BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
The global healthcare sector faces mounting challenges: rising costs, inefficiencies, limited access, and bureaucratic entanglements. In response, some economists and policymakers have turned to Austrian Economics for answers. Rooted in the works of Ludwig von Mises and Friedrich Hayek, Austrian Economics emphasizes individual choice, market-driven solutions, and skepticism toward centralized planning. But can this school of thought truly “save” healthcare?
At its core, Austrian Economics champions the idea that decentralized decision-making and free-market mechanisms lead to more efficient and responsive systems. In healthcare, this would mean reducing government control and allowing competition to drive innovation, lower costs, and improve quality. Proponents argue that when patients act as consumers and providers compete for their business, the system becomes more accountable and efficient. For example, direct primary care models—where patients pay physicians directly without insurance intermediaries—reflect Austrian principles and have shown promise in improving care and reducing administrative overhead.
Austrian theorists also critique the price distortions caused by third-party payers like insurance companies and government programs. According to them, when consumers are insulated from the true cost of care, demand becomes artificially inflated, leading to overutilization and waste. By restoring price signals—where patients see and respond to the actual cost of services—Austrian economists believe the market can better allocate resources and curb unnecessary spending.
However, critics argue that healthcare is not a typical market. Patients often lack the information, time, or capacity to make rational choices, especially in emergencies. Moreover, healthcare involves significant externalities and moral considerations that pure market logic may overlook. For instance, should access to life-saving treatment depend solely on one’s ability to pay? Austrian Economics offers little guidance on equity or universal access, which are central concerns in modern healthcare debates.
Austria itself provides an interesting case study. Despite the name, Austrian Economics is not the guiding philosophy behind Austria’s healthcare system. Instead, Austria operates a social insurance model with near-universal coverage, funded through mandatory contributions and managed by a mix of public and private actors. While recent reforms have aimed to streamline administration and reduce fragmentation he system remains largely collectivist—contrary to Austrian ideals.
In conclusion, Austrian Economics offers valuable insights into the inefficiencies of centralized healthcare systems and the potential benefits of market-based reforms. Its emphasis on individual choice, price transparency, and entrepreneurial innovation can inspire meaningful improvements. However, its limitations in addressing equity, access, and the unique nature of healthcare suggest that it cannot “save” the system on its own. A hybrid approach—blending market mechanisms with safeguards for universal access—may offer a more balanced path forward.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on October 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
DEFINED
***
***
A physician practice management corporation (PPMC) is a business entity that provides non-clinical administrative and operational support to medical practices, allowing physicians to focus on patient care while the corporation handles the business side of healthcare.
Physician practice management corporations emerged in response to the increasing complexity of running a medical practice. As healthcare regulations, insurance requirements, and operational costs grew, many physicians found it challenging to manage both clinical responsibilities and business operations. PPMCs offer a solution by taking over the administrative burdens, enabling physicians to concentrate on delivering quality care.
At their core, PPMCs are responsible for a wide range of non-medical services. These include billing and coding, human resources, payroll, marketing, compliance, information technology, and financial management. By centralizing these functions, PPMCs can achieve economies of scale, reduce overhead costs, and improve operational efficiency for the practices they manage. This model is particularly attractive to small and mid-sized practices that may lack the resources to manage these functions independently.
PPMCs typically enter into long-term management agreements with physician groups. In some cases, they may purchase the non-clinical assets of a practice—such as equipment, office space, and administrative staff—while the physicians retain control over clinical decisions and patient care. This arrangement allows for a clear division between medical and business responsibilities, which is essential for maintaining compliance with healthcare regulations like the Stark Law and the Anti-Kickback Statute.
A physician practice management corporation (PPMC) is a business entity that provides non-clinical administrative and operational support to medical practices, allowing physicians to focus on patient care while the corporation handles the business side of healthcare.
Physician practice management corporations emerged in response to the increasing complexity of running a medical practice. As healthcare regulations, insurance requirements, and operational costs grew, many physicians found it challenging to manage both clinical responsibilities and business operations. PPMCs offer a solution by taking over the administrative burdens, enabling physicians to concentrate on delivering quality care.
At their core, PPMCs are responsible for a wide range of non-medical services. These include billing and coding, human resources, payroll, marketing, compliance, information technology, and financial management. By centralizing these functions, PPMCs can achieve economies of scale, reduce overhead costs, and improve operational efficiency for the practices they manage. This model is particularly attractive to small and mid-sized practices that may lack the resources to manage these functions independently.
PPMCs typically enter into long-term management agreements with physician groups. In some cases, they may purchase the non-clinical assets of a practice—such as equipment, office space, and administrative staff—while the physicians retain control over clinical decisions and patient care. This arrangement allows for a clear division between medical and business responsibilities, which is essential for maintaining compliance with healthcare regulations like the Stark Law and the Anti-Kickback Statute.
***
***
One of the key advantages of working with a PPMC is access to capital and advanced infrastructure. PPMCs often invest in state-of-the-art electronic health record (EHR) systems, data analytics tools, and revenue cycle management platforms. These technologies can enhance patient care, streamline operations, and improve financial performance. Additionally, PPMCs may offer strategic guidance on practice expansion, mergers and acquisitions, and payer contract negotiations.
However, the relationship between physicians and PPMCs must be carefully managed. While PPMCs bring valuable expertise and resources, there is a risk that business priorities could overshadow clinical autonomy. To mitigate this, successful PPMCs prioritize physician engagement, transparent governance, and aligned incentives. They work collaboratively with physicians to ensure that business strategies support, rather than hinder, the delivery of high-quality care.
The physician practice management industry has evolved significantly over the past few decades. After a wave of failures in the 1990s due to overexpansion and misaligned incentives, modern PPMCs have adopted more sustainable and physician-centric models. Today, they play a crucial role in helping practices adapt to value-based care, population health management, and other emerging trends in healthcare delivery.
In conclusion, a physician practice management corporation serves as a strategic partner to medical practices, offering the business acumen and operational support needed to thrive in a complex healthcare environment. By offloading administrative tasks and providing access to advanced resources, PPMCs empower physicians to focus on what they do best—caring for patients—while ensuring the long-term success and sustainability of their practices.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on October 21, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITION
By Staff Reporters
***
***
Classic Definition: The Boomerang[ing] paradox is a feedback loop or cycle where events come back positively or negatively. It is an interconnection between people that looks like an ecosystem.
Modern Circumstance: When our thoughts and words energetically go out into the world, it has the same effect as the boomerang. It will go all the way out and come back around. That part of the creation model is our thinking and speaking. We’re unconscious and co-creating our reality. The Boomerang effect is everywhere: politics, business, relationships, economics, environment, marketing, psychology and healthcare, etc.
PSYCHOLOGY
Paradox Example: Research has found that teaching people and patients about psychological biases can help counteract biased behavior. On the other hand, due to the innate need for preservation of a positive self-image, it is likely that teaching people about biases they hold, may cause a boomerang paradoxical effect in cases where being associated with a specific bias implies negative social connotations
MEDICINE
Paradox Example: Recent examples of a boomerang paradoxical drug effects is withosteoporosis medications such as Actonel, Boniva and Fosamax. These all belong to a class of drugs called bisphosphonates. They are supposed to strengthen bones, but some doctors report that long-term use of these drugs may actually pose a risk of certain unusual fractures.
ECONOMICS
Paradox Example: A characteristic of advanced economies like Australia is continual growth in household income and plunging costs of electric appliances, resulting in rapid growth in peak demand. The power grid in turn requires substantial incremental generating and network capacity, which is utilized momentarily at best. The result is the Boomerang Paradox, in which the nation’s rising wealth has created the pre-conditions for fuel poverty.
***
The Medical Executive-Post is a news and information aggregator and social media professional network for medical and financial service professionals. Feel free to submit education content to the site as well as links, text posts, images, opinions and videos which are then voted up or down by other members. Comments and dialog are especially welcomed. Daily posts are organized by subject. ME-P administrators moderate the activity. Moderation may also conducted by community-specific moderators who are unpaid volunteers.
Population health and public health are two interrelated disciplines that strive to enhance the health outcomes of communities. While they share a common mission—to reduce health disparities and promote wellness—their approaches, target populations, and operational frameworks differ significantly.
***
***
Public health is traditionally defined as the science and art of preventing disease, prolonging life, and promoting health through organized efforts and informed choices of society, organizations, public and private sectors, communities, and individuals. It focuses on the health of the general population and emphasizes broad interventions such as vaccination programs, sanitation, health education, and policy advocacy. Public health professionals often work in government agencies, nonprofit organizations, and academic institutions to implement community-wide initiatives that prevent disease and promote healthy behaviors.
***
***
In contrast, population health takes a more targeted approach. It refers to the health outcomes of a specific group of individuals, including the distribution of such outcomes within the group. This field is particularly concerned with the social determinants of health—factors like income, education, environment, and access to care—that influence health disparities. Population health strategies often involve data-driven interventions tailored to the needs of defined groups, such as rural communities, ethnic minorities, or patients with chronic conditions.
One key distinction lies in scope and granularity. Public health initiatives are typically designed for the entire population, aiming to create systemic change. For example, anti-smoking campaigns or water fluoridation programs benefit everyone regardless of individual risk. Population health, however, might focus on reducing diabetes rates among Hispanic adults in a specific urban area, using targeted outreach and culturally sensitive care models.
Another difference is in data utilization. Population health relies heavily on health informatics and analytics to identify trends, allocate resources, and evaluate outcomes. This evidence-based approach supports precision in addressing health inequities. Public health also uses data, but often at a broader level to guide policy and monitor general health indicators like life expectancy or disease prevalence.
Despite these differences, the two fields are complementary. Public health lays the foundation for healthy societies through preventive infrastructure, while population health builds on this by addressing nuanced needs within subgroups. Together, they form a holistic framework for improving health outcomes across diverse communities.
In today’s healthcare landscape, the integration of public and population health is increasingly vital. The COVID-19 pandemic underscored the importance of both approaches: public health measures like mask mandates and vaccination campaigns were essential, while population health efforts ensured vulnerable groups received targeted support.
In conclusion, while public health and population health differ in focus and methodology, they are united by a shared goal: to foster healthier communities. Understanding their distinctions enables more effective collaboration and innovation in health policy, care delivery, and community engagement.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Investing may seem complicated, but today there are many ways for the newly minted physician [MD, DO, DPM, DMD or DDS] to begin, even with minimal knowledge and only a small amount to invest. Starting as soon as possible will help you get closer to the retirement you deserve.
***
Why is investing important?
Investing often feels like a luxury reserved for the already wealthy physician. Many of us find it difficult to think about investing for the future when there are so many things we need that money for right now; medical school loans, auto, home and children; etc. But, at some point, we’re going to want to stop working and enjoy retirement. And simply put, retirement is expensive.
Most calculations advise that you aim for enough savings to give you 70% to 80% of your pre-retirement income for 20 years or more. Depending on your goals for retirement, that means you could need between $500,000 and $1 million in savings by the time you retire. That may not sound attainable, but with the power of compounding growth, it’s not as hard to achieve as you think. The key is starting as soon as possible and making smart choices.
The short answer is “now,” no matter what your age. Due to the way the gains in investments can compound, the earlier you start the better. Money invested in your 20s could very easily grow over 20 times before you retire, without you having to do much.That is powerful. Even if you’re in your 50s or older, you can still make significant progress toward meeting your goals in retirement.
How much should you invest per month?
Most financial experts say you should invest 10% to 15% of your annual income for retirement. That’s the goal, but you don’t have to get there immediately. Whatever you can start investing today is going to help you down the road.
So, if 10% to 15% is too much right now, start small and build toward that goal over time. You can actually start investing with $5 if you want. And you should. Some investment products require a minimum investment, but there are plenty that don’t, and a lot of online brokerage accounts can be started for free.
The best investments for you are going to depend on your age, goals, and strategy. The important thing is to get started. You’ll learn as you go. If you have questions, a dedicated DIYer or investment advisor can help give you the guidance and options you need.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The U.S. healthcare system is often criticized for its high costs, unequal access, and inconsistent outcomes. With nearly 30 million Americans uninsured and many more underinsured, the question arises: could socialized medicine be the solution to these systemic issues?
Socialized medicine refers to a system where the government owns and operates healthcare facilities and employs medical professionals, funded primarily through taxation. While the term is often used pejoratively in American discourse, countries like the United Kingdom and Sweden have long embraced such models. These systems guarantee universal access to healthcare, regardless of income or employment status.
One of the strongest arguments in favor of socialized medicine is its potential to reduce overall healthcare costs. In the U.S., administrative expenses, profit margins, and fragmented billing systems contribute to exorbitant prices. A centralized system could streamline operations, negotiate better drug prices, and eliminate the need for private insurance middlemen. Countries with socialized systems typically spend less per capita on healthcare while achieving comparable or better health outcomes.
Moreover, socialized medicine could address the issue of healthcare access. In the current U.S. model, losing a job often means losing health insurance. Even with the Affordable Care Act, many Americans face high premiums and deductibles. A government-run system would ensure that healthcare is a right, not a privilege, and that no one is denied care due to financial constraints.
***
***
However, critics argue that socialized medicine could lead to longer wait times, reduced innovation, and lower quality of care. They point to examples in Canada and the U.K. where patients sometimes wait weeks or months for non-emergency procedures. Additionally, skeptics fear that government control could stifle competition and reduce incentives for medical advancement.
Yet, these concerns may be overstated. Many countries with socialized systems still foster innovation through public-private partnerships and maintain high standards of care. France, for example, combines universal coverage with private providers and consistently ranks among the top healthcare systems globally.
Transitioning to socialized medicine in the U.S. would be a monumental task, requiring political will, public support, and a reimagining of healthcare financing. It would disrupt entrenched interests, including insurance companies and pharmaceutical firms. But if the goal is to create a more equitable, efficient, and humane system, socialized medicine deserves serious consideration.
In conclusion, while not a panacea, socialized medicine offers a compelling framework for addressing the deep-rooted problems in U.S. healthcare. By prioritizing access, affordability, and public health over profit, it could pave the way for a healthier and more just society.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on October 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters and A.I.
***
***
Dentistry is often perceived as a stable and rewarding profession, yet beneath the surface lies a troubling reality: dentists face disproportionately high levels of stress, burnout, divorce, practice turmoil, and even suicide. These issues stem from a complex interplay of emotional, financial, and professional pressures that uniquely affect dental practitioners.
Emotional and Psychological Strain
Dentists frequently operate in high-stakes environments where precision is paramount. The pressure to deliver flawless results while managing patient anxiety and discomfort can be overwhelming. Many patients fear dental procedures, and this fear often manifests as hostility or distrust, placing emotional strain on the dentist. Over time, the cumulative effect of these interactions can lead to compassion fatigue and emotional exhaustion.
Unlike other medical professionals who often work in collaborative hospital settings, dentists typically operate in solo or small group practices. This isolation can limit opportunities for peer support and professional camaraderie. Without a strong support network, dentists may struggle to process the emotional toll of their work, increasing their vulnerability to depression and burnout.
Financial and Business Pressures
Running a dental practice involves more than clinical expertise—it requires business acumen. Dentists must manage overhead costs, staff salaries, insurance reimbursements, and patient billing. The financial burden of student loans, often exceeding six figures, adds to the stress. Economic downturns or shifts in healthcare policy can destabilize practices, leading to turmoil and uncertainty.
***
***
Work-Life Imbalance and Marital Strain
The demanding nature of dentistry often spills into personal life. Long hours, administrative responsibilities, and the emotional weight of patient care can leave little time or energy for family. This imbalance contributes to high divorce rates among dentists. The stress of maintaining a successful practice while nurturing personal relationships can become untenable, especially without adequate coping mechanisms.
Burnout and Suicide Risk
Burnout in dentistry is alarmingly common. A study by the American Dental Association found that 84% of dentists report experiencing burnout at some point in their careers.
Addressing these challenges requires systemic change. Mental health support, peer mentorship, and business education should be integrated into dental training. Encouraging open conversations about stress and providing resources for emotional well-being can help reduce stigma and promote resilience.
By acknowledging the hidden struggles of dentistry, the profession can move toward a healthier, more sustainable future.
Posted on October 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
A paradox is a logically self-contradictory statement or a statement that runs contrary to one’s expectation. It is a statement that, despite apparently valid reasoning from true or apparently true premises, leads to a seemingly self-contradictory or a logically unacceptable conclusion. A paradox usually involves contradictory-yet-interrelated elements that exist simultaneously and persist over time. They result in “persistent contradiction between interdependent elements” leading to a lasting “unity of opposites”.
THE TELE-MEDICINE PARADOX
Classic Definition: Refers specifically to the treatment of various medical conditions without seeing the patient in person. Healthcare providers may use electronic and internet platforms like live video, audio, PCs, tablets, or instant messaging to address a patient’s concerns and diagnose their condition remotely.
Modern Circumstance: This may include giving medical advice, walking them through at-home exercises, or recommending them to a local provider or facility. Even more exciting is the emergence of telemedicine apps which give patients access to care right from their phones or computer screens.
Paradox Examples: Treating certain conditions remotely can be challenging. Tele-medicine is often used to treat common illnesses, manage chronic conditions, or provide specialist services. If a patient is dealing with an emergent or serious condition, the remote provider suggests they seek in-person medical care.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on October 17, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Can a physician medical provider charge an office cancellation fee?
According to the American Medical Association’s Code of Medical Ethics, physicians can charge fees for “missed appointments or appointments not cancelled in advance in keeping with the published policy of the practice”, and they should “clearly notify patients in advance of fees charge” (Opinion 11.3. 2) [28].
And so, if you miss a doctor’s appointment these days, you could get hit with a “no-show” fee of up to $150 — or more for some specialties.
Is it legal for an insurance company to charge a cancellation fee?
These practices are typically legal. They help businesses ensure they can recoup the lost revenue due to no-shows or last-minute cancellations.
Cancellation fees are permitted, but seldom collected absent unusual circumstances, such as a great deal of work having been provided.
QUESTION: As a doctor [MD, DO, DPM or DDS], do you charge an office cancellation fee? If so, how much is it?
Why It Is Difficult to Practice Medicine Part-Time Today?
In the past, part-time medical practice offered physicians a flexible way to balance professional responsibilities with personal or family commitments. Today, however, the healthcare environment has evolved in ways that make part-time medicine increasingly challenging. From administrative burdens to economic pressures and patient expectations, the obstacles are both systemic and personal.
One of the most significant barriers is the rise in administrative complexity. Physicians are now required to navigate electronic health records (EHRs), comply with insurance documentation, and meet regulatory standards such as HIPAA and MACRA. These tasks consume hours of non-clinical time, which is difficult to compress into a part-time schedule. Even seeing fewer patients doesn’t exempt part-time doctors from the same documentation and compliance requirements as their full-time counterparts.
***
***
Another challenge is financial viability. Many physicians are paid based on productivity metrics, such as Relative Value Units (RVUs), which reward volume over quality. Part-time practitioners often struggle to meet these benchmarks, resulting in lower compensation and reduced benefits. Additionally, malpractice insurance premiums and licensing fees remain fixed regardless of hours worked, further eroding the financial appeal of part-time practice.
Continuity of care is also a concern. Patients increasingly expect immediate access to their providers, especially in primary care and specialties like psychiatry or pediatrics. Part-time physicians may not be available for urgent issues, leading to fragmented care and dissatisfaction. This can strain relationships with patients and colleagues who must cover gaps in availability.
From a professional standpoint, part-time physicians may face limited career advancement. Leadership roles, academic appointments, and research opportunities often favor full-time commitment. There’s also a perception—sometimes unfair—that part-time doctors are less dedicated or less competent, which can affect peer respect and influence within medical institutions.
Technology, while beneficial, adds another layer of complexity. Telemedicine, remote monitoring, and digital communication tools have expanded access but also increased the expectation for constant availability. Part-time physicians may find it difficult to manage asynchronous messages, follow-ups, and virtual visits without extending their work hours beyond what they intended.
***
***
Lastly, burnout and work-life balance—ironically one of the reasons doctors seek part-time roles—can still be elusive. The pressure to maintain clinical excellence, stay updated with medical advancements, and meet patient needs doesn’t diminish with reduced hours. In fact, squeezing these responsibilities into fewer days can intensify stress rather than alleviate it.
In conclusion, while part-time medical practice may seem like a solution to modern work-life challenges, the reality is far more complex. The structure of today’s healthcare system, combined with economic, technological, and cultural pressures, makes it difficult for physicians to thrive in part-time roles. Addressing these challenges will require systemic reform, flexible compensation models, and a cultural shift in how we value and support diverse medical careers.
SPEAKING: ME-P Editor Dr. David Edward Marcinko MBA MEd will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on October 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
ByAI and Staff Reporters
***
***
Alpha Male and Beta Male are terms for men derived from the designations of alpha and beta animals in ethology. They may also be used with other genders, such as women, or additionally use other letters of the Greek alphabet (such as sigma. The popularization of these terms to describe humans has been widely criticized by scientists. Both terms have been frequently used in internet memes.
The term beta is used as a pejorative self-identifier among some members of the manosphere, particularly incels, who do not believe they are assertive and/or traditionally masculine, and feel overlooked by women. It is also used to negatively describe other men who are not deemed to be assertive, particularly with women. In internet culture, the term sigma male is also frequently used, gaining popularity in the late 2010s, but has since been used jokingly, often being used with incel.
Note: Incel is a portmateau of “involuntary celibate”) is a term associated with an online subculture of mostly male and heterosexual people who define themselves as unable to find a romantic or sexual despite desiring one. They often blame, objectify and denigrate women and girls as a result.
Delta Males are very responsible and keep the world moving. Highly adaptable, deltas are known for their competence and work ethic rather than their leadership and ambition. Delta Males love learning new skills for the sake of improving themselves, not for power or extrinsic successes. Because of this, they often have a very healthy work-life balance. They’re dependable and unpretentious. Common personality traits: hardworking, loyal and responsible. Careers they excel at are accountant, dentist, engineer and firefighter. If you’re a delta male, your work often speaks for itself. People trust you, so consider being more proactive and taking initiative at work; you’ll be rewarded for it and won’t necessarily need to be in the spotlight.
Gammas Males tend to be insecure about status and may overestimate their status. They’re unhappy with their position, so they try to convince themselves that they’re Sigmas. A Gamma Male is described as intelligent, romantic, and empathetic. While he has some female traits, he has difficulty understanding and dating women. But, unlike alphas, gammas avoid conflict at all costs and care deeply about what other people think of them. They lack the leadership skills and confidence to be on top.
Omega Males are skilled introverts who don’t need external validation. Pop culture portrays them as the shyer, more reserved yin to the zeta male’s yang. They’re independent and very comfortable in their own company. They’d rather spend time coming up with (usually brilliant) new ideas and inventions of their own instead of socializing with others. They have uncouth but delightful senses of humor and their theories often change the world for the better. Common personality traits are self-motivated, strategic and quiet. Careers they excel at are chemist, composer, inventor and mathematician. If you’re an omega male, your ideas are likely ingenious.
Sigma Males are rebellious leaders with lots of life experience while delta males are responsible companions who you want by your side.Common personality traits are nurturing and wise. Careers they excel at areentrepreneur, philosopher, professor, or therapist.
Zeta Males are one-of-a-kind progressives. There’s a reason the zeta male is the least talked about personality type in pop culture. They’re rare nonconformists who don’t care what other people think. They know themselves and refuse to change to fit into the rigid social standards of society. Zeta males are fierce creatives who blaze new paths for themselves and others. Zeta Males are nonconformist creatives, gamma males are charismatic nomads, and omega males are sharp intellectuals with boundless ideas. Careers they excel at are actor, artist, musician or writer. Common personality traits are creative, independent and self-aware.
QUESTION: Doctors, Agents, Accountants and Financial Advisors: What is your male personality type?
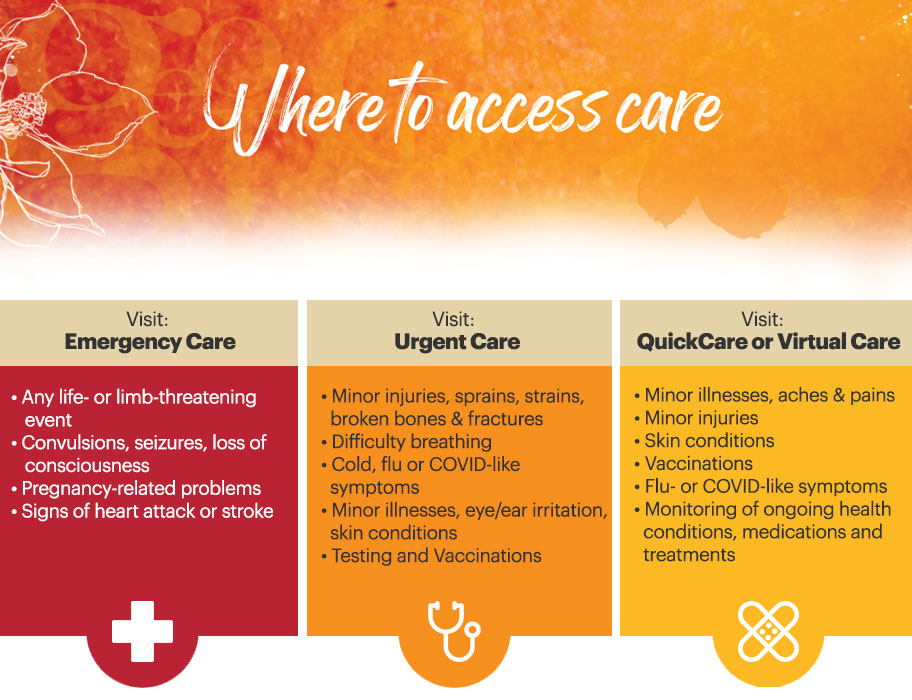
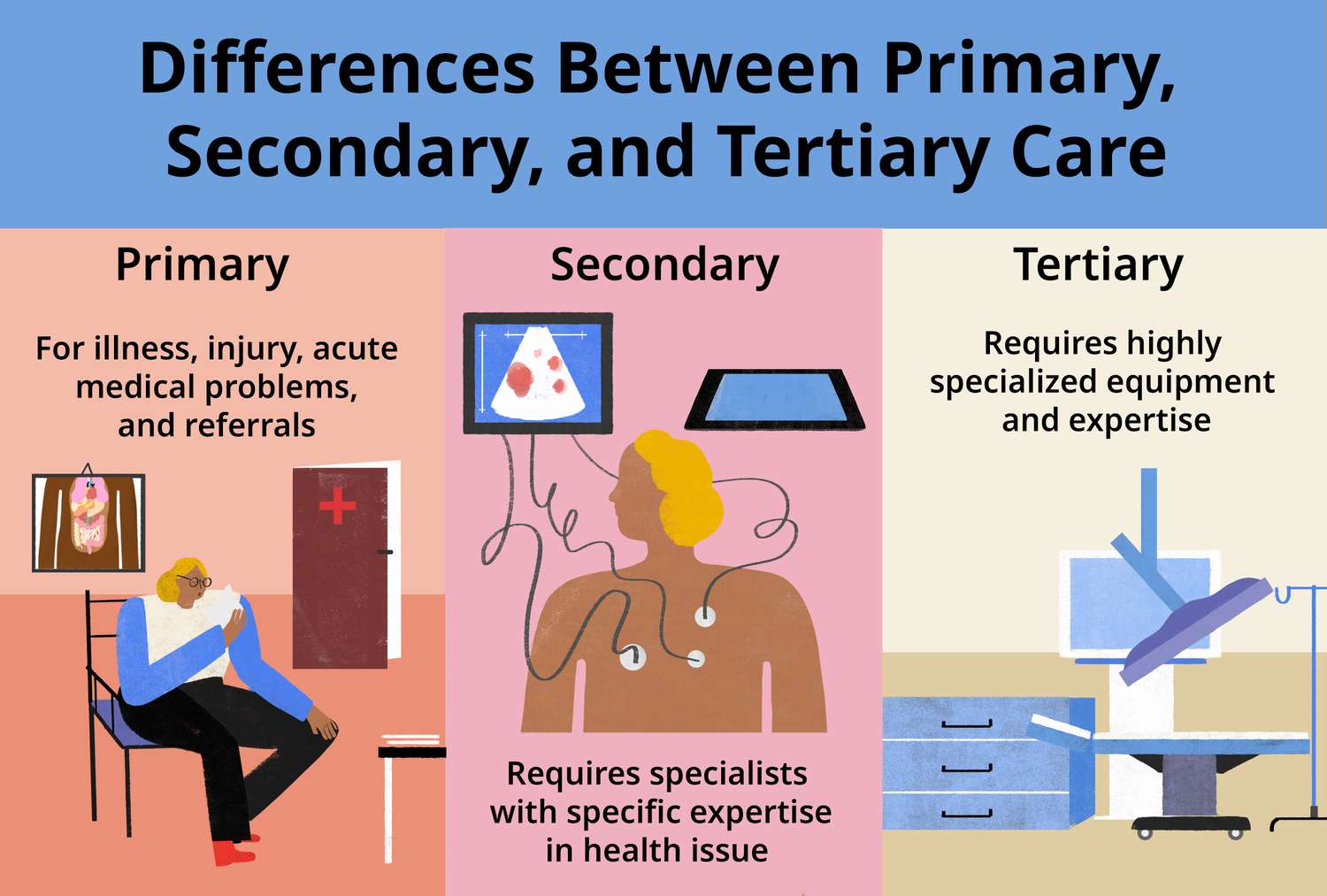
Classic: Acute care is a branch of secondary health care where a patient receives active but short-term treatment for a severe injury or episode of illness, an urgent medical condition, or during recovery from surgery. In medical terms, care for acute health conditions is the opposite from chronic care, or longer term care.
Modern: Acute care is active, short-term treatment for a severe injury or episode related to illness, an urgent medical condition or recovery from surgery.
Posted on October 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A. I.
***
***
Value-Based Medical Care: A Paradigm Shift in Healthcare
In recent years, the healthcare industry has undergone a transformative shift from volume-driven services to outcome-focused care. This evolution is embodied in the concept of value-based medical care, a model that emphasizes delivering high-quality healthcare while controlling costs and improving patient outcomes. Unlike traditional fee-for-service systems, which reward providers for the quantity of services rendered, value-based care aligns incentives with the value of care provided—measured by patient health outcomes relative to the cost of achieving them.
Core Principles of Value-Based Care
At its heart, value-based medical care is built on several foundational principles:
Patient-Centeredness: Care is tailored to individual needs, preferences, and values, promoting shared decision-making and holistic treatment.
Quality Over Quantity: Providers are rewarded for improving health outcomes, reducing hospital readmissions, and preventing disease rather than performing more procedures.
Integrated Care Delivery: Coordination among healthcare professionals ensures seamless transitions between services, reducing fragmentation and duplication.
Data-Driven Accountability: Performance metrics and health analytics guide clinical decisions and track progress toward better outcomes.
Cost Efficiency: By focusing on prevention and effective management of chronic conditions, value-based care aims to reduce unnecessary spending.
Benefits for Patients and Providers
For patients, value-based care offers a more personalized and proactive approach to health. It encourages preventive screenings, chronic disease management, and wellness programs that lead to longer, healthier lives. Providers benefit from shared savings programs, performance bonuses, and stronger relationships with their patients. Moreover, healthcare systems can allocate resources more effectively, reducing waste and improving overall population health.
Posted on October 7, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A. I.
***
***
A trio of scientists — two of them American and one Japanese — have won the Nobel Prize in Medicine for their discoveries concerning peripheral immune tolerance, a mechanism by which the body helps prevent itself from attacking its own tissues instead of foreign invaders.
Mary E. Brunkow, Fred Ramsdell and Shimon Sakaguchi will share the prize for discoveries that “launched the field of peripheral tolerance, spurring the development of medical treatments for cancer and autoimmune diseases,” the Nobel Assembly said in a news release. The trio will now share the prize money of 11 million Swedish kronor (nearly $1.2 million).
Hobson’s choice is a free choice in which only one thing is actually offered. The term is often used to describe an illusion that choices are available. The best known example is “I’ll give you a choice: Take it or leave it”, wherein “leaving it” is strongly undesirable.
The phrase is said to have originated with Thomas Hobson (1544–1631), a livery stable owner in Cambridge, England, who offered customers the choice of either taking the horse in the stall nearest to the door or taking none at all.
A CASE MODEL
Half of Physicians Plan to Change Career Paths
The Physicians Foundation recently conducted a survey on physician practice patterns and perspectives. Here are some key findings from the report:
• 31% of physicians identify as independent practice owners or partners. • Almost half (47%) of physicians plan to change career paths. • 78% of physicians sometimes, often or always experience feelings of burnout. • Nearly a quarter of physician time is spent on non-clinical paperwork.
This result is not a good Hobson’s Choice in Medicine.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 27, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
A paradox is a statement that appears at first to be contradictory, but upon reflection then makes sense. This literary device is commonly used to engage a reader to discover an underlying logic in a seemingly self-contradictory statement or phrase. As a result, paradox allows readers to understand concepts in a different and even non-traditional
***
***
GOVERNMENT HEALTH INFORMATION IS TRUSTED?
Classic Definition: Despite the PP-ACA, there is ambivalence about the role of the US Government as a source of quality healthcare information.
Modern Circumstance: Of brands presented to respondents in a Consumer Reports (50 percent), and AARP (37 percent) survey, they outpolled the “US Government Healthcare Quality Reporting Website” (36 percent) and Medicare Website (32 percent).
Paradox Example: The focus groups expressed “mixed reactions and raised doubts about government involvement in quality ratings information. At least one participant in each group expressed skepticism about trusting ‘the government’ to compile information.”
Younger consumers especially questioned the relevance of Medicare measures to the non-elderly population. Yet participants gravitated to “.gov” websites over “.org” websites as a more authoritative source.
CITE: Williams, Jason: Health Affairs, December 28, 2016
An app, which is short for “application,” is a type of software that can be installed and run on a computer, tablet, smartphone or other electronic devices. An app most frequently refers to a mobile application or a piece of software that is installed and used on a computer. Most apps have a specific and narrow function.
An easy and fairly cheap way for novices to get into investing is to use a robo-advisor. Basically, the funds you contribute will be invested by an algorithm based upon your goals, which are usually determined by taking a survey. This helps keep fees low; the algorithm doesn’t rely on a human expert to make trades, and you don’t have to spend significant amounts of time researching your investments. While this is a good way to start, it may not be the best option in the long run.
Online Brokerage or Investment Apps
More options are becoming available all the time, and they have opened trading to a much larger percentage of the population. That is a great thing, but it’s important to remember that “easier to invest” doesn’t necessarily mean it’s easy to invest well.
Be wary of apps that “gamify” trading and encourage risky choices. Keep in mind that trusted names offer more security, so do your research when you are selecting a platform.
Posted on September 23, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
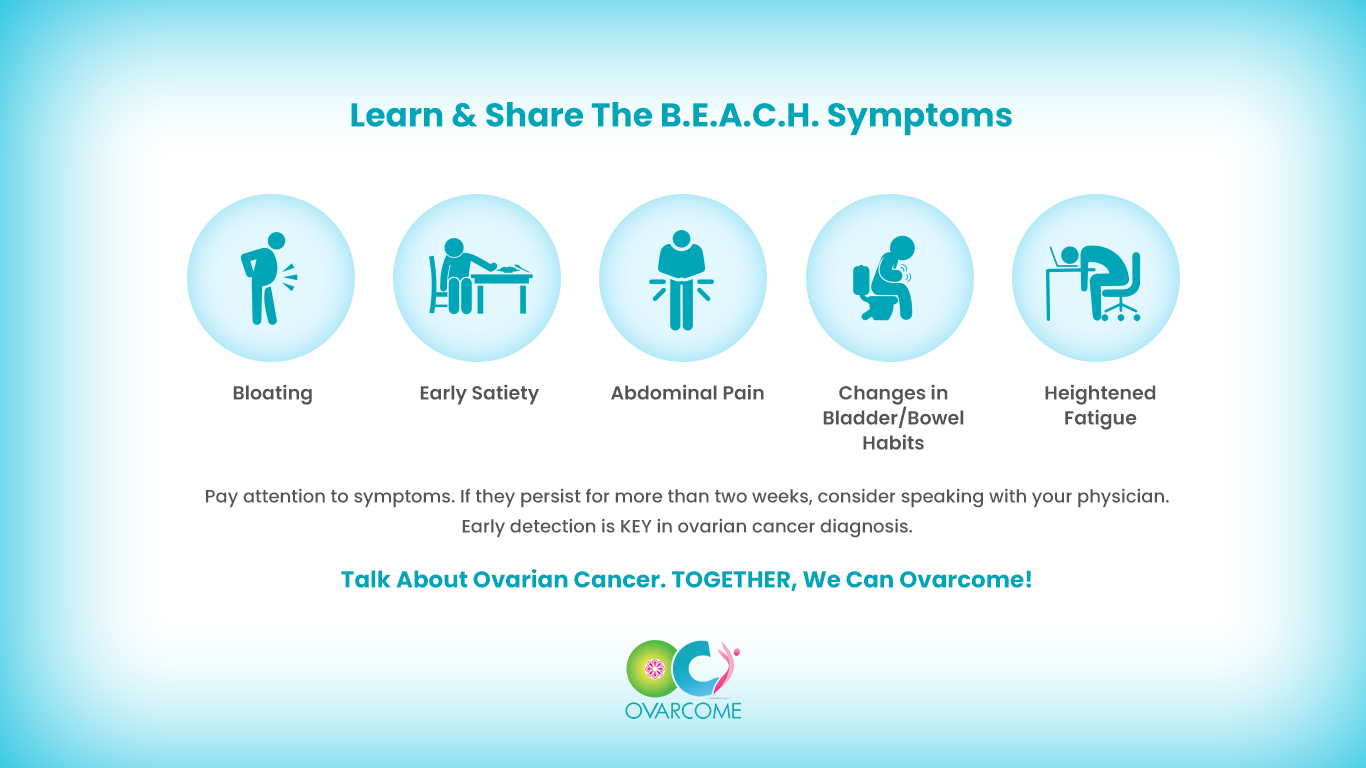
BEACH
By A.I. and Staff Reporters
***
***
Let’s talk.
September 23rd is Global Teal Talk Day, founded by Ovarcome.
Over 300,000 women are diagnosed annually with ovarian cancer, worldwide. Gather your friends, wear teal for a day out together and talk. Wearing teal is not enough.
The study of behavioral economics has revealed much about how different biases can affect our finances—often for the worse.
Take loss aversion: Because we feel a financial setback more acutely than a commensurate gain, we often cling to failed investments to avoid realizing the loss. Another potential hazard is present bias, or the tendency to prefer instant gratification over long-term reward, even if the latter gain is greater.
When it comes to money, sometimes it’s difficult to make rational decisions. Here, are three behavioral financial biases that could be impeding financial goals.
ANCHORING BIAS
Anchoring Bias happens when we place too much emphasis on the first piece of information we receive regarding a given subject. Anchoring is the mental trick your brain plays when it latches onto the first piece of information it gets, no matter how irrelevant. You might know this as a ‘first impression’ when someone relies on their own first idea of a person or situation.
Example: When shopping for a wedding ring a salesman might tell us to spend three months’ salary. After hearing this, we may feel like we are doing something wrong if we stray from this financial advice, even though the guideline provided may cause us to spend more than we can afford.
Example: Imagine you’re buying a car, and the salesperson starts with a high price. That number sticks in your mind and influences all your subsequent negotiations. Anchoring can skew our decisions and perceptions, making us think the first offer is more important than it is. Or, subsequent offers lower than they really are.
Example: Imagine an investor named Jane who purchased 100 shares of XYZ Corporation at $100 per share several years ago. Over time, the stock price declined to $60 per share. Jane is anchored to her initial price of $100 and is reluctant to sell at a loss because she keeps hoping the stock will return to her original purchase price. She continues to hold onto the stock, even as it declines, due to her anchoring bias. Eventually, the stock price drops to $40 per share, resulting in significant losses for Jane.
In this example, Jane’s nchoring bias to the original purchase price of $100 prevents her from rationalizing to sell the stock and cut her losses, even though market conditions have changed. So, the next time you’re haggling for your self, a potential customer or client, or making another big financial decision, be aware of that initial anchor dragging you down.
HERD MENTALITY BIAS
Herd Mentality Bias makes it very hard for humans to not take action when everyone around us does.
Example: We may hear stories of people making significant monetary profits buying, fixing up, and flipping homes and have the desire to get in on the action, even though we have no experience in real estate.
Example: During the dotcom bubble of the late 1990’s many investors exhibited a herd mentality. As technology stocks soared to astronomical valuations, investors rushed to buy these stocks driven by the fear of missing out on the gains others were enjoying. Even though some of these stocks had questionable fundamentals, the herd mentality led investors to follow the crowd.
In this example, the herd mentality contributed to the overvaluation of technology stocks. Eventually, it led to the dot-com bubble’s burst, causing significant losses for those who had unthinkingly followed the crowd without conducting proper research or analysis.
OVERCONFIDENT INVESTING BIAS
Overconfident Investing Bias happens when we believe we can out-smart other investors via market timing or through quick, frequent trading. This causes the results of a study to be unreliable and hard to reproduce in other research settings.
Example: Data convincingly shows that people and financial planners/advisors and wealth managers who trade most often under-perform the market by a significant margin over time. Active traders lose money.
Example: Overconfidence Investing Bias moreover leads to: (1) excessive trading (which in turn results in lower returns due to costs incurred), (2) underestimation of risk (portfolios of decreasing risk were found for single men, married men, married women, and single women), (3) illusion of knowledge (you can get a lot more data nowadays on the internet) and (4) illusion of control (on-line trading).
ASSESSMENT
Finally, questions remain after consuming this cognitive bias review.
Question: Can behavioral cognitive biases be eliminated by financial advisors in prospecting and client sales endeavors?
A: Indeed they can significantly reduce their impact by appreciating and understanding the above and following a disciplined and rational decision-making sales process.
Question: What is the role of financial advisors in helping clients and prospects address behavioral biases?
A: Financial advisors can provide an objective perspective and help investors recognize and address their biases. They can assist in creating well-structured investment and financial plans, setting realistic goals, and offering guidance to ensure investment decisions align with long-term objectives.
Question:How important is self-discipline in overcoming behavioral biases?
A; Self-discipline is crucial in overcoming behavioral biases. It helps investors and advisors adhere to their investment plans, avoid impulsive decisions, and stay focused on long-term goals reducing the influence of emotional and cognitive biases.
CONCLUSION
Remember, it is far more useful to listen to client beliefs, fears and goals, and to suggest options and offer encouragement to help them discover their own path toward financial well-being. Then, incentivize them with knowledge of the above psychological biases to your mutual success!
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
REFERENCES:
Marcinko, DE; Dictionary of Health Insurance and Managed Care. Springer Publishing Company, New York, 2007.
Marcinko, DE: Comprehensive Financial Planning Strategies for Doctors and Advisors: Best Practices from Leading Consultants and Certified Medical Planners™. Productivity Press, NY, 2016.
Marcinko, DE: Risk Management, Liability and Insurance Strategies for Doctors and Advisors: Best Practices from Leading Consultants and Certified Medical Planners™. Productivity Press, NY, 2017.
Nofsinger, JR: The Psychology of Investing. Rutledge Publishing, 2022
Winters, Scott: The 10X Financial Advisor: Your Blueprint for Massive and Sustainable Growth. Absolute Author Publishing House, 2020.
Despite their high salaries, not all doctors are wealthy, and some live paycheck to paycheck. Here are 5 reasons why many doctors today are broke, according to https://medschoolinsiders.com
1 | Believing They Are Universally Smart
The first reason so many doctors are broke is that many doctors believe they are universally smart. While most doctors have deep specialized knowledge, there’s a big difference between being smart in your profession and being smart with money. A physician’s schooling is quite thorough when it comes to the human body, but med school doesn’t include a prerequisite class on how to handle finances.
Graduating medical school is a major feat and certainly demonstrates superior work ethic and cognitive abilities. But many new doctors believe these accomplishments transcend all aspects of life. If you’re smart enough to earn an MD, you’re certainly smart enough to handle your finances, but only once you properly and intentionally educate yourself.
The truth is doctors, especially traditional graduates, haven’t had an opportunity to manage large sums of money until they become fully trained attending physicians and start pulling in low to mid six figures in income. Prior to that, there was very little of it to manage.
Far too many aspiring doctors, and students in general, don’t take the time to learn financial basics, in part because it’s uncomfortable and seems like something they can figure out “later”, whenever that may be. Their poor spending habits and lack of investment knowledge carry over into their careers, causing many to make irresponsible decisions.
The second factor is overspending too soon, and this comes up at two points in training.
First, it’s natural to want to start spending more as soon as you get into residency and start making a little more money. After all, you’ve been a broke student for 8 or more years, and now you’re finally making a reasonable and reliable wage. But that’s where young doctors get into trouble. Residency pays, but not nearly as much as you will be making once you become an attending physician. The average resident makes about $60K a year, and if you begin spending all of that money right away, thinking you’ll handle your loans once you become an attending, you delay paying off your medical school debt, which means the compounding effect through your student loan interest rate works against you.
Now that $250,000 in student loans has ballooned to over $350,000 by the time you finish residency. The compounding effect, which can be one of your greatest allies in your financial life, becomes an equally powerful enemy when working against you through debt. But of course, pinching pennies is easier said than done, especially when you’re in residency and are surrounded by peers in different professions. They’ve been earning good money much longer than you have, and they can afford more luxurious lifestyles.
They may not be worried about indulging in fine dining or how much a hotel costs when traveling. Students in college and medical school are often confident they will resist the temptations, but the desire to keep up with your friends and family can be difficult to ignore, which causes many to overspend before they technically have the money to do so.
The same is true of attending physicians. As soon as those six-figure salaries come rolling in, many physicians go overboard with spending, trying to make up for lost time and to treat yourself.
Now, we are not suggesting you shouldn’t reward yourself for completing residency, but that reward shouldn’t be a Lamborghini. It’s best to continue living like a resident in your first few years after becoming an attending to pay off loans, put a down payment on a home, and get your financial foundation built before loosening the purse strings.
3 | Decreasing Salaries
Third, doctors continue to make less money than they did before. And this includes nearly all 44 medical specialties. For example, while physician compensation technically rose from $343k to $391k between 2017 and 2022, this rise does not keep up with inflation. The real average compensation in 2022 was less than $325k—a $20k decrease in purchasing power in only six years.
For doctors who are already spending to the limits of their salaries with huge mortgages, car payments, business costs, and other luxuries, a decreased salary can have a huge impact. You might be able to cut back by going on fewer vacations or eating out less frequently, but many accrued costs are locked in, such as a mortgage payment, car loan, or leased rental space for your practice.
4 | Increasing Costs of Private Practice
In the past, running a private practice was much simpler, but recent stricter guidelines and regulations have made it difficult for solo practices to keep up. While regulations like the Health Insurance Privacy and Portability Act, or HIPAA, and mandatory Electronic Medical Records, or EMRs, are necessary to protect patients, they make costs higher for physicians who run their own private practice. These physicians need to spend their own money to set up and maintain EMRs as well as invest in security to ensure patient data is protected.
With the steep rise of inflation we’ve seen over the past couple of years, everything is more expensive, which means costs, such as business space, equipment, and even office supplies, have gone up for private practice physicians while salaries have not. 2013 to 2020 saw an annual inflation rate of anywhere from 0.7% to 2.3%. This skyrocketed to an annual inflation rate of 7.0% in 2021 and another 6.5% in 2022. In fact, the cost of running a private practice has increased by almost 40% between 2001 and 2021.
These increased costs are exacerbated by another problem plaguing private practices; decreased reimbursement. While costs increased by almost 40%, Medicare reimbursement only increased by 11%. When doctors see patients who are insured, the insurance companies pay the physicians for their time. For Medicare, the new proposed rules for 2023 would cut reimbursement by around 5%. When adjusting for inflation, Medicare reimbursement decreased by 20% in the last 20 years.
These costs add up, making it extremely difficult for physicians to thrive financially while running a private practice.
5 | Tuition Debt
Lastly, we can’t talk about a doctor’s finances without mentioning the exorbitant debt so many graduating physicians are left with. It won’t shock you to hear that med school is expensive. Extremely expensive. The average cost of tuition for a single year is nearly $60k, with significant variance from school to school, and that’s before accounting for living expenses.
In-state applicants pay less than out-of-state applicants, and students at private schools typically pay more than students at public medical schools. The astronomical costs mean the vast majority of students can’t pay for medical school out of their own pockets. And unless your family is part of the 1%, even with your parents footing the bill, it’s difficult to cover tuition, let alone rent, groceries, transportation, tech, social activities, exam fees, and application costs.
The average total student debt after college and med school is over $250k. But keep in mind that’s the average, which includes 27% of students who graduate with no debt at all. This means the vast majority of students leave medical school owing much more than $250k.
For some perspective, in 1978, the average debt for graduating MDs was $13,500, which, when adjusted for inflation, is a little over $60,000. There are multiple ways to eventually repay these loans, but time and discipline are essential to ensure this money is paid off as quickly as possible.
According to financial advisor Dr. David Edward Marcinko MEd MBA CMP™; consider the following:
Place a portion of your salary (15-20% or more) into a savings account, and another portion (10-20% or more) into wise investments [stocks, bonds, mutual funds, and/or ETFs].
Pay off your bills each month, and then use leftover spending money to purchase fun things like vacations and fancy dinners, within your means. Shop sales, buy used clothes, and use credit card points for travel.
Hire an excellent tax professional and meet with an investment advisor once or twice a year about your investment status and strategy. http://www.MarcinkoAssociates.com
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The Memory Palace Fallacy – Learning Styles Don’t Actually Exist
Remember being told you’re a “visual learner” or an “auditory learner”? Well, turns out that whole learning styles theory is pretty much bunk.
Common Learning Myths have been thoroughly debunked by modern educational research, and this is a big one. Studies consistently show that matching teaching methods to supposed learning styles doesn’t improve outcomes at all.
What actually matters is matching the teaching method to the content itself – you learn geography better with maps because geography is visual, not because you’re a “visual person.” It’s like trying to learn piano by reading about it versus actually playing keys. The activity should match what you’re trying to learn, not some made-up category about how your brain supposedly works.
Posted on September 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
What Is Pure Risk?
Pure risk is a category of risk that cannot be controlled and has two outcomes: complete loss or no loss at all. There are no opportunities for gain or profit when pure risk is involved. Pure risk is generally prevalent in situations such as natural disasters, fires, or death. These situations cannot be predicted and are beyond anyone’s control. Pure risk is also referred to as absolute risk.
***
1. Personal Risks
Now, there are basically 3 types of pure risks that concern individual physicians. These incur losses like loss of income, additional expenses and devaluation of property. There are 4 risk factors affecting them:
Premature death. This is death of a breadwinner who leaves behind financial responsibilities.
Old age / retirement. The risk of being retired without sufficient savings to support retirement years.
Health crisis. Individual with health problem may face a potential loss of income and increase in medical expenditures.
Unemployment. Jobless individual may have to live on their savings. If savings are depleted, a bigger crisis is awaiting.
2. Property Risks
This means the possibility of damage or loss to the property owned due to some cause. There are two types of losses involved.
Direct loss which means financial loss as a result of property damage.
Consequential loss which means financial loss due to the happenings of direct loss of the property.
For instance, a medical practice that burned down may incur repair costs as the direct loss. The consequential loss is being unable to run the practice business to generate income.
3. Liability Risks
A doctor is legally liable to his wrongful act that cause damage to a third party; physically, by reputation or property. S/he can be legally sued with no maximum in the compensation amount if found guilty.
Knowing how risks are classified, and the types of pure risks an individual is exposed to, will provide a fundamental overview on these risk topics and prepare you to further acquire the knowledge of how to deal with and manage them as a physician executive, leader, or manager.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
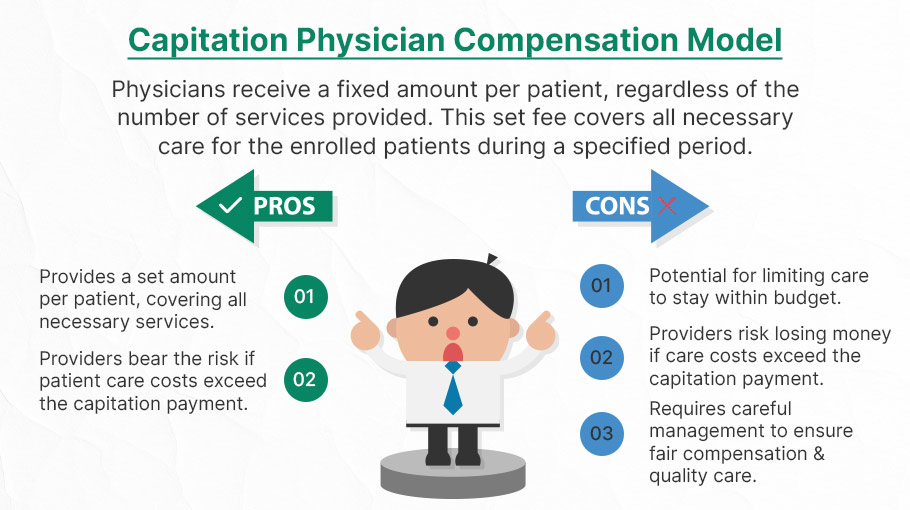
Capitation is a type of healthcare payment system in which a physician or hospital is paid a fixed amount of money per patient for a prescribed period by an insurer or physician association. The cost is based on the expected healthcare utilization costs for a group of patients for that year.
With capitation, the physician—otherwise known as the primary care physician— is paid a set amount for each enrolled patient whether a patient seeks care or not. The PCP is usually contracted with an HMO whose role it is to recruit patients.
According to Richard Eskow, CEO of Health Knowledge Systems of Los Angeles, capitated medical reimbursement has been used in one form or another, in every attempt at healthcare reform since the Norman Conquest. Some even say an earlier variant existed in ancient China [personal communication].
Initially, when Henry I assumed the throne of the newly combined kingdoms of England and Normandy, he initiated a sweeping set of healthcare reforms. Historical documents, though muddled, indicate that soon thereafter at least one “physician,” John of Essex, received a flat payment honorarium of one penny per day for his efforts. Historian Edward J. Kealey opined that sum was roughly equal to that paid to a foot-soldier or a blind person. Clearer historical evidence suggests that American doctors in the mid-19th century were receiving capitation-like payments. No less an authoritative figure than Mark Twain, in fact, is on record as saying that during his boyhood in Hannibal, MO his parents paid the local doctor $25/year for taking care of the entire family regardless of their state of health.
Later, Sidney Garfield MD [1905-1984] is noted as one of the great under-appreciated geniuses of 20th century American medicine stood in the shadow cast by his more celebrated partner, Henry J. Kaiser. Garfield was not the first physician to embrace the notion of prepayment capitation, nor was he the first to understand that physicians working together in multi-specialty groups could, through collaboration and continuity of care, outperform their solo practice colleagues in almost every measure of quality and efficiency. The Mayo brothers, of course, had prior claim to that distinction. What Garfield did, was marry prepayment to group practice, providing aligned financial incentives across every physician and specialty in his medical group, as well as a culture of group accountability for the care of every member of the affiliated health plan. He called it “the new economics of medicine,” and at its heart was a fundamentally new paradigm of care that emphasized – prevention before treatment – and health before sickness. Under his model: the fewer the sick – the greater the remuneration. And: the less serious the illness, the better off the patient and the doctors.
Such ideas were heresy to the reigning fee-for-service, solo practice, ideologues of the mainstream medical establishment of the 1940s and ‘50s, of course. Throughout the period, Garfield and his group physicians were routinely castigated by leaders of the AMA and county medical associations as socialistic and unethical. The local medical associations in Garfield’s expanding service areas – the San Francisco Bay Area, Los Angeles, and Portland, Oregon – blocked group practice physicians from association membership, effectively shutting them out of local hospitals, denying them patient referrals or specialty society accreditation. Twice in the 1940s, formal medical association charges were brought against Garfield personally, at one time temporarily succeeding in suspending his license to practice medicine.
Of course, capitation payments made a comeback in the first cost-cutting managed care era of the 1980-90s because fee-for-service medicine created perverse incentives for physicians by paying more for treating illnesses and injuries than it does for preventing them — or even for diagnosing them early and reducing the need for intensive treatment later. Nevertheless, the modern managed care industry’s experience with capitation wasn’t initially a good one. The 1980-90s saw a number of HMOs attempt to put independent physicians, especially primary care doctors, into a capitation reimbursement model. The result was often negative for patients, who found that their doctors were far less willing to see them — and saw them for briefer visits — when they were receiving no additional income for their effort. Attempts were also made to aggregate various types of health providers — including hospitals and physicians in multiple specialties — into “capitation groups” that were collectively responsible for delivering care to a defined patient group. These included healthcare facilities and medical providers of all types: physicians, osteopaths, podiatrists, dentists, optometrists, pharmacies, physical therapists, hospitals and skilled nursing homes, etc.
However, the healthcare industry isn’t collective by nature, and these efforts tended to be too complicated to succeed. One lesson that these experiments taught is that provider behavior is difficult to change unless the relationship between that behavior and its consequences is fairly direct and easy to understand.
Today, the concept of prepayment and medical capitation is to uncouple compensation from the actual number of patients seen, or treatments and interventions performed. This is akin to a fixed price restaurant menu, as opposed to an àla carte eatery.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 14, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
BREAKING NEWS
Law enforcement officials in Utah released a video of the suspected shooter in the assassination of Turning Point USA co-founder and CEO Charlie Kirk, saying that the person wore Converse tennis shoes and left a hand print and a shoe print at the scene.
The suspect in Charlie Kirk’s assassination has been identified as Tyler Robinson, a 22-year-old Utah resident. Law enforcement sources told the Daily Mail that Robinson was taken into custody as the alleged assassin who killed Kirk at a rally at Utah Valley University on Wednesday.
Before today, forensic podiatry has even made it into the public zeitgeist with the hit TV show “Bones” which premiered on September 13, 2005, and concluded on March 28, 2017, airing for 246 episodes over 12 seasons. The show was based on forensic anthropology and forensic archaeology, with each episode focusing on the mystery behind human body remains brought in for examination and identification.
In one show, eight pairs of dismembered feet washed ashore after a flood on the U.S.-Canada border, but things didn’t add up when only seven pairs of feet were identified as research corpses from a nearby university body farm.
When the fictional Canadian forensic podiatrist Dr. Douglas Filmore took the remains back to Canada, he had to form a jurisdictional alliance with the United States to match the pairs of feet and identify the victims. A rare and expensive pair of sneakers led the team to the victim’s murderer.
In 2016, an actual forensic podiatry club was started at the Barry University School of Podiatric Medicine. And, a formal class covering aspects of forensic podiatry is held at the New York College of Podiatric Medicine. Students exit the class with an in depth knowledge of forensic podiatry and other legal knowledge applicable to current cases.
More expertly, real-life colleague Michael Steven Nirenberg DPMactually testified in the murder trial of defendants Kailie Brackett and Donnell Dana with the state calling three witnesses to testify, including the podiatrist who claimed Brackett’s footprints match the ones found in blood at the apartment of the victim, Kimberly Neptune. The forensic podiatrist focused on the footprints discovered at Neptune’s apartment, using prints and images of the defendant’s feet taken by law enforcement. After study, he claimed the prints at the scene bore a resemblance to Kailie Brackett’s in the width of the foot. The defense questioned the field of forensic podiatry and pressed Dr. Nirenberg on whether the measurements would be altered depending on how thick the sock covering the foot was woven.
Dr. Nirenberg was also interviewed on National Public Radio’s Morning Edition on April 14th 2023 about the gait of the bombing suspect associated with the capital riot on Wednesday January 6th, 2021. Dr. Nirenberg is president of the American Society of Forensic Podiatry and co-editor of the textbook: “Forensic Gait Analysis: Principles and Practice”. The bombing suspect had placed bombs at the DNC and RNC headquarters in Washington, DC on the night before. NPR asked Dr. Nirenberg to comment on the features of the person’s gait.
Additionally, Nirenberg was interviewed by Nancy Grace on her TV show Crime Stories. Grace interviewed Nirenberg about his forensic podiatry work in helping to solve the murder of a mother of 3 who was killed in a church. The case remains unsolved. The episode, “Fitness-Mom Missy Bevers Bludgeoned Dead in Creekside Church” aired June 6th, 2024 and is available online at Merit+ TV.
And, Netflix’s 2023 docu-series, “Till Murder Do Us Part”, recounts the killings of Derek and Nancy Haysom by including a series of interviews with a cast of real people. The four-part docu-series revolves around the unpacking of how a wealthy couple was murdered in Virginia in 1985. It also focuses on how the suspects, Elizabeth Haysom, and her boyfriend, Jens Soehring, betrayed each other during the trial. Dr. Sarah Reel DPM was the forensic podiatrist who was involved with Jens’ and Elizabeth’s footprint examination. Dr. Reel pointed out that, statistically, there was no difference “between a bare footprint and a socked footprint.” The doctor suggested that Jens’ reference footprint matched closely with the crime scene footprint.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on September 10, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITIONS
By Staff Reporters
***
***
Rate Review & the 80/20 Rule
The health care law provides 2 ways to hold insurance companies accountable and help keep your costs down: Rate Review and the 80/20 rule.
Rate Review
Rate Review helps protect you from unreasonable rate increases. Insurance companies must now publicly explain any rate increase of 15% or more before raising your premium. This does not apply to grandfathered plans.
The 80/20 Rule generally requires insurance companies to spend at least 80% of the money they take in from premiums on health care costs and quality improvement activities. The other 20% can go to administrative, overhead, and marketing costs.
The 80/20 rule is sometimes known as Medical Loss Ratio, or MLR. If an insurance company uses 80 cents out of every premium dollar to pay for your medical claims and activities that improve the quality of care, the company has a Medical Loss Ratio of 80%.
Insurance companies selling to large groups (usually more than 50 employees) must spend at least 85% of premiums on care and quality improvement.
If your insurance company doesn’t meet these requirements, you’ll get a rebate on part of the premium that you paid.
Will I get a rebate check from my insurance company?
If your insurance company doesn’t meet its 80/20 targets for the year, you’ll get back some of the premium that you paid.
You may see the rebate in a number of ways:
A rebate check in the mail
A lump-sum deposit into the same account that was used to pay the premium, if you paid by credit card or debit card
A direct reduction in your future premium
Your employer may also use one of the above rebate methods, or apply the rebate in a way that benefits employees
If you or your employer will get a rebate, your insurance company must notify you by August 1.
If you have an individual insurance policy, you’ll get the rebate directly from your insurance company.
For small group and large group plans, the rebate is usually paid to the employer. It may use one of the above rebate methods, or apply the rebate in a way that benefits employees.
FYI: The 80/20 rebate rules don’t apply when an insurance company has fewer than 1000 enrollees in a particular state or market.
For Rate Review: These requirements don’t apply to grandfathered plans. Check your plan’s materials or ask your employer or your benefits administrator to find out if your health plan is grandfathered.
For the 80/20 Rule: These rights apply to all individual, small group, and large group health plans, whether your plan is grandfathered or not.
Classic: The portion of medical expenses a patient is responsible for paying.
Modern: Refers to the maximum you will pay during your policy period, which is typically a year, before your plan starts to pay 100% of your allowed amount. The costs of your deductible, co-pay, and co-insurance are included here, but not your premium.
Classic: “Out-of-network” health care providers do not have an agreement with your insurance company to provide care. While insurance companies may have some out-of-network benefits, medical care from an out-of-network provider will usually cost more out-of-pocket than an in-network provider.
Modern: The amount that a health care insurance plan will contribute toward out-of-network services will vary by your insurance company and is often based on a “reasonable and customary” amount that the service should cost
Example: If you go to an out-of-network dentist and are billed $300 for the service, your insurance company may contribute $200 toward paying this cost because $200 is the amount it has decided is “reasonable and customary” for this service. When out-of-network, any remaining cost above this amount ($100 in this case) may have to be fully covered by the person receiving care. When out-of-network, the usual coinsurance rates that apply in-network may not apply out-of-network. Additionally, out-of-network service costs may not count toward an annual deductible.
Posted on September 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Primary – Secondary – Tertiary Care
By A.I. and Staff Reporters
***
***
In medicine, there are four levels of care: primary, secondary, tertiary, and quaternary. The levels of care refer to the complexity of the medical cases that doctors and healthcare providers treat and the skills and specialties of the providers.
Primary care involves consulting with a primary care provider. Secondary care refers to seeing a specialist such as a dermatologist, neurologist or oncologist. Tertiary care is specialized care in a hospital setting such as brain surgery, renal dialysis or heart surgery.
Quaternary care is thus an advanced level of specialized care.
Classic: Sometimes used as an extension of tertiary medical and surgical care in reference to advanced levels of medicine which are highly specialized and not widely accessed by most patients.
Modern: A higher level of specialized care within a hospital. Experimental medicine and some types of uncommon diagnostic or surgical procedures are also considered quaternary care.
According to the Wonca International Dictionary for General/Family Practice -Quaternary Prevention [QP] – is defined as: ‘Action taken to identify patient at risk of over medicalization, to protect him/her from new medical invasion, and to suggest to him interventions, which are ethically acceptable’.
Examples: Types of quaternary care include: experimental medicine, procedures and uncommon and specialized surgeries. This includes sub-specialty services such as advanced trauma care and organ [heart, lung, liver, kidney, etc] transplantation.
If an insurer uses 80 cents out of every premium dollar to pay its customers’ medical claims and activities that improve the quality of care, the company has a medical loss ratio of 80%. A medical loss ratio of 80% indicates that the insurer is using the remaining 20 cents of each premium dollar to pay overhead expenses, such as marketing, profits, salaries, administrative costs, and agent commissions.
The Affordable Care Act sets minimum medical loss ratios for different markets, as do some state laws.
Posted on September 2, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
This September, along with survivors, caregivers, advocates, and healthcare professionals, HealthTree is commemorating Blood Cancer Awareness Month!
In this article, you’ll learn why this month receives special attention in the HealthTree community and what they will feature throughout September so you don’t miss a thing.
Posted on September 1, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
Dear Medical Executive-Post Readers and Subscribers
***
HISTORY OF LABOR DAY
The first Labor Day holiday was celebrated on Sept. 5th, 1882, in New York City, in accordance with the plans of the Central Labor Union. President Grover Cleveland signed a law on June 28th, 1894, that made the first Monday in September of each year a national holiday, according to the Department of Labor.
***
***
MY SEPTEMBER HEALTH RE-SET
To give my health a boost after Labor Day, I’m taking a complete break from alcohol, sugar, cookies, ice cream, coffee and tea for the entire month of September. Besides that, I’ll also prioritize sleep and increase my exercise from 7 to at least 10 times [hours] a week. This will allow me to focus on my diet and mental well-being. It’s essentially a month of health and wellness rejuvenation.
I’ve chosen to focus on alcohol and sugar because I want to challenge the idea that moderate drinking is part of a healthy lifestyle. In reality, only those who maintain a healthy lifestyle can afford to enjoy alcohol in moderation. But, sugar is everywhere and must be minimized for Type II diabetes and weight control.
Moreover, the long-term and excessive intake of sugary beverages and refined sugars can negatively impact your overall caloric intake and create a domino effect on your health. For example, excess sugar in the body can turn into fat deposits and lead to fatty liver disease.
A low sugar diet can help you lose weight and also help you manage and/or prevent diabetes, heart disease and stroke, reduce inflammation, and even improve your mood and the health of your skin. That’s why the low sugar approach is a key tenet of other well-known healthy eating patterns, such as the Mediterranean diet and the DASH diet.
QUESTION: And so, do you also commit to such “factory resets” now and then? Please comments.
Do, enjoy the Labor Day Weekend, Bar-B-Ques with friends, family and colleagues. And, I hope you continue to find the Medical Executive-Post useful!
Many thanks for your likes and referrals. Dr. David Edward Marcinko MBA MEd CMP [Editor and Chief]
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 31, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A.I.
***
***
Philosophy (‘love of wisdom’) is a systematic study of general and fundamental questions concerning topics like existence, reason, knowledge, value, mind and language. It is a rational and critical inquiry that reflects on its methods and assumptions.
Philosophy is broadly divided into several main branches that explore fundamental questions about reality, knowledge, ethics, logic, and values, each addressing different aspects of human thought and existence.
Metaphysics This branch explores the nature of reality and existence. It addresses questions about what things exist, the nature of objects and their properties, time and space, causality, and the mind-body relationship.
Epistemology Epistemology studies knowledge and belief. It concerns how we know what we know, the nature and limits of knowledge, justification, and skepticism.
Ethics (Moral Philosophy) Ethics examines what is right and wrong, good and bad. It investigates moral values, principles, and theories about how people ought to act and what constitutes a good life.
Logic Logic deals with the rules of correct reasoning. It studies principles of valid inference, argument structure, deduction, and induction, enabling critical thinking and sound judgment.
Aesthetics This branch explores questions related to beauty, art, and taste. It considers what constitutes aesthetic value and how art influences human experience.
Posted on August 29, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko; MBA MEd
***
***
Healthcare comes with its share of mental challenges, especially considering that clinicians often care for patients when they’re in difficult and sometimes tragic situations. New research shows that even the path to getting into the workforce can be a challenge, with some physicians burning out before they make it to graduation.
***
American medicine is undergoing vast changes, placing the status of physicians in the medical industrial complex at great risk. Most physicians feel overwhelmed by increasing bureaucratic mandates from insurers, hospitals, and government. At the same time, physicians are the front line employees of healthcare and assume the majority of the risk for patient care. This has left many in the profession with increasing disillusionment.
Samantha Meltzer-Brody a psychiatrist and director of, Taking Care of Our Own, University of North Carolina, Chapel Hill, NC states it best:
“Daily, I am contacted by good doctors who are struggling with symptoms of burnout syndrome and who have become overwhelmed by the challenges of attempting to practice medicine in today’s health care environment. As a psychiatrist who runs a program to address and treat these distressed doctors, I am troubled by the ever-growing number of calls I receive.”
What causes physician burnout?
The “Big 4” factors known to contribute to stress and burnout include:
Time pressure, especially in patient visits or documentation
Lack of control over work environment
Chaotic, fast-paced workplaces
Culture of the organization, specifically a culture that does not emphasize communication, cohesion, trust, and alignment of values between clinicians and their leaders
In addition to burnout rates, these factors can be assessed to help direct interventions toward those drivers that are most likely to be contributing to burnout at your organization.
The burned-out physician is exhausted — mentally and physically — and often no longer able to find empathy or connection with patients. The question of how to escape from what has become a highly unpleasant situation becomes a frequent one. Given the high demands of the profession and serious consequences of mistakes, the burned-out doctor is a potentially impaired one. And the impaired physician is not able to maintain the unflappable, perpetually cool under fire, always objective, professional and yet compassionate demeanor that is expected by society. Worst of all, the impaired physician is at great risk for developing depression, suicidal ideation, or a serious addiction.
The doctors who contact me report feeling beaten down by an increasingly hostile work environment. They say that they don’t have time to take care of patients the way they envisioned when they decided to apply to medical school. Many describe feeling betrayed by a system that they say seems focused on achieving the bottom line with little regard for the impact on both doctors and patients.
Most of these doctors report spending a significant amount of their time dealing with the electronic medical record and documentation. The ratio of time spent on doctor-patient
interactions compared to physician-computer ones appears so horribly skewed that it has reached the point of complete dysmorphia. These good physicians call me when they feel like they can’t continue any longer in the profession. They want to quit medicine. They report a loss of joy and meaning in their work. They describe the toll that the profession has had on their mental health, physical health, and personal lives. And most wrenchingly, they don’t see an end.
What can we do? There are no easy answers to the complex issues that threaten our profession. “The Taking Care of Our Own Program…has had an over 200% rate of growth in the first year, reflecting the enormous need…”
Burned out physicians will eventually be labeled as disruptive, impaired, an outlier or arrogant. There’s a reason it’s difficult and extremely expensive for physicians to find disability insurance; psychiatric claims. Burnout leads to depression, anxiety, PTSD, suicide, divorce, drug abuse, surly behaviors and interactions, etc. It’s nothing new; it’s been occurring for a long time. Go without routine sleep, eat erratically, work long hours, operate under constantly stressful situations and have no time for your family or self and most individuals will de-compensate physically and psychologically within weeks.
Conclusion
Physicians operate within these parameters year after year.
How are they to remain healthy, functional humans? They can’t. Even a superhero couldn’t, yet physicians are expected to endure and thrive under such conditions.
If a physician makes a single mistake, or snaps just one day, their entire career is on the line.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 26, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
A paradox is a self-contradictory statement. And, the ancient Greeks were well aware that a paradox can take us outside our usual way of thinking. They combined the prefix para – (“beyond” or “outside of”) with the verb dokein (“to think”), forming paradoxos, an adjective meaning “contrary to expectation.” Latin speakers used that word as the basis for a noun paradoxum, which English speakers borrowed during the 1500s to create paradox.
***
***
Paradox of Education: Cumulative Advantage and Disadvantage
Classic Definition: Social status snowballs in either direction because people like associating with successful people, so doors are opened for them. And, folks avoid associating with unsuccessful people, for whom doors are closed.
Modern Circumstance: Education’s positive effect on health gets larger as people age. The large socioeconomic differences in health among older Americans mostly accrue earlier in adulthood on gradients set by educational attainment. Education develops abilities that help individuals gain control of their own lives, encouraging and enabling a healthy life.
Paradox Example: The health-related consequences of education cumulate on many levels, from the socioeconomic (including work and income) and behavioral (including health behaviors like exercising) to the physiological and intra-cellular. Some accumulations even influence each other.
In particular, a low sense of control over one’s own life accelerates physical impairment, which in turn decreases the sense of control. That feedback progressively concentrates good physical functioning and a firm sense of personal control together in the better educated while concentrating physical impairment and a sense of powerlessness together in the less well educated, creating large differences in health in old age.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
The so-called money factor (abbreviated as MF on invoices) is a number in a decimal form that dealers use to calculate the APR of a car lease. It’s a major part of your monthly payment and dealers are known to jack up the money factor to pad their profits.
Most doctors don’t ask to see it because they’re not aware of it or don’t know how to calculate it. Ask to see the money factor, then multiply it by 2,400.
For example, if the money factor is .00150, you multiply it by 2,400 to get 3.6%. If that’s higher than the prevailing rate, you have room to talk them down.
How to reduce it
So how do you get a good interest rate when you lease a vehicle? The same way you do when borrowing for any other reason, whether it’s buying a home or applying for a personal loan: by having good credit. This may reduce your interest rate because you’ll represent a lower risk to a lender.
A high residual value on the car could also help you get a better interest rate. A higher residual value means you’d have lower monthly payments because there would be less depreciation on the vehicle. Since interest is applied to your monthly payment, a lower monthly payment would equate to reduced interest charges.
The money factor is one of the many numbers you may want to learn about when leasing a car. It’s one of the transactional costs that come with leasing, and allows dealers and finance companies to make a profit on every lease they execute. As a consumer, it’s a smart idea to learn the financial implications of this number and how it’ll affect your overall costs over the course of a multi-year lease.
***
***
If the interest rate is too high, you may need to shop around for a better rate, negotiate with the dealer or lender to lower the money factor, or consider leasing another vehicle that’s more in line with your budget. Either way, make sure you explore all your financial options before taking a car off the lot.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 24, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
Dr. David Edward Marcinko with non-VIP patients
***
The House Committee on Oversight and Government Reform expanded its investigation of the cover-up of former President Joe Biden’s health, prostate cancer, and mental decline.
On June 4th, Chairman James Comer subpoenaed five former senior White House aides to appear for transcribed interviews in addition to Biden’s physician, Kevin O’Connor, M.D. In May, Biden revealed he was diagnosed with advanced prostate cancer. The announcement left the public dumbfounded.
At 82, having spent more than five decades as a president, vice president and senator, Biden had access to world-class medical care. Donald Trump Jr. was one of many political observers who speculated the diagnosis might have been covered up to win the 2020 election. And, Biden’s doctors may have followed standard medical guidelines, and the recommendations about screenings for people of different ages can be controversial, writes health care economist Devon Herrick at the Goodman Institute Health Care Blog.
“Experts often say that men are more apt to die with prostate cancer than from prostate cancer,” wrote Herrick. “There is even some disagreement about whether doctors should treat most occurrences of prostate cancer in older men. That partly explains why Biden had not been screened in a decade.”
Screenings can be costly, time-consuming and uncomfortable, and false positive results can lead to invasive procedures that do not markedly extend life or health. Biden made his first public remarks about his cancer after a Memorial Day event. Biden said he was “feeling good” and expected to “be able to beat this.”
QUESTION: So, was this a case of VIP Patient Paradox?
***
DEFINITION: “VIP medical patient paradox syndrome” is a term coined in 1964 by the psychiatrist Walter Weintraub to describe an intriguing paradox: Throughout history, the rich and famous, with all their resources and fancy doctors, have often received worse medical treatment, and suffered from worse health outcomes, than the average person.
Example: When physicians afford “special privileges” to their powerful patients, from “Mad King” George III to Michael Jackson, they seem to get sicker and even die.
While Weintraub, a psychoanalyst, attributed the problem in part to doctors unconsciously resenting their influential patients, it seems doctors simply get starstruck around famous people and high-ranking figures. Despite their medical expertise, these physicians find themselves opting out of basic tests for “privacy” or prescribing dangerous medications for “comfort.”
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 22, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
Medicine today is vastly different than a generation ago, and all health care professionals need new skills to be successful and reduce the emerging risks outlined in this textbook, as well as the “unknown-unknowns” elsewhere. Traditionally, the physician was viewed as the “captain of the ship”. Today, their role may be more akin to a ship’s navigator, using clinical, teaching skills and knowledge to chart the patient’s course through a confusing morass of insurance requirements, fees, choices, rules and regulations to achieve the best attainable clinical outcomes.
This new leadership paradigm includes many classic business school principles, now modified to fit the decade long PP-ACA, the era of health reform, and modern technical connectivity and EMRs.
Thus, the physician must be a subtle guide on the side; not bombastic sage on the stage. These, newer health 3.0 leadership philosophies might include:
•Negotiation – working to optimize appropriate treatment plans; ie., quality of life versus quantity of life, •Team play – working in concert with other allied healthcare professionals to coordinate care delivery ,ithin a clinically appropriate and cost-effective framework; •Working within the limits of competence – avoiding the pitfalls of the medical generalist versus the specialist that may restrict access to treatment, medications, physicians and facilities by clearly acknowledging when a higher degree of service is needed on behalf of the patient – all while embracing holistic primary care; •Respecting different cultures and values – inherent in the support of the medical Principle of Autonomy is the acceptance of values that may differ from one’s own. As the US becomes more culturally hetero geneous, medical providers are called upon to work within, and respect, the socio-cultural and/or spiritual framework of patients, students and their families; •Seeking clarity on what constitutes marginal care – within a system of finite resources; providers are called upon to openly communicate with patients regarding access to marginal medical information and/or treatments. •Supporting evidence-based practice – healthcare providers, should utilize outcomes data to reduce variation in treatments to achieve higher efficiencies and improved care delivery thru evidence based medicine [EBM]; •Fostering transparency and openness in communications – healthcare professionals should be willing, and prepared, to discuss all aspects of care, especially when discussing end-of-life issues or when problems arise; •Exercising decision-making flexibility – treatment algorithms, templates and clinical pathways are useful tools when used within their scope; but providers must have the authority to adjust the plan if circumstances warrant.
Becoming skilled in the art of listening and interpreting — In her ground-breaking book, Narrative Ethics: Honoring the Stories of Illness, Rita Charon, MD PhD, a professor at Columbia University, writes of the extraordinary value of using the patient’s personal story in the treatment plan. She notes that, “medicine practiced with narrative competence will more ably recognize patients and diseases; convey knowledge and regard, join humbly with colleagues, and accompany patients and their families through ordeals of illness.” In many ways, attention to narrative returns medicine full circle to the compassionate and caring foundations of the patient-physician relationship.
These thoughts represent only a handful of examples to illustrate the myriad of new skills that tomorrows’ healthcare professionals must master in order to meet their timeless professional obligations of compassionate care and contemporary treatment effectiveness; all within the context modern risk management principles.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 20, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
LEADERSHIP versus MANAGEMENT
***
***
By Dr. David Edward Marcinko MBA MEd
By Professor Gary A. Cook PhD
By Professor Eugene Schmuckler PhD MBA MEd CTS
Many of us have encountered a person who may intellectually be at upper levels, but whose ability to interact with others appears to that of one who is highly immature. This is the individual who is prone to becoming angry easily, verbally attacks co-workers, is perceived as lacking in compassion and empathy, and cannot understand why it is difficult to get others to cooperate with them and their agendas.
THINK: Sheldon Cooper PhD D.Sc MA BA of the The Big Bank Theory TV show.
The concept of Emotional Intelligence [EQ] was brought into the public domain when Daniel Goleman authored a book entitled, Emotional Intelligence.” According to Goleman, emotional intelligence consists of four basic non-cognitive competencies: self awareness, social awareness, self management and social skills. These are skills which influence the manner in which people handle themselves and their relationships with others. Goleman’s position was that these competencies play a bigger role than cognitive intelligence in determining success in life and in the workplace. He and others contend that emotional intelligence involves abilities that may be categorized into five domains:
Self awareness: Observing and recognizing a feeling as it happens.
Managing emotions: Handling feelings so that they are appropriate; realizing what is behind a feeling; finding ways to handle fears and anxieties, anger and sadness.
Motivating oneself; Channeling emotions in the service of a goal; emotional self control; delaying gratification and stifling impulses.
Empathy: Sensitivity to others’ feelings and concerns and taking their perspective appreciating the differences in how people feel about things.
Handling relationships: Managing emotions in others; social competence & social skills.
In 1995, Goleman then expanded on the works of Howard Gardner, Peter Salovey and John Mayer. He further defined Emotional Intelligence as a set of competencies demonstrating the ability one has to recognize his or her behaviors, moods and impulses and to manage them best, according to the situation. Mike Poskey, in “The Importance of Emotional Intelligence in the Workplace.” continued this definition by stating that emotional intelligence is considered to involve emotional empathy; attention to, and discrimination of one’s emotions; accurate recognition of one’s own and others’ moods; mood management or control over emotions; response with appropriate emotions and behaviors in various life situations (especially to stress and difficult situations); and balancing of honest expression of emotions against courtesy, consideration, and respect.
Source: Emotional Intelligence: what is and why it matters” – Cary Cherniss, PhD, presented at the annual conference of the Society of Industrial and Organizational Psychology, April 2000.
EQ differs from what has generally been considered intelligence which is described in terms of one’s IQ.
Traditional views of intelligence focused on cognition, memory and problem solving. Even today individuals are evaluated on the basis of cognitive skills. Entrance tests for medical, law, business, undergraduate and graduate schools base admissions in large part on the scores of the SAT, GMAT, LSAT, MCAT, etc. Without question, cognitive ability is critical but has been demonstrated, it is not a very good predictor of future direct job performance and indirect liability management. In fact, in 1940, David Wechsler the developer of a widely used intelligence test made reference to “non-intellective” elements. By this Wechsler meant affective, personal and social factors.
Source: Non-Intellective factors in intelligence. Psychological Bulletin, 37, 444-445.
Goleman became aware of the work of Salovey and Mayer having trained under David McClelland and was influenced by McClelland’s concern with how little traditional tests of cognitive intelligence predicted success in life. In fact, a study of 80 PhDs in science underwent a battery of personality tests, IQ tests and interviews in the 1950s while they were graduate students at Berkeley. Forty years later they were re-evaluated and it turned out that social and emotional abilities were four times more important than IQ in determining professional success and prestige.
Source: Feist & Barron: Emotional Intelligence and academic intelligence in career and life success. Paper presented at the Annual Convention of the American Psychological Society, San Francisco, 1996.
Undoubtedly, we want to have individuals work with us who have persistence which enables to them have the energy, drive, and thick skin to develop and close new business, or to work with the patients and other members of the staff. It is important to note that working alongside one with a “good” personality may be fun, energetic, and outgoing.
However, a “good personality does not necessarily equate to success. An individual with a high EQ can manage his or her own impulses, communicate effectively, manage change well, solve problems, and use humor to build rapport in tense situations. This clarity in thinking and composure in stressful and chaotic situations is what separates top performers from weak performers.
Poskey outlined a set of five emotional intelligence competencies that have proven to contribute more to workplace achievement than technical skills, cognitive ability, and standard personality traits combined.
***
***
A. Social Competencies: Competencies that Determine How We Handle Relationships
Intuition and Empathy – Our awareness of others’ feelings, needs, and concern. He suggested that this competency is important in the workplace for the following reasons:
Understanding others: an intuitive sense of others’ feelings and perspectives, and showing an active interest in their concerns and interests
Patient service orientation: the ability to anticipate, recognize and meet customer’s’ (patients) needs
People development: ability to sense what others need in order to grow, develop, and master their strengths
Leveraging diversity: cultivating opportunities through diverse people.
B. Political Acumen and Social Skills: Our adeptness at inducing desirable responses in others. This competency is important for the following reasons:
Influencing: using effective tactics and techniques for persuasion and desired results.
Communication: sending clear and convincing messages that are understood by others
Leadership: inspiring and guiding groups of people
Change catalyst: initiating and/or managing change in the workplace
Conflict resolution: negotiating and resolving disagreements with people
Collaboration and cooperation: working with coworkers and business partners toward shared goals
Team capabilities: creating group synergy in pursuing collective goals.
C. Personal Competencies: Competencies that determine how we manage ourselves
D. Self Awareness: Knowing out internal states, preferences, resources, and intuitions. This competency is important for the following reasons.
Emotional awareness: recognizing one’s emotions and their effects and impact on those around us
Accurate self-assessment: knowing one’s strengths and limits
Self-confidence: certainty about one’s self worth and capabilities
Self-Regulation: managing one’s internal states, impulses, and resources. This competency is important in the workplace for the following reasons.
Self-control: managing disruptive emotions and impulses
Trustworthiness: maintaining standards of honesty and integrity
Conscientiousness: taking responsibility and being accountable for personal performance
Adaptability: flexibility in handling change
Innovation: being comfortable with an openness to novel ideas, approaches, and new information.
E. Self-Expectations and Motivation: Emotional tendencies that guide or facilitate reaching goals. This competency is important in the workplace for the following reasons.
Achievement drive: striving to improve or meet a standard of excellence we impose on ourselves
Commitment: aligning with the goals of the group or the organization
Initiative: readiness to act on opportunities without having to be told
Optimism: Persistence in pursuing goals despite obstacles and setbacks
A note of caution is necessary. Goleman and Salovey both stated that emotional intelligence on its own is not a strong predictor of job performance. Instead they contend that it provides the bedrock for competencies that are predictors.
Obviously, EQ is an important attribute and it behooves each of us to promote emotional intelligence in the workplace. A number of guidelines have been developed for the Consortium for Research on Emotional Intelligence in Organizations by Goleman and Cherniss. The guidelines cover 21 phases which include preparation, training, transfer and evaluation.
Assess the organization’s needs: Determine the competencies that are most critical for effective job performance in a particular type of job. In doing so, us a valid method, such as the comparison of the behavioral interviews of superior performs and average performers. Also make sure the competencies to be developed are congruent with the organization’s culture and overall strategy.
Assess the individual: This assessment should be based on the key competencies needed for a particular job, and the data should come from multiple sources using multiple methods to maximize credibility and validity.
Deliver assessments with care: Give the individual information on his/her strengths and weaknesses. In doing so, try to be accurate and clear. Also, allow plenty of time for the person to digest and integrate the information. Provide feedback in a safe and supportive environment in order to minimize resistance and defensiveness. Avoid making excuses or downplaying the seriousness of deficiencies.
Maximize choice: People are motivated to change when they freely choose to do so. As much as possible, allow people to decide whether or not they will participate in the development process, and have them change goals themselves.
Encourage people to participate: People will be more likely to participate in development efforts if they perceive them to be worthwhile and effective. Organizational policies and procedures should encourage people to participate in development activity, and supervisors should provide encouragement and the necessary support. Motivation will be enhanced if people trust the credibility of those who encourage them to undertake the training.
Link learning goals to personal values: People are most motivated to pursue change that fits with their values and hopes. If a change matters little to people, they won’t pursue it. Help people understand whether a given change fits with what matters most to them.
Adjust expectations: Builds positive expectations by showing learners that social and emotional competence can be improved and that such improvement will lead to valued outcomes. Also, make sure that the learner has a realistic expectation of what the training process will involve.
Gauge readiness: Assess whether the individual is ready for training. If the person is not ready because of insufficient motivation or other reasons, make readiness the focus of intervention efforts.
Foster a positive relationship between the trainers and learners: Trainers who are warm, genuine, and empathic our best able to engage the learners in the change process. Select trainers who have these qualities, and make sure that they use them when working with the learners.
Make change self-directed: Learning is more effective when people direct their own learning program, tailoring it to their unique needs and circumstances. In addition to allowing people to set their own learning goals, let them continue to be in charge of their learning throughout the program, and tailor the training approach to the individual’s learning style.
Set clear goals: People need to be clear about what the competence is, how to acquire it, and how to show it on the job. Spell out the specific behaviors and skills that make up the target competence. Make sure that the goals are clear, specific, and optimally challenging.
Break goals into manageable steps: change. That is more likely to occur if the change process is divided into manageable steps. Encourage both trainers and trainees to avoid being overly ambitious.
Provide opportunities to practice: Lasting change requires sustained practice on the job and elsewhere in life. An automatic habit is being unlearned and different responses are replacing it. Use naturally occurring opportunities for practice at work, and in life. Encourage the trainees to try the new behaviors repeatedly and consistently over a period of months.
Give performance feedback: Ongoing feedback encourages people and direct change. Provide focused and sustained feedback as the learners practice new behaviors. Make sure that supervisors, peers, friends, family members-or some combination of these- give periodic feedback on progress.
Rely on experiential methods: Active, concrete, experiential methods tend to work best for learning social and emotional competencies. Development activities that engage all the senses and our dramatic and powerful can be especially effective.
Build in support: Change is facilitated through ongoing support of others who are going through similar changes. Programs should encourage the formation of groups where people give each other support, throughout the change effort. Coaches and mentors also can be valuable in helping support the desired change.
Use models: Use modern webinars, patient portals, live or videotaped models that clearly show how the competency can be used in realistic situations. Encourage learners to study, analyze, and emulate the models.
Enhance insight: Self-Awareness is the cornerstone of emotional and social competence. Help learners acquire greater understanding about how their thoughts, feelings, and behavior affect themselves and others.
Prevent relapse: Use relapse prevention, which helps people use lapses and mistakes as lessons to prepare themselves for further efforts.
Moreover:
Encourage use of skills on the job: Supervisors, peers and subordinates should reinforce and reward learners for using their new skills on the job. Coaches and mentors also can serve this function. Also, provide prompts and cues, such as through periodic follow-ups. Change also is more likely to indoor. When high status persons, such as supervisors and upper-level management model it.
Develop an organizational culture that supports learning: Change will be more enduring if the organization’s culture and tone support the change and offer a safe atmosphere for experimentation.
Finally, see if the development effort has lasting effects evaluated. When possible, find a true set of measures of the competence or skill, as shown on the job, before and after training, and also at least two months later. One-year follow-ups also are highly desirable. In addition to charting progress on the acquisition of competencies, also assess the impact on important job related outcomes, such as performance measures, and indicators of adjustments such as absenteeism, grievances, health status, etc.
Managers V. Leaders
These abilities are important for one to be successful as a manager and even more so as a leader, or physician executive. But, before we begin an examination of strategic leadership, it is necessary to make a deeper distinction between a manager and a leader. There are many different definitions as well as descriptions regarding leadership and management.
Many people talk as though leadership and management is the same thing. Fundamentally, they are quite different. Management focuses on work. We manage work activities such as money, time, paperwork, materials, equipment, and personnel, among other things. As can be found in any basic book on management, management focuses on planning, organizing, controlling, coordinating, budgeting, finance and money management as well as decision making. In effect, managers are generally those individuals who have been given their authority by virtue of their role. It is the function of a manager to ensure that the work gets done as well as to oversee the activities of others. In many healthcare organizations we find that those individuals elevated to a managerial position occur as a result of being a high performer on their previous assignment. A manager receives authority on the basis of role; while a leader’ authority is more innate in nature.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 19, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
In today’s dynamic economic landscape, the concept of a “side hustle” has evolved from a mere trend to an essential component of personal financial strategy for many individuals; even doctors.
A side hustle is a way to earn extra income outside of your primary job or main source of employment. It typically involves part-time work, freelancing, small businesses, or gig-based activities that can be pursued flexibly in your free time. Unlike traditional employment, side hustles often offer more autonomy, creative freedom, and the potential to monetize skills, hobbies, or passions.
***
***
Doctor Gigs?
So, if you’re a doctor, dentist or podiatrist considering a side hustle, focus on something sustainable and long-term. Ask yourself: What am I already good at? What do people already ask me to help with? The best side hustles don’t require reinventing the wheel — just monetizing the one you’ve already been pushing uphill.
But, avoid gigs that require a huge upfront investment or promise overnight success. Instead, look for something that offers flexibility, ideally something that works with your schedule, not against your sanity.
Track your earnings and how much time you’re putting in. Side income should support your goals, whether that’s paying off debt, saving for a trip or just breathing easier when office rent comes due.
But, if it’s draining your energy from your medical practice with little to show for it, it might be time to rethink the hustle.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
An important component of hospital credit analysis is essentiality. Hospitals are unusual businesses that many times possess some form of essentiality to their communities. Health care is important to the economic vitality of every community. Many hospitals have served their communities for many years; it is not uncommon to find hospitals that have been continuously operating for more than 100 years in the same community.
Most hospitals are not-for-profit. In not-for-profit hospitals, no private party actually “owns” the hospital; control is vested in various boards, but no one explicitly owns a not-for-profit hospital. In a broad sense, communities own not-for-profit hospitals. They are considered “charities” with a “charitable purpose.” Though a not-for-profit hospital may not have owners, it has many “stakehold-ers,” parties that have vested interests in the continuing success of the hospital.
Many hospitals have broad and vast webs of stakeholders. Stakeholders are why hospitals rarely close or are shut down. Too many stakeholders have interests in the continuing successful operation of hospitals.
Another dimension of the essentiality analysis is service analysis. How significant are the hospital’s services? If the hospital shuts down, what population segments would suffer? How significant is the population that would suffer? How much would they suffer?
And so, hospital stakeholder relationships need to be considered in the analysis of essentiality. How strong are these relations? How many are there? How important is the continuing success of this hospital to these stakeholders?
Analysis of hospital’s stakeholders and services should provide a credible view of the degree of essentiality associated with a hospital. Higher degrees of essentiality suggest higher likelihoods that hospitals, one way or another, will meet their commitments, particularly their payment commitments.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
An obstetrician-gynecologist, or OB-GYN, has expertise in female reproductive health, pregnancy, and childbirth. Some OB-GYNs offer a wide range of general health services similar to a primary care doctor. Others focus on the medical care of the female reproductive system. OB-GYNs also provide routine medical services and preventive screenings. This type of doctor has studied obstetrics and gynecology. The term “OB-GYN” can refer to the doctor, an obstetrician-gynecologist, or to the sciences that the doctor specializes in, which are obstetrics and gynecology.
Obstetrician
Obstetrics is the branch of medicine related to medical and surgical care before, during, and after a woman gives birth. Obstetrics focuses on caring for and maintaining a woman’s overall health during maternity. This includes:
pregnancy
labor
childbirth
the postpartum period
OB-GYNs can conduct office visits, perform surgery, and assist with labor and delivery. Some OB-GYNs provide services through a solo or private practice. Others do so as part of a larger medical group or hospital.
***
***
Gynecologist
Gynecology is the branch of medicine that focuses on women’s bodies and their reproductive health. It includes the diagnosis, treatment, and care of women’s reproductive system. This includes the:
vagina
uterus
ovaries
fallopian tubes
This branch of medicine also includes screening for and treating issues associated with women’s breasts. Gynecology is the overarching field of women’s health from puberty through adulthood. It represents most of the reproductive care received during a lifetime. If pregnant, one goes to an obstetrician.
Mid-Wife
Midwives are registered nurses who specialize in midwifery. As such, they’re trained healthcare providers who can oversee low-risk pregnancies, labor, and birth. They can provide other obstetric and gynecological services too. They can do exams and help with basic gynecological concerns like sexually transmitted infections, urinary tract infections, or yeast infections. They help support during labor and in the postpartum period with breastfeeding and birth control.
Doula
Doulas aren’t clinical professionals and can’t give medical advice. They can’t prescribe medicines, and they can’t deliver a baby. But they can offer physical and emotional support during labor—and sometimes during and after pregnancy. Doulas can help with breathing techniques, positional changes, and relaxation strategies during labor. Studies show doulas are associated with fewer C-sections and more vaginal births.
Doctors and dentists earn money by treating patients. CPAs and Attorneys have clients, and retail stores buy items low and sell them at higher prices. This is called a business model.
More formally, a business model identifies the products or services the business plans to sell, the target market, and any anticipated expenses, in order to outline how to generate a profit. Business models are important for both new and established businesses. They help companies attract investment, recruit talent, and motivate management and staff.
Businesses should regularly update their business model, or they’ll fail to anticipate trends and challenges ahead. Business models also help investors to evaluate companies that interest them and employees to understand the future of a company they may aspire to join.
***
The Business Model of Pharmacy Benefits Managers
In the United States, health insurance providers often hire a third party to handle price negotiations, insurance claims, and distribution of prescription drugs. Providers that use such pharmacy benefit managers include commercial health plans, self-insured employer plans, Medicare Part D [drug] plans, the Federal Employees Health Benefits Program, and state government employee plans. PBMs are designed to aggregate the collective buying power of en-rollees through their client health plans, enabling plan sponsors and individuals to obtain lower prices for their prescription drugs. PBMs negotiate price discounts from retail pharmacies, rebates from pharmaceutical manufacturers, and mail-service pharmacies which home-deliver prescriptions without consulting face-to-face with a pharmacist.
Pharmacy benefit management companies can make revenue in several ways.
First, they collect administrative and service fees from the original insurance plan.
Then, they can also collect rebates from the manufacturer.
Traditional PBMs do not disclose the negotiated net price of the prescription drugs, allowing them to resell drugs at a public list price (also known as a sticker price), which is higher than the net price they negotiate with the manufacturer. This practice is known as “spread pricing”. The industry argues that savings are trade secrets. Pharmacies and insurance companies are often prohibited by PBMs from discussing costs and reimbursements. This leads to lack of transparency.
***
***
Therefore, states are often unaware of how much money they lose due to spread pricing, and the extent to which drug rebates are passed on to en-rollees of Medicare plans. In response, states like Ohio, West Virginia, and Louisiana have taken action to regulate PBMs within their Medicaid programs.
For instance, they have created new contracts that require all discounts and rebates to be reported to the states. In return, Medicaid pays PBMs a flat administrative fee.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
An ophthalmologist is a physician [MD, DO] who undergoes sub-specialty training in medical and surgical eye care. Following a medical degree, a doctor specializing in ophthalmology must pursue additional postgraduate residency training specific to that field. In the United States, following graduation from medical school, one must complete a four-year residency in ophthalmology to become an ophthalmologist. Following residency, additional specialty training (or fellowship) may be sought in a particular aspect of eye pathology.
Ophthalmologists prescribe medications to treat ailments, such as eye diseases, implement laser therapy, and perform surgery when needed. Ophthalmologists provide both primary and specialty eye care—medical and surgical. Most ophthalmologists participate in academic research on eye diseases at some point in their training and many include research as part of their career. Ophthalmology has always been at the forefront of medical research with a long history of advancement and innovation in eye care.
Optometrist
Optometrists focus on regular vision care and primary health care for the eye. After college, they spend 4 years in a professional program and get a doctor of optometry degree. But they don’t go to medical school. Some optometrists get additional clinical training or complete a specialty fellowship after optometry school. They:
Monitor eye conditions related to diseases like diabetes
Manage and treat conditions like dry eye and glaucoma
Provide low-vision aids and vision therapy
There are specialties among optometrists. They include:
Pediatric optometry. These providers work with babies, toddlers, and children, using special techniques to test their vision.
Neuro-optometry. If you have vision problems that result from a brain injury, this is the type of optometrist you might visit.
Low-vision optometry. If you have low vision—that means you can’t see well enough to perform your daily activities and your sight can’t be corrected by glasses or contact lenses, medicine, or surgery—low-vision optometrists offer devices and strategies that can improve your quality of life.
***
***
Optician
An optician is an eye care specialist who helps you choose the right eyeglasses, contact lenses or other vision correction devices. They can’t diagnose or treat conditions that affect your eyes or vision. They’ll work with you to get the right corrective lenses after your optometrist or ophthalmologist gives you a prescription.
Ocularist
An ocularist is an eye care specialist who provides care for people needing prosthetic eyes due to injury, infection or congenital disease (present at birth). Losing or damaging an eye can be a traumatic experience, and the need for a prosthetic can be overwhelming. Ocularists offer long-term care. They collaborate with your healthcare team to create or restore a more natural facial appearance with the goal of enhancing your health-related quality of life.
Trump says pharma tariffs could be as high as 250%
The president revealed that he plans to formally announce tariffs on the pharmaceutical industry “within the next week or so” in an attempt to force drug manufacturing to the US, he told CNBC several days ago.
In the early 1980s, Daniel Kahneman and Amos Tverskey proved in numerous experiments that the reality of decision making differed greatly from the assumptions held by economists. They published their findings in Prospect Theory: An analysis of decision making under risk, which quickly became one of the most cited papers in all of economics.
To understand the importance of their breakthrough, we first need to take a step back and explain a few things. Up until that point, economists were working under a normative model of decision making. A normative model is a prescriptive approach that concerns itself with how people should make optimal decisions. Basically, if everyone was rational, this is how they should act.
Amanda, an RN client, was just informed by her financial advisor that she needed to re-launch her 403-b retirement plan. Since she was leery about investing, she quietly wondered why she couldn’t DIY. Little does her Financial Advisor know that she doesn’t intend to follow his advice, anyway! So, what went wrong?
The answer may be that her advisor didn’t deploy a behavioral economics framework to support her decision-making. One such framework is the “prospect theory” model that boils client decision-making into a “three step heuristic.”
According to colleague Eugene Schmuckler PhD MBA MEd CTS, Prospect theory makes the unspoken biases that we all have more explicit. By identifying all the background assumptions and preferences that clients [patients] bring to the office, decision-making can be crafted so that everyone [family, doctor and patient] or [FA, client and spouse] is on the same page.
1. Simplify choices by focusing on the key differences between investment [treatment] options such as stock, bonds, cash, and index funds.
2. Understanding that clients [patients] prefer greater certainty when it comes to pursuing financial [health] gains and are willing to accept uncertainty when trying to avoid a loss [illness].
3. Cognitive processes lead clients and patients to overestimate the value of their choices thanks to survivor bias, cognitive dissonance, appeals to authority and hindsight biases.
CITE: Jaan E. Sidorov MD [Harrisburg, PA]
Assessment
Much like in healthcare today, the current mass-customized approaches to the financial services industry fall short of recognizing more personalized advisory approaches like prospect theory and assisted client-centered investment decision-making.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
THE ADDICTIVE INVESTING / TRADING PERSONALITY OF DOCTORS
Dr. Donald J. Mandell, a pediatrician, always needs to leave the office fifteen minutes ahead of schedule. The reason is because it takes that long to make the necessary number of trips to ensure the front door is truly locked.
Dr. Kamela A. Shaw, a general surgeon, is constantly rushing to the bath room so that she can wash her hands. As far as she is concerned, it is not possible to get one’s hands clean enough considering the COVID pandemic or recent influenza outbreak.
Although the behaviors displayed by these two doctors are different, they are consistent in that each, to some degree, display behavior that might be called an obsessive-compulsive disorder [OCD].
An obsession is a persistent, recurring preoccupation with an idea or thought. A compulsion is an impulse that is experienced as irresistible.
Obsessive-compulsive individuals feel compelled to think thoughts that they say they do not want to think or to carry out actions that they say are against their will. These individuals usually realize that their behavior is irrational, but it is beyond their control. In general, these individuals are preoccupied with orderliness, perfectionism, and mental and interpersonal control, at the expense of flexibility, openness, and efficiency. Specifically, behaviors such as the following may be seen:
Preoccupation with details.
Perfectionism that interferes with task completion.
Excessive devotion to work and office productivity.
Scrupulous and inflexible about morality (not accounted for by cultural or religious identification);
Inability to discard worn-out or worthless objects without sentimental value;
Reluctance to delegate tasks or to work with others.
Adopts a miserly spending style toward both self and others.
Demonstrates a rigid, inflexible and stubborn nature.
Most people resort to some minor obsessive-compulsive patterns under severe pressure or when trying to achieve goals that they consider critically important. In fact, many individuals refer to this as superstitious behavior. The study habits required for medical students entail a good deal of compulsive behavior.
As the above examples suggest, there are a variety of addictions possible. Recent news accounts have pointed out that even high-level governmental officials can experience sex addiction. The advent of social-media has led to what is referred to as Internet addiction where an individual is transfixed to a computer, tablet PC or smart-phone, “working” for hours on end without a specific project in mind. The simple act of “surfing”, “tweeting-X”, “texting” or merely posting opinions offers the person afflicted with the addiction some degree of satisfaction.
Still another form of addictive behavior is that of the individual with gambling disorder (GD).
GD is recognized as a mental disorder in the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders-V. This is the behavior of an individual who is unable to resist the impulse to gamble. Many reasons have been posited for this type of behavior including the death instinct; a need to lose; a history of trauma; a wish to repeat a big win; identification with adults the “gambler” knew as an adolescent; and a desire for action and excitement. There are other explanations offered for this form of compulsive behavior. The act of betting allows the individual to express an immature bravery, courage, manliness, and persistence against unfavorable odds. By actually using money and challenging reality, he puts himself into “action” and intense emotion. By means of gambling, the addicted individual is able to pretend that he is favored by “lady luck,” specially chosen, successful, able to beat the system and escape from feelings of discontent.
Greed can also have addictive qualities. In fact, a poll conducted by the Chicago Tribune revealed that folks who earned less than $30,000 a year, said that $50,000 would fulfill their dreams, whereas those with yearly incomes of over $100,000 said they would need $250,000 to be satisfied. More recent studies confirm that goals keep getting pushed upward as soon as a lower level is reached.
Edward Looney, executive director of the Trenton, New Jersey based Council on Compulsive Gambling (CCG) reports that the number of individuals calling with trading-associated problems is doubling annually. In the mid 1980s, when the council was formed, the number of people calling the council’s hotline (1 – 800 Gambler) with stock-market gambling problems was approximately 1.5 percent of all calls received. In 1998 that number grew to 3 percent, and rose to 8 percent by 2012. Today, that number is largely unknown because of its pervasiveness, but Dr. Robert Custer, an expert on compulsive gambling reported, that stock market gamblers represent over 20 percent of the gamblers that he has diagnosed. It is evident that on-line trading presents a tremendous risk to the speculator.
The CCG describes some of the consequences:
Dr. Fred B. is a 43-year-old Asian male physician with a salary above $150,000 and in debt for more than $150,000. He is married with two children. He was a day trader.
Michael Q. is a 28-year-old Hispanic male registered nurse. He is married and the father of one (7 month old) child. He earns $65,000 and lost $50,000 savings in day trading and is in debt for $30,000. He has suicidal ideation.
[B] A Question of Suitability
Since online traders are in it for many reasons, investment suitability rarely enters the picture, according to Stuart Kaswell, general counsel of the Securities Industry Association, in Washington, DC. The kind of question that has yet to be confronted, by day or online trading firms, is a statement, such as: “Equities look good this year. We favor technology stocks. We have a research report on our Web page that looks at the social media industry.” Those kinds of things are seldom considered because they do not involve a specific recommendation of a specific stock, like Apple, Google, Groupon, Facebook or Twitter.
However, if a firm makes a specific recommendation to an investor, whether over the cell-phone, iPad®, fax machine, face-to-face, instagram or over the Internet, or Twitter-X, suitability rules should apply. Opining similarly on the “know your customer” requirements is Steven Caruso, of Maddox, Koeller, Harget & Caruso of New York City. “The on-line firms obviously claim that they do not have a suitability responsibility because they do not want the liability for making a mistake as far as determining whether the investor was suitable or buying any security. I think that ultimately more firms are going to be required to make a suitability, [or eventually fiduciary] determination on every trade”.
[C] On-line Traders and Stock Market Gamblers
Some of the preferred areas of stock market gambling that attract the interest of compulsive gamblers include options, commodities, penny stocks and bit-coins, index investing, new stock offerings, certain types of CAT bonds, crowd-sourcing initiatives, and some contracts for government securities. These online traders and investment gamblers think of themselves as cautious long-term investors who prefer blue chip or dividend paying varieties. What they fail to take into consideration is that even seemingly blue chips can both rise and precipitously drop in value again, as seen in the summer of 2003, the “crash” of 2008, or the “flash crash” of May 6, 2010. On this day, the DJIA plunged 1000 points (about 9%) only to recover those losses within minutes. It was the second largest point swing 1,010.14 points, and the biggest one-day point decline, 998.5 points, on an intraday basis in Dow Jones Industrial Average history.
Regardless of investment choice, the compulsive investment gambler enjoys the anticipation of following the daily activity surrounding these investments. Newspaper, hourly radio and television reports, streaming computer, tablet and smart phone banners and hundreds of periodicals and magazines add excitement in seeking the investment edge. The name of the game is action. Investment goals are unclear, with many participating simply for the feeling it affords them as they experience the highs and lows and struggles surrounding the play. And, as documented by the North American Securities Administrators Association’s president, and Indiana Securities Commissioner, Bradley Skolnik, most day or online traders lose money. “On-line brokerage was new and cutting edge and we enjoyed the best stock market in generations, until the crashes. The message of most advertisements was “just do it”, and you’ll do well. The fact is that research and common sense suggest the more you trade, the less well you’ll do”.
Most day or online traders are young males, some who quit their day jobs before the just mentioned debacles; or more recently with the dismal economy. Many ceased these risky activities but there is some anecdotal evidence that is re-surging again with 2013-14 technology boom and market rise. Most of them start every day not owning any stock, then buy and sell all day long and end the trading day again without any stock – – just a lot of cash. Dr. Patricia Farrell, a licensed clinical psychologist states that day traders are especially susceptible to compulsive behaviors and addictive personalities. Mark Brando, registered principal for Milestone Financial, a day trading firm in Glendale, California states, “People that get addicted to trading employ the same destructive habits as a gambler. Often, it’s impossible to tell if a particular trade comes from a problem gambler or a legitimate trader.”
Arthur Levitt, former Chairman of the Securities and Exchange Commission (SEC) in discussing the risks and misconceptions of investing are only amplified by on-line trading. In a speech before the National Press Club a few years ago, he attempted to impress individuals as to the risks and difficulties involved with day trading. Levitt cited four common misconceptions that knowledgeable medical professionals, and all investors, should know:
Personal computers, tablets, mobile devices and smart-phones are not directly linked to the markets – Thanks to Level II computer software, day traders can have access to the same up-to-the-second information available to market makers on Wall Street. “Although the Internet makes it seem as if you have a direct connection to the securities market, you don’t. Lines may clog; systems may break; orders may back-up.”
The virtue of limit orders – “Price quotes are only for a limited number of shares; so only the first few investors will receive the currently quoted price. By the time you get to the front of the line, the price of the stock could be very different.”
Canceling an order – “Another misconception is that an order is canceled when you hit ‘cancel’ on your computer. But, the fact is it’s canceled only when the market gets the cancellation. You may receive an electronic confirmation, but that only mean your request to cancel was received – not that your order was actually canceled”.
Buying on margin – “if you plan to borrow money to buy a stock, you also need to know the terms of the loan your broker gave you. This is margin. In volatile markets, investors who put up an initial margin payment for a stock may find themselves required to provide additional cash if the price of the stock falls.
How then, can the medical professional or financial advisor tell if he or she is a compulsive gambler? A diagnostic may be obtained from Gamblers Anonymous. It is designed to screen for the identification of problem and compulsive gambling.
But, it is also necessary to provide a tool to be used by on-line traders. This questionnaire is as follows:
1. Are you trading in the stock market with money you may need during the next year?
2. Are you risking more money than you intended to?
3. Have you ever lied to someone regarding your on-line trading?
4. Are you risking retirement savings to try to get back your losses?
5. Has anyone ever told you that spend too much time on-line?
6. Is investing affecting other life areas (relationships, vocational pursuits, etc.)?
7. If you lost money trading in the market would it materially change your life?
8. Are you investing frequently for the excitement, and the way it makes you feel?
9. Have you become secretive about your on-line trading?
10. Do you feel sad or depressed when you are not trading in the market?
NOTE: If you answer to any of these questions you may be moving from investing to gambling.
***
***
The cost of compulsive gambling and day trading is high for the individual medical or lay professional, the family and society at large. Compulsive gamblers, in the desperation phase of their gambling, exhibit high suicide ideation, as in the case of Mark O Barton’s the murderous day-trader in Atlanta who killed 12 people and injured 13 more in July 29th 1999. His idea actually became a final act of desperation.
Less dramatically, for doctors, is a marked increase in subtle illegal activity. These acts include fraud, embezzlement, CPT® up-coding, medical over utilization, excessive full risk HMO contracting, Stark Law aberrations and other “white collar crimes.” Higher healthcare and social costs in police, judiciary (civil and criminal) and corrections result because of compulsive gambling. The impact on family members is devastating. Compulsive gamblers cause havoc and pain to all family members. The spouses and other family members also go through progressive deterioration in their lives.
In this desperation phase, dysfunctional families are left with a legacy of anger, resentment, isolation, and in many instances, outright hate.
[D] Day Trading Assessment
Internet day trading, like the Internet and telecommunications sectors, become something of a investment bubble a few years ago, suggesting that something lighter than air can pop and disappear in an instant. History is filled with examples: from the tulip mania of 1630 Holland and the British South Sea Bubble of the 1700’s; to the Florida land boom of the roaring twenties and the Great Crash of 1929; to the collapse of Japans stock and real estate market in early 1990’s; and to an all-time high of $1,926 for an ounce of commodity gold a few years ago.
Today it is Ask: $3,388.30 USD Bid: $3,367.30 USD
CONCLUSION
To this list, one might again include smart-phone or mobile day trading.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Posted on August 6, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A.I and Staff Reporters
***
***
Illinois just became the first US state to regulate AI mental health services this week when Gov. JB Pritzker signed a law banning AI therapy.
The law forbids chatbots from acting as therapists and limits how human mental health professionals can use AI to aid their work. Companies face up to $10,000 in fines if they violate the law, according to Morning Brew.
The move comes as ChatGPT users—particularly younger ones—increasingly turn to the app for what amounts to free therapy. OpenAI recently made updates to its model to encourage users to use ChatGPT in a healthier way.
An acute care inpatient hospital is a health care organization or “anchor hospital” in which a patient is treated for an acute (immediate and severe) episode of illness or the subsequent treatment of injuries related to an accident or trauma, or during recovery from surgery. Specialized personnel using complex and sophisticated technical equipment and materials usually render acute professional care in a hospital setting. Unlike chronic care, acute care is often necessary for only a short time. Measures of acute health care utilization are represented by three separate rates:
Rate of admissions per 1000 patients.
Average length of stay per admission.
Total days of care per 1000 patients.
***
***
Psychiatric Hospital
A psychiatric hospital (behavioral health, mental hospital, or asylum) specializes in the treatment of patients with mental illness or drug-related illness or dependencies. Psychiatric wards differ only in that they are a unit of a larger hospital.
Specialty Hospital
A specialty hospital is a type of health care organization that has a limited focus to provide treatment for only certain illnesses such as cardiac care, orthopedic or plastic surgery, elder care, radiology / oncology services, neurological care, or pain management cases. These organizations are often owned by doctors who refer patients to them. In recent years, single-specialty hospitals have emerged in various locations in the United States. Instead of offering a full range of inpatient services, these hospitals focus on providing services relating to a single medical specialty or cluster of specialties.
Long-Term Care Hospital
A long-term care hospital is an entity that provides assistance and patient care for the activities of daily living (ADLs), including reminders and standby help for those with physical, mental, or emotional problems. This includes physical disability or other medical problems for 3 months or more (90 days). The criteria of five ADLs may also be used to determine the need for help with the following: meal preparation, shopping, light housework, money management, and telephoning. Other important considerations include taking medications, doing laundry, and getting around outside.
Rural Hospital
The parameters of a rural hospital are determined based on distance. A rural hospital is defined as a hospital serving a geographic area 10 or more miles from the nexus of a population center of 30,000 or more.
More specifically, a rural hospital means an entity characterized by one of the following:
Type A rural hospital—small and remote, has fewer than 50 beds, and is more than 30 miles from the nearest hospital
Type B rural hospital—small and rural, has fewer than 50 beds, and is 30 miles or less from the nearest hospital
Type C rural hospital—considered rural and has 50 or more beds
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
In order to create and monitor an investment portfolio for personal or institutional use, the physician executive, financial advisor, wealth manager, or healthcare institutional endowment fund manager, should ask three questions:
How much do we have invested?
How much did we make on our investments?
How much risk did we take to get that rate of return?
Introduction to the IPS
Most doctors, and hospital endowment fund executives, know how much money they have invested. If they don’t, they can add a few statements together to obtain a total. But, few can answers the questions above or actually know the rate of return achieved last year; or so far this year. Everyone can get this number by simply subtracting the ending balance from the beginning balance and dividing the difference. But, few take the time to do it. Why? A typical response to the question is, “We’re doing fine.”
Now, ask how much risk is in the portfolio and help is needed [risk adjusted rate of return]. In fact, Nobel laureate Harry Markowitz, Ph.D. said, “If you take more risk, you deserve more return.” Using standard deviation, he referred to the “variability of returns;” in other words, how much the portfolio goes up and down, its volatility [Markowitz, H: Portfolio Selection. Journal of Finance, March, 1952].
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com