BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on May 31, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
What’s Up?
[By staff reporters]
According to Wikipedia, the hemline index is a theory presented by economist George Taylor in 1926. The theory suggests that hemlines on women’s dresses rise along with stock prices.
In good economies, we get such results as miniskirts (as seen in the 1920s and the 1960s), or in poor economic times, as shown by the 1929 Wall Street Crash, hems can drop almost overnight.
Non-peer-reviewed research in 2010 supported the correlation, suggesting that “the economic cycle leads the hemline with about three years”.
***
***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Posted on May 30, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
WHAT IS THE “MEDICARE COST CONTROL EFFICIENCY” PARADOX?
The 800 Pound Gorilla in the Medical Treatment Room
By Staff Reporters
Blogger Ezra Klein opined more than a decade ago that one of the dirty little secrets of the health-care system is that Medicare has done a much better job controlling costs than private health insurers. It is a paradox!
DEFINITION: A paradox is a seemingly absurd or self-contradictory statement or proposition that when investigated may prove to be well founded or true.
***
***
QUERY:But, what about Medicare, cost control efficiency, today?
Posted on May 28, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
Payment for order flow, or PFOF, is a tactic some brokerages use to rake in piles of cash. Payment for order flow (PFOF) is a form of compensation, usually in terms of fractions of a penny per share, that a brokerage firm receives for directing orders for trade execution to a particular market maker or exchange. Payment for order flow is common in options markets, and is increasingly found in equity (stock market) transactions.
The “P” in PFOF stands for “payment.” That’s because PFOF gets stock brokers paid. It starts when brokers direct trade orders to a particular e-trading firm (like Mountain Securities, for example) instead of routing the trades straight to exchanges. At that point, the e-trading firm may be able to collect the difference between the bid and the ask price, and the brokerages get a cut of that profit. It’s the proverbial “You scratch your broker’s back through their bespoke Ermenegildo Zegna suit, and they’ll scratch yours.”
According to Lillian Stone, some industry experts argue that PFOF is a conflict of interest. (The practice came under scrutiny last year when US brokers made billions on meme stock trading.) You want your broker to get you the best possible prices during a trade, right? Well, if your broker is incentivized to work with one specific e-trading firm, there’s a chance you may not get the sweetest deal—but they’ll line their pockets all the same.
As human beings, our brains are booby-trapped with psychological barriers that stand between making smart financial decisions and making dumb ones. The good news is that once you realize your own mental weaknesses, it’s not impossible to overcome them.
In fact, Mandi Woodruff, a financial reporter whose work has appeared in Yahoo! Finance, Daily Finance, The Wall Street Journal, The Fiscal Times and the Financial Times among others; related the following mind-traps in a September 2013 essay for the finance vertical Business Insider; as these impediments are now entering the lay-public zeitgeist.
***
Anchoring happens when we place too much emphasis on the first piece of information we receive regarding a given subject. For instance, when shopping for a wedding ring a salesman might tell us to spend three months’ salary. After hearing this, we may feel like we are doing something wrong if we stray from this advice, even though the guideline provided may cause us to spend more than we can afford.
Myopia makes it hard for us to imagine what our lives might be like in the future. For example, because we are young, healthy, and in our prime earning years now, it may be hard for us to picture what life will be like when our health depletes and we know longer have the earnings necessary to support our standard of living. This short-sightedness makes it hard to save adequately when we are young, when saving does the most good.
Gambler’s fallacy occurs when we subconsciously believe we can use past events to predict the future. It is common for the hottest sector during one calendar year to attract the most investors the following year. Of course, just because an investment did well last year doesn’t mean it will continue to do well this year. In fact, it is more likely to lag the market.
Avoidance is simply procrastination. Even though you may only have the opportunity to adjust your health care plan through your employer once per year, researching alternative health plans is too much work and too boring for us to get around to it. Consequently, we stick with a plan that may not be best for us.
Loss aversion affected many investors during the stock market crash of 2008. During the crash, many people decided they couldn’t afford to lose more and sold their investments. Of course, this caused the investors to sell at market troughs and miss the quick, dramatic recovery.
Overconfident investing happens when we believe we can out-smart other investors via market timing or through quick, frequent trading. Data convincingly shows that people who trade most often underperform the market by a significant margin over time.
Mental accounting takes place when we assign different values to money depending on where we get it from. For instance, even though we may have an aggressive saving goal for the year, it is likely easier for us to save money that we worked for than money that was given to us as a gift.
Herd mentality makes it very hard for humans to not take action when everyone around us does. For example, we may hear stories of people making significant profits buying, fixing up, and flipping homes and have the desire to get in on the action, even though we have no experience in real estate.
While financial planning rules of thumbs are useful to people as general guidelines, they may be too oversimplified in many situations, leading to underestimating or overestimating an individual’s needs. This may be especially true for physicians and many medical professionals. Rules of thumb do not account for specific circumstances or factors occurring at a particular time, or that could change over time, which should be considered for making sound financial decisions.
For example, in a tight job market, an emergency fund amounting to six months of household expenses does not consider the possibility of extended unemployment. I’ve always suggested 2-3 years for doctors. Venture capitalist lay-offs of physicians during the pandemic confirm this often criticized benchmark opinion of mine.
As another example, buying life insurance based on a multiple of income does not account for the specific needs of the surviving family, which include a mortgage, the need for college funding and an extended survivor income for a non-working spouse. Again a huge home mortgage, or several children or dependents, may be the financial bane of physician colleaguesand life insurance.
A home purchase should cost less than an amount equal to two and a half years of your annual income. I think physicians in practice for 3-5 years might go up to 3.5X annual income; ceteras paribus.
Save at least 10-15% of your take-home income for retirement. Seek to save 20% or more.
Have at least five times your gross salary in life insurance death benefit. Consider 10X this amount in term insurance if young, and/or with several children or other special circumstances.
Pay off your highest-interest credit cards first. Agreed.
The stock market has a long-term average return of 10%. Agreed, but appreciated risk adjusted rates of return..
You should have an emergency fund equal to six months’ worth of household expenses. Doctors should seek 2-3 years.
Your age represents the percentage of bonds you should have in your portfolio. Risk tolerance and assets may be more vital.
Your age subtracted from 100 represents the percentage of stocks you should have in your portfolio. Risk tolerance and assets may still be more vital.
A balanced portfolio is 60% stocks, 40% bonds. With historic low interest rates, cash may be a more flexible alternative than bonds; also avoid most bond mutual funds as they usually never mature.
There are also rules of thumb for determining how much net worth you will need to retire comfortably at a normal retirement age. Here is the calculation that Investopedia uses to determine your net worth:
If you are employed and earning income: ((your age) x (annual household income)) / 10.
If you are not earning income or you are a student: ((your age – 27) x (annual household income)) / 10.
Posted on May 11, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
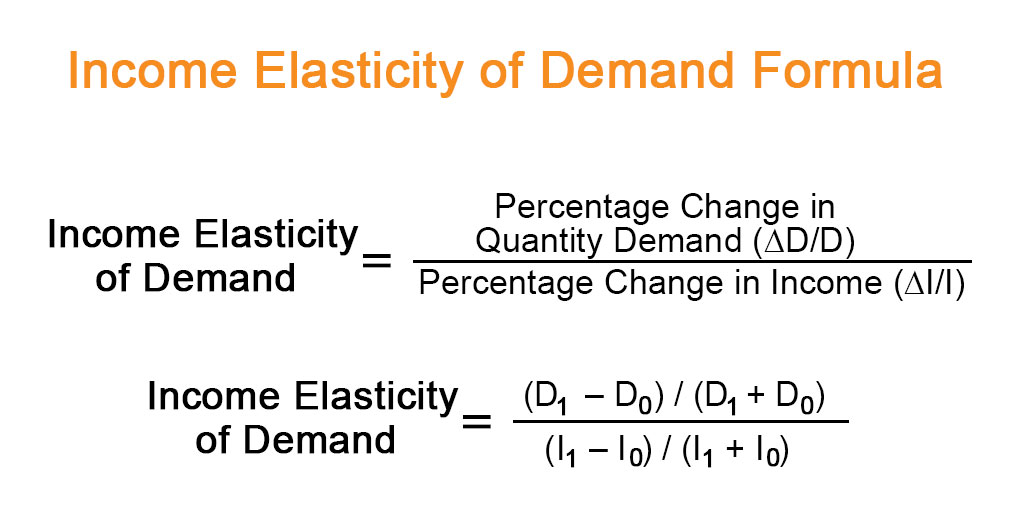
Economic Implications of Pain, Suffering and Imminent Death
***
By Eric Bricker MD
Examples of Inelastic Demand in Healthcare Are: 1) Emergencies 2) Patented Medications for Diseases That Have No Other Alternative Drugs 3) Doctor Specialties Where the Patient Has No Choice in the Services Such As Radiologists, Anesthesiologists and Pathologists [RAP]
Posted on May 11, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
About Frank Knight PhD
[By staff reporters]
In economics, Knightian uncertainty is a lack of any quantifiable knowledge about some possible occurrence, as opposed to the presence of quantifiable risk (e.g., that in statistical noise or a parameter’s confidence interval). The concept acknowledges some fundamental degree of ignorance, a limit to knowledge, and an essential unpredictability of future events.
“Uncertainty must be taken in a sense radically distinct from the familiar notion of Risk, from which it has never been properly separated…. The essential fact is that ‘risk’ means in some cases a quantity susceptible of measurement, while at other times it is something distinctly not of this character; and there are far-reaching and crucial differences in the bearings of the phenomena depending on which of the two is really present and operating…. It will appear that a measurable uncertainty, or ‘risk’ proper, as we shall use the term, is so far different from an unmeasurable one that it is not in effect an uncertainty at all.”
Although some doctors might view a budget as unnecessarily restrictive, sticking to a spending plan can be a useful tool in enhancing the wealth of a practice. And so, I will emphasize keys to smart budgeting and how to track spending and savings in these tough economic times; like today with the stock market busts, venture capitalists invading health care, corona virus the pandemic, aging baby boomer physicians and the great resignation; etc.
There is an aphorism that suggests, “Money cannot buy happiness.” Well, this may be true enough but there is also a corollary that states, “Having a little money can sure reduces the unhappiness.”
Unfortunately, today there is still more than a little financial unhappiness in all medical specialties. The challenges range from the commoditization of medicine, aging demographics, Medicare reimbursement cutbacks, ACA, and increased competition to floundering equity markets, the squeeze on credit and declines in the value of a practice. Few doctors seem immune to this “perfect storm” of economic woes. And then Covid-19, corona, and covid.
Far too many physicians are hurting and it is not limited to above-average earning professionals. However, one can strive to reduce the pain by following some basic budgeting principles. By adhering to these principles, physicians can eliminate the “too many days at the end of the month” syndrome and instead develop a foundation for building real wealth and security, even in difficult economic climates like we face today.
There are three major budget types. A flexible budget is an expenditure cap that adjusts for changes in the volume of expense items. A fixed budget does not. Advancing to the next level of rigor, a zero-based budget starts with essential expenses and adds items until the money is gone. Regardless of type, budgets can be extremely effective if one uses them at home or the office in order to spot money troubles before they develop.
For the purpose of wealth building, doctors may think of this budget as a quantitative expression of an action plan. It is an integral part of the overall cost-control process for the individual, his or her family unit or one’s medical practice.1
How To Prepare A Personal Cash Flow Budget
Preparing a net income statement (lifestyle cash flow budget) is often difficult because many doctors perceive it as punitive. Most doctors do not live a disciplined spending lifestyle and they view a budget as a compromise to it. However, a cash flow budget is designed to provide comfort when there is surplus income that can be diverted for other future needs. For example, if you treat retirement savings as just another periodic bill, you are more likely to save for it.
You may construct a personal cash budget by recording each cash receipt and cash disbursement on a spreadsheet. Only the date, amount and a brief description of the transaction are necessary. The cash budget is a simple tool that even doctors who lack accounting acumen can use. Since it is possible to track the cash-in and cash-out in the same format used for a standard check register, most doctors find that the process takes very little time. Such a budget will provide a helpful look at how well you are staying within available resources for a given period.
We then continue with an analysis of your operating checkbook and a review of various source documents such as one’s tax return, credit card statements, pay stubs and insurance policies. A typical statement will show all cash transactions that occur within one year. It is helpful to establish a monthly equivalent to all items of income and expense. For the purposes of getting started, note items of income and expense by the frequency you are accustomed to receiving or spending them.
What You Should Know About The ‘Action Plan’ Cash Budget
For a medial office, the first operations budget item might be salary for the doctor and staff. Operating assets and other big ticket items come next. Some doctors/clients review their office P&L statements monthly, line by line, in an effort to reduce expenses. Then they add back those discretionary business expenses they have some control over.
Now, do you still run out of money before the end of the month? If so, you had better cut back on entertainment, eating dinner out or that fancy, new but unproven piece of medical equipment. This sounds draconian until you remind yourself that your choice is either: live frugally later or live a simpler lifestyle now and invest the difference.
As a young doctor, it may be a difficult trade-off. By mid-life, however, you are staring retirement in the face. That is why the action plan depends on your actions concerning monetary scarcity, a plan that one can implement and measure using simple benchmarks or budgeting ratios. By using these statistics, perhaps on an annual basis, the podiatrist can spot problems, correct them and continue planning actively toward stated goals like building long-term wealth.2
Useful Calculations To Assess Your Budgeting Success
In the past, generic budgeting ratios would emphasize not spending more than 15 to 20 percent of your net salary on food or 8 percent on medical care. Now these estimates have given way to more rigorous numbers. Personal budget ratios, much like medical practice financial ratios, represent comparable benchmarks for parameters such as debt, income growth and net worth. Although these ratios are still broad, the following represent some useful personal budgeting ratios for physicians.
• Basic liquidity ratio = liquid assets / average monthly expenses. Cash-on-hand should approach 12 to 24 months or more in the case of a doctor employed by a financially insecure HMO or fragile medical group practice. Yes, chances are you have heard of the standard notion of setting enough cash aside to cover three months in a rainy day scenario. However, we have decried this older laymen standard for many years in our textbooks, white papers and speaking engagements as being wholly insufficient for the competitively unstable environment of modern healthcare.
• Debt to assets ratio = total debt / total assets. This percentage is high initially but should decrease with age as the doctor approaches a debt-free existence
• Debt to gross income ratio = annual debt repayments / annual gross income. This represents the adequacy of current income for existing debt repayments. Doctors should try to keep this below 20 to 25 percent.
• Debt service ratio = annual debt repayment / annual take-home pay. Physicians should aim to keep this ratio below 25 to 30 percent or face difficulty paying down debt.
• Investment assets to net worth ratio = investment assets / net worth. This budget ratio should increase over time as retirement approaches.
• Savings to income ratio = savings / annual income. This ratio should also increase over time as one retires major obligations like medical school debt, a practice loan or a home mortgage.
• Real growth ratio = (income this year – income last year) / (income last year – inflation rate). This budget ratio should grow faster than the core rate of inflation.
• Growth of net worth ratio = (net worth this year – net worth last year) / net worth last year – inflation rate). Again, this budgeting ratio should stay ahead of the specter of rising inflation.
In other words, these ratios will help answer the question: “How am I doing?”
Pearls For Sticking To A Budget
Far from the burden that most doctors consider it to be, budgeting in one form or another is probably one of the greatest tools for building wealth. However, it is also one of the greatest weaknesses among physicians who tend to live a certain lifestyle.3
In fact, I have found that less than one in 10 medical professionals have a personal budget. Fear, or a lack of knowledge, is a major cause of procrastination. Fortunately, the following guidelines assist in reversing this microeconomic disaster.
1. Set reasonable goals and estimate annual income. Do not keep large amounts of cash at home or office. Deposit it in an FDIC insured money-market account for safety. Do not deposit it in a money market mutual fund with net asset value (NAV) that may “break the buck” and fall below the one-dollar level. The new limit is $250,000. Track actual bills and expenses.
2. Do not pay bills early, do not have more taxes withheld from your salary than needed and develop spending estimates to pay fixed expenses first. Fixed expenses are usually contractual and usually include housing, utilities, food, Social Security, medical, debt repayments, homeowner’s or renter’s insurance, auto, life and disability insurance, etc. Reduce fixed expenses when possible. Ultimately, all expenses get paid and become variable in the long run.
3. Make it a priority to reduce variable expenses. Variable expenses are not contractual and may include clothing, education, recreational, travel, vacation, gas, cable TV, entertainment, gifts, furnishings, savings, investments, etc. Trim variable expenses by 5 to 20 percent.
4. Use “carve-outs or “set-asides” for big ticket items and differentiate true wants from frivolous needs.
5. Calculate both income and expenses as a percentage of your total budget. Determine if there is a better way to allocate resources. Review the budget on a monthly basis to notice any variance. Determine if the variance was avoidable, unavoidable or a result of inaccurate assumptions. Take corrective action as needed.
6. Know the difference between saving and investing. Savers tend to be risk adverse while investors understand risk and take steps to mitigate it. Watch mutual fund commissions and investment advisory fees, which cut into return-rates. Keep investments simple and diversified (stocks, bonds, cash, index, no-load mutual and exchange traded funds, etc.).4
How To Budget In The Midst Of A [Corona] Crisis
Sooner or later, despite the best of budgeting intentions, something will go awry. A doctor will be terminated or may be the victim of a reduction-in-force (RIF) because of cost containment initiatives of the corona pandemic. A medical practice partnership may dissolve or a local hospital or surgery center may close, hurting your practice and livelihood. Someone may file a malpractice lawsuit against you, a working spouse may be laid off or you may get divorced. Regardless of the cause, budgeting crisis management encompasses two different perspectives: awareness and execution.
First, if you become aware that you may lose your job, the following proactive steps will be helpful to your budget and overall financial condition.
• Decrease retirement contributions to the required minimum for company/practice match. • Place retirement contribution differences in an after-tax emergency fund. • Eliminate unnecessary payroll deductions and deposit the difference to cash. • Replace group term life insurance with personal term or universal life insurance. • Take your old group term life insurance policy with you if possible. • Establish a home equity line of credit to verify employment. • Borrow against your pension plan only as a last resort.
If you have lost your job or your salary has been depressed, negotiate your departure and get an attorney if you believe you lost your position through breach of contract or discrimination. Then execute the following steps to recalculate your budget and boost your wealth rebuilding activities.
• Prioritize fixed monthly bills in the following order: rent or mortgage; car payments; utility bills; minimum credit card payments; and restructured long-term debt.
• Consider liquidating assets to pay off debts in this order: emergency fund, checking accounts, investment accounts or assets held in your children’s names.
• Review insurance coverage and increase deductibles on homeowner’s and automobile insurance for needed cash.
• Then sell appreciated stocks or mutual funds; personal valuables such as furnishings, jewelry and real estate; and finally, assets not in pension or annuities if necessary.
• Keep or rollover any lump sum pension or savings plan distribution directly to a similar savings plan at your new employer, if possible, when you get rehired.
• Apply for unemployment insurance.
• Review your medical insurance and COBRA coverage after a “qualifying event” such as job loss, firing or even after quitting. It is a bit expensive due to a 2 percent administrative fee surcharge but this may be well worth it for those with preexisting conditions or who are otherwise difficult to insure. One may continue COBRA for up to 18 months.
• Consider a high deductible Health Savings Account (HSA), which allows tax-deferred dollars like a medical IRA, for a variety of costs not normally covered under traditional heath insurance plans. Self-employed doctors deduct both the cost of the premiums and the amount contributed to the HSA. Unused funds roll over until the age of 59½, when one can use the money as a supplemental retirement benefit.
• Eliminate unnecessary variable, charitable and/or discretionary expenses, and become very frugal.
Final Notes
The behavioral psychologist, Gene Schmuckler, PhD, MBA, sometimes asks exasperated doctors to recall the story of the old man who spent a day watching his physician son treating HMO patients in the office. The doctor had been working at his usual feverish pace all morning. Although he was working hard, he bitterly complained to his dad that he was not making as much money as he used to make. Finally, the old man interrupted him and said, “Son, why don’t you just treat the sick patients?” The doctor-son looked at his father with an annoyed expression and responded, “Dad, can’t you see, I do not have time to treat just the sick ones.”5
Always remember to add a bit of emotional sanity into your budgeting and economic endeavors.6
Regardless of one’s age or lifestyle, the insightful doctor realizes that it is never too late to take control of a lost financial destiny through prudent wealth building activities. Personal and practice budgeting is always a good way to start the journey.7
The Author:
Dr. Marcinko is a former university endowed chairman and professor, former certified financial planner and has been a medical management advisor for more than two decades. He is the CEO of www.MedicalBusinessAdvisors.com, a health economics and business finance consulting firm.
References:
1. Marcinko DE (Ed). The Business of Medical Practice (Advanced Profit Maximizing Techniques for Savvy Doctors). Springer Publishers, New York, NY, 2000 and 2004 2. Marcinko DE (Ed). Financial Planning for Physicians and Advisors, Jones and Bartlett Publishers, Sudbury, MA, 2005 3. Marcinko DE (Ed). Risk Management and Insurance Panning for Physicians and Advisors, Jones and Bartlett Publishers, Sudbury, MA, 2006. 4. Marcinko DE, Hetico HR. The Dictionary of Health Insurance and Managed Care. Springer Publishing, New York, 2007. 5. Marcinko DE, Hetico HR. The Dictionary of Health Economics and Finance. Springer Publishing, New York, 2008. 6. Marcinko DE, Hetico HR. Healthcare Organizations (Financial Management Strategies). Standard Technical Publishers, Blaine, WA, 2009. Additional Reference 7. Schmuckler E. Bridging Financial Planning and Human and Human Psychology. In, Marcinko DE (Ed): Financial Planning for Physicians and Healthcare Professionals. Aspen Publications, New York, NY, 2001, 2002 and 2003.
DEFINITION: Mental accounting attempts to describe the process whereby people code, categorize and evaluate economic outcomes. The concept was first named by Richard Thaler. Mental accounting deals with the budgeting and categorization of expenditures. People budget money into mental accounts for expenses or expense categories
Mental Accounting is the act of bucketizing investments and then reviewing the performance of the individual buckets separately (e.g. investing at low savings rate while paying high credit card interest rates).
***
Examples of mental accounting are: (1) matching costs to benefits (wanting to pay for vacation before taking it and getting paid for work after it was done, even though from perspective of time value of money the opposite should be preferred0, (2) aversion to debt (don’t like long-term debt for short-term benefit), (3) sunk-cost effect (illogically considering non-recoverable costs when making forward-going decisions).
In investing, treating buckets separately and ignoring interaction (correlations) induces people not to sell losers (even though they get tax benefits), prevent them from investing in the stock market because it is too risky in isolation (however much less so when looked at as part of the complete portfolio including other asset classes and labor income and occupied real estate), thus they “do not maximize the return for a given level of risk taken).
U.S. medical education began in the late eighteenth century as an apprenticeship program in which physicians taught their trade to a few pupils, a pedagogical learning style which relied heavily upon the capacity, skills, and knowledge of the individual physician.[1] However, as learning newly discovered information and utilizing new technologies became more necessary to the industry’s practice, many physicians found the apprenticeship system no longer adequate as a manner of educating the next generation of physicians.[2] As a result, the conventional concept of medical education that originated in the U.S. in the 1750s was manifested through informal courses and demonstrations by private individuals or for-profit institutions. Those individuals who were not satisfied with a typical U.S. medical education, consisting of two identical 16-week lecture terms, might venture to Europe for a more formalized and detailed manner of learning.[3]
One of these students who studied in Europe was William Shippen, who began teaching an informal course on midwifery when he returned to the American colonies in 1762.[4] He later addressed the limitations of what might be taught in one informal course when he began teaching a lecture series on anatomy to help educate those who wished to be a physician, but could not travel abroad. John Morgan, a classmate of Shippen, noticed the potential of his friend’s endeavor and proposed the idea to create a professorship for the practice of medicine to the board of trustees of the College of Philadelphia.[5] Just across town, Thomas Bond, who conceived the idea of, and successfully established, the Pennsylvania Hospital with Benjamin Franklin, recognized the value to allowing medical students to participate in bedside training.[6] When Bond agreed to a partnership with the College of Philadelphia, the University of Pennsylvania became home to America’s first medical school.[7]
In 1893, Johns Hopkins University also made history by housing the first medical school that was able to operate out of a university-owned hospital.[8] The medical school not only encouraged clinical research to be performed by every member of their faculty, but the program also included a clinical research clerkship for every student during their rotation.[9] This program quickly became the model to which schools aspired and set the foundation for national medical education by connecting science and medical research with clinical medicine.[10]
With these early examples of medical schools, America’s field of medical education and clinical medicine made monumental strides. However, the societal pressures, caused by the U.S.’s population growth and demand for educated physicians,[11] did not allow many other universities to build on Johns Hopkins’ or the University of Pennsylvania’s foundation model, and led to the development of medical schools that had their own unique set of entrance and graduation requirements. While some focused entirely on medicine, other schools (termed Studia Generalia) also incorporated law, theology, and philosophy in their curricula.[12] In an attempt to both understand and make uniform the field of medical education, the American Medical Association (AMA) founded the Council on Medical Education (CME) in 1904.[13] The CME created minimum national educational standards for training physicians, and subsequently found that many schools did not meet these established standards.[14] However, the CME did not share the ratings of any of these medical schools “outside the medical fraternity.”[15]
In 1910, the AMA commissioned the Carnegie Foundation for Advancement of Teaching to conduct a study of medical education and schools.[16] Abraham Flexner conducted the inquiry and detailed his findings in what became known as The Flexner Report.[17] In his review of the U.S. medical education system, Flexner found that many of the proprietary medical schools met the AMA’s educational goals, but an imbalance existed between the pursuit of science and medical education.[18] Professors were focused solely on student throughput, and did not ensure a high level of medical training that reflected the developments in the medical industry.[19] As aptly noted by Dr. John Roberts in his book entitled The Doctor’s Duty to the State, “[m]any of you remember the struggle to wrest from medical teachers the power to create medical practitioners with almost no real knowledge of medicine. The medical schools of that day were, in many instances, conducted merely as money-makers for the professors.”[20] As the AMA gained more influence over the provision of healthcare in the U.S., the value and power of medical education also gained recognition. Notably, teaching hospitals had the power to influence the development of their disciplines through their research initiatives, the quality of care they provided, and their ability to operate as an economy of scale, allowing them to dictate the evolution of medical education.[21]
Since the establishment of the first medical school in the U.S., medical education has been the foundation for shaping standards of care in the practice of medicine and defining medical errors as deviations from the norms of clinical care.[22] When Thomas Bond helped establish the University of Pennsylvania medical school, he envisioned a normal day where the physician:
“…meets his pupils at stated times in the Hospital, and when a case presents adapted to his purpose, he asks all those Questions which lead to a certain knowledge of the Disease and parts affected; and if the Disease baffles the power of Art and the Patient falls a Sacrifice to it, he then brings his Knowledge to the Test, and fixes Honour [sic] or discredit on his Reputation by exposing all the Morbid parts to View, and Demonstrates by what means it produced Death, and if perchance he finds something unexpected, which Betrays an Error in Judgement [sic], he like a great and good man immediately acknowledges the mistake, and, for the benefit of survivors, points out other methods by which it might have been more happily treated.”[23]
Originally, students were to study and learn from medical errors and adverse events through medical education as a means of improving the quality of care. However, it is difficult to effectively implement any significant advancement learned through the research and investigation of prior errors in a timely and cost-effective manner. Additionally, physician supply shortages have only increased the amount of patients that a physician must see daily, while simultaneously decreasing the amount of time they can spend with each patient. Although medical education continues to be one of the central underpinnings to the development of the medical industry, outside pressures that shape the clinical practice of physicians continue to limit physician effectiveness in providing quality care to patients.[24]
While improving the quality and rigor of medical education has been a constant focus throughout the history of U.S. medical education, the challenges of replicating it on a scale that produces enough qualified physicians to meet the growing demands of the U.S. population, with constantly changing technologies, has consistently been a central issue. Notably, in the 13 years preceding 1980, the ratio of actively practicing physicians to patients increased by 50%.[25] This increased physician-to-patient ratio led to concerns over quality of care and cost-effectiveness, which in turn caused the creation of a government committee to evaluate physician manpower allocation and distribution. The Graduate Medical Education National Advisory Committee (GMENAC) was first chartered in April 1976, and later extended through September 1980.[26] Its purpose was to “analyze the distribution among specialties of physicians and medical students and to evaluate alternative approaches to ensure an appropriate balance,”as well as to“encourage bodies controlling the number, types, and geographic location of graduate training positions to provide leadership in achieving the recommended balance.”[27] GMENAC produced seven volumes of recommendations regarding physician manpower supply,[28] through the development of several models by which to determine the projected number of physicians that would be needed in the future by different subspecialties to achieve “a better balance of physicians.”[29] Ignoring critics of the report, U.S. medical schools adjusted their enrollment numbers in response to the GMENAC’s recommendations, causing a significant decrease in the supply of new physicians going into the 21st century.
***
[1] “Healthcare Valuation: The Four Pillars of Healthcare Value,” Volume 1, Robert James Cimasi, MHA, ASA, FRRICS, MCBA, CVA, CM&AA, John Wiley & Sons, Hoboken, NJ: 2014, p. 22-23.RR
[2] “Before There Was Flexner,” American Medical Student Association, 2014,
[8] “Time to Heal: American Medical Education from the Turn of the Century to the Era of Managed Care,” By Kenneth M. Ludmerer, New York, NY:
Oxford University Press, 1999, p. 18-19.
[9] “Time to Heal: American Medical Education from the Turn of the Century to the Era of Managed Care,” By Kenneth M. Ludmerer, New York, NY:
Oxford University Press, 1999, p. 18-19.
[10] “Science and Social Work: A Critical Appraisal,” By Stuart A. Kirk, and William James Reid, New York, NY: Columbia University Press, 2002, Chapter 1, p. 2-3.
[11] “The Flexner Report on Medical Education in the United States and Canada in 1910,” By Abraham Flexner, Bethesda, MD: Science and Health
Publications, Inc., p. 6-7.
[12] “Western Medicine: An Illustrated History,” By Irvine Loudon, New York, NY: Oxford University Press, 1997, p. 58.
[13] “Western Medicine: An Illustrated History,” By Irvine Loudon, New York, NY: Oxford University Press, 1997, p. 58.
[14] “Western Medicine: An Illustrated History,” By Irvine Loudon, New York, NY: Oxford University Press, 1997, p. 58.
[15] “Western Medicine: An Illustrated History,” By Irvine Loudon, New York, NY: Oxford University Press, 1997, p. 58.
[16] “U.S. Health Policy and Politics: A Documentary History,” By Kevin Hillstrom, Thousand Oaks, CA: CQ Press, 2012, p. 141.
[17] “The Flexner Report on Medical Education in the United States and Canada in 1910,” By Abraham Flexner, Bethesda, MD: Science and Health
Publications, Inc., p. 3-19.
[18] “The Flexner Report on Medical Education in the United States and Canada in 1910,” By Abraham Flexner, Bethesda, MD: Science and Health
Publications, Inc., p. 3-19.
[19] “The Flexner Report on Medical Education in the United States and Canada in 1910,” By Abraham Flexner, Bethesda, MD: Science and Health
Publications, Inc., p. 3-19.
[20] “The Doctor’s Duty to the State: Essays on The Public Relations of Physicians,” By John B. Roberts, AM, MD, Chicago, IL: American Medical Association Press, 1908, p. 23.
[21] “Time to Heal: American Medical Education from the Turn of the Century to the Era of Managed Care,” By Kenneth M. Ludmerer, New York, NY:
Oxford University Press, 1999, p. 19.
[22] “Science and Social Work: A Critical Appraisal,” By Stuart A. Kirk, and William James Reid, New York: Columbia University Press, 2002, Chapter 1, p. 2-3.
[23] “Dr. Thomas Bond’s Essay on the Utility of Clinical Lectures,” By Carl Bridenbaugh, Journal of the History of Medicine (Winter 1947), p. 14; “The Flexner Report on Medical Education in the United States and Canada in 1910,” By Abraham Flexner, Bethesda, MD: Science and Health
Publications, Inc., p. 4.
[24] “Time to Heal: American Medical Education from the Turn of the Century to the Era of Managed Care,” By Kenneth M. Ludmerer, New York, NY:
Oxford University Press, 1999, p. xxi.
[25] “How many doctors are enough?” By J.E. Harris, Health Affairs, Vol. 5, No. 4 (1986), p.74.
[26] “Report of the Graduate Medical Education National Advisory Committee to the Secretary, Department of Health and Human Services – Volume VII,” Graduate Medical Education National Advisory Committee, Washington, DC: U.S. Government Printing Office, 1981, p. 5, 16.
[27] “Report of the Graduate Medical Education National Advisory Committee to the Secretary, Department of Health and Human Services – Volume VII,” Graduate Medical Education National Advisory Committee, Washington, DC: U.S. Government Printing Office, 1981, p. 73.
[28] “Report of the Graduate Medical Education National Advisory Committee to the Secretary, Department of Health and Human Services – Volume VII,” Graduate Medical Education National Advisory Committee, Washington, DC: U.S. Government Printing Office, 1981, p. 5-6.
[29] “GMENAC: Its Manpower Forecasting Framework,” By D.R. McNutt, American Journal of Public Health, Vol. 71, No. 10 (October 1981), p. 1119.
[30] “Crossing the Quality Chasm: A New Health System for the 21st Century,” Institute of Medicine, National Academy of Sciences, 2001, front matter.
[31] “Overview of Medical Errors and Adverse Events,” By Maité Garrouste-Orgeas, et al., Annals of Intensive Care, Vol. 2, No. 2 (2012), p. 6.
The investment profession has come a long way since the door-to-door stock salesmen of the 1920s sold a willing public on worthless stock certificates. The stock market crash of 1929 and ensuing Great Depression of the 1930s forever changed the way investment operations are run. A bewildering array of laws and regulations sprung up, all geared to protecting the individual investor from fraud. These laws also set out specific guidelines on what types of investment can be marketed to the general public – and allowed for the creation of a set of investment products specifically not marketed to the general public. These early-mid 20th century lawmakers specifically exempted from the definition of “general public,” for all practical purposes, those investors that meet certain minimum net worth guidelines.
The lawmakers decided that wealth brings the sophistication required to evaluate, either independently or together with wise counsel, investment options that fall outside the mainstream. Not surprisingly, an investment industry catering to such wealthy individuals, such as doctors and healthcare professionals, and qualifying institutions has sprung up.
EARLY DAYS
The original hedge fund was an investment partnership started by A.W. Jones in 1949. A financial writer prior to starting his investment management career, Mr. Jones is widely credited as being the prototypical hedge fund manager. His style of investment in fact gave the hedge fund its name – although Mr. Jones himself called his fund a “hedged fund.” Mr. Jones attempted to “hedge,” or protect, his investment partnership against market swings by selling short overvalued securities while at the same time buying undervalued securities. Leverage was an integral part of the strategy. Other managers followed in Mr. Jones’ footsteps, and the hedge fund industry was born.
In those early days, the hedge fund industry was defined by the types of investment operations undertaken – selling short securities, making liberal use of leverage, engaging in arbitrage and otherwise attempting to limit one’s exposure to market swings. Today, the hedge fund industry is defined more by the structure of the investment fund and the type of manager compensation employed.
The changing definition is largely a sign of the times. In 1949, the United States was in a unique state. With the memory of Great Depression still massively influencing common wisdom on stocks, the post-war euphoria sparked an interest in the securities markets not seen in several decades. Perhaps it is not so surprising that at such a time a particularly reflective financial writer such as A.W. Jones would start an investment operation featuring most prominently the protection against market swings rather than participation in them.
Apart from a few significant hiccups – 1972-73, 1987 and 2006-07 being most prominent – the U.S. stock markets have been on quite a roll for quite a long time now. So today, hedge funds come in all flavors – many not hedged at all. Instead, the concept of a private investment fund structured as a partnership, with performance incentive compensation for the manager, has come to dominate the mindscape when hedge funds are discussed. Hence, we now have a term in “hedge fund” that is not always accurate in its description of the underlying activity. In fact, several recent events have contributed to an even more distorted general understanding of hedge funds.
During 1998, the high profile Long Term Capital Management crisis and the spectacular currency losses experienced by the George Soros organization both contributed to a drastic reversal of fortune in the court of public opinion for hedge funds. Most hedge fund managers, who spend much of their time attempting to limit risk in one way or another, were appalled at the manner with which the press used the highest profile cases to vilify the industry as dangerous risk-takers. At one point during late 1998, hedge funds were even blamed in the lay press for the currency collapses of several developing nations; whether this was even possible got short thrift in the press.
Needless to say, more than a few managers have decided they did not much appreciate being painted with the same “hedge fund” brush. Alternative investment fund, private investment fund, and several other terms have been promoted but inadequately adopted. As the memory of 1998 and 2007 fades, “hedge fund” may once again become a term embraced by all private investment managers.
Photo by Alexander Mils
ASSESSMENT: Physicians, and all investors, should be aware, however, that several different terms defining the same basic structure might be used. Investors should therefore become familiar with the structure of such funds, independent of the label. The Securities Exchange Commission calls such funds “privately offered investment companies” and the Internal Revenue Service calls them “securities partnerships.”
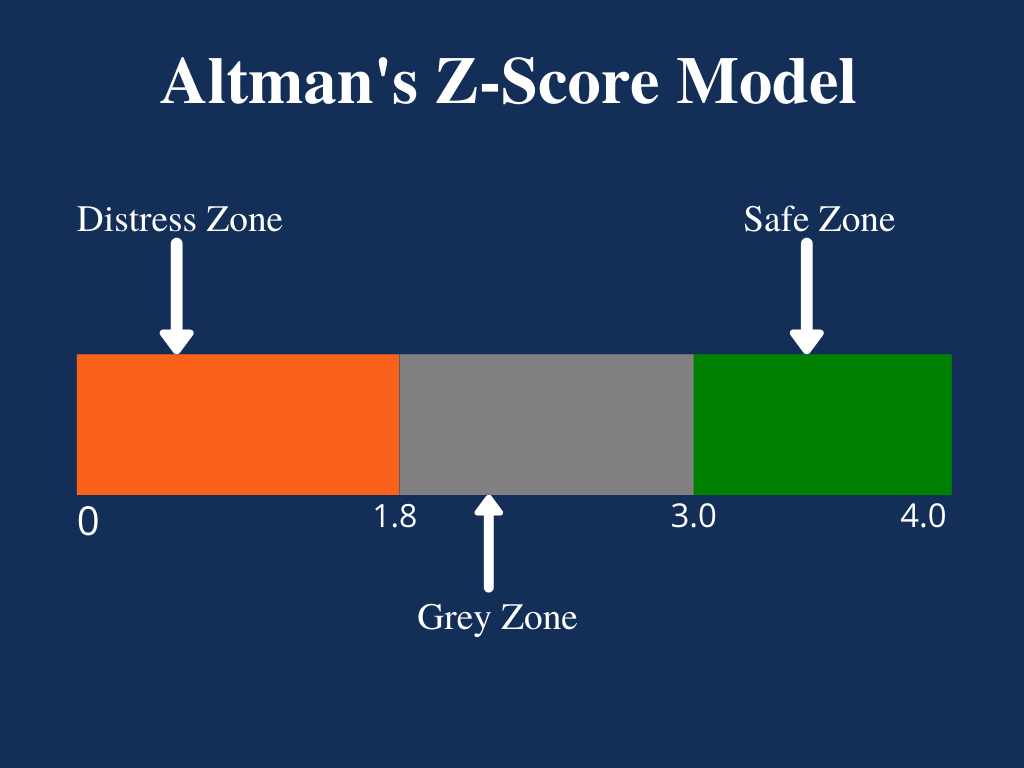
The Zeta Model is a mathematical model that estimates the chances of a public company going bankrupt within a two-year time period. The number produced by the model is referred to as the company’s Z-score (or zeta score) and is considered to be a reasonably accurate predictor of future bankruptcy.
The model was published in 1968 by New York University professor of finance Edward I. Altman. The resulting Z-score uses multiple corporate income and balance sheet values to measure the financial health of a company.
Posted on May 3, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd CMP
***
***
Medicare [Dis] Advantage Plans [Medicare Part C] commenced in 2003 or so and I have railed against them since then. First, for their low physician payments. And then as a patient advocate for the last decade. And, today, for both reasons. As a doctor and independent health insurance agent myself, believe me when I speak thusly.
Now, while Medicare Advantage plans are undoubtedly not the right choice for everyone, insurance companies still say there are some folks who will get exactly what they need from the plans and at a moderate price.
Nevertheless, Ernesto Jaboneta, the IT Director of California-based Medicare insurance agency Agent Pitstop, acknowledged there are many predatory salespeople who will jump to have you join a plan that doesn’t end up helping you in the long run. Still, there are precautions you can take to make falling into this trap less likely.
“The first thing anyone can do is invite along a family member or trusted friend to any appointments with an insurance agent,” Jaboneta told Newsweek. “Don’t feel pressured to decide right away.”
Before you commit to anything, you should compare plans and find out if your doctors will remain in your network. And if you’re unsure about some of the information you received from an insurance agent, you can also call 1-800-MEDICARE for more assistance.
Jaboneta also said there’s a big difference between captive insurance agents and independent agents, as well, and seniors should take note of this.
“A captive agent is an insurance agent who works directly for an insurance carrier,” Jaboneta said. “They have no incentive to compare options outside their own company, which is different than an independent agent who can compare all the options available. In many cases, when a beneficiary calls into an insurance company to find information, they will be talked into enrolling.”
The open enrollment period lasts from October 15th to December 8th, but there’s another enrollment period from January 1st to March 31st for anyone unhappy with their Medicare Advantage plan who wants to switch or revert to Medicare.
INVESTING UPDATE: Managed-care companies are reporting that seniors on Medicare Advantage Part C plans used far more medical services than expected in the final months of 2023. The announcements have sparked two separate selloffs over the past week: The first came January 12th, when UnitedHealth Group announced its fourth-quarter earnings. The second came after Humana just laid out preliminary fourth-quarter results, and said the high utilization trends would have a material impact on its 2024 performance “if current trends continue.”
It is critical to understand and to measure the total cost of capital. Lack of understanding and appreciation of the total cost of capital is widespread, particularly among not-for-profit hospital executives. The capital structure includes long-term debt and equity; total capital is the sum of these two. Each of these components has cost associated with it. For the long-term debt portion, this cost is explicit: it is the interest rate plus associated costs of placement and servicing.
Equity portion
For the equity portion, the cost is not explicit and is widely misunderstood. In many cases, hospital capital structures include significant amounts of equity that has accumulated over many years of favorable operations. Too many executives wrongly attribute zero cost to the equity portion of their capital structure. Although it is correct that generally accepted accounting principles continue to assign a zero cost to equity, there is opportunity cost associated with equity that needs to be considered. This cost is the opportunity available to utilize that capital in alternative ways.
***
***
In general, the cost attributed to equity is the return expected by the equity markets on hospital equity. This can be observed by evaluating the equity prices of hospital companies whose equity is traded on public stock exchanges. Usually the equity prices will imply cost of equity in the range of 10% to 14%.
Almost always, the cost of equity implied by hospital equity prices traded on public stock exchanges will substantially exceed the cost of long-term debt. Thus, while many hospital executives will view the cost of equity to be substantially less than the cost of debt (i.e., to be zero), in nearly all cases, the appropriate cost of equity will be substantially greater than the cost of debt.
Hospitals need to measure their weighted average cost of capital (WACC).
WACC is the cost of long-term debt multiplied by the ratio of long-term debt to total capital plus the cost of equity multiplied by the ratio of equity to total capital (where total capital is the sum of long-term debt and equity).
WACC is then used as the basis for capital charges associated with all capital investments. Capital investments should be expected to generate positive returns after applying this capital charge based on the WACC. Capital investments that don’t generate returns exceeding the WACC consume enterprise value; those that generate returns exceeding WACC increase enterprise value.
Assessment
Hospital executives need to be rewarded for increasing enterprise value.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on May 1, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Dr. David Edward Marcinko MBAMEd CMP
***
According to George Washington University, a hospital chargemaster is a comprehensive list of a hospital’s products, procedures, and services. Everything from prescription drugs to supplies for diagnostic tests has a unique price listing in the chargemaster, making it a go-to document for hospital administrators such as CFOs, clinical documentation improvement specialists, and revenue directors.
Chargemaster usage dates back to the mid-20th century. At that time, fee-for-service (FFS) health insurance plans, which allow patients to direct their medical care by choosing physicians and facilities and paying a portion of the billed total, had just emerged in the U.S. healthcare system.
The chargemaster originally served as something akin to an FFS dictionary, with an entry for virtually anything billable under that economic model of healthcare.
Over time, FFS itself has evolved and been challenged by alternatives like value-based care (VBC). Chargemasters built for FFS have changed accordingly, and they remain fixtures of the modern hospital revenue cycle. A standard chargemaster is a large electronic file containing multiple elements for each entry. These attributes usually include:
The charge for a single unit of the service in question
A Current Procedural Terminology (CPT) code; CPT is the official medical code set of the American Medical Association
Potentially, a Healthcare Common Practice Coding System (HCPCS) code; HCPCS is based on CPT
Alternative CPT and HCPCS codes if needed, e.g. one corresponding only to specific payers
A revenue code associated with the charge
Flag(s) indicating if the entry is scheduled for deletion, active or inactive
An internal reference number within the ledger for accounting purposes
It is critical for physician executives to understand and to measure the total cost of hospital capital. Lack of understanding and appreciation of the total cost of capital is widespread, particularly among not-for-profit hospital and physician executives. The capital structure includes long-term debt and equity; total capital is the sum of these two, and, each of these components has cost associated with it.
For the long-term debt portion, this cost is explicit—it is the interest rate plus associated costs of placement and servicing. For the equity portion, the cost is not explicit and is widely misunderstood. In many cases, hospital capital structures include significant amounts of equity that has accumulated over many years of favorable operations.
Far too many executives wrongly attribute zero cost to the equity portion of their capital structure. Although it is correct that generally accepted accounting principles continue to assign a zero cost to equity, there is opportunity cost associated with equity that needs to be considered. This cost is the opportunity available to utilize that capital in alternative ways.
***
***
In general, the cost attributed to equity is the return expected by the equity markets on hospital equity. This can be observed by evaluating the equity prices of hospital companies whose equity is traded on public stock exchanges. Usually, the equity prices will imply cost of equity in the range of 10%–14%. Almost always, the cost of equity implied by hospital equity prices traded on public stock exchanges will substantially exceed the cost of long-term debt. Thus, while many hospital executives will view the cost of equity to be substantially less than the cost of debt (i.e., to be zero) in nearly all cases, the appropriate cost of equity will be substantially greater than the cost of debt.
Hospitals need to measure their weighted average cost of capital (WACC). WACC is the cost of long-term debt multiplied by the ratio of long-term debt to total capital plus the cost of equity multiplied by the ratio of equity to total capital (where total capital is the sum of long-term debt and equity).
WACC is then used as the basis for capital charges associated with all capital investments. Capital investments should be expected to generate positive returns after applying this capital charge based on the WACC. Capital investments that do not generate returns exceeding the WACC consume enterprise value; those that generate returns exceeding WACC increase enterprise value. Therefore, physician and hospital executives need to be rewarded for increasing enterprise value.
Posted on April 26, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Big Artificial Intelligence Spending Boosts Meta’s Cost Structure!
Meta [Facebook, FB] reported record Q1 revenue yesterday, but it was overshadowed by the billions the company is spending in its efforts to win the AI race and to try to make the metaverse happen. Investors were displeased with the company’s forecast that its spending will rise by $10 billion to support AI development, sending Meta’s stock price down 15% after hours.
Now, the metaverse is a vision of a virtual reality where people can socialize, work, play, and explore in immersive digital spaces.
But CEO Mark Zuckerberg urged them to keep the faith, saying, “We’ve historically seen a lot of volatility in our stock during this phase of our product playbook.”
First held on April 22, 1970, it now includes a wide range of events coordinated globally by EARTHDAY.ORG (formerly Earth Day Network) including 1 billion people in more than 193 countries.[ The official theme for 2024 is “Planet vs. Plastics.” 2025 will be the 55th anniversary of Earth Day.
Posted on April 17, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
If you need a reprieve to prevent the government from raiding your bank account, you’re not alone—the IRS expects 19 million people to file for an extensionthis year. The agency will automatically grant you a six-month extension, although it’s recommended you remit a payment by April 15th if you expect to owe money to avoid interest and penalties. The good news is you probably won’t have to fork over as much as Mark Cuban, who said he is sending the IRS $288 million today and is proud to pay his fair share.
The stock market is coming off its worst week of the year, and the road ahead is no less bumpy. A direct military confrontation between Iran and Israel has investors on edge about a wider regional war that threatens energy supplies. Amid the uncertainty, safe-haven assets are seeing major interest: The US dollar just had its best week in more than 18 months.
Questions – from doctors – like these remind me that the workings of the financial services industry which I tend to take for granted but can be confusing to people outside the field.
The following analogy may help to explain.
Orchestra Analogy
Think of an orchestra. The investment adviser is the equivalent of the director/conductor and the money managers are the instrumentalists. Each one is a specialist who plays a particular type of instrument, and it takes a variety of these specialists to make up the orchestra.
Specialists
The broad specialties are the types of instruments, such as strings, brass, winds, and percussion. These are the equivalent of fund managers who specialize in asset classes like equities, bonds, real estate, commodities, and absolute returns.
Sub-Specialists
Within each specialty are a variety of subspecialists. Winds, for example, include clarinets, oboes, and saxophones—which are further divided into alto, soprano, tenor, and bass. The brass section has French horns, trumpets, and trombones. The divisions and sub-divisions go on and on. Similarly, within the various asset classes are a great many mutual fund managers who specialize in narrower subcategories.
Conductor
The task of the orchestra conductor-director is to pick, not just the best musicians, but the best mix of musicians. A group with only trumpets or every subspecialty of percussion, no matter how skilled, isn’t an orchestra. Before auditioning a single musician, the director’s first task is to clarify the purpose of the ensemble being created. A different mix of instruments will be required for a symphony, a marching band, an intimate chamber group, or a dance band. It all depends on what the audience wants.
The conductor-director needs to weigh the various musicians’ abilities against their cost and their specific specialties against the needs of the orchestra. When the right mix of players has been chosen, the director needs to pick the appropriate music, assemble the group, and rehearse. The director’s talent, experience, and leadership skills all serve to help the right players produce the right sound for their audiences.
***
***
It takes similar coordination and skill to put together the right mix of asset classes and mutual fund managers to produce the best results for various clients, especially since there are some 17,000 mutual funds to choose from.
Fees
Just as both the orchestra director and the musicians are paid based on their skills and their work, both mutual fund managers and investment advisers are paid based on the assets they manage. Mutual fund managers earn 0.05% to 3.0%. Financial advisers earn 0.30% to 3.0%. An informed consumer could pay as low as 0.35% while an uninformed consumer could pay up to 6% a year, which would eat up most of the investment returns.
One essential responsibility for an adviser, then, is to choose mutual fund managers whose fees are low.
However, the cost of the mutual fund manager isn’t the be-all and end-all. One must also weigh performance, just as an orchestra director might pay more to get an outstanding musician who would add significant value to the performances.
Example:
For example, my firm’s overall average fee for mutual fund managers is 0.5%. We could get that as low as 0.1%, which might be impressive at first glance.
However, we would give up 0.25% to 1.00% of net return in some areas, resulting in poorer outcomes for the clients.
***
***
Assessment
Skilled direction of an orchestra is obviously more art than science. Skilled coordination of mutual fund managers is the same. Both require knowledge, integrity, and commitment to the quality of the final product.
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on April 13, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Medial Office Equipment Interest Rate Costs
Dr. David E. Marcinko; MBA, MEd, CMP™
[Publisher in Chief]
Physicians, administrators and healthcare entrepreneurs are aware of the compounding effect of interest.However, since interest is deductible as a medical office business expense, many seem to forget about it despite the fact that it must be continually paid until the asset is either purchased or otherwise disposed.
So, what are the various types of interest rates important to the medical practitioner and commodity – money?
[1] Simple Interest
Simple interest is merely the pro rata interest on a loan or deposit and represents the most basic interest rate type.
For example, for every $100 Dr. Bill borrows at 12 percent annual interest, he pays twelve dollars per year. The interest is calculated by multiplying the principal or original amount, by the interest rate in decimal form (100 x .12).
[2] Add-On Interest
Add on interest immediately attaches the annual interest amount, to the principal amount, at the beginning of the payment period. Payments are then made according to the number of years required.
The following formula is useful:
Add-on-Interest minus Payment = Total Interest on Balance/Number of Payments
For example, if Dr. William Needy borrows $10,000 at 8 percent add-on interest, he will repay $10,000 plus $ 800 ($10,000 x 8%) or $10,800, divided by twelve months, for a total of $900 per month, since $ 900/month x 12 months equals $10,800.
[3] Discounted Interest
When using the discounted interest method, the interest amount is deducted from the principal right up front. Notice that this is the opposite of add-on-interest that is applied up front.
For example, if Dr. Bill borrows the same $ 10,000 at a discounted interest rate of 8 percent, he will only receive a $9,200 loan, since $10,000 – $800 is $9,200.
Obviously, the discount method is the most expense way to borrow money.
[4] Annual Percentage Rate
Most financial institutions advertise an annual percentage rates (APR) for loans, deposits and investments. The APR is the periodic interest rate multiplied by the number of periods a year. If the APR is 12 percent, and interest is compounded monthly, you receive (or pay) 1 percent of your balance each month, and the balance shifts with each compounding.
For example, if Dr. Bill deposits $ 100 dollars at 12 percent APR compounded monthly, he receives $ 1 interest the first month (1% of $100), $1.10 the second month (1% of $101), and so forth. If compounding is daily, the interest accumulates at the rate of 1/365 of the APR each day.
Unless interest is compounded annually, the APR will be lower than the effective annual interest rate, discussed below.
[5] Effective Interest Rate
It is important to differentiate between the effective interest rate and the APR, which is often the most prominent figure in advertisements for medical business equipment, consumer goods and financial services (loans, annuities, IRAs, CDs, investment analysis, college funding or retirement planning). Although the APR is the periodic interest rate multiplied by the number of periods per year, the effective annual interest rate is the periodic rate, compounded.
In our case, if the APR is 12 percent, compounded monthly, the monthly interest rate is 1 percent and the effective annual rate is the monthly rate compounded for 12 periods.
Therefore, if your calculation is for a single year, you can treat the effective rate as simple interest. If you deposit (or borrow) $1,000 at 12 percent APR, the effective rate is 12.68 percent, and interest for the first year is about $126.80 (12.68% of $1,000).
For longer periods, you can use the effective interest rate as the periodic interest rate, compounded annually.
[a] “Rule of 72” (Double your Money)
The number of periods required to double a lump sum of money can be quickly estimated by using what is known as the “Rule of 72”. To get the number of periods, usually years, just divide 72 by the periodic interest rate, expressed as a whole number (not a decimal).
For example, if the annual interest rate is 10 percent, it will take about 7.2 years (72/10) to double any lump cache of money. Conversely, you can also calculate the interest rate required to double your money in a given period by dividing 72 by the term.
Thus, to double your money in ten years, you need to earn about 7.2 percent annual interest (72/10) = 7.2%).
[b] “Rule of 78”
According to this method, interest is front end loaded like a home mortgage, or office condominium, to discourage prepayment of a loan and consequently preserve the lender’s profit. In other words, it is a method of calculating installment loan interest rebates.
The number 78 comes from an approved method of accelerated tax depreciation, known as the “Sum of the Years Digits” (SOYD) method (i.e., 12 + 11 + 10 + 9 . . . = 78). This fact is important because, throughout the period of a loan, even though the payments are all the same, the portions that are interest and principal are very different.
Using this method for a one year loan shows that, in the first payment, 15.38 percent of the interest due is paid off, and by the sixth month, 73.08 percent of the interest is paid off. This means, that if a physician makes a one year equipment loan with a total interest charge of $ 100 and pays the loan off in full with the sixth payments, he or she will not get an interest rebate of $ 50, but only $ 26.92, since $ 73.08 of the interest has already been prepaid.
Most ethical lenders use simple interest rates for loan rebates, and the Rule of 78 is unfair according to many authorities.
[c] “Rule of 116”
A derivative of the Rule of 72 is the Rule of 116. This determines the number of years it takes for a principal amount to be tripled and is calculated by dividing the annual interest rate into 116.
The Rules of 72 and 78 are very handy for figuring the amount of interest payments made or growth of funds invested. They can also be used in reverse to calculate at what rate of interest money must be invested to double or triple in a certain number of years.
[6] Medical Equipment Payback Cost Analysis
The payback period, expressed in years, is the length of time that it takes for the medical equipment investment to recoup its initial cost out of the cash receipts it generates. The basic premise is that the quicker the cost of an investment can be recovered, the better the investment is. It is most often used when considering equipment whose useful life is short and unpredictable.
When the same cash flow occurs every year, the formula is as follows:
Investment Required / Net Annual Cash Inflow = Payback Period
Thus, in today’s tightening medical reimbursement atmosphere, practice cost control and expense reduction is the easiest method to increase medical office profitability. Keeping the cost of the commodity money in the form of interest rate charges, as low as possible, will assist in this endeavor
Assessment
And so, how have these rules affected your medical office borrowing costs; if at all? Does these principles apply to the medical student loan crisis, today?
Posted on April 9, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Versus Di-Versification
BUSINESS MANAGEMENT: The term “diworsification” was coined by legendary investor Peter Lynch in his book, One up on Wall Street, to describe the over-expansion of a company into new growth projects and businesses they do not fully understand and which do not align with the company’s core competencies.
PORTFOLIO MANAGEMENT: The term diworsification has since grown to also refer to over-diversifying an investment portfolio in such a way that it reduces the overall risk-return characteristics.
Posted on April 4, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Bertalan Meskó, MDPhD
***
***
What are you going to do 10-20 years from now? We toyed with the idea and came up with a list of healthcare jobs we think will be born in the coming decades. In case you want to become an organ designer or an end-of-life therapist. OR telesurgery VR planner.
And before you say I’m looking too far into the future, let me remind you that researchers are experimenting with a computer made of DNA-coated microbeads, with wireless charging of electronic implants, an Osaka hospital uses smart glasses to connect remote teams, while the FDA cleared an A.I. software automatically flagging cases of pneumothorax.
I hope you will find the newsletter useful!
Best regards, Bertalan Meskó, MD PhD The Medical Futurist
Posted on April 2, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
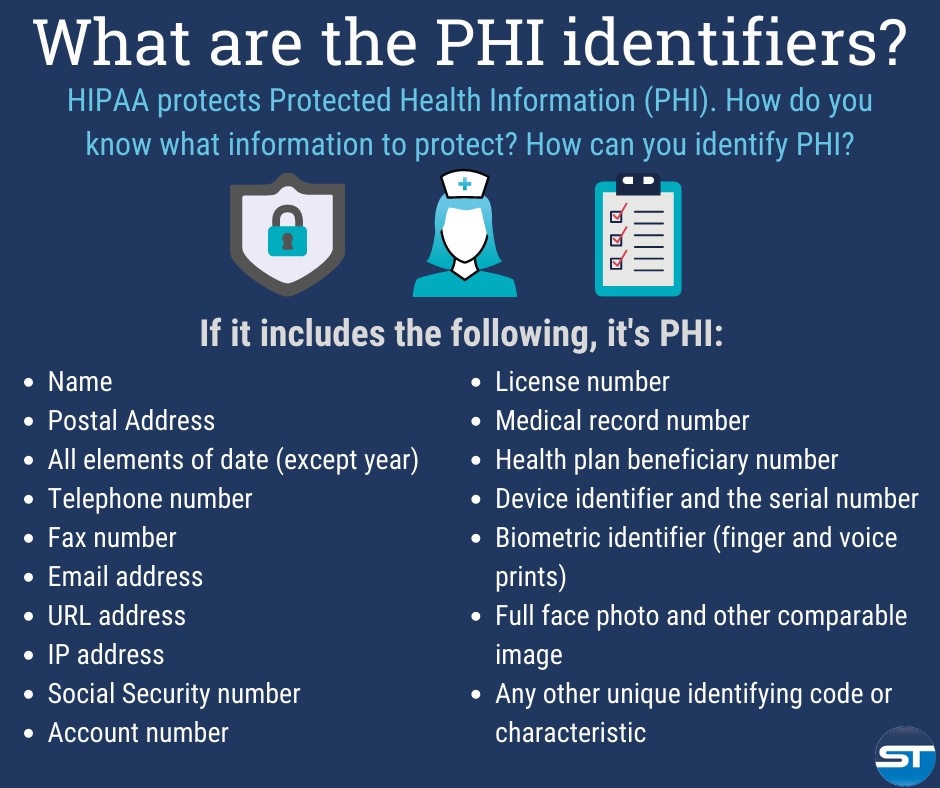
The Designated Medical Record Set [DMRS]: Contains medical and billing records and any other records that a physician, hospital, clinic and/or medical practice utilizes for making decisions about a patient; a hospital, emerging healthcare organization, or other healthcare organization. It serves to define which set of information comprises “protected health information” and which set does not; or contains medical or mixed billing records, and any other information that a physician and/or medical practice utilizes for making decisions about a patient.
It is up to the hospital or healthcare organization to define which set of information comprises “protected health information” and which does not though logically this should not differ from locale to locale. The patient has the right to know who in the lengthy data chain has seen their Protected Health Information. This sets up an audit challenge for the medical organization, especially if the accountability is programmed, and other examiners view the document without cause.
Posted on March 29, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
DIVIDEND REINVESTMENT PLANS
By Staff Reporters
***
DEFINITION
DRIPs are merely an automated strategy in which a company’s dividends are reinvested into additional shares of that company. Instead of being paid dividends in cash, you get additional shares of ownership in the company.
There are three ways to get involved in DRIPs: directly through the company, through your broker, or through a transfer agent.
Company-run DRIPs are generally only available through large, blue-chip dividend stocks.That’s because smaller companies don’t want to take on the overhead costs of tracking all their shareholders and going through the paperwork headache of calculating how much each one gets in dividends and additional fractional shares. The company benefits from gaining an additional source of capital, but most of all in creating a more stable base of shareholders, ones who are less likely to panic and sell during a market decline. This can help decrease the volatility of a company’s shares.
Finally, most large discount brokers, such as Scottrade, TD Ameritrade, and E*Trade, also offer DRIPs, though with different requirements and limitations.
While dividend reinvestment is powerful, there are a couple reasons why you might not want to reinvest your dividends.
DRIPs Drawback 1: You may need the dividend income The most obvious reason is that you need the income. If you’re in the “distribution” phase of your investing life, dividends are a perfect source of passive income. Income from qualified dividends is taxed at the long-term capital gains rate (currently 15% for investors who are in the 25% to 35% tax bracket for ordinary income, 0% for taxpayers in a lower bracket and 20% for those in the highest bracket). So if you’re going to be looking to your portfolio for income every month anyway, it makes sense to have that cash deposited in your account.
DRIPs Drawback 2: You may need to reallocate your positions You might also choose to stop reinvesting your dividends for allocation reasons. Reinvesting your dividends, through DRIP plans or otherwise, will cause your stock positions to grow over time, and if you’ve owned a particular issue for a long time, it may already be a large enough percentage of your portfolio. Higher-yielding positions will grow faster, which can throw your allocations out of whack pretty quickly. So once a stock position is as big as you want it to get (for now) feel free to turn off dividend reinvestment for that position, and either enjoy the extra income or save up the cash to invest in other stocks.
DRIPs Drawback 3: You may not want to buy that stock at that time Finally, you may also have stock-specific reasons not to reinvest dividends—if a stock is temporarily overvalued, or you simply don’t want to buy any more of it at current prices.
But bottom line, reinvesting dividends through a broker or by signing up for DRIP plans directly through the dividend-paying companies, is a surprisingly powerful tool to passively improve your investment returns.
***
NOTE: Former Microsoft CEO Steve Ballmer is on pace to earn $1 billion in dividends annually from his massive 4% stake in the software company.
Steve Ballmer is on pace to collect annual dividend payments of $1 billion from Microsoft.
He is the former CEO of Microsoft and is the largest individual shareholder of the software giant.
Ballmer’s Microsoft stake has surged to a value of $128 billion this year following Microsoft’s 55% stock rally.
TERMS & DEFINITIONS FOR PHYSICIANSAND ALL INVESTORS:
PRUDENT BUYER: The efficient purchaser of market balance between value and cost.
PRUDENT MAN RULE: An 1830 court case stating that a person in a fiduciary capacity (a trustee, executor, custodian, etc) must conduct him/herself faithfully and exercise sound judgment when investing monies under care. “He is to observe how men of prudence, discretion and intelligence manage their own affairs, not in regard to speculation, but in regard to the permanent distribution of their funds, considering the probable income as well as the probable safety of the capital to be invested.” Allows for mutual funds and variable annuities.
PRUDENT INVESTOR RULE: A fiduciary is required to conduct him/herself faithfully and exercise sound judgment when investing monies and take measured and reasonable investment risks in return for potential future rewards. Allows for mutual funds, stocks, bonds, variable annuities asset allocation & Modern Portfolio Theory.
EDITOR’SNOTE: We interviewed noted authority Ben Aikin AIF® on this topic more than a decade ago. He was ahead of his time regarding fiduciary accountability and we appreciate his insights.
Posted on March 27, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
A stalking horse bid is an initial bid on the assets of a bankrupt company. The bankrupt company will choose an entity from a pool of bidders who will make the first bid on the firm’s remaining assets. The stalking horse sets the low-end bidding bar so that other bidders can’t underbid the purchase price.
The term “stalking horse” originates from a hunter trying to be concealed behind either a real or fake horse.
A stalking horse bid is an initial bid on the assets of a bankrupt company, setting the low-end bidding bar so that other bidders can’t underbid the purchase price.
Other buyers can submit competing offers following the stalking horse bid.
A stalking horse bidder is afforded various incentives, such as expense reimbursements and breakup fees.
***
On December 17th, 2023, after defaulting on a $617 million loan, Ebix, Inc of Atlanta Georgia, declared Chapter 11 bankruptcy. Then, Ebix Reaches “Stalking Horse” Sale Agreement for Life Insurance and Annuity Business with Zinnia to Ensure Successful Recapitalization Efforts in 2024.
Posted on March 27, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
Types of Checks
A cashier’s check is a check drawn from the bank’s own funds, not yours, and signed by a cashier or teller. Unlike a regular check, the bank, not the check writer, guarantees payment of a cashier’s check. A cashier’s check can also be called an official check.
A certified check is a personal check that the payer’s bank has certified to be legitimate and has earmarked the funds for the check. It’s a type of “official” payment. People often confuse certified checks with cashier’s checks. … Then, the bank prints a check against the funds they are holding.
A money order is a method of paying for something with cash using a check from a third party. You pay for the money order, and the third party issues you a check that you can give or send to someone. This person deposits the money order in their bank account or exchanges it for cash at a business or post office.
A bank draft is a negotiable instrument where payment is guaranteed by the issuing bank. Banks verify and withdraw funds from the requester’s account and deposit them into an internal account to cover the amount of the draft. A seller may require a bank draft when they have no relationship with the buyer.
Posted on March 26, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Markets: The stock market kicked off its short trading week down as some investors questioned the enthusiasm around the Fed’s recent assurances that it’s still planning three rate cuts this year.
But Digital World Acquisition Corporation roared as the shell company that’s merging with Donald Trump’s Truth Social and will begin trading under its new ticker, DJT, today.
Digital World Acquisition Corp. (Nasdaq: DWAC) is a special purpose acquisition company formed for the purpose of effecting a merger, capital stock exchange, asset acquisition, stock purchase, reorganization or similar business combination with one or more businesses.
The more expensive something is – the less likely you are to use it. This relationship between price and product utility is graphed as an “inverted U.”
Posted on March 17, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
What is the Point?
At the ME-P, we love to educate and learn. So, here they are in brief.
In the Beginning
St. Patrick’s Day started out as a religious feast holiday celebrating the life of St. Patrick, a Christian missionary from Britain who is credited with bringing Christianity to Ireland.
And Today
Now, it’s a hodgepodge of non-religious celebrations of Irish culture, folklore and superstition. Oh, and let’s not forget [responsible] drinking.
Assessment
At the very least, you’re supposed to wear green, the national color of Ireland. If you want to get more involved, you could join one of hundreds of parades nationwide. The largest St. Patrick’s Day parade in the world is in New York City, with 150,000 marchers in a typical year. Other popular activities involve dyeing things green … everything from pancakes and beer to the Chicago River and the White House fountain.
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on March 16, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
Zeno of Elea was a pre-Socratic Greek philosopher of Magna Graecia and a member of the Eleatic School founded by Parmenides. Aristotle called him the inventor of the dialectic. He is best known for his paradoxes, which Bertrand Russell described as “immeasurably subtle and profound”
Now, Zeno’s paradoxes are a set of philosophical problems generally thought to have been devised to support Parmenides’ doctrine that contrary to the evidence of one’s senses, the belief in plurality and change is mistaken, and in particular that motion is nothingbut an illusion.
Posted on March 14, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Each Pi Day, we recall Akira Haraguchi, who in 2016 set the unofficial world record for reciting the most digits of pi: 100,000 over more than 16 hours. He did it by mentally linking each digit with a syllable and creating a collection of epic stories from the words those syllables formed.
Posted on March 5, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
The Goodhart Principle, and related
[By staff reporters]
***
Goodhart’s law is a sociological analogue of Heisenberg’s uncertainty principle in quantum mechanics. Measuring a system usually disturbs it. The more precise the measurement, and the shorter its timescale, the greater the energy of the disturbance and the greater the unpredictability of the outcome.
***
***
***
CAMPBELL’S LAW:
“The more any quantitative social indicator is used for social decision-making, the more subject it will be to corruption pressures and the more apt it will be to distort and corrupt the social processes it is intended to monitor.”
Posted on March 4, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Spiked in 2023
By Staff Reporters
***
***
Healthcare company bankruptcies spiked in 2023 amid high interest rates, rising labor and supply costs, and an uptick in denials from payers, according to a January report from healthcare restructuring firm Gibbins Advisors.
For example, Seventy-nine healthcare companies filed for bankruptcy in 2023—the highest number since 2019, which saw 51 bankruptcies, according to the report. The volume of bankruptcies last year was nearly 2x as high as 2022 and over 3x the level seen in 2021.
“We saw a dramatic increase in healthcare bankruptcy filings in 2023, continuing the trend which began in mid-2022,” Clare Moylan, co-founder and principal at Gibbins Advisors, said in a statement. “Key observations from 2023 are the return of large bankruptcy cases with over $100 million in liabilities, and a spike in hospital filings, both of which appear to primarily be a result of Covid-19 pandemic-related protections ending.”
Posted on February 28, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Pay for Performance Initiatives
[By Staff Writers]
Of course, consumer directed healthcare trends and fee transparency increasingly mandate physician economic accountability, such as in the P4P initiatives, but CMS may also begin profiling physicians and targeting those it deems inefficient sometime next year, as well.
In May 2007, Herbert Kuhn, acting deputy administrator of CMS, told a House subcommittee that the agency will have the data and computer capacity available to do tracking as soon as mid-2008.
To monitor efficiency, CMS would compare levels of tests physicians order for certain types of patients to tests ordered by other doctors who achieve similar outcomes. The agency would then contact the physicians whose testing patterns seem to be out of line. No doubt, the effects on private pay-for-performance [P4P] initiatives is obvious. Kuhn told the subcommittee that his largest concern was figuring out how to use the data to help physicians grow more efficient.
Assessment
To date, the agency hasn’t established plans to link efficiency measures with reimbursement changes. If it wants to do so, Congress would probably have to enact new legislation, according to several policymakers.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on February 24, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
OBTUSE METER?
By Staff Reporters
***
What is Delta?
FINANCE: Delta is a risk sensitivity measure used in assessing derivatives. It is one of the many measures that are denoted by a Greek letter. The series of risk measures that use such letters are fittingly referred to as the Greeks. They are often also called risk measures, hedge parameters, or risk sensitivities.
ACCOUNTING: Delta is the ratio of the change in price of an option to the change in price of the underlying asset. Also called the hedge ratio; For a call option on a stock, a delta of 0.50 means that for every $1.00 that the stock goes up, the option price rises by $0.50.
Running a business involves a constant learning curve. And that applies whether you’re a rookie entrepreneur just starting out with a great idea for a new business or a more established small business owner with a quickly growing business that needs to expand. You should always be learning as a business owner, no matter where you are in your career—there’s always a new tool to master, new problems to solve, and new vocabulary to understand.
In order to not get totally overwhelmed, it’s helpful to take things one segment at a time. For instance, feeling confident when discussing the business’s financial needs should be a priority for every small business owner. After all, you represent the heart and soul of your business in the marketplace. So knowing the “language” of business finance is an integral part of your job as the owner.
The good news is that you don’t have to be an accountant or a financial planner to negotiate in the world of business finance. Here are some business terms and finance terms that will help you find your way to successful small business funding. https://www.youtube.com/embed/0kD4X2fgxGs
Business and Finance Terms to Know
From accounting, to business loans, to general business financial operations, here’s the ultimate list to all the business finance terms and definitions you need to know:
1. Accounts Payable
Accounts payable is a business finance 101 term. This represents your small business’s obligations to pay debts owed to lenders, suppliers, and creditors. Sometimes referred to as A/P or AP for short, accounts payable can be short or long term depending upon the type of credit provided to the business by the lender.
2. Accounts Receivable
Also known as A/R (or AR, good guess), accounts receivables is another business finance 101 term that means the money owed to your small business by others for goods or services rendered. These accounts are labeled as assets because they represent a legal obligation for the customer to pay you cash for their short-term debt.
3. Accrual Basis
The accrual basis of accounting is an accounting method of recording income when it’s actually earned and expenses when they actually occur. Accrual basis accounting is the most common approach used by larger businesses to record and maintain financial transactions.
4. Accruals
A business finance term and definition referring to expenses that have been incurred but haven’t yet been recorded in the business books. Wages and payroll taxes are common examples.
5. Asset
This business finance key term is anything that has value—whether tangible or intangible—and is owned by the business is considered an asset. Typical items listed as business assets are cash on hand, accounts receivable, buildings, equipment, inventory, and anything else that can be turned into cash.
6. Balance Sheet
Along with three other reports relating to the financial health of your small business, the balance sheet is essential information that gives a “snapshot” of the company’s net worth at any given time. The report is a summary of the business assets and liabilities.
7. Bookkeeping
A method of accounting that involves the timely recording of all financial transactions for the business.
8. Capital
Refers to the overall wealth of a business as demonstrated by its cash accounts, assets, and investments. Often called “fixed capital,” it refers to the long-term worth of the business. Capital can be tangible, like durable goods, buildings, and equipment, or intangible such as intellectual property.
9. Working Capital
Not to be confused with fixed capital, working capital is another business finance 101 term. It consists of the financial resources necessary for maintaining the day-to-day operation of the business. Working capital, by definition, is the business’s cash on hand or instruments that you can convert to cash quickly.
10. Cash Flow
Every business needs cash to operate. The business finance term and definition cash flow refers to the amount of operating cash that “flows” through the business and affects the business’s liquidity. Cash flow reports reflect activity for a specified period of time, usually one accounting period or one month. Maintaining tight control of cash flow is especially important if your small business is new, since ready cash can be limited until the business begins to grow and produce more working capital.
11. Cash Flow Projections
Future business decisions will depend on your educated cash flow projections. To plan ahead for upcoming expenditures and working capital, you need to depend on previous cash flow patterns. These patterns will give you a comprehensive look at how and when you receive and spend your cash. This info is the key to unlock informed, accurate cash flow projections.
12. Depreciation
The value of any asset can be said to depreciate when it loses some of that value in increments over time. Depreciation occurs due to wear and tear. Various methods of depreciation are used by businesses to decrease the recorded value of assets.
13. Fixed Asset
A tangible, long-term asset used for the business and not expected to be sold or otherwise converted into cash during the current or upcoming fiscal year is called a fixed asset. Fixed assets are items like furniture, computer equipment, equipment, and real estate.
14. Gross Profit
This business finance term and definition can be calculated as total sales (income) less the costs (expenses) directly related to those sales. Raw materials, manufacturing expenses, labor costs, marketing, and transportation of goods are all included in expenses.
15. Income Statement
Here is one of the four most important reports lenders and investors want to see when evaluating the viability of your small business. It is also called a profit and loss statement, and it addresses the business’s bottom line, reporting how much the business has earned and spent over a given period of time. The result will be either a net gain or a net loss.
16. Intangible Asset
A business asset that is non-physical is considered intangible. These assets can be items like patents, goodwill, and intellectual property.
17. Liability
This business finance key term is a legal obligation to repay or otherwise settle a debt. Liabilities are considered either current (payable within one year or less) or long-term (payable after one year) and are listed on a business’s balance sheet. A business’s accounts payable, wages, taxes, and accrued expenses are all considered liabilities.
18. Liquidity
Liquidity is an indicator of how quickly an asset can be turned into cash for full market value. The more liquid your assets, the more financial flexibility you have.
19. Profit & Loss Statement
See “Income Statement” above.
20. Statement of Cash Flow
One of the important documents required by lenders and investors that shows a summary of the actual collection of revenue and payment of expenses for your business. The statement of cash flow should reflect activity in the areas of operating, investing, and financing and should be an integral part of your financial statement package.
21. Statement of Shareholders’ Equity
If you have chosen to fund your small business with equity financing and you have established shares and shareholders as part of the controlling interests, you are obligated to provide a financial report that shows changes in the equity section of your balance sheet.
22. Annual Percentage Rate
The business finance term and definition APR represents the yearly real cost of a loan including all interest and fees. The total amount of interest to be paid is based on the original amount loaned, or the principal, and is represented in percentage form. When shopping for the right loan for your small business, you should know the APR for the loan in question. This figure can be very helpful in comparing one financial tool with another since it represents the actual cost of borrowing.
23. Appraisal
Just like your real estate appraisal when buying a house, an appraisal is a professional opinion of market value. When closing a loan for your small business, you will probably need one or more of the three types of appraisals: real estate, equipment, and business value.
24. Balloon Loan
A loan that is structured so that the small business owner makes regular repayments on a predetermined schedule and one much larger payment, or balloon payment, at the end. These can be attractive to new businesses because the payments are smaller at the outset when the business is more likely to be facing strict financial constraints. However, be sure that your business will be capable of making that last balloon payment since it will be a large one.
25. Bankruptcy
This federal law is used as a tool for businesses or individuals who are having severe financial challenges. It provides a plan for reduction and repayment of debts over time or an opportunity to completely eliminate the majority of the outstanding debts. Turning to bankruptcy should be given careful thought because it will have a negative effect on the business credit score.
26. Bootstrapping
Using your own money to finance the start-up and growth of your small business. Think of it as being your own investor. Once the business is up and running successfully, the business finance term and definition bootstrapping refers to the use of profits earned to reinvest in the business.
27. Business Credit Report
Just like you have a personal credit report that lenders look at to determine risk factors for making personal loans, businesses also generate credit reports. These are maintained by credit bureaus that record information about a business’s financial history.
Items like how large the company is, how long has it been in business, amount and type of credit issued to the business, how credit has been managed, and any legal filings (i.e., bankruptcy) are all questions addressed by the business credit report. Lenders, investors, and insurance companies use these reports to evaluate risk exposure and financial health of a business.
28. Business Credit Score
A business credit score is calculated based on the information found in the business credit report. Using a specialized algorithm, business credit scoring companies take into account all the information found on your credit report and give your small business a credit score. Also called a commercial credit score, this number is used by various lenders and suppliers to evaluate your creditworthiness.
29. Collateral
Any asset that you pledge as security for a loan instrument is called collateral. Lenders often require collateral as a way to make sure they won’t lose money if your business defaults on the loan. When you pledge an asset for collateral, it becomes subject to seizure by the lender if you fail to meet the requirements of the loan documents.
30. Credit Limit
When a lender offers a business line of credit it usually comes with a credit limit, or a maximum amount that you can use at any given time. It is said that you reach your credit limit or “max out” your credit when you borrow up to or exceed that number. A business line of credit can be especially useful if your business is seasonal or if the income is extremely unpredictable. It is one of the fastest ways to access cash for emergencies.
31. Debt Consolidation
If your small business has several loans with various payments, you might want to consider a business debt consolidation loan. It is a process that lets you combine multiple loans into a single loan. The advantages are possibly reducing the interest rates on the borrowed funds as well as lowering the total amount you repay each month. Businesses use this tool to help improve cash flow.
32. Debt Service Coverage Ratio
The business finance term and definition debt service coverage ratio (DSCR) is the ratio of cash your small business has available for paying or servicing its debt. Debt payments include making principal and interest payments on the loan you are requesting. Generally speaking, if your DSCR is above 1, your business has enough income to meet its debt requirements.
33. Debt Financing
When you borrow money from a lender and agree to repay the principal with interest in regular payments for a specified period of time, you’re using debt financing. Traditionally, it has been the most common form of funding for small businesses.
Debt financing can include borrowing from banks, business credit cards, lines of credit, personal loans, merchant cash advances, and invoice financing. This method creates a debt that must be repaid but lets you maintain sole control of your business.
34. Equity Financing
The act of using investor funds in exchange for a piece or ”share” of your business is another way to raise capital. These funds can come from friends, family, angel investors, or venture capitalists.
Before deciding to use equity financing to raise the cash necessary for your business, decide how much control you are willing to share when it comes to decision-making and philosophy. Some investors will also want voting rights.
35. FICO Score
A FICO score is another type of credit score used by potential lenders for evaluating the wisdom of entering a contract with you and your business. FICO scores comprise a substantial part of the credit report that lenders use to assess credit risk. It was created by the Fair Isaac Corporation, hence the name FICO.
36. Financial Statements
An integral part of the loan application process is furnishing information that shows your business is a good credit risk. The standard financial statement packet includes four main reports: the income statement, the balance sheet, the statement of cash flow, and the statement of shareholders’ equity, if you have shareholders.
Lenders and investors want to see that your business is well-balanced with assets and liabilities, has positive cash flow, and will have capital to make expected repayments.
37. Fixed Interest Rate
The interest rate on a loan that is established in the beginning and does not change for the lifetime of the loan is said to be fixed. Loans with fixed interest rates are appealing to small business owners because the repayment amounts are consistent and easier to budget for in the future.
38. Floating Interest Rate
In contrast to the business finance term and definition fixed rate, the floating interest rate will change with market fluctuations. Also referred to as variable rates or adjustable rates, these amounts may often start out lower than the fixed rate percentages. This makes them more appealing in the short term if the market is trending down.
39. Guarantor
When starting a new small business, lenders might want you to provide a guarantor. This is an individual who guarantees to cover the balance owed on a debt if you or your business cannot meet the repayment obligation.
40. Interest Rate
All loans and other lending instruments are assigned the business finance key term interest rates. This is a percentage of the principal amount charged by the lender for the use of its money. Interest rates represent the current cost of borrowing.
41. Invoice Factoring or Financing
If your business has a significant amount of open invoices outstanding, you may contact a factoring company and have them purchase the invoices at a discount. By raising capital this way, there is no debt, and the factoring company assumes the financial responsibility for collecting the invoice debts.
42. Lien
This business finance term and definition is a creditor’s legal claim to the collateral pledged as security for a loan is called a lien.
43. Line of Credit
A lender may offer you an unsecured amount of funds available for your business to draw on when capital is needed. This line of credit is considered a short-term funding option, with a maximum amount available. This pre-approved pool of money is appealing because it gives you quick access to the cash.
44. Loan-to-Value
The LTV comparison is a ratio of the fair-market value of an asset compared to the amount of the loan that will fund it. This is another important number for lenders who need to know if the value of the asset will cover the loan repayment if your business defaults and fails to pay.
45. Long-Term Debt
Any loan product with a total repayment schedule lasting longer than one year is considered a long-term debt.
46. Merchant Cash Advance
A merchant may offer a funding method through a loan based on the business’s monthly sales volume. Repayment is made with a percentage of the daily or weekly sales. These tend to be short-term loans and are one of the costliest ways to fund your small business.
47. Microloan
Microloans are loans made through nonprofit, community-based organizations and they are most often for amounts under $50,000.
48. Personal Guarantee
If you’re seeking financing for a very new business and don’t have a high value asset to offer as collateral, you may be asked by the lender to sign a statement of personal guarantee. In effect, this statement affirms that you as an individual will act as guarantor for the business’s debt, making you personally liable for the balance of the loan even in the event that your business fails.
49. Principal
Any loan instrument is made of three parts—the principal, the interest, and the fees. The principal is a business finance key term and is the original amount that is borrowed or the outstanding balance to be repaid less interest. It is used to calculate the total interest and fees charged.
50. Revolving Line of Credit
This business finance term and definition is a funding option is similar to a standard line of credit. However, the agreement is to lend a specific amount of money, and once that sum is repaid, it can be borrowed again.
51. Secured Loan
Many lenders will require some form of security when loaning money. When this happens, this business finance term and definition is a secured loan. The asset being used as collateral for the loan is said to be “securing” the loan. In the event that your small business defaults on the loan, the lender can then claim the collateral and use its fair-market value to offset the unpaid balance.
52. Term Loan
These are debt financing tools used to raise needed funds for your small business. Term loans provide the business with a lump sum of cash up front in exchange for a promise to repay the principal and interest at specified intervals over a set period of time. These are typically longer term, one-time loans for start-up expenses or costs for established business expansion.
53. Unsecured Loans
Loans that are not backed by collateral are called unsecured loans. These types of loans represent a higher risk for the lender, so you can expect to pay higher interest rates and have shorter repayment time frames. Credit cards are an excellent example of unsecured loans that are a good option for small business funding when combined with other financing options.
54. Articles of Incorporation
This is legal documentation of the business’s creation, including name, type of business, and type of business structure or incorporation. This paperwork is one of the first tasks you will complete when you officially start your business. Once submitted, your articles of incorporation are kept on file with the appropriate governmental agencies.
55. Business Plan
Here is your tool for demonstrating how you want to establish your small business and how you plan to grow it into good financial health. When writing a business plan, it should include financial, operational, and marketing goals as well as how you plan to get there. The more specific you are with your business plan, the better prepared you will be in the long run.
56. Employer Identification Number (EIN) Certificate
In order to be more easily identified by the Internal Revenue Service, every business entity is assigned a unique number called an EIN. When you start your small business, an EIN will be assigned and mailed to the business address. This number never changes, and you will be asked to furnish it for many reasons.
57. Franchise Agreement
For a small business entrepreneur, entering into a franchise agreement with a larger company can be a way to enter the marketplace. The agreement made between you and the larger company gives you the right to operate as a satellite of the larger company in a certain territory for a given period of time. This lets you, the business owner, take advantage of a brand name that’s already familiar in the marketplace and a process or operation that has already been tested.
58. Net Worth
This business finance term and definition is an expression of your business’s total value, as determined by your total current assets less the total liabilities currently owed by the business. With your business’s most recent balance sheet in hand, you can calculate the net worth using a simple formula: Assets – Liabilities = Net Worth.
59. Retained Earnings
Just like it sounds, this term represents any profits earned that are retained in the business. This can also be referred to as bootstrapping.
60. Tax Lien
If your business fails to pay taxes owed to the designated government entity, namely the IRS, you may find your assets seized by the claim of a tax lien. The government can not only seize your assets for liquidation to resolve the tax debt, but they can also charge you penalties on the amount you owe.
Don’t Be Overwhelmed by Health Economics, Business and Finance Terms
As a small business owner, physicians are required to wear many different hats—often including that of chief financial officer or bookkeeper. Before you let yourself get intimidated by all the business terms and definitions, just remember that knowledge is power.
You can serve your small practice business, clinic, out-patient center or hospital most effectively by becoming familiar with terms used in business and finance and how they will affect your financial health. Armed with a basic understanding of business finance key terms, you will be prepared to face the financial challenges that go along with being a modern doctor, today!
“”Medical economics and finance is an integral component of the health care industrial complex. Its language is a diverse and broad-based concept covering many other industries: accounting, insurance, mathematics and statistics, public health, provider recruitment and retention, Medicare, health policy, forecasting, aging and long-term care, are all commingled arenas.
The Dictionary of Health Economics and Finance will be an essential tool for doctors, nurses and clinicians, benefits managers, executives and health care administrators, as well as graduate students and patients? With more than 5,000 definitions, 3,000 abbreviations and acronyms, and a 2,000 item oeuvre of resources, readings, and nomenclature derivatives? it covers the financial and economics language of every health care industry sector.”” – From the Preface byDavid Edward Marcinko “
Posted on February 15, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
A stock buyback is when a public company uses cash to buy shares of its own stock on the open market. A company may do this to return money to shareholders that it doesn’t need to fund operations and other investments
Share buybacks can create value for investors in a few ways: Repurchases return cash to shareholders who want to exit the investment. With a buyback, the company can increase earnings per share, all else equal. The same earnings pie cut into fewer slices is worth a greater share of the earnings.
A stock buyback typically means that the price of the remaining outstanding shares increases. This is simple supply-and-demand economics: there are fewer outstanding shares, but the value of the company has not changed, therefore each share is worth more, so the price goes up.
But, the practice has faced criticism from labor unions, the SEC, and even President Biden, who proposed stricter stock buyback regulations for company execs last week.
Nevertheless,
Stock buybacks from S&P 500 companies are expected to pass $1 trillion this year, after hitting a record $882 billion in 2021, according to Goldman Sachs.
In recent years, Starbucks spent $13.5 billion repurchasing shares.
Posted on February 1, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
The FOMC just held interest rates steady and interest rates probably won’t go down in March.
Most investors were expecting the Federal Reserve to finally start cutting interest rates at its next meeting in March, but after its latest meeting concluded yesterday, Jerome Powell splashed cold water on that idea.
Speaking during a press conference, Powell explained that he doesn’t think it’s likely that the Federal Reserve will have reached “a level of confidence” that inflation has come down enough to start slashing rates that soon.
However, he at least said cuts were likely coming sometime this year. And, the markets crashed. Technology stocks in particular had a rough one, giving the NASDAQ its worst day since October.
And, NY Community Bancorp—which scooped up most of failed Signature Bank’s assets last year—tanked after reporting a surprise loss for Q4, spurring fears of another regional banking crisis.
Posted on January 24, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Theranos founder and ex-CEO Elizabeth Holmes was just banned from US federal health care programs for nine decades, according to the US the health department. Holmes was sentenced in November 2022 to 11 years in prison following a trial that determined she knew her blood-testing startup, which was founded in 2003 and which claimed to be able to test for a range of diseases and risks with one finger prick, produced inaccurate and faulty results. Before government probes, Theranos raised hundreds of millions of dollars, named prominent former U.S. officials to its board, and explored a partnership with the U.S. military to use its tests on the battlefield.
So, just what is a Federal Health Care Program?
Federal Health Care Program means any plan or program that provides health benefits, whether directly, through insurance, or otherwise, which is funded directly, in whole or in part, by the United States Government, including, but not limited to, Medicare, Medicaid/MediCal, managed Medicare/Medicaid/MediCal, TriCare/VA/CHAMPUS, SCHIP, Federal Employees Health Benefit Plan, Indian Health Services, Health Services for Peace Corp Volunteers, Railroad Retirement Benefits Black Lung Program, Services Provided to Federal Prisoners, and Pre- Existing Condition Insurance Plans (PCIPs).














 8
8