BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on November 16, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
American Depository Receipts Defined
In the modern era of globalization, financial instruments that connect investors across borders have become indispensable. Among these, American Depository Receipts (ADRs) stand out as a powerful mechanism that allows U.S. investors to participate in foreign equity markets without the complexities of international trading. ADRs not only simplify access to global companies but also enhance the ability of foreign corporations to raise capital in the United States. This essay explores the origins, structure, regulatory frameworks, benefits, risks, and real-world examples of ADRs, highlighting their role in the integration of global finance.
Historical Development
The concept of ADRs emerged in 1927 when J.P. Morgan introduced the first ADR for the British retailer Selfridges. At the time, American investors faced significant hurdles in purchasing foreign shares, including currency conversion, unfamiliar trading practices, and regulatory differences. ADRs solved these problems by creating a U.S.-based certificate that represented ownership in foreign shares, denominated in dollars, and traded on American exchanges.
Over the decades, ADRs expanded rapidly, especially during the post-World War II era when globalization accelerated. By the late 20th century, ADRs had become a mainstream tool for accessing international equities, with companies from Europe, Asia, and Latin America increasingly using them to tap into U.S. capital markets.
Structure and Mechanics
An ADR is issued by a U.S. depositary bank, which holds the underlying shares of a foreign company in custody. Each ADR corresponds to a specific number of shares—sometimes one, sometimes multiple, or even a fraction. Investors buy and sell ADRs in U.S. dollars, and dividends are paid in dollars as well, eliminating the need for currency conversion.
Key structural features include:
Depositary Banks: Institutions such as J.P. Morgan, Citibank, and Bank of New York Mellon act as custodians and issuers of ADRs.
ADR Ratios: The number of foreign shares represented by one ADR can vary, allowing flexibility in pricing.
Trading Platforms: ADRs can be listed on major exchanges like the NYSE or NASDAQ, or traded over-the-counter.
Regulatory Framework
ADRs are subject to U.S. securities regulations, which vary depending on the level of ADR issued:
Level I ADRs: Traded over-the-counter, requiring minimal disclosure. They are primarily used for visibility rather than fundraising.
Level II ADRs: Listed on U.S. exchanges, requiring compliance with SEC reporting standards, including reconciliation of financial statements to U.S. GAAP or IFRS.
Level III ADRs: Allow foreign companies to raise capital directly in U.S. markets through public offerings. These require the highest level of regulatory compliance, including registration with the SEC and adherence to corporate governance standards.
This tiered system ensures that investors receive appropriate levels of transparency while giving foreign companies flexibility in their approach to U.S. markets.
Benefits for Investors
ADRs offer numerous advantages to American investors:
Convenience: Investors can buy shares in foreign companies without dealing with foreign exchanges or currencies.
Diversification: ADRs provide access to global firms across industries, enhancing portfolio diversification.
Transparency: ADRs listed on U.S. exchanges must comply with SEC regulations, ensuring reliable financial reporting.
Liquidity: ADRs trade on familiar platforms, making them easily accessible to retail and institutional investors alike.
Benefits for Companies
Foreign corporations also benefit significantly from ADRs:
Access to Capital: ADRs open the door to the world’s largest pool of investors.
Global Visibility: Listing in the U.S. enhances reputation and credibility.
Improved Liquidity: Shares become more widely traded, increasing market efficiency.
Investor Base Diversification: Companies can attract both domestic and international investors, reducing reliance on local markets.
Risks and Challenges
Despite their advantages, ADRs carry certain risks:
Currency Risk: ADR values are tied to foreign shares denominated in local currencies, making them vulnerable to exchange rate fluctuations.
Political and Economic Risk: Instability in the issuing company’s home country can affect performance.
Taxation: Dividends may be subject to foreign withholding taxes before conversion to U.S. dollars.
Regulatory Differences: Even with SEC oversight, differences in accounting standards and corporate governance can pose challenges.
Case Studies
1. Alibaba Group (China) Alibaba’s ADRs, listed on the NYSE in 2014, marked one of the largest IPOs in history, raising $25 billion. This demonstrated the power of ADRs to connect Chinese companies with American investors, despite regulatory complexities between the two countries.
2. Toyota Motor Corporation (Japan) Toyota’s ADRs have long provided U.S. investors with access to one of the world’s largest automakers. By listing ADRs, Toyota expanded its investor base and strengthened its global presence.
3. Royal Dutch Shell (Netherlands/UK) Shell’s ADRs illustrate how multinational corporations use ADRs to maintain visibility in U.S. markets while managing complex cross-border structures.
The Role of ADRs in Global Finance
ADRs embody the globalization of capital markets. They facilitate cross-border investment, enhance market efficiency, and foster economic integration. For investors, ADRs represent a gateway to international diversification. For companies, they provide access to the deepest capital markets in the world.
Conclusion
American Depositary Receipts are more than just financial instruments; they are symbols of global interconnectedness. By bridging the gap between U.S. investors and foreign companies, ADRs have reshaped the landscape of international finance. They balance convenience with exposure to global risks, offering both opportunities and challenges. As globalization continues to evolve, ADRs will remain a vital tool for investors and corporations alike, reinforcing their role as a cornerstone of modern capital markets.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
BASIC DEFINITIONS
***
***
The velocity of money is a fundamental concept in macroeconomics that measures how quickly money circulates through the economy. It reflects the frequency with which a unit of currency is used to purchase goods and services within a given time period. This metric is crucial for understanding economic activity, inflation, and the effectiveness of monetary policy.
At its core, the velocity of money is calculated using the formula:
This equation shows how many times money turns over in the economy to support a given level of economic output. For example, if the GDP is $20 trillion and the money supply (say, M2) is $10 trillion, the velocity is 2—meaning each dollar is used twice in a year to purchase goods and services.
There are different measures of money supply used in this calculation, most commonly M1 and M2. M1 includes the most liquid forms of money, such as cash and checking deposits, while M2 includes M1 plus savings accounts and other near-money assets. The choice of which measure to use depends on the context and the specific economic analysis being conducted.
The velocity of money is influenced by several factors:
Consumer and business confidence: When people feel optimistic about the economy, they are more likely to spend rather than save, increasing velocity.
Interest rates: Higher interest rates can encourage saving and reduce spending, lowering velocity. Conversely, lower rates can stimulate borrowing and spending.
Inflation expectations: If people expect prices to rise, they may spend more quickly, increasing velocity.
Technological and structural changes: Innovations in digital payments and shifts in consumer behavior can also affect how quickly money moves.
Historically, the velocity of money has fluctuated with economic cycles. During periods of economic expansion, velocity tends to rise as spending increases. In contrast, during recessions or periods of uncertainty, velocity often falls as consumers and businesses hold onto cash. For instance, during the 2008 financial crisis and the early stages of the COVID-19 pandemic, velocity dropped sharply due to reduced consumer spending and increased saving.
In recent years, the U.S. has experienced persistently low velocity, even amid significant increases in the money supply. This phenomenon has puzzled economists and raised questions about the effectiveness of monetary policy. Despite aggressive stimulus measures, much of the new money has remained in savings or financial markets rather than circulating through the real economy.
Understanding the velocity of money is essential for policymakers. A low velocity may signal weak demand and justify expansionary fiscal or monetary policies. Conversely, a high velocity could indicate overheating and the need for tightening measures to prevent inflation.
In conclusion, the velocity of money is a dynamic indicator of economic vitality. It helps economists and central banks assess the flow of money, the strength of demand, and the potential for inflation.
While often overlooked by the public, it plays a vital role in shaping economic policy and understanding the broader health of the economy.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Physicians are increasingly facing car repossessions in 2025 due to rising debt, high vehicle prices, and economic pressures that are reshaping the financial landscape for medical professionals.
Traditionally viewed as financially secure, doctors are now among the growing number of Americans struggling to keep up with auto loan payments. The surge in car repossessions—expected to reach a record 10.5 million assignments by the end of 2025—has not spared the medical community. While physicians often earn higher-than-average incomes, they also carry significant financial burdens, including student loan debt, practice overhead, and personal expenses. These pressures are being amplified by macroeconomic forces such as inflation, high interest rates, and stagnant reimbursement rates.
One of the key contributors to this trend is the soaring cost of vehicles. In 2025, the average price of a new car in the U.S. surpassed $50,000, a dramatic increase from just a decade ago. For physicians who rely on vehicles for commuting between hospitals, clinics, and private practices, owning a reliable car is not a luxury—it’s a necessity. However, the combination of high sticker prices and elevated interest rates—averaging 7.3% for used cars and 11.5% for new cars—has made financing increasingly difficult.
***
***
Even high-income professionals are not immune to the broader auto loan crisis. Subprime auto loan delinquencies reached 6.6% in early 2025, the highest rate in over 30 years.While physicians typically fall into the prime or super-prime credit categories, many are still affected by cash flow disruptions, especially those in private practice or rural areas where patient volumes and insurance reimbursements have declined. Additionally, younger doctors with substantial student debt may find themselves overleveraged, making it harder to keep up with car payments.
The emotional and professional toll of a car repossession can be significant. Beyond the embarrassment and logistical challenges, losing a vehicle can disrupt a physician’s ability to provide care, attend emergencies, or maintain a consistent work schedule. This can lead to further income loss, creating a vicious cycle of financial instability.
To combat this trend, some physicians are turning to financial advisors to restructure their debt, refinance auto loans, or downsize to more affordable vehicles. Others are advocating for systemic reforms, such as student loan forgiveness, higher Medicare reimbursements, and better financial literacy training during medical education.
In conclusion, the rise in car repossessions among doctors is a stark reminder that no profession is immune to economic volatility. As the cost of living continues to climb and financial pressures mount, even those in traditionally stable careers must adapt to protect their assets and livelihoods.
Addressing this issue requires both individual financial planning and broader policy changes to ensure that physicians can continue to serve their communities without the looming threat of personal financial collapse.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
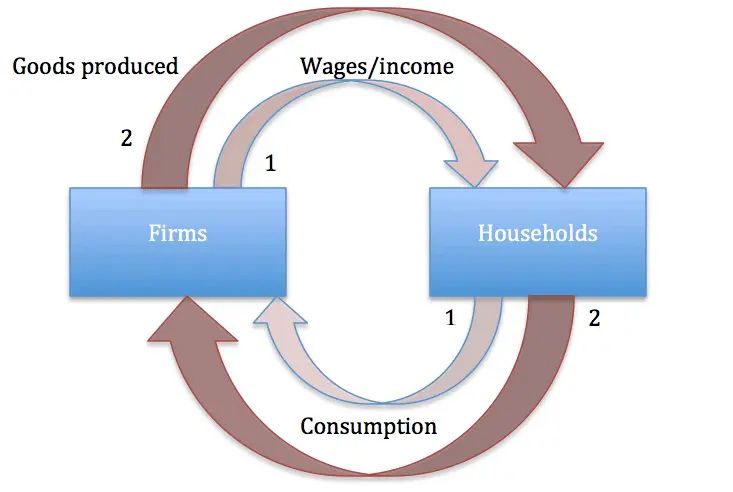
Say’s Law, named after the French economist Jean‑Baptiste Say, is a foundational idea in classical economics. Often summarized as “supply creates its own demand,” the law suggests that the act of producing goods and services inherently generates the income necessary to purchase them. This principle shaped economic thought throughout the 19th century and continues to influence debates about markets, government intervention, and the causes of economic crises.
Origins and Meaning Jean‑Baptiste Say introduced his law in the early 1800s in his Treatise on Political Economy. He argued that production is the source of demand: when producers create goods, they pay wages, rents, and profits, which in turn become purchasing power. In this view, general overproduction is impossible because every supply of goods corresponds to an equivalent demand. If imbalances occur, they are temporary and limited to specific sectors, not the economy as a whole.
Core Principles Say’s Law rests on several assumptions:
Markets are self‑correcting: Any surplus in one area leads to adjustments in prices and production.
Money is neutral: It serves only as a medium of exchange, not as a driver of demand.
Production drives prosperity: Economic growth depends on increasing output, not stimulating consumption.
No long‑term unemployment: Since supply creates demand, workers displaced in one industry will eventually find employment elsewhere.
These ideas aligned with classical economists’ belief in minimal government intervention and the efficiency of free markets.
Influence on Classical Economics Say’s Law became a cornerstone of classical economics, reinforcing the belief that recessions or depressions were temporary and self‑correcting. Economists like David Ricardo and John Stuart Mill adopted versions of the law, using it to argue against policies aimed at stimulating demand. The law supported laissez‑faire approaches, suggesting that governments should avoid interfering with markets, as production itself would ensure economic balance.
Criticism and Keynesian Revolution Say’s Law faced its greatest challenge during the Great Depression of the 1930s. Widespread unemployment and idle factories contradicted the idea that supply automatically generates demand. John Maynard Keynes famously rejected Say’s Law in his General Theory of Employment, Interest, and Money (1936). Keynes argued that demand, not supply, drives economic activity. He showed that insufficient aggregate demand could lead to prolonged recessions, requiring government intervention through fiscal and monetary policies.
Keynes’s critique marked a turning point in economics. While Say’s Law emphasized production, Keynesian economics highlighted consumption and demand management. This shift reshaped economic policy, leading to active government roles in stabilizing economies.
Modern Perspectives Today, Say’s Law is not accepted in its original form, but elements of it remain relevant. Supply‑side economists, for example, argue that policies encouraging production—such as tax cuts and deregulation—can stimulate growth. In contrast, Keynesians stress the importance of demand management. The debate reflects a broader tension in economics: whether prosperity depends more on producing goods or ensuring people have the means and willingness to buy them.
Conclusion: Say’s Law was a bold attempt to explain the self‑sustaining nature of markets. While its claim that “supply creates its own demand” proved too simplistic in the face of modern economic realities, it remains a vital part of the history of economic thought. The controversy surrounding Say’s Law highlights the evolving nature of economics, where theories are tested against real‑world crises and adapted to new circumstances. Even today, discussions of supply‑side versus demand‑side policies echo the enduring influence of Say’s original insight.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The singularity promises to revolutionize medicine by accelerating diagnostics, treatment, and longevity—but it also demands ethical vigilance and systemic transformation.
The concept of the technological singularity refers to a hypothetical future moment when artificial intelligence (AI) surpasses human intelligence, triggering exponential advances in technology. In medicine, this could mark a turning point where AI-driven systems outperform human clinicians in diagnosis, treatment planning, and even biomedical research. While the singularity remains speculative, its implications for healthcare are profound and multifaceted.
One of the most promising impacts is in diagnostics and precision medicine. AI systems trained on vast datasets of medical images, genetic profiles, and patient histories could detect diseases earlier and more accurately than human doctors. For example, algorithms already outperform radiologists in identifying certain cancers from imaging scans. As we approach the singularity, these systems may evolve into autonomous diagnostic agents capable of real-time analysis and personalized recommendations, tailored to each patient’s unique biology.
Another transformative area is drug discovery and development. Traditional pharmaceutical research is slow and costly, often taking over a decade to bring a new drug to market. AI could dramatically shorten this timeline by simulating molecular interactions, predicting therapeutic targets, and optimizing clinical trial designs. With superintelligent systems, the pace of innovation could accelerate to the point where treatments for currently incurable diseases—like Alzheimer’s or certain cancers—become feasible within months.
The singularity also opens doors to radical longevity and human enhancement. Advances in nanotechnology, genomics, and regenerative medicine may converge to extend human lifespan significantly. AI could help decode the aging process, identify biomarkers of cellular decline, and engineer interventions that slow or reverse it. Some theorists even envision a future where aging is treated as a curable condition, and mortality becomes a choice rather than a biological inevitability.
However, these breakthroughs come with serious ethical and societal challenges. Data privacy, algorithmic bias, and access inequality are critical concerns. If singularity-level AI is controlled by a few corporations or governments, it could exacerbate global health disparities. Moreover, the replacement of human clinicians with machines raises questions about empathy, trust, and accountability in care. Who is responsible when an AI makes a life-altering mistake?
To navigate this future responsibly, medicine must embrace interdisciplinary collaboration. Ethicists, technologists, clinicians, and policymakers must work together to ensure that AI systems are transparent, equitable, and aligned with human values. Regulatory frameworks must evolve to keep pace with innovation, and medical education must prepare practitioners to work alongside intelligent machines.
In conclusion, the singularity represents both a promise and a peril for medicine. It offers unprecedented opportunities to enhance human health, but also demands careful stewardship to avoid unintended consequences.
As we edge closer to this horizon, the challenge will be not just technological, but deeply human: to harness intelligence beyond our own in service of healing, compassion, and justice.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on November 10, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Taxation is a cornerstone of modern governance, providing the financial resources necessary for governments to deliver public services, maintain infrastructure, and support social programs. While paying taxes is a legal obligation, individuals and businesses often seek ways to reduce their tax burden. This pursuit gives rise to two distinct concepts: tax avoidance and tax evasion. Though they may sound similar, the difference between them is profound, hinging on legality, ethics, and consequences.
Tax avoidance refers to the use of lawful strategies to minimize tax liability. It involves taking advantage of deductions, exemptions, credits, and other provisions explicitly allowed by tax laws. For example, individuals may contribute to retirement accounts, claim mortgage interest deductions, or invest in tax-free municipal bonds. Businesses may structure operations to benefit from tax incentives or credits designed to encourage innovation, sustainability, or job creation. In essence, tax avoidance is legal tax planning—a way to reduce obligations while staying within the boundaries of the law.
***
***
By contrast, tax evasion is illegal. It involves deliberately misrepresenting or concealing information to avoid paying taxes. Common forms of evasion include underreporting income, overstating deductions, hiding assets offshore, or falsifying records. Unlike avoidance, which is permitted and often encouraged, evasion constitutes fraud against the government. The consequences are severe: individuals and corporations found guilty of tax evasion may face hefty fines, penalties, and even imprisonment.
The distinction between the two lies in compliance versus deception. Tax avoidance complies with the letter of the law, even if it sometimes exploits loopholes. Tax evasion, however, breaks the law outright. This difference is critical not only legally but also ethically. While avoidance is lawful, aggressive avoidance strategies—especially by wealthy individuals or multinational corporations—can raise moral questions. Critics argue that such practices undermine fairness, shifting the tax burden onto ordinary citizens. Governments often respond by reforming tax codes to close loopholes and ensure equity.
Tax evasion, on the other hand, is universally condemned. It erodes trust in the tax system, deprives governments of essential revenue, and places greater strain on compliant taxpayers. Moreover, evasion can damage reputations, leading to loss of credibility and public backlash for businesses or individuals caught engaging in fraudulent practices.
In summary, tax avoidance is legal and strategic, while tax evasion is illegal and punishable. Both aim to reduce tax liability, but they differ fundamentally in method and consequence. Avoidance leverages lawful opportunities provided by tax codes, whereas evasion relies on deception and concealment. Understanding this distinction is vital for taxpayers, as crossing the line from avoidance into evasion can result in serious legal and financial repercussions. Ultimately, responsible tax planning requires not only knowledge of the law but also an awareness of ethical considerations, ensuring that efforts to minimize taxes do not compromise legality or fairness.
In the competitive world of financial services, attracting and retaining clients is a constant challenge. To stand out, many financial advisors employ strategic marketing tactics known as “loss leaders”—free or discounted services designed to showcase value and build trust. These offerings serve as entry points for potential clients, allowing advisors to demonstrate expertise and initiate long-term relationships.
One of the most common loss leaders is the free initial consultation. This no-obligation meeting gives prospective clients a chance to discuss their financial goals, ask questions, and get a feel for the advisor’s approach. For the advisor, it’s an opportunity to assess the client’s needs and present tailored solutions. While no revenue is generated from this meeting, it often leads to paid engagements once the client feels confident in the advisor’s capabilities.
Another popular tactic is offering a complimentary financial plan or portfolio review. These services provide tangible insights into a client’s current financial situation and suggest improvements. By delivering real value upfront, advisors build credibility and demonstrate their analytical skills. Clients who receive actionable advice are more likely to continue working with the advisor on a paid basis.
Educational content also plays a key role in loss leader strategy. Advisors frequently host free webinars, workshops, or seminars on topics like retirement planning, tax strategies, or investment basics. These events not only educate attendees but also position the advisor as a thought leader. Attendees often leave with a better understanding of their financial needs and a desire to seek personalized guidance.
In the digital realm, advisors may offer free tools and assessments on their websites. These include retirement readiness calculators, risk tolerance quizzes, and budgeting templates. Such tools engage users and provide personalized feedback, creating a natural segue into one-on-one consultations. Additionally, offering free newsletters or eBooks helps advisors stay top-of-mind while delivering ongoing value.
Some advisors go further by waiving fees for introductory services, such as account setup or the first few months of investment management. This lowers the barrier to entry and encourages hesitant clients to try the service. Once clients experience the benefits, they’re more likely to commit long-term.
Loss leaders are not limited to high-net-worth individuals. Advisors targeting younger or less affluent clients may offer free debt management plans or budgeting assistance. These services address immediate concerns and build loyalty among clients who may become more profitable as their financial situations improve.
Ultimately, loss leaders are about building relationships. By offering something of value without immediate compensation, financial advisors demonstrate their commitment to helping clients succeed. This fosters trust, encourages engagement, and often leads to lasting partnerships. In a field where reputation and reliability are paramount, loss leaders serve as powerful tools for growth and differentiation.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 9, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Thought
By Dr. David Edward Marcinko MBA MEd
***
***
Thought experiments have long been a powerful tool in science and philosophy, allowing thinkers to explore complex ideas without the need for immediate empirical testing. Among the most famous is Schrödinger’s Cat,devised in 1935 by physicist Erwin Schrödinger to highlight the strange implications of quantum mechanics. In this scenario, a cat is placed in a sealed box with a radioactive atom, a Geiger counter, and a vial of poison. If the atom decays, the Geiger counter triggers the release of poison, killing the cat. According to the Copenhagen interpretation of quantum mechanics, until the box is opened and observed, the atom exists in a superposition of decayed and undecayed states. Consequently, the cat is simultaneously alive and dead until observation collapses the wavefunction. This paradox illustrates the difficulty of applying quantum principles to macroscopic objects and remains a central discussion point in debates about the nature of reality.
Schrödinger’s Cat is not unique in its ability to provoke deep reflection. Throughout history, scientists and philosophers have used thought experiments to challenge assumptions and clarify theories. For example, Galileo’s falling bodies experiment imagined two objects of different weights tied together and dropped from a tower. By reasoning through the scenario, Galileo demonstrated that heavier objects do not fall faster than lighter ones, contradicting Aristotelian physics and paving the way for Newtonian mechanics.
Another influential thought experiment is Einstein’s elevator, which he used to develop the theory of general relativity. Einstein imagined an observer inside a sealed elevator, unable to see outside. If the elevator were accelerating upward in space, the observer would feel pressed to the floor, just as if gravity were acting on them. This equivalence between acceleration and gravity became the foundation of Einstein’s revolutionary insight that gravity is not a force but the curvature of spacetime.
In thermodynamics, Maxwell’s demon presents a paradox about the second law of entropy. James Clerk Maxwell imagined a tiny demon controlling a door between two chambers of gas. By selectively allowing fast-moving molecules to pass one way and slow-moving molecules the other, the demon could seemingly decrease entropy without expending energy. This thought experiment sparked debates about the nature of information, energy, and the limits of physical laws, influencing modern discussions in statistical mechanics and information theory.
Philosophy also abounds with thought experiments. Descartes’ evil demon questioned whether our perceptions could be manipulated, casting doubt on the certainty of knowledge. More recently, John Searle’s Chinese Room challenged the idea that computers can truly “understand” language, distinguishing between syntax and semantics in artificial intelligence.
In conclusion, Schrödinger’s Cat remains a symbol of quantum strangeness, but it is part of a broader tradition of thought experiments that have shaped human understanding. From Galileo’s tower to Einstein’s elevator, Maxwell’s demon to Searle’s room, these imaginative scenarios allow us to probe the boundaries of knowledge, test the coherence of theories, and confront paradoxes that empirical experiments alone cannot resolve. They remind us that science is not only about observation but also about the creative power of the human mind to envision possibilities beyond immediate reality.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Diworsification is a term coined by Peter Lynch to describe when investors over‑diversify their portfolios, adding too many holdings and ultimately reducing returns instead of improving them.
Diversification has long been heralded as one of the cornerstones of sound investing. By spreading capital across different asset classes, industries, and geographies, investors can reduce risk and protect themselves against the volatility of individual securities. Yet, as with many strategies, there exists a point where the benefits diminish and the practice becomes counterproductive. This phenomenon, known as diworsification, was popularized by legendary investor Peter Lynch to describe the tendency of investors and corporations to dilute their strengths by expanding too broadly.
At its core, diworsification occurs when the pursuit of safety leads to excessive complexity. For individual investors, this often manifests in portfolios bloated with dozens or even hundreds of stocks, mutual funds, or exchange‑traded funds. While the intention is to minimize risk, the result is frequently a portfolio that mirrors the market index but with higher costs and less focus. Instead of achieving superior returns, the investor ends up with average performance weighed down by management fees, trading expenses, and the difficulty of monitoring so many positions. In essence, the investor has sacrificed the potential for meaningful gains in exchange for a false sense of security.
Corporations are not immune to this trap. In the corporate world, diworsification describes the tendency of firms to expand into unrelated businesses, diluting their competitive advantage. A company that excels in consumer electronics, for example, may attempt to branch into unrelated industries such as food services or real estate. Without the expertise, synergies, or strategic fit, these ventures often fail to deliver value, distracting management and eroding shareholder wealth. History is replete with examples of conglomerates that grew too large, too fast, only to later divest their non‑core businesses in recognition of the inefficiencies created.
The dangers of diworsification are not merely theoretical. They highlight the importance of discipline in both investing and corporate strategy. For investors, the lesson is clear: diversification should be purposeful, not indiscriminate. A well‑constructed portfolio might include a mix of equities, bonds, and alternative assets, but each holding should serve a specific role—whether it is growth, income, or risk mitigation. Beyond a certain point, adding more securities does not reduce risk meaningfully; instead, it complicates decision‑making and reduces the chance of outperforming the market.
Similarly, for corporations, strategic focus is paramount. Expansion should be guided by core competencies and long‑term vision rather than the allure of short‑term growth. Firms that resist the temptation to chase every opportunity are better positioned to strengthen their brand, innovate within their domain, and deliver sustainable value to shareholders.
In conclusion, diworsification serves as a cautionary tale against the excesses of diversification. While spreading risk is essential, overdoing it can undermine performance and clarity. Both investors and corporations must strike a balance between breadth and focus, ensuring that every addition to a portfolio or business strategy enhances rather than dilutes overall strength. In other words, “diversification means you will always have to say you’re sorry.”
True wisdom lies not in owning everything, but in owning the right things.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
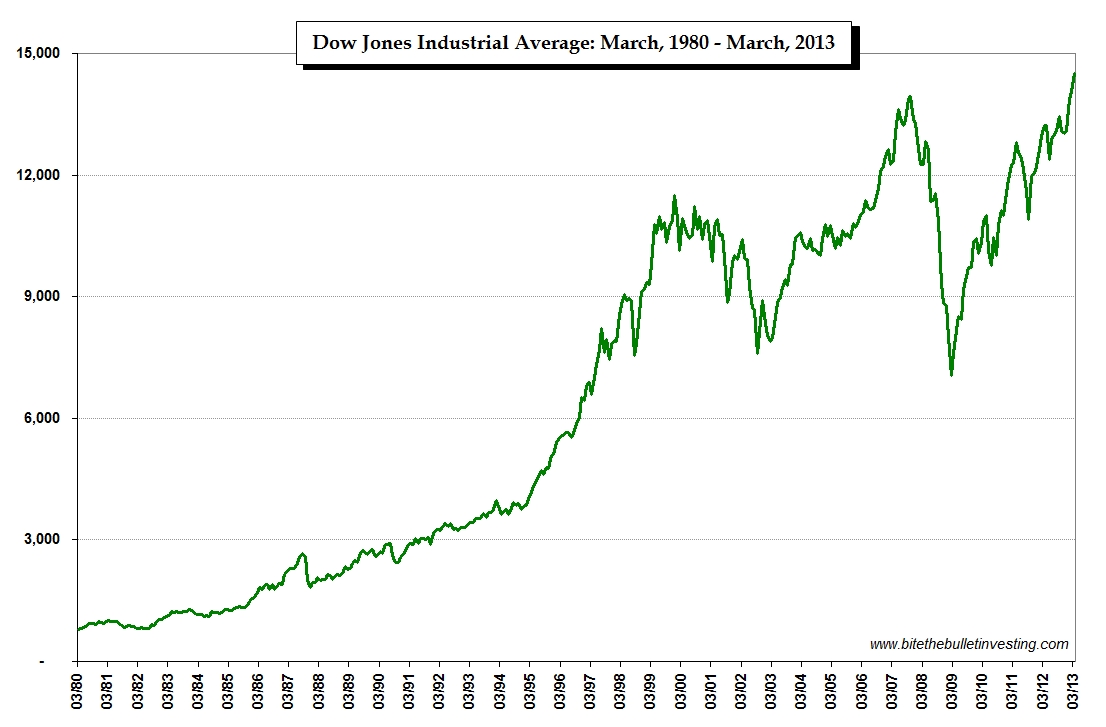
The thirty companies included in the Dow Jones Industrial Average are listed in the updated chart below.
The list is sorted by each component’s weight in the index. The weight of each company is determined by the price of the stock. A $100 stock will be weighted more than a $30 stock. If a stock splits its corresponding weighting in the Dow Jones will be reduced as its price will be about half of what it was prior to the split.
Historian Cyril Parkinson’s wrote in his book Parkinson’s Law,
“The time spent on any item of the agenda will be in inverse proportion to the sum [of money] involved.”
EXAMPLE: Parkinson described a fictional finance committee with three tasks: approval of a $10 million nuclear reactor, $400 for an employee bike shed, and $20 for employee refreshments in the break room.
The committee approves the $10 million nuclear reactor immediately, because the number is too big to contextualize, alternatives are too daunting to consider, and no one on the committee is an expert in nuclear power.
Bike Shed Effect: The bike shed gets considerably more debate. Committee members argue whether a bike rack would suffice and whether a shed should be wood or aluminum, because they have some experience working with those materials at home.
Employee refreshments take up two-thirds of the debate, because everyone has a strong opinion on what’s the best coffee, the best cookies, the best chips, etc.
Absurd: The world is filled with these absurdities. In personal finance, Ramit Sethi recently said we should stop asking $3 questions (should I buy coffee?) and ask more $30,000 questions (should I buy a smaller home?). Most people don’t, because it’s hard and intimidating. In any given moment the easiest way to deal with a big problem is to ignore it and fill your time thinking about a smaller one.
***
***
Assessment: Your thoughts and comments related to the post Corona Virus Pandemic, meetings and time management and psychology are appreciated.
Posted on November 4, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
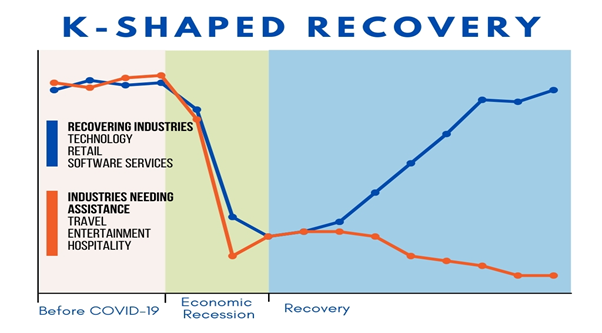
The term “K-shaped economy” emerged during the COVID-19 pandemic to describe a recovery marked by stark divergence—where some sectors and social groups rebound rapidly while others continue to decline. Unlike traditional V-shaped or U-shaped recoveries, which imply uniform economic improvement, the K-shaped model reflects a split trajectory: the upward arm of the “K” represents those who thrive, while the downward arm captures those left behind. This phenomenon has profound implications for economic policy, social equity, and long-term stability.
At the heart of the K-shaped economy is inequality. High-income individuals, white-collar professionals, and large corporations often benefit from technological advances, remote work flexibility, and access to capital. For example, tech giants like Apple, Microsoft, and Alphabet saw record profits during the pandemic, fueled by digital transformation and cloud services. Meanwhile, lower-income workers—especially in hospitality, retail, and service industries—faced job losses, reduced hours, and limited access to healthcare or financial safety nets. This divergence widened existing income and wealth gaps, exacerbating social tensions.
Sectoral performance also illustrates the K-shaped divide. Industries such as e-commerce, software, and logistics surged, while travel, entertainment, and small businesses struggled. The rise of automation and artificial intelligence further tilted the scales, favoring companies that could invest in innovation while displacing low-skilled labor. In education, students from affluent families adapted to online learning with ease, while those from disadvantaged backgrounds faced digital barriers and learning loss. These disparities underscore how economic recovery is not just uneven—it’s structurally imbalanced.
Geography plays a role too. Urban centers with diversified economies and strong tech sectors rebounded faster than rural or manufacturing-heavy regions. Housing markets in affluent areas soared, driven by low interest rates and remote work migration, while renters and first-time buyers faced affordability crises. Even within cities, neighborhoods with better infrastructure and public services recovered more quickly, deepening the urban-suburban divide.
Policymakers face a daunting challenge in addressing the K-shaped recovery. Traditional stimulus measures may not reach the most vulnerable populations without targeted interventions. Expanding access to education, healthcare, and digital infrastructure is essential to leveling the playing field. Progressive taxation, wage support, and small business aid can help bridge the gap, but require political will and fiscal discipline. Central banks must balance inflation control with inclusive growth, avoiding policies that disproportionately benefit asset holders.
The long-term consequences of a K-shaped economy are significant. Persistent inequality can erode trust in institutions, fuel populism, and hinder social mobility. Economic growth may slow if large segments of the population remain underemployed or financially insecure. To build a resilient and inclusive future, governments, businesses, and civil society must collaborate to ensure that recovery lifts all boats—not just the yachts.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 3, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko; MBA MEd
***
***
Classic Definition: In “The Exercise Paradox,” Herman Pontzer asserts that greater physical activity does not allow people to control weight. He goes on to describe studies on how the human body burns calories that help to explain why this is so.
Modern Circumstance: But in one of these studies, “couch potatoes” expended an average of around 200 fewer calories a day, compared with moderately active subjects. A difference of 200 fewer calories a day equates to more than 20 fewer pounds a year. Year after year after year, that really adds up.
Paradox Example: Cyclists participating in the Tour de France are said to ingest more than 5,000 calories a day. This would seem to be way too much. So why do they do it? And why don’t they become obese?
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Turning 50 with little to no savings can be daunting, especially for a doctor who has spent decades in a demanding profession. Yet, all is not lost. With strategic planning, discipline, and a willingness to adapt, a broke 50-year-old physician can still build a solid retirement foundation by age 65.
First, it’s essential to confront the financial reality. This means calculating current income, expenses, debts, and any assets, however small. A clear picture allows for realistic goal-setting. The target should be to save aggressively—ideally 30–50% of income—over the next 15 years. While this may seem steep, doctors often have above-average earning potential, even in their later years, which can be leveraged.
Next, lifestyle adjustments are crucial. Downsizing housing, eliminating unnecessary expenses, and avoiding new debt can free up significant cash flow. If possible, relocating to a lower-cost area or refinancing existing loans can also help. Every dollar saved should be redirected into retirement accounts such as a 401(k), IRA, or a solo 401(k) if self-employed. Catch-up contributions for those over 50 allow for higher annual deposits, which can accelerate growth.
Investing wisely is non-negotiable. A diversified portfolio with a mix of stocks, bonds, and alternative assets can provide both growth and stability. Working with a fiduciary financial advisor ensures that investments align with retirement goals and risk tolerance. Time is limited, so the focus should be on maximizing returns without taking reckless risks.
Increasing income is another powerful lever. Many doctors can boost earnings through side gigs like telemedicine, consulting, teaching, or locum tenens work. These flexible options can add tens of thousands annually without requiring a full career shift. Additionally, monetizing expertise—writing, speaking, or creating online courses—can generate passive income streams.
Debt reduction must be prioritized. High-interest loans, especially credit card debt, can erode savings potential. Paying off these balances aggressively while avoiding new liabilities is key. For student loans, exploring forgiveness programs or refinancing options may offer relief.
Finally, mindset matters. Retirement at 65 doesn’t have to mean complete cessation of work. It can mean transitioning to part-time roles, passion projects, or advisory positions that provide income and fulfillment. The goal is financial independence, not necessarily total inactivity.
In conclusion, while starting late is challenging, a broke 50-year-old doctor can still retire comfortably at 65. It requires a blend of financial discipline, income optimization, smart investing, and lifestyle changes. With focus and determination, the next 15 years can be transformative—turning a precarious situation into a secure and dignified retirement.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on October 25, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
PODCAST: National Prescription Drug Take Back Day
October 25, 2025
By Dr. David Edward Marcinko MBA MEd
***
The National Prescription Drug Take Back Day aims to provide a safe, convenient, and responsible means of disposing of prescription drugs, while also educating the general public about the potential for abuse of medications.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
President Donald Trump signed a pardon on Wednesday for convicted crypto executive Changpeng Zhao, who founded the Binance crypto exchange, White House Press Secretary Karoline Leavitt said in a statement. “President Trump exercised his constitutional authority by issuing a pardon for Mr. Zhao, who was prosecuted by the Biden Administration in their war on cryptocurrency,” Leavitt said. “In their desire to punish the cryptocurrency industry, the Biden Administration pursued Mr. Zhao despite no allegations of fraud or identifiable victims.”
Zhao was sentenced to four months in prison after reaching a deal with the Justice Dept. to plead guilty to charges of enabling money laundering at Binance, which he ran at the time. The U.S. also ordered Binance to pay more than $4 billion in fines and forfeiture, while Zhao agreed to pay $50 million in fines. A spokesperson for Binance did not immediately respond to a request for comment yesterday.
***
The History of Cryptocurrency: From Concept to Revolution
Cryptocurrency has transformed the global financial landscape, offering a decentralized alternative to traditional banking systems. Its history is rooted in decades of technological innovation, philosophical ideals, and economic experimentation.
🌐 Early Foundations
The concept of digital currency predates Bitcoin by several decades. In 1982, cryptographer David Chaum published a groundbreaking paper on secure digital transactions, laying the foundation for future developments in electronic money. Chaum later founded DigiCash in the 1990s, which introduced the idea of anonymous digital payments using cryptographic protocols. Although DigiCash eventually failed, it was a crucial stepping stone in the evolution of cryptocurrency.
The Birth of Bitcoin
The true revolution began in 2008 when an anonymous figure—or group—known as Satoshi Nakamoto released the Bitcoin whitepaper titled “Bitcoin: A Peer-to-Peer Electronic Cash System.” This document proposed a decentralized digital currency that used blockchain technology to record transactions transparently and securely without the need for a central authority.
On January 3, 2009, Nakamoto mined the first block of the Bitcoin blockchain, known as the Genesis Block. The first real-world Bitcoin transaction occurred in May 2010, when programmer Laszlo Hanyecz paid 10,000 BTC for two pizzas—an event now celebrated annually as Bitcoin Pizza Day.
Blockchain and Beyond
Bitcoin’s success inspired the development of other cryptocurrencies and blockchain platforms. Ethereum, launched in 2015 by Vitalik Buterin, introduced smart contracts—self-executing agreements coded directly into the blockchain. This innovation expanded the use of cryptocurrency beyond simple transactions to decentralized applications (dApps), finance (DeFi), and even digital art (NFTs).
Other notable cryptocurrencies include Litecoin, Ripple (XRP), and Cardano, each offering unique features such as faster transaction speeds, improved scalability, or enhanced privacy.
***
***
⚖️ Challenges and Controversies
Despite its promise, cryptocurrency has faced significant hurdles. Regulatory uncertainty, security breaches, and market volatility have raised concerns among governments and investors. High-profile hacks, such as the Mt. Gox exchange collapse in 2014, highlighted the risks associated with digital assets.
Governments around the world have responded differently—some embracing crypto innovation, others imposing strict regulations or outright bans. The rise of central bank digital currencies (CBDCs) reflects an effort to merge the benefits of crypto with the stability of fiat systems.
🚀 The Future of Crypto
Today, cryptocurrency is more than a niche technology—it’s a global phenomenon. Major companies accept Bitcoin, institutional investors hold crypto assets, and blockchain is being integrated into industries from healthcare to supply chain management.
As the technology matures, the focus is shifting toward scalability, sustainability, and interoperability. Whether it becomes a mainstream financial tool or remains a disruptive alternative, cryptocurrency has undeniably reshaped how we think about money, trust, and digital ownership.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on October 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Diwali, Deepavali or Dipavali
By Dr. David Edward Marcinko MBA Med
Diwali, Deepavali or Dipavali is the Hindu festival of lights, which is celebrated every autumn in the northern hemisphere.
One of the most popular festivals of Hinduism, Diwali symbolizes the spiritual “victory of light over darkness, good over evil and knowledge over ignorance”.
***
***
During the celebration, temples, homes, shops and office buildings are brightly illuminated. The preparations, and rituals, for the festival typically last five days, with the climax occurring on the third day coinciding with the darkest night of the Hindu Lunisolar month Kartika.
In the Gregorian calendar, the festival generally falls between mid-October and mid-November.
🏦 100 Minus Age Rule: Subtract your age from 100 to estimate the percentage of your portfolio to invest in stocks. The rest goes to bonds or safer assets.
Rule of 110 or 120: A modern twist—subtract your age from 110 or 120 to allow for more stock exposure in a low-interest environment.
Diversify, Don’t Speculate: Spread investments across asset classes to reduce risk.
Don’t Invest What You Can’t Afford to Lose: Especially for speculative assets like crypto or startups.
📈 Growth & Returns
Rule of 72: Divide 72 by your annual return rate to estimate how many years it takes to double your money.
Time in the Market Beats Timing the Market: Staying invested long-term usually outperforms trying to predict short-term moves.
Start Early, Compound Often: The earlier you invest, the more compound interest works in your favor.
🧾 Budgeting & Saving
50/30/20 Rule: Allocate 50% of income to needs, 30% to wants, and 20% to savings/investments.
Emergency Fund Rule: Save 3–6 months of living expenses before investing aggressively.
Pay Yourself First: Automatically invest a portion of your income before spending.
🧠 Behavioral & Strategy Tips
Buy What You Understand: Don’t invest in companies or assets you don’t comprehend.
Avoid Emotional Decisions: Fear and greed are the enemies of smart investing.
Rebalance Annually: Adjust your portfolio to maintain your target asset allocation.
Don’t Chase Past Performance: What worked last year may not work this year.
🏦 Retirement & Withdrawal
The 4% Rule: Withdraw 4% of your retirement savings annually to make it last ~30 years.
Save 15% of Income for Retirement: A common target for long-term financial security.
Max Out Tax-Advantaged Accounts First: Prioritize 401(k), IRA, or Roth IRA before taxable accounts.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The U.S. healthcare system is often criticized for its high costs, unequal access, and inconsistent outcomes. With nearly 30 million Americans uninsured and many more underinsured, the question arises: could socialized medicine be the solution to these systemic issues?
Socialized medicine refers to a system where the government owns and operates healthcare facilities and employs medical professionals, funded primarily through taxation. While the term is often used pejoratively in American discourse, countries like the United Kingdom and Sweden have long embraced such models. These systems guarantee universal access to healthcare, regardless of income or employment status.
One of the strongest arguments in favor of socialized medicine is its potential to reduce overall healthcare costs. In the U.S., administrative expenses, profit margins, and fragmented billing systems contribute to exorbitant prices. A centralized system could streamline operations, negotiate better drug prices, and eliminate the need for private insurance middlemen. Countries with socialized systems typically spend less per capita on healthcare while achieving comparable or better health outcomes.
Moreover, socialized medicine could address the issue of healthcare access. In the current U.S. model, losing a job often means losing health insurance. Even with the Affordable Care Act, many Americans face high premiums and deductibles. A government-run system would ensure that healthcare is a right, not a privilege, and that no one is denied care due to financial constraints.
***
***
However, critics argue that socialized medicine could lead to longer wait times, reduced innovation, and lower quality of care. They point to examples in Canada and the U.K. where patients sometimes wait weeks or months for non-emergency procedures. Additionally, skeptics fear that government control could stifle competition and reduce incentives for medical advancement.
Yet, these concerns may be overstated. Many countries with socialized systems still foster innovation through public-private partnerships and maintain high standards of care. France, for example, combines universal coverage with private providers and consistently ranks among the top healthcare systems globally.
Transitioning to socialized medicine in the U.S. would be a monumental task, requiring political will, public support, and a reimagining of healthcare financing. It would disrupt entrenched interests, including insurance companies and pharmaceutical firms. But if the goal is to create a more equitable, efficient, and humane system, socialized medicine deserves serious consideration.
In conclusion, while not a panacea, socialized medicine offers a compelling framework for addressing the deep-rooted problems in U.S. healthcare. By prioritizing access, affordability, and public health over profit, it could pave the way for a healthier and more just society.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Do you ever wish you could acquire specific information for your career activities without having to complete a university Master’s Degree or finish our entire Certified Medical Planner™ professional designation program? Well, Micro-Certifications from the Institute of Medical Business Advisors, Inc., might be the answer. Read on to learn how our three Micro-Certifications offer new opportunities for professional growth in the medical practice, business management, health economics and financial planning, investing and advisory space for physicians, nurses and healthcare professionals.
Micro-Certification Basics
Stock-Brokers, Financial Advisors, Investment Advisors, Accountants, Consultants, Financial Analyists and Financial Planners need to enhance their knowledge skills to better serve the changing and challenging healthcare professional ecosystem. But, it can be difficult to learn and demonstrate mastery of these new skills to employers, clients, physicians or medical prospects. This makes professional advancement difficult. That’s where Micro-Certification and Micro-Credentialing enters the online educational space. It is the process of earning a Micro-Certification, which is like a mini-degree or mini-credential, in a very specific topical area.
Micro-Certification Requirements
Once you’ve completed all of the requirements for our Micro-Certification, you will be awarded proof that you’ve earned it. This might take the form of a paper or digital certificate, which may be a hard document or electronic image, transcript, file, or other official evidence that you’ve completed the necessary work.
Uses of Micro-Certifications
Micro-Certifications may be used to demonstrate to physicians prospective medical clients that you’ve mastered a certain knowledge set. Because of this, Micro-Certifications are useful for those financial service professionals seeking medical clients, employment or career advancement opportunities.
Examples of iMBA, Inc., Micro-Certifications
Here are the three most popular Micro-Certification course from the Institute of Medical Business Advisors, Inc:
1. Health Insurance and Managed Care: To keep up with the ever-changing field of health care physician advice, you must learn new medical practice business models in order to attract and assist physicians and nurse clients. By bringing together the most up-to-date business and medical prctice models [Medicare, Medicaid, PP-ACA, POSs, EPOs, HMOs, PPOs, IPA’s, PPMCs, Accountable Care Organizations, Concierge Medicine, Value Based Care, Physician Pay-for-Performance Initiatives, Hospitalists, Retail and Whole-Sale Medicine, Health Savings Accounts and Medical Unions, etc], this iMBA Inc., Mini-Certification offers a wealth of essential information that will help you understand the ever-changing practices in the next generation of health insurance and managed medical care.
2. Health Economics and Finance: Medical economics, finance, managerial and cost accounting is an integral component of the health care industrial complex. It is broad-based and covers many other industries: insurance, mathematics and statistics, public and population health, provider recruitment and retention, health policy, forecasting, aging and long-term care, and Venture Capital are all commingled arenas. It is essential knowledge that all financial services professionals seeking to serve in the healthcare advisory niche space should possess.
3. Health Information Technology and Security: There is a myth that all physician focused financial advisors understand Health Information Technology [HIT]. In truth, it is often economically misused or financially misunderstood. Moreover, an emerging national HIT architecture often puts the financial advisor or financial planner in a position of maximum uncertainty and minimum productivity regarding issues like: Electronic Medical Records [EMRs] or Electronic Health Records [EHRs], mobile health, tele-health or tele-medicine, Artificial Intelligence [AI], benefits managers and human resource professionals.
Other Topics include: economics, finance, investing, marketing, advertising, sales, start-ups, business plan creation, financial planning and entrepreneurship, etc.
How to Start Learning and Earning Recognition for Your Knowledge
Now that you’re familiar with Micro-Credentialing, you might consider earning a Micro-Certification with us. We offer 3 official Micro-Certificates by completing a one month online course, with a live instructor consisting of twelve asynchronous lessons/online classes [3/wk X 4/weeks = 12 classes]. The earned official completion certificate can be used to demonstrate mastery of a specific skill set and shared with current or future employers, current clients or medical niche financial advisory prospects.
Mini-Certification Tuition, Books and Related Fees
The tuition for each Mini-Certification live online course is $1,250 with the purchase of one required dictionary handbook. Other additional guides, white-papers, videos, files and e-content are all supplied without charge. Alternative courses may be developed in the future subject to demand and may change without notice.
***
Contact: For more information, or to speak with an academic representative, please contact Ann Miller RN MHA CMP™ at Email: MarcinkoAdvisors@msn.com [24/7].
Posted on October 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
A paradox is a logically self-contradictory statement or a statement that runs contrary to one’s expectation. It is a statement that, despite apparently valid reasoning from true or apparently true premises, leads to a seemingly self-contradictory or a logically unacceptable conclusion. A paradox usually involves contradictory-yet-interrelated elements that exist simultaneously and persist over time. They result in “persistent contradiction between interdependent elements” leading to a lasting “unity of opposites”.
THE TELE-MEDICINE PARADOX
Classic Definition: Refers specifically to the treatment of various medical conditions without seeing the patient in person. Healthcare providers may use electronic and internet platforms like live video, audio, PCs, tablets, or instant messaging to address a patient’s concerns and diagnose their condition remotely.
Modern Circumstance: This may include giving medical advice, walking them through at-home exercises, or recommending them to a local provider or facility. Even more exciting is the emergence of telemedicine apps which give patients access to care right from their phones or computer screens.
Paradox Examples: Treating certain conditions remotely can be challenging. Tele-medicine is often used to treat common illnesses, manage chronic conditions, or provide specialist services. If a patient is dealing with an emergent or serious condition, the remote provider suggests they seek in-person medical care.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The October 2025 Stock Market Crash: A Perfect Storm of Geopolitics and Investor Panic
The weekend of October 10–12, 2025, marked one of the most dramatic downturns in global financial markets in recent memory. What began as a series of unsettling headlines quickly snowballed into a full-blown market crash, sending shockwaves through economies and portfolios worldwide. This event was not the result of a single catalyst but rather a convergence of geopolitical tensions, speculative excess, and investor psychology.
At the heart of the crisis was a sudden escalation in U.S.–China trade relations. President Donald Trump abruptly canceled a scheduled diplomatic meeting with Chinese President Xi Jinping and announced a sweeping 100% tariff on all Chinese imports. This move reignited fears of a prolonged trade war, reminiscent of the economic standoff that rattled markets in the late 2010s. Investors, already jittery from months of uncertainty, interpreted the announcement as a signal of deteriorating global cooperation and retaliatory economic measures to come.
The impact was immediate and severe. Major U.S. indices plummeted: the S&P 500 dropped 2.7%, the Nasdaq fell 3.6%, and the Dow Jones Industrial Average lost 1.9%. These declines marked the worst single-day performance since April and triggered automatic trading halts in several sectors. The selloff was not confined to the United States; European and Asian markets mirrored the panic, with steep losses across the board.
Compounding the crisis was a massive liquidation in the cryptocurrency market. As traditional assets tumbled, investors rushed to offload digital holdings, leading to the largest crypto wipeout in history. Trillions of dollars in value evaporated within hours, further destabilizing investor confidence and draining liquidity from the broader financial system.
Another underlying factor was growing concern over the valuation of artificial intelligence (AI) stocks. The International Monetary Fund (IMF) had recently issued a warning that the AI sector was exhibiting signs of a speculative bubble, drawing parallels to the dot-com era. With many AI companies trading at astronomical price-to-earnings ratios, the crash exposed the fragility of investor sentiment and the dangers of overexuberance in emerging technologies.
Perhaps most telling was the psychological shift among investors. The weekend saw widespread capitulation, with many choosing to exit the market entirely rather than weather further volatility. This behavior—marked by fear-driven decision-making and herd mentality—is often a hallmark of deeper financial crises. It underscores the importance of trust and stability in maintaining market equilibrium.
In conclusion, the October 2025 stock market crash was a multifaceted event driven by geopolitical shocks, speculative risk, and emotional contagion. It serves as a stark reminder of how interconnected and fragile global markets have become. As policymakers and investors assess the damage, the focus must shift toward restoring confidence, recalibrating risk, and ensuring that future growth is built on sustainable foundations rather than speculative fervor.
COMMENTS APPRECIATED
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
“THE INVESTOR’S CHIEF problem—even his worst enemy—is likely to be himself.” So wrote Benjamin Graham, the father of modern investment analysis.
With these words, written in 1949, Graham acknowledged the reality that investors are human. Though he had written an 800 page book on techniques to analyze stocks and bonds, Graham understood that investing is as much about human psychology as it is about numerical analysis.
In the decades since Graham’s passing, an entire field has emerged at the intersection of psychology and finance. Known as behavioral finance, its pioneers include Daniel Kahneman, Amos Tversky and Richard Thaler. Together, they and their peers have identified countless human foibles that interfere with our ability to make good financial decisions. These include hindsight bias, recency bias and overconfidence, among others. On my bookshelf, I have at least as many volumes on behavioral finance as I do on pure financial analysis, so I certainly put stock in these ideas.
At the same time, I think we’re being too hard on ourselves when we lay all of these biases at our feet. We shouldn’t conclude that we’re deficient because we’re so susceptible to biases. Rather, the problem is that finance isn’t a scientific field like math or physics. At best, it’s like chaos theory. Yes, there is some underlying logic, but it’s usually so hard to observe and understand that it might as well be random. The world of personal finance is bedeviled by paradoxes, so no individual—no matter how rational—can always make optimal decisions.
As we plan for our financial future, I think it’s helpful to be cognizant of these paradoxes. While there’s nothing we can do to control or change them, there is great value in being aware of them, so we can approach them with the right tools and the right mindset.
Here are just seven of the paradoxes that can bedevil financial decision-making:
There’s the paradox that all of the greatest fortunes—Carnegie, Rockefeller, Buffett, Gates—have been made by owning just one stock. And yet the best advice for individual investors is to do the opposite: to own broadly diversified index funds.
There’s the paradox that the stock market may appear overvalued and yet it could become even more overvalued before it eventually declines. And when it does decline, it may be to a level that is even higher than where it is today.
There’s the paradox that we make plans based on our understanding of the rules—and yet Congress can change the rules on us at any time, as it did just last year.
There’s the paradox that we base our plans on historical averages—average stock market returns, average interest rates, average inflation rates and so on—and yet we only lead one life, so none of us will experience the average.
There’s the paradox that we continue to be attracted to the prestige of high-cost colleges, even though a rational analysis that looks at return on investment tells us that lower-cost state schools are usually the better bet.
There’s the paradox that early retirement seems so appealing—and has even turned into a movement—and yet the reality of early retirement suggests that we might be better off staying at our desks.
There’s the paradox that retirees’ worst fear is outliving their money and yet few choose the financial product that is purpose-built to solve that problem: the single-premium immediate annuity.
How should you respond to these paradoxes? As you plan for your financial future, embrace the concept of “loosely held views.”
In other words, make financial plans, but continuously update your views, question your assumptions and rethink your priorities.
Population health has been defined as “the health outcomes of a group of individuals, including the distribution of such outcomes within the group”. It is an approach to health that aims to improve the health of an entire human population or cohort. http://www.HealthDictionarySeries.org
History
In fact, the nominal “father of population health” is colleague and Dean David B. Nash MD MBA of Jefferson Medical School in Philadelphia. And, although I attended Temple University down the street, David still wrote the Foreword to my textbook years later; Financial Management Strategies for Hospitals and Healthcare Organizations [Tools, Techniques, Checklists and Case Studies].
Now age, income, location, race, gender and education are just a few characteristics that differentiate the world’s population. These are called ”disparities” and they have a major impact on people’s lives; especially their healthcare. And, I’ve written about them before. Perform a ME-P “search” for more.
So, it’s only natural that we’re keeping an eye on two major demographic trends: aging baby boomers and maturing Millennials [1982-2002 approximately].
Why it’s important
The impact of large population shifts propagate throughout an economy benefitting certain sectors more than others and influencing a country’s growth prospects; tantalizing investing ideas?
Example:
For example, as baby boomers retire, we’ll likely see higher spending on health care, but less on education and raising children. Likewise, tech-savvy Millennials will likely prioritize consumption on experiences over cars and houses [leading economic indicator].
So, can we profit from these trends?
Assessment
Well maybe – maybe not! Overall economic prospects may not be completely affected by these trends. Spending habits on combined goods and services will shift, rather than rise or decline.
So, be careful. What matters most for your investment success is your demographics and investing according to your personal circumstances and goals [paradox-of-thrift].
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
ME-P readers might believe the hedge fund industry is a small, exclusive club of elites, rich investors. But a new count by Preqin shows that it’s actually a large—and growing—sector of investing.
In fact, there may be more hedge funds globally (30,000+) than Burger King locations (18,700), and more more hedge fund managers than Taco Bell managers, per the FTE
Most all investors and physician executives are aware of the concept of financial beta.
BETA: A Systemic risk measurement benchmark correlating with a change in a specific index.
EXAMPLE: The measure of a stock’s volatility relative to the market, where a beta lower than 1 means the stock is less sensitive than the market as a whole; higher than 1 indicates the stock is more volatile than the market. The healthcare industry is considered to be increasingly volatile and hence possess a higher beta.
[An Internet WIKI CROWD-SOURCED Curation Project]*
To keep up with the ever-changing healthcare industrial complex, we must learn new definitions and re-learn old terminology in order to correctly apply it to practice. By aggregating the most up-to-date abbreviations, acronyms, definitions and terms, the Health DictionarySeries offers a wealth of information to help understand the ever-changing terms-of-art in healthcare today.
Each 10,000 item handbook is essential for doctors, nurses, benefits managers and insurance agents, CPAs, and administrators; as well as graduate and under graduate students and professors. Our goal to for each dictionary to be designated as a Doody’s Core Title.
Dictionary of Health Insurance and Managed Care
With more than 8,000 definitions, 4,000 abbreviations and acronyms, and a 3,000 item oeuvre of resources, readings, and nomenclature derivatives, this dictionary covers the Medicare, managed care and Medicaid, private insurance, Veteran’s Administration and PP-ACA language of the entire health and long-term care insurance sector.
Dictionary of Health Economics and Finance
Health economics and finance is an integral component of the health care industrial complex. Its language is a diverse and broad-based concept covering many other industries: accounting, mathematics, the actuarial sciences, stochastics and statistics, salary reimbursements, physician payments, compensation and forecasting are all commingled arenas.
Dictionary of Health Information Technology Security
There is a myth that all healthcare stakeholders understand the meaning of information technology jargon. In truth, the vernacular of contemporary systems is unique, and often misused or misunderstood. Moreover, emerging Heath Information Technology (HIT) thru the HITECG initiatives; in the guise of terms, definitions, acronyms, abbreviations and standards; often puts the non-expert in a position of maximum uncertainty and minimum productivity.
*NOTE: A wiki website allows users to add or update content using their browser thru a hosted server created by the collaborative effort of site visitors. The Hawaiian term “wiki wiki” means “super fast.”
A Financial Self Discovery Questionnairefor Medical Professionals
For understanding your relationship with money, it is important to be aware of yourself in the contexts of culture, family, value systems and experience. These questions will help you. This is a process of self-discovery. To fully benefit from this exploration, please address them in writing. You will simply not get the full value from it if you just breeze through and give mental answers. While it is recommended that you first answer these questions by yourself, many people relate that they have enjoyed the experience of sharing them with others who are important to them.
As you answer these questions, be conscious of your feelings, actually describing them in writing as part of your process.
Childhood
What is your first memory of money?
What is your happiest moment with Money? Your most unhappy?
Name the miscellaneous money messages you received as a child.
How were you confronted with the knowledge of differing economic circumstances among people, that there were people “richer” than you and people “poorer” than you?
Cultural heritage
What is your cultural heritage and how has it interfaced with money?
To the best of your knowledge, how has it been impacted by the money forces? Be specific.
To the best of your knowledge, does this circumstance have any motive related to Money?
Speculate about the manners in which your forebears’ money decisions continue to affect you today?
Family
How is/was the subject of money addressed by your church or the religious traditions of your forebears?
What happened to your parents or grandparents during the Depression?
How did your family communicate about money?
How? Be as specific as you can be, but remember that we are more concerned about impacts upon you than historical veracity.
When did your family migrate to America (or its current location)?
What else do you know about your family’s economic circumstances historically?
Your parents
How did your mother and father address money?
How did they differ in their money attitudes?
How did they address money in their relationship?
Did they argue or maintain strict silence?
How do you feel about that today?
Please do your best to answer the same questions regarding your life or business partner(s) and their parents.
Childhood: Revisited
How did you relate to money as a child? Did you feel “poor” or “rich”? Relatively? Or, absolutely? Why?
Were you anxious about money? Did you receive an allowance? If so, describe amounts and responsibilities.
Did you have household responsibilities?
Did you get paid regardless of performance?
Did you work for money?
If not, please describe your thoughts and feelings about that.
***
***
Same questions, as a teenager, young adult, older adult.
Credit
When did you first acquire something on credit?
When did you first acquire a credit card?
What did it represent to you when you first held it in your hands?
Describe your feelings about credit.
Do you have trouble living within your means?
Do you have debt?
Adulthood
Have your attitudes shifted during your adult life? Describe.
Why did you choose your personal path? a) Would you do it again? b) Describe your feelings about credit.
Adult attitudes
Are you money motivated? If so, please explain why? If not, why not? How do you feel about your present financial situation? Are you financially fearful or resentful? How do you feel about that?
Will you inherit money? How does that make you feel?
If you are well off today, how do you feel about the money situations of others? If you feel poor, same question.
How do you feel about begging? Welfare? If you are well off today, why are you working?
Do you worry about your financial future?
Are you generous or stingy? Do you treat? Do you tip?
Do you give more than you receive or the reverse? Would others agree?
Could you ask a close relative for a business loan? For rent/grocery money?
Could you subsidize a non-related friend? How would you feel if that friend bought something you deemed frivolous?
Do you judge others by how you perceive they deal with their Money? Do you feel guilty about your prosperity? Are your siblings prosperous?
What part does money play in your spiritual life?
Do you “live” your Money values?
Conclusion
There may be other questions that would be useful to you. Others may occur to you as you progress in your life’s journey. The point is to know your personal money issues and their ramifications for your life, work, and personal mission.
This will be a “work-in-process” with answers both complex and incomplete. Don’t worry.
Just incorporate fine-tuning into your life’s process.
Posted on September 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
What Is Pure Risk?
Pure risk is a category of risk that cannot be controlled and has two outcomes: complete loss or no loss at all. There are no opportunities for gain or profit when pure risk is involved. Pure risk is generally prevalent in situations such as natural disasters, fires, or death. These situations cannot be predicted and are beyond anyone’s control. Pure risk is also referred to as absolute risk.
***
1. Personal Risks
Now, there are basically 3 types of pure risks that concern individual physicians. These incur losses like loss of income, additional expenses and devaluation of property. There are 4 risk factors affecting them:
Premature death. This is death of a breadwinner who leaves behind financial responsibilities.
Old age / retirement. The risk of being retired without sufficient savings to support retirement years.
Health crisis. Individual with health problem may face a potential loss of income and increase in medical expenditures.
Unemployment. Jobless individual may have to live on their savings. If savings are depleted, a bigger crisis is awaiting.
2. Property Risks
This means the possibility of damage or loss to the property owned due to some cause. There are two types of losses involved.
Direct loss which means financial loss as a result of property damage.
Consequential loss which means financial loss due to the happenings of direct loss of the property.
For instance, a medical practice that burned down may incur repair costs as the direct loss. The consequential loss is being unable to run the practice business to generate income.
3. Liability Risks
A doctor is legally liable to his wrongful act that cause damage to a third party; physically, by reputation or property. S/he can be legally sued with no maximum in the compensation amount if found guilty.
Knowing how risks are classified, and the types of pure risks an individual is exposed to, will provide a fundamental overview on these risk topics and prepare you to further acquire the knowledge of how to deal with and manage them as a physician executive, leader, or manager.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Dr. Harry Markowitz is credited with developing the framework for constructing investment portfolios based on the risk-return tradeoff. William Sharpe, John Lintner, and Jan Mossin are credited with developing the Capital Asset Pricing Model (CAPM).
CAPM is an economic model based upon the idea that there is a single portfolio representing all investments (i.e., the market portfolio) at the point of the optimal portfolio on the Capital Market Line (CML) and a single source of systematic risk, beta, to that market portfolio. The resulting conclusion is that there should be a “fair” return investors should expect to receive given the level of risk (beta) they are willing to assume.
The excess return, or return above the risk-free rate, that may be expected from an asset is equal to the risk-free return plus the excess return of the market portfolio times the sensitivity of the asset’s excess return to the market portfolio excess return. Beta, then, is a measure of the sensitivity of an asset’s returns to the market as a whole. A particular security’s beta depends on the volatility of the individual security’s returns relative to the volatility of the market’s returns, as well as the correlation between the security’s returns and the markets returns.
While a stock may have significantly greater volatility than the market, if that stock’s returns are not highly correlated with the returns of the overall market (i.e., the stock’s returns are independent of the overall market’s returns), then the stock’s beta would be relatively low. A beta in excess of 1.0 implies that the security is more exposed to systematic risk than the overall market portfolio, and likewise, a beta of less 1.0 means that the security has less exposure to systematic risk than the overall market.
MPT has helped focus investors on two extremely critical elements of investing that are central to successful investment strategies.
First, MPT offers the first framework for investors to build a diversified portfolio. Furthermore, an important conclusion that can be drawn from MPT is that diversification does in fact help reduce portfolio risk.
Thus, MPT approaches are generally consistent with the first investment rule of thumb, “understand and diversify risk to the extent possible.”
Additionally, the risk/return tradeoff (i.e., higher returns are generally consistent with higher risk) central to MPT based strategies has helped investors recognize that if it looks too good to be true, it probably is.
Passive Investing
Passive investing is a monetary plan in which an investor invests in accordance with a pre-determined strategy that doesn’t necessitate any forecasting of the economy or an individual company’s prospects. The primary premise is to minimize investing fees and to avoid the unpleasant consequences of failing to correctly predict the future. The most accepted method to invest passively is to mimic the performance of a particular index. Investors typically do this today by purchasing one or more ‘index funds’. By tracking an index, an investor will achieve solid diversification with low expenses.
An ivestor could potentially earn a higher rate of return than an investor paying higher management fees. Passive management is most widespread in the stock markets. But with the explosion of exchange traded funds on the major exchanges, index investing has become more popular in other categories of investing. There are now literally hundreds of different index funds.
Passive management is based upon the Efficient Market Hypothesis theory. The Efficient Market Hypothesis (EMH) states that securities are fairly priced based on information regarding their underlying cash flows and that investors should not anticipate to consistently out-perform the market over the long-term.
The Efficient Market Hypothesis evolved in the 1960s from the Ph.D. dissertation of Eugene Fama. Fama persuasively made the case that in an active market that includes many well-informed and intelligent investors, securities will be appropriately priced and reflect all available information. If a market is efficient, no information or analysis can be expected to result in out-performance of an appropriate benchmark. There are three distinct forms of EMH that vary by the type of information that is reflected in a security’s price:
Weak Form
This form holds that investors will not be able to use historical data to earn superior returns on a consistent basis. In other words, the financial markets price securities in a manner that fully reflects all information contained in past prices.
Semi-Strong Form
This form asserts that security prices fully reflect all publicly available information. Therefore, investors cannot consistently earn above normal returns based solely on publicly available information, such as earnings, dividend, and sales data.
Strong Form
This form states that the financial markets price securities such that, all information (public and non-public) is fully reflected in the securities price; investors should not expect to earn superior returns on a consistent basis, no matter what insight or research they may bring to the table.
While a rich literature has been established regarding whether EMH actually applies in any of its three forms in real world markets, probably the most difficult evidence to overcome for backers of EMH is the existence of a vibrant money management and mutual fund industry charging value-added fees for their services.
The notion of passive management is counterintuitive to many investors. Passive investing proponents follow the strong market theory of EMH. These proponents argue several points including;
In the long term, the average investor will have a typical before-costs performance equal to the market average. Therefore the standard investor will gain more from reducing investment costs than from attempting to beat the market over time.
The efficient-market hypothesis argues that equilibrium market prices fully reflect all existing market information. Even in the case where some of the market information is not currently reflected in the price level, EMH indicates that an individual investor still cannot make use of that information. It is widely interpreted by many academics that to try and systematically “beat the market” through active management is a fools game.
Not everyone believes in the efficient market. Numerous researchers over the previous decades have found stock market anomalies that indicate a contradiction with the hypothesis. The search for anomalies is effectively the hunt for market patterns that can be utilized to outperform passive strategies. Such stock market anomalies that have been proven to go against the findings of the EMH theory include;
Low Price to Book Effect
January Effect
The Size Effect
Insider Transaction Effect
The Value Line Effect
All the above anomalies have been proven over time to outperform the market. For example, the first anomaly listed above is the Low Price to Book Effect. The first and most discussed study on the performance of low price to book value stocks was by Dr. Eugene Fama and Dr. Kenneth R. French. The study covered the time period from 1963-1990 and included nearly all the stocks on the NYSE, AMEX and NASDAQ. The stocks were divided into ten subgroups by book/market and were re-ranked annually. In the study, Fama and French found that the lowest book/market stocks outperformed the highest book/market stocks by a substantial margin (21.4 percent vs. 8 percent). Remarkably, as they examined each upward decile, performance for that decile was below that of the higher book value decile. Fama and French also ordered the deciles by beta (measure of systematic risk) and found that the stocks with the lowest book value also had the lowest risk.
Today, most researchers now deem that “value” represents a hazard feature that investors are compensated for over time. The theory being that value stocks trading at very low price book ratios are inherently risky, thus investors are simply compensated with higher returns in exchange for taking the risk of investing in these value stocks. The Fama and French research has been confirmed through several additional studies. In a Forbes Magazine 5/6/96 column titled “Ben Graham was right–again,” author David Dreman published his data from the largest 1500 stocks on Compustat for the 25 years ending 1994. He found that the lowest 20 percent of price/book stocks appreciably outperformed the market.
One item a medical professional should be aware of is the strong paradox of the efficient market theory. If each investor believes the stock market were efficient, then all investors would give up analyzing and forecasting. All investors would then accept passive management and invest in index funds. But if this were to happen, the market would no longer be efficient because no one would be scrutinizing the markets. In actuality, the efficient market hypothesis actually depends on active investors attempting to outperform the market through diligent research.
The case for passive investing and in favor of the EMH is that a preponderance of active managers do actually underperform the markets over time. The latest study by Standard and Poor’s (S&P) confirms this fact. S&P recently compared the performance of actively-managed mutual funds to passive market indexes twice per year. The 2012 S&P study indicated that indexes were once again outperforming actively-managed funds in nearly every asset class, style and fund category. The lone exception in the 2012 report was international equity, where active outperformed the index that S&P chose. The study examined one-year, three-year and five-year time periods. Within the U.S. equity space, active equity managers in all the categories failed to outperform the corresponding benchmarks in the past five year period. More than 65 percent of the large-cap active managers lagged behind the S&P 500 stock index. More than 81 percent of mid-cap mutual funds were outperformed by the S&P MidCap 400 index.
Lastly, 77 percent of the small-cap mutual funds were outperformed by the S&P SmallCap 600 index. U.S. bond active managers fared no better that equity managers over a five year period. More than 83 percent of general municipal mutual funds under-performed the S&P National AMT-Free Municipal Bond index, 93 percent of government long-term funds under-performed the Barclays Long Government index, nearly 95 percent of high yield corporate bond funds under-performed the Barclays High Yield index. Although the performance measurements for index investing are very strong, many analysts find three negative elements of passive investing;
Downside Protection: When the stock market collapses like in 2008, an index investor will assume the same loss as the market. In the case of 2008, the S&P 500 stock index fell by more than 50 percent, offering index investors no downside protection.
Portfolio Control: An index investor has no control over the holdings in the fund. In the event that a certain sector becomes over-owned (i.e. technology stocks in 2000), an index investor maintains the same weight as the index.
Average Returns: An index investor will never have the opportunity to outperform the market, but will always follow. Although the markets are very efficient, an investor can perhaps take advantage of market anomalies and invest with those managers who have maintained a long-term performance edge over the respective index.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 20, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
LEADERSHIP versus MANAGEMENT
***
***
By Dr. David Edward Marcinko MBA MEd
By Professor Gary A. Cook PhD
By Professor Eugene Schmuckler PhD MBA MEd CTS
Many of us have encountered a person who may intellectually be at upper levels, but whose ability to interact with others appears to that of one who is highly immature. This is the individual who is prone to becoming angry easily, verbally attacks co-workers, is perceived as lacking in compassion and empathy, and cannot understand why it is difficult to get others to cooperate with them and their agendas.
THINK: Sheldon Cooper PhD D.Sc MA BA of the The Big Bank Theory TV show.
The concept of Emotional Intelligence [EQ] was brought into the public domain when Daniel Goleman authored a book entitled, Emotional Intelligence.” According to Goleman, emotional intelligence consists of four basic non-cognitive competencies: self awareness, social awareness, self management and social skills. These are skills which influence the manner in which people handle themselves and their relationships with others. Goleman’s position was that these competencies play a bigger role than cognitive intelligence in determining success in life and in the workplace. He and others contend that emotional intelligence involves abilities that may be categorized into five domains:
Self awareness: Observing and recognizing a feeling as it happens.
Managing emotions: Handling feelings so that they are appropriate; realizing what is behind a feeling; finding ways to handle fears and anxieties, anger and sadness.
Motivating oneself; Channeling emotions in the service of a goal; emotional self control; delaying gratification and stifling impulses.
Empathy: Sensitivity to others’ feelings and concerns and taking their perspective appreciating the differences in how people feel about things.
Handling relationships: Managing emotions in others; social competence & social skills.
In 1995, Goleman then expanded on the works of Howard Gardner, Peter Salovey and John Mayer. He further defined Emotional Intelligence as a set of competencies demonstrating the ability one has to recognize his or her behaviors, moods and impulses and to manage them best, according to the situation. Mike Poskey, in “The Importance of Emotional Intelligence in the Workplace.” continued this definition by stating that emotional intelligence is considered to involve emotional empathy; attention to, and discrimination of one’s emotions; accurate recognition of one’s own and others’ moods; mood management or control over emotions; response with appropriate emotions and behaviors in various life situations (especially to stress and difficult situations); and balancing of honest expression of emotions against courtesy, consideration, and respect.
Source: Emotional Intelligence: what is and why it matters” – Cary Cherniss, PhD, presented at the annual conference of the Society of Industrial and Organizational Psychology, April 2000.
EQ differs from what has generally been considered intelligence which is described in terms of one’s IQ.
Traditional views of intelligence focused on cognition, memory and problem solving. Even today individuals are evaluated on the basis of cognitive skills. Entrance tests for medical, law, business, undergraduate and graduate schools base admissions in large part on the scores of the SAT, GMAT, LSAT, MCAT, etc. Without question, cognitive ability is critical but has been demonstrated, it is not a very good predictor of future direct job performance and indirect liability management. In fact, in 1940, David Wechsler the developer of a widely used intelligence test made reference to “non-intellective” elements. By this Wechsler meant affective, personal and social factors.
Source: Non-Intellective factors in intelligence. Psychological Bulletin, 37, 444-445.
Goleman became aware of the work of Salovey and Mayer having trained under David McClelland and was influenced by McClelland’s concern with how little traditional tests of cognitive intelligence predicted success in life. In fact, a study of 80 PhDs in science underwent a battery of personality tests, IQ tests and interviews in the 1950s while they were graduate students at Berkeley. Forty years later they were re-evaluated and it turned out that social and emotional abilities were four times more important than IQ in determining professional success and prestige.
Source: Feist & Barron: Emotional Intelligence and academic intelligence in career and life success. Paper presented at the Annual Convention of the American Psychological Society, San Francisco, 1996.
Undoubtedly, we want to have individuals work with us who have persistence which enables to them have the energy, drive, and thick skin to develop and close new business, or to work with the patients and other members of the staff. It is important to note that working alongside one with a “good” personality may be fun, energetic, and outgoing.
However, a “good personality does not necessarily equate to success. An individual with a high EQ can manage his or her own impulses, communicate effectively, manage change well, solve problems, and use humor to build rapport in tense situations. This clarity in thinking and composure in stressful and chaotic situations is what separates top performers from weak performers.
Poskey outlined a set of five emotional intelligence competencies that have proven to contribute more to workplace achievement than technical skills, cognitive ability, and standard personality traits combined.
***
***
A. Social Competencies: Competencies that Determine How We Handle Relationships
Intuition and Empathy – Our awareness of others’ feelings, needs, and concern. He suggested that this competency is important in the workplace for the following reasons:
Understanding others: an intuitive sense of others’ feelings and perspectives, and showing an active interest in their concerns and interests
Patient service orientation: the ability to anticipate, recognize and meet customer’s’ (patients) needs
People development: ability to sense what others need in order to grow, develop, and master their strengths
Leveraging diversity: cultivating opportunities through diverse people.
B. Political Acumen and Social Skills: Our adeptness at inducing desirable responses in others. This competency is important for the following reasons:
Influencing: using effective tactics and techniques for persuasion and desired results.
Communication: sending clear and convincing messages that are understood by others
Leadership: inspiring and guiding groups of people
Change catalyst: initiating and/or managing change in the workplace
Conflict resolution: negotiating and resolving disagreements with people
Collaboration and cooperation: working with coworkers and business partners toward shared goals
Team capabilities: creating group synergy in pursuing collective goals.
C. Personal Competencies: Competencies that determine how we manage ourselves
D. Self Awareness: Knowing out internal states, preferences, resources, and intuitions. This competency is important for the following reasons.
Emotional awareness: recognizing one’s emotions and their effects and impact on those around us
Accurate self-assessment: knowing one’s strengths and limits
Self-confidence: certainty about one’s self worth and capabilities
Self-Regulation: managing one’s internal states, impulses, and resources. This competency is important in the workplace for the following reasons.
Self-control: managing disruptive emotions and impulses
Trustworthiness: maintaining standards of honesty and integrity
Conscientiousness: taking responsibility and being accountable for personal performance
Adaptability: flexibility in handling change
Innovation: being comfortable with an openness to novel ideas, approaches, and new information.
E. Self-Expectations and Motivation: Emotional tendencies that guide or facilitate reaching goals. This competency is important in the workplace for the following reasons.
Achievement drive: striving to improve or meet a standard of excellence we impose on ourselves
Commitment: aligning with the goals of the group or the organization
Initiative: readiness to act on opportunities without having to be told
Optimism: Persistence in pursuing goals despite obstacles and setbacks
A note of caution is necessary. Goleman and Salovey both stated that emotional intelligence on its own is not a strong predictor of job performance. Instead they contend that it provides the bedrock for competencies that are predictors.
Obviously, EQ is an important attribute and it behooves each of us to promote emotional intelligence in the workplace. A number of guidelines have been developed for the Consortium for Research on Emotional Intelligence in Organizations by Goleman and Cherniss. The guidelines cover 21 phases which include preparation, training, transfer and evaluation.
Assess the organization’s needs: Determine the competencies that are most critical for effective job performance in a particular type of job. In doing so, us a valid method, such as the comparison of the behavioral interviews of superior performs and average performers. Also make sure the competencies to be developed are congruent with the organization’s culture and overall strategy.
Assess the individual: This assessment should be based on the key competencies needed for a particular job, and the data should come from multiple sources using multiple methods to maximize credibility and validity.
Deliver assessments with care: Give the individual information on his/her strengths and weaknesses. In doing so, try to be accurate and clear. Also, allow plenty of time for the person to digest and integrate the information. Provide feedback in a safe and supportive environment in order to minimize resistance and defensiveness. Avoid making excuses or downplaying the seriousness of deficiencies.
Maximize choice: People are motivated to change when they freely choose to do so. As much as possible, allow people to decide whether or not they will participate in the development process, and have them change goals themselves.
Encourage people to participate: People will be more likely to participate in development efforts if they perceive them to be worthwhile and effective. Organizational policies and procedures should encourage people to participate in development activity, and supervisors should provide encouragement and the necessary support. Motivation will be enhanced if people trust the credibility of those who encourage them to undertake the training.
Link learning goals to personal values: People are most motivated to pursue change that fits with their values and hopes. If a change matters little to people, they won’t pursue it. Help people understand whether a given change fits with what matters most to them.
Adjust expectations: Builds positive expectations by showing learners that social and emotional competence can be improved and that such improvement will lead to valued outcomes. Also, make sure that the learner has a realistic expectation of what the training process will involve.
Gauge readiness: Assess whether the individual is ready for training. If the person is not ready because of insufficient motivation or other reasons, make readiness the focus of intervention efforts.
Foster a positive relationship between the trainers and learners: Trainers who are warm, genuine, and empathic our best able to engage the learners in the change process. Select trainers who have these qualities, and make sure that they use them when working with the learners.
Make change self-directed: Learning is more effective when people direct their own learning program, tailoring it to their unique needs and circumstances. In addition to allowing people to set their own learning goals, let them continue to be in charge of their learning throughout the program, and tailor the training approach to the individual’s learning style.
Set clear goals: People need to be clear about what the competence is, how to acquire it, and how to show it on the job. Spell out the specific behaviors and skills that make up the target competence. Make sure that the goals are clear, specific, and optimally challenging.
Break goals into manageable steps: change. That is more likely to occur if the change process is divided into manageable steps. Encourage both trainers and trainees to avoid being overly ambitious.
Provide opportunities to practice: Lasting change requires sustained practice on the job and elsewhere in life. An automatic habit is being unlearned and different responses are replacing it. Use naturally occurring opportunities for practice at work, and in life. Encourage the trainees to try the new behaviors repeatedly and consistently over a period of months.
Give performance feedback: Ongoing feedback encourages people and direct change. Provide focused and sustained feedback as the learners practice new behaviors. Make sure that supervisors, peers, friends, family members-or some combination of these- give periodic feedback on progress.
Rely on experiential methods: Active, concrete, experiential methods tend to work best for learning social and emotional competencies. Development activities that engage all the senses and our dramatic and powerful can be especially effective.
Build in support: Change is facilitated through ongoing support of others who are going through similar changes. Programs should encourage the formation of groups where people give each other support, throughout the change effort. Coaches and mentors also can be valuable in helping support the desired change.
Use models: Use modern webinars, patient portals, live or videotaped models that clearly show how the competency can be used in realistic situations. Encourage learners to study, analyze, and emulate the models.
Enhance insight: Self-Awareness is the cornerstone of emotional and social competence. Help learners acquire greater understanding about how their thoughts, feelings, and behavior affect themselves and others.
Prevent relapse: Use relapse prevention, which helps people use lapses and mistakes as lessons to prepare themselves for further efforts.
Moreover:
Encourage use of skills on the job: Supervisors, peers and subordinates should reinforce and reward learners for using their new skills on the job. Coaches and mentors also can serve this function. Also, provide prompts and cues, such as through periodic follow-ups. Change also is more likely to indoor. When high status persons, such as supervisors and upper-level management model it.
Develop an organizational culture that supports learning: Change will be more enduring if the organization’s culture and tone support the change and offer a safe atmosphere for experimentation.
Finally, see if the development effort has lasting effects evaluated. When possible, find a true set of measures of the competence or skill, as shown on the job, before and after training, and also at least two months later. One-year follow-ups also are highly desirable. In addition to charting progress on the acquisition of competencies, also assess the impact on important job related outcomes, such as performance measures, and indicators of adjustments such as absenteeism, grievances, health status, etc.
Managers V. Leaders
These abilities are important for one to be successful as a manager and even more so as a leader, or physician executive. But, before we begin an examination of strategic leadership, it is necessary to make a deeper distinction between a manager and a leader. There are many different definitions as well as descriptions regarding leadership and management.
Many people talk as though leadership and management is the same thing. Fundamentally, they are quite different. Management focuses on work. We manage work activities such as money, time, paperwork, materials, equipment, and personnel, among other things. As can be found in any basic book on management, management focuses on planning, organizing, controlling, coordinating, budgeting, finance and money management as well as decision making. In effect, managers are generally those individuals who have been given their authority by virtue of their role. It is the function of a manager to ensure that the work gets done as well as to oversee the activities of others. In many healthcare organizations we find that those individuals elevated to a managerial position occur as a result of being a high performer on their previous assignment. A manager receives authority on the basis of role; while a leader’ authority is more innate in nature.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Whatever the statistics regarding physician standard of living, the reality is that within most marriages the husband more frequently takes responsibility for understanding and managing the finances. Additionally, women are more likely to remain in the marital home following a separation, thus inheriting a large fixed expense that may prove be an excessive, albeit short-term burden to them. At the time the decision is made to separate or divorce, many women do not have an understanding of how to manage their household budget, or how to manage their assets and liabilities.
An issue many divorcing physicians face is that the other spouse (in the past the wife), may have concentrated their energies on managing the home, while the physician concentrated on earning and managing the finances. The problems of the spouse of a physician are often compounded in divorce; not only do they not understand their personal finances, but that their absence from the work force has made them financially dependent on the other.
At what probably be the most emotionally taxing time in their lives, they are forced to play catch-up.
***
***
Taking a more active role in their own financial planning during the marriage may help the spouse of a physician avoid some of the financial pitfalls of separation and divorce.
NOTE: Barbara Stanny provides an excellent overview and reading bibliography on how people can get smart about money in her book Prince Charming Isn’t Coming. [1]
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
In order to create and monitor an investment portfolio for personal or institutional use, the physician executive, financial advisor, wealth manager, or healthcare institutional endowment fund manager, should ask three questions:
How much do we have invested?
How much did we make on our investments?
How much risk did we take to get that rate of return?
Introduction to the IPS
Most doctors, and hospital endowment fund executives, know how much money they have invested. If they don’t, they can add a few statements together to obtain a total. But, few can answers the questions above or actually know the rate of return achieved last year; or so far this year. Everyone can get this number by simply subtracting the ending balance from the beginning balance and dividing the difference. But, few take the time to do it. Why? A typical response to the question is, “We’re doing fine.”
Now, ask how much risk is in the portfolio and help is needed [risk adjusted rate of return]. In fact, Nobel laureate Harry Markowitz, Ph.D. said, “If you take more risk, you deserve more return.” Using standard deviation, he referred to the “variability of returns;” in other words, how much the portfolio goes up and down, its volatility [Markowitz, H: Portfolio Selection. Journal of Finance, March, 1952].
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
ORGANIZATIONAL BEHAVIOR ANDCLASSIFICATION OF RISKS
DEFINITION EMOTIONAL INTELLIGENCE: Emotional intelligence [EI] refers to the ability to identify and manage one’s own emotions, as well as the emotions of others. Emotional intelligence is generally said to include a few skills: namely emotional awareness, or the ability to identify and name one’s own emotions; the ability to harness those emotions and apply them to tasks like thinking and problem solving; and the ability to manage emotions, which includes both regulating one’s own emotions when necessary and helping others to do the same.
DEFINITIONAL ORGANIZATIONAL BEHAVIOR: Organizational behavior (OB) is the study of how individuals, groups, and organizations interact and influence one another. Though it is largely used within the field of business management as means to understand–and more effectively manage–groups of people. The reason businesses look to OB is because it can help organizations increase employee performance, while also creating a positive working environment.
CITE: Eugene Schmuckler; PhD MBA MEd CTS®
***
***
And so, as we review the concept of Emotional Intelligence and Organizational Behavior, it is possible to set up five EI/OB risk classes, based on the economic consequences of the occurrence of specific individual risks:
1. Prevented risks: Risks whose cost of occurrence is higher than their cost of management and whose occurrence may invoke additional legal sanctions. This class would include intentional torts and injuries caused by gross negligence.
2. Normally prevented risks: Risks whose cost of occurrence is greater than the cost of their management but whose occurrence will be considered only as negligent. This class includes most negligent injuries and most types of product liability actions.
3. Managed risks: Risks whose cost of occurrence is only slightly greater than their cost of management. The plaintiff usually has the burden of showing that the defendant owed the plaintiff a special duty to recover for one of these risks.
4. Un-Prevented risks: Risks whose cost of occurrence is less than their cost of management. The classic example of this class is the cost of railroad crossing barriers compared to the cost of people being hit by trains.
5. Un-Preventable risks: Risks whose occurrence is unmanageable. The assignment of a risk to one of these classes is a major problem in medical and healthcare quality control, because the class of a risk determines how much effort must be expended to prevent the risk. The misclassification of a prevented or normally prevented risk as a managed or un-prevented risk can result in large financial losses.
***
For example: A medical clinic that does not update obsolete equipment, such as inaccurate oxygen monitors, would be liable for any injuries attributable to the obsolete equipment. The classifications of risk must be reviewed periodically to determine if the cost of the risk-taking behavior has changed, thereby altering the classification.
***
***
For example: A small hospital in a rural area would not be expected to have the sophisticated equipment as a major hospital in a city. If an accident victim is brought into the rural facility, the hospital’s duty may be to transfer the patient to a better-equipped facility. The patient will face the risk of dying because of the delay in treatment, but the risk of insufficient treatments outweighs the risk of transfer. If the same victim were brought into a hospital in a major metropolitan center, the duty would be to treat the patient without a transfer. The risk of transfer has not changed, but the risk of insufficient treatment has disappeared.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
It’s hard to believe that just 30 years ago, physician investors had only two primary asset classes from which to choose: U.S. equities and U.S. bonds.
Today, the marketplace offers a daunting array of investment choices. Rapid market globalization, technology advancements and investor sophistication have spawned a host of new asset classes, from the mundane to the mysterious.
Even neophyte medical investors can now buy and sell international equities, emerging market debt, mortgage securities, commodities, derivatives, indexes and currencies, offering infinitely more opportunities to make, or lose, money.
Amidst this ongoing proliferation, a unique asset class has emerged, one that is complex, non-traditional and not easily understood like stocks or bonds. It does, however, offer one invaluable advantage; its returns are virtually uncorrelated with any other asset class. When this asset class is introduced into a traditional investment portfolio, a wonderful thing occurs; the risk-return profile of the overall portfolio improves dramatically.
This asset class is known as a Market-Neutral strategy. The reason few medical professionals have heard of market neutral strategies is that most of them are offered by private investment partnerships otherwise known as hedge funds.
To the uninitiated, “hedge fund” means risky, volatile or speculative. With a market-neutral strategy however, just the opposite is true. Funds utilizing market-neutral strategies typically emphasize the disciplined use of investment and risk control processes. As a result, they have consistently generated returns that display both low volatility and a low correlation with traditional equity or fixed income markets.
Definition of Market-Neutral
All market-neutral funds share a common objective: to achieve positive returns regardless of market direction. Of course, they are not without risk; these funds can and do lose money. But a key to their performance is that it is independent of the behavior of the markets at large, and this feature can add tremendous value to the rest of a portfolio.
A typical market-neutral strategy focuses on the spread relationship between related securities, which is what makes them virtually independent of underlying debt or equity markets. When two related securities are mispriced in relation to one another, the disparity will eventually disappear as the result of some external event. This event is called convergence and may take the form of a bond maturity, completion of a merger, option exercise, or simply a market recognizing the inefficiency and eliminating it through supply and demand.
Here’s how it might work
When two companies announce a merger, there is an intended future convergence, when the shares of both companies will converge and become one. At the time of the announcement, there is typically a trading spread between two shares. A shrewd trader, seeing the probability of the successful merger, will simultaneously buy the relatively cheaper share and sell short the relatively more expensive share, thus locking in the future gain.
Another example of convergence would be the relationship between a convertible bond and its underlying stock. At the time of convergence, such as bond maturity, the two securities will be at parity. However, the market forces of supply and demand make the bond underpriced relative to the underlying stock. This mispricing will disappear upon convergence, so simultaneously buying the convertible bond and selling short an equivalent amount of underlying stock, locks in the relative spread between the two.
Yet another example would be two bonds of the same company – one junior and one senior. For various reasons, the senior bond may become cheaper relative to the junior bond and thus display a temporary inefficiency that would disappear once arbitrageurs bought the cheaper bond and sold the more expensive bond.
While these examples involve different types of securities, scenarios and market factors, they are all examples of a market-neutral strategy. Locking a spread between two related securities and waiting for the convergence to take place is a great way to make money without ever taking a view on the direction of the market.
How large are these spreads, you may ask? Typically, they are tiny. The markets are not quite fully efficient, but they are efficient enough to not allow large price discrepancies to occur.
In order to make a meaningful profit, a market-neutral fund manager needs sophisticated technology to help identify opportunities, the agility to rapidly seize those opportunities, and have adequate financing resources to conduct hundreds of transactions annually.
The universe of market-neutral strategies is vast, spanning virtually every asset class, country and market sector. The spectrum varies in risk from highly volatile to ultra conservative. Some market-neutral strategies are more volatile than risky low-cap equity strategies, while others offer better stability than U.S Treasuries.
One unifying factor across this vast ocean of seemingly disparate strategies is that they all attempt to take advantage of a relative mispricing between various securities, and all offer a high degree of “market neutrality,” that is, a low correlation with underlying markets.
[A] Convertible Arbitrage
Convertible arbitrage is the oldest market-neutral strategy. Designed to capitalize on the relative mispricing between a convertible security (e.g. convertible bond or preferred stock) and the underlying equity, convertible arbitrage was employed as early as the 1950s.
Since then, convertible arbitrage has evolved into a sophisticated, model-intensive strategy, designed to capture the difference between the income earned by a convertible security (which is held long) and the dividend of the underlying stock (which is sold short). The resulting net positive income of the hedged position is independent of any market fluctuations. The trick is to assemble a portfolio wherein the long and short positions, responding to equity fluctuations, interest rate shifts, credit spreads and other market events offset each other.
A convertible arbitrage strategy involves taking long positions in convertible securities and hedging those positions by selling short the underlying common stock. A manager will, in an effort to capitalize on relative pricing inefficiencies, purchase long positions in convertible securities, generally convertible bonds, convertible preferred stock or warrants, and hedge a portion of the equity risk by selling short the underlying common stock. Timing may be linked to a specific event relative to the underlying company, or a belief that a relative mispricing exists between the corresponding securities.
Convertible securities and warrants are priced as a function of the price of the underlying stock, expected future volatility of returns, risk free interest rates, call provisions, supply and demand for specific issues and, in the case of convertible bonds, the issue-specific corporate/Treasury yield spread.
Thus, there is ample room for relative misvaluations.Because a large part of this strategy’s gain is generated by cash flow, it is a relatively low-risk strategy.
[B] Fixed-Income Arbitrage
Fixed-income arbitrage managers seek to exploit pricing inefficiencies across global markets.
Examples of these anomalies would be arbitrage between similar bonds of the same company, pricing inefficiencies of asset-backed securities and yield curve arbitrage (price differentials between government bonds of different maturities). Because the prices of fixed-income instruments are based on interest rates, expected cash flows, credit spreads, and related factors, fixed-income arbitrageurs use sophisticated quantitative models to identify pricing discrepancies.
Similarly to convertible arbitrageurs, fixed-income arbitrageurs rely on investors less sophisticated than themselves to misprice a complex security.
[C] Equity Market-Neutral Arbitrage
This strategy attempts to offset equity risk by holding long and short equity positions. Ideally, these positions are related to each other, as in holding a basket of S&P500 stocks and selling S&P500 futures against the basket. If the manager, presumably through stock-picking skill, is able to assemble a basket cheaper than the index, a market-neutral gain will be realized.
A related strategy is identifying a closed-end mutual fund trading at a significant discount to its net asset value. Purchasing shares of the fund gains access to a portfolio of securities valued significantly higher. In order to capture this mispricing, one needs only to sell short every holding in the fund’s portfolio and then force (by means of a proxy fight, perhaps) conversion of the fund from a closed-end to an open-end (creating convergence).
Sounds easy, right?
In considering equity market-neutral, you must be careful to differentiate between true market-neutral strategies (where long and short positions are related) and the recently popular long/short equity strategies.
In a long/short strategy, the manager is essentially a stock-picker, hopefully purchasing stocks expected to go up, and selling short stocks expected to depreciate. While the dollar value of long and short positions may be equivalent, there is often little relationship between the two, and the risk of both bets going the wrong way is always present.
[D] Merger Arbitrage (a.k.a. Risk Arbitrage)
Merger arbitrage, while a subset of a larger strategy called event-driven arbitrage, represents a sufficient portion of the market-neutral universe to warrant separate discussion.
Merger arbitrage earned a bad reputation in the 1980s when Ivan Boesky and others like him came to regard insider trading as a valid investment strategy. That notwithstanding, merger arbitrage is a respected stratagey, and when executed properly, can be highly profitable. It bets on the outcomes of mergers, takeovers and other corporate events involving two stocks which may become one.
A textbook example was the acquisition of SDL Inc (SDLI), by JDS Uniphase Corp (JDSU). On July 10, 2000 JDSU announced its intent to acquire SDLI by offering to exchange 3.8 shares of its own shares for one share of SDLI.
At that time, the JDSU shares traded at $101 and SDLI at $320.5. It was apparent that there was almost 20 percent profit to be realized if the deal went through (3.8 JDSU shares at $101 are worth $383 while SDLI was worth just $320.5). This apparent mispricing reflected the market’s expectation about the deal’s outcome. Since the deal was subject to the approval of the U.S. Justice Department and shareholders, there was some doubt about its successful completion. Risk arbitrageurs who did their homework and properly estimated the probability of success bought shares of SDLI and simultaneously sold short shares of JDSU on a 3.8 to 1 ratio, thus locking in the future profit.
Convergence took place about eight months later, in February 2001, when the deal was finally approved and the two stocks began trading at exact parity, eliminating the mispricing and allowing arbitrageurs to realize a profit.
Merger Arbitrage, also known as risk arbitrage, involves investing in securities of companies that are the subject of some form of extraordinary corporate transaction, including acquisition or merger proposals, exchange offers, cash tender offers and leveraged buy-outs. These transactions will generally involve the exchange of securities for cash, other securities or a combination of cash and other securities.
Typically, a manager purchases the stock of a company being acquired or merging with another company, and sells short the stock of the acquiring company. A manager engaged in merger arbitrage transactions will derive profit (or loss) by realizing the price differential between the price of the securities purchased and the value ultimately realized when the deal is consummated. The success of this strategy usually is dependent upon the proposed merger, tender offer or exchange offer being consummated.
When a tender or exchange offer or a proposal for a merger is publicly announced, the offer price or the value of the securities of the acquiring company to be received is typically greater than the current market price of the securities of the target company.
Normally, the stock of an acquisition target appreciates while the acquiring company’s stock decreases in value. If a manager determines that it is probable that the transaction will be consummated, it may purchase shares of the target company and in most instances, sell short the stock of the acquiring company. Managers may employ the use of equity options as a low-risk alternative to the outright purchase or sale of common stock. Many managers will hedge against market risk by purchasing S&P put options or put option spreads.
[E] Event-Driven Arbitrage
Funds often use event-driven arbitrage to augment their primary market-neutral strategy. Generally, any convergence which is produced by a future corporate event would fall into this category.
Accordingly,Event-Driven investment strategies or “corporate life cycle investing” involves investments in opportunities created by significant transactional events, such as spin-offs, mergers and acquisitions, liquidations, reorganizations, bankruptcies, recapitalizations and share buybacks and other extraordinary corporate transactions.
Event-Driven strategies involve attempting to predict the outcome of a particular transaction as well as the optimal time at which to commit capital to it. The uncertainty about the outcome of these events creates investment opportunities for managers who can correctly anticipate their outcomes.
As such, Event-Driven trading embraces merger arbitrage, distressed securities and special situations investing. Event-Driven managers do not generally rely on market direction for results; however, major market declines, which would cause transactions to be repriced or break, may have a negative impact on the strategy.
Event-driven strategies are research-intensive, requiring a manager to do extensive fundamental research to assess the probability of a certain corporate event, and in some cases, to take an active role in determining the event’s outcome.
Risk and Reward Characteristics
To help understand market-neutral performance and risk, let’s take a look at the distribution of returns of individual strategies and compare it to that of traditional asset classes.
Table 1: Average Return / Volatility of Market Neutral Strategies And Selected Traditional Asset Classes
Strategy
Average Return
Annualized Volatility
Convertible Arbitrage
11.95%
3.57%
Fixed Income Arbitrage
8.33%
4.90%
Equity Market-Neutral
11.62%
4.95%
Merger Arbitrage
13.29%
3.51%
Relative Value Arbitrage
15.69%
4.31%
Traditional Asset Classes:
S&P 500
12.62%
13.72%
MSCI World
8.57%
13.05%
High Grade U.S. Corp. Bonds
7.26%
3.73%
World Government Bonds
5.91%
5.96%
The most important observation about this chart is that the Market Neutral funds exhibits considerably lower risk than most traditional asset classes.
While market-neutral strategies vary greatly and involve all types of securities, the risk-adjusted returns are amazingly stable across all strategies. The annualized volatility – a standard measure of performance risk – varies between 3.5 and 5 percent, comparable to a conservative fixed-income strategy.
Another interesting statistics is the correlation between Market Neutral strategies and traditional asset classes and traditional asset classes
Table 2: Correlation between Market Neutral Strategies and Traditional Asset Classes
Asset Class/Strategy
S&P500
MSCI World
GovBonds
CorpBonds
The correlation of all market neutral strategies to traditional assets is quite low, or negative in some cases. This suggests that these strategies would indeed play a useful role in the ultimate goal of efficient portfolio diversification.
To test the “market neutrality” of these strategies, we asked, “How well, on average, did these strategies perform during bad, as well as good, market months?”
It turns out, in good times and bad, these strategies displayed consistent solid performance.From 12/31/91, in months when S&P 500 was down, the average down month was 3.03 percent. Market Neutral strategies performed as follows:
Strategy
Average Monthly Return
Convertible Arbitrage
+ 0.65%
Fixed Income Arbitrage
+ 0.50%
Equity Market-Neutral
+ 1.19%
Merger Arbitrage
+ 0.88%
Relative Value Arbitrage
+ 0.81%
In months when S&P 500 was up, the average up month was +3.24 percent. Market Neutral strategies performed as follows:
Strategy
Average Monthly Return
Convertible Arbitrage
+1.17%
Fixed Income Arbitrage
+1.20%
Equity Market-Neutral
+1.37%
Merger Arbitrage
+0.60%
Relative Value Arbitrage
+1.25%
Clearly, a compelling picture emerges. While these strategies, on average, underperform during good times, they show a positive average return during both good and bad markets.
Inclusion of Market-Neutral in a Long-term Investment Portfolio
A critical concern for any medical investor considering a foray into a new asset class is how it will alter the long-term risk/reward profile of the overall portfolio. To better understand this, we constructed several hypothetical portfolios consisting of traditional asset classes:
·US Blue chip equities (Dow Jones Industrial Average)
·US mid-cap equities (S&P 400 Midcap Index)
·US small-cap equities (S&P 600 Smallcap Index)
Portfolios varied in the level of risk from 100 percent U.S Treasuries (least risky) to 100 percent small-cap equities (most risky), and are ranked from 1 to 10, 1 representing the least risky portfolio.Each portfolio was analyzed on a Risk/Return basis using monthly return data since December 1991. The results are shown in Chart 1.Predictably, the least risky portfolio produced the smallest return, while the riskiest produced the highest return. This is perfectly understandable – you would expect to be compensated for taking a higher level of risk.
Chart 1: Risk/Return characteristics of traditional portfolios vs. Market Neutral strategies
Clearly, the risk-return picture offered by Market Neutral strategies is much more compelling (lower risk, higher return) than that offered by portfolios of traditional assets. What happens if we introduce these market-neutral strategies into traditional portfolios? Let’s take 20 percent of the traditional investments in our portfolio and reinvest them in market-neutral strategies.
The change is dramatic: the new portfolios (denoted 1a through 10a) offer significantly less risk for the same return. The riskiest portfolio, for instance (number 10) offered 20 percent less risk for a similar return of a new portfolio containing market-neutral strategies (number 10a).
Chart 2: Result of inclusion of 20% of Market Neutral strategies in traditional portfolios
This is quite a difference. Everything else being equal, anyone would choose the new, “improved” portfolios over the traditional ones.
How to invest
The mutual fund world does not offer a great choice of market neutral strategies.
Currently, there are only a handful of good mutual funds that label themselves market-neutral (AXA Rosenberg Market Netural fund and Calamos Market Neutral fund are two examples).
Mutual fund offerings are slim due to excessive regulations imposed by the SEC with respect to short selling and leverage, and consequently these funds lack flexibility in constructing truly hedged portfolios. The dearth of market-neutral offerings among mutual funds is offset by a vast array of choices in the hedge fund universe. Approximately 400 market-neutral funds, managing $60 billion, represent roughly 25% of all hedge funds.
Therefore, further focus will relate to the hedge fund universe, rather than the limited number of market-neutral mutual funds.
Direct investing in a market-neutral hedge fund is restricted to qualifying individuals who must meet high net worth and/or income requirements, and institutional investors, such as corporations, qualifying pension plans, endowments, foundations, banks, insurance companies, etc.
This does not mean that retail investors cannot get access to hedge fund exposure. Various private banking institutions offer funds of funds with exposure to hedge funds. Maaket-neutral funds are nontraditional investments. They are part of a larger subset of strategies known as alternative investments, and there is nothing traditional in the way doctors invest in them.
Hedge funds are private partnerships, which gives them maximum flexibility in constructing and managing portfolios, but also requires medical investors to do a little extra work.
[A] Lockup Periods
One of the main differences between mutual funds and hedge funds is liquidity. Market-neutral strategies have less liquidity than traditional portfolios. Quarterly redemption policies with 45- or 60-days notice are common. Many funds allow redemptions only once a year and some also have lock-up periods. In addition, few of these funds pay dividends or make distributions. These investments should be regarded strictly as long-term strategies.
[B] Managerial Risks
Success of a market-neutral strategy depends much less on the market direction than on the manager’s skill in identifying arbitrage opportunities and capitalizing on them.
Thus, there is significantly more risk with the manager than with the market. It’s vital for investors to understand a manager’s style and to monitor any deviations from it due to growth, personnel changes, bad decisions, or other factors.
[C] Fees
If you are accustomed to mutual fund fees, brace yourself; market-neutral investing does not come cheap.
Typical management fees range from 1 to 2 percent per year, plus a performance fee averaging 20 percent of net profits. Most managers have a “high watermark” provision; they cannot collect the performance fees until investors recoup any previous losses. Look for this provision in the funds’ prospectus and avoid any fund that lacks it. Even with higher fees, market-neutral investing is superior to most traditional mutual fund investing on a risk-adjusted return basis.
[D] Transparency
Mutual funds report their positions to the public regularly. This is not the case with market-neutral hedge funds. Full transparency could jeopardize accumulation of a specific position. It also generates front running: buying or selling securities before the fund is able to do so. While you should not expect to see individual portfolio positions, many hedge fund managers do provide a certain level of transparency by indicating their geographical or sector exposures, level of leverage and extent of hedging.
It does take a bit of education to understand these numbers, but the effort is definitely worthwhile.
[E] Taxation
The issue of hedge fund taxation is quite complex and is often dependent on the fund and the personal situation of the investor. Advice from a competent accountant, specialized financial advisor, tax attorney with relevant experience is worthwhile. The bottom line is that investing in market-neutral funds is not a tax-planning exercise and it will not minimize your taxes.
On the other hand, it should not generate any more or fewer taxes than if you invested in more traditional funds.
From the medical investor’s perspective, the principal advantages of market-neutral investing are attractive risk-adjusted returns and enhanced diversification.
Ten years of data indicate that market-neutral portfolios have produced risk-adjusted returns superior to traditional investments. In addition, the correlation between the returns of market-neutral funds and traditional asset classes has been historically negligible.
Adding exposure of market-neutral return strategies to the asset mix within a consistent, long-term investment program offers a medical investor the opportunity to improve overall returns, as well as achieving some protection against negative market movements.
Now, after all of the above, has your impression of hedge funds in general or MN funds in particular, changed?
APPENDIX:
Asset class weighting in traditional portfolios:
Portfolio
US Treasuries
US High Grade Corp Bonds
US Low Grade Corp Bonds
Large Cap Stocks
Mid Cap Stocks
Small Cap Stocks
1
50%
50%
2
50%
50%
3
10%
30%
50%
40%
4
50%
50%
5
10%
10%
50%
30%
6
10%
50%
20%
20%
7
10%
30%
20%
40%
8
20%
20%
60%
9
20%
80%
10
100%
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on July 4, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
Happy Fourth of July! It’s a good day to avoid the emergency department, so leave the fireworks shows to the pros—and perhaps use your extra hands to double-fist some BBQ instead.
Posted on July 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
The Complete Guide to July 4th Fireworks
Gather your novelty flag apparel and preheat your grills: Independence Day 2024 is upon us. And, what’s a July 4th celebration without some explosions in the sky?
Assessment
This info-graphic takes a closer look at the less glamorous side of fireworks — from the dollars that go up in smoke to the fingers we burn.
Experts estimate that it can cost more than $1 million to recruit and train a replacement for a doctor who leaves the profession because of burnout. But, as no broad calculation of burnout costs exists, Dr. Tait Shanafelt [Mayo Clinic researcher and Stanford Medicine’s first Chief Physician Wellness Officer] said Stanford, Harvard Business School, Mayo Clinic and the American Medical Association (AMA) are further cost estimating the issue. Nevertheless, Shanafelt and other researchers have shown that burnout erodes job performance, increases medical errors, and leads doctors to leave a profession they once loved.
Fortunately, we can help. From formal coaching to second career opinions, mentoring and advising, we can help with our remediation executive career programs. Regardless of what is happening in your life, it is wonderful to have a non-partial, confidential and informed career coach and sounding board on your side.
CITE: JAMA Internal Medicine [Effect of a Professional Coaching Intervention on the Well-Being and Distress of Physicians].
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on June 30, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By AI
CBOE Volatility Index
***
***
There’s a lot of confidence in markets these days, and nowhere is that more apparent than in the VIX, aka the CBOE Volatility Index, aka aka the Fear Index.
According to Brew Markets, the VIX literally measures the market’s expectation of volatility based on S&P 500 index options, but it’s become a shorthand way of quantifying investors’ fear or confidence. Any time the VIX rises above 30, it’s taken as a sign of some serious trepidation in the market—but anytime it falls below 20, the market is calm, cool, and collected.
The VIX skyrocketed to over 50 on Liberation Day as investors fretted over what tariffs meant for their portfolios, but it’s been gradually falling ever since. As the chart above shows, the VIX just fell below its key support level of 17—a mark it has failed to break below recently, and a move that underlines investors’ confidence that the good times will keep rolling.
Posted on June 29, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A.I.
***
***
Markets: That feeling when you have a $10 trillion rally. To wit:
The S&P 500 closed at a record high this week despite a brief dip as trade tensions with Canada ratcheted up. That puts the index about 20% up from its April low, when the broad tariff announcement sent it spiraling, and up ~5% for the year.
NVIDIA also hit an all-time high, and it keeps edging closer to becoming the first company to hit a $4 trillion valuation.
Posted on June 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A.I.
***
***
Deals: The US and China revealed the details of their trade deal framework, easing restrictions on rare earth metals and semiconductor chips. Commerce Secretary Howard Lutnick promised up to 10 more deals are on their way ahead of the July 9th tariff-pause deadline, but that probably won’t include Canada: President Trump ended all trade discussions with the country thanks to a dispute over the digital services tax.
Stocks: Indexes climbed at the open thanks to the deal with China, but they tumbled on news of a fallout with Canada. Still, the S&P 500 managed to post its 1,245th new all-time high, while the NASDAQ booked its own record close. The Dow trundled higher as well, though it’s still about 1,600 points below its previous record.
If you’re looking at this tab, chances are you are fed up with your financial brokerage accounts, thinking of finances, investing, retirement or all of the above.
And so, we can help
An investment portfolio second opinion, also called a “ portfolio review,” is an analysis of your financial holdings and associated strategies, allocations, fees and performance to determine whether the most effective instruments and methodologies are being utilized to reach your goals.
No Worries! You may have come to the right place.
E-Mail Ann Miller RN MHA CPHQ for an Initial Appointment: MarcinkoAdvisors@outlook.com
The purpose of this initial appointment is for you to ask a lot of questions to make sure you are comfortable with potentially working with us. It also helps if you are prepared to provide a verbal summary of your current situation.
Here are some questions to consider asking us during your first meeting:
1) Can you tell us about your financial qualifications, experience, education and training; if any?
2) Can you provide some information about your current financial advisory team?
3) On what type of investments do you typically purchase and own?
5) How much do pay your financial management firm?
6) How long have you been working with your current financial management firm?
8) What other services does your financial team provide?
Assets under management (AUM) is a significant parameter in the financial world. It answers financial questions like – how many investments does a company manage? What is the net value of the investments that the company manages? Finally, how many investors have trusted their assets with the company? The higher the answer to these three questions, the more glory to the company.
A wealthy investor who is not concerned by higher fees but wants maximum returns of their asset will probably choose an asset manager based on its AUM. Thus, the AUM indicates the financial performance of the firm. Also, based on the funds under management, the firm collects fees from other clients.
So, what are the investments which qualify as AUM? Any liquid asset of the investor they have entrusted the asset manager with monitoring and control. For example, bank deposits, cash balances, equity shares, bonds, mutual funds, and other investments.
What are the services an asset manager provides to their clients? The most important function is decision-making. With the constant fluctuations and rapid movements in the market, an asset manager has to make decisions about holding or selling an investment. The firm communicates with the investors and advises them about the necessary action.
Once the decision is taken, the firm acts on the decision, i.e., the investor does not have to enter the field. In addition, the asset management company will buy, sell, and make any other transactions on behalf of the investor. Finally, the firm also renders services like accounting, tax reporting, proxy voting (equity shares), client reporting, and other financial services.
What are Assets Under Advisement?
Assets under advisement refer to assets on which your firm provides advice or consultation but for which your firm does either does not have discretionary authority or does not arrange or effectuate the transaction. Such services would include financial planning or other consulting services where the assets are used for the informational purpose of gaining a full perspective of the client’s financial situation, but you are not actually placing the trade.
Assets under advisement could also be those which you monitor for a client on a non-discretionary basis, where you may make recommendations but where the client is the party responsible for arranging or effecting the purchase or sale. A common example of this scenario is when an adviser reviews a participant’s 401(k) allocations. If the adviser does not have the authority or ability to effect changes in the portfolio, these assets are likely considered assets under advisement rather than regulatory assets under management.
Assets under advisement are permitted to be disclosed on Form ADV Part 2A as a separate asset figure from the assets under management. There is no requirement to disclose the assets under advisement figure, but some advisers opt to include the figure to give prospective clients a more complete picture of the firm’s responsibilities. If you choose to report your assets under advisement, be sure to make a clear distinction between this figure and your regulatory assets under management.
Much has been written and much has been opined on the topic of health information technology, electronic health records and medical security liability for physicians and healthcare providers in this textbook. But occasionally, we all still get lost in a wide array of acronyms, jargon and terms that are constantly changing in this ecosystem. And so, this brief glossary serves as a ready reference for those who want to know about these definitions in a quick and ready fashion.
Access control: The process of controlling the access of a user
Access security: To allow computer or healthcare network entry using ID / password / secure socket layer (SSL) encryption / biometrics, etc; unique identification and password assignments are usually made to medical staff members for access to medical information on a need-to-know basis, and only upon written authority of the owner of the data.
Access level authorization: Establishes a procedure to determine the computer or network access level granted to individuals working on or near protected health information, medical data or secure health data.
Accredited standards committee: Organization that helps develop American National Standards (ANS) for computer and health information technology; accredited by ANSI for the development of American National Standards; ASC X12N develops medical electronic business exchange controls like 835-Health Care Claim Payment/Advice and 837-Health Care Claim.
Accountability: The security goal that generates the requirement for actions of an entity to be traced uniquely to that entity. This supports nonrepudiation, deterrence, fault isolation, intrusion detection and prevention, and after-action recovery and legal action.
Accounting: Creating an historical record of who was authenticated, at what time, and how long they accessed the computer system.
Administrative simplification: The use of electronic standard code sets for health information exchange; Title II, Subtitle F of HIPAA gives HHS the authority to mandate the use of standards for the electronic exchange of health care data; to specify what medical and administrative code sets should be used within those standards; to require the use of national identification systems for health care patients, providers, payers (or plans), and employers (or sponsors); and to specify the types of measures required to protect the security and privacy of personally identifiable health care and medical information.
Alternative backup sites: Off-site locations that are used for transferring computer operations in the event of an emergency.
American Health Information Management Association: A large trade association of health information and medical data management professionals.
American Medical Informatics Association: An organization that promotes the use of electronic medical management and healthcare informatics for clinical and administrative endeavors.
American Telemedicine Association: Established in 1993 as a leading resource and advocate promoting access to medical care for patients and health professionals via telecommunications technology; membership open to individuals, companies, and other organizations with an interest in promoting the deployment of telemedicine throughout the world.
Anti-virus software: A software package or subscription service used to thwart malicious computer or network attacks, such as: Symantec®, McAfee®, Trend Micro®, Panda Software®, Sunbelt Software®, Computer Associates®, AVG® or MS-FF ®, etc.
ASC X12N: HIPAA transmission standards, specifications and implementation guides from the Washington Publishing Company; or the National Council of Prescription Drug Programs.
Assurance: Grounds for confidence that the other four security goals (integrity, availability, confidentiality, and accountability) have been adequately met by a specific implementation. “Adequately met” includes (1) functionality that performs correctly, (2) sufficient protection against unintentional errors (by users or software), and (3) sufficient resistance to intentional penetration or bypass.
Asymmetric cryptology: The use of two different but mathematically related electronic keys for secure health data and medical information storage, transmission and manipulation.
Asymmetric encryption: Encryption and decryption performed using two different keys, one of which is referred to as the public key and one of which is referred to as the private key; also known as public-key encryption.
Asymmetric key: A half of a key pair used in an asymmetric “public-key” encryption system with two important properties: (1) the key used for encryption is different from the one used for decryption, (2) neither key can feasibly be derived from the other.
Attack tree: An inverted tree diagram that provides a visual image of the attacks that may occur against an asset.
Audio teleconferencing: A multi-simultaneous dual voice communications between two parties at remote locations; two way communications between physician and patient at various locations.
Authentication: The process of verifying and confirming the identity of a user.
Availability: The security goal that generates the requirement for protection against – Intentional or accidental attempts to (1) perform unauthorized deletion of data or (2) otherwise cause a denial of service or data.
Back door: A means to access to a computer program that bypasses security mechanisms, sometimes installed by a programmer so that the program can be accessed for troubleshooting or other purposes.
Back door trojans or bots: Currently, the biggest threat to healthcare and all PC users worldwide according to the MSFT Corporation.®
Bandwidth: The amount of information that can be carried over a communications link.
Bar coding systems: Final FDA ruling issued in February 2004 that required bar codes on most prescription and non-prescription medications used in hospitals and dispensed based on a physician’s order; the bar code must contain at least the National Drug Code (NDC) number, which specifically identifies the drug; although hospitals are not required at this time to have a bar code reading system on the wards, this ruling has heightened the priority of implementing hospital-wide systems for patient-drug matching using bar codes.
Baud: A unit of digital transmission that indicates the speed of information flow. The rate indicates the number of events able to be processed in one second and is expressed as bits per second (bps). The baud rate is the standard unit of measure for data transmission capability; typical older rates were 1200, 2400, 9600, and 14,400 baud; the signaling rate of a telephone line in the number of transitions made in a second; 1/300 sec = 300 baud.
Beta test: The secondary or final stress examination of newly developed computer hardware, software or peripheral devices; site, etc.
Bibliographic database: Indexed computer or printed source of citations of journal articles and other reports in the literature; typically include author, title, source, abstract, and/or related information; MEDLINE® and EMBASE®.
Bioinformatics: The application of medical and biological science to the health information management field.
Biological Information technology: Cross industry alliance of the Microsoft Corporation to enhance the ability to use and share digital health and biomedical data.
Biometric: Personal security identity characteristics, such as a signature, fingerprints, voice, iris or retinal scan, hand or foot vein geometry, facial characteristics, hair analysis, eye, blood vessel or DNA; uses the unique human characteristics of a person as a means of authenticating.
Biometric identification: Secure identification using biometrics that identifies a human from a measurement of a physical feature or repeatable action of the individual (for example, hand geometry, retinal scan, iris scan, fingerprint patterns, facial characteristics, DNA sequence characteristics, voice prints, and hand written signature).
Biopassword: Start-up healthcare IT security pioneer of keyboarding patterns to boost online security through neural network patterns.
Bluetooth® device: Machines, like cell phone with headset, transmitting across communications channels 1 to 14, over time.
Bluetooth® technology: Wireless mobile technology standard built into millions of mobile phones, headsets, portable computers, desktops and notebooks; named after Harold Bluetooth, a 10th century Viking king; healthcare telemetry and rural data transmissions; the Bluetooth Special Interest Group (BSIG) advocates measures aimed at pushing healthcare interoperability for wireless devices and other computers designed for use in the medical field; other wireless stands include: Wi-Fi, ZigBe®, IrDA and RFID.
Buffer: A temporary storage area.
Buffer overflow: A security breach that occurs when a computer program attempts to stuff more data into a temporary storage area than it can hold
Business continuity plan: A plan that outlines the procedures to follow after a business experiences an attack on its security.
California Database Security Breach Act: A state act that requires disclosure to California residents if a breach of personal information has or is believed to have occurred.
Certification authority: An independent third-party organization that assigns digital certificates.
Chain of custody: A process that documents everyone who has had contact with or direct possession of the evidence.
Chain of trust: Suggestion that each and every covered entity and business associate share responsibility and accountability for confidential PHI.
Chain of trust agreement: Contract entered into by two business partners in which it is agreed to exchange data and that the first party will transmit information to the second party, where the data transmitted is agreed to be protected between the partners; sender and receiver depend upon each other to maintain the integrity and confidentiality of the transmitted information; multiple two-party contracts may be involved in moving information from the originator to the ultimate recipient; for example, a provider may contract with a clearing house to transmit claims to the clearing house; the clearing house, in turn, may contract with another clearing house or with a payer for the further transmittal of those same claims.
Children’s Online Privacy Protection Act: A federal act that requires operators of online services or Web sites directed at children under the age of 13 to obtain parental consent prior to the collection, use, disclosure, or display of a child’s personal information.
Cipher lock: A combination lock that uses buttons that must be pushed in the proper sequence in order to open the door.
Clearing house: HIPAA medical invoice, healthcare data transaction exchange and medical data implementation service center that that meets or exceeds Federally-mandated standardized Electronic Data Interchange (EDI) transaction requirements.
Clinger-Cohen Act: Public Law 104-106; Information Technology Management Reform Act (ITMRA) of 1996.
Clinical data: Protected Health Information (PHI) from patient, physician, laboratory, clinic, hospital and/or payer, etc; identifiable patient medical information.
Clinical data information systems: Automatic and securely connected system of integrated computers, central severs and the Internet that transmits Protected Health Information (PHI) from patient, physician, laboratory, clinic, hospital and/or payer, etc.
Clinical data repository: Electronic storehouse of encrypted patient medical information; clinical data storage.
Clinical informatics: The management of medical and clinical data; the use of computers, networks and IT for patient care and health administration.
Clinical information: All the related medical information about a patient; Protected Health Information (PHI) from patients, providers, laboratories, clinics, hospitals and/or payers or other stakeholders, etc.
Clinical information system: A computer network systems that supports patient care; relating exclusively to the information regarding the care of a patient, rather than administrative data, this hospital-based information system is designed to collect and organize data.
Clinical regional health information system: Electronic entity committed to securely share private patient health information among entities like medical providers, clinics, laboratories, hospitals, outpatient centers, hospice and other healthcare facilities; Community Health Management Information Systems (CHMIS), Enterprise Information Networks (EINs), Regional Health Information Networks (RHINs) and Health Information Networks (HINs).
Cold site: An alternative backup site that provides the basic computing infrastructure, such as wiring and ventilation, but very little equipment.
Compact disc – read only memory (CD-ROM): A computer drive that can read CD-R and CD-RW discs.
Compact disc – recordable (CD-R): An optical disc that contains up to 650 megabytes of data and cannot be changed once recorded.
Compact disc – rewriteable (CD-RW): An optical disc that can be used to record data, erase it, and re-record again.
Computer security: A computer or network that is free from threats against it.
Computerized Physician Order Entry System: Automatic medical provider electronic medical chart ordering system that usually includes seven features: medication analysis, system order clarity, increased work efficiency, point of care utilization, benchmarking and performance tracking, on-line alerts and regulatory reporting.
Confidential health information: Protected Health Information (PHI) that is prohibited from free-use and secured from unauthorized dissemination or use; patient specific medical data.
Counter signature: The ability to prove the order of application of signatures; analogous to the normal business practice of signing a document which has already been signed by another party (ASTM E 1762 -95); part of a digital signature.
Covered entity: 42 CFR § 164.504(e)(2)(i)(B). Any of three broadly defined entities that deal with protected health information (PHI): providers, individuals or group health plans, and clearinghouses.
Cracker: A person who breaks into or otherwise violates the system security with a malicious intent.
Cryptography: The science of transforming information so that it is secure while it is being transmitted or stored.
Cyber-terrorism: Attacks by a terrorist group using computer technology and the Internet to cripple or disable a nation’s electronic infrastructure.
Data backup: The process of copying data to another media and storing it in a secure location.
Data encryption standard: An older health or medical data private key cryptology federal protocol for secure information exchange; replaced by AES.
Data interchange standard: X12 HIPAA health data transmission standard format.
Data interchange standard association: The organization that provides X12 HIPAA transmission standards and formats.
Deadbolt lock: A lock that extends a solid metal bar into the door frame for extra security.
Decision support system: Computer tools or applications to assist physicians in clinical decisions by providing evidence-based knowledge in the context of patient-specific data; examples include drug interaction alerts at the time medication is prescribed and reminders for specific guideline-based interventions during the care of patients with chronic disease; information should be presented in a patient-centric view of individual care and also in a population or aggregate view to support population management and quality improvement.
Decryption: Changing an encrypted message back to its original form.
Definition files: Files that contain updated antivirus information.
De-identified health information: Protected health information that is no longer individually identifiable health information; a covered entity may determine that health information is not individually identifiable health information only if: (1) a person with appropriate knowledge of and experience with generally accepted statistical and scientific principles and methods for rendering information not individually identifiable determines that the risk is very small that the information could be used, alone or in combination with other available information, to identify an individual, and documents the methods and results of the analysis; or (2) the following identifiers of the individual, relatives, employers or household members of the individual are removed.
Denial of service: The prevention of authorized access to resources or the delaying of time critical operations.
Designated record set: Contains medical and billing records and any other records that a physician and/or medical practice utilizes for making decisions about a patient; a hospital, emerging healthcare organization, or other healthcare organization is to define which set of information comprises “protected health information” and which set does not; contains medical or mixed billing records, and any other information that a physician and/or medical practice utilizes for making decisions about a patient. It is up to the hospital, EHO, or healthcare organization to define which set of information comprises “protected health information” and which does not though logically this should not differ from locale to locale. The patient has the right to know who in the lengthy data chain has seen their PHI. This sets up an audit challenge for the medical organization, especially if the accountability is programmed, and other examiners view the document without cause.
Designated standard: HIPAA standard as assigned by the department of HHS
Device lock: A steel cable and a lock used to secure a notebook computer.
Digital certificate: A certificate that binds a specific person to a public key.
Digital imaging and communications in medicine: Technology broadband transmission imaging standards for X-rays, MRIs, CT and PET scans, etc; health IT standard transmissions platform aimed at enabling different computing platforms to share image data without compatibility problems; a set of protocols describing how radiology images are identified and formatted that is vendor-independent and developed by the American College of Radiology and the National Electronic Manufacturers Association.
Digital radiology: Medical digital imaging applied to x-rays, CT, PET scans and related non-invasive and invasive technology; broadband intensive imaging telemedicine.
Digital rights management: The control and protection of digital intellectual property.
Digital signature: Encrypted electronic authorization with verification and security protection; private and public key infrastructure; based upon cryptographic methods of originator authentication, computed by using a set of rules and a set of parameters so that the identity of the signer and the integrity of medical or other data can be verified.
Digital signature standard: Encryption technology to ensure electronic medical data transmission integrity and authentication of both sender and receiver; date and time stamps; public and private key infrastructure.
Digital versatile disc – recordable (DVD-R): An optical disc technology that can record once up to 3.95 gigabytes of data on a single-sided disc and 7.9 GB on a double-sided disc.
Digital versatile disc – rewriteable (DVD-RAM): An optical disc technology that can record, erase, and re-record data and has a capacity of 2.6 GB (single side) or 5.2 GB (double side).
Digital versatile disc (DVD): A technology that permits large amounts of data to be stored on an optical disc.
Disaster recovery plan: A process to restore vital health and/or critical healthcare technology systems in the event of a medical practice, clinic, hospital or healthcare business interruption from human, technical or natural causes; focuses mainly on technology systems, encompassing critical hardware, operating and application software, and any tertiary elements required to support the operating environment; must support the process requirements to restore vital company data inside the defined business requirements; does not take into consideration the overall operating environment; an emergency mode operation plan is still necessary.
Disclosure: Release of PHI outside a covered entity or business agreement space, under HIPAA; the release, transfer, provision of access to or divulging of medical information outside the entity holding the information.
Disc – rewriteable (DVD-RW): An optical disc technology that allows data to be recorded, erased, and re-recorded.
Due care: Managers and their organizations have a duty to provide for information security to ensure that the type of control, the cost of control, and the deployment of control are appropriate for the system being managed.
e-health: Emerging field in the intersection of medical informatics, public health and business, referring to health services and information delivered or enhanced through the Internet and related technologies; characterizes not only a technical development, but also a state-of-mind, attitude, and a commitment for networked, global thinking, to improve health care worldwide by using information and communication technology.
Electronic data interchange: Inter healthcare organization computer-to-computer transmission of business or health information in a standard format; direct transmission from the originating application program to the receiving, or processing, application program; an EDI transmission consists only of business or health data, not any accompanying verbiage or free-form messages; a standard format is one that is approved by a national or international standards organization, as opposed to formats developed by health industry groups, medical practices, clinics or companies; the electronic transmission of secure medical and financial data in the healthcare industrial complex; X12 and similar variable-length formats for the electronic exchange of structured health data. The Centers for Medicare and Medicaid Services (CMS) regulates security and Electronic Data Interchange (EDI).
Electronic data interchange standards: The American National Standards Institute (ANSI) set of EDI standards known as the X12 standards. These standards have been developed by private sector standards development organizations (SDOs) and are maintained by the Accredited Standards Committee (ASC) X12. ANSI ASC X12N standards, Version 4010, were chosen for all of the transactions except retail pharmacy transactions, which continue to use the standard maintained by the National Council for Prescription Drug Programs (NCPDP) because it is already in widespread use. The NCPDP Telecommunications Standard Format Version 5.1 and equivalent NCPDP Batch Standard Version 1.0 have been adopted in this rule (health plans will be required to support one of these two NCPDP formats). The standards are designed to work across industry and company boundaries. Changes and updates to the standards are made by consensus, reflecting the needs of the entire base of standards users, rather than those of a single organization or business sector. Specifically, the following nine healthcare transactions were required to use X12N standard electronic claim formats by October 16, 2003.
Electronic health record: A real-time patient health record with access to evidence-based decision support tools that can be used to aid clinicians in decision-making; the EHR can automate and streamline a clinician’s workflow, ensuring that all clinical information is communicated; prevents delays in response that result in gaps in care; can also support the collection of data for uses other than clinical care, such as billing, quality management, outcome reporting, and public health disease surveillance and reporting; electronic medical record.
Electronic medication administrative record: Electrical file keeping computerized system for tracking clinical medication dispensation and use; integrated with TPAs, PBMs, robotic dispensing devices and CPOEs, etc.
Electronic medical (media) claims: Usually refers to a flat file format used to transmit or transport medical claims, such as the 192-byte UB-92 Institutional EMC format and the 320-byte Professional EMC-NSF.
Electronic prescribing: A type of computer technology whereby physicians use handheld or personal computer devices to review drug and formulary coverage and to transmit prescriptions to a printer or to a local pharmacy; e-prescribing software can be integrated into existing clinical information systems to allow physician access to patient-specific information to screen for drug interactions and allergies.
Electronic preventive services selector: A digital tool for primary care clinicians to use when recommending preventive services for their patients unveiled by the Department of Health and Human Services’ Agency for Healthcare Research and Quality (AHRQ), in November 2006; designed for use on a personal digital assistant (PDA) or desktop computer to allow clinicians to access the latest recommendations from the AHRQ-sponsored U.S. Preventive Services Task Force; designed to serve as an aid to clinical decision-making at the point of care and contains 110 recommendations for specific populations covering 59 separate preventive services topics; a real time search function allows a clinician to input a patient’s age, gender, and selected behavioral risk factors, such as whether or not they smoke, in the appropriate fields, while the software cross-references the patient characteristics entered with the applicable Task Force recommendations and generates a report specifically tailored for that patient.
Electronic signature: Various date and time stamped electronic security verification systems, such as passwords, encryption, ID numbers, biometrics identifiers, etc; electrical transmission and authentication of real signatories; signatory attribute that is affixed to an electronic health document to bind it to a particular entity; an electronic signature process secures the user authentication (proof of claimed health identity, such as by biometrics (fingerprints, retinal scans, hand written signature verification, etc.), tokens or passwords) at the time the signature is generated; creates the logical manifestation of signature (including the possibility for multiple parties to sign a medical document and have the order of application recognized and proven) and supplies additional information such as time stamp and signature purpose specific to that user; and ensures the integrity of the signed document to enable transportability, interoperability, independent verifiability, and continuity of signature capability; verifying a signature on a document verifies the integrity of the document and associated attributes and verifies the identity of the signer; there are several technologies available for user authentication, including passwords, cryptography, and biometrics (ASTM 1762-95).
Encryption: Changing the original text to a secret message.
Gigabytes (GB): Billions of bytes of data.
Gramm-Leach-Bliley Act: A federal act that requires private data be protected by banks and financial institutions.
Hacker: A person who possesses advanced computer skills and is adept at exploring computers and networks in order to break into them.
HEALTH 1.0: This is the dying healthcare system of yesterday and today. Information is communicated from doctors to patients. It is a basic B2C [business-to-consumer] website as the internet became one big encyclopedia by aggregating knowledge silos. Some doctors maintain websites, others do not. Nevertheless, Health 1.0 has a command and control hierarchy; doctors on top of the pyramid, patients on the bottom.
HEALTH 2.0:According to Matthew Holt [personal communication] Healthcare 2.0 may be defined as: “The foundation of healthcare 2.0 is information exchange plus technology. It employs user-generated content, social networks and decision support tools to address the problems of inaccessible, fragmentary or unusable health care information. Healthcare 2.0 connects users to new kinds of information, fundamentally changing the consumer experience (e.g., buying insurance or deciding on/managing treatment), clinical decision-making (e.g., risk identification or use of best practices) and business processes (e.g., supply-chain management or business analytics)”.
And so, if Health 1.0 was a static book, Health 2.0 is a dynamic discussion
Example: The power of the internet is illustrated in the phenomenon of “crowd-sourcing.” In this context, the term means to harvest the reach of social networking [wisdom of crowds] to solve a problem. A knowledge seeker asks a question and participants respond. For example, readers can participate on the www.MedicalExecutivePost.com or www.BusinessofMedicalPractice.com sites to improve the administration of any medical practice. And, www.PodiatryPrep.com is an example of how podiatrists connect for global board certification assistance.
***
***
HEALTH 2.0 Plus:The Dictionary of Health Insurance and Managed Care defines this emerging hybrid as a bridge uniting the philosophy of contemporary Health 2.0 with futuristic Health 3.0 technologies. Cisco System’s HealthPresence is one example developed in 2010, by Dr. T. Warner Hudson. Using the network as a platform, HealthPresence combines video, audio and information to create an environment similar to what patients experience when they visit their own doctor.
HEALTH 3.0: Soon, patients will not only be seeking information; but actionable intelligence – whether it is artificial or real. Patients will communicate almost as with another patient or doctor. The internet won’t just blindly do what we tell it to do – it will think and represent some amazing opportunities. For example, imagine your toilet running a SMAC 20 and then being instantly notified of the results by your smart phone? Or; use your iPhone to send pictures and streaming videos of conditions for a second opinion www.KnockingLive.com
Health information technology: The application of information processing involving both computer hardware and software that deals with the storage, retrieval, sharing, and use of health care information, medical data, and knowledge for communication and decision making.
Health information technology auditor: An expert who evaluate a health organization’s computer systems to ensure the proper safeguards are in place to protect and maintain the integrity of the firm’s data; While the position has existed since the mid-1960s, companies that previously employed just a handful of HIT auditors are now significantly adding to their ranks, sometimes doubling, tripling or quadrupling current staff levels; much current demand is due to the Sarbanes-Oxley Act and other legislation aimed at improving corporate governance in the wake of major accounting scandals earlier in the decade; publicly traded hospital systems require the expertise of HIT auditors to meet ongoing compliance requirements; the Gramm-Leach-Bliley Act and the Health Insurance Portability and Accountability Act (HIPAA), among other regulations, also are fueling the need for HIT auditors. Health IT auditors must have a general understanding of accounting principles and the strategic vision to ensure a health organization’s HIT systems allow it to achieve its short- and long-term objectives. Many hospitals promote from within for this role. Health facilities who look outside the organization for these professionals usually seek candidates with experience, knowledge of healthcare of emerging technologies and issues, and increasingly, certifications such as the certified information systems auditor (CISA) designation.
Health information technology promotion act: Legislation to accelerate the adoption of interoperable electronic health records by ensuring uniform standards, championed by Rep. Nancy Johnson, R-Conn, (H.R. 4157) which would: codify the Office of the National Coordinator for Health Information Technology in statute and delineate its ongoing responsibilities; create exceptions to the fraud and abuse statutes to allow certain providers to fund health information technology equipment and services for other providers; and provide for a study of federal and state health privacy policies.
Health Insurance Portability and Accountability Act (HIPAA): A federal act that requires enterprises in the health sector to guard protected health information and implement policies and procedures to safeguard it.
Health level seven: An international community of healthcare subject matter experts and information technology physicians and scientists collaborating to create standards for the exchange, management and integration of protected electronic healthcare information; the Ann Arbor, Mich.-based Health Level Seven (HL7) standards developing organization has evolved Version 3 of its standard, which includes the Reference Information Model (RIM) and Data Type Specification (both ANSI standards); HL7 Version 3 is the only standard that specifically deals with creation of semantically interoperable healthcare information, essential to building the national infrastructure; HL7 promotes the use of standards within and among healthcare organizations to increase the effectiveness and efficiency of healthcare delivery for the benefit of all patient, payers, and third parties; uses an Open System Interconnection (OSI) and high level seven healthcare electronic communication protocol that is unique in the medical information management technology space and modeled after the International Standards Organization (ISO) and American National Standards Institute (ANSI); each has a particular healthcare domain such as pharmacy, medical devices, imaging or insurance (claims processing) transactions. Health Level Seven’s domain is clinical and administrative data.
Hot site: An alternative backup site that contains the same equipment as found in the organization’s actual IT center.
Human firewall: An employee who practices good security techniques to prevent any security attacks from passing through them.
Incident response team: An employee team charged with gathering and handling the digital evidence of an attack.
Individually identifiable health information: Medical information that is created or received by a covered entity; relates to the physical or mental health condition of an individual, provision of health care or the payment for the provision of health care; identifies the individual or there is reasonable belief that the information can be used to identify the individual.
Information security: A computer or network that is free from threats against it.
Integrity: The security goal that generates the requirement for protection against either intentional or accidental attempts to violate data integrity (the property that data has when it has not been altered in an unauthorized manner) or system integrity (the quality that a system has when it performs its intended function in an unimpaired manner, free from unauthorized manipulation).
Intellectual property: Works created by others such as books, music, plays, paintings, and photographs.
IT-related risk: The net mission impact considering (1) the probability that a particular threat-source will exercise (accidentally trigger or intentionally exploit) system vulnerability and (2) the resulting impact if this should occur. IT-related risks arise from legal liability or mission loss due to:
* Unauthorized (malicious or accidental) disclosure, modification, or destruction of information
* Unintentional errors and omissions
* IT disruptions due to natural or man-made disasters
* Failure to exercise due care and diligence in the implementation and operation of the IT system.
Key-in-knob lock: A basic lock that has the lock mechanism embedded in the knob or handle.
Keystroke logger: A type of hardware spyware that captures keystrokes as they are typed.
Logic bombs: A computer program that lies dormant until it is triggered by a specific event.
Lossless: To compress electronic digital data.
Malicious code: Programs that are intentionally created to break into secure computers or to create havoc after the computers are accessed.
Master patient index: Healthcare facility composite that links and assists in tracking patient, person, or member activity within an organization (or health enterprise) and across patient care settings; hardcopy or electronic identification of all patients treated in a facility or enterprise and lists the medical record or identification number associated with the name; can be maintained manually or as part of a computerized system; typically, those for healthcare facilities are retained permanently, while those for insurers, registries, or others may have different retention periods; a database of all the patients ever registered (within reason) at a facility; name, demographics, insurance, next of kin, spouse, etc.
Medically unbelievablE event: Implemented on Jan. 1, 2007, the CMS blockage of payments for medical services that make no sense based on “anatomic considerations” or medical reasonableness when the same patient, date of service, HCPCS code or provider is involved; unlike other National Correct Coding Initiative (NCCI) edits, MUEs can’t be overridden by a modifier because there will never be a scenario where the physician had a good reason to submit a claim for removing a second appendix from the same person; etc.
Megabytes (MB): Millions of bytes of storage.
Memory stick: USB flash or non-volatile storage device; Sony CompactFlash®, pen or mini-drive; flash card, smart media, slang terms.
Mesh: Medical Subject Headings, the controlled vocabulary of about 16,000 terms used for MEDLINE and certain other MEDLARS databases.
Minimum necessary: The amount of protected health information shared among internal or external parties determined to me the smallest amount needed to accomplish its purpose for Use or Disclosure; the amount of health information or medical data needed to accomplish a purpose varies by job title, CE or job classification.
Minimum necessary rule: HIPAA regulation that suggests any PHI used to identify a patient, such as a social security number, home address or phone number; divulge only essential elements for use in transferring information from patient record to anyone else that requires the information; especially important with financial information; changes the way software is written and vendor access is provided. The “Minimum Necessary” Rule states the minimum use of PHI that can be used to identify a person, such as a social security number, home address or phone number. Only the essential elements are to be used in transferring information from the patient record to anyone else that needs this information. This is especially important when financial information is being addressed. Only the minimum codes necessary to determine the cost should be provided to the financial department. No other information should be accessed by that department. Many institutions have systems where a registration or accounting clerk can pull up as much information as a doctor or nurse, but this is now against HIPAA policy and subject to penalties. The “minimum necessary” rule is also changing the way software is set up and vendor access is provided.
Mirror site: A secondary location identical to the primary IT site that constantly receives a copy of data from the primary site.
National health information network: The technologies, standards, laws, policies, programs and practices that enable health information to be shared among health decision makers, including consumers and patients, to promote improvements in health and healthcare; vision for the NHII began more than a decade ago with publication of an Institute of Medicine report, The Computer-Based Patient Record. The path to a national network of healthcare information is through the successful establishment of Regional Health Information Organizations (RHIO).
National provider identifier: Originally was an eight-digit alphanumeric identifier. However, the healthcare industry widely criticized this format, claiming that major information systems incompatibilities would make it too expensive and difficult to implement. DHHS therefore revised its recommendation, instead specifying a 10-position numeric identifier with a check digit in the last position to help detect keying errors. The NPI carries no intelligence; in other words, its characters will not in themselves provide information about the provider. More recently, CMS announced that HIPAA-covered entities such as providers completing electronic transactions, healthcare clearinghouses, and large health plans, must use only the NPI to identify covered healthcare providers in standard transactions by May 23, 2007. Small health plans must use only the NPI by May 23, 2008. The proposal for a Standard Unique National Health Plan (Payer) Identifier was withdrawn on February, 2006. (According to CMS, “withdrawn” simply means that there is not a specific publication date at this time. Development of the rule has been delayed; however, when the exact date is determined, the rule will be put back on the agenda.)
Network: A group of interconnected computers.
Notebook safe: A special safe secured to a wall or the trunk of a car used for storing a notebook computer.
Operating system hardening: Steps that can be taken to make a personal computer operating system more secure.
Optical disc: A disc that uses laser technology to record data.
Password: A secret combination of words or numbers that authenticates or identifies the user.
Patch: A software update to correct a problem.
Patch management: Tools, utilities, and processes for keeping computers up to date with new software updates that are developed after a software product is released.
Pharmacy information system: Drug tracking and dispensation related health management information system for hospitals and healthcare organizations.
PhisHing: An attempt to fraudulent gather confidential information by masquerading as a trustworthy entity, person or business in an apparently official email, text message or website; carding or spoofing; video vishing; phish-tank; vish-tank; slang terms.
Physical security: The process of protecting the computer itself.
Port scanning: Sending a flood of information to all of the possible network connections on a computer.
Ports: The network connections on a computer.
Preset lock: A basic lock that has the lock mechanism embedded in the knob or handle.
Privacy: The quality or state of being hidden, encrypted, obscure, or undisclosed; especially medical data or PHI.
Privacy act: Federal legislature of 1974 which required giving patient some control over their PHI.
Privacy enhanced mail: Email message standard protocol for enhanced medical, health data or other security.
Privacy officer: A medical entity’s protected client information and security officer; required by each covered entity, to be responsible for “the development and implementation of the policies and procedures” necessary for compliance.
Privacy rule: The Federal privacy regulations promulgated under the Health Insurance Portability and Accountability Act (HIPAA) of 1996 that created national standards to protect medical records and other protected health information. The Office of Civil Rights (OCR) within the Department of Health and Human Services (DHHS) regulates the privacy rules.
Privacy standards: Any protocol to ensure the confidentiality of PHI.
Private key system: A means of cryptography where the same key is used to both encrypt and decrypt a message.
Public key system: A means of cryptography where two keys are used.
* Psychotherapy notes recorded (in any medium) by a health care provider who is a mental health professional documenting or analyzing the contents of conversation during a private counseling session or a group, joint, or family counseling session and that are separated from the rest of the individual’s medical record; excludes medication prescription and monitoring, counseling session start and stop times, the modalities and frequencies of treatment furnished, results of clinical tests, and any summary of the following items: diagnosis, functional status, the treatment plan, symptoms, prognosis, and progress to date.
* Public health authority means an agency or authority of the United States, a State, a territory, a political subdivision of a State or territory, or an Indian tribe, or a person or entity acting under a grant of authority from or contract with such public agency, including the employees or agents of such public agency or its contractors or persons or entities to whom it has granted authority, that is responsible for public health matters as part of its official mandate.
* Required by law means a mandate contained in law that compels a covered entity to make a use or disclosure of protected health information and that is enforceable in a court of law; includes but is not limited to, court orders and court-ordered warrants; subpoenas or summons issued by a court, grand jury, a governmental or tribal inspector general, or an administrative body authorized to require the production of information; a civil or an authorized investigative demand; Medicare conditions of participation with respect to health care providers participating in the program; and statutes or regulations that require the production of information, including statutes or regulations that require such information if payment is sought under a government program providing public benefits.
Regional health information organization: A multi-stakeholder organization that enables the exchange and use of health information, in a secure manner, for the purpose of promoting the improvement of health quality, safety and efficiency; the U.S. Department of Health and Human Services see RHIOs as the building blocks for the national health information network (NHIN) that will provide universal access to electronic health records; other experts maintain that RHIOs will help eliminate some administrative costs associated with paper-based patient records, provide quick access to automated test results and offer a consolidated view of a patient’s history.
Risk assessment: The process of identifying the risks to system security and determining the probability of occurrence, the resulting impact, and additional safeguards that would mitigate this impact.
Risk management: The total process of identifying, controlling, and mitigating information system–related risks. It includes risk assessment; cost-benefit analysis; and the selection, implementation, test, and security evaluation of safeguards. This overall system security review considers both effectiveness and efficiency, including impact on the mission and constraints due to policy, regulations, and laws.
Royalties: Payment to the owner or creator of intellectual property for their work.
Sarbanes-Oxley Act (Sarbox): A federal act that enforces reporting requirements and internal controls on electronic financial reporting systems.
Scanning: Locating a computer that can be broken into.
Script kiddies: Younger and less sophisticated users who break into a computer with malicious intent.
Secure virtual private network: Cryptographic tunneling protocols to provide the necessary health data confidentiality (preventing snooping), sender authentication (preventing identity spoofing), and message integrity (preventing message alteration) to achieve the medical privacy intended. When properly chosen, implemented, and used, such techniques can provide secure communications over unsecured networks.
Security: A set of healthcare information technology system characteristic and mechanisms which span the system both logically and physically; electronic access control against unauthorized intervention, both friendly or malicious; encompasses all of the safeguards in an information system, including hardware, software, personnel policies, information practice policies, disaster preparedness, and the oversight of all these areas; the purpose of health information security is to protect both the system and the information it contains from unauthorized access from without and from misuse from within; through various security measures, a health information system can shield confidential information from unauthorized access, disclosure and misuse, thus protecting privacy of the individuals who are the subjects of the stored data; security life cycle.
Security administration: The physical and electrical protection features of an IT health system needed to be managed in order to meet the needs of a specific installation and to account for changes in the healthcare entities operational environment.
Security compromise: Physical or electronic data, file, program or transmission error due to malicious miscreants or software interventions; health data confidentiality breach.
Security configuration: Measures, practices, and procedures for the safety of information systems that must be coordinated and integrated with each other and other methods, practices, and procedures of the organization established in order to credential safekeeping policy; provides written security plans, rules, procedures, and instructions concerning all components of a healthcare entity’s security; procedures must give instructions on how to report breaches and how those breaches are to be handled within the organization.
Security configuration management: The measurement of practices and procedures for the security of information systems that is coordinated and integrated with each other and other measures, practices and procedures of the organization so as to create a coherent system of health data security (NIST Pub 800-14).
Security domain: A set of subjects, their information objects, and a common security policy; foundation for IT security is the concept of security domains and enforcement of data and process flow restrictions within and between these domains.
Security goals: The five security goals are integrity, availability, confidentiality, accountability, and assurance.
Security information system: security is a system characteristic and a set of mechanisms that span the system both logically and physically.
Security policy: A formal written policy that outlines the importance of security to the organization and establishes how the security program is organized.
Share: An object that is shared with others over a computer network.
Signature files: Files that contain updated antivirus information.
Smart card: A device that contains a chip that stores the user’s private key, login information, and public key digital certificate.
Sniffing: Listening to the traffic on a computer network and then analyzing it.
Social engineering: Relying on trickery and deceit to break security and gain access to computers.
Spam: Unsolicited e-mail messages.
Spy: A person who has been hired to break into a computer and steal data.
Spyware: Hardware or software that “spies” on what the user is doing and captures that activity without their knowledge.
Stealth signal transmitter: Software installed on a notebook computer that sends a signal that can be traced.
Threat analysis: The examination of threat-sources against system vulnerabilities to determine the threats for a particular system in a particular operational environment.
Threat modeling: A process of constructing scenarios of the types of threats that assets face.
Threat: The potential for a threat-source to exercise (accidentally trigger or intentionally exploit) a specific vulnerability.
Threat-source: Either (1) intent and method targeted at the intentional exploitation of a vulnerability or (2) a situation and method that may accidentally trigger a vulnerability.
Token: A security device used to authenticate the user by having the appropriate permission (like a password) embedded into the device.
USA Patriot Act: A federal act designed to broaden the surveillance of law enforcement agencies to enhance the detection and suppression of terrorism.
Username: A unique identifier of a person used to access a computer system.
Virus: A program that secretly attaches itself to other programs and when executed causes harm to a computer.
Vulnerability: A flaw or weakness in system security procedures, design, implementation, or internal controls that could be exercised (accidentally triggered or intentionally exploited) and result in a security breach or a violation of the system’s security policy.
Vulnerability assessment: A process to determine what vulnerabilities exist in the current system against these attacks.
Vulnerability assessment managed services: Agencies that use scanning devices connected to probe an organization’s security to look for vulnerabilities.
War driving: A technique used to locate wireless local area networks (WLANs).
WiMax: A more powerful version of Wi-Fi that can provide wireless Internet access over wider geographic location such as a city; an acronym that stands for Worldwide Interoperability for Microwave Access, and is a certification mark for products that pass conformity and interoperability tests for the IEEE 802.16 standards. IEEE 802.16 is working group number 16 of IEEE 802, specializing in point-to-multipoint broadband wireless access.
Wireless hot spot: Specific geographic location in which an access point provides public wireless broadband network services; security is risky for PHI; hotspot.
Wireless local area networks: A computer network that uses radio waves instead of wires to connect computers.
Worm: A program that does not attach itself to other programs or need user intervention to execute.
Posted on June 18, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
***
***
By Dr. David Edward Marcinko MBA MED CMP™
SPONSOR: wwwCertifiedMedicalPlanner.org
***
Crisis Management is the precautions and identification of threats to an organization and its stakeholders, and the methods used by the organization to deal with these threats.
For example, recall in 1982, that Tylenol™ commanded 35 percent of the over-the-counter analgesic market in America and it represented nearly 17 percent of Johnson & Johnson’s profits. But, when seven people died from consuming the tainted drug, a national panic ensued. Moreover, Americans started to question the safety of all over-the-counter medications.
Fortunately, J&J commenced the proto-typical good crisis response in the following way:
J&J acted quickly, with complete candidness about what happened and within hours of learning of the deaths, J&J installed toll-free numbers for consumers, sent alerts to healthcare providers nationwide, and stopped advertising the product. J&J recalled 31 million bottles of Tylenol™ capsules and offered replacement products free of charge. J&J did not wait for evidence to see whether the contamination might be more widespread.
J&J’s leadership was in the lead and seemed in full control throughout the crisis. The chairman was admired for his leadership to pull Tylenol™ capsules off the market and his forthrightness in dealing with the media. The Tylenol™ crisis led the news every night on every station for six weeks.
J&J placed consumers first. J&J spent more than $100 million for the recall and re-launch of Tylenol™. The stock had been trading near a 52-week high just before the tragedy, dropped for a time, but recovered to its highs only two months later.
J&J accepted responsibility. The disaster could have been described in many different ways: as an assault on the company, as a problem somewhere in the process of getting Tylenol™ from J&J factories to retail stores, or as the acts of a crazed criminal.
J&J sought to ensure that measures were taken to prevent a recurrence of the problem. J&J introduced tamper-proof packaging that would make it much more difficult for a similar incident to occur in the future.
J&J presented itself prepared to handle the short-term damage in the name of consumer safety. Within a year of the disaster, J&J’s share of the analgesic market, which had fallen to 7 percent from 37 percent following the poisoning, had climbed back to 30 percent.
This wildly successful response in now the stuff of graduate and business school case models for excellence in teaching!
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
here are many ways for a doctor, osteopath, podiatrist or dentist to financially invest. Traditionally, this meant picking individual stocks and bonds. Today, there are many other ways to purchase securities en mass. For example:
MUTUAL FUND: A regulated investment company that manages a portfolio of securities for its shareholders.
Open End Mutual Funds: An investment company that invests money in accordance with specific objectives on behalf of investors. Fund assets expand or contract based on investment performance, new investments and redemptions. Trade at Net Asset Value or the price the fund shares scheduled with the US Securities and Exchange Commission (SEC) trade. NAV can change on a daily basis. Therefore, per-share NAV can, as well.
Closed End Mutual Funds: Older than open end mutual funds and more complex. A CEMF is an investment company that registers shares SEC regulations and is traded in securities markets at prices determined by investments. Shares of closed-end funds can be purchased and sold anytime during stock market hours. CEMF managers don’t need to maintain a cash reserve to redeem or / repurchase shares from investors. This can reduce performance drag that may otherwise be attributable to holding cash. CEMFs may be able to offer higher returns due to the heavier use of leverage [debt]. They are subject to volatility, less liquid than open-end funds, available only through brokers and may sells at a heavily discount or premium to [NAV] determined by subtracting its liabilities from its assets. The fund’s per-share NAV is then obtained by dividing NAV by the number of shares outstanding. .
Sector Mutual Funds: Sector funds are a type of mutual fund or Exchange-Traded Fund (ETF) that invests in a specific sector or industry such as technology, healthcare, energy, finance, consumer goods, or real estate. Sector funds focus on a particular industry, allowing investors to gain targeted exposure to specific market areas. The goal is to outperform the overall market by investing in companies within a specific sector that is expected to perform well. However, they are also more susceptible to market fluctuations and specific sector risks, making them a more specialized and potentially higher-risk investment option.
EXCHANGE TRADED FUNDS: ETFs are a type of fund that owns various kinds of securities, often of one type. For example, a stock ETF holds stocks, while a bond ETF holds bonds. One share of the ETF gives buyers ownership of all the stocks or bonds in the fund. If an ETF held 100 stocks, then those who owned the fund would own a stake – albeit a very tiny one – in each of those 100 stocks.
ETFs are typically passively managed, meaning that the fund usually holds a fixed number of securities based on a specific preset index of investments. These are tax efficient. In contrast, many mutual funds are actively managed, with professional investors trying to select the investments that will rise and fall.
The Standard & Poor’s 500 Index is perhaps the world’s best-known index, and it forms the basis of many ETFs. Other popular indexes include the Dow Jones Industrial Average and the National Association of Securities Dealers Automated Quotations [NASDAQ] Composite Index.
ETFs based on these funds are called Index Funds and just buy and hold whatever is in the index and make no active trading decisions. ETFs trade on a stock exchange during the day, unlike mutual funds that trade only after the market closes. With an ETF you can place a trade whenever the market is open and know exactly the price you’re paying for the fund.
INDEX FUNDS: Index funds mirror the performance of benchmarks like the DJIA. These passive investments are an unimaginative way to invest. Passive index funds tracking market benchmarks accounted for just 21% of the U.S. equity fund market in 2012. By 2024, passive index funds had grown to about half of all U.S. fund assets. This rise of passive funds has come as they often outperform their actively managed peers. According to the widely followed S&P Indices Versus Active (SPIVA) scorecards, about 9 out of 10 actively managed funds didn’t match the returns of the S&P 500 benchmark in the past 15 years.
ASSESSMENT
Investing in individual stocks is psychologically and academically different than investing in the above funds, according to psychiatrist and colleague Ken Shubin-Stein MD, MPH, MS, CFA who is a professor of finance at the Columbia University Graduate School of Business When you buy shares of a company, you are putting all your eggs in one basket. If the company does well, your investment will go up in value. If the company does poorly, your investment will go down. Fund diversification helps reduce this risk.
CONCLUSION
Investing in the above fund types will help mitigate single company security risk.
References:
1. Fenton, Charles, F: Non-Disclosure Agreements and Physician Restrictive Covenants. In, Marcinko, DE and Hetico, HR: Risk Management, Liability Insurance, and Asset Protection Strategies for Doctors and Advisors [Best Practices from Leading Consultants and Certified Medical Planners™]. Productivity Press, New York, 2015.
Readings:
1. Marcinko, DE and Hetico, HR; Comprehensive Financial Planning Strategies for Doctors and Advisors [Best Practices from Leading Consultants and Certified Medical Planners™] Productivity Press, New York, 2017
2. Marcinko, DE: Dictionary of Health Economics and Finance. Springer Publishing Company, NY 2006
4. Shubin-Stein, Kenneth: Unifying the Psychological and Financial Planning Divide [Holistic Life Planning, Behavioral Economics, Trading Addiction and the Art of Money]. Marcinko, DE and Hetico, HR; Comprehensive Financial Planning Strategies for Doctors and Advisors [Best Practices from Leading Consultants and Certified Medical Planners™] Productivity Press, New York, 2017
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com