BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on May 5, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITION
By Staff Reporters
***
***
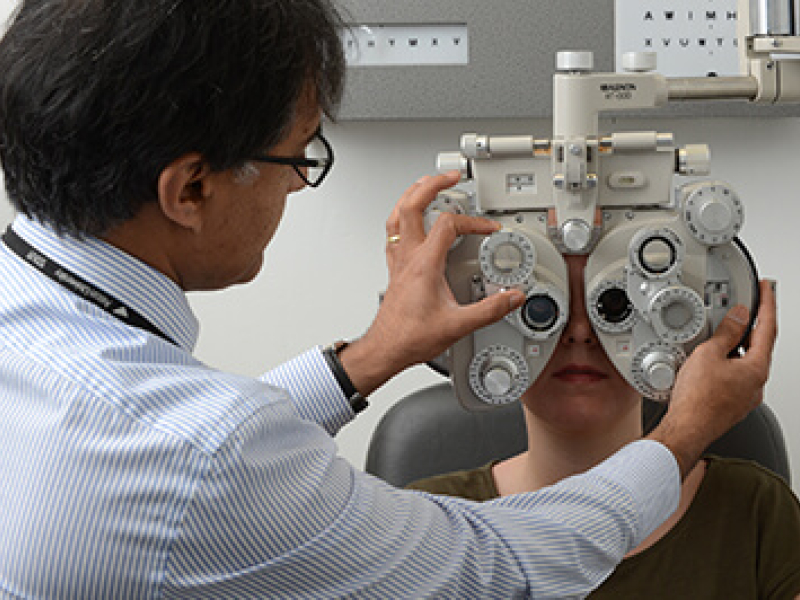
Classic: Despite a wide variety of empirical methods and data sources, the demand for health care is consistently found to be price inelastic
Modern: If you are sick, you will not be very price sensitive. There are exceptions to this rule (e.g., elective surgery such as plastic surgery, purchases of eyeglasses) but most studies find that patients are fairly insensitive to changes in health care prices.
Examples: For instance, the RAND Health Insurance Experiment found that the price elasticity of medical expenditures is -0.2.
***
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Posted on May 4, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants LLC
***
***
During the first 90 days of the Republican Party’s government trifecta (controlling the White House, Senate, and House of Representatives), both the Trump Administration and Congress have laid the groundwork for seismic change to the U.S. healthcare industry.
In an attempt to track the latest actions of the federal government’s legislative and executive branches affecting the healthcare industry since the first installment in our February issue, this Health Capital Topics article summarizes recent events in Washington and the impact of these changes on providers and patients. (Read more…)
An emergency medicine physician is a medical doctor who specializes in the diagnosis, treatment, and management of acute and life-threatening medical conditions that require immediate intervention. These physicians work in hospital emergency departments, urgent care centers, and other acute care settings, where they provide rapid assessment, stabilization, and treatment to patients of all ages with a wide range of medical emergencies.
Emergency medicine physicians are trained to handle diverse medical emergencies, including trauma, cardiac emergencies, respiratory distress, severe infections, neurological emergencies, and obstetric emergencies, among others. They play a vital role in the front line management of medical emergencies, ensuring that patients receive prompt and appropriate care to improve outcomes and save lives.
***
Classic: Emergent Room or Emergency Department care is the provision of immediate medical service offering outpatient care for the treatment of acute and chronic illness and injury. It requires a broad and comprehensive fund of knowledge to provide such care. Excellence in care for patients with complex and or unusual conditions is founded on the close communication and collaboration between the urgent care medicine physician, the specialists and the primary physicians.
Modern: Urgent care does not replace your primary care physician. An urgent care center is a convenient option when someone’s regular physician is on vacation or unable to offer a timely appointment. Or, when illness strikes outside of regular office hours, urgent care offers an alternative to waiting for hours in a hospital Emergency Room.
Examples: Chest pain, bleeding that cannot be stopped and loss of consciousness; etc.
***
***
SOME ER DOCTORS WORK FOR FREE
The new president of emergency medicine for the Alberta Medical Association says Emergency Room physicians already coping with long hours, staff shortages and jammed waiting rooms are also being obligated, in some cases, to work for free. Dr. Warren Thirsk says the government has yet to follow through on a promise to reimburse emergency room doctors for so-called “good faith” payments.
“There’s been lots of excuses, but the bottom line is no one has actually received a penny for those suspended good-faith payments,” Thirsk said in an interview. “On average, every emergency physician in this province is out thousands of dollars for free work.” Good-faith payments reimburse ER doctors when they see patients who don’t have identification and can’t prove an Alberta Health Care Insurance Plan billing number.
Thirsk said the United Conservative government stopped those payments when it ripped up the master agreement with the AMA in early 2020. He said it promised to bring back those payments when the two sides agreed to a new deal in September 2022. But to date that hasn’t happened, he said.
“I’m legally and morally bound to look after you [if] you’re unidentified [as a patient],” said Thirsk, an emergency room doctor at Edmonton’s Royal Alexandra Hospital.
“I’m going to look after you because it’s the right thing to do no matter what the problem is.”
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
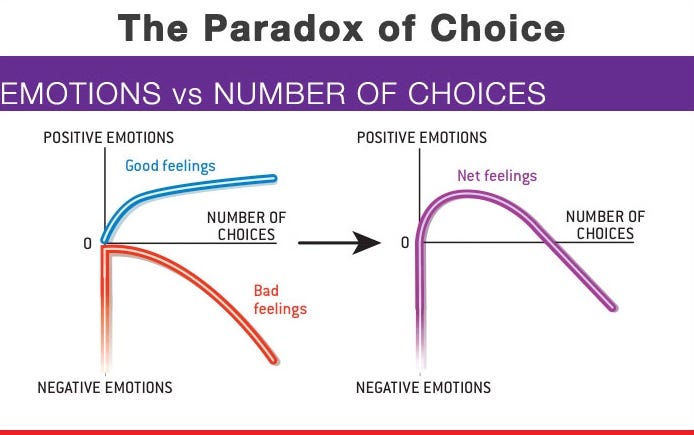
Some retired people live on a fixed income and many of them live right on the edge of their financial capability. At some time in their life, they may have to make a choice regarding many purchases.
In this case, we will illustrate “choice” using a couple’s purchase of Long-Term-Care Insurance [LTCI]. Of course, economics is the study of choice; wants, needs and scarcity, etc. In our case, if they decide to make the purchase they commit to a lifetime of premium payments. The financial tradeoff is this; if they make the commitment to purchase LTCI, they must give up something else.
EXAMPLE: In order to maintain a monthly premium of $100 ($1,200per year), an elderly patient, retired layman or couple must essentially relegate about $30,000 of financial assets to generate the $100 necessary to make an average premium payment (assumes a 7% rate of return with 4% withdrawal rate) or [4% X $30,000 = $1,200 year]. Thus, if the monthly premium cost is $500 per month, the elder must give up the use of $150,000 of retirement asset just to generate enough cash flow to pay for the LTC insurance.
***
***
The married elder couple has to make the Hobson’s Choice decision among lifestyle (dinners, vacations, gifts to children, prescription drugs, medical care or food and shelter) versus paying an insurance premium to provide for nursing home coverage for a need, which may be very real, but will not occur until sometime in the ambiguous future.
And so, when faced with such a tough economics Hobson’s Medicine Choice, neither of which delivers peace of mind or a respectable solution; many will simply decide that, in either case, they may already end up impoverished. Thus, many will often opt for the better lifestyle now … while they can enjoy it … together.
Cite: Anonymous Health Insurance Agent, Norcross, Georgia
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals.
Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed.
Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Posted on May 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
The National Nurses in Business Association (NNBA) is the premier nursing organization for nurse entrepreneurs, and a springboard for nurses transitioning from employees to entrepreneurs and business owners. The NNBA is an invaluable resource for existing nurse business owners seeking to expand, and maximize their business success.
Members’ resumes include thousands of nurse owned businesses, local, national and international awards, and millions of dollars in revenue. The experience, knowledge and impact of the NNBA community is amazing, as well as the support provided to fellow nurse entrepreneurs and aspiring entrepreneurs.
As the forerunner of the nurse entrepreneur movement, the NNBA provides valuable business information customized for nurses on how to start, plan, expand and grow your nurse owned business. They provide expert guidance, marketing and promotional opportunities, and continuing education in professional growth and career development.
Posted on May 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Meta Platforms jumped 4.23% after the big tech giant reported that its advertising revenue came in at $41.39 billion, beating analyst projections of $40.44 billion, thanks to higher ad price growth than expected. Daily active users rose to 3.43 billion, up from 3.35 billion last quarter, while nearly 1 billion people use its digital AI assistant every month. Management expects Q2 sales to come in between $42.5 billion and $45.5 billion, in-line with analyst forecasts of $44.03 billion.
EPS: $6.43 per share, crushing estimates of $5.28
Revenue: $42.31 billion, above the $41.10 expected
Microsoft leaped 7.63% after reporting its profit jumped a staggering 18% from a year earlier. That wasn’t the only good news: Revenue from Microsoft’s Azure cloud software grew 33% year over year, higher than the 31% expected by analysts. But perhaps the best news of all was management’s upbeat guidance—Microsoft projected revenue between $73.15 billion and $74.25 billion for the current quarter, well above expectations of $72.26 billion.
EPS: $3.46 per share, beating forecasts of $3.22
Revenue: $70.07 billion, above the $68.42 billion projected
Eli Lilly dropped 11.66% today, despite the fact that the pharmaceutical giant reported that sales skyrocketed 45% year over year thanks to its lucrative GLP-1 drugs, Zepbound and Mounjaro. Two things spooked investors today: The company lowered its profit outlook well below its preview estimate due its acquisition of a cancer drug from Scorpion Therapeutics, and CVS Health dropped Zepbound from its preferred drug list in lieu of arch-rival Novo Nordisk’s Wegovy this morning.—LB
EPS: $3.34 adjusted, beating the $3.02 expected
Revenue: $12.73 billion, compared to the $12.67 projected
Carrier Global climbed 11.61% after the air conditioning company boosted its fiscal forecast. Turns out everyone needs AC regardless of economic uncertainty.
People also need straight teeth: Dental products manufacturer Align Technology rose 1.98% on solid earnings.
Quanta Services gained 9.99% after the construction engineering company beat Wall Street estimates on both the top and bottom line.
What’s down
Qualcomm may have beaten earnings expectations, but shares fell 8.92% after investors were disappointed by the chipmaker’s lower guidance.
GM was in the same boat: Earnings beat forecasts, but poor guidance and warnings that tariffs could cost the company up to $5 billion this year pushed shares 0.42% lower.
Robinhood Markets enjoyed a 50% increase in revenue last quarter as traders played the volatile market, but the stock still sank 5.07%.
Moderna fell 5.29% after the vaccine maker missed revenue expectations and said it’s planning another $1.5 billion in cost cuts.
Church & Dwight, maker of household goods like Arm & Hammer Baking Soda, missed revenue forecasts last quarter and sank 6.87%.
Becton Dickinson & Co. lost 18.13% after the medical device maker warned of the adverse effects of, what else, tariffs.
Posted on May 1, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants LLC
***
***
While the healthcare industry has been dealing with high employee turnover since the start of the COVID-19 pandemic, that turnover was largely among clinical staff.
However, a recent survey found that significant healthcare leadership turnover may also be on the horizon. AMN Healthcare subsidiary B.E. Smith found that nearly half of healthcare executives plan to leave their organization in the next year.
This Health Capital Topics article reviews the survey and the reasons behind the intended exits. (Read more…)
Posted on April 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants LLC
***
***
On April 7, 2025, the Centers for Medicare & Medicaid Services (CMS) published their 2026 Rate Announcement for Medicare Advantage (MA) and Medicare Part D Prescription Drug Plans.
For 2026, the payment rate to MA plans will increase 5.06%, the largest increase in the past ten years, and up significantly from the 2.2% rate increase proposed by the Biden Administration.
This Health Capital Topics article will review the Rate Announcement.(Read more…)
In a discussion of competitive healthcare economic models, assumptions must include normal demand quantities, many fully informed patients and the fact that physicians cannot directly influence demand for medical care. These assumptions, although fluid, also preclude that patient buyers are large enough to have any influence over price and result in the following”:
In a “pure monopoly”, there is only one provider with a unique service. The doctor is a “price maker” and charges whatever s/he wishes.
In an “oligopoly”, there are a few physicians who provide similar services. For example, when it becomes clear to Dr. Smith and Dr. Jones that neither can win their price war, oli-gopolists return prices to prior, but still inflated levels!
In “monopolistic competition”, there are many providers with differentiated services. For example, should Dr. Jones decide to have evening hours, she may charge a premium for her fees if Dr. Jones doe not follow suit.
Finally, when “pure competition” occurs, there are many physicians, providing providing similar and substitutable services. Marketing and advertising does not affect fees, and prices are determined by supply and demand. The doctors become “price takers” by accepting fees arrived at by practicing competitively.
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals.
Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed.
Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Posted on April 24, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
OpenAI would be open to buying Chrome if Google is forced by a federal court to sell the web browser, the company’s ChatGPT head said yesterday.
The FDA suspended milk quality tests in some dairy products due to reduced capacity stemming from federal workforce cuts, Reuters reported.
Roche, the Swiss pharmaceutical giant, is investing $50 billion in US manufacturing to circumvent President Trump’s tariffs, the company said yesterday.
Rite Aid is preparing to sell itself in pieces ahead of a possible second bankruptcy, Bloomberg reported.
Oklo gained 8.60% after OpenAI CEO Sam Altman announced he’s stepping down as chairman of the board of the nuclear power startup.
Duolingo popped 10.01% after Morgan Stanley initiated coverage of the language learning company, calling it a “best-in-class consumer internet asset.”
Cava climbed 6.29% due to an upgrade from analysts at Bernstein, who think the bowl slop stock will not only survive but thrive in an economic downturn.
Amphenol rose 8.21% thanks to impressive earnings for the high-speed cable company, coupled with a solid fiscal outlook.
Vertiv Holdings jumped 8.60% after the data center company posted an impressive quarterly profit and raised its fiscal forecast.
Stocks surged first thing this morning after President Trump said the media blew things out of proportion and that he has “no intention” of firing Jerome Powell. He also said he would be “very nice” to China in tariff negotiations.
Treasury Secretary Scott Bessent also did some damage control, touting the opportunity for a “big deal” between the US and China.
The combination sent a relief rally sweeping through markets, and while the euphoria faded by mid-afternoon, all three indexes ended the day in the green.
Gold fell and bitcoin rose as investors took on more risk (see below), while oil dropped on reports that OPEC+ may hike its crude output after its meeting next month.
Posted on April 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Classic Definition: Suppose someone tells you “I am lying.” If what he/she tells you is true, then he/she is lying, in which case what he/she tells you are false. On the other hand, if what he/she tells you is false, then he/she is not lying, in which case what he/she tells you is true.
Modern Circumstance: In short: if “I am lying” is true then it is false, and if it is false then it is true.
Paradox Example: The paradox arises for any sentence that says or implies of itself that it is false (the simplest example being “This sentence is false”). It is attributed to the ancient Greek seer Epimenides (fl. c. 6th century BCE), an inhabitant of Crete, who famously declared that “All Cretans are liars” (consider what follows if the declaration is true). The paradox is important in part because it creates severe difficulties for logically rigorous theories of truth; it was not adequately addressed (which is not to say solved) until the 20th century.
Paradox Example: Doctors lie because, as caretakers, our role isto improve the lives of their patients. Re-assuring patients during some of the most difficult times of their lives counts as improving their well being! This is an acceptable practice because it does not cause harm.
Paradox Example: Cultural differences may make a lie of omission or the practice of withholding information from the patient, prudent. For instance, some cultures and religions dictate that the husband or head male family members make all medical decisions for women.
Paradox Example: Many physicians don’t report “near misses” to their patients. But, concealing serious medical errors is something we recommend against.
COMMENTS APPRECIATED
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals.
Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed.
Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
There’s often a disconnect between physicians, insurance agents and financial advisors and the patients and clients they’d like to serve. Both might ostensibly share the same goal but there’s often a big difference in perspective. Advisors / Physicians and would-be clients / patients likely have different communication styles, especially in an age where technology has greatly changed the way we talk with one another. Their expectations and priorities can also often dramatically diverge. Those structural gaps can hinder collaboration and trust.
To bridge this divide, you must understand how prospective clients and patients think nowadays and be able to adjust your M.A.S. approach accordingly.
THE BASICS
Marketing is the business process of identifying, anticipating and satisfying patient’s, client’s or customers’ needs and wants. It is your unique value proposition or strategic competitive advantage. Marketers can direct product to other businesses or directly to consumers. But, we believe it is actually your strategic competitive advantage [SCA] which differentiates yourself from competitors. It is the “moat” around your business.
Advertising is a marketing communication that employs an openly sponsored, non-personal message to promote or sell a product, service or idea. Sponsors of advertising are typically businesses wishing to promote their products or services. Advertising is communicated through various mass media outlet, including traditional media such as newspapers, magazines, television, radio, outdoor advertising or direct mail; and new media such as search results, blogs, social media, websites or text messages. The actual presentation of the message in a medium is referred to as an advertisement, or “ad” or advert for short. But, we believe that is simply how you disseminate your strategic competitive advantage [SCM] to potential clients.
Sales close the deal and collects money. Sales are activities related to selling or the number of goods or services sold in a given targeted time period. The seller, or the provider of the goods or services, completes a sale in response to an acquisition, appropriation, requisition, or a direct interaction with the buyer at the point of sale. There is a passing of title (property or ownership) of the item, and the settlement of a price, in which agreement is reached on a price for which transfer of ownership of the item will occur. The seller, not the purchaser, typically executes the sale and it may be completed prior to the obligation of payment. In the case of indirect interaction, a person who sells goods or service on behalf of the owner is known as a salesman or saleswoman or salesperson, but this often refers to someone selling goods in a store/shop, in which case other terms are also common, including salesclerk, shop assistant, and retail clerk.
***
***
DERIVATIVE THOUGHTS
Public Relations [PR] is differentiated than advertising from in that an advertiser pays for and has control over the message. It differs from personal selling in that the message is non-personal, i.e., not directed to a particular individual. We pay for advertising but pray for public relations. But public relations are not controllable but it is free, while advertising is not. PR suggests that “good news or bad news”; just spell the name correctly
Change Management is the discipline that guides how we prepare, equip and support individuals to successfully adopt to change in order to drive organizational success and outcomes.
Crisis Management is the precautions and identification of threats to an organization and its stakeholders, and the methods used by the organization to deal with these threats.
MODERNITY NOW
CRM stands for Customer Relationship Management, which is a system for managing all interactions with current and potential customers, clients or patients. The goal is simple: improve relationships to grow your business or medical practice. CRM technology helps companies stay connected to customers, streamline processes, and improve profitability.
When people talk about CRM, they’re usually referring to a CRM system: software that helps track each interaction you have with a prospect, patient or customer. That can include sales calls, treatment plans or service interactions, marketing e-mails, and more. CRM tools can unify customer and company data from many sources and even use Artificial Intelligene [AI] to help better manage relationships across the entire customer – patient lifecycle – spanning departments described in the M.A.S. basics, above.
Classic: An arrangement by which a patient requests that their health benefit payments be made directly to a designated person or facility, such as a physician or hospital. It is a legally binding agreement between patient and Insurance company asking them to send your reimbursement checks directly to your doctor.
Modern: To accept assignment means that the provider agrees to accept what ever the insurance company allows or approves as payment in full for the claim. The patient signs paperwork requiring his health insurance provider to pay his physician or hospital directly. EXAMPLES:
CMS: The approved amount, also known as the Medicare-approved amount, is the fee that Medicare sets as how much a provider or supplier should be paid for a particular service or item. Original Medicare calls this “assignment.”
Tardiness: When a medical office accepts an assignment of benefits, the insured patients may have to wait several months for their insurance reimbursement to arrive.
Posted on April 15, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
A recent study published in the Annals of Internal Medicine found that in 2021, UnitedHealth Group received just under $14 billion in extra Medicare Advantage payments after using a code that made its members appear sicker. It’s another tough break for the plan and provider that has faced allegations of illegally taking additional money from patients and taxpayers, especially after its CEO was fatally shot in early December.
US stocks edged higher on Monday as investors focused on tech’s temporary reprieve from President Trump’s tariffs.
The S&P 500 (^GSPC) trimmed bigger gains to rise a healthy 0.8%. The tech-heavy NASDAQ (^IXIC) also closed off its session high, up 0.6%. The Dow Jones Industrial Average (^DJI) was up around 0.7%, or more than 300 points.
Posted on April 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
ACCOUNTABLE CARE ORGANIZATIONS
Realizing Equity, Access, and Community Health
By Staff Reporters
***
***
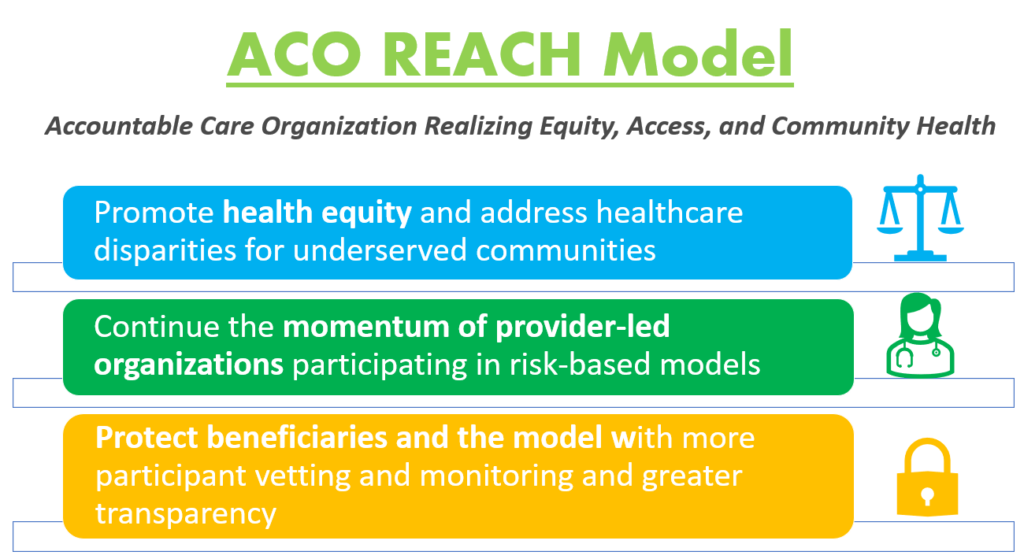
Model Overview
The ACO REACH Model provides novel tools and resources for health care providers to work together in an ACO to improve the quality of care for people with Traditional Medicare. REACH ACOs are comprised of different types of providers, including primary and specialty care physicians.
The ACO REACH Model makes important changes to the previous Global and Professional Direct Contracting (GPDC) Model which include:
***
***
Promote Provider Leadership and Governance. The ACO REACH Model includes policies to ensure doctors and other health care providers continue to play a primary role in accountable care. At least 75% control of each ACO’s governing body generally must be held by participating providers or their designated representatives, compared to 25% during the first two Performance Years of the GPDC Model. In addition, the ACO REACH Model goes beyond prior ACO initiatives by requiring at least two beneficiary advocates on the governing board (at least one Medicare beneficiary and at least one consumer advocate), both of whom must hold voting rights.
Protect Beneficiaries and the Model with More Participant Vetting, Monitoring and Greater Transparency. CMS will ask for additional information on applicants’ ownership, leadership, and governing board to gain better visibility into ownership interests and affiliations to ensure participants’ interests align with CMS’s vision. We will employ increased up-front screening of applicants, robust monitoring of participants, and greater transparency into the model’s progress during implementation, even before final evaluation results, and will share more information on the participants and their work to improve care. Last, CMS will also explore stronger protections against inappropriate coding and risk score growth.
On March 15th, 2025, President Donald Trump signed a continuing resolution (CR) that avoided a government shutdown and funds the federal government for the rest of the fiscal year, i.e., through September 30th, 2025.
Perhaps more notable than what was included in the spending bill was what was once again excluded. While the COVID-era tele-health waivers were temporarily extended, Medicare physician payment rates were not addressed, meaning physicians will continue experiencing a 2.93% pay cut for 2025.
This Health Capital Topics article discusses the healthcare provisions included in and excluded from the CR, and the impacts on healthcare providers. (Read more…)
Posted on April 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Ann Miller RN MHA CPHQ CMP™
***
***
Finally … Fiduciary second investing and financial planning opinions right here!
Telephonic or electronic advice for medical professionals that is:
Objective, affordable, medically focused and financially personalized
Rendered by a pre-screened financial consultant for doctors and medical professionals
Offered on a pay-as-you-go basis, by phone or secure e-mail transmission
The iMBA Discussion Forum™ is a physician-to-financial advisor telephone or e-mail portal that connects independent financial professionals to doctors, nurses or healthcare executives desiring affordable and unbiased financial planning advice.
Medical professionals and healthcare executives can now receive direct access to pre-screened iMBA professionals in the areas of Investing, Financial Planning, Asset Allocation, Portfolio Management, Insurance, Mortgage and Lending, Human Resources, Retirement Planning and Employee Benefits. To assist our medical professional and healthcare executive members, we can be contracted with per-minute or per-project fees, and contacted by client phone, email or secure instant messaging.
Suppose that in a new Accountable Care Organization [ACO] contract, a certain medical practice was awarded a new global payment or capitation styled contract that increased revenues by $100,000 for the next fiscal year. The practice had a gross margin of 35% that was not expected to change because of the new business. However, $10,000 was added to medical overhead expenses for another assistant and all Account’s Receivable (AR) are paid at the end of the year, upon completion of the contract.
Cost of Medical Services Provided (COMSP):
The Costs of Medical Services Provided (COMSP) for the ACO business contract represents the amount of money needed to service the patients provided by the contract. Since gross margin is 35% of revenues, the COMSP is 65% or $65,000. Adding the extra overhead results in $75,000 of new spending money (cash flow) needed to treat the patients. Therefore, divide the $75,000 total by the number of days the contract extends (one year) and realize the new contract requires about $ 205.50 per day of free cash flows.
Assumptions
Financial cash flow forecasting from operating activities allows a reasonable projection of future cash needs and enables the doctor to err on the side of fiscal prudence. It is an inexact science, by definition, and entails the following assumptions:
All income tax, salaries and Accounts Payable (AP) are paid at once.
Durable medical equipment inventory and pre-paid advertising remain constant.
Gains/losses on sale of equipment and depreciation expenses remain stable.
Gross margins remain constant.
The office is efficient so major new marginal costs will not be incurred.
***
***
Physician Reactions:
Since many physicians are still not entirely comfortable with global reimbursement, fixed payments, capitation or ACO reimbursement contracts; practices may be loath to turn away short-term business in the ACA era. Physician-executives must then determine other methods to generate the additional cash, which include the following general suggestions:
1. Extend Account’s Payable
Discuss your cash flow difficulties with vendors and emphasize their short-term nature. A doctor and her practice still has considerable cache’ value, especially in local communities, and many vendors are willing to work them to retain their business
2. Reduce Accounts Receivable
According to most cost surveys, about 30% of multi-specialty group’s accounts receivable (ARs) are unpaid at 120 days. In addition, multi-specialty groups are able to collect on only about 69% of charges. The rest was written off as bad debt expenses or as a result of discounted payments from Medicare and other managed care companies. In a study by Wisconsin based Zimmerman and Associates, the percentages of ARs unpaid at more than 90 days is now at an all time high of more than 40%. Therefore, multi-specialty groups should aim to keep the percentage of ARs unpaid for more than 120 days, down to less than 20% of the total practice. The safest place to be for a single specialty physician is probably in the 30-35% range as anything over that is just not affordable.
The slowest paid specialties (ARs greater than 120 days) are: multi-specialty group practices; family practices; cardiology groups; anesthesiology groups; and gastroenterologists, respectively. So work hard to get your money, faster. Factoring, or selling the ARs to a third party for an immediate discounted amount is not usually recommended.
3. Borrow with Short-Term Bridge Loans
Obtain a line of credit from your local bank, credit union or other private sources, if possible in an economically constrained environment. Beware the time value of money, personal loan guarantees, and onerous usury rates. Also, beware that lenders can reduce or eliminate credit lines to a medical practice, often at the most inopportune time.
4. Cut Expenses
While this is often possible, it has to be done without demoralizing the practice’s staff.
5. Reduce Supply Inventories
If prudently possible; remember things like minimal shipping fees, loss of revenue if you run short, etc.
6. Taxes
Do not stop paying withholding taxes in favor of cash flow because it is illegal.
Hyper-Growth Model:
Now, let us again suppose that the practice has attracted nine more similar medical contracts. If we multiple the above example tenfold, the serious nature of potential cash flow problem becomes apparent. In other words, the practice has increased revenues to one million dollars, with the same 35% margin, 65% COMSP and $100,000 increase in operating overhead expenses.
Using identical mathematical calculations, we determine that $750,000 / 365days equals $2,055.00 per day of needed new free cash flows! Hence, indiscriminate growth without careful contract evaluation and cash flow analysis is a prescription for potential financial disaster.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
In the latest iteration of Trump Administration healthcare cuts, the Centers for Medicare & Medicaid Services (CMS) announced on March 12th, 2025 that four Center for Medicare and Medicaid Innovation (CMMI) payment models would be sunset at the end of 2025, earlier than originally scheduled.
Cutting these models, which decision was based on “a comprehensive and data-driven review of [CMS’s] model portfolio,” are anticipated to save nearly $750 million (although the source of these savings was not detailed).
This Health Capital Topics article discusses the models being ended and the impact on healthcare stakeholders. (Read more…)
In the first month of 2025, hospital revenue and expenses both increased, balancing each other out and resulting in continued steady financial performance for hospitals, according to Kaufman Hall’s January 2025 National Hospital Flash Report.
Revenues grew more quickly in the inpatient setting, as more patients were treated in the hospital and emergency department than in outpatient settings. While expense increases were largely driven by drug costs, the rate of that growth has significantly slowed.
This Health Capital Topics article reviews the report and the current state of hospital operations. (Read more…)
Posted on March 29, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
EDITOR-IN-CHIEF
By Dr. David Edward Marcinko; FACFAS MBA MEd
***
***
NATIONAL PHYSICIANS WEEK
National Physicians Week sets out March 25-31 to honor the healers dedicated to the art of medicine. In 2017, National Physicians Week highlighted the shortage of physicians in the United States against a growing landscape of minorities joining the ranks.
#NationalPhysiciansWeek
“In hindsight, I am proud of what we have accomplished in a short period of time, including raising the recognition of our group and spotlighting the years of sacrifice by those in our profession to serve our patients. We are poised to initiate actionable efforts to engage and educate our physician community.”
Cite: Dr. Kimberly Funches Jackson, President
Today in 2025, let’s explore the invaluable contributions of physicians, celebrate their hard work during National Physicians Week, and highlight the essential role that locum doctors play in enhancing healthcare delivery.
A Week to Honor All Physicians
National Physicians Week is a celebration of the remarkable work that doctors do every single day. From diagnosing complex conditions to providing life-saving treatments, physicians dedicate themselves to improving the health and well-being of their patients. It’s a week for healthcare professionals, patients, and communities to come together and show appreciation for the doctors who make a difference in our lives.
Physicians work long hours, face immense pressure, and make critical decisions daily. Their contributions go beyond the walls of the hospital, as many are also involved in research, teaching, and community outreach.
So, this week, it’s important to acknowledge not only their professional expertise but also the compassion and resilience they exhibit in their work.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on March 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
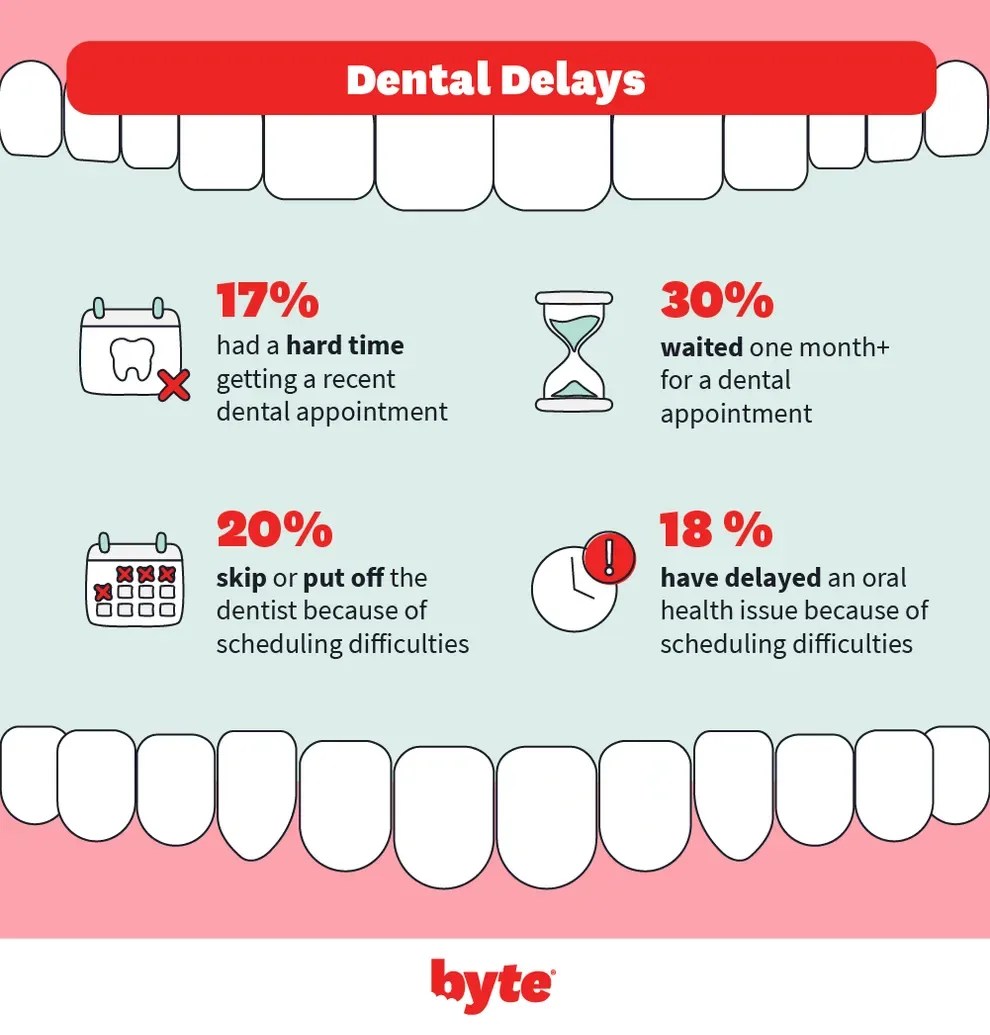
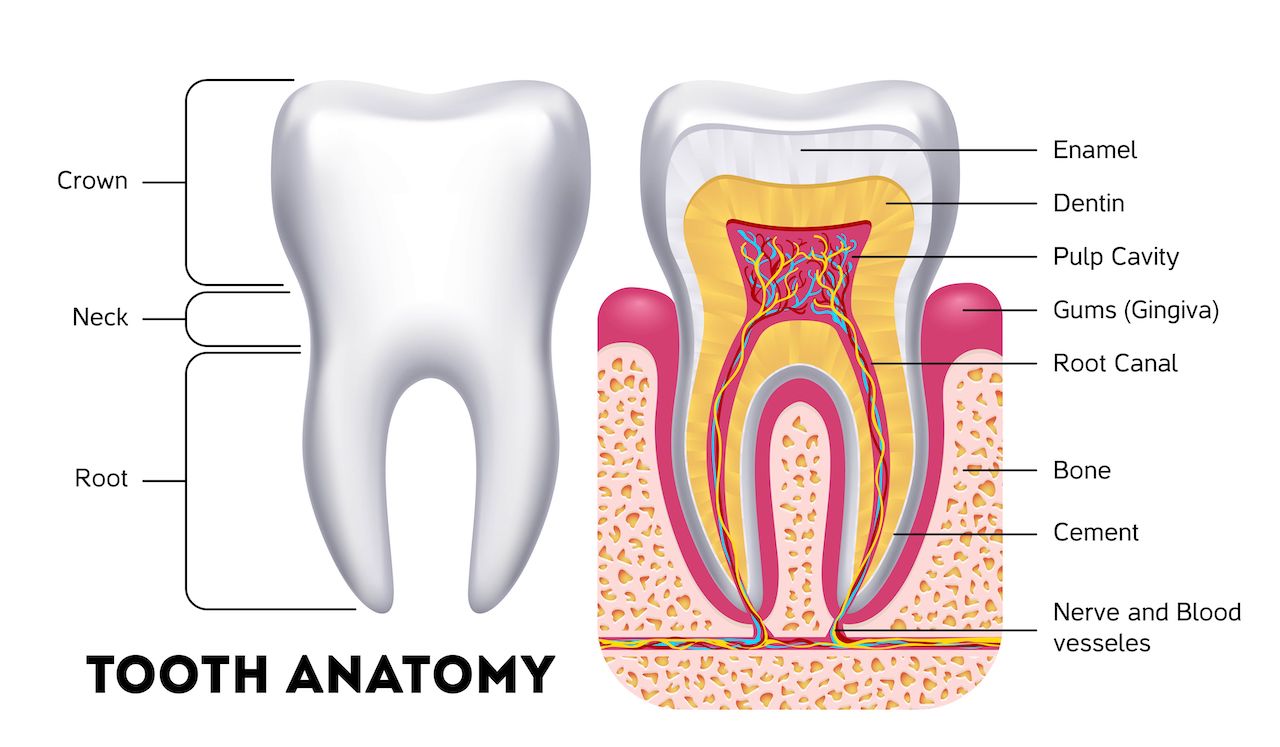
Dental care in America divides people into two camps: those who can afford regular preventive care and cleanings, and those who can’t.
These so-called dental deserts contribute to a deep disparity in overall health. People who live in these places are more likely to get tooth decay and develop severe health problems. They also spend more money on care, and more time seeking health assistance in an emergency.
***
***
Stat: 25 million. That’s how many US residents live in areas without enough dentists, according to a recent Harvard University study.
A growing movement against fluoride is adding to the risk of tooth decay in these “dental deserts.” (NPR)
The recent horrifying murder of UnitedHealthcare Group CEO Brian Thompson has called attention to the anger many Americans feel about our health care system. This tragedy has thrust the very real issue of health care costs back into the headlines.
One article on the topic, from Ken Alltucker for USA Today, offered seven reasons why Americans pay so much for health care with such poor results. When I saw the headline, I thought, “Finally, someone’s going to bring up the elephant in the room: taxes.”
The seven reasons included bloated administrative costs, lack of price transparency, overpaid specialists, higher prescription drug prices, and more. But I didn’t see a word about how, compared to other developed nations with “cheaper” health care, Americans pay far lower taxes. That omission feels like leaving a critical piece of the puzzle off the table.
***
***
In reality, countries with universal health care are not pulling off some magic trick of efficiency. They are simply collecting the money differently—through significantly higher taxes. Americans, on the other hand, pay for health care more directly, through out-of-pocket costs and insurance premiums.
In a column last year, I did the math. Americans spend about 17.8% of GDP on health care, plus 27.7% of GDP in taxes. That’s a total of 45.5%. Now compare that to twelve European countries with universal health care. They spend a median of 11.5% of GDP on health care and collect 41.9% of GDP in taxes. Total? 53.4%. In other words, Americans are spending 7.9% less overall on healthcare and taxes combined.
The saving isn’t what it appears, though. A fair comparison of healthcare costs and taxes needs to account for the fact that universal healthcare systems cover 100% of their populations, while the U.S. system currently leaves about 8% uninsured. If you factor in the cost of covering our uninsured residents, the U.S. likely spends a comparable percentage of income on healthcare as European countries with universal systems.
***
***
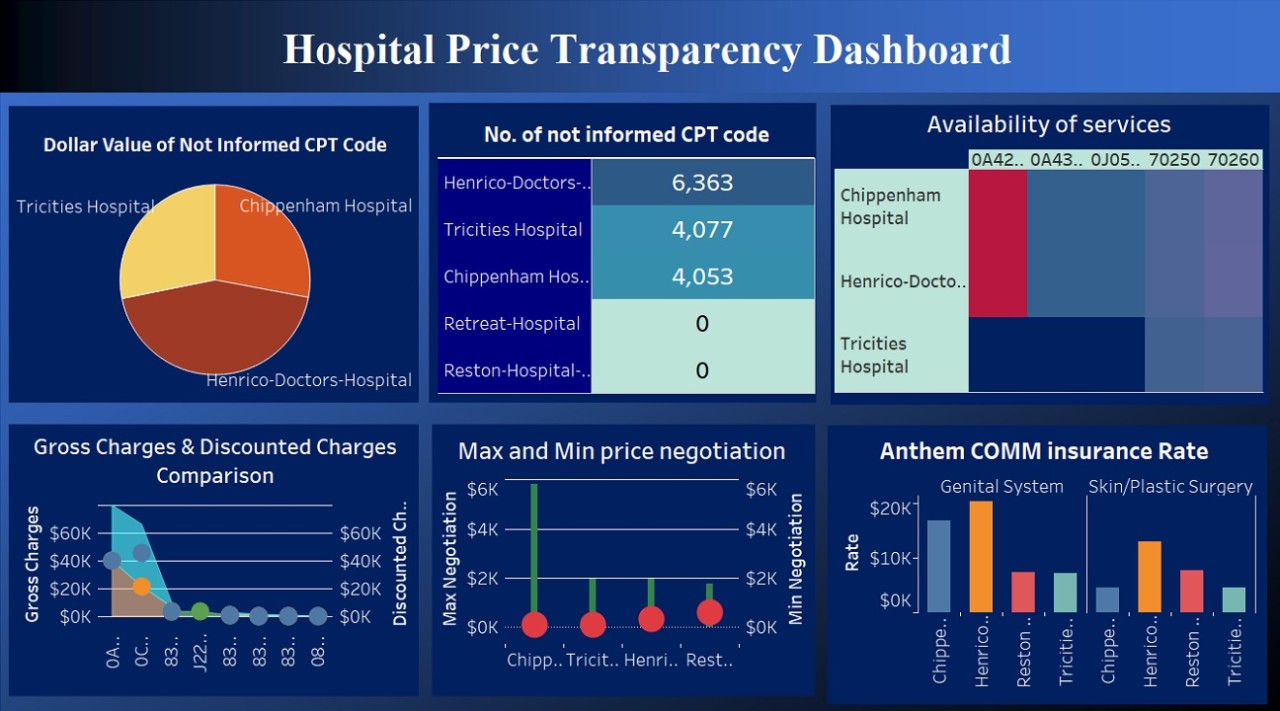
Our system is far from perfect. As the USA Todayarticle points out, administrative costs are bloated. Harvard’s David Cutler estimates up to 25% of our health spending goes toward paperwork, phone calls, and processing. Price transparency is practically nonexistent. The cost of a diagnostic test might vary from $300 to $3,000 depending on where you go. We pay much more for prescription drugs and many procedures than those same treatments cost in other developed nations. Another issue is the fee-for-service model that rewards doctors for ordering more tests and procedures, whether or not patients get better.
We can do better. Innovations like value-based care, where providers are paid for outcomes rather than procedures, could help shift the system toward real results. Greater price transparency would empower patients to make informed choices and force providers to compete. And addressing administrative inefficiencies could save billions.
Yet fixing the system requires being honest about trade-offs. If we want universal health care at European price rates, we need to accept European tax rates. That’s the part of the conversation that often gets left out. It’s easy to be angry at hospitals, insurance companies, and drug manufacturers—and yes, they all have plenty to answer for. But we also need to face the reality that we’ve chosen a system that prioritizes lower taxes over centralized health care.
Anger may have put the flaws in our health care system in the spotlight. Finding genuine solutions will require moving beyond expressions of anger and frustration. It will demand thoughtful discussions about what kind of health care system, as individuals and as a nation, that we want and how we are willing to fund it.
Posted on March 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
While some medical practitioners and facilities can operate without Professional Liability Insurance coverage, one business related insurance that cannot / should not be avoided is Worker’s Compensation. Employers in all but seven states – so-called “monopolistic” states because they have their own state funds, are under statutory obligation to provide coverage for their employees. Historically, Worker’s Compensation pre-dates Social Security entitlements and well before the emergence of employer sponsored group benefits.
The coverage under worker’s compensation provides for lost income due to on-the-job accidents or work-related disability or death and the amount of benefits vary by state. In some instances, the coverage will reimburse the employee for medical expenses incurred with the accident.
The four general benefits covered under Worker’s Compensation are:
Medical Care – for expenses incurred usually without limitations on amount or period of care.
Disability Income – payable for both total and partial disability and is usually based on 66 2/3 percent of their wage base.
Death Benefits – generally fall into two categories; one a flat amount for “burial” insurance; and two, survivor benefits. Though varying by state, these benefits are similar to the disability payment (a percentage of weekly base wages) but may be capped as to total benefit, such as $50,000 or a period, such as 10 years
Rehabilitation Benefits – includes not only medical rehabilitation, but vocational rehabilitation, vocational counseling, retraining or educational benefits, and job placement
Traditionally, the secondary purpose of Worker’s Compensation was to reduce potential litigation because employees accepting the benefits from a Worker’s Compensation claim generally waived their right to sue their employer.
***
***
However, in our litigious society, this “protective shelter” has been severely tested and is crumbling.
Employers may provide their Worker’s Compensation three ways:
Private commercial insurance
State government funds
Self-insurance
Very few factors drive the premium structure – the occupation of the workers is the single most important determinant of premiums. An office worker may have premiums as low as $.10 per hundred of wages and a coal miner may exceed $50.00 per hundred of wages. Generally speaking, however, Worker’s Compensation premiums for the medical profession or healthcare worker are among the lowest available.
Therefore, for the medical practice, some physicians may consider self-insurance because the weekly benefits are typically below $500, thus making this decision attractive.
Alternatively, because officers and owners can elect not to be covered by Worker’s Compensation, the decision to purchase coverage from a private insurance company may afford inexpensive assurance that the benefits will be conveniently provided, and administered, by a private insurance company for their employees.
Posted on March 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
A CONTROVERSY?
By Staff Reporters
***
***
DEFINITION
State medical boards are the agencies that license medical doctors, investigate complaints, discipline physicians who violate the medical practice act, and refer physicians for evaluation and rehabilitation when appropriate. The overriding mission of medical boards is to serve the public by protecting it from incompetent, unprofessional, and improperly trained physicians. Medical boards accomplish this by striving to ensure that only qualified physicians are licensed to practice medicine and that those physicians provide their patients with a high standard of care.
The right to practice medicine is a privilege granted by the state. Each state has laws and regulations that govern the practice of medicine and specify the responsibilities of the medical board in regulating that practice. These regulations are laid out in a state statute, usually called a medical practice act. State medical boards establish the standards for the profession through their interpretation and enforcement of this act.
Assembling a quality physician population to meet the needs of the public begins with licensure. During the process of evaluating applicants for medical licensure, state medical boards’ primary focus is on a physician’s qualifications, including undergraduate and graduate medical education, work history, and personal character.
Candidates for licensure also must successfully complete a rigorous examination designed to assess their ability to apply knowledge, concepts, and principles of health and disease that constitute the basis for safe and effective patient care.
The Federation of State Medical Boards of the United States, Inc., and the National Board of Medical Examiners (NBME) have collaborated to establish a single, 3-step examination for medical licensure in the United States, known as the United States Medical Licensing Examination (USMLE). The USMLE provides state medical boards with a common evaluation system for all licensure applicants. To assure the continued relevance of the exam, the NBME uses basic science and clinical faculty from the nation’s medical schools as well as practicing physicians, some of whom serve on state medical boards, to generate the examinations.
“… I am persuaded that licensure has reduced both the quantity and quality of medical practice…It has reduced the opportunities for people to become physicians, it has forced the public to pay more for less satisfactory service, and it has retarded technological development…I conclude that licensure should be eliminated as a requirement for the practice of medicine”
-Milton Friedman, Nobel prize-winning economist
“As a rule, regulation is acquired by the industry and is designed and operated primarily for its benefit”
-George J. Stigler Nobel Prize-winning economist
“Licensing has served to channel the development of health care services by granting an exclusive privilege and high status to practitioners relying on a particular approach to health care, a disease-oriented intrusive approach rather than a preventive approach….By granting a monopoly to a particular approach to health care, the licensing laws may serve to assure an ineffective health care system”
-Lori B. Andrews, Professor of Law, Chicago-Kent College
“Let us allow physicians, hospitals and schools to spring up where they’re needed, abolish the restrictive licensure laws, and simply invoke the laws against fraud to insure honesty among all providers of health care …That will make health care affordable for everyone”
Posted on March 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The S&P 500 edged up 0.1%. The index finished with a 0.5% gain for the week. It’s still down 4.8% so far this month. The Dow Jones Industrial Average eked out a 0.1% gain, while the NASDAQ composite rose 0.5%.
It appears Medicare coverage for tele-health is here to stay—at least for the next six months. When the House of Representatives and Senate passed a budget on March 11t and 14th, respectively, they not only avoided a government shutdown, but also extended a resolution for Medicare to cover non-behavioral health tele-health appointments until September 30th.
Visualize: How private equity tangled banks in a web of debt, from the Financial Times.
9. We act with honesty, integrity and are always straightforward. 8. We strive to be innovative, creative, iconoclastic, and flexible. 7. We admit and learn from mistakes and don’t repeat them. 6. We work hard always as competitors are trying to catch up. 5. We treat others with dignity and respect. 4. We are the onus of consulting advice for the well being of others. 3. We fight complacency as former success is in the past. 2. The best management styles are timeless, not timely. 1. Our clients are colleagues and always come first.
SPEAKING: Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements.
***
***
CONTACT: Ann Miller RN MHA at: MarcinkoAdvisors@outlook.com
When analyzing a set of financial statements to determine practice value, adjustments (normalizations) generally are needed to produce a clearer picture of likely future income and distributable cash flow. It also allows more of an “apples to apples” line item comparison. This normalization process usually consists of making three main adjustments to a medical practice’s net income (profit and loss) statement.
1. Non-Recurring Items: Estimates of future distributable cash flow should exclude non-recurring items. Proceeds from the settlement of litigation, one-time gains/losses from the selling of assets or equipment, and large write-offs that are not expected to reoccur, each represent potential nonrecurring items. The impact of nonrecurring events should be removed from the practice’s financial statements to produce a clearer picture of likely future income and cash flow.
2. Perquisites: The buyer of a medical practice may plan to spend more or less than the current doctor-owner for physician executive compensation, travel and entertainment expenses, and other perquisites of current management. When determining future distributable cash flow, income adjustments to the current level of expenditures should be made for these items.
3. Non-cash Expenses: Depreciation expense, amortization expense, and bad debt expense are all non-cash items which impact reported profitability. When determining distributable cash flow, you must analyze the link between non-cash expenses and expected cash expenditures.
The annual depreciation expense is a proxy for likely capital expenditures over time. When capital expenditures and depreciation are not similar over time, an adjustment to expected cash flow is necessary. Some practices reduce income through the use of bad debt expense rather than direct write-offs. Bad debt expense is a non-cash expense that represents an estimate of the dollar volume of write-offs that are likely to occur during a year. If bad debt expense is understated, practice profitability will be overstated.
***
***
Balance Sheet Adjustments
Adjustments also can be made to a practice’s balance sheet to remove non-operating assets and liabilities, and to restate asset and liability value at market rates (rather than cost rates). Assets and liabilities that are unrelated to the core practice being valued should be added to or subtracted from the value, depending on whether they are acquired by the buyer.
Examples include the asset value less outstanding debt of a vacant parcel of land, and marketable securities that are not needed to operate the practice. Other non-operating assets, such as the cash surrender value of officer life insurance, generally are liquidated by the seller and are not part of the business transaction.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: CONTACT: MarcinkoAdvisors@outlook.com
Posted on March 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Drugs: (List of Schedule I-V Controlled Drugs)
By Staff Reporters
***
***
Any discussion on narcotics, prescription drugs, or other controlled substances is usually peppered with the word schedule. One substance may be Schedule I, while another is Schedule II, III, IV, or V.
Drugs, substances, and certain chemicals used to make drugs are classified into five (5) distinct categories or schedules depending upon the drug’s acceptable medical use and the drug’s abuse or dependency potential. The abuse rate is a determinate factor in the scheduling of the drug; for example, Schedule I drugs have a high potential for abuse and the potential to create severe psychological and/or physical dependence. As the drug schedule changes — Schedule II, Schedule III, etc., so does the abuse potential — Schedule V drugs represents the least potential for abuse.
A Listing of drugs and their schedule are located at Controlled Substance Act (CSA) Scheduling or CSA Scheduling by Alphabetical Order. These lists describes the basic or parent chemical and do not necessarily describe the salts, isomers and salts of isomers, esters, ethers and derivatives which may also be classified as controlled substances. These lists are intended as general references and are not comprehensive listings of all controlled substances.
Please note that a substance need not be listed as a controlled substance to be treated as a Schedule I substance for criminal prosecution. A controlled substance analogue is a substance which is intended for human consumption and is structurally or pharmacologically substantially similar to or is represented as being similar to a Schedule I or Schedule II substance and is not an approved medication in the United States.
Schedule I Schedule I drugs, substances, or chemicals are defined as drugs with no currently accepted medical use and a high potential for abuse. Some examples of Schedule I drugs are: heroin, lysergic acid diethylamide (LSD), marijuana (cannabis), 3,4-methylenedioxymethamphetamine (ecstasy), methaqualone, and peyote.
Schedule II Schedule II drugs, substances, or chemicals are defined as drugs with a high potential for abuse, with use potentially leading to severe psychological or physical dependence. These drugs are also considered dangerous. Some examples of Schedule II drugs are: combination products with less than 15 milligrams of hydrocodone per dosage unit (Vicodin), cocaine, methamphetamine, methadone, hydromorphone (Dilaudid), meperidine (Demerol), oxycodone (OxyContin), fentanyl, Dexedrine, Adderall, and Ritalin
Schedule III Schedule III drugs, substances, or chemicals are defined as drugs with a moderate to low potential for physical and psychological dependence. Schedule III drugs abuse potential is less than Schedule I and Schedule II drugs but more than Schedule IV. Some examples of Schedule III drugs are: products containing less than 90 milligrams of codeine per dosage unit (Tylenol with codeine), ketamine, anabolic steroids, testosterone
Schedule IV Schedule IV drugs, substances, or chemicals are defined as drugs with a low potential for abuse and low risk of dependence. Some examples of Schedule IV drugs are: Xanax, Soma, Darvon, Darvocet, Valium, Ativan, Talwin, Ambien, Tramadol
Schedule V Schedule V drugs, substances, or chemicals are defined as drugs with lower potential for abuse than Schedule IV and consist of preparations containing limited quantities of certain narcotics. Schedule V drugs are generally used for antidiarrheal, antitussive, and analgesic purposes. Some examples of Schedule V drugs are: cough preparations with less than 200 milligrams of codeine or per 100 milliliters (Robitussin AC), Lomotil, Motofen, Lyrica, Parepectolin
During the January 2025 J.P. Morgan Healthcare Conference, Teladoc’s executives announced the company has partnered with Amazon Health Services, joining its Health Benefits Connector program. The program was rolled out in January 2024 and connects Amazon customers with virtual care benefits covered by their insurance plan or employer; if eligible, customers are able to apply to join the program(s).
Teladoc is the fifth company to join Amazon’s Health Benefits Connector program (formerly known as Health Conditions Programs), along with digital physical therapy company Hinge Health; chronic condition management company Omada; online therapy and mental health firm Rula; and behavioral healthcare provider Talkspace. (Read more…)
Posted on March 9, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITION
By Staff Reporters
***
***
FACILITY CHARGEDEFINED
Classic: Service fee submitted for payment by a healthcare facility, such as a clinic, hospital or ambulatory care center.
Modern: Facility fees are expenses charged by hospitals to cover their overhead – the funding needed to keep the lights on, machines running, and doors open, etc. People who receive outpatient care at hospital-owned buildings are charged a facility fee, in addition to treatment costs and fees charged, individually, by doctors.
Examples: How to Fight Facility Fees:
Check with your health agent or insurer. Many insurers don’t cover facility fees or cover only a portion.
Talk to your doctor. It’s hard to tell whether a facility is hospital-run or whether your doctor works for a health system.
Posted on March 9, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DENTAL ADA DEGREES
By Colgate and Staff Reporters
***
***
DDS vs. DMD Degree
DDS and DMD are the acronyms of the degrees dentists earn after finishing dental school. DDS means Doctor of Dental Surgery, and DMD can mean either Doctor of Medicine in Dentistry or Doctor of Dental Medicine. While the names are different, the American Dental Association (ADA) explains that they represent the same education. Some universities may grant dental graduates with a DDS, and others grant a DMD, but both degrees have the same requirements.
According to the ADA, the Baltimore College of Dental Surgery established the first Doctor of Dental Surgery degrees in 1840. When Harvard University started its dental school in 1867, their degrees were called Dentariae Medicinae Doctorate (Doctor of Medicine in Dentistry) because Harvard uses Latin names for their degrees. Even though these degrees are based on the same educational requirements, they still have different names.
Difference Between a DDS and a DMD Degree?
Today, many universities award a DMD degree. Dentists with either a DDS or a DMD are educated to practice general dentistry. All dentists receive a rigorous education. First, dental schools typically require a four-year undergraduate education. Afterward, graduates go to dental school for another four years of classroom training, clinical training, and dental laboratory training.
Dental students spend the first two years of dental school studying biomedical sciences courses like anatomy, biochemistry, pathology, and pharmacology. The last two years are focused on clinical and laboratory training.
After graduating from dental school, dentists must pass a national written examination called the National Board Dental Examination, followed by a regional clinical board examination. Dentists must also pass a jurisprudence examination about state laws before being given a license to practice dentistry in that state.
Post Graduate Education After a DDS or DMD
Most dentists stick with practicing general dentistry. However, some choose to specialize in a particular area of dentistry after earning their degree. Training programs range from two to six years, depending upon the specialty area. There are several dental specialties, including endodontics, orthodontics, periodontics, prosthodontics, oral surgery, and pediatric dentistry. The ADA can help you find a dentist with a specialty that fits you best.
Dentists receive a rigorous education and have to pass several exams to be able to practice. Whether they have a DDS or DMD after their name, you should choose a dentist based on their skills, types of services provided, communication, and professionalism.
RISK MANAGEMENT, LIABILITY INSURANCE AND ASSET PROTECTION ABBREVIATIONS
[Glossary of Important Acronyms]
Much has been written and much has been opined on the topic of medical risk management, insurance, asset protection and professional liability for physicians and healthcare providers in this textbook; and elsewhere.
But occasionally, we all still get lost in a wide array of abbreviations, acronyms, and initialisms that are constantly changing in this ecosystem.
And so, this glossary serves as a ready reference for those who want to know about these medical risk management definitions in a quick and ready fashion.
Acronyms and Abbreviations
AAASC American Association of Ambulatory Surgery Centers
AAHP American Association of Health Plans
ABN advance beneficiary notice
ABQAUR American Board of Quality Assurance and Utilization Review
ACE acute care episode
ACHCE American College of Health Care Executives
ACS American College of Surgeons
ADA Americans with Disabilities Act
ADC average daily census
ADL activities of daily living
ADT Admission/Discharge/Transfer
AHA American Hospital Association
AHIMA American Health Information Management Association
AHRQ Agency for Healthcare Research and Quality
AI average inventory
AIMR Association for Investment Management and Research
AIR assumed interest rate
ALE annualized loss expectancy
ALF assisted living facility
ALOS average length of stay
AMA American Medical Association
AMBAC AMBAC Indemnity Corporation
AMGA American Medical Group Association
ANSI American National Standards Institute
AP accounts payable
APA American Psychiatric Association
APC ambulatory payment classification
APG ambulatory payment group
APR annual percentage rate
AR accounts receivable
ASA American Society of Appraisers
ASC ambulatory surgery centers; also Accredited Standards Committee
ASHA American Surgical Hospital Association
ASO administrative services only
ASTC ancillary service technical component
ATM asynchronous transfer mode
AVG ambulatory visit group
BANTA best alternative to negotiated agreement
BBA Balanced Budget Act of 1997
BBRA Balanced Budget Refinement Act [1999]
BCP business continuity planning
BEA break-even analysis
BEP break-even point
BIPA Benefits Improvement and Protection Act [2000]
BLS Bureau of Labor Statistics
BPD border protection device
BS balance sheet
BSA Bank Secrecy Act
BVS business valuation standard
CA certificate authority
CAC Carrier Advisory Committee
CAS cost accounting standards
CASB Cost Accounting Standards Board
CC common criteria [for IT Security Evaluation —ISO/IEC 15408]; complication or comorbidity [for MS-DRGs]
CCA certified cost accountant
CCC cash conversion cycle
CCEVS common criteria evaluation and validation scheme
CCHIT Certification Commission for Healthcare Information Technology
CCU critical care unit
CDC Centers for Disease Control and Prevention
CDH consumer-directed healthcare
CDHP consumer-directed healthcare plan
CDPM Clinical Data Project Manager
CDSS clinical decision support system
CEO Chief Executive Officer
CF conversion factor
CFA Chartered Financial Analyst
CFO Chief Financial Officer
CFR Code of Federal Regulations
CHAMP Children’s Health and Medicare Protection Act of 2007
CHAMPUS Civilian Health and Medical Program of the Uniformed Services
CHE Certified Healthcare Executive
CHIPS Center for Healthcare Industry Performance Studies
CIA Corporate Integrity Agreement
CIO Chief Information Officer
CIP Customer Identification Program
CIS computer information systems
CLIA Clinical Laboratory Improvement Act
CLT capitation liability theory
CME continuing medical education
CMI case mix index
CMIO Chief Medical Information Officer
CMIS contribution margin income statement
CMN Certificate of Medical Necessity
CMP Certified Medical Planner ™
CMS Centers for Medicare and Medicaid Services [formerly HCFA]
COD cash on delivery
COGME Council of Graduate Medical Education
COH cash on hand
COLA cost of living allowance
CON Certificate of Need
COO Chief Operating Officer
COSO Committee of Sponsoring Organizations
COTS commercial off-the-shelf
CPHQ Certified Physician in Healthcare Quality
CPIM Certificate in Production and Inventory Management
CPI-U Consumer Price Index—urban
CPM critical (clinical) path method
CPOE computerized physician order entry [system]
CPR computer-based patient record
CPT current procedural terminology
CQI continuous quality improvement
CRL Certification Revocation List
CRM customer relationship management
CRVS California Relative Value Studies
CSO Chief Security Officer
CT scan computed tomography scan [also called CAT scan]
CUSIP Committee on Uniform Security Identification Procedures
Candid CIO: Will Weider, CIO of Ministry Health Care and Affinity Health System, offers his perspectives on administration issues in this blog.
Christina’s Considerations: Christina Thielst is a hospital and healthcare administrator and entrepreneur with a deep desire for continually improving the health of the community being served. This is her blog.
Healing Hospitals — Formerly Ask a Hospital President: F. Nicholas “Nick” Jacobs has more than 20 years experience in hospital management, with an acknowledged reputation for innovation and consumer-centered leadership.
Hospital Impact: Part of the Fierce network of health sites, this site is becoming popular among healthcare administrators for its news updates, tips and opinions on health care matters.
Leading the Way to Medical Excellence: the president of McLeod Health non-profit institutions provides weekly insights into his facilities and health care in general.
Let’s Talk Health Care: Bruce Bullen, Interim Chief Executive Officer at Harvard Pilgrim in Massachusetts, provides and open and ongoing conversation about health care administration.
Life as a Healthcare CIO: Dr. John Halamka records his experiences with infrastructure, applications, policies, management, and governance as he supports 3,000 doctors, 18,000 faculty and about three million patients.
Managed Care Matters: Joe Paduda shares his knowledge on managed care for group health, health policy, health research, and medical news for insurers, employers, and healthcare providers.
More than Medicine: Tom Quinn, president and CEO of Community General Hospital in Syracuse, New York, began his career as a hospital kitchen worker. His perspective on administration reflects his knowledge on how hospitals work from every angle.
Running a Hospital: A CEO of a large Boston hospital shares thoughts on hospitals, medicine and health care issues.
St. Joseph Medical Center: Chief Executive Officer at St. Joseph Medical Center in Missouri, Mr. Kashman, provides personal insight into administrative matters and general topics.
Todd’s Perspective: Todd Linden, president and CEO of Grinnell Regional Medical Center, offers insights into medical administration and guest bloggers provide insight into various departments.
Wachter’s World: This blog focuses on hospitals, hospitalists, quality, safety, policy and much more from Robert M. Wachter, MD, Professor and Associate Chairman of the Department of Medicine at the University of California, San Francisco.
Legal Matters
Drug and Device Law: This blog contains an attorney’s personal views (and those of several other Dechert attorneys) on topics that arise in the defense of pharmaceutical and medical device product liability litigation.
Drug Injury Watch: Learn more about drug injury lawsuits from an attorney who represents patients and their families.
FDA Law Blog: Hyman, Phelps & McNamara, P.C. is the largest dedicated food and drug law firm in the country. Their knowledge about laws and regulations governing drugs, medical devices, foods, dietary supplements, and cosmetics is helpful to anyone interested in these topics.
Health Care Law Blog: Bob Coffield’s expertise lies in helping businesses and health care providers weave through a variety of state and federal health care regulations and assisting them in business transactions.
Health Plan Law: This site contains information about group health plans, claims administration and related ERISA fiduciary issues. This site also contains tutorials.
HealthBlawg: this is David Harlow’s popular health care law blog, offering expert insights and easy-to-understand analysis.
Healthcare Law Blog: Holland & Hart’s healthcare practice provides insight into this arena, including HIPAA, Stark law, the Anti-kickback Statute and more.
HIPAA Blog: Join in on this discussion of medical privacy issues often buried in “political arcana.”
HIPAA, HiTech & HIT: This updated blog brings insight into legal issues, developments and other pertinent information that relates to the creation, use and exchange of electronic health records.
HIT Blawg: This blog is focused on national health information technology legal trends and current news on this topic.
Home Care Law Blog: Learn more about legal and policy issues in the home health care, private duty and hospice industries from Gilliland & Markette LLP.
Med Law Blog: This law blog focuses on topics that range from compliance to contracts and from employee benefits to HIPAA and HIT.
Physician Law: This blog provides and easy way to stay on top of current news, updates and useful tips relating to legal issues that affect physicians and non-institutional providers.
eHealth and Health IT
Chilmark Research: This blog provides perspectives on key IT trends in the healthcare sector.
davidrothman.net: David is the Information Services Specialist at the Community General Hospital Medical Library, but he also provides great ideas for 2.0 tools and tips for healthcare industry professionals on this blog.
e-CareManagement blog: Vince Kuraitis, owner of Better Health Technologies, LLC, has a passion for disease management and care coordination that dates back to 1995.
e-HealthExpert: A non-profit organization provides a free and open forum to support the development of expertise in the field of eHealth, Healthcare Information Systems, and Health IT (Clinical IT).
eHealth: John Sharp is an IT Manager for a major medical center in Northeast Ohio, with a focus on ehealth, personal health records, Web 2.0 technologies, Windows Sharepoint Services and project management.
Found In Cache: If you would prefer a professional’s take on social media matters, Web sites and all things technological, then follow Ed Bennett, a technology expert for a Maryland medical care system.
Future Health IT: A health IT and EPR advocate from the UK provides a format to discuss the future of health care and IT.
Informaticopia: This UK blogger provides eclectic news and views on health informatics and elearning.
MedGadget: Stay ahead of the gadget curve with this site, which offers information about the newest health care gadgets on the market as well as emerging medical technologies.
Neil Versel’s Healthcare IT Blog: A healthcare journalist’s provides his views on the major segment of the industry he covers — and, he provides a ton of links to other sites as well.
Schwartz Healthcare IT Blog: A variety of authors from Schwartz Communications provide insights into ways to use IT effectively within healthcare facilities.
The Health IT Channel: For a different perspective on IT and EHR as well as other health care issues, watch a few videos at this site.
The Healthcare IT Guy: The CEO of Netspective, a Java/.NET consultancy that specializes in healthcare IT with an emphasis on e-health, EMRs, data integration, and legacy modernization, supplies tips and information for physicians and healthcare administration.
ACKNOWLEDGEMENTS: To Mackenzie H. Marcinko PhD of iMBA Inc., Perry D’Alessio CPA CMP™ [Hon] New York, NY; and Daniel B. Moisand CFP®, Principal for Moisand Fitzgerald Tamayo, Melbourne, FL.
Posted on March 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Walgreens Boots Alliance says it has agreed to be acquired by private equity firm Sycamore Partners as the struggling retailer looks to turn itself around after years of losing money. Walgreens said Thursday that Sycamore will pay $11.45 per share, giving the deal an equity value just under $10 billion. Shareholders could eventually receive up to an
Posted on March 6, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
March 6th is National Dentist Day, a day to celebrate the men and women who keep our chompers chomping, our gnashers gnashing, and our whites pearly.
Dentists (DDS/DMD) are doctors who specialize in oral health. It’s their job to prevent, diagnose, and treat oral diseases, monitor the growth of our teeth and jaws, and perform surgical procedures on our teeth and mouths!
Dental health is integral to our overall health, so today we salute them not just for keeping our teeth looking good, but keeping our bodies in tip-top shape.
Posted on March 1, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Rx – What Dentists Can’t Do
By Staff Reporters
***
***
Dentists are limited to prescribing medications that address oral and dental health only.
For example, they cannot provide prescriptions for conditions unrelated to dentistry, such as chronic illnesses like diabetes or respiratory infections. Additionally, dentists do not prescribe medications for mental health or hormonal issues.
These limitations ensure that dental professionals focus strictly on oral health and leave more complex medical issues to general physicians or specialists. This distinction helps protect patients from receiving inappropriate or harmful treatments outside the dentist’s expertise.
Posted on February 26, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
BREAKING NEWS
By Staff Reporters
***
***
WASHINGTON, Feb 25 (Reuters) – U.S. President Donald Trump signed an executive order on Tuesday aiming to improve price transparency on healthcare costs by directing federal agencies to strictly enforce a 2019 order he signed during his first term.
The order directs the Departments of the Treasury, Labor, and Health and Human Services to within 90 days come up with a framework to enforce Trump’s 2019 executive order forcing health insurers and hospitals to disclose healthcare cost details.
***
***
This includes requiring the disclosure of actual prices not estimates, update existing guidance or proposing new regulations that ensure price information is standardized, and updating or issuing enforcement policies that guarantee compliance.
“You’re not allowed to even talk about it when you’re going to a hospital or see a doctor. And this allows you to go out and talk about it,” Trump told reporters as he signed the order. “It’s been unpopular in some circles because people make less money, but it’s great for the patient.”
Posted on February 26, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
AMERICAN DENTAL ASSOCIATION
By ADA and Staff Reporters
***
Every day should be about children’s dental health
This is the message behind the ADA’s National Children’s Dental Health Month resources for 2025. Observed nationally each February, the recognition brings together thousands of dedicated professionals, health care providers and educators to promote the benefits of good oral health to children, their caregivers, teachers and many others.
The ADA is offering new materials to celebrate and promote the importance of children’s dental health, not only during the month of February, but all year.
Posters and flyers emphasizing the importance of brushing are available for free download in two kid-friendly, topical designs and two sizes, 8.5″x11″ and 11″x17″. Matching coloring sheets are offered in 8.5″x11″. All materials have instructions for proper brushing and are available in English and Spanish from ADA.org/NCDHM.
***
***
In addition, the ADA’s 2025 Brushing Calendar is available for free download. This 12-month calendar is valuable year-round for promoting healthy behaviors like brushing twice a day with a fluoride toothpaste to help prevent dental disease. Kids can track their daily brushing and flossing routines and exercise their creativity by coloring the calendar image for each month.
Another tool, the NCDHM Program Planning Guide, provides resources for program coordinators, dental societies, teachers and parents to promote the benefits of good oral health to children. The guide includes easy-to-do activities, program planning tips, a sample NCDHM proclamation and more.
“The sooner children understand the value of good oral health habits, the more likely they are to continue these habits well into adulthood,” said ADA President Brett Kessler, D.D.S. “The ADA is proud that NCDHM will once again equip some of the most influential figures in kids’ lives — like parents, educators and health care providers — to help set our nation’s kids on the path to a lifetime of healthy smiles and healthier lives.”
National Children’s Dental Health Month observances began with a one-day event in Cleveland and a one-week celebration in Akron, Ohio, in February 1941. Since then, the concept has evolved into a nationwide program.
The ADA held the first national observance of Children’s Dental Health Day on February 8th, 1949. The one-day event became a week long event in 1955, and in 1981 the program was extended to a month long celebration known today as National Children’s Dental Health Month.
Posted on February 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
ORIGINAL: May 2021 | Matt Cohlmia
As the future of healthcare becomes digitized, the threat of disruption to health systems has never been greater. Despite their best intentions, the flood of new competitors and ever-proliferating modalities of care each compete for patient attention, creating the potential for a fragmented, confusing, and impersonal patient experience. At the same time, health systems possess the breadth of care, the access to data, and the patient trust to become their community’s preferred partner in care.
But to achieve success, they must leverage these resources to create easy to navigate and personalized experiences for their patients, and for the first time ever, those are within reach.
9. We act with honesty, integrity and are always straightforward. 8. We strive to be innovative, creative, iconoclastic, and flexible. 7. We admit and learn from mistakes and don’t repeat them. 6. We work hard always as competitors are trying to catch up. 5. We treat others with dignity and respect. 4. We are the onus of consulting advice for the well being of others. 3. We fight complacency as former success is in the past. 2. The best management styles are timeless, not timely. 1. Our clients are colleagues and always come first.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit a RFP for speaking engagements: MarcinkoAdvisors@outlook.com
Posted on February 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Optometry Doctor [OD]: An optometrist has an Optometry Doctor (OD) degree and can assess overall eye health and the quality of a person’s vision through a comprehensive examination. They diagnose and treat many eye disorders that do not require surgery or further specialized care. An optometrist can also identify symptoms of other health conditions that may affect the eyes, such as diabetes. Some also specialize in a field like pediatric care.
Optometrists [OD] and ophthalmologists [MD/DO] are both eye doctors, but they have different types of training and areas of expertise. If you need an eye exam—and think you may need glasses or contact lenses—an optometrist is a good first choice. To become an optometrist, a person needs to complete four years of additional education after a bachelor’s degree. Sometimes they complete a residency as well.
Now, ODs are licensed doctors and can prescribe medication. However, optometrists have a defined scope of practice that that revolves largely around the eyes. Optometrists can not prescribe all the same medications that your family doctor or ophthalmologist can.
So, if your eye issue requires surgery, or for specific conditions related to your eyes or overall health, you’ll want to visit an ophthalmologist [MD/DO].
On average, an optometrist in the U.S. makes about $131,860 per year, according to 2023 statistics.
Posted on February 18, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITION
By Staff Reporters
***
***
Variable Universal Life Insurance: Permanent life insurance that allows the policyholder to vary the amount and timing of premiums and, by extension, the death benefit. Universal life insurance policies accumulate cash value which grows tax deferred. Within certain limits, policyholders can direct how this cash value will be allocated among sub-accounts offered within the policy.
Several factors will affect the cost and availability of life insurance, including age, health, and the type and amount of insurance purchased. Life insurance policies have expenses, including mortality and other charges. If a policy is surrendered prematurely, the policyholder also may pay surrender charges and have income tax implications. You should consider determining whether you are insurable before implementing a strategy involving life insurance.
Any guarantees associated with a policy are dependent on the ability of the issuing insurance company to continue making claim payments.
Posted on February 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MSFT-HUG Update
By Dr. David Edward Marcinko; MBA MEd
***
***
MSHUG: Microsoft Healthcare Users Group (MS-HUG) unified with the Healthcare Information and Management Systems Society (HIMSS) as part of the HIMSS Users Group Alliance Program in October 2003.
Today, the unification strengthens the commitment of HIMSS and MS-HUG to better serve their members and the industry through a shared strategic vision to provide leadership and healthcare information technology solutions that improve the delivery of patient care.
Posted on February 15, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Bigorexia is a psychological condition and type of body dysmorphic disorder which involves a distorted self-image that focuses specifically on muscle size and physical appearance,” Kara Becker, a certified eating disorder therapist and national director of eating disorder programs at Newport Healthcare, told HuffPost.
With bigorexia, the afflicted person is obsessed with becoming more muscular and preoccupied with the idea that their body isn’t brawny enough ― even if they actually have the physique of a bodybuilder. And, although muscle dysmorphia can affect anyone, it’s more common in males, and research indicates the disorder is on the rise.
In fact, a 2019 study indicated that 22% of adolescent boys engaged in “muscularity-oriented disordered eating behaviors” in an attempt to bulk up or gain weight and found that supplements, dietary changes and even steroid use were common among young adult males.
Posted on February 13, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
The “Second Wind” paradox is a sudden period of increased wakefulness in individuals deprived of sleep that tends to coincide with the individual’s circadian rhythm.
Although the individual is more wakeful and aware of their surroundings, they are continuing to accrue sleep debt and thus are actually exacerbating their sleep deprivation.
Posted on February 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
PharmD – Doctor of Pharmacy
A Doctor of Pharmacy [ParrmD] is the professional degree required to become a pharmacist in the US. Practicing pharmacists complete an average of six years in school—including their pre-pharmacy education—before passing required exams and completing post-graduate training.
Here’s where things often get confusing. The word “pharmacist” is sometimes used in casual conversation to refer to healthcare professionals who aren’t technically licensed to be pharmacists.
For example, pharmacy technicians assist licensed pharmacists. They work behind the counter among the medications right alongside the pharmacist. However, they don’t need a Doctor of Pharmacy to do their job. A pharmaceutical sales representative typically needs four years of a bachelor’s degree with a foundation in chemistry and biology, though this is not always a requirement. Neither of these professionals is technically a pharmacist, although laypeople may mistakenly describe them that way.
And pursuing a PharmD doesn’t always mean you’ll work in a community pharmacy. In fact, just slightly fewer than half of all PharmD recipients end up in this role. Another 15 percent practice in other healthcare settings—hospitals, nursing homes, and managed care centers, for example. Other pharmacy students pursue research roles, government regulation positions, or work in highly specialized areas like oncology or geriatric pharmacy.
A PharmD or RPH [registered pharmacist] fills the electronic or written prescriptions of a MD/DO/DPM/DDS/DMD. They generally can not prescribe drugs or write prescriptions, however.
As of February 01, 2025, the average annual pay of Doctor of Pharmacy in the United States was $196,904. While Salary.com suggests that a Doctor of Pharmacy salary in the US can go up to $236,908 or down to $149,197, most earn between $171,932 and $217,844.
Posted on February 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
DEFINITION BAR SLIDES LEFT TO RIGHT
Understanding Insurance Jargon
1. Premiums
When you purchase an insurance policy, you'll be required to make regular payments, known as premiums. These payments are typically made monthly or annually and are the cost of maintaining your insurance coverage.
2. Deductible
Think of a deductible as the money you have to shell out from your own pocket before your insurance kicks in to help cover your expenses. It's like the upfront cost you need to cover before your insurance really starts working for you.For example, if you have a $500 deductible and make a claim for $1,000, you'll need to pay $500, and your insurer will cover the remaining $500.
3. Policyholder
The policyholder is the person who owns an insurance policy. This individual is responsible for paying premiums and making claims under the policy.
4. Coverage Limit
Every insurance policy has a coverage limit, which is the maximum amount your insurer will pay out for a covered claim. It's crucial to understand your policy's limits to ensure you have adequate coverage.
5. Underwriting
Underwriting is the process insurers use to assess the risk of providing coverage to an individual or entity. It involves evaluating factors such as age, health, and driving record to determine premium rates and eligibility.
Types of Insurance
6. Auto Insurance
Auto insurance provides financial protection in case of accidents, theft, or damage to your vehicle. It's a legal requirement in many places and typically includes liability, collision, and comprehensive coverage.
7. Health Insurance
Health insurance covers medical expenses, including doctor visits, hospital stays, and prescription medications. It can be provided by employers or purchased individually.
8. Homeowners Insurance
Homeowners insurance is like a safety net for your home and stuff. It steps in to help if your place or belongings get damaged or stolen. Plus, it's got your back with liability coverage in case someone gets hurt while on your property.
9. Life Insurance
Life insurance pays out a death benefit to beneficiaries when the policyholder passes away. It can provide financial security to loved ones and cover funeral expenses.
10. Liability Insurance
Liability insurance covers you in case you're responsible for injuring someone or damaging their property. It's often included in auto and homeowners insurance policies.
Navigating Insurance Policies
11. Exclusions
Exclusions are specific events or circumstances that your insurance policy doesn't cover. It's essential to review these carefully to understand what situations won't be reimbursed.
12. Riders
Riders are add-ons to insurance policies that provide additional coverage for specific situations. For example, you can add a rider to your homeowners policy to cover expensive jewelry.
13. Claim
A claim is a formal request to your insurance company for coverage or reimbursement for a loss or damage. It's essential to follow the claims process outlined in your policy.
14. Grace Period
The grace period is the amount of time you have to pay your premium after the due date without your coverage lapsing. Be aware of your policy's grace period to avoid a lapse in coverage.
15. No-Claims Discount
Many insurance companies offer a no-claims discount to policyholders who haven't filed any claims within a specified period. This can lead to lower premiums over time.
Specialized Insurance Terms
16. Subrogation
Subrogation is the process by which an insurance company seeks reimbursement from a third party for a claim it has already paid out. This often occurs in auto accidents when your insurer goes after the at-fault driver's insurance company.
17. Actuary
An actuary is a professional who uses mathematics and statistics to assess risk and set premium rates for insurance policies. They play a crucial role in the insurance industry's financial stability.
18. Adjuster
An insurance adjuster is responsible for investigating claims, evaluating damage, and determining how much the insurance company should pay. They work to ensure fair settlements for policyholders.
19. Premium Credit
Premium credit is a discount offered by insurers to policyholders who meet specific criteria, such as having a good driving record or installing safety features in their home.
20. Salvage Value
When an insured item is damaged or totaled, it may still have some value. Salvage value refers to the amount the insurer can recover by selling the damaged item.
Protecting Your Financial Future
21. Risk Management
Effective risk management involves identifying potential risks and taking steps to minimize or mitigate them. Insurance is one tool in your risk management toolkit.
22. Beneficiary
A beneficiary is the person or entity designated to receive the proceeds of a life insurance policy when the policyholder passes away. It's essential to keep this information up to date.
23. Policy Term
The policy term is the duration for which your insurance policy is valid. It's crucial to renew your policy before it expires to maintain coverage.
24. Umbrella Policy
An umbrella policy provides additional liability coverage beyond the limits of your primary insurance policies. It can protect your assets in the event of a costly lawsuit.
25. Coinsurance
Coinsurance is the percentage of costs that you and your insurance company share after you've met your deductible. It's often seen in health insurance policies.
Insurance in Practice
26. Premium Increase
Your insurance premium may increase due to factors such as claims history, changes in coverage, or external economic conditions. It's essential to shop around for the best rates.
27. Depreciation
Depreciation is the decrease in the value of an asset over time. Insurance policies may account for depreciation when settling claims for damaged property.
28. Reinstatement
If your insurance policy lapses due to non-payment, you may have the option to reinstate it by paying any outstanding premiums and fees.
29. Excess
Excess, also known as a deductible, is the portion of a claim that you're responsible for paying. It's designed to prevent small, frequent claims.
30. Pre-Existing Condition
In health insurance, a pre-existing condition is a medical condition you had before obtaining coverage. Within the framework of the Affordable Care Act, insurance providers are prohibited from refusing coverage or imposing elevated premiums due to pre-existing medical conditions.
Insurance Regulations
31. State Insurance Department
Each state in the United States has a department or commission responsible for regulating insurance within its borders. They oversee insurers' operations and protect consumers.
32. Consumer Reports
Consumer reports provide information on insurance companies' financial strength, customer satisfaction, and claims-handling. They can help you choose a reputable insurer.
33. Guaranteed Renewal
Guaranteed renewal is a provision in some insurance policies that ensures the insurer cannot refuse to renew your policy as long as you pay your premiums.
34. Non-Cancelable Policy
A non-cancelable policy is one that the insurer cannot cancel or change the terms of as long as you pay your premiums. This provides certainty in coverage.
35. Market Conduct Examination
Insurance regulators conduct market conduct examinations to assess insurers' business practices and ensure they comply with laws and regulations.
Insurance for Businesses
36. Business Interruption Insurance
Business interruption insurance provides coverage for lost income and expenses when a covered event, such as a fire or natural disaster, forces your business to close temporarily.
37. Workers’ Compensation
Workers' compensation insurance covers medical expenses and lost wages for employees who are injured on the job. It's typically required by law for businesses with employees.
38. Professional Liability Insurance
Professional liability insurance, often called errors and omissions insurance, protects professionals from liability claims resulting from errors or negligence in their work.
39. Business Owner’s Policy (BOP)
A business owner's policy bundles essential coverages, such as property and liability insurance, into a single policy designed for small businesses. It's a cost-effective option.
40. D&O Insurance
Directors and officers (D&O) insurance protects the personal assets of company leaders in case they are sued for alleged wrongful acts while managing the business.
Advanced Insurance Concepts
41. Aggregate Limit
The aggregate limit is the maximum amount an insurance policy will pay out during a policy term, regardless of the number of claims made.
42. Risk Pooling
Insurance works on the principle of risk pooling, where policyholders collectively share the financial burden of covered losses.
43. Loss Ratio
The loss ratio is a measure of an insurance company's claims payouts compared to its earned premiums. A high loss ratio may indicate financial instability.
44. Surplus Lines Insurance
Surplus lines insurance covers risks that standard insurers won't or can't cover. It's often used for unique or high-risk situations.
45. Rescission
Rescission is the cancellation of an insurance policy retroactively, often due to misrepresentation or fraud on the policyholder's part.
Future of Insurance
46. Insurtech
Insurtech refers to the use of technology, such as artificial intelligence and data analytics, to streamline and improve the insurance industry's processes.
47. Telematics
Telematics devices track driving behavior and can lead to personalized auto insurance rates based on individual habits.
48. Microinsurance
Microinsurance provides affordable coverage to low-income individuals and communities, helping them mitigate risks and protect their assets.
49. Blockchain in Insurance
Blockchain technology can enhance transparency and security in insurance by creating immutable records of policies and claims.
50. Climate Change and Insurance
Climate change poses significant challenges to the insurance industry as it leads to more frequent and severe weather events. Insurers must adapt to these changing risk landscapes.
Insurance is a complex field with a language of its own, but understanding these 50 common insurance terms can help you navigate the world of insurance with confidence. Whether you're looking for auto, health, home, or any other type of insurance, being informed about these terms and concepts is essential to making informed decisions about your coverage.
Posted on February 12, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Blue Cross Blue Shield will soon begin paying out $2.67 billion to customers follow a years-long lawsuit alleging that the health insurance giant broke antitrust laws. The litigation began in 2013, when a class-action lawsuit was filed against more than 35 Blue Cross Blue Shield health insurance plans. The lawsuit claims the company broke antitrust laws by limiting market competition, resulting in increased premiums and reduced options for customers.
US stocks closed mixed on Tuesday as investors assessed more tariff policy shifts from President Donald Trump and looked ahead to upcoming inflation data.
Traders also digested the start of Federal Chair Jerome Powell’s two-day testimony in Congress. In his opening remarks, Powell told lawmakers the Fed is not in a rush to adjust interest rates and reiterated the central bank’s stance of not commenting on trade policy.
The Dow Jones Industrial Average (^DJI) edged around 0.3% higher, while the benchmark S&P 500 (^GSPC) closed just above the flatline. The tech-heavy NASDAQ Composite (^IXIC) pulled back about 0.4%.
Posted on February 10, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
EVIDENCE BASED DENTISTRY
By Staff Reporters
***
***
Evidence Based Dentistry?
Despite the high praise for evidence-based dentistry, there are a number of limitation and criticism that has been given to the process. Chambers DW provides quite a bit of criticism, as well as a number of limitations that evidence-based dentistry provides. In no particular order of importance, a number of mentioned objections towards this format are:
Evidence-based dentistry is too clumsy due to the concept being poorly defined
The implementation of evidence-based dentistry has been distorted by too heavy of an emphasis of computerized searches for research findings that meet the standards of academics
Although EBD advocates enjoy sharing anecdotal accounts of mistakes others have made, faulting others is not proof that one’s own position is correct
There is no systematic, high-quality evidence that EBD is effective
Patient and practitioner values are the shortest leg of the stool. As they are so little recognized, their integration in EBD is problematic and ethical tensions exist where paternalism privileges science over patient’s self-determined best interests.
Although dentists, dental hygienists, and dental assistants may not formally recite the Hippocratic Oath, its principles undeniably apply in their practice, particularly in the high-stakes context of emergency medical care.
By embodying these principles, dental professionals not only fulfill their commitment to ethical patient care but also ensure the safety and well-being of those they serve.
Posted on February 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Implicit or unconscious bias is not intentional, but it has a detrimental impact. Implicit bias in nursing affects nurses’ quality of life and patient outcomes. In a Robert Wood Johnson Foundation study, researchers found that 79% of nurses experienced or observed racism or discrimination from patients and 59% saw or experienced it from colleagues.
Asian and Black nurses are particularly likely to have experienced racial aggression, and 94% of Asian and 93% of Black nurses report that it has affected their mental well-being.
Explore more about implicit bias, including how it impacts nurses and patients. Discover some components of effective implicit bias training for nurses.