BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Multiple‑choice tests are everywhere—schools, professional certifications, job assessments, even driver’s license exams. They’re popular because they can measure a wide range of knowledge quickly, but for the test‑taker, they can feel deceptively tricky. A question with four options looks simple on the surface, yet the difference between two answers may hinge on a single word. Doing well on a multiple‑choice test isn’t just about knowing the material; it’s about approaching the test strategically. With the right mindset and techniques, you can turn what feels like a guessing game into a controlled, confident performance.
The first step in mastering a multiple‑choice test happens before you even look at the questions: managing your time and your mindset. Walking into a test with a calm, focused attitude gives you a huge advantage. Anxiety narrows your thinking, while confidence opens it up. A few deep breaths, a quick mental reset, and a reminder that you’re prepared can shift your entire experience. Once the test begins, skim through it quickly to get a sense of its length and difficulty. This brief overview helps you pace yourself and avoid spending too much time on any single question.
When you begin answering, read each question carefully—more carefully than you think you need to. Multiple‑choice tests often rely on subtle wording. A single phrase like “most likely,” “least effective,” or “except” can completely change what the question is asking. Many students lose points not because they don’t know the material, but because they misread the prompt. Slow down enough to understand the question before you even glance at the answer choices. Sometimes, it helps to cover the options and try to answer the question in your head first. If your internal answer matches one of the choices, that’s a strong sign you’re on the right track.
Once you start evaluating the answer choices, eliminate the obviously wrong ones. Even if you’re unsure of the correct answer, narrowing the field increases your odds and helps you think more clearly. Some choices are designed to distract you—answers that sound familiar, include key terms from the question, or resemble something you studied but don’t actually fit. Cross out anything that is clearly incorrect, overly extreme, or unrelated to the core of the question. This process of elimination is one of the most powerful tools in multiple‑choice testing.
***
***
Another important strategy is to watch out for patterns in the answer choices. Test writers often include distractors that are partially correct or correct in a different context. If two answers seem almost identical, they’re probably not both right; look for the subtle difference that makes one more accurate. Conversely, if one answer is noticeably longer or more detailed than the others, it may be the correct one, since test writers sometimes add qualifiers to ensure accuracy. These patterns aren’t foolproof, but they can help when you’re stuck between options.
Context clues within the test itself can also be surprisingly helpful. Sometimes, one question will indirectly answer another. If you notice repeated terms, definitions, or concepts, use that information to your advantage. Tests are written by humans, and humans tend to repeat themselves. Just be careful not to over‑interpret patterns; use them as hints, not guarantees.
When you encounter a question that completely stumps you, don’t panic. Mark it, skip it, and move on. Getting stuck early can drain your time and confidence. Often, answering other questions jogs your memory or clarifies your thinking, and when you return to the difficult one later, it feels more manageable. This approach keeps your momentum going and prevents frustration from derailing your performance.
Guessing, when necessary, should be strategic rather than random. If you’ve eliminated even one or two options, your odds improve significantly. Look for clues in the wording: answers with absolute terms like “always” or “never” are often incorrect because they leave no room for exceptions. More moderate phrasing tends to be safer. If two answers contradict each other, one of them is likely correct. And if you truly have no idea, choose the option that seems most consistent with the overall logic of the test. A calm, reasoned guess is far better than a panicked one.
As you work through the test, keep an eye on your pacing. Divide the total time by the number of questions to get a rough sense of how long you can spend on each one. If you’re spending too long on a single question, move on. It’s better to answer all the questions you know first and return to the harder ones with whatever time remains. This approach ensures you don’t leave easy points on the table.
***
***
When you finish the last question, resist the urge to submit immediately. Use any remaining time to review your answers. Look especially for questions where you felt uncertain or rushed. However, avoid the temptation to change answers impulsively. Research and experience both show that your first instinct is often correct. Only change an answer if you have a clear, specific reason—such as noticing a misread word or recalling a relevant fact.
Finally, remember that multiple‑choice tests reward clarity of thinking as much as content knowledge. The more you practice these strategies, the more natural they become. Over time, you’ll start to recognize patterns, avoid common traps, and approach each test with greater confidence. Multiple‑choice tests may never be fun, but with the right techniques, they become far less intimidating and far more manageable.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The breakup of the Medical Act represents one of the most significant turning points in the evolution of modern healthcare governance. For decades, the Act served as a foundational framework that regulated medical practice, established professional standards, and defined the relationship between the state, medical institutions, and practitioners. Its dissolution did not occur suddenly; rather, it emerged from a complex interplay of political pressures, professional disputes, and shifting societal expectations. Understanding the breakup requires examining both the structural weaknesses within the Act itself and the broader forces that made its continuation untenable.
At its core, the Medical Act was designed to centralize authority over medical licensing and professional conduct. When it was first introduced, this centralization was seen as a necessary step toward ensuring uniform standards and protecting the public from unqualified practitioners. Over time, however, the rigidity of the Act became a source of tension. Medical knowledge expanded rapidly, new specialties emerged, and healthcare delivery became increasingly complex. Yet the Act remained anchored in assumptions that no longer reflected the realities of modern medicine. Many practitioners argued that the Act constrained innovation, limited professional autonomy, and failed to adapt to new models of care.
One of the major catalysts for the breakup was the growing dissatisfaction among medical professionals who felt that the Act imposed excessive bureaucratic oversight. Licensing procedures, disciplinary mechanisms, and continuing education requirements were often criticized as outdated or overly punitive. Younger practitioners, in particular, viewed the Act as an obstacle to entering the profession, citing long delays, inconsistent evaluation standards, and a lack of transparency. These frustrations fueled calls for reform, but attempts to revise the Act repeatedly stalled due to political disagreements and resistance from established institutions that benefited from the status quo.
Another factor contributing to the breakup was the increasing involvement of non‑physician healthcare providers in delivering essential services. Nurses, physician assistants, pharmacists, and other allied health professionals sought expanded scopes of practice to meet rising patient demand. However, the Medical Act was built around a physician‑centric model that did not easily accommodate these shifts. As collaborative care models became more common, the Act’s limitations became more apparent. Conflicts emerged over authority, responsibility, and professional boundaries, creating friction within the healthcare system. The inability of the Act to adapt to these new dynamics weakened its legitimacy and fueled arguments for its dissolution.
Public expectations also played a significant role. Patients became more informed, more vocal, and more demanding of accountability. They expected transparency in medical decision‑making, greater access to care, and more equitable treatment across communities. Yet the Medical Act was often criticized for protecting professional interests rather than prioritizing patient welfare. High‑profile cases involving malpractice, discrimination, or regulatory failures eroded public trust. Advocacy groups argued that the Act lacked sufficient mechanisms for patient representation and that its disciplinary processes were opaque and slow. As public pressure mounted, political leaders found it increasingly difficult to defend the existing framework.
***
***
The breakup of the Medical Act was ultimately driven by a convergence of these pressures. When reform efforts repeatedly failed, stakeholders began to explore alternative regulatory models. Some advocated for decentralization, arguing that regional or specialty‑specific bodies could respond more effectively to local needs. Others pushed for a more integrated system that would regulate all healthcare professionals under a unified framework, promoting collaboration and reducing duplication. The eventual dissolution of the Act opened the door to these new possibilities, though not without controversy.
The consequences of the breakup have been far‑reaching. On one hand, it created opportunities for modernization. New regulatory structures have been more flexible, more responsive to emerging trends, and more inclusive of diverse healthcare professions. Licensing processes have been streamlined, interdisciplinary collaboration has improved, and patient advocacy has gained a stronger voice in governance. Many practitioners feel that the new system better reflects the realities of contemporary healthcare and supports innovation rather than hindering it.
On the other hand, the transition has not been without challenges. The breakup initially created uncertainty, as practitioners and institutions navigated shifting rules and responsibilities. Some critics argue that decentralization has led to inconsistencies in standards, making it harder to ensure uniform quality of care. Others worry that the new system may lack the strong oversight mechanisms that once protected the public. Balancing flexibility with accountability remains an ongoing struggle, and debates continue over how best to regulate a rapidly evolving healthcare landscape.
In many ways, the breakup of the Medical Act symbolizes a broader transformation in society’s understanding of healthcare. It reflects a shift away from rigid, hierarchical models toward more dynamic, collaborative, and patient‑centered approaches. While the dissolution of such a longstanding framework inevitably brought disruption, it also created space for innovation and reform. The legacy of the Medical Act lives on in the structures that replaced it, shaped by the lessons learned from its strengths and its shortcomings.
Ultimately, the breakup was not merely a legal or administrative event; it was a reflection of changing values, expectations, and realities. As healthcare continues to evolve, the story of the Medical Act serves as a reminder that regulatory systems must remain adaptable, transparent, and responsive to the needs of both practitioners and the public.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
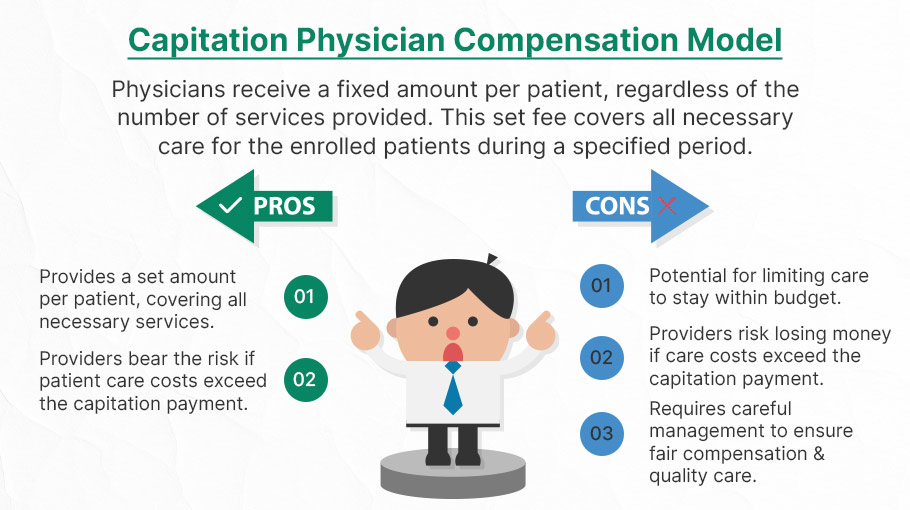
Risk‑based medical payment models have become one of the most significant shifts in modern health‑care financing. They move providers away from the traditional fee‑for‑service structure, where every test, visit, or procedure generates a separate payment, and toward arrangements that reward value, outcomes, and cost‑conscious care. This shift reflects a broader recognition that paying for volume alone can unintentionally encourage overuse, fragmentation, and rising costs. Risk‑based models attempt to realign incentives so that providers are financially accountable for the quality and efficiency of the care they deliver.
At the core of these models is the idea of financial risk transfer. Instead of insurers or government programs bearing the full cost of patient care, providers accept some degree of responsibility for spending that exceeds predetermined benchmarks. The level of risk can vary widely. Upside‑only arrangements allow providers to share in savings if they keep costs below expectations, while downside risk requires them to repay losses if spending surpasses targets. Full‑risk or global‑capitation models go even further, giving providers a fixed per‑patient payment to cover all necessary services. The more risk a provider assumes, the greater the potential reward—but also the greater the potential financial exposure.
***
***
One of the most widely used risk‑based models is the accountable care organization, or ACO. In an ACO, groups of physicians, hospitals, and other clinicians coordinate care for a defined population. They are measured on quality metrics such as preventive care, chronic disease management, and patient experience. If they meet quality standards while keeping total spending below a benchmark, they share in the savings. If they take on two‑sided risk, they may also owe money back when costs exceed expectations. The structure encourages collaboration, data sharing, and proactive management of high‑risk patients, all of which are difficult to achieve in a purely fee‑for‑service environment.
Bundled payments represent another important risk‑based approach. Instead of paying separately for each component of a treatment episode, such as a surgery and its follow‑up care, a bundled payment provides a single, predetermined amount for the entire episode. Providers must work together to deliver care efficiently within that budget. If they can do so while maintaining quality, they keep the difference as savings. If complications or inefficiencies drive costs above the bundle price, they absorb the loss. Bundled payments are particularly effective for procedures with predictable care pathways, such as joint replacements or cardiac interventions, and they encourage standardization and reduction of unnecessary variation.
Capitation, one of the oldest risk‑based models, assigns providers a fixed per‑member, per‑month payment to cover all or most services. This model creates strong incentives for preventive care, early intervention, and careful resource management. When implemented well, capitation can support integrated care delivery and long‑term population health strategies. However, it also requires robust infrastructure, accurate risk adjustment, and safeguards to ensure that cost control does not come at the expense of necessary care. Providers must be able to manage complex patients effectively, and payment rates must reflect the true needs of the population.
Risk adjustment is a critical component across all risk‑based models. Without it, providers who care for sicker or more socially complex patients could be unfairly penalized. Risk adjustment uses demographic and clinical data to estimate expected costs for each patient, ensuring that benchmarks and payments reflect the underlying health status of the population. Accurate risk adjustment protects against adverse selection and supports fairness, but it also requires sophisticated data systems and careful oversight to prevent gaming or upcoding.
Despite their promise, risk‑based payment models face challenges. Providers must invest in care‑management teams, data analytics, and interoperable technology to succeed. Smaller practices may struggle with the administrative and financial demands of taking on risk. Patients may also experience confusion if networks narrow or if care pathways become more structured. Policymakers and payers must balance incentives for efficiency with protections that ensure access and quality.
***
***
Even with these complexities, risk‑based models continue to expand because they offer a path toward a more sustainable and patient‑centered health‑care system. By rewarding outcomes rather than volume, they encourage providers to focus on prevention, coordination, and long‑term health. They also create opportunities for innovation in care delivery, from telehealth to home‑based services to integrated behavioral health. As health‑care costs continue to rise, risk‑based payment models represent a strategic attempt to align financial incentives with the goals of better care, healthier populations, and more efficient use of resources.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The Doctor of Science (ScD) degree occupies a distinctive place within the landscape of advanced academic and professional education. Although less commonly discussed than the PhD, the ScD represents a rigorous pathway for individuals seeking to contribute original, high‑level research to scientific and technical fields. Its history, structure, and contemporary relevance reveal a degree designed to cultivate deep expertise, methodological sophistication, and the capacity to solve complex problems through systematic inquiry.
At its core, the ScD is a research doctorate. Like the PhD, it requires candidates to demonstrate mastery of a discipline, identify a meaningful research question, and produce a dissertation that advances knowledge. The distinction between the two degrees is often more cultural than structural. In many institutions, the ScD is awarded in fields with a strong quantitative or applied scientific orientation, such as engineering, public health, computer science, or biostatistics. This association with technical disciplines has shaped the perception of the ScD as a degree emphasizing analytical rigor and practical impact.
The structure of ScD programs typically mirrors that of PhD programs: coursework, comprehensive examinations, and a multi‑year research project culminating in a dissertation. However, the ScD often places additional emphasis on methodological training and the application of scientific principles to real‑world challenges. Students may engage in interdisciplinary collaborations, work with industry or government partners, or contribute to large‑scale research initiatives. This applied orientation reflects the degree’s historical roots in scientific problem‑solving and its ongoing relevance in fields where research is closely tied to practice.
***
***
One of the defining features of the ScD is its flexibility across institutions. Some universities treat the ScD and PhD as interchangeable, differing only in name. Others reserve the ScD for specific departments or use it to signal a particular research tradition. This variability can create confusion, but it also highlights the degree’s adaptability. Rather than being constrained by a single definition, the ScD evolves to meet the needs of the disciplines it serves. In engineering, for example, the ScD may emphasize design, modeling, and innovation. In public health, it may focus on epidemiological methods, population‑level analysis, and the development of evidence‑based interventions.
Despite these variations, the ScD consistently demands a high level of intellectual independence. Candidates are expected not only to master existing knowledge but also to generate new insights. This process requires creativity, persistence, and the ability to navigate uncertainty. The dissertation, as the capstone of the degree, serves as a demonstration of these qualities. It is both a scholarly contribution and a testament to the candidate’s readiness to join the community of researchers and practitioners who shape scientific progress.
The value of the ScD extends beyond academia. Graduates often pursue careers in government agencies, research institutes, private industry, and nonprofit organizations. Their training equips them to analyze complex systems, design data‑driven solutions, and lead interdisciplinary teams. In an era defined by rapid technological change and global challenges—from climate science to public health—these skills are increasingly essential. The ScD prepares individuals not only to understand scientific problems but to address them with rigor and creativity.
Another important dimension of the ScD is its role in promoting scientific leadership. The degree cultivates the ability to communicate research findings, mentor emerging scholars, and contribute to the development of scientific policy and practice. Graduates may become faculty members, research directors, or technical experts whose work influences both scientific understanding and societal outcomes. The ScD thus serves as a bridge between advanced scholarship and practical impact.
In contemporary discussions about doctoral education, the ScD stands as a reminder that scientific inquiry is both a theoretical and applied endeavor. While the PhD remains the most widely recognized research doctorate, the ScD offers an alternative pathway that aligns closely with the needs of technical and scientific fields. Its emphasis on methodological depth, interdisciplinary collaboration, and real‑world application makes it a compelling option for individuals committed to advancing science in ways that directly benefit society.
Ultimately, the Doctor of Science degree represents a commitment to rigorous research and meaningful contribution. It embodies the belief that scientific knowledge, when pursued with discipline and imagination, has the power to illuminate complex problems and drive innovation. For students drawn to this mission, the ScD offers a challenging and rewarding journey into the heart of scientific discovery.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
A multiple‑choice test is one of the most widely used assessment formats in education, professional certification, and psychological measurement. Its defining feature is simple: each question presents a prompt and a set of possible answers, from which the test‑taker must select the correct or best option. Although the structure appears straightforward, the multiple‑choice test is a sophisticated tool shaped by decades of research on learning, cognition, and measurement. Understanding what a multiple‑choice test is requires looking beyond its surface format and examining its purpose, design, strengths, limitations, and the ways it influences how people learn and demonstrate knowledge.
The Structure and Purpose of Multiple‑Choice Tests
At its core, a multiple‑choice test is designed to measure knowledge, skills, or reasoning in a standardized and efficient way. Each question—often called an “item”—contains two main parts: the stem and the alternatives. The stem presents the problem, scenario, or question. The alternatives include one correct answer, known as the key, and several incorrect answers, known as distractors. The test‑taker’s task is to identify the key among the distractors.
This structure serves a clear purpose: to evaluate whether someone can recognize accurate information or apply knowledge to a specific situation. Because the answer choices are predetermined, scoring can be objective and consistent. This makes multiple‑choice tests particularly useful in large‑scale settings such as school exams, professional licensing tests, and standardized assessments. They allow thousands—or even millions—of people to be evaluated using the same criteria, with results that can be compared fairly across individuals and groups.
Designing Effective Multiple‑Choice Questions
Although the format seems simple, writing high‑quality multiple‑choice questions is a demanding process. A good item must be clear, unambiguous, and aligned with the skill or concept being assessed. The stem should present a meaningful problem rather than a trivial fact, and the distractors must be plausible enough to challenge someone who has not fully mastered the material.
The best multiple‑choice questions do more than test memorization. They can assess higher‑order thinking by asking test‑takers to analyze scenarios, apply principles, evaluate evidence, or solve problems. For example, a question in a biology exam might present a real‑world situation and ask which explanation best fits the observed data. In this way, multiple‑choice tests can measure complex reasoning when they are carefully constructed.
Another important aspect of design is fairness. A well‑designed test avoids cultural bias, overly tricky wording, or clues that unintentionally reveal the answer. The goal is to measure knowledge or skill—not reading speed, test‑taking tricks, or familiarity with a particular cultural reference. Achieving this level of fairness requires careful review, pilot testing, and revision.
***
***
Strengths of Multiple‑Choice Tests
One of the major strengths of multiple‑choice tests is efficiency. They allow instructors and institutions to assess a large amount of content in a relatively short time. Because scoring is objective, results can be processed quickly and consistently, reducing the potential for human error or subjective judgment.
Another advantage is reliability. When items are well‑designed, multiple‑choice tests can produce stable and repeatable results. This reliability is crucial in high‑stakes settings such as medical licensing exams or university admissions, where decisions must be based on trustworthy measures.
Multiple‑choice tests also offer diagnostic value. Patterns of correct and incorrect responses can reveal which concepts students understand and which require further instruction. For teachers, this information can guide lesson planning and targeted support. For learners, it can highlight strengths and weaknesses, helping them focus their study efforts more effectively.
Finally, multiple‑choice tests can assess a wide range of cognitive skills. While they are often associated with factual recall, they can also measure comprehension, application, analysis, and even aspects of critical thinking. The key is thoughtful item design that challenges students to use knowledge rather than simply recognize it.
Limitations and Criticisms
Despite their strengths, multiple‑choice tests are not without limitations. One common criticism is that they encourage guessing. Because the correct answer is always present, a test‑taker might select it by chance rather than through understanding. While this effect can be reduced by including more distractors or using statistical scoring methods, it cannot be eliminated entirely.
Another limitation is that multiple‑choice tests may oversimplify complex skills. Some abilities—such as writing, creativity, collaboration, or open‑ended problem solving—cannot be captured well through fixed response options. For example, evaluating a student’s ability to construct a persuasive argument or design an experiment requires formats that allow for extended responses.
Multiple‑choice tests can also create a narrow focus on test preparation. When students know they will be assessed through this format, they may prioritize memorizing isolated facts rather than developing deeper understanding. This phenomenon, sometimes called “teaching to the test,” can limit the richness of learning experiences.
Additionally, poorly written items can introduce bias or confusion. Ambiguous wording, irrelevant details, or distractors that are obviously incorrect can distort results. In such cases, the test may measure test‑taking ability more than actual knowledge.
The Role of Multiple‑Choice Tests in Learning
Multiple‑choice tests influence not only how knowledge is measured but also how it is learned. When used thoughtfully, they can reinforce learning by encouraging retrieval practice—the act of recalling information from memory. Research shows that retrieval strengthens memory and improves long‑term retention. Taking a multiple‑choice test can therefore help students learn, not just demonstrate what they know.
However, the impact depends on how the tests are integrated into instruction. Frequent low‑stakes quizzes can support learning by providing regular opportunities for practice and feedback. In contrast, high‑stakes exams that determine grades or advancement may create anxiety and narrow students’ focus to short‑term performance.
Multiple‑choice tests can also support metacognition. When students review their results, they gain insight into what they understand and where they need improvement. This self‑awareness is a key component of effective learning.
Why Multiple‑Choice Tests Persist
Despite ongoing debates about their limitations, multiple‑choice tests remain a central part of modern assessment. Their persistence is not simply a matter of convenience. They offer a combination of efficiency, reliability, and scalability that few other formats can match. In large educational systems, they provide a practical way to evaluate learning across diverse populations.
Moreover, advances in test design have expanded what multiple‑choice tests can measure. Computer‑based testing allows for adaptive assessments that adjust difficulty based on performance, providing a more precise measure of ability. Scenario‑based items can simulate real‑world decision‑making, making the test more authentic and meaningful.
Conclusion
A multiple‑choice test is far more than a set of questions with predetermined answers. It is a carefully designed tool for measuring knowledge, reasoning, and understanding. Its structure allows for efficient, objective, and reliable assessment, making it invaluable in educational and professional contexts. At the same time, its limitations remind us that no single format can capture the full range of human abilities.
When used thoughtfully, multiple‑choice tests can support learning, provide meaningful feedback, and help institutions make informed decisions. Understanding what they are—and what they are not—allows educators and learners to use them more effectively. Ultimately, the multiple‑choice test endures because it strikes a balance between practicality and precision, offering a structured way to evaluate what people know in an increasingly complex world.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
A forensic accountant is a financial professional who blends traditional accounting expertise with investigative skills to uncover, analyze, and explain financial irregularities. While many people associate accounting with routine bookkeeping or tax preparation, forensic accounting operates in a very different arena—one where money trails intersect with legal disputes, fraud schemes, and complex financial conflicts. The role requires not only technical knowledge of accounting principles but also the curiosity of an investigator and the clarity of a communicator who can translate intricate financial data into understandable conclusions.
At its core, forensic accounting involves the examination of financial information for use in legal settings. The word “forensic” itself means “suitable for use in court,” which captures the essence of the profession. Forensic accountants are often called upon when financial information must be scrutinized with a level of detail and rigor that can withstand legal scrutiny. Their work may support civil litigation, criminal investigations, insurance claims, business valuations, or internal corporate inquiries. Because of this, they frequently collaborate with attorneys, law enforcement agencies, regulatory bodies, and corporate leadership.
One of the most recognized responsibilities of a forensic accountant is the detection and investigation of fraud. Fraud can take many forms—embezzlement, financial statement manipulation, asset misappropriation, or complex schemes involving shell companies and hidden transactions. Forensic accountants use a combination of analytical procedures, data mining techniques, and professional skepticism to identify patterns that suggest wrongdoing. They may trace the flow of funds through multiple accounts, reconstruct destroyed or incomplete records, or analyze inconsistencies in financial statements. Their goal is not only to uncover what happened but also to determine how it happened and who was responsible.
Beyond fraud detection, forensic accountants play a crucial role in litigation support. In legal disputes involving financial matters, attorneys rely on forensic accountants to provide objective, evidence‑based analysis. This may include calculating economic damages, evaluating the value of a business, assessing lost profits, or determining the financial impact of a breach of contract. In divorce proceedings, forensic accountants may help identify hidden assets or evaluate the true income of a spouse. Their findings often become part of expert reports submitted to the court, and they may be called to testify as expert witnesses. In this capacity, they must present complex financial information in a clear, concise manner that judges and juries can understand.
Another important aspect of forensic accounting is prevention. Organizations increasingly recognize the value of proactive measures to reduce the risk of fraud and financial misconduct. Forensic accountants may design internal controls, conduct risk assessments, or evaluate corporate governance practices to help organizations strengthen their defenses. By identifying vulnerabilities before they are exploited, they contribute to a healthier financial environment and help protect stakeholders from potential losses.
The skill set required for forensic accounting is broad and demanding. Technical proficiency in accounting and auditing is essential, but equally important are analytical thinking, attention to detail, and strong communication skills. Forensic accountants must be able to interpret large volumes of financial data, identify anomalies, and draw logical conclusions. They must also be comfortable working with digital tools, as modern investigations often involve electronic records, data analytics, and specialized software. Integrity and objectivity are critical, given the legal implications of their work and the trust placed in their findings.
The profession also requires adaptability. Every case is different, and forensic accountants must be prepared to navigate unfamiliar industries, evolving fraud techniques, and changing regulatory environments. They may work in public accounting firms, government agencies, law enforcement units, insurance companies, or as independent consultants. Regardless of the setting, the common thread is their role as financial detectives who bring clarity to situations where the truth is obscured by complexity or deception.
In summary, a forensic accountant is far more than a traditional number‑cruncher. They are investigators, analysts, communicators, and trusted advisors who operate at the intersection of finance and law. Their work uncovers hidden truths, supports the pursuit of justice, and helps organizations safeguard their financial integrity. As financial systems grow more complex and fraud schemes become more sophisticated, the role of the forensic accountant continues to expand in importance. Their unique blend of skills makes them indispensable in a world where transparency and accountability are more critical than ever.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The Net Investment Income Tax (NIIT) occupies a distinctive place in the modern U.S. tax landscape. Introduced as part of the Affordable Care Act, it was designed to generate revenue from higher‑income households by taxing certain forms of unearned income. Although it affects a relatively small portion of taxpayers, its implications reach into investment strategy, tax planning, and broader debates about fairness and economic policy. Understanding how the NIIT works—and why it exists—offers insight into the evolving relationship between tax policy and wealth in the United States.
At its core, the NIIT is a 3.8 percent surtax applied to specific types of investment income for individuals whose modified adjusted gross income exceeds statutory thresholds. These thresholds—$200,000 for single filers and $250,000 for married couples filing jointly—are not indexed for inflation. As a result, over time, more taxpayers may find themselves subject to the tax even if their real purchasing power has not increased. This “bracket creep” is one of the subtle but important features of the NIIT, shaping its long‑term reach.
The tax applies only to “net investment income,” a term that includes interest, dividends, capital gains, rental income, royalties, and passive business income. It does not apply to wages, self‑employment earnings, or distributions from qualified retirement plans. The logic behind this distinction is straightforward: the NIIT targets income derived from wealth rather than labor. In practice, this means that two taxpayers with identical total income may face different NIIT liabilities depending on how much of their income comes from investments versus work.
The mechanics of the NIIT involve a comparison between two amounts: net investment income and the excess of modified adjusted gross income over the applicable threshold. The tax is applied to whichever of these two figures is smaller. This structure ensures that the NIIT functions as a surtax on high‑income households without taxing investment income for those below the threshold. It also means that taxpayers with large investment portfolios but modest overall income may avoid the tax entirely, while those with high wages and relatively small investment income may still owe it.
One of the most significant effects of the NIIT is its influence on investment behavior. Because the tax applies to capital gains, it can affect decisions about when to sell appreciated assets. Taxpayers may choose to time sales to avoid pushing their income above the threshold in a given year. Others may shift toward tax‑exempt investments, such as municipal bonds, or toward assets that generate unrealized rather than realized gains. The NIIT therefore becomes not just a revenue tool but a factor shaping the broader investment landscape.
The tax also interacts with other parts of the tax code in ways that can be complex. For example, rental real estate income is generally subject to the NIIT unless the taxpayer qualifies as a real estate professional and materially participates in the activity. Trusts and estates face their own NIIT rules, often reaching the surtax threshold at much lower income levels than individuals. These layers of complexity mean that the NIIT is often a central topic in tax planning for high‑income households, especially those with diverse investment portfolios.
Beyond its technical features, the NIIT reflects broader policy debates about equity and the distribution of tax burdens. Supporters argue that it helps ensure that high‑income individuals contribute a fair share to the cost of public programs, particularly those related to health care. Because investment income is disproportionately concentrated among wealthier households, the NIIT is seen as a way to align tax policy with ability to pay. Critics, however, contend that the tax discourages investment, adds unnecessary complexity, and imposes an additional layer of taxation on income that may already be subject to corporate taxes or other levies.
Despite these debates, the NIIT has become a stable part of the federal tax system. It raises billions of dollars annually and plays a role in funding health‑related initiatives. As discussions about tax reform continue, the NIIT often resurfaces as policymakers consider how best to balance revenue needs with economic incentives. Whether it remains unchanged, is expanded, or is modified in future legislation, the NIIT will continue to shape the financial decisions of high‑income taxpayers and contribute to the ongoing conversation about how the United States taxes wealth.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The history of U.S. recessions reflects the nation’s evolving economy, shaped by wars, financial crises, policy shifts, and global events. Since 1857, the U.S. has experienced over 30 recessions, each offering lessons in resilience and reform.
The United States has endured a long and varied history of economic recessions, defined as periods of significant decline in economic activity lasting more than a few months. These downturns are typically marked by falling GDP, rising unemployment, and reduced consumer spending. Since the mid-19th century, recessions have been triggered by a range of factors—from banking panics and inflation to global conflicts and pandemics.
The earliest recorded U.S. recession began in 1857, sparked by a banking crisis and declining international trade. This was followed by the Long Depression of 1873–1879, which lasted a staggering 65 months, making it the longest in U.S. history. The downturn was triggered by the collapse of a major bank and a speculative bubble in railroad investments.
The Great Depression remains the most severe economic crisis in American history. Beginning in 1929 after the stock market crash, it lasted until 1933 and saw unemployment soar to 25%. The Depression reshaped U.S. economic policy, leading to the creation of Social Security, the FDIC, and other New Deal programs aimed at stabilizing the economy and protecting citizens.
Post-World War II recessions were generally shorter and less severe. The 1945 recession, for example, lasted eight months and was caused by the transition from wartime to peacetime production. The 1973–75 recession, however, was more prolonged, driven by an oil embargo and stagflation—a combination of stagnant growth and high inflation.
The early 1980s recession was triggered by the Federal Reserve’s aggressive interest rate hikes to combat inflation. Though painful, it ultimately helped stabilize prices and set the stage for a long period of growth. The early 1990s recession followed a savings and loan crisis and a slowdown in defense spending after the Cold War.
The Great Recession of 2007–2009 was the most significant downturn since the Great Depression. It was caused by the collapse of the housing bubble and widespread failures in financial institutions. Unemployment peaked at 10%, and the crisis led to sweeping reforms in banking and mortgage lending practices.
Most recently, the COVID-19 recession in 2020 was the shortest in U.S. history, lasting just two months. Despite its brevity, it was severe, with unemployment briefly reaching 14.7% due to lockdowns and global supply chain disruptions.
Throughout its history, the U.S. has shown remarkable resilience in recovering from recessions. Each downturn has prompted changes in fiscal and monetary policy, regulatory reform, and shifts in public perception about the role of government and markets. As the economy becomes more interconnected globally, future recessions may be shaped by international events as much as domestic ones.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Did you know that desperate doctors of all ages are turning to knowledgeable financial advisors and medical management consultants for help? Symbiotically too, generalist advisors are finding that the mutual need for knowledge and extreme niche synergy is obvious.
***
***
But, there was no established curriculum or educational program; no corpus of knowledge or codifying terms-of-art; no academic gravitas or fiduciary accountability; and certainly no identifying professional designation that demonstrated integrated subject matter expertise for the increasingly unique healthcare focused financial advisory niche … Until Now!
So, if you are looking to supplement your knowledge, income and designations; and find other qualified professionals you may want to consider the CMP® program.
Enter the Certified Medical Planner™ charter professional designation. And, CMPs™ are FIDUCIARIES, 24/7.
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
***
***
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
The economics of information explores how knowledge—or the lack of it—affects decision-making, market behavior, and resource allocation. It reveals why perfect competition rarely exists and why information itself can be a powerful economic asset.
Economics of Information: Understanding the Value and Impact of Knowledge
In traditional economic models, markets are often assumed to operate under perfect information—where all participants have equal access to relevant data. However, in reality, information is often incomplete, asymmetric, or costly to obtain. The field known as economics of information emerged to address these discrepancies, fundamentally reshaping how economists understand markets, incentives, and efficiency.
One of the core concepts in this field is information asymmetry, where one party in a transaction possesses more or better information than the other. This imbalance can lead to adverse selection and moral hazard. For example, in the insurance market, individuals who know they are high-risk are more likely to seek coverage, while insurers may struggle to differentiate between high- and low-risk clients. Similarly, in lending, borrowers may have private knowledge about their ability to repay, which lenders cannot easily verify.
To mitigate these problems, economists have developed mechanisms such as signaling and screening. Signaling occurs when the informed party takes action to reveal their type—like a job applicant earning a degree to signal competence. Screening, on the other hand, involves the uninformed party designing tests or contracts to elicit information—such as offering different insurance packages to separate risk levels.
Another important area is the cost of acquiring information. Gathering data, analyzing trends, or verifying facts requires time and resources. This leads to decisions being made under uncertainty, where individuals rely on heuristics or limited data. The economics of information examines how these costs influence behavior, pricing, and market structure. For instance, consumers may not compare every available product due to search costs, allowing firms to maintain price dispersion.
The rise of digital technology has intensified the relevance of this field. In the age of big data, companies like Google and Amazon thrive by collecting and analyzing vast amounts of user information. This data allows them to personalize services, predict behavior, and gain competitive advantages. However, it also raises concerns about privacy, market power, and inequality—issues that economists of information are increasingly addressing.
Moreover, information goods—such as software, media, and research—have unique economic properties. They are often non-rivalrous and can be reproduced at near-zero marginal cost. This challenges traditional pricing models and calls for innovative approaches like freemium strategies, bundling, and subscription services.
In public policy, the economics of information plays a crucial role in designing regulations, transparency standards, and consumer protections. Governments must balance the need for open access to information with incentives for innovation and investment. For example, patent laws aim to encourage research by granting temporary monopolies, while disclosure requirements in finance promote market integrity.
In conclusion, the economics of information reveals that knowledge is not just a passive input but a dynamic force shaping economic outcomes. By understanding how information is produced, distributed, and used, economists can better explain real-world phenomena and design systems that promote fairness, efficiency, and innovation.
In the world of financial advising, few principles are as foundational—and as misunderstood—as diversification. Clients often come to advisors hoping for bold moves and big wins. Yet the most prudent strategy we offer is not a thrilling stock pick or a market-timing miracle, but a quiet, calculated spread of risk. Diversification, in essence, is the art of saying “sorry” in advance—for not chasing every hot trend, for not going all-in, and for not promising perfection. But it’s also the strategy that earns trust, builds resilience, and delivers long-term value.
Diversification means allocating assets across different sectors, geographies, and investment vehicles to reduce exposure to any single point of failure. For financial advisors, it’s not just a portfolio tactic—it’s a philosophy of humility. It acknowledges that markets are unpredictable, that no one can consistently forecast winners, and that protecting capital is just as important as growing it.
Clients may initially resist this approach. They might question why their portfolio includes lagging sectors or why we’re not doubling down on tech or crypto. This is where our role as educators becomes critical. We explain that diversification isn’t about avoiding risk—it’s about managing it. It’s the reason why, when tech stumbles, healthcare or consumer staples might hold steady. It’s why international exposure can buffer domestic volatility. And it’s why fixed income still matters, even in a rising-rate environment.
The challenge for advisors is that diversification rarely feels heroic. It doesn’t make headlines. It doesn’t deliver overnight gains. Instead, it delivers consistency. It smooths out the ride. It allows clients to sleep at night. And over time, it compounds into something powerful: confidence.
***
***
One of the most effective ways to communicate this is through behavioral coaching. We remind clients that diversification is designed to protect them from their own impulses—from chasing trends, reacting to headlines, or panicking during downturns. It’s a guardrail against emotional investing. And when markets inevitably wobble, diversified portfolios give us the credibility to say, “This is why we planned ahead.”
Moreover, diversification is a relationship tool. It shows clients that we’re not betting their future on a single idea. We’re building something durable. We’re thinking about their retirement, their children’s education, their legacy. And we’re doing it with a strategy that’s built to last.
In short, diversification may feel like an apology to the thrill-seeker in every investor. But it’s also a promise: that we’re here to protect, to guide, and to deliver results that matter—not just today, but for decades to come.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Pet insurance offers financial protection and peace of mind for pet owners, helping cover unexpected veterinary costs and ensuring pets receive timely care. It’s a growing industry that reflects the deepening bond between humans and their animal companions.
Pet insurance is a specialized health coverage designed to offset the cost of veterinary care for pets. As veterinary medicine advances, treatments for pets have become more sophisticated—and expensive. From emergency surgeries to chronic illness management, the financial burden can be overwhelming for pet owners. Pet insurance helps mitigate these costs, allowing owners to prioritize their pet’s health without worrying about the price tag.
One of the primary benefits of pet insurance is financial security. Veterinary bills can range from hundreds to thousands of dollars depending on the condition. For example, treating a torn ACL in a dog can cost upwards of $3,000, while cancer treatments may exceed $10,000. With pet insurance, a significant portion of these expenses can be reimbursed, reducing out-of-pocket costs and making advanced care more accessible.
Another advantage is flexibility in care. Pet insurance empowers owners to choose treatments based on medical need rather than financial constraints. Whether it’s a late-night emergency or a long-term condition like diabetes or arthritis, insurance gives pet parents the freedom to pursue the best care options available.
Policies typically cover accidents, illnesses, surgeries, medications, and sometimes routine care like vaccinations and dental cleanings. However, coverage varies widely by provider and plan. Most policies exclude pre-existing conditions and have waiting periods before coverage begins. It’s crucial for pet owners to read the fine print and understand what’s included and what’s not. The cost of pet insurance depends on factors such as the pet’s species, breed, age, and location. Monthly premiums can range from $20 to $70 for dogs and $10 to $40 for cats. While this may seem like an added expense, it can be a worthwhile investment in the long run—especially for breeds prone to genetic conditions or pets with active lifestyles.
Pet insurance also reflects a broader cultural shift in how society views pets. No longer just animals, pets are considered family members. This emotional bond drives owners to seek the best possible care, and insurance helps make that care attainable. It’s not just about saving money—it’s about ensuring quality of life for beloved companions.
Critics argue that pet insurance isn’t always cost-effective, especially if a pet remains healthy. So, pet insurance may not be worth it if:
Your pet is a senior or has health problems.
A big vet bill wouldn’t be a financial hardship for you.
You’d rather take the risk of an expensive diagnosis than pay for insurance you might never use.
However, the unpredictability of accidents and illness makes it a valuable safety net. Like any insurance, it’s about preparing for the unexpected.
In conclusion, pet insurance is a practical and compassionate tool for modern pet ownership. It offers financial relief, expands treatment options, and supports the emotional commitment people have to their pets.
As veterinary costs continue to rise, pet insurance provides a way to protect both your wallet and your furry friend’s well-being.; maybe!
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
In the competitive world of financial services, attracting and retaining clients is a constant challenge. To stand out, many financial advisors employ strategic marketing tactics known as “loss leaders”—free or discounted services designed to showcase value and build trust. These offerings serve as entry points for potential clients, allowing advisors to demonstrate expertise and initiate long-term relationships.
One of the most common loss leaders is the free initial consultation. This no-obligation meeting gives prospective clients a chance to discuss their financial goals, ask questions, and get a feel for the advisor’s approach. For the advisor, it’s an opportunity to assess the client’s needs and present tailored solutions. While no revenue is generated from this meeting, it often leads to paid engagements once the client feels confident in the advisor’s capabilities.
Another popular tactic is offering a complimentary financial plan or portfolio review. These services provide tangible insights into a client’s current financial situation and suggest improvements. By delivering real value upfront, advisors build credibility and demonstrate their analytical skills. Clients who receive actionable advice are more likely to continue working with the advisor on a paid basis.
Educational content also plays a key role in loss leader strategy. Advisors frequently host free webinars, workshops, or seminars on topics like retirement planning, tax strategies, or investment basics. These events not only educate attendees but also position the advisor as a thought leader. Attendees often leave with a better understanding of their financial needs and a desire to seek personalized guidance.
In the digital realm, advisors may offer free tools and assessments on their websites. These include retirement readiness calculators, risk tolerance quizzes, and budgeting templates. Such tools engage users and provide personalized feedback, creating a natural segue into one-on-one consultations. Additionally, offering free newsletters or eBooks helps advisors stay top-of-mind while delivering ongoing value.
Some advisors go further by waiving fees for introductory services, such as account setup or the first few months of investment management. This lowers the barrier to entry and encourages hesitant clients to try the service. Once clients experience the benefits, they’re more likely to commit long-term.
Loss leaders are not limited to high-net-worth individuals. Advisors targeting younger or less affluent clients may offer free debt management plans or budgeting assistance. These services address immediate concerns and build loyalty among clients who may become more profitable as their financial situations improve.
Ultimately, loss leaders are about building relationships. By offering something of value without immediate compensation, financial advisors demonstrate their commitment to helping clients succeed. This fosters trust, encourages engagement, and often leads to lasting partnerships. In a field where reputation and reliability are paramount, loss leaders serve as powerful tools for growth and differentiation.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Classic Definition: Scientific research depends on the referencing and citing of other research.
Modern Circumstance: The Google Scholar Paradox is that research which gets cited most often is whatever shows up in the top results of Google Scholar searches; regardless of its contribution to the field.
Paradox Example: The Google Scholar effect is a phenomenon when some medical and healthcare researchers pick and cite works appearing in the top results on Google Scholar regardless of their contribution to the citing publication.
Paradoxically they automatically assume these works’ credibility and believe that editors, reviewers, and readers expect to see these citations.
Insurance agents are primarily paid through commissions, but may also earn salaries, bonuses, and fees depending on their employment model and the types of policies they sell.
Insurance agents play a vital role in helping individuals and businesses navigate the complex world of insurance. Their compensation structures vary widely, influenced by factors such as the type of insurance they sell, whether they work independently or for a company, and the specific agreements they have with insurers. Understanding how insurance agents are paid is essential for consumers who want to make informed decisions and for aspiring agents considering a career in the industry.
The most common form of compensation for insurance agents is commission-based pay. Agents earn a percentage of the premium paid by the customer when they successfully sell a policy. These commissions can vary depending on the type of insurance. For example, first-year commissions for auto and homeowners insurance typically range from 5% to 20%, while commercial property and casualty policies may offer 10% to 15%. Life insurance policies often provide higher initial commissions, sometimes exceeding 50% of the first-year premium, followed by smaller renewal commissions in subsequent years.
There are two main types of insurance agents: captive agents and independent agents. Captive agents work exclusively for one insurance company and usually receive a combination of salary and commissions. Their compensation may also include performance bonuses and incentives tied to sales targets. Independent agents, on the other hand, represent multiple insurers and rely more heavily on commissions. They have the flexibility to offer a wider range of products, but their income is directly tied to their ability to sell policies and maintain client relationships.
***
***
In addition to commissions, some agents earn fees for services such as policy reviews, risk assessments, or consulting. These fees are more common in commercial insurance or financial planning contexts, where agents provide specialized expertise. However, fee-based compensation is less prevalent in personal lines of insurance like auto or home coverage.
Bonuses and incentives are another component of agent compensation. Insurance companies often reward agents for meeting sales quotas, retaining clients, or selling specific types of policies. These bonuses can significantly boost an agent’s income, but they may also create potential conflicts of interest if agents prioritize higher-paying products over client needs.
Some agents, particularly those employed by large firms or call centers, receive a fixed salary. This model provides stability but may limit earning potential compared to commission-based roles. Salaried agents may still receive performance bonuses or profit-sharing depending on company policy.
Ultimately, an insurance agent’s earnings depend on their business model, experience, and ability to build a loyal client base. While commissions remain the cornerstone of insurance compensation, the rise of fee-based services and hybrid models reflects a shift toward more transparent and client-focused practices.
Consumers should feel empowered to ask agents about their compensation structure to ensure they receive unbiased advice tailored to their needs.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
A paradox is a figure of speech that can seem silly or contradictory in form, yet it can still be true, or at least make sense in the context given. This is sometimes used to illustrate thoughts or statements that differ from traditional ideas. So, instead of taking a given statement literally, an individual must comprehend it from a different perspective. Using paradoxes in speeches and writings can also add wit and humor to one’s work, which serves as the perfect device to grab a reader or a listener’s attention.
But paradoxes can be quite difficult to explain by definition alone, which is why it is best to refer to a few examples to further your understanding.
A good paradox example is in the famous television show House. Here, Dr. House is a rude, selfish, and narcissistic character who alienates everyone around him, even his own colleagues. However, he is also a brilliant doctor who is committed to saving lives. Regardless of his mean exterior, Dr. House is a moral and compassionate man who cares about his patients. The paradox here is how the character strives to save people’s lives despite his ruthless personality and behavior.
Modern health care appears to be rich in contradictions, and it is claimed to be paradoxical in a number of ways. In particular health care is held to be a paradox itself: it is supposed to do good; but is also accused of doing harm.
The expression “first do no harm,” which is a Latin phrase, is not part of the original or modern versions of the Hippocratic Oath, which was originally written in Greek (“primum non nocere,” the Latin translation from the original Greek.)
The Hippocratic Oath, written in the 5th century BCE, does contain language suggesting that the physician and his assistants should not cause physical or moral harm to a patient.
The first known published version of “do no harm” dates to medical texts from the mid-19th century, and is attributed to the 17th century English physician Thomas Sydenham.
Difference between Paradox and Oxymoron
Most people tend to confuse a paradox with an oxymoron, and it’s not hard to see why. Most oxymoron examples appear to be compressed version of a paradox, in which it is used to add a dramatic effect and to emphasize contrasting thoughts. Although they may seem greatly similar in form, there are slight differences that set them apart.
A paradox consists of a statement with opposing definitions, while an oxymoron combines two contradictory terms to form a new meaning. But because an oxymoron can play out with just two words, it is often used to describe a given object or idea imaginatively. As for a paradox, the statement itself makes you question whether something is true or false. It appears to contradict the truth, but if given a closer look, the truth is there but is merely implied.
The Paradox in Medicine and Health Care
Dr. Bernard Brom [Editor: SA Journal of Natural Medicine] suggests modem medicine is riddled with paradoxes. Most doctors live with these paradoxes without being aware of the conflict of interest that these paradoxes represent. Intrinsic to a general understanding of science is the idea that science frees us from misunderstanding and guides us towards clear decision making.
Most veteran doctors with experience know that medical science still does not give definitive answers, that each individual is unique, that one can never be sure how a patient will respond to a particular drug, or what the outcome of a particular operation will be. Human beings are not machines and therefore do not respond according to Newtonian logic, and therefore a paradox in medicine is not surprising. Medicine is an art which uses scientific techniques and approaches. It is, however, important to face these paradoxes. It is both humbling and enlightening, enriching those who consider the implications deeply enough.
The Compensation versus Value Paradox
Regardless of specialty, degree designation or delivery model, private practice physician salary is traditionally inversely related to independent medical practice business value.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Valuing a medical practice involves assessing its financial performance, assets, and intangible factors like goodwill and patient loyalty to determine its fair market worth.
Determining the value of a medical practice is a nuanced process that blends financial analysis with strategic insight. Whether you’re preparing to sell, merge, or bring in a partner, understanding how to value your practice ensures informed decision-making and fair negotiations.
There are several recognized methods for valuing a medical practice, each suited to different scenarios. The most common include the income approach, market approach, asset-based approach, and the rule-of-thumb method.
The income approach focuses on the practice’s ability to generate future earnings. This method involves analyzing historical financial statements, projecting future cash flows, and discounting them to present value using a risk-adjusted rate. It’s particularly useful when the practice has stable revenue and predictable expenses. Key metrics include net income, physician productivity, and reimbursement rates.
The market approach compares the practice to similar ones that have recently sold. It relies on data from comparable transactions, adjusted for differences in size, specialty, location, and profitability. This method is ideal when reliable market data is available, though such data can be scarce for niche specialties or rural practices.
The asset-based approach calculates the value of tangible and intangible assets. Tangible assets include medical equipment, office furniture, and real estate. Intangible assets—like patient records, brand reputation, and goodwill—are harder to quantify but can significantly impact value. Goodwill, for instance, reflects the practice’s reputation, patient loyalty, and referral networks.
The rule-of-thumb method uses industry benchmarks, such as a multiple of annual revenue or earnings. For example, a general practice might be valued at 60–80% of annual gross revenue. While quick and easy, this method oversimplifies and may not reflect the unique strengths or weaknesses of a specific practice.https:/https://medicalexecutivepost.com/2025/03/17/medial-practice-valuation-adjustments//medicalexecutivepost.com/2025/03/17/medial-practice-valuation-adjustments/
Beyond these methods, several qualitative factors influence valuation. These include the size and diversity of the patient base, the practice’s specialty, use of technology (like EHR systems or telemedicine), and whether key physicians will remain post-sale. A practice heavily reliant on one provider may be less valuable than one with a strong team and succession plan.
Timing also matters. Economic conditions, regulatory changes, and shifts in healthcare reimbursement can affect practice value. Tax implications and deal structure—such as asset sale vs. stock sale—should also be considered during negotiations.
Ultimately, valuing a medical practice is both art and science. Engaging a professional appraiser or valuation expert can help ensure accuracy and objectivity. They bring experience, access to market data, and the ability to tailor valuation methods to your specific situation.
In summary, a comprehensive valuation considers financial performance, assets, market trends, and intangible factors. By understanding these elements, practice owners can make strategic decisions that reflect the true worth of their medical enterprise.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Population health and public health are two interrelated disciplines that strive to enhance the health outcomes of communities. While they share a common mission—to reduce health disparities and promote wellness—their approaches, target populations, and operational frameworks differ significantly.
***
***
Public health is traditionally defined as the science and art of preventing disease, prolonging life, and promoting health through organized efforts and informed choices of society, organizations, public and private sectors, communities, and individuals. It focuses on the health of the general population and emphasizes broad interventions such as vaccination programs, sanitation, health education, and policy advocacy. Public health professionals often work in government agencies, nonprofit organizations, and academic institutions to implement community-wide initiatives that prevent disease and promote healthy behaviors.
***
***
In contrast, population health takes a more targeted approach. It refers to the health outcomes of a specific group of individuals, including the distribution of such outcomes within the group. This field is particularly concerned with the social determinants of health—factors like income, education, environment, and access to care—that influence health disparities. Population health strategies often involve data-driven interventions tailored to the needs of defined groups, such as rural communities, ethnic minorities, or patients with chronic conditions.
One key distinction lies in scope and granularity. Public health initiatives are typically designed for the entire population, aiming to create systemic change. For example, anti-smoking campaigns or water fluoridation programs benefit everyone regardless of individual risk. Population health, however, might focus on reducing diabetes rates among Hispanic adults in a specific urban area, using targeted outreach and culturally sensitive care models.
Another difference is in data utilization. Population health relies heavily on health informatics and analytics to identify trends, allocate resources, and evaluate outcomes. This evidence-based approach supports precision in addressing health inequities. Public health also uses data, but often at a broader level to guide policy and monitor general health indicators like life expectancy or disease prevalence.
Despite these differences, the two fields are complementary. Public health lays the foundation for healthy societies through preventive infrastructure, while population health builds on this by addressing nuanced needs within subgroups. Together, they form a holistic framework for improving health outcomes across diverse communities.
In today’s healthcare landscape, the integration of public and population health is increasingly vital. The COVID-19 pandemic underscored the importance of both approaches: public health measures like mask mandates and vaccination campaigns were essential, while population health efforts ensured vulnerable groups received targeted support.
In conclusion, while public health and population health differ in focus and methodology, they are united by a shared goal: to foster healthier communities. Understanding their distinctions enables more effective collaboration and innovation in health policy, care delivery, and community engagement.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Investing may seem complicated, but today there are many ways for the newly minted physician [MD, DO, DPM, DMD or DDS] to begin, even with minimal knowledge and only a small amount to invest. Starting as soon as possible will help you get closer to the retirement you deserve.
***
Why is investing important?
Investing often feels like a luxury reserved for the already wealthy physician. Many of us find it difficult to think about investing for the future when there are so many things we need that money for right now; medical school loans, auto, home and children; etc. But, at some point, we’re going to want to stop working and enjoy retirement. And simply put, retirement is expensive.
Most calculations advise that you aim for enough savings to give you 70% to 80% of your pre-retirement income for 20 years or more. Depending on your goals for retirement, that means you could need between $500,000 and $1 million in savings by the time you retire. That may not sound attainable, but with the power of compounding growth, it’s not as hard to achieve as you think. The key is starting as soon as possible and making smart choices.
The short answer is “now,” no matter what your age. Due to the way the gains in investments can compound, the earlier you start the better. Money invested in your 20s could very easily grow over 20 times before you retire, without you having to do much.That is powerful. Even if you’re in your 50s or older, you can still make significant progress toward meeting your goals in retirement.
How much should you invest per month?
Most financial experts say you should invest 10% to 15% of your annual income for retirement. That’s the goal, but you don’t have to get there immediately. Whatever you can start investing today is going to help you down the road.
So, if 10% to 15% is too much right now, start small and build toward that goal over time. You can actually start investing with $5 if you want. And you should. Some investment products require a minimum investment, but there are plenty that don’t, and a lot of online brokerage accounts can be started for free.
The best investments for you are going to depend on your age, goals, and strategy. The important thing is to get started. You’ll learn as you go. If you have questions, a dedicated DIYer or investment advisor can help give you the guidance and options you need.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Do you ever wish you could acquire specific information for your career activities without having to complete a university Master’s Degree or finish our entire Certified Medical Planner™ professional designation program? Well, Micro-Certifications from the Institute of Medical Business Advisors, Inc., might be the answer. Read on to learn how our three Micro-Certifications offer new opportunities for professional growth in the medical practice, business management, health economics and financial planning, investing and advisory space for physicians, nurses and healthcare professionals.
Micro-Certification Basics
Stock-Brokers, Financial Advisors, Investment Advisors, Accountants, Consultants, Financial Analyists and Financial Planners need to enhance their knowledge skills to better serve the changing and challenging healthcare professional ecosystem. But, it can be difficult to learn and demonstrate mastery of these new skills to employers, clients, physicians or medical prospects. This makes professional advancement difficult. That’s where Micro-Certification and Micro-Credentialing enters the online educational space. It is the process of earning a Micro-Certification, which is like a mini-degree or mini-credential, in a very specific topical area.
Micro-Certification Requirements
Once you’ve completed all of the requirements for our Micro-Certification, you will be awarded proof that you’ve earned it. This might take the form of a paper or digital certificate, which may be a hard document or electronic image, transcript, file, or other official evidence that you’ve completed the necessary work.
Uses of Micro-Certifications
Micro-Certifications may be used to demonstrate to physicians prospective medical clients that you’ve mastered a certain knowledge set. Because of this, Micro-Certifications are useful for those financial service professionals seeking medical clients, employment or career advancement opportunities.
Examples of iMBA, Inc., Micro-Certifications
Here are the three most popular Micro-Certification course from the Institute of Medical Business Advisors, Inc:
1. Health Insurance and Managed Care: To keep up with the ever-changing field of health care physician advice, you must learn new medical practice business models in order to attract and assist physicians and nurse clients. By bringing together the most up-to-date business and medical prctice models [Medicare, Medicaid, PP-ACA, POSs, EPOs, HMOs, PPOs, IPA’s, PPMCs, Accountable Care Organizations, Concierge Medicine, Value Based Care, Physician Pay-for-Performance Initiatives, Hospitalists, Retail and Whole-Sale Medicine, Health Savings Accounts and Medical Unions, etc], this iMBA Inc., Mini-Certification offers a wealth of essential information that will help you understand the ever-changing practices in the next generation of health insurance and managed medical care.
2. Health Economics and Finance: Medical economics, finance, managerial and cost accounting is an integral component of the health care industrial complex. It is broad-based and covers many other industries: insurance, mathematics and statistics, public and population health, provider recruitment and retention, health policy, forecasting, aging and long-term care, and Venture Capital are all commingled arenas. It is essential knowledge that all financial services professionals seeking to serve in the healthcare advisory niche space should possess.
3. Health Information Technology and Security: There is a myth that all physician focused financial advisors understand Health Information Technology [HIT]. In truth, it is often economically misused or financially misunderstood. Moreover, an emerging national HIT architecture often puts the financial advisor or financial planner in a position of maximum uncertainty and minimum productivity regarding issues like: Electronic Medical Records [EMRs] or Electronic Health Records [EHRs], mobile health, tele-health or tele-medicine, Artificial Intelligence [AI], benefits managers and human resource professionals.
Other Topics include: economics, finance, investing, marketing, advertising, sales, start-ups, business plan creation, financial planning and entrepreneurship, etc.
How to Start Learning and Earning Recognition for Your Knowledge
Now that you’re familiar with Micro-Credentialing, you might consider earning a Micro-Certification with us. We offer 3 official Micro-Certificates by completing a one month online course, with a live instructor consisting of twelve asynchronous lessons/online classes [3/wk X 4/weeks = 12 classes]. The earned official completion certificate can be used to demonstrate mastery of a specific skill set and shared with current or future employers, current clients or medical niche financial advisory prospects.
Mini-Certification Tuition, Books and Related Fees
The tuition for each Mini-Certification live online course is $1,250 with the purchase of one required dictionary handbook. Other additional guides, white-papers, videos, files and e-content are all supplied without charge. Alternative courses may be developed in the future subject to demand and may change without notice.
***
Contact: For more information, or to speak with an academic representative, please contact Ann Miller RN MHA CMP™ at Email: MarcinkoAdvisors@msn.com [24/7].
Posted on October 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters and A.I.
***
***
Dentistry is often perceived as a stable and rewarding profession, yet beneath the surface lies a troubling reality: dentists face disproportionately high levels of stress, burnout, divorce, practice turmoil, and even suicide. These issues stem from a complex interplay of emotional, financial, and professional pressures that uniquely affect dental practitioners.
Emotional and Psychological Strain
Dentists frequently operate in high-stakes environments where precision is paramount. The pressure to deliver flawless results while managing patient anxiety and discomfort can be overwhelming. Many patients fear dental procedures, and this fear often manifests as hostility or distrust, placing emotional strain on the dentist. Over time, the cumulative effect of these interactions can lead to compassion fatigue and emotional exhaustion.
Unlike other medical professionals who often work in collaborative hospital settings, dentists typically operate in solo or small group practices. This isolation can limit opportunities for peer support and professional camaraderie. Without a strong support network, dentists may struggle to process the emotional toll of their work, increasing their vulnerability to depression and burnout.
Financial and Business Pressures
Running a dental practice involves more than clinical expertise—it requires business acumen. Dentists must manage overhead costs, staff salaries, insurance reimbursements, and patient billing. The financial burden of student loans, often exceeding six figures, adds to the stress. Economic downturns or shifts in healthcare policy can destabilize practices, leading to turmoil and uncertainty.
***
***
Work-Life Imbalance and Marital Strain
The demanding nature of dentistry often spills into personal life. Long hours, administrative responsibilities, and the emotional weight of patient care can leave little time or energy for family. This imbalance contributes to high divorce rates among dentists. The stress of maintaining a successful practice while nurturing personal relationships can become untenable, especially without adequate coping mechanisms.
Burnout and Suicide Risk
Burnout in dentistry is alarmingly common. A study by the American Dental Association found that 84% of dentists report experiencing burnout at some point in their careers.
Addressing these challenges requires systemic change. Mental health support, peer mentorship, and business education should be integrated into dental training. Encouraging open conversations about stress and providing resources for emotional well-being can help reduce stigma and promote resilience.
By acknowledging the hidden struggles of dentistry, the profession can move toward a healthier, more sustainable future.
Doctorate, or doctoral, is an umbrella term for many degrees — PhD among them — at the height of the academic ladder. Doctorate degrees fall under two categories, and here is where the confusion often lies.
The first category, Research (also referred to as Academic) includes, among others:
Doctor of Philosophy (PhD)
Doctor of Business Administration (DBA)
Doctor of Education (EdD)
Doctor of Theology (ThD)
The second category, Applied (also referred to as Professional) includes, among others:
Doctor of Medicine (MD)
Doctor of Podiatric Medicine (DPM)
Doctor Of Osteopathic Medicine (DO)
Doctor of Dental Surgery (DDS)
Doctor of Optometry (OD)
Doctor of Psychology (PsyD)
Juris Doctor (JD)
As you can see, applied doctorates are generally paired with very specific careers – medical doctors, podiatrists, dentists, optometrists, psychologists, and law professionals.
When it comes to outlining the differences between a PhD and doctorate, the real question should be, “What is the difference between a PhD and an applied doctorate?” The answer, again, can be found in the program outcomes. The online Doctor of Psychology at UAGC, for example, lists outcomes that are heavily focused on the ability to put theory into practice in a professional setting. For example:
Apply best practices in the field regarding professional values, ethics, attitudes, and behaviors
Exhibit culturally diverse standards in working professionally with individuals, groups, and communities who represent various cultural and personal backgrounds
Utilize a comprehensive psychology knowledge base grounded in theoretical models, evidence-based methods, and research in the discipline
Integrate leadership skills appropriate in the field of psychology
Critically evaluate applied psychology research methods, trends, and concepts
Bottom line: As the PhD is more academic, research-focused, and heavy on theory, an applied doctorate degree is intended to master a subject in both theory and practice.
Can a PhD Be Called a Doctor?
The debate over whether a PhD graduate should be called a doctor has existed for decades, and if you’re a member of this exclusive club, you’ll no doubt hear both sides of the argument during your lifetime. After all, if a PhD is a doctor, can a person with a doctoral degree in music – the Doctor of Musical Arts (DMA) – be called a doctor as well?
Those in favor argue that having “Dr.” attached to your name indicates that you are an expert and should be held in higher regard. For some, the debate is at the heart of modern gender disparity. For example, on social media and in some academic circles, there is an argument that female PhD holders should use the “Dr.” title in order to reject the notion that women are less worthy of adding the title to their name once they have earned a doctoral degree.
Why It Is Difficult to Be a Part-Time Financial Planner Today
In theory, part-time financial planning offers flexibility and work-life balance, making it an attractive option for professionals seeking reduced hours. However, in practice, the role of a financial planner has evolved into a demanding, full-time commitment. The complexity of financial markets, client expectations, regulatory requirements, and technological advancements make part-time financial planning increasingly difficult to sustain.
One of the primary challenges is client relationship management. Financial planning is deeply personal and trust-based. Clients expect consistent communication, timely updates, and proactive advice. A part-time planner may struggle to maintain the same level of responsiveness as full-time counterparts, especially during volatile market conditions or life-changing events like retirement, divorce, or inheritance. Delayed responses or limited availability can erode client confidence and damage long-term relationships.
***
***
Another obstacle is the rapid pace of financial change. Tax laws, investment products, insurance regulations, and retirement planning strategies are constantly evolving. Staying current requires ongoing education, certifications, and industry engagement. For part-time planners, keeping up with these changes while managing clients and administrative tasks can be overwhelming. Falling behind risks offering outdated or suboptimal advice, which could lead to compliance issues or client dissatisfaction.
Regulatory compliance adds another layer of complexity. Financial planners must adhere to strict standards set by organizations like FINRA, the SEC, and state regulators. These include documentation, disclosures, fiduciary responsibilities, and continuing education. Compliance is non-negotiable and time-consuming, regardless of hours worked. Part-time planners face the same scrutiny and liability as full-time professionals, but with fewer hours to manage the workload.
Technology, while a powerful tool, also presents challenges. Clients increasingly expect digital access to their portfolios, real-time updates, and virtual meetings. Managing these platforms requires technical proficiency and regular maintenance. Part-time planners may find it difficult to keep systems updated, troubleshoot issues, or provide tech support, especially if they lack dedicated staff.
Business development is another hurdle. Building and maintaining a client base requires networking, marketing, and referrals. Part-time planners often have limited time to attend events, follow up with leads, or cultivate relationships. This can hinder growth and make it difficult to compete with full-time advisors who are more visible and accessible.
Finally, there’s the issue of income and scalability. Many financial planners earn through commissions, assets under management (AUM), or fee-based models. Part-time work often means fewer clients and lower revenue, which can make it hard to justify the costs of licensing, insurance, software, and office space. Without scale, profitability becomes a challenge.
In conclusion, while the idea of part-time financial planning may seem appealing, the realities of the profession make it difficult to execute effectively. The demands of client care, compliance, education, and business development require consistent attention and availability. Unless the industry adapts to support flexible models, part-time financial planners will continue to face significant barriers to success.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Investment fees still matter for physicians and all of us, despite dropping dramatically over the past several decades due to computer automation, algorithms and artificial intelligence, etc. And, they can make a big difference to your financial health. So, before buying any investment thru a financial advisor, planner, manager, stock broker, etc., it’s vital to understand these two often confusing costs.
***
***
Fee Only: Paid directly by clients for their services and can’t receive other sources of compensation, such as payments from fund providers. Act as a fiduciary, meaning they are obligated to put their clients’ interests first
Fee Based: Paid by clients but also via other sources, such as commissions from financial products that clients purchase. Brokers and dealers (registered representatives) are simply required to sell products that are “suitable” for their clients. Not a fiduciary.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Classic: Acute care is a branch of secondary health care where a patient receives active but short-term treatment for a severe injury or episode of illness, an urgent medical condition, or during recovery from surgery. In medical terms, care for acute health conditions is the opposite from chronic care, or longer term care.
Modern: Acute care is active, short-term treatment for a severe injury or episode related to illness, an urgent medical condition or recovery from surgery.
A hedge fund is a limited partnership of private investors whose money is pooled and managed by professional fund managers. These managers use a wide range of strategies, including leverage (borrowed money) and the trading of nontraditional assets, to earn above-average investment returns. A hedge fund investment is often considered a risky, alternative investment choice and usually requires a high minimum investment or net worth. Hedge funds typically target wealthy investors.
The hedge fund manager I am considering also runs an offshore fund under a “master feeder” arrangement.
A PHYSICIAN’S QUESTION:What does this mean? In which fund should I invest?
The master feeder arrangement is a two-tiered investment structure whereby investors invest in the feeder fund. The feeder fund in turn invests in the master fund. The master fund is therefore the one that is actually investing in securities. There may be multiple feeder funds under one master fund. Feeder funds under the same master can differ drastically in terms of fees charged, minimums required, types of investors, and many other features – but the investment style will be the same because only the master actually invests in the market.
A master feeder structure is a very popular arrangement because it allows a portfolio manager to pool both onshore and offshore assets into one investment vehicle (the master fund) that allocates gains and losses in an asset-based, proportional manner back to the onshore and offshore investors. All investors, both offshore and onshore, get the same return. In this manner, the portfolio manager, despite offering more than one fund with different characteristics to different populations, is not faced with the dilemma of which fund to favor with the best investment ideas.
A manager may offer an offshore fund because there is demand for that manager’s skill either abroad, where investors may wish to preserve anonymity, or more commonly where investors simply do not wish to become entangled with the United States tax code. American citizens should generally avoid the offshore fund, since American citizens are taxed on their allocated share of offshore corporation profits whether or not a distribution occurs. Therefore, there is no benefit for most American taxpayers investing in an offshore fund.
Tax-exempt institutions, such as medical foundations, in the United States may have reason to consider an offshore hedge fund, however. Domestic tax-exempt organizations are generally not subject to unrelated business taxable income (UBTI) – the portion of hedge fund income that comes about as a result of the use of leverage – when investing with an offshore corporation. If the same tax-exempt organization were to invest in a domestic fund, and if UBTI was generated, then the organization would have to pay taxes on that UBTI. Most domestic hedge funds generate UBTI.
After a lifetime of hard work practicing medicine and saving, you’re at the retirement finish line. Instead of a paycheck, you’re relying on your nest egg and investment income to cover the bills. Picking the right investments is even more important, as you won’t have much chance to recover as a retired MD, DO, DPM or DDS.
“You made it to the top of the mountain through a systematic approach and are trying to make your way down safely,” says retirement planner John Gillet John Gillet in Hollywood, Fla. “Why throw all caution to the wind and try something different now?”
***
***
Definitions
An annuity is an insurance contract designed to grow your money and then repay it as income. There are different versions. An immediate annuity turns your lump sum into future guaranteed income payments, like your own personal pension. They are simple to understand with no or small fees.
Fixed annuities pay a guaranteed interest rate over a set period to grow your money, like 5% a year for five years. These options could make sense as part of a retirement plan.
A variable annuity, on the other hand, invests your savings in mutual funds. While you can buy riders that guarantee a minimum income, you’ll be paying very much for it. “All in, the annual fees can be 3% or more of your balance,” says Jeff Bailey, an advisor from Nashville. “That’s a huge withdrawal rate from your portfolio versus investing on your own.”
The variable annuity will lock up your money for years. If you cancel early, you owe a surrender charge that could start at 7% or more of your annuity balance before gradually going down as time goes by. “Clients believe they can walk away with their contract value, but that’s often not true,” says Bailey.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Asset allocation is one of the key factors contributing to long-term investment success.
When designing a portfolio that represents their risk tolerance, investors should be aware that a portfolio that is 50% stocks is likely to obtain approximately half of the gain when the market advances but suffer only half the loss when the market declines.
This general principle frequently holds true over extended investing cycles, but can waiver during shorter holding periods.
Case Model
For example, a fairly typical physician client of mine who has a 50% stock, 50% bond portfolio has obtained a return of 4.62% over the last 12 months, while the S&P 500 has obtained a return of 14.31% over the same time period (as of 10/30/14).
An investor expecting to obtain half the return of the index would anticipate a return of 7.15%, and by this measuring stick, has underperformed the market by over 2.50% during the last year.
What caused this differential?
Answer
The issue resides in how we define “the market.” In this example, we use the S&P 500 index as a measure for how the market as a whole is performing. As you may know, the S&P 500 (and the Dow Jones Industrial Average, for that matter) consists solely of large company U.S. stocks.
Of course, a diversified portfolio owns a mixture of large, mid, and small cap U.S. stocks, as well as international and emerging market equities. Consequently, comparing the performance of a basket of only large cap stocks to the performance of a diversified portfolio made up of a variety of different asset classes isn’t an apples-to-apples comparison.
***
***
Frequently, the diversified portfolio will outperform the non-diversified large cap index because several of the components of the diversified portfolio will obtain higher returns than those achieved by large cap holdings.
However, the past 12 months has been a case where a diversified portfolio underperformed the large cap index because large cap stocks were the best performing asset class over the time period. In fact, over the last twelve months, there has been a direct correlation between company size and stock performance (as of 10/30/14):
Large Cap Stocks (S&P 500): 14.92%
Mid Cap Stocks (Russell Mid Cap): 11.08%
Small Cap Stocks (Russell 2000): 4.45%
International Stocks (Dow Jones Developed Markets): -1.05%
Since large cap stocks were the best performing element of a diversified portfolio over the last 12 months, in retrospect, an investor would have obtained a superior return by owning only large cap stocks during the period as opposed to owning a diversified mix of different equities. Does this mean owning only large cap stocks rather than a diversified portfolio is the best investment approach going forward? Of course not.
Year after year, we don’t know which asset category will provide the best return and a diversified portfolio ensures we have exposure to each year’s big winner. Additionally, although large caps were this year’s winner, they could easily be next year’s big loser, and a diversified portfolio ensures we don’t have all our investment eggs in one basket.
Don’t be overly concerned if your diversified portfolio is underperforming a non-diversified benchmark over a short period of time. As always, long-term results should be more heavily weighted than short-term swings, and having a diversified portfolio is likely to maximize the probability of coming out ahead over an extended period.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Classic: A pre-payment plan refers to health insurance plans that provide medical or hospital benefits in service rather than dollars, such as the plans offered by various Health Maintenance Organizations. A method providing in advance for the cost of predetermined benefits for a population group, through regular periodic payments in the form of premiums, dues, or contributions including those contributions that are made to a health and welfare fund by employers on behalf of their employees!
Modern: A Prepaid Group Practice Plan specifies health services are rendered by participating physicians to an enrolled group of persons, with a fixed periodic payment made in advance by (or on behalf of) each person or family. If a health insurance carrier is involved, a contract to pay in advance for the full range of health services to which the insured is entitled under the terms of the health insurance contract.
Examples:
Pre-Paid Hospital Service Plan: The common name for a health maintenance organization (HMO), a plan that provides comprehensive health care to its members, who pay a flat annual fee for services.
Pre-Paid Premium: An insurance or other premium payment paid prior to the due date. In insurance, payment by the insured of future premiums, through paying the present (discounted) value of the future premiums or having interest paid on the deposit.
Pre-Paid Prescription Plan: A drug reimbursement plan that is paid in advance.
Hobson’s choice is a free choice in which only one thing is actually offered. The term is often used to describe an illusion that choices are available. The best known example is “I’ll give you a choice: Take it or leave it”, wherein “leaving it” is strongly undesirable.
The phrase is said to have originated with Thomas Hobson (1544–1631), a livery stable owner in Cambridge, England, who offered customers the choice of either taking the horse in the stall nearest to the door or taking none at all.
A CASE MODEL
Half of Physicians Plan to Change Career Paths
The Physicians Foundation recently conducted a survey on physician practice patterns and perspectives. Here are some key findings from the report:
• 31% of physicians identify as independent practice owners or partners. • Almost half (47%) of physicians plan to change career paths. • 78% of physicians sometimes, often or always experience feelings of burnout. • Nearly a quarter of physician time is spent on non-clinical paperwork.
This result is not a good Hobson’s Choice in Medicine.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The Series 65 exam — the NASAA Investment Advisers Law Examination — is a North American Securities Administrators Association (NASAA) exam administered by FINRA.
The exam consists of 130 scored questions and 10 unscored questions. Candidates have 180 minutes to complete the exam. In order for a candidate to pass the Series 65 exam, they must correctly answer at least 92 of the 130 scored questions.
Posted on September 27, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
A paradox is a statement that appears at first to be contradictory, but upon reflection then makes sense. This literary device is commonly used to engage a reader to discover an underlying logic in a seemingly self-contradictory statement or phrase. As a result, paradox allows readers to understand concepts in a different and even non-traditional
***
***
GOVERNMENT HEALTH INFORMATION IS TRUSTED?
Classic Definition: Despite the PP-ACA, there is ambivalence about the role of the US Government as a source of quality healthcare information.
Modern Circumstance: Of brands presented to respondents in a Consumer Reports (50 percent), and AARP (37 percent) survey, they outpolled the “US Government Healthcare Quality Reporting Website” (36 percent) and Medicare Website (32 percent).
Paradox Example: The focus groups expressed “mixed reactions and raised doubts about government involvement in quality ratings information. At least one participant in each group expressed skepticism about trusting ‘the government’ to compile information.”
Younger consumers especially questioned the relevance of Medicare measures to the non-elderly population. Yet participants gravitated to “.gov” websites over “.org” websites as a more authoritative source.
CITE: Williams, Jason: Health Affairs, December 28, 2016
Economy: Headline PCE rose from 2.6% on an annual basis in July to 2.7% in August, while core PCE stayed flat at 2.9%—all in line with analyst expectations.
Stocks: Solid inflation numbers helped equities arrest their recent selloff and offset the latest batch of tariffs. However, all three major indexes still ended the week lower than where they started.
Commodities: Oil climbed as Ukrainian drones continue to strike Russian energy infrastructure. Meanwhile, gold hit another all-time high, and rose above $3,800 for the first time ever at one point today.
According to Wayne Firebaugh CPA, CFP®, CMP™ alpha measures non-systematic return on investment [ROI], or the return that cannot be attributed to the market.
It shows the difference between a fund’s actual return and its expected performance given the level of systematic (or market) risk (as measured by beta).
Example
For example, a fund with a beta of 1.2 in a market that returns 10% would be expected to earn 12%. If, in fact, the fund earns a return of 14%, it then has an alpha of 2 which would suggest that the manager has added value. Conversely, a return below that expected given the fund’s beta would suggest that the manager diminished value.
In a truly efficient market, no manager should be able to consistently generate positive alpha. In such a market, the endowment manager would likely employ a passive strategy that seeks to replicate index returns. Although there is substantial evidence of efficient domestic markets, there is also evidence to suggest that certain managers do repeat their positive alpha performance.
In fact, a 2002 study by Roger Ibbotson and Amita Patel found that “the phenomenon of persistence does exist in domestic equity funds.” The same study suggested that 65% of mutual funds with the highest style-adjusted alpha repeated with positive alpha performances in the following year.
More Research
Additional research suggests that active management can add value and achieve positive alpha in concentrated portfolios.
A pre 2008 crash study of actively managed mutual funds found that “on average, higher industry concentration improves the performance of the funds. The most concentrated funds generate, after adjusting for risk … the highest performance. They yield an average abnormal return [alpha] of 2.56% per year before deducting expenses and 1.12% per year after deducting expenses.”
FutureMetrics
FutureMetrics, a pension plan consulting firm, calculated that in 2006 the median pension fund achieved record alpha of 3.7% compared to a 60/40 benchmark portfolio, the best since the firm began calculating return data in 1988. Over longer periods of time, an endowment manager’s ability to achieve positive alpha for their entire portfolio is more hotly debated. Dimensional Fund Advisors, a mutual fund firm specializing in a unique form of passive management, compiled FutureMetrics data on 192 pension funds for the period of 1988 through 2005.
Their research showed that over this period of time approximately 75% of the pension funds underperformed the 60/40 benchmark. The end result is that many endowments will use a combination of active and passive management approaches with respect to some portion of the domestic equity segment of their allocation.
Assessment
One approach is known as the “core and satellite” method in which a “core” investment into a passive index is used to capture the broader market’s performance while concentrated satellite positions are taken in an attempt to “capture” alpha. Since other asset classes such as private equity, foreign equity, and real assets are often viewed to be less efficient, the endowment manager will typically use active management to obtain positive alpha from these segments.
Notes:
Ibbotson, R.G. and Patel, A.K. Do Winners Repeat with Style? Summary of Findings – Ibbotson & Associates, Chicago (February 2002).
Kacperczyk, M.T., Sialm, C., and Lu Zheng. On Industry Concentration of Actively Managed Equity Mutual Funds. University of Michigan Business School. (November 2002).
2007 Annual US Corporate Pension Plan Best and Worst Investment Performance Report. FutureMetrics, April 20, 2007.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@outlook.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Public Relations [PR] is differentiated than advertising in that an advertiser pays for and has control over the message. It differs from personal selling in that the message is non-personal, i.e., not directed to a particular individual patient. We pay for advertising but pray for public relations. Public relations are not controllable but it is free; advertising is not free. PR suggests that “good news or bad news”; just spell the doctors name correctly
Change Management is the discipline that guides how we prepare, equip and support individuals to successfully adopt to change in order to drive organizational success and outcomes.
For example, a senior doctor may retire, become ill, or a junior associate might become a practice partner. How will patients be affected?
Crisis Management is the precautions and identification of threats to an organization and its stakeholders, and the methods used by the organization to deal with these threats.
For example, recall in 1982, that Tylenol™ commanded 35 percent of the over-the-counter analgesic market in America and it represented nearly 17 percent of Johnson & Johnson’s profits. But, when seven people died from consuming the tainted drug, a national panic ensued. Moreover, Americans started to question the safety of all over-the-counter medications.
Fortunately, J&J commenced the proto-typical positive crisis response in the following way:
J&J acted quickly, with complete candidness about what happened and within hours of learning of the deaths, J&J installed toll-free numbers for consumers, sent alerts to healthcare providers nationwide, and stopped advertising the product. J&J recalled 31 million bottles of Tylenol™ capsules and offered replacement products free of charge. J&J did not wait for evidence to see whether the contamination might be more widespread.
J&J’s leadership was in the lead and seemed in full control throughout the crisis. The chairman was admired for his leadership to pull Tylenol™ capsules off the market and his forthrightness in dealing with the media. The Tylenol™ crisis led the news every night on every station for six weeks.
J&J placed consumers first. J&J spent more than $100 million for the recall and re-launch of Tylenol™. The stock which had been trading near a 52-week high just before the tragedy, dropped for a time, but recovered to its highs only two months later.
J&J accepted responsibility. The disaster could have been described in many different ways: as an assault on the company, as a problem somewhere in the process of getting Tylenol™ from J&J factories to retail stores, or as the acts of a crazed criminal. Yet, the company accepted full responsibility.
J&J sought to ensure that measures were taken to prevent a recurrence of the problem. J&J introduced tamper-proof packaging that would make it much more difficult for a similar incident to occur in the future.
J&J presented itself prepared to handle the short-term damage in the name of consumer safety. Within a year of the disaster, J&J’s share of the analgesic market, which had fallen to 7 percent from 37 percent following the poisoning, had climbed back to 30 percent.
This wildly successful response in now the stuff of graduate and business school case models for excellence in teaching!
PRM stands for Patient Relationship Management, which is a system for managing all interactions with current and potential patients, families, friends, referring physicians, clinics and hospitals. The goal is simple: improve relationships to grow your medical practice. PRM technology helps medical practices and clinics stay connected to patients, streamline processes, and improve profitability.
When people talk about PRM, they’re usually referring to a PRM system: software that helps track each interaction with a patient or elated others. That can include practice sales calls, treatment or service plans, marketing e-mails, website, social media and more. PRM tools can unify patient and practice data from many sources and even use Artificial Intelligence [AI] to help better manage relationships across the entire doctor– patient lifecycle – spanning departments described elsewhere in the Marketing, Advertising and Sales ME-Ps.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
References:
1. Purcarea, Victor: The impact of marketing strategies in healthcare systems. J. Med Life. 2019 Apr-Jun;12(2):93–96. doi: 10.25122/jml-2019-1003
READINGS:
Marcinko, DE and Hetico, HR: The Business of Medical Practice [3rd Edition]. Springer Publishing, New York, 2010.
Marcinko, DE and Hetico, HR: Hospitals & Healthcare Organizations [Management Strategies, Operational Techniques, Tools, Templates and Case Studies]. Productivity Press, New York, 2012.
Marcinko, DE and Hetico, HR: Financial Management Strategies for Hospitals and Healthcare Organizations [Tools, Techniques, Checklists and Case Studies]. Productivity Press, New York, 2012.
An app, which is short for “application,” is a type of software that can be installed and run on a computer, tablet, smartphone or other electronic devices. An app most frequently refers to a mobile application or a piece of software that is installed and used on a computer. Most apps have a specific and narrow function.
An easy and fairly cheap way for novices to get into investing is to use a robo-advisor. Basically, the funds you contribute will be invested by an algorithm based upon your goals, which are usually determined by taking a survey. This helps keep fees low; the algorithm doesn’t rely on a human expert to make trades, and you don’t have to spend significant amounts of time researching your investments. While this is a good way to start, it may not be the best option in the long run.
Online Brokerage or Investment Apps
More options are becoming available all the time, and they have opened trading to a much larger percentage of the population. That is a great thing, but it’s important to remember that “easier to invest” doesn’t necessarily mean it’s easy to invest well.
Be wary of apps that “gamify” trading and encourage risky choices. Keep in mind that trusted names offer more security, so do your research when you are selecting a platform.
A Financial Self Discovery Questionnairefor Medical Professionals
For understanding your relationship with money, it is important to be aware of yourself in the contexts of culture, family, value systems and experience. These questions will help you. This is a process of self-discovery. To fully benefit from this exploration, please address them in writing. You will simply not get the full value from it if you just breeze through and give mental answers. While it is recommended that you first answer these questions by yourself, many people relate that they have enjoyed the experience of sharing them with others who are important to them.
As you answer these questions, be conscious of your feelings, actually describing them in writing as part of your process.
Childhood
What is your first memory of money?
What is your happiest moment with Money? Your most unhappy?
Name the miscellaneous money messages you received as a child.
How were you confronted with the knowledge of differing economic circumstances among people, that there were people “richer” than you and people “poorer” than you?
Cultural heritage
What is your cultural heritage and how has it interfaced with money?
To the best of your knowledge, how has it been impacted by the money forces? Be specific.
To the best of your knowledge, does this circumstance have any motive related to Money?
Speculate about the manners in which your forebears’ money decisions continue to affect you today?
Family
How is/was the subject of money addressed by your church or the religious traditions of your forebears?
What happened to your parents or grandparents during the Depression?
How did your family communicate about money?
How? Be as specific as you can be, but remember that we are more concerned about impacts upon you than historical veracity.
When did your family migrate to America (or its current location)?
What else do you know about your family’s economic circumstances historically?
Your parents
How did your mother and father address money?
How did they differ in their money attitudes?
How did they address money in their relationship?
Did they argue or maintain strict silence?
How do you feel about that today?
Please do your best to answer the same questions regarding your life or business partner(s) and their parents.
Childhood: Revisited
How did you relate to money as a child? Did you feel “poor” or “rich”? Relatively? Or, absolutely? Why?
Were you anxious about money? Did you receive an allowance? If so, describe amounts and responsibilities.
Did you have household responsibilities?
Did you get paid regardless of performance?
Did you work for money?
If not, please describe your thoughts and feelings about that.
***
***
Same questions, as a teenager, young adult, older adult.
Credit
When did you first acquire something on credit?
When did you first acquire a credit card?
What did it represent to you when you first held it in your hands?
Describe your feelings about credit.
Do you have trouble living within your means?
Do you have debt?
Adulthood
Have your attitudes shifted during your adult life? Describe.
Why did you choose your personal path? a) Would you do it again? b) Describe your feelings about credit.
Adult attitudes
Are you money motivated? If so, please explain why? If not, why not? How do you feel about your present financial situation? Are you financially fearful or resentful? How do you feel about that?
Will you inherit money? How does that make you feel?
If you are well off today, how do you feel about the money situations of others? If you feel poor, same question.
How do you feel about begging? Welfare? If you are well off today, why are you working?
Do you worry about your financial future?
Are you generous or stingy? Do you treat? Do you tip?
Do you give more than you receive or the reverse? Would others agree?
Could you ask a close relative for a business loan? For rent/grocery money?
Could you subsidize a non-related friend? How would you feel if that friend bought something you deemed frivolous?
Do you judge others by how you perceive they deal with their Money? Do you feel guilty about your prosperity? Are your siblings prosperous?
What part does money play in your spiritual life?
Do you “live” your Money values?
Conclusion
There may be other questions that would be useful to you. Others may occur to you as you progress in your life’s journey. The point is to know your personal money issues and their ramifications for your life, work, and personal mission.
This will be a “work-in-process” with answers both complex and incomplete. Don’t worry.
Just incorporate fine-tuning into your life’s process.
The Series 6 exam — the Investment Company and Variable Contracts Products Representative Qualification Examination (IR) — assesses the competency of an entry-level representative to perform their job as an investment company and variable contracts products representative.
The exam measures the degree to which each candidate possesses the knowledge needed to perform the critical functions of an investment company and variable contract products representative, including sales of mutual funds and variable annuities.
Candidates must pass the Securities Industry Essentials (SIE) exam and the Series 6 exam to obtain the Investment Company and Variable Contracts Products registration.
The study of behavioral economics has revealed much about how different biases can affect our finances—often for the worse.
Take loss aversion: Because we feel a financial setback more acutely than a commensurate gain, we often cling to failed investments to avoid realizing the loss. Another potential hazard is present bias, or the tendency to prefer instant gratification over long-term reward, even if the latter gain is greater.
When it comes to money, sometimes it’s difficult to make rational decisions. Here, are three behavioral financial biases that could be impeding financial goals.
ANCHORING BIAS
Anchoring Bias happens when we place too much emphasis on the first piece of information we receive regarding a given subject. Anchoring is the mental trick your brain plays when it latches onto the first piece of information it gets, no matter how irrelevant. You might know this as a ‘first impression’ when someone relies on their own first idea of a person or situation.
Example: When shopping for a wedding ring a salesman might tell us to spend three months’ salary. After hearing this, we may feel like we are doing something wrong if we stray from this financial advice, even though the guideline provided may cause us to spend more than we can afford.
Example: Imagine you’re buying a car, and the salesperson starts with a high price. That number sticks in your mind and influences all your subsequent negotiations. Anchoring can skew our decisions and perceptions, making us think the first offer is more important than it is. Or, subsequent offers lower than they really are.
Example: Imagine an investor named Jane who purchased 100 shares of XYZ Corporation at $100 per share several years ago. Over time, the stock price declined to $60 per share. Jane is anchored to her initial price of $100 and is reluctant to sell at a loss because she keeps hoping the stock will return to her original purchase price. She continues to hold onto the stock, even as it declines, due to her anchoring bias. Eventually, the stock price drops to $40 per share, resulting in significant losses for Jane.
In this example, Jane’s nchoring bias to the original purchase price of $100 prevents her from rationalizing to sell the stock and cut her losses, even though market conditions have changed. So, the next time you’re haggling for your self, a potential customer or client, or making another big financial decision, be aware of that initial anchor dragging you down.
HERD MENTALITY BIAS
Herd Mentality Bias makes it very hard for humans to not take action when everyone around us does.
Example: We may hear stories of people making significant monetary profits buying, fixing up, and flipping homes and have the desire to get in on the action, even though we have no experience in real estate.
Example: During the dotcom bubble of the late 1990’s many investors exhibited a herd mentality. As technology stocks soared to astronomical valuations, investors rushed to buy these stocks driven by the fear of missing out on the gains others were enjoying. Even though some of these stocks had questionable fundamentals, the herd mentality led investors to follow the crowd.
In this example, the herd mentality contributed to the overvaluation of technology stocks. Eventually, it led to the dot-com bubble’s burst, causing significant losses for those who had unthinkingly followed the crowd without conducting proper research or analysis.
OVERCONFIDENT INVESTING BIAS
Overconfident Investing Bias happens when we believe we can out-smart other investors via market timing or through quick, frequent trading. This causes the results of a study to be unreliable and hard to reproduce in other research settings.
Example: Data convincingly shows that people and financial planners/advisors and wealth managers who trade most often under-perform the market by a significant margin over time. Active traders lose money.
Example: Overconfidence Investing Bias moreover leads to: (1) excessive trading (which in turn results in lower returns due to costs incurred), (2) underestimation of risk (portfolios of decreasing risk were found for single men, married men, married women, and single women), (3) illusion of knowledge (you can get a lot more data nowadays on the internet) and (4) illusion of control (on-line trading).
ASSESSMENT
Finally, questions remain after consuming this cognitive bias review.
Question: Can behavioral cognitive biases be eliminated by financial advisors in prospecting and client sales endeavors?
A: Indeed they can significantly reduce their impact by appreciating and understanding the above and following a disciplined and rational decision-making sales process.
Question: What is the role of financial advisors in helping clients and prospects address behavioral biases?
A: Financial advisors can provide an objective perspective and help investors recognize and address their biases. They can assist in creating well-structured investment and financial plans, setting realistic goals, and offering guidance to ensure investment decisions align with long-term objectives.
Question:How important is self-discipline in overcoming behavioral biases?
A; Self-discipline is crucial in overcoming behavioral biases. It helps investors and advisors adhere to their investment plans, avoid impulsive decisions, and stay focused on long-term goals reducing the influence of emotional and cognitive biases.
CONCLUSION
Remember, it is far more useful to listen to client beliefs, fears and goals, and to suggest options and offer encouragement to help them discover their own path toward financial well-being. Then, incentivize them with knowledge of the above psychological biases to your mutual success!
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
REFERENCES:
Marcinko, DE; Dictionary of Health Insurance and Managed Care. Springer Publishing Company, New York, 2007.
Marcinko, DE: Comprehensive Financial Planning Strategies for Doctors and Advisors: Best Practices from Leading Consultants and Certified Medical Planners™. Productivity Press, NY, 2016.
Marcinko, DE: Risk Management, Liability and Insurance Strategies for Doctors and Advisors: Best Practices from Leading Consultants and Certified Medical Planners™. Productivity Press, NY, 2017.
Nofsinger, JR: The Psychology of Investing. Rutledge Publishing, 2022
Winters, Scott: The 10X Financial Advisor: Your Blueprint for Massive and Sustainable Growth. Absolute Author Publishing House, 2020.
Despite their high salaries, not all doctors are wealthy, and some live paycheck to paycheck. Here are 5 reasons why many doctors today are broke, according to https://medschoolinsiders.com
1 | Believing They Are Universally Smart
The first reason so many doctors are broke is that many doctors believe they are universally smart. While most doctors have deep specialized knowledge, there’s a big difference between being smart in your profession and being smart with money. A physician’s schooling is quite thorough when it comes to the human body, but med school doesn’t include a prerequisite class on how to handle finances.
Graduating medical school is a major feat and certainly demonstrates superior work ethic and cognitive abilities. But many new doctors believe these accomplishments transcend all aspects of life. If you’re smart enough to earn an MD, you’re certainly smart enough to handle your finances, but only once you properly and intentionally educate yourself.
The truth is doctors, especially traditional graduates, haven’t had an opportunity to manage large sums of money until they become fully trained attending physicians and start pulling in low to mid six figures in income. Prior to that, there was very little of it to manage.
Far too many aspiring doctors, and students in general, don’t take the time to learn financial basics, in part because it’s uncomfortable and seems like something they can figure out “later”, whenever that may be. Their poor spending habits and lack of investment knowledge carry over into their careers, causing many to make irresponsible decisions.
The second factor is overspending too soon, and this comes up at two points in training.
First, it’s natural to want to start spending more as soon as you get into residency and start making a little more money. After all, you’ve been a broke student for 8 or more years, and now you’re finally making a reasonable and reliable wage. But that’s where young doctors get into trouble. Residency pays, but not nearly as much as you will be making once you become an attending physician. The average resident makes about $60K a year, and if you begin spending all of that money right away, thinking you’ll handle your loans once you become an attending, you delay paying off your medical school debt, which means the compounding effect through your student loan interest rate works against you.
Now that $250,000 in student loans has ballooned to over $350,000 by the time you finish residency. The compounding effect, which can be one of your greatest allies in your financial life, becomes an equally powerful enemy when working against you through debt. But of course, pinching pennies is easier said than done, especially when you’re in residency and are surrounded by peers in different professions. They’ve been earning good money much longer than you have, and they can afford more luxurious lifestyles.
They may not be worried about indulging in fine dining or how much a hotel costs when traveling. Students in college and medical school are often confident they will resist the temptations, but the desire to keep up with your friends and family can be difficult to ignore, which causes many to overspend before they technically have the money to do so.
The same is true of attending physicians. As soon as those six-figure salaries come rolling in, many physicians go overboard with spending, trying to make up for lost time and to treat yourself.
Now, we are not suggesting you shouldn’t reward yourself for completing residency, but that reward shouldn’t be a Lamborghini. It’s best to continue living like a resident in your first few years after becoming an attending to pay off loans, put a down payment on a home, and get your financial foundation built before loosening the purse strings.
3 | Decreasing Salaries
Third, doctors continue to make less money than they did before. And this includes nearly all 44 medical specialties. For example, while physician compensation technically rose from $343k to $391k between 2017 and 2022, this rise does not keep up with inflation. The real average compensation in 2022 was less than $325k—a $20k decrease in purchasing power in only six years.
For doctors who are already spending to the limits of their salaries with huge mortgages, car payments, business costs, and other luxuries, a decreased salary can have a huge impact. You might be able to cut back by going on fewer vacations or eating out less frequently, but many accrued costs are locked in, such as a mortgage payment, car loan, or leased rental space for your practice.
4 | Increasing Costs of Private Practice
In the past, running a private practice was much simpler, but recent stricter guidelines and regulations have made it difficult for solo practices to keep up. While regulations like the Health Insurance Privacy and Portability Act, or HIPAA, and mandatory Electronic Medical Records, or EMRs, are necessary to protect patients, they make costs higher for physicians who run their own private practice. These physicians need to spend their own money to set up and maintain EMRs as well as invest in security to ensure patient data is protected.
With the steep rise of inflation we’ve seen over the past couple of years, everything is more expensive, which means costs, such as business space, equipment, and even office supplies, have gone up for private practice physicians while salaries have not. 2013 to 2020 saw an annual inflation rate of anywhere from 0.7% to 2.3%. This skyrocketed to an annual inflation rate of 7.0% in 2021 and another 6.5% in 2022. In fact, the cost of running a private practice has increased by almost 40% between 2001 and 2021.
These increased costs are exacerbated by another problem plaguing private practices; decreased reimbursement. While costs increased by almost 40%, Medicare reimbursement only increased by 11%. When doctors see patients who are insured, the insurance companies pay the physicians for their time. For Medicare, the new proposed rules for 2023 would cut reimbursement by around 5%. When adjusting for inflation, Medicare reimbursement decreased by 20% in the last 20 years.
These costs add up, making it extremely difficult for physicians to thrive financially while running a private practice.
5 | Tuition Debt
Lastly, we can’t talk about a doctor’s finances without mentioning the exorbitant debt so many graduating physicians are left with. It won’t shock you to hear that med school is expensive. Extremely expensive. The average cost of tuition for a single year is nearly $60k, with significant variance from school to school, and that’s before accounting for living expenses.
In-state applicants pay less than out-of-state applicants, and students at private schools typically pay more than students at public medical schools. The astronomical costs mean the vast majority of students can’t pay for medical school out of their own pockets. And unless your family is part of the 1%, even with your parents footing the bill, it’s difficult to cover tuition, let alone rent, groceries, transportation, tech, social activities, exam fees, and application costs.
The average total student debt after college and med school is over $250k. But keep in mind that’s the average, which includes 27% of students who graduate with no debt at all. This means the vast majority of students leave medical school owing much more than $250k.
For some perspective, in 1978, the average debt for graduating MDs was $13,500, which, when adjusted for inflation, is a little over $60,000. There are multiple ways to eventually repay these loans, but time and discipline are essential to ensure this money is paid off as quickly as possible.
According to financial advisor Dr. David Edward Marcinko MEd MBA CMP™; consider the following:
Place a portion of your salary (15-20% or more) into a savings account, and another portion (10-20% or more) into wise investments [stocks, bonds, mutual funds, and/or ETFs].
Pay off your bills each month, and then use leftover spending money to purchase fun things like vacations and fancy dinners, within your means. Shop sales, buy used clothes, and use credit card points for travel.
Hire an excellent tax professional and meet with an investment advisor once or twice a year about your investment status and strategy. http://www.MarcinkoAssociates.com
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The Memory Palace Fallacy – Learning Styles Don’t Actually Exist
Remember being told you’re a “visual learner” or an “auditory learner”? Well, turns out that whole learning styles theory is pretty much bunk.
Common Learning Myths have been thoroughly debunked by modern educational research, and this is a big one. Studies consistently show that matching teaching methods to supposed learning styles doesn’t improve outcomes at all.
What actually matters is matching the teaching method to the content itself – you learn geography better with maps because geography is visual, not because you’re a “visual person.” It’s like trying to learn piano by reading about it versus actually playing keys. The activity should match what you’re trying to learn, not some made-up category about how your brain supposedly works.
The Series 7 exam — the General Securities Representative Qualification Examination (GS) — assesses the competency of an entry-level registered representative to perform their job as a general securities representative.
The exam measures the degree to which each candidate possesses the knowledge needed to perform the critical functions of a general securities representative, including sales of corporate securities, municipal securities, investment company securities, variable annuities, direct participation programs, options and government securities.
A computer that could break the encryption that safeguards your private information on the internet. A machine that can design powerful new drugs by precisely simulating the behavior of individual molecules. A device that optimizes complex supply chains to help companies get the parts they need and assemble them in the most efficient way possible.
These are all examples of how an emerging technology — the quantum computer — could change our world.
These computers work by harnessing quantum physics — the strange, often counterintuitive laws that govern the universe at its smallest scales and coldest temperatures. Today’s quantum computers are rudimentary and error-prone. But if more advanced and robust versions can be made, they have the potential to rapidly crunch through certain problems that would take current computers years. That’s why governments, companies and research labs around the world are working feverishly toward this goal.
Quantum computers will not replace our familiar “classical” computers. Rather, the two types of machines could work together to solve problems that stymie classical computers, potentially supercharging scientific research in fields such as materials and drug discovery, giving a boost to industry and upending cybersecurity as we know it.
A paradox is a statement or situation that seems contradictory but actually makes sense when you think about it more deeply. It challenges logic and often reveals a hidden truth.
FLEXIBLY DOGMATIC PARADOX
The Flexibly Dogmatic Paradox suggests that no matter how sensible your financial planning, investing or wealth management process is there will be uncomfortably long periods when it looks broken. And process is the best way of ensuring you keep standing for something because if you don’t stand for something, you’ll fall for anything. This is why, when assessing an investment fund, focus 50% on the manager’s character and 50% on their process. Everything else is detail. There are few guarantees in investing, but the fact that markets will batter you emotionally is one of them.
Example: During volatile times, the temptation to abandon the process is strong. But that’s why it’s there. Process is what forces one fund manager to keep buying unbroken companies when everyone else thinks they’re bust, and another to keep faith with a top-quality company when the mob says it’s too expensive The best fund managers dogmatically stick to their process when it’s out of favor. Then, when it returns to favor, the elastic pings back: they recapture lost ground surprisingly fast. However, every rule has an exception. And spotting the exceptions to their process is something the true greats have a knack for buying and selling.
***
***
Example: In 2007, US value manager Bill Miller had the makings of an investment legend, but the financial crisis wrecked all that. His process told him to double down into falling share prices, which had worked well for years. But it doesn’t work if the companies go bust, which many of his financial stocks did in 2008.
The fact is that no matter how good it is, a process operated without human judgment is just an algorithm. The best fund managers and financial prospectors and sales men/women know this.
They stick dogmatically to their process but somehow remain flexible enough to spot the occasions when it’s about to drive them into a brick wall.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Capitation is a type of healthcare payment system in which a physician or hospital is paid a fixed amount of money per patient for a prescribed period by an insurer or physician association. The cost is based on the expected healthcare utilization costs for a group of patients for that year.
With capitation, the physician—otherwise known as the primary care physician— is paid a set amount for each enrolled patient whether a patient seeks care or not. The PCP is usually contracted with an HMO whose role it is to recruit patients.
According to Richard Eskow, CEO of Health Knowledge Systems of Los Angeles, capitated medical reimbursement has been used in one form or another, in every attempt at healthcare reform since the Norman Conquest. Some even say an earlier variant existed in ancient China [personal communication].
Initially, when Henry I assumed the throne of the newly combined kingdoms of England and Normandy, he initiated a sweeping set of healthcare reforms. Historical documents, though muddled, indicate that soon thereafter at least one “physician,” John of Essex, received a flat payment honorarium of one penny per day for his efforts. Historian Edward J. Kealey opined that sum was roughly equal to that paid to a foot-soldier or a blind person. Clearer historical evidence suggests that American doctors in the mid-19th century were receiving capitation-like payments. No less an authoritative figure than Mark Twain, in fact, is on record as saying that during his boyhood in Hannibal, MO his parents paid the local doctor $25/year for taking care of the entire family regardless of their state of health.
Later, Sidney Garfield MD [1905-1984] is noted as one of the great under-appreciated geniuses of 20th century American medicine stood in the shadow cast by his more celebrated partner, Henry J. Kaiser. Garfield was not the first physician to embrace the notion of prepayment capitation, nor was he the first to understand that physicians working together in multi-specialty groups could, through collaboration and continuity of care, outperform their solo practice colleagues in almost every measure of quality and efficiency. The Mayo brothers, of course, had prior claim to that distinction. What Garfield did, was marry prepayment to group practice, providing aligned financial incentives across every physician and specialty in his medical group, as well as a culture of group accountability for the care of every member of the affiliated health plan. He called it “the new economics of medicine,” and at its heart was a fundamentally new paradigm of care that emphasized – prevention before treatment – and health before sickness. Under his model: the fewer the sick – the greater the remuneration. And: the less serious the illness, the better off the patient and the doctors.
Such ideas were heresy to the reigning fee-for-service, solo practice, ideologues of the mainstream medical establishment of the 1940s and ‘50s, of course. Throughout the period, Garfield and his group physicians were routinely castigated by leaders of the AMA and county medical associations as socialistic and unethical. The local medical associations in Garfield’s expanding service areas – the San Francisco Bay Area, Los Angeles, and Portland, Oregon – blocked group practice physicians from association membership, effectively shutting them out of local hospitals, denying them patient referrals or specialty society accreditation. Twice in the 1940s, formal medical association charges were brought against Garfield personally, at one time temporarily succeeding in suspending his license to practice medicine.
Of course, capitation payments made a comeback in the first cost-cutting managed care era of the 1980-90s because fee-for-service medicine created perverse incentives for physicians by paying more for treating illnesses and injuries than it does for preventing them — or even for diagnosing them early and reducing the need for intensive treatment later. Nevertheless, the modern managed care industry’s experience with capitation wasn’t initially a good one. The 1980-90s saw a number of HMOs attempt to put independent physicians, especially primary care doctors, into a capitation reimbursement model. The result was often negative for patients, who found that their doctors were far less willing to see them — and saw them for briefer visits — when they were receiving no additional income for their effort. Attempts were also made to aggregate various types of health providers — including hospitals and physicians in multiple specialties — into “capitation groups” that were collectively responsible for delivering care to a defined patient group. These included healthcare facilities and medical providers of all types: physicians, osteopaths, podiatrists, dentists, optometrists, pharmacies, physical therapists, hospitals and skilled nursing homes, etc.
However, the healthcare industry isn’t collective by nature, and these efforts tended to be too complicated to succeed. One lesson that these experiments taught is that provider behavior is difficult to change unless the relationship between that behavior and its consequences is fairly direct and easy to understand.
Today, the concept of prepayment and medical capitation is to uncouple compensation from the actual number of patients seen, or treatments and interventions performed. This is akin to a fixed price restaurant menu, as opposed to an àla carte eatery.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
When owners of a security spread false information to pump up the price of the security and subsequently sell off their shares, making a profit—the “dump.”
Refer to attempts by investors to move the price of a stock opportunistically by selling large numbers of shares short. The investors pocket the difference between the initial price and the new, lower price after this maneuver. This technique is illegal under SEC rules, which stipulate that every short sale must be on an uptick. For more information on this complex tactic, read on in this piece from the Wharton School of Business.
Wash Trading
Involves the simultaneous or near-simultaneous sale and repurchase of the same security for the purpose of generating activity and increasing the price.
When fraudsters manipulate the market through matched orders, they enter trades to buy or sell securities with the knowledge that a matching order on the opposite side has been or will be entered. During his tenure at the Commission, our partner Jordan Thomas was involved in a case where the SEC won summary judgement and obtained settlements with an astonishing 16 defendants who engaged in matched trades, among other illicit tactics.
Painting the Tape
Painting the tape refers to placing successive orders in small amounts at increasing or decreasing prices.
Spoofing & Layering
High frequency traders are known to use the tactics of Spoofing & Layering to manipulate share prices. Spoofing is the placing of a bid or offer with the intent to cancel before execution. Layering is a form of spoofing in which the trader places multiple orders on one side of the book, in order to create a false impression of heavy buying or selling.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Although 97% of people aren’t yet millionaires, many could eventually meet that target if they start investing sooner rather than later; especially doctors [MD, DO, DPM, DDS or DMD].
A 20-year-old, for instance, needs to invest just $330 a month into an asset class that delivers a 7% to 8% annual return to reach $1.26 million by the time s/he turns 65 years old. The luxury of time significantly boosts your chances of becoming a millionaire.
This doesn’t mean it’s too late for middle-aged savers to reach that millionaire milestone, but it will take a significantly greater investment. If a 50-year-old doctor hasn’t started saving for retirement, s/he would need to invest $3,958 a month at a steady 7% return to reach $1.26 million by retirement.
However, according to one Goldman Sachs report, investors could expect the S&P 500 to deliver just 3% annualized nominal returns over the next 10 years.
After an average 13% yearly return for the past decade, a new strategy outside of the stock market may be needed for that level of outsized gain, especially if you’re late to investing.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Classic: The portion of medical expenses a patient is responsible for paying.
Modern: Refers to the maximum you will pay during your policy period, which is typically a year, before your plan starts to pay 100% of your allowed amount. The costs of your deductible, co-pay, and co-insurance are included here, but not your premium.
Classic: “Out-of-network” health care providers do not have an agreement with your insurance company to provide care. While insurance companies may have some out-of-network benefits, medical care from an out-of-network provider will usually cost more out-of-pocket than an in-network provider.
Modern: The amount that a health care insurance plan will contribute toward out-of-network services will vary by your insurance company and is often based on a “reasonable and customary” amount that the service should cost
Example: If you go to an out-of-network dentist and are billed $300 for the service, your insurance company may contribute $200 toward paying this cost because $200 is the amount it has decided is “reasonable and customary” for this service. When out-of-network, any remaining cost above this amount ($100 in this case) may have to be fully covered by the person receiving care. When out-of-network, the usual coinsurance rates that apply in-network may not apply out-of-network. Additionally, out-of-network service costs may not count toward an annual deductible.
According to Medical Economics, there were 10 clinic and physician practices filing bankruptcy in 2024, making it the highest level of the last six years, according to a new analysis of cases with liabilities of at least $10 million.
Meanwhile, the Steward Health Care System bankruptcy, which was based in Massachusetts but making headlines across the nation, has become “the largest hospital sector bankruptcy by far in the last 30 years,” according to a new analysis by Gibbins Advisors, based in Nashville, Tennessee.
Health care bankruptcy filings totaled 57 last year, down from 79 in 2023, said “Healthcare Restructuring: Trends and Outlook.” The report analyzed Chapter 11 health care bankruptcy cases with liabilities of at least $10 million, since 2019.
Last year’s total was down 28% from 2023’s peak, but greater than the 2019 to 2022 average of 42 filings a year, the report said.
Bankruptcy, often considered a last financial resort, is a legal process that can help alleviate outstanding debts for individuals and businesses. Reasons to file for bankruptcy can include divorce, job loss, exorbitant medical bills or credit card debt.
There are several types of bankruptcy — six, as a matter of fact. The two most common types of bankruptcy for individuals are Chapter 7 and Chapter 13.
But there are four other types as well: Chapter 9, Chapter 11, Chapter 12 and Chapter 15. And, the type of bankruptcy filed depends on the situation.
Regardless of which type, the process is typically the same: You’ll usually retain an attorney and make your case before a judge, who will then erase some debts or set up a repayment plan.
Also note that an eligibility requirement — for all bankruptcy chapters — is that you must undergo credit counseling within the 180 days before filing.