BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on April 28, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Markets: The NASDAQ stayed flat at its lowest level this year.Spotify shares sank to a record low. Facebook is having a rough go, but it’s not the only one. Netflix stock plunged nearly 70% this year after hitting a ceiling on subscriber growth. At one point, it was worth more than Disney; now, it’s not even half as valuable. Even Google is googling “ways to make more money.” Its parent company, Alphabet, reported a slowdown in growth last quarter because, like Facebook, YouTube’s also being been dinged by TikTok and Apple’s privacy changes: The video platform’s revenue came in more than $500 million below expectations.
Energy: Russia’s halted oil shipments to Poland and Bulgaria yesterday.
Posted on April 22, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
April 22nd, 2022
***
By Dr. David Edward Marcinko MBA
Founding Editor-in-Chief
Go Green!
At this Medical Executive-Post, we are trying to go GREEN! Our green mindset permeates brightly whenever we conduct business. However, green is more than just a color, it’s a way of working and living that honors our environment and helps preserve it for future generations. And so, below is a list of our environment-friendly green initiatives.
***
Initiatives
We have the ability to remotely monitor our phone and internet systems. Not only is this a cost savings for our colleagues, members, visitors, customers and us, it reduces fuel usage by keeping third-party vendor delivery service fleets off the road.
Inbound technicians have an 85% first-call resolution rate. Our folks ask the right questions and take the time to solve issues without scheduling an in-person or vendor service call.
We telephone re-use jacks and cables, when possible.
We recycle all paper, plastic and glass in our office.
We use an eFax service, cutting down on paper usage.
We have a paperless billing system.
We have a virtual library of “how to” resources for all of our ME-P products and services.
We sent our old phone systems to a re-cycler who uses the parts for plastic.
Posted on April 17, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Russia: Shut its stock market all week in a bid to curb panic-selling after the invasion of Ukraine. The ruble cratered to trade below 1 cent as Western sanctions effectively weaponized the financial system.
Posted on April 14, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
DEFINITION: A rate of return (RoR) is the net gain or loss of an investment over a specified time period, expressed as a percentage of the investment’s initial cost. When calculating the rate of return, you are determining the percentage change from the beginning of the period until the end.
***
And so, according to Greg McBride CFA, before you invest your money, you’re likely wondering how much you’re going to earn. This is known as the rate of return. The rate of return is expressed as a percentage of the total amount you invested. If you invest $1,000 and get back your original investment plus an additional $100 in interest, you’ve earned a 10 percent return.
However, numbers don’t always tell the full story. You’ll also need to think about how long you plan to keep the money invested, how your investment options have performed historically and how inflation will impact your bottom line.
Key return on investment statistics
When you’re trying to get the best return on your investment, you’ll likely start combing through loads of data. A good place to start is looking at the past decade of returns on some of the most common investments:
As our private iMBA Inc clients, ME-P subscribers, textbook and dictionary purchasers, seminar attendees and most ME-P readers know, Ken Arrow is my favorite economist. Why?
About Kenneth J. Arrow, PhD
Well, in 1972, Nobel Laureate Kenneth J. Arrow, PhD shocked Academe’ by identifying health economics as a separate and distinct field. Yet, the seemingly disparate insurance, asset allocation, econometric, statistical and portfolio management principles that he studied have been transparent to most financial professionals and wealth management advisors for years; at least until now.
Nevertheless, to informed cognoscenti, they served as predecessors to the modern healthcare advisory era. In 2004, Arrow was selected as one of eight recipients of the National Medal of Science for his innovative views. And, we envisioned the ME-P at that time to present these increasingly integrated topics to our audience.
Healthcare Economics Today
Today – as 2022 passes – savvy medical professionals, management consultants and financial advisors are realizing that the healthcare industrial complex is in flux; along with the Russian war, domestic inflation and this dynamic may be reflected in the overall flagging economy.
Like many laymen seeking employment, for example, physicians are frantically searching for new ways to improve office revenues and grow personal assets, because of the economic dislocation that is Managed Care, Medi Care and Obama Care [ACA], the depressed business cycle, etc.
Moreover, the largest transfer of wealth in US history is – or was – taking place as our lay elders and mature doctors sell their practices or inherit parents’ estates. Increasingly, the artificial academic boundary between the traditional domestic economy, financial planning and contemporaneous medical practice management is blurring.
I’m Not a Cassandra
Yet, I am no gloom and doom Cassandra like I have been accused, of late. I am not cut from the same cloth as a Jason Zweig, Jeremy Grantham or Nouriel Roubini PhD, for example.
However, I do subscribe to the philosophy of Hope for the Best – Plan for the Worst.
And so dear colleagues, I ask you, “Are the latest swings in the economic, healthcare and financial headlines making you wonder when it will ever stop?”
The short answer is: “It will never stop” because what’s been happening isn’t any “new normal”; it’s just the old normal playing out before a new audience; sans the war.
What audience?
The next-generation of investors, FAs, management consultants and the medical professionals of Health 2.0.
How do I know all this?
History tells me so! Just read this work, and opine otherwise, or reach a different conclusion.
Evidence from the American Financial Scene, circa 1861-1935
The work was created by L. Merle Hostetler in 1936, while he was at Cleveland College of Western Reserve University (now known as Case Western Reserve University). I learned of him while in B-School, back in the day.
At some point after it was printed, he added the years 1936-1938. Mr. Hostetler became a Financial Economist at the Federal Reserve Bank of Cleveland in 1943. In 1953 he was made Director of Research. He resigned from the Bank in 1962 to work for Union Commerce Bank in Cleveland. He died in 1990.
The volume appears to be self published and consists of a chart, approximately 85′ long, fan-folded into 40 pages with additional years attached to the last page. It also includes a “topical index” to the chart and some questions of technical interest which can be answered by the chart.
And so, as with Sir John Templeton’s [whose son is an MD] four most dangerous words in investing (It’s different this time), Hostetler effectively illustrates that it wasn’t so different in his era, and maybe—just maybe—it isn’t so different today for all these conjoined fields.
Conclusion
Your thoughts and comments on this ME-P are appreciated. While not exactly a “sacred cow,” there is a current theory that investors will experience higher volatility and lower global returns for the foreseeable future.
In fact, it has gained widespread acceptance, from the above noted Cassandra’s and others, as problems in Europe persist and threats of a double-dip recession loom. But, how true is this notion; really?
Is Hostetler correct, or not; and why?
Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on March 8, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
BY JONATHAN MASER.N.
***
***
Being an entrepreneur is not necessarily easy, and many people that try to become entrepreneurs wind up failing. It’s important to recognize the risk of failure before you decide to walk down this path. Being an entrepreneur is very rewarding, and you can find success if you can do things right.
Keep reading to learn about common entrepreneurial mistakes that you can avoid to give yourself a better chance of realizing your entrepreneurial goals.
Posted on March 4, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
Stocks fell and oil prices eased back after another bumpy day of trading on Wall Street as markets remained anxious about the broader impact of Russia’s invasion of Ukraine.
Okta shares were down 8.06% while Snowflake plummeted 15.37%.
***
INTEL: Intel stock (NASDAQ: INTC) fell 2.5% after Morgan Stanley and Bank of America Securities cut their targets to $47, according to StreetInsider. The stock fell to a low of $47.62, not far from its 52-week low of $43.63. Morgan Stanley (NYSE:MS) analyst Joseph Moore also downgraded the stock to underweight from equal weight while BofA’s Vivek Arya maintained his under perform rating.
INDEXES: Major indexes veered up and down for much of the day before a late-day slide pushed them into the red. The S&P 500 shed a 0.7% gain to close 0.5% lower, while the Dow Jones Industrial Average fell 0.3%. The NASDAQ composite fell 1.6%, weighed down by technology stocks, which accounted for a big share of the market’s decline.
The Dow is down 0.9% for the week, on track for its fourth negative week in a row. The S&P 500 is down about 0.5% for the week, while the NASDAQ Composite is down more than 1%.
BUYBACKS: In the third quarter of 2021, Apple, Inc. (NASDAQ: AAPL) led all S&P 500 companies with $20.4 billion in buybacks. Alphabet, Inc. (NASDAQ: GOOG) (NASDAQ: GOOGL) was a distant second with $15 billion in buybacks, followed by Meta Platforms Inc (NASDAQ: FB) with $12.6 billion.
Over the last decade, no company has come close to Apple in the buyback department. Apple has bought back $487.6 billion in stock since 2012. Microsoft Corporation (NASDAQ: MSFT) is a very distant second with $147.1 billion in buybacks, followed by JPMorgan Chase & Co (NYSE: JPM) with $146.2 billion.
Why Buybacks Matter: It should come as no surprise to investors that all three of the stocks that have been most aggressive in buying back shares over the last 10 years have outperformed the SPDR S&P 500 ETF (NYSE: SPY) total return by a wide margin in that period.
BONDS: Bond yields were mostly steady. The yield on the 10-year Treasury slipped to 1.85% from 1.86% late Wednesday.
When trying to decide whether to buy a used car or a new one, it’s typically financially wiser to buy used. But if you want to buy new, you should plan to drive the car for 10 years or more.
Better yet – do not buy a new vehicle.
***
The 20/4/10 rule for buying a vehicle
If you have to borrow when buying a car, to avoid spending more than you can afford you should put down at least 20%, keep the loan limited to no more than four years (to avoid interest), and spend no more than 10% of your gross income on transportation costs (which includes the car payment, parking, gas, and insurance).
Book Dr. David E. Marcinko MBA MBBSfor your Next Medical, Pharma or Financial Services Seminar orPersonal and Corporate Coaching Sessions
Dr. Marcinko enjoys personal coaching and public speaking and gives as many talks each year as possible, at a variety of medical society and financial services conferences around the country and world.
These include lectures and visiting professorships at major academic centers, keynote lectures for hospitals, economic seminars and health systems, endnote lectures at city and statewide financial coalitions, and annual engagements for a variety of internal and external yearly meetings.
After an understandable slowdown in 2020, due to the onset of the COVID-19 pandemic, merger & acquisition (M&A) activity in the healthcare industry accelerated in 2021, and the industry is expected to continue the high number of deals and high deal volume in 2022.
***
***
This Health Capital Topics article will review the U.S. healthcare industry’s M&A activity in 2021, and discuss what these trends may mean for 2022. (Read more…)
Posted on February 24, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Staff Reporters
***
OIL: Brent crude, the world benchmark, briefly climbed above $100 a barrel for the first time since 2014. US crude jumped 3.3% to $95.15 a barrel.
U.S. stock indexes: All closed sharply lower with the DJIA narrowly avoiding a slip into correction, as U.S. officials warned that Russian troops were poised to attack, and are attacking, the Ukraine raising anxieties among investors who are also wrangling with changing monetary policy and surging inflation.
How did stock indexes trade? The Dow Jones Industrial Average fell 464.85 points, or 1.4%, to end at 33,131.76. A finish below 33,119.69 would mark a 10% decline from the Dow’s Jan. 4 record close, meeting the commonly used definition of a correction. The S&P 500 index fell 79.26 points, or 1.8%, to around 4,225.50, deepening its stumble into correction territory. The NASDAQ Composite Index declined 344.03 points, or 2.6%, at 13,037.49, with 12,845.95 representing the level that would represent a bear market for the technology-laden index.
Asia: Hong Kong’s Hang Seng Index declined 3.2%. Korea’s Kospi dropped 2.7%. Japan’s Nikkei 225 lost 2.4% after coming back from a holiday. China’s Shanghai Composite moved 0.9% lower.
Posted on February 23, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Staff Reporters
***
MARKETS: The S&P 500 fell into a correction for the first time in two years, joining the NASDAQ Composite, as Russia sent troops into pro-Russian regions in Ukraine. The S&P 500 index ended down 1% at 4,304.76, below the correction level at 4,316.91, which would represent a 10% drop from its January 3rd record close. A correction is commonly defined by market technicians as a fall of at least 10% (but not greater than 20%) from a recent peak. The last time the S&P 500 entered a correction was February 27th 2020, when the market was being whipsawed by fears about the outbreak of the COVID pandemic.
And, this bearish market isn’t sparing 2021 winners like Home Depot, which fell the most in nearly two years after supply-chain bottlenecks squeezed its margins. HD was the Dow’s biggest gainer last year.
IRS: According to a news release issued by the IRS, taxpayers now have the option to verify their identities during live, virtual interviews with agents. The agency stresses that no bio-metric data will be required for those interviews.
However, taxpayers once again have the option to verify their identity using ID.me’s facial recognition services. Addressing privacy concerns, the IRS says new requirements are in place to ensure that images provided will be deleted upon verification. That would apply to any new IRS accounts created and those where selfies have already been collected.
Posted on February 22, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Staff Reporters
***
***
Markets: The domestic markets were closed yesterday as stocks around the world tumbled.
Crypto: Bitcoin was trading at $36,649 at 2:30 a.m. ET, falling nearly 6.5% in the last 24 hours, according to data from CoinDesk. The world’s most valuable cryptocurrency fell below $40,000 over the weekend, and has continued to slide as the Ukraine crisis intensifies. The currency has lost almost half its value since its November high of $68,990 due to geopolitical tensions, the prospect of interest rate hikes by the US Federal Reserve and curbs by some major economies on digital assets. Bitcoin’s peers have also been faring poorly. Ethereum, the world’s second most valuable cryptocurrency, fell over 8% in the last 24 hours and was trading at $2,520.
Putin: Russian President Vladimir Putin dramatically escalated the Ukrainian conflict. He recognized two separatist regions in eastern Ukraine as independent and ordered Russian troops to enter those areas, which may provide the pretext for an invasion of other parts of the country. Western leaders condemned the move as a violation of international law and the US said it will impose sanctions on those regions.
Posted on February 16, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
MARKETS: The Dow jumped 422 points, or 1.2%. The S&P 500 surged 1.5% and the NASDAQ was 2.5% higher.
OIL: US oil futures tumbled 3.7% to just under $92 a barrel. That’s despite the fact that Russia stressed that major military exercises would continue.
CPI: The Producer Price Index rose 1% last month, marking a significant acceleration from December’s 0.2% jump.
Meta: As Varietyreports, the company has agreed to pay $90 million to settle a 2012 class action lawsuit accusing it of violating users’ privacy. Facebook allegedly overstepped its bounds in 2010 and 2011 by using tracking cookies that monitored browsing after users signed out despite promises to the contrary.
MODERNA: Moderna Inc (NASDAQ: MRNA) shares were down more than 40% since the start of the year and continues to trend lower. Vaccine stocks are facing selling pressure as the COVID-19 omicron variant fades, but Moderna investors have been expressing concerns about recent stock sales from CEO Stéphane Bancel, as well as the presumed deletion of his Twitter account.
Posted on February 6, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
****
***
It’s February – American Heart Month – a time when the nation spotlights heart disease, the No. 1 killer of Americans.
President Lyndon B. Johnson, among the millions of people in the country who’d had heart attacks, issued the first proclamation in 1964. Since then, U.S. presidents have annually declared February American Heart Month.
Throughout the month, the American Heart Association’s “Heart to Heart: Why Losing One Woman Is Too Many” campaign will raise awareness about how 1 in 3 women are diagnosed with heart disease annually.
The first Friday of American Heart Month, Feb. 5, is also National Wear Red Day as part of the AHA’s Go Red for Women initiative. Coast to coast, landmarks, news anchors and neighborhoods go red to raise awareness and support for the fight against heart disease. For more information on the event and other activities during the month, visit goredforwomen.org.
This year, the federally designated event is even more important due to the impact of the coronavirus on the public’s heart health, including potential harmful effects on the heart and vascular system, according to recent research.
Also, during the COVID-19 pandemic, many people have delayed or avoided going to hospitals for heart attacks and strokes – netting poorer outcomes and prompting the AHA to create “Don’t Die of Doubt,” a national awareness campaign that reminds people that hospitals are the safest place to go when you have symptoms.
And while in lock-down, more people have engaged in unhealthy lifestyle behaviors, such as eating poorly, drinking more alcohol and limiting physical activity, that can contribute to heart disease.
Meanwhile, heart disease continues to be the greatest health threat to Americans and is still the leading cause of death worldwide, according to the AHA’s Heart Disease and Stroke Statistics – 2021 Update.
The update, published in the association’s flagship journal Circulation, reports that nearly 18.6 million people across the globe died of cardiovascular disease in 2019, the latest year for which worldwide statistics are calculated. That’s a 17.1% increase over the past decade. And 523.2 million cases of cardiovascular disease were reported in 2019, a 26.6% increase over 2010.
During American Heart Month, the AHA and other organizations reinforce the importance of heart health, the need for more research and efforts to ensure that millions of people live longer and healthier.
In most cases, heart disease is preventable when people adopt a healthy lifestyle, which includes not smoking, maintaining a healthy weight, controlling blood sugar and cholesterol, treating high blood pressure, getting at least 150 minutes of moderate-intensity physical activity a week and getting regular checkups.
Posted on February 4, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
A recent Johns Hopkins analysis of 676 U.S. health systems found that these 4 health systems contributed to healthcare overuse the most:
• St. Dominic Health Services in Jackson, Mississippi • USMD Health System in Irving, Texas • Community Medical Centers in Clovis, California • Care New England Health System in Providence, Rhode Island
Posted on January 31, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Ann Miller RN MHACMP®
Executive Director
***
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism.
We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial.
And, our consultants “got fly”, just like U.
Read it! Write it! Post it! “Medical Executive-Post”.
Call or email us for your FREE advertising and sales consultation TODAY [770.448.0769]
Posted on January 26, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
Maestro Health: Top 5 Ranked Risk Areas
Maestro Health surveyed 600 U.S.-based HR professionals. Survey respondents anticipate their company’s medical costs will increase. The top areas at risk are:
• Decreases in annual physicals/screenings: 62% • Increased pharmaceutical costs: 49% • Unvaccinated employees: 47% • More elective surgeries: 46% • Increased urgent care costs: 45%
The business cycle is also known as the economic cycle and reflects the expansion or contraction in economic activity. Understanding the business cycle and the indicators used to determine its phases may influence investment or economic business decisions and financial or medical planning expectations. Although often depicted as the regular rising and falling of an episodic curve, the business cycle is very irregular in terms of amplitude and duration.
Moreover, many elements move together during the cycle and individual elements seldom carry enough momentum to cause the cycle to move. However, elements may have a domino effect on one another, and this is ultimately drives the cycle. We can also have a large positive cycle, coincident with a smaller but still negative cycle, as seen in the current healthcare climate of today.
First Phase: Trough to Recovery (production driven)
Scenario: A depressed GNP leads to declining industrial production and capacity utilization. Decreased workloads result in improved labor productivity and reduced labor (unit) costs until actual producer (wholesale) prices decline.
Second Phase: Recovery to Expansion (consumer driven)
Scenario: CPI declines (due to reduced wholesale prices) and consumer real income rises, improving consumer sentiment and actual demand for consumer goods.
Third Phase: Expansion to Peak (production driven)
Scenario: GNP rises leading to increased industrial production and capacity utilization. But, labor productivity declines and unit labor costs and producer (wholesale) prices rise.
Fourth Phase: Peak to Contraction (consumer driven)
Scenario: CPI rises making consumer real income and sentiment erode until consumer demand, and ultimately purchases, shrink dramatically. Recessions may occur and economists have an alphabet used to describe them.
For example, with a V, the drop and recovery is quick. For U, the economy moves up more sluggishly from the bottom. A W is what you would expect: repeated recoveries and declines. An L shaper recession describes a prolonged dry economic spell or even depression.
NOTE: Historically, contractions have had a shorter duration than expansions.
Bull and Bear Markets for Medical Professionals
A bull market is generally one of rising stock prices, while a bear market is the opposite. There are usually two bulls for every one bear market over the long term.
More specifically, a bear market is defined as a drop of twenty percent or more in a market index from its high, and can vary in duration and severity. While a bull market has no such threshold requirement to exist, other than they exist between these two periods of sharp decline.
Whither the Bear?
As a doctor, your action plan in a bear market depends on many variables, with perhaps your age being the most important:
In your 30s:
Pay off debts, school or practice loans.
Invest in safe money market mutual funds, cash or CDs.
Start retirement plan or 401-K account.
In your 40s:
Increase your pension plan or 401-K contributions.
Stay weighted more toward equity investments.
Review your goals, risk tolerance and portfolio.
In your 50s:
Position assets for ready cash instruments.
Diversify into stock, bonds and cash.
Retirement:
Maintain 3 years of ready cash living expenses.
Reduce, but still maintain your exposure to equities.
ASSESSMENT: So, where are we right now in the economic business cycle? Your thoughts are appreciated.
Whether you do contract work or have your own small business, tax deductions for the self-employed physician consultant and/or medical executive or nurse consultant, etc., can add up to substantial tax savings.
With self-employment comes freedom, responsibility, and a lot of expense. While most self-employed people celebrate the first two, they cringe at the latter, especially at tax time. They might not be aware of some of the tax write-offs to which they are entitled.
When it comes time to file your returns, don’t hesitate to claim the benefits you get for being the boss. As a self-employed success story, you’ve earned them.
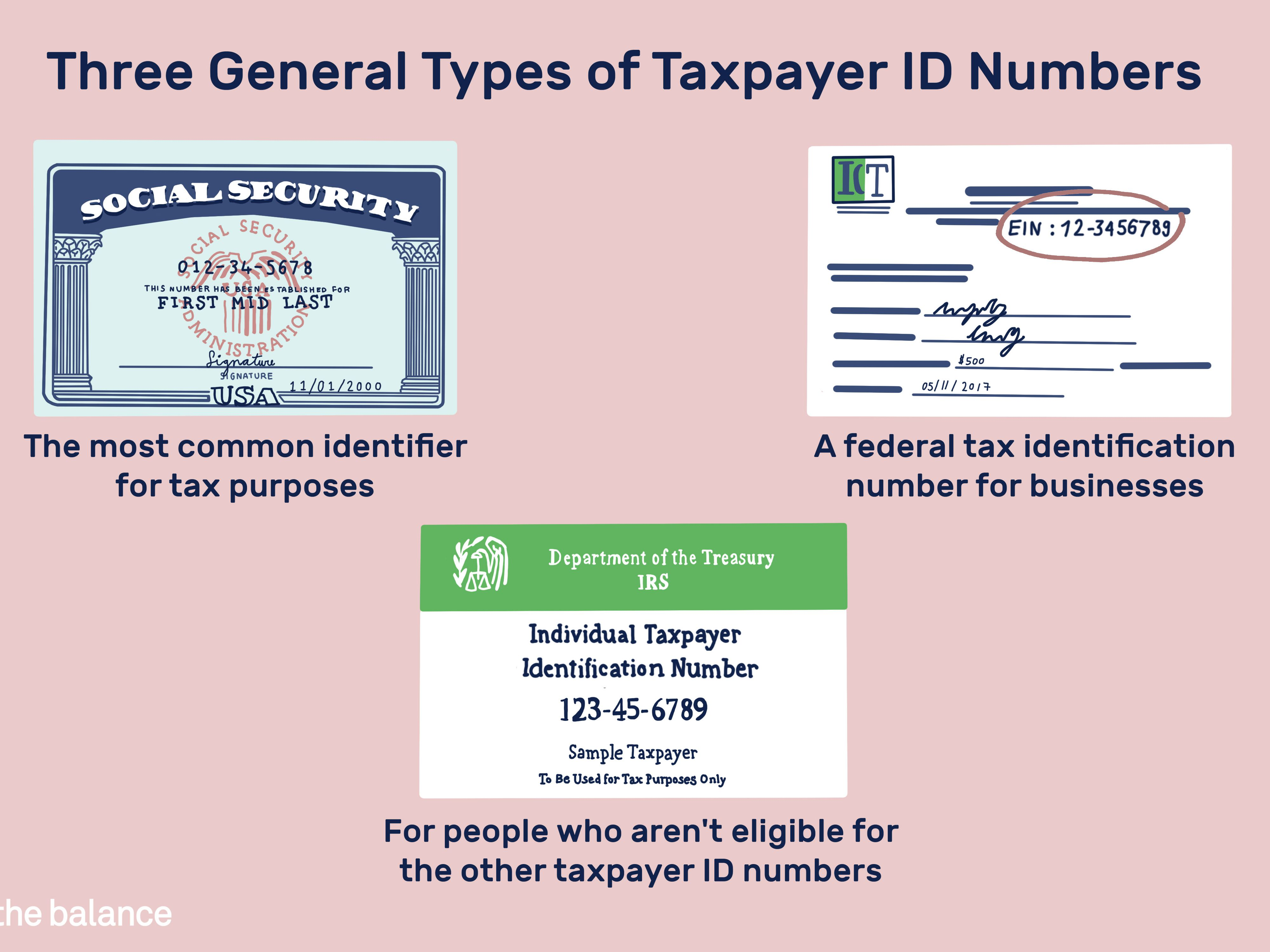
FORM 1099NEC: Form 1099 NEC is one of several IRS tax forms used in the United States to prepare and file an information return to report various types of income other than wages, salaries, and tips. The term information return is used in contrast to the term tax return although the latter term is sometimes used colloquially to describe both kinds of returns.
“Many times an overlooked deduction is educational expenses. If one is taking courses or buying research material to be more effective in their work, this can be deductible.”
Individual Retirement Plans (IRAs)
One of the best tax write-offs for the self-employed physician consultant is a retirement plan. A person with no employees can set up an individual 401 (k). “You can contribute $19,500 in 2021 as a 401(k) deferral, plus 25 percent of net income.”
If you have employees, consider a SIMPLE (Savings Incentive Match Plan for Employees) IRA—an IRA-based plan that gives small employers a simplified method to make contributions to their employees’ retirement. As of 2021, an employee may defer up to $13,500 and employees over 50 may contribute an additional $3,000.
“A third retirement plan is Simplified Employee Pension IRA (SEP IRA).” The employer may contribute the lesser of 25 percent of income or $58,000 in 2021. If the employer has eligible employees, an equal percentage of their income must be contributed.
Recall that retirement plans are “absolutely the No. 1 tax deduction. The government is helping fund retirement.”
Business use of home or dwelling
Now, most self-employed taxpayers’ businesses start as home-based businesses. These people need to know portions of business costs are deductible and so “It is very important that you keep track of expenses relating to your housing costs.”
If your gross income from your business exceeds your total expenses, then you can deduct all of your expenses related to the business use of your home. If your gross income is less than your total expenses, your deduction will be limited to the difference between your gross income and the sum of all business expenses you would pay if the business was not in your home. Those expenses could include telephone lines, the Internet, and other costs to do business.
You must also have a home office that is truly used for work and the Internal Revenue Service may require you to document this.
***
Deducting automobile expenses
If you travel for business, even short distances within your own city, you may deduct the dollar value of business miles traveled on your tax return. The taxpayer may file the actual expense s/he incurred, or use the standard mileage rate prescribed by the IRS, which is 56 cents as of 2021. The IRS allowable mileage rates should be checked every year as they can change.
“If you decide to use actual car expenses, be sure to include payments, depreciation, registration, insurance, garage rent, licenses, repairs and maintenance, and parking and toll fees.” AND, “If you decide to use the standard mileage rate, it would be in your best interest to keep a log—daily, weekly or monthly—of miles driven to distinguish personal use from business use.”
Depreciation of property and equipment
Some self-employed people may purchase property and equipment for a business. If they expect that property to last longer than one year, it should be depreciated on the tax return.
Claims regarding property, according to the IRS, must meet the following criteria: You must own the property and it must be used or held to generate income. The property should have an estimated useful life, meaning you should be able to guess how long you can generate income with it. It may not have a useful life of one year or less, and may not be purchased and disposed of in the same year.
Certain repairs on property used for business may also be deducted.
Educational expenses
Any educational expense is potentially tax-deductible.
“Many times an overlooked deduction is educational expenses. “If one is taking courses or buying research material to be more effective in their work, this can be deductible.”
Think about any books, web courses, local college courses, or other classes or materials that you have purchased to improve your job or business. It’s easy to forget a work-related webinar or business e-book that was purchased online, so remember to save e-receipts.
Also recall that subscriptions to trade or professional publications and donations to business organizations, both of which are frequently necessary for the continuation and growth of your business.
Other areas to explore
Other deductions that can be easily missed are advertising and promotional expenses, banking fees, and air, bus, or train fare. Restaurant meals and other entertainment costs may be written off as long as they are necessary business expenses.
And, consider health insurance premiums, which in most cases represent a credit rather than a tax deduction. “A credit goes directly against one’s taxes, rather than a reduction of income.”
Regardless of which expenses you discover that you may write off, the most important thing is to keep accurate records throughout the year. Save receipts, including e-mail receipts, and file or log them so you have easy access to them at tax time. Not only does keeping receipts, mileage logs, and other expense records make filing taxes easier, but it also facilitates a system that allows you to track changes from year to year.
***
Long-term tax-saving strategies
Don’t just look at last-minute write-offs when considering self-employment tax deductions. Think about laying down some long-term strategies for money savings from year to year—particularly if you are a high earner.
“Accountants typically tell you what you have to pay but they don’t always tell you strategies to reduce your payments.”
To reduce your gross taxable income, consider setting up a defined-benefit pension plan. This plan is based on your age and income: The older you are and the higher your earnings, the more you are allowed to contribute. An alternative plan is an age-weighted profit-sharing plan, which is similar and can benefit those who have several employees.
Another strategy for high-earning business owners who own their own building through a limited liability company or similar business structure is to pay themselves rent. This rent is used to pay down the mortgage, but it is also considered a business expense for tax purposes.
Self-employed professionals required to have liability insurance should consider setting up their own insurance company. A captive insurance company is one that insures the risks of the business—or businesses, in the case of a cooperative. Its premiums can be tax-deductible.
But, if money accumulates and claims are minimal, the money taken out is taxable under capital gains. This is not a retirement strategy, but that it can save you money by allowing you to “pay yourself” instead of an insurance company and still deduct the premiums.
Assessment
With any of these more complicated, long-term strategies, consult with a business attorney, CPA/EA or financial planner to ensure you have the best plan possible for your business.
Posted on January 24, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
Stock Markets: The S&P is off to its worst start to a year since 2016. The NASDAQ is in a correction. And the week ahead features a busy earnings slate and a Federal Reserve meeting.
CovisPandemic: Tony Dr. Fauci said he is “confident as you can be” that the Omicron wave in the US will peak by mid-February. In a growing number of states, that peak has already come and gone and cases are plunging in states like New York and Florida. Other states, such as Oklahoma, Idaho, and Wyoming, are still reporting an uptick in new Covid cases.
Crypto-Currency: Crypto investors, meanwhile, wish they got the weekend off like stock traders, because bitcoin, ethereum, and other digital tokens continued to sink.
Federal Reserve: Federal Reserve officials will get together on Tuesday and Wednesday against the backdrop of quaking markets. Investors will want to hear an update on Chair Jerome Powell’s views on inflation. This Fed meeting will likely be the last before an anticipated interest rate hike in March. And, a blizzard of companies will report including nearly half of the Dow’s 30 giants (American Express, 3M, IBM, and more) and tech heavyweights such as Apple, Microsoft, and Tesla.
Tax Season: The income tax filing season opens today and government officials warn it could be bumpy due to a depleted IRS. The Treasury says to file early, file online, and request your refund via direct deposit to avoid the severe headaches.
Posted on January 18, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
Markets: The stock market was closed for Martin Luther King Jr. Day. Maybe a day off is just what the market needs to score its first winning week of 2022. But … For many stocks, 2022 was a real bear of a year. More than 220 US-listed companies with a market cap of $10+ billion are down at least 20% from their peaks. And things are even worse in the tech-heavy NASDAQ, where 39% of companies have dropped at least half from their all-time highs.
Economy: A combo of Omicron disruptions, higher inflation, and shortages of everything has caused forecasters to lower their projections for economic growth this quarter. Analysts surveyed by the WSJ dropped their Q1 forecast to 3% annual growth from 4.2% back in October.
China: World shares were mixed after China reported that its economy expanded at an 8.1% annual pace in 2021, though growth slowed to half that level in the last quarter. And, Paris, Frankfurt, Tokyo and Shanghai advanced while Hong Kong and Seoul declined.
Posted on January 16, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
The 2-Ps [80/20] Rule
[By staff reporters]
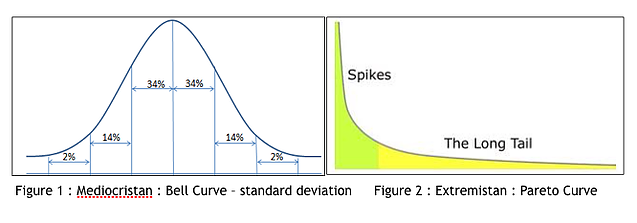
Pareto’s law is either of the following closely related ideas: Pareto principle or law of the vital few, stating that 80% of the effects come from 20% of the causes Pareto distribution
Pareto distribution
The Pareto distribution, named after the Italian civil engineer, economist, and sociologist Vilfredo Pareto, is a power law probability distribution that is used in description of social, scientific, geophysical, actuarial, and many other types of observable phenomena. en.wikipedia.org
Posted on January 16, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Mitigations for the Digital Health Era
By Shahid N. Shah MS
There has been a tremendous explosion of information technology (IT) in healthcare caused by billions of dollars of government incentives for usage of digital healthcare tools. But, IT systems face threats with significant adverse impacts on institutional assets, patients, and partners if sensitive data is ever compromised. Every health enterprise is required to confidentiality, integrity and availability of its information assets (this is called “information assurance” or IA). Confidentiality means private or confidential information must not be disclosed to unauthorized persons. Integrity means that the information can be changed only in an authorized manner so as to maintain the correctness of the information. Availability defines the characteristic that information systems work as intended and all services are available to its users whenever necessary.
It is well known that healthcare organizations face and have been mitigating many risks such as investment risk, budgetary risk, program management risk, safety risk, and inventory risk for many years. What’s new in the last decade or so is that organizations must now manage risks related to information systems because operating systems [OSs] are also at risk. IT is now just as a critical an asset as most other infrastructure managed by health systems. It is important that information security risks are given the same or more importance and priority as given to other organizational risks.
As health records move from paper native to digital native, it’s vital that organizations have information risk management programs and security procedures that woven into the culture of the organization. For this to happen, basic requirements of information security must be defined and implemented as part of both the operational and management processes. A framework that provides guidance on how to perform these activities, and the co-ordination required between these activities is needed.
INTRODUCTION
The Risk Management Framework (RMF), supported by the National Institute of Standards and Technology (NIST) provides this framework. The NIST 800 series publications provide a structured approach to achieve risk management. It provides broad guidance and not necessarily all the prescriptions, which means it can be tailored to meet the organization’s specific needs and providing the flexibility needed for the different organizations. Using the NIST RMF helps organizations with risk management not only in a repeatable manner, but also with greater efficiency and effectiveness. Healthcare information assurance is complex and without a framework that takes into account a broad risk management approach, it is difficult to consider all the intricacies involved.
NIST Risk Management Framework
The NIST Risk Management Framework consists of a six step process designed to guide organizations in managing the risks in their information systems. The various steps as defined in the NIST specifications are the following:
Categorize the information system and the information processed, stored, and transmitted by that system based on an impact analysis.
Select an initial set of baseline security controls for the information system based on the security categorization; tailoring and supplementing the security control baseline as needed based on an organizational assessment of risk and local conditions
Implement the security controls and describe how the controls are employed within the information system and its environment of operation.
Assess the security controls using appropriate assessment procedures to determine the extent to which the controls are implemented correctly, operating as intended, and producing the desired outcome with respect to meeting the security requirements for the system.
Authorize information system operation based on a determination of the risk to organizational operations and assets, individuals, other organizations, and the Nation resulting from the operation of the information system and the decision that this risk is acceptable.
Monitor the security controls in the information system on an ongoing basis including assessing control effectiveness, documenting changes to the system or its environment of operation, conducting security impact analyses of the associated changes, and reporting the security state of the system to designated organizational officials.
All information systems process, store and transmit information. What is the possible impact if a worst case scenario occurs that causes endangers this information? A structured way to find out the potential impact on the confidentiality, integrity and availability of information can be done through the first step of NIST RMP, the categorization of information systems. The NIST SP 800-60 provides such guidance. The potential impact is assigned qualitative values – low, moderate, or high. Based on these impact levels for each of the information type contained in the system, the high water mark level is calculated, that helps in selecting the appropriate controls in the subsequent steps.
Organizations need to mitigate risks adequately by selecting an appropriate set of controls that would work effectively. In the selection of security controls step, the set of controls are chosen based on the categorization of the information system, the high water mark and the goals of the organizations. These baseline controls are selected from NIST SP 800-53 specification, one of three sets of baseline controls, corresponding to low, moderate, high impact rating of the information system. These baseline controls can be modified to meet specific business needs and organization goals. These tailored controls can be supplemented with additional controls, if needed, to meet unique organizational policies and environment factors and its security requirements and its risk appetite. The minimum assurance requirements need to be specified here.
All the activities necessary for having the selected controls in place, is done in the implementation of security controls step. The implementation of the selected security controls will have an impact on the organization risks and its effects. NIST SP 800-70 can be used as guidance for the implementation. An implementation strategy has to be planned and the actions have to be defined and the implementation plan needs to be reviewed and approved, before the implementation is done.
Once the controls are implemented, then the assessment of security controls is done to find out whether the controls have been correctly implemented, working as intended, and giving the desired output with respect to the security requirements. In short, whether the applied security controls are indeed the right ones, done in the right way, giving the right outcome. NIST SP 800-53,, NIST 800-53A, NIST 800-115 can provide the necessary guidance, here.
IS authorization
The authorization of information systems is an official management decision, authorizing that the information system can be made operational, with the identified risks mitigated and the residual risks accepted, and is accountable for any adverse impacts on the confidentiality, integrity and availability of information systems. If the authorizing personnel find that the risks are not mitigated and hence can compromise the sensitive information, they can deny authorizing the information system. NIST SP 800-37 provides guidance on authorization. The authorizing personnel are to be involved actively throughout the risk management process.
Risk management is not one-time process, that once it is done, it is forgotten. It is a continuous process, to be integrated with day-to-day activities. One of the key aspects of any risk management is the monitoring of security controls to check whether the controls are performing as intended. The main focus of monitoring security controls is to know whether the controls are still effective over a period time, given the changes that occur in the information systems — the changes in hardware, software and firmware, the changes in environment factors, operating conditions etc. NIST SP 800-37 provides guidance about this. And if the security controls are found to be ineffective, the cycle starts again, with either re-categorization or selecting another set of baseline controls, or assessing the effectiveness of the controls once more etc.
And, in all the steps in risk management framework, one of the important aspects is communication. Appropriate documents needed to be generated in all the steps, reviewed and kept up-to-date.
Assessment
Organizational risk management provides great benefits to the organization because it helps to prioritize the resources, increase interoperability, and reduce costs incurred due to the adverse effects. It helps to prevent unauthorized access to personally identifiable information which will lead to security breaches.
Posted on January 11, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
BY ERIC BRICKER MD
With 43 Million Americans Having Lost Their Job at Some Point During the Pandemic and About 1/2 Those Jobs Providing Health Insurance… the 1st Group–People Who Do Not Have Health Insurance–Needs to Be Aware of How These Programs Work.
In this Video You Will Learn the Patient Assistance Program Process for:
1) 2 of the Most Common Types of Insulin
2) The Highest-Revenue Medication in America: Humira
**Note: At the Time of the Video’s Recording, the Unemployment Rate in the US was 15%. As of November 2021, the Unemployment Rate is 4.2%.
Posted on January 10, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
Markets: Stocks are off to a sputtering start in 2022, and they could be in for more upheaval this week with a big inflation report due, Fed Chair Jerome Powell’s confirmation hearing on Capitol Hill, and the beginning of earnings season.
NASDAQ: Last week, the tech-heavy NASDAQ fell 4.5% for its worst week since February 2021. And the ARK Innovation ETF, which is full of high-growth tech companies, plunged 11%.
Bonds: Over in the bond market, yields (or the return you can get from buying a bond) are surging. On Friday, the yield for the 10-year Treasury note hit its highest level since January 2020. Now, While rising yields are generally a bullish sign for the economy, they also make riskier assets—like expensive tech stocks—less attractive compared to other names that may get a boost from higher interest rates. The Dow, for example, with its many financial services companies, lost just 0.29% last week.
Good News: Billionaire investor Chamath Palihapitiya said US stocks could rebound rapidly after the recent sell-off. He said there’s “a ton” of money waiting on the sidelines in products such as money market accounts.
Posted on January 6, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
Markets: Already through a rough day, stocks dove even lower after the Fed released the minutes from its December meeting. Tech companies continued to get clobbered as rising bond yields make their shares less attractive.
About the Federal Reserve Minutes: Inflation anxiety was real at the central bank’s previous meeting, and officials signaled they could hike interest rates “sooner or at a faster pace” than previously expected to cool down prices.
Posted on January 4, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
Dear Dr. David Marcinko,
With warm wishes for a joyful holiday, we are please to announce that the layout of AJPH is almost back on schedule, following COVID-19 related impacts to our production team. To keep these monthly highlight emails synched, we are going to highlight articles in two issues of AJPH.
The December issue of AJPH features multiple articles focused on surveillance, surveys and COVID-19, along with articles discussing physical and mental health of home health care workers, racial and ethnic disparities in the impact of COVID-19 in the active U.S. military and firearm injury & gun violence. Here are a few of the many articles in the December 2021 issue:
The mission of AJPH is to advance public health research, policy, practice and education. Toward that goal, the journal also produces monthly podcasts available in English and Chinese at ajph.org. The monthly podcasts are also on iTunes and Google Play.
AJPH and the Centers for Disease Control and Prevention are seeking papers for an issue on “Ubiquitous Lead: Risks, Prevention-Mitigation Programs and Emerging Sources of Exposure.” Manuscripts must be submitted to AJPH by Jan. 30. For additional information about the supplement, contact T. LeBlanc.
Happy Holidays!
Alfredo Morabia, MD, PhD Editor-in-Chief, AJPH @AlfredoMorabia @AMJPublicHealth Join APHA and get full access to AJPH, the official journal of the American Public Health Association.
Posted on January 3, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
WHAT IT IS – HOW IT WORKS – WHY?
By Staff Reporters
***
What it is: With its use as a commodity tracing back to Ancient Lydian merchants over 2,500 years ago, gold has the most staying power of any indicator on this list. When investors talk about gold prices today, they’re most likely referring to the price per ounce of gold bullion (those gold bars bad guys keep in briefcases).
How it works: Gold is priced in U.S. dollars around the world. Investors can buy physical gold in the form of bullion or coins or go for more intangible gold securities, such as futures, ETF shares, or investments in gold mining companies.
Why it matters: In a 21st century economy where currencies aren’t pegged to the gold standard and credit cards are the medium of exchange, some investors argue gold is a relic. But others turn to the metal for diversification or as a “safe-haven asset”—something to buy during times of geopolitical or economic uncertainty because it holds onto its value.
Posted on December 13, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
ALL TIME HIGHS?
***
Markets: The S&P begins the week after closing at an all-time high last Friday. The index has closed at a record more times this year (67) than in any other year since 1995. It needs 10 more to tie the mark.
More S&P fun facts: Microsoft, Alphabet, Apple, Nvidia, and Tesla alone account for over a third of the S&P’s gains this year.
Posted on November 15, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
CELEBRATE AND GIVE TODAY?
By Staff Reporters
National Philanthropy Day is an observance designated by the Association of Fundraising Professionals.
It is a day to celebrate charitable activities, in the form of donated financial, in-kind and volunteering support. It is celebrated with blog postings by AFP highlighting outstanding charitable activities, as well as luncheons and awards throughout the USA by different AFP chapters.
Posted on November 10, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
For Doctors and Advisors
BOOK REVIEWS WITH FOREWORD
Reviews
Written by doctors and healthcare professionals, this textbook should be mandatory reading for all medical school students―highly recommended for both young and veteran physicians―and an eliminating factor for any financial advisor who has not read it. The book uses jargon like ‘innovative,’ ‘transformational,’ and ‘disruptive’―all rightly so! It is the type of definitive financial lifestyle planning book we often seek, but seldom find. ―LeRoy Howard MA CMPTM,Candidate and Financial Advisor, Fayetteville, North Carolina I taught diagnostic radiology for over a decade. The physician-focused niche information, balanced perspectives, and insider industry transparency in this book may help save your financial life. ―Dr. William P. Scherer MS, Barry University, Ft. Lauderdale, Florida This book was crafted in response to the frustration felt by doctors who dealt with top financial, brokerage, and accounting firms. These non-fiduciary behemoths often prescribed costly wholesale solutions that were applicable to all, but customized for few, despite ever-changing needs. It is a must-read to learn why brokerage sales pitches or Internet resources will never replace the knowledge and deep advice of a physician-focused financial advisor, medical consultant, or collegial Certified Medical Planner™ financial professional. ―Parin Khotari MBA,Whitman School of Management, Syracuse University, New York In today’s healthcare environment, in order for providers to survive, they need to understand their current and future market trends, finances, operations, and impact of federal and state regulations. As a healthcare consulting professional for over 30 years supporting both the private and public sector, I recommend that providers understand and utilize the wealth of knowledge that is being conveyed in these chapters. Without this guidance providers will have a hard time navigating the supporting system which may impact their future revenue stream. I strongly endorse the contents of this book.
―Carol S. Miller BSN MBA PMP,President, Miller Consulting Group, ACT IAC Executive Committee Vice-Chair at-Large, HIMSS NCA Board Member This is an excellent book on financial planning for physicians and health professionals. It is all inclusive yet very easy to read with much valuable information. And, I have been expanding my business knowledge with all of Dr. Marcinko’s prior books. I highly recommend this one, too. It is a fine educational tool for all doctors.
―Dr. David B. Lumsden MD MS MA,Orthopedic Surgeon, Baltimore, Maryland There is no other comprehensive book like it to help doctors, nurses, and other medical providers accumulate and preserve the wealth that their years of education and hard work have earned them. ―Dr. Jason Dyken MD MBA, Dyken Wealth Strategies, Gulf Shores, Alabama I plan to give a copy of this book written ‘by doctors and for doctors’ to all my prospects, physician, and nurse clients. It may be the definitive text on this important topic. ―Alexander Naruska CPA, Orlando, Florida
Health professionals are small business owners who need to apply their self-discipline tactics in establishing and operating successful practices. Talented trainees are leaving the medical profession because they fail to balance the cost of attendance against a realistic business and financial plan. Principles like budgeting, saving, and living below one’s means, in order to make future investments for future growth, asset protection, and retirement possible are often lacking. This textbook guides the medical professional in his/her financial planning life journey from start to finish. It ranks a place in all medical school libraries and on each of our bookshelves. ―Dr. Thomas M. DeLauro DPM, Professor and Chairman – Division of Medical Sciences, New York College of Podiatric Medicine
Physicians are notoriously excellent at diagnosing and treating medical conditions. However, they are also notoriously deficient in managing the business aspects of their medical practices. Most will earn $20-30 million in their medical lifetime, but few know how to create wealth for themselves and their families. This book will help fill the void in physicians’ financial education. I have two recommendations: 1) every physician, young and old, should read this book; and 2) read it a second time! ―Dr. Neil Baum MD, Clinical Associate Professor of Urology, Tulane Medical School, New Orleans, Louisiana
I worked with a Certified Medical Planner™ on several occasions in the past, and will do so again in the future. This book codified the vast body of knowledge that helped in all facets of my financial life and professional medical practice. ―Dr. James E. Williams DABPS, Foot and Ankle Surgeon, Conyers, Georgia
Posted on November 8, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
NOT About the Sharpe Financial Ratio
[By Dr. David Edward Marcinko MBA]
SHARPE FINANCIAL RATIO
The Sharpe Ratio is the ‘excess’ return of an asset over the return of a risk free asset divided by the variability or standard deviation of returns.
The information ratio is the active return to the most relevant benchmark index divided by the standard deviation of the ‘active’ return or tracking error.
***
***
SHARP PHYSICIAN-SUICIDE INDEX
Janae Sharp is a physician suicide survivor and the founder of the “Sharp Index”. The Sharp Index has a mission to reduce physician suicide and provide meaningful tools to improve provider quality of life. The epidemic of physician suicide is costing us lives. Not only the lives of physicians themselves, but also patient lives.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
“Physicians who don’t understand modern risk management, insurance, business, and asset protection principles are sitting ducks waiting to be taken advantage of by unscrupulous insurance agents and financial advisors; and even their own prospective employers or partners. This comprehensive volume from Dr. David Marcinko and his co-authors will go a long way toward educating physicians on these critical subjects that were never taught in medical school or residency training.” —Dr. James M. Dahle, MD, FACEP, Editor of The White Coat Investor, Salt Lake City, Utah, USA
“With time at a premium, and so much vital information packed into one well organized resource, this comprehensive textbook should be on the desk of everyone serving in the healthcare ecosystem. The time you spend reading this frank and compelling book will be richly rewarded.” —Dr. J. Wesley Boyd, MD, PhD, MA, Harvard Medical School, Boston, Massachusetts, USA
“Physicians have more complex liability challenges to overcome in their lifetime, and less time to do it, than other professionals. Combined with a focus on practicing their discipline, many sadly fail to plan for their own future. They need trustworthy advice on how to effectively protect themselves, their family, and their practice from the many overt and covert risks that could potentially disrupt years of hard work.
Fortunately, this advice is contained within Risk Management, Liability Insurance, and Asset Protection Strategies for Doctors and Advisors: Best Practices from Leading Consultants and Certified Medical Planners™. Written by Dr. David Edward Marcinko, Nurse Hope Rachel Hetico, and their team of risk managers, accountants, insurance agents, attorneys, and physicians, it is uniquely positioned as an integration of applied, academic, and peer-reviewed strategies and research, with case studies from top consultants and Certified Medical Planners™. It contains the latest principles of risk management and asset protection strategies for the specific challenges of modern physicians. My belief is that any doctor who reads and applies even just a portion of this collective wisdom will be fiscally rewarded. The Institute of Medical Business Advisors has produced another outstanding reference for physicians that provide peace of mind inthis unique marketplace! In my opinion, it is a mandatory read for all medical professionals.” —David K. Luke, MS-PFP, MIM, CMP™, Net Worth Advisory Group, Inc., Sandy, Utah, USA
“This book is a well-constructed, comprehensive, and experiential view of risk management throughout the entire medical practice life-cycle. It is organized in an accessible, high-yield style that is familiar to doctors. Each chapter has case models, examples, insider tips, and useful pearls. I was pleased to see multi-degreed physicians sharing their professional experiences in a textbook on something other than clinical medicine. I can’t decide if this book is right on – over the top – or just plain prescient. Now, after a re-read, I conclude it is all of the above; and much more.” —Dr. Peter P. Sidoriak, Pottsville, Pennsylvania, USA
“When a practicing physician thinks about the risk exposure resulting from providing patient care, medical malpractice risk immediately comes to mind. But, malpractice and liability risk are barely the tip of the iceberg, and likely not even the biggest risk in the daily practice of medicine. There are risks from having medical records to keep private, risks related to proper billing and collections, risks from patients tripping on your office steps, risks from medical board actions, risk arising from divorce, and the list goes on and on. These liabilities put a doctor’s hard earned assets and career in a very vulnerable position. This new book from Dr. David Marcinko and Prof. Hope Hetico shows doctors the multiple types of risk they face and provides examples of steps to take to minimize them. It is written clearly and to the point, and is a valuable reference for any well-managed practice. Every doctor who wants to take preventive action against the risks coming at them… from all sides needs to read this book.” —Richard Berning, MD, FACC, New Haven, Connecticut, USA
“This is an excellent companion book to Dr. Marcinko’s Comprehensive Financial Planning Strategies For Doctors and Advisors: Best Practices from Leading Consultants and Certified Medical Planners™. It is all inclusive, yet easy to read, with current citations, references, and much frightening information. I highly recommend this text. It is a fine educational and risk management tool for all doctors and medical professionals.”—Dr. David B. Lumsden, MD, MS, MA, Orthopedic Surgeon, Baltimore, Maryland, USA
“This comprehensive text book provides an in-depth presentation of the cyber security and real risk management, asset protection, and insurance issues facing all medical professions today. It is far beyond the mere medical malpractice concerns I faced when originally entering practice decades ago.” —Dr. Barbara s. Schlefman, DPM, MS, Family Foot Care, PA, Tucker, Georgia, USA
“Am I over-insured and thus wasting money? Am I under-insured and thus at risk for a liability or other disaster? I never really had the means of answering these questions; until now.” —Dr. Lloyd M. Krieger, MD, MBA, Rodeo Drive Plastic Surgery, Beverly Hills, California, USA
“I read and use this book and several others from Dr. David Edward Marcinko and his team of advisors.” —Dr. John Kelley, DO, Orthopedic Surgeon, Tucker, Georgia, USA
“An important step in the risk management, insurance planning, and asset protection process is the assessment of needs. One can create a strong foundation for success only after all needs have been analyzed so that a plan can be constructed and then implemented. This book does an excellent job of recognizing those needs and addressing strategies to reduce them.“ —Shikha Mittra, MBA, CFP®, CRPS®, CMFC®, AIF®, President – Retire Smart Consulting LLC, Princeton, New Jersey, USA
“The Certified Medical Planner™ professional designation and education program was created by the Institute of Medical Business Advisors Inc., and Dr. David Edward Marcinko and his team (who wrote this book). It is intended for financial advisors who aim specifically to serve physicians and the medical community. Content focuses not only on the insurance and professional liability issues relevant to physicians, but also provides an understanding of the risky business of medical practice so advisors can help work more successfully with their doctor-clients.” —Michael E. Kitces, MSFS, MTAX, CFP®, CLU, ChFC, RHU, REBC, CASL Reston, Virginia, USA
“I have read this text and used consulting services from the Institute of Medical Business of Advisors, Inc. on several occasions.” —Dr. Marsha Lee, DO, Radiologists, Norcross, Georgia, USA
“The medical education system is grueling and designed to produce excellence in medical knowledge and patient care. What it doesn’t prepare us for are the slings and arrows that come our way once we actually start practicing medicine. Successfully avoiding these land mines can make all the difference in the world when it comes to having a fulfilling practice. Given the importance of risk management and mitigation, you would think these subjects would be front and center in both medical school and residency – ‘they aren’t.’ Thankfully, the brain trust over at iMBA Inc. has compiled this comprehensive guide designed to help you navigate these mine fields so that you can focus on what really matters – patient care.” —Dennis Bethel, MD, Emergency Medicine Physician
Posted on October 29, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Impact of Moving Older Adults from Employer Coverage to Medicare
Peterson-KFF’s recent brief “How Lowering the Medicare Eligibility Age Might Affect Employer-Sponsored Insurance Costs” explores potential percent reduction in employer health plan spending if all enrollees in age group leave large employer-sponsored coverage.
The brief found:
• Ages 60-64 would cause a 15% reduction • Ages 55-64 would cause a 30% reduction • Ages 50-64 would cause a 43% reduction
Posted on October 18, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
OCTOBER 18th, 2021
By Staff Reporters
***
October 18, 2021 (every third Monday in October) is Multicultural Diversity Day, a national day created by Cleorah Scruggs, a fourth-grade teacher in Flint, Michigan.
The day was adopted as a national event by the NEA’s 1993 Representative Assembly to “increase awareness of the tremendous need to celebrate our diversity collectively.”
The first World Financial Planning Day was held on October 4, 2017. The Financial Planning Standards Board (FPSB) hosts the day. Every year, the FPSB partners with the International Organization of Securities Commissions (IOSCO).
***
Today, it is always held during the first Wednesday of October during IOSCO’s World Investor Week.
***
QUERY: But, what about the entire ecosystem of personal and professional financial planning, investing, risk, business and medical practice management for physicians and healthcare professionals? A vital, unique and complicated niche!
ANSWER: According to the Institute of Medical Business Advisors, Inc., WFP Day is every day for CERTIFIED MEDICAL PLANNER® professional certification holders.
So – If you are in this WFPD industry – Become a fiduciary focused board CERTIFIED MEDICAL PLANNER with extreme healthcare industry ecosystem specificity.
Posted on October 2, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Bertalan Meskó, MD PhD
***
Two years ago, I was searching in the FDA’s database of artificial intelligence-based medical devices. The database had no such segment. What could I do? Started creating our own.
Together with fellow researchers at The Medical Futurist Institute, we created the first open-access, online database of FDA-approved A.I.-based technologies that got published in the prestigious journal npj Digital Medicine last year. Since then, we have repeatedly called upon the FDA to do its own database (and even offered ours), and finally, this past week the breakthrough happened: the FDA listed our database as a publicly available resource on the subject. I tell you why this step is important below.
Take care, Berci Bertalan Meskó, MD The Medical Futurist
How much will it cost you to start a dental practice – with Business Plan?
There are many costs to consider to set up a successful dental practice. Note that the following values are not the exact amount but an average of setting up a dental practice:
Purchase price – this includes valuation fees of between $1,000-4,500, solicitor fees of between $4,000 – 17,000, accountancy and bank fees of around $3,000, and bank solicitors, which can be up to $3,500. Many of these can be reduced or obliterated.
Materials – $40,000
Lab fees – $36,000
Staff costs – $82,000
Other costs (associates fees) – [$245,000 – $295,000]
Other Factors
“Big” Tech – Many startup doctors want to include CBCT or CAD/CAM or 3D printing in their startup, any of which can add $25,000-$175,000. In other situations, waiting is the best option.
Cabinetry Preferences – Costs for cabinetry can range from $5,000 to $175,000.
Practice Management Software (PMS) – Pricing will range from a few thousand dollars to $25,000; OR none at all.
Mechanical Delivery – Typically referred to as chairs, lights, and units, this category of dental equipment costs will range between $5,000 and $100,000 based on your startup plans.
Vision – Ignore the so-called “experts” who will try to create a cookie-cutter model for your equipment costs. That is the thinking of corporate dentistry. You want a customized private practice vision that allows you to create a model matching your standards. Prioritize your vision, so your values and philosophy will lead your dental equipment budget and purchasing decisions. Your equipment budget will be—and should be—customized.
































































 ***
***