BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on May 17, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
America’s oldest popular stock index, the Dow Jones Industrial Average, hit a brief record high yesterday morning when it traded above 40,000, reflecting renewed hope for the market’s health after Wednesday’s promising inflation report.
The S&P 500® index (SPX) fell 11.05 points (0.2%) to 5,297.10; the Dow Jones Industrial Average declined 38.62 points (0.1%) to 39,869.38; the NASDAQ Composite® ($COMP) shed 44.07 points (0.3%) to 16,698.32.
The 10-year Treasury note yield (TNX) rose more than 2 basis points to 4.381%.
The CBOE Volatility Index® (VIX) dropped 0.03 to 12.42.
Walmart’s strength fueled a strong day for consumer staples shares. The S&P 500 Consumer Staples ($SP500#30), which includes Walmart as well as companies like Coca-Cola (KO) and Procter & Gamble (PG), surged 1.5% to its highest level in over two years.
Among other companies, Applied Materials (AMAT) fell 1.6% ahead of the semiconductor industry supplier’s quarterly earnings report, which is expected after Thursday’s close.
And, Core CPI, which tracks the price of goods and services excluding volatile food and energy prices and is closely watched as an inflation indicator, rose 3.6% from the same period last year. That’s the smallest annual increase since April 2021. On a monthly basis, core CPI rose 0.3%, marking the first time in six months that its growth slowed from the prior month. Other good signs include:
Grocery prices dropped 0.2% from March, the first decrease in a year.
Health insurance and car insurance increased more slowly in April than in March.
A separate report released yesterday showed consumer spending stayed steady last month.
Finally, Joe Manchin (D-W.Va.) and a group of Republican senators are moving to overturn a retirement investment planning rule that was finalized by the Labor Department last month. The Labor Department unveiled the new rule last month that would update the definition of an investment advice fiduciary under the Employee Retirement Income Security Act. Manchin and 15 Republican senators joined in co-sponsoring a Congressional Review Act (CRA) resolution that would overturn this new rule.
Posted on May 16, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
More people are interested in determining their “heart age” using new tests and tech tools, but some skeptics say it’s not a healthy data point to focus on. (the Wall Street Journal)
The Cathie Wood-led Ark Invest just made some significant trades. The most prominent among them were the increased stakes in Palantir Technologies Inc (NYSE:PLTR) and the reduced holdings in Coinbase Global Inc (NASDAQ: COIN).
Here’s where the major benchmarks ended:
The S&P 500 index rose 61.47 points (1.2%) to 5,308.15; the Dow Jones Industrial Average added 349.89 points (0.9%) to 39,908.00; the NASDAQ Composite rallied 231.21 points (1.4%) to 16,742.39.
The 10-year Treasury note yield fell almost 10 basis points to 4.348%.
The CBOE Volatility Index® (VIX) dropped 0.97 to 12.45.
Chipmaker shares led the way higher Wednesday, lifting the Philadelphia Semiconductor Index (SOX) almost 3% to a 10-week high. Interest-rate-sensitive sectors like real estate and utilities were also strong. The small-cap Russell 2000® Index (RUT) advanced 1.1% to a seven-week high. The U.S. Dollar Index ($DXY) slumped to its weakest level in five weeks, reflecting expectations for lower interest rates that may reduce the appeal of U.S. fixed income assets.
Among companies, Cisco Systems (CSC) surged 1.5% ahead of its quarterly results expected after Wednesday’s close. Dow member Walmart (WMT) is expected to release results Thursday morning as the unofficial retail earnings season accelerates.
And … The U.S. Department of Justice (DOJ) announced it has established a new task force to take on healthcare monopolies and collusion. The task force, made up of prosecutors, economists, healthcare industry experts and others, will guide the division’s enforcement strategy and policy approach in healthcare, including by facilitating policy advocacy, investigations and, where warranted, civil and criminal enforcement in healthcare markets.
CUSTOMIZABLE CMS & AGENCY FOR HEALTHCARE RESEARCH AND QUALITY STYLED PROTOCOLS, CHECKLISTS AND TEMPLATES
.… Specifically for Podiatrists ….
e-Podiatry Consent Forms™ is an innovative new suite of software programs from the Institute of Medical Business Advisors [iMBA, Inc]. Our products solve your informed consent problems and enhance the education, discussion and documentation of the informed consent process for all podiatrists performing foot, ankle and leg reconstructive surgical procedures.
THE PROBLEM
All podiatrists are being pressured by the Centers for Medicare and Medicaid Services [CMS], the Joint Commission on Accreditation of Healthcare Organizations [JCAHO], liability carriers and private insurance payers to make their consent process more patient-friendly, informed and easily understood. And, the pressure to standardize and comply is great.
Most recently, based on the need to make healthcare even safer, the Agency for Healthcare Research and Quality (AHRQ) undertook a major study to identify patient safety issues and develop recommendations for “best practices”.
The AHRQ Evidence Report
The AHRQ report identified the challenge of addressing shortcomings such as missed, incomplete or not fully comprehended informed consent, as a significant patient safety issue and opportunity for improvement.
The authors of the AHRQ report hypothesized that better informed patients:
“are less likely to experience errors by acting as another layer of protection.”
And, the AHRQ study ranked a “more interactive informed consent process” among the top 11 practices supporting more widespread implementation; especially for surgical consent forms.
One answer to the modern risk-management problem of “informed consent interactivity” may be e-Podiatry Consent Forms™ We license two core interactive surgical products, and a reference library, with related concepts and products in development:
Forefoot, Mid-Foot and Simple Rear-Foot Version
Complex Rear-Foot, Ankle and Lower Leg Version
Comprehensive content library for extreme customization.
Each e-Podiatry Consent Forms™ CD-ROM [secure email delivery is now available] is increasingly trusted as the simple solution to standardized communications across the entire office-enterprise; from managing-risk, informing-patients and complying with modern regulatory requirements through enhanced patient-centric informed consent encounters.
Thus, by improving the consistency, details, documentation and effectiveness of the informed consent process, e-Podiatry Consent Forms™ equips all podiatric surgeons with the tools needed to augment quality standards, reduce litigation potential and improve patient outcomes and safety.
Today’s electronic media makes physician-patient communication possible; yet there is another kind of intimacy. ICTs—information and communication technologies—enable 24/7 monitoring of basic information such as blood pressure, glucose levels, pulse, and respiration, etc.
Example:
In one study, an ICT not only made it easier for patients to stay in touch with their doctors, the outcomes were also significantly better.[i] Today, Hippocrates is no longer trailing patients around the house to keep track of their snacks and moods. But Hippocrates has gone digital in the form of a wearable device that records subtle changes in biological markers and communicates them instantaneously to a health provider.
While this is obviously a great advance, we suggest you pause for a moment before plugging in.
Why?
ICTs and social media tools can make a difference to one of the most important dimensions—physiological outcomes. But you can have the latest interactive technology at your disposal and still fail to be connected.
Example:
A story that a friend told me shows how.
***
One morning, her elderly father was touching up the paint on his sailboat. Nearby, another boat-owner, who happened to be an emergency medical technician, noticed her father was struggling to breathe and that his lips had turned purple. A trip to the local community hospital led to a barrage of high-tech tests and procedures, a diagnosis of emphysema, later complications with cerebral hematomas, and hospitalizations and re-hospitalizations that brought him into contact with a neurologist, a neurosurgeon, a cardiologist, and a pulmonologist.
Throughout her father’s medical ordeal, the team of specialists stayed in touch with each other and the primary care physician via various electronic media. But one person remained out of the loop—her father. One day, six months into the experience, the primary care physician phoned our friend’s mother to check on his patient. Her father recalls thinking, “Why was he calling her?”
The physician was communicating, but he was emotionally disconnected.
***
The Moral
The moral of the story: communication needs to be patient-centered in both electronic and psychological terms. That means understanding how someone likes to communicate and making sure the medium fits the message. Electronic media are just part of the equation. The other is the doctor-patient relationship. Once a relationship is established, it may be fine to use e-mail to send information about dosage.
But, delivering a new diagnosis may require the extra effort of scheduling a phone call or a face-to-face visit. Today, since you have so many Health 2.0 choices, it takes some effort to select the right way to communicate in a particular situation.
Use the Right Relationship Strategy
A colleague recently shared another story about an encounter with a specialist.
Example:
***
After an examination for a minor ailment, he was told that there might be a medicated lotion that could ameliorate his condition. The doctor thought for a moment, then swiveled around to the computer on his desk. As our colleague watched the screen, his physician typed a few words into a search engine. Up popped a list and he wrote out a script. “Try this,” his doctor concluded. “I think it will help.”
It did, almost overnight.
***
The Moral
Even though his physical problem had disappeared completely, our colleague felt there was something missing in the interaction. “It bothered me that my doctor turned to the Web for help at that moment. He found a cure, but I felt he wasn’t paying attention to me.”
The physician is supposed to be an authority who has a special relationship to the patient. “Anybody can Google,” our colleague complained. Was he being unreasonable? Maybe.
But; this story tells us something important about technology—it cuts both ways.
***
***
Assessment
Everyone has their own preferences when it comes to how they want to interact with each other and with technology. If these preferences are explicit and aligned, the chances for a productive partnership are high. The preferences, however, are many and complex. You can easily get lost in the tangled thicket of interpersonal styles and virtual mediums.
In the Web 2.0 environment, it helps to narrow down the endless choices to just a few options.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on May 15, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The S&P 500® index (SPX) rose 25.26 points (0.5%) to 5,246.68, the highest since a record close March 28; the Dow Jones Industrial Average® ($DJI) gained 126.60 points (0.3%) to 39,558.11; the NASDAQ Composite climbed 122.94 points (0.8%) to 16,511.18.
The 10-year Treasury note yield (TNX) fell more than 3 basis points to 4.449%.
The CBOE Volatility Index® (VIX) decreased 0.18 to 13.42.
Among companies, Home Depot’s (HD) quarterly results reported earlier Tuesday kicked off the unofficial start of the retail earnings season. The home improvement retailer’s earnings topped expectations, but revenue missed forecasts, initially sending the company’s shares down sharply.
Home Depot also reaffirmed its full-year guidance for a 1% decline in comparable-store sales and a 1% increase in total sales. The company’s shares bounced back to end with a 0.1% loss.
And, the Cathie Wood-led Ark Invest just made some significant trades. The most prominent among them were the increased stakes in Palantir Technologies Inc (NYSE PLTR) and the reduced holdings in Coinbase Global Inc (NASDAQ: COIN).
Moreover, the website-building platform Squarespace is to go private, which it announced it’ll be doing in an all-cash deal with Permira, a private equity firm. Squarespace, which was public for nearly three years, joins a group of other smaller tech companies like Qualtrics that have recently pulled themselves off the public market. (CNBC)
Employers and private insurers are paying hospitals more for inpatient and outpatient services than in previous years, a study from RAND Corporation finds. The American Hospital Association dismissed the report saying it offers a “skewed and incomplete picture.”
And finally … Kaiser Permanente began its 2024 earnings season with more than $2.7 billion in net income and $935 million in operating income, just months after sharing plans to lay off workers.
Posted on May 14, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The S&P 500® index (SPX) fell 1.26 points (0.02%) to 5,221.42; the Dow Jones Industrial Average lost 81.33 points (0.2%) to 39,431.51; the NASDAQ Composite® ($COMP) gained 47.37 points (0.3%) to 16,388.24.
The 10-year Treasury note yield (TNX) dropped almost 2 basis points to 4.487%.
The CBOE Volatility Index® (VIX) surged 1.05 to 13.60.
Biotechnology and food and beverage shares were among the market’s strongest sectors Monday, while communication services stocks were among the biggest laggards. Energy shares took pressure despite a jump of 1.2% in WTI Crude Oil (/CL) futures, which ended above $79 per barrel after slumping last week to two-month lows.
Moderna is “bleeding money” as its forthcoming RSV vaccine doesn’t appear to deliver better results than other RSV shots already on the market. (Bloomberg)
***
It’s ChatGPT-4o’s time to shine. The “o” stands for omni, and it’s the latest iteration of OpenAI’s signature chatbot. According to the company, it’s much faster with enhanced “capabilities across text, vision, and audio.”
One relatively recent performance evaluation approach that was developed to help improve the relevance of comparisons is the separation of stock universes and managers by style. This classification method attempts to distinguish between stocks or manager philosophies based upon general financial characteristics of the investments.
The Managers
In very general terms, a manager is often a growth manager if the investment approach that the manager uses focuses on stocks showing growth and momentum in its earnings and price.
A value manager is generally considered to be a manager that attempts to identify under-valued securities based upon fundamental analysis of the company. A stock may be considered either “growth” or “value” based on a given set of valuation measures such as price-to-earnings, price-to-book value, and dividend yield.
The Style
The goal of style-based performance comparisons is to take some of the biases of the market environment out of the comparison, since a portfolio’s returns will ideally be evaluated versus a universe of alternatives that represent similar investment characteristics facing the same basic market environment. Thus, if the environment is one in which investors in stocks with strong past earnings and price momentum have generally performed better than those using fundamental analysis to find under-valued stocks, comparing the growth/momentum portfolio to a growth index or universe should help eliminate the bias.
Style-based universes can help the medical professional better understand the basic environment captured over a given performance time period.
However, there are significant limitations with the various approaches to constructing style-based stock and manager universes that should be understood if they are to be used in direct performance comparisons. Taking style-based stock universes separately from style-based manager universe, one of the most significant issues regarding the categorization of stocks by “growth” and “value” styles is the lack of agreement in the specification of what a growth stock is versus a value stock. With some universes divided by price-to-book value, others by price-to-earnings and/or dividend yields and some by combinations of similar variables, stocks are often classified very differently by two different stock universes. Further, stocks move across a broad spectrum as their price and fundamentals change, resulting in stocks constantly moving between growth and value categories for any given universe. If there is ambiguity in the rating of a given stock, then the difficulty is only compounded when we attempt to boil what may be complex investment processes of an investment manager or mutual fund portfolio manager to a simple classification of growth or value. A beaten down cyclical stock that no self-respecting growth/momentum manager would purchase may be classified as “growth” because it has a high price-to-earnings ratio (i.e., from low earnings) or a high price-to-book value (i.e., from asset write-offs). Value managers are not the only ones to own low valuation stocks that have improving earnings.
***
***
The second problem with style categorization is that managers are often misclassified or they purposefully “game” the categorization of their own process in order to appear more competitive. As an example, if a manager that typically looks for relatively strong earnings/price momentum is lagging in a period when “growth” managers are outperforming, the rank of the manager can be improved simply by claiming a “value” approach. Morningstar’s “style box” classification of mutual funds by size and style of the current portfolio highlight this problem for any given fund by showing how their portfolio has changed its classification annually.
Current Events
The stock market has been booming lately. Up almost 100% since March 2009, after being down almost 50%. And so, perhaps this is a good time to re-evaluate the performance of your investment portfolio[s].
Assessment
However, this leads to an interesting question for the medical professional or his/her advisor: If a manager is still using the same basic investment philosophy and disciplines, but their “style” category has changed according to the ratings service, should you fire them? If the answer is “yes”, then the burden of monitoring and the cost of manager turnover are an inevitable part of narrow style based performance comparisons.
But, if the answer is “no,” then it is easy to see the difficulty of fitting every management approach into a simple style box. The more reasonable alternative is to use style-based stock and manager universes as a tool for understanding the environment, rather than an absolute performance benchmark.
Conclusion
And so, your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Sponsors Welcomed: And, credible sponsors and like-minded advertisers are always welcomed.
Posted on May 13, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
While Buy Now-Pay Later (BNPL) reduces friction when purchasing, it’s giving some economy watchers unease. As Americans’ budgets buckle under the weight of inflation and higher interest payments, some worry BNPL is more of an invisible burden than a boon, Bloomberg reports. Beware the “phantom debt,” a Wells Fargo economist recently warned, referring to the BNPL industry’s short-term loans, which go largely unaccounted for by those tracking Americans’ debt load. That’s because, unlike credit cards and auto loan providers, Afterpay, Affirm, Klarna, and other BNPL providers don’t usually report transactions to credit scoring agencies.
The Cathie Wood-led Ark Invest just made some significant trades. The most prominent among them were the increased stakes in Palantir Technologies Inc (NYSE: PLTR) and her reduced holdings in Coinbase Global Inc (NASDAQ: COIN).
Dell has recently seen a decline in its revenue. In its most recent earnings report, it revealed that its net revenue shrunk by 11% year-over-year during its fiscal 2024 fourth quarter. For full year 2023, the company’s revenue was down by 14% to $88.4 billion. Partly that was due to a weak personal-computer market and the costs associated with more than 6,000 layoffs. But investors are excited by Dell’s growth potential for its server and computer businesses because of artificial intelligence, the Motley Fool reported.
Posted on May 12, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Fat Brands is the parent company of Fatburger, Johnny Rockets, and a few other restaurant chains. Last year, former CEO Andy Wiederhornstepped down after the Los Angeles Times reported that the federal government was investigating him for fraud. He has since stayed on as the company’s chairman, but on Friday the Justice Department charged him with perpetuating a $47 million fraud against his own shareholders.
In a recent Becker’s Health Care Newsletter, it is reported that a large multi-state hospital system is suing Multiplan for illegal price fixing and automatic significant price reductions, in particular, for out-of-network providers. The story states that Multiplan, by bombarding healthcare providers with automatic reductions in pricing, has made it impossible for providers to deliver healthcare.
National Nurses Week, which ends today on May 12th, Florence Nightingale’s birthday
Rite Aid has announced that 39 stores are set to close their doors for good, this follows the decision to declare Chapter 11 bankruptcy back in October, 2023.
The strategy? Reduce the total number of stores to 1,600 nationwide.
A hedge fund in the United States is generally a limited partnership providing a limited number of qualified investors with access to general partner investment decisions with little restriction in the type of investments or use of leverage. While the flexibility available to a hedge fund from a regulatory standpoint implies a high degree of potential risk, there is a wide range of investment philosophies, strategies, security types and objectives captured under the broad title of hedge fund.
Thus, generalizations regarding the characteristics of hedge funds are even less appropriate than with mutual funds, and evaluation of the investment characteristics and merits of a hedge fund strategy must be on a case-by-case basis. Likewise, the cost structure of a hedge fund often includes a base management fee to the general partner plus a performance-based fee or percentage of the profits, and must be evaluated on a case-by-case basis.
Several different investment vehicles operate under the oversight of varying regulatory bodies which provide access to an investment-managers’ discretionary decisions. While each approach generally represents ownership of an underlying pool of securities, there is usually a great deal of flexibility for the manager to deviate from a specific asset class or investment approach. Also, the fee structure of each vehicle can vary greatly and be quite large once distribution fees and sales charges are taken into account.
Thus, it is important for a medical professional to remember the following:
1. Evaluate the features and costs of an investment vehicle carefully;
2. Consider the cash flows and valuations of the securities that the manager or management approach will focus on as if the investments were being made directly, and above all;
3. Read the prospectus or agreement carefully before making any investment.
Posted on May 11, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd CMP
Understanding the Prisoner’s Dilemma
[From Wikipedia, the free encyclopedia]
As all economists and psychologists know, the prisoner’s dilemma is a standard example of a game analyzed in game theory that shows why two completely “rational” individuals might not cooperate, even if it appears that it is in their best interests to do so. It was originally framed by Merrill Flood and Melvin Dresher working at RAND in 1950. Albert W. Tucker formalized the game with prison sentence rewards and named it, “prisoner’s dilemma” (Poundstone, 1992), presenting it as follows:
Two members of a criminal gang are arrested and imprisoned. Each prisoner is in solitary confinement with no means of communicating with the other. The prosecutors lack sufficient evidence to convict the pair on the principal charge. They hope to get both sentenced to a year in prison on a lesser charge.
Simultaneously, the prosecutors offer each prisoner a bargain. Each prisoner is given the opportunity either to: betray the other by testifying that the other committed the crime, or to cooperate with the other by remaining silent.
The offer is:
If A and B each betray the other, each of them serves 2 years in prison
If A betrays B but B remains silent, A will be set free and B will serve 3 years in prison (and vice versa)
If A and B both remain silent, both of them will only serve 1 year in prison (on the lesser charge)
It is implied that the prisoners will have no opportunity to reward or punish their partner other than the prison sentences they get, and that their decision will not affect their reputation in the future. Because betraying a partner offers a greater reward than cooperating with him, all purely rational self-interested prisoners would betray the other, and so the only possible outcome for two purely rational prisoners is for them to betray each other.
***
***
The interesting part of this result is that pursuing individual reward logically leads both of the prisoners to betray, when they would get a better reward if they both kept silent.
In reality, humans display a systemic bias towards cooperative behavior in this and similar games, much more so than predicted by simple models of “rational” self-interested action. A model based on a different kind of rationality, where people forecast how the game would be played if they formed coalitions and then they maximize their forecasts, has been shown to make better predictions of the rate of cooperation in this and similar games given only the payoffs of the game.
An extended “iterated” version of the game also exists, where the classic game is played repeatedly between the same prisoners, and consequently, both prisoners continuously have an opportunity to penalize the other for previous decisions. If the number of times the game will be played is known to the players, then (by backward induction) two classically rational players will betray each other repeatedly, for the same reasons as the single shot variant. In an infinite or unknown length game there is no fixed optimum strategy, and Prisoner’s Dilemma tournaments have been held to compete and test algorithms.
In Health Economics
Advertising is sometimes cited as a real-example of the prisoner’s dilemma.
When cigarette advertising was legal in the United States, competing cigarette manufacturers had to decide how much money to spend on advertising. The effectiveness of Firm A’s advertising was partially determined by the advertising conducted by Firm B. Likewise, the profit derived from advertising for Firm B is affected by the advertising conducted by Firm A. If both Firm A and Firm B chose to advertise during a given period, then the advertising cancels out, receipts remain constant, and expenses increase due to the cost of advertising. Both firms would benefit from a reduction in advertising.
***
***
However, should Firm B choose not to advertise, Firm A could benefit greatly by advertising. Nevertheless, the optimal amount of advertising by one firm depends on how much advertising the other undertakes. As the best strategy is dependent on what the other firm chooses there is no dominant strategy, which makes it slightly different from a prisoner’s dilemma. The outcome is similar, though, in that both firms would be better off were they to advertise less than in the equilibrium. Sometimes cooperative behaviors do emerge in business situations.
For instance, cigarette manufacturers endorsed the making of laws banning cigarette advertising, understanding that this would reduce costs and increase profits across the industry. This analysis is likely to be pertinent in many other business situations involving advertising
Without enforceable agreements, members of a cartel are also involved in a (multi-player) prisoners’ dilemma. ‘Cooperating’ typically means keeping prices at a pre-agreed minimum level. ‘Defecting’ means selling under this minimum level, instantly taking business (and profits) from other cartel members. Anti-trust authorities want potential cartel members to mutually defect, ensuring the lowest possible prices for consumers.
The prisoner’s dilemma game can be used as a model for many real world situations involving cooperative behavior. In casual usage, the label “prisoner’s dilemma” may be applied to situations not strictly matching the formal criteria of the classic or iterative games: for instance, those in which two entities could gain important benefits from cooperating or suffer from the failure to do so, but find it merely difficult or expensive, not necessarily impossible, to coordinate their activities to achieve cooperation.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
COMMENTS APPRECIATED
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on May 11, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Novavax, the Covid vaccine-maker’s value doubled after it announced a $1.2 billion deal to develop new shots with Sanofi.
And, Mortgage rates fell for the first time since March, to just over 7%.
Here’s where the major stock market benchmarks ended:
The S&P 500 index rose 8.60 points (0.2%) to 5,222.68, up 1.9% for the week; the Dow Jones Industrial Average® ($DJI) advanced 125.08 points (0.3%) to 39,512.84, up 2.2% for the week and its eighth straight daily gain; the NASDAQ Composite® ($COMP) fell 5.40 points (0.03%) to 16,340.87, up 1.1% for the week.
The 10-year Treasury note yield (TNX) increased more than 5 basis points to 4.50%.
The CBOE Volatility Index® (VIX) fell 0.14 to 12.55.
Chip makers ranked among top gainers Friday after Taiwan Semiconductor Manufacturing (TSM) shares surged 4.5% after the company said its April revenue soared 60% behind AI-driven demand. The Philadelphia Semiconductor Index (SOX) climbed 1% and posted a 1.9% gain for the week. Consumer staples and transportation shares were also strong. Energy shares slipped behind a 1.2% drop in WTI Crude Oil (/CL) futures, though oil still ended slightly higher for the week.
National hospital operator Ascension said a “cyber security event” has disrupted some of its clinical operations, according to a news release. Ascension, a St. Louis-based nonprofit and Catholic healthcare network, announced it had detected “unusual activity” on some of its systems. In response, the company kicked off an investigation and remediation efforts—including turning to outside cybersecurity firm Mandiant for help, as well as notifying the “appropriate authorities,” per the release.
Planet Fitness to raise membership price for the first time since 1998. It’s going to take more than $10/month to join a gym once Planet Fitness raises the price of a basic membership for new members to $15 per month this summer. The $10 amount, which has held steady for 26 years, was considered a sweet spot where people were happy to sign up and wouldn’t bother to cancel once they gave up on their fitness goals. But after posting weaker-than-expected Q1 results, the gym chain decided it’s time to change, even though execs acknowledged that customers are looking to save rather than spend.
Posted on May 10, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The S&P 500 index gained 26.41 points (0.5%) to 5,214.08; the Dow Jones Industrial Average rose 331.37 points (0.9%) to 39,387.76; the NASDAQ Composite® ($COMP) advanced 43.51 points (0.3%) to 16,346.26.
The 10-year Treasury note yield (TNX) lost more than 2 basis points to 4.459%.
The CBOE Volatility Index® (VIX) fell 0.31 to 12.69.
Interest-rate-sensitive sectors, such as real estate and utilities, were among the strongest performers Thursday. Energy shares were also strong after WTI Crude Oil (/CL) futures rose for a second straight day after sinking to a two-month low earlier this week. Semiconductor shares were under pressure after disappointing revenue guidance from chip designer Arm Holdings (ARM) sent its shares down 2.3%.
The Dowjumped for the seventh straight day while the S&P 500 closed above 5,200 for the first time in a month as stocks climbed across the board, possibly a reaction to data showing that the cooling labor market could translate into a Federal Reserve interest rate cut in a few months. But, Roblox,tanked 22% yesterday after the company cut its annual bookings forecast. The rough patch suggests that the game’s pandemic-induced popularity has likely peaked.
Last year, Uber boasted its first full-year profit since going public. But yesterday, the company reported a surprise loss for the first quarter of 2024, dashing investors’ hopes for steady profits and sending its stock way down.
Meanwhile, Uber’s smaller rival Lyft appears to have its foot on the gas pedal. It posted better-than-expected quarterly results on Tuesday and saw a stock bump yesterday.
Microsoft plans to put the cash toward creating an AI data center. President Biden was on hand in Wisconsin to help announce the news—and not just to tout a big investment that’s expected to create jobs.
Although some doctors might view a budget as unnecessarily restrictive, sticking to a spending plan can be a useful tool in enhancing the wealth of a practice. And so, I will emphasize keys to smart budgeting and how to track spending and savings in these tough economic times; like today with the stock market busts, venture capitalists invading health care, corona virus the pandemic, aging baby boomer physicians and the great resignation; etc.
There is an aphorism that suggests, “Money cannot buy happiness.” Well, this may be true enough but there is also a corollary that states, “Having a little money can sure reduces the unhappiness.”
Unfortunately, today there is still more than a little financial unhappiness in all medical specialties. The challenges range from the commoditization of medicine, aging demographics, Medicare reimbursement cutbacks, ACA, and increased competition to floundering equity markets, the squeeze on credit and declines in the value of a practice. Few doctors seem immune to this “perfect storm” of economic woes. And then Covid-19, corona, and covid.
Far too many physicians are hurting and it is not limited to above-average earning professionals. However, one can strive to reduce the pain by following some basic budgeting principles. By adhering to these principles, physicians can eliminate the “too many days at the end of the month” syndrome and instead develop a foundation for building real wealth and security, even in difficult economic climates like we face today.
There are three major budget types. A flexible budget is an expenditure cap that adjusts for changes in the volume of expense items. A fixed budget does not. Advancing to the next level of rigor, a zero-based budget starts with essential expenses and adds items until the money is gone. Regardless of type, budgets can be extremely effective if one uses them at home or the office in order to spot money troubles before they develop.
For the purpose of wealth building, doctors may think of this budget as a quantitative expression of an action plan. It is an integral part of the overall cost-control process for the individual, his or her family unit or one’s medical practice.1
How To Prepare A Personal Cash Flow Budget
Preparing a net income statement (lifestyle cash flow budget) is often difficult because many doctors perceive it as punitive. Most doctors do not live a disciplined spending lifestyle and they view a budget as a compromise to it. However, a cash flow budget is designed to provide comfort when there is surplus income that can be diverted for other future needs. For example, if you treat retirement savings as just another periodic bill, you are more likely to save for it.
You may construct a personal cash budget by recording each cash receipt and cash disbursement on a spreadsheet. Only the date, amount and a brief description of the transaction are necessary. The cash budget is a simple tool that even doctors who lack accounting acumen can use. Since it is possible to track the cash-in and cash-out in the same format used for a standard check register, most doctors find that the process takes very little time. Such a budget will provide a helpful look at how well you are staying within available resources for a given period.
We then continue with an analysis of your operating checkbook and a review of various source documents such as one’s tax return, credit card statements, pay stubs and insurance policies. A typical statement will show all cash transactions that occur within one year. It is helpful to establish a monthly equivalent to all items of income and expense. For the purposes of getting started, note items of income and expense by the frequency you are accustomed to receiving or spending them.
What You Should Know About The ‘Action Plan’ Cash Budget
For a medial office, the first operations budget item might be salary for the doctor and staff. Operating assets and other big ticket items come next. Some doctors/clients review their office P&L statements monthly, line by line, in an effort to reduce expenses. Then they add back those discretionary business expenses they have some control over.
Now, do you still run out of money before the end of the month? If so, you had better cut back on entertainment, eating dinner out or that fancy, new but unproven piece of medical equipment. This sounds draconian until you remind yourself that your choice is either: live frugally later or live a simpler lifestyle now and invest the difference.
As a young doctor, it may be a difficult trade-off. By mid-life, however, you are staring retirement in the face. That is why the action plan depends on your actions concerning monetary scarcity, a plan that one can implement and measure using simple benchmarks or budgeting ratios. By using these statistics, perhaps on an annual basis, the podiatrist can spot problems, correct them and continue planning actively toward stated goals like building long-term wealth.2
Useful Calculations To Assess Your Budgeting Success
In the past, generic budgeting ratios would emphasize not spending more than 15 to 20 percent of your net salary on food or 8 percent on medical care. Now these estimates have given way to more rigorous numbers. Personal budget ratios, much like medical practice financial ratios, represent comparable benchmarks for parameters such as debt, income growth and net worth. Although these ratios are still broad, the following represent some useful personal budgeting ratios for physicians.
• Basic liquidity ratio = liquid assets / average monthly expenses. Cash-on-hand should approach 12 to 24 months or more in the case of a doctor employed by a financially insecure HMO or fragile medical group practice. Yes, chances are you have heard of the standard notion of setting enough cash aside to cover three months in a rainy day scenario. However, we have decried this older laymen standard for many years in our textbooks, white papers and speaking engagements as being wholly insufficient for the competitively unstable environment of modern healthcare.
• Debt to assets ratio = total debt / total assets. This percentage is high initially but should decrease with age as the doctor approaches a debt-free existence
• Debt to gross income ratio = annual debt repayments / annual gross income. This represents the adequacy of current income for existing debt repayments. Doctors should try to keep this below 20 to 25 percent.
• Debt service ratio = annual debt repayment / annual take-home pay. Physicians should aim to keep this ratio below 25 to 30 percent or face difficulty paying down debt.
• Investment assets to net worth ratio = investment assets / net worth. This budget ratio should increase over time as retirement approaches.
• Savings to income ratio = savings / annual income. This ratio should also increase over time as one retires major obligations like medical school debt, a practice loan or a home mortgage.
• Real growth ratio = (income this year – income last year) / (income last year – inflation rate). This budget ratio should grow faster than the core rate of inflation.
• Growth of net worth ratio = (net worth this year – net worth last year) / net worth last year – inflation rate). Again, this budgeting ratio should stay ahead of the specter of rising inflation.
In other words, these ratios will help answer the question: “How am I doing?”
Pearls For Sticking To A Budget
Far from the burden that most doctors consider it to be, budgeting in one form or another is probably one of the greatest tools for building wealth. However, it is also one of the greatest weaknesses among physicians who tend to live a certain lifestyle.3
In fact, I have found that less than one in 10 medical professionals have a personal budget. Fear, or a lack of knowledge, is a major cause of procrastination. Fortunately, the following guidelines assist in reversing this microeconomic disaster.
1. Set reasonable goals and estimate annual income. Do not keep large amounts of cash at home or office. Deposit it in an FDIC insured money-market account for safety. Do not deposit it in a money market mutual fund with net asset value (NAV) that may “break the buck” and fall below the one-dollar level. The new limit is $250,000. Track actual bills and expenses.
2. Do not pay bills early, do not have more taxes withheld from your salary than needed and develop spending estimates to pay fixed expenses first. Fixed expenses are usually contractual and usually include housing, utilities, food, Social Security, medical, debt repayments, homeowner’s or renter’s insurance, auto, life and disability insurance, etc. Reduce fixed expenses when possible. Ultimately, all expenses get paid and become variable in the long run.
3. Make it a priority to reduce variable expenses. Variable expenses are not contractual and may include clothing, education, recreational, travel, vacation, gas, cable TV, entertainment, gifts, furnishings, savings, investments, etc. Trim variable expenses by 5 to 20 percent.
4. Use “carve-outs or “set-asides” for big ticket items and differentiate true wants from frivolous needs.
5. Calculate both income and expenses as a percentage of your total budget. Determine if there is a better way to allocate resources. Review the budget on a monthly basis to notice any variance. Determine if the variance was avoidable, unavoidable or a result of inaccurate assumptions. Take corrective action as needed.
6. Know the difference between saving and investing. Savers tend to be risk adverse while investors understand risk and take steps to mitigate it. Watch mutual fund commissions and investment advisory fees, which cut into return-rates. Keep investments simple and diversified (stocks, bonds, cash, index, no-load mutual and exchange traded funds, etc.).4
How To Budget In The Midst Of A [Corona] Crisis
Sooner or later, despite the best of budgeting intentions, something will go awry. A doctor will be terminated or may be the victim of a reduction-in-force (RIF) because of cost containment initiatives of the corona pandemic. A medical practice partnership may dissolve or a local hospital or surgery center may close, hurting your practice and livelihood. Someone may file a malpractice lawsuit against you, a working spouse may be laid off or you may get divorced. Regardless of the cause, budgeting crisis management encompasses two different perspectives: awareness and execution.
First, if you become aware that you may lose your job, the following proactive steps will be helpful to your budget and overall financial condition.
• Decrease retirement contributions to the required minimum for company/practice match. • Place retirement contribution differences in an after-tax emergency fund. • Eliminate unnecessary payroll deductions and deposit the difference to cash. • Replace group term life insurance with personal term or universal life insurance. • Take your old group term life insurance policy with you if possible. • Establish a home equity line of credit to verify employment. • Borrow against your pension plan only as a last resort.
If you have lost your job or your salary has been depressed, negotiate your departure and get an attorney if you believe you lost your position through breach of contract or discrimination. Then execute the following steps to recalculate your budget and boost your wealth rebuilding activities.
• Prioritize fixed monthly bills in the following order: rent or mortgage; car payments; utility bills; minimum credit card payments; and restructured long-term debt.
• Consider liquidating assets to pay off debts in this order: emergency fund, checking accounts, investment accounts or assets held in your children’s names.
• Review insurance coverage and increase deductibles on homeowner’s and automobile insurance for needed cash.
• Then sell appreciated stocks or mutual funds; personal valuables such as furnishings, jewelry and real estate; and finally, assets not in pension or annuities if necessary.
• Keep or rollover any lump sum pension or savings plan distribution directly to a similar savings plan at your new employer, if possible, when you get rehired.
• Apply for unemployment insurance.
• Review your medical insurance and COBRA coverage after a “qualifying event” such as job loss, firing or even after quitting. It is a bit expensive due to a 2 percent administrative fee surcharge but this may be well worth it for those with preexisting conditions or who are otherwise difficult to insure. One may continue COBRA for up to 18 months.
• Consider a high deductible Health Savings Account (HSA), which allows tax-deferred dollars like a medical IRA, for a variety of costs not normally covered under traditional heath insurance plans. Self-employed doctors deduct both the cost of the premiums and the amount contributed to the HSA. Unused funds roll over until the age of 59½, when one can use the money as a supplemental retirement benefit.
• Eliminate unnecessary variable, charitable and/or discretionary expenses, and become very frugal.
Final Notes
The behavioral psychologist, Gene Schmuckler, PhD, MBA, sometimes asks exasperated doctors to recall the story of the old man who spent a day watching his physician son treating HMO patients in the office. The doctor had been working at his usual feverish pace all morning. Although he was working hard, he bitterly complained to his dad that he was not making as much money as he used to make. Finally, the old man interrupted him and said, “Son, why don’t you just treat the sick patients?” The doctor-son looked at his father with an annoyed expression and responded, “Dad, can’t you see, I do not have time to treat just the sick ones.”5
Always remember to add a bit of emotional sanity into your budgeting and economic endeavors.6
Regardless of one’s age or lifestyle, the insightful doctor realizes that it is never too late to take control of a lost financial destiny through prudent wealth building activities. Personal and practice budgeting is always a good way to start the journey.7
The Author:
Dr. Marcinko is a former university endowed chairman and professor, former certified financial planner and has been a medical management advisor for more than two decades. He is the CEO of www.MedicalBusinessAdvisors.com, a health economics and business finance consulting firm.
References:
1. Marcinko DE (Ed). The Business of Medical Practice (Advanced Profit Maximizing Techniques for Savvy Doctors). Springer Publishers, New York, NY, 2000 and 2004 2. Marcinko DE (Ed). Financial Planning for Physicians and Advisors, Jones and Bartlett Publishers, Sudbury, MA, 2005 3. Marcinko DE (Ed). Risk Management and Insurance Panning for Physicians and Advisors, Jones and Bartlett Publishers, Sudbury, MA, 2006. 4. Marcinko DE, Hetico HR. The Dictionary of Health Insurance and Managed Care. Springer Publishing, New York, 2007. 5. Marcinko DE, Hetico HR. The Dictionary of Health Economics and Finance. Springer Publishing, New York, 2008. 6. Marcinko DE, Hetico HR. Healthcare Organizations (Financial Management Strategies). Standard Technical Publishers, Blaine, WA, 2009. Additional Reference 7. Schmuckler E. Bridging Financial Planning and Human and Human Psychology. In, Marcinko DE (Ed): Financial Planning for Physicians and Healthcare Professionals. Aspen Publications, New York, NY, 2001, 2002 and 2003.
Posted on May 9, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
It’s the first anniversary of the Medicaid unwinding for many states, a process that kicked off when federal rules that had kept people on Medicaid and the Children’s Health Insurance Program (CHIP) through the pandemic expired. And while states could redetermine eligibility again, things have “unwound” more than some experts predicted. Children were kicked off the rolls at higher rates than adults, according to a new study the Urban Institute released May 2. Twelve states—Montana, Iowa, South Dakota, Alabama, Idaho, Georgia, Texas, Arkansas, Oklahoma, Florida, Mississippi, Colorado—exceeded 100% of their total projections for disenrolling children.
The S&P 500® index (SPX) was little changed at 5,187.67; the Dow Jones Industrial Average gained 172.13 points (0.4%) to 39,056.39; the NASDAQ Composite® ($COMP) declined 29.80 points (0.2%) to 16,302.76.
The 10-year Treasury note yield (TNX) rose more than 3 basis points to 4.496%.
The CBOE Volatility Index® (VIX) fell 0.23 to 13.00.
Retail and real estate shares were among the weakest areas Wednesday, while banks and utilities were firm. Utility shares extended a nearly month-long rally, which may in part reflect greater expectations for Fed rate cuts. Lower interest rates can make utility shares with high dividend yields relative to Treasuries more appealing. The Dow Jones Utility Average ($DJU) rose 0.5% to end at its highest level since late July and is up 12% from a mid-April low.
And, Shopify’s value plunged by nearly $20 billion after the online payments company released a gloomy forecast for this quarter. It’s the latest pandemic darling to stumble: According to the Financial Times, the firms that skyrocketed during lockdowns have lost a collective $1.5 trillion in value since the end of 2020.
Steward Health Care System, the largest U.S. physician-owned hospital operator, is expected to file for chapter 11 bankruptcy as soon as Sunday, according to a WSJ report, which cited people familiar with the matter. Steward Health Care is the largest tenant of Medical Properties Trust (NYSE: MPW). Steward Health Care hired restructuring advisers to improve its liquidity and restore its balance sheet in January 2024.
DEFINITION: Mental accounting attempts to describe the process whereby people code, categorize and evaluate economic outcomes. The concept was first named by Richard Thaler. Mental accounting deals with the budgeting and categorization of expenditures. People budget money into mental accounts for expenses or expense categories
Mental Accounting is the act of bucketizing investments and then reviewing the performance of the individual buckets separately (e.g. investing at low savings rate while paying high credit card interest rates).
***
Examples of mental accounting are: (1) matching costs to benefits (wanting to pay for vacation before taking it and getting paid for work after it was done, even though from perspective of time value of money the opposite should be preferred0, (2) aversion to debt (don’t like long-term debt for short-term benefit), (3) sunk-cost effect (illogically considering non-recoverable costs when making forward-going decisions).
In investing, treating buckets separately and ignoring interaction (correlations) induces people not to sell losers (even though they get tax benefits), prevent them from investing in the stock market because it is too risky in isolation (however much less so when looked at as part of the complete portfolio including other asset classes and labor income and occupied real estate), thus they “do not maximize the return for a given level of risk taken).
Posted on May 8, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Here’s where the major stock market benchmarks ended:
The S&P 500 index rose 6.96 points (0.1%) to 5,187.70; the Dow Jones Industrial Average gained 31.99 points (0.1%) to 38,884.26; the NASDAQ Composite® ($COMP) eased 16.70 points (0.1%) to 16,332.56.
The 10-year Treasury note yield dropped more than 3 basis points to 4.457%.
The CBOE Volatility Index® (VIX) fell 0.26 to 13.23.
Interest-rate-sensitive sectors, such as real estate and utilities, were among the market’s strongest performers Tuesday. The Philadelphia Utility Index (UTY) rose 1.3%, its fifth straight daily gain, and hit its highest level in almost a year. The recent strength may in part reflect heightened expectations for lower interest rates, which may make utility shares with relatively high dividend yields compared to Treasuries more appealing. The utilities sector is also coming off a strong April, during which it was the only S&P 500 sector with a positive return, with chart patterns suggesting a bullish long-term momentum shift.
The semiconductor sector was among the weakest sectors Tuesday, partly behind a 1.7% drop in Nvidia (NVDA). The shares fell after billionaire investor Stanley Druckenmiller told CNBC he reduced his stake in the chipmaker in late March, saying that artificial intelligence may be a “little overhyped” for the short term.
***
Peloton is reportedly being circled by private equity firms for a potential buyout of the enfeebled fitness company.
The SEC is preparing to sue over Robinhood’s crypto business. Robinhood just revealed that it’s been notified that the SEC plans to bring an enforcement action against its crypto unit for alleged securities violations. But the online brokerage said it’s not sweating: “We firmly believe that the assets listed on our platform are not securities and we look forward to engaging with the SEC to make clear just how weak any case against Robinhood Crypto would be on both the facts and the law,” Dan Gallagher, Robinhood’s chief legal, compliance, and corporate affairs officer, wrote in a blog post. Such a notice doesn’t always mean a suit will follow, but crypto companies and the agency have been sparring for years over whether crypto tokens count as securities.
The Biden administration were quick to praise a new report that extends the lifespan of the Hospital Insurance Trust Fund, but the report renewed calls for increasing physician payments.
Amwell, a telehealth company, continues to struggle in the stock market, and both its bottom- and top-line results in the first quarter missed Street analysts’ estimates.
And … between the Change Healthcare cyberattack and Medicare Advantage headwinds, major insurers faced unique challenges in the first quarter.
Stat: 8.7%. That’s the level to which US consumers can expect the 30-year mortgage rate to rise over the next year, which marks a series high, according to a New York Federal Reserve survey (MarketWatch)
The investment profession has come a long way since the door-to-door stock salesmen of the 1920s sold a willing public on worthless stock certificates. The stock market crash of 1929 and ensuing Great Depression of the 1930s forever changed the way investment operations are run. A bewildering array of laws and regulations sprung up, all geared to protecting the individual investor from fraud. These laws also set out specific guidelines on what types of investment can be marketed to the general public – and allowed for the creation of a set of investment products specifically not marketed to the general public. These early-mid 20th century lawmakers specifically exempted from the definition of “general public,” for all practical purposes, those investors that meet certain minimum net worth guidelines.
The lawmakers decided that wealth brings the sophistication required to evaluate, either independently or together with wise counsel, investment options that fall outside the mainstream. Not surprisingly, an investment industry catering to such wealthy individuals, such as doctors and healthcare professionals, and qualifying institutions has sprung up.
EARLY DAYS
The original hedge fund was an investment partnership started by A.W. Jones in 1949. A financial writer prior to starting his investment management career, Mr. Jones is widely credited as being the prototypical hedge fund manager. His style of investment in fact gave the hedge fund its name – although Mr. Jones himself called his fund a “hedged fund.” Mr. Jones attempted to “hedge,” or protect, his investment partnership against market swings by selling short overvalued securities while at the same time buying undervalued securities. Leverage was an integral part of the strategy. Other managers followed in Mr. Jones’ footsteps, and the hedge fund industry was born.
In those early days, the hedge fund industry was defined by the types of investment operations undertaken – selling short securities, making liberal use of leverage, engaging in arbitrage and otherwise attempting to limit one’s exposure to market swings. Today, the hedge fund industry is defined more by the structure of the investment fund and the type of manager compensation employed.
The changing definition is largely a sign of the times. In 1949, the United States was in a unique state. With the memory of Great Depression still massively influencing common wisdom on stocks, the post-war euphoria sparked an interest in the securities markets not seen in several decades. Perhaps it is not so surprising that at such a time a particularly reflective financial writer such as A.W. Jones would start an investment operation featuring most prominently the protection against market swings rather than participation in them.
Apart from a few significant hiccups – 1972-73, 1987 and 2006-07 being most prominent – the U.S. stock markets have been on quite a roll for quite a long time now. So today, hedge funds come in all flavors – many not hedged at all. Instead, the concept of a private investment fund structured as a partnership, with performance incentive compensation for the manager, has come to dominate the mindscape when hedge funds are discussed. Hence, we now have a term in “hedge fund” that is not always accurate in its description of the underlying activity. In fact, several recent events have contributed to an even more distorted general understanding of hedge funds.
During 1998, the high profile Long Term Capital Management crisis and the spectacular currency losses experienced by the George Soros organization both contributed to a drastic reversal of fortune in the court of public opinion for hedge funds. Most hedge fund managers, who spend much of their time attempting to limit risk in one way or another, were appalled at the manner with which the press used the highest profile cases to vilify the industry as dangerous risk-takers. At one point during late 1998, hedge funds were even blamed in the lay press for the currency collapses of several developing nations; whether this was even possible got short thrift in the press.
Needless to say, more than a few managers have decided they did not much appreciate being painted with the same “hedge fund” brush. Alternative investment fund, private investment fund, and several other terms have been promoted but inadequately adopted. As the memory of 1998 and 2007 fades, “hedge fund” may once again become a term embraced by all private investment managers.
Photo by Alexander Mils
ASSESSMENT: Physicians, and all investors, should be aware, however, that several different terms defining the same basic structure might be used. Investors should therefore become familiar with the structure of such funds, independent of the label. The Securities Exchange Commission calls such funds “privately offered investment companies” and the Internal Revenue Service calls them “securities partnerships.”
Posted on May 6, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
A cooling labor market raises hopes for a rate cut in the summer. The latest Labor Department data shows the US added 175,000 jobs in April, but much less than the 300,000 added in March and also less than economists expected. Meanwhile, the unemployment rate ticked up to 3.9% from 3.8% in March, and wages rose less than anticipated. All that bad news for us was music to the ears of investors who are holding out hope that the Federal Reserve might still cut interest rates this summer despite most recent economic data showing that inflation is sticking around.
Rate cuts appear to be back on the 2024 menu following Friday’s softer-than-expected jobs report, fueling gains for all three major stock indexes last week. With the report calming worries that inflation is ticking back up, investors now project a 50% likelihood that the Federal Reserve will reduce rates in September.
Coinbase is benefiting from the hype around new bitcoin ETFs. The crypto exchange reported a $1.2 billion quarterly profit last week, and net revenue rose by 115%.
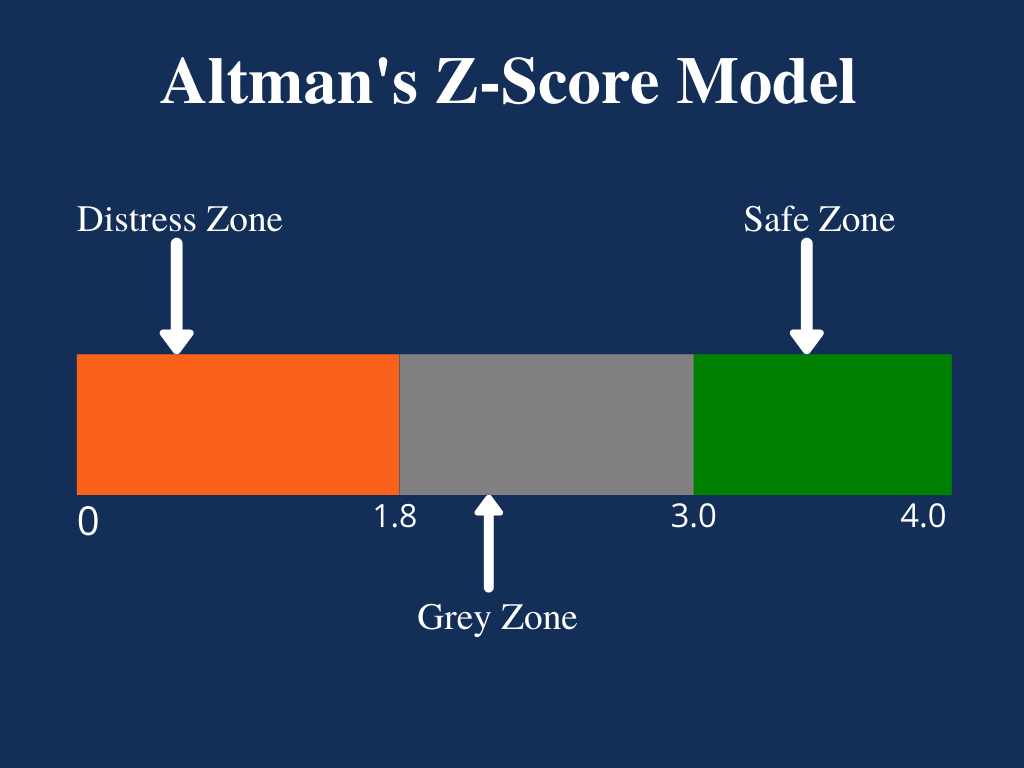
The Zeta Model is a mathematical model that estimates the chances of a public company going bankrupt within a two-year time period. The number produced by the model is referred to as the company’s Z-score (or zeta score) and is considered to be a reasonably accurate predictor of future bankruptcy.
The model was published in 1968 by New York University professor of finance Edward I. Altman. The resulting Z-score uses multiple corporate income and balance sheet values to measure the financial health of a company.
Posted on May 4, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The S&P 500 index rose 63.59 points (1.3%) to 5,127.79, up 0.6% for the week; the Dow Jones Industrial Average® ($DJI) gained 450.02 points (1.2%) to 38,675.68, up 1.1% for the week; the NASDAQ Composite surged 315.37 points (2.0%) to 16,156.33, up 1.4% for the week.
The 10-year Treasury note yield (TNX) fell about 7 basis points to 4.50%, down about 16 basis points for the week.
The CBOE Volatility Index® (VIX) fell 1.19 to 13.49.
Technology shares were among the strongest performers Friday behind a 6% rally in shares of Apple (AAPL), which late Thursday reported stronger-than-expected quarterly results and said it will repurchase $110 billion in shares. Amgen (AMGN) soared nearly 12%, leading Dow gainers after the biotechnology company beat earnings expectations.
In other markets, WTI Crude Oil futures (/CL) extended a week-long slump to end just above $78 per barrel, the lowest since mid-March. Crude futures dropped almost 7% this week, partly reflecting rising U.S. supplies and signs of slower fuel demand.
Posted on May 3, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Yesterday, sales of Wegovy more than doubled last quarter, and at least 25,000 people are starting to take it in the US per week. It also posted a $3.65 billion net profit and increased its sales outlook for 2024. But its stock Novo Nordisk still dropped yesterday.
***
iPhone sales are down but Apple share buybacks are up. Apple managed to keep investors happy, sending its stock shooting up after-hours yesterday, despite selling fewer iPhones last quarter. Sales of the signature phone dipped 10% year over year, and revenue fell 4.3% to $90.8 billion. But Apple also announced $110 billion in share buybacks, the largest in the company’s history, per CNBC. And sales in China, which has been a sore spot, came in at $16.4 billion, less than a year earlier but more than analysts had predicted.
***
Stocks rose yesterday as investors digested Jerome Powell’s recent comments and decided they only had to fear fear itself—and not interest rate hikes. Investors changed into the fast lane to buy Carvana after the used car sales site reported its best earnings ever Wednesday evening.
***
Stat: 16%. That’s the percentage by which CVS stocks plummeted Wednesday after the company reported earnings below expectations and cut its annual outlook, according to (CNBC).
But – Here’s where the major stock market benchmarks ended Thursday:
The S&P 500® index (SPX) rose 45.81 points (0.9%) to 5,064.20; the Dow Jones Industrial Average® ($DJI) added 322.37 points (0.9%) to 38,225.66; the NASDAQ Composite® ($COMP) surged 235.48 points (1.5%) to 15,840.96.
The 10-year Treasury note yield (TNX) dropped about 1 basis point to 4.583%.
The CBOE Volatility Index® (VIX) fell 0.71 to 14.68.
Transportation shares helped lead the market higher after C.H. Robinson (CHRW) reported stronger-than-expected quarterly results, sending the freight logistics and trucking company’s stock up 12%. The Dow Jones Transportation Average ($DJT) jumped 2.5%. Semiconductors were also strong after Qualcomm (QCOM) advanced 9.7% in the wake of the chip maker’s better-than-expected earnings.
Apple (AAPL) shares advanced 2.2% ahead of the company’s quarterly earnings report scheduled after Thursday’s close.
In other markets, WTI Crude Oil (/CL) futures bounced back to end with a slight gain after earlier dropping to a seven-week low under $78.50 per barrel.
Posted on May 3, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd CMP
***
***
Medicare [Dis] Advantage Plans [Medicare Part C] commenced in 2003 or so and I have railed against them since then. First, for their low physician payments. And then as a patient advocate for the last decade. And, today, for both reasons. As a doctor and independent health insurance agent myself, believe me when I speak thusly.
Now, while Medicare Advantage plans are undoubtedly not the right choice for everyone, insurance companies still say there are some folks who will get exactly what they need from the plans and at a moderate price.
Nevertheless, Ernesto Jaboneta, the IT Director of California-based Medicare insurance agency Agent Pitstop, acknowledged there are many predatory salespeople who will jump to have you join a plan that doesn’t end up helping you in the long run. Still, there are precautions you can take to make falling into this trap less likely.
“The first thing anyone can do is invite along a family member or trusted friend to any appointments with an insurance agent,” Jaboneta told Newsweek. “Don’t feel pressured to decide right away.”
Before you commit to anything, you should compare plans and find out if your doctors will remain in your network. And if you’re unsure about some of the information you received from an insurance agent, you can also call 1-800-MEDICARE for more assistance.
Jaboneta also said there’s a big difference between captive insurance agents and independent agents, as well, and seniors should take note of this.
“A captive agent is an insurance agent who works directly for an insurance carrier,” Jaboneta said. “They have no incentive to compare options outside their own company, which is different than an independent agent who can compare all the options available. In many cases, when a beneficiary calls into an insurance company to find information, they will be talked into enrolling.”
The open enrollment period lasts from October 15th to December 8th, but there’s another enrollment period from January 1st to March 31st for anyone unhappy with their Medicare Advantage plan who wants to switch or revert to Medicare.
INVESTING UPDATE: Managed-care companies are reporting that seniors on Medicare Advantage Part C plans used far more medical services than expected in the final months of 2023. The announcements have sparked two separate selloffs over the past week: The first came January 12th, when UnitedHealth Group announced its fourth-quarter earnings. The second came after Humana just laid out preliminary fourth-quarter results, and said the high utilization trends would have a material impact on its 2024 performance “if current trends continue.”
It is critical to understand and to measure the total cost of capital. Lack of understanding and appreciation of the total cost of capital is widespread, particularly among not-for-profit hospital executives. The capital structure includes long-term debt and equity; total capital is the sum of these two. Each of these components has cost associated with it. For the long-term debt portion, this cost is explicit: it is the interest rate plus associated costs of placement and servicing.
Equity portion
For the equity portion, the cost is not explicit and is widely misunderstood. In many cases, hospital capital structures include significant amounts of equity that has accumulated over many years of favorable operations. Too many executives wrongly attribute zero cost to the equity portion of their capital structure. Although it is correct that generally accepted accounting principles continue to assign a zero cost to equity, there is opportunity cost associated with equity that needs to be considered. This cost is the opportunity available to utilize that capital in alternative ways.
***
***
In general, the cost attributed to equity is the return expected by the equity markets on hospital equity. This can be observed by evaluating the equity prices of hospital companies whose equity is traded on public stock exchanges. Usually the equity prices will imply cost of equity in the range of 10% to 14%.
Almost always, the cost of equity implied by hospital equity prices traded on public stock exchanges will substantially exceed the cost of long-term debt. Thus, while many hospital executives will view the cost of equity to be substantially less than the cost of debt (i.e., to be zero), in nearly all cases, the appropriate cost of equity will be substantially greater than the cost of debt.
Hospitals need to measure their weighted average cost of capital (WACC).
WACC is the cost of long-term debt multiplied by the ratio of long-term debt to total capital plus the cost of equity multiplied by the ratio of equity to total capital (where total capital is the sum of long-term debt and equity).
WACC is then used as the basis for capital charges associated with all capital investments. Capital investments should be expected to generate positive returns after applying this capital charge based on the WACC. Capital investments that don’t generate returns exceeding the WACC consume enterprise value; those that generate returns exceeding WACC increase enterprise value.
Assessment
Hospital executives need to be rewarded for increasing enterprise value.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on May 2, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Here’s where the major stock market benchmarks ended:
The S&P 500® index (SPX) fell 17.30 points (0.3%) to 5,018.39; the Dow Jones Industrial Average® ($DJI) gained 87.37 points (0.2%) to 37,903.29; the NASDAQ Composite® ($COMP) lost 52.34 points (0.3%) to 15,605.48.
The 10-year Treasury note yield (TNX) dropped more than 5 basis points to 4.63%.
The CBOE Volatility Index® (VIX) decreased 0.28 to 15.37.
Banks and other financial shares led the market’s afternoon upswing, reflecting renewed optimism over the outlook for interest rates. The KBW Regional Bank Index (KRX) jumped 2.4% and posted its first gain in five days. Biotechnology and communication services were also strong.
Energy shares were among the weakest performers as WTI Crude Oil (/CL) futures extended a week-long nosedive and dropped under $80 per barrel for the first time since mid-March. Crude futures sank over 3% after the Energy Information Administration reported U.S. oil inventories surged 1.6% last week.
Among top companies, Amazon (AMZN) gained 2.2% after reporting stronger-than-expected earnings and revenue late Tuesday. Starbucks (SBUX) tumbled 16% following unexpectedly soft quarterly results. Apple (AAPL) eased 0.6% ahead of its quarterly results, expected after Thursday’s close.
Speaking of stock companies, however big you think UnitedHealth is, it’s bigger than that. For example:
With a market cap of nearly $450 billion, it’s the fourth-largest company in the US by revenue this year, beating out Alphabet and Microsoft.
The company is eyeing a $24.7 billion profit in 2024.
One analyst estimated that more than 5% of US GDP flows through UnitedHealth’s systems daily.
And so, lawmakers in Washington are prepared to grill UnitedHealth CEO Andrew Witty in two congressional hearings today, months after a cyberattack on a subsidiary of the healthcare giant, Change Healthcare, rattled the industry and left pharmacies, doctors, and hospitals in the dark. Change processes roughly half of all Americans’ medical claims. Congress wants Witty to clarify how UnitedHealth handled the breach of patient data. But beyond that, it wants to investigate whether the company—the nation’s largest private health insurer—has grown too big and taken on too much risk.
Retailer Walmart announced plans Tuesday to shutter its network of 51 health clinics in five states, along with its telehealth business. The impending closures signify that Walmart is scuttling its initial plans to expand the services, citing escalating operation costs and “challenging reimbursement environment,” the company said in a news release.
Finally – Happy Women’s Health Month! Women and people assigned female at birth are disproportionately affected by a range of health conditions, including autoimmune diseases, chronic pain, and dementia. The month of May is intended to raise awareness of these disparities and educate women on steps they can take to improve their health, such as getting annual breast exams. For all our woman-identifying readers, take some time to prioritize your health this month!
Posted on May 1, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Dr. David Edward Marcinko MBAMEd CMP
***
According to George Washington University, a hospital chargemaster is a comprehensive list of a hospital’s products, procedures, and services. Everything from prescription drugs to supplies for diagnostic tests has a unique price listing in the chargemaster, making it a go-to document for hospital administrators such as CFOs, clinical documentation improvement specialists, and revenue directors.
Chargemaster usage dates back to the mid-20th century. At that time, fee-for-service (FFS) health insurance plans, which allow patients to direct their medical care by choosing physicians and facilities and paying a portion of the billed total, had just emerged in the U.S. healthcare system.
The chargemaster originally served as something akin to an FFS dictionary, with an entry for virtually anything billable under that economic model of healthcare.
Over time, FFS itself has evolved and been challenged by alternatives like value-based care (VBC). Chargemasters built for FFS have changed accordingly, and they remain fixtures of the modern hospital revenue cycle. A standard chargemaster is a large electronic file containing multiple elements for each entry. These attributes usually include:
The charge for a single unit of the service in question
A Current Procedural Terminology (CPT) code; CPT is the official medical code set of the American Medical Association
Potentially, a Healthcare Common Practice Coding System (HCPCS) code; HCPCS is based on CPT
Alternative CPT and HCPCS codes if needed, e.g. one corresponding only to specific payers
A revenue code associated with the charge
Flag(s) indicating if the entry is scheduled for deletion, active or inactive
An internal reference number within the ledger for accounting purposes
Posted on May 1, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
THE ENTREPRENEURIAL M.D.
In this episode we are joined by Dr. Brent Jackson, Chief Medical Officer for Mercy General in Sacramento, CA to discuss the physician life-cycle, burnout, and transitioning into leadership within healthcare.
Posted on April 30, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
It’ll be a big week for hot takes on the US economy, after the Federal Reserve meeting Tuesday and Wednesday and the April jobs report dropping Friday. Because inflation has been sticking around, the FOMC is expected to hold interest rates steady at this meeting and for the foreseeable future. On the jobs front, economists are projecting another strong month for employment growth.
In 2022, with bipartisan support, Congress passed the CHIPS and Science Act, an ambitious plan to juice domestic manufacturing of a product vital to national security: semiconductors. Two years later, the government has doled out more than half of the CHIPS Act’s $39 billion in incentives. According to the Financial Times …
Chip companies and their suppliers have announced US investments of $327 billion over the next 10 years, per the Semiconductor Industry Association.
Construction of manufacturing facilities for computing and electronics devices has jumped 15x, government data shows.
By 2030, the US will likely produce around 20% of the world’s most advanced chips, according to USCommerce Secretary Gina Raimondo. Right now, it’s making 0%.
The proposed factories are massive and could transform regional economies. Micron, which received $6.1 billion in federal grants last week, plans to invest $100 billion in a manufacturing campus near Syracuse.
The S&P 500® index (SPX) rose 16.21 points (0.3%) to 5,116.17, its highest close in over two weeks; the Dow Jones Industrial Average® ($DJI) gained 146.43 points (0.4%) to 38,386.09, the NASDAQ Composite® ($COMP) advanced 55.18 points (0.4%) to 15,983.08.
The 10-year Treasury note yield (TNX) fell more than 5 basis points to 4.616%.
The CBOE Volatility Index® (VIX) declined 0.36 to 14.67.
Communication services shares were among the market’s weakest performers Monday, reversing last Friday’s upswing as Alphabet (GOOGL) dropped more than 3% and Meta Platforms (META) lost 2.4%. Banks and retailers were also soft. The Philadelphia Semiconductor Index (SOX) climbed for the sixth-straight day and ended near a three-week high even though its biggest member, Nvidia (NVDA), ended little changed.
In other markets, the U.S. Dollar Index ($DXY) faded from early gains but is still up about 1% in April, driven by expectations domestic rates will remain high. “The U.S. dollar’s strength continues to reflect the relative strength of the economy and the wide interest rate differentials between the United States and other major developed markets,” Schwab Center for Financial Research analysts said in a report.
Despite last week’s strength, the S&P 500 index and the NASAQ Composite are still down 2.6% and 2.4%, respectively, for April and on track to break five-month winning streaks.
Humana expects to exit Medicare Advantage (MA) markets in 2025, company executives told investors. The company reported its first quarter earnings April 24th. Humana posted $741 million in net income in the first quarter of 2024, beating investor expectations, but pulled its 2025 earnings guidance.
Modern Portfolio Theory approaches investing by examining the complete market and the full economy. MPT places a great emphasis on the correlation between investments.
DEFINITION:
Correlation is a measure of how frequently one event tends to happen when another event happens. High positive correlation means two events usually happen together – high SAT scores and getting through college for instance. High negative correlation means two events tend not to happen together – high SATs and a poor grade record.
No correlation means the two events are independent of one another. In statistical terms two events that are perfectly correlated have a “correlation coefficient” of 1; two events that are perfectly negatively correlated have a correlation coefficient of -1; and two events that have zero correlation have a coefficient of 0.
Correlation has been used over the past twenty years by institutions and financial advisors to assemble portfolios of moderate risk. In calculating correlation, a statistician would examine the possibility of two events happening together, namely:
If the probability of A happening is 1/X;
And the probability of B happening is 1/Y; then
The probability of A and B happening together is (1/X) times (1/Y), or 1/(X times Y).
There are several laws of correlation including;
Combining assets with a perfect positive correlation offers no reduction in portfolio risk. These two assets will simply move in tandem with each other.
Combining assets with zero correlation (statistically independent) reduces the risk of the portfolio. If more assets with uncorrelated returns are added to the portfolio, significant risk reduction can be achieved.
Combing assets with a perfect negative correlation could eliminate risk entirely. This is the principle with “hedging strategies”. These strategies are discussed later in the book.
In the real world, negative correlations are very rare
Most assets maintain a positive correlation with each other. The goal of a prudent investor is to assemble a portfolio that contains uncorrelated assets. When a portfolio contains assets that possess low correlations, the upward movement of one asset class will help offset the downward movement of another. This is especially important when economic and market conditions change.
As a result, including assets in your portfolio that are not highly correlated will reduce the overall volatility (as measured by standard deviation) and may also increase long-term investment returns. This is the primary argument for including dissimilar asset classes in your portfolio. Keep in mind that this type of diversification does not guarantee you will avoid a loss. It simply minimizes the chance of loss.
In the table provided by Ibbotson, the average correlation between the five major asset classes is displayed. The lowest correlation is between the U.S. Treasury Bonds and the EAFE (international stocks). The highest correlation is between the S&P 500 and the EAFE; 0.77 or 77 percent. This signifies a prominent level of correlation that has grown even larger during this decade. Low correlations within the table appear most with U.S. Treasury Bills.
It is critical for physician executives to understand and to measure the total cost of hospital capital. Lack of understanding and appreciation of the total cost of capital is widespread, particularly among not-for-profit hospital and physician executives. The capital structure includes long-term debt and equity; total capital is the sum of these two, and, each of these components has cost associated with it.
For the long-term debt portion, this cost is explicit—it is the interest rate plus associated costs of placement and servicing. For the equity portion, the cost is not explicit and is widely misunderstood. In many cases, hospital capital structures include significant amounts of equity that has accumulated over many years of favorable operations.
Far too many executives wrongly attribute zero cost to the equity portion of their capital structure. Although it is correct that generally accepted accounting principles continue to assign a zero cost to equity, there is opportunity cost associated with equity that needs to be considered. This cost is the opportunity available to utilize that capital in alternative ways.
***
***
In general, the cost attributed to equity is the return expected by the equity markets on hospital equity. This can be observed by evaluating the equity prices of hospital companies whose equity is traded on public stock exchanges. Usually, the equity prices will imply cost of equity in the range of 10%–14%. Almost always, the cost of equity implied by hospital equity prices traded on public stock exchanges will substantially exceed the cost of long-term debt. Thus, while many hospital executives will view the cost of equity to be substantially less than the cost of debt (i.e., to be zero) in nearly all cases, the appropriate cost of equity will be substantially greater than the cost of debt.
Hospitals need to measure their weighted average cost of capital (WACC). WACC is the cost of long-term debt multiplied by the ratio of long-term debt to total capital plus the cost of equity multiplied by the ratio of equity to total capital (where total capital is the sum of long-term debt and equity).
WACC is then used as the basis for capital charges associated with all capital investments. Capital investments should be expected to generate positive returns after applying this capital charge based on the WACC. Capital investments that do not generate returns exceeding the WACC consume enterprise value; those that generate returns exceeding WACC increase enterprise value. Therefore, physician and hospital executives need to be rewarded for increasing enterprise value.
Posted on April 27, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Here’s where the major stock market benchmarks ended:
The S&P 500 index gained 51.54 points (1.0%) to 5,099.96, up 2.7% for the week; the Dow Jones Industrial Average® ($DJI) increased 153.86 points (0.4%) to 38,239.66, up 0.7% for the week; the NASDAQ Composite jumped 316.14 points (2.0%) to 15,927.90, up 4.2% for the week.
The 10-year Treasury note yield (TNX) lost about 4 basis points to 4.665%.
The CBOE Volatility Index® (VIX) fell 0.34 to 15.03.
Alphabet’s rally helped communication services reverse Thursday’s downturn, which was driven by disappointing quarterly results from Meta Platforms (META). The S&P 500 Communication Services index ($SP500#50) surged 4.7% Friday and ended the week with a 2.7% gain. Semiconductor shares were also strong, led by a 6% gain in Nvidia (NVDA). The Russell 2000® Index (RUT) added 1.1% Friday and posted a 2.8% advance for the week.
In other markets, WTI Crude Oil (/CL) futures rose slightly Friday, ending around $83.65 per barrel and shutting down a three-week losing streak.
Midi Health, a health clinic geared toward women in midlife, raised $60 million in Series B funding to expand its network to 150 clinicians by the end of the year, among other efforts. (MobiHealthNews)
“We’re fooling ourselves if we think that’s cheap or can be done less expensively.”—Carmela Coyle, president and CEO of the California Hospital Association, on hospital finances and cutting costs (AP)
The federal government implemented new staffing rules to improve patient care, but most nursing homes won’t be able to meet that demand. (KFF Health News/NPR)
The Biden administration is considering a change that would downgrade cannabis from a Schedule I drug to a Schedule III drug this year. The reclassification would have major effects on the business of cannabis, but for that to happen, the Drug Enforcement Agency needs proof of medical effectiveness.
Posted on April 26, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
New GDP numbers out yesterday show a worrying combo of stubborn inflation + waning growth that dampens hopes for a potential interest rate cut. Per the latest data from the Bureau of Economic Analysis, the first quarter of 2024 was a confounding one:
GDP increased at a 1.6% annualized rate, far below projections of 2.4% and notably down from 3.4% at the end of 2023.
While slow growth would typically signal that the Fed could cut rates, another metric complicates matters: Consumer prices (excluding volatile categories), a solid indicator of inflation, shot up to a much higher than anticipated 3.7%.
***
Meta reported record Q1 revenue yesterday, but it was overshadowed by the billions of dollars the company is spending in its efforts to win the Artificial Intelligence race and make the Metaverse happen. Investors were unhappy with the company’s forecast that its spending will rise by $10 billion dollars to support Artificial Intelligence development, sending Meta’s stock price down 15% after hours.
Here’s where the major benchmarks ended:
The S&P 500 index fell 23.21 points (0.5%) to 5,048.42; the Dow Jones Industrial Average lost 375.12 points (1.0%) to 38,085.80; the NASDAQ Composite® ($COMP) shed 100.99 points (0.6%) to 15,611.76.
The 10-year Treasury note yield (TNX) rose about 5 basis points to 4.704%.
The CBOE Volatility Index® (VIX) fell 0.64 to 15.33.
Communication services shares were the weakest S&P 500 sector Thursday behind the plunge in Meta Platforms. Late Wednesday, the Facebook parent provided lighter-than-expected second-quarter revenue guidance, while CEO Mark Zuckerberg discussed spending in currently unprofitable pursuits such as artificial intelligence (AI) and mixed reality. Meta’s first-quarter earnings and revenue both came above analysts ‘ estimates, however.
Meta’s slump helped send the S&P 500 Communication Services index ($SP500#50) down 4%. Banks were also particularly soft amid concern that persistently high interest rates may compress lender margins. Semiconductor and transportation shares were among the few pockets of strength.
But, Alphabet, Microsoft, and Snap reported Q1 earnings yesterday, and were generally good. Alphabet issued its first-ever dividend and authorized $70 billion in stock buybacks, after it beat Wall Street’s revenue expectations. Microsoft also beat revenue forecasts on the strength of its cloud services. And Snap shares soared after it topped estimates and impressed investors with its 422 million global daily active users. It was a much-needed boost for the sector after Meta spooked the market with how much it’s spending on AI.
Posted on April 25, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Otherwise known as “National Prescription Drug Take Back Day,” National Drug Take Back Day on April 25th is sponsored by the Drug Enforcement Agency. Its goal is to keep the public aware of the dangers of prescription drug use and misuse. Many Americans don’t know how to safely dispose of the prescription drugs that have been sitting in the medicine cabinet past their prime. Using these expired drugs, or using someone else’s, is dangerous and puts both the public and the environment at risk.
Spotify made money in Q1. According to Morning Brew, the streaming music giant grew its revenue last quarter by 20% to $3.8 billion on a record $180 million in profit, it announced yesterday. The smash report comes after Spotify cut costs last year, which included laying off more than a quarter of its workforce. The company also raised prices in 2023 for the first time in a decade as it further expanded beyond music into audio books and other categories. Spotify shares soared ~11% following the news.
***
Here’s where the major benchmarks ended:
The S&P 500 index® (SPX) rose 1.08 points (0.02%) to 5,071.63; the Dow Jones Industrial Average® ($DJI) fell 42.77 points (0.1%) to 38,460.92; the NASDAQ Composite® ($COMP) added 16.11 points (0.1%) to 15,712.75.
The 10-year Treasury note yield rose more than 4 basis points to 4.644%.
The CBOE Volatility Index® (VIX) rose 0.28 to 15.97.
Transportation shares were among the market’s weakest performers Wednesday behind a drop of more than 10% in Old Dominion Freight Line (ODFL), which reported lighter-than-expected quarterly revenue. The shipper’s nosedive helped send the Dow Jones Transportation Average ($DJT) down 2.3%. Consumer staples, semiconductors, and utilities posted moderate advances. The Dow Jones Utility Index ($DJU) gained for the sixth straight day and ended at a three-and-a-half-month high.
***
The National Association of Realtors’ $418 million settlement over an alleged conspiracy to inflate commissions received preliminary approval yesterday. It’s a new world order: Sellers won’t have to pay buyers’ agents anymore. There’s been talk of a metaphorical death of real estate agents, or a mass extinction; the jury is still out, but RE/MAX cofounder and chairman Dave Liniger doesn’t seem too concerned.
The Labor Department announced it has finalized its Retirement Security Rule, which aims to protect American workers who are saving for retirement and relying on advice from fiduciaries for it. The new rule will update the definition of an investment advice fiduciary under the Employee Retirement Income Security Act and the Internal Revenue Code.
Clinicians don’t always get it right, and their mistakes can be costly: Studies show misdiagnoses lead to roughly 800,000 patient deaths or permanent disabilities each year in the US and cost the healthcare system an estimated $20 billion annually. Cleveland Clinic is using telehealth to try to combat misdiagnoses via its virtual second opinions program, which has saved an average of $8,705 per patient by avoiding unnecessary treatments, according to an analysis released in March.
We have partnered with fiduciary focused financial advisors and fee-only financial consultants who understand the needs of doctors, dentists and medical professionals. More importantly, they understand how the healthcare industrial complex is currently in flux.
Posted on April 24, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Stat: 740. That’s how many employees Nike will lay off at its Oregon HQ before the end of June. In February, Nike CEO John Donahoe informed employees of the company’s plan to reduce 2% of its workforce, which would mean around 1,600 employees in total. (USA Today)
Let’s say you leave your job at any time during or after the calendar year you turn 55 (or age 50 if you’re a public safety employee with a government defined-benefit plan). Under a little-known separation-of-service provision, often referred to as the “rule of 55,” you may be able take distributions (though some plans may allow only one lump-sum withdrawal) from your 401(k), 403(b), or other qualified retirement planfree of the usual 10% early-withdrawal penalties. However, be aware that you’ll still owe ordinary income taxes on the amount distributed. This exception applies only to the plan (including any consolidated accounts) that you were contributing to when you separated from service. It does not extend to IRAs.
The S&P 500 index rose 59.95 points (1.2%) to 5,070.55; the Dow Jones Industrial Average gained 263.71 points (0.7%) to 38,503.69; the NASDAQ Composite® ($COMP) surged 245.33 points (1.6%) to 15,696.64.
The 10-year Treasury note yield (TNX) decreased about 2 basis points to 4.602%.
The CBOE Volatility Index® (VIX) fell 1.25 to 15.69.
Similar to Monday, chipmakers were among the market’s strongest areas, carrying the Philadelphia Semiconductor Index (SOX) to a 2.2% advance. Retailers and communication services shares were also strong. The Dow Jones Utility Index ($DJU) gained for the fifth straight day and ended at its highest level in over three months. The Russell 2000® Index (RUT) surged nearly 2%.
Posted on April 20, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
A group of 15 financial officers representing 13 states issued a warning to Bank of America over its alleged practices of “politicized de-banking” targeting conservatives. In a letter to Bank of America CEO Brian Moynihan, the officials said the bank’s practices threaten its own financial health and reputation with customers while simultaneously harming the U.S. economy and Americans’ civil liberties. They pointed to examples of Bank of America shuttering the accounts belonging to Christian groups and leaders and joining a net-zero climate alliance in addition to its poor viewpoint diversity rating.
Texas and Missouri will soon have about two dozen Walmart health centers, the retail giant announced this month, adding to its 50-site roster. The company plans to open eight clinics in the Houston metro area, 10 sites in the Dallas-Fort Worth area, and four facilities in Kansas City by the end of 2024, Modern Healthcare reported.
Hospitals reported the strongest quarter of mergers and acquisitions since 2020, according to consulting firm Kaufman Hall. Four of the 20 announced transactions in the first quarter of 2024 were “megamergers” and brought in $12 billion in revenue in that time period, per the firm’s analysis. The era of consolidation is here.
The S&P 500 index fell 43.89 points (0.9%) to 4,967.23, down 3% for the week; the Dow Jones Industrial Average gained 211.02 points (0.6%) to 37,986.40, little changed for the week; the NASDAQ Composite lost 319.49 points (2.1%) to 15,282.01, down 5.5% for the week.
The 10-year Treasury note yield (TNX) dropped more than 2 basis points to 4.623%, still up about 10 basis points for the week.
The CBOE Volatility Index® (VIX) rose 0.71 to 18.71.
Nvidia (NVDA) plunged 10% to lead the chip sector lower, sending the Philadelphia Semiconductor Index (SOX) down 4.1% to a two-and-a-half-month low. Communication Services shares were also among the weakest sectors, fueled by Netflix weakness. There were several pockets of strength, however. Banking shares posted firm gains Friday behind stronger-than-expected quarterly results from some regional lenders. Utilities also advanced.
The S&P 500 has fallen 5.5% from a record close March 28, more than halfway to the 10% threshold that’s traditionally viewed as a correction. The NASDAQ Composite is down 7.1% from a record close on April 11th.
Posted on April 19, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
If the practice makes a reasonable effort to collect from a patient who is experiencing financial hardship (e.g., job loss due to COVID-19), providers may be able to offer a discount (e.g., settle for 70% of the amount owed) without violating Stark Law, says Reed Tinsley, CPA, healthcare consultant in Houston, Texas. “But remember that just because even if someone doesn’t have a job, they could still have money,” he adds. “There are a lot of people out there with big savings accounts.”
Source: Lisa A. Eramo, MA, Keith A. Reynolds, Physicians Practice [4/3/24]
23andMe cofounder and CEO Anne Wojcicki wants to take the once-hot DNA company private. 23andMe said a Special Committee would evaluate the proposal in light of other options. The company’s valuation has tumbled since its stock market debut in 2021. The struggling DNA company once valued in the billions — was essentially worthless as of Wednesday.
But,shares soared Thursday less than three years after it began selling shares. Wojcicki told board members she is proposing to acquire the company in a potential go-private transaction, according to a filing with the Securities and Exchange Commission.
The S&P 500 index fell 11.09 points (0.2%) to 5,011.12; the Dow Jones Industrial Average® ($DJI) rose 22.07 points (0.1%) to 37,775.38; the NASDAQ Composite lost 81.88 points (0.5%) to 15,601.50.
The 10-year Treasury note yield (TNX) gained almost 5 basis points to 4.633%.
The CBOE Volatility Index® (VIX) dropped 0.22 to 17.99.
Weakness in chip maker shares pushed the Philadelphia Semiconductor Index (SOX) down 1.7% to a two-month low. Biotechnology and consumer discretionary shares were also among the weakest sectors. Energy companies eroded as WTI Crude Oil (/CL) futures dropped for a third straight trading day and closed at a three-week low.
The S&P 500 is on track for its third consecutive weekly decline, its weakest stretch since September, while the NASDAQ Composite appears headed for a fourth straight weekly slide.
Posted on April 18, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Pharmacy Benefits Managers often need more transparency regarding their pricing structures and the rebates they negotiate with drug manufacturers. Some argue that PBMs might receive hidden fees or undisclosed profits from drug manufacturers in exchange for favorable positioning on their formularies (lists of covered medications). This can be seen as a form of kickback, which is illegal.
Lawmakers Express Fury Toward UnitedHealth in Change Attack Hearing on the fallout surrounding the unprecedented cyberattack on Change Healthcare in late February. Individuals representing the American Hospital Association, private cybersecurity groups and providers testified before members of the House Energy and Commerce Committee on April 16th to discuss the healthcare industry’s response to the attack and how the federal government should act.
In March, the cyber criminal organization received $22 million in bitcoins, though UnitedHealth Group has not addressed whether the company paid the ransom. On April 15th, ransomware group RansomHub posted files on its dark web leak site comprising of personal and protected health information on patients whose data was taken in the hack. The files also include contracts and agreements between Change and its clients, marking the first time hackers have posted data from the attack.
Stocks started the day strong yesterday but ended up slumping before the market closed as investors pulled back on tech stocks, including Nvidia. United Airlines took off after releasing a strong forecast for the year despite saying it took a $200 million hit because of Boeing’s troubles.
Here’s where the major benchmarks ended:
The S&P 500 index lost 29.20 points (0.6%) to 5,022.21; the Dow Jones Industrial Average declined 45.66 points (0.1%) to 37,753.31; the NASDAQ Composite dropped 181.88 points (1.2%) to 15,683.37.
The 10-year Treasury note yield (TNX) decreased more than 7 basis points to 4.585%.
The CBOE Volatility Index® (VIX) fell 0.20 to 18.20.
ASML’s slump helped send the Philadelphia Semiconductor Index (SOX) down 3.3% to its lowest level since late February. Transportation shares were also under pressure after trucking company J.B. Hunt Transport Services (JBHT) dropped 8.1% in the wake of disappointing quarterly numbers. Energy shares slipped as WTI Crude Oil (/CL) futures fell 3% to a three-week low.
Did you know that desperate doctors of all ages are turning to knowledgeable financial advisors and medical management consultants for help? Symbiotically too, generalist advisors are finding that the mutual need for knowledge and extreme niche synergy is obvious.
***
***
But, there was no established curriculum or educational program; no corpus of knowledge or codifying terms-of-art; no academic gravitas or fiduciary accountability; and certainly no identifying professional designation that demonstrated integrated subject matter expertise for the increasingly unique healthcare focused financial advisory niche … Until Now!
So, if you are looking to supplement your knowledge, income and designations; and find other qualified professionals you may want to consider the CMP® program.
Enter the Certified Medical Planner™ charter professional designation. And, CMPs™ are FIDUCIARIES, 24/7.
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
***
***
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Many financial planning websites mention fees, as required, but still remain opaque to potential clients because the advisor wants to control the discussion and understandably wishes to avoid the website shopper phenomenon.
But, physicians and all investors can still control the discussion, and still provide transparency, because posting up front pricing information doesn’t mean presenting information in a vacuum!
For example, a 1%/year fee doesn’t have to just be 1%; it can be 1%, compared to an industry average cost of X%, where the average cost of an actively managed mutual fund is Y%.
***
***
Similarly, it doesn’t have to be a retainer fee of $1,000/year; it can be a retainer fee for less than the cost of a monthly cable bill! And, a financial plan doesn’t cost $1,500; it costs 8-12 hours of staff time to craft extensive, customized solutions; but saves the doctor-client so much more!
And, if services have a range of potential prices, they might be provided with some insight into the factors that impact the price. Modern young and internet savvy doctors expect this sort of information.
Investment banking is so back. All of the biggest banks have reported their first-quarter 2024 results, and their earnings have been as good as, if not better than, expected. Higher interest rates ate into the spoils—Bank of America reported yesterday that its profit dropped 18% compared to the same period last year—but investment banking arms did well, especially since many banks increased their fees, and deal making and IPOs started to pick up again. But despite perking up, investment banking activity is still below where it used to be. Strong consumer spending also helped banks out, with credit card income rising and people and businesses continuing to need loans.
[PART 1 OF 8]
NOTE: This is an eight part ME-P series based on a weekend lecture I gave more than a decade ago to an interested group of graduate, business and medical school students. The material is a bit dated and some facts and specifics may have changed since then. But, the overall thought-leadership information of the essay remains interesting and informative. We trust you will enjoy it.
Introduction
The history, function and processes of the investment banking industry, and the rules and regulations of the securities industry and their respective markets, as well as the use of brokerage accounts, margin and debt, will be briefly reviewed in this ME-P series.
An understanding of these concepts is required of all doctors and medical professionals as they pursue a personal investment strategy.
INVESTMENT BANKING AND SECURITIES UNDERWRITING
New economy corporate events of the past several years have provided many financial signs and symptoms that indicate a creeping securitization of the for-profit healthcare industrial complex. Similarly, fixed income medical investors should understand how Federal and State regulations impact upon personal and public debt needs. For, without investment banking firms, it would be almost impossible for private industry, medical corporations and government to raise needed capital.
Introduction
When a corporation such as a physician practice management company (PPMC), or similar entity needs, to raise capital for growth or expansion, there are two methods. Raising debt or equity. If equity is used, the corporation can market securities directly to the public by contacting its current stockholders and asking them to purchase the new securities in a rights offering, by advertising or by hiring salespeople. Although this last example is somewhat exaggerated, it illustrates that there is a cost to selling new securities, which may be considerable if the firm itself undertakes the task.
For this reason, most corporations employ help in marketing new securities by using the services of investment bankers who sell new securities to the general public. Although the investment banking is an exciting and vital industry, many SEC rules regulating it are not. Nevertheless, it is important for all physician executives to understand basic concepts of the industry if raising public money is ever a possibility or anticipated goal. It is also important for individual healthcare investors to understand something about securities underwriting to reduce the likelihood of fraudulent investment schemes or ill-conceived transactions which ultimately result in monetary loss.
Fundamentals of the Investment Banking Industry
Investment bankers are not really bankers at all. The fact that the word banker appears in the name is partially responsible for the false impressions that exist in the medical community regarding the functions they perform.
For example, they are not permitted to accept deposit, provide checking accounts, or perform other activities normally construed to be commercial banking activities. An investment bank is simply a firm that specializes in helping other corporations obtain the money they need under the most advantageous terms possible.
When it comes to the actual process of having securities issued, the corporation approaches an investment banking firm, either directly, or through a competitive selection process and asks it to act as adviser and distributor. Investment bankers, or under writers, as they are sometimes called, are middlemen in the capital markets for corporate securities.
The medical corporation requiring the funds discuss the amount, type of security to be issued, price and other features of the security, as well as the cost to issuing the securities. All of these factors are negotiated in a process known as known as negotiated underwriting. If mutually acceptable terms are reached, the investment banking firm will be the middle man through which the securities are sold to the general public. Since such firms have many customers, they are able to sell new securities, without the costly search that individual corporations may require to sell its own security. Thus, although the firm in need of additional capital must pay for the service, it is usually able to raise the additional capital at less expense through the use of an investment banker, than by selling the securities itself.
The agreement between the investment banker and the corporation may be one of two types. The investment bank may agree to purchase, or underwrite, the entire issue of securities and to re-offer them to the general public. This is known as a firm commitment.
When an investment banker agrees to underwrite such a sale, it agrees to supply the corporation with a specified amount of money. The firm buys the securities with the intention to resell them. If it fails to sell the securities, the investment banker must still pay the agreed upon sum. Thus, the risk of selling rests with the underwriter and not with the company issuing the securities.
The alternative agreement is a best efforts agreement in which the investment banker makes his best effort to sell the securities acting on behalf of the issuer, but does not guarantee a specified amount of money will be raised.
When a corporation raises new capital through a public offering of stock, on might inquire from where does the stock come? The only source the corporation has is authorized, but previously un-issued stock. Anytime authorized, but previously un-issued stock (new stock) is issued to the public, it is known as a primary offering. If it’s the very first time the corporation is making the offering, it’s also known as the Initial Public Offering (IPO). Anytime there is a primary offering of stock, the issuing corporation is raising additional equity capital.
A secondary offering, or distribution, on the other hand, is defied as an offering of a large block of outstanding stock. Most frequently, a secondary offering is the sale of a large block of stock owned by one or more stockholders. It is stock that has previously been issued and is now being re-sold by investors. Another case would be when a corporation re-sells its treasury stock.
Prior to any further discussions of investment banking, there are several industry terms that’s should be defined.
For example, an agent buys or sells securities for the account and risk of another party, and charges a commission. In the securities business, the terms broker and agent are used synonymously. This is not true of the insurance industry.
On the other hand, a principal is one who acts as a dealer rather than an agent or broker. A dealer buys and sells for his own account Finally, the dealer makes money by buying at one price and selling at a higher price. Thus, it is easy to understand how an investment banking firm earns money handling a best efforts offering; they make a commission on every share they sell.
The Securities Act of 1933 (Act of Full Disclosure)
When a corporation makes a public offering of its stock, it is bound by the provisions of the Securities Act of 1933, which is also known as the Act of Full Disclosure. The primary requirement of the Act is that the corporation must file a registration statement (full disclosure) with the Securities and Exchange Commission (SEC); containing some of the following items:
Description of the business entity raising the money.
Biographical data regarding officers and directors of the issuer.
Listing of share holdings of officers, directors, and holders of more than 10% of the issuer’s securities (insiders).
Financial statements including a breakdown of existing capitalization (existing debt and equity structure).
Intended use of offering proceeds.
Legal proceedings involving the issuer, such as suits, antitrust actions or strikes.
Acting in its capacity as an adviser to the corporation, the investment banking firm files out the registration statement with the SEC. It then takes the SEC a period of time to review the information in the registration statement. This is the “cooling off period” and the issue is said to be “in registration” during this time. When the Act written in 1933, Congress thought that 20 days would be enough time from the filing date, until the effective date the sale of securities is permitted.
In reality, it frequently takes much longer than 20 days for the SEC to complete its review. But, regardless of how long it lasts, it’s known as the cooling off period. At the end of the cooling off period, the SEC will either accept the issue or they will send a letter back to the issuer, and the underwriter, explaining that there is incomplete information in the registration statement. This letter is known as a deficiency letter. It will postpone the effectiveness of the registration statement until the deficiency is remedied. Even if initially, or eventually approved, an effective registration does not mean that the SEC has approved the issue.
For example, the following well known disclaimer statement written in bold red ink, is required to be placed in capital letters on the front cover page of every prospectus:
###
THESE SECURITIES HAVE NOT BEEN APPROVED OR DISAPPROVED BY THE SECURITIES AND EXCHANGE COMMISSION NOR HAS THE COMMISSION PASSED UPON THE ACCURACY OR ADEQUACY OF THIS PROSPECTUS. ANY REPRESENTATION TO THE CONTRARY IS A CRIMINAL OFFENSE.
###
During the cooling off period, the investment bank tries to create interest in the market place for the issue. In order to do that, it distributes a preliminary prospectus, more commonly known as a “red herring”. It is known as a red herring because of the red lettering on the front page. The statement on the very top with the date is printed in red as well as the statements on the left hand margin of the preliminary prospectus.
The cost of printing the red herring is borne by the investment bank, since they are trying to market it.. The red herring includes information from the registration statement that will be most helpful for potential medical investors trying to make a decision. It describes the company and the securities to be issued; includes the firm’s financial statements; its current activities; the regulatory bodies to which it is subject; the nature of its competition; the management of the corporation, and what the expected proceeds will be used for. Two very important items missing from the red herringare the public offering price and the effective date of the issue, as neither are known for certain at this point in time.
The public offering price is generally determined on the date that the securities become effective for sale (effective date). Waiting until the last minute enables the investment bankers to price the new issue in line with current market conditions. Since the investment banker uses the red herring to try to create interest in the market place, stock brokers [aka: Registered Representatives (RRs) with a Series # 7 general securities license – After a 2 hour multiple-choice computerize test, I held this license for a decade ) will send copies of the red herring to their clients for whom they feel the issue is a suitable investment. The SEC is very strict on what can be said about an issue, in registration.
In fact, during the pre-filing period (the time when the negotiations are going on between the issuer\and underwriter), absolutely nothing can be said about it to anyone. For example, if the regulators find out that your stock broker discussed with you the fact that his firm was negotiating with an issuer for a possible public offering, he could be fined, or jailed.
During the cooling off period (the time when the red herring is being distributed), nothing may be sent to you; not a research report, nor a recommendation from another firm, or even the sales literature. The only thing you are permitted to receive is the red herring. The red herring is used to acquaint prospects with essential information about the offering. If you are interested in purchasing the security, then you will receive an “indication of interest”, but you can still not make a purchase or send money.
No sales may be made until the effective date; all that can be used to generate interest is the red herring.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES
Posted on April 17, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Stat: 10%. That’s the percentage of Tesla employees that will be impacted by its global workforce reduction. Elon Musk sent an email to employees on Monday informing them of the layoffs, which he said were made to “reduce costs and increase productivity,” according to the WSJ. The move comes as the electric vehicle maker deals with a wider slowdown in EV sales. (the Wall Street Journal)
UnitedHealth Group, reeling from the Change cyberattack, recorded a loss of $1.4 billion in the first quarter. Still, its EPS exceeded expectations and the stock is trading up.
And … physicians made steady pay gains last year, but increases were undercut by inflation rates. See how other specialties fared, according to a report from Medscape.
The social determinants of health can impact a woman’s chance of being up to date with her mammogram, according to a recent Centers for Disease Control and Prevention report. Women are less likely to get a mammogram if they feel socially isolated, have lost a job or don’t have reliable transportation.
And…A major House subcommittee is considering whether to issue another short-term extension on telehealth flexibilities as they continue to evaluate cost and quality issues or to enact permanent changes to virtual care reimbursement. The American Telemedicine Association is pushing Congress to make permanent the Medicare telehealth flexibilities implemented during the COVID-19 pandemic.
The S&P 500® index (SPX) declined 10.41 points (0.2%) to 5,051.41, its lowest close in almost two months; the Dow Jones Industrial Average® ($DJI) advanced 63.86 points (0.2%) to 37,798.97; the NASDAQ Composite® ($COMP) eased 19.77 points (0.1%) to 15,865.25.
The 10-year Treasury note yield gained almost 4 basis points to 4.667%.
The CBOE Volatility Index® (VIX) fell 0.83 to 18.40.
Scaled-back expectations for Fed rate cuts continued to burden interest-rate-sensitive sectors, such as banks and utilities. The KBW Regional Bank Index (KRX) lost 1.4% and ended near a five-month low. The small-cap Russell 2000® Index (RUT) dropped 0.4% and ended at a two-month low.
In other markets, the U.S. dollar index (DXY) strengthened for the fifth consecutive trading day and hit its highest level since late October, reflecting expectations rates will stay elevated.
A closed-end fund (CEF) or closed-ended fund is a collective investment model based on issuing a fixed number of shares which are not redeemable from the fund.
Unlike open-end funds, new shares in a closed-end fund are not created by managers to meet demand from investors. Instead, the shares can be purchased and sold only in the market, which is the original design of the mutual fund, which predates open-end mutual funds but offers the same actively-managed pooled investments.
Posted on April 16, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Here’s where the major stock market benchmarks ended:
The S&P 500 index fell 61.59 points (1.2%) to 5,061.82; the Dow Jones Industrial Average lost 248.13 points (0.7%) to 37,735.11; the NASDAQ Composite® ($COMP) dropped 290.08 points (1.8%) to 15,885.02.
The 10-year Treasury note yield (TNX) surged almost 12 basis points to 4.618%.
The CBOE Volatility Index® (VIX) rose 1.92 to 19.23.
Interest-rate-sensitive sectors like real estate and utilities were among the weakest performers Monday. Technology shares were also under pressure. The small-cap Russell 2000® Index (RUT) shed 1.4% and ended at a two-month low.
In other markets, the U.S. dollar index (DXY) strengthened for the fourth consecutive trading day and hit its highest level since early November, reflecting expectations rates will stay elevated. Volatility based on the VIX jumped near 19.50, its highest level since late October.
Monday’s session also produced technical damage on the charts of benchmarks like the S&P 500, which closed under its 50-day simple moving average, currently around 5,114, for the first time since early November. The S&P 500 has dropped almost 4% from a record intraday high posted March 28th.
And, after a tough funding year for digital health startups, the first quarter of 2024 saw a flurry of deals announced—a “positive signal” that the funding landscape is looking up, according to Adriana Krasniansky, head of research at digital health strategy group and venture fund Rock Health’s advisory arm. Overall, the number of digital health funding deals (133) that closed in Q1 was the highest in six quarters, though the average deal size ($20.6 million) was smaller, according to a Rock Health report. Total funding for digital health startups was $2.7 billion, the lowest level since 2019. An increase in the frequency of deals—even if they’re smaller—is a good sign, according to Krasniansky.
Dental startup Tend aims to simplify the patient billing process via a partnership with health tech startup Cedar, the companies announced on April 11th, 2024. The US spends roughly $165 billion per year on dental services as of 2022, according to professional organization the American Dental Association—but the payment experience can be “opaque” and “confusing,” Matthew Fitzgerald, chief marketing officer at Tend, told Healthcare Brew. “From the outset, Tend has sought to innovate the dental experience by leveraging technology and hospitality to build a company around the patient,” Tend CEO Troy Bage said in a statement. “By partnering with Cedar, we’ll be able to streamline and simplify the payment process for all our members—further enhancing their overall experience with Tend, while unlocking new ways for us to elevate engagement.”
An attractive investment and a polished sales pitch can often hide the underlying costs of the investment, leading some medical professionals to give up a significant portion of the long-term growth of their assets to fees. Fees absolutely matter.
In a good market investors have a propensity to ignore them and in challenging markets they are scrutinized, but in the end no matter what type of market we are in fees do make a substantial difference in your long-term investment returns.
Assessing the Worth of the Investment
The first step in assessing the worth of the investment under consideration is figuring out what the fees actually are. If a medical professional is investing in a mutual fund, these costs are found in mutual fund company’s now obligatory “Fund Facts”.
This manuscript clearly outlines all the fees paid – including upfront fees (or commissions/loads), deferred sales charges, and any switching fees. Fund management expense ratios are also part of the overall cost of ownership. Trading costs within the mutual fund can also impact performance.
The List of Fees Keep Coming … and Coming!
Here is a list of the traditional fees from investing in a mutual fund:
Front end load: It is the commission charged to purchase the fund through a broker or financial advisor. The commission reduces the amount you have available to invest. Thus if you start with $100,000 to invest and the advisor charges a 5 percent front end load, you end up actually investing $95,000.
Deferred Sales Charge (DSC) or back end load: Charge imposed if you sell your position in the mutual fund within a pre-specified period of time (normally five years). It is initiated at a higher start percentage (i.e. as high as 10 percent) and declines over a specific period of time.
Operating Fees: These are costs charged by the mutual fund including the management fee rewarded to the manager for investment services. It also includes legal, custodial, auditing and marketing.
Annual Administration Fee: Many mutual fund companies also charge an additional fee just for administering the account – usually under $150 per year. A 1 percent disparity in fees for a medical professional may not seem like a lot. But fees do make a considerable impact over a longer time period. [For example, a $100,000 portfolio that earns 8 percent before fees, grows to $320,714 after 20 years if the client pays a 2 percent operating fee. In comparison, if the investor opted for a fund that charges a more reasonable 1 percent fee, after 20 years, the portfolio grows to be $386,968 – a divergence of over $66,000! For many investors, this is the value of passive or index investing. In the case of an index fund, fees are generally under 0.5 percent, thus offering even more fee savings over an elongated period of time].
***
[The Carousel of Fees]
Assessment
Fees and expenses can have significant impact on the performance of your investments. Always monitor the costs of an investment program to ensure that fees and expenses are reasonable for the services provided and are not consuming a disproportionate amount of the investment returns.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on April 14, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Texas Governor Greg Abbott has issued a sharp warning about proposed changes to Medicaid, claiming they could “strip millions of Americans” from access to healthcare. In February 2023, the Centers for Medicare & Medicaid Services (CMS) issued a new proposed rule that would change long-standing practices for how states fund the non-federal share of Medicaid payments. In particular, the CMS is pushing for greater oversight of how states use of healthcare provider taxes to help fund their programs.
Democratic lawmakers Sen. Richard Blumenthal and Rep. Andy Kim have partnered up with RepublicanRep. Jen Kiggans to introduce legislation aiming to give army reservists and members of the National Guard that also work for the federal government options on the type of health care plans they can receive. The bill, which could impact thousands of federal employees that are also in the U.S. Army, plans to give this group of Americans the ability to decide whether they want military or civilian health care. The lawmakers said in a shared statement that their proposal will fix current regulations that limit service members who also work for the government to enroll in the cheaper Tricare Reserve Select (TRS) health plan when they also qualify for federal health plans.
Stocks tanked last Friday after the big banks reported underwhelming earnings and the sheen from the Magnificent Seven’s AI-driven surge earlier this week wore off. Meanwhile, oil prices continue to rise near six-month highs as concern grows over geopolitical tensions in the Middle East. The tech sector was highlighted in this market, particularly due to the exceptional performance of a group of mega-cap tech giants last year nicknamed the “Magnificent Seven.” This elite group includes Apple (AAPL), Amazon (AMZN), Alphabet (GOOGL), Meta Platforms (META), Microsoft (MSFT), Nvidia (NVDA) and Tesla (TSLA).
Colleagues know that I enjoy personal coaching and public speaking and give as many talks each year as possible, at a variety of medical society and financial services conferences around the country and world.
These include lectures and visiting professorships at major academic centers, keynote lectures for hospitals, economic seminars and health systems, keynote lectures at city and statewide financial coalitions, and annual keynote lectures for a variety of internal yearly meetings.
Posted on April 13, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Medial Office Equipment Interest Rate Costs
Dr. David E. Marcinko; MBA, MEd, CMP™
[Publisher in Chief]
Physicians, administrators and healthcare entrepreneurs are aware of the compounding effect of interest.However, since interest is deductible as a medical office business expense, many seem to forget about it despite the fact that it must be continually paid until the asset is either purchased or otherwise disposed.
So, what are the various types of interest rates important to the medical practitioner and commodity – money?
[1] Simple Interest
Simple interest is merely the pro rata interest on a loan or deposit and represents the most basic interest rate type.
For example, for every $100 Dr. Bill borrows at 12 percent annual interest, he pays twelve dollars per year. The interest is calculated by multiplying the principal or original amount, by the interest rate in decimal form (100 x .12).
[2] Add-On Interest
Add on interest immediately attaches the annual interest amount, to the principal amount, at the beginning of the payment period. Payments are then made according to the number of years required.
The following formula is useful:
Add-on-Interest minus Payment = Total Interest on Balance/Number of Payments
For example, if Dr. William Needy borrows $10,000 at 8 percent add-on interest, he will repay $10,000 plus $ 800 ($10,000 x 8%) or $10,800, divided by twelve months, for a total of $900 per month, since $ 900/month x 12 months equals $10,800.
[3] Discounted Interest
When using the discounted interest method, the interest amount is deducted from the principal right up front. Notice that this is the opposite of add-on-interest that is applied up front.
For example, if Dr. Bill borrows the same $ 10,000 at a discounted interest rate of 8 percent, he will only receive a $9,200 loan, since $10,000 – $800 is $9,200.
Obviously, the discount method is the most expense way to borrow money.
[4] Annual Percentage Rate
Most financial institutions advertise an annual percentage rates (APR) for loans, deposits and investments. The APR is the periodic interest rate multiplied by the number of periods a year. If the APR is 12 percent, and interest is compounded monthly, you receive (or pay) 1 percent of your balance each month, and the balance shifts with each compounding.
For example, if Dr. Bill deposits $ 100 dollars at 12 percent APR compounded monthly, he receives $ 1 interest the first month (1% of $100), $1.10 the second month (1% of $101), and so forth. If compounding is daily, the interest accumulates at the rate of 1/365 of the APR each day.
Unless interest is compounded annually, the APR will be lower than the effective annual interest rate, discussed below.
[5] Effective Interest Rate
It is important to differentiate between the effective interest rate and the APR, which is often the most prominent figure in advertisements for medical business equipment, consumer goods and financial services (loans, annuities, IRAs, CDs, investment analysis, college funding or retirement planning). Although the APR is the periodic interest rate multiplied by the number of periods per year, the effective annual interest rate is the periodic rate, compounded.
In our case, if the APR is 12 percent, compounded monthly, the monthly interest rate is 1 percent and the effective annual rate is the monthly rate compounded for 12 periods.
Therefore, if your calculation is for a single year, you can treat the effective rate as simple interest. If you deposit (or borrow) $1,000 at 12 percent APR, the effective rate is 12.68 percent, and interest for the first year is about $126.80 (12.68% of $1,000).
For longer periods, you can use the effective interest rate as the periodic interest rate, compounded annually.
[a] “Rule of 72” (Double your Money)
The number of periods required to double a lump sum of money can be quickly estimated by using what is known as the “Rule of 72”. To get the number of periods, usually years, just divide 72 by the periodic interest rate, expressed as a whole number (not a decimal).
For example, if the annual interest rate is 10 percent, it will take about 7.2 years (72/10) to double any lump cache of money. Conversely, you can also calculate the interest rate required to double your money in a given period by dividing 72 by the term.
Thus, to double your money in ten years, you need to earn about 7.2 percent annual interest (72/10) = 7.2%).
[b] “Rule of 78”
According to this method, interest is front end loaded like a home mortgage, or office condominium, to discourage prepayment of a loan and consequently preserve the lender’s profit. In other words, it is a method of calculating installment loan interest rebates.
The number 78 comes from an approved method of accelerated tax depreciation, known as the “Sum of the Years Digits” (SOYD) method (i.e., 12 + 11 + 10 + 9 . . . = 78). This fact is important because, throughout the period of a loan, even though the payments are all the same, the portions that are interest and principal are very different.
Using this method for a one year loan shows that, in the first payment, 15.38 percent of the interest due is paid off, and by the sixth month, 73.08 percent of the interest is paid off. This means, that if a physician makes a one year equipment loan with a total interest charge of $ 100 and pays the loan off in full with the sixth payments, he or she will not get an interest rebate of $ 50, but only $ 26.92, since $ 73.08 of the interest has already been prepaid.
Most ethical lenders use simple interest rates for loan rebates, and the Rule of 78 is unfair according to many authorities.
[c] “Rule of 116”
A derivative of the Rule of 72 is the Rule of 116. This determines the number of years it takes for a principal amount to be tripled and is calculated by dividing the annual interest rate into 116.
The Rules of 72 and 78 are very handy for figuring the amount of interest payments made or growth of funds invested. They can also be used in reverse to calculate at what rate of interest money must be invested to double or triple in a certain number of years.
[6] Medical Equipment Payback Cost Analysis
The payback period, expressed in years, is the length of time that it takes for the medical equipment investment to recoup its initial cost out of the cash receipts it generates. The basic premise is that the quicker the cost of an investment can be recovered, the better the investment is. It is most often used when considering equipment whose useful life is short and unpredictable.
When the same cash flow occurs every year, the formula is as follows:
Investment Required / Net Annual Cash Inflow = Payback Period
Thus, in today’s tightening medical reimbursement atmosphere, practice cost control and expense reduction is the easiest method to increase medical office profitability. Keeping the cost of the commodity money in the form of interest rate charges, as low as possible, will assist in this endeavor
Assessment
And so, how have these rules affected your medical office borrowing costs; if at all? Does these principles apply to the medical student loan crisis, today?
Posted on April 13, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Medical colleague and our financial planning for physicians textbook contributor Michael Burry MD predicted a second inflation surge, and price growth re-accelerated in March,. 2024.
The “Big Short” investor first warned of inflation in April 2020, over two years before it peaked.
Burry expected a recession, rate cuts, and stimulus spending to reignite inflation.
A growing number of drugs are in short supply around the U.S., according to pharmacists.
In the first three months of the year, there were 323 active medication shortages, surpassing the previous high of 320 shortages in 2014, according to a survey by the American Society of Health-System Pharmacists (ASHP) and Utah Drug Information Service. It also amounts to the most shortages since the trade group started keeping track in 2001. “All drug classes are vulnerable to shortages. Some of the most worrying shortages involve generic sterile injectable medications, including cancer chemotherapy drugs and emergency medications stored in hospital crash carts and procedural areas,” ASHP said in a statement.
Scheduling an appointment with a primary care doctor who belongs to a large health system might cause an increase in health care spending, according to a recent study. Such physicians tend to make more referrals to specialists, and emergency room visits and hospitalizations sometimes increase, according to the research out of Harvard T.H. Chan School of Public Health.
In short, physicians who work for health care systems like hospitals are more likely to recommend that patients use other services within those systems, compared with independent physicians. For the study — which was published in JAMA Health Forum, a journal of the American Medical Association — researchers analyzed the experiences of more than 4 million patients in Massachusetts.
UnitedHealth ChairmanStephen Hemsley and other executives sold $102 million in company stock months before a federal antitrust probe became public, Bloomberg reported.
***
Small physician practices are still struggling in the wake of February’s Change Healthcare cyberattack, according to an American Medical Association (AMA) survey released Wednesday.
More than half of ~1,400 respondents (55%) reported that they’ve had to use personal funds to cover their practice’s expenses due to the cyberattack’s effects on cash flow. Practices across the country have been unable to fill prescriptions or process insurance claims as Change Healthcare systems went offline, Healthcare Brew previously reported. About two-thirds of respondents said they’ve experienced restrictions to core functions, such as suspending claim payments (36%), not being able to submit claims (32%), and not being able to obtain electronic remittance advice (39%), according to the survey.
The S&P 500 index fell 75.65 points (1.5%) to 5,123.41, down 1.6% for the week; the Dow Jones Industrial Averagelost 475.84 points (1.2%) to 37,983.24, down 2.4% for the week; the NASDAQ Composite® ($COMP) dropped 267.10 points (1.6%) to 16,175.09, down 0.5% for the week.
The 10-year Treasury note yield (TNX) fell more than 5 basis points to 4.52%, still up about 12 basis points for the week.
The CBOE Volatility Index® (VIX) rose 2.38 to 17.30.
Semiconductor shares were also among the weakest performers Friday as chip makers reversed Thursday’s sharp gains. The Philadelphia Semiconductor Index (SOX) dropped more than 3% and ended with its third straight weekly decline. Energy companies were also under pressure after crude oil prices retreated from the morning rally. Oil futures are still up 20% this year. The small-cap Russell 2000® Index (RUT) lost 1.9% and posted a 2.9% drop for the week.
In other markets, the U.S. dollar index (DXY) strengthened to a five-month high and gained 1.7% this week, reflecting beliefs the hotter-than-expected inflation readings earlier this week will keep interest rates elevated. Volatility based on the VIX jumped to its highest level since late October.
Posted on April 12, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Essay on the Eight-Hundred Pound Gorilla in the Medical Treatment Room
By Dr. David E. Marcinko MBA MEd CMP
[Editor-in-Chief]
According to economist Austin Frakt PhD, and others, there is a school of thought that says Congress is incapable of controlling costs in the Medicare and Medicaid System [CMS].
And, then there is the reality known by all practicing medical professionals regardless of specialty orientation or degree designation. That is to say, CMS really can control healthcare costs and with great ferocity and efficiency, and to non-public sectors as well …. PARADOXICAL?
On Getting What You Wish For
Blogger Ezra Klein opines that one of the dirty little secrets of the health-care system is that Medicare has done a much better job controlling costs than private health insurers.
Of course, we doctors know that the real problem is that Medicare seemingly [think Seinfeld’s character George Costanza] controls costs all too well; but not really. It is just that CMS pays doctors too little and thus it appears costs are controlled. What really is happening is that physician fees are being reduced carte’ blanche.
Nevertheless, and regardless of semantics, CMS will never control costs much more efficiently than private insurance companies or doctors will simply abandon Medicare for related payment models like direct reimbursement or concierge medicine. This is happening right now. Physicians, osteopaths and podiatrists etc, are opting out of Medicare in increasingly large numbers. In a world where there’s only Medicare and Medicare to control costs, doctors can either take the pay cut or stop seeing patients, and stop being doctors. “Taking what they are given – because they’re working for a livin.”
So sorry that this seems like a forehead-palm moment for Ezra, but not for healthcare practitioners or the ME-P!
Too Much Demand Elsewhere
And, as we see from other countries, many young bright folks want to be doctors, even if being a doctor doesn’t make one particularly wealthy [high demand and high eventual supply produces lower provider costs in the long term?]. Think medical tourism.
Not so much the case anymore in this country [lower demand and lower eventual supply produces higher reimbursement costs to the doctor survivors in the very long term?].
Our Domestic World
But, we are not elsewhere. In fact, in our present domestic healthcare ecosystem, when Medicare decides to control costs, many doctors can simply stop accepting Medicare patients, and the politicians will lose their jobs. One political party then declares that Medicare is rationing and will hurt senior citizens. The other party capitulates and pays MDs more [SGR]. Then, the federal budget looks bad as it does now. The circle is complete when one party asserts that Medicare actually can’t contain costs but the private insurance companies will. It all fails, in an unending circular Boolean-like loop of illogic.
Listen Up!
So, listen up AARP, politicians, CMS and seniors as I admonish you to be careful what you wish for [medical cost controls]. It might just come true. As Ezra rightly says; rinse, repeat – rinse, repeat – ad nausea. You simply can’t have it both ways. You either choose to spend less and offend certain cohorts, or spend more and offend different factions. Either way, you’re going to piss someone off. A good healthcare reimbursement system would try to make that decision rationally [a-politically]. But, at least it would make an economics driven decision; wouldn’t it?
Assessment
Is CMS really the eight hundred pound cost-controlled gorilla in the increasingly large Medicare treatment room? Why or why not? Now, relative to the ACA of 2010, please read: The Case for Public Plan Choice in National Health Reform [Key to Cost Control and Quality Coverage], by Jacob S. Hacker, PhD. Link:Jacob Hacker Public Plan Choice
Conclusion
And so, your thoughts and comments on this ME-P are appreciated. Do we have a Medicare cost control efficiency paradox? Or, are the economists just reveling in the publication banal? Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Sponsors Welcomed: And, credible sponsors and like-minded advertisers are always welcomed.