BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Investment bankers are not really bankers at all. The fact that the word banker appears in the name is partially responsible for the false impressions that exist in the medical community regarding the functions they perform.
For example, they are not permitted to accept deposit, provide checking accounts, or perform other activities normally construed to be commercial banking activities. An investment bank is simply a firm that specializes in helping other corporations obtain money they need under the most advantageous terms possible. When it comes to the actual process of having securities issued, the corporation approaches an investment banking firm, either directly, or through a competitive selection process and asks it to act as adviser and distributor.
Investment bankers, or under writers, as they are sometimes called, are middlemen in the capital markets for corporate securities. The corporation requiring the funds discusses the amount, type of security to be issued, price and other features of the security, as well as the cost to issuing the securities. All of these factors are negotiated in a process known as negotiated underwriting. If mutually acceptable terms are reached, the investment banking firm will be the middle man through which the securities are sold to the general public. Since such firms have many customers, they are able to sell new securities, without the costly search that individual corporations may require to sell its own security.
Thus, although the firm in need of additional capital must pay for the service, it is usually able to raise the additional capital at less expense through the use of an investment banker, than by selling the securities itself. The agreement between the investment banker and the corporation may be one of two types. The investment bank may agree to purchase, or underwrite, the entire issue of securities and to re-offer them to the general public. This is known as a firm commitment.
When an investment banker agrees to underwrite such a sale; it agrees to supply the corporation with a specified amount of money. The firm buys the securities with the intention to resell them. If it fails to sell the securities, the investment banker must still pay the agreed upon sum.
Thus, the risk of selling rests with the underwriter and not with the company issuing the securities.
The alternative agreement is a best efforts agreement in which the investment banker makes his best effort to sell the securities acting on behalf of the issuer, but does not guarantee a specified amount of money will be raised. When a corporation raises new capital through a public offering of stock, one might inquire where the stock comes from. The only source the corporation has is authorized, but previously un-issued stock. Anytime authorized, but previously un-issued stock (new stock) is issued to the public, it is known as a primary offering.
If it’s the very first time the corporation is making the offering, it’s also known as the Initial Public Offering (IPO). Anytime there is a primary offering of stock, the issuing corporation is raising additional equity capital.
A secondary offering, or distribution, on the other hand, is defined as an offering of a large block of outstanding stock. Most frequently, a secondary offering is the sale of a large block of stock owned by one or more stockholders. It is stock that has previously been issued and is now being re-sold by investors. Another case would be when a corporation re-sells its treasury stock.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
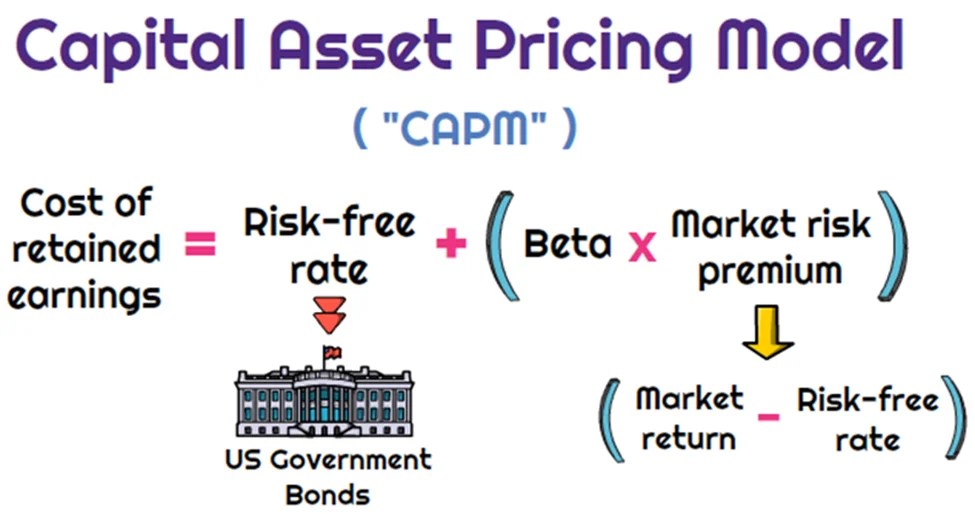
Dr. Harry Markowitz is credited with developing the framework for constructing investment portfolios based on the risk-return tradeoff. William Sharpe, John Lintner, and Jan Mossin are credited with developing the Capital Asset Pricing Model (CAPM).
CAPM is an economic model based upon the idea that there is a single portfolio representing all investments (i.e., the market portfolio) at the point of the optimal portfolio on the Capital Market Line (CML) and a single source of systematic risk, beta, to that market portfolio. The resulting conclusion is that there should be a “fair” return investors should expect to receive given the level of risk (beta) they are willing to assume.
The excess return, or return above the risk-free rate, that may be expected from an asset is equal to the risk-free return plus the excess return of the market portfolio times the sensitivity of the asset’s excess return to the market portfolio excess return. Beta, then, is a measure of the sensitivity of an asset’s returns to the market as a whole. A particular security’s beta depends on the volatility of the individual security’s returns relative to the volatility of the market’s returns, as well as the correlation between the security’s returns and the markets returns.
While a stock may have significantly greater volatility than the market, if that stock’s returns are not highly correlated with the returns of the overall market (i.e., the stock’s returns are independent of the overall market’s returns), then the stock’s beta would be relatively low. A beta in excess of 1.0 implies that the security is more exposed to systematic risk than the overall market portfolio, and likewise, a beta of less 1.0 means that the security has less exposure to systematic risk than the overall market.
MPT has helped focus investors on two extremely critical elements of investing that are central to successful investment strategies.
First, MPT offers the first framework for investors to build a diversified portfolio. Furthermore, an important conclusion that can be drawn from MPT is that diversification does in fact help reduce portfolio risk.
Thus, MPT approaches are generally consistent with the first investment rule of thumb, “understand and diversify risk to the extent possible.”
Additionally, the risk/return tradeoff (i.e., higher returns are generally consistent with higher risk) central to MPT based strategies has helped investors recognize that if it looks too good to be true, it probably is.
Passive Investing
Passive investing is a monetary plan in which an investor invests in accordance with a pre-determined strategy that doesn’t necessitate any forecasting of the economy or an individual company’s prospects. The primary premise is to minimize investing fees and to avoid the unpleasant consequences of failing to correctly predict the future. The most accepted method to invest passively is to mimic the performance of a particular index. Investors typically do this today by purchasing one or more ‘index funds’. By tracking an index, an investor will achieve solid diversification with low expenses.
An ivestor could potentially earn a higher rate of return than an investor paying higher management fees. Passive management is most widespread in the stock markets. But with the explosion of exchange traded funds on the major exchanges, index investing has become more popular in other categories of investing. There are now literally hundreds of different index funds.
Passive management is based upon the Efficient Market Hypothesis theory. The Efficient Market Hypothesis (EMH) states that securities are fairly priced based on information regarding their underlying cash flows and that investors should not anticipate to consistently out-perform the market over the long-term.
The Efficient Market Hypothesis evolved in the 1960s from the Ph.D. dissertation of Eugene Fama. Fama persuasively made the case that in an active market that includes many well-informed and intelligent investors, securities will be appropriately priced and reflect all available information. If a market is efficient, no information or analysis can be expected to result in out-performance of an appropriate benchmark. There are three distinct forms of EMH that vary by the type of information that is reflected in a security’s price:
Weak Form
This form holds that investors will not be able to use historical data to earn superior returns on a consistent basis. In other words, the financial markets price securities in a manner that fully reflects all information contained in past prices.
Semi-Strong Form
This form asserts that security prices fully reflect all publicly available information. Therefore, investors cannot consistently earn above normal returns based solely on publicly available information, such as earnings, dividend, and sales data.
Strong Form
This form states that the financial markets price securities such that, all information (public and non-public) is fully reflected in the securities price; investors should not expect to earn superior returns on a consistent basis, no matter what insight or research they may bring to the table.
While a rich literature has been established regarding whether EMH actually applies in any of its three forms in real world markets, probably the most difficult evidence to overcome for backers of EMH is the existence of a vibrant money management and mutual fund industry charging value-added fees for their services.
The notion of passive management is counterintuitive to many investors. Passive investing proponents follow the strong market theory of EMH. These proponents argue several points including;
In the long term, the average investor will have a typical before-costs performance equal to the market average. Therefore the standard investor will gain more from reducing investment costs than from attempting to beat the market over time.
The efficient-market hypothesis argues that equilibrium market prices fully reflect all existing market information. Even in the case where some of the market information is not currently reflected in the price level, EMH indicates that an individual investor still cannot make use of that information. It is widely interpreted by many academics that to try and systematically “beat the market” through active management is a fools game.
Not everyone believes in the efficient market. Numerous researchers over the previous decades have found stock market anomalies that indicate a contradiction with the hypothesis. The search for anomalies is effectively the hunt for market patterns that can be utilized to outperform passive strategies. Such stock market anomalies that have been proven to go against the findings of the EMH theory include;
Low Price to Book Effect
January Effect
The Size Effect
Insider Transaction Effect
The Value Line Effect
All the above anomalies have been proven over time to outperform the market. For example, the first anomaly listed above is the Low Price to Book Effect. The first and most discussed study on the performance of low price to book value stocks was by Dr. Eugene Fama and Dr. Kenneth R. French. The study covered the time period from 1963-1990 and included nearly all the stocks on the NYSE, AMEX and NASDAQ. The stocks were divided into ten subgroups by book/market and were re-ranked annually. In the study, Fama and French found that the lowest book/market stocks outperformed the highest book/market stocks by a substantial margin (21.4 percent vs. 8 percent). Remarkably, as they examined each upward decile, performance for that decile was below that of the higher book value decile. Fama and French also ordered the deciles by beta (measure of systematic risk) and found that the stocks with the lowest book value also had the lowest risk.
Today, most researchers now deem that “value” represents a hazard feature that investors are compensated for over time. The theory being that value stocks trading at very low price book ratios are inherently risky, thus investors are simply compensated with higher returns in exchange for taking the risk of investing in these value stocks. The Fama and French research has been confirmed through several additional studies. In a Forbes Magazine 5/6/96 column titled “Ben Graham was right–again,” author David Dreman published his data from the largest 1500 stocks on Compustat for the 25 years ending 1994. He found that the lowest 20 percent of price/book stocks appreciably outperformed the market.
One item a medical professional should be aware of is the strong paradox of the efficient market theory. If each investor believes the stock market were efficient, then all investors would give up analyzing and forecasting. All investors would then accept passive management and invest in index funds. But if this were to happen, the market would no longer be efficient because no one would be scrutinizing the markets. In actuality, the efficient market hypothesis actually depends on active investors attempting to outperform the market through diligent research.
The case for passive investing and in favor of the EMH is that a preponderance of active managers do actually underperform the markets over time. The latest study by Standard and Poor’s (S&P) confirms this fact. S&P recently compared the performance of actively-managed mutual funds to passive market indexes twice per year. The 2012 S&P study indicated that indexes were once again outperforming actively-managed funds in nearly every asset class, style and fund category. The lone exception in the 2012 report was international equity, where active outperformed the index that S&P chose. The study examined one-year, three-year and five-year time periods. Within the U.S. equity space, active equity managers in all the categories failed to outperform the corresponding benchmarks in the past five year period. More than 65 percent of the large-cap active managers lagged behind the S&P 500 stock index. More than 81 percent of mid-cap mutual funds were outperformed by the S&P MidCap 400 index.
Lastly, 77 percent of the small-cap mutual funds were outperformed by the S&P SmallCap 600 index. U.S. bond active managers fared no better that equity managers over a five year period. More than 83 percent of general municipal mutual funds under-performed the S&P National AMT-Free Municipal Bond index, 93 percent of government long-term funds under-performed the Barclays Long Government index, nearly 95 percent of high yield corporate bond funds under-performed the Barclays High Yield index. Although the performance measurements for index investing are very strong, many analysts find three negative elements of passive investing;
Downside Protection: When the stock market collapses like in 2008, an index investor will assume the same loss as the market. In the case of 2008, the S&P 500 stock index fell by more than 50 percent, offering index investors no downside protection.
Portfolio Control: An index investor has no control over the holdings in the fund. In the event that a certain sector becomes over-owned (i.e. technology stocks in 2000), an index investor maintains the same weight as the index.
Average Returns: An index investor will never have the opportunity to outperform the market, but will always follow. Although the markets are very efficient, an investor can perhaps take advantage of market anomalies and invest with those managers who have maintained a long-term performance edge over the respective index.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
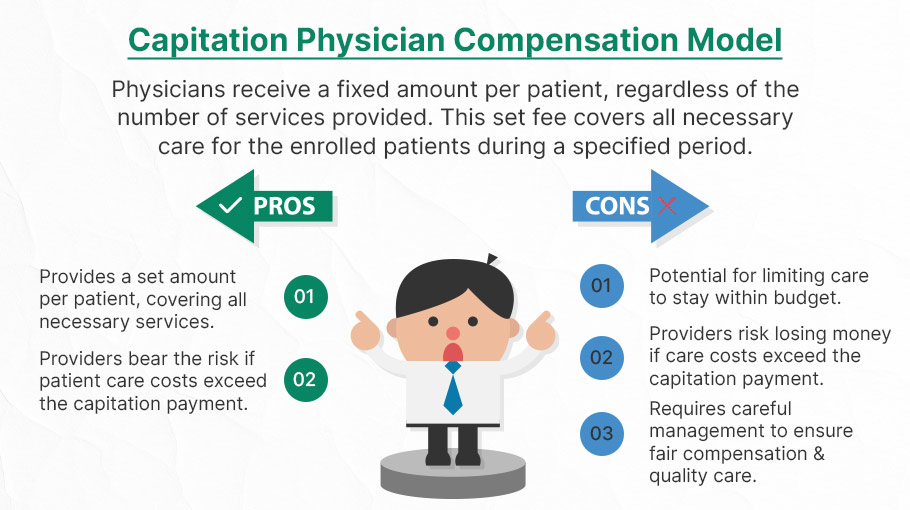
Capitation is a type of healthcare payment system in which a physician or hospital is paid a fixed amount of money per patient for a prescribed period by an insurer or physician association. The cost is based on the expected healthcare utilization costs for a group of patients for that year.
With capitation, the physician—otherwise known as the primary care physician— is paid a set amount for each enrolled patient whether a patient seeks care or not. The PCP is usually contracted with an HMO whose role it is to recruit patients.
According to Richard Eskow, CEO of Health Knowledge Systems of Los Angeles, capitated medical reimbursement has been used in one form or another, in every attempt at healthcare reform since the Norman Conquest. Some even say an earlier variant existed in ancient China [personal communication].
Initially, when Henry I assumed the throne of the newly combined kingdoms of England and Normandy, he initiated a sweeping set of healthcare reforms. Historical documents, though muddled, indicate that soon thereafter at least one “physician,” John of Essex, received a flat payment honorarium of one penny per day for his efforts. Historian Edward J. Kealey opined that sum was roughly equal to that paid to a foot-soldier or a blind person. Clearer historical evidence suggests that American doctors in the mid-19th century were receiving capitation-like payments. No less an authoritative figure than Mark Twain, in fact, is on record as saying that during his boyhood in Hannibal, MO his parents paid the local doctor $25/year for taking care of the entire family regardless of their state of health.
Later, Sidney Garfield MD [1905-1984] is noted as one of the great under-appreciated geniuses of 20th century American medicine stood in the shadow cast by his more celebrated partner, Henry J. Kaiser. Garfield was not the first physician to embrace the notion of prepayment capitation, nor was he the first to understand that physicians working together in multi-specialty groups could, through collaboration and continuity of care, outperform their solo practice colleagues in almost every measure of quality and efficiency. The Mayo brothers, of course, had prior claim to that distinction. What Garfield did, was marry prepayment to group practice, providing aligned financial incentives across every physician and specialty in his medical group, as well as a culture of group accountability for the care of every member of the affiliated health plan. He called it “the new economics of medicine,” and at its heart was a fundamentally new paradigm of care that emphasized – prevention before treatment – and health before sickness. Under his model: the fewer the sick – the greater the remuneration. And: the less serious the illness, the better off the patient and the doctors.
Such ideas were heresy to the reigning fee-for-service, solo practice, ideologues of the mainstream medical establishment of the 1940s and ‘50s, of course. Throughout the period, Garfield and his group physicians were routinely castigated by leaders of the AMA and county medical associations as socialistic and unethical. The local medical associations in Garfield’s expanding service areas – the San Francisco Bay Area, Los Angeles, and Portland, Oregon – blocked group practice physicians from association membership, effectively shutting them out of local hospitals, denying them patient referrals or specialty society accreditation. Twice in the 1940s, formal medical association charges were brought against Garfield personally, at one time temporarily succeeding in suspending his license to practice medicine.
Of course, capitation payments made a comeback in the first cost-cutting managed care era of the 1980-90s because fee-for-service medicine created perverse incentives for physicians by paying more for treating illnesses and injuries than it does for preventing them — or even for diagnosing them early and reducing the need for intensive treatment later. Nevertheless, the modern managed care industry’s experience with capitation wasn’t initially a good one. The 1980-90s saw a number of HMOs attempt to put independent physicians, especially primary care doctors, into a capitation reimbursement model. The result was often negative for patients, who found that their doctors were far less willing to see them — and saw them for briefer visits — when they were receiving no additional income for their effort. Attempts were also made to aggregate various types of health providers — including hospitals and physicians in multiple specialties — into “capitation groups” that were collectively responsible for delivering care to a defined patient group. These included healthcare facilities and medical providers of all types: physicians, osteopaths, podiatrists, dentists, optometrists, pharmacies, physical therapists, hospitals and skilled nursing homes, etc.
However, the healthcare industry isn’t collective by nature, and these efforts tended to be too complicated to succeed. One lesson that these experiments taught is that provider behavior is difficult to change unless the relationship between that behavior and its consequences is fairly direct and easy to understand.
Today, the concept of prepayment and medical capitation is to uncouple compensation from the actual number of patients seen, or treatments and interventions performed. This is akin to a fixed price restaurant menu, as opposed to an àla carte eatery.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
BREAKING NEWS
Law enforcement officials in Utah released a video of the suspected shooter in the assassination of Turning Point USA co-founder and CEO Charlie Kirk, saying that the person wore Converse tennis shoes and left a hand print and a shoe print at the scene.
The suspect in Charlie Kirk’s assassination has been identified as Tyler Robinson, a 22-year-old Utah resident. Law enforcement sources told the Daily Mail that Robinson was taken into custody as the alleged assassin who killed Kirk at a rally at Utah Valley University on Wednesday.
Before today, forensic podiatry has even made it into the public zeitgeist with the hit TV show “Bones” which premiered on September 13, 2005, and concluded on March 28, 2017, airing for 246 episodes over 12 seasons. The show was based on forensic anthropology and forensic archaeology, with each episode focusing on the mystery behind human body remains brought in for examination and identification.
In one show, eight pairs of dismembered feet washed ashore after a flood on the U.S.-Canada border, but things didn’t add up when only seven pairs of feet were identified as research corpses from a nearby university body farm.
When the fictional Canadian forensic podiatrist Dr. Douglas Filmore took the remains back to Canada, he had to form a jurisdictional alliance with the United States to match the pairs of feet and identify the victims. A rare and expensive pair of sneakers led the team to the victim’s murderer.
In 2016, an actual forensic podiatry club was started at the Barry University School of Podiatric Medicine. And, a formal class covering aspects of forensic podiatry is held at the New York College of Podiatric Medicine. Students exit the class with an in depth knowledge of forensic podiatry and other legal knowledge applicable to current cases.
More expertly, real-life colleague Michael Steven Nirenberg DPMactually testified in the murder trial of defendants Kailie Brackett and Donnell Dana with the state calling three witnesses to testify, including the podiatrist who claimed Brackett’s footprints match the ones found in blood at the apartment of the victim, Kimberly Neptune. The forensic podiatrist focused on the footprints discovered at Neptune’s apartment, using prints and images of the defendant’s feet taken by law enforcement. After study, he claimed the prints at the scene bore a resemblance to Kailie Brackett’s in the width of the foot. The defense questioned the field of forensic podiatry and pressed Dr. Nirenberg on whether the measurements would be altered depending on how thick the sock covering the foot was woven.
Dr. Nirenberg was also interviewed on National Public Radio’s Morning Edition on April 14th 2023 about the gait of the bombing suspect associated with the capital riot on Wednesday January 6th, 2021. Dr. Nirenberg is president of the American Society of Forensic Podiatry and co-editor of the textbook: “Forensic Gait Analysis: Principles and Practice”. The bombing suspect had placed bombs at the DNC and RNC headquarters in Washington, DC on the night before. NPR asked Dr. Nirenberg to comment on the features of the person’s gait.
Additionally, Nirenberg was interviewed by Nancy Grace on her TV show Crime Stories. Grace interviewed Nirenberg about his forensic podiatry work in helping to solve the murder of a mother of 3 who was killed in a church. The case remains unsolved. The episode, “Fitness-Mom Missy Bevers Bludgeoned Dead in Creekside Church” aired June 6th, 2024 and is available online at Merit+ TV.
And, Netflix’s 2023 docu-series, “Till Murder Do Us Part”, recounts the killings of Derek and Nancy Haysom by including a series of interviews with a cast of real people. The four-part docu-series revolves around the unpacking of how a wealthy couple was murdered in Virginia in 1985. It also focuses on how the suspects, Elizabeth Haysom, and her boyfriend, Jens Soehring, betrayed each other during the trial. Dr. Sarah Reel DPM was the forensic podiatrist who was involved with Jens’ and Elizabeth’s footprint examination. Dr. Reel pointed out that, statistically, there was no difference “between a bare footprint and a socked footprint.” The doctor suggested that Jens’ reference footprint matched closely with the crime scene footprint.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
When owners of a security spread false information to pump up the price of the security and subsequently sell off their shares, making a profit—the “dump.”
Refer to attempts by investors to move the price of a stock opportunistically by selling large numbers of shares short. The investors pocket the difference between the initial price and the new, lower price after this maneuver. This technique is illegal under SEC rules, which stipulate that every short sale must be on an uptick. For more information on this complex tactic, read on in this piece from the Wharton School of Business.
Wash Trading
Involves the simultaneous or near-simultaneous sale and repurchase of the same security for the purpose of generating activity and increasing the price.
When fraudsters manipulate the market through matched orders, they enter trades to buy or sell securities with the knowledge that a matching order on the opposite side has been or will be entered. During his tenure at the Commission, our partner Jordan Thomas was involved in a case where the SEC won summary judgement and obtained settlements with an astonishing 16 defendants who engaged in matched trades, among other illicit tactics.
Painting the Tape
Painting the tape refers to placing successive orders in small amounts at increasing or decreasing prices.
Spoofing & Layering
High frequency traders are known to use the tactics of Spoofing & Layering to manipulate share prices. Spoofing is the placing of a bid or offer with the intent to cancel before execution. Layering is a form of spoofing in which the trader places multiple orders on one side of the book, in order to create a false impression of heavy buying or selling.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Although 97% of people aren’t yet millionaires, many could eventually meet that target if they start investing sooner rather than later; especially doctors [MD, DO, DPM, DDS or DMD].
A 20-year-old, for instance, needs to invest just $330 a month into an asset class that delivers a 7% to 8% annual return to reach $1.26 million by the time s/he turns 65 years old. The luxury of time significantly boosts your chances of becoming a millionaire.
This doesn’t mean it’s too late for middle-aged savers to reach that millionaire milestone, but it will take a significantly greater investment. If a 50-year-old doctor hasn’t started saving for retirement, s/he would need to invest $3,958 a month at a steady 7% return to reach $1.26 million by retirement.
However, according to one Goldman Sachs report, investors could expect the S&P 500 to deliver just 3% annualized nominal returns over the next 10 years.
After an average 13% yearly return for the past decade, a new strategy outside of the stock market may be needed for that level of outsized gain, especially if you’re late to investing.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Ikea Effect Bias describes the tendency of people to place a higher value on products they have partially created or assembled themselves. This phenomenon is named after the Swedish furniture retailer Ikea, known for selling furniture in flat-pack kits that customers must assemble at home.
he IKEA effect was identified and named by Michael Norton of Harvard Business School, Daniel Mochon of Yale University and colleague Dan Ariely PhD of Duke University, who published the results of three studies in 2011. They described the IKEA effect as “labor alone can be sufficient to induce greater liking for the fruits of one’s labor: even constructing a standardized bureau, an arduous, solitary task, can lead people to overvalue their (often poorly constructed) creations.”
Example: A prospect is more likely to pursue his/her own financial plan than that one from an informed financial planner, CPA or professional advisor.
2011 study found that subjects were willing to pay 63% more for furniture they had assembled themselves than for equivalent pre-assembled items.
IN FINANCE AND INVESTING
The IKEA effect can contribute to reducing panic selling. Investors typically reduce their stock market exposure after a financial crash which often results in “buy high, sell low” strategy that is detrimental to long-run wealth accumulation.
Ashtiani et al.’s study proposes a nudge utilizing the IKEA effect to counteract this phenomenon: “actively involving investors in the selection process of the risky investments, while restricting their selections in a way that preserves a large degree of diversification.”
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 1, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Dear Medical Executive-Post Readers and Subscribers
***
HISTORY OF LABOR DAY
The first Labor Day holiday was celebrated on Sept. 5th, 1882, in New York City, in accordance with the plans of the Central Labor Union. President Grover Cleveland signed a law on June 28th, 1894, that made the first Monday in September of each year a national holiday, according to the Department of Labor.
***
***
MY SEPTEMBER HEALTH RE-SET
To give my health a boost after Labor Day, I’m taking a complete break from alcohol, sugar, cookies, ice cream, coffee and tea for the entire month of September. Besides that, I’ll also prioritize sleep and increase my exercise from 7 to at least 10 times [hours] a week. This will allow me to focus on my diet and mental well-being. It’s essentially a month of health and wellness rejuvenation.
I’ve chosen to focus on alcohol and sugar because I want to challenge the idea that moderate drinking is part of a healthy lifestyle. In reality, only those who maintain a healthy lifestyle can afford to enjoy alcohol in moderation. But, sugar is everywhere and must be minimized for Type II diabetes and weight control.
Moreover, the long-term and excessive intake of sugary beverages and refined sugars can negatively impact your overall caloric intake and create a domino effect on your health. For example, excess sugar in the body can turn into fat deposits and lead to fatty liver disease.
A low sugar diet can help you lose weight and also help you manage and/or prevent diabetes, heart disease and stroke, reduce inflammation, and even improve your mood and the health of your skin. That’s why the low sugar approach is a key tenet of other well-known healthy eating patterns, such as the Mediterranean diet and the DASH diet.
QUESTION: And so, do you also commit to such “factory resets” now and then? Please comments.
Do, enjoy the Labor Day Weekend, Bar-B-Ques with friends, family and colleagues. And, I hope you continue to find the Medical Executive-Post useful!
Many thanks for your likes and referrals. Dr. David Edward Marcinko MBA MEd CMP [Editor and Chief]
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL PROVIDER PAYMENTS LOWERED
***
***
Statistic: $2.8+ billion dollars
That’s how much Blue Cross and Blue Shield plans agreed to pay to settle litigation over claims they conspired to lower payments to providers. (Healthcare Dive)
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
A silent, non-directed, ghost, blind, faux, or “mirror” PPO, HMO, or other provider model is not really a formalized managed care organization [MCO] at all. Rather, it was simply an intermediary attempt, and Ponzi-like scheme, to negotiate practitioner fees downward, by promising a higher volume of patients in exchange for the discount.
Of course, the intermediary [discount-broker] then resells the packaged contract product to any willing insurance company, HMO, PPO or other payer, thereby pocketing the difference as a nice profit. Sometime, these virtual organizations are just indemnity companies in disguise.
NOTE: The term indemnity insurance refers to an insurance policy that compensates an insured party for certain unexpected damages or losses up to a certain limit—usually the amount of the loss itself. Insurance companies provide coverage in exchange for premiums paid by the insured parties.
These policies are commonly designed to protect professionals and business owners when they are found to be at fault for a specific event such as misjudgment or malpractice. They generally take the form of a letter o indemnity.
***
As part of a silent PPO scheme, insurers try to pass off the discount as legitimate on Explanation of Benefit [EOB] forms. Physicians should not fall for this ploy, since pricing pressure will be forced even lower in the next round of “real” PPO negotiations!
Medical providers should also be on guard for silent HMOs, MCOs and any other silent insurance variation, since these virtual organizations do not exist, except as exploitable arbitrage situations for the middleman.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
It is normal for physician litigants to develop a case of “buyer’s remorse” after any mediation or divorce settlement. They may feel disappointed after entering into a settlement agreement or feel that they received a bad deal.
Mediation: Some advantages of divorce mediation over divorce litigation include:
◊ Mediation is generally faster and less costly.
◊ Mediation is voluntary, private and confidential.
◊ Mediation facilitates creative and realistic solutions.
◊ Mediation allows parties to control their agreements.
◊ Mediation eliminates a win-lose atmosphere and result.
◊ Mediation provides a forum for addressing future disputes.
◊ Mediation fosters communication and helps mend relationships.
***
***
Settlement
And so, in a vast majority of cases, mediation and settlement is probably a good deal. In fact, it is probably a great deal because you are receiving something without having to risk losing. Remember, trial can be a crap-shoot, and nothing is worse than losing it all at the time of trial.
Bench trial verdict by a trial judge.
Jury trial verdict by your “peers.”
Instead, you entered into a settlement agreement and now your divorce case is over.
But beware since trying to get out of a settlement agreement reached at mediation or settlement is virtually impossible.
Why? Well, there is a strong interest by the court to enforce mediation and settlement agreements. The court wants your divorce case to be over and off its docket. There are a few very narrow exceptions; for example, if one party was truly coerced because someone held a gun to their head. But that rarely happens, and it certainly doesn’t happen to most doctors or dentists.
Of course, you can fight against your mediation or settlement agreement if you like, but you won’t get too far. There’s an old adage in the law that a bad settlement is better than a great trial. That’s because no one knows how a judge or jury will rule come time of trial.
***
***
This buyers remorse phenomenon also isn’t uncommon among people who receive sudden wealth, whether through divorce settlements, inheritances, lottery winnings, or other windfalls.
Assessment
Financial advisors often see clients struggle with “sudden wealth syndrome”—the inability to properly manage a large sum of money they’re not accustomed to having.
Common mistakes include:
Lifestyle inflation without sustainable income to support it.
Poor investment decisions or lack of investment planning.
Emotional spending following traumatic life events like divorce.
Failure to set aside money for taxes on the settlement.
Not creating a long-term financial plan for the money.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Medicine today is vastly different than a generation ago, and all health care professionals need new skills to be successful and reduce the emerging risks outlined in this textbook, as well as the “unknown-unknowns” elsewhere. Traditionally, the physician was viewed as the “captain of the ship”. Today, their role may be more akin to a ship’s navigator, using clinical, teaching skills and knowledge to chart the patient’s course through a confusing morass of insurance requirements, fees, choices, rules and regulations to achieve the best attainable clinical outcomes.
This new leadership paradigm includes many classic business school principles, now modified to fit the decade long PP-ACA, the era of health reform, and modern technical connectivity and EMRs.
Thus, the physician must be a subtle guide on the side; not bombastic sage on the stage. These, newer health 3.0 leadership philosophies might include:
•Negotiation – working to optimize appropriate treatment plans; ie., quality of life versus quantity of life, •Team play – working in concert with other allied healthcare professionals to coordinate care delivery ,ithin a clinically appropriate and cost-effective framework; •Working within the limits of competence – avoiding the pitfalls of the medical generalist versus the specialist that may restrict access to treatment, medications, physicians and facilities by clearly acknowledging when a higher degree of service is needed on behalf of the patient – all while embracing holistic primary care; •Respecting different cultures and values – inherent in the support of the medical Principle of Autonomy is the acceptance of values that may differ from one’s own. As the US becomes more culturally hetero geneous, medical providers are called upon to work within, and respect, the socio-cultural and/or spiritual framework of patients, students and their families; •Seeking clarity on what constitutes marginal care – within a system of finite resources; providers are called upon to openly communicate with patients regarding access to marginal medical information and/or treatments. •Supporting evidence-based practice – healthcare providers, should utilize outcomes data to reduce variation in treatments to achieve higher efficiencies and improved care delivery thru evidence based medicine [EBM]; •Fostering transparency and openness in communications – healthcare professionals should be willing, and prepared, to discuss all aspects of care, especially when discussing end-of-life issues or when problems arise; •Exercising decision-making flexibility – treatment algorithms, templates and clinical pathways are useful tools when used within their scope; but providers must have the authority to adjust the plan if circumstances warrant.
Becoming skilled in the art of listening and interpreting — In her ground-breaking book, Narrative Ethics: Honoring the Stories of Illness, Rita Charon, MD PhD, a professor at Columbia University, writes of the extraordinary value of using the patient’s personal story in the treatment plan. She notes that, “medicine practiced with narrative competence will more ably recognize patients and diseases; convey knowledge and regard, join humbly with colleagues, and accompany patients and their families through ordeals of illness.” In many ways, attention to narrative returns medicine full circle to the compassionate and caring foundations of the patient-physician relationship.
These thoughts represent only a handful of examples to illustrate the myriad of new skills that tomorrows’ healthcare professionals must master in order to meet their timeless professional obligations of compassionate care and contemporary treatment effectiveness; all within the context modern risk management principles.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 20, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
LEADERSHIP versus MANAGEMENT
***
***
By Dr. David Edward Marcinko MBA MEd
By Professor Gary A. Cook PhD
By Professor Eugene Schmuckler PhD MBA MEd CTS
Many of us have encountered a person who may intellectually be at upper levels, but whose ability to interact with others appears to that of one who is highly immature. This is the individual who is prone to becoming angry easily, verbally attacks co-workers, is perceived as lacking in compassion and empathy, and cannot understand why it is difficult to get others to cooperate with them and their agendas.
THINK: Sheldon Cooper PhD D.Sc MA BA of the The Big Bank Theory TV show.
The concept of Emotional Intelligence [EQ] was brought into the public domain when Daniel Goleman authored a book entitled, Emotional Intelligence.” According to Goleman, emotional intelligence consists of four basic non-cognitive competencies: self awareness, social awareness, self management and social skills. These are skills which influence the manner in which people handle themselves and their relationships with others. Goleman’s position was that these competencies play a bigger role than cognitive intelligence in determining success in life and in the workplace. He and others contend that emotional intelligence involves abilities that may be categorized into five domains:
Self awareness: Observing and recognizing a feeling as it happens.
Managing emotions: Handling feelings so that they are appropriate; realizing what is behind a feeling; finding ways to handle fears and anxieties, anger and sadness.
Motivating oneself; Channeling emotions in the service of a goal; emotional self control; delaying gratification and stifling impulses.
Empathy: Sensitivity to others’ feelings and concerns and taking their perspective appreciating the differences in how people feel about things.
Handling relationships: Managing emotions in others; social competence & social skills.
In 1995, Goleman then expanded on the works of Howard Gardner, Peter Salovey and John Mayer. He further defined Emotional Intelligence as a set of competencies demonstrating the ability one has to recognize his or her behaviors, moods and impulses and to manage them best, according to the situation. Mike Poskey, in “The Importance of Emotional Intelligence in the Workplace.” continued this definition by stating that emotional intelligence is considered to involve emotional empathy; attention to, and discrimination of one’s emotions; accurate recognition of one’s own and others’ moods; mood management or control over emotions; response with appropriate emotions and behaviors in various life situations (especially to stress and difficult situations); and balancing of honest expression of emotions against courtesy, consideration, and respect.
Source: Emotional Intelligence: what is and why it matters” – Cary Cherniss, PhD, presented at the annual conference of the Society of Industrial and Organizational Psychology, April 2000.
EQ differs from what has generally been considered intelligence which is described in terms of one’s IQ.
Traditional views of intelligence focused on cognition, memory and problem solving. Even today individuals are evaluated on the basis of cognitive skills. Entrance tests for medical, law, business, undergraduate and graduate schools base admissions in large part on the scores of the SAT, GMAT, LSAT, MCAT, etc. Without question, cognitive ability is critical but has been demonstrated, it is not a very good predictor of future direct job performance and indirect liability management. In fact, in 1940, David Wechsler the developer of a widely used intelligence test made reference to “non-intellective” elements. By this Wechsler meant affective, personal and social factors.
Source: Non-Intellective factors in intelligence. Psychological Bulletin, 37, 444-445.
Goleman became aware of the work of Salovey and Mayer having trained under David McClelland and was influenced by McClelland’s concern with how little traditional tests of cognitive intelligence predicted success in life. In fact, a study of 80 PhDs in science underwent a battery of personality tests, IQ tests and interviews in the 1950s while they were graduate students at Berkeley. Forty years later they were re-evaluated and it turned out that social and emotional abilities were four times more important than IQ in determining professional success and prestige.
Source: Feist & Barron: Emotional Intelligence and academic intelligence in career and life success. Paper presented at the Annual Convention of the American Psychological Society, San Francisco, 1996.
Undoubtedly, we want to have individuals work with us who have persistence which enables to them have the energy, drive, and thick skin to develop and close new business, or to work with the patients and other members of the staff. It is important to note that working alongside one with a “good” personality may be fun, energetic, and outgoing.
However, a “good personality does not necessarily equate to success. An individual with a high EQ can manage his or her own impulses, communicate effectively, manage change well, solve problems, and use humor to build rapport in tense situations. This clarity in thinking and composure in stressful and chaotic situations is what separates top performers from weak performers.
Poskey outlined a set of five emotional intelligence competencies that have proven to contribute more to workplace achievement than technical skills, cognitive ability, and standard personality traits combined.
***
***
A. Social Competencies: Competencies that Determine How We Handle Relationships
Intuition and Empathy – Our awareness of others’ feelings, needs, and concern. He suggested that this competency is important in the workplace for the following reasons:
Understanding others: an intuitive sense of others’ feelings and perspectives, and showing an active interest in their concerns and interests
Patient service orientation: the ability to anticipate, recognize and meet customer’s’ (patients) needs
People development: ability to sense what others need in order to grow, develop, and master their strengths
Leveraging diversity: cultivating opportunities through diverse people.
B. Political Acumen and Social Skills: Our adeptness at inducing desirable responses in others. This competency is important for the following reasons:
Influencing: using effective tactics and techniques for persuasion and desired results.
Communication: sending clear and convincing messages that are understood by others
Leadership: inspiring and guiding groups of people
Change catalyst: initiating and/or managing change in the workplace
Conflict resolution: negotiating and resolving disagreements with people
Collaboration and cooperation: working with coworkers and business partners toward shared goals
Team capabilities: creating group synergy in pursuing collective goals.
C. Personal Competencies: Competencies that determine how we manage ourselves
D. Self Awareness: Knowing out internal states, preferences, resources, and intuitions. This competency is important for the following reasons.
Emotional awareness: recognizing one’s emotions and their effects and impact on those around us
Accurate self-assessment: knowing one’s strengths and limits
Self-confidence: certainty about one’s self worth and capabilities
Self-Regulation: managing one’s internal states, impulses, and resources. This competency is important in the workplace for the following reasons.
Self-control: managing disruptive emotions and impulses
Trustworthiness: maintaining standards of honesty and integrity
Conscientiousness: taking responsibility and being accountable for personal performance
Adaptability: flexibility in handling change
Innovation: being comfortable with an openness to novel ideas, approaches, and new information.
E. Self-Expectations and Motivation: Emotional tendencies that guide or facilitate reaching goals. This competency is important in the workplace for the following reasons.
Achievement drive: striving to improve or meet a standard of excellence we impose on ourselves
Commitment: aligning with the goals of the group or the organization
Initiative: readiness to act on opportunities without having to be told
Optimism: Persistence in pursuing goals despite obstacles and setbacks
A note of caution is necessary. Goleman and Salovey both stated that emotional intelligence on its own is not a strong predictor of job performance. Instead they contend that it provides the bedrock for competencies that are predictors.
Obviously, EQ is an important attribute and it behooves each of us to promote emotional intelligence in the workplace. A number of guidelines have been developed for the Consortium for Research on Emotional Intelligence in Organizations by Goleman and Cherniss. The guidelines cover 21 phases which include preparation, training, transfer and evaluation.
Assess the organization’s needs: Determine the competencies that are most critical for effective job performance in a particular type of job. In doing so, us a valid method, such as the comparison of the behavioral interviews of superior performs and average performers. Also make sure the competencies to be developed are congruent with the organization’s culture and overall strategy.
Assess the individual: This assessment should be based on the key competencies needed for a particular job, and the data should come from multiple sources using multiple methods to maximize credibility and validity.
Deliver assessments with care: Give the individual information on his/her strengths and weaknesses. In doing so, try to be accurate and clear. Also, allow plenty of time for the person to digest and integrate the information. Provide feedback in a safe and supportive environment in order to minimize resistance and defensiveness. Avoid making excuses or downplaying the seriousness of deficiencies.
Maximize choice: People are motivated to change when they freely choose to do so. As much as possible, allow people to decide whether or not they will participate in the development process, and have them change goals themselves.
Encourage people to participate: People will be more likely to participate in development efforts if they perceive them to be worthwhile and effective. Organizational policies and procedures should encourage people to participate in development activity, and supervisors should provide encouragement and the necessary support. Motivation will be enhanced if people trust the credibility of those who encourage them to undertake the training.
Link learning goals to personal values: People are most motivated to pursue change that fits with their values and hopes. If a change matters little to people, they won’t pursue it. Help people understand whether a given change fits with what matters most to them.
Adjust expectations: Builds positive expectations by showing learners that social and emotional competence can be improved and that such improvement will lead to valued outcomes. Also, make sure that the learner has a realistic expectation of what the training process will involve.
Gauge readiness: Assess whether the individual is ready for training. If the person is not ready because of insufficient motivation or other reasons, make readiness the focus of intervention efforts.
Foster a positive relationship between the trainers and learners: Trainers who are warm, genuine, and empathic our best able to engage the learners in the change process. Select trainers who have these qualities, and make sure that they use them when working with the learners.
Make change self-directed: Learning is more effective when people direct their own learning program, tailoring it to their unique needs and circumstances. In addition to allowing people to set their own learning goals, let them continue to be in charge of their learning throughout the program, and tailor the training approach to the individual’s learning style.
Set clear goals: People need to be clear about what the competence is, how to acquire it, and how to show it on the job. Spell out the specific behaviors and skills that make up the target competence. Make sure that the goals are clear, specific, and optimally challenging.
Break goals into manageable steps: change. That is more likely to occur if the change process is divided into manageable steps. Encourage both trainers and trainees to avoid being overly ambitious.
Provide opportunities to practice: Lasting change requires sustained practice on the job and elsewhere in life. An automatic habit is being unlearned and different responses are replacing it. Use naturally occurring opportunities for practice at work, and in life. Encourage the trainees to try the new behaviors repeatedly and consistently over a period of months.
Give performance feedback: Ongoing feedback encourages people and direct change. Provide focused and sustained feedback as the learners practice new behaviors. Make sure that supervisors, peers, friends, family members-or some combination of these- give periodic feedback on progress.
Rely on experiential methods: Active, concrete, experiential methods tend to work best for learning social and emotional competencies. Development activities that engage all the senses and our dramatic and powerful can be especially effective.
Build in support: Change is facilitated through ongoing support of others who are going through similar changes. Programs should encourage the formation of groups where people give each other support, throughout the change effort. Coaches and mentors also can be valuable in helping support the desired change.
Use models: Use modern webinars, patient portals, live or videotaped models that clearly show how the competency can be used in realistic situations. Encourage learners to study, analyze, and emulate the models.
Enhance insight: Self-Awareness is the cornerstone of emotional and social competence. Help learners acquire greater understanding about how their thoughts, feelings, and behavior affect themselves and others.
Prevent relapse: Use relapse prevention, which helps people use lapses and mistakes as lessons to prepare themselves for further efforts.
Moreover:
Encourage use of skills on the job: Supervisors, peers and subordinates should reinforce and reward learners for using their new skills on the job. Coaches and mentors also can serve this function. Also, provide prompts and cues, such as through periodic follow-ups. Change also is more likely to indoor. When high status persons, such as supervisors and upper-level management model it.
Develop an organizational culture that supports learning: Change will be more enduring if the organization’s culture and tone support the change and offer a safe atmosphere for experimentation.
Finally, see if the development effort has lasting effects evaluated. When possible, find a true set of measures of the competence or skill, as shown on the job, before and after training, and also at least two months later. One-year follow-ups also are highly desirable. In addition to charting progress on the acquisition of competencies, also assess the impact on important job related outcomes, such as performance measures, and indicators of adjustments such as absenteeism, grievances, health status, etc.
Managers V. Leaders
These abilities are important for one to be successful as a manager and even more so as a leader, or physician executive. But, before we begin an examination of strategic leadership, it is necessary to make a deeper distinction between a manager and a leader. There are many different definitions as well as descriptions regarding leadership and management.
Many people talk as though leadership and management is the same thing. Fundamentally, they are quite different. Management focuses on work. We manage work activities such as money, time, paperwork, materials, equipment, and personnel, among other things. As can be found in any basic book on management, management focuses on planning, organizing, controlling, coordinating, budgeting, finance and money management as well as decision making. In effect, managers are generally those individuals who have been given their authority by virtue of their role. It is the function of a manager to ensure that the work gets done as well as to oversee the activities of others. In many healthcare organizations we find that those individuals elevated to a managerial position occur as a result of being a high performer on their previous assignment. A manager receives authority on the basis of role; while a leader’ authority is more innate in nature.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
In today’s dynamic economic landscape, the concept of a “side hustle” has evolved from a mere trend to an essential component of personal financial strategy for many individuals; even doctors.
A side hustle is a way to earn extra income outside of your primary job or main source of employment. It typically involves part-time work, freelancing, small businesses, or gig-based activities that can be pursued flexibly in your free time. Unlike traditional employment, side hustles often offer more autonomy, creative freedom, and the potential to monetize skills, hobbies, or passions.
***
***
Doctor Gigs?
So, if you’re a doctor, dentist or podiatrist considering a side hustle, focus on something sustainable and long-term. Ask yourself: What am I already good at? What do people already ask me to help with? The best side hustles don’t require reinventing the wheel — just monetizing the one you’ve already been pushing uphill.
But, avoid gigs that require a huge upfront investment or promise overnight success. Instead, look for something that offers flexibility, ideally something that works with your schedule, not against your sanity.
Track your earnings and how much time you’re putting in. Side income should support your goals, whether that’s paying off debt, saving for a trip or just breathing easier when office rent comes due.
But, if it’s draining your energy from your medical practice with little to show for it, it might be time to rethink the hustle.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
UnitedHealth Group soared almost 12%, its biggest one-day gain in nearly five years, after getting the “Buffett Bounce.” Buffett’s Berkshire Hathaway revealed it bought ~5 million shares worth nearly $1.6 billion, giving a much-needed vote of confidence to the struggling health giant.
The White House is considering buying part of Intel, Bloomberg reported this week, which would be the latest big business deal the president pursues on behalf of the government. The Trump administration might acquire a stake in the struggling computer chip-maker using CHIPS Act funding—nearly $11 billion of which was already earmarked for Intel.
Saudi Arabia’s Public Investment Fund took an $8 billion write-down on five mega-projects it’s building, due to lower oil prices and higher costs.
Pimco, the asset management giant, warned that President Trump’s plan to IPO Fannie Mae and Freddie Mac could push mortgage rates higher.
Whatever the statistics regarding physician standard of living, the reality is that within most marriages the husband more frequently takes responsibility for understanding and managing the finances. Additionally, women are more likely to remain in the marital home following a separation, thus inheriting a large fixed expense that may prove be an excessive, albeit short-term burden to them. At the time the decision is made to separate or divorce, many women do not have an understanding of how to manage their household budget, or how to manage their assets and liabilities.
An issue many divorcing physicians face is that the other spouse (in the past the wife), may have concentrated their energies on managing the home, while the physician concentrated on earning and managing the finances. The problems of the spouse of a physician are often compounded in divorce; not only do they not understand their personal finances, but that their absence from the work force has made them financially dependent on the other.
At what probably be the most emotionally taxing time in their lives, they are forced to play catch-up.
***
***
Taking a more active role in their own financial planning during the marriage may help the spouse of a physician avoid some of the financial pitfalls of separation and divorce.
NOTE: Barbara Stanny provides an excellent overview and reading bibliography on how people can get smart about money in her book Prince Charming Isn’t Coming. [1]
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
An important component of hospital credit analysis is essentiality. Hospitals are unusual businesses that many times possess some form of essentiality to their communities. Health care is important to the economic vitality of every community. Many hospitals have served their communities for many years; it is not uncommon to find hospitals that have been continuously operating for more than 100 years in the same community.
Most hospitals are not-for-profit. In not-for-profit hospitals, no private party actually “owns” the hospital; control is vested in various boards, but no one explicitly owns a not-for-profit hospital. In a broad sense, communities own not-for-profit hospitals. They are considered “charities” with a “charitable purpose.” Though a not-for-profit hospital may not have owners, it has many “stakehold-ers,” parties that have vested interests in the continuing success of the hospital.
Many hospitals have broad and vast webs of stakeholders. Stakeholders are why hospitals rarely close or are shut down. Too many stakeholders have interests in the continuing successful operation of hospitals.
Another dimension of the essentiality analysis is service analysis. How significant are the hospital’s services? If the hospital shuts down, what population segments would suffer? How significant is the population that would suffer? How much would they suffer?
And so, hospital stakeholder relationships need to be considered in the analysis of essentiality. How strong are these relations? How many are there? How important is the continuing success of this hospital to these stakeholders?
Analysis of hospital’s stakeholders and services should provide a credible view of the degree of essentiality associated with a hospital. Higher degrees of essentiality suggest higher likelihoods that hospitals, one way or another, will meet their commitments, particularly their payment commitments.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
According to Wikipedia, Phantom debt or zombie debt is a debt that is old, defaulted, or not owed and is somehow still being pursued for collection to be paid by the presumed debtor. It generally refers to debt that is more than 3 years old, is long forgotten about or belonged to someone else – like someone with the same name or a deceased parent. The amount owed can grow to hundreds or thousands of dollars more than what was originally owed.
An example of this is from George Miller. George missed an 11 cent Verizon bill and seven years later it had grown to $4,000.00.
Sometimes it was never owed, was owed by a deceased parent, or that was previously owed by the presumed debtor, but was previously paid in full, settled, discharged via bankruptcy or a dismissed court case, is beyond the statute of limitations, or is otherwise not legally collectible, but that a collection agency or other similar service is aggressively attempting to collect, often fraudulently.
While the concept of phantom debt is quite old, it has gotten a lot of attention since the 1990s.
Very often, collectors of phantom debt use intimidating, abusive, or otherwise illegal tactics in an attempt to collect phantom debt that include frequent phone calls, calls to the victim’s place of employment, or threats of scary consequences against the victim that sometimes include arrest and/or criminal prosecution. In the USA, such tactics violate the Fair Debt Collection Practices Act [FDCPA]
The source of phantom debt may be from collectors who buy the debt from other collectors for pennies on the dollar, some of which take action that is not legal in order to collect that debt. Unlawful techniques used include suing or threatening to sue, re-aging the debt on the victim’s credit report to circumvent limits on reporting, or falsely promising to remove a negative credit report entry in exchange for a partial payment.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Doctors and dentists earn money by treating patients. CPAs and Attorneys have clients, and retail stores buy items low and sell them at higher prices. This is called a business model.
More formally, a business model identifies the products or services the business plans to sell, the target market, and any anticipated expenses, in order to outline how to generate a profit. Business models are important for both new and established businesses. They help companies attract investment, recruit talent, and motivate management and staff.
Businesses should regularly update their business model, or they’ll fail to anticipate trends and challenges ahead. Business models also help investors to evaluate companies that interest them and employees to understand the future of a company they may aspire to join.
***
The Business Model of Pharmacy Benefits Managers
In the United States, health insurance providers often hire a third party to handle price negotiations, insurance claims, and distribution of prescription drugs. Providers that use such pharmacy benefit managers include commercial health plans, self-insured employer plans, Medicare Part D [drug] plans, the Federal Employees Health Benefits Program, and state government employee plans. PBMs are designed to aggregate the collective buying power of en-rollees through their client health plans, enabling plan sponsors and individuals to obtain lower prices for their prescription drugs. PBMs negotiate price discounts from retail pharmacies, rebates from pharmaceutical manufacturers, and mail-service pharmacies which home-deliver prescriptions without consulting face-to-face with a pharmacist.
Pharmacy benefit management companies can make revenue in several ways.
First, they collect administrative and service fees from the original insurance plan.
Then, they can also collect rebates from the manufacturer.
Traditional PBMs do not disclose the negotiated net price of the prescription drugs, allowing them to resell drugs at a public list price (also known as a sticker price), which is higher than the net price they negotiate with the manufacturer. This practice is known as “spread pricing”. The industry argues that savings are trade secrets. Pharmacies and insurance companies are often prohibited by PBMs from discussing costs and reimbursements. This leads to lack of transparency.
***
***
Therefore, states are often unaware of how much money they lose due to spread pricing, and the extent to which drug rebates are passed on to en-rollees of Medicare plans. In response, states like Ohio, West Virginia, and Louisiana have taken action to regulate PBMs within their Medicaid programs.
For instance, they have created new contracts that require all discounts and rebates to be reported to the states. In return, Medicaid pays PBMs a flat administrative fee.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
In the early 1980s, Daniel Kahneman and Amos Tverskey proved in numerous experiments that the reality of decision making differed greatly from the assumptions held by economists. They published their findings in Prospect Theory: An analysis of decision making under risk, which quickly became one of the most cited papers in all of economics.
To understand the importance of their breakthrough, we first need to take a step back and explain a few things. Up until that point, economists were working under a normative model of decision making. A normative model is a prescriptive approach that concerns itself with how people should make optimal decisions. Basically, if everyone was rational, this is how they should act.
Amanda, an RN client, was just informed by her financial advisor that she needed to re-launch her 403-b retirement plan. Since she was leery about investing, she quietly wondered why she couldn’t DIY. Little does her Financial Advisor know that she doesn’t intend to follow his advice, anyway! So, what went wrong?
The answer may be that her advisor didn’t deploy a behavioral economics framework to support her decision-making. One such framework is the “prospect theory” model that boils client decision-making into a “three step heuristic.”
According to colleague Eugene Schmuckler PhD MBA MEd CTS, Prospect theory makes the unspoken biases that we all have more explicit. By identifying all the background assumptions and preferences that clients [patients] bring to the office, decision-making can be crafted so that everyone [family, doctor and patient] or [FA, client and spouse] is on the same page.
1. Simplify choices by focusing on the key differences between investment [treatment] options such as stock, bonds, cash, and index funds.
2. Understanding that clients [patients] prefer greater certainty when it comes to pursuing financial [health] gains and are willing to accept uncertainty when trying to avoid a loss [illness].
3. Cognitive processes lead clients and patients to overestimate the value of their choices thanks to survivor bias, cognitive dissonance, appeals to authority and hindsight biases.
CITE: Jaan E. Sidorov MD [Harrisburg, PA]
Assessment
Much like in healthcare today, the current mass-customized approaches to the financial services industry fall short of recognizing more personalized advisory approaches like prospect theory and assisted client-centered investment decision-making.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
THE ADDICTIVE INVESTING / TRADING PERSONALITY OF DOCTORS
Dr. Donald J. Mandell, a pediatrician, always needs to leave the office fifteen minutes ahead of schedule. The reason is because it takes that long to make the necessary number of trips to ensure the front door is truly locked.
Dr. Kamela A. Shaw, a general surgeon, is constantly rushing to the bath room so that she can wash her hands. As far as she is concerned, it is not possible to get one’s hands clean enough considering the COVID pandemic or recent influenza outbreak.
Although the behaviors displayed by these two doctors are different, they are consistent in that each, to some degree, display behavior that might be called an obsessive-compulsive disorder [OCD].
An obsession is a persistent, recurring preoccupation with an idea or thought. A compulsion is an impulse that is experienced as irresistible.
Obsessive-compulsive individuals feel compelled to think thoughts that they say they do not want to think or to carry out actions that they say are against their will. These individuals usually realize that their behavior is irrational, but it is beyond their control. In general, these individuals are preoccupied with orderliness, perfectionism, and mental and interpersonal control, at the expense of flexibility, openness, and efficiency. Specifically, behaviors such as the following may be seen:
Preoccupation with details.
Perfectionism that interferes with task completion.
Excessive devotion to work and office productivity.
Scrupulous and inflexible about morality (not accounted for by cultural or religious identification);
Inability to discard worn-out or worthless objects without sentimental value;
Reluctance to delegate tasks or to work with others.
Adopts a miserly spending style toward both self and others.
Demonstrates a rigid, inflexible and stubborn nature.
Most people resort to some minor obsessive-compulsive patterns under severe pressure or when trying to achieve goals that they consider critically important. In fact, many individuals refer to this as superstitious behavior. The study habits required for medical students entail a good deal of compulsive behavior.
As the above examples suggest, there are a variety of addictions possible. Recent news accounts have pointed out that even high-level governmental officials can experience sex addiction. The advent of social-media has led to what is referred to as Internet addiction where an individual is transfixed to a computer, tablet PC or smart-phone, “working” for hours on end without a specific project in mind. The simple act of “surfing”, “tweeting-X”, “texting” or merely posting opinions offers the person afflicted with the addiction some degree of satisfaction.
Still another form of addictive behavior is that of the individual with gambling disorder (GD).
GD is recognized as a mental disorder in the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders-V. This is the behavior of an individual who is unable to resist the impulse to gamble. Many reasons have been posited for this type of behavior including the death instinct; a need to lose; a history of trauma; a wish to repeat a big win; identification with adults the “gambler” knew as an adolescent; and a desire for action and excitement. There are other explanations offered for this form of compulsive behavior. The act of betting allows the individual to express an immature bravery, courage, manliness, and persistence against unfavorable odds. By actually using money and challenging reality, he puts himself into “action” and intense emotion. By means of gambling, the addicted individual is able to pretend that he is favored by “lady luck,” specially chosen, successful, able to beat the system and escape from feelings of discontent.
Greed can also have addictive qualities. In fact, a poll conducted by the Chicago Tribune revealed that folks who earned less than $30,000 a year, said that $50,000 would fulfill their dreams, whereas those with yearly incomes of over $100,000 said they would need $250,000 to be satisfied. More recent studies confirm that goals keep getting pushed upward as soon as a lower level is reached.
Edward Looney, executive director of the Trenton, New Jersey based Council on Compulsive Gambling (CCG) reports that the number of individuals calling with trading-associated problems is doubling annually. In the mid 1980s, when the council was formed, the number of people calling the council’s hotline (1 – 800 Gambler) with stock-market gambling problems was approximately 1.5 percent of all calls received. In 1998 that number grew to 3 percent, and rose to 8 percent by 2012. Today, that number is largely unknown because of its pervasiveness, but Dr. Robert Custer, an expert on compulsive gambling reported, that stock market gamblers represent over 20 percent of the gamblers that he has diagnosed. It is evident that on-line trading presents a tremendous risk to the speculator.
The CCG describes some of the consequences:
Dr. Fred B. is a 43-year-old Asian male physician with a salary above $150,000 and in debt for more than $150,000. He is married with two children. He was a day trader.
Michael Q. is a 28-year-old Hispanic male registered nurse. He is married and the father of one (7 month old) child. He earns $65,000 and lost $50,000 savings in day trading and is in debt for $30,000. He has suicidal ideation.
[B] A Question of Suitability
Since online traders are in it for many reasons, investment suitability rarely enters the picture, according to Stuart Kaswell, general counsel of the Securities Industry Association, in Washington, DC. The kind of question that has yet to be confronted, by day or online trading firms, is a statement, such as: “Equities look good this year. We favor technology stocks. We have a research report on our Web page that looks at the social media industry.” Those kinds of things are seldom considered because they do not involve a specific recommendation of a specific stock, like Apple, Google, Groupon, Facebook or Twitter.
However, if a firm makes a specific recommendation to an investor, whether over the cell-phone, iPad®, fax machine, face-to-face, instagram or over the Internet, or Twitter-X, suitability rules should apply. Opining similarly on the “know your customer” requirements is Steven Caruso, of Maddox, Koeller, Harget & Caruso of New York City. “The on-line firms obviously claim that they do not have a suitability responsibility because they do not want the liability for making a mistake as far as determining whether the investor was suitable or buying any security. I think that ultimately more firms are going to be required to make a suitability, [or eventually fiduciary] determination on every trade”.
[C] On-line Traders and Stock Market Gamblers
Some of the preferred areas of stock market gambling that attract the interest of compulsive gamblers include options, commodities, penny stocks and bit-coins, index investing, new stock offerings, certain types of CAT bonds, crowd-sourcing initiatives, and some contracts for government securities. These online traders and investment gamblers think of themselves as cautious long-term investors who prefer blue chip or dividend paying varieties. What they fail to take into consideration is that even seemingly blue chips can both rise and precipitously drop in value again, as seen in the summer of 2003, the “crash” of 2008, or the “flash crash” of May 6, 2010. On this day, the DJIA plunged 1000 points (about 9%) only to recover those losses within minutes. It was the second largest point swing 1,010.14 points, and the biggest one-day point decline, 998.5 points, on an intraday basis in Dow Jones Industrial Average history.
Regardless of investment choice, the compulsive investment gambler enjoys the anticipation of following the daily activity surrounding these investments. Newspaper, hourly radio and television reports, streaming computer, tablet and smart phone banners and hundreds of periodicals and magazines add excitement in seeking the investment edge. The name of the game is action. Investment goals are unclear, with many participating simply for the feeling it affords them as they experience the highs and lows and struggles surrounding the play. And, as documented by the North American Securities Administrators Association’s president, and Indiana Securities Commissioner, Bradley Skolnik, most day or online traders lose money. “On-line brokerage was new and cutting edge and we enjoyed the best stock market in generations, until the crashes. The message of most advertisements was “just do it”, and you’ll do well. The fact is that research and common sense suggest the more you trade, the less well you’ll do”.
Most day or online traders are young males, some who quit their day jobs before the just mentioned debacles; or more recently with the dismal economy. Many ceased these risky activities but there is some anecdotal evidence that is re-surging again with 2013-14 technology boom and market rise. Most of them start every day not owning any stock, then buy and sell all day long and end the trading day again without any stock – – just a lot of cash. Dr. Patricia Farrell, a licensed clinical psychologist states that day traders are especially susceptible to compulsive behaviors and addictive personalities. Mark Brando, registered principal for Milestone Financial, a day trading firm in Glendale, California states, “People that get addicted to trading employ the same destructive habits as a gambler. Often, it’s impossible to tell if a particular trade comes from a problem gambler or a legitimate trader.”
Arthur Levitt, former Chairman of the Securities and Exchange Commission (SEC) in discussing the risks and misconceptions of investing are only amplified by on-line trading. In a speech before the National Press Club a few years ago, he attempted to impress individuals as to the risks and difficulties involved with day trading. Levitt cited four common misconceptions that knowledgeable medical professionals, and all investors, should know:
Personal computers, tablets, mobile devices and smart-phones are not directly linked to the markets – Thanks to Level II computer software, day traders can have access to the same up-to-the-second information available to market makers on Wall Street. “Although the Internet makes it seem as if you have a direct connection to the securities market, you don’t. Lines may clog; systems may break; orders may back-up.”
The virtue of limit orders – “Price quotes are only for a limited number of shares; so only the first few investors will receive the currently quoted price. By the time you get to the front of the line, the price of the stock could be very different.”
Canceling an order – “Another misconception is that an order is canceled when you hit ‘cancel’ on your computer. But, the fact is it’s canceled only when the market gets the cancellation. You may receive an electronic confirmation, but that only mean your request to cancel was received – not that your order was actually canceled”.
Buying on margin – “if you plan to borrow money to buy a stock, you also need to know the terms of the loan your broker gave you. This is margin. In volatile markets, investors who put up an initial margin payment for a stock may find themselves required to provide additional cash if the price of the stock falls.
How then, can the medical professional or financial advisor tell if he or she is a compulsive gambler? A diagnostic may be obtained from Gamblers Anonymous. It is designed to screen for the identification of problem and compulsive gambling.
But, it is also necessary to provide a tool to be used by on-line traders. This questionnaire is as follows:
1. Are you trading in the stock market with money you may need during the next year?
2. Are you risking more money than you intended to?
3. Have you ever lied to someone regarding your on-line trading?
4. Are you risking retirement savings to try to get back your losses?
5. Has anyone ever told you that spend too much time on-line?
6. Is investing affecting other life areas (relationships, vocational pursuits, etc.)?
7. If you lost money trading in the market would it materially change your life?
8. Are you investing frequently for the excitement, and the way it makes you feel?
9. Have you become secretive about your on-line trading?
10. Do you feel sad or depressed when you are not trading in the market?
NOTE: If you answer to any of these questions you may be moving from investing to gambling.
***
***
The cost of compulsive gambling and day trading is high for the individual medical or lay professional, the family and society at large. Compulsive gamblers, in the desperation phase of their gambling, exhibit high suicide ideation, as in the case of Mark O Barton’s the murderous day-trader in Atlanta who killed 12 people and injured 13 more in July 29th 1999. His idea actually became a final act of desperation.
Less dramatically, for doctors, is a marked increase in subtle illegal activity. These acts include fraud, embezzlement, CPT® up-coding, medical over utilization, excessive full risk HMO contracting, Stark Law aberrations and other “white collar crimes.” Higher healthcare and social costs in police, judiciary (civil and criminal) and corrections result because of compulsive gambling. The impact on family members is devastating. Compulsive gamblers cause havoc and pain to all family members. The spouses and other family members also go through progressive deterioration in their lives.
In this desperation phase, dysfunctional families are left with a legacy of anger, resentment, isolation, and in many instances, outright hate.
[D] Day Trading Assessment
Internet day trading, like the Internet and telecommunications sectors, become something of a investment bubble a few years ago, suggesting that something lighter than air can pop and disappear in an instant. History is filled with examples: from the tulip mania of 1630 Holland and the British South Sea Bubble of the 1700’s; to the Florida land boom of the roaring twenties and the Great Crash of 1929; to the collapse of Japans stock and real estate market in early 1990’s; and to an all-time high of $1,926 for an ounce of commodity gold a few years ago.
Today it is Ask: $3,388.30 USD Bid: $3,367.30 USD
CONCLUSION
To this list, one might again include smart-phone or mobile day trading.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
There’s an aspect to retirement that many physicians do not plan for … the transition from work and practice to retirement. Your work has been an important part of your life. That’s why the emotional adjustments of retirement may be some of the most difficult ones.
For example, what would you like to do in retirement? Your retirement vision will be unique to you. You are retiring to something not from something that you envisioned. When you have more time, you would like to do more traveling, play golf or visit more often, family and friends. Would you relocate closer to your kids? Learn a new art or take a new class? Fund your grandchildren’s education? Do you have philanthropic goals? Perhaps you would like to help your church, school or favorite charity? If your net worth is above certain limits, it would be wise to take a serious look at these goals. With proper planning, there might be some tax benefits too. Then you have to figure how much each goal is going to cost you.
If you have a list of retirement goals, you need to prioritize which goal is most important. You can rate them on a scale of 1 to 10; 10 being the most important. Then, you can differentiate between wants and needs. Needs are things that are absolutely necessary for you to retire; while wants are things that still allow retirement but would just be nice to have.
Recent studies indicate there are three phases in retirement, each with a different spending pattern [Richard Greenberg CFP®, Gardena CA, personal communication]. The three phases are:
The Early Retirement Years. There is a pent-up demand to take advantage of all the free time retirement affords. You can travel to exotic places, buy an RV and explore forty-nine states, go on month-long sailing vacations. It’s possible during these years that after-tax expenses increase during these initial years, especially if the mortgage hasn’t been paid off yet. Usually the early years last about ten years until most retirees are in their 70’s.
Middle Years. People decide to slow down on the exploration. This is when people start simplifying their life. They may sell their house and downsize to a condo or townhouse. They may relocate to an area they discovered during their travels, or to an area close to family and friends, to an area with a warm climate or to an area with low or no state taxes. People also do their most important estate planning during these years. They are concerned about leaving a legacy, taking care of their children and grandchildren and fulfilling charitable intent. This a time when people spend more time in the local area. They may start taking extension or college classes. They spend more time volunteering at various non-profits and helping out older and less healthy retirees. People often spend less during these years. This period starts when a retiree is in his or her mid to late 70’s and can last up to 20 years, usually to mid to late-80’s.
Late Years. This is when you may need assistance in our daily activities. You may receive care at home, in a nursing home or an assisted care facility. Most of the care options are very expensive. It’s possible that these years might be more expensive than your pre-retirement expenses. This is especially true if both spouses need some sort of assisted care. This period usually starts when the retiree is their 80’s; however they can sometimes start in the middle to the late 70’s.
***
***
[A] Planning issues – early career
Most retirement lifestyle issues do not have to be addressed at this point. Keeping a healthy, balanced lifestyle will help to ensure a more productive retirement. This is the time to focus on the financial aspects of retirement planning.
[B] Planning issues – mid career
If early retirement is a major objective, start thinking about activities that will fill up your time during retirement. Maintaining your health is more critical, since your health habits at this time will often dictate how healthy you will be in retirement
[C] Planning issues – late career
Three to five years before you retire, start making the transition from work to retirement.
Try out different hobbies;
Find activities that will give you a purpose in retirement;
Establish friendships outside of the office or hospital;
Discuss retirement plans with your spouse.
If you plan to relocate to a new place, it is important to rent a place in that area and stay for few months and see if you like it. Making a drastic change like relocating and then finding you don’t like the new town or state might be very costly mistake. The key is to gradually make the transition.
For physicians, like most folks, retirement is the stage in life when one chooses to leave the workforce and live off sources of income or savings that do not require active work. The age at which a person retires, their lifestyle during retirement, and the way they fund that lifestyle, will vary from one person to the next, depending on individual preferences and financial planning. Usually it is age 65.
Some doctors may opt for early retirement to enjoy their hobbies and travel, while others may continue working part-time to stay engaged and supplement their income. Effective retirement planning often involves a combination of savings, investments, and possibly pension benefits to ensure a comfortable and secure post-work life.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Named after Monte Carlo, Monaco, which is famous for its games of chance, MCS is a software technique that randomly changes a variable over numerous iterations in order to simulate an outcome and develop a probability forecast of successfully achieving an outcome.
Endowment Fund Perspective
In private portfolio and fund endowment management, MCS is used to demonstrate the probability of “success” as defined by achieving the endowment’s asset growth and payout goals. In other words, MCS can provide the endowment manager with a comfort level that a given payout policy and asset allocation success will not deplete the real value of the endowment.
Divorce from Judgment
The problem with many quantitative software and other tools is the divorce of judgment from their use. Although useful, both mean variance optimization MVO and MCS have limitations that make it so they should not supplant the physician investor or endowment manager’s experience. MVO generates an efficient frontier by relying upon several inputs: expected return, expected volatility, and correlation coefficients. These variables are commonly input using historical measures as proxies for estimated future performance. This poses a variety of problems.
Problems with MCS
First, the MVO will generally assume that returns are normally distributed and that this distribution is stationary. As such, asset classes with high historical returns are assumed to have high future returns.
Second, an MVO optimizer is not generally time sensitive. In other words, the optimizer may ignore current environmental conditions that would cause a secular shift in a given asset class returns.
Finally, an MVO optimizer may be subject to selection bias for certain asset classes. For example, private equity firms that fail will no longer report results and will be eliminated from the index used to provide the optimizer’s historical data [1].
Example:
As an example, David Loeper, CEO of Wealthcare Capital Management, made the following observation regarding optimization:
Take a small cap “bet” for our theoretical [endowment] with an S&P 500 investment policy. It is hard to imagine that someone in 1979, looking at a 9% small cap stock return premium and corresponding 14% higher standard deviation for the last twenty years, would forecast the relationship over the next twenty years to shift to small caps under-performing large caps by nearly 2% and their standard deviation being less than 2% higher than the 20-year standard deviation of large caps in 1979 [2].
Table: Compares the returns, standard deviations for large and small cap stocks for the 20-year periods ended in 1979 and 1999. Twenty Year Risk & Return Small Cap vs. Large Cap (Ibbotson Data).
1979
1999
Risk
Return
Correlation
Risk
Return
Correlation
Small Cap Stocks
30.8%
17.4%
78.0%
18.1%
16.9%
59.0%
Large Cap Stocks
16.5%
8.1%
13.1%
18.6%
*Reproduced from “Asset Allocation Math, Methods and Mistakes.” Wealthcare Capital Management White Paper, David B. Loeper, CIMA, CIMC (June 2, 2001).
More Problems with MCS
David Nawrocki identified a number of problems with typical MCS as being that most optimizers assume “normal distributions and correlation coefficients of zero, neither of which are typical in the world of financial markets.”
Dr. Nawrocki subsequently describes a number of other issues with MCS including nonstationary distributions and nonlinear correlations.
Finally, Dr. Nawrocki quotes Harold Evensky who eloquently notes that “[t]he problem is the confusion of risk with uncertainty.
Risk assumes knowledge of the distribution of future outcomes (i.e., the input to the Monte Carlo simulation).
Uncertainty or ambiguity describes a world (our world) in which the shape and location of the distribution is open to question.
Contrary to academic orthodoxy, the distribution of U.S. stock market returns is far from “normal”. Other critics have noted that many MCS simulators do not run enough iterations to provide a meaningful probability analysis.
Assessment
Some of these criticisms have been addressed by using MCS simulators with more robust correlation assumptions and with a greater number of iterative trials. In addition, some simulators now combine MVO and MCS to determine probabilities along the efficient frontier.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on March 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Rocking Financial Planning … Old School Advice!
By Dr. David E. Marcinko MBBS MBA MEd CMP®
The economic platitude of the past, such as don’t spend more than 15-20 percent of your net salary on food, or 5-10 percent on medical care, among others, have given rise to the more individualized personal financial ratio concept. Personal ratios, like business ratios, represent benchmarks to compare such parameters as debt, income growth and net worth.
According to Edward McCarthy MIB CFP® – a personal financial expert from Warwick, Rhode Island whom I interviewed about a decade ago – the following represented useful ratios for the lay as well as medical professional [personal communication].
The Ratios:
Basic Liquidity Ratio = liquid assets / average monthly expenses. Should be 4-6 months, or even longer, in the case of a medical professional employed by a financially insecure HMO. In a low interest rate environment, iMBA Inc offers 12-24 months for consideration.
Debt to Assets Ratio = total debt / total assets. A percentage which is high initially, and should decrease with age as the medical professional approaches a debt free existence
Debt to Gross Income Ratio = annual debt repayments / annual gross income. A percentage representing the adequacy of current income for existing debt repayments. Medial professionals should try to keep this below 25-30%.
Debt Service Ratio = annual debt re-payment / annual take-home pay. Medical professionals should try to keep this ratio below about 40%, or have difficulty paying down debt.
Investment Assets to Net Worth-Ratio = investment assets / net worth. This ratio should increase over time, as retirement for the medical professional approaches.
Savings to Income Ratio = savings / annual income. This ratio should also increase over time, especially as major obligations are retired.
Real Growth Ratio = (income this year – income last year) / (income last year – inflation rate). It is desirable for the medical professional to keep this ratio growing faster than the core rate f inflation.
Growth of Net-Worth Ratio = (net worth this year – net worth last year) / net worth last year – inflation rate. Again, this ratio should stay ahead of inflation.By calculating these ratios, perhaps on an annual basis, the medical professional can spot problems, correct them, and continue progressing toward stated financial goals.
Assessment
Now, after ten years, are these traditional ratios and advice still valid today: why or why not?
***
***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Marcinko Associates is a financial guide. We help answer your questions in an empowering way. We educate and empower medical colleagues to understand their financial picture and to make better financial decisions. We strive to simplify everything, clear up confusion, and address specific needs and goals.
Whatever your financial situation, we do not shame, criticize, or sell. We enrich, educate and empower. We work with medical colleagues at every stage of their financial journey, through big life personal changes to annual employment reviews, in order to help them understand, invest, and protect their money and autonomy.
And, like the famed ‘Tibetan Sherpas“, we guide physician entrepreneurs from medical practice business plan creation, funding, start-up operations and strategic management improvement to maximize profits and stream-line patient care quality initiatives.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Book Dr. David E. MarcinkoMBA MEd CMPfor your Next Medical, Pharma or Financial Services Seminar orPersonal and Corporate Coaching Sessions
Dr. Marcinko enjoys personal coaching and public speaking and gives as many talks each year as possible, at a variety of medical society and financial services conferences around the country and world. These have included lectures and visiting professorships at major academic centers, keynote lectures for hospitals, economic seminars and health systems, keynote lectures at city and statewide financial coalitions, and annual keynote lectures for a variety of internal yearly meetings.
His talks tend to be engaging, iconoclastic, and humorous. His most popular presentations include a diverse variety of topics and typically include those in all iMBA, Inc’s textbooks, handbooks, white-papers and most topics covered on this blog.
Did you know that at MARCINKO & Associates, all medical colleagues throughout the United States may contact us when they are considering the sale, purchase, strategic operating improvement, merger, acquisition and/or other financial business or related personal financial planning transaction?
Our difference is “hard” knowledge and insider financial guidance that helps medical colleagues, nurses, private practitioners, clinics, ambulatory surgery, radiology and outpatient wound care centers realize their ultimate economic goals. This typically includes managerial and cost accounting, financial ratio analysis, fair market valuation business appraisals, business plan creation and personal financial planning.
Our “expert witness” business litigation support service and divorce mediation, arbitration, asset division, settlement and second opinion offerings are always available, as well.
And, our “soft” skill professional career guidance and mentoring center includes executive coaching, consulting and mentoring advisory programs for stressed, conflicted or burned-out physicians and medical practitioners.
Most importantly, our professional fees are reasonable and always transparent.
MARCINKO & Associates also serves universities, medical, business, graduate and nursing schools; physicians, dentists, podiatrists, optometrists and legal societies. This includes accountants, financial service providers, wealth and hedge fund managers, emerging entities, hospitals, CEOs and their BODs, the press, media and related organizations.
Achieving your financial, wealth and medical practice management goals is important, but handling everything on your own can be overwhelming. That’s where we come in. At D. E. Marcinko & Associates, our team of dual degree experienced physician advisors and medical consultants is here to guide you every step of the way. We believe in providing unbiased, high-quality financial and business advice.
For example, we offer a one-time written financial plan with oral evaluation for a flat fee with no ongoing sales or assets under management fees or commissions. Together, we can create a personalized financial plan tailored to your unique goals, empowering you to make confident, informed decisions as you navigate your financial future.
Other Services Include:
Estate Planning We have a network of qualified legal professionals that we can refer you to for state specific estate planning needs.
Tax Strategy We can work alongside your CPA for tax planning purposes. If needed, we can refer you to a qualified tax professional.
Investment Analysis If you have investments, we review your accounts to make sure they are aligned with your long-term goals.
401-k Allocations We evaluate your 401(k) allocations and provide recommendations that align with your goals.
Education Savings We help you explore the various ways to plan and save for education expenses.
Insurance & Risk Management We assess your insurance coverage to ensure it adequately protects you against potential risks; as well as evaluate and provide expert litigation witnesses, as needed.
Medical Practice Management We evaluate your current or potential medical practice to determine value and/or private equity offers or physician practice management formats [PPMC] for new, mid-career or retiring physicians, nurses and dentists.
D. E. Marcinko & Associates is unique and fully committed to all phases of a medical professionals personal and business life cycle. We are at your service 24/7: Email MarcinkoAdvisors@outlook.com
The www.MedicalBusinessAdvisors.com is focused solely on appraising medical practices, surgery centers [ASCs], medicine, podiatry, optometry and allied healthcare businesses.
Working with our affiliated partners, like the ME-P and others, we are also available for behemoth multi-specialty medical practices, major clinics, hospitals, related healthcare organizations and networks, and PHOs, etc.
We are backed by the expertise of dedicated appraisers and valuation analysts who are trained by the foremost organizations in our industry www.CertifiedMedicalPlanner.org
Practice owners, attorneys and accountants retain us for projects including, but not limited to the following:.
There are a Myriad of Reasons for Obtaining a Medical Practice Valuation and Appraisal Engagement
Outright selling-buying
Partnership and Associate buy-in / buy-out
Mergers and Acquisitions
Organic growth tracking
Hospital integrations
Private and public reporting
Financing and Venture Capital
Estate and tax planning
Our Capability
We have the ability to provide extensive analysis of value components in healthcare practices and provide appraisals based on business, economic, and market conditions. This involves detailed examination of financials and clinical data in the context of numerous factors including medical specialty, physician supply and demand, payer mix, regulatory environment, regional dynamics, and risk premium.
Assessment
Our methods and approaches adhere to accepted standards of healthcare practice appraisal and utilize direct market data to reach justifiable conclusions. These are documented in a comprehensive report which is tailored to meet the need of the specific engagement.
SAMPLE ENGAGEMENTS: See partial engagement list below.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Frequently, we hear the axiom that asset allocation is the most important investment decision, explaining 93.6% of portfolio returns. The presumption has been that once the risk tolerance and time horizon have been established, investing is simply a matter of implementing a fixed mix of stocks, bonds, and cash using mutual funds selected for this purpose. This axiom is based on a famous study by Brinson, Hood, and Beebower (BHB) published in the Financial Analysts Journal in July/August 1986. It is the stuff of most modern business school and graduate students in economics and finance.
Enter the Critics
One critic claims that BHB’s conclusions and the interpretation of their conclusions are wrong, stating that because of several methodological problems, BHB needed to make certain assumptions for their analysis to go forward. They assumed that the average asset-class weights for the 10-year period studied are the same as the actual normal policy weights; that investments in foreign stocks, real estate, private placements, and venture capital can be proxied by a mix of stocks, bonds, and cash; and that the benchmarks for stocks, bonds, and cash against which fund performance was measured are appropriate. The author believes that each of these assumptions can lead to a faulty measurement of success or failure at market timing and stock selection.
The Jahnke Study
William Jahnke claims that BHB erred in their focus on explaining the variation of quarterly portfolio returns rather than portfolio returns over the 10-year period studied. According to the study, asset allocation policy explains only a small fraction of the range of 10-year portfolio returns earned by the pension funds reported in the study. The author concluded that this discrepancy is caused by the effect of compounding returns. He adds that BHB were wrong to use variance of quarterly returns rather than the standard deviation. Use of standard deviation would reduce the often cited 93.6% to about 79%. Moreover, BHB did not consider the cost of investing, such as operating expenses, management fees, brokerage commissions, and other trading costs, which are more significant for individual investors than for the pension plans studied. Jahnke claims that excessive costs can reduce wealth accumulation by 50%.
Note: (“The Asset Allocation Hoax,” William W. Jahnke, Journal of Financial Planning, February 1997, Institute of Certified Financial Planners [303] 759-4900).
Assessment
Finally, the author takes issue with establishing long-term fixed asset class weights. Asset allocation should be a dynamic process. Higher equity return expectations should in turn produce larger equity allocations, other things being equal.
Conclusion
Are doctors different than the average investor noted in this essay?
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
The Society of Physician Entrepreneurs (SoPE) was established as a community of interest in 2008 by several members of the American Academy of Otolaryngology – Head and Neck Surgery (AAO-HNS), including Dr. Arlen Meyers, the founding past President & CEO. SoPE became a separate and independent legal entity; incorporating in Washington, D.C. in January 2011. It is a 501 (c) 6 member organization with the stated purpose of providing support; idea stage through funding, for physician entrepreneurs with ideas on how to improve healthcare.
SoPE’s vision is to accelerate physician originated biomedical innovation.
The mission of SoPE is to foster scholarship in biomedical entrepreneurship and provide education, training and support; idea stage through funding, to primarily community-based physician entrepreneurs in the interest of better healthcare.
SoPE membership is open to all physicians and also accepts individuals as associate members; representatives of medical device, legal, venture capital, and other firms with an interest in serving and/or supporting physician entrepreneurs.
The science of the modern medical practice valuation can be traced to the Estate of Edgar A. Berg v. Commissioner (T. C. Memo 1991-279). In this case, the Court criticized CPAs as not being qualified to perform business valuations, failing to provide analysis of an appropriate discount rates, and making only general references to justify their “Opinion of Value.”
In rejecting accountants, the Court accepted IRS economists because of background, education and training, as well as discount rate calculations and reproducible evidence applied to the assets being examined. This marked the beginning of the Tax Court leaning toward the side with the most comprehensive appraisal. Previously, it had a tendency to “split the difference.” Now, some feel the Berg case launched the valuation profession; especially for contemporaneous health economists.
But, it was not until after 1995 that the IRS issued guidelines for the valuation of physician practices. As a result, the Uniform Standards of Professional Appraisal Practice [USPAP] requires that a blended constellation of three recognized valuation approaches (income, market, and cost approaches) be considered when estimating fair market value.
Operative Valuation Definitions
When pursuing any discussion of medical practice worth, two key elements must be understood: (1) the valuation process, and (2) fair market value. According to the Dictionary of Health Economics and Finance
Practice valuation is the “the formal process of determining the worth of a healthcare or other medical business entity, at a specific point in time, and the act or process of determining fair market value.”
Fair market value [FMV] is “a legal term generally meaning the price at which a willing buyer will buy, and a willing seller will sell an asset in an open free market with full disclosure.” IRS Revenue Ruling 59-60 clearly states that FMV “is essentially a future prophesy and must be based on facts available at the required date of appraisal”
Unfortunately, the value of a medical practice cannot be directly observed by activity in thinly traded private markets. Perhaps this is why we continually observe the following valuation blunders? They are committed by both sellers and buyers who are pursuing opposite objectives; sale price maximization versus price minimization?
Top 10 Blunders:
Not Understanding What a Medical Practice Valuation Is and Is Not
Valuations are not source document fraud audits.
Valuations are material representations providing a range of transferable worth.
Valuations are reproducible estimates based on economic assumptions.
Valuations are not “back-of-the envelope multiples” using specious benchmarks.
Valuations are defensible and “signed-off” attesting to USPAP/IRS formats.
Financial accounting value [book-value] is not fair market value.
Professional valuators represent only one party at arm’s length; not both sides.
Engagement solicitor and/or valuation payer is the client.
Unbiased valuators do not provide financing or equity-participation schemes. Although not standardized, the Institute of Medical Business Advisors, Inc uses the following three levels that approximate engagement types for the industry.
2. A Limited Valuation lacks additional suggested USPAP procedures. It is considered an “agreed-upon-procedure”, used in circumstances where the client is the only user [i.e., updating a buy-sell agreement, or practice buy-in for a valued associate] and not for external purposes. No onsite visit is needed. A formal Opinion of Value is not rendered.
3. Not Observing Industry Standards, Rules and Regulations
Specifically, in USPAP transactions involving physician practices, the IRS implied:
Ad-Hoc Valuation is low level engagement that provides a gross and non-specific approximation of value based on limited meters by involved parties. Neither a written report, nor an Opinion of Value is rendered. It is often used periodically as an internal organic growth / decline gauge.
A Comprehensive Valuation is an extensive service designed to provide an unambiguous Opinion of Value range. It is supported by all procedures that valuators deem relevant with mandatory onsite review. This “gold-standard” is suitable for contentious situations like divorce, partnership dissolution, estate planning and gifting, etc. The written Opinion of Value is applicable for litigation support activities like depositions and trial. It is also useful for external reporting to bankers, investors, the public and IRS, etc.
4. Not Understanding Engagement Types and Levels
Discounted cash flow (DCF) analysis is the most relevant income approach and must be done on an “after-tax” basis.
Practice collections must be projected based on reasonable assumptions for the practice and market; etc.
Physician compensation must be based on market rates consistent with age, experience and productivity.
Majority premiums and minority discounts are to be considered.Goodwill represents the difference between practice purchase price and the value of the net assets. Personal goodwill results from the charisma, skills and reputation of a specific doctor. Its attributes accrue solely to the individual, are not transferable and can’t be sold. It has little or no economic value as it “goes to the grave” with the doctor. Transferable medical practice goodwill has value, may be transferred, and is defined as the unidentified residual attributes that contribute to the propensity of patients and managed care contracts (and their revenue streams) to return in the future (Schilbach v. Commissioner, T.C. Memo 1991-556). And so, one must also appreciate the: (i) impact of a changing environment; (ii) practice transfer in a local market which can augment or blunt goodwill value; and the (iii) determination of whether patients or HMOs return because of true goodwill, or are mandated by contractual obligations; among many other multi-variable determinants.
Even the Goodwill Registry however, a classic source used to determine the average percentage of revenue contributed to practice goodwill, may be dated for some specialties leading to abnormally high values.
5. Not Understanding the Value of Practice Goodwill: Unlimited life span.
6. Not Understanding the Value of Personal Goodwill: Limited life span.
Now, to further confuse the issue, how each kind of goodwill is allocated in situations like divorce depends on state law. For example, some courts include both kinds of goodwill to be apportioned – some exclude both – and others pursue a case-by-case approach.
7. Not Understanding “Excess Earnings Capitalization”
Another way to determine goodwill value is through “excess earnings capitalization.” This economic method looks at the difference between salary, and what you’d have to pay a comparable doctor replacement.
As an example, when you subtract the numbers, and divide the result by 20%, an important percentage referred to as the Capitalization Rate emerges. The final number gives a dollar value for practice goodwill. Courts seem to prefer this method in divorces because it tends to reflect a practice’s current value.
8. Not Understanding the Present Compensation versus Future Value Paradox
Regardless of practice business model, physician compensation is inversely related to practice value. In other words, the more a doctor takes home in above-average salary, the less the practice is generally worth, and vice versa; ceteris paribus
9. Substituting Benchmarks and Formulas for Practice Specificity
In the stable economic past, industry benchmarks might have been used as quick and inexpensive substitutes for professionally prepared valuations. Muck like preparing one’s own income tax return today – while legal – it is a fraught with peril if challenged. The Courts seem to frown on this simplistic and dated methodology.
Moreover, generic benchmark formulas assume a financial statement reporting standard that just does not exist in public accounting.
Therefore, most every competitive issue that impacts value should be addressed with each practice engagement. This includes, but is not limited to contemporary dislocations by third parties, Medicare and commercial payers; retail clinics and changes in supply/demand and specialty trends; rise of ambulatory surgery centers and specialty hospitals; outsourced care and medical tourism, alterations in resource based-relative value units, APCs, DRGs and newer MS-DRGs; the Medicare Modernization Act, HIPAA, OSHA, EEOC, Sarbanes-Oxley and US Patriot Acts, PP-CA, and ACOs; among other regulations.
Current employee trends to high-deductible health care plans [HD-HCPs] and private concierge medicine must also be considered, as well as demographic and employer shifts to defined contribution plans – from defined benefits plans – to name just a few more complicating issues.
10. Not Aggregating or “Normalizing” Financial Information
Employees may be interviewed and financial information must be gathered before a medical practice can be properly valued. The following data, for the most recent three year period, serves as a starting point:
Sample medical record chart review is increasingly being demanded.
It is especially important to eliminate one-time, non-recurring practice expenses. These are adjusted for excessive or below normal expenses on the profit and loss statement. Such “normalization” can produce a big surprise for benchmark proponents and formula-driven advocates when a selling doctor runs personal expenditures through the practice that a buyer [or Court] wouldn’t consider legitimate. Of course, such shenanigans are less noted using professional USPAP/IRS guidelines. Conversely, you may have to defend legitimate business expenses that an appraiser may seek to normalize. For example, doctors may pay for a vehicle through their practice, but if used to travel between multiple offices and hospitals, the expense may be legitimate. Of course, normalization is a sophisticated and time-intensive process. But, it is where the expert earns his/her professional fee, and defends the resulting valuation range when challenged.The most important credential to look for is fiduciary experience, specificity and independence. Some doctors mistakenly turn to those who may have never appraised a practice before. And, just because an appraiser has initials behind his name, doesn’t mean he understands the peculiarities of medical specialties, especially podiatry. We believe that only an independent health economist, who will be your advocate under Securities Exchange Commission [SEC] fiduciary [not lower “suitability”] guidelines, should be selected. Of course, it is almost impossible to answer concerns regarding fees without specific information. The cost of a valuation can range from $0 (benchmarks-rule of thumb) to $50,000 for an onsite team of experts for behemoth practices and ambulatory surgery centers. Keep in mind that in most cases you want to ensure the value determination will stand up to IRS scrutiny, so the $0 rule-of-thumb is not an optionExternal appraisals, or poorly aggregated financial information, onsite reviews and litigation support services incur additional costs; yet most doctors find the money well spent. Expect to pay a retainer and sign a formal professional engagement letter.
Assessment
Don’t be surprised if a sales-broker does not consider the above issues as the modern health era emerges. Most agent-appraisers are predominantly concerned with earning commissions by working both transaction parties, and may not represent your best interests. And, they are usually not obliged to disclose conflicts-of-interest and don’t provide legal testimony.
As a result, a good medical practice is no longer necessarily a good business; and retiring doctors can no longer automatically expect to extract premium sales prices. Moreover, uninformed young physicians should not be goaded to over-pay. Regardless of your dismay – or delight – in the changing healthcare milieu, always be foreword thinking and remember the admonition, Trust-but Verify, for any business transaction.
But, it is a fait accompli that medical practice worth is presently deteriorating. As the population ages and third-party reimbursements plummet, doctors are commoditized and traditional retail medicine is replaced by more efficient wholesale business models like workplace health clinics. The recent sub-prime mortgage de-fault fiasco, potential tax-reform law expiration and the political specter of a nationalized healthcare system, only adds fuel to the macro-economic fires of uncertainly.
Finally, once practice price is mutually agreed upon, sales contract terms and agreements present a plethora of financing challenges for both involved parties to consider [bank loan payment rates and length, personal promissory guarantees, down-payment offsets, earn-out arrangements, Uniform Commercial Codes-1 asset guarantees, etc] in their due-diligence efforts.
However, most reputable firms use a blended fee-schedule of fixed and hourly rates (plus expenses). So, doctors should expect to spend approximately $5,000-15,000 for an average sized – limited appraisal – that is completely suitable for most internal activities.
Moreover, look-out if the valuation not done at an-arm’s-length and independent manner; or worse still, if it is performed for both parties simultaneously.
Selecting the Wrong Valuator and Not Understanding Professional Fees
Realize too, that the appraiser may also add expenses that have not been incurred; like an office manager’s salary if your spouse is in that role for free. This produces a lower appraised value and is common in small medical practices. Honoraria are another example that does not figure into value calculations.
For example, we recall one doctor who painted his personal residence and wrote it-off as a valid business expense. Deleting other major expenses such as country club memberships, make a practice look more profitable—good news if you’re selling it, bad news if you’re getting a divorce.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Marcinko & Associates is financial guide. We help answer your questions in an empowering way. We educate and guide medical colleagues to understand their financial picture and to make better financial decisions. We strive to simplify everything, clear up confusion, and address specific needs and goals.
Simply put, we’re a financial services company on a mission to empower financial freedom for all healthcare professionals; only. We work with doctors, nurses, medical providers, individuals and all sizes of organizations to offer investment, wealth management and retirement solutions so everyone can have a clear and simple understanding of where their finances and career is today and where it is headed tomorrow.
Whatever your financial situation, we do not shame, criticize, or sell. We enrich, educate and empower. We work only with medical colleagues at every stage of their financial journey [students, interns, residents, practitioners, mid-career and mature physicians], through big life personal changes to annual employment reviews, in order to help them understand, invest, and protect their money and lifestyle.
Assess, develop, and align financial retirement and estate planning goals
Risk Management: Malpractice, home, life, medical, auto and personal indemnity
Life Insurance Need Reviews: whole, universal and term
Business, operations, HR, employment negotiations and medical practice management
Annuity Need Reviews: Indexed and Fixed [Pros and Cons].
***
***
At Marcinko & Associates we discuss specific needs and answer specific questions. We educate and make personalized recommendations that you are free to use, incorporate or disregard. Referrals to trusted specialists and strategic alliance partners then occur if – and as – needed [pro re nata].
According to Wikipedia, Front Running, also known as Tailgating, is the prohibited practice of entering into an equity (stock) trade, option, futures contract, derivative, or security-based swap to capitalize on advance, nonpublic knowledge of a large pending transaction that will influence the price of the underlying security.
Front running is considered a form of market manipulation in many markets. Cases typically involve individual brokers or brokerage firms trading stock in and out of undisclosed, un-monitored accounts of relatives or confederates. Institutional and individual investors may also commit a front running violation when they are privy to inside information. A front running firm either buys for its own account before filling customer buy orders that drive up the price, or sells for its own account before filling customer sell orders that drive down the price.
Front running is prohibited since the front-runner profits from nonpublic information, at the expense of its own customers, the block trade, or the public market.
Scandals
In 2003, several hedge fund and mutual fund companies became embroiled in an illegal late trading scandal made public by a complaint against Bank of America brought by New York Attorney General Eliot Spitzer. A resulting U.S. Securities and Exchange Commission investigation into allegations of front-running activity implicated Edward D. Jones & Co., Inc., Goldman Sachs, Morgan Stanley, Strong Mutual Funds, Putnam Investments, Invesco, and Prudential Securities.
Following interviews in 2012 and 2013, the FBI said front running had resulted in profits of $50 million to $100 million for the bank. Wall Street traders may have manipulated a key derivatives market by front running Fannie Mae and Freddie Mac.
Term Origins
The terms originate from the era when stock market trades were executed via paper carried by hand between trading desks. The routine business of hand-carrying client orders between desks would normally proceed at a walking pace, but a broker could literally run in front of the walking traffic to reach the desk and execute his own personal account order immediately before a large client order.
Likewise, a broker could tail behind the person carrying a large client order to be the first to execute immediately after. Such actions amount to a type of insider trading, since they involve non-public knowledge of upcoming trades, and the broker privately exploits this information by controlling the sequence of those trades to favor a personal position.
Assessment
So, was front-running implicated in the market drop today? OR, a technical correction or Panic selling? Any thoughts.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
The modern medical practice is both similar, and unlike, other businesses today. This disparity often adds to confusion for the private practitioner. And so, the experts at iMBA Inc, list the top 25 most urgent questions in practice financial management, asked by clients to date.
Assessment
Since inception in 2000, the Institute of Medical Business Advisors Inc., has become one of North America’s leading professional health consulting and valuation firms; and focused provider of textbooks, CDs, tools, templates, onsite and distance education for the health economics, administration and financial management policy space. As competition and litigation support activities increase and the cognitive demands of the global marketplace change, iMBA Inc is well positioned with offices in five states and Europe, to meet the needs of medical colleagues, related advisory clients and corporate customers today; and into the future.
And so, your thoughts and comments on this Medical Executive-Post are appreciated. Tell us what you think. Send in your own questions. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Sponsors Welcomed
And, credible sponsors and like-minded advertisers are always welcomed.
“A reliable way to make people believe in falsehoods is frequent repetition, because familiarity is not easily distinguished from truth.” – Daniel Kahneman
As I was watching with interest more [fake] news such as stories surrounding evidence by citations of Russian involvement in US elections and fake prices leading to some violent market gyrations as in Bitcoin and the Corona Virus Pandemic, and societal musings around the thematic of hoaxes … we decided to offer this theme.
Enter the WOOZLE
And so, the Woozle effect, also known as evidence by citation, or a woozle, occurs when frequent citation of previous publications that lack evidence misleads individuals, groups and the public into thinking or believing there is evidence, and non-facts become urban myths and factoids.
Posted on September 26, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Physician Due Diligence is Important
[By Daniel B. Moisand; CFP®, and the ME-P Staff]
While the merits of hiring the right financial advisor [FA] may be clear, hiring the wrong one can be devastating. Medical professionals still tend to have higher incomes and are an attractive target for most financial institutions and scam artists. This fear is a poor excuse for not getting the assistance necessary. Advice about who to engage for financial assistance comes from a hodge-podge of disjointed sources. This leads to good intentions and bad results. Take caution when using the following as sources of advice.
Relying on Family and Friends
By far more people seek financial advice from trusted family members and friends than any other source. This is only natural. It is essential to trust that you are getting advice from a source that means well. It is also important that you get along well with your advisors. Hesitating to communicate with your advisor, even a great advisor, can cause problems even more problematic that getting bad advice from someone you like. While these sources have a good handle on the essential elements of trust and rapport, it is the competence of the advice that is most often the issue. The life and money experiences of those who are close to you certainly have value, but they are not necessarily relevant to your unique goals and circumstances. THINK: Bernie Madoff.
Media
A few years ago, the dominant media force in consumer oriented financial matters was the print media. Magazines and newsletters proliferated with the bull market. More recently however, television has supplanted print even in the bear market. For example, a study now estimates that 80 percent of what the average American knows about current events comes from TV. Why wait three weeks for the next issue when you can get a commentary instantly on the television? There is nothing wrong with watching shows that cover the markets or subscribing to a consumer finance magazine. It is certainly a good idea to be informed. However, be wary of the quality and applicability of information put out by the media.
The Internet
It is easy to run across an ad for prescriptions drugs on television. Images prance across the screen followed by a litany of potential side effects and the obligatory, “Ask your doctor about”. With the expansion of the information superhighway, more and more companies are going direct to the consumer in some manner or another.
Financially speaking this information can be of great benefit but should also generate more concern. It is very easy to project a particular image via the web. The webmaster controls the interaction from what you see to what you hear. One of the results of this is that the Internet has already garnered a reputation as a breeding ground for new scams. More prevalent, however, is the presentation of information meant to be useful that is simply wrong, misinterpreted, or misapplied. The most terrifying source of misinformation on the net is the chat rooms. Here the entire interaction is clouded by anonymity. Some people enter chat rooms because there is a comfort in anonymity when asking a question. There is also a danger in an anonymous answer. When it comes to something as important as your finances or your health, the prudent course should be to take all the advice with a grain of salt. A great deal of consideration to the quality of the source is in order. It is also essential that one understand the level of accountability a source may possess.
Assessment
Much has been written on financial advisor selection, here on the ME-P and elsewhere; but little on how not to select an advisor. We trust this information will be of assistance to the medical professional in some small increment. Send in your FA stories; both good and bad.
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
The enterprise value [EV] tends to be thought of as a theoretical takeover price if a company were to be bought. It is calculated as market capitalization plus debt, minority interest and preferred shares, minus total cash and cash equivalents.
Enterprise value = common equity at market value (this line item is also known as “market cap”) + debt at market value (here debt refers to interest-bearing liabilities, both long-term and short-term) + minority interest at market value, if any + preferred equity at market value + unfunded pension liabilities and other debt-deemed provisions – value of associate companies – cash and cash equivalents.
Posted on September 22, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
WHAT IS IT?
On an earnings call last year Microsoft CEO Satya Nadella said the term “enterprise metaverse.”
By [Avatar] Dr. David Edward Marcinko MBA
DEFINITION: The Metaverse is a collective virtual shared space, created by the convergence of virtually enhanced physical reality and physically persistent virtual space, including the sum of all virtual worlds, augmented reality, and the Internet.
The word “metaverse” is made up of the prefix “meta” (meaning beyond) and the stem “verse” (a back formation from “universe“); the term is typically used to describe the concept of a future iteration of the internet, made up of persistent, shared, 3D virtual spaces linked into a perceived virtual universe.
Once the value of all personal assets and liabilities is known, net worth can be determined with the following formula: Net worth = assets minus liabilities. Obviously, higher is better.
In The Millionaire Next Door, Thomas H. Stanley, PhD, and William H. Danko give the following benchmark for net worth accumulation. Although conservative for physicians of a past generation, it may be more applicable in the future because of current managed care environment. Here is the guide: Multiple your age by your annual pre-tax income from all sources; except inheritances, and then divide by ten.
Example:
As an HMO pediatrician, Dr. Curtis earned $ 90,000 last year. So, if she is 35, her net worth should be at least $ 315,000.
How do you get to that point? In a word, consume less and save more. Stanley and Danko found that the typical millionaire set aside 15 percent of earned income annually and has enough invested to survive 10 years, at current income levels if he stopped working.
Question: If Dr. Curtis lost her job tomorrow, how long could she pay herself the same salary? Could you?
Marcinko & Associates is financial guide. We help answer your questions in an empowering way. We educate and guide medical colleagues to understand their financial picture and to make better financial decisions. We strive to simplify everything, clear up confusion, and address specific needs and goals.
Simply put, we’re a financial services company on a mission to empower financial freedom for all healthcare professionals; only. We work with doctors, nurses, medical providers, individuals and all sizes of organizations to offer investment, wealth management and retirement solutions so everyone can have a clear and simple understanding of where their finances and career is today and where it is headed tomorrow.
Whatever your financial situation, we do not shame, criticize, or sell. We enrich, educate and empower. We work only with medical colleagues at every stage of their financial journey [students, interns, residents, practitioners, mid-career and mature physicians], through big life personal changes to annual employment reviews, in order to help them understand, invest, and protect their money and lifestyle.
Assess, develop, and align financial retirement and estate planning goals
Risk Management: Malpractice, home, life, medical, auto and personal indemnity
Life Insurance Need Reviews: whole, universal and term
Business, operations, HR, employment negotiations and medical practice management
Annuity Need Reviews: Indexed and Fixed [Pros and Cons].
***
***
At Marcinko & Associates we discuss specific needs and answer specific questions. We educate and make personalized recommendations that you are free to use, incorporate or disregard. Referrals to trusted specialists and strategic alliance partners then occur if – and as – needed [pro re nata].
Did you know that at MARCINKO & Associates, all medical colleagues throughout the United States may contact us when they are considering the sale, purchase, strategic operating improvement, merger, acquisition and/or other financial business or related personal financial planning transaction?
Our difference is “hard” knowledge and insider financial guidance that helps medical colleagues, nurses, private practitioners, clinics, ambulatory surgery, radiology and outpatient wound care centers realize their ultimate economic goals. This typically includes managerial and cost accounting, financial ratio analysis, fair market valuation business appraisals, business plan creation and personal financial planning.
Our “expert witness” business litigation support service and divorce mediation, arbitration, asset division, settlement and second opinion offerings are always available, as well.
And, our “soft” skill professional career guidance and mentoring center includes executive coaching, consulting and mentoring advisory programs for stressed, conflicted or burned-out physicians and medical practitioners.
Most importantly, our professional fees are reasonable and always transparent.
MARCINKO & Associates also serves universities, medical, business, graduate and nursing schools; physicians, dentists, podiatrists, optometrists and legal societies. This includes accountants, financial service providers, wealth and hedge fund managers, emerging entities, hospitals, CEOs and their BODs, the press, media and related organizations.
According to colleague David K. Luke MIM, MS-PFP, CMP™ the current structure of the life insurance industry regarding cash-value life insurance policies with most major insurance companies is to reward the selling agent with the entire commission upfront on a newly issued policy. The criticism to this practice is that this of course reduces the needed client-agent reviews and interaction and generates more “churning” and “flipping”. Unscrupulous agents are tempted to sell physician-clients another policy for another commission rather than encourage them to maintain and keep their existing policy, which most likely would have lower costs than any new policy considering the client was younger and most likely in better health with the existing contract. A model in which the insurance agent would have a financial incentive for their client’s continued patronage could create a win-win for both parties. We see this “pay as you” model currently operating successfully with wealth advisors and property/casualty agents, why not life insurance agents [personal communication]?
There are some flaws to this argument. The reality is that the captive life insurance industry and their agents prefer this form of lump compensation. The claim is that selling an individual a life insurance policy (the ultimate intangible product) is hard work, and likewise the 70% – 110% of the first year premium is fair compensation for the efforts. For existing agents to reduce their current income to a fraction of this commission upfront, but convert it into a trail over a multiyear period is actually quite distasteful. Therefore, this change will likewise not be initiated from the Insurance agent or insurance industry side unless other forces prevail.
The drive by the consumer to change this up front lump form of compensation has not yet presented itself in full force. After all, why does the consumer care about how the agent is paid if the consumer is satisfied with the end result? One must acknowledge that the drive to reduce commissions and up front loads in the investment advisory business was driven by the consumer that insisted on lower fees and costs.
However, the relevant costs of a life insurance policy are not quite as obvious. Only by comparing a quote from different companies can a consumer compare costs, and even then it is unknown and not understood how the pricing mechanisms used by the insurance company work. The advent of non-agent sold policies however is decreasing the cost of life insurance (there is no big commission check written to the selling agent) and is hitting the radar of consumers. The consumer can notice this difference if the consumer compares the proposed agent sold policy premium with one sold directly by a financial institution such as USAA or AARP. These companies have a work force of sales people that are compensated primarily on salary. Likewise the company can structure more competitive pricing, and in effect offers a levelized cost (in place of commission) insurance product.
For example, Mark Maurer CFP® of Low Load Insurance Services believes that a levelized compensation basis will not occur unless all the insurance companies were to go to such a plan all at once. If an agent can “pick and choose” he/she may use a “levelized compensation” policy when in a competitive situation, as such a policy should in theory make a policy more inexpensive. An agent would then use the higher “front-end” policy when there is a large up-front premium or in a scenario with limited competition. Mark believes the answer to the whole argument is full disclosure. Both agents and home offices would not want the purchaser to know that 100% or more of their premium is going to sales costs and then products would then get better [personal communication].
The insurance industry has a powerful lobby in Washington. Only market pressure will cause a change in this decades old insurance industry practice that has made many life insurance policies expensive and inefficient. Pricing from non-agent sold life insurance companies will be the impetus that drives the old-line Insurance companies to restructure their commissions to agents.
Insurance agents also remember the days of 8% load mutual fund commissions and minimum $60 dollar commissions on stock trades in the late 1980’s! That is an inflation equivalent of more than $130 per trade, minimum commission, today. The current investing world would laugh at these costs [charges] today. When the physician-consumer realizes, through full disclosure and outside competitive market pressures, that life insurance protection can be more affordable from other non-traditional channels, then s/he will insist on a better, more affordable product.
Ultimately, the big agent driven life insurance companies will have to change their commission structure. The transition is currently in process. Only time will tell now [personal communication].
Did you know that Federal and state laws require Registered Investment Advisors [RIAs] be held to a fiduciary standard? To satisfy this extremely high legal standard, an advisor must act solely in the best interest of the client, even if that interest is in conflict with the advisor’s own financial interests. Investment Advisors [IAs] must disclose any conflict, or potential conflict, to the client prior to and throughout a business engagement. Investment Advisors must fully disclose, in writing, how they are compensated. In addition, most adopt a Code of Ethics to ensure that fiduciary obligations are achieved.
Brokers or Advisors
Unfortunately, not all “financial advisors” work for federally or state-registered investment advisory firms. Many so-called financial advisors are registered representatives, better known as stock-brokers, and are employed by brokerage firms [broker-dealers]. Generally, these registered representatives [RRs] need not comply with the fiduciary duty standard that is owed when you are dealing with a registered investment advisory firm. Because broker-dealers are not necessarily acting in your best interest, the SEC [remember what a fine job former Commissioner Chris Cox did for investors in the Bernie Madoff incident?] and FINRA [NASD] require them to add the following disclosure to your client agreement.
Disclosure
Read this disclosure, and decide if this is the type of relationship you want to dictate your financial security:
“Your account is a brokerage account and not an advisory account. Our interests may not always be the same as yours. Please ask us questions to make sure you understand your rights and our obligations to you, including the extent of our obligations to disclose conflicts of interest and to act in your best interest. We are paid both by you and, sometimes, by people who compensate us based on what you buy. Therefore, our profits, and our salespersons’ compensation, may vary by product and over time.”
Disclaimers
If this disclaimer appears in agreements you are signing, or have already signed, you should ask questions of your advisor. S/he’s probably a broker. Obtain complete disclosure about how he or she is compensated, and where his or her first loyalties lie. Then decide if the relationship is in your best interest [Source: www.focusonfiduciary.com NAPFA Consumer Education Foundation]. Also, consider mediation and arbitration clauses very carefully. Do not wave your rights to litigation. Your patients do not; and neither should you!
Assessment
I am a doctor, former stock-broker, registered-rep, certified financial planner and licensed insurance agent who decided there must be a better way to help physician colleagues. As a health economist, and Founder of www.CertifiedMedicalPlanner.org I’ve believe I’ve found that way.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on September 4, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Fundamentals of Physician Investing
By Daniel B. Moisand CFP®, and ME-P staff
It used to be that the only way to get investments and investment information was through paying commissions to a traditional broker. Then in the 70’s (specifically, May, 1975) the brokerage industry went through significant deregulation allowing for the discounting of commissions. Charles Schwab and Company, among others, was able to eliminate the advice component and offer trades at dramatically reduced rates. The full service brokerage business responded by emphasizing the scope of their services namely research and advice in order to compete. The demand for both has continued to grow, even though research information is now readily available through many sources. These brokerage firms continue to thrive despite their poor performance in analyzing tech stocks and the Enron and Global Grossing debacles. More recent debacles in 2008-09, the flash crash a decade ago and more recent developments are legion, as well.
Fundamental Flaws
The fundamental flaw with these firms is the array of conflicts of interest between the firm and its customers. While the incentive to trade has been well chronicled as a conflict, these firms have not let consumer’s demand for a better-aligned compensation arrangement go unnoticed. Fee-based account relationships have proliferated accordingly. In theory, this type of arrangement, usually a percentage of assets, gives an incentive for performance and service rather than trade activity. This certainly has merit. However, conflicts remain that should be considered.
Pay to Play
The practice of paying brokers, higher levels of compensation for in-house products was commonplace. Today, explicitly higher payouts still exist but are less common. Instead, many firms use the sale of proprietary mutual funds and other products as part of management’s compensation. Other forms of non-monetary compensation such as a better office can be used as incentive for the brokers. The greater profitability of these in-house offerings will keep this conflict around for some time.
Subtle Conflicts of Interest
Less obvious is the conflict between the investment banking arm, the research department, and the retail brokerage operations of a firm. Even firms with no proprietary funds to sell may grapple with this issue. Here, research is pressured to say favorable things about a particular company’s stock by the investment bankers in hopes of obtaining more of that company’s business. When a firm brings a company public odds are great that a “strong buy” rating will come with the IPO. Of course, the lesson remains – consider the source.
Assessment
Traditional brokers have a somewhat higher standard of accountability than the on-line firms as to their accountability. If you buy the stock of a company that goes bankrupt through an on-line broker you have little recourse. After all, that was your choice. If a full-service broker recommended the stock to you, that broker will have to defend the recommendation.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
In recent years, the physician practice market has experienced a noticeable increase in practice merging and acquisitions. Medical practices are being acquired by health systems as a result of Accountable Care Organization (ACO) delivery models; etc.
For physicians, the decision to buy, sell, or merge a medical practice is more complicated than ever, and determining a medical practice’s worth is crucial to this process.
Value Isn’t an Absolute Number
A medical practice’s tangible and intangible assets can be grouped into two broad categories:
Physical assets: Examples are real estate, medical records, leaseholds, medical equipment and furnishings, and accounts receivable (A/R).
Non-physical assets: These include goodwill, restrictive covenants, buy/sell agreements, managed care contracts, and an assembled workforce.
Estimates of value differ markedly, depending on the purpose of the appraisal, the acumen of the appraiser, etc. To help determine the value, some important questions to consider are:
What is the value of the practice for purchase or sale?
What is the value of a practice for merger?
What is the value of practice assets for joint venture with a corporate partner?
What is the value to establish buy-in or buy-out arrangements for partners?
What is the value of practice assets for purchase or sale, apart from ongoing operations?
To answer these questions, physicians (buyers and sellers) must understand how practices are valuated—beginning with the following informal, and then more formal, definitions:
Informal Terms of Valuation
The “asking price” is often arbitrary and difficult to substantiate, and typically is reduced 25-50 percent after negotiations.
The “creative price” is derived by way of creative financing. For example, the practice may provide the down payment.
The “emotional price” may involve either a motivated buyer or seller, who pays an under- or overinflated price for the practice.
The “friendly price” is reserved for associates, partners, or other colleagues.
The “realistic price” is one that both buyer and seller believe is fair.
Formal Terms of Valuation
Most appraisers use “fair market value” (FMV) as the standard to derive a reasonable value for a practice. FMV means an arm’s length transaction between an unpressured, informed buyer and an unpressured, informed seller.
The “business enterprise value” of a practice equals a combination of all assets (tangible and intangible), and the working capital, of a continuing business.
The value of “owner’s equity” equals the combined values of all practice assets (tangible and intangible), less all practice liabilities (booked and contingent).
The “working capital value” equals the excess of current assets (cash, A/R, supplies, inventory, prepaid expenses, etc.) over current liabilities (accounts payable, accrued liabilities, etc.).
Realizing that there is no absolute sales price is the essence of FMV. When determining valuation, look for a price range with a reasonable floor and ceiling.
Understand The Lingo
If you are a practice buyer or seller, make sure you understand terms and appraisal definitions.
That’s a lesson George Farmer, a primary care physician in Florida, learned the hard way. He asked his accountant to appraise his business. When he was ready to sell, his attorney (who also happens to be his brother-in-law) drew up the sales contract. Farmer was pleased that the practice sold quickly for its full asking price.
What he didn’t know (but would discover) is that accounting or “book” value—the figure his accountant gave him—is far different than the FMV that he could have received.
Was the CPA wrong? Not really. Was the doctor incorrect? No. But each was operating under a different set of terms and definitions, without knowledge of each other’s perspectives.
How to Begin Valuation
The following steps should occur before the practice appraisal process begins:
Retain an appraiser (for each side) who understands the changing health care industry.
Aggregate historic practice business information and consolidated financial statements, operating statistics, payer mix, CPT® utilization, acuity rates, etc.
Eliminate one-time, non-recurring expenses, adjusted or normalized for excessive or below normal expenses.
Understand key assumptions used in financial projections.
To determine value, appraisers should follow the American Society of Appraisers’ Principles of Appraisal Practice and Code of Ethics. The IRS issued guidelines in 1995 further suggesting that appraisers use the general methods of the Uniform Standards of Professional Appraisal Practices (USPAP), which recognize three approaches to medical practice valuation.
1. Income Methods
There are two methods to value a practice by income:
(a) Capitalization Method: The excess earnings or capitalization method estimates value by dividing normalized historical or current income by an appropriate rate of return for the buyer. This method does not require assumptions.
(b) Discounted Method: Discounted Cash Flow (DCF): Analysis requires assumptions to estimate practice value by discounting future net cash flows to their present worth based on market rates of return required by an investor. Understanding the key assumptions produces a meaningful estimate of practice value. These assumptions may include:
projections of future practice revenue, productivity, reimbursement trends, and shifts in payer mix
projections of practice cost structures and projected physician compensation
after-tax practice cash flows
reinvestments to replace equipment or other assets
residual practice value at the end of the forecast period
discount rate based on the practice specific weighted average cost of capital
practice efficiencies, operations, and competitive market conditions
The DCF analysis consistently produces higher values than other methods of estimating practice value because there may be supportable reasons to forecast improvements in future practice performance.
2. Marketplace Multiples
Market transaction multiples are ratios developed by correlating actual practice sale prices to key practice performance measurements. Common multiples include comparisons of sale price to revenue, sale price to earnings before interest and taxes (EBIT), sale price to earnings before interest, taxes, and depreciation allowance (EBITDA), gross revenue, net revenue, and the sale price to number of physicians.
Market transaction multiples are typically limited to serving as a benchmark for testing the reasonableness of the other approaches. They are becoming less common and less useful.
3. Cost Approach
The cost approach calls for identification and separate valuation of all the practice assets, including goodwill, depreciated over 15 years.
The cost approach is more labor intensive than using the enterprise analysis to estimate practice value; especially for a new practice, which typically includes the expenses to acquire space, office furnishings, equipment, marketing, advertising, staff development, and losses incurred during the startup period. This estimate of “replacement cost or cost avoidance” value represents an upper limit (or ceiling) of value, and generally is not considered useful in estimating the value of an established medical practice.
Net Income Statement Adjustments
When analyzing a set of financial statements to determine practice value, adjustments (normalizations) generally are needed to produce a clearer picture of likely future income and distributable cash flow. It also allows more of an “apples to apples” line item comparison. This normalization process usually consists of making three main adjustments to a medical practice’s net income (profit and loss) statement.
1. Non-Recurring Items: Estimates of future distributable cash flow should exclude non-recurring items. Proceeds from the settlement of litigation, one-time gains/losses from the selling of assets or equipment, and large write-offs that are not expected to reoccur, each represent potential nonrecurring items. The impact of nonrecurring events should be removed from the practice’s financial statements to produce a clearer picture of likely future income and cash flow.
2. Perquisites: The buyer of a medical practice may plan to spend more or less than the current doctor-owner for physician executive compensation, travel and entertainment expenses, and other perquisites of current management. When determining future distributable cash flow, income adjustments to the current level of expenditures should be made for these items.
3. Non-cash Expenses: Depreciation expense, amortization expense, and bad debt expense are all non-cash items which impact reported profitability. When determining distributable cash flow, you must analyze the link between non-cash expenses and expected cash expenditures.
The annual depreciation expense is a proxy for likely capital expenditures over time. When capital expenditures and depreciation are not similar over time, an adjustment to expected cash flow is necessary.
Some practices reduce income through the use of bad debt expense rather than direct write-offs. Bad debt expense is a non-cash expense that represents an estimate of the dollar volume of write-offs that are likely to occur during a year. If bad debt expense is understated, practice profitability will be overstated.
Balance Sheet Adjustments
Adjustments also can be made to a practice’s balance sheet to remove non-operating assets and liabilities, and to restate asset and liability value at market rates (rather than cost rates).
Assets and liabilities that are unrelated to the core practice being valued should be added to or subtracted from the value, depending on whether they are acquired by the buyer. Examples include the asset value less outstanding debt of a vacant parcel of land, and marketable securities that are not needed to operate the practice. Other non-operating assets, such as the cash surrender value of officer life insurance, generally are liquidated by the seller and are not part of the business transaction.
Assessment
With a basic understanding of practice valuation and the steps involved, buyers and sellers will be better prepared for next steps.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Cimasi, Robert James: Valuation of Hospital in a Changing Reimbursement and Regulatory Environment. Marcinko, DE (Editor): Healthcare Organizations (Financial Management Strategies). Institute of Medical Business Advisors Inc., Atlanta, Ga., 2011
Marcinko, DE: “Getting it Right,” How Much is a Plastic Surgery Practice Really worth? Plastic Surgery Products, August 2006.
Marcinko, DE and Hetico, HR: The Business of Medical Practice (third edition). Springer Publishing,New York, N.Y., 2011.
Marcinko, DE and Hetico; HR: Risk Management and Insurance Planning for Physicians and Advisors, Jones and Bartlett Publishers, Sudbury,Mass., 2007.
Marcinko, DE and Hetico; HR: Financial Planning for Physicians and Advisors, Jones and Bartlett Publishers, Sudbury, Mass., 2007.
Marcinko, DE and Hetico, HR: Dictionary of Health Insurance and Managed Care, Springer Publishing, New York, N.Y., 2007.
Marcinko, DE and Hetico, HR: Dictionary of Health Economics and Finance, Springer Publishing, New York, N.Y., 2007.
In Part 1, we discussed how to establish fair market value (FMV) for a medical practice in the article, “Establish Your Practice’s Fair Market Value.” This time, we’ll review important terms and conditions for the sale acquisition and transaction.
Unfortunately, as a general rule, medical practice worth is presently deteriorating. A good medical practice is no longer a good business necessarily, and selling doctors can no longer automatically expect to extract a premium sale price. Nevertheless, appraising your medical practice on a periodic basis can play a key role in obtaining maximum value for it.
Competent practice valuation specialists typically charge a retainer to cover out-of-pocket expenses. Fees should not be based on a percentage of practice value, and may take 30-45 days to complete. Flat fees should be the norm because a sliding scale or percentage fee may be biased toward over-valuation in a declining marketplace. Fees range from $7,500-$50,000 for the small to large medical practice or clinic.
Expect to pay a retainer and sign a formal, professional engagement letter. Seek an unbiased and independent viewpoint. Buyer and sellers should each have their own independent appraisal done, using similar statistics, accounting measures, and economic assumptions.
At the Institute of Medical Business Advisors, Inc www.MedicalBusinessAdvisors.com we use three engagement levels that vary in intensity, purpose, and cost:
1. A comprehensive valuation provides an unambiguous value range. It is supported by most all procedures that valuators deem relevant, with mandatory onsite review. This gold standard is suitable for contentious situations. A written “opinion of value” is applicable for litigation support activities like depositions and trial. It is also useful for external reporting to bankers, investors, the public, Internal Revenue Service (IRS), etc.
2. A limited valuation lacks additional suggested Uniform Standards of Professional Appraisal Practice (USPAP) procedures. It is considered to be an “agreed upon engagement,” when the client is the only user. For example, it may be used when updating a buy/sell agreement, or when putting together a practice buy-in for a valued associate. This limited valuation would not be for external purposes, so no onsite visit is necessary and a formal opinion of value is not rendered.
3. An ad-hoc valuation is a low level engagement that provides a gross non-specific approximation of value based on limited parameters or concerns involved parties. Neither a written report nor an opinion of value is rendered. It is often used periodically as an internal organic growth/decline gauge.
Structure Sales Transactions and Acquisitions
When the practice price has been determined and agreed on, the actual sales deal can be structured in a couple of ways:
(1) Stock Purchase v. Asset Purchase
In an asset transaction, the buyer will receive a tax amortization benefit associated with the intangible value of the business. This tax amortization represents a non-cash expense benefiting the buyer. In this case, the present value of those future tax benefits is added to the business enterprise value.
(2) Corporate Transactions
Typical private deals in the past involved some multiple (ratio) of earning before income taxes (EBIT)—usually a combination of cash, restricted stock, notes receivable, and possibly assumption of liabilities. For some physician hospital organizations, and public deals, the receipt of common stock can increase the practice price by as much as 40-50 percent (to accept the corresponding business risk, in lieu of cash).
Complete the Deal
The deal structure will vary depending on whether the likely buyer is a private practitioner, health system or a corporate partner. Some key issues to consider in the “art of the deal” include:
Working capital (in or out?): Including working capital in the transaction will increase the sale price.
Stock vs. asset transaction: Structuring the deal as an asset purchase will increase practice value due to the tax amortization benefits received by the buyer for intangible assets of the practice.
Common stock premium: The total sale price can be significantly higher than a cash equivalent price for accepting the risk and relative illiquidity of common stock as part of the payment.
Physician compensation: If your goal is to maximize practice value, take home a lower salary to increase practice sale price. The reverse is also true.
Understand Private Deal Structure
Assuming a practice sale is a private transaction, deal negotiations are based on the following pricing methodologies:
Seller financing: Many transactions involve an earn-out arrangement where the buyer puts money down and pays the balance under a formula based on future revenues, or gives the seller a promissory note under similar terms. Seller financing decreases a buyer’s risks (the longer the terms, the lower the risk). Longer terms demand premiums, while shorter terms demand discounts. Premiums that buyers pay for a typical seller-financed practice are usually more than what you would expect from a simple time value of money calculation, as a result of buyer risk reduction from paying over time, rather than up front with a bank loan or all cash. Remember to obtain a life insurance policy on the buyer.
Down payment: The greater the down payment for acquisition of a medical practice, the greater the risk is to the buyer. Consequently, sellers who will take less money up front can command a higher than average price for their practice, while sellers who want more down usually receive less in the end.
Taxation: Tax consequences can have a major impact on the price of a medical practice. For instance, a seller who obtains the majority of the sales price as capital gains can often afford to sell for a much lower price and still pocket as much or more than if the sales price were paid as ordinary income. Value attributed to the seller’s patient list, medical records, name brand, good will, and files qualifies for capital gains treatment. Value paid for the selling doctor’s continuing assistance after the sale and value attributed to a non-compete agreement are taxed at ordinary income. A buyer willing to allocate more for items with capital gains treatment, or a seller willing to take more in ordinary income, can frequently negotiate a better price. This is the essence of economically prudent practice transition planning.
Sidestep Common Buyer Blunders
Here are 10 blunders to avoid, as a buyer:
1. Believing the selling doctor’s attestations. Always verify data through an independent appraisal.
2. Wanting to change the culture of the practice. Be careful: Patients may not adjust quickly to change.
3. Using all available cash without keeping a reserve for potential contingencies.
4. Creating a conflict with the seller by recognizing a weakness and continually focusing on it for a bargain price.
5. Failing to realize that managed care plan contracts can be lost quickly or may not be always transferable.
6. Suffering from analysis paralysis. Money cannot be made by continually checking out a medical practice, only by actually running one.
7. Not appreciating the uniqueness of each practice, and using inaccurate “rules of thumb” from the golden age of medicine.
8. Not realizing that practice worth and goodwill value have plummeted lately and continue to decline in most parts of the country.
9. Not understanding that practice brokers may play both sides of the buy/sell equation for profit. Brokers usually are not obligated to disclose conflicts of interest, are not fiduciaries, and do not provide testimony as a court-approved expert witness.
10. Not hiring an appraisal professional who will testify in court, if need be, using the IRS-approved USPAP methods of valuation. Always assume that the appraisal will be contested (many times, it is).
After pricing and contracting due diligence has been performed, the next step in the medical practice sale process—as Donald Trump might say—is just good, old-fashioned negotiation.
Cimasi, R.J., A.P. Sharamitaro, T.A. Zigrang, L.A.Haynes. Valuation of Hospitals in a Changing Reimbursement and Regulatory Environment. Edited by David E. Marcinko. Healthcare Organizations: Financial Management Strategies. Specialty Technical Publishers, 2008.
Marcinko, D.E. “Getting it Right: How much is a plastic surgery practice really worth?” Plastic Surgery Practice, August 2006.
Marcinko, D.E., H.R. Hetico. The Business of Medical Practice (3rd ed). Springer Publishing,New York,N.Y., 2011.
Marcinko, D.E. and H.R. Hetico. Risk Management and Insurance Planning for Physicians and Advisors. Jones and Bartlett Publishers, Sudbury, Mass., 2007.
Marcinko, D.E. and H.R. Hetico. Financial Planning for Physicians and Advisors. Jones and Bartlett Publishers, Sudbury, Mass., 2007.
Marcinko, D.E. and H.R. Hetico. Dictionary of Health Insurance and Managed Care. Springer Publishers, New York, N.Y., 2007.
Marcinko, D.E. and H.R. Hetico. Dictionary of Health Economics and Finance. Springer Publishers,New York,N.Y., 2007.
There are a Myriad of Reasons for Obtaining a Medical Practice Valuation and Appraisal Engagement:
Outright selling-buying
Partnership and Associate buy-in / buy-out
Mergers and Acquisitions
Organic growth tracking
Hospital integrations
Private and public reporting
Financing and Venture Capital
Estate and tax planning
Our Capability
We have the ability to provide extensive analysis of value components in healthcare practices and provide appraisals based on business, economic, and market conditions. This involves detailed examination of financials and clinical data in the context of numerous factors including medical specialty, physician supply and demand, payer mix, regulatory environment, regional dynamics, and risk premium.
According to colleagues Jeffrey S. Coons PhD CFA, the Efficient Market Hypothesis (EMH) states that securities are fairly priced based on information about their underlying cash flows and that physician investors should not expect to consistently outperform the market over the long-term.
There are three distinct forms of EMH that vary by the type of information that is reflected in a security’s price:
Weak Form: This form holds that investors will not be able to use historical data to earn superior returns on a consistent basis. In other words, the financial markets price securities in a manner that fully reflects all information contained in past prices.
Semi-Strong Form: This form asserts that security prices fully reflect all publicly available information. Therefore, investors cannot consistently earn above normal returns based solely on publicly available information, such as earnings, dividend, and sales data.
Strong Form: This form states that the financial markets price securities such that, all information (public and non-public) is fully reflected in the securities price; investors should not expect to earn superior returns on a consistent basis, no matter what insight or research they may bring to the table.
While a rich literature has been established for doctors regarding to test whether EMH actually applies in any of its three forms in real world markets – probably the most difficult evidence to overcome for backers of EMH is the existence of a vibrant money management and mutual fund industry charging value-added fees for their services.
In fact, no less than Warren Buffett has suggested that the markets are decidedly not efficient.
As a physician executive or investor, if you don’t ordinarily deal in options or other financial derivatives, you may need to brush up on puts and calls, straddles, strangles (or combinations), forwards, futures, swaps, spreads, and non-equity options such as stock index options. Options and other financial derivatives can be used by astute physicians, financial advisors and investment managers not only as a tool to better manage the investment risks potentially affecting portfolio returns, but to craft truly value-added investment strategies customized to meet investors’ needs. The three main types of risk of equity securities (individual company, industry, and market) can be mitigated with options.
Individual Company Risk
Individual company risk can be addressed with equity options in that company’s stock. Industry risk can be reduced through the use of narrow-based index options, while market risk can be mitigated with broad-based index options. Sophisticated hedging and risk management strategies can be designed using both equity and stock index options.
Exotic Stock Options?
Some doctors feel that options have been generally thought of as too risky or exotic or requiring too much capital, resulting in a general lack of comfort. A decade ago, these opinions have no doubt been shaped by the collapse of Bearings and the resulting bitter litigation by Proctor & Gamble and Gibson Greetings against Bankers Trust. Last decade, it was Enron, Tyco, WorldCom, Lehman Brothers, AIG, BA, Fannie, Freddie and all those involved in the “flash-crash” of 2008-09; etc.
Assessment
Generally, premiums paid in buying puts or calls are nondeductible capital expenditures and may produce a capital gain or loss depending upon whether the option is sold prior to exercise, the call expires unexercised, or, if the option is exercised, it is added to the basis of the stock (call) or deducted from it (put). Premiums received for writing puts or calls are not included in income upon receipt but are deferred until the option expires, is exercised, or a closing transaction is entered into. Non-equity options (index options) are marked to market at year end (same as for futures) with 60% considered long-term capital gain and 40% considered short-term.
Note: “An Introduction to Options and Other Financial Derivative Strategies,” by Thomas J. Boczar, Trust & Estates, February 1997, pp. 43–68, INTERTEC/K-III Publishing.
The primary objectives in using derivatives are:
1. Risk management and hedging (reducing or eliminating downside risk, monetizing a position, deferring and possibly avoiding capital gains taxes)
2. Leveraging investment capital
3. Enhancing after-tax returns
4. Creating customized risk/return profiles
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES: