BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on November 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
⚠️ Cons of Compounding Pharmacies
1. Quality and Safety Concerns
Medications are not FDA-approved, meaning they don’t go through the same rigorous testing as commercial drugs.
Risk of contamination or incorrect formulation if strict standards aren’t followed.
Potency can vary between batches, leading to inconsistent therapeutic effects.
2. Limited Regulation
Oversight is less stringent compared to mass-produced pharmaceuticals.
Standards may differ depending on the state or the specific pharmacy.
Patients may not always know whether their compounding pharmacy meets high-quality benchmarks.
3. Insurance and Cost Issues
Compounded medications are often not covered by insurance.
They can be more expensive due to customization and small-scale production.
4. Availability and Accessibility
Not all pharmacies offer compounding services.
Patients may need to travel farther or wait longer to receive their medication.
***
***
5. Evidence and Efficacy
Limited clinical trials or scientific evidence supporting compounded formulations.
Effectiveness may rely heavily on anecdotal reports rather than standardized studies.
6. Risk of Errors
Human error in measuring, mixing, or labeling can lead to incorrect dosages.
Lack of standardized packaging may increase confusion for patients.
👉 In short: while compounding pharmacies can provide personalized solutions, the downsides include less regulation, higher costs, safety risks, and limited evidence of efficacy compared to FDA-approved medications.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 21, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
BASIC DEFINITIONS
***
***
Money supply measures—M0, M1, M2, and M3—are essential tools used by economists and policymakers to assess liquidity, guide monetary policy, and understand economic health. Each measure reflects a different level of liquidity and plays a unique role in financial analysis.
The money supply refers to the total amount of monetary assets available in an economy at a specific time. It includes various forms of money, ranging from physical currency to more liquid financial instruments. To better understand and manage economic activity, central banks and economists categorize money into different measures based on liquidity: M0, M1, M2, and M3.
M0, also known as the monetary base or base money, includes all physical currency in circulation—coins and paper money—plus reserves held by commercial banks at the central bank. It represents the most liquid form of money and is directly controlled by the central bank through tools like open market operations and reserve requirements.
M1 builds on M0 by adding demand deposits (checking accounts) and other liquid deposits that can be quickly converted into cash. It includes:
Physical currency held by the public
Traveler’s checks
Demand deposits at commercial banks
M1 is a key indicator of immediate spending power in the economy. A rapid increase in M1 can signal rising consumer activity, while a decline may indicate tightening liquidity.
M2 expands further by including near-money assets—those that are not as liquid as M1 but can be converted into cash relatively easily. M2 includes:
All components of M1
Savings deposits
Money market securities
Certificates of deposit (under $100,000)
M2 is widely used by economists and the Federal Reserve to gauge intermediate-term economic trends. It reflects both spending and saving behavior, making it a critical tool for forecasting inflation and guiding interest rate decisions.
M3, though no longer published by the Federal Reserve since 2006, includes M2 plus large time deposits, institutional money market funds, and other larger liquid assets. M3 provides a broader view of the money supply, especially useful for analyzing long-term investment trends and credit expansion. Some countries, like the UK and India, still track M3 for macroeconomic planning.
These measures are not just academic—they have real-world implications. For instance, during the COVID-19 pandemic, the U.S. saw a historic surge in M2 due to stimulus payments and quantitative easing. This expansion raised concerns about future inflation, which materialized in subsequent years. Monitoring money supply helps central banks adjust monetary policy to maintain price stability and support economic growth.
In conclusion, money supply measures offer a layered view of liquidity in the economy, from the most liquid (M0) to broader aggregates (M3).
Understanding these categories helps policymakers, investors, and businesses anticipate economic shifts, manage inflation, and make informed financial decisions.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 18, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
The singularity promises to revolutionize medicine by accelerating diagnostics, treatment, and longevity—but it also demands ethical vigilance and systemic transformation.
The concept of the technological singularity refers to a hypothetical future moment when artificial intelligence (AI) surpasses human intelligence, triggering exponential advances in technology. In medicine, this could mark a turning point where AI-driven systems outperform human clinicians in diagnosis, treatment planning, and even biomedical research. While the singularity remains speculative, its implications for healthcare are profound and multifaceted.
One of the most promising impacts is in diagnostics and precision medicine. AI systems trained on vast datasets of medical images, genetic profiles, and patient histories could detect diseases earlier and more accurately than human doctors. For example, algorithms already outperform radiologists in identifying certain cancers from imaging scans. As we approach the singularity, these systems may evolve into autonomous diagnostic agents capable of real-time analysis and personalized recommendations, tailored to each patient’s unique biology.
Another transformative area is drug discovery and development. Traditional pharmaceutical research is slow and costly, often taking over a decade to bring a new drug to market. AI could dramatically shorten this timeline by simulating molecular interactions, predicting therapeutic targets, and optimizing clinical trial designs. With superintelligent systems, the pace of innovation could accelerate to the point where treatments for currently incurable diseases—like Alzheimer’s or certain cancers—become feasible within months.
The singularity also opens doors to radical longevity and human enhancement. Advances in nanotechnology, genomics, and regenerative medicine may converge to extend human lifespan significantly. AI could help decode the aging process, identify biomarkers of cellular decline, and engineer interventions that slow or reverse it. Some theorists even envision a future where aging is treated as a curable condition, and mortality becomes a choice rather than a biological inevitability.
However, these breakthroughs come with serious ethical and societal challenges. Data privacy, algorithmic bias, and access inequality are critical concerns. If singularity-level AI is controlled by a few corporations or governments, it could exacerbate global health disparities. Moreover, the replacement of human clinicians with machines raises questions about empathy, trust, and accountability in care. Who is responsible when an AI makes a life-altering mistake?
To navigate this future responsibly, medicine must embrace interdisciplinary collaboration. Ethicists, technologists, clinicians, and policymakers must work together to ensure that AI systems are transparent, equitable, and aligned with human values. Regulatory frameworks must evolve to keep pace with innovation, and medical education must prepare practitioners to work alongside intelligent machines.
In conclusion, the singularity represents both a promise and a peril for medicine. It offers unprecedented opportunities to enhance human health, but also demands careful stewardship to avoid unintended consequences.
As we edge closer to this horizon, the challenge will be not just technological, but deeply human: to harness intelligence beyond our own in service of healing, compassion, and justice.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on November 16, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Dr. David Edward Marcinko MBA MEd
***
***
Crisis Management in Medical Practice
Healthcare is a field where crises are not hypothetical but expected realities. From pandemics and natural disasters to cyberattacks and sudden staff shortages, medical practices must be prepared to respond swiftly and effectively. Crisis management in medical practice refers to the structured approach of anticipating, preparing for, responding to, and recovering from disruptive events that threaten patient safety, organizational stability, or community trust.
🌐 Nature of Crises in Healthcare
Crises in medical practice can take many forms:
Public Health Emergencies: Outbreaks of infectious diseases, such as COVID-19, demand rapid adaptation of protocols and resources.
Operational Disruptions: Power outages, supply chain breakdowns, or IT failures can halt essential services.
Human Resource Challenges: Sudden staff shortages due to illness or burnout can compromise patient care.
Reputation and Legal Risks: Medical errors or breaches of patient confidentiality can escalate into crises requiring immediate management.
Each type of crisis requires tailored strategies, but all share the common need for preparedness and resilience.
🔑 Principles of Crisis Management
Effective crisis management in medical practice rests on several key principles:
Leadership and Decision-Making: Strong leadership is critical for making rapid, evidence-based decisions under pressure.
Communication: Transparent, timely communication with staff, patients, and external stakeholders reduces panic and builds trust.
Collaboration: Coordinating with hospitals, public health agencies, and community organizations strengthens response capacity.
Flexibility: Crises are unpredictable; adaptability in protocols and resource allocation is essential.
⚙️ Crisis Management Frameworks
Healthcare organizations often adopt structured frameworks:
Incident Command System (ICS): Provides a standardized hierarchy for managing emergencies.
Risk Assessment Models: Identify vulnerabilities and prioritize mitigation strategies.
Business Continuity Planning: Ensures essential services continue despite disruptions.
These frameworks help medical practices move from reactive responses to proactive resilience.
***
***
💡 Challenges in Crisis Management
Despite planning, medical practices face significant challenges:
Resource Limitations: Smaller practices may lack the financial or logistical capacity to implement robust crisis plans.
Staff Stress and Burnout: Crises often demand long hours and emotional resilience, which can strain healthcare workers.
Rapidly Changing Information: In public health emergencies, evolving guidelines can create confusion.
Patient Expectations: Maintaining quality care during disruptions is difficult but essential to preserve trust.
Addressing these challenges requires investment in training, mental health support, and technology infrastructure.
🌱 Importance of Resilience
Crisis management is not only about survival but about building resilience. Practices that learn from crises, adapt policies, and strengthen systems emerge stronger. For example, the COVID-19 pandemic accelerated telemedicine adoption, which continues to benefit patients today. Resilience ensures that medical practices can withstand future disruptions while continuing to deliver safe, effective care.
✅ Conclusion
Crisis management in medical practice is a vital competency that safeguards both patients and providers. By preparing for diverse scenarios, fostering strong leadership, and prioritizing communication, healthcare organizations can navigate crises with confidence. Ultimately, effective crisis management transforms challenges into opportunities for growth, innovation, and improved patient care.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on November 16, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
American Depository Receipts Defined
In the modern era of globalization, financial instruments that connect investors across borders have become indispensable. Among these, American Depository Receipts (ADRs) stand out as a powerful mechanism that allows U.S. investors to participate in foreign equity markets without the complexities of international trading. ADRs not only simplify access to global companies but also enhance the ability of foreign corporations to raise capital in the United States. This essay explores the origins, structure, regulatory frameworks, benefits, risks, and real-world examples of ADRs, highlighting their role in the integration of global finance.
Historical Development
The concept of ADRs emerged in 1927 when J.P. Morgan introduced the first ADR for the British retailer Selfridges. At the time, American investors faced significant hurdles in purchasing foreign shares, including currency conversion, unfamiliar trading practices, and regulatory differences. ADRs solved these problems by creating a U.S.-based certificate that represented ownership in foreign shares, denominated in dollars, and traded on American exchanges.
Over the decades, ADRs expanded rapidly, especially during the post-World War II era when globalization accelerated. By the late 20th century, ADRs had become a mainstream tool for accessing international equities, with companies from Europe, Asia, and Latin America increasingly using them to tap into U.S. capital markets.
Structure and Mechanics
An ADR is issued by a U.S. depositary bank, which holds the underlying shares of a foreign company in custody. Each ADR corresponds to a specific number of shares—sometimes one, sometimes multiple, or even a fraction. Investors buy and sell ADRs in U.S. dollars, and dividends are paid in dollars as well, eliminating the need for currency conversion.
Key structural features include:
Depositary Banks: Institutions such as J.P. Morgan, Citibank, and Bank of New York Mellon act as custodians and issuers of ADRs.
ADR Ratios: The number of foreign shares represented by one ADR can vary, allowing flexibility in pricing.
Trading Platforms: ADRs can be listed on major exchanges like the NYSE or NASDAQ, or traded over-the-counter.
Regulatory Framework
ADRs are subject to U.S. securities regulations, which vary depending on the level of ADR issued:
Level I ADRs: Traded over-the-counter, requiring minimal disclosure. They are primarily used for visibility rather than fundraising.
Level II ADRs: Listed on U.S. exchanges, requiring compliance with SEC reporting standards, including reconciliation of financial statements to U.S. GAAP or IFRS.
Level III ADRs: Allow foreign companies to raise capital directly in U.S. markets through public offerings. These require the highest level of regulatory compliance, including registration with the SEC and adherence to corporate governance standards.
This tiered system ensures that investors receive appropriate levels of transparency while giving foreign companies flexibility in their approach to U.S. markets.
Benefits for Investors
ADRs offer numerous advantages to American investors:
Convenience: Investors can buy shares in foreign companies without dealing with foreign exchanges or currencies.
Diversification: ADRs provide access to global firms across industries, enhancing portfolio diversification.
Transparency: ADRs listed on U.S. exchanges must comply with SEC regulations, ensuring reliable financial reporting.
Liquidity: ADRs trade on familiar platforms, making them easily accessible to retail and institutional investors alike.
Benefits for Companies
Foreign corporations also benefit significantly from ADRs:
Access to Capital: ADRs open the door to the world’s largest pool of investors.
Global Visibility: Listing in the U.S. enhances reputation and credibility.
Improved Liquidity: Shares become more widely traded, increasing market efficiency.
Investor Base Diversification: Companies can attract both domestic and international investors, reducing reliance on local markets.
Risks and Challenges
Despite their advantages, ADRs carry certain risks:
Currency Risk: ADR values are tied to foreign shares denominated in local currencies, making them vulnerable to exchange rate fluctuations.
Political and Economic Risk: Instability in the issuing company’s home country can affect performance.
Taxation: Dividends may be subject to foreign withholding taxes before conversion to U.S. dollars.
Regulatory Differences: Even with SEC oversight, differences in accounting standards and corporate governance can pose challenges.
Case Studies
1. Alibaba Group (China) Alibaba’s ADRs, listed on the NYSE in 2014, marked one of the largest IPOs in history, raising $25 billion. This demonstrated the power of ADRs to connect Chinese companies with American investors, despite regulatory complexities between the two countries.
2. Toyota Motor Corporation (Japan) Toyota’s ADRs have long provided U.S. investors with access to one of the world’s largest automakers. By listing ADRs, Toyota expanded its investor base and strengthened its global presence.
3. Royal Dutch Shell (Netherlands/UK) Shell’s ADRs illustrate how multinational corporations use ADRs to maintain visibility in U.S. markets while managing complex cross-border structures.
The Role of ADRs in Global Finance
ADRs embody the globalization of capital markets. They facilitate cross-border investment, enhance market efficiency, and foster economic integration. For investors, ADRs represent a gateway to international diversification. For companies, they provide access to the deepest capital markets in the world.
Conclusion
American Depositary Receipts are more than just financial instruments; they are symbols of global interconnectedness. By bridging the gap between U.S. investors and foreign companies, ADRs have reshaped the landscape of international finance. They balance convenience with exposure to global risks, offering both opportunities and challenges. As globalization continues to evolve, ADRs will remain a vital tool for investors and corporations alike, reinforcing their role as a cornerstone of modern capital markets.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 15, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
For centuries, doctors have occupied one of the highest earning and most respected positions in society. Their extensive education, specialized knowledge, and critical role in preserving human life have traditionally guaranteed them financial security and social prestige. Yet in recent years, a growing conversation has emerged: could skilled tradesmen—electricians, plumbers, welders, carpenters, and other hands‑on professionals—eventually out‑earn doctors in the future? While the answer is complex, shifting economic dynamics suggest that the gap between these professions may narrow, and in certain contexts, tradesmen could indeed surpass doctors in earnings.
One of the most significant factors driving this possibility is supply and demand. The medical profession requires years of schooling, residency, and licensing, which creates a steady pipeline of doctors but also limits entry. By contrast, skilled trades have suffered from declining interest among younger generations, many of whom were encouraged to pursue college degrees instead of vocational training. As a result, there is now a shortage of tradesmen in many regions. When demand for services like plumbing or electrical work rises but supply remains low, wages naturally increase. Already, some master tradesmen charge hourly rates that rival or exceed those of general practitioners.
Another consideration is student debt and overhead costs. Doctors often graduate with hundreds of thousands of dollars in debt, and many must work in hospital systems or private practices with high administrative expenses. Tradesmen, on the other hand, typically face lower educational costs and can enter the workforce much earlier. Many start their own businesses with relatively modest investments, allowing them to keep a larger share of their earnings. In an era where entrepreneurship and independence are highly valued, tradesmen may find themselves financially freer than doctors burdened by debt and bureaucracy.
***
***
The changing economy also plays a role. Automation and artificial intelligence are beginning to reshape medicine, with diagnostic tools, telehealth, and robotic surgery reducing the need for certain human tasks. While doctors will always be essential, parts of their work may become less lucrative as technology takes over. Skilled trades, however, are far harder to automate. Repairing a leaking pipe, rewiring a house, or welding a custom structure requires physical presence, adaptability, and problem‑solving in unpredictable environments—skills machines struggle to replicate. This resilience against automation could make tradesmen’s work increasingly valuable.
That said, doctors will likely continue to command high salaries in specialized fields such as surgery, cardiology, or oncology. The prestige and necessity of medical expertise ensure that society will always reward them. Yet the notion that tradesmen are “lesser” careers is fading. In fact, many tradesmen already earn six‑figure incomes, particularly those who own successful businesses or operate in regions with acute labor shortages.
Ultimately, whether tradesmen will out‑earn doctors depends on how society values different forms of expertise. If current trends continue—rising demand for trades, shortages of skilled labor, resistance to automation, and lower educational barriers—it is plausible that many tradesmen will match or surpass doctors in income. The future may not be defined by one profession dominating the other, but by a more balanced recognition that both healers and builders are indispensable to modern life. In that sense, the financial gap may close, reflecting a broader cultural shift toward valuing practical skills as highly as academic ones.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Silver occupies a distinctive position within the realm of investment assets, functioning simultaneously as a precious metal and an industrial commodity. This dual nature imbues silver with characteristics that make it a valuable component of a diversified portfolio, offering both defensive qualities and growth potential. While its volatility necessitates careful consideration, silver’s unique attributes warrant attention from investors seeking balance between risk mitigation and opportunity.
Silver as a Hybrid Asset
Unlike gold, which is primarily regarded as a store of value, silver derives a substantial portion of its demand from industrial applications. It is indispensable in sectors such as electronics, renewable energy, and medical technology, with photovoltaic cells in solar panels representing a particularly significant driver of consumption. This industrial utility ensures that silver’s price is influenced not only by macroeconomic uncertainty but also by technological innovation and global manufacturing trends. Consequently, silver provides investors with exposure to both traditional safe-haven dynamics and cyclical industrial growth.
Accessibility and Cost Efficiency
Silver’s affordability relative to gold enhances its appeal to a broad spectrum of investors. Physical silver, in the form of coins and bars, allows individuals with modest capital to participate in the precious metals market. Moreover, financial instruments such as exchange-traded funds (ETFs) and mining equities provide liquid and scalable avenues for investment. This accessibility ensures that silver can serve as an entry point into alternative assets, particularly for those seeking to hedge against inflation without committing substantial resources.
Inflation Hedge and Currency Protection
Historically, silver has demonstrated resilience during periods of inflation and currency depreciation. As fiat currencies lose purchasing power, tangible assets such as silver tend to appreciate, preserving wealth for investors. Although gold is often considered the primary hedge, silver’s similar properties, combined with its lower cost, render it a practical complement. In times of geopolitical instability or monetary expansion, silver can function as a safeguard against systemic risks.
Volatility and Associated Risks
Despite its advantages, silver is characterized by pronounced price volatility. Its smaller market size relative to gold renders it more susceptible to speculative trading and abrupt shifts in investor sentiment. Furthermore, fluctuations in industrial demand can amplify short-term price movements. While this volatility can generate significant returns, it also exposes investors to heightened risk. Accordingly, silver is best employed as a long-term holding within a diversified portfolio rather than as a vehicle for short-term speculation.
Portfolio Diversification and Investment Vehicles
Incorporating silver into a portfolio enhances diversification by introducing an asset class with low correlation to equities and fixed income securities. This non-correlation reduces overall portfolio risk and provides stability during market downturns. Investors may access silver through several channels: physical bullion for tangible ownership, ETFs for liquidity, mining stocks for leveraged exposure, and futures contracts for advanced strategies. Each vehicle entails distinct risk-reward profiles, enabling investors to tailor their approach according to objectives and tolerance.
Conclusion
Silver’s dual identity as both a precious metal and an industrial commodity distinguishes it from other investment assets. Its affordability, inflation-hedging capacity, and diversification benefits make it a compelling addition to portfolios. While volatility requires prudent management, silver’s potential to balance defensive and growth-oriented strategies underscores its enduring relevance in contemporary investment practice.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
BASIC DEFINITIONS
***
***
The velocity of money is a fundamental concept in macroeconomics that measures how quickly money circulates through the economy. It reflects the frequency with which a unit of currency is used to purchase goods and services within a given time period. This metric is crucial for understanding economic activity, inflation, and the effectiveness of monetary policy.
At its core, the velocity of money is calculated using the formula:
This equation shows how many times money turns over in the economy to support a given level of economic output. For example, if the GDP is $20 trillion and the money supply (say, M2) is $10 trillion, the velocity is 2—meaning each dollar is used twice in a year to purchase goods and services.
There are different measures of money supply used in this calculation, most commonly M1 and M2. M1 includes the most liquid forms of money, such as cash and checking deposits, while M2 includes M1 plus savings accounts and other near-money assets. The choice of which measure to use depends on the context and the specific economic analysis being conducted.
The velocity of money is influenced by several factors:
Consumer and business confidence: When people feel optimistic about the economy, they are more likely to spend rather than save, increasing velocity.
Interest rates: Higher interest rates can encourage saving and reduce spending, lowering velocity. Conversely, lower rates can stimulate borrowing and spending.
Inflation expectations: If people expect prices to rise, they may spend more quickly, increasing velocity.
Technological and structural changes: Innovations in digital payments and shifts in consumer behavior can also affect how quickly money moves.
Historically, the velocity of money has fluctuated with economic cycles. During periods of economic expansion, velocity tends to rise as spending increases. In contrast, during recessions or periods of uncertainty, velocity often falls as consumers and businesses hold onto cash. For instance, during the 2008 financial crisis and the early stages of the COVID-19 pandemic, velocity dropped sharply due to reduced consumer spending and increased saving.
In recent years, the U.S. has experienced persistently low velocity, even amid significant increases in the money supply. This phenomenon has puzzled economists and raised questions about the effectiveness of monetary policy. Despite aggressive stimulus measures, much of the new money has remained in savings or financial markets rather than circulating through the real economy.
Understanding the velocity of money is essential for policymakers. A low velocity may signal weak demand and justify expansionary fiscal or monetary policies. Conversely, a high velocity could indicate overheating and the need for tightening measures to prevent inflation.
In conclusion, the velocity of money is a dynamic indicator of economic vitality. It helps economists and central banks assess the flow of money, the strength of demand, and the potential for inflation.
While often overlooked by the public, it plays a vital role in shaping economic policy and understanding the broader health of the economy.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
For generations, the prevailing belief in healthcare has been that physicians [MD, DO and DPM], with their high salaries and prestige, inevitably retire wealthier than nurses. Yet this assumption overlooks the financial realities of different nursing specialties and the long‑term impact of debt, lifestyle, and retirement planning. In fact, some Registered Nurses (RNs)—particularly Certified Registered Nurse Anesthetists (CRNAs), visiting nurses, and those who participate in structured pay programs like the Baylor plan—can retire richer than physicians. The reasons lie in the interplay of education costs, career flexibility, income potential, and disciplined financial planning.
Education Costs and Debt Burden
One of the most decisive factors shaping retirement wealth is the cost of education. Physicians often spend over a decade in training, including undergraduate studies, medical school, and residency. This path not only delays their earning years but also saddles them with substantial student debt. The median medical school debt in the United States exceeds $200,000, and many physicians spend years paying it down.
By contrast, RNs typically complete their training in two to four years, with advanced practice nurses such as CRNAs requiring graduate‑level education. Even so, their debt burden is far lighter, often less than half of what physicians carry. This difference means nurses can begin earning earlier, save for retirement sooner, and avoid the crushing interest payments that erode physicians’ wealth. A CRNA who starts practicing in their late twenties may already be investing in retirement accounts while a physician is still in residency earning a modest stipend.
Income Potential of Specialized Nurses
While physicians generally earn more annually than nurses, the gap is narrower in certain specialties. CRNAs, for example, are among the highest‑paid nursing professionals, with average salaries often exceeding $200,000 per year. This places them in direct competition with some physician specialties, especially primary care doctors, who may earn similar or even lower salaries.
Visiting nurses also benefit from unique financial advantages. Many work on flexible schedules, contract arrangements, or per‑visit compensation models. This allows them to maximize income while minimizing burnout. By avoiding the overhead costs of private practice and the administrative burdens physicians face, visiting nurses can channel more of their earnings directly into savings and investments.
When combined with lower debt and earlier career starts, these income streams can compound into significant retirement wealth.
The Baylor plan, a structured pay program used by some hospitals, allows nurses to work full‑time hours compressed into fewer days—often weekends—while still receiving full‑time pay and benefits. This arrangement provides several financial advantages. First, it enables nurses to earn competitive wages while freeing up weekdays for additional work, education, or entrepreneurial ventures. Second, it reduces commuting and childcare costs, allowing more income to be saved. Third, the plan often includes robust retirement benefits, such as employer‑matched contributions to 401(k) or pension programs.
Nurses who consistently participate in such structured pay plans can accumulate substantial nest eggs, often surpassing physicians who delay retirement savings due to debt repayment or lifestyle inflation. The Baylor plan highlights the importance of systematic investing: by automating contributions and focusing on long‑term growth, nurses can harness the power of compound interest. A nurse who invests steadily for 35 years may accumulate more wealth than a physician who begins saving late and inconsistently, despite earning a higher salary.
Lifestyle and Work‑Life Balance
Another overlooked factor is lifestyle. Physicians often face grueling schedules, high stress, and the temptation to maintain expensive lifestyles commensurate with their social status. Luxury homes, cars, and vacations can erode their financial base. Nurses, while not immune to lifestyle inflation, often maintain more modest spending habits.
Visiting nurses, in particular, enjoy flexibility that allows them to balance work with personal life. This reduces burnout and healthcare costs while enabling consistent employment into later years. By living within their means and prioritizing savings, nurses can accumulate wealth steadily without the financial pitfalls that sometimes accompany physician lifestyles.
Retirement Wealth Beyond Salary
Retirement wealth is not solely determined by annual income. It is shaped by debt management, savings discipline, investment strategies, and lifestyle choices. Nurses who leverage high‑paying specialties like anesthesia, flexible arrangements like visiting nursing, and structured programs like the Baylor plan can outperform physicians in these areas.
Consider two professionals: a physician earning $250,000 annually but burdened by $200,000 in debt and high living expenses, and a CRNA earning $200,000 with minimal debt and disciplined savings. Over decades, the CRNA may accumulate more net wealth, retire earlier, and enjoy greater financial security.
Conclusion
The assumption that physicians always retire richer than nurses is outdated. While physicians command higher salaries, their delayed earnings, heavy debt, and lifestyle pressures often undermine long‑term wealth. Nurses, particularly CRNAs, visiting nurses, and those who participate in structured pay programs like the Baylor plan, can retire wealthier by combining lower debt, earlier savings, competitive incomes, and disciplined financial planning.
Ultimately, retirement wealth is not about prestige but about strategy. Nurses who recognize this truth and act accordingly may find themselves enjoying more financial freedom than the very physicians they once assisted.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Physicians are increasingly facing car repossessions in 2025 due to rising debt, high vehicle prices, and economic pressures that are reshaping the financial landscape for medical professionals.
Traditionally viewed as financially secure, doctors are now among the growing number of Americans struggling to keep up with auto loan payments. The surge in car repossessions—expected to reach a record 10.5 million assignments by the end of 2025—has not spared the medical community. While physicians often earn higher-than-average incomes, they also carry significant financial burdens, including student loan debt, practice overhead, and personal expenses. These pressures are being amplified by macroeconomic forces such as inflation, high interest rates, and stagnant reimbursement rates.
One of the key contributors to this trend is the soaring cost of vehicles. In 2025, the average price of a new car in the U.S. surpassed $50,000, a dramatic increase from just a decade ago. For physicians who rely on vehicles for commuting between hospitals, clinics, and private practices, owning a reliable car is not a luxury—it’s a necessity. However, the combination of high sticker prices and elevated interest rates—averaging 7.3% for used cars and 11.5% for new cars—has made financing increasingly difficult.
***
***
Even high-income professionals are not immune to the broader auto loan crisis. Subprime auto loan delinquencies reached 6.6% in early 2025, the highest rate in over 30 years.While physicians typically fall into the prime or super-prime credit categories, many are still affected by cash flow disruptions, especially those in private practice or rural areas where patient volumes and insurance reimbursements have declined. Additionally, younger doctors with substantial student debt may find themselves overleveraged, making it harder to keep up with car payments.
The emotional and professional toll of a car repossession can be significant. Beyond the embarrassment and logistical challenges, losing a vehicle can disrupt a physician’s ability to provide care, attend emergencies, or maintain a consistent work schedule. This can lead to further income loss, creating a vicious cycle of financial instability.
To combat this trend, some physicians are turning to financial advisors to restructure their debt, refinance auto loans, or downsize to more affordable vehicles. Others are advocating for systemic reforms, such as student loan forgiveness, higher Medicare reimbursements, and better financial literacy training during medical education.
In conclusion, the rise in car repossessions among doctors is a stark reminder that no profession is immune to economic volatility. As the cost of living continues to climb and financial pressures mount, even those in traditionally stable careers must adapt to protect their assets and livelihoods.
Addressing this issue requires both individual financial planning and broader policy changes to ensure that physicians can continue to serve their communities without the looming threat of personal financial collapse.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
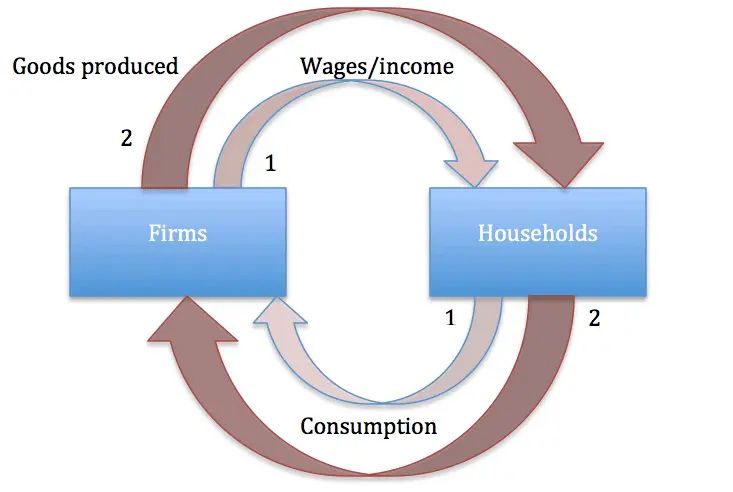
Say’s Law, named after the French economist Jean‑Baptiste Say, is a foundational idea in classical economics. Often summarized as “supply creates its own demand,” the law suggests that the act of producing goods and services inherently generates the income necessary to purchase them. This principle shaped economic thought throughout the 19th century and continues to influence debates about markets, government intervention, and the causes of economic crises.
Origins and Meaning Jean‑Baptiste Say introduced his law in the early 1800s in his Treatise on Political Economy. He argued that production is the source of demand: when producers create goods, they pay wages, rents, and profits, which in turn become purchasing power. In this view, general overproduction is impossible because every supply of goods corresponds to an equivalent demand. If imbalances occur, they are temporary and limited to specific sectors, not the economy as a whole.
Core Principles Say’s Law rests on several assumptions:
Markets are self‑correcting: Any surplus in one area leads to adjustments in prices and production.
Money is neutral: It serves only as a medium of exchange, not as a driver of demand.
Production drives prosperity: Economic growth depends on increasing output, not stimulating consumption.
No long‑term unemployment: Since supply creates demand, workers displaced in one industry will eventually find employment elsewhere.
These ideas aligned with classical economists’ belief in minimal government intervention and the efficiency of free markets.
Influence on Classical Economics Say’s Law became a cornerstone of classical economics, reinforcing the belief that recessions or depressions were temporary and self‑correcting. Economists like David Ricardo and John Stuart Mill adopted versions of the law, using it to argue against policies aimed at stimulating demand. The law supported laissez‑faire approaches, suggesting that governments should avoid interfering with markets, as production itself would ensure economic balance.
Criticism and Keynesian Revolution Say’s Law faced its greatest challenge during the Great Depression of the 1930s. Widespread unemployment and idle factories contradicted the idea that supply automatically generates demand. John Maynard Keynes famously rejected Say’s Law in his General Theory of Employment, Interest, and Money (1936). Keynes argued that demand, not supply, drives economic activity. He showed that insufficient aggregate demand could lead to prolonged recessions, requiring government intervention through fiscal and monetary policies.
Keynes’s critique marked a turning point in economics. While Say’s Law emphasized production, Keynesian economics highlighted consumption and demand management. This shift reshaped economic policy, leading to active government roles in stabilizing economies.
Modern Perspectives Today, Say’s Law is not accepted in its original form, but elements of it remain relevant. Supply‑side economists, for example, argue that policies encouraging production—such as tax cuts and deregulation—can stimulate growth. In contrast, Keynesians stress the importance of demand management. The debate reflects a broader tension in economics: whether prosperity depends more on producing goods or ensuring people have the means and willingness to buy them.
Conclusion: Say’s Law was a bold attempt to explain the self‑sustaining nature of markets. While its claim that “supply creates its own demand” proved too simplistic in the face of modern economic realities, it remains a vital part of the history of economic thought. The controversy surrounding Say’s Law highlights the evolving nature of economics, where theories are tested against real‑world crises and adapted to new circumstances. Even today, discussions of supply‑side versus demand‑side policies echo the enduring influence of Say’s original insight.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Money is a powerful tool. It can provide security, open opportunities, and help build a fulfilling life. Yet, when mismanaged, it can quickly become a source of stress and regret. Understanding the worst ways to use money is essential for anyone who wants to avoid financial pitfalls and build lasting stability.
1. Impulse Spending
One of the most damaging habits is spending without thought. Buying items on impulse—whether it’s clothes, gadgets, or luxury goods—often leads to regret and wasted resources. These purchases rarely align with long‑term goals and can drain savings meant for emergencies or investments.
2. High‑Interest Debt
Credit cards and payday loans can trap people in cycles of debt. Paying 20% or more in interest means that even small purchases balloon into massive financial burdens. Using debt irresponsibly is one of the fastest ways to erode wealth.
3. Ignoring Savings and Investments
Failing to save for the future is another critical mistake. Without an emergency fund, unexpected expenses like medical bills or car repairs can derail financial stability. Similarly, neglecting investments means missing out on compound growth that builds wealth over time.
4. Chasing Get‑Rich‑Quick Schemes
From pyramid schemes to speculative “hot tips,” chasing unrealistic returns is a recipe for disaster. These schemes prey on greed and impatience, often leaving participants with nothing but losses. Sustainable wealth comes from patience and discipline, not shortcuts.
5. Overspending on Status
Many people waste money trying to impress others—buying luxury cars, designer clothes, or extravagant experiences they cannot afford. This pursuit of status often leads to debt and financial insecurity, while providing only fleeting satisfaction.
6. Neglecting Insurance
Skipping health, auto, or home insurance to save money may seem smart in the short term, but it can be catastrophic when disaster strikes. Without protection, one accident or emergency can wipe out years of savings.
7. Failing to Budget
Living without a plan is like sailing without a map. Without a budget, it’s easy to overspend, miss bills, or fail to allocate money toward goals. Budgeting is not restrictive—it’s empowering, because it ensures money is used intentionally.
8. Ignoring Education and Skills
Spending money without investing in personal growth is another hidden mistake. Education, training, and skill development often yield lifelong returns. Neglecting these opportunities can limit earning potential and financial independence.
Conclusion
The worst things to do with money often stem from short‑term thinking, lack of discipline, or the desire for instant gratification. Impulse spending, high‑interest debt, chasing schemes, and neglecting savings all undermine financial health. By avoiding these traps and focusing on budgeting, investing wisely, and protecting against risks, money can serve as a foundation for security and freedom rather than a source of stress.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 9, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEdand Copilot A.I.
***
***
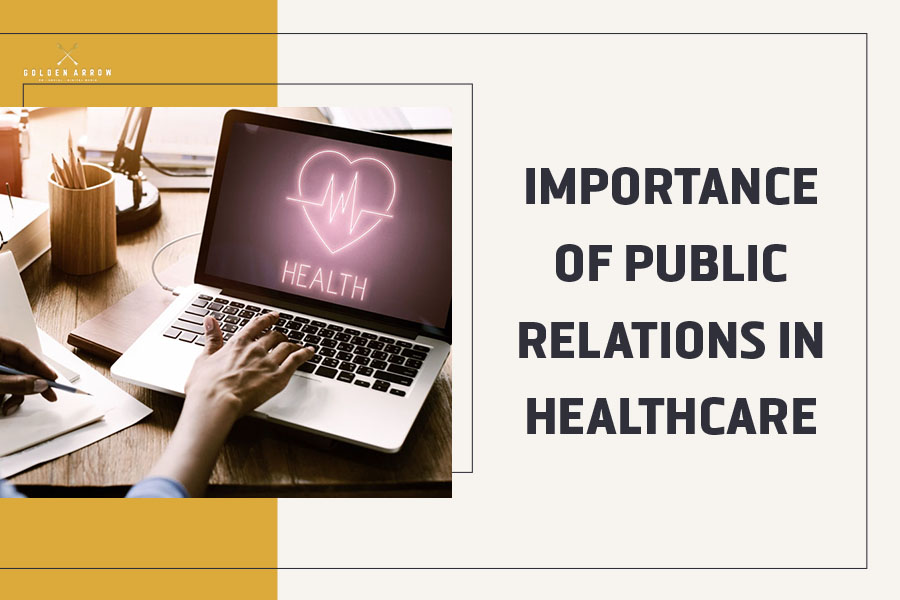
Public relations (PR) in medicine is a specialized field that focuses on managing communication between healthcare organizations, medical professionals, and the public. Unlike traditional marketing, which emphasizes selling services, PR in medicine emphasizes trust, credibility, and education. In a sector where lives and well-being are at stake, effective communication is not optional—it is essential.
1. Building Trust and Reputation
Healthcare institutions rely heavily on public trust. Patients must feel confident in the competence and integrity of hospitals, clinics, and medical professionals. PR strategies such as press releases, community outreach, and media engagement help establish credibility. For example, when hospitals share success stories of medical breakthroughs or highlight patient-centered initiatives, they reinforce their reputation as reliable and compassionate providers.
2. Health Education and Awareness
One of the most important functions of PR in medicine is educating the public. Medical jargon can be complex, and PR professionals translate it into accessible language. Campaigns about preventive care, vaccination, or chronic disease management empower communities to make informed health decisions. By bridging the knowledge gap, PR ensures that medical information is not confined to professionals but reaches the wider population in a clear and actionable way.
3. Crisis Communication
Healthcare organizations often face crises—ranging from disease outbreaks to medical errors. In such moments, PR becomes the frontline defense. Transparent communication, timely updates, and empathy are crucial in maintaining public confidence. For instance, during the COVID-19 pandemic, hospitals and health agencies relied on PR to disseminate accurate information, counter misinformation, and reassure anxious populations. Effective crisis communication can prevent panic and sustain trust even in challenging times.
4. Advocacy and Community Engagement
PR in medicine also involves advocacy for public health policies and community engagement. Hospitals and medical associations often use PR campaigns to support initiatives such as mental health awareness, anti-smoking drives, or nutrition education. By engaging with communities through events, seminars, and social media, healthcare organizations position themselves as partners in public well-being rather than distant institutions.
5. Digital Transformation in Medical PR
The rise of digital media has transformed healthcare PR. Social media platforms, blogs, and online forums allow medical institutions to communicate directly with patients. This immediacy enhances transparency but also requires careful management to avoid misinformation. Digital PR strategies now include online reputation management, patient testimonials, and interactive health campaigns. In this way, PR adapts to modern communication channels while maintaining its core mission of trust and education.
6. Ethical Responsibility
Unlike other industries, PR in medicine carries a profound ethical responsibility. Misleading information can have life-threatening consequences. Therefore, PR professionals in healthcare must prioritize accuracy, sensitivity, and compassion. Their role is not only to protect the image of institutions but also to safeguard public health.
Conclusion
Public relations in medicine is more than a communication tool—it is a bridge between science and society. By fostering trust, educating communities, managing crises, and advocating for health, PR ensures that medical institutions remain credible and compassionate. In an era of rapid medical advancements and global health challenges, the importance of PR in medicine continues to grow, making it an indispensable part of modern healthcare.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Insurance agents are primarily paid through commissions, but may also earn salaries, bonuses, and fees depending on their employment model and the types of policies they sell.
Insurance agents play a vital role in helping individuals and businesses navigate the complex world of insurance. Their compensation structures vary widely, influenced by factors such as the type of insurance they sell, whether they work independently or for a company, and the specific agreements they have with insurers. Understanding how insurance agents are paid is essential for consumers who want to make informed decisions and for aspiring agents considering a career in the industry.
The most common form of compensation for insurance agents is commission-based pay. Agents earn a percentage of the premium paid by the customer when they successfully sell a policy. These commissions can vary depending on the type of insurance. For example, first-year commissions for auto and homeowners insurance typically range from 5% to 20%, while commercial property and casualty policies may offer 10% to 15%. Life insurance policies often provide higher initial commissions, sometimes exceeding 50% of the first-year premium, followed by smaller renewal commissions in subsequent years.
There are two main types of insurance agents: captive agents and independent agents. Captive agents work exclusively for one insurance company and usually receive a combination of salary and commissions. Their compensation may also include performance bonuses and incentives tied to sales targets. Independent agents, on the other hand, represent multiple insurers and rely more heavily on commissions. They have the flexibility to offer a wider range of products, but their income is directly tied to their ability to sell policies and maintain client relationships.
***
***
In addition to commissions, some agents earn fees for services such as policy reviews, risk assessments, or consulting. These fees are more common in commercial insurance or financial planning contexts, where agents provide specialized expertise. However, fee-based compensation is less prevalent in personal lines of insurance like auto or home coverage.
Bonuses and incentives are another component of agent compensation. Insurance companies often reward agents for meeting sales quotas, retaining clients, or selling specific types of policies. These bonuses can significantly boost an agent’s income, but they may also create potential conflicts of interest if agents prioritize higher-paying products over client needs.
Some agents, particularly those employed by large firms or call centers, receive a fixed salary. This model provides stability but may limit earning potential compared to commission-based roles. Salaried agents may still receive performance bonuses or profit-sharing depending on company policy.
Ultimately, an insurance agent’s earnings depend on their business model, experience, and ability to build a loyal client base. While commissions remain the cornerstone of insurance compensation, the rise of fee-based services and hybrid models reflects a shift toward more transparent and client-focused practices.
Consumers should feel empowered to ask agents about their compensation structure to ensure they receive unbiased advice tailored to their needs.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
High-frequency trading (HFT) is a form of algorithmic trading that uses powerful computers and complex programs to execute thousands of trades in fractions of a second. It has transformed modern financial markets by increasing speed, liquidity, and efficiency—but also raised concerns about fairness and stability.
High-frequency trading emerged in the early 2000s as technological advances allowed financial firms to process market data and execute trades faster than ever before. HFT firms use sophisticated algorithms to analyze multiple markets and identify short-term opportunities. These trades are often held for mere seconds or milliseconds, and profits are made by exploiting tiny price discrepancies across assets or exchanges.
One of the defining features of HFT is its reliance on speed. Firms invest heavily in infrastructure—such as co-location services near exchange servers and fiber-optic cables—to gain microsecond advantages over competitors. This race for speed has led to a technological arms race, where milliseconds can mean millions in profit.
HFT contributes significantly to market liquidity, meaning it helps ensure that buyers and sellers can transact quickly at stable prices. By constantly placing and updating orders, HFT firms narrow bid-ask spreads and reduce transaction costs for other market participants. This has made markets more efficient and accessible, especially for retail investors.
However, HFT is not without controversy. Critics argue that it creates an uneven playing field, where firms with access to advanced technology and capital can dominate markets. Concerns about market manipulation—such as quote stuffing (flooding the market with orders to slow competitors) or spoofing (placing fake orders to move prices)—have led to increased regulatory scrutiny.
The 2010 Flash Crash is often cited as a cautionary example of HFT’s potential risks. During this event, the Dow Jones Industrial Average plunged nearly 1,000 points in minutes before rebounding. Investigations revealed that automated trading systems, including HFT algorithms, contributed to the sudden loss of liquidity and extreme volatility.
Regulators have responded by implementing safeguards such as circuit breakers, which pause trading during extreme price movements, and requiring firms to register and disclose their trading strategies. The Securities and Exchange Commission (SEC) and Commodity Futures Trading Commission (CFTC) continue to monitor HFT’s impact on market integrity.
Despite its challenges, HFT remains a dominant force in global finance. It accounts for a significant portion of trading volume in equities, futures, and foreign exchange markets. Many institutional investors rely on HFT strategies to manage large portfolios and hedge risks.
In conclusion, high-frequency trading represents both the promise and peril of technological innovation in finance. While it enhances market efficiency and liquidity, it also introduces new risks and ethical dilemmas.
As markets evolve, balancing innovation with fairness and stability will be essential to ensuring that HFT serves the broader interests of investors and the economy.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on November 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
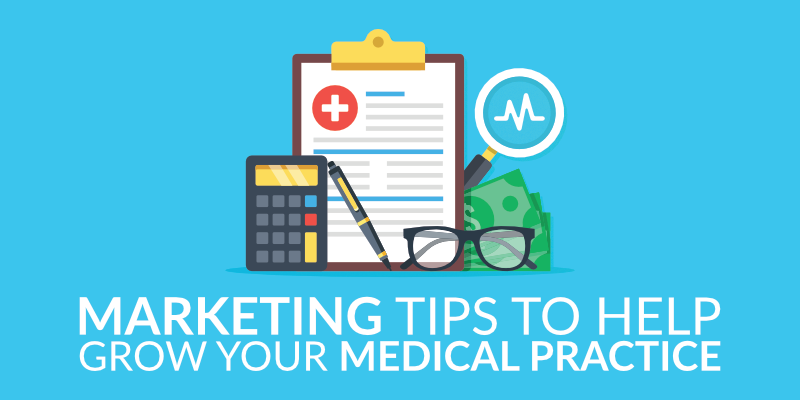
In today’s competitive healthcare landscape, effective marketing is essential for the growth and sustainability of a medical practice. Gone are the days when word-of-mouth alone could sustain a clinic. Patients now seek providers who not only offer excellent care but also communicate their value clearly and consistently. Strategic marketing helps medical practices attract new patients, retain existing ones, and build a strong reputation in the community.
🎯 Understanding the Target Audience
The foundation of any successful marketing strategy is a deep understanding of the target audience. Medical practices must identify the demographics, needs, and preferences of their ideal patients. For example, a pediatric clinic will focus on parents, while a dermatology practice may target young adults concerned with skin health. Tailoring messages to resonate with these groups ensures that marketing efforts are relevant and effective.
🌐 Building a Strong Online Presence
In the digital age, a robust online presence is non-negotiable. A professional, user-friendly website serves as the virtual front door of the practice. It should include essential information such as services offered, provider bios, contact details, and online appointment scheduling. Search engine optimization (SEO) ensures the site ranks well on Google, making it easier for potential patients to find the practice.
Social media platforms like Facebook, Instagram, and LinkedIn offer additional avenues to engage with the community. Regular posts about health tips, staff spotlights, and patient testimonials humanize the practice and foster trust. Paid advertising on these platforms can also target specific demographics, increasing visibility and driving traffic to the website.
🗣️ Leveraging Patient Reviews and Testimonials
Online reviews are a powerful form of social proof. Encouraging satisfied patients to leave positive feedback on platforms like Google, Yelp, and Healthgrades can significantly influence prospective patients. Testimonials can also be featured on the practice’s website and social media channels. Responding to reviews—both positive and negative—demonstrates attentiveness and a commitment to patient satisfaction.
📬 Utilizing Email and Content Marketing
Email marketing remains a cost-effective way to stay connected with patients. Monthly newsletters can include health tips, updates on services, and reminders for annual checkups or vaccinations. Content marketing, such as blog posts and educational videos, positions the practice as a trusted authority in healthcare. This not only boosts SEO but also builds credibility and patient loyalty.
***
***
🤝 Community Engagement and Partnerships
Participating in local events, offering free health screenings, or partnering with schools and businesses can enhance visibility and goodwill. These efforts show that the practice is invested in the well-being of the community, which can translate into increased patient referrals and long-term relationships.
📊 Measuring Success
Finally, tracking the performance of marketing campaigns is crucial. Metrics such as website traffic, appointment bookings, social media engagement, and patient acquisition rates provide insights into what’s working and what needs adjustment. Regular analysis ensures that marketing efforts remain aligned with business goals.
Marketing a medical practice requires a thoughtful blend of digital tools, patient engagement, and community outreach. When done right, it not only drives growth but also reinforces the practice’s mission to provide compassionate, high-quality care.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on November 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
The Sraffa–Hayek debate stands as a pivotal moment in the history of economic thought, highlighting deep philosophical and methodological differences between two influential schools: the Austrian School, represented by Friedrich Hayek, and the neo-Ricardian or Cambridge School, represented by Piero Sraffa. Taking place primarily in the 1930s, this intellectual exchange centered on the nature of capital, the role of equilibrium, and the validity of marginalist theory.
Friedrich Hayek, a staunch advocate of Austrian economics, had developed a theory of business cycles rooted in the mis allocation of capital due to artificially low interest rates. In his framework, interest rates serve as signals that coordinate inter temporal production decisions. When central banks distort these signals, they cause over investment in capital-intensive industries, leading to unsustainable booms followed by inevitable busts. Hayek’s theory was grounded in a time-structured view of capital, emphasizing the importance of temporal coordination in production.
Piero Sraffa, a Cambridge economist and close associate of John Maynard Keynes, challenged Hayek’s assumptions in a 1932 review of Hayek’s book Prices and Production. Sraffa’s critique was both technical and philosophical. He questioned the coherence of Hayek’s notion of a uniform natural rate of interest in a complex economy with heterogeneous capital goods. Sraffa argued that in such an economy, there could be multiple natural rates of interest, making it impossible to define a single rate that equilibrates savings and investment across all sectors.
Moreover, Sraffa criticized the Austrian reliance on equilibrium analysis in a world characterized by uncertainty and institutional complexity. He contended that Hayek’s model was overly abstract and detached from real-world dynamics. This critique foreshadowed Sraffa’s later work, Production of Commodities by Means of Commodities (1960), which laid the foundation for the neo-Ricardian critique of marginalist economics. In that work, Sraffa demonstrated that prices and distribution could be determined without recourse to subjective utility or marginal productivity, challenging the core of neoclassical theory.
The debate had far-reaching implications. For the Austrian School, it exposed vulnerabilities in their capital theory and prompted refinements in their approach to intertemporal coordination. For the broader economics profession, Sraffa’s critique contributed to a growing skepticism about the internal consistency of marginalist value theory, influencing the Cambridge capital controversies of the 1950s and 1960s.
While the Sraffa–Hayek debate did not produce a definitive victor, it underscored the importance of foundational assumptions in economic modeling. It also highlighted the tension between abstract theoretical elegance and empirical relevance—a tension that continues to shape economic discourse today. Ultimately, the debate enriched the intellectual landscape by forcing economists to confront the limitations of their models and to grapple with the complex realities of capital, time, and uncertainty.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
The Life Cycle Hypothesis (LCH) is a foundational theory in economics and personal finance that explains how individuals plan their consumption and savings behavior over the course of their lives. Developed in the 1950s by economists Franco Modigliani and Richard Brumberg, the LCH posits that people aim to smooth their consumption throughout their lifetime, regardless of fluctuations in income. This theory has had a profound impact on how economists, financial planners, and policymakers understand saving patterns, retirement planning, and fiscal policy.
At its core, the LCH assumes that individuals are forward-looking and rational. They anticipate changes in income—such as those caused by retirement, unemployment, or career progression—and adjust their saving and spending accordingly. During high-income periods, typically in mid-career, individuals save more to prepare for low-income phases, such as retirement. Conversely, in early adulthood and old age, when income is lower, individuals are expected to dissave, or spend from their accumulated savings.
One of the key insights of the LCH is that consumption is not directly tied to current income but rather to expected lifetime income. This means that temporary changes in income should not significantly affect consumption patterns, as individuals base their spending decisions on long-term expectations. For example, a young professional may take out a loan to buy a car, anticipating higher future earnings that will allow them to repay the debt without drastically altering their lifestyle.
The LCH also provides a framework for understanding the role of pensions, social security, and other retirement savings mechanisms. By recognizing that individuals need to save during their working years to maintain consumption levels in retirement, the theory supports the development of policies that encourage long-term savings and financial literacy. It also helps explain why some people may under-save or over-consume if they misjudge their future income or lack access to financial planning resources.
Despite its elegance, the Life Cycle Hypothesis has faced criticism and refinement. Behavioral economists argue that individuals are not always rational and may struggle with self-control, procrastination, or lack of financial knowledge. These limitations have led to the development of the Behavioral Life Cycle Hypothesis, which incorporates psychological factors such as mental accounting and framing effects. Moreover, empirical studies have shown that many people do not smooth consumption as predicted, often due to liquidity constraints, uncertainty, or cultural influences.
Nevertheless, the LCH remains a powerful tool for analyzing financial behavior across different stages of life. It has influenced retirement planning strategies, tax policy, and the design of financial products. By emphasizing the importance of long-term planning and the intertemporal nature of financial decisions, the Life Cycle Hypothesis continues to shape how individuals and institutions approach economic well-being.
In conclusion, the Life Cycle Hypothesis offers a compelling lens through which to view personal finance. While it may not capture every nuance of human behavior, its emphasis on lifetime income and consumption smoothing provides a valuable foundation for understanding and improving financial decision-making.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Product costing deals with determining the total costs involved in the production of a good or service. Costs may be broken down into subcategories, such as variable, fixed, direct, or indirect costs. Cost accounting is used to measure and identify those costs, in addition to assigning overhead to each type of product created by the company.
Managerial accountants calculate and allocate overhead charges to assess the full expense related to the production of a good. The overhead expenses may be allocated based on the number of goods produced or other activity drivers related to production, such as the square footage of the facility. In conjunction with overhead costs, managerial accountants use direct costs to properly value the cost of goods sold and inventory that may be in different stages of production.
Marginal costing (sometimes called cost-volume-profit analysis) is the impact on the cost of a product by adding one additional unit into production. It is useful for short-term economic decisions. The contribution margin of a specific product is its impact on the overall profit of the company. Margin analysis flows into break-even analysis, which involves calculating the contribution margin on the sales mix to determine the unit volume at which the business’s gross sales equals total expenses. Break-even point analysis is useful for determining price points for products and services.
Cash Flow Analysis
Managerial accountants perform cash flow analysis in order to determine the cash impact of business decisions. Most companies record their financial information on the accrual basis of accounting. Although accrual accounting provides a more accurate picture of a company’s true financial position, it also makes it harder to see the true cash impact of a single financial transaction. A managerial accountant may implement working capital management strategies in order to optimize cash flow and ensure the company has enough liquid assets to cover short-term obligations.
When a managerial accountant performs cash flow analysis, he will consider the cash inflow or outflow generated as a result of a specific business decision. For example, if a department manager is considering purchasing a company vehicle, he may have the option to either buy the vehicle outright or get a loan. A managerial accountant may run different scenarios by the department manager depicting the cash outlay required to purchase outright upfront versus the cash outlay over time with a loan at various interest rates.
Inventory Turnover Analysis
Inventory turnover is a calculation of how many times a company has sold and replaced inventory in a given time period. Calculating inventory turnover can help businesses make better decisions on pricing, manufacturing, marketing, and purchasing new inventory. A managerial accountant may identify the carrying cost of inventory, which is the amount of expense a company incurs to store unsold items.
If the company is carrying an excessive amount of inventory, there could be efficiency improvements made to reduce storage costs and free up cash flow for other business purposes.
Constraint Analysis
Managerial accounting also involves reviewing the constraints within a production line or sales process. Managerial accountants help determine where bottlenecks occur and calculate the impact of these constraints on revenue, profit, and cash flow. Managers then can use this information to implement changes and improve efficiencies in the production or sales process.
Financial Leverage Metrics
Financial leverage refers to a company’s use of borrowed capital in order to acquire assets and increase its return on investments. Through balance sheet analysis, managerial accountants can provide management with the tools they need to study the company’s debt and equity mix in order to put leverage to its most optimal use.
Performance measures such as return on equity, debt to equity, and return on invested capital help management identify key information about borrowed capital, prior to relaying these statistics to outside sources. It is important for management to review ratios and statistics regularly to be able to appropriately answer questions from its board of directors, investors, and creditors.
Accounts Receivable (AR) Management
Appropriately managing accounts receivable (AR) can have positive effects on a company’s bottom line. An accounts receivable aging report categorizes AR invoices by the length of time they have been outstanding. For example, an AR aging report may list all outstanding receivables less than 30 days, 30 to 60 days, 60 to 90 days, and 90+ days.
Through a review of outstanding receivables, managerial accountants can indicate to appropriate department managers if certain customers are becoming credit risks. If a customer routinely pays late, management may reconsider doing any future business on credit with that customer.
Budgeting, Trend Analysis, and Forecasting
Budgets are extensively used as a quantitative expression of the company’s plan of operation. Managerial accountants utilize performance reports to note deviations of actual results from budgets. The positive or negative deviations from a budget also referred to as budget-to-actual variances, are analyzed in order to make appropriate changes going forward.
Managerial accountants analyze and relay information related to capital expenditure decisions. This includes the use of standard capital budgeting metrics, such as net present value and internal rate of return, to assist decision-makers on whether to embark on capital-intensive projects or purchases. Managerial accounting involves examining proposals, deciding if the products or services are needed, and finding the appropriate way to finance the purchase. It also outlines payback periods so management is able to anticipate future economic benefits.
Managerial accounting also involves reviewing the trendline for certain expenses and investigating unusual variances or deviations. It is important to review this information regularly because expenses that vary considerably from what is typically expected are commonly questioned during external financial audits. This field of accounting also utilizes previous period information to calculate and project future financial information. This may include the use of historical pricing, sales volumes, geographical locations, customer tendencies, or financial information.
Nepo babies often go broke due to a mix of financial mismanagement, lack of resilience, and the illusion of inherited success. Their privileged upbringing can mask the need for discipline, adaptability, and long-term planning—traits essential for sustaining wealth.
The term nepo baby—short for nepotism baby—refers to children of celebrities or influential figures who benefit from family connections to launch careers, especially in entertainment, fashion, or media. While these individuals often start with significant advantages, including wealth, fame, and access, many struggle to maintain financial stability over time. The reasons are complex and rooted in both personal and systemic factors.
First, many nepo babies lack financial literacy. Growing up in environments where money flows freely, they may never learn budgeting, investing, or the value of money. Without these skills, they’re prone to overspending, poor investments, and unsustainable lifestyles. Lavish purchases—designer clothes, luxury cars, expensive homes—can quickly drain even sizable inheritances if not managed wisely.
Second, the illusion of guaranteed success can be dangerous. Nepo babies often enter industries where their family name opens doors, but that doesn’t guarantee longevity. Fame is fickle, and public interest can fade. If they don’t develop their own talents or work ethic, they may find themselves unemployable once the novelty wears off. This overreliance on family reputation can lead to complacency, making it harder to adapt when challenges arise.
Third, many nepo babies face identity crises and public scrutiny. Constant comparisons to their successful parents can erode confidence and create pressure to live up to unrealistic expectations. Some rebel by distancing themselves from their family’s legacy, while others try to prove themselves in unrelated fields. Either way, this struggle can lead to erratic career choices and unstable income streams.
Fourth, fame without privacy can fuel destructive habits. The entertainment world is rife with stories of young stars—many of them nepo babies—falling into substance abuse, reckless behavior, or toxic relationships. These issues not only affect mental health but also lead to legal troubles and financial loss. Without strong support systems or accountability, it’s easy to spiral.
Finally, inherited wealth can disappear quickly without proper estate planning. Trust funds and inheritances may be mismanaged or depleted by taxes, lawsuits, or poor financial advisors. Some nepo babies assume the money will last forever and fail to plan for long-term sustainability. Others are exploited by opportunistic friends or partners who take advantage of their naivety.
In contrast, those who succeed often do so by acknowledging their privilege, developing their own skills, and surrounding themselves with trustworthy mentors. They treat their inherited platform as a launchpad—not a safety net—and work to build something lasting.
In short, nepo babies go broke not because they lack opportunity, but because opportunity without discipline is a recipe for downfall. Wealth and fame are fleeting without the grit to sustain them. The lesson here isn’t just about celebrity—it’s a universal truth: success inherited must still be earned.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on October 30, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Cryonics is a scientific and philosophical endeavor that seeks to preserve human life by freezing individuals at ultra-low temperatures after legal death, with the hope that future medical advancements may allow for revival and healing. Though still a speculative and controversial field, cryonics has captured the imagination of futurists, scientists, and ethicists alike.
What Is Cryonics?
Cryonics involves the process of cryopreservation—cooling the body, or sometimes just the brain, to -196°C using liquid nitrogen. The goal is to halt all biological activity, particularly decay, immediately after death. This is not the same as freezing; rather, it involves vitrification, a process that turns bodily fluids into a glass-like state to prevent ice crystal formation, which can damage cells. Once preserved, the body is stored indefinitely in a cryogenic chamber until such time that revival is theoretically possible.
***
***
Scientific and Technological Challenges
Despite its futuristic appeal, cryonics remains highly experimental. No human has ever been revived from a cryopreserved state, and current technology cannot reverse the damage caused by the preservation process itself. While scientists have successfully frozen and revived small biological samples like sperm and embryos, scaling this to entire human bodies presents enormous challenges.
The hope lies in future breakthroughs in nanotechnology, regenerative medicine, and artificial intelligence that could repair cellular damage and cure the diseases that led to death in the first place.
Posted on October 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
In the evolving landscape of digital health care, Amazon Pharmacy and GoodRx have emerged as two leading platforms offering consumers affordable and convenient access to prescription medications. While both aim to simplify the process of obtaining prescriptions, they differ significantly in their approach, pricing models, and user experience.
Amazon Pharmacy, launched in 2020, is a full-service online pharmacy that allows customers to order medications directly through Amazon. It offers fast, free delivery for Prime members and integrates with most insurance plans. One of its standout features is RxPass, a subscription service available to Prime members for $5 per month, which covers unlimited eligible generic medications. This model is particularly attractive to individuals who take multiple generics regularly, as it can significantly reduce out-of-pocket costs.
In contrast, GoodRx, founded in 2011, operates primarily as a price comparison and discount platform. It does not dispense medications itself but partners with local and mail-order pharmacies to help users find the lowest prices. GoodRx provides coupons that can be used at thousands of pharmacies nationwide, often resulting in substantial savings—especially for those without insurance. It also offers GoodRx Gold, a paid membership that unlocks deeper discounts and telehealth services.
***
***
When comparing the two, pricing transparency is a key differentiator. GoodRx excels in showing users a range of prices across different pharmacies, empowering them to choose the most cost-effective option. Amazon Pharmacy, while competitive, typically offers fixed prices and focuses more on convenience and integration with its broader ecosystem.
Convenience is another area where Amazon Pharmacy shines. With its streamlined ordering process, automatic refills, and integration with Amazon’s delivery network, it appeals to users who prioritize ease and speed. GoodRx, while convenient in its own right, requires users to present coupons at the pharmacy or use mail-order services, which may involve more steps.
Insurance compatibility also varies. Amazon Pharmacy accepts most major insurance plans, making it a viable option for insured individuals. GoodRx, on the other hand, is often used by those without insurance or with high deductibles, as its discounts can sometimes beat insurance copays.
However, both platforms have limitations. Amazon Pharmacy’s RxPass is restricted to generic medications and excludes certain states due to regulatory issues. GoodRx’s discounts may not apply to all medications, and prices can fluctuate depending on location and pharmacy.
In terms of user experience, Amazon offers a seamless, tech-driven interface with customer support and medication management tools. GoodRx provides educational resources, price alerts, and a mobile app that helps users track savings and prescriptions.
Ultimately, the choice between Amazon Pharmacy and GoodRx depends on individual needs. For those seeking a one-stop solution with predictable costs and fast delivery, Amazon Pharmacy may be ideal. For users who want to shop around for the best deal or lack insurance, GoodRx offers unmatched flexibility and savings.
As digital health continues to grow, both platforms are reshaping how Americans access medications—making prescriptions more affordable, transparent, and accessible than ever before.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
The global healthcare sector faces mounting challenges: rising costs, inefficiencies, limited access, and bureaucratic entanglements. In response, some economists and policymakers have turned to Austrian Economics for answers. Rooted in the works of Ludwig von Mises and Friedrich Hayek, Austrian Economics emphasizes individual choice, market-driven solutions, and skepticism toward centralized planning. But can this school of thought truly “save” healthcare?
At its core, Austrian Economics champions the idea that decentralized decision-making and free-market mechanisms lead to more efficient and responsive systems. In healthcare, this would mean reducing government control and allowing competition to drive innovation, lower costs, and improve quality. Proponents argue that when patients act as consumers and providers compete for their business, the system becomes more accountable and efficient. For example, direct primary care models—where patients pay physicians directly without insurance intermediaries—reflect Austrian principles and have shown promise in improving care and reducing administrative overhead.
Austrian theorists also critique the price distortions caused by third-party payers like insurance companies and government programs. According to them, when consumers are insulated from the true cost of care, demand becomes artificially inflated, leading to overutilization and waste. By restoring price signals—where patients see and respond to the actual cost of services—Austrian economists believe the market can better allocate resources and curb unnecessary spending.
However, critics argue that healthcare is not a typical market. Patients often lack the information, time, or capacity to make rational choices, especially in emergencies. Moreover, healthcare involves significant externalities and moral considerations that pure market logic may overlook. For instance, should access to life-saving treatment depend solely on one’s ability to pay? Austrian Economics offers little guidance on equity or universal access, which are central concerns in modern healthcare debates.
Austria itself provides an interesting case study. Despite the name, Austrian Economics is not the guiding philosophy behind Austria’s healthcare system. Instead, Austria operates a social insurance model with near-universal coverage, funded through mandatory contributions and managed by a mix of public and private actors. While recent reforms have aimed to streamline administration and reduce fragmentation he system remains largely collectivist—contrary to Austrian ideals.
In conclusion, Austrian Economics offers valuable insights into the inefficiencies of centralized healthcare systems and the potential benefits of market-based reforms. Its emphasis on individual choice, price transparency, and entrepreneurial innovation can inspire meaningful improvements. However, its limitations in addressing equity, access, and the unique nature of healthcare suggest that it cannot “save” the system on its own. A hybrid approach—blending market mechanisms with safeguards for universal access—may offer a more balanced path forward.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Valuing a medical practice involves assessing its financial performance, assets, and intangible factors like goodwill and patient loyalty to determine its fair market worth.
Determining the value of a medical practice is a nuanced process that blends financial analysis with strategic insight. Whether you’re preparing to sell, merge, or bring in a partner, understanding how to value your practice ensures informed decision-making and fair negotiations.
There are several recognized methods for valuing a medical practice, each suited to different scenarios. The most common include the income approach, market approach, asset-based approach, and the rule-of-thumb method.
The income approach focuses on the practice’s ability to generate future earnings. This method involves analyzing historical financial statements, projecting future cash flows, and discounting them to present value using a risk-adjusted rate. It’s particularly useful when the practice has stable revenue and predictable expenses. Key metrics include net income, physician productivity, and reimbursement rates.
The market approach compares the practice to similar ones that have recently sold. It relies on data from comparable transactions, adjusted for differences in size, specialty, location, and profitability. This method is ideal when reliable market data is available, though such data can be scarce for niche specialties or rural practices.
The asset-based approach calculates the value of tangible and intangible assets. Tangible assets include medical equipment, office furniture, and real estate. Intangible assets—like patient records, brand reputation, and goodwill—are harder to quantify but can significantly impact value. Goodwill, for instance, reflects the practice’s reputation, patient loyalty, and referral networks.
The rule-of-thumb method uses industry benchmarks, such as a multiple of annual revenue or earnings. For example, a general practice might be valued at 60–80% of annual gross revenue. While quick and easy, this method oversimplifies and may not reflect the unique strengths or weaknesses of a specific practice.https:/https://medicalexecutivepost.com/2025/03/17/medial-practice-valuation-adjustments//medicalexecutivepost.com/2025/03/17/medial-practice-valuation-adjustments/
Beyond these methods, several qualitative factors influence valuation. These include the size and diversity of the patient base, the practice’s specialty, use of technology (like EHR systems or telemedicine), and whether key physicians will remain post-sale. A practice heavily reliant on one provider may be less valuable than one with a strong team and succession plan.
Timing also matters. Economic conditions, regulatory changes, and shifts in healthcare reimbursement can affect practice value. Tax implications and deal structure—such as asset sale vs. stock sale—should also be considered during negotiations.
Ultimately, valuing a medical practice is both art and science. Engaging a professional appraiser or valuation expert can help ensure accuracy and objectivity. They bring experience, access to market data, and the ability to tailor valuation methods to your specific situation.
In summary, a comprehensive valuation considers financial performance, assets, market trends, and intangible factors. By understanding these elements, practice owners can make strategic decisions that reflect the true worth of their medical enterprise.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
What Medical School Didn’t Teach Doctors About Money
Medical school is designed to mold students into competent, compassionate physicians. It teaches anatomy, pathology, pharmacology, and clinical skills with precision and rigor. Yet, despite the depth of medical knowledge imparted, one critical area is often overlooked: financial literacy. For many doctors, the transition from student to professional comes with a steep learning curve—not in medicine, but in money. From managing debt to understanding taxes, investing, and retirement planning, medical school leaves a financial education gap that can have long-term consequences.
The Debt Dilemma
One of the most glaring omissions in medical education is how to manage student loan debt. The average medical student graduates with over $200,000 in debt, yet few are taught how to navigate repayment options, interest accrual, or loan forgiveness programs. Many doctors enter residency with little understanding of income-driven repayment plans or Public Service Loan Forgiveness (PSLF), missing opportunities to reduce their financial burden. Without guidance, some make costly mistakes—such as refinancing federal loans prematurely or choosing repayment plans that don’t align with their career trajectory.
Income ≠ Wealth
Medical students often assume that a high salary will automatically lead to financial security. While physicians do earn more than most professionals, income alone doesn’t guarantee wealth. Medical school rarely addresses the importance of budgeting, saving, and investing. As a result, many doctors fall into the “HENRY” trap—High Earner, Not Rich Yet. They spend lavishly, assuming their income will always cover expenses, only to find themselves living paycheck to paycheck. Without a solid financial foundation, even high earners can struggle to build net worth.
***
***
Taxes and Business Skills
Doctors are also unprepared for the complexities of taxes. Whether employed by a hospital or running a private practice, physicians face unique tax challenges. Medical school doesn’t teach how to track deductible expenses, optimize retirement contributions, or navigate self-employment taxes. For those who open their own clinics, the lack of business education is even more pronounced. Understanding profit margins, payroll, insurance billing, and compliance regulations is essential—but rarely covered in medical training.
Investing and Retirement Planning
Another blind spot is investing. Medical students are rarely taught the basics of compound interest, asset allocation, or retirement accounts. Many don’t know the difference between a Roth IRA and a traditional 401(k), or how to evaluate mutual funds and index funds. This lack of knowledge delays retirement planning and can lead to missed opportunities for long-term growth. Some doctors rely on financial advisors without understanding the fees or conflicts of interest involved, putting their wealth at risk.
Insurance and Risk Management
Medical school also fails to educate students on insurance—life, disability, malpractice, and health. Doctors need robust coverage to protect their income and assets, but many don’t know how to evaluate policies or understand terms like “own occupation” or “elimination period.” Inadequate coverage can leave physicians vulnerable to financial disaster in the event of illness, injury, or litigation.
Emotional and Behavioral Finance
Beyond technical knowledge, medical school overlooks the emotional side of money. Physicians often face pressure to maintain a certain lifestyle, especially after years of sacrifice. The desire to “catch up” can lead to impulsive spending, luxury purchases, and financial stress. Without tools to manage money mindset and behavioral habits, doctors may struggle with guilt, anxiety, or burnout related to finances.
The Case for Financial Education
Fortunately, awareness of this gap is growing. Organizations like Medics’ Money and podcasts such as “Docs Outside the Box” are working to fill the void by offering financial education tailored to physicians.
These resources cover everything from budgeting and debt management to investing and entrepreneurship. Some medical schools are beginning to incorporate financial literacy into their curricula, but progress is slow and inconsistent.
Conclusion
Medical school equips doctors to save lives, but it doesn’t prepare them to secure their own financial future. The lack of financial education leaves many physicians vulnerable to debt, poor investment decisions, and lifestyle inflation. To thrive both professionally and personally, doctors must seek out financial knowledge beyond the classroom. Whether through self-study, mentorship, or professional guidance, understanding money is as essential as understanding medicine. After all, financial health is a cornerstone of overall well-being—and every doctor deserves to master both.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
According to the Daily Beast, First Lady Melania Trump was allegedly used as “window dressing” in a multi-million-dollar memecoin scheme that deceived investors and enriched its crypto creators, according to a lawsuit filed in federal court. The suit involves the $Melania coin, which the 55-year-old First Lady promoted to her social media on the eve of President Donald Trump’s inauguration in January, writing, “The Official Melania Meme is live! You can buy $MELANIA now.” Many of Trump’s supporters purchased the coin, pushing it to trade at an all-time high price of $13.73 apiece. $Melania was trading at less than 10 cents per coin by Wednesday—a staggering crash in value. Investors in the coin filed a federal class action lawsuit in April against Benjamin Chow, co-founder of crypto exchange Meteora, and Hayden Davis, co-founder of crypto venture capital firm Kelsier Labs, among others, WIRED reported Tuesday.
***
Meme stock prices have shown dramatic volatility, with the Roundhill MEME ETF reflecting sharp swings driven by retail investor sentiment and social media hype.
The phenomenon of meme stocks—equities that gain popularity through online communities rather than traditional financial metrics—has reshaped market dynamics since early 2021. Companies like GameStop and AMC became emblematic of this trend, as retail investors coordinated on platforms like Reddit to drive prices to unprecedented highs. To capture this movement, the Roundhill Meme Stock ETF (ticker: MEME) was launched, bundling popular meme stocks into a single investment vehicle.
The price history of the MEME ETF illustrates the volatility inherent in meme stock investing. In October 2025 alone, the ETF experienced dramatic fluctuations. On October 13, it closed at $10.85, marking a 14.57% gain from the previous day. Just three days later, on October 16, it dropped to $9.97, an 8.95% decline. These swings reflect the influence of social media sentiment, short squeezes, and speculative trading rather than company fundamentals.
Over the past year, the MEME ETF has seen a 74.5% decline, underscoring the risks of investing in stocks driven by hype rather than earnings or growth potential. Despite occasional rallies, the overall trend has been downward, with the ETF trading around $8.93 as of the latest close.
This price history highlights the speculative nature of meme stocks. While they can offer short-term gains, they are highly susceptible to rapid reversals. Investors drawn to meme stocks should be aware of the emotional and social dynamics that drive their prices, and consider whether such volatility aligns with their risk tolerance and investment goals.
In essence, meme stock price history is a story of community-driven market disruption, where traditional valuation models are often sidelined in favor of viral momentum.
The MEME ETF serves as a barometer for this cultural shift, capturing both the excitement and the instability of this new investing frontier.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
An automobile is one of the biggest purchases after a home; for many physicians and most all of us. But, unlike the typical home, it is usually a depreciating asset – today morning you purchase a car for X-amount of dollars and by the evening it will be worth less. After 5 years it will not be even half-value but still, many folks keep buying cars regularly – buy at 10, sell at 4 & lose 6 (repeat the cycle).
So, here are few financial rules of thumb that you can follow:
The value of a car should not be more than 50% of the annual income of the owner.
Purchase a used car or buy a new & use it for 10 years.
While buying a car with a loan stick to Rule 20/4/10 – Minimum 20% down payment, loan tenure not more than 4 years & EMI should not be higher than 10% of your income.
Note: Equated Monthly Installment [EMI]
Caution: The phrase rule of thumb refers to an approximate method for doing something, based on practical experience rather than theory. This usage of the phrase can be traced back to the 17th century and has been associated with various trades where quantities were measured by comparison to the width or length of a human adult thumb.
Posted on October 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
DEFINED
***
***
A physician practice management corporation (PPMC) is a business entity that provides non-clinical administrative and operational support to medical practices, allowing physicians to focus on patient care while the corporation handles the business side of healthcare.
Physician practice management corporations emerged in response to the increasing complexity of running a medical practice. As healthcare regulations, insurance requirements, and operational costs grew, many physicians found it challenging to manage both clinical responsibilities and business operations. PPMCs offer a solution by taking over the administrative burdens, enabling physicians to concentrate on delivering quality care.
At their core, PPMCs are responsible for a wide range of non-medical services. These include billing and coding, human resources, payroll, marketing, compliance, information technology, and financial management. By centralizing these functions, PPMCs can achieve economies of scale, reduce overhead costs, and improve operational efficiency for the practices they manage. This model is particularly attractive to small and mid-sized practices that may lack the resources to manage these functions independently.
PPMCs typically enter into long-term management agreements with physician groups. In some cases, they may purchase the non-clinical assets of a practice—such as equipment, office space, and administrative staff—while the physicians retain control over clinical decisions and patient care. This arrangement allows for a clear division between medical and business responsibilities, which is essential for maintaining compliance with healthcare regulations like the Stark Law and the Anti-Kickback Statute.
A physician practice management corporation (PPMC) is a business entity that provides non-clinical administrative and operational support to medical practices, allowing physicians to focus on patient care while the corporation handles the business side of healthcare.
Physician practice management corporations emerged in response to the increasing complexity of running a medical practice. As healthcare regulations, insurance requirements, and operational costs grew, many physicians found it challenging to manage both clinical responsibilities and business operations. PPMCs offer a solution by taking over the administrative burdens, enabling physicians to concentrate on delivering quality care.
At their core, PPMCs are responsible for a wide range of non-medical services. These include billing and coding, human resources, payroll, marketing, compliance, information technology, and financial management. By centralizing these functions, PPMCs can achieve economies of scale, reduce overhead costs, and improve operational efficiency for the practices they manage. This model is particularly attractive to small and mid-sized practices that may lack the resources to manage these functions independently.
PPMCs typically enter into long-term management agreements with physician groups. In some cases, they may purchase the non-clinical assets of a practice—such as equipment, office space, and administrative staff—while the physicians retain control over clinical decisions and patient care. This arrangement allows for a clear division between medical and business responsibilities, which is essential for maintaining compliance with healthcare regulations like the Stark Law and the Anti-Kickback Statute.
***
***
One of the key advantages of working with a PPMC is access to capital and advanced infrastructure. PPMCs often invest in state-of-the-art electronic health record (EHR) systems, data analytics tools, and revenue cycle management platforms. These technologies can enhance patient care, streamline operations, and improve financial performance. Additionally, PPMCs may offer strategic guidance on practice expansion, mergers and acquisitions, and payer contract negotiations.
However, the relationship between physicians and PPMCs must be carefully managed. While PPMCs bring valuable expertise and resources, there is a risk that business priorities could overshadow clinical autonomy. To mitigate this, successful PPMCs prioritize physician engagement, transparent governance, and aligned incentives. They work collaboratively with physicians to ensure that business strategies support, rather than hinder, the delivery of high-quality care.
The physician practice management industry has evolved significantly over the past few decades. After a wave of failures in the 1990s due to overexpansion and misaligned incentives, modern PPMCs have adopted more sustainable and physician-centric models. Today, they play a crucial role in helping practices adapt to value-based care, population health management, and other emerging trends in healthcare delivery.
In conclusion, a physician practice management corporation serves as a strategic partner to medical practices, offering the business acumen and operational support needed to thrive in a complex healthcare environment. By offloading administrative tasks and providing access to advanced resources, PPMCs empower physicians to focus on what they do best—caring for patients—while ensuring the long-term success and sustainability of their practices.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Turning 65 is often seen as the gateway to retirement—a time to slow down, reflect, and enjoy the fruits of decades of labor. But for some, including doctors who may have faced financial setbacks, poor planning, or unexpected life events, reaching this milestone without financial security can be deeply unsettling. The image of a broke 65-year-old doctor may seem paradoxical, given the profession’s reputation for high earnings. Yet, reality paints a more nuanced picture. Fortunately, even in the face of financial hardship, retirement is not a closed door—it’s a challenge that can be met with creativity, resilience, and strategic planning.
Understanding the Situation
Before exploring solutions, it’s important to understand how a physician might arrive at retirement age without adequate savings. Medical school debt, late career starts, divorce, health issues, poor investment decisions, or supporting family members can all contribute. Some doctors work in lower-paying specialties or underserved areas, sacrificing income for impact. Others may have lived beyond their means, assuming their high salary would always be enough. Regardless of the cause, the key is to shift focus from regret to action.
Traditional retirement—ceasing work entirely—is not the only option. For a broke 65-year-old doctor, retirement may mean transitioning to a less demanding role, reducing hours, or shifting to a new field. The goal is to create a sustainable lifestyle that balances income, purpose, and well-being.
Leveraging Medical Expertise
Even if full-time clinical practice is no longer viable, a physician’s knowledge remains valuable. Here are several ways to continue earning while easing into retirement:
Telemedicine: Remote consultations are in high demand, especially in primary care, psychiatry, and chronic disease management. Telemedicine offers flexibility, reduced overhead, and the ability to work from home.
Locum Tenens: Temporary assignments can fill staffing gaps in hospitals and clinics. These roles often pay well and allow for travel or seasonal work.
Medical Writing and Reviewing: Physicians can write for journals, websites, or pharmaceutical companies. Peer reviewing, editing, and content creation are viable options.
Teaching and Mentoring: Medical schools, nursing programs, and residency programs need experienced educators. Adjunct teaching or mentoring can be fulfilling and financially helpful.
Consulting: Doctors can advise healthcare startups, legal teams, or insurance companies. Their insights are valuable in product development, litigation, and policy.
Exploring Non-Clinical Opportunities
Some physicians may wish to pivot entirely. Transferable skills—critical thinking, communication, leadership—open doors in other industries:
Health Coaching or Life Coaching: With certification, doctors can guide clients in wellness, stress management, or career transitions.
Entrepreneurship: Starting a small business, such as a tutoring service, online course, or specialty clinic, can generate income and autonomy.
Real Estate or Investing: With careful planning, investing in rental properties or learning about the stock market can create passive income.
Maximizing Government and Community Resources
At 65, individuals become eligible for Medicare, which can significantly reduce healthcare costs. Additionally, Social Security benefits may be available, depending on work history. While delaying benefits until age 70 increases monthly payments, some may need to claim earlier to meet immediate needs.
***
***
Other resources include:
Supplemental Security Income (SSI): For those with limited income and assets.
SNAP (food assistance) and LIHEAP (energy assistance): These programs help cover basic living expenses.
Community Organizations: Nonprofits and religious groups often provide support with housing, transportation, and social engagement.
Downsizing and Budgeting
Reducing expenses is a powerful way to stretch limited resources. Consider:
Relocating: Moving to a lower-cost area or state with favorable tax policies can reduce housing and living expenses.
Selling Assets: A large home, unused vehicle, or collectibles may be converted into cash.
Shared Housing: Living with family, roommates, or in co-housing communities can cut costs and reduce isolation.
Minimalist Living: Prioritizing needs over wants and embracing simplicity can lead to financial and emotional freedom.
Creating a realistic budget is essential. Track income and expenses, eliminate unnecessary costs, and prioritize essentials. Free budgeting tools and financial counseling services can help.
Financial stress can take a toll on mental health. It’s important to cultivate resilience and maintain a sense of purpose. Strategies include:
Staying Active: Physical activity improves mood and health. Walking, yoga, or swimming are low-cost options.
Volunteering: Giving back can provide structure, community, and fulfillment.
Learning New Skills: Online courses, hobbies, or certifications can reignite passion and open new doors.
Building a Support Network: Friends, family, and peer groups offer emotional support and practical advice.
Planning for the Future
Even at 65, it’s not too late to plan. Consider:
Debt Management: Negotiate payment plans, consolidate loans, or seek professional help.
Estate Planning: Create a will, designate healthcare proxies, and organize important documents.
Insurance Review: Ensure adequate coverage for health, life, and long-term care.
Financial Advising: A fee-only advisor can help create a sustainable plan without selling products.
Embracing a New Chapter
Retirement is not a destination—it’s a transition. For a broke 65-year-old doctor, it may not look like the glossy brochures, but it can still be rich in meaning. By leveraging experience, reducing expenses, accessing resources, and nurturing well-being, retirement becomes a journey of reinvention.In many ways, doctors are uniquely equipped for this challenge. They’ve faced long hours, high stakes, and complex problems. That same grit and adaptability can guide them through financial hardship and into a fulfilling retirement.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Population health and public health are two interrelated disciplines that strive to enhance the health outcomes of communities. While they share a common mission—to reduce health disparities and promote wellness—their approaches, target populations, and operational frameworks differ significantly.
***
***
Public health is traditionally defined as the science and art of preventing disease, prolonging life, and promoting health through organized efforts and informed choices of society, organizations, public and private sectors, communities, and individuals. It focuses on the health of the general population and emphasizes broad interventions such as vaccination programs, sanitation, health education, and policy advocacy. Public health professionals often work in government agencies, nonprofit organizations, and academic institutions to implement community-wide initiatives that prevent disease and promote healthy behaviors.
***
***
In contrast, population health takes a more targeted approach. It refers to the health outcomes of a specific group of individuals, including the distribution of such outcomes within the group. This field is particularly concerned with the social determinants of health—factors like income, education, environment, and access to care—that influence health disparities. Population health strategies often involve data-driven interventions tailored to the needs of defined groups, such as rural communities, ethnic minorities, or patients with chronic conditions.
One key distinction lies in scope and granularity. Public health initiatives are typically designed for the entire population, aiming to create systemic change. For example, anti-smoking campaigns or water fluoridation programs benefit everyone regardless of individual risk. Population health, however, might focus on reducing diabetes rates among Hispanic adults in a specific urban area, using targeted outreach and culturally sensitive care models.
Another difference is in data utilization. Population health relies heavily on health informatics and analytics to identify trends, allocate resources, and evaluate outcomes. This evidence-based approach supports precision in addressing health inequities. Public health also uses data, but often at a broader level to guide policy and monitor general health indicators like life expectancy or disease prevalence.
Despite these differences, the two fields are complementary. Public health lays the foundation for healthy societies through preventive infrastructure, while population health builds on this by addressing nuanced needs within subgroups. Together, they form a holistic framework for improving health outcomes across diverse communities.
In today’s healthcare landscape, the integration of public and population health is increasingly vital. The COVID-19 pandemic underscored the importance of both approaches: public health measures like mask mandates and vaccination campaigns were essential, while population health efforts ensured vulnerable groups received targeted support.
In conclusion, while public health and population health differ in focus and methodology, they are united by a shared goal: to foster healthier communities. Understanding their distinctions enables more effective collaboration and innovation in health policy, care delivery, and community engagement.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Investing may seem complicated, but today there are many ways for the newly minted physician [MD, DO, DPM, DMD or DDS] to begin, even with minimal knowledge and only a small amount to invest. Starting as soon as possible will help you get closer to the retirement you deserve.
***
Why is investing important?
Investing often feels like a luxury reserved for the already wealthy physician. Many of us find it difficult to think about investing for the future when there are so many things we need that money for right now; medical school loans, auto, home and children; etc. But, at some point, we’re going to want to stop working and enjoy retirement. And simply put, retirement is expensive.
Most calculations advise that you aim for enough savings to give you 70% to 80% of your pre-retirement income for 20 years or more. Depending on your goals for retirement, that means you could need between $500,000 and $1 million in savings by the time you retire. That may not sound attainable, but with the power of compounding growth, it’s not as hard to achieve as you think. The key is starting as soon as possible and making smart choices.
The short answer is “now,” no matter what your age. Due to the way the gains in investments can compound, the earlier you start the better. Money invested in your 20s could very easily grow over 20 times before you retire, without you having to do much.That is powerful. Even if you’re in your 50s or older, you can still make significant progress toward meeting your goals in retirement.
How much should you invest per month?
Most financial experts say you should invest 10% to 15% of your annual income for retirement. That’s the goal, but you don’t have to get there immediately. Whatever you can start investing today is going to help you down the road.
So, if 10% to 15% is too much right now, start small and build toward that goal over time. You can actually start investing with $5 if you want. And you should. Some investment products require a minimum investment, but there are plenty that don’t, and a lot of online brokerage accounts can be started for free.
The best investments for you are going to depend on your age, goals, and strategy. The important thing is to get started. You’ll learn as you go. If you have questions, a dedicated DIYer or investment advisor can help give you the guidance and options you need.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on October 20, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Understanding the Differences Between Microeconomics and Macroeconomics
Economics is the study of how societies allocate scarce resources to meet the needs and wants of individuals. It is broadly divided into two main branches: microeconomics and macroeconomics. While both aim to understand economic behavior and decision-making, they differ significantly in scope, focus, and application. Understanding these differences is essential for grasping how economies function at both individual and national levels.
Microeconomics focuses on the behavior of individual economic agents—such as consumers, firms, and households—and how they make decisions regarding resource allocation. It examines how these entities interact in specific markets, how prices are determined, and how supply and demand influence economic outcomes.
Key concepts in microeconomics include:
Demand and Supply: Microeconomics analyzes how the quantity of goods demanded by consumers and the quantity supplied by producers interact to determine market prices.
Elasticity: This measures how responsive demand or supply is to changes in price or income.
Consumer Behavior: Microeconomics studies how individuals make choices based on preferences, budget constraints, and utility maximization.
Production and Costs: It explores how firms decide on the optimal level of output and the costs associated with production.
Market Structures: Microeconomics categorizes markets into perfect competition, monopolistic competition, oligopoly, and monopoly, each with distinct characteristics and implications for pricing and output.
Microeconomic analysis is crucial for understanding how specific sectors operate, how businesses strategize, and how consumers respond to changes in prices or income. For example, a company might use microeconomic principles to determine the price point that maximizes profit or to assess the impact of a new competitor entering the market.
Macroeconomics: The Study of the Economy as a Whole
Macroeconomics, on the other hand, deals with the performance, structure, and behavior of an entire economy. It looks at aggregate indicators and phenomena, such as national income, unemployment, inflation, and economic growth. Macroeconomics seeks to understand how the economy functions at a broad level and how government policies can influence economic outcomes.
Key areas of macroeconomics include:
Gross Domestic Product (GDP): This measures the total value of goods and services produced within a country and serves as a key indicator of economic health.
Unemployment: Macroeconomics examines the causes and consequences of unemployment and the effectiveness of policies aimed at reducing it.
Inflation and Deflation: It studies changes in the general price level and their impact on purchasing power and economic stability.
Fiscal and Monetary Policy: Macroeconomics evaluates how government spending, taxation, and central bank actions influence economic activity.
International Trade and Finance: It explores exchange rates, trade balances, and the impact of globalization on national economies.
Macroeconomic analysis is essential for policymakers, economists, and financial institutions. For instance, central banks use macroeconomic data to set interest rates, while governments design fiscal policies to stimulate growth or curb inflation.
Despite their differences, microeconomics and macroeconomics are deeply interconnected. Micro-level decisions collectively shape macroeconomic outcomes. For example, widespread consumer spending boosts aggregate demand, influencing GDP and employment levels. Conversely, macroeconomic conditions—such as inflation or interest rates—affect individual behavior. A rise in interest rates may discourage borrowing and reduce consumer spending, impacting businesses at the micro level.
Economists often use insights from both branches to develop comprehensive models and forecasts. For instance, understanding consumer behavior (micro) helps predict changes in aggregate consumption (macro), which in turn informs policy decisions.
Microeconomics and macroeconomics offer distinct yet complementary perspectives on economic activity. Microeconomics provides a granular view of individual decision-making and market dynamics, while macroeconomics offers a broader understanding of national and global economic trends. Together, they form the foundation of economic theory and practice, guiding businesses, governments, and individuals in making informed decisions.
A well-rounded grasp of both branches is essential for anyone seeking to understand how economies function and evolve in an increasingly complex world.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The following are 4 common financial psychological biases. Some are learned while others are genetically determined (and often socially reinforced). While this essay focuses on the financial and investing implications of these biases, they are prevalent in most areas in life.
Loss aversion affected many investors during the stock market crash of 2007-08 or the flash crash of May 6, 2010 also known as the crash of 2:45. During the crash, many people decided they couldn’t afford to lose more and sold their investments.
Of course, this caused the investors to sell at market troughs and miss the quick, dramatic recovery.
Overconfident investing happens when we believe we can out-smart other investors via market timing or through quick, frequent trading.
Data convincingly shows that people who trade most often under-perform the market by a significant margin over time.
Mental accounting takes place when we assign different values to money depending on where we got it.
For instance, even though we may have an aggressive saving goal for the year, it is likely easier for us to save money that we worked for than money that was given to us as a gift.
Herd mentality makes it very hard for humans to not take action when everyone around us does.
For example, we may hear stories of people making significant profits buying, fixing up, and flipping homes and have the desire to get in on the action, even though we have no experience in real estate.
Posted on October 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
A paradox is a logically self-contradictory statement or a statement that runs contrary to one’s expectation. It is a statement that, despite apparently valid reasoning from true or apparently true premises, leads to a seemingly self-contradictory or a logically unacceptable conclusion. A paradox usually involves contradictory-yet-interrelated elements that exist simultaneously and persist over time. They result in “persistent contradiction between interdependent elements” leading to a lasting “unity of opposites”.
THE TELE-MEDICINE PARADOX
Classic Definition: Refers specifically to the treatment of various medical conditions without seeing the patient in person. Healthcare providers may use electronic and internet platforms like live video, audio, PCs, tablets, or instant messaging to address a patient’s concerns and diagnose their condition remotely.
Modern Circumstance: This may include giving medical advice, walking them through at-home exercises, or recommending them to a local provider or facility. Even more exciting is the emergence of telemedicine apps which give patients access to care right from their phones or computer screens.
Paradox Examples: Treating certain conditions remotely can be challenging. Tele-medicine is often used to treat common illnesses, manage chronic conditions, or provide specialist services. If a patient is dealing with an emergent or serious condition, the remote provider suggests they seek in-person medical care.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on October 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Can a physician medical provider charge an office cancellation fee?
According to the American Medical Association’s Code of Medical Ethics, physicians can charge fees for “missed appointments or appointments not cancelled in advance in keeping with the published policy of the practice”, and they should “clearly notify patients in advance of fees charge” (Opinion 11.3. 2) [28].
And so, if you miss a doctor’s appointment these days, you could get hit with a “no-show” fee of up to $150 — or more for some specialties.
Is it legal for an insurance company to charge a cancellation fee?
These practices are typically legal. They help businesses ensure they can recoup the lost revenue due to no-shows or last-minute cancellations.
Cancellation fees are permitted, but seldom collected absent unusual circumstances, such as a great deal of work having been provided.
QUESTION: As a doctor [MD, DO, DPM or DDS], do you charge an office cancellation fee? If so, how much is it?
Why It Is Difficult to Practice Medicine Part-Time Today?
In the past, part-time medical practice offered physicians a flexible way to balance professional responsibilities with personal or family commitments. Today, however, the healthcare environment has evolved in ways that make part-time medicine increasingly challenging. From administrative burdens to economic pressures and patient expectations, the obstacles are both systemic and personal.
One of the most significant barriers is the rise in administrative complexity. Physicians are now required to navigate electronic health records (EHRs), comply with insurance documentation, and meet regulatory standards such as HIPAA and MACRA. These tasks consume hours of non-clinical time, which is difficult to compress into a part-time schedule. Even seeing fewer patients doesn’t exempt part-time doctors from the same documentation and compliance requirements as their full-time counterparts.
***
***
Another challenge is financial viability. Many physicians are paid based on productivity metrics, such as Relative Value Units (RVUs), which reward volume over quality. Part-time practitioners often struggle to meet these benchmarks, resulting in lower compensation and reduced benefits. Additionally, malpractice insurance premiums and licensing fees remain fixed regardless of hours worked, further eroding the financial appeal of part-time practice.
Continuity of care is also a concern. Patients increasingly expect immediate access to their providers, especially in primary care and specialties like psychiatry or pediatrics. Part-time physicians may not be available for urgent issues, leading to fragmented care and dissatisfaction. This can strain relationships with patients and colleagues who must cover gaps in availability.
From a professional standpoint, part-time physicians may face limited career advancement. Leadership roles, academic appointments, and research opportunities often favor full-time commitment. There’s also a perception—sometimes unfair—that part-time doctors are less dedicated or less competent, which can affect peer respect and influence within medical institutions.
Technology, while beneficial, adds another layer of complexity. Telemedicine, remote monitoring, and digital communication tools have expanded access but also increased the expectation for constant availability. Part-time physicians may find it difficult to manage asynchronous messages, follow-ups, and virtual visits without extending their work hours beyond what they intended.
***
***
Lastly, burnout and work-life balance—ironically one of the reasons doctors seek part-time roles—can still be elusive. The pressure to maintain clinical excellence, stay updated with medical advancements, and meet patient needs doesn’t diminish with reduced hours. In fact, squeezing these responsibilities into fewer days can intensify stress rather than alleviate it.
In conclusion, while part-time medical practice may seem like a solution to modern work-life challenges, the reality is far more complex. The structure of today’s healthcare system, combined with economic, technological, and cultural pressures, makes it difficult for physicians to thrive in part-time roles. Addressing these challenges will require systemic reform, flexible compensation models, and a cultural shift in how we value and support diverse medical careers.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
A Market Maker exists to “create a market” for specific company securities by being willing to buy and sell those securities at a specified displayed price and quantity to broker-dealer firms that are members of the exchange.
These firms help keep financial markets liquid by making it easier for investors to buy and sell securities–they ensure that there is always someone to buy and sell to at the time of trade.
The S&P 500, short for the Standard & Poor’s 500 Index, is one of the most widely followed stock market indices in the world. It tracks the performance of 500 of the largest publicly traded companies in the United States, offering a broad snapshot of the overall health and direction of the U.S. economy. Created in 1957 by the financial services company Standard & Poor’s, the index has become a benchmark for investors, analysts, and economists alike.
Composition and Criteria The S&P 500 includes companies from a wide range of industries, such as technology, healthcare, finance, energy, and consumer goods. To be included in the index, a company must meet specific criteria: it must be based in the U.S., have a market capitalization of at least $14.5 billion (as of 2025), be highly liquid, and have a public float of at least 50% of its shares. Additionally, the company must have positive earnings in the most recent quarter and over the sum of its most recent four quarters.
Some of the most recognizable names in the S&P 500 include Apple, Microsoft, Amazon, Johnson & Johnson, JPMorgan Chase, and ExxonMobil. These companies are selected by a committee that reviews eligibility and ensures the index remains representative of the broader market.
How It Works The S&P 500 is a market-capitalization-weighted index, meaning that companies with larger market values have a greater influence on the index’s performance. For example, a significant movement in Apple’s stock price will affect the index more than a similar movement in a smaller company’s stock. This weighting system helps reflect the real impact of large corporations on the economy.
The index is updated in real time during trading hours and is used by investors to gauge market trends. It also serves as the basis for many investment products, such as mutual funds and exchange-traded funds (ETFs), which aim to replicate its performance.
Why It Matters The S&P 500 is considered a leading indicator of U.S. equity markets and the economy as a whole. When the index rises, it often signals investor confidence and economic growth. Conversely, a decline may indicate uncertainty or economic slowdown. Because it includes companies from diverse sectors, the S&P 500 provides a more balanced view than narrower indices like the Dow Jones Industrial Average, which only tracks 30 companies.
Investment and Strategy Many investors use the S&P 500 as a benchmark to measure the performance of their portfolios. Passive investment strategies, such as index funds, aim to match the returns of the S&P 500 rather than beat it. This approach has gained popularity due to its low fees and consistent long-term performance.
In summary, the S&P 500 is more than just a number—it’s a powerful tool that reflects the pulse of the American economy. By tracking the performance of 500 major companies, it offers insights into market trends, investor sentiment, and economic health. Whether you’re a seasoned investor or just starting out, understanding the S&P 500 is essential to navigating the world of finance.
Investment fees still matter for physicians and all of us, despite dropping dramatically over the past several decades due to computer automation, algorithms and artificial intelligence, etc. And, they can make a big difference to your financial health. So, before buying any investment thru a financial advisor, planner, manager, stock broker, etc., it’s vital to understand these two often confusing costs.
***
***
Fee Only: Paid directly by clients for their services and can’t receive other sources of compensation, such as payments from fund providers. Act as a fiduciary, meaning they are obligated to put their clients’ interests first
Fee Based: Paid by clients but also via other sources, such as commissions from financial products that clients purchase. Brokers and dealers (registered representatives) are simply required to sell products that are “suitable” for their clients. Not a fiduciary.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Critical thinking allows a Financial Advisor [FA] to analyze information and make an objective judgment. By impartially evaluating the facts related to a matter, Financial Planners [FPs] can draw realistic conclusions that will help make a sound decision. The ability of being able to properly analyze a situation and come up with a logical and reasonable conclusion is highly valued by employers, as well as current and potential clients.
Now, according to Indeed, we present the six main critical thinking and examples that will help you evaluate your own thought process as a FA, FP or Wealth Manager, etc.
What is critical thinking?
Critical thinking is the ability to objectively analyze information and draw a rational conclusion. It involves gathering information on a subject and determining which pieces of information apply to the subject and which don’t, based on deductive reasoning. The ability to think critically helps people in both their personal and professional lives and is valued by most clients and employers.
Why do employers value critical thinking?
Critical thinking skills are a valuable asset for an employee, as employers, brokerages and Registered Investment Advisors [RIAs] typically appreciate candidates who can correctly assess a situation and come up with a logical resolution. Time is a valuable resource for most managers, and an employee able to make correct decisions without supervision will save both that manager and the whole company much valuable time.
***
***
Six main types of critical thinking skills
There are six main critical thinking skills you can develop to successfully analyze facts and situations and come up with logical conclusions:
1. Analytical thinking
Being able to properly analyze information is the most important aspect of critical thinking. This implies gathering information and interpreting it, but also skeptically evaluating data. When researching a work topic, analytical thinking helps you separate the information that applies to your situation from that which doesn’t.
2. Good communication
Whether you are gathering information or convincing others that your conclusions are correct, good communication is crucial in the process. Asking people to share their ideas and information with you and showing your critical thinking can help step further towards success. If you’re making a work-related decision, proper communication with your coworkers can help you gather the information you need to make the right choice.
3. Creative thinking
Being able to discover certain patterns of information and make abstract connections between seemingly unrelated data helps improve your critical thinking. When analyzing a work procedure or process, you can creatively come up with ways to make it faster and more efficient. Creativity is a skill that can be strengthened over time and is valuable in every position, experience level and industry.
4. Open-mindedness
Previous education and life experiences leave their mark on a person’s ability to objectively evaluate certain situations. By acknowledging these biases, you can improve your critical thinking and overall decision process. For example, if you plan to conduct a meeting in a certain way and your firm suggests using a different strategy, you should let them speak and adjust your approach based on their input.
5. Ability to solve problems
The ability to correctly analyze a problem and work on implementing a solution is another valuable skill.
6. Asking thoughtful questions:
In both private and professional situations, asking the right questions is a crucial step in formulating correct conclusions. Questions can be categorized in various forms as mentioned below:
***
***
* Open-ended questions
Asking open-ended questions can help the person you’re communicating with provide you with relevant and necessary information. These are questions that don’t allow a simple “yes” or “no” as an answer, requiring the respondent to elaborate on the answer.
* Outcome-based questions
When you feel like another person’s experience and skills could help you work more effectively, consider asking outcome-based questions. Asking someone how they would act in a certain hypothetical situation, such as a stock market correction, can give you an insight into their perspective, helping you see things you hadn’t thought about before.
Reflective questions
You can gain insight by asking a client to reflect and evaluate an experience and explain their thought processes during that time. This can help you develop your critical thinking by providing you real-world examples.
* Structural questions
An easy way to understand something is to ask how something works. Any working system results from a long process of trial and error, and properly understanding the steps that needed to be taken for a positive result could help you be more efficient in your own endeavors.
CONCLUSION
Critical thinking is like a muscle that can be exercised and built over time. It is a skill that can help propel your career to new heights. You’ll be able to solve workplace issues, use trial and error to troubleshoot ideas, and more.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
The Dow Jones Industrial Average (DJIA), often referred to simply as “the Dow,” is one of the oldest and most well-known stock market indices in the world. It was created in 1896 by Charles Dow, the co-founder of The Wall Street Journal, and is designed to represent the performance of the broader U.S. stock market, specifically focusing on 30 large, publicly traded companies. These companies are considered leaders in their respective industries and serve as a barometer for the overall health of the U.S. economy.
The Composition of the DJIA
The DJIA includes 30 companies, which are selected by the editors of The Wall Street Journal based on various factors such as market influence, reputation, and the stability of the company. These companies represent a wide array of sectors, including technology, finance, healthcare, consumer goods, and energy. Notably, the companies chosen for the DJIA are not necessarily the largest companies in the U.S. by market capitalization, but rather those that are most indicative of the broader economy. Some of the prominent companies listed in the DJIA include names like Apple, Microsoft, Coca-Cola, and Johnson & Johnson.
However, the list of 30 companies is not static. Over time, companies may be added or removed to reflect changes in the economic landscape. For example, if a company experiences significant decline or no longer represents a leading sector, it might be replaced with another company that better reflects modern economic trends. This periodic reshuffling ensures that the DJIA continues to be a relevant measure of economic activity.
How the DJIA is Calculated
The DJIA is a price-weighted index, which means that the value of the index is determined by the share price of the component companies, rather than their market capitalization. To calculate the DJIA, the sum of the stock prices of all 30 companies is divided by a special divisor. This divisor adjusts for stock splits, dividends, and other corporate actions to maintain the integrity of the index over time. The price-weighted method means that higher-priced stocks have a greater impact on the movement of the index, regardless of the overall size or economic weight of the company.
For instance, if a company with a higher stock price like Apple experiences a significant change in value, it will influence the DJIA more than a company with a lower stock price, even if the latter has a larger market capitalization. This makes the DJIA somewhat different from other indices, like the S&P 500, which is weighted by market cap and gives more weight to larger companies in terms of their economic impact.
Significance of the DJIA
The DJIA is widely regarded as a barometer of the U.S. stock market’s performance. Investors and analysts closely monitor the movements of the Dow to gauge the overall health of the economy. When the DJIA rises, it generally suggests that investors are optimistic about the economic outlook and that large companies are performing well. Conversely, when the DJIA falls, it often signals economic uncertainty or a downturn in market conditions.
Despite being a narrow index, with only 30 companies, the DJIA holds substantial sway in financial markets. It is widely covered in the media and is often cited in discussions about the state of the economy. In fact, the performance of the DJIA is considered a key indicator of investor sentiment and economic confidence.
However, the DJIA has its limitations. Since it only includes 30 companies, it does not necessarily represent the broader market or capture the performance of smaller companies. Other indices, like the S&P 500, which includes 500 companies, offer a more comprehensive view of the market’s performance.
Conclusion
The Dow Jones Industrial Average is a key metric for understanding the state of the U.S. economy and the stock market. Although it has evolved over the years, it continues to provide valuable insights into the performance of large, influential companies. While it is not a perfect reflection of the market as a whole, the DJIA remains one of the most important and widely recognized indices in global finance. Through its historical significance and its role in shaping market sentiment, the Dow has cemented its place as a cornerstone of financial analysis.
A hedge fund is a limited partnership of private investors whose money is pooled and managed by professional fund managers. These managers use a wide range of strategies, including leverage (borrowed money) and the trading of nontraditional assets, to earn above-average investment returns. A hedge fund investment is often considered a risky, alternative investment choice and usually requires a high minimum investment or net worth. Hedge funds typically target wealthy investors.
The hedge fund manager I am considering also runs an offshore fund under a “master feeder” arrangement.
A PHYSICIAN’S QUESTION:What does this mean? In which fund should I invest?
The master feeder arrangement is a two-tiered investment structure whereby investors invest in the feeder fund. The feeder fund in turn invests in the master fund. The master fund is therefore the one that is actually investing in securities. There may be multiple feeder funds under one master fund. Feeder funds under the same master can differ drastically in terms of fees charged, minimums required, types of investors, and many other features – but the investment style will be the same because only the master actually invests in the market.
A master feeder structure is a very popular arrangement because it allows a portfolio manager to pool both onshore and offshore assets into one investment vehicle (the master fund) that allocates gains and losses in an asset-based, proportional manner back to the onshore and offshore investors. All investors, both offshore and onshore, get the same return. In this manner, the portfolio manager, despite offering more than one fund with different characteristics to different populations, is not faced with the dilemma of which fund to favor with the best investment ideas.
A manager may offer an offshore fund because there is demand for that manager’s skill either abroad, where investors may wish to preserve anonymity, or more commonly where investors simply do not wish to become entangled with the United States tax code. American citizens should generally avoid the offshore fund, since American citizens are taxed on their allocated share of offshore corporation profits whether or not a distribution occurs. Therefore, there is no benefit for most American taxpayers investing in an offshore fund.
Tax-exempt institutions, such as medical foundations, in the United States may have reason to consider an offshore hedge fund, however. Domestic tax-exempt organizations are generally not subject to unrelated business taxable income (UBTI) – the portion of hedge fund income that comes about as a result of the use of leverage – when investing with an offshore corporation. If the same tax-exempt organization were to invest in a domestic fund, and if UBTI was generated, then the organization would have to pay taxes on that UBTI. Most domestic hedge funds generate UBTI.
After a lifetime of hard work practicing medicine and saving, you’re at the retirement finish line. Instead of a paycheck, you’re relying on your nest egg and investment income to cover the bills. Picking the right investments is even more important, as you won’t have much chance to recover as a retired MD, DO, DPM or DDS.
“You made it to the top of the mountain through a systematic approach and are trying to make your way down safely,” says retirement planner John Gillet John Gillet in Hollywood, Fla. “Why throw all caution to the wind and try something different now?”
***
***
Definitions
An annuity is an insurance contract designed to grow your money and then repay it as income. There are different versions. An immediate annuity turns your lump sum into future guaranteed income payments, like your own personal pension. They are simple to understand with no or small fees.
Fixed annuities pay a guaranteed interest rate over a set period to grow your money, like 5% a year for five years. These options could make sense as part of a retirement plan.
A variable annuity, on the other hand, invests your savings in mutual funds. While you can buy riders that guarantee a minimum income, you’ll be paying very much for it. “All in, the annual fees can be 3% or more of your balance,” says Jeff Bailey, an advisor from Nashville. “That’s a huge withdrawal rate from your portfolio versus investing on your own.”
The variable annuity will lock up your money for years. If you cancel early, you owe a surrender charge that could start at 7% or more of your annuity balance before gradually going down as time goes by. “Clients believe they can walk away with their contract value, but that’s often not true,” says Bailey.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Sometimes debt is a necessary tool in building wealth
Using debt to build wealth might seem counterintuitive. After all, when you calculate your wealth, you look at what you own (assets) and subtract what you owe (debts and liabilities) to determine what your net worth (wealth) is.
It’s easy to oversimplify that debt is bad and is harmful to your wealth. Because some debt is really harmful, like credit cards, automobile, debt gets lumped into the category of “bad.”
But some types of debt can be useful and sometimes necessary to create wealth; home, education, business, etc. For folks that don’t readily have access to large sums of cash or capital, debt may be the tool that allows them to expand.
Yourmedical practice. Your personal goals. Your financial plan. Our experienced confirmation guide.
***
***
When you know exactly where you are today, have a vision of where you want to be tomorrow, and have trusted counsel at your side, you have already achieved so much success. Marcinko Associates works to keep you at that level of confidence every day. We use a comprehensive economic process to uncover what’s most important to you and then develop a financial strategy that gives you the highest probability of achieving your monetary goals.
We assess, plan, and opine for your success
To accurately see where you are today, chart a strategic path to your goals and help you make the most informed decisions to keep you on financial track, our key services for physicians and high net worth medical clients include:
Investment Portfolio Review
Fee, Charge and Cost Review
Comprehensive Financial Planning
Insurance Reviews
Estate Planning
Investment and Asset Management Second Opinions
We take a deep dive into your financial retirement plans
Physicians and dental employers now have options for how to design and deliver retirement benefits and we can help you make the best choice for your healthcare business. Our services for retirement plans include:
Fee, Charges & Fiduciary Review
Portfolio Analysis
Single Employer Retirement Plan Advisory
Retirement Plans Risk Analysis
Capital Funding and Financing
Business Planning and Practice Valuations
Career Development
and more!
We take a broad and balanced look at your financial life life
We coordinate our recommendations with your other advisors, including attorneys, accountants, insurance professionals and others, to ensure each decision is consistent with your goals and overall strategy. For example, through our partnerships we offer physician colleagues deeper expanded advisory services, like:
Hobson’s choice is a free choice in which only one thing is actually offered. The term is often used to describe an illusion that choices are available. The best known example is “I’ll give you a choice: Take it or leave it”, wherein “leaving it” is strongly undesirable.
The phrase is said to have originated with Thomas Hobson (1544–1631), a livery stable owner in Cambridge, England, who offered customers the choice of either taking the horse in the stall nearest to the door or taking none at all.
A CASE MODEL
Half of Physicians Plan to Change Career Paths
The Physicians Foundation recently conducted a survey on physician practice patterns and perspectives. Here are some key findings from the report:
• 31% of physicians identify as independent practice owners or partners. • Almost half (47%) of physicians plan to change career paths. • 78% of physicians sometimes, often or always experience feelings of burnout. • Nearly a quarter of physician time is spent on non-clinical paperwork.
This result is not a good Hobson’s Choice in Medicine.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Public Relations [PR] is differentiated than advertising in that an advertiser pays for and has control over the message. It differs from personal selling in that the message is non-personal, i.e., not directed to a particular individual patient. We pay for advertising but pray for public relations. Public relations are not controllable but it is free; advertising is not free. PR suggests that “good news or bad news”; just spell the doctors name correctly
Change Management is the discipline that guides how we prepare, equip and support individuals to successfully adopt to change in order to drive organizational success and outcomes.
For example, a senior doctor may retire, become ill, or a junior associate might become a practice partner. How will patients be affected?
Crisis Management is the precautions and identification of threats to an organization and its stakeholders, and the methods used by the organization to deal with these threats.
For example, recall in 1982, that Tylenol™ commanded 35 percent of the over-the-counter analgesic market in America and it represented nearly 17 percent of Johnson & Johnson’s profits. But, when seven people died from consuming the tainted drug, a national panic ensued. Moreover, Americans started to question the safety of all over-the-counter medications.
Fortunately, J&J commenced the proto-typical positive crisis response in the following way:
J&J acted quickly, with complete candidness about what happened and within hours of learning of the deaths, J&J installed toll-free numbers for consumers, sent alerts to healthcare providers nationwide, and stopped advertising the product. J&J recalled 31 million bottles of Tylenol™ capsules and offered replacement products free of charge. J&J did not wait for evidence to see whether the contamination might be more widespread.
J&J’s leadership was in the lead and seemed in full control throughout the crisis. The chairman was admired for his leadership to pull Tylenol™ capsules off the market and his forthrightness in dealing with the media. The Tylenol™ crisis led the news every night on every station for six weeks.
J&J placed consumers first. J&J spent more than $100 million for the recall and re-launch of Tylenol™. The stock which had been trading near a 52-week high just before the tragedy, dropped for a time, but recovered to its highs only two months later.
J&J accepted responsibility. The disaster could have been described in many different ways: as an assault on the company, as a problem somewhere in the process of getting Tylenol™ from J&J factories to retail stores, or as the acts of a crazed criminal. Yet, the company accepted full responsibility.
J&J sought to ensure that measures were taken to prevent a recurrence of the problem. J&J introduced tamper-proof packaging that would make it much more difficult for a similar incident to occur in the future.
J&J presented itself prepared to handle the short-term damage in the name of consumer safety. Within a year of the disaster, J&J’s share of the analgesic market, which had fallen to 7 percent from 37 percent following the poisoning, had climbed back to 30 percent.
This wildly successful response in now the stuff of graduate and business school case models for excellence in teaching!
PRM stands for Patient Relationship Management, which is a system for managing all interactions with current and potential patients, families, friends, referring physicians, clinics and hospitals. The goal is simple: improve relationships to grow your medical practice. PRM technology helps medical practices and clinics stay connected to patients, streamline processes, and improve profitability.
When people talk about PRM, they’re usually referring to a PRM system: software that helps track each interaction with a patient or elated others. That can include practice sales calls, treatment or service plans, marketing e-mails, website, social media and more. PRM tools can unify patient and practice data from many sources and even use Artificial Intelligence [AI] to help better manage relationships across the entire doctor– patient lifecycle – spanning departments described elsewhere in the Marketing, Advertising and Sales ME-Ps.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
References:
1. Purcarea, Victor: The impact of marketing strategies in healthcare systems. J. Med Life. 2019 Apr-Jun;12(2):93–96. doi: 10.25122/jml-2019-1003
READINGS:
Marcinko, DE and Hetico, HR: The Business of Medical Practice [3rd Edition]. Springer Publishing, New York, 2010.
Marcinko, DE and Hetico, HR: Hospitals & Healthcare Organizations [Management Strategies, Operational Techniques, Tools, Templates and Case Studies]. Productivity Press, New York, 2012.
Marcinko, DE and Hetico, HR: Financial Management Strategies for Hospitals and Healthcare Organizations [Tools, Techniques, Checklists and Case Studies]. Productivity Press, New York, 2012.
An app, which is short for “application,” is a type of software that can be installed and run on a computer, tablet, smartphone or other electronic devices. An app most frequently refers to a mobile application or a piece of software that is installed and used on a computer. Most apps have a specific and narrow function.
An easy and fairly cheap way for novices to get into investing is to use a robo-advisor. Basically, the funds you contribute will be invested by an algorithm based upon your goals, which are usually determined by taking a survey. This helps keep fees low; the algorithm doesn’t rely on a human expert to make trades, and you don’t have to spend significant amounts of time researching your investments. While this is a good way to start, it may not be the best option in the long run.
Online Brokerage or Investment Apps
More options are becoming available all the time, and they have opened trading to a much larger percentage of the population. That is a great thing, but it’s important to remember that “easier to invest” doesn’t necessarily mean it’s easy to invest well.
Be wary of apps that “gamify” trading and encourage risky choices. Keep in mind that trusted names offer more security, so do your research when you are selecting a platform.