BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Podiatry, a specialized branch of medicine focused on diagnosing and treating conditions of the foot, ankle, and lower extremities, is often perceived as a stable and rewarding career. However, beneath the surface of clinical success and professional prestige lies a growing concern: the emotional and psychological toll of the profession. Stress, burnout, divorce, and practice turmoil are increasingly common among podiatrists, threatening not only their personal well-being but also the sustainability of their practices and the quality of patient care.
The Nature of Stress in Podiatry
Stress in podiatry arises from multiple sources. Clinical responsibilities, administrative burdens, patient expectations, and financial pressures converge to create a high-stakes environment. Podiatrists often work long hours, manage complex cases, and juggle the demands of running a business. The pressure to maintain high standards of care while navigating insurance reimbursements, staffing issues, and regulatory compliance can be overwhelming.
Moreover, podiatrists frequently deal with chronic conditions that require ongoing management rather than quick resolution. This can lead to emotional fatigue, especially when patients experience limited improvement or express dissatisfaction. The cumulative effect of these stressors can erode a podiatrist’s sense of purpose and satisfaction, leading to burnout.
Burnout: A Silent Epidemic
Burnout is characterized by emotional exhaustion, depersonalization, and a reduced sense of personal accomplishment. In podiatry, it manifests as fatigue, irritability, cynicism, and a decline in empathy toward patients. Burnout not only affects the practitioner’s mental health but also compromises patient safety, increases the risk of medical errors, and contributes to staff turnover.
Studies have shown that healthcare professionals, including podiatrists, are at a higher risk of burnout compared to other professions. The isolation of solo practice, lack of peer support, and limited access to mental health resources exacerbate the problem. Without intervention, burnout can progress to depression, substance abuse, and even suicidal ideation.
The personal lives of podiatrists are not immune to the pressures of the profession. Divorce rates among physicians, including podiatrists, are notably high. The demands of the job often leave little time for family, leading to strained relationships and emotional disconnect. The stress of managing a practice can spill over into home life, creating tension and conflict.
Divorce, in turn, can intensify professional stress. Legal proceedings, financial settlements, and emotional upheaval can distract from clinical duties and disrupt practice operations. The dual burden of personal and professional turmoil can be devastating, leading to a downward spiral that affects every aspect of life.
Practice Turmoil: The Business of Healing
Running a podiatry practice is akin to managing a small business. Beyond clinical expertise, podiatrists must master marketing, human resources, billing, and compliance. Practice turmoil can arise from staff conflicts, financial mismanagement, poor patient retention, or changes in healthcare regulations.
For example, a sudden drop in reimbursements or a lawsuit can destabilize a practice. Staff turnover, especially among key personnel like office managers or billing specialists, can disrupt workflow and erode morale. Inadequate leadership or poor communication can lead to a toxic work environment, further fueling stress and burnout.
Addressing the Crisis
To combat these challenges, podiatrists must prioritize self-care, seek support, and implement systemic changes. Here are several strategies:
Mental Health Support: Regular counseling, peer support groups, and wellness programs can help podiatrists process stress and prevent burnout.
Work-Life Balance: Setting boundaries, delegating tasks, and scheduling personal time are essential for maintaining emotional health.
Practice Management Training: Investing in leadership and business education can improve operational efficiency and reduce turmoil.
Staff Engagement: Creating a positive work culture, recognizing achievements, and fostering open communication can enhance team cohesion.
Technology Integration: Utilizing electronic health records, telemedicine, and automation can streamline administrative tasks and reduce workload.
Professional organizations also play a vital role. The American Podiatric Medical Association (APMA) and similar bodies can offer resources, advocacy, and continuing education to support practitioners. Medical schools and residency programs should incorporate wellness training and stress management into their curricula to prepare future podiatrists for the realities of the profession.
Podiatry is a noble and essential field, but it is not without its challenges. Stress, burnout, divorce, and practice turmoil are real and pressing issues that demand attention. By acknowledging these problems and taking proactive steps, podiatrists can safeguard their well-being, strengthen their practices, and continue to provide compassionate care to their patients. The path to healing begins not just with treating others, but with caring for oneself.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
A medical economic white elephant is a healthcare-related investment—such as a hospital, device, or system—that consumes vast resources but fails to deliver proportional value, often becoming a financial burden rather than a benefit to public health.
In economic terms, a white elephant refers to an asset whose cost of upkeep far exceeds its utility. In the medical field, this concept manifests in projects or technologies that are expensive to build, maintain, or operate, yet offer limited practical use, accessibility, or return on investment. These ventures often begin with noble intentions—improving care, advancing technology, or expanding access—but end up draining resources due to poor planning, misaligned incentives, or lack of demand.
One prominent example is the construction of underutilized hospitals or specialty centers in regions with low patient volume. Governments or private entities may invest heavily in state-of-the-art facilities without conducting thorough needs assessments. The result: gleaming buildings with advanced equipment but few patients, high operating costs, and staff shortages. These facilities often struggle to stay open, becoming financial sinkholes that divert funds from more pressing healthcare needs.
Medical devices and technologies can also become white elephants. For instance, robotic surgical systems or high-end imaging machines are sometimes purchased by hospitals to boost prestige or attract patients, despite limited clinical necessity or trained personnel. These devices require costly maintenance, specialized training, and may not significantly improve outcomes compared to traditional methods. When reimbursement rates don’t justify their use, they become liabilities.
***
***
Electronic health record (EHR) systems offer another cautionary tale. While digitizing patient records is essential, some EHR implementations have ballooned into multi-million-dollar projects plagued by inefficiencies, poor interoperability, and user dissatisfaction. Hospitals may invest in proprietary systems that are difficult to integrate with others, leading to fragmented care and wasted resources. In extreme cases, these systems are abandoned or replaced, compounding the financial loss.
The consequences of medical white elephants are far-reaching. They can strain public budgets, increase healthcare costs, and erode trust in institutions. In developing countries, such projects may be funded by international aid or loans, saddling governments with debt while failing to improve population health. Even in wealthier nations, misallocated resources can mean fewer funds for primary care, preventive services, or community health initiatives.
***
***
Avoiding medical white elephants requires rigorous planning, stakeholder engagement, and evidence-based decision-making. Health systems must assess actual needs, forecast demand, and consider long-term sustainability. Cost-benefit analyses should include not only financial metrics but also health outcomes, equity, and accessibility. Transparency and accountability are key to ensuring that investments serve the public good.
In conclusion, the concept of a medical economic white elephant highlights the importance of aligning healthcare investments with real-world needs and outcomes. While innovation and expansion are vital, they must be grounded in practicality and sustainability.
By learning from past missteps, health systems can prioritize value-driven care and avoid the costly pitfalls of overambitious or poorly conceived projects.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Short Interest Theory suggests that high levels of short interest in a stock may actually signal a potential price increase, contrary to traditional bearish interpretations.
Short Interest Theory is a contrarian investment concept that challenges conventional wisdom in financial markets. Traditionally, a high short interest—meaning a large percentage of a company’s shares are being sold short—is seen as a bearish signal, indicating that many investors expect the stock’s price to decline. However, Short Interest Theory flips this assumption, proposing that a high short interest can actually be a bullish indicator, suggesting a potential upward price movement due to a phenomenon known as a “short squeeze.”
To understand this theory, it’s important to grasp the mechanics of short selling. When investors short a stock, they borrow shares and sell them on the open market, hoping to repurchase them later at a lower price and pocket the difference. However, if the stock price rises instead of falling, short sellers face mounting losses. To limit these losses, they may be forced to buy back the stock at higher prices, which increases demand and drives the price up even further. This chain reaction is what’s known as a short squeeze.
Short Interest Theory posits that when short interest reaches unusually high levels, the stock becomes a prime candidate for a short squeeze. Investors who follow this theory look for stocks with high short interest ratios—often measured as the number of shares sold short divided by the stock’s average daily trading volume. A high ratio suggests that it would take many days for all short sellers to cover their positions, increasing the likelihood of a rapid price surge if positive news or buying pressure emerges.
This theory gained widespread attention during the GameStop (GME) saga in early 2021. Retail investors noticed that GME had an extremely high short interest—more than 100% of its float—and began buying shares en masse. This triggered a historic short squeeze, sending the stock price soaring and forcing institutional short sellers to cover their positions at massive losses. The event served as a real-world validation of Short Interest Theory and highlighted the power of collective investor behavior in modern markets.
Despite its appeal, Short Interest Theory is not without risks. Betting on a short squeeze can be speculative and volatile. Not all heavily shorted stocks experience upward momentum; some may continue to decline if the negative sentiment is justified by poor fundamentals or weak earnings. Moreover, timing a short squeeze is notoriously difficult, and investors can suffer significant losses if the anticipated rebound fails to materialize.
In conclusion, Short Interest Theory offers a compelling contrarian perspective on market sentiment. By interpreting high short interest as a potential bullish signal, it encourages investors to look beyond surface-level indicators and consider the dynamics of market psychology and trading behavior. While it can lead to lucrative opportunities, especially in the context of short squeezes, it also demands careful analysis and risk management. As with any investment strategy, understanding the underlying fundamentals and market context is essential for making informed decisions.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Valuing a medical practice involves assessing its financial performance, assets, and intangible factors like goodwill and patient loyalty to determine its fair market worth.
Determining the value of a medical practice is a nuanced process that blends financial analysis with strategic insight. Whether you’re preparing to sell, merge, or bring in a partner, understanding how to value your practice ensures informed decision-making and fair negotiations.
There are several recognized methods for valuing a medical practice, each suited to different scenarios. The most common include the income approach, market approach, asset-based approach, and the rule-of-thumb method.
The income approach focuses on the practice’s ability to generate future earnings. This method involves analyzing historical financial statements, projecting future cash flows, and discounting them to present value using a risk-adjusted rate. It’s particularly useful when the practice has stable revenue and predictable expenses. Key metrics include net income, physician productivity, and reimbursement rates.
The market approach compares the practice to similar ones that have recently sold. It relies on data from comparable transactions, adjusted for differences in size, specialty, location, and profitability. This method is ideal when reliable market data is available, though such data can be scarce for niche specialties or rural practices.
The asset-based approach calculates the value of tangible and intangible assets. Tangible assets include medical equipment, office furniture, and real estate. Intangible assets—like patient records, brand reputation, and goodwill—are harder to quantify but can significantly impact value. Goodwill, for instance, reflects the practice’s reputation, patient loyalty, and referral networks.
The rule-of-thumb method uses industry benchmarks, such as a multiple of annual revenue or earnings. For example, a general practice might be valued at 60–80% of annual gross revenue. While quick and easy, this method oversimplifies and may not reflect the unique strengths or weaknesses of a specific practice.https:/https://medicalexecutivepost.com/2025/03/17/medial-practice-valuation-adjustments//medicalexecutivepost.com/2025/03/17/medial-practice-valuation-adjustments/
Beyond these methods, several qualitative factors influence valuation. These include the size and diversity of the patient base, the practice’s specialty, use of technology (like EHR systems or telemedicine), and whether key physicians will remain post-sale. A practice heavily reliant on one provider may be less valuable than one with a strong team and succession plan.
Timing also matters. Economic conditions, regulatory changes, and shifts in healthcare reimbursement can affect practice value. Tax implications and deal structure—such as asset sale vs. stock sale—should also be considered during negotiations.
Ultimately, valuing a medical practice is both art and science. Engaging a professional appraiser or valuation expert can help ensure accuracy and objectivity. They bring experience, access to market data, and the ability to tailor valuation methods to your specific situation.
In summary, a comprehensive valuation considers financial performance, assets, market trends, and intangible factors. By understanding these elements, practice owners can make strategic decisions that reflect the true worth of their medical enterprise.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on October 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
DEFINED
***
***
A physician practice management corporation (PPMC) is a business entity that provides non-clinical administrative and operational support to medical practices, allowing physicians to focus on patient care while the corporation handles the business side of healthcare.
Physician practice management corporations emerged in response to the increasing complexity of running a medical practice. As healthcare regulations, insurance requirements, and operational costs grew, many physicians found it challenging to manage both clinical responsibilities and business operations. PPMCs offer a solution by taking over the administrative burdens, enabling physicians to concentrate on delivering quality care.
At their core, PPMCs are responsible for a wide range of non-medical services. These include billing and coding, human resources, payroll, marketing, compliance, information technology, and financial management. By centralizing these functions, PPMCs can achieve economies of scale, reduce overhead costs, and improve operational efficiency for the practices they manage. This model is particularly attractive to small and mid-sized practices that may lack the resources to manage these functions independently.
PPMCs typically enter into long-term management agreements with physician groups. In some cases, they may purchase the non-clinical assets of a practice—such as equipment, office space, and administrative staff—while the physicians retain control over clinical decisions and patient care. This arrangement allows for a clear division between medical and business responsibilities, which is essential for maintaining compliance with healthcare regulations like the Stark Law and the Anti-Kickback Statute.
A physician practice management corporation (PPMC) is a business entity that provides non-clinical administrative and operational support to medical practices, allowing physicians to focus on patient care while the corporation handles the business side of healthcare.
Physician practice management corporations emerged in response to the increasing complexity of running a medical practice. As healthcare regulations, insurance requirements, and operational costs grew, many physicians found it challenging to manage both clinical responsibilities and business operations. PPMCs offer a solution by taking over the administrative burdens, enabling physicians to concentrate on delivering quality care.
At their core, PPMCs are responsible for a wide range of non-medical services. These include billing and coding, human resources, payroll, marketing, compliance, information technology, and financial management. By centralizing these functions, PPMCs can achieve economies of scale, reduce overhead costs, and improve operational efficiency for the practices they manage. This model is particularly attractive to small and mid-sized practices that may lack the resources to manage these functions independently.
PPMCs typically enter into long-term management agreements with physician groups. In some cases, they may purchase the non-clinical assets of a practice—such as equipment, office space, and administrative staff—while the physicians retain control over clinical decisions and patient care. This arrangement allows for a clear division between medical and business responsibilities, which is essential for maintaining compliance with healthcare regulations like the Stark Law and the Anti-Kickback Statute.
***
***
One of the key advantages of working with a PPMC is access to capital and advanced infrastructure. PPMCs often invest in state-of-the-art electronic health record (EHR) systems, data analytics tools, and revenue cycle management platforms. These technologies can enhance patient care, streamline operations, and improve financial performance. Additionally, PPMCs may offer strategic guidance on practice expansion, mergers and acquisitions, and payer contract negotiations.
However, the relationship between physicians and PPMCs must be carefully managed. While PPMCs bring valuable expertise and resources, there is a risk that business priorities could overshadow clinical autonomy. To mitigate this, successful PPMCs prioritize physician engagement, transparent governance, and aligned incentives. They work collaboratively with physicians to ensure that business strategies support, rather than hinder, the delivery of high-quality care.
The physician practice management industry has evolved significantly over the past few decades. After a wave of failures in the 1990s due to overexpansion and misaligned incentives, modern PPMCs have adopted more sustainable and physician-centric models. Today, they play a crucial role in helping practices adapt to value-based care, population health management, and other emerging trends in healthcare delivery.
In conclusion, a physician practice management corporation serves as a strategic partner to medical practices, offering the business acumen and operational support needed to thrive in a complex healthcare environment. By offloading administrative tasks and providing access to advanced resources, PPMCs empower physicians to focus on what they do best—caring for patients—while ensuring the long-term success and sustainability of their practices.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Historically, the term “risk management” has brought to mind one subject for the practicing physician – medical malpractice. Unfortunately, physicians today face a multitude of other risks which may be more insidious and daunting than malpractice. It is important to recognize these risks, and to have the appropriate procedures and policies in place to mitigate the risks. These risks come from the federal government, state government, insurance companies, patients, employees, and even prospective employees. Some risks, many unique to small businesses and medical practices, include the following:
Medicare recoupment risk – challenges to coding and subsequent billing by the physician.
Medicare fraud. Numerous laws can be used by the federal government to go after the physician, including the Medicare and Medicaid Anti-Fraud and Abuse Statute, the RICO statute, and the Federal False Claims Act. The recently enacted Patient Protection & Affordable Care Act aims to save money by increasing funding for anti-fraud efforts.
Insurance fraud. An inquiry from Medicare to look for fraud in a physician’s practice is often followed by similar efforts by insurance companies.
The HIPPA Act of 1996 creates new definitions and penalties to use against the physician.
Self referral risks. Federal regulations in this area include the Medicare Anti-Fraud and Abuse Statute, the Medicare Safe Harbor Regulations, and the Stark Amendment.
Federal agency risks. These include regulations from the Occupational Health and Safety Agency (OSHA), Health and Human Services (HHS), the Drug Enforcement agency (DEA), and even the Environmental Protection Agency (EPA).
Anti-trust risks. The Department of Justice (DOJ) and Federal Trade Commission (FTC) formulate regulations in this arena.
Managed care contractual risks. Most managed care contracts require the individual physician rather than the professional corporation to sign the contract, thus placing the physician’s personal assets at risk.
Medical malpractice risks. Although the vast majority of claims are paid by the insurance carrier, there can be other adverse consequences for the physician. These include the risk of increased premiums, non-renewal of policies, and difficulty in getting replacement insurance.
Loss of income due to death or disability. Most physicians recognize the importance of life insurance, but the medical professional is actually much more likely to lose income due to disability at some point in his or her career.
The practicing physician should seek the advice of professionals with expertise in these areas. Every practice should have an experienced attorney on retainer. It is very important to seek advice from fiduciaries – experts who have no conflicts of interest and who can therefore act in the best interest of the client. A Certified Medical Planner is such a fiduciary with training and expertise in these areas.
It can be particularly challenging to find an insurance advisor with no conflicts of interest, as this industry is built upon product sales and commissions. One such insurance advisor is Scott Witt, a fee-only insurance advisor with Witt Actuarial Services (www.wittactuarialservices.com).
Others can be found with an internet search for “fee only insurance advisor”.
Conclusion
Your comments on this ME-P are appreciated. How do you select an advisor? Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now:Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Sponsors Welcomed:And, credible sponsors and like-minded advertisers are always welcomed.
Posted on October 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters and A.I.
***
***
Dentistry is often perceived as a stable and rewarding profession, yet beneath the surface lies a troubling reality: dentists face disproportionately high levels of stress, burnout, divorce, practice turmoil, and even suicide. These issues stem from a complex interplay of emotional, financial, and professional pressures that uniquely affect dental practitioners.
Emotional and Psychological Strain
Dentists frequently operate in high-stakes environments where precision is paramount. The pressure to deliver flawless results while managing patient anxiety and discomfort can be overwhelming. Many patients fear dental procedures, and this fear often manifests as hostility or distrust, placing emotional strain on the dentist. Over time, the cumulative effect of these interactions can lead to compassion fatigue and emotional exhaustion.
Unlike other medical professionals who often work in collaborative hospital settings, dentists typically operate in solo or small group practices. This isolation can limit opportunities for peer support and professional camaraderie. Without a strong support network, dentists may struggle to process the emotional toll of their work, increasing their vulnerability to depression and burnout.
Financial and Business Pressures
Running a dental practice involves more than clinical expertise—it requires business acumen. Dentists must manage overhead costs, staff salaries, insurance reimbursements, and patient billing. The financial burden of student loans, often exceeding six figures, adds to the stress. Economic downturns or shifts in healthcare policy can destabilize practices, leading to turmoil and uncertainty.
***
***
Work-Life Imbalance and Marital Strain
The demanding nature of dentistry often spills into personal life. Long hours, administrative responsibilities, and the emotional weight of patient care can leave little time or energy for family. This imbalance contributes to high divorce rates among dentists. The stress of maintaining a successful practice while nurturing personal relationships can become untenable, especially without adequate coping mechanisms.
Burnout and Suicide Risk
Burnout in dentistry is alarmingly common. A study by the American Dental Association found that 84% of dentists report experiencing burnout at some point in their careers.
Addressing these challenges requires systemic change. Mental health support, peer mentorship, and business education should be integrated into dental training. Encouraging open conversations about stress and providing resources for emotional well-being can help reduce stigma and promote resilience.
By acknowledging the hidden struggles of dentistry, the profession can move toward a healthier, more sustainable future.
Why It Is Difficult to Practice Medicine Part-Time Today?
In the past, part-time medical practice offered physicians a flexible way to balance professional responsibilities with personal or family commitments. Today, however, the healthcare environment has evolved in ways that make part-time medicine increasingly challenging. From administrative burdens to economic pressures and patient expectations, the obstacles are both systemic and personal.
One of the most significant barriers is the rise in administrative complexity. Physicians are now required to navigate electronic health records (EHRs), comply with insurance documentation, and meet regulatory standards such as HIPAA and MACRA. These tasks consume hours of non-clinical time, which is difficult to compress into a part-time schedule. Even seeing fewer patients doesn’t exempt part-time doctors from the same documentation and compliance requirements as their full-time counterparts.
***
***
Another challenge is financial viability. Many physicians are paid based on productivity metrics, such as Relative Value Units (RVUs), which reward volume over quality. Part-time practitioners often struggle to meet these benchmarks, resulting in lower compensation and reduced benefits. Additionally, malpractice insurance premiums and licensing fees remain fixed regardless of hours worked, further eroding the financial appeal of part-time practice.
Continuity of care is also a concern. Patients increasingly expect immediate access to their providers, especially in primary care and specialties like psychiatry or pediatrics. Part-time physicians may not be available for urgent issues, leading to fragmented care and dissatisfaction. This can strain relationships with patients and colleagues who must cover gaps in availability.
From a professional standpoint, part-time physicians may face limited career advancement. Leadership roles, academic appointments, and research opportunities often favor full-time commitment. There’s also a perception—sometimes unfair—that part-time doctors are less dedicated or less competent, which can affect peer respect and influence within medical institutions.
Technology, while beneficial, adds another layer of complexity. Telemedicine, remote monitoring, and digital communication tools have expanded access but also increased the expectation for constant availability. Part-time physicians may find it difficult to manage asynchronous messages, follow-ups, and virtual visits without extending their work hours beyond what they intended.
***
***
Lastly, burnout and work-life balance—ironically one of the reasons doctors seek part-time roles—can still be elusive. The pressure to maintain clinical excellence, stay updated with medical advancements, and meet patient needs doesn’t diminish with reduced hours. In fact, squeezing these responsibilities into fewer days can intensify stress rather than alleviate it.
In conclusion, while part-time medical practice may seem like a solution to modern work-life challenges, the reality is far more complex. The structure of today’s healthcare system, combined with economic, technological, and cultural pressures, makes it difficult for physicians to thrive in part-time roles. Addressing these challenges will require systemic reform, flexible compensation models, and a cultural shift in how we value and support diverse medical careers.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on October 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Efficient New Patient-Scheduling Models
[By Staff Writers]
Most doctors follow a linear (series-singular) time allocation strategy for scheduling patients (i.e., every 15 or 20 minutes). This can create bottlenecks because of emergencies, late patients, traffic jams, absent office personal, paperwork delays, etc.
Therefore, as first proposed by Dr. Neal Baum, a practicing urologist in New Orleans, one of these three newer scheduling approaches might prove more useful.
Customized Scheduling
The bottleneck problem may be reduced by trying to customize, estimate or project the time needed for the patient’s next office visit.
For example: CPT #99211 (15 minutes), #99212 (25 minutes), #99213 (35 minutes), or #99214 (45 minutes). Occasionally, extra time is need, and can be accommodated, if the allocated times are not too tightly scheduled.
Wave Scheduling
Most patients do not mind a brief 20-30 minute wait prior to seeing the doctor. Wave scheduling assumes that no patient will wait longer than this time period, and that for every three patients; two will be on time and one will be late.
This model begins by scheduling the three patients on the hour; and works like this.The first patient is seen on schedule, while the second and third wait for a few minutes. The later two patients are booked at 20 minutes past the hour and one or both may wait a brief time. One patient is scheduled for 40 minutes past the hour. The doctor then has 20 minutes to finish with the last three patients and may then get back on schedule before the end of the hour.
Bundle Scheduling
Bundling involves scheduling like-patient activities in blocks of time to increase efficiency.
For example, schedule minor surgical checkups on Monday morning, immunizations on Tuesday afternoon, and routine physical examinations on Wednesday evening, or make Thursday kid’s day and Friday senior citizens day. Do not be too rigid, but by scheduling similar activities together, assembly-line efficiency is achieved without assembly line mentality, and allows you to develop the most economically profitable operational flow process possible for the office.
Patient Self Scheduling (Internet Based Access Management)
New software programs allow patients to schedule their own appointments over the internet. The software allows solo or individual group physicians with a practice to set their own parameters of time, availability and even insurance plans. Through a series of interrogatories, the program confirms each appointment. When the patient arrives, a software tracker communicates with office staff and follows the patients from check-in, to procedures, to checkout.
Today, many hospitals have even abandoned the check-in or admissions, department. It has been replaced by Access Management.
Assessment
The traditional inear patient scheduling system is slowly being abandoned by modern medical practitioners; an all venues (medical practices, clinics, hospitals and various other healthcare entireties).
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Yourmedical practice. Your personal goals. Your financial plan. Our experienced confirmation guide.
***
***
When you know exactly where you are today, have a vision of where you want to be tomorrow, and have trusted counsel at your side, you have already achieved so much success. Marcinko Associates works to keep you at that level of confidence every day. We use a comprehensive economic process to uncover what’s most important to you and then develop a financial strategy that gives you the highest probability of achieving your monetary goals.
We assess, plan, and opine for your success
To accurately see where you are today, chart a strategic path to your goals and help you make the most informed decisions to keep you on financial track, our key services for physicians and high net worth medical clients include:
Investment Portfolio Review
Fee, Charge and Cost Review
Comprehensive Financial Planning
Insurance Reviews
Estate Planning
Investment and Asset Management Second Opinions
We take a deep dive into your financial retirement plans
Physicians and dental employers now have options for how to design and deliver retirement benefits and we can help you make the best choice for your healthcare business. Our services for retirement plans include:
Fee, Charges & Fiduciary Review
Portfolio Analysis
Single Employer Retirement Plan Advisory
Retirement Plans Risk Analysis
Capital Funding and Financing
Business Planning and Practice Valuations
Career Development
and more!
We take a broad and balanced look at your financial life life
We coordinate our recommendations with your other advisors, including attorneys, accountants, insurance professionals and others, to ensure each decision is consistent with your goals and overall strategy. For example, through our partnerships we offer physician colleagues deeper expanded advisory services, like:
Posted on September 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
BREAKING NEWS
Law enforcement officials in Utah released a video of the suspected shooter in the assassination of Turning Point USA co-founder and CEO Charlie Kirk, saying that the person wore Converse tennis shoes and left a hand print and a shoe print at the scene.
The suspect in Charlie Kirk’s assassination has been identified as Tyler Robinson, a 22-year-old Utah resident. Law enforcement sources told the Daily Mail that Robinson was taken into custody as the alleged assassin who killed Kirk at a rally at Utah Valley University on Wednesday.
Before today, forensic podiatry has even made it into the public zeitgeist with the hit TV show “Bones” which premiered on September 13, 2005, and concluded on March 28, 2017, airing for 246 episodes over 12 seasons. The show was based on forensic anthropology and forensic archaeology, with each episode focusing on the mystery behind human body remains brought in for examination and identification.
In one show, eight pairs of dismembered feet washed ashore after a flood on the U.S.-Canada border, but things didn’t add up when only seven pairs of feet were identified as research corpses from a nearby university body farm.
When the fictional Canadian forensic podiatrist Dr. Douglas Filmore took the remains back to Canada, he had to form a jurisdictional alliance with the United States to match the pairs of feet and identify the victims. A rare and expensive pair of sneakers led the team to the victim’s murderer.
In 2016, an actual forensic podiatry club was started at the Barry University School of Podiatric Medicine. And, a formal class covering aspects of forensic podiatry is held at the New York College of Podiatric Medicine. Students exit the class with an in depth knowledge of forensic podiatry and other legal knowledge applicable to current cases.
More expertly, real-life colleague Michael Steven Nirenberg DPMactually testified in the murder trial of defendants Kailie Brackett and Donnell Dana with the state calling three witnesses to testify, including the podiatrist who claimed Brackett’s footprints match the ones found in blood at the apartment of the victim, Kimberly Neptune. The forensic podiatrist focused on the footprints discovered at Neptune’s apartment, using prints and images of the defendant’s feet taken by law enforcement. After study, he claimed the prints at the scene bore a resemblance to Kailie Brackett’s in the width of the foot. The defense questioned the field of forensic podiatry and pressed Dr. Nirenberg on whether the measurements would be altered depending on how thick the sock covering the foot was woven.
Dr. Nirenberg was also interviewed on National Public Radio’s Morning Edition on April 14th 2023 about the gait of the bombing suspect associated with the capital riot on Wednesday January 6th, 2021. Dr. Nirenberg is president of the American Society of Forensic Podiatry and co-editor of the textbook: “Forensic Gait Analysis: Principles and Practice”. The bombing suspect had placed bombs at the DNC and RNC headquarters in Washington, DC on the night before. NPR asked Dr. Nirenberg to comment on the features of the person’s gait.
Additionally, Nirenberg was interviewed by Nancy Grace on her TV show Crime Stories. Grace interviewed Nirenberg about his forensic podiatry work in helping to solve the murder of a mother of 3 who was killed in a church. The case remains unsolved. The episode, “Fitness-Mom Missy Bevers Bludgeoned Dead in Creekside Church” aired June 6th, 2024 and is available online at Merit+ TV.
And, Netflix’s 2023 docu-series, “Till Murder Do Us Part”, recounts the killings of Derek and Nancy Haysom by including a series of interviews with a cast of real people. The four-part docu-series revolves around the unpacking of how a wealthy couple was murdered in Virginia in 1985. It also focuses on how the suspects, Elizabeth Haysom, and her boyfriend, Jens Soehring, betrayed each other during the trial. Dr. Sarah Reel DPM was the forensic podiatrist who was involved with Jens’ and Elizabeth’s footprint examination. Dr. Reel pointed out that, statistically, there was no difference “between a bare footprint and a socked footprint.” The doctor suggested that Jens’ reference footprint matched closely with the crime scene footprint.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Medicine today is vastly different than a generation ago, and all health care professionals need new skills to be successful and reduce the emerging risks outlined in this textbook, as well as the “unknown-unknowns” elsewhere. Traditionally, the physician was viewed as the “captain of the ship”. Today, their role may be more akin to a ship’s navigator, using clinical, teaching skills and knowledge to chart the patient’s course through a confusing morass of insurance requirements, fees, choices, rules and regulations to achieve the best attainable clinical outcomes.
This new leadership paradigm includes many classic business school principles, now modified to fit the decade long PP-ACA, the era of health reform, and modern technical connectivity and EMRs.
Thus, the physician must be a subtle guide on the side; not bombastic sage on the stage. These, newer health 3.0 leadership philosophies might include:
•Negotiation – working to optimize appropriate treatment plans; ie., quality of life versus quantity of life, •Team play – working in concert with other allied healthcare professionals to coordinate care delivery ,ithin a clinically appropriate and cost-effective framework; •Working within the limits of competence – avoiding the pitfalls of the medical generalist versus the specialist that may restrict access to treatment, medications, physicians and facilities by clearly acknowledging when a higher degree of service is needed on behalf of the patient – all while embracing holistic primary care; •Respecting different cultures and values – inherent in the support of the medical Principle of Autonomy is the acceptance of values that may differ from one’s own. As the US becomes more culturally hetero geneous, medical providers are called upon to work within, and respect, the socio-cultural and/or spiritual framework of patients, students and their families; •Seeking clarity on what constitutes marginal care – within a system of finite resources; providers are called upon to openly communicate with patients regarding access to marginal medical information and/or treatments. •Supporting evidence-based practice – healthcare providers, should utilize outcomes data to reduce variation in treatments to achieve higher efficiencies and improved care delivery thru evidence based medicine [EBM]; •Fostering transparency and openness in communications – healthcare professionals should be willing, and prepared, to discuss all aspects of care, especially when discussing end-of-life issues or when problems arise; •Exercising decision-making flexibility – treatment algorithms, templates and clinical pathways are useful tools when used within their scope; but providers must have the authority to adjust the plan if circumstances warrant.
Becoming skilled in the art of listening and interpreting — In her ground-breaking book, Narrative Ethics: Honoring the Stories of Illness, Rita Charon, MD PhD, a professor at Columbia University, writes of the extraordinary value of using the patient’s personal story in the treatment plan. She notes that, “medicine practiced with narrative competence will more ably recognize patients and diseases; convey knowledge and regard, join humbly with colleagues, and accompany patients and their families through ordeals of illness.” In many ways, attention to narrative returns medicine full circle to the compassionate and caring foundations of the patient-physician relationship.
These thoughts represent only a handful of examples to illustrate the myriad of new skills that tomorrows’ healthcare professionals must master in order to meet their timeless professional obligations of compassionate care and contemporary treatment effectiveness; all within the context modern risk management principles.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on July 21, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Rick Kahler MSFP CFP™
***
***
When Maria needed $400,000 for a down payment on a new home, her broker at a large Wall Street firm offered a solution: “Don’t sell investments and trigger capital gains. Just take out a margin loan.”
A margin loan is a line of credit from a brokerage firm, secured by the client’s investment portfolio. It offers quick access to cash with no immediate tax consequences and minimal paperwork. But the convenience comes at a cost. As of mid-2025, margin loan interest rates range from 6.25% to over 11%.
Margin loan recommendations are often presented by brokers as tax-savvy strategies that allow clients to access “tax-free” cash while keeping their portfolios intact. In many cases, however, the math benefits the advisor more than the investor. The cost of borrowing often exceeds what an investor is likely to earn by holding on.
For example, let’s assume an interest rate of 7.5% on Maria’s $400,000 margin loan. While borrowing delayed the payment of $20,000 in capital gains tax, she will eventually have to pay that tax anyway unless she holds the investments until her death. Two years later, with portfolio returns of 4% annually, she had earned around $32,000 from the $400,000 in investments she might have sold. Meanwhile, she had paid $60,000 in interest—leaving her some $28,000 worse off. That’s without factoring in ongoing interest payments, or the risks of a margin call if the investments securing the loan drop in value.
Why do advisors keep recommending margin loans? Because selling investments reduces the portfolio size and the advisor’s fee. Borrowing keeps the portfolio intact and the compensation unchanged—while the firm receives additional income from interest on the loan. In some cases, advisors suggest using margin loans to buy more investments, increasing both the portfolio and the fee they collect.
None of this is illegal. But when the borrowing cost is higher than expected returns and the advisor benefits financially, the ethics are questionable. The client takes the risk, while the advisor keeps the revenue.
This kind of conflict appears more often in portfolios where compensation is tied to asset volume and the company’s primary culture rewards gathering assets over delivering unbiased advice. By contrast, fee-only financial planning and investment advisors typically operate on simpler hourly, flat, or tiered fee structures. Their compensation doesn’t depend on whether a client borrows, sells, or holds. The culture of the firm focuses on conflict-free advice aligned with the client’s best interest.
Wall Street brokers are often held to a fiduciary standard, but structure still matters. In 2024 the SEC reported their examinations of brokers would continue to focus on advisor recommendations unduly influenced by the company’s compensation and incentives.
There are rare situations where a margin loan may be appropriate. A client with large unrealized gains might use a short-term margin loan to minimize taxes. An elderly investor might borrow tax-free rather than sell assets that will receive a step-up in basis at their death. Even in those cases, the math must be exact and the client must clearly understand the risks, including the possibility of a margin call.
If your advisor recommends a margin loan, especially to buy more investments, ask strong questions. What’s the interest rate? What return is realistic? What are the tax consequences of selling? How does this affect the advisor’s income?
In a high-rate, low-return environment, margin loans rarely favor the client. The exceptions are narrow. The risks are significant. And the conflict of interest is measurable.
Sometimes the smartest move is the simplest: sell what you need, pay the tax, and leave leverage out of your plan.
Posted on July 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A.I.
***
***
Stocks: Markets shrugged off President Trump’s weekend threat of 30% levies against the EU and Mexico, as well as his proposed 100% secondary tariffs against Russia today. Stocks eked out a win across the board, with the NASDAQ climbing to a new record close.
Commodities: Oil prices fell while gold took a breather, but the big winner was orange juice futures, which hit a four-month high thanks to Trump’s promise of 50% tariffs on all imports from Brazil. Coffee prices also climbed.
Posted on July 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A.I.
***
***
Medical doctors, dentists, and podiatrists have to undergo extensive training before they can practice medicine independently. Once they receive training, there are opportunities to increase pay and prestige in the medical field through a series of promotions. As a doctor, how much training, experience and skills you have can determine your ability to move upward in these levels. But, personal branding strategies may even be more vital in today’s social media age?
***
Physician, medical and healthcare branding is more than just the creation of logos, taglines, or specific brand messaging. It’s about creating a meaningful connection between your mission, vision and values and the people served – from patients and their families to local and global communities.
While there are many different types of branding strategies in marketing science, they all share key elements that serve as the foundation for the strategy. These 9 elements for all physicians and medical professionals include the following:
Brand purpose: The reason the physician is in practice and what he/she is trying to achieve.
Brand vision: The ideas and goals behind the dentist which serve as inspiration for practice growth.
Brand values: The osteopaths beliefs and what they stand for.
Target audience: The demographic(s) and patient targets that the podiatrist is aiming to reach.
Market analysis: An analysis of the marketplace that identifies gaps where the chiropractor has an opportunity to position him/her self based on a unique value proposition.
Awareness goals: The initiatives the doctor will take in order to reach a target market patient demographic.
Brand personality: The human-like attributes of the physician that will help build relationships with patients, consumers and other physicians and practitioners.
Brand voice: The language and tone the doctor uses to communicate with patients, physicians and consumers.
Brand tagline: A memorable slogan that sums up the physician and their medical offering in a few choice words.
And so, physician branding is the development of a easily recognizable identity for a medical practice, clinic or healthcare organization that helps to shape perception by current and prospective patients and the wider world.
Posted on June 29, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A.I.
***
***
Markets: That feeling when you have a $10 trillion rally. To wit:
The S&P 500 closed at a record high this week despite a brief dip as trade tensions with Canada ratcheted up. That puts the index about 20% up from its April low, when the broad tariff announcement sent it spiraling, and up ~5% for the year.
NVIDIA also hit an all-time high, and it keeps edging closer to becoming the first company to hit a $4 trillion valuation.
Life planning and behavioral finance as proposed for physicians and integrated by the Institute of Medical Business Advisors Inc., is unique in that it emanates from a holistic union of personal financial planning, human physiology and medical practice management, solely for the healthcare space. Unlike pure life planning, pure financial planning, or pure management theory, it is both a quantitative and qualitative “hard and soft” science, with an ambitious economic, psychological and managerial niche value proposition never before proposed and codified, while still representing an evolving philosophy. Its’ first-mover practitioners are called Certified Medical Planners™.
Financial Life Planning is an approach to financial planning that places the history, transitions, goals, and principles of the client at the center of the planning process. For the financial advisor or planner, the life of the client becomes the axis around which financial planning develops and evolves.
Financial Life Planning is about coming to the right answers by asking the right questions. This involves broadening the conversation beyond investment selection and asset management to exploring life issues as they relate to money.
Financial Life Planning is a process that helps advisors move their practice from financial transaction thinking, to life transition thinking. The first step is aimed to help clients “see” the connection between their financial lives and the challenges and opportunities inherent in each life transition.
But, for informed physicians, life planning’s quasi-professional and informal approach to the largely isolate disciplines of financial planning and medical practice management is inadequate. Today’s practice environment is incredibly complex, as compressed economic stress from HMOs managed care, financial insecurity from insurance companies, ACOs and VBC, Washington DC and Wall Street; liability fears from attorneys, criminal scrutiny from government agencies, and IT mischief from malicious electronic medical record [eMR] hackers. And economic bench marking from hospital employers; lost confidence from patients; and the Patient Protection and Affordable Care Act [PP-ACA] more than a decade ago. All promote “burnout” and converge to inspire a robust new financial planning approach for physicians and most all medical professionals.
The iMBA Inc., approach to financial planning, as championed by the Certified Medical Planner™ professional certification designation program, integrates the traditional concepts of financial life planning, with the increasing complex business concepts of medical practice management. The former topics are presented in this textbook, the later in our recent companion text: The Business of Medical Practice [Transformational Health 2.0 Skills for Doctors].
***
***
For example, views of medical practice, personal lifestyle, investing and retirement, both what they are and how they may look in the future, are rapidly changing as the retail mentality of medicine is replaced with a wholesale and governmental philosophy. Or, how views on maximizing current practice income might be more profitably sacrificed for the potential of greater wealth upon eventual practice sale and disposition.
Or, how the ultimate fear represented by Yale University economist Robert J. Shiller, in The New Financial Order: Risk in the 21st Century, warns that the risk for choosing the wrong profession or specialty, might render physicians obsolete by technological changes, managed care systems or fiscally unsound demographics. OR, if a medical degree is even needed for future physicians?
Say, what medical license?
Dr. Shirley Svorny, chair of the economics department at California State University, Northridge, holds a PhD in economics from UCLA. She is an expert on the regulation of health care professionals who participated in health policy summits organized by Cato and the Texas Public Policy Foundation. She argues that medical licensure not only fails to protect patients from incompetent physicians, but, by raising barriers to entry, makes health care more expensive and less accessible. Institutional oversight and a sophisticated network of private accrediting and certification organizations, all motivated by the need to protect reputations and avoid legal liability, offer whatever consumer protections exist today.
Yet, the opportunity to revise the future at any age through personal re-engineering, exists for all of us, and allows a joint exploration of the meaning and purpose in life. To allow this deeper and more realistic approach, the informed transformation advisor and the doctor client, must build relationships based on trust, greater self-knowledge and true medical business management and personal financial planning acumen.
[A] The iMBA Philosophy
As you read this ME-P website, we hope you will embrace the opportunity to receive the focused and best thinking of some very smart people. Hopefully, along the way you will self-saturate with concrete information that proves valuable in your own medical practice and personal money journey. Maybe, you will even learn something that is so valuable and so powerful, that future reflection will reveal it to be of critical importance to your life. The contributing authors certainly hope so.
At the Institute of Medical Business Advisors, and thru the Certified Medical Planner™ program, we suggest that such an epiphany can be realized only if you have extraordinary clarity regarding your personal, economic and [financial advisory or medical] practice goals, your money, and your relationship with it. Money is, after only, no more or less than what we make of it.
Ultimately, your relationship with it, and to others, is the most important component of how well it will serve you.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on April 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
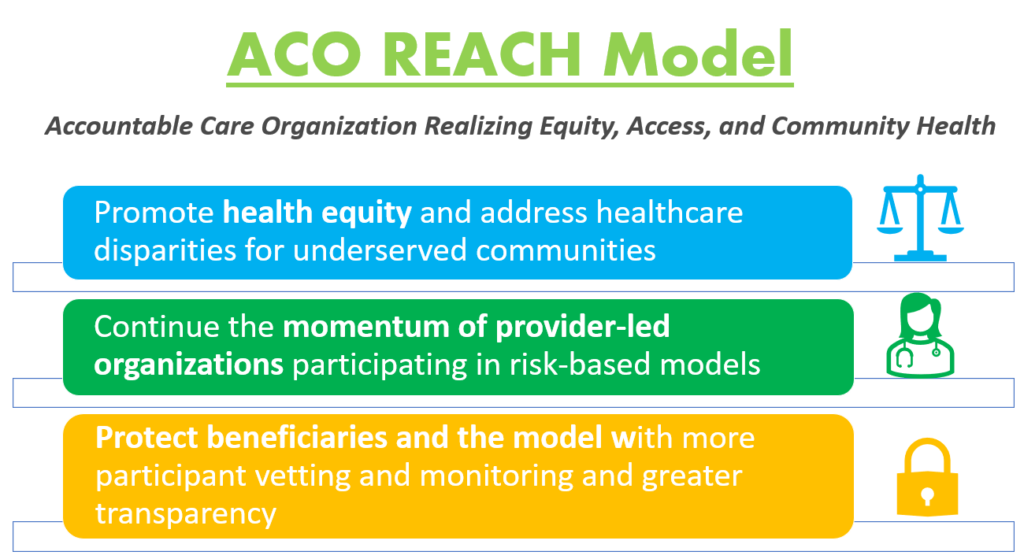
ACCOUNTABLE CARE ORGANIZATIONS
Realizing Equity, Access, and Community Health
By Staff Reporters
***
***
Model Overview
The ACO REACH Model provides novel tools and resources for health care providers to work together in an ACO to improve the quality of care for people with Traditional Medicare. REACH ACOs are comprised of different types of providers, including primary and specialty care physicians.
The ACO REACH Model makes important changes to the previous Global and Professional Direct Contracting (GPDC) Model which include:
***
***
Promote Provider Leadership and Governance. The ACO REACH Model includes policies to ensure doctors and other health care providers continue to play a primary role in accountable care. At least 75% control of each ACO’s governing body generally must be held by participating providers or their designated representatives, compared to 25% during the first two Performance Years of the GPDC Model. In addition, the ACO REACH Model goes beyond prior ACO initiatives by requiring at least two beneficiary advocates on the governing board (at least one Medicare beneficiary and at least one consumer advocate), both of whom must hold voting rights.
Protect Beneficiaries and the Model with More Participant Vetting, Monitoring and Greater Transparency. CMS will ask for additional information on applicants’ ownership, leadership, and governing board to gain better visibility into ownership interests and affiliations to ensure participants’ interests align with CMS’s vision. We will employ increased up-front screening of applicants, robust monitoring of participants, and greater transparency into the model’s progress during implementation, even before final evaluation results, and will share more information on the participants and their work to improve care. Last, CMS will also explore stronger protections against inappropriate coding and risk score growth.
Profitability ratios measure a company’s ability to generate income relative to revenue, balance sheet assets, operating costs, and equity. Common profitability financial ratios include the following:
The gross margin ratio compares the gross profit of a company to its net sales to show how much profit a company makes after paying its cost of goods sold:
Gross margin ratio = Gross profit / Net sales
The operating margin ratio, sometimes known as the return on sales ratio, compares the operating income of a company to its net sales to determine operating efficiency:
Operating margin ratio = Operating income / Net sales
The return on assets ratio measures how efficiently a company is using its assets to generate profit:
Return on assets ratio = Net income / Total assets
The return on equity ratio measures how efficiently a company is using its equity to generate profit:
Return on equity ratio = Net income / Shareholder’s equity
Patient satisfaction occurs when patient perceptions exceed their expectations. They get an intangible “something extra” from their visit, above what they paid for. When patient expectations match their perceptions, mutual obligations are fulfilled, making both practitioner and patient “break-even”.
The clinical result, within a relevant range, is only part of the patient’s perceptions. Numerous sub-conscious impressions comprise the remainder. We’ve all had patients love us despite a less than optimal result. We’ve all had patients angrily leave the practice over some non-clinical matter like a trivial billing dispute. A patient’s perception of any health care service is colored by a vast array of prior experiences that set up current expectations. The patient is pleased to the extent that his current perceptions exceed his/her pre existing expectations. This encompasses far more than the clinical result (within a relevant range), and includes such non-treatment issues as the demeanor of the staff, condition of the physical premises, psychological comfort during the visit, etc.
Remember, all patients talk about you anyway. In the past, a happy patient told four others about what a nice doctor you are. Today, patients post website comments or blogs immediately after their visits. They are more likely to complete treatment and follow instructions, thus obtaining a better medical outcome, and, generating additional fees for the practice. They pay quicker, cause less bad-debt and help create a pleasant environment for us to work in.
An unhappy patient vehemently tells nine others, onground or online, what a nasty greedy rip-off artist you are. Sad, but true! They are not as likely to complete treatment, thus incurring a less than optimal result, and generate fewer fees. They pay slower, if at all, create a stressed environment and detrimentally affect the attitude of other patients in the office.
Try to eliminate problems that might cause negative perceptions (i.e., a filthy restroom) and implement controls that help assure positive perceptions. Patient satisfaction is a soft managerial science. It is a numbers game. Most patients don’t pre-define what would be “acceptable” from this encounter, but have vaguely defined ranges of prior expectations anyway, gleaned from a lifetime of health care related experience. Any variance between these this “acceptable” range of expectations and each trivial encounter invokes some degree positive or negative feeling in the patient.
***
***
The total perception of the office experience is an aggregate of multiple trivial, often subliminal, observations. Patient satisfaction is an intangible and amorphous process complicated by:
Inter patient variables: Significant differences between patients in their “expectations”. Intra patient variables: A single patient can perceive the same thing or situation differently at different times, depending on uncontrollable variables like mood, or, context of occurrence which may (sometimes and/or partially) be controllable by the practice. Luck of the draw” in physical variables: Does Sally or Mary escort the patient to the exam room? Was it the blue or green exam room? Did the last patient to use the rest room, five minutes ago, leave a disgusting mess? Heterogeneous staff variables: Even with appropriate training, people are not machines and have their own quirks.
ASSESSMENT
By proactively anticipating the entire visit, from the patient’s perspective, the practitioner can structure and arrange things such that most patients have, mostly positive perceptions, most of the time. This can be done despite all the potential hetero-genicity of the above factors. Patient satisfaction can be improved in any office, and can be done by anyone.
CONCLUSION
Because patient satisfaction is a multi-faceted amorphous subject, there are multiple correct approaches to the subject and no “cook book” recipe on how to proceed. Try and get the big picture. Identify the worst areas and fix them. Identify the best areas and reinforce them. Proceed slowly. It can be done one facet at a time. Adapt things to your own managerial style and personality. Be completely open to suggestion and change.
Finally, be aware that patient relationship and satisfaction implementation strategies frequently overlap.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on March 31, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
[Reviewing Terms, Conditions and Selling Agreements]
By Dr. Charles F. Fenton III JD
***
***
Dealing with many issues concerning the actual contract that affect the purchase or sale of a medical practice can be daunting. For example, this chapter will not deal with issue of determining whether or not a physician should retire. Nor will it determine the proper Fair Market Value [FMV] of the practice. However, physicians may be assisted in both instances by a medically focused financial advisor, or valuation specialist. [AVA, CPA-CVA, Certified Medical Planner™; etc] working in conjunction with an experience health care contract attorney to act as an advocate and determine certain contingencies that might occur, and protect him/her from them.
THE PARTIES
The first determination is whether the party at interest is an individual, group of individuals, or an entity (such as a partnership, limited liability partnership, limited partnership, limited liability company, or corporation – whether an S corporation, C corporation or a professional corporation). In many instances, even if the party at interest is an individual is an entity, the individual or individuals behind the entity should be made parties to the agreement.
From the buyer’s perspective, the purchase of a medical practice is a highly person-oriented business. The practice value depends much upon the personality of the current treating physicians. If the current treating physicians are also the owners of the entity, then binding those individuals (especially as applies to the restrictive covenant) is of primary importance.
If the current treating physicians are not owners of the entity, but rather employees, then a determination of whether they will continue in their same positions or whether the buyer will be taking over the treatment of patients becomes the prime focus. If the current treating physicians will be continuing in their same positions, then their current employment contract must be reviewed to determine whether the rights of the seller will accrue to the buyer.
If the rights of the seller will not accrue to the buyer, then the Purchase and Sale Agreement must have a provision that makes the continued employment of those current-treating physicians a condition to consummation of the sale. In such instances, the new employment agreement might be an exhibit to the main agreement and executed contemporaneously with the main agreement.
If the current treating physicians will not be continuing in their same position and if the purchaser will be assuming treatment of the patients, then the main agreement must provide for the dissolution of the employment agreement and provision must be made for restricting the ability of those physicians from competing with the buyer. If the employment contract with the seller contains a restrictive covenant, then the buyer must ensure that such covenants will accrue to the buyers benefit. Otherwise, the buyer should insist that those physicians sign restrictive covenants. In such an instance, a portion of the purchase price may need to be allocated towards the consideration for those restrictive covenants and paid directly to those physicians.
DATE OF AGREEMENT AND CLOSING DATE
In general, it usually does not matter when the agreement is dated. It should usually be dated once all the terms are agreed to and the parties desire to bind each other and to be bound. In certain instance, the parties may have reached an agreement, but certain issues (such as the obtaining of a state license to practice medicine) may be outstanding. In such a case, then an option can be given by either the seller or the buyer to bind the other to sell or buy the practice upon exercise of the option. Giving an option can also push the agreement date into the future. The option will usually be given with token consideration (e.g., one hundred dollars) and will have a fixed expiration date (e.g., thirty to ninety days).
The determination of the closing date is more important than the date that the agreement is dated. Just like in the purchase of a house where certain issues (such as obtaining a mortgage and home inspection) must occur before closing, in the purchase of a practice, there may be certain issues which require time to undertake before the actual transfer can be consummated. For example, the buyer may still need to obtain financing or the landlord may need to approve the assignment of the lease.
RECITALS
The recitals – or “whereas” clauses – traditionally enunciate the reasons the parties are entering into the agreement. In the sale of the practice the recitals may simply state that the buyer wishes to buy the practice and the seller wishes to sell the practice. Yet, there is a modern growing tendency among contract attorneys to eliminate the “whereas” clauses as some attorneys feel that such language is antiquated. In such instances, the agreement will simply have a paragraph or two delineation of the “Purpose” of the agreement.
ARTICLES, SECTIONS, AND PARAGRAPHS
The agreement will often be divided and numbered in some logical fashion, either into articles, sections, paragraphs, or a combination of these. The reason for doing so is twofold. First, it allows ready reference to the numbered paragraph, and secondly it allows the agreement to be divided and grouped in logical associations.
BINDING THE PARTIES
The first paragraph of the first article will often bind the seller to sell and the buyer to buy the practice under the terms of the agreement. The rest of the agreement simply spells out those terms.
WHAT IS PURCHASED?
The agreement must disclose the items which are being transferred and the items which are not considered part of the agreement. This section should be crystal clear, so that anybody reading the contract (and hence a court which may be called upon to enforce the contract) and not privy to the preliminary negotiations will know what is part of the agreement and what is not part of the agreement.
[1] Sale of Stock vs. Sale of Assets
In most cases, well-informed financial advisors [FAs] will recommend that the buyer solely purchase the assets of the practice and not the stock of the practice. By purchasing selected assets, the buyer is ensured that he will not become responsible for the known or unknown liabilities of the corporation. In prior days, avoiding purchasing the stock of the corporation was a wise recommendation.
However, with the advent of managed care, the purchase of the stock of the corporation can provide the new practitioner with certain competitive advantages. It may take a new practitioner three to nine months to get onto enough managed care panels to make the practice profitable. Purchase of the stock of the corporation ensures the new practitioner of acquiring the Federal Tax Identification Number [TIN], Personal Identification Number [PIN], Drug Enforcement Agency [DEA], Centers for Medicare and Medicaid [CMS], Global Location Number [GLN] , National Provider Identifier [NPI], HIE-Form 834 transmission number, Durable Medical Equipment Number [DME] etc, of the corporate entity. Since most managed care corporations identify providers by the Federal TIN, purchase of the stock of the corporation should allow the new practitioner to be enrolled on managed care panels in a shorter period of time.
[2] Items Purchased
Items purchased often lists the tangible and intangible property of the seller which will be transferred to the buyer. Such items often include:
A detailed inventory of the tangible assets to be purchased;
A detailed listing of the inventory of the practice;
The names and addresses of all of the patients of record treated by the seller;
The patient medical records maintained by seller;
The computer records maintained by seller;
All licenses, permits, accreditation and franchises issued by any federal, state, municipal, or quasi-government authority relating to the use, maintenance or operation of the practice, running to or in favor of seller, but only to the extent that they are accepted by buyer;
All of sellers’ right, title, and interest in and to all real estate and equipment leases, if any, services agreements, employment and professional service contracts relating to the practice but only to the extent that the foregoing are accepted by buyer;
Assignment of lease should be attached and be incorporated to the agreement;
All existing telephone numbers used in connection with the operation of the practice and all yellow page advertising of the practice; and
The goodwill of the practice, which includes seller’s assistance and cooperation in transfer of all sellers’ rights and interests in the practice to buyer and any other intangible assets of the practice not listed in any other category.
Certain items purchased, such as [paper or electronic] medical records, governmental licenses, fax, email, website and telephone numbers have special considerations as discussed below.
[3] Medical Records
The seller should protect its future need to use the transferred patient medical records. In the current managed care environment, providers are subject to strict scrutiny. Even after leaving practice the provider may find himself subject to a government or third party audit or subject to a medical malpractice lawsuit. Therefore, the provider should ensure that the contract allows for him to take future possession of the specific medical record(s) of the practice in order to mount an appropriate defense.
[4] Governmental Licenses
Certain government licenses and permits may be nontransferable. These would include items such as the federal and state employer identification numbers, as these are unique to seller as a corporate entity. Likewise, other items unique to seller include Medicare identification numbers, Medicaid identification numbers, NPIs and UPINs. The buyer would have to purchase the stock of the corporation order to acquire such items, which is another advantage of a stock transaction versus an asset transaction. Likewise, some local business licenses may or may not be transferable.
[5] Telephone and Fax Numbers, Website URLs and Twitter [X] Accounts, etc
Transference of the telephone numbers often requires that a special local telephone company form authorizing transfer of the telephone numbers to the buyer. Often the new owner of the telephone number will also become liable for any current yellow page advertisement monthly fees. It is the same with an URL or website or e-mail address or office Twitter X account, etc.
[6] Items Not Purchased
Items not purchased or “excluded items” often list the personal items of the parties or of the employees of the parties. Such items would often include:
All cash on hand or on deposit;
All accounts receivable generated prior to the closing date;
All prepaid expenses, utility deposits, tax rebates, insurance claims, credits due from suppliers and other allowances after Closing Date;
The personal effects, including but not limited to photographs, diplomas, uniforms, books, mementos, memorabilia, personally owned art and any personal property owned by them;
Life insurance, disability insurance, and disability buy-out insurance on seller;
Motor vehicles used in connection with the practice;
Any or all tangible-intangible assets used in conjunction with another practice of seller; and
All other assets owned by seller other than those specifically described as items purchased.
The exact items transferred will often depend upon the prior negotiations of the parties. For example, the parties may have agreed that the accounts receivable will be transferred with the practice. In such an instance, the accounts receivable will be listed as an item to be purchased.
PURCHASE PRICE AND TERMS
The price of the transaction (or the value of the practice) is often the one item that is aggressively negotiated between the parties. That is because both the buyer and the seller are overly concerned with “how much?” As this chapter demonstrates, there are a lot more details that go into the negotiation and final contract than just the price. The buyer or seller would be doing themselves a disservice to consider the other factors simply “lawyer details.” Many additional terms of the agreement should be considered by one side or the other as “walk-way” conditions. The party that fully adheres to their additional terms is likely to find the other party capitulating to them. This is because the other party will most likely be fixated on the price.
The purchase price should be delineated in the agreement. Furthermore, the method of payment of the purchase price should be delineated. Although the usual method of payment would be cash, there are other methods available as well.
Cash payment can be made by an official bank cashier’s check, by a certified check, by deposit of funds into an escrow account, or by other method agreed upon by the parties.
Non-cash type transactions include loan agreements and exchanges. Exchanges can provide certain tax benefits if the exchange is a “like kind” exchange. A like kind exchange would occur when parties swap practices. For example, a group practice might have several offices. As part of the breakup of the group, the parties might exchange their stock of one office for all of the stock of another office. Like kind exchanges have strict guidelines that must be adhered to or the tax advantages will disappear. The reader is cautioned to get current legal and financial advice prior to the time of exchange.
It is in the seller’s best interest to get all cash at the time of closing. Then the seller can walk away and not worry about the success or failure of his predecessor. The seller will not have to worry about collecting periodic payments. The seller will not have to worry about placing the buyer in default or about eventually having to repossess the practice and begin to practice medicine at that office again. If a seller repossesses a practice, the buyer may have driven the patients away or lost the managed care contracts (why else would the buyer not be able to honor the loan agreement?). So the repossessed practice will have a significantly lower market value – if it is even marketable at that time.
On the opposite end of the spectrum, it is in the buyer’s best interest to get long and lean loan terms. First, by getting loan terms, the buyer will often have to come up with much less initial capital. Second, because of the discussion in the preceding paragraph, the seller has a vested interest in ensuring that the buyer succeeds once the practice changes hands.
If the transaction involves a seller-financed loan, then the agreement should specify the terms. Additionally, a separate loan agreement and security agreement should be attached as exhibits to the agreement. Finally, in order to perfect the security agreement, the lien should be recorded at the local courthouse in accordance to local rules and customs.
***
***
ALLOCATION OF PURCHASE PRICE
The final purchase price will actually be the amalgamation of various assets of the practice. Those assets include the tangible and intangible assets. The tangible assets include the hard assets (such as computers, treatment tables, chairs and furniture, DME and x-ray machines, etc) and the soft assets (such as Q-tips, paper and cotton balls). The intangible assets will include going concern value, goodwill, and the value of any restrictive covenant.
The parties should delineate the allocation of the purchase price amongst those various categories to reach a mutual best fit with the potential tax obligations. The buyer is the one who should strive to make the allocation fit his needs as best as possible.
Generally, the sale of the assets will be ordinary income to the seller and taxed at the seller’s usual rate. The buyer will be able to depreciate the purchased items. However, the characterization of those assets and the allocated portion of the purchase price will determine how much can be depreciated and over what time period the items can be depreciated.
As a general rule, soft assets can be depreciated fully in the year of purchase. Generally, hard assets can be depreciated over a three to seven year time period, depending upon the class of the asset. Also, under Section §179, a certain dollar amount can be “expensed” or deducted in the year of purchase. The sooner and the faster that the assets can be deducted the less current taxes that the buyer will be required to pay. However, intangible assets generally must be deducted over a 15-year period. This prolongs the tax benefits of any payments characterized as such.
Nonetheless, purchase of the assets results in better tax consequences that purchase of the stock of the practice. When stock is purchased, there is no depreciation allowance allocated in the current or subsequent years. Instead, the cost of the stock becomes the “basis” of the buyer in the practice. Any gain or loss from that basis will only have tax benefits or tax consequences in the year that the stock is sold or becomes worthless.
Because of the tax consequences of the characterization of the allocations of the purchase price, it is important that the agreement delineate the portion of the practice price which is allocated to each category. Each party should further agree never to claim a different allocation in any future tax filings. Generally, the soft and hard assets will be valued at their current actual cash value. In no event should the purchase price allocated to the soft and hard assets exceed the actual initial cost that the seller paid for the item. The only exception to the foregoing would be if the sale involved the transfer of an appreciable asset.
LEASE ASSIGNMENT
The agreement should provide that upon closing that the seller will assign the lease to the buyer. The buyer then acquires possession of the premises and assumes responsibility for the lease payments.
Sellers often do not understand that even though they do not practice at the leased premises and even though the buyer is making the lease payments, that the seller still remains liable to the landlord under the original lease. Usually this does not present a problem for the seller. But if the buyer abandons the premises or stops making the lease payments, then the landlord will look to the seller for the lease payments through the expiration of the lease.
If the seller has signed a restrictive covenant, then the seller may find himself in the unenviable position of making lease payments for the premises and prohibited from practicing at the premises. The seller should protect himself from this possibility. Therefore, the seller should ensure that the original agreement contains a provision that if the seller becomes liable under the lease that the seller can enter onto the premises, take possession of the practice and the practice assets and can practice medicine at the location until the seller’s liabilities are extinguished.
INDEMNIFICATION AND EXCLUSION/INCLUSION OF LIABILITIES
During the sale of a medical practice, each party will have certain liabilities that the other party should not assume and should not be required to assume. A mutual indemnification clause will act to ensure that each party remains liable for its own liabilities.
In a medical practice, the most common liability is a claim of medical malpractice against the provider. The seller has an interest in insuring that he is not liable for any claim brought by a patient that resulted after he leaves the practice and the buyer has an interest in insuring that she is not liable for any claim brought by a patient that resulted before she acquired the practice.
There are other areas of liability in the sale of a medical practice that may not be readily apparent. These include premise liability (e.g., slip and fall claims), employment claims (e.g., unemployment liability, sexual harassment, discrimination, and wrongful termination claims), tax claims (e.g., unpaid employment taxes and income or sales tax liabilities), and third party payer claims (e.g., Medicare recoupment claims). Consult your insurance agent to determine whether you can obtain insurance coverage to limit your liability under these clauses.
Medical practitioners should understand the full risk of signing an indemnification or hold harmless clause. If a claim is brought against the other party, then the party giving indemnification can be forced to pay any judgment or settlement incurred by that other party. The party giving indemnification can even be required to pay the other party’s attorney bills. This is an important point that the reader should consider carefully: Even if the other party successfully defends a claim, the indemnifying party can be held liable for the other party’s attorney’s fees. Since attorney fees can mount up rapidly, the indemnifying party can find itself responsible for thousands or even tens or thousands of dollars of attorneys’ fees.
If at all possible, one should never sign an indemnification agreement, whether in the sale of a medical practice, a managed care contract, or even a home security monitoring contract. Sometimes, one has no choice but to assume the risk and sign the contract. If at all possible, one should strive to sign such clauses in a corporate capacity and not in an individual capacity. If that is not possible, then seek insurance to minimize the risk. Indemnification clauses and the potential unlimited risk that they pose is one reason why the professional should undertake a carefully planned asset protection program.
***
***
OTHER FACTORS AND CLAUSES
[A] Integration
As a general rule, once parties have seen fit to put their agreement in writing, then no prior oral agreement regarding the same subject is binding. A paragraph stating that the written agreement contains the entire understanding of the parties simply reflects this rule of contract construction. Such a paragraph also places the parties on notice that any oral representation of the other party that has not been placed in the contract will be worthless.
[B] Construction
At times a court may hold any ambiguities in a contract against the party that prepared the agreement or that had the agreement prepared for them. If the party on the other side of the contract is an individual that was not represented by counsel and especially if that party has had very little business experience (such as a physician or medical provider recently in practice), courts are much more likely to hold ambiguities against the drafter of the agreement.
A paragraph regarding the construction of the agreement and stating that the agreement was formed from negotiation (as opposed to a “take-it-or-leave-it” proposition) can identify for any court constructing the contract that the court should not hold any ambiguities against the drafter. After all, even with negotiated contracts, one party or the other draws up the agreement.
[C] Choice of Law
In the United States today, it is common for parties in different states to have business dealings with each other. Likewise, in the sale of a medical practice, the buyer may begin negotiations in one state and then move to the practice state after consummation of the sale. In a similar vein, following the sale the buyer may move to another state.
In most cases, the various state laws should be similar on the contractual issues involved in the sale of a medical practice. However, a statement in the contract identifying the state whose laws will govern the contract will eliminate one possible source of dispute involving a side issue to the contract. In the vast majority of contracts, the laws of the state where the practice is physically located should be chosen by the parties to govern the contract
[D] Choice of Venue
Just like providing for choice of law, a side issue to the contract can be eliminated by choosing ahead of time the venue to resolve any conflicts that may arise. The venue is simply the place where the conflict will be decided. In most cases, the parties should choose the trial court of the county in which the practice is located.
[E] Survival of Obligations
An agreement to purchase a medical practice contains two aspects. First is the transference of the practice assets in exchange for the purchase price. Second are the various other terms, such as preservation of the medical records. By providing that these obligations survive the closing, each party is assured that the other party will not claim that the actual closing of the agreement extinguished the rights of the parties under the agreement.
[F] No Waiver Clause
A provision providing that a party does not waive its rights unless such a waiver is committed to writing allows a party to be a “nice guy” without risking its future rights. In some instances, if a party does not insist upon full compliance by the other party, then the first party may be considered to have waived its rights and may have no recourse against the other party.
There may be instances when the forbearance to exercise a right under the contract will benefit both parties. For example, if the buyer cannot pay the seller an installment on time, the seller may agree to extend the time for payment of that installment. The no waiver clause allows the seller to refuse to extend the time for payment of a future installment. Without the clause the buyer might be able to argue that the seller had waived its future rights to timely payments.
[G] Notices
There may be various reasons under the contract why one party may need to give a notice to the other party. Most often such notice will be that a party is claiming that the other is in breach of some provision of the agreement.
By specifying the address and method of delivery of any notice, the sending party can be assured that a court will rule that the receiver had actual or constructive notice.
Such a provision should also provide that one type of notice would be a change of address. Such a change of address notification would then supersede the address delineated in the agreement.
In most cases, the agreement should provide that the counsel to the party would receive a copy of any notice. This accomplishes two goals. First, there is a greater likelihood that the receiving party would receive actual notice. If the receiving party had moved and had failed to provide notice of the change of address, then the party’s counsel would have received the notice. Secondly, the party’s counsel would have received the notice in a timely manner and could take any immediate action that may be necessary.
[H] Severability Clause
A severability clause helps to ensure that if one provision is held by a court to be illegal or unenforceable, then the offending clause will be stricken from the agreement and the parties will be held to the agreement without the clause.
Without a severability clause, if a court finds that one provision of the agreement illegal or unenforceable, then the court has the power to strike down the entire agreement. Although even with a severability clause a court could strike down the entire agreement, the severability clause tells the court that the intent of the parties was that only the offending clause be stricken and essentially asks the court to honor the parties’ intent.
[I] Further Assurances Clause
After execution of the agreement, the parties may discover that certain other documents are necessary to complete the transaction. Unless such documents materially change the meaning and purpose of the agreement, a further assurance clause requires the party of parties to execute and deliver the document.
***
***
CLOSING – SETTLEMENT
The closing or settlement date should be chosen for a mutually time and place. Generally the date will be between 30 and 90 days from the execution of the agreement. This will allow the buyer and the seller adequate time to complete any conditions precedent to closing. At closing, the buyer will tender to the seller the agreed upon funds and will execute any loan and security agreements required under the purchase and sale agreement. If the restrictive covenant also contains a buyer’s covenant, then the buyer will execute that document. The seller will deliver to the buyer a bill of sale for the assets of the practice, will execute the restrictive covenant, will deliver the keys to the practice, and will surrender the assets and the premises to the buyer. Both the buyer and the seller will execute the lease assignment.
Many of the provisions of the agreement will survive the closing. This includes any agreement to prorate expenses not allocated in at the closing, the restrictive covenant agreement, the indemnifications, and any seller’s right maintained in the medical records.
TRANSITION
Both the seller and the buyer have certain interests to protect after the closing which would require the seller to stay with the practice for a period of time following the closing. The seller may have ongoing treatment plans with certain patients (such as post-operative follow-up treatment). The agreement should specify that the seller be allowed to continue at the practice location for the purpose of finishing such treatment plans. Although the buyer may be fully capable of completing such treatment plans, both the buyer and seller should be cognizant that the patient may claim abandonment. Allowing the seller to complete treatment plans in progress will mitigate against any perceived or actual claims of abandonment.
The buyer will want to require the seller to stay with the practice for a certain period of time, usually between three to six months. During that time, the seller will act to introduce the buyer to the current patients and the buyer will begin treatment of any new patients to the practice. In this way, the transition will appear smooth and natural to the current patients.
Of course, during the transition period, the seller will have the right to be paid by the buyer. To avoid misunderstanding, the method of payment should be reduced to writing. Usually the rate of compensation will be the profit margin percentage of the practice allocated to all income collected from the seller’s efforts during the time period in question. An astute negotiator might be able to require the seller to function during the transition period as an implicit condition for the payment of the practice price.
RESTRICTIVE COVENANTS
As part of the purchase price the buyer is paying for intangible assets of the practice. A medical practice is a highly individual based business. The practice depends in large part upon the reputation of the selling physician. For that reason, the buyer must ensure that the seller cannot use that highly individualized asset to compete against the practice for which she has just paid a high sum. The restrictive covenant protects this interest of the buyer.
A restrictive covenant actually contains several covenants to protect the buyer’s interests. These include not only the obvious covenant not to compete, but also a covenant regarding financial interests, a covenant regarding solicitations, and a covenant regarding proprietary information.
The first covenant is the covenant not to compete. In this covenant, the seller agrees not to compete with the practice in the geographic area during the time term of the agreement. This covenant prohibits the seller from actually practicing or from practicing indirectly. For example, the seller could not set up a clinic within the geographic area during the time period and employ a nurse practitioner to treat patients under his medical license.
The next covenant would be the covenant regarding financial interests. In this covenant, the seller is prohibited from investing in a competing business (i.e., medical practice), within the geographic area during the time period. This provision prevents the seller from investing in such a medical practice, even if he does not directly treat patients at that location.
The third covenant would be the covenant regarding solicitation. In this covenant the seller agrees not only to refrain from contacting patients of the practice during the time period, but also to refrain from contacting employees of the practice. If the seller maintains another office location which will not be sold, then the seller should ensure that the agreement provides that the seller is allowed to treat patients which find themselves to that practice location. Otherwise, the seller may be liable for patient abandonment and may also violate managed care contracts.
A final covenant would be a covenant regarding proprietary information. Simply by the fact of operating the practice, the seller has obtained certain proprietary information about the practice. This includes patient lists, accounting information, managed care contracts, and forms and handbooks. The seller should be prohibited from using such knowledge to the detriment of the practice.
[A] Time and Distance
The time and distance covered by the restrictive covenants must be reasonable. If either the time or distance is unreasonable, then a court might strike down the entire restrictive covenant.
A reasonable time is usually between two to five years. A two-year time period should be the minimum that the buyer should insist upon. The purpose of the time period is to allow sufficient time for the practice patients to consider the buyer as their “doctor” and to lose confidence in the selling doctor. For that reason, any time period over five years is likely to be considered an unreasonable restraint.
On the other hand, a reasonable distance depends upon many individual factors. A reasonable distance in an urban area like New York City would most likely be completely unreasonable in rural areas, such as rural Iowa. In most metropolitan areas, a five to ten mile radius from the practice location is likely to be considered reasonable. In rural areas, an entire county or even several contiguous counties may be considered reasonable. The main determination of the reasonableness of the distance factor is the total area from which the practice draws its patients.
Most practice management software programs allow for delineation of the practice patient base determined by zip code. That will provide the parties a starting point from which to negotiate the distance factor of the restrictive covenant.
[B] Buyer’s Covenants
The restrictive covenant should also contain buyer’s covenants, although it may seem counterintuitive that the buyer, having paid the seller tens of thousands of dollars for the practice, should be required to sign buyer’s covenants. However, a buyer’s covenant is an important part of the restrictive covenant. Under the purchase agreement, the seller might retain the right to repossess the practice, the practice assets, and the premises. This is most likely to happen when the seller finances the purchase price and the buyer defaults on the payments. It can also happen when the seller assigns the lease to the buyer and the buyer either abandons the premises or otherwise causes a default under the lease. The seller then remains liable as principle under the lease.
For those reasons, the restrictive covenant should provide that if the seller is required to enter onto the premises and take possession of the practice, then the Seller is relieved of his obligations under the restrictive covenants and the buyer now becomes bound by those same obligations. Such buyer’s covenants will prevent the buyer from abandoning the practice and then setting up a nearby competing practice.
CORPORATE RESOLUTION
Most medical practices being sold are corporate entities. If the transaction is a sale for stock, then the transaction is between private parties – the buyer paying cash and the seller transferring the stock.
However, in those cases where the buyer is purchasing the assets of the corporate practice, then the corporation must take certain prerequisite steps. Generally, a corporation, through its officers and directors, is prohibited from selling significant assets without permission of the shareholders.
For that reason, a shareholder meeting must be held and the shareholders at that meeting must approve a resolution allowing the officers and directors to sell significant assets of the corporation.
ASSESSMENT
The contract regarding the sale of a medical practice is the final agreement of the parties. Such a contract should only be executed after sufficient investigation into the practice and upon consultation with proficient professionals, including attorneys, accountants, FAs and practice management consultants. Understanding the basic terms and conditions of a contract regarding the sale of a medical practice is the first step in successfully negotiating the best agreement possible. Before one can negotiate for a certain provision, one must first be aware of the possibility of such a provision and its possible ramifications.
So, what else can FAs and consultants do to help plan properly for the sale of a medical practice, physician succession planning, and this major life liquidity event? Some experience FAs suggest constructing a “dry run template analysis” so the doctor can envision what life will be like after the sale, and what their corresponding financial needs might be. When the practice is sold, life is very different because many expenses that the practice paid become expenses the doctor now must pay. And so, the use of an astute financial advisor, practice valuation specialist, and healthcare contract attorney is highly advised.
CONCLUSION
As we have seen, the purchase price of a medical practice, although am important part of any sale, should only be considered one element of the negotiations. There are many clauses and provisions of a contract regarding the sale of the medical practice, which if not negotiated favorably should be considered factors to initiate the party to walk away from the sale.
Boundy, Charles: Business Contracts Handbook Gower Pub, NY 2010
Fenton, CF: Contracts Regarding the Sales of a Medical Practice. Financial Planning for Physicians and Healthcare Professionals; Aspen Publishers, New York, NY, 2003.
Hekman, K: Buying, Selling & Merging a Medical Practice. Keneth Hekman, New York 2008.
Walker, Lewis: The Ultimate Transition. Financial Advisor, page 33, 2014.
Schatzki, M: Negotiation Speak: Winning Words and Phrases for Sales, Purchasing, Contract and Other Business Negotiations – All the Dialogue and Skills You Need to Come Out Ahead, Dynamic Negotiations, Chicago, IL 2009.
UCC, Commercial Contracts and Business Law Blog: LexisNexis 2010.
9. We act with honesty, integrity and are always straightforward. 8. We strive to be innovative, creative, iconoclastic, and flexible. 7. We admit and learn from mistakes and don’t repeat them. 6. We work hard always as competitors are trying to catch up. 5. We treat others with dignity and respect. 4. We are the onus of consulting advice for the well being of others. 3. We fight complacency as former success is in the past. 2. The best management styles are timeless, not timely. 1. Our clients are colleagues and always come first.
SPEAKING: Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements.
***
***
CONTACT: Ann Miller RN MHA at: MarcinkoAdvisors@outlook.com
Marcinko Associates is a financial guide. We help answer your questions in an empowering way. We educate and empower medical colleagues to understand their financial picture and to make better financial decisions. We strive to simplify everything, clear up confusion, and address specific needs and goals.
Whatever your financial situation, we do not shame, criticize, or sell. We enrich, educate and empower. We work with medical colleagues at every stage of their financial journey, through big life personal changes to annual employment reviews, in order to help them understand, invest, and protect their money and autonomy.
And, like the famed ‘Tibetan Sherpas“, we guide physician entrepreneurs from medical practice business plan creation, funding, start-up operations and strategic management improvement to maximize profits and stream-line patient care quality initiatives.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
9. We act with honesty, integrity and are always straightforward. 8. We strive to be innovative, creative, iconoclastic, and flexible. 7. We admit and learn from mistakes and don’t repeat them. 6. We work hard always as competitors are trying to catch up. 5. We treat others with dignity and respect. 4. We are the onus of consulting advice for the well being of others. 3. We fight complacency as former success is in the past. 2. The best management styles are timeless, not timely. 1. Our clients are colleagues and always come first.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
With international stock markets comprising about 40 percent of the world’s capitalization as of 2023, a broad range of investment opportunities exist outside the borders of the U.S.
For investors who are looking to diversify their mutual fund portfolio with exposure to companies located outside the U.S., there exist two basic choices: A global mutual fund or an international mutual fund.
By definition, international funds invest in non-U.S. markets, while global funds may invest in U.S. stocks alongside non-U.S. stocks.
Make a Choice: The definition may seem clear, but what may seem less clear is why an investor might select one over the other. The reason that an investor may select a global fund is to provide the portfolio manager with the latitude to move the fund’s investments among non-U.S. markets and the U.S. market in order to take advantage of the shifts in relative opportunities these markets may present at any given moment.
By investing in a global fund, the challenge for the investor is that he or she may not know at any point in time their total exposure to the U.S. market within the context of their overall portfolio.
An Inside Look: As a consequence, some investors want to manage their allocation risk by setting the broad asset allocation for their portfolio and then identifying funds that are within those asset classes. For these investors, an international fund may make more sense since it allows them to maintain a greater adherence to their desired domestic/international stock allocation.
Keep in mind that asset allocation is an approach to help manage investment risk. Asset allocation does not guarantee against investment loss. As you consider a global or an international fund, you should also be aware of the fund’s approach to the inherent currency risks. Some funds choose to engage in strategies that may mitigate the effects of currency fluctuations, while others consider currency movements – up and down – to be an element of portfolio performance.
Book Dr. David E. MarcinkoMBA MEd CMPfor your Next Medical, Pharma or Financial Services Seminar orPersonal and Corporate Coaching Sessions
Dr. Marcinko enjoys personal coaching and public speaking and gives as many talks each year as possible, at a variety of medical society and financial services conferences around the country and world. These have included lectures and visiting professorships at major academic centers, keynote lectures for hospitals, economic seminars and health systems, keynote lectures at city and statewide financial coalitions, and annual keynote lectures for a variety of internal yearly meetings.
His talks tend to be engaging, iconoclastic, and humorous. His most popular presentations include a diverse variety of topics and typically include those in all iMBA, Inc’s textbooks, handbooks, white-papers and most topics covered on this blog.
Academic Team of Internationally Known Contributors
D. E. Marcinko & Associates is one of the most academically published authorities on the topic of financial planning and private wealth management for physicians, nurses and medical professionals. We have published 33 major peer reviewed textbooks redacted in the Library of Medicine, Institute of Health and the Library of Congress, in four languages, with over 5,025 online white papers, web-posts and related publications. These cover a range of financial planning topics from medical malpractice, risk management and insurance, to investment policy statement analysis and endowment funding management, and to taxation, retirement, estate and legacy planning.
Financial planning, business and strategic management, FMV for practice and clinics and related “hard” topics are included.
***
We also include “soft” subjects from investor psychology, ethics and lost fortunes to luxury spending, from understanding the middle-class millionaire to the political philosophies of physicians and the affluent. Our corpus of work is regularly consulted by doctors, medical, business, graduate and nursing schools, to elite advisors, private and investment bankers, wealth managers, venture capitalists, academics and the press.
Did you know that at MARCINKO & Associates, all medical colleagues throughout the United States may contact us when they are considering the sale, purchase, strategic operating improvement, merger, acquisition and/or other financial business or related personal financial planning transaction?
Our difference is “hard” knowledge and insider financial guidance that helps medical colleagues, nurses, private practitioners, clinics, ambulatory surgery, radiology and outpatient wound care centers realize their ultimate economic goals. This typically includes managerial and cost accounting, financial ratio analysis, fair market valuation business appraisals, business plan creation and personal financial planning.
Our “expert witness” business litigation support service and divorce mediation, arbitration, asset division, settlement and second opinion offerings are always available, as well.
And, our “soft” skill professional career guidance and mentoring center includes executive coaching, consulting and mentoring advisory programs for stressed, conflicted or burned-out physicians and medical practitioners.
Most importantly, our professional fees are reasonable and always transparent.
MARCINKO & Associates also serves universities, medical, business, graduate and nursing schools; physicians, dentists, podiatrists, optometrists and legal societies. This includes accountants, financial service providers, wealth and hedge fund managers, emerging entities, hospitals, CEOs and their BODs, the press, media and related organizations.
Posted on December 21, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Ann Miller RN MHACMP™
INTRODUCING OUR NEXT GENERATION e-BOOK LIBRARYFROM iMBA, Inc.
An e-book is an electronic or digital book that can be read on a computer or a handheld device.
Our new e-books consists of text, images, and are fixed to a specific spot on the page.
And, our e-books are a data files similar in content and structure to a word-processing document that comes in a PDF format. To use our e-books, you need to purchase and download it to a device that has a .pdf file reader app, such as ADOBE® or similar on a smartphone, tablet or computer. A PDF, also known as a portable document format, is the format most people are familiar with and used in our e-books. PDFs are known for their ease of use and ability to hold custom layouts. They are the most commonly used e-Book formats, especially by professionals and adult-learners.
You can then access the e-book and read it, or highlight pages and even take side notes.
e-Books Save Money
With no manufacturing, printing, binding or shipping costs, e-Books are cheaper than traditional hard or paper back books.The price of each specialized and highly niche focused e-Book [50-100 pages] is only $25, whereas similar paperback printed books of this type generally cost $145, or more!
Achieving your financial, wealth and medical practice management goals is important, but handling everything on your own can be overwhelming. That’s where we come in. At D. E. Marcinko & Associates, our team of dual degree experienced physician advisors and medical consultants is here to guide you every step of the way. We believe in providing unbiased, high-quality financial and business advice.
For example, we offer a one-time written financial plan with oral evaluation for a flat fee with no ongoing sales or assets under management fees or commissions. Together, we can create a personalized financial plan tailored to your unique goals, empowering you to make confident, informed decisions as you navigate your financial future.
Other Services Include:
Estate Planning We have a network of qualified legal professionals that we can refer you to for state specific estate planning needs.
Tax Strategy We can work alongside your CPA for tax planning purposes. If needed, we can refer you to a qualified tax professional.
Investment Analysis If you have investments, we review your accounts to make sure they are aligned with your long-term goals.
401-k Allocations We evaluate your 401(k) allocations and provide recommendations that align with your goals.
Education Savings We help you explore the various ways to plan and save for education expenses.
Insurance & Risk Management We assess your insurance coverage to ensure it adequately protects you against potential risks; as well as evaluate and provide expert litigation witnesses, as needed.
Medical Practice Management We evaluate your current or potential medical practice to determine value and/or private equity offers or physician practice management formats [PPMC] for new, mid-career or retiring physicians, nurses and dentists.
D. E. Marcinko & Associates is unique and fully committed to all phases of a medical professionals personal and business life cycle. We are at your service 24/7: Email MarcinkoAdvisors@outlook.com
Posted on November 29, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Is it Good for Retailers … but Bad for Doctors and Consumers?
***
If Black Friday 2024 is anything like 2023, retailers may not be swimming in cash while shoppers bathe in savings. Black Friday deals drew 212 million shoppers to stores in fabulous 2010 and collectively spent $39 billion on products and services.
And, the average amount spent by a Black Friday shopper in 2010 was a whopping $365.34.
***
***
Assessment
We predict Black Friday 2024 sales surpass 2023 with a slight increase over 20222 because of fewer shopping days; and the COVID pandemic explosion..
QUESTION: But, is Black Friday good for the [healthcare] economics sector post [thu] the pandemic? Do patients go shopping rather than to the doctor? What about inflation?
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
The www.MedicalBusinessAdvisors.com is focused solely on appraising medical practices, surgery centers [ASCs], medicine, podiatry, optometry and allied healthcare businesses.
Working with our affiliated partners, like the ME-P and others, we are also available for behemoth multi-specialty medical practices, major clinics, hospitals, related healthcare organizations and networks, and PHOs, etc.
We are backed by the expertise of dedicated appraisers and valuation analysts who are trained by the foremost organizations in our industry www.CertifiedMedicalPlanner.org
Practice owners, attorneys and accountants retain us for projects including, but not limited to the following:.
There are a Myriad of Reasons for Obtaining a Medical Practice Valuation and Appraisal Engagement
Outright selling-buying
Partnership and Associate buy-in / buy-out
Mergers and Acquisitions
Organic growth tracking
Hospital integrations
Private and public reporting
Financing and Venture Capital
Estate and tax planning
Our Capability
We have the ability to provide extensive analysis of value components in healthcare practices and provide appraisals based on business, economic, and market conditions. This involves detailed examination of financials and clinical data in the context of numerous factors including medical specialty, physician supply and demand, payer mix, regulatory environment, regional dynamics, and risk premium.
Assessment
Our methods and approaches adhere to accepted standards of healthcare practice appraisal and utilize direct market data to reach justifiable conclusions. These are documented in a comprehensive report which is tailored to meet the need of the specific engagement.
SAMPLE ENGAGEMENTS: See partial engagement list below.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Our guest on this episode is Dr. Farzad Mostashari. Farzad is the co-founder and CEO of Aledade, a primary care enablement company that partners with independent PCPs to transition to value-based care and, as a result, maintain their independence.
Founded in 2014, Aledade works with 11,000 physicians across 40 states and DC, accounting for 1.7M patients under management in Medicare, Medicare Advantage, Commercial and Medicaid contracts. Farzad previously served as the National Coordinator for Health IT in the Department of Health and Human Services, he completed medical school at the Yale School of Medicine and a Master’s in Population Health from Harvard’s T.H. Chan School of Public Health. Earlier this year, Aledade raised a $123M Series E round of funding led by OMERS Growth Equity.
***
In this episode, colleague Shahid N. Shah will discuss with Farzad about (1) his journey to starting Aledade and the role policy expertise and evidence have played in the company’s success (2) why he and the company are betting on independent physicians as the drivers of change in value-based care and (3) how Aledade became the rare profitable health tech company.
Posted on October 25, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By: Christian Hernandez MBA – Apple Health Care Services
Richard Melnyck MBA MS
Mark Friedman PhD Department of Accounting
Howard Gitlow PhD Department of Management Science University Miami
***
BACKGROUND
***
Homecare has long been one the most cost-effective methods of treating patients. Yet today, homecare providers face significant challenges: reimbursement cuts, mandatory accreditation, and influencing policy changes. So, how can homecare managers efficiently sustain a cutting edge, consistent and quality focused practice amidst this changing landscape?
***
It is time the homecare industry tap into the high-tech tools and proven management theories that together make up “Six sigma” management. This article will provide a solid point of reference for managers interested in adopting “Six Sigma” management. In today’s stiff economic climate, organizations are once again turning to “Six Sigma”strategies as a means to reduce their bottom lines.
***
However, its cost cutting aspect is technically more of a by product than the core of its theory. “Six Sigma” management is practiced in many organizations across all sectors of the global economy. Companies such as drug giant Merck, Cadbury, and Dunkin’ Brands are increasingly turning to Six Sigma to lift their bottom lines.
***
The term “Lean Management” is an old buzz word that still excites managers. Lean Management stems from the term Lean Manufacturing, which was a derivative of Total Quality Management (TQM) —considered one of the earlier versions of “Six Sigma”.
***
Over the years, “Six Sigma” has evolved from a ground-breaking management system to one of the most proven methods for instituting change, reducing errors and eliminating inefficiencies. These management utilities run through the entire spectrum of organizational applications, from confronting the serious issues mentioned above to routine business functions.
***
The resurgence of Japan’s economy in the 70’s and 80’s is largely attributed to TQM. “In the auto industry, manufacturers such as Toyota and Honda became major players. In the consumer goods market, companies such as Toshiba and Sony led the way. These foreign competitors were producing lower-priced products with considerably higher quality.”
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on October 23, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
How would you restart your career in medicine?
[By Dr. David Edward Marcinko MBA MEd CMP™]
We’ve known this physician-client-friend for 10 years, and while he didn’t tell us what he wanted to discuss, we knew it was important.
After exchanging pleasantries, he shocked me: He said he’s totally unfulfilled in his current job and wants to do something new.
We were floored because he is an outstanding doctor – at the top of his game. From the outside looking in, he appears to be “living the dream”.
After that bombshell, we asked him the question we couldn’t get out of our mind: “Are you afraid?”
“Yes,” he said; “Afraid and relieved.”
His relief stemmed from the fact that he is going to shed the tremendous demands of being a doctor at the highest levels. He was afraid because he didn’t know what was next.
We thought afterward, “What a courageous and totally refreshing move.”
A Fantasy Reboot
That dialogue triggered a larger internal conversation within; and with others.
What would you do if you could start from scratch?
How would you proceed if you could just wipe the slate clean and restart your career in medicine?
For those quietly pondering a similar path, three great opportunities seem crystal clear.
First, we would create our own practice playbook. Discard the ready-made choices served up by your old practice. For the independent physician today, there’s almost infinite variety. The pleasure in creating your own approach is that there are so many options. Your patients will appreciate the greater choice and flexibility, too.
Second, we would whole-heartedly embrace technology; but not necessarily EHRs at this time. Rather, build your own HIT framework to complement your medical practice. Innovate across your entire operations – everything from medical records, to online appointment access, secure FAX machines, to patient portals and laboratory results reporting to your own mobile phone app. Freeing yourself from your current archaic technology will be life altering by itself.
Third, cull the difficult people from your life. These are the naysayers who weigh you down – superiors, colleagues or patients. Negativity is corrosive, and it always lingers. It also distracts you from giving others your best. While you’re at it, cull the skills you mastered to survive in your career so you can focus on those that really matter.
Case Model
So, we wanted to share one of the all-time greatest reboots we know because it shows what is possible if you believe in yourself.
A decade ago, one of our osteopathic physician clients delivered some bad news. She was quitting her job as a medical associate, to transition into her own direct pay concierge practice.
At the time, this was unheard of: No one walked away from a potential medical practice partnership to become a solo physician. But, Sue had a different vision. She wasn’t fulfilled and she knew it. With the support of her husband, she decided there was a better way. So she started from scratch.
How did it work out?
Unbelievably well – but NOT overnight!
With our meager assistance, Sue’s been cash flow positive for the last 7 years, and now earns more money than before, with less stress; and she is the captain of her ship. A few colleagues who have worked with her have even gone on to achieve comparable success. She’s become a role model to others too, and she remains one our heroes.
The Decision
Starting from scratch may or may not translate into more money, but it often means this: More happiness in your life. Sue’s decision, just like our friend who bared his soul to us over coffee, were both made for the right reasons.
We wish our friend well on his journey, confident knowing that a happy ending is just over the horizon for him, too.
Assessment
Send us your own success/failure story, so we might learn from you. Would you even stay in medicine or transition/begin another career; anew?
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on October 22, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Re-Thinking a Popular Practice from the Past
By Dr. David Edward Marcinko; MBA, MEd, CMP™
[Publisher-in-Chief]
More personal than a corporate home care medical business model, most people view house calls as a popular practice from the past.
Although less than 5% of the nation’s doctors regularly make house calls today, the medical house call industry is swiftly picking up momentum once again. It is a move that is greatly benefiting physicians and patients alike.
Why House Calls?
It’s because we live in a society that has become technology focused. While this emergence has benefited many in terms of medical advancements, there are a growing number of patients who are uncomfortable with next-generation medical practices. These people, particularly the rapidly aging elders of the nation, want to be cared for in a friendly, nurturing, and convenient way. As people age and fall ill, it becomes increasingly difficult to leave the home for office visits. Not to mention, there are many handicapped patients as well who have to arrange for wheelchair vans or ambulances just to visit the doctor. The COVID pandemic and tele-health are illustrative.
Meeting a Niche Market Need
Thanks to the desire of physicians seeking to open their own medical house call practices, these patient needs are slowly being met. Some of these physicians are strictly open for house call visits only and have no physical office. They commonly take appointment requests via phone calls and emails with the overall goal to combine the service of an old-time, small town doctor with the latest technology designed to meet people’s emotional, and financial, needs. Patients are also able to save a considerable amount of time by not having to leave the house to go to the doctor’s office, and not having to fill prescriptions. After all, many medical house call physicians travel along with certain medications that can be dispensed on location. Narcotics, however, will likely still need to be filled with a paper or e-prescription.
While highly convenient for patients who wish to receive medical house call services, the reviving industry is fitting for physicians. In recent years, Medicare has increased its level or reimbursements for physicians who travel to patients. Just in the past few years alone, Medicare has been billed approximately $1.75 million annually for house calls.
Enter the DNPs and NPs
Even nurse practitioners [NPs] and Doctors of Nursing Practice [DNPs] who make a small number of house calls are typically unaware that they can maximize profit potential with medical house calls. Some NPs have even offset operating expenses by offering house calls to make their office based practice more appealing to their patients.
Also, significant advances in technology have enabled popular medical equipment to be smaller and portable. Physicians are able to perform standard procedures, such as skin biopsies and blood draws while outside the office. They are also able to easily access patient medical records through usage of a laptop, as well as resources such as the Physicians’ Desk Reference [PDS] through usage of a hand-held personal digital assistant or smart cell phone.
Assessment
For example, this firm educates patients and supports physicians who are ready to make a transition from office-based positions to medical house call practices. There are no royalty or membership fees, and this is not a franchise. It helps transition to a reportedly more pleasing, profitable way to practice medicine today.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Marcinko & Associates is financial guide. We help answer your questions in an empowering way. We educate and guide medical colleagues to understand their financial picture and to make better financial decisions. We strive to simplify everything, clear up confusion, and address specific needs and goals.
Simply put, we’re a financial services company on a mission to empower financial freedom for all healthcare professionals; only. We work with doctors, nurses, medical providers, individuals and all sizes of organizations to offer investment, wealth management and retirement solutions so everyone can have a clear and simple understanding of where their finances and career is today and where it is headed tomorrow.
Whatever your financial situation, we do not shame, criticize, or sell. We enrich, educate and empower. We work only with medical colleagues at every stage of their financial journey [students, interns, residents, practitioners, mid-career and mature physicians], through big life personal changes to annual employment reviews, in order to help them understand, invest, and protect their money and lifestyle.
Assess, develop, and align financial retirement and estate planning goals
Risk Management: Malpractice, home, life, medical, auto and personal indemnity
Life Insurance Need Reviews: whole, universal and term
Business, operations, HR, employment negotiations and medical practice management
Annuity Need Reviews: Indexed and Fixed [Pros and Cons].
***
***
At Marcinko & Associates we discuss specific needs and answer specific questions. We educate and make personalized recommendations that you are free to use, incorporate or disregard. Referrals to trusted specialists and strategic alliance partners then occur if – and as – needed [pro re nata].
Posted on October 12, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
On Patient Satisfaction
[By Dr. David Edward Marcinko MBA MEd]
The traditional linear patient scheduling system is slowly being abandoned by modern medical practitioners; in all venues (medical practices, clinics, hospitals and various other healthcare entities).
Why? Waiting room times are too long!
According to this infographic put together by the folks at evisit.com the amount of time patients spend waiting in your office have a huge effect when it comes to patient satisfaction.
For example, did you know that the national average wait time is currently around 21 minutes!
***
[Click to Enlarge]
Patient Scheduling Issues
Most mature doctors follow a linear (series-singular) time allocation strategy for scheduling patients (i.e., every 15 or 20 minutes). This can create bottlenecks because of emergencies, late patients, traffic jams, absent office personal, paperwork delays, etc.
Therefore, as proposed by colleague Dr. Neal Baum MD, a practicing urologist in New Orleans, one of these three newer scheduling approaches might prove more useful.
1. Customized Scheduling
The bottleneck problem may be reduced by trying to customize, estimate or project the time needed for the patient’s next office visit. For example: CPT #99211 (5 minutes), #99212 (10 minutes), #99213 (15 minutes), #99214 (25 minutes), or #99215 (40 minutes). Occasionally, extra time is need, and can be accommodated, if the allocated times are not too tightly scheduled.
2. Wave Scheduling
Some patient populations do not mind a brief 20-30 minute wait prior to seeing the doctor. Wave scheduling assumes that no patient will wait longer than this time period, and that for every three patients; two will be on time and one will be late. This model begins by scheduling the three patients on the hour; and works like this. The first patient is seen on schedule, while the second and third wait for a few minutes. The later two patients are booked at 20 minutes past the hour and one or both may wait a brief time. One patient is scheduled for 40 minutes past the hour. The doctor then has 20 minutes to finish with the last three patients and may then get back on schedule before the end of the hour.
3. Bundle Scheduling
Bundling involves scheduling like-patient activities in blocks of time to increase efficiency. For example, schedule minor surgical checkups on Monday morning, immunizations on Tuesday afternoon, and routine physical examinations on Wednesday evening, or make Thursday kid’s day and Friday senior citizens day. Do not be too rigid, but by scheduling similar activities together, assembly-line efficiency is achieved without assembly line mentality, and allows you to develop the most economically profitable operational flow process possible for the office.
Patient Self Scheduling (Internet Based Access Management)
New software programs, and internet cloud applications, allow patients to schedule their own appointments over the internet. The software allows solo or individual group physicians with a practice to set their own parameters of time, availability and even insurance plans. Through a series of interrogatories, the program confirms each appointment. When the patient arrives, a software tracker communicates with office staff and follows the patients from check-in, to procedures, to checkout.
Today, many hospitals have even abandoned the check-in or admissions, department. It has been replaced by access management systems.
***
***
Waiting Room Strategies
In any potentially detrimental situation, delineate what the staff can do to make it right. A service paradox exists and timely, appropriate action can sometimes build more patient internal satisfaction than if the situation had never occurred.
Take the wait for example. It is not enough to just have policies in place that help prevent a prolonged wait from occurring. There must also be policies in place that ameliorate an adverse situation when it does arise. This can involve placating a patient over long wait, or, reassuring a patient about an empty waiting room.
An apology form you and/or the staff might be one technique, “I’m so sorry to keep you waiting. Doctor X and I really try to stay on schedule because we know how valuable your time is.”
Offering some refreshments might be another.
In extreme cases, giving the patient a beeper and turning them loose until you see them may work.
Many patients will be impressed you have even considered how the wait affects them. Sometimes the above management techniques, if the wait is not too offensive, can actually build more patient satisfaction than just seeing them on time.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on October 11, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Understanding Horizontal and Vertical Integration
ENCORE PRESENTATION
[By Robert James Cimasi MHA, AVA, CMP™]
Health Capital Consultants, LLC
St. Louis MO
Several potential benefits are associated with the integration of companies in the same or related industries. These synergistic benefits depend upon the type of companies and their integration strategies, as well as whether the anticipated transaction is a manifestation of horizontal consolidation or vertical integration.
Horizontal consolidation is “the acquisition and consolidation of like organizations or business ventures under a single corporate management, in order to produce synergy, reduce redundancies and duplication of efforts or products, and achieve economies of scale while increasing market share.”
Vertical integration involves the joining of organizations that are fundamentally different in their product and/or services offerings, i.e., “the aggregation of dissimilar but related business units, companies, or organizations under a single ownership or management in order to provide a full range of related products and services.”
Healthcare Locality
As healthcare is essentially a local business, horizontal integration within the local market has been limited by antitrust laws. Therefore, in order to control greater market share, a hospital’s strategy has required vertical integration. Healthcare providers and organizations have placed much emphasis on the benefits of vertical system integration in the last 10 or more years, whereby a single healthcare organization owns all of the elements needed to provide a continuum of care for all the needs of a given patient population. Much of this effect has stemmed from the desire to be able provide a “continuum of care,” i.e., to be able to single source contract for the healthcare needs of a patient population and to profit from implementing preventative healthcare and utilization management measures. The relative economic benefits of this type of vertical integration versus horizontal integration strategies remain the subject of great debate in academia and among the strategic managers of other industries. One lesson that may be drawn from other industries is that neither of these forms of integration is universally applicable or beneficial to every organization and market. There are also great costs to integration, which must be outweighed by the benefits. Each specific benefit should be identified and researched when examining the probable effects of integration, consolidation, mergers or divestitures as a competitive strategy.
Rapid Consolidation Periods
During the rapid consolidation and integration of healthcare providers, insurers, and purchasers, in recent years, there was much discussion of a concept termed “managed competition.” This term appears to have been an outgrowth of the term “managed care” and was viewed by many as the logical result of the integration of healthcare markets nationally. The concept of “managed competition” apparently related to an idealized vision of competition between very large, integrated providers (organized into integrated delivery systems), large, national managed care payors, and purchasing group coalitions that could achieve a balance of power between these interacting groups. However, many believe that the result of such an arrangement would more likely be a reduction in competition between members of each of these three groups and the creation of powerful bureaucratic and intractable organizations. Further, this scenario does not appear to effectively remove any of the existing barriers to competition and therefore doesn’t introduce any additional incentives for innovation to produce value for consumers which, of course, is the “sine qua non” of competition.
Disadvantages
The disadvantages of integration are becoming apparent, including:
the loss of autonomy;
increased bureaucracy;
difficulty in aligning incentives; and
other failed expectations.
Many organizations that sought strategic advantage through integration are ending those arrangements and now divesting acquired organizations.
Other Industries
In other industries, specialized providers of goods and services are increasingly able to offer customers a full range of services through affiliation and affinity with other independent specialists, made more seamless through the use of increasingly sophisticated communications and computing technologies. However, this move to “dis-integration” must also be carefully considered if organizations are not to make further costly organizational changes inspired by a rushed judgment of general market trends.
Porter Speaks
Michael Porter (et al.) wrote in the Harvard Business Review that,
In industry after industry, the underlying dynamic is the same: competition compels companies to deliver increasing value to customers. The fundamental driver of this continuous quality improvement and cost reduction is innovation. Without incentives to sustain innovation in health care, short-term cost savings will soon be overwhelmed by the desire to widen access, the growing health needs of an aging population, and the unwillingness of Americans to settle for anything less than the best treatments available. Inevitably, the failure to promote innovation will lead to lower quality or more rationing of care — two equally undesirable results.
Assessment
Therefore, if the emerging healthcare industry is to respond successfully to the Affordable Care Act [ACA] and related market pressures to reduce costs, then the healthcare market must first create incentives for innovation. The barriers to competition cannot include barriers to innovation as many do now. Physicians, nurses, healthcare purchasers, managers, and legislators must ensure innovation takes the forefront of any reform, if it is to be effective.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on October 8, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Dental Managed Care [DMC] is Substandard Care – count on it!
By D. Kellus Pruitt DDS
Have you noticed most employer-sponsored dental plans boast savings of 30% and more on dental care, without mentioning how unsustainable discounts harms their employees?
Dental Managed Care [DMC] is substandard care: Discount dentistry, like virtually all underfunded handwork, has always been substandard … Or perhaps someone would like to argue that intricate surgery in sensitive mouths of nervous patients is improved when rushed.
Discounts are popular
Those who market obscure, hard to understand managed care plans to clueless, perhaps non-caring employers, do not control the quality of the discounted dentistry they sell.
Think about it: Discount dentistry without quality control. Can you think of a worse idea in healthcare?
What’s more, not one Delta Dental, Humana or Cigna executive can be held accountable for causing harm to equally clueless dental patients through under financed dentistry they sell. Employees who must choose their dentists from preferred provider lists have forfeited freedom of choice, whether they realize it or not. Their underfunded, substandard dentistry is subsidized by tax payers as a special tax-free benefit, benefiting unaccountable third parties most of all.
For example:
Want to know what you get with managed care dentistry? Quick prophys.
How many of you get your teeth cleaned in 30 minutes or less? Do they feel clean?
One Hour
l always allowed my hygienists 1 hour to clean patients’ teeth simply because it often takes that long to do the job right – regardless what insurers say hygienists’ time is worth. The economic climate is tough on fee-for-service.
As I am considering signing on as a preferred provider – not because I want to – I notice that the fees allowed by insurers do not cover the hourly rate of most hygienists… unless they can “clean” teeth, take x-rays, take blood pressure, go over patients’ medical history, allow time for the doctor to do a quick exam and turn around the room in less than 30 minutes.
***
***
Assessment
The motto of my practice is “Dentistry Unhurried.” I don’t want to compete in a race to the bottom which uninformed dental patients always lose.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
The modern medical practice is both similar, and unlike, other businesses today. This disparity often adds to confusion for the private practitioner. And so, the experts at iMBA Inc, list the top 25 most urgent questions in practice financial management, asked by clients to date.
Assessment
Since inception in 2000, the Institute of Medical Business Advisors Inc., has become one of North America’s leading professional health consulting and valuation firms; and focused provider of textbooks, CDs, tools, templates, onsite and distance education for the health economics, administration and financial management policy space. As competition and litigation support activities increase and the cognitive demands of the global marketplace change, iMBA Inc is well positioned with offices in five states and Europe, to meet the needs of medical colleagues, related advisory clients and corporate customers today; and into the future.
And so, your thoughts and comments on this Medical Executive-Post are appreciated. Tell us what you think. Send in your own questions. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Sponsors Welcomed
And, credible sponsors and like-minded advertisers are always welcomed.
ACOs are groups of doctors, hospitals, and other health care providers, who come together voluntarily to give coordinated high-quality care to their Medicare patients. The goal of coordinated care is to ensure that patients get the right care at the right time, while avoiding unnecessary duplication of services and preventing medical errors.
When an ACO succeeds both in delivering high-quality care and spending health care dollars more wisely, the ACO will share in the savings it achieves for the Medicare program.
Now, suppose that in a new Accountable Care Organization [ACO] contract, a certain medical practice was awarded a new global payment or capitation styled contract that increased revenues by $100,000 for the next fiscal year. The practice had a gross margin of 35% that was not expected to change because of the new business. However, $10,000 was added to medical overhead expenses for another assistant and all Account’s Receivable (AR) are paid at the end of the year, upon completion of the contract.
Cost of Medical Services Provided (COMSP):
The Costs of Medical Services Provided (COMSP) for the ACO business contract represents the amount of money needed to service the patients provided by the contract. Since gross margin is 35% of revenues, the COMSP is 65% or $65,000. Adding the extra overhead results in $75,000 of new spending money (cash flow) needed to treat the patients. Therefore, divide the $75,000 total by the number of days the contract extends (one year) and realize the new contract requires about $ 205.50 per day of free cash flows.
Assumptions
Financial cash flow forecasting from operating activities allows a reasonable projection of future cash needs and enables the doctor to err on the side of fiscal prudence. It is an inexact science, by definition, and entails the following assumptions:
All income tax, salaries and Accounts Payable (AP) are paid at once.
Durable medical equipment inventory and pre-paid advertising remain constant.
Gains/losses on sale of equipment and depreciation expenses remain stable.
Gross margins remain constant.
The office is efficient so major new marginal costs will not be incurred.
Physician Reactions:
Since many physicians are still not entirely comfortable with global reimbursement, fixed payments, capitation or ACO reimbursement contracts; practices may be loath to turn away short-term business in the ACA era. Physician-executives must then determine other methods to generate the additional cash, which include the following general suggestions:
1. Extend Account’s Payable
Discuss your cash flow difficulties with vendors and emphasize their short-term nature. A doctor and her practice still has considerable cache’ value, especially in local communities, and many vendors are willing to work them to retain their business
2. Reduce Accounts Receivable
According to most cost surveys, about 30% of multi-specialty group’s accounts receivable (ARs) are unpaid at 120 days. In addition, multi-specialty groups are able to collect on only about 69% of charges. The rest was written off as bad debt expenses or as a result of discounted payments from Medicare and other managed care companies. In a study by Wisconsin based Zimmerman and Associates, the percentages of ARs unpaid at more than 90 days is now at an all time high of more than 40%. Therefore, multi-specialty groups should aim to keep the percentage of ARs unpaid for more than 120 days, down to less than 20% of the total practice. The safest place to be for a single specialty physician is probably in the 30-35% range as anything over that is just not affordable.
The slowest paid specialties (ARs greater than 120 days) are: multi-specialty group practices; family practices; cardiology groups; anesthesiology groups; and gastroenterologists, respectively. So work hard to get your money, faster. Factoring, or selling the ARs to a third party for an immediate discounted amount is not usually recommended.
3. Borrow with Short-Term Bridge Loans
Obtain a line of credit from your local bank, credit union or other private sources, if possible in an economically constrained environment. Beware the time value of money, personal loan guarantees, and onerous usury rates. Also, beware that lenders can reduce or eliminate credit lines to a medical practice, often at the most inopportune time.
4. Cut Expenses
While this is often possible, it has to be done without demoralizing the practice’s staff.
5. Reduce Supply Inventories
If prudently possible; remember things like minimal shipping fees, loss of revenue if you run short, etc.
6. Taxes
Do not stop paying withholding taxes in favor of cash flow because it is illegal.
Hyper-Growth Model:
Now, let us again suppose that the practice has attracted nine more similar medical contracts. If we multiple the above example tenfold, the serious nature of potential cash flow problem becomes apparent. In other words, the practice has increased revenues to one million dollars, with the same 35% margin, 65% COMSP and $100,000 increase in operating overhead expenses. Using identical mathematical calculations, we determine that $750,000 / 365days equals $2,055.00 per day of needed new free cash flows! Hence, indiscriminate growth without careful contract evaluation and cash flow analysis is a prescription for potential financial disaster.
Dr. Michel Accad is a practicing cardiologist who blogs for a medical audience at alertandoriented.com
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on September 18, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
On the Crucial Online Presence
[By John Deutsch]
A strong online presence is crucial to running a successful business, and healthcare is no exception.
However with constant change, especially in the past two years, many businesses are experiencing underperforming campaigns and struggling to figure out where to spend their marketing dollars. Should you invest heavily in pay-per-click (PPC) advertising, focus your efforts on search engine optimization (SEO) or hit the ground running with social media?
The answer is that you should never focus solely on one marketing channel, as it could take months or even years to recover when changes in the marketing industry occur – and they inevitably will occur. Another reason to diversify your efforts is that the success of some channels depends on the success of others – for example, social media influences your search rankings and display advertising heavily influences your brand recognition.
As a healthcare marketing company with over ten years of experience in internet marketing, we have seen the industry get flipped upside down more than once and have seen it affect organizations that have weak marketing campaigns with little to no diversification. A good mix of tactics is the best way to reach your target audience while allowing you to adapt quickly in the face of changes.
Three Elements Crucial to Any Marketing Campaign
Search marketing, direct marketing and social media are three components that healthcare organizations should incorporate for a healthy marketing campaign. Here’s what you need to know about these marketing elements, including the changes each channel has gone through in the last few years and what we could expect to see in the future.
Search Marketing
Search marketing typically refers to PPC and SEO, the paid and unpaid efforts used to increase online visibility in search engine results. Early marketers were able to easily leverage SEO to gain top search engine rankings and also invest minimally in PPC for quick leads, but the search marketing landscape has changed significantly in the last three to four years, altering the online marketing game.
We might say it all started when Google modified its PageRank algorithm in 2011 and then again in 2012 (the update often referred to as “the death of SEO”), causing many organizations’ rankings to plummet. Marketers were forced to rethink their organic SEO efforts to stay in Google’s good graces. Instead of relying heavily on getting backlinks (even from low-quality websites) and stuffing content with keywords, the focus switched to creating quality content in order to get real clicks and page views.
Meanwhile, companies like Google started trying harder than ever to monetize their services. The highly saturated market contributed to driving advertising costs up – and beyond that, the actual efficacy of online ads went down. In some of our own campaigns, we have seen over 30% inflation in ad prices per year and a loss of efficacy (decreased traffic and leads) despite increasing ad spend to match inflation – and this isn’t just a result of market saturation. It also has to do with the fact that consumers are less and less receptive to online advertising due to the over publicizing of ads.
As a result of this, organizations have to constantly innovate so that their ads are seen among all the online advertising noise. This, in addition to rising ad prices means that a return on investment can be difficult to realize. Working with a true PPC expert who knows your industry well is the only way to make your budget go a long way.
The bottom line: SEO and PPC are still the number one ways to draw leads online, but they have both seen significant change in the past years and are likely to keep changing, so your marketing strategy should not depend on either channel alone.
Direct Marketing
With SEO having lost some importance and PPC advertising requiring a skill set that many health organizations lack, we are seeing trends shifting towards a more direct form of marketing. This is evident by the number of lead generation companies that have cropped up in the last few years, such as Healthgrades and Vitals, which allow providers to attract more patients and referrals, often for a nominal fee. Similarly, in the medical software industry, SoftwareAdvice dominates the SEO/PPC channels.
Organizations are also increasingly employing alternative marketing channels like email newsletters and direct email marketing to reach out to clients and potential opportunities. This starts with a simply crafted email addressing a very specific issue to a specific audience. It is an extremely effective and budget-friendly tactic to diversify a marketing strategy.
Social Media
Just like other marketing channels, social media is constantly evolving and also increasing in price. This is due, in large part, to major social media companies becoming publicly traded companies in recent years (i.e. Facebook in 2012 and Twitter in 2013), but also to market saturation.
According to a LinkedIn study, 81 percent of small- and medium-sized businesses are using social media and, of those, 94 percent do so for marketing purposes. While networks like Facebook and Twitter remain free to use, they have started trying to capitalize on their popularity by pushing paid advertisement, often to the point of risking the integrity of their sites.
Whereas prior to companies like Facebook and Twitter having gone public, a well-crafted social media post (text, video or image) could go “viral” naturally, we are now seeing this happen less and less, often requiring an initial advertising spend to get the ball rolling. Facebook is a good example of this. In December 2013, Facebook changed the algorithm that determines what stories and updates users see in their News Feeds. This resulted in business pages losing viewership of their posts, as Facebook decided that brands would have to “pay to play.”
Assessment
While we don’t recommend social media being the focal point of any healthcare organization’s marketing campaign, much less the only element, it is an integral component – and definitely one you should stay on top of if you want to remain competitive. Social media is also a major factor in Google’s algorithm for organic search engine rankings, so there is some added value to having a strong social media presence.
John is the President and CEO of Medical Web Experts, developer of Bridge Patient Portal, the leading 2014 ONC certified solution for patient engagement and improved practice profitability. A vital component in the exponential growth of numerous healthcare IT and Internet companies over the last ten years, John has benefited immensely from a unique mix of professional experiences, boasting a strong background in both marketing and technology.
Channel Surfing the ME-P Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on September 18, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Why Hospitals, Clinics and Medical Offices are Not Hotels, or Manufacturing Plants or Production Assembly Lines, etc!
By Dr. David E. Marcinko FACFAS, MBA, MEd, CMP™
[Editor-in-Chief]
The rising cost of health insurance remains a major concern for business; despite the Affordable Care Act [ACA] of March 2010. Local and national news publications have trumpeted that healthcare costs are not just rising but are growing in proportion to the cost of other goods and services.
Many of these publications have expressed the widely held view that because of the “inflation gap,” the cost of medical expenses needs curbing. Proponents of this viewpoint attribute the growth in the gross domestic product (GDP) devoted to personal medical services (from 5% in 1965 to approximately 14% in 2005 and 17% in 2012) to increases in both total national medical expenditures as well as prices for specific services, and then conclude that there is a need to rein in the growing costs of healthcare services for the average American, even if it be through a legislative mandate.
Healthcare Is the Economy
According to colleague Robert James Cimasi MHA, AVA, CMP™ of Health Capital Consultants LLC in St. Louis, MO, healthcare cannot be separated from the economy at large. Although economists have cited the aging population as the reason for the increase in healthcare’s share of the GDP, other voices assert that financial greed among HMOs, pharmaceutical companies, hospitals, and medical providers like doctors and nurses is responsible. In reality, the rise in healthcare expenditures is, at least in large part, the result of a much deeper economic force.
As economist William J. Baumol of New York University explained in a November 1993 New Republic article: “the relative increase in healthcare costs compared with the rest of the economy is inevitable and an ineradicable part of a developed economy. The attempt [to control relative costs] may be as foolhardy as it is impossible”.
Baumol’s observation is based on documented and significant differences in productivity growth between the healthcare sector of the economy and the economy as a whole.
Low Productivity Growth
Healthcare services have experienced significantly lower productivity growth rates than other industry sectors for three reasons, according to Cimasi:
1) Healthcare services are inherently resistant to automation. Innovation in the form of technological advancement has not made the same impact on healthcare productivity as it has in other industry sectors of the economy. The manufacturing process can be carried out on an assembly line where thousands of identical (or very similar) items can be produced under the supervision of a few humans utilizing robots and statistical sampling techniques (e.g., defects per 1,000 units). The robot increases assembly line productivity by accelerating the process and reducing labor input. In medicine, most technology is still applied in a patient-by-patient manner — a labor-intensive process. Patients are cared for one at a time. Hospitals and physician offices cannot (and, most would agree, should not) try to operate as factories because patients are each unique and disease is widely variable.
2) Healthcare is local. Unlike other labor-intensive industries (e.g., shoe making), healthcare services are essentially local in nature. They cannot regularly be delivered from Mexico, India or Malaysia. They must be provided locally by local labor. Healthcare organizations must compete within a local community with low or no unemployment among skilled workers for high quality and higher cost labor.
3) Healthcare quality is — or is believed to be — correlated with the amount of labor expended. For example, a 30-minute office visit with a physician is perceived to be of higher quality than a 10-minute office visit. In mass production, the number of work-hours per unit is not as important a predictor of product quality as the skills and talents of a small engineering team, which may quickly produce a single design element for thousands of products (e.g., a common car chassis).
Assessment
Healthcare suffers a number of serious consequences when its productivity grows at a slower rate than other industries, the most serious being higher relative costs for healthcare services. The situation is an inevitable and ineradicable part of a developed economy.
For example, as technological advancements increase productivity in the computer, and eHR, manufacturing industry, wages for computer industry labor likewise increase. However, the total cost per computer produced actually declines. But in healthcare (where technological advancements do not currently have the same impact on productivity), wage increases that would be consistent with other sectors of the economy yield a problem: the cost per unit of healthcare produced increases.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.