Emerging Problems
By Dr. David Edward Marcinko; MBA, CMP™
[Publisher-in-Chief]
According to the Dictionary of Health Insurance and Managed Care, informed consent is the oral and written communication process between a patient and physician that results in the agreement to undergo a particular procedure, surgical intervention or medical treatment.
Unfortunately, a lack of standardization surrounding this process represents a major risk for patients and surgeons, and may lead to inaccurate patient expectations, lost or incomplete consent forms, missing encounter documentation and delays in critical surgeries and procedures.
History: Render S. Davis of Emory University [2008 recipient of the Health Care Ethics Consortium’s Heroes in Healthcare Ethics Award] writes for us in the Business of Medical Practice www.MedicalBusinessAdvisors.com that the concept of informed consent is rooted in medical ethics and codified as a legal principle. It is based on the assertion that a competent person has the right to determine what is done to him or her [self-regulated autonomy].
Rationale: The American Medical Association recommends that its members disclose and discuss the following with their patients:
-
The patient’s diagnosis, if known,
-
The nature and purpose of a proposed treatment or procedure,
-
The risks and benefits of a proposed treatment or procedure,
-
Alternatives (regardless of cost or health insurance coverage),
-
The risks and benefits of the alternative treatments and,
-
The risks and benefits of not the procedure.
The requirements for informed consent are spelled out in statutes and case law in all 50 states. It is a necessary protocol for all hospitals, medical clinics, podiatry practices and ASCs.
Inadequacy of Traditional Consent Forms-to-Date
The typical informed consent process, particularly one that relies solely on traditional generic consent forms, is often inadequate, incomplete or offers the potential for not fully explaining and documenting a particular procedure to a given patient.
Traditional consent forms are subject to errors and omissions, such as missing signatures (patient, provider or witness), missing procedure(s), and missing dates that place the validity of consent at risk. Lost or misplaced forms may result in delayed or postponed procedures often at the expensive of costly operating room time. Moreover, far too many forms are generic in nature and wholly unsuited for a specific patient or increasingly sophisticated medical procedure.
Patient Safety Background
According to the Institute of Medicine’s [IOM] repot, To Err is Human, more than 1 million injuries and nearly 100,000 deaths occur annually in the United States due to mistakes in medical care. Wrong patient, wrong-side, wrong-procedure and wrong-toe surgery are particularly egregious. In fact, these are among several other “never-events” that Medicare, and an increasing number of private insurance companies are refusing to reimburse.
Based on the need to make healthcare safer, the Agency for Healthcare Research and Quality (AHRQ) undertook a study to identify patient safety issues and develop recommendations for “best practices”.
AHRQ Evidence Report
The AHRQ report identified the challenge of addressing shortcomings such as missed, incomplete or not fully comprehended informed consent, as a significant patient safety opportunity for improvement.
The authors of the AHRQ report hypothesized that better informed patients “are less likely to experience errors by acting as another layer of protection.” And, the AHRQ study ranked a more interactive informed consent process among the top 11 practices supporting more widespread implementation.
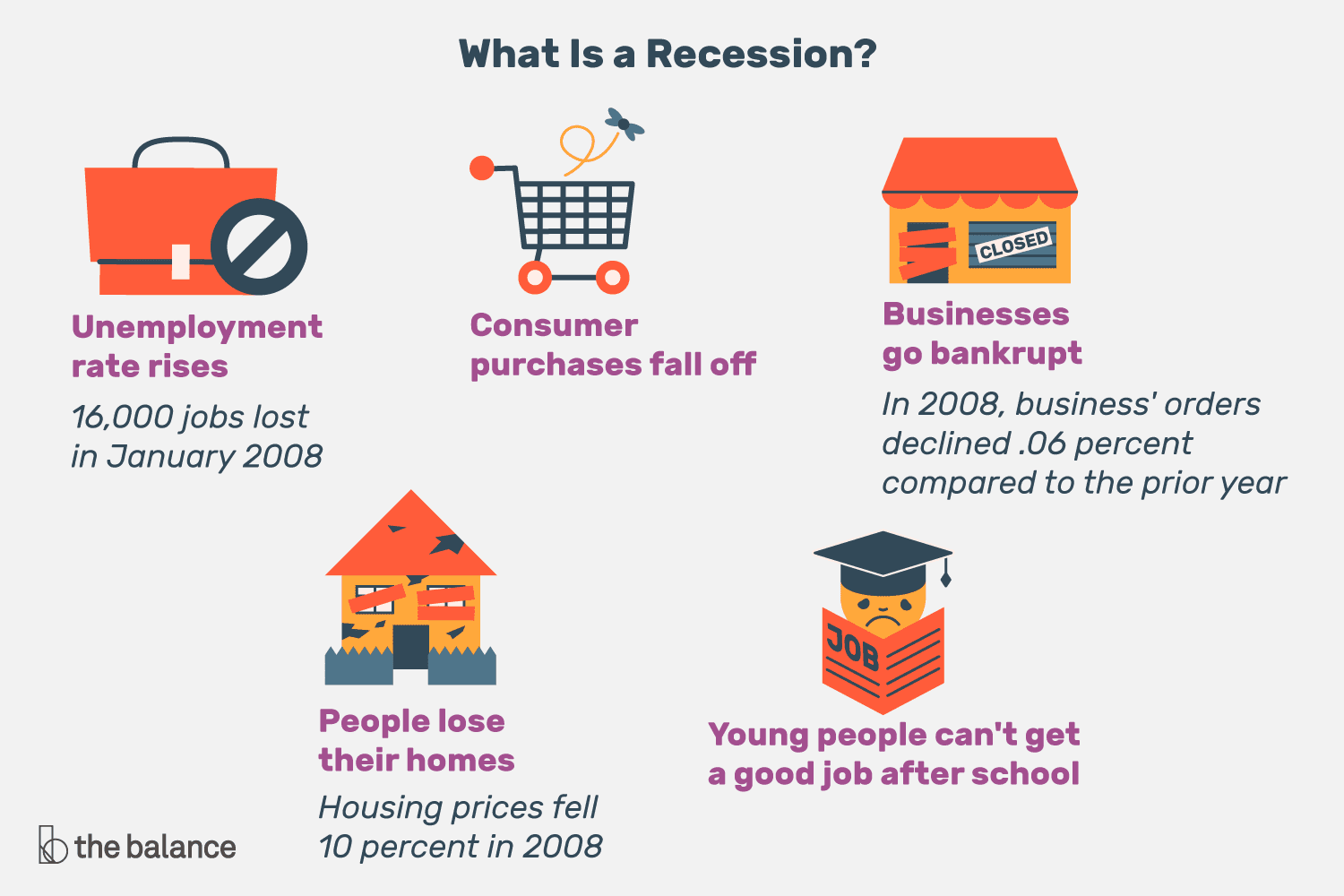
General Accounting Office report found that malpractice insurance premiums were relatively flat for most of the 1990’s, but projections began to increase dramatically to 2010.
Results of Improper Informed Consent
Failure to obtain adequate informed consent, depending on state law, may place surgeons, resident, fellows, ambulatory and office surgery centers, medical clinics and hospitals at risk for litigation ranging from medical negligence to assault and battery.
Proceedings Involving Informed Consent
Informed consent is often a factor in medical malpractice litigation. Some attorneys note that physicians are liable, and that plaintiffs may be able to recover damages, in cases involving improper informed consent, even if the procedure is successful. Inadequate informed consent is often cited as a secondary cause in malpractice complaints and anecdotal evidence suggests this strategy may be especially pursued in podiatric malpractices cases.
Avoiding Litigation
The AMA advises its membership of the following regarding informed consent:
“To protect yourself in litigation, in addition to carrying adequate liability insurance, it is important that the communications process itself be documented. Good documentation can serve as evidence in a court of the law that the process indeed took place. A timely and thorough documentation in the patient’s chart by the physician providing the treatment and/or performing the procedure can be a strong piece of evidence that the physician engaged the patient in an appropriate discussion.”
Impact of Comprehensive Informed Consent Forms
Another study found that providing informed consent information to patients in written form increased comprehension of the procedure. It was also hypothesized that:
-
Better informed patients are more compliant with medical advice and recover faster.
-
Informed consent discussions strengthen physician-patient relationships and increase patients’ confidence in their doctor.
-
Well informed patients are more engaged in their own care, and are thus less likely to experience surgical errors than more passive, or less informed patients.
Medical Ethics
The ethical foundation of informed consent is based on the creation of an environment that supports respect for patients and protects their right to autonomous, informed participation in all collaborative Healthcare 2.0 decisions.
Assessment
Thus, the essence of the informed consent problems of modern medicine today!
More: http://www.ePodiatryConsentForms.com
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:


Filed under: Health Insurance, Health Law & Policy, Insurance Matters, Practice Management, Quality Initiatives, Research & Development, Risk Management, Uncategorized | Tagged: AHRQ, informed consent, medical consent, medical consent forms | 6 Comments »