Re-thinking the Ratios-of-Costs-to-Charges [RCCs] Financial Meter
By Russ Richmond MD
 Using the ratios-of-costs-to-charges [RCCs] can lead hospitals down a garden-variety strategic path that’s wrong for them.
Using the ratios-of-costs-to-charges [RCCs] can lead hospitals down a garden-variety strategic path that’s wrong for them.
A strategically safer method of cost estimation can more accurately reveal costs.
At a Glance
- Using ratios of costs to charges (RCCs) to estimate costs can cause hospitals to significantly over- or under-invest in service lines.
- A focus on improving cost estimation in cost centers where physicians have significant control over operating expenses, such as drugs or implants, can strengthen decision making and strategic planning.
- Connecting patient file information to purchasing data can lead to more accurate reflections of actual costs and help hospitals gain better visibility across service lines.
To put it bluntly, there is an almost complete lack of understanding of how much it costs to deliver patient care, much less how those costs compare with the outcomes achieved. Instead of focusing on the costs of treating individual patients with specific medical conditions over their full cycle of care, providers aggregate and analyze costs at the specialty or service department level.
—Professors Robert Kaplan and Michael Porter, “The Big Idea: How to Solve the Cost Crisis in Health Care,” Harvard Business Review, September 2011.
Of all the challenges hospitals face in today’s uncertain healthcare environment, estimating their costs might not be their top concern. However, the method most hospitals use to estimate their costs can have serious strategic and financial ramifications on their bottom line.
More than 60 percent of hospitals today use ratios of costs to charges (RCCs) as their primary cost estimation method, because true cost accounting is viewed as prohibitively expensive. But using RCCs to estimate costs can lead to significant problems for hospitals. For example, results of a recent study disclose that among 184 mid-sized community hospitals (i.e., with roughly 300 beds), the use of RCCs led 85 percent of the hospitals to overestimate the profitability of orthopedic surgery service lines. On average, the overestimates amounted to $1.2 million per year per hospital.
Such incorrect cost estimates can cascade into potentially serious strategic, financial, and operational issues. Because of faulty cost estimates, hospitals can over-invest—or under-invest—in service lines based only on high-level insight into the actual profitability of these areas. Either scenario has the potential to produce negative consequences.
Suboptimal strategic decision making based on faulty data and conclusions leads to suboptimal results. No hospital can afford such results and stay competitive in an industry of increased cost and pricing transparency.
So what’s the solution for hospitals? Even without switching to a full procedural cost-accounting system, hospitals can make adjustments that improve their cost estimating and thus strengthen their decision making and strategic planning. The operative principle is that hospitals should focus on improving cost estimating in cost centers where physicians have the most control of operating expenses—namely, drugs and implants.
Making the Right Cost Connections
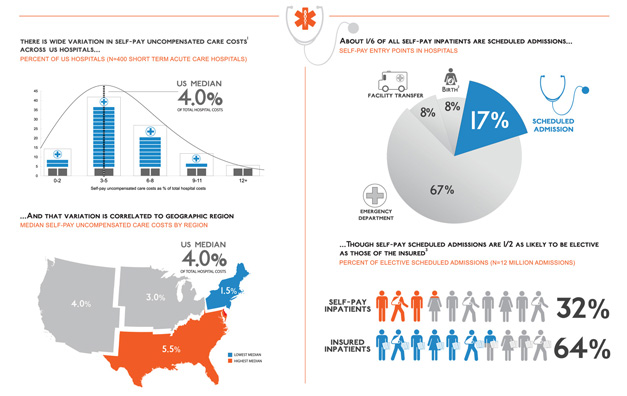
Connecting patient file information, where costs are estimated, with purchasing data, which reflect actual costs, can produce a significant impact on a hospital’s pricing methodology. Drugs and implants, which represent 17 percent of a typical hospital’s total costs, are a good starting point for adoption of this approach.
Drugs. To better estimate drug prices, hospitals should make the patient file/purchasing data connection based on generic class, route of administration, and dosage. The patient charge file and the purchasing file can be connected using a common taxonomy. For instance, a hospital’s purchasing file may record a box of 10 Tylenol tablets as “10 Tylenol tablets of 325 mg,” while the charge may be recorded in the patient charge file as “Acetaminophen cap 325.” This results in a direct text mismatch for calculating cost, which can ultimately lead to faulty cost-estimating data. A common taxonomy would group these two entries into a common bucket to produce an accurate mapping of costs.
Implants. Implants are also a major price item for hospitals. To better estimate implant costs, the patient charge file and the purchasing file should be mapped using the implant log, using the same process described for mapping drug costs. The implant log is used by surgeons after an operation to log the type of procedure, detailed description of supplies used, and general comments.
When a physician orders a knee implant, the implant stock-keeping unit (SKU) number is often recorded in the implant log. If the SKU number in the implant log were mapped to the SKU number in the hospital’s purchasing file, the hospital would be better able to determine the actual cost for the implant. The cost could then be assigned to the patient file, resulting in a more accurate cost picture for orthopedic cases.
For example, to assign true implant costs to a patient who has undergone a knee replacement, a hospital would look up the implant SKU recorded in the implant log by the physician—in this example, SKU123. Then, the hospital would open the purchasing file and locate, for that particular month, the description and price for SKU123 (in this instance, XYZ knee replacement part; cost: $4,950). Next, the hospital would map the more detailed description and price for the implant to the patient charge file. This process can help to ensure that the true cost of the implant used by the physician is assigned to the patient’s charge file.
In some hospitals, the implant log, purchasing file, and patient charge file are part of the same system. For the majority of hospitals, however, the implant log is a separate electronic file, not connected with the other file system or systems. And in some hospitals, the implant log is manually managed.
A hospital can complement this process by comparing its drug and implant costs with price benchmarks from subscription-based national databases or with databases maintained by consulting firms. In our experience, a 65 percent match can be achieved by connecting the drug and implant purchasing files with the detailed charge files, as outlined above. By comparing these costs with price benchmarks from subscription-based or consulting-firm databases, a hospital can better determine how the prices it is paying for drugs and implants compare with national averages.
By connecting these data sets, hospitals can gain better visibility of what they are really spending across various service lines and operational functions.
Understanding a Rural Hospital’s True Costs
The experience of a 250-bed rural hospital in the north central United States provides a good example of the pitfalls of using RCCs to estimate costs. This hospital found itself making key strategic planning decisions based on misleading cost data.
In analyzing the drug usage data from two physicians (A and B) at the hospital, physician B appeared more cost-efficient than physician A at treating the same disease. However, on examining physician B’s actual drug expenditures, hospital leaders realized this physician’s costs were in fact higher than those of physician A (see the exhibitbelow).
###

###
If RCC costs are considered, physician A seems to be treating patients at a higher average cost per case than physician B. But if actual costs are considered, physician A is actually treating at a lower cost per case than physician B. Strategically, based on the RCC analysis, if the hospital encouraged all of its physicians to emulate physician B’s treatment approach, it would lose the opportunity to save money on every case.
The data generated by RCCs can be especially problematic in measuring the profitability of various hospital services lines. Because of these misleading cost data, the team at this rural hospital was under the impression it was making a healthy $477,000 profit annually from its orthopedic surgery group.
The reality was the hospital’s profit from this key service line was about $170,000 less—a material difference for a rural community hospital.
For years, the provider thought it was making money on hip replacement surgery, but those profits were much lower because costs of implants used in these orthopedic procedures were continually underestimated. An incorrect profitability picture such as this can wreak havoc on vital strategic-planning efforts.
The rural hospital is by no means an outlier in regard to its problems with cost estimation. The research finding cited at the beginning of this article suggests institutions regularly underestimate costs per orthopedic procedure (and the costs of implants) because of their use of RCCs.
Rising costs are at the heart of the cost challenges that are prevalent in health care. Healthcare reform was designed, in part, to help alleviate this persistent cost problem, but much work still needs to be done to fully understand the true costs of health care. Once these costs are better understood, the goal then must be to manage costs more effectively, efficiently, and sustainably. A critical starting point is for healthcare providers to have a more accurate and realistic picture of what their current costs are, not what they think costs may be.
By connecting key data sets and analyzing costs in a more systematic way, hospitals can develop a stronger and more accurate understanding of their actual costs. This system will provide more data visibility to enable hospital leaders to enhance strategic decision making related to key service lines, improving value.
Russ Richmond, MD, is CEO, Objective Health, Waltham, Mass., and a member of HFMA’s Massachusetts-Rhode Island Chapter (russell_richmond@mckinsey.com).
Footnotes:
a. This amount is based on an average overestimation in contribution per orthopedic surgery case of $1,200 multiplied by an average of 1,000 cases annually per hospital.
###
Sidebar 1: A Step-by-Step Guide to Improving Hospital Cost-Estimating Processes
Hospital leaders should follow four relatively easy-to-implement steps to improve their cost-estimating processes related to drugs and implants—two cost centers where physicians have significant control over operating expenses.
Step 1: Establish the Data Foundation
Ensure that the hospital has core data sets on which to develop. Keep the following practices in mind:
- All encounters and detailed charges should be available in corresponding files.
- All purchased drugs, implants, and other medical/surgical products should be available in a purchasing file (often provided by the group purchasing organization or distributor).
- All implants should be tracked in electronic implant logs (e.g., in the operating room, intensive care unit, and cath lab).
Step 2: Assemble a Cost-Estimate Improvement Team
This team, which will lead the project, should include the following representatives:
- Director of pharmacy, to provide guidance and sign-off on drug cost estimates
- Materials manager, to provide guidance and sign-off on implant cost estimates
- Chargemaster manager, to incorporate input from pharmacy and materials departments into the granular charge codes that are charged to patients
- Analytics expert, to connect purchasing files, implant logs, and patient charge files
- Strategy and finance leaders, to leverage the improved cost accounting to derive savings and align on growth strategy.
Step 3: Connect the Data Sets
The analytics expert connects the data sets as described in the “Making the Right Cost Connections” section of this article.
Step 4: Leverage Insights from True Cost Data
Three areas of understanding or capability can ensure that a hospital can put the cost data to effective strategic use.
Understanding of actual profitability of service lines/departments and definition of growth strategies.
A hospital with true cost data can understand which service lines drive most of its profit and which departments lead to maximum losses. This understanding enables hospitals to strategically define departments they should invest in and areas where they should become leaner. On the other hand, a hospital that uses ratios of costs to charges (RCCs) can, at best, give average estimates of service-line profitability, with the potential for categorizing unprofitable service lines as profitable and vice versa.
Ability to accurately measure clinical variation in the hospital and use the measurements to guide meaningful conversations with your physicians.
A hospital with true cost data can run physician-level data profiles, such as average cost per case for each physician treating a particular disease. Such insight can support meaningful discussions with physician outliers that can influence changes in behavior and thus potentially reduce costs. Hospitals using RCCs cannot approach physicians with the same level of credibility, as seen in the rural hospital example on page 89. If hospitals instead focus on using actual costs in specific strategic costs centers, physicians once considered the hospital’s most cost-efficient may be exposed as the organization’s most costly.
Understanding of the impact of macro-purchasing factors such as drug shortages on the profitability of key service lines.
A hospital that tracks actual costs can take macro-purchasing actors, such as drug shortages, and assign true costs on a daily or monthly basis, thereby allowing the effects of drug shortages on service-line profitability to be quantified. Alternatively, hospitals using RCC-based costing would average out the effects over a year, leading to inaccurate service-line profitability insight during times of drug shortages.
Sidebar 2: Improving Cost Estimates for Drugs: Action Steps by Department
IT Department
- Create a taxonomy-based categorization tool. Assign each drug description into broad therapeutic class, dosage, and route of administration categories. This can be a string search and categorization tool, using regular expressions, to match a specific set of characters in a string (word).
- Maintain a central database of drugs and categorizations to be used each month.
Pharmacy Department
- When documenting purchased drugs, be sure to include compound, dosage, and route of administration information in the entry.
- Ensure the detailed charge file has charge codes that reflect the individual drugs purchased each month.
Sidebar 3: Improving Cost Estimates for Implants: Action Steps by Department
IT Department
- Bridge the implant log and the purchasing file. Identify the SKU number for the implant in the purchasing file as well as the implant log. Maintain or create a central database of implants and their SKUs (both the implant-log SKU and the purchasing-file SKU).
- Connect the detailed charge file with the implant log, using the patient account number.
Purchasing Department
- Ensure that purchased implants are assigned an internal SKU that can be mapped to the implant log SKU.
- Ensure that the detailed charge file has charge codes that reflect the individual implants purchased each month.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:



Filed under: Health Economics, Healthcare Finance | Tagged: By Russ Richmond MD, costs to charges, drug prices, michael porter, Objective Health, ratio of costs to charges, RCCs | 3 Comments »










 A decade ago, Editor Gregory J. Kelley of Physician’s MONEY DIGEST and I reported that a 47 year old-doctor with $184,000 annual income would need about $5.5 million dollars for retirement at age 65. Then came the “flash-crash’ of 2007-08, the home mortgage fiasco and the Patient Protection and Accountable Care Act [PP-ACA] of 2010; etc.
A decade ago, Editor Gregory J. Kelley of Physician’s MONEY DIGEST and I reported that a 47 year old-doctor with $184,000 annual income would need about $5.5 million dollars for retirement at age 65. Then came the “flash-crash’ of 2007-08, the home mortgage fiasco and the Patient Protection and Accountable Care Act [PP-ACA] of 2010; etc.