BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
An Internet Protocol (IP) address is a numerical identifier assigned to network interfaces participating in an IP‑based network. It functions as the cornerstone of packet‑switched communication, enabling devices to locate, identify, and exchange data across interconnected networks. At a technical level, an IP address encodes both host identity and network topology, allowing routers to forward packets efficiently through hierarchical addressing structures.
IP Address Structure and Protocol Versions
The two dominant versions of the Internet Protocol—IPv4 and IPv6—define the format and semantics of IP addressing.
IPv4, defined in RFC 791, uses a 32‑bit address space. These 32 bits are typically represented in dotted‑decimal notation, divided into four octets. The address space provides possible addresses, roughly 4.3 billion. IPv4 addresses are logically divided into network and host portions, historically using classful addressing (Classes A, B, C), though modern networks rely on Classless Inter‑Domain Routing (CIDR). CIDR allows arbitrary prefix lengths, expressed as a suffix such as /24, enabling more efficient allocation and route aggregation.
IPv6, defined in RFC 8200, expands the address space to 128 bits, represented in eight groups of hexadecimal values separated by colons. The enormous address space— possible addresses—supports hierarchical routing, stateless address autoconfiguration (SLAAC), and built‑in support for multicast and anycast addressing. IPv6 eliminates broadcast traffic entirely, replacing it with more efficient multicast mechanisms.
Address Types and Scopes
IP addresses can be categorized by scope and function:
Unicast: Identifies a single network interface. Most traffic on the internet is unicast.
Multicast: Identifies a group of interfaces; packets are delivered to all group members.
Broadcast (IPv4 only): Targets all hosts on a local network segment.
Anycast (primarily IPv6): Assigned to multiple interfaces; packets are routed to the nearest instance based on routing metrics.
Additionally, addresses can be public (globally routable) or private (RFC 1918 for IPv4, Unique Local Addresses for IPv6). Private addresses require Network Address Translation (NAT) to communicate with the public internet, a workaround that became essential due to IPv4 exhaustion.
Static vs. Dynamic Assignment
IP addresses may be assigned statically or dynamically:
Static addressing involves manual configuration and is common for servers, routers, and infrastructure requiring predictable reachability.
Dynamic addressing uses the Dynamic Host Configuration Protocol (DHCP). DHCP automates address assignment, lease renewal, and configuration of parameters such as default gateways and DNS servers.
In IPv6 networks, dynamic assignment may use DHCPv6 or SLAAC. SLAAC allows hosts to generate their own addresses using router advertisements and interface identifiers, reducing administrative overhead.
Routing and Packet Delivery
IP addresses are integral to routing—the process by which packets traverse networks. When a host sends a packet, it encapsulates data in an IP header containing source and destination addresses. Routers examine the destination address and consult their routing tables to determine the next hop. Routing protocols such as OSPF, BGP, and IS‑IS maintain these tables by exchanging topology information.
The hierarchical nature of IP addressing enables route aggregation, reducing the size of global routing tables. For example, a provider may advertise a single /16 prefix representing thousands of customer networks.
DNS and Address Resolution
Human‑readable domain names must be translated into IP addresses before communication can occur. The Domain Name System (DNS) performs this translation. When a user enters a URL, the system queries DNS resolvers, which return the corresponding A (IPv4) or AAAA (IPv6) records.
On local networks, the Address Resolution Protocol (ARP) maps IPv4 addresses to MAC addresses. IPv6 uses Neighbor Discovery Protocol (NDP) for similar functionality, leveraging ICMPv6 messages.
Security and Privacy Considerations
IP addresses reveal network topology and can expose approximate geographic location. Attackers may use them for reconnaissance, scanning, or targeted attacks. Techniques such as NAT, VPNs, and IPv6 privacy extensions help mitigate exposure by masking or rotating interface identifiers.
Conclusion
An IP address is far more than a simple identifier; it is a fundamental component of the Internet Protocol suite, enabling routing, addressing, and communication across global networks. Its structure, allocation mechanisms, and interaction with routing and resolution protocols form the backbone of modern digital infrastructure. As the internet continues to scale and diversify, the role of IP addressing—particularly IPv6—remains central to the performance, security, and scalability of global communication systems.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Risk management has become an essential component of modern medical practice, shaping how physicians deliver care, communicate with patients, and navigate an increasingly complex healthcare environment. While medicine has always involved uncertainty, today’s physicians face heightened scrutiny, evolving regulations, and rising patient expectations. Effective risk management is not merely about avoiding lawsuits; it is about fostering safer clinical environments, strengthening trust, and supporting high‑quality care. When approached proactively, it becomes a framework that protects both patients and practitioners.
At its core, risk management begins with recognizing the areas where errors, misunderstandings, or system failures are most likely to occur. Clinical decision‑making is an obvious focal point. Physicians must constantly balance diagnostic possibilities, weigh treatment options, and consider potential complications. Even with strong clinical judgment, risks arise when information is incomplete, when symptoms are ambiguous, or when time pressures limit thorough evaluation. To mitigate these challenges, physicians increasingly rely on structured clinical protocols, decision‑support tools, and multidisciplinary collaboration. These strategies help reduce variability in care and ensure that critical steps are not overlooked.
Communication is another central pillar of risk management. Many malpractice claims stem not from clinical mistakes but from breakdowns in communication—unclear explanations, unmet expectations, or perceived dismissiveness. Physicians who take the time to listen carefully, explain diagnoses and treatment plans in accessible language, and invite questions create a foundation of trust that can prevent conflict later. Informed consent is a particularly important aspect of this process. When patients fully understand the benefits, risks, and alternatives of a proposed intervention, they are better equipped to make decisions and less likely to feel blindsided if complications arise. Clear documentation of these conversations further strengthens the physician’s position and ensures continuity of care.
Documentation itself is a powerful risk‑management tool. Accurate, timely, and thorough medical records serve multiple purposes: they guide clinical decision‑making, support communication among care teams, and provide a factual account of events if questions arise later. Physicians who document not only what they did but why they made certain decisions create a transparent narrative that reflects thoughtful, patient‑centered care. Conversely, incomplete or inconsistent records can create vulnerabilities, even when the care provided was appropriate.
***
***
Another important dimension of risk management involves staying current with medical knowledge and regulatory requirements. Medicine evolves rapidly, and outdated practices can expose physicians to unnecessary risk. Continuing education, peer review, and participation in quality‑improvement initiatives help physicians maintain competence and identify areas for improvement. Regulatory compliance—whether related to privacy laws, prescribing rules, or reporting obligations—is equally critical. Violations, even unintentional ones, can lead to legal consequences and damage professional credibility.
Systems‑based risk management has also gained prominence. Many errors arise not from individual negligence but from flawed processes or communication gaps within healthcare organizations. Physicians who engage in system‑level improvements—such as refining hand off procedures, participating in morbidity and mortality reviews, or advocating for safer workflows—contribute to a culture of safety that benefits everyone. This collaborative approach recognizes that risk management is not solely the responsibility of individual clinicians but a shared commitment across the healthcare team.
Emotional intelligence plays a surprisingly influential role as well. When adverse events occur, patients and families often look to the physician for honesty, empathy, and reassurance. A compassionate response can de‑escalate tension and preserve the therapeutic relationship, even in difficult circumstances. Many institutions now encourage physicians to participate in disclosure training, which helps them navigate these conversations with clarity and sensitivity. Addressing the emotional impact on physicians themselves is equally important; burnout, fatigue, and stress can impair judgment and increase the likelihood of errors. Supporting physician well‑being is therefore an indirect but vital component of risk management.
Ultimately, effective risk management is not about practicing defensively or avoiding complex cases. It is about creating an environment where safety, transparency, and continuous improvement are woven into everyday practice. Physicians who embrace these principles are better equipped to navigate uncertainty, maintain strong patient relationships, and deliver care that aligns with both ethical and professional standards. In a healthcare landscape that continues to evolve, risk management remains a dynamic and indispensable part of responsible medical practice.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on February 2, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
The Role of Artificial Intelligence in Insurance and Risk Management
Artificial Intelligence (AI) is revolutionizing the insurance and risk management industries by enhancing efficiency, accuracy, and customer experience. As data becomes increasingly central to decision-making, AI offers powerful tools to analyze vast datasets, predict outcomes, and automate complex processes. Its integration is reshaping traditional models and enabling insurers to better assess risk, detect fraud, and personalize services.
One of the most transformative applications of AI in insurance is in underwriting. Traditionally, underwriting relied on manual evaluation of risk factors, which was time-consuming and prone to human error. AI algorithms can now process structured and unstructured data—from medical records to social media activity—to assess risk profiles with greater precision. Machine learning models continuously improve as they ingest more data, allowing insurers to refine their risk assessments and pricing strategies dynamically.
Claims processing is another area where AI is making a significant impact. Through natural language processing (NLP) and image recognition, AI can automate the evaluation of claims, reducing the time and cost associated with manual reviews. For example, AI can analyze photos of vehicle damage to estimate repair costs or flag inconsistencies in a claim that may indicate fraud. This not only speeds up the claims cycle but also enhances fraud detection, a critical concern in the industry.
Risk management benefits from AI’s predictive capabilities. By analyzing historical data and identifying patterns, AI can forecast potential risks and suggest mitigation strategies. In property insurance, AI can assess the likelihood of natural disasters by combining satellite imagery with climate data. In health insurance, predictive analytics can identify individuals at higher risk of chronic conditions, enabling early interventions and reducing long-term costs.
***
***
Customer experience is also being transformed by AI. Chatbots and virtual assistants provide 24/7 support, answering queries, guiding users through policy selection, and even initiating claims. These tools improve accessibility and responsiveness, fostering customer satisfaction and loyalty. Moreover, AI-driven personalization allows insurers to tailor products and communications to individual preferences and behaviors, enhancing engagement.
Despite its advantages, the adoption of AI in insurance and risk management raises ethical and regulatory challenges. Data privacy is a major concern, as AI systems require access to sensitive personal information. Ensuring transparency in AI decision-making is also critical, especially when algorithms influence coverage eligibility or claim outcomes. Regulators are increasingly scrutinizing AI applications to ensure fairness, accountability, and compliance with legal standards.
In conclusion, AI is a game-changer for insurance and risk management, offering tools to streamline operations, improve accuracy, and enhance customer service. As the technology evolves, insurers must balance innovation with ethical responsibility, ensuring that A.I. serves both business goals and societal interests. The future of insurance lies in intelligent systems that not only manage risk but also anticipate and prevent it—ushering in a new era of proactive, data-driven protection.
Posted on January 30, 2026 by Dr. David Edward Marcinko MBA MEd CMP™
A FINANCIAL THEORY
By Staff Reporters
***
***
FINANCIAL THEORY
Theories of finance are essential for understanding and analyzing various financial phenomena. They provide the conceptual framework for investment strategies, risk management, and financial decision-making.
***
Merton’s Credit Risk Model: Innovations in Corporate Debt Valuation
Merton’s Model for Credit Risk, developed by Robert C. Merton in 1974, represents a significant advancement in the field of financial economics, particularly in the assessment of credit risk. Building upon the foundations of the Black-Scholes Model for options pricing, Merton’s approach introduced a novel method for valuing corporate debt and assessing the probability of default.
Merton’s model conceptualizes a company’s equity as a call option on its assets, with the strike price equivalent to the debt’s face value maturing at the debt’s due date. In this framework, if the value of the company’s assets falls below the debt’s face value at maturity, the firm defaults, as it is more beneficial for equity holders to hand over the assets to the debt holders rather than repay the debt. Conversely, if the asset value exceeds the debt value, the firm pays off its debt and equity holders retain control of the company.
The model calculates the risk of default by analyzing the volatility of the firm’s assets and the level of its liabilities. The key insight of the model is that the safer a company’s debt (lower probability of default), the less valuable the equity as a call option, and vice versa. This approach provides a more dynamic and market-based view of credit risk, as opposed to traditional static measures.
***
***
One of the model’s critical assumptions is that the firm’s assets follow a random walk and are normally distributed. The model also presumes that markets are efficient, and there is no friction in trading. Furthermore, Merton’s model assumes that the firm’s capital structure only comprises equity and zero-coupon debt, which simplifies the real-world complexities of corporate finance.
Despite these simplifications, Merton’s model has had a profound impact on the field of credit risk analysis. It laid the groundwork for the development of more sophisticated credit risk models and tools used in the financial industry, such as Moody’s KMV Model. These models have become integral in the risk management practices of banks and financial institutions, particularly in the assessment of counter-party risk and the pricing of risky debt.
In conclusion, Merton’s Model for Credit Risk has been instrumental in bridging the gap between corporate finance and asset pricing theory. It has provided a more comprehensive and market-based framework for understanding and managing credit risk, which has been pivotal for both academia and the financial industry. The model’s influence extends beyond credit risk analysis, affecting the broader areas of corporate finance, risk management, and financial regulation.
Gold has long been regarded as a cornerstone of wealth preservation, and its role within modern investment portfolios continues to attract scholarly attention. As both a tangible asset and a financial instrument, gold embodies characteristics that distinguish it from equities, fixed income securities, and other commodities. Its historical resilience, inflation-hedging capacity, and diversification benefits render it a subject of considerable importance in portfolio construction and risk management.
Historical and Monetary Significance
Gold’s enduring appeal is rooted in its function as a monetary standard and store of value. For centuries, gold underpinned global currency systems, most notably through the gold standard, which provided stability in international trade and monetary policy. Although fiat currencies have supplanted gold in official circulation, its symbolic and practical role as a measure of wealth persists. This historical continuity reinforces investor confidence in gold as a reliable repository of value during periods of economic uncertainty.
Inflation Hedge and Safe-Haven Asset
A substantial body of empirical research demonstrates that gold serves as a hedge against inflation and currency depreciation. When consumer prices rise and fiat currencies weaken, gold tends to appreciate, thereby preserving purchasing power. Moreover, gold’s status as a safe-haven asset is particularly evident during geopolitical crises, financial market turbulence, and systemic shocks. In such contexts, investors reallocate capital toward gold, seeking protection from volatility in traditional asset classes. This defensive quality underscores gold’s utility in stabilizing portfolios during adverse conditions.
Diversification and Risk Management
From the perspective of modern portfolio theory, gold offers diversification benefits due to its low correlation with equities and bonds. Incorporating gold into a portfolio reduces overall variance and enhances risk-adjusted returns. Studies suggest that even modest allocations—typically ranging from 5 to 10 percent—can improve portfolio resilience by mitigating downside risk. This non-correlation is especially valuable in environments characterized by heightened uncertainty, where traditional diversification strategies may prove insufficient.
Investment Vehicles and Accessibility
Gold’s versatility as an investment is reflected in the variety of instruments available to investors. Physical bullion, in the form of coins and bars, provides tangible ownership but entails storage and insurance costs. Exchange-traded funds (ETFs) offer liquidity and ease of access, while mining equities provide leveraged exposure to gold prices, albeit with operational risks. Futures contracts and derivatives enable sophisticated strategies, though they demand expertise and tolerance for volatility. The breadth of these vehicles ensures that gold remains accessible across diverse investor profiles.
Limitations and Critical Considerations
Despite its strengths, gold is not without limitations. Unlike equities or bonds, gold does not generate income, such as dividends or interest. This absence of yield can constrain long-term portfolio growth, particularly in low-inflation environments. Furthermore, gold prices are subject to volatility, influenced by investor sentiment, central bank policies, and global demand dynamics. Overexposure to gold may therefore hinder portfolio performance, underscoring the necessity of balanced allocation.
Conclusion
Gold’s dual identity as a historical store of value and a contemporary financial instrument secures its relevance in portfolio construction. Its inflation-hedging capacity, safe-haven qualities, and diversification benefits justify its inclusion as a strategic asset. Nevertheless, prudent management is essential, given its lack of yield and susceptibility to volatility. Within a scholarly framework of portfolio theory, gold emerges not as a panacea but as a complementary asset, enhancing resilience and stability in the face of evolving economic landscapes.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
What Medical School Didn’t Teach Doctors About Money
Medical school is designed to mold students into competent, compassionate physicians. It teaches anatomy, pathology, pharmacology, and clinical skills with precision and rigor. Yet, despite the depth of medical knowledge imparted, one critical area is often overlooked: financial literacy. For many doctors, the transition from student to professional comes with a steep learning curve—not in medicine, but in money. From managing debt to understanding taxes, investing, and retirement planning, medical school leaves a financial education gap that can have long-term consequences.
The Debt Dilemma
One of the most glaring omissions in medical education is how to manage student loan debt. The average medical student graduates with over $200,000 in debt, yet few are taught how to navigate repayment options, interest accrual, or loan forgiveness programs. Many doctors enter residency with little understanding of income-driven repayment plans or Public Service Loan Forgiveness (PSLF), missing opportunities to reduce their financial burden. Without guidance, some make costly mistakes—such as refinancing federal loans prematurely or choosing repayment plans that don’t align with their career trajectory.
Income ≠ Wealth
Medical students often assume that a high salary will automatically lead to financial security. While physicians do earn more than most professionals, income alone doesn’t guarantee wealth. Medical school rarely addresses the importance of budgeting, saving, and investing. As a result, many doctors fall into the “HENRY” trap—High Earner, Not Rich Yet. They spend lavishly, assuming their income will always cover expenses, only to find themselves living paycheck to paycheck. Without a solid financial foundation, even high earners can struggle to build net worth.
***
***
Taxes and Business Skills
Doctors are also unprepared for the complexities of taxes. Whether employed by a hospital or running a private practice, physicians face unique tax challenges. Medical school doesn’t teach how to track deductible expenses, optimize retirement contributions, or navigate self-employment taxes. For those who open their own clinics, the lack of business education is even more pronounced. Understanding profit margins, payroll, insurance billing, and compliance regulations is essential—but rarely covered in medical training.
Investing and Retirement Planning
Another blind spot is investing. Medical students are rarely taught the basics of compound interest, asset allocation, or retirement accounts. Many don’t know the difference between a Roth IRA and a traditional 401(k), or how to evaluate mutual funds and index funds. This lack of knowledge delays retirement planning and can lead to missed opportunities for long-term growth. Some doctors rely on financial advisors without understanding the fees or conflicts of interest involved, putting their wealth at risk.
Insurance and Risk Management
Medical school also fails to educate students on insurance—life, disability, malpractice, and health. Doctors need robust coverage to protect their income and assets, but many don’t know how to evaluate policies or understand terms like “own occupation” or “elimination period.” Inadequate coverage can leave physicians vulnerable to financial disaster in the event of illness, injury, or litigation.
Emotional and Behavioral Finance
Beyond technical knowledge, medical school overlooks the emotional side of money. Physicians often face pressure to maintain a certain lifestyle, especially after years of sacrifice. The desire to “catch up” can lead to impulsive spending, luxury purchases, and financial stress. Without tools to manage money mindset and behavioral habits, doctors may struggle with guilt, anxiety, or burnout related to finances.
The Case for Financial Education
Fortunately, awareness of this gap is growing. Organizations like Medics’ Money and podcasts such as “Docs Outside the Box” are working to fill the void by offering financial education tailored to physicians.
These resources cover everything from budgeting and debt management to investing and entrepreneurship. Some medical schools are beginning to incorporate financial literacy into their curricula, but progress is slow and inconsistent.
Conclusion
Medical school equips doctors to save lives, but it doesn’t prepare them to secure their own financial future. The lack of financial education leaves many physicians vulnerable to debt, poor investment decisions, and lifestyle inflation. To thrive both professionally and personally, doctors must seek out financial knowledge beyond the classroom. Whether through self-study, mentorship, or professional guidance, understanding money is as essential as understanding medicine. After all, financial health is a cornerstone of overall well-being—and every doctor deserves to master both.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Authentication:
The verification of the identity of an individual, system, machine, or any other unique entity
Authorization:
The process of allowing access to specific areas of a system based on the role and needs of the user
Committee Charter:
A document that defines the purposes and responsibilities of the oversight committee
Compliance Risk Profile:
The current and prospective risk to earnings or capital arising from violations of or nonconformance with laws, rules, regulations, prescribed practices, internal policies and procedures, or ethical standards
Control Assessment:
A high-level review and analysis of controls relating to a process; should encompass both current and missing controls
Controls:
Methods that preserve the integrity of important information, meet operational or financial targets, and/or communicate management policies (See also: Key Control, Secondary Control, Tertiary Control)
ERM Policy Statement:
Defines an organization’s approach to and method of enterprise risk management
Governance:
Processes and structures implemented to communicate, manage, and monitor organizational activities
Impact:
The influence and effect of a risk
Inherent Risk:
Risk that is inherent to a process, taking into consideration the likelihood and impact of a risk
Key Control:
A primary control that is essential for a business process; typically takes place during the process it applies to
Key Indicators:
Measurements that are important for organizations to monitor for potential issues; examples include key performance indicators (KPIs) and key risk indicators (KRIs)
Key Performance Indicator (KPI):
A measurement with a defined set of goals and tolerances that gauges the performance of an important business activity
Key Risk Indicator (KRI):
A proactive measurement for future and emerging risks that indicates the possibility of an event that adversely affects business activities
Likelihood:
The probability of a risk occurring
Mitigation Actions:
The necessary steps, or action items, to reduce the likelihood and/or impact of a potential risk
Operation Risk Profile:
1) The risk arising from the execution of an organization’s business processes; 2) The risk of loss resulting from failed or inadequate internal processes, systems, people, or other entities
Price Risk Profile:
The risk to earning or capital arising from adverse changes in portfolio values
Process:
1) The principle elements of essential business functions within work groups or business units; 2) A set of tasks completed by business continuity plan owners within a department
Reputation Risk Profile:
The current and prospective risk to earnings or capital arising from negative public opinion or perception
Residual Risk:
Risk remaining after considering the existing control environment
Risk:
A potential event or action that would have an adverse effect on the organization
Risk Appetite:
A statement that broadly considers the risk levels that management deems acceptable
Risk Assessment:
The prioritization of potential business disruptions based on the impact and likelihood of occurrence; includes an analysis of threats based on the impact to the organization, its customers, and financial markets
Risk Tolerance:
A metric that sets the acceptable level of variation around organizational objectives and provides assurance that the organization remains within its risk appetite
Secondary Control:
An important control that typically takes place after the process it applies to (i.e., reporting or ongoing monitoring)
Strategic Risk Profile:
The current and prospective risk to earnings or capital raising from adverse business decisions, improperly implemented decisions, or lack of responsiveness to industry changes
Tertiary Control:
A non-essential control that can still be applied effectively to a business process
Velocity:
The time it takes a risk event to manifest itself
Vulnerability:
An entity’s susceptibility to a risk event as determined by the entity’s preparedness, agility, and adaptability
Posted on September 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
What Is Pure Risk?
Pure risk is a category of risk that cannot be controlled and has two outcomes: complete loss or no loss at all. There are no opportunities for gain or profit when pure risk is involved. Pure risk is generally prevalent in situations such as natural disasters, fires, or death. These situations cannot be predicted and are beyond anyone’s control. Pure risk is also referred to as absolute risk.
***
1. Personal Risks
Now, there are basically 3 types of pure risks that concern individual physicians. These incur losses like loss of income, additional expenses and devaluation of property. There are 4 risk factors affecting them:
Premature death. This is death of a breadwinner who leaves behind financial responsibilities.
Old age / retirement. The risk of being retired without sufficient savings to support retirement years.
Health crisis. Individual with health problem may face a potential loss of income and increase in medical expenditures.
Unemployment. Jobless individual may have to live on their savings. If savings are depleted, a bigger crisis is awaiting.
2. Property Risks
This means the possibility of damage or loss to the property owned due to some cause. There are two types of losses involved.
Direct loss which means financial loss as a result of property damage.
Consequential loss which means financial loss due to the happenings of direct loss of the property.
For instance, a medical practice that burned down may incur repair costs as the direct loss. The consequential loss is being unable to run the practice business to generate income.
3. Liability Risks
A doctor is legally liable to his wrongful act that cause damage to a third party; physically, by reputation or property. S/he can be legally sued with no maximum in the compensation amount if found guilty.
Knowing how risks are classified, and the types of pure risks an individual is exposed to, will provide a fundamental overview on these risk topics and prepare you to further acquire the knowledge of how to deal with and manage them as a physician executive, leader, or manager.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
ORGANIZATIONAL BEHAVIOR ANDCLASSIFICATION OF RISKS
DEFINITION EMOTIONAL INTELLIGENCE: Emotional intelligence [EI] refers to the ability to identify and manage one’s own emotions, as well as the emotions of others. Emotional intelligence is generally said to include a few skills: namely emotional awareness, or the ability to identify and name one’s own emotions; the ability to harness those emotions and apply them to tasks like thinking and problem solving; and the ability to manage emotions, which includes both regulating one’s own emotions when necessary and helping others to do the same.
DEFINITIONAL ORGANIZATIONAL BEHAVIOR: Organizational behavior (OB) is the study of how individuals, groups, and organizations interact and influence one another. Though it is largely used within the field of business management as means to understand–and more effectively manage–groups of people. The reason businesses look to OB is because it can help organizations increase employee performance, while also creating a positive working environment.
CITE: Eugene Schmuckler; PhD MBA MEd CTS®
***
***
And so, as we review the concept of Emotional Intelligence and Organizational Behavior, it is possible to set up five EI/OB risk classes, based on the economic consequences of the occurrence of specific individual risks:
1. Prevented risks: Risks whose cost of occurrence is higher than their cost of management and whose occurrence may invoke additional legal sanctions. This class would include intentional torts and injuries caused by gross negligence.
2. Normally prevented risks: Risks whose cost of occurrence is greater than the cost of their management but whose occurrence will be considered only as negligent. This class includes most negligent injuries and most types of product liability actions.
3. Managed risks: Risks whose cost of occurrence is only slightly greater than their cost of management. The plaintiff usually has the burden of showing that the defendant owed the plaintiff a special duty to recover for one of these risks.
4. Un-Prevented risks: Risks whose cost of occurrence is less than their cost of management. The classic example of this class is the cost of railroad crossing barriers compared to the cost of people being hit by trains.
5. Un-Preventable risks: Risks whose occurrence is unmanageable. The assignment of a risk to one of these classes is a major problem in medical and healthcare quality control, because the class of a risk determines how much effort must be expended to prevent the risk. The misclassification of a prevented or normally prevented risk as a managed or un-prevented risk can result in large financial losses.
***
For example: A medical clinic that does not update obsolete equipment, such as inaccurate oxygen monitors, would be liable for any injuries attributable to the obsolete equipment. The classifications of risk must be reviewed periodically to determine if the cost of the risk-taking behavior has changed, thereby altering the classification.
***
***
For example: A small hospital in a rural area would not be expected to have the sophisticated equipment as a major hospital in a city. If an accident victim is brought into the rural facility, the hospital’s duty may be to transfer the patient to a better-equipped facility. The patient will face the risk of dying because of the delay in treatment, but the risk of insufficient treatments outweighs the risk of transfer. If the same victim were brought into a hospital in a major metropolitan center, the duty would be to treat the patient without a transfer. The risk of transfer has not changed, but the risk of insufficient treatment has disappeared.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on May 4, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
If getting answers from ChatGPT makes you feel dystopian, you may not want to hear about OpenAI CEO Sam Altman’s other co-founded venture, now rolling out stateside. It scans your eyeballs in exchange for cryptocurrency.
What in the Demolition Man? The device, which creates a unique user ID for your scan, is meant to address a problem that Altman had a hand in creating: how to verify identities and confirm humanity in a world full of artificial intelligence.
The project, called World (formerly Worldcoin), went live in other countries in 2023. Its US expansion, announced this week, featured retail outlets in five cities where you can get your eyes scanned:
Tools for Humanity, the company behind the orbs, says 12+ million people around the world have participated so far.
It claims to keep your data private, but authorities in more than a dozen places have suspended World’s operations or investigated its data practices, per the WSJ.
Posted on April 15, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
WARNING – WARNING
By Staff Reporters
***
***
A “retirement account scam” is a type of online fraud that occurs when a third party administrator (TPA) for retirement investment accounts is tricked into authorizing a money distribution to an imposter posing as the true account holder.
The imposter often starts the scam by calling the TPA, identifying himself or herself as an actual account holder, and requesting a withdrawal distribution form. Once the imposter receives the withdrawal distribution form, the imposter returns the completed form to the TPA. The form is completed with the account holder’s real personal identifying information (PII)—often stolen via schemes, data breaches, and other hacking offenses—and bank account information for an account controlled by the imposter or the imposter’s conspirators.
***
***
After the TPA processes the fraudulent request, the request is forwarded to the investment firm responsible for managing the account holder’s investments, and the funds—often the account holder’s life savings—are then directed to the imposter’s designated bank account.
The vast majority of physicians and medical professionals major in one of the hard science while in college; biology, engineering, chemistry, mathematics, computer science or physics; etc. Few take undergraduate courses in finance, business management, securities analysis, accounting or economics; although this paradigm is changing with modernity. These course are not particularly difficult for the pre-medical baccalaureate major, they are just not on the radar screen for time compressed and highly competitive students; nor are they needed for medical or nursing school admission, or the many related allied health professional schools.
In fact, William C. Roberts MD, originally from Emory University in Atlanta, and former editor for the Baylor University Medical Center Proceedings and The American Journal of Cardiology, opined just a decade ago:
“Of the 125 medical schools in the USA, only one of them to my knowledge offers a class related to saving or investing money.”
And so, it is important to review some basic principles of economics, finance and accounting as they relate to financial planning in thees two textbooks; and this ME-P.
Posted on April 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
WARNING – WARNING
By Dr. DavidEdwardMarcinko; MBA MEd
***
***
According to www.NPR.org, there are more than120,000 health care forums on the Internet with opinions ranging from pharmaceuticals, to sexual dysfunction, to acne. The same goes for commercial doctor blogs that promote lotions, balms and potions, diets and vitamins, minerals, herbs, drinks and elixirs, or various other ingest-ants, digest-ants or pharmaceuticals, etc.
And, to other doctors, the blogging craze is a new novelty where there are no rules, protocols, standards or precise figures on how many “medical-doctor” or related physician-blogs are “out there.” Unfortunately, too many recount gory ER scenes, or pictorially illustrate horrific medical conditions, or serious and traumatic injuries. Of course, others simply are medical practice websites, or those that entice patients into more lucrative plastic surgery or concierge medical practices. Some are from self-serving/credible plaintiff-seeking attorneys wishing to assist patients.
Not all physician blogs are geared toward practice information, marketing or medical sensationalism. In fact, just the opposite seems to be the case in extremely candid blogs, like “Ranting Docs”, “White Coat Rants,” “Grunt Docs”, “Cancer Doc,” “The Happy Hospitalist,” “Mom MD”, “Cross-Over Health”, “Angry Docs” and “M.D.O.D.,” which bills itself as “Random Thoughts from a Few Cantankerous American Physicians.”
According to some of these, they are more like personal journals, or public diaries, where doctors vent about reimbursement rates, difficult cases, medical mistakes, declining medical prestige and control, and/or what a “bummer” it is to have so many patients die; not pay, or who are indigent, noncompliant. We call these the “disgruntled doctor sites.” Some even talk about their own patients, coding issues, or various doctor-patient shenanigans.
But, according to psychiatrist and blogger Dr. Deborah Peel and others, the problem with blogging about patients is the danger that one will be able to identify themselves – the doctor – or that others who know them will be able to identify them.” Her affiliation, Patient Privacy Rights, rightly worries that patients might track back to the individual, and adversely affect their employment, health insurance or other aspects of life.
***
***
And, according to Dr. Jay S. Grife; MA Esq., it is certainly true that if a doctor violates a patient’s privacy there could be legal consequences. Under HIPAA, physicians could face fines or even jail time. In some states, patients can file a civil lawsuit if they believe a doctor has violated their privacy. Still, internet privacy issues are an evolving gray-area that if not wrong, may still be morally and ethically questionable [personal communication].
Our colleague Robert Wachter MD, author of the blog called “Wachter’s World,” says it’s important for doctors to be able to share cases, as long as they change the facts substantially. On the other hand, the author of “Wachter’s World” and a leading expert on patient safety alternately suggests “You might say we as doctors should never be talking about experiences with our patients online or in books or in articles.” But, he says that “patients shouldn’t take all the information on blogs at face value. Taken for what they are — unedited opinions, and in some cases entertainment — blogs can give readers some useful insight into the good, the bad and the ugly of the medical profession”. Link: http://www.the-hospitalist.org/blogs
Well, fair enough! But, doctors unhappy with their current medical career choice, or its modern evolution, should probably consider counseling or even career change guidance, re-education and re-engineering. It is very inappropriate to vent career frustrations in a public venue. It’s far better for the blog to be private and/or by invitation only; if at all [Personal communication].
We believe that a hybrid mash-up of both views can be wholly appropriate, or grossly inappropriate in some cases. Of course the devil is in the details; linguistics and semantics aside. Nevertheless; what is not addressed in electronic physician “mea-culpas” are the professional liability risks and concerns that are evolving in this quasi-professional, quasi-lay, communication forum.
***
***
Example: We have seen medical mistakes, and liability admissions of all sorts, freely and glibly presented. In fact,
“Some physicians find that the act of liability blogging as a professional confession that is useful in moving past their malpractice mistakes. And, it is also a useful way to begin a commitment to a better professional life of caring in the future. It helps eliminate the toxic residue and angst of professional liability and guilt. Moreover, as they are unburdened of past acts of omission or commission, doctors should remember to also forgive those who have wronged them. This helps greatly with the process and brings additional peace.”
However, although some may say that this electronic confession is good for the soul, it may not be good for your professional liability carrier, or you, when plaintiff’s attorneys release a legion of IT focused interns, or automated bots, searching online for your self-admissions and scouring for your self-incriminations. Of course, a direct connection to a specific patient may still not be made and no HIPAA violation is involved. But, a vivid imagination is not need needed to envision this type of blind medical malpractice discovery deposition query even now.
QUESTION:“Doctor Smith, I noted all the medical errors admitted on your blog. What other mistakes did you make in the care and treatment of my client?”
And so, the question of plausible deniability, or culpability, is easily raised. If you must journalize your thoughts for sanity or stress release; do it in print. And, don’t tell anyone about it so the diary won’t be subpoenaed. Then tear it up and throw it away. Remember, with risk management, “It is all about credibility.” Don’t trash yours! These thoughts may be especially important if you covet a medical career as a researcher, editor, educator, medical expert or something other than a working-class or employed physician.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on April 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Ann Miller RN MHA CPHQ CMP™
***
***
Finally … Fiduciary second investing and financial planning opinions right here!
Telephonic or electronic advice for medical professionals that is:
Objective, affordable, medically focused and financially personalized
Rendered by a pre-screened financial consultant for doctors and medical professionals
Offered on a pay-as-you-go basis, by phone or secure e-mail transmission
The iMBA Discussion Forum™ is a physician-to-financial advisor telephone or e-mail portal that connects independent financial professionals to doctors, nurses or healthcare executives desiring affordable and unbiased financial planning advice.
Medical professionals and healthcare executives can now receive direct access to pre-screened iMBA professionals in the areas of Investing, Financial Planning, Asset Allocation, Portfolio Management, Insurance, Mortgage and Lending, Human Resources, Retirement Planning and Employee Benefits. To assist our medical professional and healthcare executive members, we can be contracted with per-minute or per-project fees, and contacted by client phone, email or secure instant messaging.
Merger risk arbitrage, while a subset of a larger strategy called event-driven arbitrage, represents a sufficient portion of the market-neutral universe to warrant separate discussion.
Merger arbitrage earned a bad reputation in the 1980s when Ivan Boesky and others like him came to regard insider trading as a valid investment strategy. That notwithstanding, merger arbitrage is a respected strategy and when executed properly, can be highly profitable. It bets on the outcomes of mergers, takeovers and other corporate events involving two stocks which may become one.
Example:
A classic example is acquisition of SDL Inc. (SDLI) by JDS Uniphase Corp (JDSU). On July 10, 2010 JDSU announced its intent to acquire SDLI by offering to exchange 3.8 shares of its own shares for one share of SDLI. At that time, the JDSU shares traded at $101 and SDLI at $320.5. It was apparent that there was almost 20 percent profit to be realized if the deal went through (3.8 JDSU shares at $101 are worth $383 while SDLI was worth just $320.5).
This apparent mispricing reflected the market’s expectation about the deal’s outcome. Since the deal was subject to the approval of the U.S. Justice Department and shareholders, there was some doubt about its successful completion.
Risk arbitrageurs who did their homework and properly estimated the probability of success bought shares of SDLI and simultaneously sold short shares of JDSU on a 3.8 to 1 ratio, thus locking in the future profit. Convergence took place about eight months later, in February 2011, when the deal was finally approved and the two stocks began trading at exact parity, eliminating the mis-pricing and allowing arbitrageurs to realize a profit.
***
***
Hedge Fund Research defines the strategy as follows:
Merger Arbitrage,also known as risk arbitrage, involves investing in securities of companies that are the subject of some form of extraordinary corporate transaction, including acquisition or merger proposals, exchange offers, cash tender offers and leveraged buy-outs. These transactions will generally involve the exchange of securities for cash, other securities or a combination of cash and other securities. Typically, a manager purchases the stock of a company being acquired or merging with another company, and sells short the stock of the acquiring company. A manager engaged in merger arbitrage transactions will derive profit (or loss) by realizing the price differential between the price of the securities purchased and the value ultimately realized when the deal is consummated. The success of this strategy usually is dependent upon the proposed merger, tender offer or exchange offer being consummated.
When a tender or exchange offer or a proposal for a merger is publicly announced, the offer price or the value of the securities of the acquiring company to be received is typically greater than the current market price of the securities of the target company. Normally, the stock of an acquisition target appreciates while the acquiring company’s stock decreases in value. If a manager determines that it is probable that the transaction will be consummated, it may purchase shares of the target company and in most instances, sell short the stock of the acquiring company. Managers may employ the use of equity options as a low-risk alternative to the outright purchase or sale of common stock. Many managers will hedge against market risk by purchasing S&P put options or put option spreads.
Posted on March 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Split-Dollar Life Insurance: An arrangement under which a life insurance policy’s premium, cash values, and death benefit are split between two parties—usually a corporation and a key employee or executive. Under such an arrangement an employer may own the policy and pay the premiums and give a key employee or executive the right to name the recipient of the death benefit.
***
***
Several factors will affect the cost and availability of life insurance, including age, health, and the type and amount of insurance purchased. Life insurance policies have expenses, including mortality and other charges. If a policy is surrendered prematurely, the policy holder also may pay surrender charges and have income tax implications. You should consider determining whether you are insurable before implementing a strategy involving life insurance.
Any guarantees associated with a policy are dependent on the ability of the issuing insurance company to continue making claim payments.
“Malta has quietly leveraged the rising tide of the financial transparency imperative to attract hedge funds.“
There was a time when the quaint island sought to play on the traditional terrain, offering anonymity and a “laissez-faire regulatory regime,” not to mention very low taxes, as in no capital gains taxes and no taxes on dividends; all while English speaking and USD currency denominated.
***
***
While many leading domiciles for offshore hedge funds remain in the Caribbean – notably the Cayman Islands, the British Virgin Islands, Bermuda, and the Bahamas – the island of Malta is drawing attention, especially from European funds.
Health actuaries analyze potential risks, profits and trends that will affect their employers, which are often in the health insurance, government health services and medical provider industries. They advise companies on issuing policies to consumers based on risks, calculated premiums and upcoming changes in health-care costs.
It’s common for an actuary to have a bachelor’s degree or higher in actuary studies, mathematics or statistics. Coursework on medical terminology and hierarchy of the medical field is also beneficial. In addition to academic education, certification is also necessary to reach “professional status,” which is required by most employers.
***
***
The professional organization, Society of Actuaries, certifies actuaries in the health and medical field. Their statistical work is commonly done with predictive tables, probability tables and life tables that are created on customized statistical analysis software such as Stata or XLSTAT.
The actuary field as a whole is growing faster than other fields, according to the Bureau of Labor Statistics [BLS]. In 2020, it expanded by 27 percent. The average annual salary for an actuary in 2010 was $87,650. More specifically, in the health insurance field, the salary was slightly higher at $91,000.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on March 16, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
DEFINITION
***
***
According to Wikipedia, a tontine (/ˈtɒntaɪn, -iːn, ˌtɒnˈtiːn/) is an investment linked to a living person which provides an income for as long as that person is alive. Such schemes originated as plans for governments to raise capital in the 17th century and became relatively widespread in the 18th and 19th centuries.
Tontines enable subscribers to share the risk of living a long life by combining features of a group annuity with a kind of mortality lottery. Each subscriber pays a sum into a trust and thereafter receives a periodical payout. As members die, their payout entitlements devolve to the other participants, and so the value of each continuing payout increases. On the death of the final member, the trust scheme is usually wound up.
Tontines are still common in France. They can be issued by European insurers under the Directive 2002/83/EC of the European Parliament. The Pan-European Pension Regulation passed by the European Commission in 2019 also contains provisions that specifically permit next-generation pension products that abide by the “tontine principle” to be offered in the 27 EU member states.
Questionable practices by U.S. life insurers in 1906 led to the Armstrong Investigation in the United States restricting some forms of tontines. Nevertheless, in March 2017, The New York Times reported that tontines were getting fresh consideration as a way for people to get steady retirement income.
According to Patricia Salber MD [personal communication], there are a number of reasons why direct patient access to laboratory medical results is a good idea:
Between 8 and 26% of abnormal test results, including those suspicious for cancer, are not followed up in a timely manner. Direct access could help reduce the number of times this occurs
Self-management, particularly of chronic illness has known benefits. Just like the QS people, many folks with chronic illness obtain and manage to self-acquired lab results every day via gluco-meters, home pulmonary function tests, blood pressure measurements, and so forth. Direct access to laboratory-acquired data, one could argue is a continuation of that personal responsibility
Patients want to be notified about their results in what they perceive as a timely fashion. In one study, patients who received direct notification of their bone density tests results were more likely to perceive they had timely notification compared to usual care even though there was no measurable effect on actual treatment received after three months
Being more responsible for test results could encourage consumers to try to learn more about the meaning of the test results, conceivably increasing their health literacy.
But, the arguments against direct access discussed include the following:
Patients prefer their physicians contact them directly when they have abnormal test results, although the major studies published in 2005 and 2009, preceded the extraordinary use of the internet to access health information that exists today.
There is concern over whether patients will know what to do when they receive the results – will they make erroneous interpretations or fail to contact their docs? This could be, but the intent of the proposed rule is shared access to the results. We suspect if the rule become law, docs will develop better notification mechanisms so that they reach the patient before the patient directly accesses the results or lab companies will design better lab test notifications with easy-to-understand interpretations or a whole new industry will appear that can provide instantly available individualized lab interpretation…or maybe all three of these would happen and that would be a very good thing.
Unknown impact of dual notification (doctors and patients) of lab test results on physician behavior…would docs simply shift responsibility for initiating follow-up care from themselves to their patients?
Would direct access of life-changing lab tests, such as HIV or malignancy, lead to unnecessary patient anxiety – or worse? (Conversely, is there less anxiety, desperation, or suicidal ideation if the bad news is delivered face to face?
Individuals likely may contact their physicians immediately after getting the lab results asking for a telephonic or face-to-face interpretation … it is not known how this would impact physician workload and/or potential for reimbursement [personal communication, Richard Hudson DO, Atlanta, GA].
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on March 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters and IRS
***
***
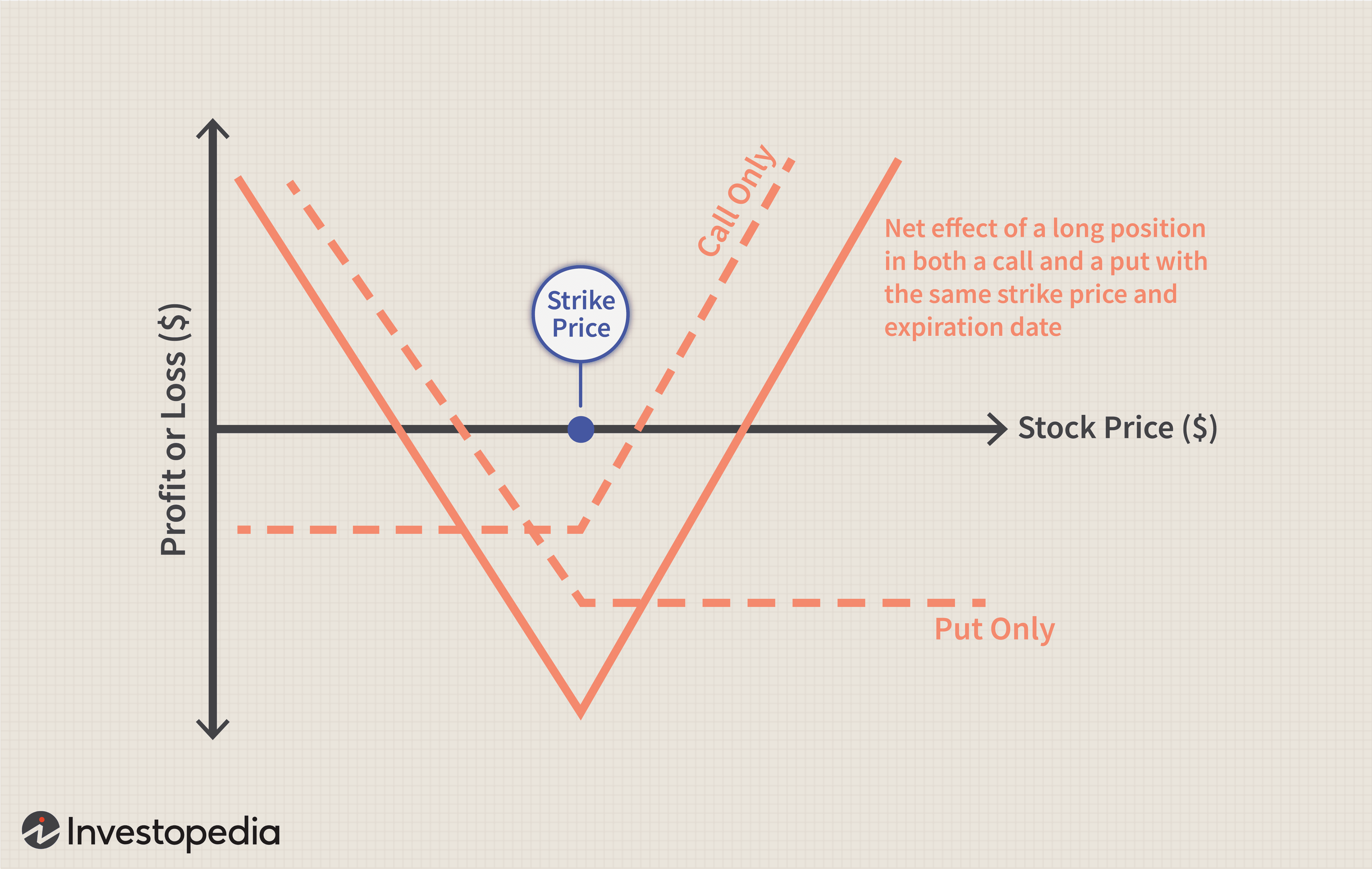
Straddles: A straddle is any set of offsetting positions on personal property. For example, a straddle may consist of a purchased option to buy and a purchased option to sell on the same number of shares of the security, with the same exercise price and period.
Personal property.
This is any actively traded property. It includes stock options and contracts to buy stock but generally does not include stock.
Straddle rules for stock.
Although stock is generally excluded from the definition of personal property when applying the straddle rules, it is included in the following two situations.
The stock is of a type that is actively traded, and at least one of the offsetting positions is a position on that stock or substantially similar or related property.
The stock is in a corporation formed or availed of to take positions in personal property that offset positions taken by any shareholder.
Note
For positions established before October 22, 2004, condition 1 above does not apply. Instead, personal property includes stock if condition 2 above applies or the stock was part of a straddle in which at least one of the offsetting positions was:
An option to buy or sell the stock or substantially identical stock or securities,
A securities futures contract on the stock or substantially identical stock or securities, or
A position on substantially similar or related property (other than stock).
Position
A position is an interest in personal property. A position can be a forward or futures contract or an option.
An interest in a loan denominated in a foreign currency is treated as a position in that currency. For the straddle rules, foreign currency for which there is an active inter bank market is considered to be actively traded personal property.
Offsetting position
This is a position that substantially reduces any risk of loss you may have from holding another position. However, if a position is part of a straddle that is not an identified straddle, do not treat it as offsetting to a position that is part of an identified straddle.
Presumed offsetting positions
Two or more positions will be presumed to be offsetting if:
The positions are established in the same personal property (or in a contract for this property), and the value of one or more positions varies inversely with the value of one or more of the other positions;
The positions are in the same personal property, even if this property is in a substantially changed form, and the positions’ values vary inversely as described in the first condition;
The positions are in debt instruments with a similar maturity, and the positions’ values vary inversely as described in the first condition;
The positions are sold or marketed as offsetting positions, whether or not the positions are called a straddle, spread, butterfly, or any similar name; or
The aggregate margin requirement for the positions is lower than the sum of the margin requirements for each position if held separately.
Related persons
To determine if two or more positions are offsetting, you will be treated as holding any position your spouse holds during the same period. If you take into account part or all of the gain or loss for a position held by a flow-through entity, such as a partnership or trust, you are also considered to hold that position.
RISK MANAGEMENT, LIABILITY INSURANCE AND ASSET PROTECTION ABBREVIATIONS
[Glossary of Important Acronyms]
Much has been written and much has been opined on the topic of medical risk management, insurance, asset protection and professional liability for physicians and healthcare providers in this textbook; and elsewhere.
But occasionally, we all still get lost in a wide array of abbreviations, acronyms, and initialisms that are constantly changing in this ecosystem.
And so, this glossary serves as a ready reference for those who want to know about these medical risk management definitions in a quick and ready fashion.
Acronyms and Abbreviations
AAASC American Association of Ambulatory Surgery Centers
AAHP American Association of Health Plans
ABN advance beneficiary notice
ABQAUR American Board of Quality Assurance and Utilization Review
ACE acute care episode
ACHCE American College of Health Care Executives
ACS American College of Surgeons
ADA Americans with Disabilities Act
ADC average daily census
ADL activities of daily living
ADT Admission/Discharge/Transfer
AHA American Hospital Association
AHIMA American Health Information Management Association
AHRQ Agency for Healthcare Research and Quality
AI average inventory
AIMR Association for Investment Management and Research
AIR assumed interest rate
ALE annualized loss expectancy
ALF assisted living facility
ALOS average length of stay
AMA American Medical Association
AMBAC AMBAC Indemnity Corporation
AMGA American Medical Group Association
ANSI American National Standards Institute
AP accounts payable
APA American Psychiatric Association
APC ambulatory payment classification
APG ambulatory payment group
APR annual percentage rate
AR accounts receivable
ASA American Society of Appraisers
ASC ambulatory surgery centers; also Accredited Standards Committee
ASHA American Surgical Hospital Association
ASO administrative services only
ASTC ancillary service technical component
ATM asynchronous transfer mode
AVG ambulatory visit group
BANTA best alternative to negotiated agreement
BBA Balanced Budget Act of 1997
BBRA Balanced Budget Refinement Act [1999]
BCP business continuity planning
BEA break-even analysis
BEP break-even point
BIPA Benefits Improvement and Protection Act [2000]
BLS Bureau of Labor Statistics
BPD border protection device
BS balance sheet
BSA Bank Secrecy Act
BVS business valuation standard
CA certificate authority
CAC Carrier Advisory Committee
CAS cost accounting standards
CASB Cost Accounting Standards Board
CC common criteria [for IT Security Evaluation —ISO/IEC 15408]; complication or comorbidity [for MS-DRGs]
CCA certified cost accountant
CCC cash conversion cycle
CCEVS common criteria evaluation and validation scheme
CCHIT Certification Commission for Healthcare Information Technology
CCU critical care unit
CDC Centers for Disease Control and Prevention
CDH consumer-directed healthcare
CDHP consumer-directed healthcare plan
CDPM Clinical Data Project Manager
CDSS clinical decision support system
CEO Chief Executive Officer
CF conversion factor
CFA Chartered Financial Analyst
CFO Chief Financial Officer
CFR Code of Federal Regulations
CHAMP Children’s Health and Medicare Protection Act of 2007
CHAMPUS Civilian Health and Medical Program of the Uniformed Services
CHE Certified Healthcare Executive
CHIPS Center for Healthcare Industry Performance Studies
CIA Corporate Integrity Agreement
CIO Chief Information Officer
CIP Customer Identification Program
CIS computer information systems
CLIA Clinical Laboratory Improvement Act
CLT capitation liability theory
CME continuing medical education
CMI case mix index
CMIO Chief Medical Information Officer
CMIS contribution margin income statement
CMN Certificate of Medical Necessity
CMP Certified Medical Planner ™
CMS Centers for Medicare and Medicaid Services [formerly HCFA]
COD cash on delivery
COGME Council of Graduate Medical Education
COH cash on hand
COLA cost of living allowance
CON Certificate of Need
COO Chief Operating Officer
COSO Committee of Sponsoring Organizations
COTS commercial off-the-shelf
CPHQ Certified Physician in Healthcare Quality
CPIM Certificate in Production and Inventory Management
CPI-U Consumer Price Index—urban
CPM critical (clinical) path method
CPOE computerized physician order entry [system]
CPR computer-based patient record
CPT current procedural terminology
CQI continuous quality improvement
CRL Certification Revocation List
CRM customer relationship management
CRVS California Relative Value Studies
CSO Chief Security Officer
CT scan computed tomography scan [also called CAT scan]
CUSIP Committee on Uniform Security Identification Procedures
Candid CIO: Will Weider, CIO of Ministry Health Care and Affinity Health System, offers his perspectives on administration issues in this blog.
Christina’s Considerations: Christina Thielst is a hospital and healthcare administrator and entrepreneur with a deep desire for continually improving the health of the community being served. This is her blog.
Healing Hospitals — Formerly Ask a Hospital President: F. Nicholas “Nick” Jacobs has more than 20 years experience in hospital management, with an acknowledged reputation for innovation and consumer-centered leadership.
Hospital Impact: Part of the Fierce network of health sites, this site is becoming popular among healthcare administrators for its news updates, tips and opinions on health care matters.
Leading the Way to Medical Excellence: the president of McLeod Health non-profit institutions provides weekly insights into his facilities and health care in general.
Let’s Talk Health Care: Bruce Bullen, Interim Chief Executive Officer at Harvard Pilgrim in Massachusetts, provides and open and ongoing conversation about health care administration.
Life as a Healthcare CIO: Dr. John Halamka records his experiences with infrastructure, applications, policies, management, and governance as he supports 3,000 doctors, 18,000 faculty and about three million patients.
Managed Care Matters: Joe Paduda shares his knowledge on managed care for group health, health policy, health research, and medical news for insurers, employers, and healthcare providers.
More than Medicine: Tom Quinn, president and CEO of Community General Hospital in Syracuse, New York, began his career as a hospital kitchen worker. His perspective on administration reflects his knowledge on how hospitals work from every angle.
Running a Hospital: A CEO of a large Boston hospital shares thoughts on hospitals, medicine and health care issues.
St. Joseph Medical Center: Chief Executive Officer at St. Joseph Medical Center in Missouri, Mr. Kashman, provides personal insight into administrative matters and general topics.
Todd’s Perspective: Todd Linden, president and CEO of Grinnell Regional Medical Center, offers insights into medical administration and guest bloggers provide insight into various departments.
Wachter’s World: This blog focuses on hospitals, hospitalists, quality, safety, policy and much more from Robert M. Wachter, MD, Professor and Associate Chairman of the Department of Medicine at the University of California, San Francisco.
Legal Matters
Drug and Device Law: This blog contains an attorney’s personal views (and those of several other Dechert attorneys) on topics that arise in the defense of pharmaceutical and medical device product liability litigation.
Drug Injury Watch: Learn more about drug injury lawsuits from an attorney who represents patients and their families.
FDA Law Blog: Hyman, Phelps & McNamara, P.C. is the largest dedicated food and drug law firm in the country. Their knowledge about laws and regulations governing drugs, medical devices, foods, dietary supplements, and cosmetics is helpful to anyone interested in these topics.
Health Care Law Blog: Bob Coffield’s expertise lies in helping businesses and health care providers weave through a variety of state and federal health care regulations and assisting them in business transactions.
Health Plan Law: This site contains information about group health plans, claims administration and related ERISA fiduciary issues. This site also contains tutorials.
HealthBlawg: this is David Harlow’s popular health care law blog, offering expert insights and easy-to-understand analysis.
Healthcare Law Blog: Holland & Hart’s healthcare practice provides insight into this arena, including HIPAA, Stark law, the Anti-kickback Statute and more.
HIPAA Blog: Join in on this discussion of medical privacy issues often buried in “political arcana.”
HIPAA, HiTech & HIT: This updated blog brings insight into legal issues, developments and other pertinent information that relates to the creation, use and exchange of electronic health records.
HIT Blawg: This blog is focused on national health information technology legal trends and current news on this topic.
Home Care Law Blog: Learn more about legal and policy issues in the home health care, private duty and hospice industries from Gilliland & Markette LLP.
Med Law Blog: This law blog focuses on topics that range from compliance to contracts and from employee benefits to HIPAA and HIT.
Physician Law: This blog provides and easy way to stay on top of current news, updates and useful tips relating to legal issues that affect physicians and non-institutional providers.
eHealth and Health IT
Chilmark Research: This blog provides perspectives on key IT trends in the healthcare sector.
davidrothman.net: David is the Information Services Specialist at the Community General Hospital Medical Library, but he also provides great ideas for 2.0 tools and tips for healthcare industry professionals on this blog.
e-CareManagement blog: Vince Kuraitis, owner of Better Health Technologies, LLC, has a passion for disease management and care coordination that dates back to 1995.
e-HealthExpert: A non-profit organization provides a free and open forum to support the development of expertise in the field of eHealth, Healthcare Information Systems, and Health IT (Clinical IT).
eHealth: John Sharp is an IT Manager for a major medical center in Northeast Ohio, with a focus on ehealth, personal health records, Web 2.0 technologies, Windows Sharepoint Services and project management.
Found In Cache: If you would prefer a professional’s take on social media matters, Web sites and all things technological, then follow Ed Bennett, a technology expert for a Maryland medical care system.
Future Health IT: A health IT and EPR advocate from the UK provides a format to discuss the future of health care and IT.
Informaticopia: This UK blogger provides eclectic news and views on health informatics and elearning.
MedGadget: Stay ahead of the gadget curve with this site, which offers information about the newest health care gadgets on the market as well as emerging medical technologies.
Neil Versel’s Healthcare IT Blog: A healthcare journalist’s provides his views on the major segment of the industry he covers — and, he provides a ton of links to other sites as well.
Schwartz Healthcare IT Blog: A variety of authors from Schwartz Communications provide insights into ways to use IT effectively within healthcare facilities.
The Health IT Channel: For a different perspective on IT and EHR as well as other health care issues, watch a few videos at this site.
The Healthcare IT Guy: The CEO of Netspective, a Java/.NET consultancy that specializes in healthcare IT with an emphasis on e-health, EMRs, data integration, and legacy modernization, supplies tips and information for physicians and healthcare administration.
ACKNOWLEDGEMENTS: To Mackenzie H. Marcinko PhD of iMBA Inc., Perry D’Alessio CPA CMP™ [Hon] New York, NY; and Daniel B. Moisand CFP®, Principal for Moisand Fitzgerald Tamayo, Melbourne, FL.
You can also listen to a professional narration of this article on iTunes & online.
ENCORE: March 22, 2004
A basic property of religion is that the believer takes a leap of faith: to believe without expecting proof. Often you find this property of religion in other, unexpected places – for example, in the stock market. It takes a while for a company to develop a “religious” following: only a few high-quality, well-respected companies with long track records ever become worshipped by millions of investors. My partner, Michael Conn, calls these “religion stocks.” The stock has to make a lot of shareholders happy for a long period of time to form this psychological link.
The stories (which are often true) of relatives or friends buying few hundred shares of the company and becoming millionaires have to fester a while for a stock to become a religion. Little by little, the past success of the company turns into an absolute – and eternal – truth. Investors’ belief becomes set: the past success paints a clear picture of the future.
Gradually, investors turn from cautious shareholders into loud cheerleaders. Management is praised as visionary. The stock becomes a one-decision stock: buy. This euphoria is not created overnight. It takes a long time to build it, and a lot of healthy pessimists have to become converted into believers before a stock becomes a “religion.”
Once a stock is lifted up to “religion” status, beware: Logic is out the window. Analysts start using T-bills to discount the company’s cash flows in order to justify extraordinary valuations. Why, they ask, would you use any other discount rate if there is no risk? When a T-bill doesn’t do the trick, suddenly new and “more appropriate” valuation metrics are discovered.
Other investors don’t even try to justify the valuation – the stock did well for me in the past, why would it stop working in the future? Faith has taken over the stock. Fundamentals became a casualty of “stock religion.” These stocks are widely held. The common perception is that they are not risky.
The general public loves these companies because they can relate to the companies’ brands. A dying husband would tell his wife, “Never sell _______ (fill in the blank with the company name).” Whenever a problem surfaces at a “religion stock,” it is brushed away with the comment that “it’s not like the company is going to go out of business.” True, a “religion stock” company is a solid leader in almost every market segment where it competes and the company’s products carry a strong brand name. However, one should always remember to distinguish between good companies and good stocks.
Coca-Cola is a classic example of a “religion stock.” There are very few companies that have delivered such consistent performance for so long and have such a strong international brand name as Coca-Cola. It is hard not to admire the company.
But admiration of Coca-Cola achieved an unbelievable level in the late nineties. In the ten years leading up to 1999, Coca-Cola grew earnings at 14.5% a year, very impressive for a 103-year-old company. It had very little debt, great cash flow and a top-tier management. This admiration came at a steep price: Coca-Cola commanded a P/E of 47.5. That P/E was 2.7 times the market P/E. Even after T-bills could no longer justify Coke’s valuation, analysts started to price “hidden” assets – Coke’s worldwide brand. No money manager ever got fired for owning Coca-Cola.
The company may not have had a lot of business risk. But in 1999, the high valuation was pricing in expectations that were impossible for any mature company to meet. “The future ain’t what it used to be” – Yogi Berra never lets us down. Success over a prolonged period of time brings a problem to any company – the law of large numbers.
Enormous domestic and international market share, combined with maturity of the soft drink market, has made it very difficult for Coca-Cola to grow earnings and sales at rates comparable to the pre-1999 years. In the past five years, earnings and sales have grown 2.5% and 1.5% respectively. After Roberto C. Goizueta’s death, Coke struggled to find a good replacement – which it acutely needed.
Old age and arthritis eventually catch up with “religion stocks.” No company can grow at a fast pace forever. Growth in earnings and sales eventually decelerates. That leads to a gradual deflation of the “religion” premium. For Coke, the descent from its “religious” status resulted in a drop of nearly 20% in the share price – versus an increase of 65% in the broad market over the same time. And at current prices, the stock still is not cheap by any means. It trades at 25 times December 2004 earnings, despite expectations for sales growth in the mid single digits and EPS growth in the low double digits.
It takes a while for the religion premium to be totally deflated because faith is a very strong emotion. A lot of frustration with sub-par performance has to come to the surface.
Disappointment chips away at faith one day at a time. “Religion” stocks are not safe stocks. The leap of faith and perception of safety come at a large cost: the hidden risk of reduction in the “religion premium.” The risk is hidden because it never showed itself in the past. “Religion” stocks by definition have had an incredibly consistent track record. Risk was rarely observed.
However, this hidden risk is unique because it is not a question of if it will show up but a question of when. It is very hard to predict how far the premium will inflate before it deflates – but it will deflate eventually. When it does, the damage to the portfolio can be huge.
Religion stocks generally have a disproportionate weight in portfolios because they are never sold – exposing the trying-to-be-cautious investor to even greater risks. Coca-Cola is not alone in this exclusive club. General Electric, Gillette, Berkshire Hathaway are all proud members of the “religion stock” club as well. Past members would include: Polaroid – bankrupt; Eastman Kodak – in a major restructuring; AT&T – struggling to keep its head above water. That stock is down from over $80 in 1999 to $18 today.
Emotions have no place in investing. Faith, love, hate, and disgust should be left for other aspects of our life. More often than not, emotions guide us to do the opposite of what we need to do to be successful. Investors need to be agnostic towards “religion stocks.” The comfort and false sense of certainty that those stocks bring to the portfolio come at a huge cost: prolonged under performance.
My thoughts today (20+ years later)
This is one of the first investment articles I ever wrote. I had just started writing for TheStreet.com. It’s interesting to read this article more than 20 years later. I am surprised my writing was not as bad as I had feared (though in many cases it was worse than I feared when I read my other early articles).
So much has happened since then – I am a different person today than I was back then. I have two more kids; I have written three more books and a thousand articles. The last two decades were my formative years as an investor and adult.
The goal of the article was not to make predictions but to warn readers that the long-term success of certain companies creates a cult-like following and deforms thinking. In fact, my original article – the one I submitted to TheStreet.com – did not mention any companies other than Coke. The editors wanted me to include more names so that the article would show up on more pages of Yahoo! Finance.
With the exception of Berkshire Hathaway, all of these companies have produced mediocre or horrible returns. In the best case, their fundamental returns in their old age were only a fraction of what they were when these companies were younger and the world was their oyster.
To my surprise, Coke’s stock is still trading at a high valuation. Its business has performed like the old-timer it is, with revenue and earnings growing by only 3–4% a year. The days of double-digit revenue and earnings growth were left in the 80s and 90s, though the high valuation remained.
Leverage ratios measure the amount of capital that comes from debt. In other words, leverage financial ratios are used to evaluate a company’s debt levels. Common leverage ratios include the following:
The debt ratio measures the relative amount of a company’s assets that are provided from debt:
Debt ratio = Total liabilities / Total assets
The debt to equity ratio calculates the weight of total debt and financial liabilities against shareholders’ equity:
Debt to equity ratio = Total liabilities / Shareholder’s equity
While health care is not “do-it-yourself,” an informed patient can be an asset. A poorly informed patient, on the other hand, clearly complicates treatment. Assume the responsibility of being the primary information source and educator for your patient. To help deal with a self-diagnosing patient, consider the following as suggested by: David B. Troxel, MD, Medical Consultant to The Doctors Company:
Encourage patients to always check with you about the accuracy of information obtained from external sources. Use the intake time to find out what Internet information the patient has found.
Directly discuss what the patient has read, even if the patient’s external source is a good one in your professional opinion. The exchange enhances your relationship with the patient and can increase treatment compliance. Welcome questions, and help put the patient’s information in the appropriate context.
Provide your patient with a list of Web sites that provide accurate information, such as the Centers for Disease Control and Prevention (www.cdc.gov). Make sure the patient understands the limitations of the Internet.
Document in the patient’s chart your diagnosis, your treatment management plan, and medication prescribed, as well as the reasons behind your decisions.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on February 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
ORIGINAL: May 2021 | Matt Cohlmia
As the future of healthcare becomes digitized, the threat of disruption to health systems has never been greater. Despite their best intentions, the flood of new competitors and ever-proliferating modalities of care each compete for patient attention, creating the potential for a fragmented, confusing, and impersonal patient experience. At the same time, health systems possess the breadth of care, the access to data, and the patient trust to become their community’s preferred partner in care.
But to achieve success, they must leverage these resources to create easy to navigate and personalized experiences for their patients, and for the first time ever, those are within reach.
Posted on February 11, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Life Insurance: A contract under which an insurance company promises, in exchange for premiums, to pay a set benefit when the policyholder dies.
Several factors will affect the cost and availability of life insurance, including age, health and the type and amount of insurance purchased. Life insurance policies have expenses, including mortality and other charges. If a policy is surrendered prematurely, the policyholder also may pay surrender charges and have income tax implications. You should consider determining whether you are insurable before implementing a strategy involving life insurance.
Any guarantees associated with a policy are dependent on the ability of the issuing insurance company to continue making claim payments.
Posted on February 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Term Insurance: Life insurance that provides coverage for a specific period. If the policyholder dies during that time, his or her beneficiaries receive the benefit from the policy. If the policyholder outlives the term of the policy, it is no longer in effect. Several factors will affect the cost and availability of life insurance, including age, health, and the type and amount of insurance purchased.
Life insurance policies have expenses, including mortality and other charges. If a policy is surrendered prematurely, the policyholder also may pay surrender charges and have income tax implications.
And, you should consider determining whether you are insurable before implementing a strategy involving life insurance. Any guarantees associated with a policy are dependent on the ability of the issuing insurance company to continue making claim payments.
Posted on January 21, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
According to colleague Dan Ariely PhD,Pre-Procurement Ownership is when you start to feel ownership over something before you actually have it. It’s like mentally moving into a house or car before you’ve signed the papers and moved in or driven away
This psychological quirk makes us more likely to commit to purchases because we’ve already imagined them as ours. Marketers exploit this by encouraging us to “try before you buy.”
So, next time you’re trying on a new men’s suit or woman’s skirt, be aware: your brain might already be claiming ownership.
Posted on December 29, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Habituation is your brain’s way of tuning out repetitive stimuli. It’s like background noise – after a while, you stop noticing it. This mental autopilot helps us focus on new and important information, but it can also make us overlook the familiar. It’s why you might not notice a smell in your house that’s obvious to a visitor.
To combat habituation, according to colleague Dan Ariely PhD, try changing up your routine and environment. Fresh experiences keep your brain engaged and alert.
Posted on December 23, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
DEFINED
***
***
Witness Stress is caused by witnessing a traumatic event and can lead to memory issues and confusion, affecting how accurately we remember details. This stress makes eyewitness testimonies more prone to error.
According to colleague Dan Ariily PhD, it highlights the role of stress in memory distortion and why additional support is often necessary for witnesses.
Posted on December 11, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Headline risk refers to the risk that a negative news media headline about one security issuer, incident or sector could affect the demand for and pricing of a much wider swath of securities, including those that have no direct relation to the securities headlined and whose fundamentals (defined above) remain intact.
Financial analyst Meredith Whitney’s appearance on “Sixty Minutes” in December 2010 was a classic example of the potential impact of headline risk, when her prediction of “a spate of municipal bond defaults” helped trigger a massive municipal bond market selloff, even though most municipal bonds actually faced no immediate default threat at that time, and the number of municipal defaults actually declined in the subsequent 12 months.
Achieving your financial, wealth and medical practice management goals is important, but handling everything on your own can be overwhelming. That’s where we come in. At D. E. Marcinko & Associates, our team of dual degree experienced physician advisors and medical consultants is here to guide you every step of the way. We believe in providing unbiased, high-quality financial and business advice.
For example, we offer a one-time written financial plan with oral evaluation for a flat fee with no ongoing sales or assets under management fees or commissions. Together, we can create a personalized financial plan tailored to your unique goals, empowering you to make confident, informed decisions as you navigate your financial future.
Other Services Include:
Estate Planning We have a network of qualified legal professionals that we can refer you to for state specific estate planning needs.
Tax Strategy We can work alongside your CPA for tax planning purposes. If needed, we can refer you to a qualified tax professional.
Investment Analysis If you have investments, we review your accounts to make sure they are aligned with your long-term goals.
401-k Allocations We evaluate your 401(k) allocations and provide recommendations that align with your goals.
Education Savings We help you explore the various ways to plan and save for education expenses.
Insurance & Risk Management We assess your insurance coverage to ensure it adequately protects you against potential risks; as well as evaluate and provide expert litigation witnesses, as needed.
Medical Practice Management We evaluate your current or potential medical practice to determine value and/or private equity offers or physician practice management formats [PPMC] for new, mid-career or retiring physicians, nurses and dentists.
D. E. Marcinko & Associates is unique and fully committed to all phases of a medical professionals personal and business life cycle. We are at your service 24/7: Email MarcinkoAdvisors@outlook.com
Posted on September 3, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
A quantum computer is a computer that exploits quantum mechanical phenomena. At small scales, physical matter exhibits properties of both particles and waves, and quantum computing leverages this behavior using specialized hardware. Classic physics cannot explain the operation of these quantum devices, and a scalable quantum computer could perform some calculations exponentially faster than any modern “classical” computer. In particular, a large-scale quantum computer could break widely used encryption schemes and aid physicists in performing physical simulations; however, the current state of the art is largely experimental and impractical.
The basic unit of information in quantum computing is the qubit, similar to the bit in traditional digital electronics. Unlike a classical bit, a qubit can exist in a superposition of its two “basis” states, which loosely means that it is in both states simultaneously. When measuring a qubit, the result is a probabilistic output of a classical bit. If a quantum computer manipulates the qubit in a particular way, wave interference effects can amplify the desired measurement results. The design of quantum algorithms involves creating procedures that allow a quantum computer to perform calculations efficiently and quickly.
Quantum Computing in Finance
Quantum-computing use cases in finance are slightly further in the future. The long-term promise of quantum computing in finance lies in portfolio and risk management.
Posted on April 27, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
FTC Votes 3-2 to Ban Non-Compete Agreements, but Legal Challenges Expected
The Federal Trade Commission (FTC) just voted 3-2 to issue a final rule striking new non-compete agreements for all workers and phasing out existing non-competes for all but senior executives across “most employers.” The ban does not apply to non-profits including many of the country’s healthcare provider organizations due to the limitations of the FTC’s jurisdiction, one of several points of contention that has been raised by hospital industry groups that have opposed the ban.
The final rule will take effect 120 days after its publication in the Federal Register. To be in compliance, impacted employers will need to stop enforcing existing non-competes with workers other than senior executives, inform those who are no longer bound by existing non-competes and stop initiating new non-competes for all workers going forward, FTC staff said during an open meeting on the final rule held last week.
Source: Dave Muoio, Fierce Healthcare [4/23/24]
Moreover, the stay-or-pay contract practice requires nurses to put in a certain amount of time “or be required to pay money to their employer for an alleged debt, which could be tied to so-called training, a sign-on bonus, or other costs their employer claims are related to their employment,” according to National Nurses United (NNU), a union that represents about a quarter of a million registered nurses (RNs).
“The new FTC rule is a step in the right direction for nurses and those aspiring to take on this critical role in our communities,” NNU President Nancy Hagans said in a statement.
Posted on March 28, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
NOBEL PRIZE WINNER AND FATHER OF BEHAVIORAL ECONOMICS
By Staff Reporters
DEFINITION: According to Wikipedia, behavioral economics is the study of the psychological, cognitive, emotional, cultural and social factors involved in the decisions of individuals or institutions, and how these decisions deviate from those implied by classical economic theory.
Behavioral economics is primarily concerned with the bounds of rationality of economic agents. Behavioral models typically integrate insights from psychology, neuroscience and microeconomic theory. The study of behavioral economics includes how market decisions are made and the mechanisms that drive public opinion.
Behavioral economics began as a distinct field of study in the 1970s and ’80s, but can be traced back to 18th-century economists, such as Adam Smith, who deliberated how the economic behavior of individuals could be influenced by their desires.
The status of behavioral economics as a subfield of economics is a fairly recent development; the breakthroughs that laid the foundation for it were published through the last three decades of the 20th century. Behavioral economics is still growing as a field, being used increasingly in research and in teaching.
***
***
Daniel Kahneman PhD, the father of behavioral economics, died yesterday at age 90 years old. He’s best known for applying psychology to economics and uncovering biases and mental shortcuts that make people act irrationally, as he chronicled in his best-selling book Thinking, Fast and Slow.
Kahneman, along with his long-time collaborator and friend Amos Tversky PhD, developed “prospect theory,” or loss-aversion theory, which earned him the Nobel Prize in Economics in 2002 (which he shared with fellow economist Vernon Smith). The idea is that people value losses and gains differently, so we feel more bad about losing $100 than we feel good about making the same amount. He applied this theory to investors, who had previously been considered rational decision-makers. It shows up elsewhere, too—for example, golfers putt better when they’re facing the loss of a stroke than when they might gain one.
Two other biases he identified include:
The “peak-end rule” that people remember an experience primarily based on how they felt at its most intense moment and the final part of it. It’s why you consider a whole vacation good if the last day was good—or the opposite.
The conjunction fallacy where people erroneously think the probability of two things being true is more likely than just one thing, which the famous “Linda the Bank Teller” problem illustrates.
[Human Nature, Medical and Financial Ethics and Modern Principles]
In any medical blog or investing treatise of gravitas, thoughts on human nature are usually placed at the end of the work, or an afterthought if included at all. However, we elected to prominently place this material as a stand alone feature. Why?
In the end, the success of any financial advisor or physician endeavor ultimately comes down to changing human behavior – helping a doctor/nurse/technician alter whatever s/he was doing toward something that will better allow them to avoid errors and pursue quality care and investing or practice management goals.
Yet, there is still remarkably little education or training for financial planners or medical professionals focused directly on motivation or change theory, in any related area except psychiatry/psychology or perhaps professional liability. Instead, doctors and advisors/planners are increasingly turning to professional consultants to learn best practices on how to help them actually make the behavioral changes necessary to achieve their medical quality improvement and client acquisition goals; as we attempt to answer these questions:
Are you and your medical practice, or financial advisory practice, ready for change?
How to transition from [traditional] solo practitioner B-models to modern forms?
What are leadership, management and governance?
In group practices, how is leadership shared?
What issues need be considered when hiring a financial planner or practice administrator or clinic CEO?
What is medical ethics and financial munificence? Why is it needed? How does it work?
What are the types of risk?
How are risks managed in the medical practice space or financial advisory eco-system?
In addition, medical and financial planning practitioners need to strive to avoid what Zenger and Folkman describe as the 10 most common leadership shortcomings based on a survey of 11,000 leaders. They include:
Lacks energy and enthusiasm
Accepts mediocre self performance
Lacks clear vision and direction
Poor judgment
Not collaboration
Not following standards
Resistant to new ideas
Doesn’t learn from mistakes
Lacks interpersonal skills
Fails to develop others.
Source: Zenger and Folkman: The Daily Stat: The 10 Most Common Failures of Business Leaders, Harvard Business Publishing, June 4, 2009.
Posted on November 23, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
***
Thanksgiving is a trading holiday. Both the New York Stock Exchange and the Nasdaq are closed. Black Friday, one of the biggest shopping days of the year, is a half day for the stock market. Both stock exchanges close at 1:00 p.m. ET, with eligible options trading until 1:15 p.m. Normal trading hours resume on the Monday after Thanksgiving, also known as Cyber Monday, when many online retailers host major sales.
***
***
Thanks to plummeting prices at the pump, US drivers will save a collective $1.2 billion this Thanksgiving travel period, and day, compared to last year, according to GasBuddy. The average price per gallon is down nearly 46 cents from a year ago, and more than 50,000 stations now show gas prices at $2.99/gallon or less.
***
Narrow traffic lanes are safer than wide ones. Researchers at Johns Hopkins analyzed more than 1,000 streets in seven major cities across the US and found that narrower roads mitigated traffic collisions in certain conditions. The study did not find a significant difference between roads 9-feet wide and those 10- or 11-feet wide, but it did conclude that traffic accidents increase 1.5x when a road widens from 9 feet to 12 feet. Traffic fatalities are the leading cause of death for Americans aged 1–54.
***
Walgreens will close most of its pharmacies and stores on Thanksgiving Day for the first time in the company’s history, executives said last Thursday. The move to close more than 8,700 stores for the federal holiday comes as some Walgreens workers staged a three-day walkout this fall to push for improved working conditions and increased staffing numbers, Reuters reported.
***
***
Here is where the major benchmarks ended on Wednesday:
The S&P 500 Index was up 18.43 points (0.4%) at 4,556.62, near a four-month high close; the Dow Jones Industrial Average®(DJI) was up 184.74 points (0.5%) at 35,273.03; the NASDAQ Composite was up 65.88 points (0.5%) at 14,265.86.
The 10-year Treasury note yield (TNX) was down about 1 basis point at 4.41%, after earlier dropping to a two-month low under 4.37%.
CBOE Volatility Index (VIX) was down 0.50 at 12.85.
Communications services and technology were among the strongest performers Wednesday. Food and beverage companies were also firm. Energy shares were among the weakest performers Wednesday behind a drop of over 1% in WTI Crude Oil futures (/CL). ), which fell following reports OPEC delayed a weekend meeting until November 30th, a possible reflection of cartel members struggling to reach consensus over production cuts. WTI crude ended just under $77 a barrel, down 19% from a 2023 high above $95 in late October.
Posted on September 15, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
Public Company Accounting Oversight Board
By Staff Reporters
DEFINITION: The Public Company Accounting Oversight Board (PCAOB) is a Congressionally-established nonprofit that assesses audits of public companies in the United States to protect investors’ interests. The PCAOB also oversees broker-dealer audits, including compliance reports filed under federal securities laws. In addition, the PCAOB establishes auditing and related professional practice standards for registered public accounting firms to help prepare and issue audit reports. The firms registered with the PCAOB range in size from sole proprietorships to large global organizations.
And now, audit quality declined for a second straight year, the PCAOB announced last week. Around 40% of the audit firms it inspected in 2022 had Part I.A deficiencies, “up from 34% in 2021 and 29% in 2020. Deficiencies are mentioned in Part I.A of an inspection report when the PCAOB finds that an audit firm did not present sufficient evidence to back up its opinion on a “company’s financial statements and/or internal controls over financial reporting.”.
PCAOB Chair Erica Williams expressed disappointment with the findings in a statement. “Let me be clear: a 40% Part I.A deficiency rate is completely unacceptable,” she said. “The PCAOB will continue demanding firms do better and deliver the high-quality audits investors deserve.”
Williams asked investors to encourage audit committees to choose auditors with “proven track records on quality,” and pointed them to resources on the PCAOB’s website that let viewers see and compare audit firms’ deficiency rates.
Posted on January 21, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
As the US just crashed into the $31.4 trillion debt ceiling as the Treasury Department began taking what it called “extraordinary measures” to prevent the government from defaulting on its debts and sparking an economic crisis.
These measures are a series of deep-cut accounting moves that allow the Treasury to continue making its payments. They include:
Suspending reinvestments into government funds for retired federal employees, such as the Civil Service Retirement and Disability Fund.
Selling existing investments in those funds to free up more outstanding debt.
And while these measures definitely aren’t ordinary…they probably aren’t so “extra,” either. The Treasury has resorted to them more than 12 times since 1985, including during the last debt-ceiling standoff in 2021.
Still, these steps amount to chugging water after eating a ghost pepper—the pain will return. Treasury Secretary Janet Yellen said her extraordinary measures will last through early June, giving lawmakers about five months to work out a deal to raise the debt ceiling.
NOTE: The US has never defaulted on its debt, but even the threat of it could be disastrous. The country’s first credit downgrade in history came during a debt-ceiling showdown in 2011.
Posted on July 30, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
What is stop-loss insurance AND how does it work?
By Staff Reporters
***
***
A stop-loss health insurance policy covers claims above a health insurance plan’s retained claims. The claims fund of a self-funded employer will pay claims up to the predetermined deductible for each of the company’s covered employees. The role of the stop-loss is to cover all claims above these deductible levels.
According to RoundStone Insurance, aggregate stop-loss insurance is designed to protect an employer who self-funds their employee health plan from higher-than-anticipated payouts for claims. Stop-loss insurance is similar to high-deductibleinsurance, and the employer remains responsible for claims below the deductible amount.
An individual stop-loss insurance carrier determines the average expected monthly claims per employee / per month PEPM based on the employer’s history. Then, this figure is multiplied by a percentage ranging from 110%-150%. That determined amount is then multiplied by the enrollment on a monthly basis to establish the aggregate deductible.
“Physicians who don’t understand modern risk management, insurance, business, and asset protection principles are sitting ducks waiting to be taken advantage of by unscrupulous insurance agents and financial advisors; and even their own prospective employers or partners. This comprehensive volume from Dr. David Marcinko and his co-authors will go a long way toward educating physicians on these critical subjects that were never taught in medical school or residency training.” —Dr. James M. Dahle, MD, FACEP, Editor of The White Coat Investor, Salt Lake City, Utah, USA
“With time at a premium, and so much vital information packed into one well organized resource, this comprehensive textbook should be on the desk of everyone serving in the healthcare ecosystem. The time you spend reading this frank and compelling book will be richly rewarded.” —Dr. J. Wesley Boyd, MD, PhD, MA, Harvard Medical School, Boston, Massachusetts, USA
“Physicians have more complex liability challenges to overcome in their lifetime, and less time to do it, than other professionals. Combined with a focus on practicing their discipline, many sadly fail to plan for their own future. They need trustworthy advice on how to effectively protect themselves, their family, and their practice from the many overt and covert risks that could potentially disrupt years of hard work.
Fortunately, this advice is contained within Risk Management, Liability Insurance, and Asset Protection Strategies for Doctors and Advisors: Best Practices from Leading Consultants and Certified Medical Planners™. Written by Dr. David Edward Marcinko, Nurse Hope Rachel Hetico, and their team of risk managers, accountants, insurance agents, attorneys, and physicians, it is uniquely positioned as an integration of applied, academic, and peer-reviewed strategies and research, with case studies from top consultants and Certified Medical Planners™. It contains the latest principles of risk management and asset protection strategies for the specific challenges of modern physicians. My belief is that any doctor who reads and applies even just a portion of this collective wisdom will be fiscally rewarded. The Institute of Medical Business Advisors has produced another outstanding reference for physicians that provide peace of mind inthis unique marketplace! In my opinion, it is a mandatory read for all medical professionals.” —David K. Luke, MS-PFP, MIM, CMP™, Net Worth Advisory Group, Inc., Sandy, Utah, USA
“This book is a well-constructed, comprehensive, and experiential view of risk management throughout the entire medical practice life-cycle. It is organized in an accessible, high-yield style that is familiar to doctors. Each chapter has case models, examples, insider tips, and useful pearls. I was pleased to see multi-degreed physicians sharing their professional experiences in a textbook on something other than clinical medicine. I can’t decide if this book is right on – over the top – or just plain prescient. Now, after a re-read, I conclude it is all of the above; and much more.” —Dr. Peter P. Sidoriak, Pottsville, Pennsylvania, USA
“When a practicing physician thinks about the risk exposure resulting from providing patient care, medical malpractice risk immediately comes to mind. But, malpractice and liability risk are barely the tip of the iceberg, and likely not even the biggest risk in the daily practice of medicine. There are risks from having medical records to keep private, risks related to proper billing and collections, risks from patients tripping on your office steps, risks from medical board actions, risk arising from divorce, and the list goes on and on. These liabilities put a doctor’s hard earned assets and career in a very vulnerable position. This new book from Dr. David Marcinko and Prof. Hope Hetico shows doctors the multiple types of risk they face and provides examples of steps to take to minimize them. It is written clearly and to the point, and is a valuable reference for any well-managed practice. Every doctor who wants to take preventive action against the risks coming at them… from all sides needs to read this book.” —Richard Berning, MD, FACC, New Haven, Connecticut, USA
“This is an excellent companion book to Dr. Marcinko’s Comprehensive Financial Planning Strategies For Doctors and Advisors: Best Practices from Leading Consultants and Certified Medical Planners™. It is all inclusive, yet easy to read, with current citations, references, and much frightening information. I highly recommend this text. It is a fine educational and risk management tool for all doctors and medical professionals.”—Dr. David B. Lumsden, MD, MS, MA, Orthopedic Surgeon, Baltimore, Maryland, USA
“This comprehensive text book provides an in-depth presentation of the cyber security and real risk management, asset protection, and insurance issues facing all medical professions today. It is far beyond the mere medical malpractice concerns I faced when originally entering practice decades ago.” —Dr. Barbara s. Schlefman, DPM, MS, Family Foot Care, PA, Tucker, Georgia, USA
“Am I over-insured and thus wasting money? Am I under-insured and thus at risk for a liability or other disaster? I never really had the means of answering these questions; until now.” —Dr. Lloyd M. Krieger, MD, MBA, Rodeo Drive Plastic Surgery, Beverly Hills, California, USA
“I read and use this book and several others from Dr. David Edward Marcinko and his team of advisors.” —Dr. John Kelley, DO, Orthopedic Surgeon, Tucker, Georgia, USA
“An important step in the risk management, insurance planning, and asset protection process is the assessment of needs. One can create a strong foundation for success only after all needs have been analyzed so that a plan can be constructed and then implemented. This book does an excellent job of recognizing those needs and addressing strategies to reduce them.“ —Shikha Mittra, MBA, CFP®, CRPS®, CMFC®, AIF®, President – Retire Smart Consulting LLC, Princeton, New Jersey, USA
“The Certified Medical Planner™ professional designation and education program was created by the Institute of Medical Business Advisors Inc., and Dr. David Edward Marcinko and his team (who wrote this book). It is intended for financial advisors who aim specifically to serve physicians and the medical community. Content focuses not only on the insurance and professional liability issues relevant to physicians, but also provides an understanding of the risky business of medical practice so advisors can help work more successfully with their doctor-clients.” —Michael E. Kitces, MSFS, MTAX, CFP®, CLU, ChFC, RHU, REBC, CASL Reston, Virginia, USA
“I have read this text and used consulting services from the Institute of Medical Business of Advisors, Inc. on several occasions.” —Dr. Marsha Lee, DO, Radiologists, Norcross, Georgia, USA
“The medical education system is grueling and designed to produce excellence in medical knowledge and patient care. What it doesn’t prepare us for are the slings and arrows that come our way once we actually start practicing medicine. Successfully avoiding these land mines can make all the difference in the world when it comes to having a fulfilling practice. Given the importance of risk management and mitigation, you would think these subjects would be front and center in both medical school and residency – ‘they aren’t.’ Thankfully, the brain trust over at iMBA Inc. has compiled this comprehensive guide designed to help you navigate these mine fields so that you can focus on what really matters – patient care.” —Dennis Bethel, MD, Emergency Medicine Physician
To start, let us all recall the Canadian physician Sir William Osler MD, one of the founders of Johns Hopkins Hospital in my hometown of Baltimore Maryland, and where I played stickball in the parking lot as a kid. He left a sizeable body of wisdom that has guided many physicians in the practice of medicine. So, allow me to share with you some of that accumulated wisdom and the quotes that have served me well over the years.
From Dr. Osler, I learned the art of putting myself in the patient’s shoes. “The motto of each of you as you undertake the examination and treatment of a case should be ‘put yourself in his place.’ Realize, so far as you can, the mental state of the patient, enter into his feelings.” Osler further stresses that we should “scan gently (the patient’s) faults” and offer the “kindly word, the cheerful greeting, the sympathetic look.”1
“In some of us, the ceaseless panorama of suffering tends to dull that fine edge of sympathy with which we started,” writes Osler in his famous essay “Aequanimitas.”2 “Against this benumbing influence, we physicians and nurses, the immediate agents of the Trust, have but one enduring corrective — the practice towards patients of the Golden Rule of Humanity as announced by Confucius: ‘What you do not like when done to yourself, do not do to others.’”
Medicine can be both art and science as many physicians have discovered. As Osler tells us, “Errors in judgment must occur in the practice of an art which consists largely of balancing probabilities.”2 Osler notes that “Medicine is a science of uncertainty and an art of probability” and also weighs in with the idea that “The practice of medicine is an art, based on science.”3,4
Osler emphasized that excellence in medicine is not an inheritance and is more fully realized with the seasoning of experience. “The art of the practice of medicine is to be learned only by experience,” says Osler. “Learn to see, learn to hear, learn to feel, learn to smell, and know that by practice alone can you become expert.”5
Finally, some timeless wisdom on patient care came from Osler in an address to St. Mary’s Hospital Medical School in London in 1907: “Gain the confidence of a patient and inspire him with hope, and the battle is half won.”6
***
***
Osler has also imparted plenty of advice on the business of medicine. In “Aequanimitas,” Osler says there are only two types of doctors: “those who practice with their brains, and those who practice with their tongues.”7
In a valedictory address to medical school graduates at McGill University, Osler suggested treating money as a side consideration in a medical career.8 “You have of course entered the profession of medicine with a view of obtaining a livelihood; but in dealing with your patients let this always be a secondary consideration.”
“You are in this profession as a calling, not as a business: as a calling which exacts from you at every turn self-sacrifice, devotion, love and tenderness to your fellow man,” explains Osler in the address to St. Mary’s Hospital Medical School.6 “Once you get down to a purely business level, your influence is gone and the true light of your life is dimmed. You must work in the missionary spirit, with a breadth of charity that raises you far above the petty jealousies of life.”
It is not easy for doctors to combine a passion for patient care, a knowledge of science and the maintenance of business, according to Osler in the British Medical Journal.9 “In the three great professions, the lawyer has to consider only his head and pocket, the parson the head and heart, while with us the head, heart, and pocket are all engaged.”
While some aspects of practice may fall short or be devoid of appropriate financial remuneration, the giving of one’s time, expertise and experience in improving patient outcomes and the quality of their lives may be the greatest gift. “The ‘good debts’ of practice, as I prefer to call them … amount to a generous sum by the end of each year,” says Osler.9
And so, as you practice medicine and reflect on your career, always remember the words and wisdom of Dr. William Osler, and keep patient welfare as your first priority.
References
1. Penfield W. Neurology in Canada and the Osler centennial. Can Med Assoc J. 1949; 61(1): 69-73
2. Osler W. Aequanimitas. Chapter 9, P. Blakiston’s Son and Co., Philadelphia, 1925, p. 159
3. Bean WB. William Osler: Aphorisms, CC Thomas, Springfield, IL, p. 129.
4. Osler W. Aequanimitas. Chapter 3, P. Blakiston’s Son and Co., Philadelphia, 1925, p. 34
5. Thayer WS. Osler the teacher. In: Osler and Other Papers. Johns Hopkins Press, Baltimore, 1931, p. 1.
6. Osler W. The reserves of life. St. Mary’s Hosp Gaz. 1907;13 (1):95-8.
7. Osler W. Aequanimitas. Chapter 7, P. Blakiston’s Son and Co., Philadelphia, 1925, p. 124
8. Osler W. Valedictory address to the graduates in medicine and surgery, McGill University. Can Med Surg J. 1874; 3:433-42.
9. Osler W. Remarks on organization in the profession. Brit Med J. 1911; 1(2614):237-9.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
A couple years ago you posted an earlier version of the attached Asset Protection Outline. I updated it to include quite a bit more discussion of different protection levels for various kinds of accounts, and included more discussion of states other than Ohio, including a 50 state chart with IRA/403b protections.
So please delete the old one and replace with this one which contains more topics, including some substantial discussion of issues regarding current class action litigation jeopardizing asset protection for Schwab and Merrill Lynch IRAs.
Regards Ed
###
The Importance of Asset Protection as Part of Financial and Estate Planning for Doctor’s and Medical Professionals
Asset Protection has become a ubiquitous buzz-word in the legal and financial community. It often means different things to different people. It may encompass anything from buying umbrella liability insurance to funding offshore trusts.
What is most likely to wipe out a client’s entire net worth? An investment scam, investment losses, a lawsuit, divorce or long-term health care expenses? “Asset Protection” may be construed to address all of these scenarios, but this outline will cover risk from non-spousal creditors as opposed to risk from bad investments, divorce, medical bills or excessive spending. Prudent business practice and limited liability entity use (LP, LLP, LLC, Corporation, etc) is the first line of defense against such risks. Similarly, good liability insurance and umbrella insurance coverage is paramount.
However, there is a palpable fear among many of frivolous lawsuits and rogue juries [especially among physicians and medical professionals]. Damages may exceed coverage limits. Moreover, insurance policies often have large gaps in coverage (e.g. intentional torts, “gross” negligence, asbestos or mold claims, sexual harassment).
As many doctors in Ohio know all too well, malpractice insurance companies can fail, too. Just as we advise clients regarding legal ways to legitimately avoid income and estate taxes or qualify for benefits, so we advise how to protect family assets from creditors. Ask your clients, “What level of asset protection do you want for yourself?
For the inheritance you leave to your family?” Do any clients answer “none” or “low”? Trusts that are mere beneficiary designation form or POD/TOD substitutes are going out of style in favor of “beneficiary-controlled trusts”, “inheritance trusts” and the like.
Table of Contents
While effort is made to ensure the material is accurate, this material is not intended as legal advice and no one may rely on it as such. Sections II(d), II(i), V, VI and XI were updated Feb 2012, but much of the material and citations have not been verified since 2010. Permission to reprint and share with fellow bar members is granted, but please contact author for updates if more than a year old.
T.O.C. [Page Number]
I. Importance of Asset Protection 2
II. State and Federal Protections Outside ERISA or Bankruptcy 4
a. Non-ERISA Qualified Plans: SEP, SIMPLE IRAs 5
b. Traditional and Roth IRAs, “Deemed IRAs” 7
c. Life Insurance 9
d. Long-Term Care, Accident/Disability Insurance 13
e. Non-Qualified Annuities 13
f. Education IRAs (now Coverdell ESAs) 16
g. 529 Plans 17
h. Miscellaneous State and Federal Benefits 18
i. HSAs, MSAs, FSAs, HRAs 18
III. Federal ERISA Protection Outside Bankruptcy 20
IV. Federal Bankruptcy Scheme of Creditor Protection 26
V. Non-Qualified Deferred Comp – Defying Easy Categorization 30
VI. Breaking the Plan – How Owners Can Lose Protection 32
(incl Prohibited Transactions and Schwab/Merrill Lynch IRA problems) 35
VII. Post-Mortem – Protections for a Decedent’s Estate 51
VIII. Post-Mortem – State Law Protections for Beneficiaries 52
IX. Post-Mortem – Bankruptcy Protections for Beneficiaries 54
X. Dangers and Advantages of Inheriting Through Trusts 56
XI. Piercing UTMA/UGMA and Other Third Party Created Trusts 59
XII. Exceptions for Spouses, Ex-Spouses and Dependents 61
XIII. Exceptions when the Federal Government (IRS) is Creditor 62
XIV. Fraudulent Transfer (UFTA) and Other Exceptions 68
XV. Disclaimer Issues – Why Ohio is Unique 69
XVI. Medicaid/Government Benefit Issues 71
XVII. Liability for Advisors 72
XVIII. Conflicts of Law – Multistate Issues 73
XIX. Conclusions 75
Appendices
A. Ohio exemptions – R.C. §2329.66 (excerpt), §3911.10, §3923.19 78
B. Bankruptcy exemptions – 11 U.S.C. § 522 excerpts 80
C. Florida IRA exemption – Fla Stat. § 222.21 (note-may be outdated) 85
D. Sal LaMendola’s Inherited IRA Win/Loss Case Chart 86
E. Multistate Statutory Debtor Exemption Chart 88
###
Assessment
This outline will discuss the sometimes substantial difference in legal treatment and protection for various investment vehicles and retirement accounts, with some further discussion of important issues to consider when trusts receive such assets.
Beware of general observations like: “retirement plans, insurance, IRAs and annuities are protected assets” – that may often be true, but Murphy’s law will make your client the exception to the general rules. The better part of this outline is pointing out those exceptions.
Mr. Edwin P. Morrow III, a friend of the Medical Executive-Post, is a Wealth Specialist and Manager, Wealth Strategies Communications Ohio State Bar Association Certified Specialist, Estate Planning, Probate and Trust Law Key Private Bank Wealth Advisory Services. 10 W. Second St., 27th Floor Dayton, OH 45402. He is an ME-P “thought leader”.
Constructive criticism or other comments welcome.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on June 23, 2014 by Dr. David Edward Marcinko MBA MEd CMP™
Sensitive Data for Sale
[By Dr. David Edward Marcinko MBA]
I received this email recently. Are you as incensed over it, as I? OR, am I being overly sensitive? Feel free to call or email John Edward, the sender, to tell him what you think: pro or con?
Hi ME-P,
I’m writing to check if you would be interested in reaching Physicians or Healthcare Executives?
We at AccurateB2Blist maintain a permission passed email list for physician practitioners with NPI numbers.
Our Lists
Below given are few additional lists we maintain within Medical Industry
Nurses
Dentists
Veterinarians
Healthcare Executives Email List
Physicians – Offices and Clinics of Doctors of Medicine
Physicians – Offices and Clinics of Doctors of Osteopathy
Doctors, Physicians and Surgeons Email List with NPI Number
Healthcare executives: 518,900 out of which 123,200 contacts are senior management level contacts.
Assessment
Please let me know if you would like to discuss further on your target audience? Looking forward to hearing from you. And, please do not print this email unless it is absolutely necessary. To opt out reply with ‘Leave out’ in the subject line!
By John Edward [Business Development Executive] AccurateB2Blist
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES: