BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on July 28, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Markets: Stocks soared yesterday after the Fed said it was hiking interest rates by 75 basis points (its fourth rate hike this year) in order to stamp out inflation. Another rate increase could be on its way this fall, Fed Chair Jerome Powell said, depending on the economic data. Powell also rejected claims that the US was currently in a recession.
The DJIA rallied 400 points as Powell hinted the Fed could slow the pace of rate hikes, and the NASDAQ jumped 4%.
Prices for goods in the U.S. are expected to continue rising through 2023. The Federal Reserve [FOMC] waited too long to respond to early signals of inflation. The central bank is correcting the course by raising its interest rate targets at the fastest pace in more than two decades.
Meta, the company formerly known as Facebook, reported a 1 percent decline in quarterly revenue from the previous year. It was the first time the social media giant’s revenue had fallen since it went public a decade ago, as it confronts increased regulatory scrutiny and a turbulent economy while trying to build a new frontier of digital communication.
Posted on July 28, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Eric Bricker MD
Healthcare Stock and IPO Investing Can Be Confusing. The Story of Privia Health is a Good Case Study in Understanding the Underlying Economics in Healthcare Investing:
Posted on July 23, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
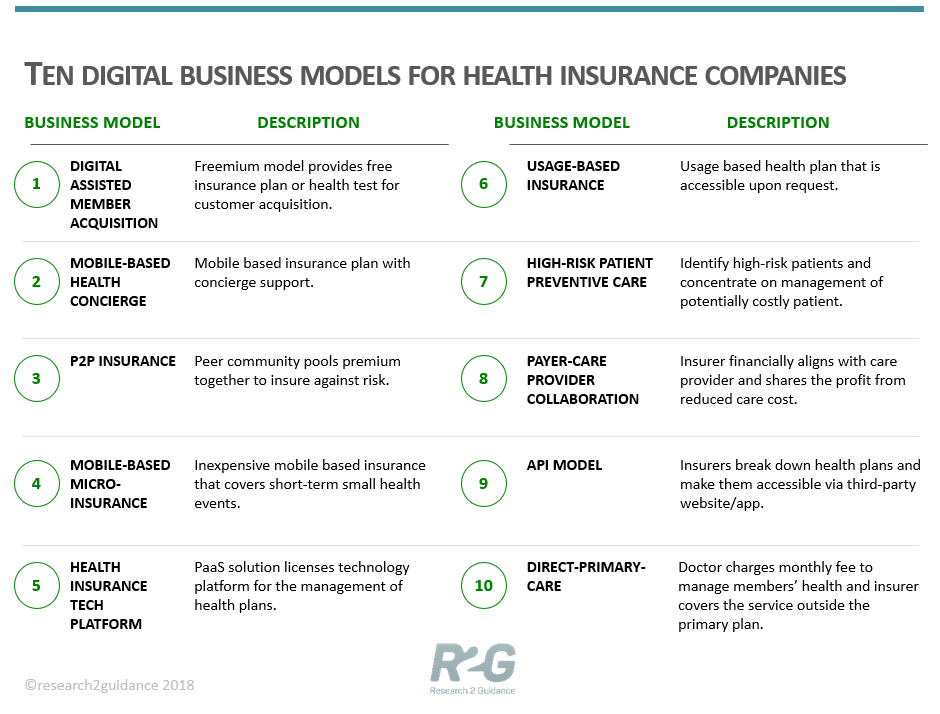
The Top 10 [Ten] Disruptive Digital Business Models For Health Insurers
By Zhang Jie
Digital technologies will transform the health insurance business. Early adopters have started to implement new digital business models with initial success. A new report describes ten digital business models for health insurers that will disrupt the industry.
Advances in higher-quality digital technology—especially apps, sensors, and artificial intelligence (AI)—along with their proliferation among members have spurred the emergence of new business models.
The new report “The 10 Disruptive Digital Business Models for Health Insurers” published by Research2Guidance describes how start-ups, health insurance and general payer organizations have started using these technologies to venture into new forms of health insurance offerings and increasingly step into the healthcare provider role.
New digital models change the way the insurers interact with patients. For example, digital insurers have reworked the trust equation with the patient, outsourced much of their value chain to their members, and now know much more about them. Digital business models tend to also blur the lines between payer and care giver organizations. Some of the first-movers already crossed the line and started to offer services which have previously been provided exclusively by doctors and nurses. The ten digital business models are defined as follows:
Digitally assisted member acquisition is a freemium business model concept.
Mobile health concierge is a business approach designed for members to complete all health insurance tasks using mobile phones with the support from a concierge team.
Peer-to-peer (P2P) insurance refers to a risk-sharing community.
Mobile micro-insurance refers to the health insurance plans that cover short-term small health events or minimal ongoing health insurance.
Health insurers tech platforms license their technology for the management of health plans and members to their customers.
On-demand insurance is a usage-based model that enables members to access desired health plans upon request with the help of a mobile app.
High-risk patient preventive care model concentrates on insuring and managing potentially costly patient groups.
The payer & provider collaboration model stands for a closer, digitally enabled partnership between payers and care providers, especially hospitals.
The API health insurance model uses a list of pre-defined health insurance products accessible to websites and app providers via an application programming interface (API).
Direct primary care model. Within this model, a care provider or a hospital act like a health insurance company using a monthly subscription model.
First implementations of these models indicate the positive impact that they have on the company evaluation, the ability to attract new members, the cost structure, and new revenue streams. Currently, the main impact of digital business models is on company evaluation, which reflects the hype that some companies have created in the investor community. Companies like Oscar, Clover Health, and Bright Health are valued at over $1 billion USD each after only a few years of operation.
Health insurers and start-ups from the USA and China are the most aggressive in adopting new digital business models. Companies from other regions tend to choose a follower approach or implement copycats.
ASSESSMENT
The report also profiles first-mover digital implementations. Profiles include their target groups, operating models, service offerings, and early evidence for success where available.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
Posted on July 20, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Health Capital Consultants, LLC
***
***
Biden Administration to Overhaul Vertical Merger Guidelines
The U.S. healthcare industry has seen a rise in vertical integration transactions since the passage of the ACA, especially among physician groups integrating with health systems or insurers, as providers seek to fill gaps in their continuum of care. In response to these trends and resulting market imbalances, the Biden Administration is aggressively pursuing antitrust enforcement by updating and revising U.S. antitrust law guidance.
This Health Capital Topics article will discuss the vertical integration movement and the proposed changes to antitrust laws that may affect the future of healthcare. (Read more…)
Posted on July 16, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
A Real or False Linguistic Conundrum?
By Dr. David E. Marcinko MBA
Heterodox Economics
Heterodox Economics refers to methodologies or schools of economic thought that are considered outside of “mainstream economics”, often represented by expositors as contrasting with or going beyond neoclassical economics. “Heterodox economics” is an umbrella term used to cover various approaches, schools, or traditions.
***
***
Health Economics [not healthcare economics]
***
Health Economics is a branch of economics concerned with issues related to efficiency, effectiveness, value and behavior in the production and consumption of health and healthcare. In broad terms, health economists study the functioning of healthcare systems and health-affecting behaviors such as smoking.
Assessment: So, is health economics now mainstream; or still heterodoxic in 2019? OR, is the definitial conundrum just a matter of linguistics and terms-of-art. Your thoughts are appreciated.
Posted on July 13, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
A Nationwide Database Review
This “Guide to Travel Nursing Jobs” presents data obtained from a nationwide information database of travel nurses including motivational factors in choosing a travel nurse career, age demographics, benefits information, and social media usage.
***
In addition, the guide highlights the salary info for travel RNs as well as a timeline of the travel nursing process.
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
My how things have changed post pandemic. Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on July 12, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
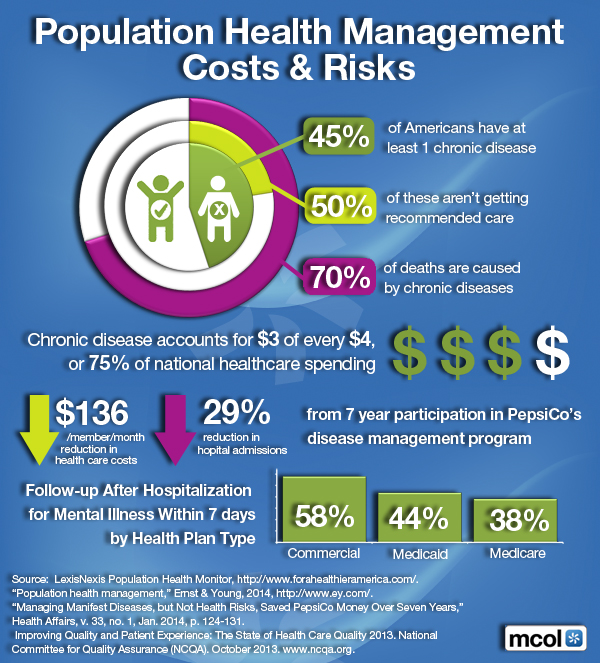
Understanding the Costs and Risks
[By Dr. David Edward Marcinko MBA]
Gratefully, our book, Financial Management Strategies of Hospitals and Healthcare Organizations [Tools, Techniques, Case Studies and Checklists] has become an academic best seller.
It contains a chapter on Wellness andPopulation Health 2.0; included here for your review [By Jennifer Tomasik, Carey Huntington, and Fabian Poliak]. .
I am especially proud of this work. This managerial book mimics the popular style of colleague Atul Gawande MD in his acclaimed work The Checklist Manifesto.
Why? All hospitals are still subject to the imperative: No Margin – No Mission.
***
***
Assessment
In an example of population health management and policy leadership, another colleague, David B. Nash MD MBA of the Wharton School, and Endowed Dean of Jefferson University Medical School [father of population health], even wrote the “Foreword”.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on July 12, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
PROFESSIONAL Human Resources Options
By Eric Galtress
“In-house service and support activities are monopolies. They have little incentive to improve productivity. In fact, they have considerable disincentive to improve their productivity. Clerical, maintenance and support work, do not make a direct and measurable contribution to the bottom line.”
“Sell the Mailroom” by Peter F. Drucker
***
Labor Law
Labor Law compliance begins with the hire of your very first employee, thus a well managed human resources (HR) function should be an area of strategic focus by the medical executive, regardless of practice size or the number of employees. Consideration of this vital role can help contribute to an efficient, highly effective and productive professional staff committed to the goals of the practice encompassing a positive and nurturing culture evident to your patients, while maintaining your competitive edge.
HR
Human Resources are the major expense driver of today’s medical practice and addresses staffing requirements, wages and other compensation, payroll and tax compliance, labor law compliance, employee benefits, training, employee turnover, safety, risk management and workers’ compensation. These responsibilities must be performed in accordance with State and Federal guidelines, beginning with the hire of your very first employee.
At specific employee level thresholds, employers are required to comply with a growing number of employee-related requirements including State and Federal Laws. These laws govern the proper method of how employees must be treated and paid, as well as ensuring that their rights in the workplace are protected. State and Federal Regulators each create vast amounts of workplace legislation every year, many of which become law.
In most cases, the specific requirement (either State or Federal) that affords the employee the most workplace rights and/or protection and benefits takes precedence over the other. Non-compliance can subject the practitioner/business owner to hefty fines, penalties, business interruption, litigation, and in some cases, even practice failure.
Moreover, these HR efforts are backed by labor attorneys, service providers, brokers and other consultants. Given the typical size of a medical practice, this presents a compelling argument that practices should consider taking advantage of an innovative alternative: being able to delegate (outsource) part or most of the HR burden as well as the employee / employerrelated liabilities.
Outsourcing
Simply put, instead of the practitioner/staff performing the HR requirements, part or most of this responsibility can be outsourced to an off-site HR services provider that specializes in labor law compliance, employee management and cost control. The practitioner retains functional control of the employees and the service provider handles the HR issues.
Added value is achieved by the practice in receiving these services more cost effectively since their needs are combined with those of the many other practices and businesses the provider already serves. Outsourcing is a matter of simple economics, enabling the practitioner to gain relief from cumbersome employee administration, while enhancing productivity and benefits for the staff members.
The HR outsourcing relationship is not to be confused with a Physician Practice Management Company (PPMC). The HR services provider has no financial interest or ownership whatsoever in the practice.
***
***
DEFINITIONS
To have an outside firm take responsibility and much of the liability to perform activities traditionally handled by internal staff and resources because:
They can do it cheaper and/or faster.
They can do it better because of their expertise and experience.
They have all of the required professional staff and/or facilities.
They take all or part of the risk and the liability to do it right.
They can expand their service offering commensurate with your growth needs
They save you the time of doing it yourself or having one or more of your key staff members distracted from the priorities of the practice.
They help safeguard against chaos should the key person handling HR suddenly leave
They help maintain the high standards of the practice with regard to the employees and the workplace.
Outsourcing can benefit all parties.
Human resource management
In general, HR management consists of the activities, responsibilities and issues of any practice/business, corporation, partnership or other business entity that comes as a result of having employees (IRS1099 independent contractors are not considered employees).
Some of these requirements are mandatory such as paying minimum wage and providing workers’ compensation insurance protection; other aspects and their related administrative functions can be at the discretion of the owner(s) of the practice or business such as sponsoring health benefits, retirement plans for their employees or paid vacation and sick time.
Employer POV
What follows is an overview of the HR requirements of being the employer. This includes a condensed view of employment and labor laws, government compliance issues, employee related costs and the alarming upsurge in employee litigation. The last poses a growing level of liability, vulnerability and distraction to today’s medical executive and practitioner/owner, second only to that of medical malpractice.
Assessment
As a result, many physicians without available HR expertise are finding it increasingly difficult to focus on growing their practices.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on July 11, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
A Very Brief Review
By Dr. Mark Matthews with Dr. David Marcinko MBA
As most medical and healthcare executives and consultants are aware, there are a few tools and techniques that are unique to the world of Lean process improvement and management.
These include: Kaizen Events, The 5-S Technique, Standard Work, Visual Controls and Human Factors Engineering.
We will review the first two techniques in this ME-P. Of course, the last three are reviewed in much greater detail in our new book complete with checklists, figures, tables, drawings, graphs and other illustrations.
Kaizen Events
Kaizen is one of the most powerful tools in the Lean methodology. These events involve intense work sessions aimed at making concrete decisions in a short time period without the need for much data collection. Kaizen events are fairly narrow in scope, ideally concentrating on making one or two decisions at the most.
For example, there may be competing improvement ideas that require more exploration. Using a Kaizen event can provide the necessary structure to make the decision needed to move forward with implementation. The steps in a typical Kaizen Event often include:
Determine and define the objectives
Determine the current state of the process
Determine the requirements of the process
Create a plan for implementation
Implement the improvements
Check the effectiveness of the improvements
Document and standardize the improved process
Continue the cycle
The 5-S Technique
This technique was developed to allow employees to visually control their work area around visual management techniques. The principles involved in visual management include:
Improving workspace efficiency and productivity
Helping people share workstations by providing standard layouts
Reducing the time required to look for needed supplies or tools
Improving the work environment
Each “S” in 5S stands for a step in the process:
Sort – classify every item in the designated area as either needed or not needed
Set (Straighten) – put “everything in its place”
Shine (Sweep) – clean all work environments for order and organization
Standardize – document what goes where, who will clean and who will inspect and on what schedule
Sustain-design a system for monitoring process, providing feedback, and rewarding good outcomes
Assessment
Prior to conducting a 5S event, a significant amount of planning is vital. It is important to scope the target area as something that is manageable, draw a physical map of the area under consideration [hospital, ED, OR, clinic, office, etc], and assemble a list of current items in that area. This is usually accomplished by taking photographs (both before and after) of the area.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, urls and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on June 28, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Writers
***
***
Venture capitalists who are in a rut should stop talking about how hard it is to raise a $100 million fund. Instead, raise a $5 million fund.
Rather, they should stop trying to invest $5 million at a time (with an 18-month window before going public). A better strategy is to start doing smaller investments with longer time horizons.
Posted on June 17, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Dr. Anthony Fauci, the leader of the U.S. government’s Covid pandemic response effort tested positive for the coronavirus. Fauci, who is fully vaccinated against Covid, is experiencing mild symptoms. “Dr. Fauci will isolate and continue to work from home,” a statement said. “He has not recently been in close contact with President [Joe] Biden or other senior government officials.”
The yen fell after Japan’s central bank kept its ultra-low interest rates on hold even as policy makers around the world hike cost of borrowing to tackle rising prices. The Bank of Japan (BOJ) also says it will continue its program of buying huge amounts of government bonds. This week central banks in the US, UK and Switzerland raised interest rates as they try to curb inflation. After the announcement, the US dollar climbed to 134.64 yen, not far from the 24-year peak of 135.6 earlier this week. So far this year the dollar has climbed by 15% against the yen, as the gap between interest rates in Japan and much of the rest of the world continues to grow.
Markets: Stocks took a big tumble over recession concerns, and blue-chip companies such as Home Depot, Intel, Walgreens, and JPMorgan touched 52-week lows.
Global economy: European central banks including the Bank of England, the Swiss National Bank, and the National Bank of Hungary increased interest rates yesterday to tame inflation.
Posted on June 9, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Global venture capital investment was a healthy $39 billion in May, according to Crunchbase. But, the figure declined for the second month in a row, reaching the lowest point since December 2020. In monthly terms, VC investments declined by nearly 16%. In yearly terms, it fell by 20%.
Nobel laureate and economist Robert Shiller said the US has a good chance of entering a recession. He told Bloomberg the odds of a recession in the next few years are 50%, which is “much higher than normal.” Shiller predicted in 2005 that the housing bubble would burst and also warned a new one may be forming. And, Ray Dalio said the FMOC will cut interest rates to combat stagflation in a recent Market Insider interview. “We are in a tighttening mode … the pain of that will become great.”
Additionally, former EY Global Chairman and CEO Mark Weinberger warned that inflation will not go down in the near future, causing the economy to “turn for the worse.”
Gemini, a crypto exchange and custodian founded by Cameron and Tyler Winklevoss faced a loss in February in the form of a $36 million breach. And now the company is being sued over its alleged failure to protect its customers.
The Stock Markets have been a bit dull recently. The S&P 500 has been directionless trading within a roughly 100-point range for the past two weeks. The only energy in the market seems to belong to Exxon Mobil which notched a record close; first since 2014.
Posted on May 20, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
ArkInvestment Management’s Cathie Wood says “exploding” inventories at major retailers like Walmart Inc. and Target Corp. paired with declining US consumer sentiment portend slower inflation on the horizon. The money manager was responding on Thursday to a tweet quoting world’s richest man Elon Musk saying the recent inflation surge was due to government pandemic stimulus, even as money velocity held constant.
Home sales slowed for the third consecutive month in April as mortgage rates surged, driving up borrowing costs for would-be buyers as home prices soared to new highs. Existing home sales fell 2.4% last month from March to a seasonally adjusted annual rate of 5.61 million, the National Association of Realtors said Thursday.
And, in April, the median U.S.rent hit a record high for the 14th month in a row of $1,827, according to Realtor.com, a residential real estate information service. “If recent trends continue, we expect the typical U.S. asking rent to eclipse $2,000 by August,” it said. April rent increased 16.7% from a year earlier. That’s the third straight month in which year-over-year rent growth has dipped, down from 17.1% in January. Higher rents are taking money away from renters’ budgets for regular expenses and savings, Realtor.com said. Rent represents the biggest strain on renters’ overall finances, according to a Realtor.com survey.
Incidentally, a number of American corporate giants, including Walmart, Target, Bank of America, Charles Schwab, and Intel, hit 52-week lows yesterday.
Posted on May 19, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
Target Corp. is on pace for its worst stock drop since 1987’s Black Monday crash after becoming the second big retailer in two days to trim its profit forecast. A surge in costs during the first quarter shows little sign of easing, said Chief Executive Officer Brian Cornell. Operating profit will amount to only about 6% of sales this year, 2 percentage points below the previous forecast, Target said Wednesday. And the company’s first-quarter adjusted profit missed the lowest of 23 analyst estimates compiled by Bloomberg.
Netflix continues to hemorrhage subscribers, as the streaming service laid off 150 more employees representing 2% of its workforce. In a statement, a company rep clarified “the changes are primarily driven by business needs rather than individual performance.”
***
***
And, socks plunged as deepening concern about the economic impact of high inflation and rising interest rates drove the Dow Jones Industrial Average to its worst day since March 2020.
The Dow closed with a loss of 1,161 points, dropping 3.6 percent Wednesday for its steepest one-day drop since the onset of the coronavirus pandemic. The S&P 500 closed 4 percent lower and the NASDAQ closed 4.7 percent lower Wednesday.
A failure by the CBOE Volatility Index [VIX] sometimes referred to as Wall Street’s fear gauge, to push above the mid-30 range was seen as one sign that investors hadn’t made the sort of “capitulation” that often clears the way for a sustained rebound. However, some positive market internals on the upside during Friday’s and Tuesday’s bounce have some analysts looking for some near-term upside, which could continue to confound market bears.
More Americans were considered “equity rich” in the first quarter of 2022 — meaning that they owed no more than 50% of their home’s total value — amid a rise in home prices, according to new data from ATTOM Data Solutions. The number of equity-rich homeowners grew to 44.9% of mortgage holders in the first quarter, up from 41.9% in the fourth quarter of 2021 and 31.9% in the first quarter of 2021, according to the company’s first-quarter 2022 U.S. Home Equity and Underwater Report.
Finally, Litecoin (LTC-USD) is getting ready for its newest upgrade on Thursday, May 19th. The MimbleWimble (MWEB) upgrade will turn the Litecoin crypto into a more fungible, private currency. Privacy coins like Monero (XMR-USD) and Zcash (ZEC-USD) have been hot investments in recent weeks
Posted on May 10, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Altered and Poorly Written Rx for Vicodin
By Dr. David Edward Marcinko MBA
***
***
Poorly-written Rx for vicodin
Drug: Rx Vicodin
Disp: # 10
Sig: Take I, as needed for pain.
Refills: 1 2 3 4 or 5
AM2685591
David Edward Marcinko, MBBS DPMMBA
The patient abuser may change drug quantity numbers, copy or remember the doctors’ DEA number, or take extra Rx pads. For this reason, a physician’s Rx pad should contain his/her name, address and telephone number. The doctor’s DEA number should not be pre-printed on the pad, for fear of mis-use.
Example:
Increase the quantity 10, to 100, by adding a zero, so that the additional capsules can be used, sold or bartered with on the street.
Change the directions to take 2 capsules, rather than 1 in order to produce greater euphoria.
Increase the Rx refills, from one to two, by extending the underline, or checking an additional quantity box.
Pre-printed DEA number can be stolen, sold or reused.
Pre-printed (not original) physician signature can be reproduced and widely distributed for more prescriptions.
Altered Rx for vicodin
Drug: Rx Vicodin
Disp: # 100
Sig: Take II, as needed for pain.
Refills: 1 2 3 4 or 5
AM2675591
David Edward Marcinko, MDBBS DPM MBA
The doctor drug addict, or a doc in need of funds, may write for more narcotic agent than needed, and receive the additional pills back from the patient-shill for personal consumption, sell them on the street himself for money, or receive a monetary kickback from the patient-shill.
A pharmacist may also indirectly alter a prescription using the above methods, or simply short-change the patient with fewer narcotic capsules than the prescription intends. This is more difficult to do with pills or tablets in the out patient setting, but easy to do in the in-patient setting when liquid IV drugs are used, by dilution and placing less than the full amount in IV bottles or bags. The harm to patients, of course, may be fatal.
Well-written Rx for vicodin
Drug: Rx Vicodin
Disp: # 10 (ten) capsules
Sig: Take one or two capsules, po, prn pain.
Refills: 1 2 3 4 or 5
AM2685591
David Edward Marcinko, MBBS DPM MBA
Example:
Drug quantity can-not be changed.
Directions can-not be changed. Route of administration (by mouth) indicated.
Rx refills clearly indicated.
Handwritten, not pre-printed, DEA number.
Original physician signature, only.
Doctor Rx prescription abuse foibles are legendary in the DEA and include a Maryland podiatrist who wrote prescriptions for more than 1,235 Mepergan Fortis capsules ostensibly for his wife following minor foot surgery. Or, the Florida physician who prescribed more than 2,150 Vicodin capsules for a patient with whom he was having an extra-marital affair in order that his consort not disclose the fling to his wife. Or, the osteopath from New Jersey who wrote more than 100 narcotic prescriptions every 8 hour day, for more than a year, to any patient standing in a line in front of his office. And, finally the California dentist whose excuse for writing more than 1,845 narcotic tablet prescriptions in a six month period for the same patient was that they would be needed in his next reincarnation. Yes, all of these incidents are laughable if not for their serious consequences to the involved individuals, and society, alike. The bastards!
Fortunately, unlike drug local domestic drug kingpins or international narco-traffickers who ply their trade virtually undetected, these naive white-collared nerds, always get caught by the Drug Enforcement Agency. Their Rx abuse tactics are so amateurish!
Posted on May 9, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Dr. David Edwarrd Marcinko MBA
Rx DRUG ABUSE
Traditional medicinal agents come in a variety of ways, known as dispensing vehicles. Drugs may be in liquid, pill or inject able form, they may be compounded in capsules, caplets, gelatin tablets, powders or suppositories, or they may come in creams or ointments for the eye, anus and vagina. They may be ingested into the stomach, placed and dissolved under the tongue, put into the eyes, popped, injected or smeared and transported through the human skin from patches.
A valid drug prescription is a written order, by a doctor, to a pharmacist. In this country, prescriptions are written by physicians, podiatrists, osteopaths, dentists. and some optometrists, physician assistants and nurse practitioners. In addition to the name of the patient and that of the medical prescriber, the prescription contains the name of the drug (not necessarily a narcotic), its quantity, instructions to the pharmacist, and directions to the patient. Narcotic prescriptions may not be prescribed to a drug addict to prevent withdrawal symptoms, as there must be some other therapeutic purpose for such an order.
The art of medicinal prescription writing, and pharmaceutical compounding, has declined in modern medicine for several reasons. Most drugs are made by pharmaceutical companies, and the role of the pharmacist, in most cases, consists only of compounding and error prevention. Many drugs are even automatically dispensed, and tracked, in the hospital setting with bar coding technology and modern inventory tracking mechanisms. Also, the practice of writing long and complicated prescriptions, containing many active ingredients, adjuvants, correctives, and elegant vehicles, has been abandoned in favor of using pure compounds.
Drugs may be prescribed by their official names, which were first given by the United States Pharmacopeia (USP), in 1920, or by the National Formulary (NF), since 1906. Unofficial or generic names may be used, known as New and Non-Official Drugs (NND) or by the United States Adopted Names (USAN), or by the manufactures trade name. For example, the generic narcotic meperidine or pithidine, is also known by the trade named, demerol. The designation USAN does not imply endorsement by the American Medical Association (AMA) Council on Drugs (CODs), or by the USP.
Of course, there is an advantage and disadvantages to prescribing drugs by their trade name, or generic names. Advantages of generics include economies of scale for both the patient and pharmacist, and although the active ingredient in generics are identical to trade drugs, they are often less expensive since research and development costs are absent, and various binders, colorizing agents, preservatives or dispersing agents are of an inferior quality, and hence cheaper for the patient. Appearance, size and taste issues are common. For the pharmacist, generics are cheaper since a multiplicity of very similar drugs need not be shelved.
***
***
For example, the tablet or capsular form of many drugs contains inactive ingredients, such as: ammonio methacrylate copolymer, hydroxypropyl methylcellulose, lactose, magnesium stearate, povidone, redironoxide, stearyl alcohol, talc, titanium dioxide, triacetin, yellowironoxide, yellowironoxide with FD&C blue No.2 (80 mgstrengthtablet only), FD&C blue No.2 and other ingredients. And yes, I’ve seen an addict do into shock, or die from acute anaphylaxis, after taking drugs containing ingredient he was highly allergic to.
Shock is a life-threatening condition where blood pressure falls too low to sustain life. It occurs when low blood volume (due to severe bleeding, excessive fluid loss or inadequate fluid uptake), inadequate pumping action of the heart or excessive dilation of the blood vessel walls (vasodilation) causes low blood pressure. This in turn results in inadequate blood supply to body cells, which can quickly die or be irreversibly damaged.
Anaphylactic shock is the severest form of allergy that is a medical emergency. It is a Type I reaction according to the Gell and Coombs medical classification, and is often severe and sometimes fatal systemic reaction in a susceptible individual upon exposure to a specific antigen (such as wasp venom or penicillin) following previous sensitization, or drug use. Characterized especially by respiratory symptoms, fainting, itching, itching and swelling of the throat or other mucous membranes and a sudden decline in blood pressure! The victim literally cannot breathe and drowns in its own congested and fluid filled lungs
So, patients in need of routine drugs for acute or chronic conditions like arthritis, high blood pressure, asthma, acne, hay fever, performance enhancing steroids or, so called life style drugs, like Viagra for a limp woody, or hair growth stimulator Rogaine, may get a good deal by going to Canada or Mexico for generics. But for important drugs, like nitroglycerine fro your heart, blood thinner coumadin, birth control pills or various anti-cancer agents, stick with brand names.
The main disadvantage of trade drugs is increased cost, due to R & D, patents, trademarks, marketing and company advertising expenses. Of course, trade drug are first to market, and hence may be beneficial as a new treatment modality, or injurious if significant side affects or other complications arise.
Today, the prime source for drug information is probably the well known, Physicians Desk Reference (PDR). Now, in its 58th edition, the PDR® provides the latest information on prescription, but not illegal street drugs. It is considered the standard reference that can be found in virtually every physician’s office, hospital and pharmacy in the United States. The current edition is over 3,000 pages long, and is where you can find data on more than 4,000 drugs, by brand and generic name, manufacturer and product categories. The PDR also provides usage information and warnings, drug interactions, plus full-size, full-color photos cross-referenced to specific drugs. For the layman, it also includes: phonetic spelling for each listing, a key to controlled substances, adverse reactions and contraindications, pregnancy ratings, dosages and all other FDA-required information. Of course, on the street, or in Mexico, none of this information matters.
Latin abbreviations, sometimes still used by doctors on prescription blanks include:
Rx = take thou (receipe)
po = by mouth (para orbis)
prn = as needed (pro re’nata)
hs = at bed time (hora somnae)
BID = twice daily
TID = three times daily
QID = four times daily
M = Mix
Traditionally, a medical prescription is written in a certain order, well known to drug abusers, and DEA agents, and consist of six basic parts:
Superscription: This is the Rx, or recipe. In Latin it means take thou.
Inscription: Represents the ingredients and amounts.
Subscription: Represent the description for drug dispensing, and may be represented by the letter M, for mix.
Signature: Often abbreviated as Sig, and contains the directions for patient use.
Refill Status: Indicates the number of refills allowed.
DEA Number: This is nine-character alpha-numeric sequence, used by all licensed physicians who prescribe narcotic agents. An example is AM2685591. The second letter is the first letter of the doctor’s last name, (ie, Marcinko) and the first two digits add up to the third (ie, 2+6=8).
Finally, in addition to the basic parts of a prescription, it should have the patient’s name, and physician signature written in ink, followed by degree designation, such as MD, DPM, DO or DDS, etc.
***
***
Perhaps the most egregious narcotic prescribing habits recently encountered by DEA agents have been by doctors of all degrees and medical designations. Reasons are generally two-fold. First, the doctor may become a drug addict himself, either by accident or through initial legitimate therapeutic use, and over-prescribe the narcotics. Or, increasing office costs, and decreased reimbursement fee reductions of many managed medical care have so economically destabilized the medical community, that economically impoverished doctors desperately sell prescriptions to finance their personal lifestyles, automobiles, clothes, fancy vacations or own addictions.
For example, a staggering medical student loan debt burden of $100,000-$250,000 is not unusual for new practitioners. In fact, the federal Health Education Assistance Loan (HEAL) program reported that for the Year 2001, it squeezed significant repayment settlements from its Top 5 list of deadbeat doctor debtors. This included a $303,000 settlement from a New York dentist, $186,000 from a Florida osteopath, $158,000 from a New Jersey podiatrist, $128,000 from a Virginia podiatrist, and $120 from a Virginia dentist. The agency also excluded 303 practitioners from Medicare, Medicaid and other federal healthcare programs and had their cases referred for non-payment of debt.
These facts indicate that the current healthcare reimbursement climate has caused more pain and tumult to doctors than the pubic realizes. Older medical practitioners are retiring prematurely, mature providers are frustrated and in despair, and young physicians have no concept of the economic servitude to which they are about to be subjected. Frustration is high and physician suicides have been documented. Many doctors get divorced at the start of their careers. Even the U.S. Inspector General has declared healthcare providers to be public enemy #2,behind international narco-traffickers, for their federal drug, fraud and abuse initiatives. Still, the statistic above lends itself to narcotic drug prescription abuse, either on the part of the doctor or patient, since only these two parties that can directly alter a prescription for illicit drug use, as illustrated by this poorly written prescription for a narcotic pain killer, vicodin.
During this period, the standard deviation of quarterly real gross domestic product (GDP) declined by half and the standard deviation of inflation declined by two-thirds, according to figures reported by former U.S. Federal Reserve Chair Ben Bernanke. The Great Moderation can be summed up as a multi-decade period of low inflation and positive economic growth.
But, what about health economics, writ large? And, the actual practice of medicine by physicians in the trenches. Consider this historical review.
GOLDEN AGE OF MEDICINE
The ‘golden age of medicine’ – the first half of the 20th century, reaching its zenith with Jonas Salk’s 1955 polio vaccine – was a time of profound advances in surgical techniques, immunization, drug discovery, and the control of infectious disease; however, when the burden of disease shifted to lifestyle-driven, chronic, non-communicable diseases, the golden era slipped away. Although modifiable lifestyle practices now account for some 80% of premature mortality, medicine remains loathe to embrace lifestyle interventions as medicine Here, we argue that a 21st century golden age of medicine can be realized; the path to this era requires a transformation of medical school recruitment and training in ways that prioritize a broad view of lifestyle medicine. Moving beyond the basic principles of modifiable lifestyle practices as therapeutic interventions, each person/community should be viewed as a biological manifestation of accumulated experiences (and choices) made within the dynamic social, political, economic and cultural ecosystems that comprise their total life history. This requires an understanding that powerful forces operate within these ecosystems; marketing and neoliberal forces push an exclusive ‘personal responsibility’ view of health – blaming the individual, and deflecting from the large-scale influences that maintain health inequalities and threaten planetary health. The latter term denotes the interconnections between the sustainable vitality of person and place at all scales. We emphasize that barriers to planetary health and the clinical application of lifestyle medicine – including authoritarianism and social dominance orientation – are maintaining an unhealthy status quo.
To listen to all those desperate to reform health care, you get the impression that physicians are pretty horrible people. We are all sexist, greedy, money grubbing tyrants who will perform unnecessary tests and procedures just to make money. We don’t care about quality or cost. We are killing off 250,000 patients every year with our ignored “errors.”
We purposely keep our patients in pain, or we addict them to narcotics just to shut them up. We are constantly told by lawyers that lawsuits are necessary to protect patients from doctors. We provide unsafe drugs just because the drug reps give us free pens and coffee cups. The government must step in to clean up the mess.
On April 5, 2022, the Internal Revenue Service (IRS) proposed a rule change to its eligibility requirements for families to receive premium tax credits toward purchasing high-quality health coverage on the insurance marketplaces established by the Patient Protection and Affordable Care Act (ACA). This proposed change comes on the heels of two Biden Administration executive orders calling for improvements to the ACA and Medicaid. This Health Capital Topics article will discuss the proposed solution to a decade-long problem and how it will affect millions of Americans. (Read more…)
Posted on April 28, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Markets: The NASDAQ stayed flat at its lowest level this year.Spotify shares sank to a record low. Facebook is having a rough go, but it’s not the only one. Netflix stock plunged nearly 70% this year after hitting a ceiling on subscriber growth. At one point, it was worth more than Disney; now, it’s not even half as valuable. Even Google is googling “ways to make more money.” Its parent company, Alphabet, reported a slowdown in growth last quarter because, like Facebook, YouTube’s also being been dinged by TikTok and Apple’s privacy changes: The video platform’s revenue came in more than $500 million below expectations.
Energy: Russia’s halted oil shipments to Poland and Bulgaria yesterday.
Posted on April 22, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
April 22nd, 2022
***
By Dr. David Edward Marcinko MBA
Founding Editor-in-Chief
Go Green!
At this Medical Executive-Post, we are trying to go GREEN! Our green mindset permeates brightly whenever we conduct business. However, green is more than just a color, it’s a way of working and living that honors our environment and helps preserve it for future generations. And so, below is a list of our environment-friendly green initiatives.
***
Initiatives
We have the ability to remotely monitor our phone and internet systems. Not only is this a cost savings for our colleagues, members, visitors, customers and us, it reduces fuel usage by keeping third-party vendor delivery service fleets off the road.
Inbound technicians have an 85% first-call resolution rate. Our folks ask the right questions and take the time to solve issues without scheduling an in-person or vendor service call.
We telephone re-use jacks and cables, when possible.
We recycle all paper, plastic and glass in our office.
We use an eFax service, cutting down on paper usage.
We have a paperless billing system.
We have a virtual library of “how to” resources for all of our ME-P products and services.
We sent our old phone systems to a re-cycler who uses the parts for plastic.
Posted on April 17, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Russia: Shut its stock market all week in a bid to curb panic-selling after the invasion of Ukraine. The ruble cratered to trade below 1 cent as Western sanctions effectively weaponized the financial system.
Posted on April 14, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
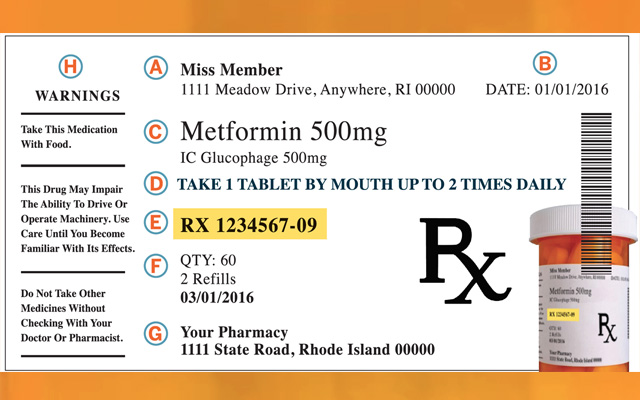
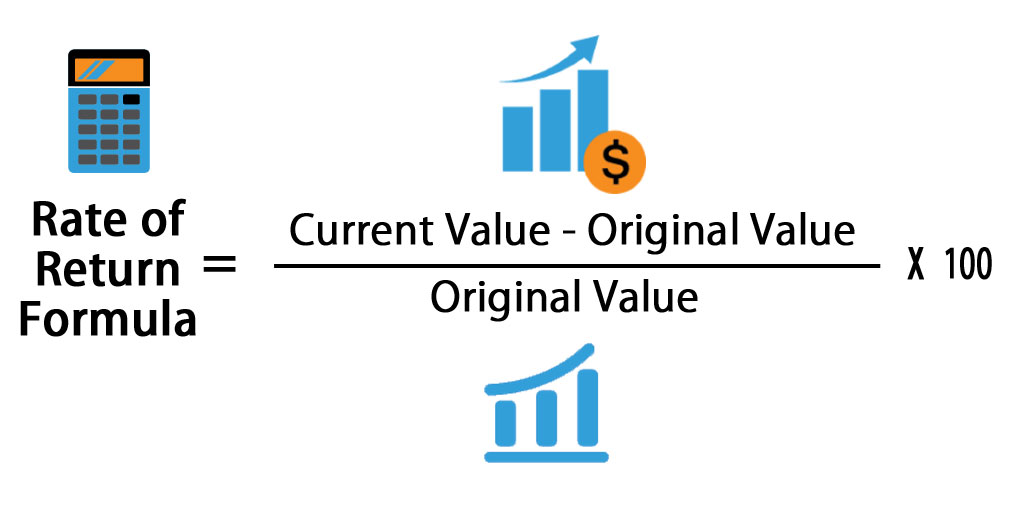
DEFINITION: A rate of return (RoR) is the net gain or loss of an investment over a specified time period, expressed as a percentage of the investment’s initial cost. When calculating the rate of return, you are determining the percentage change from the beginning of the period until the end.
***
And so, according to Greg McBride CFA, before you invest your money, you’re likely wondering how much you’re going to earn. This is known as the rate of return. The rate of return is expressed as a percentage of the total amount you invested. If you invest $1,000 and get back your original investment plus an additional $100 in interest, you’ve earned a 10 percent return.
However, numbers don’t always tell the full story. You’ll also need to think about how long you plan to keep the money invested, how your investment options have performed historically and how inflation will impact your bottom line.
Key return on investment statistics
When you’re trying to get the best return on your investment, you’ll likely start combing through loads of data. A good place to start is looking at the past decade of returns on some of the most common investments:
As our private iMBA Inc clients, ME-P subscribers, textbook and dictionary purchasers, seminar attendees and most ME-P readers know, Ken Arrow is my favorite economist. Why?
About Kenneth J. Arrow, PhD
Well, in 1972, Nobel Laureate Kenneth J. Arrow, PhD shocked Academe’ by identifying health economics as a separate and distinct field. Yet, the seemingly disparate insurance, asset allocation, econometric, statistical and portfolio management principles that he studied have been transparent to most financial professionals and wealth management advisors for years; at least until now.
Nevertheless, to informed cognoscenti, they served as predecessors to the modern healthcare advisory era. In 2004, Arrow was selected as one of eight recipients of the National Medal of Science for his innovative views. And, we envisioned the ME-P at that time to present these increasingly integrated topics to our audience.
Healthcare Economics Today
Today – as 2022 passes – savvy medical professionals, management consultants and financial advisors are realizing that the healthcare industrial complex is in flux; along with the Russian war, domestic inflation and this dynamic may be reflected in the overall flagging economy.
Like many laymen seeking employment, for example, physicians are frantically searching for new ways to improve office revenues and grow personal assets, because of the economic dislocation that is Managed Care, Medi Care and Obama Care [ACA], the depressed business cycle, etc.
Moreover, the largest transfer of wealth in US history is – or was – taking place as our lay elders and mature doctors sell their practices or inherit parents’ estates. Increasingly, the artificial academic boundary between the traditional domestic economy, financial planning and contemporaneous medical practice management is blurring.
I’m Not a Cassandra
Yet, I am no gloom and doom Cassandra like I have been accused, of late. I am not cut from the same cloth as a Jason Zweig, Jeremy Grantham or Nouriel Roubini PhD, for example.
However, I do subscribe to the philosophy of Hope for the Best – Plan for the Worst.
And so dear colleagues, I ask you, “Are the latest swings in the economic, healthcare and financial headlines making you wonder when it will ever stop?”
The short answer is: “It will never stop” because what’s been happening isn’t any “new normal”; it’s just the old normal playing out before a new audience; sans the war.
What audience?
The next-generation of investors, FAs, management consultants and the medical professionals of Health 2.0.
How do I know all this?
History tells me so! Just read this work, and opine otherwise, or reach a different conclusion.
Evidence from the American Financial Scene, circa 1861-1935
The work was created by L. Merle Hostetler in 1936, while he was at Cleveland College of Western Reserve University (now known as Case Western Reserve University). I learned of him while in B-School, back in the day.
At some point after it was printed, he added the years 1936-1938. Mr. Hostetler became a Financial Economist at the Federal Reserve Bank of Cleveland in 1943. In 1953 he was made Director of Research. He resigned from the Bank in 1962 to work for Union Commerce Bank in Cleveland. He died in 1990.
The volume appears to be self published and consists of a chart, approximately 85′ long, fan-folded into 40 pages with additional years attached to the last page. It also includes a “topical index” to the chart and some questions of technical interest which can be answered by the chart.
And so, as with Sir John Templeton’s [whose son is an MD] four most dangerous words in investing (It’s different this time), Hostetler effectively illustrates that it wasn’t so different in his era, and maybe—just maybe—it isn’t so different today for all these conjoined fields.
Conclusion
Your thoughts and comments on this ME-P are appreciated. While not exactly a “sacred cow,” there is a current theory that investors will experience higher volatility and lower global returns for the foreseeable future.
In fact, it has gained widespread acceptance, from the above noted Cassandra’s and others, as problems in Europe persist and threats of a double-dip recession loom. But, how true is this notion; really?
Is Hostetler correct, or not; and why?
Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on March 8, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
BY JONATHAN MASER.N.
***
***
Being an entrepreneur is not necessarily easy, and many people that try to become entrepreneurs wind up failing. It’s important to recognize the risk of failure before you decide to walk down this path. Being an entrepreneur is very rewarding, and you can find success if you can do things right.
Keep reading to learn about common entrepreneurial mistakes that you can avoid to give yourself a better chance of realizing your entrepreneurial goals.
Posted on March 4, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
Stocks fell and oil prices eased back after another bumpy day of trading on Wall Street as markets remained anxious about the broader impact of Russia’s invasion of Ukraine.
Okta shares were down 8.06% while Snowflake plummeted 15.37%.
***
INTEL: Intel stock (NASDAQ: INTC) fell 2.5% after Morgan Stanley and Bank of America Securities cut their targets to $47, according to StreetInsider. The stock fell to a low of $47.62, not far from its 52-week low of $43.63. Morgan Stanley (NYSE:MS) analyst Joseph Moore also downgraded the stock to underweight from equal weight while BofA’s Vivek Arya maintained his under perform rating.
INDEXES: Major indexes veered up and down for much of the day before a late-day slide pushed them into the red. The S&P 500 shed a 0.7% gain to close 0.5% lower, while the Dow Jones Industrial Average fell 0.3%. The NASDAQ composite fell 1.6%, weighed down by technology stocks, which accounted for a big share of the market’s decline.
The Dow is down 0.9% for the week, on track for its fourth negative week in a row. The S&P 500 is down about 0.5% for the week, while the NASDAQ Composite is down more than 1%.
BUYBACKS: In the third quarter of 2021, Apple, Inc. (NASDAQ: AAPL) led all S&P 500 companies with $20.4 billion in buybacks. Alphabet, Inc. (NASDAQ: GOOG) (NASDAQ: GOOGL) was a distant second with $15 billion in buybacks, followed by Meta Platforms Inc (NASDAQ: FB) with $12.6 billion.
Over the last decade, no company has come close to Apple in the buyback department. Apple has bought back $487.6 billion in stock since 2012. Microsoft Corporation (NASDAQ: MSFT) is a very distant second with $147.1 billion in buybacks, followed by JPMorgan Chase & Co (NYSE: JPM) with $146.2 billion.
Why Buybacks Matter: It should come as no surprise to investors that all three of the stocks that have been most aggressive in buying back shares over the last 10 years have outperformed the SPDR S&P 500 ETF (NYSE: SPY) total return by a wide margin in that period.
BONDS: Bond yields were mostly steady. The yield on the 10-year Treasury slipped to 1.85% from 1.86% late Wednesday.
When trying to decide whether to buy a used car or a new one, it’s typically financially wiser to buy used. But if you want to buy new, you should plan to drive the car for 10 years or more.
Better yet – do not buy a new vehicle.
***
The 20/4/10 rule for buying a vehicle
If you have to borrow when buying a car, to avoid spending more than you can afford you should put down at least 20%, keep the loan limited to no more than four years (to avoid interest), and spend no more than 10% of your gross income on transportation costs (which includes the car payment, parking, gas, and insurance).
Book Dr. David E. Marcinko MBA MBBSfor your Next Medical, Pharma or Financial Services Seminar orPersonal and Corporate Coaching Sessions
Dr. Marcinko enjoys personal coaching and public speaking and gives as many talks each year as possible, at a variety of medical society and financial services conferences around the country and world.
These include lectures and visiting professorships at major academic centers, keynote lectures for hospitals, economic seminars and health systems, endnote lectures at city and statewide financial coalitions, and annual engagements for a variety of internal and external yearly meetings.
After an understandable slowdown in 2020, due to the onset of the COVID-19 pandemic, merger & acquisition (M&A) activity in the healthcare industry accelerated in 2021, and the industry is expected to continue the high number of deals and high deal volume in 2022.
***
***
This Health Capital Topics article will review the U.S. healthcare industry’s M&A activity in 2021, and discuss what these trends may mean for 2022. (Read more…)
Posted on February 24, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Staff Reporters
***
OIL: Brent crude, the world benchmark, briefly climbed above $100 a barrel for the first time since 2014. US crude jumped 3.3% to $95.15 a barrel.
U.S. stock indexes: All closed sharply lower with the DJIA narrowly avoiding a slip into correction, as U.S. officials warned that Russian troops were poised to attack, and are attacking, the Ukraine raising anxieties among investors who are also wrangling with changing monetary policy and surging inflation.
How did stock indexes trade? The Dow Jones Industrial Average fell 464.85 points, or 1.4%, to end at 33,131.76. A finish below 33,119.69 would mark a 10% decline from the Dow’s Jan. 4 record close, meeting the commonly used definition of a correction. The S&P 500 index fell 79.26 points, or 1.8%, to around 4,225.50, deepening its stumble into correction territory. The NASDAQ Composite Index declined 344.03 points, or 2.6%, at 13,037.49, with 12,845.95 representing the level that would represent a bear market for the technology-laden index.
Asia: Hong Kong’s Hang Seng Index declined 3.2%. Korea’s Kospi dropped 2.7%. Japan’s Nikkei 225 lost 2.4% after coming back from a holiday. China’s Shanghai Composite moved 0.9% lower.
Posted on February 23, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Staff Reporters
***
MARKETS: The S&P 500 fell into a correction for the first time in two years, joining the NASDAQ Composite, as Russia sent troops into pro-Russian regions in Ukraine. The S&P 500 index ended down 1% at 4,304.76, below the correction level at 4,316.91, which would represent a 10% drop from its January 3rd record close. A correction is commonly defined by market technicians as a fall of at least 10% (but not greater than 20%) from a recent peak. The last time the S&P 500 entered a correction was February 27th 2020, when the market was being whipsawed by fears about the outbreak of the COVID pandemic.
And, this bearish market isn’t sparing 2021 winners like Home Depot, which fell the most in nearly two years after supply-chain bottlenecks squeezed its margins. HD was the Dow’s biggest gainer last year.
IRS: According to a news release issued by the IRS, taxpayers now have the option to verify their identities during live, virtual interviews with agents. The agency stresses that no bio-metric data will be required for those interviews.
However, taxpayers once again have the option to verify their identity using ID.me’s facial recognition services. Addressing privacy concerns, the IRS says new requirements are in place to ensure that images provided will be deleted upon verification. That would apply to any new IRS accounts created and those where selfies have already been collected.
Posted on February 22, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Staff Reporters
***
***
Markets: The domestic markets were closed yesterday as stocks around the world tumbled.
Crypto: Bitcoin was trading at $36,649 at 2:30 a.m. ET, falling nearly 6.5% in the last 24 hours, according to data from CoinDesk. The world’s most valuable cryptocurrency fell below $40,000 over the weekend, and has continued to slide as the Ukraine crisis intensifies. The currency has lost almost half its value since its November high of $68,990 due to geopolitical tensions, the prospect of interest rate hikes by the US Federal Reserve and curbs by some major economies on digital assets. Bitcoin’s peers have also been faring poorly. Ethereum, the world’s second most valuable cryptocurrency, fell over 8% in the last 24 hours and was trading at $2,520.
Putin: Russian President Vladimir Putin dramatically escalated the Ukrainian conflict. He recognized two separatist regions in eastern Ukraine as independent and ordered Russian troops to enter those areas, which may provide the pretext for an invasion of other parts of the country. Western leaders condemned the move as a violation of international law and the US said it will impose sanctions on those regions.
Posted on February 16, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
MARKETS: The Dow jumped 422 points, or 1.2%. The S&P 500 surged 1.5% and the NASDAQ was 2.5% higher.
OIL: US oil futures tumbled 3.7% to just under $92 a barrel. That’s despite the fact that Russia stressed that major military exercises would continue.
CPI: The Producer Price Index rose 1% last month, marking a significant acceleration from December’s 0.2% jump.
Meta: As Varietyreports, the company has agreed to pay $90 million to settle a 2012 class action lawsuit accusing it of violating users’ privacy. Facebook allegedly overstepped its bounds in 2010 and 2011 by using tracking cookies that monitored browsing after users signed out despite promises to the contrary.
MODERNA: Moderna Inc (NASDAQ: MRNA) shares were down more than 40% since the start of the year and continues to trend lower. Vaccine stocks are facing selling pressure as the COVID-19 omicron variant fades, but Moderna investors have been expressing concerns about recent stock sales from CEO Stéphane Bancel, as well as the presumed deletion of his Twitter account.
Posted on February 6, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
****
***
It’s February – American Heart Month – a time when the nation spotlights heart disease, the No. 1 killer of Americans.
President Lyndon B. Johnson, among the millions of people in the country who’d had heart attacks, issued the first proclamation in 1964. Since then, U.S. presidents have annually declared February American Heart Month.
Throughout the month, the American Heart Association’s “Heart to Heart: Why Losing One Woman Is Too Many” campaign will raise awareness about how 1 in 3 women are diagnosed with heart disease annually.
The first Friday of American Heart Month, Feb. 5, is also National Wear Red Day as part of the AHA’s Go Red for Women initiative. Coast to coast, landmarks, news anchors and neighborhoods go red to raise awareness and support for the fight against heart disease. For more information on the event and other activities during the month, visit goredforwomen.org.
This year, the federally designated event is even more important due to the impact of the coronavirus on the public’s heart health, including potential harmful effects on the heart and vascular system, according to recent research.
Also, during the COVID-19 pandemic, many people have delayed or avoided going to hospitals for heart attacks and strokes – netting poorer outcomes and prompting the AHA to create “Don’t Die of Doubt,” a national awareness campaign that reminds people that hospitals are the safest place to go when you have symptoms.
And while in lock-down, more people have engaged in unhealthy lifestyle behaviors, such as eating poorly, drinking more alcohol and limiting physical activity, that can contribute to heart disease.
Meanwhile, heart disease continues to be the greatest health threat to Americans and is still the leading cause of death worldwide, according to the AHA’s Heart Disease and Stroke Statistics – 2021 Update.
The update, published in the association’s flagship journal Circulation, reports that nearly 18.6 million people across the globe died of cardiovascular disease in 2019, the latest year for which worldwide statistics are calculated. That’s a 17.1% increase over the past decade. And 523.2 million cases of cardiovascular disease were reported in 2019, a 26.6% increase over 2010.
During American Heart Month, the AHA and other organizations reinforce the importance of heart health, the need for more research and efforts to ensure that millions of people live longer and healthier.
In most cases, heart disease is preventable when people adopt a healthy lifestyle, which includes not smoking, maintaining a healthy weight, controlling blood sugar and cholesterol, treating high blood pressure, getting at least 150 minutes of moderate-intensity physical activity a week and getting regular checkups.
Posted on February 4, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
A recent Johns Hopkins analysis of 676 U.S. health systems found that these 4 health systems contributed to healthcare overuse the most:
• St. Dominic Health Services in Jackson, Mississippi • USMD Health System in Irving, Texas • Community Medical Centers in Clovis, California • Care New England Health System in Providence, Rhode Island
Posted on January 31, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Ann Miller RN MHACMP®
Executive Director
***
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism.
We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial.
And, our consultants “got fly”, just like U.
Read it! Write it! Post it! “Medical Executive-Post”.
Call or email us for your FREE advertising and sales consultation TODAY [770.448.0769]
Posted on January 26, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
Maestro Health: Top 5 Ranked Risk Areas
Maestro Health surveyed 600 U.S.-based HR professionals. Survey respondents anticipate their company’s medical costs will increase. The top areas at risk are:
• Decreases in annual physicals/screenings: 62% • Increased pharmaceutical costs: 49% • Unvaccinated employees: 47% • More elective surgeries: 46% • Increased urgent care costs: 45%
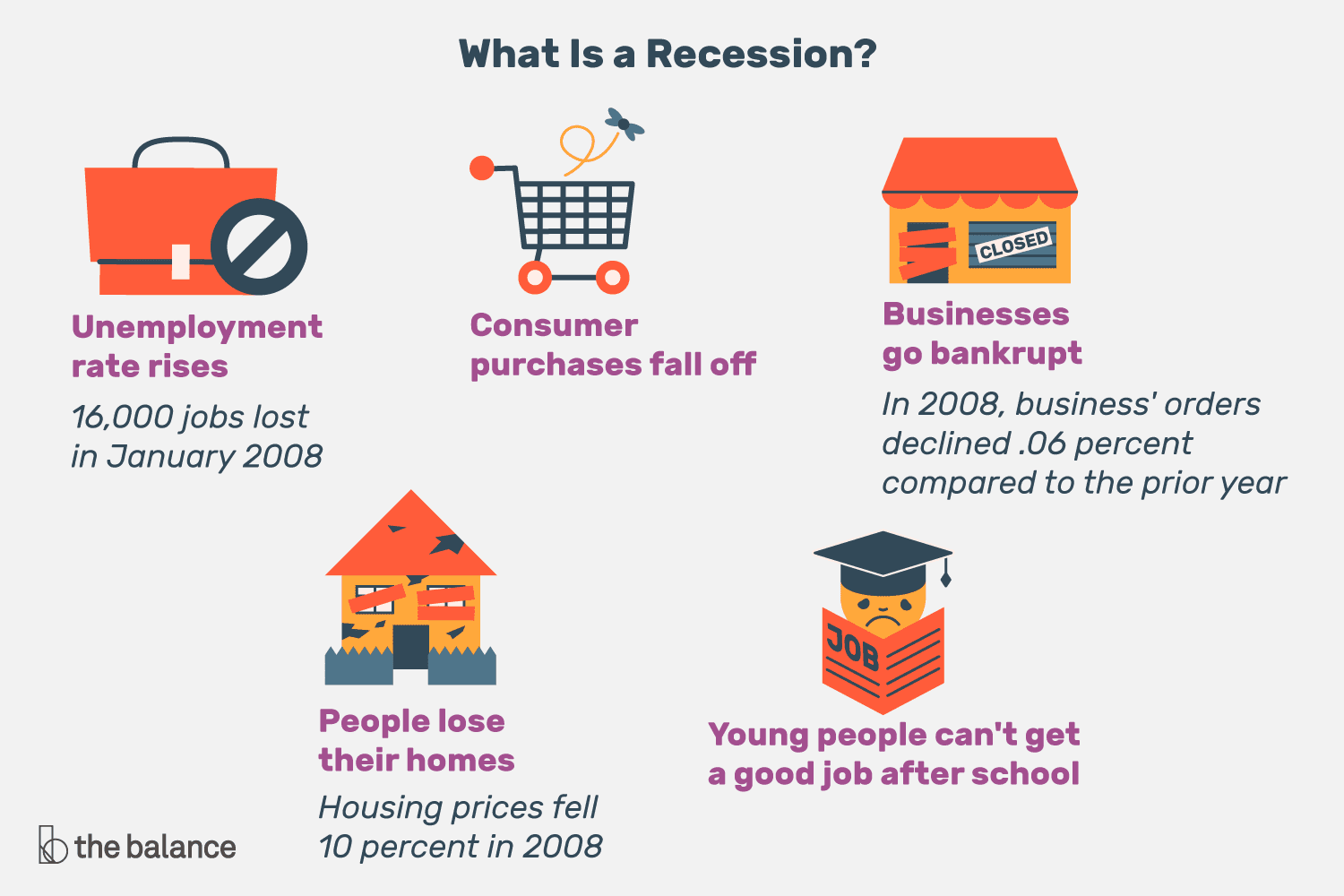
The business cycle is also known as the economic cycle and reflects the expansion or contraction in economic activity. Understanding the business cycle and the indicators used to determine its phases may influence investment or economic business decisions and financial or medical planning expectations. Although often depicted as the regular rising and falling of an episodic curve, the business cycle is very irregular in terms of amplitude and duration.
Moreover, many elements move together during the cycle and individual elements seldom carry enough momentum to cause the cycle to move. However, elements may have a domino effect on one another, and this is ultimately drives the cycle. We can also have a large positive cycle, coincident with a smaller but still negative cycle, as seen in the current healthcare climate of today.
First Phase: Trough to Recovery (production driven)
Scenario: A depressed GNP leads to declining industrial production and capacity utilization. Decreased workloads result in improved labor productivity and reduced labor (unit) costs until actual producer (wholesale) prices decline.
Second Phase: Recovery to Expansion (consumer driven)
Scenario: CPI declines (due to reduced wholesale prices) and consumer real income rises, improving consumer sentiment and actual demand for consumer goods.
Third Phase: Expansion to Peak (production driven)
Scenario: GNP rises leading to increased industrial production and capacity utilization. But, labor productivity declines and unit labor costs and producer (wholesale) prices rise.
Fourth Phase: Peak to Contraction (consumer driven)
Scenario: CPI rises making consumer real income and sentiment erode until consumer demand, and ultimately purchases, shrink dramatically. Recessions may occur and economists have an alphabet used to describe them.
For example, with a V, the drop and recovery is quick. For U, the economy moves up more sluggishly from the bottom. A W is what you would expect: repeated recoveries and declines. An L shaper recession describes a prolonged dry economic spell or even depression.
NOTE: Historically, contractions have had a shorter duration than expansions.
Bull and Bear Markets for Medical Professionals
A bull market is generally one of rising stock prices, while a bear market is the opposite. There are usually two bulls for every one bear market over the long term.
More specifically, a bear market is defined as a drop of twenty percent or more in a market index from its high, and can vary in duration and severity. While a bull market has no such threshold requirement to exist, other than they exist between these two periods of sharp decline.
Whither the Bear?
As a doctor, your action plan in a bear market depends on many variables, with perhaps your age being the most important:
In your 30s:
Pay off debts, school or practice loans.
Invest in safe money market mutual funds, cash or CDs.
Start retirement plan or 401-K account.
In your 40s:
Increase your pension plan or 401-K contributions.
Stay weighted more toward equity investments.
Review your goals, risk tolerance and portfolio.
In your 50s:
Position assets for ready cash instruments.
Diversify into stock, bonds and cash.
Retirement:
Maintain 3 years of ready cash living expenses.
Reduce, but still maintain your exposure to equities.
ASSESSMENT: So, where are we right now in the economic business cycle? Your thoughts are appreciated.























 ***
***