutions provides weekly insights into his facilities and health care in general.
Let’s Talk Health Care: Bruce Bullen, Interim Chief Executive Officer at Harvard Pilgrim in Massachusetts, provides and open and ongoing conversation about health care administration.
Life as a Healthcare CIO: Dr. John Halamka records his experiences with infrastructure, applications, policies, management, and governance as he supports 3,000 doctors, 18,000 faculty and about three million patients.
Managed Care Matters: Joe Paduda shares his knowledge on managed care for group health, health policy, health research, and medical news for insurers, employers, and healthcare providers.
More than Medicine: Tom Quinn, president and CEO of Community General Hospital in Syracuse, New York, began his career as a hospital kitchen worker. His perspective on administration reflects his knowledge on how hospitals work from every angle.
Running a Hospital: A CEO of a large Boston hospital shares thoughts on hospitals, medicine and health care issues.
St. Joseph Medical Center: Chief Executive Officer at St. Joseph Medical Center in Missouri, Mr. Kashman, provides personal insight into administrative matters and general topics.
Todd’s Perspective: Todd Linden, president and CEO of Grinnell Regional Medical Center, offers insights into medical administration and guest bloggers provide insight into various departments.
Wachter’s World: This blog focuses on hospitals, hospitalists, quality, safety, policy and much more from Robert M. Wachter, MD, Professor and Associate Chairman of the Department of Medicine at the University of California, San Francisco.
Legal Matters
Drug and Device Law: This blog contains an attorney’s personal views (and those of several other Dechert attorneys) on topics that arise in the defense of pharmaceutical and medical device product liability litigation.
Drug Injury Watch: Learn more about drug injury lawsuits from an attorney who represents patients and their families.
FDA Law Blog: Hyman, Phelps & McNamara, P.C. is the largest dedicated food and drug law firm in the country. Their knowledge about laws and regulations governing drugs, medical devices, foods, dietary supplements, and cosmetics is helpful to anyone interested in these topics.
Health Care Law Blog: Bob Coffield’s expertise lies in helping businesses and health care providers weave through a variety of state and federal health care regulations and assisting them in business transactions.
Health Plan Law: This site contains information about group health plans, claims administration and related ERISA fiduciary issues. This site also contains tutorials.
HealthBlawg: this is David Harlow’s popular health care law blog, offering expert insights and easy-to-understand analysis.
Healthcare Law Blog: Holland & Hart’s healthcare practice provides insight into this arena, including HIPAA, Stark law, the Anti-kickback Statute and more.
HIPAA Blog: Join in on this discussion of medical privacy issues often buried in “political arcana.”
HIPAA, HiTech & HIT: This updated blog brings insight into legal issues, developments and other pertinent information that relates to the creation, use and exchange of electronic health records.
HIT Blawg: This blog is focused on national health information technology legal trends and current news on this topic.
Home Care Law Blog: Learn more about legal and policy issues in the home health care, private duty and hospice industries from Gilliland & Markette LLP.
Med Law Blog: This law blog focuses on topics that range from compliance to contracts and from employee benefits to HIPAA and HIT.
Physician Law: This blog provides and easy way to stay on top of current news, updates and useful tips relating to legal issues that affect physicians and non-institutional providers.
eHealth and Health IT
Chilmark Research: This blog provides perspectives on key IT trends in the healthcare sector.
davidrothman.net: David is the Information Services Specialist at the Community General Hospital Medical Library, but he also provides great ideas for 2.0 tools and tips for healthcare industry professionals on this blog.
e-CareManagement blog: Vince Kuraitis, owner of Better Health Technologies, LLC, has a passion for disease management and care coordination that dates back to 1995.
e-HealthExpert: A non-profit organization provides a free and open forum to support the development of expertise in the field of eHealth, Healthcare Information Systems, and Health IT (Clinical IT).
eHealth: John Sharp is an IT Manager for a major medical center in Northeast Ohio, with a focus on ehealth, personal health records, Web 2.0 technologies, Windows Sharepoint Services and project management.
Found In Cache: If you would prefer a professional’s take on social media matters, Web sites and all things technological, then follow Ed Bennett, a technology expert for a Maryland medical care system.
Future Health IT: A health IT and EPR advocate from the UK provides a format to discuss the future of health care and IT.
Informaticopia: This UK blogger provides eclectic news and views on health informatics and elearning.
MedGadget: Stay ahead of the gadget curve with this site, which offers information about the newest health care gadgets on the market as well as emerging medical technologies.
Neil Versel’s Healthcare IT Blog: A healthcare journalist’s provides his views on the major segment of the industry he covers — and, he provides a ton of links to other sites as well.
Schwartz Healthcare IT Blog: A variety of authors from Schwartz Communications provide insights into ways to use IT effectively within healthcare facilities.
The Health IT Channel: For a different perspective on IT and EHR as well as other health care issues, watch a few videos at this site.
The Healthcare IT Guy: The CEO of Netspective, a Java/.NET consultancy that specializes in healthcare IT with an emphasis on e-health, EMRs, data integration, and legacy modernization, supplies tips and information for physicians and healthcare administration.
ACKNOWLEDGEMENTS: To Mackenzie H. Marcinko PhD of iMBA Inc., Perry D’Alessio CPA CMP™ [Hon] New York, NY; and Daniel B. Moisand CFP®, Principal for Moisand Fitzgerald Tamayo, Melbourne, FL.
A common stock is the least senior of securities issued by a company. A preferred stock, in contrast, is slightly more senior to common stock, since dividends owed to the preferred stockholders should be paid before distributions are made to common stockholders.
However, distributions to preferred stockholders are limited to the level outlined in the preferred stock agreement (i.e., the stated dividend payments). Like a fixed income security, preferred stocks have a specific periodic payment that is either a fixed dollar amount or an amount adjusted based upon short-term market interest rates. However, unlike fixed income securities, preferred stocks typically do not have a specific maturity date and preferred stock dividend payments are made from the corporation’s after tax income rather than its pre-tax income. Likewise, dividends paid to preferred stockholders are considered income distributions to the company’s equity owners rather than creditors, so the issuing corporation does not have the same requirement to make dividend distributions to preferred stockholders.
Preferred Stock
Thus, preferred stock is generally referred to as a “hybrid” security, since it has elements similar to both fixed income securities (i.e., a stated periodic payments) and equity securities (i.e., shareholders are considered owners of the issuing company rather than creditors).
Hybrid Securities
Convertible preferred stocks (and convertible corporate bonds) are also considered hybrid securities since they have both equity and fixed income characteristics. A convertible security whether a preferred stock or a corporate bond, generally includes a provision that allow the security to be exchanged for a given number of common stock shares in the issuing corporation. The holder of a convertible security essentially owns both the preferred stock (or the corporate bond) and an option to exchange the preferred stock (or corporate bond) for shares of common stock in the company.
Thus, at times the convertible security may behave more like the issuing company’s common stock than it does the issuing company’s preferred stock (or corporate bonds), depending upon how close the common stock’s market price is to the designated conversion price of the convertible security.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements:
Posted on February 26, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
In great news for investors, a new study found that major healthcare companies have paid out $2.6 trillion to shareholders over the past 20 years in the form of dividends and share buybacks, and those payments are increasing. Bad news for patients: Some of that money could’ve been spent on, well, healthcare. The study, published Februrary 10th in JAMA, found that publicly traded S&P 500 healthcare companies paid shareholders a total of $170.2 billion in 2022, up 315% from payouts of just $54 billion in 2001.
The S&P 500 fell 0.5%. The NASDAQ 100 slid 1.2%. A gauge of the “Magnificent Seven” mega-caps sank 2.2%. Nvidia Corp.’s shares slid 2.8% on the eve of the company’s results, while Tesla slumped 8.4% to fall below $1 trillion in market value. The DJIA was up.
Posted on February 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
ORIGINAL: May 2021 | Matt Cohlmia
As the future of healthcare becomes digitized, the threat of disruption to health systems has never been greater. Despite their best intentions, the flood of new competitors and ever-proliferating modalities of care each compete for patient attention, creating the potential for a fragmented, confusing, and impersonal patient experience. At the same time, health systems possess the breadth of care, the access to data, and the patient trust to become their community’s preferred partner in care.
But to achieve success, they must leverage these resources to create easy to navigate and personalized experiences for their patients, and for the first time ever, those are within reach.
Posted on February 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
A Doctor of Physical Therapy (DPT) helps people improve their mobility and physical functioning, manage pain, and prevent disability. After earning an undergraduate degree, a person can enroll in a DPT program, which is typically three years. The curriculum includes courses in biology, anatomy, physiology, kinesiology (movement), neurology, cardiopulmonary (heart and lung) rehabilitation, behavioral sciences, and pharmacology.
Clinical rotations are a major component of DPT education. They may perform clinical rotations in various settings including a PT clinic, hospital, nursing care facility, rehabilitation clinic, and school. At the end of their coursework and clinical rotation, a student earns a DPT degree but still must pass a state licensure exam to practice as a physical therapist.2
On average, a DPT in the U.S. makes $105,710 per year, according to 2024 statistics.
While a DPT may use the title “Dr,” they are different from an MD/DO/DPM/DDS. A DPT cannot write prescriptions or perform surgery. A DPT is also different from a PhD (Doctor of Philosophy). DPT is treatment-focused, whereas the PhD is research-focused.
Posted on February 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
PharmD – Doctor of Pharmacy
A Doctor of Pharmacy [ParrmD] is the professional degree required to become a pharmacist in the US. Practicing pharmacists complete an average of six years in school—including their pre-pharmacy education—before passing required exams and completing post-graduate training.
Here’s where things often get confusing. The word “pharmacist” is sometimes used in casual conversation to refer to healthcare professionals who aren’t technically licensed to be pharmacists.
For example, pharmacy technicians assist licensed pharmacists. They work behind the counter among the medications right alongside the pharmacist. However, they don’t need a Doctor of Pharmacy to do their job. A pharmaceutical sales representative typically needs four years of a bachelor’s degree with a foundation in chemistry and biology, though this is not always a requirement. Neither of these professionals is technically a pharmacist, although laypeople may mistakenly describe them that way.
And pursuing a PharmD doesn’t always mean you’ll work in a community pharmacy. In fact, just slightly fewer than half of all PharmD recipients end up in this role. Another 15 percent practice in other healthcare settings—hospitals, nursing homes, and managed care centers, for example. Other pharmacy students pursue research roles, government regulation positions, or work in highly specialized areas like oncology or geriatric pharmacy.
A PharmD or RPH [registered pharmacist] fills the electronic or written prescriptions of a MD/DO/DPM/DDS/DMD. They generally can not prescribe drugs or write prescriptions, however.
As of February 01, 2025, the average annual pay of Doctor of Pharmacy in the United States was $196,904. While Salary.com suggests that a Doctor of Pharmacy salary in the US can go up to $236,908 or down to $149,197, most earn between $171,932 and $217,844.
Posted on February 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Blue Cross Blue Shield will soon begin paying out $2.67 billion to customers follow a years-long lawsuit alleging that the health insurance giant broke antitrust laws. The litigation began in 2013, when a class-action lawsuit was filed against more than 35 Blue Cross Blue Shield health insurance plans. The lawsuit claims the company broke antitrust laws by limiting market competition, resulting in increased premiums and reduced options for customers.
US stocks closed mixed on Tuesday as investors assessed more tariff policy shifts from President Donald Trump and looked ahead to upcoming inflation data.
Traders also digested the start of Federal Chair Jerome Powell’s two-day testimony in Congress. In his opening remarks, Powell told lawmakers the Fed is not in a rush to adjust interest rates and reiterated the central bank’s stance of not commenting on trade policy.
The Dow Jones Industrial Average (^DJI) edged around 0.3% higher, while the benchmark S&P 500 (^GSPC) closed just above the flatline. The tech-heavy NASDAQ Composite (^IXIC) pulled back about 0.4%.
A century ago, one fifth of the country was involved in agriculture. Due to the transformation of farming technology, only 1% of the country is now involved in farming, while our supermarkets are flooded with cheap food. I could be wrong, but I don’t see the 19% of the country who used to farm wandering around unemployed. They have retrained to do other things.
Innovation disrupts, but it also creates new jobs and improves the standard of living of society. A century ago, you could not have imagined most of the jobs we have today. I’m not just talking about social media celebrities; think about software engineers, data scientists, cybersecurity experts, etc. In fact, most white-collar jobs you see today did not exist 100 years ago. Yes, if you specialized in driving horse-powered carriages, you had to acquire new skills.
AI will displace many jobs, but it will also empower people with new productivity tools. Microsoft Excel replaced jobs that required people to add up rows of numbers with calculators, but it created many more. In the 1960s, corporations had departments filled with typists. A photocopier and then the personal computer put these hardworking folks out of a job, but they retrained to do other things.
If we have a victim mentality, AI will run us over; if we embrace it and adapt it to our lives, it may become our best friend to do the jobs we are doing, while our soon-to-be-unemployed coworkers complain about AI.
AI may have a similar impact on our lives as electricity did. Unless it becomes sentient and just like the Terminator, it turns against us (smarter people than me cannot agree on this, especially on a reasonable time frame, so I withhold my opinion on it), it will likely improve our lives significantly. One industry that immediately comes to mind is healthcare – we need major disruption in that sector.
AI may disrupt and completely reshuffle the power dynamics in some industries. Travel, for example, comes to mind; we may start looking for trips and booking tickets with the help of our AI assistant without going to the travel websites. Some companies will adapt and become winners, while others won’t and will become market-share donors.
As I am typing this, I realize (again, something I do daily now) how important management is. In our analysis, we should pay close attention to how companies are embracing AI. Are they giving it lip service or are they really adopting it and changing the business to take advantage of it?
ChatGPT is a statistical representation of things found on the web, which will increasingly include ITS OWN output (directly and secondhand). You post something picked up from it and it will use it to reinforce its own knowledge. Progressively a self-licking lollipop.
If you want to see ChatGPT creating art, for the fun of it, spend some time on myfavoriteclassical.com, where I post music articles. Every single picture there is created by AI. I love impressionist artists, and thus I love these little AI creations. However, if you zoom in closer, you’ll find violinists playing with toothpicks, pianists with three hands and cellists with multiple arms and legs.
This self-licking lollipop is impressive, but it still has a lot to learn. (By the way, if you have not signed up to receive my classical music-only articles, you have an opportunity to do it here).
Finally, the more we rely on AI and the more content it creates, the less creative it and we become.
Posted on February 6, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
One year after forming an alliance with pharmacy schools, Walgreens says it has taken steps to get more people interested in the profession and improve working conditions at the chain.
Walgreens announced the Deans Advisory Council last February, framing it as a collaboration with pharmacy schools to boost the number of students enrolling and address some of the broader issues in the industry, like burnout and declining reimbursements from pharmacy benefit managers.
US stocks recovered from losses on Wednesday to close higher on the day. Earnings from Alphabet (GOOG, GOOGL) and AMD (AMD) fell short, but Big Tech got a boost from a jump in Nvidia (NVDA) shares.
The tech-heavy NASDAQ Composite (^IXIC) rose 0.2%, while the benchmark S&P 500 (^GSPC) added 0.4%. The Dow Jones Industrial Average (^DJI) led the gains, rising 0.7%, or more than 300 points.
Posted on February 1, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
US stocks lost ground on Friday after the White House said tariffs against Mexico, Canada, and China will take effect on Saturday, reigniting fears of a coming trade war with the nation’s closest trading partners. White House Press Secretary Karoline Leavitt said the president would impose 25% tariffs on goods from Mexico and Canada, as well as a 10% tariff on goods from China.
All three major gauges fell into the red Friday. The S&P 500 (^GSPC) lost 0.5% at the closing bell, while the Dow Jones Industrial Average (^DJI) shed 0.8%. The tech-heavy NASDAQ Composite (^IXIC) gave up 0.3%, reversing earlier gains.
The dramatic tariff news pushed aside more optimistic updates from earlier in the day, which had buoyed stocks. Solid earnings from Apple (AAPL) and an inflation reading that matched expectations lifted market sentiment for much of the day.
Finally, the S&P and the Nasdaq posted losses for the week of 1% and 1.6%, respectively. The Dow, meanwhile, recorded a weekly gain of 0.3%.
Posted on January 31, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
In the first days of his second (nonconsecutive) presidential term, Donald Trump and his administration took a number of actions that will affect the healthcare industry in the near- and long-term. Further, the Trump Administration is reportedly poised to take a number of additional actions to pause, end, or otherwise change Biden-era initiatives.
Meanwhile, President Trump’s cabinet pick for the Department of Health & Human Services (HHS) hangs in the balance. This Health Capital Topics article reviews the new administration’s actions impacting the healthcare industry as of the date of publication. (Read more...)
Posted on January 27, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITIONS
By Staff Reporters
***
***
Registered Nurse [RN]
RNs must complete an accredited Associate Degree in Nursing (ADN) or Bachelor of Science in Nursing (BSN) program (or, in rare cases, diploma programs). After that, they become eligible to sit the NCLEX-RN exam and apply for registered nurse licensure in their state.
As a registered nurse, duties include basic patient care but expand to more technical responsibilities like medication administration, performing diagnostic tests, and operating medical equipment. Depending on the role, one may also supervise other healthcare workers like LPNs, certified nursing assistants (CNAs), or even other RNs.
Licensed Practical Nurses [LPN]
LPNs may also be called licensed vocational nurses (LVNs), and like registered nurses, LPNs must also complete an education program before becoming eligible for licensure. LPN programs typically take around one year, and you can find them at community colleges or vocational schools.
Prospective LPNs must then take and pass the NCLEX-PN exam to become licensed. As an LPN, focus is on patient care tasks like monitoring vitals and changing bandages as part of a care team supervised by a physician or RN.
Posted on January 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Stocks ended firmly higher on Tuesday, with the S&P 500 rising 0.88% and reclaiming the 6,000 point mark amid a pullback in Treasury yields and optimism over Donald Trump’s focus on deregulation, focused tariff strategies and the prospect of solid corporate earnings into the fourth quarter reporting season.
Tech stocks are likely to pace early gains in the Wednesday session, however, following the unveiling of a new AI joint venture called ‘Stargate’ that will include an initial $100 billion investment from SoftBank, Oracle Corp. (ORCL) and OpenAI.
Executive Order 14009, titled “Strengthening Medicaid and the Affordable Care Act,” includes several key components designed to increase access to affordable health care and reduce the number of uninsured Americans:
Reversal of Trump administration policies: The order sought to undo measures that limited ACA provisions or made healthcare less accessible.
Longer enrollment periods: The order encouraged states to lengthen enrollment periods and provided additional federal support. As a result, many states extended their enrollment windows to ensure broader access to affordable healthcare.
Restoration of pre-existing condition protections: Reaffirmed protections for individuals with pre-existing conditions and reinforced nondiscrimination policies in healthcare.
Immediate review of agency actions: The order directed various executive departments and agencies to review existing regulations, orders, and policies to ensure they align with the goal of strengthening Medicaid and the ACA.
xecutive Order 14070, titled “Continuing To Strengthen Americans’ Access to Affordable, Quality Health Coverage,” aimed to maintain and enhance Medicaid and the ACA. Key components included:
Enhanced marketplace subsidies: The order highlights the positive impact of the American Rescue Plan Act on access to coverage, including enhanced marketplace subsidies.
Extended postpartum Medicaid coverage: It provides options for states to extend postpartum Medicaid coverage.
New incentives for Medicaid expansion: The order includes new incentives for states to expand their Medicaid programs.
MBBS Degree [Bachelor of Medicine, Bachelor of Surgery]
The MBBS is usually a five-year undergraduate degree that medical students complete when they want to become doctors. However, some programs take six years to complete because the institution expects you to earn a Bachelor of Science (BSc) in your training.
By the time a student applies to a medical program, they have likely taken several foundational science courses as part of their high school (or secondary) education. For example, medical applicants in the United Kingdom are often expected to show high scores on their General Certificate of Secondary Education (GCSE) and A-levels.
Earning an MBBS means that students are certified to care for patients as junior physicians without specialized training. Graduates are expected to complete two years of additional training, which rotates them through different specialties. Once they identify a specialty they like, they can apply for additional training, which can take anywhere between three and eight years.
MD Degree [Doctor of Medicine]
The acronym “MD” stands for the Latin term “Medicinae Doctor,” which translates to “Doctor of Medicine” in English.
It refers to the title that students from the United States of America obtain after finishing medical school. Some countries consider the “MD” title a postgraduate doctoral degree that MBBS graduates can obtain with additional years of training.
Posted on January 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The FTC’s second interim staff report on consolidated pharmacy benefit managers (PBMs) found that the three largest of these middlemen—CVS Health’s Caremark Rx, Cigna Group’s Express Scripts, and UnitedHealth Group’s OptumRx—”marked up two specialty generic cancer drugs by thousands of percent and then paid their affiliated pharmacies hundreds of millions of dollars of dispensing revenue in excess of estimated acquisition costs for each drug annually.”
The S&P 500 fell 0.2%. The NASDAQ 100 lost 0.7%. The Dow Jones Industrial Average slid 0.2%. A gauge of the “Magnificent Seven” megacaps slipped 1.9%. The Russell 2000 added 0.2%. The KBW Bank Index declined 0.2%.
The yield on 10-year Treasuries declined four basis points to 4.61%. The Bloomberg Dollar Spot Index rose 0.1%.
Posted on January 16, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The U.S. Department of Labor reported a 0.4% increase in the monthly CPI after seasonal adjustment, overshooting the forecast of 0.3% and the previous value of 0.3%. On an annual basis, inflation climbed to 2.9%, up from 2.7% in November, the highest rate since July 2024.
US stocks ripped higher on Wednesday as high hopes for bank earnings paid off and a crucial consumer inflation update showed key prices increased less than expected in December.
The benchmark S&P 500 (^GSPC) popped more than 1.8%, while the Dow Jones Industrial Average (^DJI) rose more than 1.6%, or over 700 points. Meanwhile, the tech-heavy NASDAQ Composite (^IXIC) soared 2.5%.
Stocks took a leg higher after the Consumer Price Index (CPI) showed progress toward the Fed’s 2% inflation target in December. Prices climbed 0.2% month-on-month on a “core” basis, which strips out the more volatile costs of food and gas, an easing from November’s 0.3% gain. Over last year, core CPI rose 3.2%.
Capital One is being sued by the US government’s consumer watchdog agency for “cheating millions of consumers” and not paying more than $2 billion in interest to holders of its high-interest savings accounts.
As of January 1st 2025, beneficiaries enrolled in Part D prescription drug plans will have their out-of-pocket spending capped at $2,000 for the year. This new policy was part of President Joe Biden’s 2022 Inflation Reduction Act (IRA), which included other drug pricing measures such as capping the cost of insulin at $35 per month for seniors.
But only a small share of Medicare enrollees will benefit from the cap, according to an analysis from nonprofit organization AARP’s Public Policy Institute, as most don’t spend more than $2,000 annually on their medications after hitting their deductible (which is up to $590 for standard plans in 2025). Beneficiaries spent an average of $400 to $500 per year as of 2022, the Hill reported, citing data from the US Department of Health and Human Services (HHS).
Posted on January 7, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
US stocks largely rose on Monday as chip names popped and investors awaited the release of key monthly jobs data later this week.
The S&P 500 (^GSPC) was up about 0.5%, while the Dow Jones Industrial Average (^DJI) fell about 0.1% after being higher for most of the session. The tech-heavy NASDAQ Composite (^IXIC) led the gains, adding about 1.2%, after a tech-led rally on Friday.
Posted on January 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Anthem Blue Cross and Scripps Health will part ways impacting thousands of patients.
Scripps Health and Anthem Blue Cross officially just parted ways on January 1st, 2025, leaving about 125,000 patients uncertain of what their healthcare and insurance will look like in 2025.
Posted on December 28, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
US stocks closed the holiday week on a downbeat note as Wall Street slogged to the finish of a largely triumphant year.
The S&P 500 (^GSPC) lost 1.1%, while the tech-heavy NASDAQ Composite (^IXIC) shed 1.5% Friday at the close. The Dow Jones Industrial Average (^DJI) gave up 0.8%. Meanwhile, the 10-year Treasury yield (^TNX) hovered near seven-month highs around 4.6%.
After stacking impressive gains this year, some of the biggest names in tech lost ground as investors took profits, rebalance portfolios, or reassessed their lofty valuations. Tesla (TSLA) lost 5%. Nvidia (NVDA) gave up c2%, while Amazon (AMZN) decreased by 1%.
Wall Street has just three trading days remaining in a 2024 full of big gains, but markets have been unable to mount a “Santa Claus” rally into the end of the year.
Posted on December 27, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Absent Congressional action, beginning January 1sy, 2025, the statutory limitations that were in place for Medicare telehealth services prior to the COVID-19 PHE will retake effect for most telehealth services.
This means most telehealth visits will not be covered by Medicare in 2025, unless Congress acts by the end of December 2024.
***
(Reuters) -The Dow Jones Industrial Average closed fractionally higher on Thursday, stretching its winning streak to five sessions despite light trading volumes and rising U.S. Treasury yields weighing on some of the dominant technology megacaps.
While the NASDAQ Composite and the S&P 500 were broadly unchanged, the indexes both finished slightly in negative territory. This snapped the NASDAQ’s four-session run of higher closes, and ended the S&P 500’s own run at three sessions.
On a day of few catalysts, investors responded to yields on U.S. government bonds inching higher, including the yield on the benchmark 10-year Treasury note hitting its highest since early May at 4.64% earlier in the session. And, a strong auction of seven-year notes early in the afternoon though helped yields come off slightly, with the 10-year note at 4.58% in late-afternoon trade.
Higher yields are traditionally seen as negative for growth stocks, as it raises the cost of their borrowing to fund expansion. With markets increasingly dominated by the megacap technology stocks known as the Magnificent Seven, crimping their performance – especially in lieu of other market catalysts – will put downward pressure on benchmark indexes.
The S&P 500 slipped 2.45 points, or 0.04%, to 6,037.59 points, while the NASDAQ Composite lost 10.77 points, or 0.05%, to 20,020.36. The Dow Jones Industrial Average rose 28.77 points, or 0.07%, to 43,325.80.
Six of the megacaps fell, with Tesla leading decliners with a 1.8% fall. The outlier was Apple, rising 0.3% and continuing to edge closer to becoming the first company in the world to hit a market value of $4 trillion.
Posted on December 18, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Stat: 97%. That’s how many healthcare leaders think A.I. will become important in healthcare over the next five years.
***
Pharmacy benefit managers (PBMs) are once again under pressure from federal leaders. A group of Democratic and Republican congresspeople proposed legislation that would attempt to prevent pharmacies from also owning PBMs. The three largest PBMs—CVS Health’s Caremark, Cigna’s Express Scripts, and UnitedHealth Group’s Optum Rx—currently operate pharmacies and administer more than 80% of the prescriptions in the US, and officials have linked this practice to drug price increases.
US stocks fell across the board on Tuesday, with the Dow logging its biggest losing streak in 46 years. The Dow Jones Industrial Average (^DJI) finished the session down roughly 0.6%, registering its ninth straight day of losses. The last 9-day losing streak for the Dow was Feb. 1978. Prior to that, the index suffered an 11-day losing streak in 1974 and another in 1971.
The other major indexes dropped in tandem on Tuesday, with the benchmark S&P 500 (^GSPC) falling around 0.4% and the NASDAQ Composite (^IXIC) losing about 0.3% after the tech-heavy index closed at a record high on Monday.