BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on October 28, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA MEd
***
***
In the evolving landscape of digital health care, Amazon Pharmacy and GoodRx have emerged as two leading platforms offering consumers affordable and convenient access to prescription medications. While both aim to simplify the process of obtaining prescriptions, they differ significantly in their approach, pricing models, and user experience.
Amazon Pharmacy, launched in 2020, is a full-service online pharmacy that allows customers to order medications directly through Amazon. It offers fast, free delivery for Prime members and integrates with most insurance plans. One of its standout features is RxPass, a subscription service available to Prime members for $5 per month, which covers unlimited eligible generic medications. This model is particularly attractive to individuals who take multiple generics regularly, as it can significantly reduce out-of-pocket costs.
In contrast, GoodRx, founded in 2011, operates primarily as a price comparison and discount platform. It does not dispense medications itself but partners with local and mail-order pharmacies to help users find the lowest prices. GoodRx provides coupons that can be used at thousands of pharmacies nationwide, often resulting in substantial savings—especially for those without insurance. It also offers GoodRx Gold, a paid membership that unlocks deeper discounts and telehealth services.
***
***
When comparing the two, pricing transparency is a key differentiator. GoodRx excels in showing users a range of prices across different pharmacies, empowering them to choose the most cost-effective option. Amazon Pharmacy, while competitive, typically offers fixed prices and focuses more on convenience and integration with its broader ecosystem.
Convenience is another area where Amazon Pharmacy shines. With its streamlined ordering process, automatic refills, and integration with Amazon’s delivery network, it appeals to users who prioritize ease and speed. GoodRx, while convenient in its own right, requires users to present coupons at the pharmacy or use mail-order services, which may involve more steps.
Insurance compatibility also varies. Amazon Pharmacy accepts most major insurance plans, making it a viable option for insured individuals. GoodRx, on the other hand, is often used by those without insurance or with high deductibles, as its discounts can sometimes beat insurance copays.
However, both platforms have limitations. Amazon Pharmacy’s RxPass is restricted to generic medications and excludes certain states due to regulatory issues. GoodRx’s discounts may not apply to all medications, and prices can fluctuate depending on location and pharmacy.
In terms of user experience, Amazon offers a seamless, tech-driven interface with customer support and medication management tools. GoodRx provides educational resources, price alerts, and a mobile app that helps users track savings and prescriptions.
Ultimately, the choice between Amazon Pharmacy and GoodRx depends on individual needs. For those seeking a one-stop solution with predictable costs and fast delivery, Amazon Pharmacy may be ideal. For users who want to shop around for the best deal or lack insurance, GoodRx offers unmatched flexibility and savings.
As digital health continues to grow, both platforms are reshaping how Americans access medications—making prescriptions more affordable, transparent, and accessible than ever before.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com
Posted on October 8, 2025 by Dr. David Edward Marcinko MBA MEd CMP™
By A. I.
***
***
Value-Based Medical Care: A Paradigm Shift in Healthcare
In recent years, the healthcare industry has undergone a transformative shift from volume-driven services to outcome-focused care. This evolution is embodied in the concept of value-based medical care, a model that emphasizes delivering high-quality healthcare while controlling costs and improving patient outcomes. Unlike traditional fee-for-service systems, which reward providers for the quantity of services rendered, value-based care aligns incentives with the value of care provided—measured by patient health outcomes relative to the cost of achieving them.
Core Principles of Value-Based Care
At its heart, value-based medical care is built on several foundational principles:
Patient-Centeredness: Care is tailored to individual needs, preferences, and values, promoting shared decision-making and holistic treatment.
Quality Over Quantity: Providers are rewarded for improving health outcomes, reducing hospital readmissions, and preventing disease rather than performing more procedures.
Integrated Care Delivery: Coordination among healthcare professionals ensures seamless transitions between services, reducing fragmentation and duplication.
Data-Driven Accountability: Performance metrics and health analytics guide clinical decisions and track progress toward better outcomes.
Cost Efficiency: By focusing on prevention and effective management of chronic conditions, value-based care aims to reduce unnecessary spending.
Benefits for Patients and Providers
For patients, value-based care offers a more personalized and proactive approach to health. It encourages preventive screenings, chronic disease management, and wellness programs that lead to longer, healthier lives. Providers benefit from shared savings programs, performance bonuses, and stronger relationships with their patients. Moreover, healthcare systems can allocate resources more effectively, reducing waste and improving overall population health.
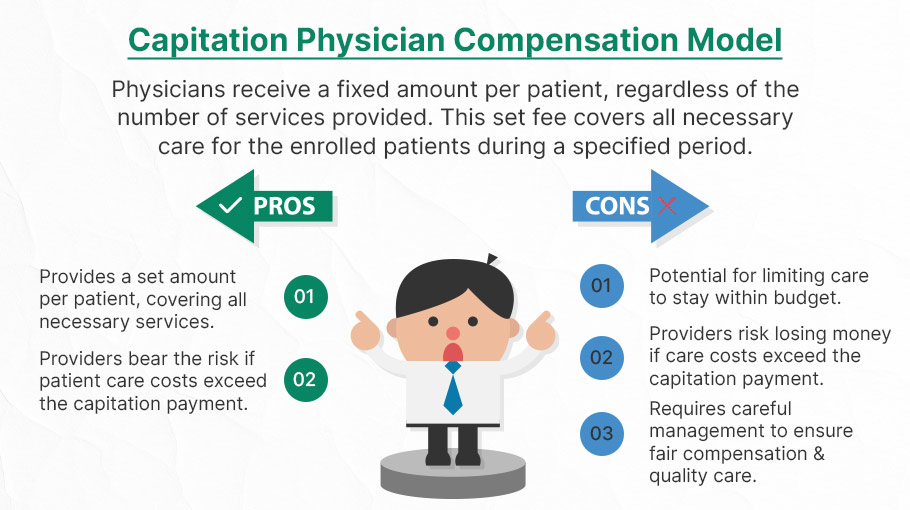
Capitation is a type of healthcare payment system in which a physician or hospital is paid a fixed amount of money per patient for a prescribed period by an insurer or physician association. The cost is based on the expected healthcare utilization costs for a group of patients for that year.
With capitation, the physician—otherwise known as the primary care physician— is paid a set amount for each enrolled patient whether a patient seeks care or not. The PCP is usually contracted with an HMO whose role it is to recruit patients.
According to Richard Eskow, CEO of Health Knowledge Systems of Los Angeles, capitated medical reimbursement has been used in one form or another, in every attempt at healthcare reform since the Norman Conquest. Some even say an earlier variant existed in ancient China [personal communication].
Initially, when Henry I assumed the throne of the newly combined kingdoms of England and Normandy, he initiated a sweeping set of healthcare reforms. Historical documents, though muddled, indicate that soon thereafter at least one “physician,” John of Essex, received a flat payment honorarium of one penny per day for his efforts. Historian Edward J. Kealey opined that sum was roughly equal to that paid to a foot-soldier or a blind person. Clearer historical evidence suggests that American doctors in the mid-19th century were receiving capitation-like payments. No less an authoritative figure than Mark Twain, in fact, is on record as saying that during his boyhood in Hannibal, MO his parents paid the local doctor $25/year for taking care of the entire family regardless of their state of health.
Later, Sidney Garfield MD [1905-1984] is noted as one of the great under-appreciated geniuses of 20th century American medicine stood in the shadow cast by his more celebrated partner, Henry J. Kaiser. Garfield was not the first physician to embrace the notion of prepayment capitation, nor was he the first to understand that physicians working together in multi-specialty groups could, through collaboration and continuity of care, outperform their solo practice colleagues in almost every measure of quality and efficiency. The Mayo brothers, of course, had prior claim to that distinction. What Garfield did, was marry prepayment to group practice, providing aligned financial incentives across every physician and specialty in his medical group, as well as a culture of group accountability for the care of every member of the affiliated health plan. He called it “the new economics of medicine,” and at its heart was a fundamentally new paradigm of care that emphasized – prevention before treatment – and health before sickness. Under his model: the fewer the sick – the greater the remuneration. And: the less serious the illness, the better off the patient and the doctors.
Such ideas were heresy to the reigning fee-for-service, solo practice, ideologues of the mainstream medical establishment of the 1940s and ‘50s, of course. Throughout the period, Garfield and his group physicians were routinely castigated by leaders of the AMA and county medical associations as socialistic and unethical. The local medical associations in Garfield’s expanding service areas – the San Francisco Bay Area, Los Angeles, and Portland, Oregon – blocked group practice physicians from association membership, effectively shutting them out of local hospitals, denying them patient referrals or specialty society accreditation. Twice in the 1940s, formal medical association charges were brought against Garfield personally, at one time temporarily succeeding in suspending his license to practice medicine.
Of course, capitation payments made a comeback in the first cost-cutting managed care era of the 1980-90s because fee-for-service medicine created perverse incentives for physicians by paying more for treating illnesses and injuries than it does for preventing them — or even for diagnosing them early and reducing the need for intensive treatment later. Nevertheless, the modern managed care industry’s experience with capitation wasn’t initially a good one. The 1980-90s saw a number of HMOs attempt to put independent physicians, especially primary care doctors, into a capitation reimbursement model. The result was often negative for patients, who found that their doctors were far less willing to see them — and saw them for briefer visits — when they were receiving no additional income for their effort. Attempts were also made to aggregate various types of health providers — including hospitals and physicians in multiple specialties — into “capitation groups” that were collectively responsible for delivering care to a defined patient group. These included healthcare facilities and medical providers of all types: physicians, osteopaths, podiatrists, dentists, optometrists, pharmacies, physical therapists, hospitals and skilled nursing homes, etc.
However, the healthcare industry isn’t collective by nature, and these efforts tended to be too complicated to succeed. One lesson that these experiments taught is that provider behavior is difficult to change unless the relationship between that behavior and its consequences is fairly direct and easy to understand.
Today, the concept of prepayment and medical capitation is to uncouple compensation from the actual number of patients seen, or treatments and interventions performed. This is akin to a fixed price restaurant menu, as opposed to an àla carte eatery.
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR-http://www.MarcinkoAssociates.com
Much has been written and much has been opined on the topic of health information technology, electronic health records and medical security liability for physicians and healthcare providers in this textbook. But occasionally, we all still get lost in a wide array of acronyms, jargon and terms that are constantly changing in this ecosystem. And so, this brief glossary serves as a ready reference for those who want to know about these definitions in a quick and ready fashion.
Access control: The process of controlling the access of a user
Access security: To allow computer or healthcare network entry using ID / password / secure socket layer (SSL) encryption / biometrics, etc; unique identification and password assignments are usually made to medical staff members for access to medical information on a need-to-know basis, and only upon written authority of the owner of the data.
Access level authorization: Establishes a procedure to determine the computer or network access level granted to individuals working on or near protected health information, medical data or secure health data.
Accredited standards committee: Organization that helps develop American National Standards (ANS) for computer and health information technology; accredited by ANSI for the development of American National Standards; ASC X12N develops medical electronic business exchange controls like 835-Health Care Claim Payment/Advice and 837-Health Care Claim.
Accountability: The security goal that generates the requirement for actions of an entity to be traced uniquely to that entity. This supports nonrepudiation, deterrence, fault isolation, intrusion detection and prevention, and after-action recovery and legal action.
Accounting: Creating an historical record of who was authenticated, at what time, and how long they accessed the computer system.
Administrative simplification: The use of electronic standard code sets for health information exchange; Title II, Subtitle F of HIPAA gives HHS the authority to mandate the use of standards for the electronic exchange of health care data; to specify what medical and administrative code sets should be used within those standards; to require the use of national identification systems for health care patients, providers, payers (or plans), and employers (or sponsors); and to specify the types of measures required to protect the security and privacy of personally identifiable health care and medical information.
Alternative backup sites: Off-site locations that are used for transferring computer operations in the event of an emergency.
American Health Information Management Association: A large trade association of health information and medical data management professionals.
American Medical Informatics Association: An organization that promotes the use of electronic medical management and healthcare informatics for clinical and administrative endeavors.
American Telemedicine Association: Established in 1993 as a leading resource and advocate promoting access to medical care for patients and health professionals via telecommunications technology; membership open to individuals, companies, and other organizations with an interest in promoting the deployment of telemedicine throughout the world.
Anti-virus software: A software package or subscription service used to thwart malicious computer or network attacks, such as: Symantec®, McAfee®, Trend Micro®, Panda Software®, Sunbelt Software®, Computer Associates®, AVG® or MS-FF ®, etc.
ASC X12N: HIPAA transmission standards, specifications and implementation guides from the Washington Publishing Company; or the National Council of Prescription Drug Programs.
Assurance: Grounds for confidence that the other four security goals (integrity, availability, confidentiality, and accountability) have been adequately met by a specific implementation. “Adequately met” includes (1) functionality that performs correctly, (2) sufficient protection against unintentional errors (by users or software), and (3) sufficient resistance to intentional penetration or bypass.
Asymmetric cryptology: The use of two different but mathematically related electronic keys for secure health data and medical information storage, transmission and manipulation.
Asymmetric encryption: Encryption and decryption performed using two different keys, one of which is referred to as the public key and one of which is referred to as the private key; also known as public-key encryption.
Asymmetric key: A half of a key pair used in an asymmetric “public-key” encryption system with two important properties: (1) the key used for encryption is different from the one used for decryption, (2) neither key can feasibly be derived from the other.
Attack tree: An inverted tree diagram that provides a visual image of the attacks that may occur against an asset.
Audio teleconferencing: A multi-simultaneous dual voice communications between two parties at remote locations; two way communications between physician and patient at various locations.
Authentication: The process of verifying and confirming the identity of a user.
Availability: The security goal that generates the requirement for protection against – Intentional or accidental attempts to (1) perform unauthorized deletion of data or (2) otherwise cause a denial of service or data.
Back door: A means to access to a computer program that bypasses security mechanisms, sometimes installed by a programmer so that the program can be accessed for troubleshooting or other purposes.
Back door trojans or bots: Currently, the biggest threat to healthcare and all PC users worldwide according to the MSFT Corporation.®
Bandwidth: The amount of information that can be carried over a communications link.
Bar coding systems: Final FDA ruling issued in February 2004 that required bar codes on most prescription and non-prescription medications used in hospitals and dispensed based on a physician’s order; the bar code must contain at least the National Drug Code (NDC) number, which specifically identifies the drug; although hospitals are not required at this time to have a bar code reading system on the wards, this ruling has heightened the priority of implementing hospital-wide systems for patient-drug matching using bar codes.
Baud: A unit of digital transmission that indicates the speed of information flow. The rate indicates the number of events able to be processed in one second and is expressed as bits per second (bps). The baud rate is the standard unit of measure for data transmission capability; typical older rates were 1200, 2400, 9600, and 14,400 baud; the signaling rate of a telephone line in the number of transitions made in a second; 1/300 sec = 300 baud.
Beta test: The secondary or final stress examination of newly developed computer hardware, software or peripheral devices; site, etc.
Bibliographic database: Indexed computer or printed source of citations of journal articles and other reports in the literature; typically include author, title, source, abstract, and/or related information; MEDLINE® and EMBASE®.
Bioinformatics: The application of medical and biological science to the health information management field.
Biological Information technology: Cross industry alliance of the Microsoft Corporation to enhance the ability to use and share digital health and biomedical data.
Biometric: Personal security identity characteristics, such as a signature, fingerprints, voice, iris or retinal scan, hand or foot vein geometry, facial characteristics, hair analysis, eye, blood vessel or DNA; uses the unique human characteristics of a person as a means of authenticating.
Biometric identification: Secure identification using biometrics that identifies a human from a measurement of a physical feature or repeatable action of the individual (for example, hand geometry, retinal scan, iris scan, fingerprint patterns, facial characteristics, DNA sequence characteristics, voice prints, and hand written signature).
Biopassword: Start-up healthcare IT security pioneer of keyboarding patterns to boost online security through neural network patterns.
Bluetooth® device: Machines, like cell phone with headset, transmitting across communications channels 1 to 14, over time.
Bluetooth® technology: Wireless mobile technology standard built into millions of mobile phones, headsets, portable computers, desktops and notebooks; named after Harold Bluetooth, a 10th century Viking king; healthcare telemetry and rural data transmissions; the Bluetooth Special Interest Group (BSIG) advocates measures aimed at pushing healthcare interoperability for wireless devices and other computers designed for use in the medical field; other wireless stands include: Wi-Fi, ZigBe®, IrDA and RFID.
Buffer: A temporary storage area.
Buffer overflow: A security breach that occurs when a computer program attempts to stuff more data into a temporary storage area than it can hold
Business continuity plan: A plan that outlines the procedures to follow after a business experiences an attack on its security.
California Database Security Breach Act: A state act that requires disclosure to California residents if a breach of personal information has or is believed to have occurred.
Certification authority: An independent third-party organization that assigns digital certificates.
Chain of custody: A process that documents everyone who has had contact with or direct possession of the evidence.
Chain of trust: Suggestion that each and every covered entity and business associate share responsibility and accountability for confidential PHI.
Chain of trust agreement: Contract entered into by two business partners in which it is agreed to exchange data and that the first party will transmit information to the second party, where the data transmitted is agreed to be protected between the partners; sender and receiver depend upon each other to maintain the integrity and confidentiality of the transmitted information; multiple two-party contracts may be involved in moving information from the originator to the ultimate recipient; for example, a provider may contract with a clearing house to transmit claims to the clearing house; the clearing house, in turn, may contract with another clearing house or with a payer for the further transmittal of those same claims.
Children’s Online Privacy Protection Act: A federal act that requires operators of online services or Web sites directed at children under the age of 13 to obtain parental consent prior to the collection, use, disclosure, or display of a child’s personal information.
Cipher lock: A combination lock that uses buttons that must be pushed in the proper sequence in order to open the door.
Clearing house: HIPAA medical invoice, healthcare data transaction exchange and medical data implementation service center that that meets or exceeds Federally-mandated standardized Electronic Data Interchange (EDI) transaction requirements.
Clinger-Cohen Act: Public Law 104-106; Information Technology Management Reform Act (ITMRA) of 1996.
Clinical data: Protected Health Information (PHI) from patient, physician, laboratory, clinic, hospital and/or payer, etc; identifiable patient medical information.
Clinical data information systems: Automatic and securely connected system of integrated computers, central severs and the Internet that transmits Protected Health Information (PHI) from patient, physician, laboratory, clinic, hospital and/or payer, etc.
Clinical data repository: Electronic storehouse of encrypted patient medical information; clinical data storage.
Clinical informatics: The management of medical and clinical data; the use of computers, networks and IT for patient care and health administration.
Clinical information: All the related medical information about a patient; Protected Health Information (PHI) from patients, providers, laboratories, clinics, hospitals and/or payers or other stakeholders, etc.
Clinical information system: A computer network systems that supports patient care; relating exclusively to the information regarding the care of a patient, rather than administrative data, this hospital-based information system is designed to collect and organize data.
Clinical regional health information system: Electronic entity committed to securely share private patient health information among entities like medical providers, clinics, laboratories, hospitals, outpatient centers, hospice and other healthcare facilities; Community Health Management Information Systems (CHMIS), Enterprise Information Networks (EINs), Regional Health Information Networks (RHINs) and Health Information Networks (HINs).
Cold site: An alternative backup site that provides the basic computing infrastructure, such as wiring and ventilation, but very little equipment.
Compact disc – read only memory (CD-ROM): A computer drive that can read CD-R and CD-RW discs.
Compact disc – recordable (CD-R): An optical disc that contains up to 650 megabytes of data and cannot be changed once recorded.
Compact disc – rewriteable (CD-RW): An optical disc that can be used to record data, erase it, and re-record again.
Computer security: A computer or network that is free from threats against it.
Computerized Physician Order Entry System: Automatic medical provider electronic medical chart ordering system that usually includes seven features: medication analysis, system order clarity, increased work efficiency, point of care utilization, benchmarking and performance tracking, on-line alerts and regulatory reporting.
Confidential health information: Protected Health Information (PHI) that is prohibited from free-use and secured from unauthorized dissemination or use; patient specific medical data.
Counter signature: The ability to prove the order of application of signatures; analogous to the normal business practice of signing a document which has already been signed by another party (ASTM E 1762 -95); part of a digital signature.
Covered entity: 42 CFR § 164.504(e)(2)(i)(B). Any of three broadly defined entities that deal with protected health information (PHI): providers, individuals or group health plans, and clearinghouses.
Cracker: A person who breaks into or otherwise violates the system security with a malicious intent.
Cryptography: The science of transforming information so that it is secure while it is being transmitted or stored.
Cyber-terrorism: Attacks by a terrorist group using computer technology and the Internet to cripple or disable a nation’s electronic infrastructure.
Data backup: The process of copying data to another media and storing it in a secure location.
Data encryption standard: An older health or medical data private key cryptology federal protocol for secure information exchange; replaced by AES.
Data interchange standard: X12 HIPAA health data transmission standard format.
Data interchange standard association: The organization that provides X12 HIPAA transmission standards and formats.
Deadbolt lock: A lock that extends a solid metal bar into the door frame for extra security.
Decision support system: Computer tools or applications to assist physicians in clinical decisions by providing evidence-based knowledge in the context of patient-specific data; examples include drug interaction alerts at the time medication is prescribed and reminders for specific guideline-based interventions during the care of patients with chronic disease; information should be presented in a patient-centric view of individual care and also in a population or aggregate view to support population management and quality improvement.
Decryption: Changing an encrypted message back to its original form.
Definition files: Files that contain updated antivirus information.
De-identified health information: Protected health information that is no longer individually identifiable health information; a covered entity may determine that health information is not individually identifiable health information only if: (1) a person with appropriate knowledge of and experience with generally accepted statistical and scientific principles and methods for rendering information not individually identifiable determines that the risk is very small that the information could be used, alone or in combination with other available information, to identify an individual, and documents the methods and results of the analysis; or (2) the following identifiers of the individual, relatives, employers or household members of the individual are removed.
Denial of service: The prevention of authorized access to resources or the delaying of time critical operations.
Designated record set: Contains medical and billing records and any other records that a physician and/or medical practice utilizes for making decisions about a patient; a hospital, emerging healthcare organization, or other healthcare organization is to define which set of information comprises “protected health information” and which set does not; contains medical or mixed billing records, and any other information that a physician and/or medical practice utilizes for making decisions about a patient. It is up to the hospital, EHO, or healthcare organization to define which set of information comprises “protected health information” and which does not though logically this should not differ from locale to locale. The patient has the right to know who in the lengthy data chain has seen their PHI. This sets up an audit challenge for the medical organization, especially if the accountability is programmed, and other examiners view the document without cause.
Designated standard: HIPAA standard as assigned by the department of HHS
Device lock: A steel cable and a lock used to secure a notebook computer.
Digital certificate: A certificate that binds a specific person to a public key.
Digital imaging and communications in medicine: Technology broadband transmission imaging standards for X-rays, MRIs, CT and PET scans, etc; health IT standard transmissions platform aimed at enabling different computing platforms to share image data without compatibility problems; a set of protocols describing how radiology images are identified and formatted that is vendor-independent and developed by the American College of Radiology and the National Electronic Manufacturers Association.
Digital radiology: Medical digital imaging applied to x-rays, CT, PET scans and related non-invasive and invasive technology; broadband intensive imaging telemedicine.
Digital rights management: The control and protection of digital intellectual property.
Digital signature: Encrypted electronic authorization with verification and security protection; private and public key infrastructure; based upon cryptographic methods of originator authentication, computed by using a set of rules and a set of parameters so that the identity of the signer and the integrity of medical or other data can be verified.
Digital signature standard: Encryption technology to ensure electronic medical data transmission integrity and authentication of both sender and receiver; date and time stamps; public and private key infrastructure.
Digital versatile disc – recordable (DVD-R): An optical disc technology that can record once up to 3.95 gigabytes of data on a single-sided disc and 7.9 GB on a double-sided disc.
Digital versatile disc – rewriteable (DVD-RAM): An optical disc technology that can record, erase, and re-record data and has a capacity of 2.6 GB (single side) or 5.2 GB (double side).
Digital versatile disc (DVD): A technology that permits large amounts of data to be stored on an optical disc.
Disaster recovery plan: A process to restore vital health and/or critical healthcare technology systems in the event of a medical practice, clinic, hospital or healthcare business interruption from human, technical or natural causes; focuses mainly on technology systems, encompassing critical hardware, operating and application software, and any tertiary elements required to support the operating environment; must support the process requirements to restore vital company data inside the defined business requirements; does not take into consideration the overall operating environment; an emergency mode operation plan is still necessary.
Disclosure: Release of PHI outside a covered entity or business agreement space, under HIPAA; the release, transfer, provision of access to or divulging of medical information outside the entity holding the information.
Disc – rewriteable (DVD-RW): An optical disc technology that allows data to be recorded, erased, and re-recorded.
Due care: Managers and their organizations have a duty to provide for information security to ensure that the type of control, the cost of control, and the deployment of control are appropriate for the system being managed.
e-health: Emerging field in the intersection of medical informatics, public health and business, referring to health services and information delivered or enhanced through the Internet and related technologies; characterizes not only a technical development, but also a state-of-mind, attitude, and a commitment for networked, global thinking, to improve health care worldwide by using information and communication technology.
Electronic data interchange: Inter healthcare organization computer-to-computer transmission of business or health information in a standard format; direct transmission from the originating application program to the receiving, or processing, application program; an EDI transmission consists only of business or health data, not any accompanying verbiage or free-form messages; a standard format is one that is approved by a national or international standards organization, as opposed to formats developed by health industry groups, medical practices, clinics or companies; the electronic transmission of secure medical and financial data in the healthcare industrial complex; X12 and similar variable-length formats for the electronic exchange of structured health data. The Centers for Medicare and Medicaid Services (CMS) regulates security and Electronic Data Interchange (EDI).
Electronic data interchange standards: The American National Standards Institute (ANSI) set of EDI standards known as the X12 standards. These standards have been developed by private sector standards development organizations (SDOs) and are maintained by the Accredited Standards Committee (ASC) X12. ANSI ASC X12N standards, Version 4010, were chosen for all of the transactions except retail pharmacy transactions, which continue to use the standard maintained by the National Council for Prescription Drug Programs (NCPDP) because it is already in widespread use. The NCPDP Telecommunications Standard Format Version 5.1 and equivalent NCPDP Batch Standard Version 1.0 have been adopted in this rule (health plans will be required to support one of these two NCPDP formats). The standards are designed to work across industry and company boundaries. Changes and updates to the standards are made by consensus, reflecting the needs of the entire base of standards users, rather than those of a single organization or business sector. Specifically, the following nine healthcare transactions were required to use X12N standard electronic claim formats by October 16, 2003.
Electronic health record: A real-time patient health record with access to evidence-based decision support tools that can be used to aid clinicians in decision-making; the EHR can automate and streamline a clinician’s workflow, ensuring that all clinical information is communicated; prevents delays in response that result in gaps in care; can also support the collection of data for uses other than clinical care, such as billing, quality management, outcome reporting, and public health disease surveillance and reporting; electronic medical record.
Electronic medication administrative record: Electrical file keeping computerized system for tracking clinical medication dispensation and use; integrated with TPAs, PBMs, robotic dispensing devices and CPOEs, etc.
Electronic medical (media) claims: Usually refers to a flat file format used to transmit or transport medical claims, such as the 192-byte UB-92 Institutional EMC format and the 320-byte Professional EMC-NSF.
Electronic prescribing: A type of computer technology whereby physicians use handheld or personal computer devices to review drug and formulary coverage and to transmit prescriptions to a printer or to a local pharmacy; e-prescribing software can be integrated into existing clinical information systems to allow physician access to patient-specific information to screen for drug interactions and allergies.
Electronic preventive services selector: A digital tool for primary care clinicians to use when recommending preventive services for their patients unveiled by the Department of Health and Human Services’ Agency for Healthcare Research and Quality (AHRQ), in November 2006; designed for use on a personal digital assistant (PDA) or desktop computer to allow clinicians to access the latest recommendations from the AHRQ-sponsored U.S. Preventive Services Task Force; designed to serve as an aid to clinical decision-making at the point of care and contains 110 recommendations for specific populations covering 59 separate preventive services topics; a real time search function allows a clinician to input a patient’s age, gender, and selected behavioral risk factors, such as whether or not they smoke, in the appropriate fields, while the software cross-references the patient characteristics entered with the applicable Task Force recommendations and generates a report specifically tailored for that patient.
Electronic signature: Various date and time stamped electronic security verification systems, such as passwords, encryption, ID numbers, biometrics identifiers, etc; electrical transmission and authentication of real signatories; signatory attribute that is affixed to an electronic health document to bind it to a particular entity; an electronic signature process secures the user authentication (proof of claimed health identity, such as by biometrics (fingerprints, retinal scans, hand written signature verification, etc.), tokens or passwords) at the time the signature is generated; creates the logical manifestation of signature (including the possibility for multiple parties to sign a medical document and have the order of application recognized and proven) and supplies additional information such as time stamp and signature purpose specific to that user; and ensures the integrity of the signed document to enable transportability, interoperability, independent verifiability, and continuity of signature capability; verifying a signature on a document verifies the integrity of the document and associated attributes and verifies the identity of the signer; there are several technologies available for user authentication, including passwords, cryptography, and biometrics (ASTM 1762-95).
Encryption: Changing the original text to a secret message.
Gigabytes (GB): Billions of bytes of data.
Gramm-Leach-Bliley Act: A federal act that requires private data be protected by banks and financial institutions.
Hacker: A person who possesses advanced computer skills and is adept at exploring computers and networks in order to break into them.
HEALTH 1.0: This is the dying healthcare system of yesterday and today. Information is communicated from doctors to patients. It is a basic B2C [business-to-consumer] website as the internet became one big encyclopedia by aggregating knowledge silos. Some doctors maintain websites, others do not. Nevertheless, Health 1.0 has a command and control hierarchy; doctors on top of the pyramid, patients on the bottom.
HEALTH 2.0:According to Matthew Holt [personal communication] Healthcare 2.0 may be defined as: “The foundation of healthcare 2.0 is information exchange plus technology. It employs user-generated content, social networks and decision support tools to address the problems of inaccessible, fragmentary or unusable health care information. Healthcare 2.0 connects users to new kinds of information, fundamentally changing the consumer experience (e.g., buying insurance or deciding on/managing treatment), clinical decision-making (e.g., risk identification or use of best practices) and business processes (e.g., supply-chain management or business analytics)”.
And so, if Health 1.0 was a static book, Health 2.0 is a dynamic discussion
Example: The power of the internet is illustrated in the phenomenon of “crowd-sourcing.” In this context, the term means to harvest the reach of social networking [wisdom of crowds] to solve a problem. A knowledge seeker asks a question and participants respond. For example, readers can participate on the www.MedicalExecutivePost.com or www.BusinessofMedicalPractice.com sites to improve the administration of any medical practice. And, www.PodiatryPrep.com is an example of how podiatrists connect for global board certification assistance.
***
***
HEALTH 2.0 Plus:The Dictionary of Health Insurance and Managed Care defines this emerging hybrid as a bridge uniting the philosophy of contemporary Health 2.0 with futuristic Health 3.0 technologies. Cisco System’s HealthPresence is one example developed in 2010, by Dr. T. Warner Hudson. Using the network as a platform, HealthPresence combines video, audio and information to create an environment similar to what patients experience when they visit their own doctor.
HEALTH 3.0: Soon, patients will not only be seeking information; but actionable intelligence – whether it is artificial or real. Patients will communicate almost as with another patient or doctor. The internet won’t just blindly do what we tell it to do – it will think and represent some amazing opportunities. For example, imagine your toilet running a SMAC 20 and then being instantly notified of the results by your smart phone? Or; use your iPhone to send pictures and streaming videos of conditions for a second opinion www.KnockingLive.com
Health information technology: The application of information processing involving both computer hardware and software that deals with the storage, retrieval, sharing, and use of health care information, medical data, and knowledge for communication and decision making.
Health information technology auditor: An expert who evaluate a health organization’s computer systems to ensure the proper safeguards are in place to protect and maintain the integrity of the firm’s data; While the position has existed since the mid-1960s, companies that previously employed just a handful of HIT auditors are now significantly adding to their ranks, sometimes doubling, tripling or quadrupling current staff levels; much current demand is due to the Sarbanes-Oxley Act and other legislation aimed at improving corporate governance in the wake of major accounting scandals earlier in the decade; publicly traded hospital systems require the expertise of HIT auditors to meet ongoing compliance requirements; the Gramm-Leach-Bliley Act and the Health Insurance Portability and Accountability Act (HIPAA), among other regulations, also are fueling the need for HIT auditors. Health IT auditors must have a general understanding of accounting principles and the strategic vision to ensure a health organization’s HIT systems allow it to achieve its short- and long-term objectives. Many hospitals promote from within for this role. Health facilities who look outside the organization for these professionals usually seek candidates with experience, knowledge of healthcare of emerging technologies and issues, and increasingly, certifications such as the certified information systems auditor (CISA) designation.
Health information technology promotion act: Legislation to accelerate the adoption of interoperable electronic health records by ensuring uniform standards, championed by Rep. Nancy Johnson, R-Conn, (H.R. 4157) which would: codify the Office of the National Coordinator for Health Information Technology in statute and delineate its ongoing responsibilities; create exceptions to the fraud and abuse statutes to allow certain providers to fund health information technology equipment and services for other providers; and provide for a study of federal and state health privacy policies.
Health Insurance Portability and Accountability Act (HIPAA): A federal act that requires enterprises in the health sector to guard protected health information and implement policies and procedures to safeguard it.
Health level seven: An international community of healthcare subject matter experts and information technology physicians and scientists collaborating to create standards for the exchange, management and integration of protected electronic healthcare information; the Ann Arbor, Mich.-based Health Level Seven (HL7) standards developing organization has evolved Version 3 of its standard, which includes the Reference Information Model (RIM) and Data Type Specification (both ANSI standards); HL7 Version 3 is the only standard that specifically deals with creation of semantically interoperable healthcare information, essential to building the national infrastructure; HL7 promotes the use of standards within and among healthcare organizations to increase the effectiveness and efficiency of healthcare delivery for the benefit of all patient, payers, and third parties; uses an Open System Interconnection (OSI) and high level seven healthcare electronic communication protocol that is unique in the medical information management technology space and modeled after the International Standards Organization (ISO) and American National Standards Institute (ANSI); each has a particular healthcare domain such as pharmacy, medical devices, imaging or insurance (claims processing) transactions. Health Level Seven’s domain is clinical and administrative data.
Hot site: An alternative backup site that contains the same equipment as found in the organization’s actual IT center.
Human firewall: An employee who practices good security techniques to prevent any security attacks from passing through them.
Incident response team: An employee team charged with gathering and handling the digital evidence of an attack.
Individually identifiable health information: Medical information that is created or received by a covered entity; relates to the physical or mental health condition of an individual, provision of health care or the payment for the provision of health care; identifies the individual or there is reasonable belief that the information can be used to identify the individual.
Information security: A computer or network that is free from threats against it.
Integrity: The security goal that generates the requirement for protection against either intentional or accidental attempts to violate data integrity (the property that data has when it has not been altered in an unauthorized manner) or system integrity (the quality that a system has when it performs its intended function in an unimpaired manner, free from unauthorized manipulation).
Intellectual property: Works created by others such as books, music, plays, paintings, and photographs.
IT-related risk: The net mission impact considering (1) the probability that a particular threat-source will exercise (accidentally trigger or intentionally exploit) system vulnerability and (2) the resulting impact if this should occur. IT-related risks arise from legal liability or mission loss due to:
* Unauthorized (malicious or accidental) disclosure, modification, or destruction of information
* Unintentional errors and omissions
* IT disruptions due to natural or man-made disasters
* Failure to exercise due care and diligence in the implementation and operation of the IT system.
Key-in-knob lock: A basic lock that has the lock mechanism embedded in the knob or handle.
Keystroke logger: A type of hardware spyware that captures keystrokes as they are typed.
Logic bombs: A computer program that lies dormant until it is triggered by a specific event.
Lossless: To compress electronic digital data.
Malicious code: Programs that are intentionally created to break into secure computers or to create havoc after the computers are accessed.
Master patient index: Healthcare facility composite that links and assists in tracking patient, person, or member activity within an organization (or health enterprise) and across patient care settings; hardcopy or electronic identification of all patients treated in a facility or enterprise and lists the medical record or identification number associated with the name; can be maintained manually or as part of a computerized system; typically, those for healthcare facilities are retained permanently, while those for insurers, registries, or others may have different retention periods; a database of all the patients ever registered (within reason) at a facility; name, demographics, insurance, next of kin, spouse, etc.
Medically unbelievablE event: Implemented on Jan. 1, 2007, the CMS blockage of payments for medical services that make no sense based on “anatomic considerations” or medical reasonableness when the same patient, date of service, HCPCS code or provider is involved; unlike other National Correct Coding Initiative (NCCI) edits, MUEs can’t be overridden by a modifier because there will never be a scenario where the physician had a good reason to submit a claim for removing a second appendix from the same person; etc.
Megabytes (MB): Millions of bytes of storage.
Memory stick: USB flash or non-volatile storage device; Sony CompactFlash®, pen or mini-drive; flash card, smart media, slang terms.
Mesh: Medical Subject Headings, the controlled vocabulary of about 16,000 terms used for MEDLINE and certain other MEDLARS databases.
Minimum necessary: The amount of protected health information shared among internal or external parties determined to me the smallest amount needed to accomplish its purpose for Use or Disclosure; the amount of health information or medical data needed to accomplish a purpose varies by job title, CE or job classification.
Minimum necessary rule: HIPAA regulation that suggests any PHI used to identify a patient, such as a social security number, home address or phone number; divulge only essential elements for use in transferring information from patient record to anyone else that requires the information; especially important with financial information; changes the way software is written and vendor access is provided. The “Minimum Necessary” Rule states the minimum use of PHI that can be used to identify a person, such as a social security number, home address or phone number. Only the essential elements are to be used in transferring information from the patient record to anyone else that needs this information. This is especially important when financial information is being addressed. Only the minimum codes necessary to determine the cost should be provided to the financial department. No other information should be accessed by that department. Many institutions have systems where a registration or accounting clerk can pull up as much information as a doctor or nurse, but this is now against HIPAA policy and subject to penalties. The “minimum necessary” rule is also changing the way software is set up and vendor access is provided.
Mirror site: A secondary location identical to the primary IT site that constantly receives a copy of data from the primary site.
National health information network: The technologies, standards, laws, policies, programs and practices that enable health information to be shared among health decision makers, including consumers and patients, to promote improvements in health and healthcare; vision for the NHII began more than a decade ago with publication of an Institute of Medicine report, The Computer-Based Patient Record. The path to a national network of healthcare information is through the successful establishment of Regional Health Information Organizations (RHIO).
National provider identifier: Originally was an eight-digit alphanumeric identifier. However, the healthcare industry widely criticized this format, claiming that major information systems incompatibilities would make it too expensive and difficult to implement. DHHS therefore revised its recommendation, instead specifying a 10-position numeric identifier with a check digit in the last position to help detect keying errors. The NPI carries no intelligence; in other words, its characters will not in themselves provide information about the provider. More recently, CMS announced that HIPAA-covered entities such as providers completing electronic transactions, healthcare clearinghouses, and large health plans, must use only the NPI to identify covered healthcare providers in standard transactions by May 23, 2007. Small health plans must use only the NPI by May 23, 2008. The proposal for a Standard Unique National Health Plan (Payer) Identifier was withdrawn on February, 2006. (According to CMS, “withdrawn” simply means that there is not a specific publication date at this time. Development of the rule has been delayed; however, when the exact date is determined, the rule will be put back on the agenda.)
Network: A group of interconnected computers.
Notebook safe: A special safe secured to a wall or the trunk of a car used for storing a notebook computer.
Operating system hardening: Steps that can be taken to make a personal computer operating system more secure.
Optical disc: A disc that uses laser technology to record data.
Password: A secret combination of words or numbers that authenticates or identifies the user.
Patch: A software update to correct a problem.
Patch management: Tools, utilities, and processes for keeping computers up to date with new software updates that are developed after a software product is released.
Pharmacy information system: Drug tracking and dispensation related health management information system for hospitals and healthcare organizations.
PhisHing: An attempt to fraudulent gather confidential information by masquerading as a trustworthy entity, person or business in an apparently official email, text message or website; carding or spoofing; video vishing; phish-tank; vish-tank; slang terms.
Physical security: The process of protecting the computer itself.
Port scanning: Sending a flood of information to all of the possible network connections on a computer.
Ports: The network connections on a computer.
Preset lock: A basic lock that has the lock mechanism embedded in the knob or handle.
Privacy: The quality or state of being hidden, encrypted, obscure, or undisclosed; especially medical data or PHI.
Privacy act: Federal legislature of 1974 which required giving patient some control over their PHI.
Privacy enhanced mail: Email message standard protocol for enhanced medical, health data or other security.
Privacy officer: A medical entity’s protected client information and security officer; required by each covered entity, to be responsible for “the development and implementation of the policies and procedures” necessary for compliance.
Privacy rule: The Federal privacy regulations promulgated under the Health Insurance Portability and Accountability Act (HIPAA) of 1996 that created national standards to protect medical records and other protected health information. The Office of Civil Rights (OCR) within the Department of Health and Human Services (DHHS) regulates the privacy rules.
Privacy standards: Any protocol to ensure the confidentiality of PHI.
Private key system: A means of cryptography where the same key is used to both encrypt and decrypt a message.
Public key system: A means of cryptography where two keys are used.
* Psychotherapy notes recorded (in any medium) by a health care provider who is a mental health professional documenting or analyzing the contents of conversation during a private counseling session or a group, joint, or family counseling session and that are separated from the rest of the individual’s medical record; excludes medication prescription and monitoring, counseling session start and stop times, the modalities and frequencies of treatment furnished, results of clinical tests, and any summary of the following items: diagnosis, functional status, the treatment plan, symptoms, prognosis, and progress to date.
* Public health authority means an agency or authority of the United States, a State, a territory, a political subdivision of a State or territory, or an Indian tribe, or a person or entity acting under a grant of authority from or contract with such public agency, including the employees or agents of such public agency or its contractors or persons or entities to whom it has granted authority, that is responsible for public health matters as part of its official mandate.
* Required by law means a mandate contained in law that compels a covered entity to make a use or disclosure of protected health information and that is enforceable in a court of law; includes but is not limited to, court orders and court-ordered warrants; subpoenas or summons issued by a court, grand jury, a governmental or tribal inspector general, or an administrative body authorized to require the production of information; a civil or an authorized investigative demand; Medicare conditions of participation with respect to health care providers participating in the program; and statutes or regulations that require the production of information, including statutes or regulations that require such information if payment is sought under a government program providing public benefits.
Regional health information organization: A multi-stakeholder organization that enables the exchange and use of health information, in a secure manner, for the purpose of promoting the improvement of health quality, safety and efficiency; the U.S. Department of Health and Human Services see RHIOs as the building blocks for the national health information network (NHIN) that will provide universal access to electronic health records; other experts maintain that RHIOs will help eliminate some administrative costs associated with paper-based patient records, provide quick access to automated test results and offer a consolidated view of a patient’s history.
Risk assessment: The process of identifying the risks to system security and determining the probability of occurrence, the resulting impact, and additional safeguards that would mitigate this impact.
Risk management: The total process of identifying, controlling, and mitigating information system–related risks. It includes risk assessment; cost-benefit analysis; and the selection, implementation, test, and security evaluation of safeguards. This overall system security review considers both effectiveness and efficiency, including impact on the mission and constraints due to policy, regulations, and laws.
Royalties: Payment to the owner or creator of intellectual property for their work.
Sarbanes-Oxley Act (Sarbox): A federal act that enforces reporting requirements and internal controls on electronic financial reporting systems.
Scanning: Locating a computer that can be broken into.
Script kiddies: Younger and less sophisticated users who break into a computer with malicious intent.
Secure virtual private network: Cryptographic tunneling protocols to provide the necessary health data confidentiality (preventing snooping), sender authentication (preventing identity spoofing), and message integrity (preventing message alteration) to achieve the medical privacy intended. When properly chosen, implemented, and used, such techniques can provide secure communications over unsecured networks.
Security: A set of healthcare information technology system characteristic and mechanisms which span the system both logically and physically; electronic access control against unauthorized intervention, both friendly or malicious; encompasses all of the safeguards in an information system, including hardware, software, personnel policies, information practice policies, disaster preparedness, and the oversight of all these areas; the purpose of health information security is to protect both the system and the information it contains from unauthorized access from without and from misuse from within; through various security measures, a health information system can shield confidential information from unauthorized access, disclosure and misuse, thus protecting privacy of the individuals who are the subjects of the stored data; security life cycle.
Security administration: The physical and electrical protection features of an IT health system needed to be managed in order to meet the needs of a specific installation and to account for changes in the healthcare entities operational environment.
Security compromise: Physical or electronic data, file, program or transmission error due to malicious miscreants or software interventions; health data confidentiality breach.
Security configuration: Measures, practices, and procedures for the safety of information systems that must be coordinated and integrated with each other and other methods, practices, and procedures of the organization established in order to credential safekeeping policy; provides written security plans, rules, procedures, and instructions concerning all components of a healthcare entity’s security; procedures must give instructions on how to report breaches and how those breaches are to be handled within the organization.
Security configuration management: The measurement of practices and procedures for the security of information systems that is coordinated and integrated with each other and other measures, practices and procedures of the organization so as to create a coherent system of health data security (NIST Pub 800-14).
Security domain: A set of subjects, their information objects, and a common security policy; foundation for IT security is the concept of security domains and enforcement of data and process flow restrictions within and between these domains.
Security goals: The five security goals are integrity, availability, confidentiality, accountability, and assurance.
Security information system: security is a system characteristic and a set of mechanisms that span the system both logically and physically.
Security policy: A formal written policy that outlines the importance of security to the organization and establishes how the security program is organized.
Share: An object that is shared with others over a computer network.
Signature files: Files that contain updated antivirus information.
Smart card: A device that contains a chip that stores the user’s private key, login information, and public key digital certificate.
Sniffing: Listening to the traffic on a computer network and then analyzing it.
Social engineering: Relying on trickery and deceit to break security and gain access to computers.
Spam: Unsolicited e-mail messages.
Spy: A person who has been hired to break into a computer and steal data.
Spyware: Hardware or software that “spies” on what the user is doing and captures that activity without their knowledge.
Stealth signal transmitter: Software installed on a notebook computer that sends a signal that can be traced.
Threat analysis: The examination of threat-sources against system vulnerabilities to determine the threats for a particular system in a particular operational environment.
Threat modeling: A process of constructing scenarios of the types of threats that assets face.
Threat: The potential for a threat-source to exercise (accidentally trigger or intentionally exploit) a specific vulnerability.
Threat-source: Either (1) intent and method targeted at the intentional exploitation of a vulnerability or (2) a situation and method that may accidentally trigger a vulnerability.
Token: A security device used to authenticate the user by having the appropriate permission (like a password) embedded into the device.
USA Patriot Act: A federal act designed to broaden the surveillance of law enforcement agencies to enhance the detection and suppression of terrorism.
Username: A unique identifier of a person used to access a computer system.
Virus: A program that secretly attaches itself to other programs and when executed causes harm to a computer.
Vulnerability: A flaw or weakness in system security procedures, design, implementation, or internal controls that could be exercised (accidentally triggered or intentionally exploited) and result in a security breach or a violation of the system’s security policy.
Vulnerability assessment: A process to determine what vulnerabilities exist in the current system against these attacks.
Vulnerability assessment managed services: Agencies that use scanning devices connected to probe an organization’s security to look for vulnerabilities.
War driving: A technique used to locate wireless local area networks (WLANs).
WiMax: A more powerful version of Wi-Fi that can provide wireless Internet access over wider geographic location such as a city; an acronym that stands for Worldwide Interoperability for Microwave Access, and is a certification mark for products that pass conformity and interoperability tests for the IEEE 802.16 standards. IEEE 802.16 is working group number 16 of IEEE 802, specializing in point-to-multipoint broadband wireless access.
Wireless hot spot: Specific geographic location in which an access point provides public wireless broadband network services; security is risky for PHI; hotspot.
Wireless local area networks: A computer network that uses radio waves instead of wires to connect computers.
Worm: A program that does not attach itself to other programs or need user intervention to execute.
Incentives: It is broadly accepted that incenting someone to do something is effective, whether it be paying office staff a commissions to sell more healthcare products, or giving bonuses to office employees if they work efficiently to see more HMO patients. Some experts even suggest there are five specific components1 that should be built into an overall physician incentive program:
Appropriate financial incentives.
Managed-care efficiency incentives.
Group citizenship.
Patient satisfaction.
Group profitability.
What is not well understood is that the incentives cause a sub-conscious distortion of decision-making ability in the incented person. This distortion causes the affected person – whether it is yourself or someone else – to truly believe in a certain decision, even if it is the wrong choice when viewed objectively. Service professionals, including financial advisors and lawyers, are affected by this bias, and it causes them to honestly offer recommendations that may be inappropriate, and that they would recognize as being inappropriate if they did not have this bias.
According to colleague Dan Ariely PhD, the existence of this bias makes it important for each one of us to examine our incentive biases and take extra care when advising physician clients, or to make sure we are appropriately considering non-incented alternatives.
Posted on June 20, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Demanding High Professional Moral Standards of Self and Financing Organizations
By Dr. David Edward Marcinko MBAMEd
ByRender Davis MBA
***
***
It has been argued that physicians have abdicated the “moral high ground” in health care by their interest in seeking protection for their high incomes, their highly publicized self-referral arrangements, and their historical opposition toward reform efforts that jeopardized their clinical autonomy.
In his book Medicine at the Crossroads, Emory University professor Melvin Konnor, M.D., noted that “throughout its history, organized medicine has represented, first and foremost, the pecuniary interests of doctors.” He goes on to lay significant blame for the present problems in health care at the doorstep of both insurers and doctors, stating that “the system’s ills are pervasive and all its participants are responsible.” In order to reclaim their once esteemed moral position, physicians must actively reaffirm their commitment to the highest standards of the medical profession and call on other participants in the health care delivery system also to elevate their values and standards to the highest level.
In the evolutionary shifts in models for care, physicians have been asked to embrace business values of efficiency and cost effectiveness, sometimes at the expense of their professional judgment and personal values. While some of these changes have been inevitable as our society sought to rein in out-of-control costs, it is not unreasonable for physicians to call on payers, regulators and other parties to the health care delivery system to raise their ethical bar.
Harvard University physician-ethicist Linda Emmanuel noted that “health professionals are now accountable to business values (such as efficiency and cost effectiveness), so business persons should be accountable to professional values including kindness and compassion.
”Within the framework of ethical principles, John La Puma, M.D., wrote in Managed Care Ethics, that “business’s ethical obligations are integrity and honesty. Medicine’s are those plus altruism, beneficence, nonmaleficence, respect, and fairness.”
Incumbent in these activities is the expectation that the forces that control our health care delivery system, the payers, the regulators, and the providers will reach out to the larger community, working to eliminate the inequities that have left so many Americans with limited access to even basic health care. Charles Dougherty clarified this obligation in Back to Reform, when he noted that “behind the daunting social reality stands a simple moral value that motivates the entire enterprise. Health care is grounded in caring. It arises from a sympathetic response to the suffering of others.”
Posted on May 6, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By National Council on Disability
The origins of managed care can be traced back to at least 1929, when Michael Shadid, a physician in Elk City, Oklahoma, established a health cooperative for farmers in a small community without medical specialists or a nearby general hospital. He sold shares to raise money to establish a local hospital and created an annual fee schedule to cover the costs of providing care. By 1934, 600 family memberships were supporting a staff that included Dr. Shadid, four newly recruited specialists, and a dentist. That same year, two Los Angeles physicians, Donald Ross and Clifford Loos, entered into a prepaid contract to provide comprehensive health services to 2,000 employees of a local water company
Development of Prepaid Health Plans
Other major prepaid group practice plans were initiated between 1930 and 1960, including the Group Health Association in Washington, DC, in 1937, the Kaiser-Permanente Medical Program in 1942, the Health Cooperative of Puget Sound in Seattle in 1947, the Health Insurance Plan of Greater New York in New York City in 1947, and the Group Health Plan of Minneapolis in 1957. These plans encountered strong opposition from the medical establishment, but they also attracted a large number of enrollees.
Today, such prepaid health plans are commonly referred to as health maintenance organizations (HMOs). The term “health maintenance organization,” however, was not coined until 1970, with the aim of highlighting the importance that prepaid health plans assign to health promotion and prevention of illness. HMOs are what most Americans think of when the term “managed care” is used, even though other managed care models have emerged over the past 40 years.
Public Managed Care Plans
The enactment of the Health Maintenance Organization Act of 1973 (P. L. 93-222) provided a major impetus to the expansion of managed health care. The legislation was proposed by the Nixon Administration in an attempt to restrain the growth of health care costs and also to preempt efforts by congressional Democrats to enact a universal health care plan. P. L. 93-222 authorized $375 million to assist in establishing and expanding HMOs, overrode state laws restricting the establishment of prepaid health plans, and required employers with 25 or more employees to offer an HMO option if they furnished health insurance coverage to their workers. The purpose of the legislation was to stimulate greater competition within health care markets by developing outpatient alternatives to expensive hospital-based treatment. Passage of this legislation also marked an important turning point in the U.S. health care industry because it introduced the concept of for-profit health care corporations to an industry long dominated by a not-for-profit business model.
In the decade following the passage of P. L. 93-222, enrollment in HMOs grew slowly. Stiff opposition from the medical profession led to the imposition of regulatory restrictions on HMO operations. But the continued, rapid growth in health care outlays forced government officials to look for new solutions. National health expenditures grew as a proportion of the overall gross national product (GNP) from 5.3 percent in 1960 to 9.5 percent in 1980. In response, Congress in 1972 authorized Medicare payments to free-standing ambulatory care clinics providing kidney dialysis to beneficiaries with end-stage renal disease. Over the following decade, the Federal Government authorized payments for more than 2,400 Medicare procedures performed on an outpatient basis.
Responding to the relaxed regulatory environment, physicians began to form group practices and open outpatient centers specializing in diagnostic imaging, wellness and fitness, rehabilitation, surgery, birthing, and other services previously provided exclusively in hospital settings. As a result, the number of outpatient clinics skyrocketed from 200 in 1983 to more than 1,500 in 1991, and the percentage of surgeries performed in hospitals was halved between 1980 (83.7%) and 1992.
The Influence of Medicare Prospective Payments
Health care costs, however, continued to spiral upward, consuming 10.8 percent of GNP by 1983. In an attempt to slow the growth rate, Congress in 1982 capped hospital reimbursement rates under the Medicare program and directed the secretary of HHS to develop a case mix methodology for reimbursing hospitals based on diagnosis-related groups (DRGs). As an incentive to the hospital industry, the legislation (the Tax Equity and Fiscal Responsibility Act (P. L. 97-248)) included a provision allowing hospitals to avoid a Medicare spending cap by reaching an agreement with HHS on implementing a prospective payment system (PPS) to replace the existing FFS system. Following months of intense negotiations involving federal officials and representatives of the hospital industry, the Reagan Administration unveiled a Medicare PPS. Under the new system, health conditions were divided into 468 DRGs, with a fixed hospital payment rate assigned to each group.
Once the DRG system was fully phased in, Medicare payments to hospitals stabilized. However, since DRGs applied to inpatient hospital services only, many hospitals, like many group medical practices, began to expand their outpatient services in order to offset revenues lost as a result of shorter hospital stays. Between 1983 and 1991, the percentage of hospitals with outpatient care departments grew from 50 percent to 87 percent. Hospital revenues derived from outpatient services doubled over the period, reaching 25 percent of all revenues by 1992
Since DRGs were applied exclusively to Medicare payments, hospitals began to shift unreimbursed costs to private health insurance plans. As a result, average per employee health plan premiums doubled between 1984 and 1991, rising from $1,645 to $3,605. With health insurance costs eroding profits, many employers took aggressive steps to control health care expenditures. Plan benefits were reduced. Employees were required to pay a larger share of health insurance premiums. More and more employers—especially large corporations—decided to pay employee health costs directly rather than purchase health insurance. And a steadily increasing number of large and small businesses turned to managed health care plans in an attempt to rein in spiraling health care outlays.
Managed Long-Term Services and Supports
Arizona became the first state to apply managed care principles to the delivery and financing of Medicaid-funded LTSS in 1987, when the federal Health Care Financing Administration (later renamed the Centers for Medicare and Medicaid Services) approved the state’s request to expand its existing Medicaid managed care program. Medicaid recipients with physical and developmental disabilities became eligible to participate in the Arizona Long-Term Care System as a result of this program expansion. Over the following two decades, a number of other states joined Arizona in providing managed LTSS, and by the summer of 2012, 16 states were operating Medicaid managed LTSS programs
Growth of Commercial Managed Care Plans
During the late 1980s and early 1990s, managed care plans were credited with curtailing the runaway growth in health care costs. They achieved these efficiencies mainly by eliminating unnecessary hospitalizations and forcing participating physicians and other health care providers to offer their services at discounted rates. By 1993, a majority (51%) of Americans receiving health insurance through their employers were enrolled in managed health care plans. Eventually, however, benefit denials and disallowances of medically necessary services led to a public outcry and the enactment of laws in many states imposing managed care standards. According to one analysis, nearly 900 state laws governing managed health practices were enacted during the 1990s. Among the measures approved were laws permitting women to visit gynecologists and obstetricians without obtaining permission from their primary care physician, establishing the right of patients to receive emergency care, and establishing the right of patients to appeal decisions made by managed care firms. Congress even got into the act in 1997 when it passed the Newborns’ Mother Health Protection Act, prohibiting so-called “drive-through deliveries” (overly restrictive limits on hospital stays following the birth of a child).
Research studies have yielded little evidence that managed health care excesses have undermined the quality of health care services. For example, in a survey of 2,000 physicians, Remler and colleagues found that managed care insurance plans denied only about 1 percent of recommended hospitalizations, slightly more than 1 percent of recommended surgeries, and just over 2.5 percent of referrals to specialists. In another study, Franks and colleagues found that medical outcomes were similar for participants in HMOs versus FFS health plans. Franks also reported that HMO patients were hospitalized 40 percent less frequently than FFS patients, and the rate of inappropriate hospitalizations was lower among HMO patients.
Over the past 15 to 20 years, the public outcry against draconian managed care practices has waned, primarily due to the expanded out-of-network options afforded to participants in HMOs, PPOs, and POS health plans. But the perception that managed care represents an overly cost-conscious, mass market approach to delivering medical services lingers among the American public, even though more than 135 million people with health insurance coverage now receive their primary, preventive, and acute health services through a managed care plan. People with disabilities, especially high users of medical care and LTSS, share many of the same negative perceptions of managed care as the general public.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Managed care insurers have profited handsomely from Medicare Advantage plans, scoring billions in annual profits. They credit this financial wizardry to their use of sophisticated data analytics, preventative care, cost optimization, provider networks, evidence and value-based care and risk mitigation strategies. However, doctors, hospitals, and medical providers assert something else.
In fact, Medicare Advantage plans have been making headlines in 2024, but not in a positive light, at least for health insurance companies. Medicare is a government-sponsored health insurance benefit; generally for retired people aged 65 and older.
For most, the money for Medicare Part B medical insurance or Part C Medicare Advantage plans is withdrawn directly from Social Security benefits monthly, coupled with a relatively small monthly payment from the patient. Nearly half of the Medicare population is enrolled in Part C Medicare Advantage plans.
***
***
However, there have been rumblings in the medical sector between medical providers and medical insurers coming to a head. So, where do you stand?
Posted on May 15, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
NARROW NETWORKS
By Staff Reporters
An increasing number of insurers now promote “narrow network” plans that can be less expensive than more traditional offerings. However, that added affordability comes with a tradeoff that could leave you with fewer options for covered medical services.
Understanding Narrow Networks: Narrow network plans are similar to the health maintenance organizations (HMOs). Like standard HMOs, these plans limit coverage to a select group of physicians, specialists and hospitals. However, narrow network plans can be even more restrictive in the number of providers they include. Those providers generally have been proven to have higher measured quality and better outcomes for patients. They also typically agree to lower reimbursements from insurers, which can mean lower premiums and out-of-pocket expenses for consumers. You’re more likely to see narrow networks — which include narrow pharmacy networks — if you shop for your own health insurance on HealthCare.gov or your state’s insurance exchange. They’re less common in the plan options provided by private employers.
Advantages Beyond the Savings The fact that narrow network plans include fewer providers doesn’t mean you’ll be getting lower quality care. In fact, many insurers require providers to have a proven track record that’s focused on their patients’ health outcomes. And they can offer a number of additional advantages, beyond just lower costs:
Coordinated care. Working within a single health system can mean better communication between your doctors. You might also have easier access to all your medical records through a dedicated online portal.
No referrals. Traditional HMO plans generally require a referral from your primary care physician for any consultations with a specialist. Many narrow network plans eliminate this requirement.
Added benefits. Many narrow network plans offer benefits designed to keep high-risk patients healthier. These can include options like free health coaching and live video services that enable remote, online medical consultations.
CONS: The biggest disadvantage to narrow network plans is less choice. Insurers keep these plans more affordable by negotiating lower reimbursements with health care providers. In return, those providers could see patient rosters grow, because smaller networks also mean less competition for those within the network. Smaller networks also can mean:
A need to change physicians. Your current primary care physician and specialists might not be included in the plan. This can mean starting over with new doctors who aren’t familiar with your particular health concerns.
Longer drives. With fewer choices, you may be forced into a longer commute to see an in-network physician. This could become a hardship for those in rural locations.
Lack of specialty options. A smaller network might not include the broad range of specialists large networks typically include.
Managed Care Organizations (MCOs) that accept capitated risk contracts face a potentially significant tax burden for Incurred but Not Reported (IBNR) claims. It is not uncommon that IBNR claims at the end of a reporting period equal one to two months premiums for MCOs under a fee-for-service model. The Internal Revenue Service (IRS) has taken a very strong position relative to the deductibility of these claims by saying that an MCO cannot deduct such losses if they are based on estimates.
Incurred But Not Reported [IBNR]Claims
IBNR is a term that refers to the costs associated with a medical service that has been provided, but for which the carrier has not yet received a claim. The carrier to account for estimated liability based on studies of prior lags in claim submission records IBNR reserves. In capitated contracts, MCOs are responsible for IBNR claims of their enrollees (Kennedy, 1).
For example, if an enrollee is treated in an emergency room, a plan may not know it is liable for this care for at least 30-60 days. Well-run plans devote considerable attention to accurately estimating such claims because a plan can look healthy based on claims submitted and be financially unhealthy if IBNR claims experience is increasing substantially but is unknown.
Why a Problem for HMO’s/MCOs
Section 809(d)(1) of the Code provides that, for purposes of determining the gain and loss from operations, a insurance company shall be allowed a deduction for all claims and benefits accrued, and all losses incurred (whether or not ascertained), during the taxable year on insurance and annuity contracts. Section 1.809-5(a) (1) of the Income Tax Regulations provides that the term “losses incurred (whether or not ascertained)” includes a reasonable estimate of the amount of the losses (based upon the facts in each case and the company’s experiences with similar cases) incurred but not reported by the end of the taxable year as well as losses reported but where the amount thereof cannot be ascertained by the end of the year. By taking into account for its prior years only the reported losses but not the unreported losses, the taxpayer has established a consistent pattern of treating a material item as a deduction. The effect of the taxpayer’s claim for the first time of a deduction for an estimate of losses incurred but unreported under section 809(d)(1) of the Code, was to change the timing for taking the deduction for the incurred but unreported losses.
Due to the taxpayer consistently deducting losses incurred in the taxable year in which reported, a change in the time for deducting losses incurred under section 809(d)(1) is a change in the method of accounting for such losses to which the provisions of section 446(e) apply (IRS, 14-30).
In order to qualify for an insurance company under the current IRS regulations, the MCO must have the following criteria (Kongstvedt, 235-256):
· At least 50% of the MCO must come from insurance related activities.
· The MCO must have an insurance company license.
If an MCO did not have these two criteria, the IRS will not deem the manage care company as an eligible insurance company. Therefore, the MCO would not be able to file for IBNRs with the IRS.
How MCOs/HMOs Intensify IBRN Claims
There is a high degree of uncertainty inherent in the estimates of ultimate losses underlying the liability for unpaid claims. The only reason the IRS would not allow an MCO to deduct IBNR because the financial statements is based on an estimate (IRS, 134-155).
Except through the insurance company exclusion IRS does not allow any taxpayer to deduct losses based on estimates. There has been some precedence set that the IRS will accept an amount for incurred but not reported claims if the amount is supported by valid receipts of claims that the company has in-house prior to the filing of the tax return.
There has been some controversy as to how long of a period of reporting time the IRS will allow you to include in those estimates. There are ranges from 3-6 months to file a claim (IRS, 137). The process by which these reserves are established requires reliance upon estimates based on known facts and on interpretations of circumstances, including the business’ experience with similar cases and historical trends involving claim payment patterns, claim payments, pending levels of unpaid claims and product mix, as well as other factors including court decisions, economic conditions and public attitudes.
There has been no clear indication from the IRS that it will accept an accrual for these losses and entities. Therefore, companies deducting such losses may eventually find themselves in a position where the IRS may challenge the relating deductibility of those losses.
Evaluating IBNRs from a New Present Value Perspective
The best measure of whether or not a stream of future cash flows actually adds value to the organization is the net present value (NPV). The best decision rule for NPV to accept or reject a decision problem is if the NPV is greater than zero, the project adds value to the organization. Although – if the NPV is exactly zero it neither adds nor subtracts value from the organization (McLean 193). In either case, the project is acceptable. In addition, if the NPV is less than zero, the project subtracts value from the organization and should not be undertaken (McLean, 193).
The provision for unpaid claims represents an estimate of the total cost of outstanding claims to the year-end date. Included in the estimate are reported claims, claims incurred but not reported and an estimate of adjustment expenses to be incurred on these claims. The losses are necessarily subject to uncertainty and are selected from a range of possible outcomes (Veal, 11). During the life of the claim, adjustments to the losses are made as additional information becomes available. The change in outstanding losses plus paid losses is reported as claims incurred in the current period.
All but the smallest organizations have predictable and unpredictable losses. It is important mentally to separate the two since predictable losses are not risks but normal business expenses. Risk is the degree to which losses vary from the expected. If losses average $85,000 per year but could be as much as $20 million, the risk is $20 million minus $85,000. The $85,000 figure represents reasonably predictable losses (Veal, 12).
IBNR Challenges and Solutions
While I was unable to find an actual amount of the cost of the penalties that can be incurred, the IRS is able to impose penalty fees under Section 4958 of the IRS code (IRS, 255). While penalties differ depending on individual bases, MCOs will be penalizing for any misconduct either by IRS Codes or Court Jurisdiction.
It is prudent that MCOs ensure their organization that they will not incur a financial “meltdown”. They further need to ensure IBNR is funded for period of at least 2-3 months. In some states, the state laws make the MCO financially responsible to pay the providers for a second time if the intermediary fails to pay or becomes insolvent (Cagle, 1).
Paid losses, paid expenses and net premiums are usually deductible; reserves for incurred-but-unpaid losses generally are not, unless the taxpaying entity is an insurance company. Consequently, if a corporation has a high effective tax rate and concedes that it cannot deduct self-insured loss reserves, some of its more cost-effective options may be a paid-loss retro (if state rules are not too restrictive), a compensating balance plan, or the formation of a pool or industry captive. Even these plans may be subject to IRS challenge. To qualify as a tax-deductible expense, a premium or other payment must satisfy two criteria (Cagle, 2):
There must be transfer of risk: an insurance risk. This differs from investment risk, but there is no authoritative definition of “risk transfer” other than various court decisions (primarily Helvering v. Le Gierse, 312 US 531 — U.S. Supreme Court 1941).
There must be both risk shifting and risk distribution. “Risk shifting” means that one party shifts the risk of loss to another, generally not in the same corporate family. “Risk distribution” means that the party assuming the risk distributes the potential liability, in part, among others.
The deductibility of an insurance expense may also be questioned if it is contingent upon a future happening, such as a loss payment, right to a dividend or other credit, or possible forgiveness of future loans or notes (Cagle, 3). This may seem a broad statement, but the Cost Accounting Standards Board states in its Standards for Accounting for Insurance Expense that any expense which is recoverable if there are no losses shall be accounted as a deposit, not an expense. This is essentially the IRS position (IRS, 145).
Assessment
While there are a few solutions to this matter, the IRS is making sure that MCOs will be penalized if MCOs improperly handle IBNRs. It is also important for organizations to understand the MCO’s policies regarding IBNR reserves and their contractual obligations. And, while the IRS has set limitations for MCOs to file their IBNR claims, MCOs have the major responsibility of allocating these IBNR claims appropriately. There are severe penalties for not properly filing the IBNR claims appropriately. However, there is several tax saving strategies to help MCOs properly file their IBNR claims with the IRS. It imperative that MCO executives and accounting manager consult an expert to properly plan an ethical strategy that will help them build a stable business that is trustworthy and reliable.
Bibliography
1. Cagle, Jason, Esq., Interview, June 8, 2004, interview performed by Ana Vassallo.
2. McLean, Robert A., Net Profit Value, Pages 193-194, 2nd Edition, Thomson/Delmar Learning, Financial Management in Heath Care Organization, 2003.
3. Patient-Physician Network, Managed Care Glossary, Printed 6/11/04 http:/www.drppg.com/managed_care.asp.
6. Kongstvedt, Peter R., Managed Care – What It Is and How it Works, Pages 235-256, Jones and Bartlett Publishers, 2003.
7. Veale, Tom, The Return of Captives in the Hard Market, Tristar Risk Management Aug. 22, 2002, San Diego RIMS.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on August 19, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Designated a Doody’s CORE TITLE
To keep up with the ever-changing field of health care, we must learn new and re-learn old terminology in order to correctly apply it to practice. By bringing together the most up-to-date abbreviations, acronyms, definitions, and terms in the health care industry, the Dictionary offers a wealth of essential information that will help you understand the ever-changing policies and practices in health insurance and managed care today. For Further Information.
Review
The Dictionary of Health Insurance and Managed Care lifts the fog of confusion surrounding the most contentious topic in the health care industrial complex today. My suggestion therefore is to ‘read it, refer to it, recommend it, and reap’.” —Michael J. Stahl,PhD, Physician Executive MBA Program, William B. Stokely Distinguished Professor of Business, The University of Tennessee, College of Business Administration
Posted on March 14, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Prior Authorization and Patient Harm
• 34% of physicians report that PA has led to a serious adverse event for a patient in their care. • 24% of physicians report that PA has led to a patient’s hospitalization. • 18% of physicians report that PA has led to a life-threatening event or required intervention to prevent permanent impairment or damage. • 8% of physicians report that PA has led to a patient’s disability/permanent bodily damage, congenital anomaly/birth defect or death.
Posted on July 22, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
BOOK REVIEW
“The Dictionary of Health Insurance and Managed Care lifts the fog of confusion surrounding the most contentious topic in the health care industrial complex today. My suggestion therefore is to ‘read it, refer to it, recommend it, and reap’.”
—Michael J. Stahl, PhD, Physician Executive MBA Program [William B. Stokely Distinguished Professor of Business]
The University of Tennessee, College of Business Administration
Managed care is a prospective payment method where medical care is delivered regardless of the quantity or frequency of service, for a fixed payment, in the aggregate. It is not traditional fee-for-service medicine or the individual personal care of the past, but is essentially utilitarian in nature and collective in intent. Will new-age healthcare reform be even more draconian?
Unhappy Physicians
There are many reasons why doctors are professionally and financially unhappy, some might even say desperate, because of managed care; not to mention the specter of healthcare reform from the Obama administration. For example:
A staggering medical student loan debt burden of $100,000-250,000 is not unusual for new practitioners. The federal Health Education Assistance Loan (HEAL) program reported that for the Year 2000, it squeezed significant repayment settlements from its Top 5 list of deadbeat doctor debtors. This included a $303,000 settlement from a New York dentist, $186,000 from a Florida osteopath, $158,000 from a New Jersey podiatrist, $128,000 from a Virginia podiatrist, and $120,000 from a Virginia dentist. The agency also excluded 303 practitioners from Medicare, Medicaid, and other federal healthcare programs and had their cases referred for nonpayment of debt.
Because of the flagging economy, medical school applications nationwide have risen. “Previously, there were a lot of different opportunities out there for young bright people”; according to Rachel Pentin-Maki; RN, MHA”; not so today. In fact, Physicians Practice Digest recently stated, “Medicine is fast becoming a job in which you work like a slave, eke out a middle class existence, and have patients, malpractice insurers, and payers questioning your motives.” Remarkably, the Cornell University School of Continuing Education has designed a program to give prospective medical school students a real-world peek, both good and bad.
The Ripple Effects of Managed Care and Reform
“Many people who are currently making a great effort and investment to become doctors may be heading for a role and a way of life that are fundamentally different from what they expect and desire,” according to Stephen Scheidt, MD, director of the $1,000 Cornell fee program; why?
Fewer fee-for-service patients and more discounted patients.
More paperwork and scrutiny of decisions with lost independence and morale.
Reputation equivalency (i.e., all doctors in the plan must be good), or commoditization (i.e., a doctor is a doctor is a doctor).
The provider is at risk for (a) utilization and acuity, (b) actuarial accuracy, (c) cost of delivering medical care, and (d) adverse patient selection.
Practice costs are increasing beyond the core rate of inflation.
Medicare reimbursements are continually cut.
Early Opinions
Richard Corlin MD, opined back in 2002 that “these are circumstances that cannot continue because we are going to see medical groups disappearing.” Furthermore, he stated, “This is an emergency that lawmakers have to address.” Such cuts also stand to hurt physicians with private payers since commercial insurers often tie their reimbursement schedules to Medicare’s resources. “That’s the ripple effect here,” says Anders Gilberg, the Washington lobbyist for the Medical Group Management Associations (MGMA).
Assessment
And so, some desperate doctors are pursing these sources of relief, among many others:
A growing number of doctors are abandoning traditional medicine to start “boutique” practices that are restricted to patients who pay an annual retainer of $1,500 and up for preferred services and special attention. Franchises for the model are also available.
Regardless of location, the profession of medicine is no longer ego-enhancing or satisfying; some MDs retire early or leave the profession all together. Few recommend it, as a career anymore.
Assessment
To compound the situation, it is well known that doctors are notoriously poor investors and do not attend to their own personal financial well being, as they expertly minister to their patients’ physical illnesses.
Conclusion
And so, your thoughts and comments on this Medical Executive-Post are appreciated. Tell us what you think? Are you a desperate doctor? Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe to the ME-P. It is fast, free and secure.
Posted on June 1, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
By HEALTH CAPITAL CONSULTANTS, LLC
On May 4, 2021, the National Academies for Sciences, Engineering and Medicine (NASEM) released a major report expressing a dire need to improve primary care in the U.S.
Since January 2020, an extensive committee within NASEM has worked to develop an implementation plan that will reopen the discussion of improving primary care as a means to improving overall health and achieving health equity.
I wish to make one clarification and one prediction regarding employed physicians.
The clarification is this: There is a common misconception that if healthcare operated under free market conditions, it would primarily be a cottage industry of solo practices and of small physician-owned hospitals. Such operations would not develop the capabilities of large healthcare entities that we commonly associate with central planning.
ASSESSMENT: In reality, however, the opposite would be the case.
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on May 4, 2012 by Dr. David Edward Marcinko MBA MEd CMP™
By Paul Esselman
Dear Medical Executive-Post Readers,
Cejka Executive Search is actively seeking an accomplished nurse executive with recent managed care experience to direct and coordinate the medical management, quality improvement and credentialing functions on behalf of a newly developed, Chicago based Medicaid managed care plan.
Would you have individuals within your professional network that you could recommend for this role?
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on May 24, 2011 by Dr. David Edward Marcinko MBA MEd CMP™
Clinical Care versus Finance
By Render S. Davis MHA CHE
Conflicts of interest are not a new phenomenon in medicine. In the fee-for-service system, physicians controlled access to medical facilities and technology, and they benefited financially from nearly every order or prescription they wrote. Consequently, there was an inherent temptation to over-treat patients. Even marginal diagnostic or therapeutic procedures were justified on the grounds of both clinical necessity and legal protection against threats of negligence.
Costs Rarely Considered
While it could be construed that this represented a direct conflict of interest, it could also be argued that most patients were well served in this system because the emphasis was on thorough, comprehensive treatment – where cost was rarely a consideration. It was a well known adage that physicians “could do well, by doing good.”
Managed Care
In managed care, the potential conflicts between patients and physicians took on a completely different dimension. By design, in health plans where medical care was financed through prepayment arrangements, the physician’s income was enhanced not by doing more for his or her patients, but by doing less.Patients, confronted with the realization that their doctor would be rewarded for the use of fewer resources, could no longer rely with certainty on the motives underlying a physician’s treatment plans. One inevitable outcome was the continuing decline in patients’ trust in their physicians. This has been exacerbated to some degree by revelations of significant financial remuneration to physicians by pharmaceutical and medical products firms for their services as researchers or active participants on corporate-funded advisory panels, calling into question the physician’s objectivity in promoting the use of company products to their peers or patients.
Conflicts of Interest
Conflicts of interest may also create concerns at a much higher level, as evidenced by the issues raised in 2008 litigation against Ingenix, a company that for more than a decade, provided information to the insurance industry on payments to out-of-network physicians for their “usual and customary rates (UCR).” As noted in court documents, Ingenix was a wholly-owned subsidiary of United Healthcare and the UCR information sold by the company to insurers may have been fundamentally biased in favor of the insurers, causing patients to pay larger out-of-pocket fees.
Assessment
As a result, New York attorney general Andrew Cuomo filed suit against Ingenix. This action was followed by suits brought against major insurers by the American Medical Association and several state medical groups for systematic underpayment to members, based on the biased data. To date there have been monetary settlements, but the issue continues to raise growing concerns regarding conflicts of interest among the key payers for health care.
Conclusion
And so, your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on November 5, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
Part Two
By Dr. David Edward Marcinko MBA
[Publisher-in-Chief]
If you read this ME-P regularly or have read my earlier blogs, you know that I am writing a book on practice management for the private medical practitioner.
A recent story in the Chicago Tribune on the difficult business life of private practitioners today reminds me that I need to keep my nose to the grindstone.
For example, according to the sanofi-aventis Pharmaceutical Company Managed Care Digest Series, for 2008-10, the following patterns and comparative trend information has been empirically determined and may provide a basic starting point for medical practitioners to share business management, facilities, personnel, and records information for enhanced success www.managedcaredigest.com
Mid-Level Provider and Staffing Trends
Mid-level provider use increased among multi-specialty groups, especially in those with more than half of their revenue from capitated contracts. Use also rose with the size of the practice and was highest with OB/GYN groups.
Medical support staff for all multi-specialty groups fell and was lowest in medical groups with less than 10 full-time equivalent (FTE) physicians. However, groups with a large amount of capitated revenue actually added support staff. Smaller groups limited support staff.
Compensation costs of support staff increased and the percentages of total operating costs associated with laboratories, professional liability insurance, IT services, and imaging also increased. Support staff costs increase with capitation levels and more than half of all operating costs are tied to support staff endeavors.
Managed Care Activity and Contracting Trends
More medical group practices are likely to own interests in preferred provider organizations (PPOs) than in HMOs and the percentages of groups with managed care revenue continues to rise. Multi-specialty and large groups also derive more revenue from MCOs than single specialty or smaller groups.
Managed care has little effect on physician payment methods that are still predominantly based on productivity. Physicians were paid differently for at-risk managed care contracts in only a small percentage of cases.
Most medical groups (75%) participating in managed care medicine have PPO contracts. Group practices contract with network HMOs more often than solo practices. Single-specialty groups more often have PPO contracts.
Capitated lives often raise capitation revenues in large group practices. Group practices are more highly capitated than smaller groups or solo practices. Almost 30% of highly capitated medical groups have more than 15 contracts and 22% have globally capitated contracts.
Higher capitation is linked with increased risk contracting. Larger groups have more risk contracting than smaller groups.
Financial Profile Trends
Medicare fee-for-service reimbursement is decreasing. Highly capitated groups incur high consulting fees.
The share of total gross charges for OB/GYN groups associated with managed care at-risk contracts is rising while non-managed care, or not-at-risk charges are declining.
Capitated contracts have little effect on the amount of on-site office non-surgical work. Off-site surgeries are most common for surgery groups, not medical groups.
Half of all charges are for on-site non-surgical procedures.
Highly capitated medical groups have higher operating costs and lower net profits.
Groups without capitation have higher laboratory expenses than those who do.
Physician costs are highest in orthopedic surgery group practices. Generally, median costs at most specialty levels are rising and profits shrinking.
Assessment
Obviously, the above information is only a gauge since regional differences, and certain medical sub-specialty practices and carve-outs, do exist.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on October 27, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
Part One of Two
By Dr. David Edward Marcinko MBA
[Publisher-in-Chief]
If you read this ME-P regularly or have read my earlier blogs, you know that I am writing a book on practice management for the private medical practitioner.
And, a recent story in the Chicago Tribune on the difficult business life of private practitioners today reminds me that I need to keep my nose to the grindstone.
For example, knowing your medical contract negotiation objectives, gathering information on the choices of contracts and discount payment systems, and understanding the pitfalls to watch for when evaluating a contract are the keys to any successful negotiation process.
Reimbursement Contract Negotiations
According to the sanofi-aventis Pharmaceutical Company Managed Care Digest Series, for 2008-10, the following pattern and trend comparative information has been empirically determined and may provide a basic starting point for practitioners to share business management, facilities, personnel, and other records for enhanced contract negotiation success.
Among all physicians in a single-specialty group practice, invasive cardiologists averaged the most encounters with total hospital inpatient admissions down from the prior year. However, encounters rose for cardiologists in multispeciality group practices.
Echocardiography was the most commonly performed procedure on HMO seniors, followed by coronary artery bypass graft surgery. Group practices performed cardiovascular stress tests for circulatory problems most often.
CT studies of the brain and chest were the most common studies for HMO seniors, while MRI head studies were the most common diagnostic test on commercial HMO members.
Colonoscopy was the most common digestive system procedure on senior HMO members, while barium enemas were more common on commercial members.
Hospital admission volume decreased for allergists, family practitioners, internists, OB/GYNs, pediatricians, and general surgeons.
Internists ordered more in-hospital laboratory procedures than any other physicians in single-specialty groups.
Non-hospital MD/DOs used in-hospital radiology services most frequently, continuing a three-year upward trend.
Pediatricians averaged the most ambulatory encounters, down from the prior year.
Non-hospitalist internists ordered a higher number of in-hospital laboratory procedures than any other single medical specialty group, but allergists and immunologists increased their laboratory usage.
The number of ambulatory encounters increased for general surgeons, while group surgeons had the most cases. Capitated surgeons, of all types, had a lower mean number of surgical cases than surgeons in groups without capitation. Surgeons in internal medical groups also had more cases than those in multi-specialty groups.
The average number of total office visits per commercial and senior HMO visits fell, along with the number of institutional visits for both commercial and senior HMO members.
The average length of hospital stay for all commercial HMO members increased to 3.6 days but decreased to 6 days for all HMO members.
The total number of births increased for commercial HMO members served by medical group practices, and decreased for solo practitioners.
More than one-third of all medical groups use treatment protocols, rising from the year before. Multi-specialty groups were more likely to use them than single-specialty groups, who often develop their own protocols. The use of industry benchmarks to judge the quality of healthcare delivery also increased.
Outcome studies are most common at larger medical groups, and multi-specialty groups pursue quality assurance activities more often than single-specialty groups.
Provider interaction during office visits is increasingly coming under scrutiny. Patients approve of cardiologists more frequently than allergists and ophthalmologists.
Assessment
Obviously, the above information is only a gauge since regional differences, and certain medical sub-specialty practices and carve-outs, do exist.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on July 14, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
A Man Lived by the Side of the Road
By Dr. David Edward Marcinko MBA, CMP™
The “Quiet”
An old man lived by the side of the road and sold hot dogs. He was hard of hearing, so he had no radio. He had trouble with his eyes, so he had no newspaper.
But, he sold really – really good hot dogs. He put up a sign on the highway telling how good they were. He stood by the side of the road and cried, “Buy a hot dog, mister.” And people bought. He increased his meat and bun orders and he bought a bigger stove to take care of his trade.
The “Noise”
Soon, his son came home from college to help him. But, then something happened. His son said, “Father, haven’t you been listening to the radio? There’s a big depression on. The international situation is terrible and the domestic situation is even worse.”
Whereupon the father thought, “Well, my son has been to college. He listens to the radio and reads the papers, so he ought to know.” So, the father cut down his bun order, took down his advertising signs, and no longer bothered to stand on the highway to sell hot dogs. His hot dog sales fell almost overnight. “You were right, son,” the father said to the boy. “We are certainly in the middle of a great depression.”
-Author Unknown
Assessment
As a physician, professor or entrepreneur, how do you feel about this story? Does the managed care situation, PP-ACA and new healthcare reform focus, depress you? Do you feel alienated from your patients, profession or self?
What about you, financial advisors? Do layoffs in the industry affect your earning capacity? Or, does the market situation just hurt your self esteem? Which is worse; a real or psychologically negative impact? What about failed mortgage derivative products, collapsed banks, and related ethical scandals? Demoralizing!
And so, are you an optimist or pessimist about life and career? Is it really “different this time?”
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on June 5, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
Dictionary of Health Insurance and Managed Care
ADVERTISEMENT
Health care and health insurance have become increasingly complicated for the average citizen. While we at the Benefits Group do our best to assist individuals and businesses with their insurance needs, we appreciate and understand the value of educating yourself on the subject.
With that in mind, we’re offering a no strings attached opportunity to win a book that will provide many answers to your health care questions.
The book up for grabs is the Dictionary of Health Insurance and Managed Care by Dr. David E. Marcinko; FACFAS, MBA, CFP™, CMP™ [Editor-in-Chief] and Hope Rachel Hetico; RN, MHA, CPHQ, CMP™ [Managing Editor].
Beyond that, all you need to do to win is provide your email below. We will not be using this email for any marketing purposes, nor do we participate with any lists. We just need your email to contact the winner so we know where to send the book.
The only rules are that participants be at least 18 years of age and live in the residential United States. Also, only one entry per person (our software knows how to sniff you out if you cheat, so please don’t bother). We will be announcing a winner on July 1st, 2010 and will be accepting entries until midnight EST on June 30th, 2010.
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on May 31, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
A MEMORIAL DAY OPINION – EDITORIAL
[Innovation – Not Nationalization – Can Again Lead]
By Dr. David Edward Marcinko; FACFAS, MBA, CPHQ, CMP™
[Publisher-in-Chief]
By Hope Rachel Hetico; RN, MHA, CPHQ, CMP™
[Managing Editor]
Ann Miller; RN, MHA
[Executive-Director]
On this 2010 Memorial Day weekend, please allow us to directly reflect for a moment on the decline of the healthcare, banking and financial services industry in America. And; then somewhat indirectly comment on the hopeful emergence of the web 2.0 phenomena of which we all are a part. The competitive applicability to these sectors should be appreciated by the insightful ME-P reader.
Collapse of Command and Control Monopolies and Oligarchies
Old monopolies everywhere are crumbling because of tougher new competitors and the transparency wrought by electronic connectedness. For example, our old newspaper has to compete with the internet, your electric utility company battles low-cost local start-ups, telephone companies must begin installing fiber optic lines to fend off cable companies; and RIAs and fiduciary focused financial advisors [FAs] will supplant BDs and stock brokers in the financial services sector.
The airline industry collapsed a few years ago, the banking industry has just collapsed, and the auto industry is recovering as we pen this post. [We have a particular affinity for the auto sector however, as the son of a UAW member and step-daughter of Michiganders]. Regardless, the rush to more intense competition cannot be stopped. As a doctor, FA or other business competitor; you either keep pace or get crushed by quasi-oligarchic organizations like the American Medical Association [AMA], American Podiatric Medical Association [FPMA], American Dental Association [ADA], American Osteopathic Medical Association AOMA], Financial Planning Association [FPA], Certified Financial Planner Board of Standards [CFP BoS], College for Financial Planning [CFP] or the National Association of Personal Financial Advisors [NAPFA], etc. What have they, and Wall Street, done for you … lately? Scandal, taint, doubt, lost-credibility, a business-as-usual ennui, lethargy and ruin! Enter www.Sermo.com
In the last-generation of health insurance companies and related fraternal medical organizations, patients exercised great control over physician selection, had quicker access to specialists and encountered fewer restrictions on care. The reverse was true with financial services. But, because of advancing technology, aging demographics, intense R&D, global manufacturing, and escalating domestic HR costs – competitive market forces against traditional and structured staff model managed care companies – many industry analysts [like us] predicted growth would decline [Yes, greed was also involved as healthcare was presumed a recession-proof sector; and didn’t we all own behemoth big-pharma and HMO stocks in our 401-K, and 403-B plans]? But now, many former stock-brokers and FAs are going rogue; er – independent!
“Although inefficiencies in any business often open up in the short term, and can be greatly exploited by creative and visionary entrepreneurs – as in most business structures – market forces will prevail in the long run”.
Leo F. Mullin, MBA
[Former CEO – Delta Airlines]
Next-Gen with “Fly”
Fortunately, a new generation of enlightened physician and FA entrepreneurs is coming “out-of-the-shadows” as new-wave web 2.0 corporations and RIAs are becoming more flexible, competitive and market responsive. Simultaneously, monolithic and collectivist political ideas keep trying to regulate the medical and financial services workplace with rules, regulations and contracts to control entire populations. Yet, in the new healthcare economy, this new generation of doctors and FAs with “fly,” is headed toward more competition; not less – with more collaboration with patients and clients – regaining self autonomy.
Physician and FA Advocates
Meanwhile, as medical professionals, FAs and patient advocates, we must all choose between staying flexible to ride out tough times – or – adopting a hard, brittle line that will crack under the pressure of competition. We know where we stand at the ME-P, do you?
Flexibility and Virtual Reality
In recent years, many large corporations and top-down business models were not market responsive and change was not inherent in their DNA. These traditional organizations represented a rigid or “used-to-be” mentality, not a flexible or “wanna-be”mindset; according to business columnist Alan Webber. Somefinancial advisory corporations, and today’s emerging health 2.0 initiatives, may possess the market nimbleness that cannot be recreated in a controlled or collectivist [nationalistic] environment. And so, going forward, it is not difficult to imagine the following new rules for the new financial and virtual medical ecosystem.
[A] Rule No. 1
Forget about “SEC suitability and FINRA rules”, large office suites, surgery centers, fancy equipment, larger hospitals and the bricks and mortar that comprised traditional medical practices or financial product delivery systems. One doctor or niche focused FA with a great idea, good bedside manners or competitive advantage, can outfox a slew of public servants, the AMA, SEC, ADA or FINRA “faux copy-cat examiners”, while still serving the public – and patients – and making money. It’s now a unit-of-one economy where “Me Inc.”, is the standard. Physicians and FAs must maneuver for advantages that boost their standing and credibility among patients, peers, payers, customers and clients. Examples include patient satisfaction surveys; outcomes research analysis, evidence-based-medicine, physician economics credentialing and true integrated fiduciary-focused financial planning.
However, we should also realize the power of networking, vertical integration and the establishment of virtual RIAs or medical practices, which come together to treat a patient, or help a client, and then disband when a successful outcome is achieved. Job security is earned with more successful outcomes; not necessarily a degree, automatic AUMs, certifications or onsite presence. In fact, some competition experts, like Shirley Svorny PhD, a professor of economics and chair of the Department of Economics at California State University, wonder if a medical degree is a barrier – rather than enabler – of affordable healthcare.
Others even presume the establishment of virtual medical schools and hospitals, where students and doctors learn and practice their art on cyber-entities that look and feel like real patients, but are generated electronically through the wonders of virtual reality units. The same can be said for the financial services industry, although much farther down-line given its current slow rate of real education and quasi-professional acceptance.
[B] Rule No. 2
Challenge conventional wisdom, think outside the traditional box, recapture your dreams and ambitions, disregard conventional gurus and work harder than you have ever worked before. Remember the old saying, “if everyone is thinking alike, then nobody is thinking”. Do collective-nistas and nationalized healthcare advocates react rationally; or irrationally? [THINK: Wall Street, medical unions]
[C] Rule No 3
Differentiateyourself among your healthcare and financial advisory peers. Do or learn something new and unknown by your competitors. Market your accomplishments and let the world know. Be a non-conformist. Conformity is an operational standardand a straitjacket on creativity. Doctors and FAs should create and innovate, not blindly follow organization or political “union” leaders [shop stewards, BDs, etc] into oblivion.
[D] Rule No 4
Realize that the present situation is not necessarily the future. Attempt to see the future and discern your place in it. Master the art of the quick change with fast but informed decision making. Do what you love, disregard what you don’t, and let the fates have their way with you. Then, decide for yourself if you are of this ilk – and adhere to any of the above rules? Or, just become an employed [government, BD] doctor or FA shill. Just remember that the political party, or monopoly that can give you a job, can also take it away [THINK: LB, ML, Wachovia, national healthcare, etc].
Memorial Day Considerations
Finally, on this Memorial Day weekend, consider that life and career is a journey, and that in this country we have the choice to ponder or pursue any, and all of the above options, and more. We have the ability to think, cogitate and ruminate, as we have done here today. So – please – thank those who have helped turn this idealistic philosophy, into pragmatic daily reality.
For us personally, we thank Bonze Star Medal Winner Captain Cecelia T. Perez, RN. Now – ponder and consider – who do you thank? If no one has impacted you up-close on this Memorial Day weekend and national holiday, please visit our military channel to reflect, comment and opine.
And so, your thoughts and comments on this Medical Executive-Post are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com or Bio: www.stpub.com/pubs/authors/MARCINKO.htm
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
A new-wave West-Coast managed care organization (MCO) wanted a multi-specialty medical group to contract with them to provide medical services to all subscribers. Compensation would be in the form of a fixed-rate capitated payment system, a.k.a. per member / per month (PM/PM).
Ask an Advisor
The medical group practice administrator reviewed their request for proposal (RFP) very carefully, but is still not sure what to do. So, allow us to “crowd-source” as we ask ME-P readers, advisors and management consultants for a solution.
Key Issues
Facts to know for an informed PM/PM capitated reimbursement decision:
annual frequency or service-rate per 1,000 patients
unit cost of medical services per unit-patient
co-payment dollar amount per patient
co-payment frequency rate per 1,000 patients
variable cost per patient
under-capacity medical group office utilization rates, and
And so, your thoughts and comments on this ME-P are appreciated. What is your solution; accept or reject the contract proposal? Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe. It is fast, free and secure.
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on April 9, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
The Impact of Health Care Reform
[By Christopher de Garay]
Please find attached below, the Early April 2010 edition of Plan Management Navigator.
Link: Navigator April 2010
Review
In this month’s edition, we review how health care reform will impact the top line of plans offering government managed care programs such as Medicare Advantage and Medicaid. Combined with new minimum health benefit ratios, these pressures will force health plans to look at their administrative expenses. In the next several issues of Navigator, we will look at specific operational metrics and their impact on functional areas such as claims processing.
2010 Benchmark Studies
This edition of Navigator also summarizes the timing for the 2010 benchmarking studies, which includes a new Third-Party Administrator universe.
Christopher de Garay
Senior Health Care Analyst
Sherlock Company www.sherlockco.com 215-628-2289 Phone
215-542-0690 Fax cgaray@sherlockco.com P.O. Box 413
Gwynedd, PA 19436
Editor’s
If your plan would like to consider participation, we invite you to give Chris a call at 215-628-2289 or email him at sherlock@sherlockco.com.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on March 1, 2010 by Dr. David Edward Marcinko MBA MEd CMP™
ADVERTISEMENT
Events-Planner: MARCH 2010
By Staff Writers
“Keeping track of important health economics and financial industry meetings, conferences and summits”
Welcome to this issue of the Medical Executive-Post and our Events-Planner. It contains the latest information on conferences, news, and relevant resources in healthcare finance, economics, research and development, business management, pharmaceutical pricing, and physician/entity reimbursement! Watch for a new Events-Planner each month.
First, a little about us! The MedicalExecutive-Post is still a relative newcomer. But today, we have almost 17,500 visitors and readers each month from all over the country, in addition to our growing subscriber base. We have been a successful collaborative effort, thanks to your contributions. As a result, we are adding new resources daily. And, we hope the website continues to provide the best place to go for journals, books, conferences, educational resources, tools, and other things you need to establish the value your healthcare consulting and financial advisory intervention. And so, enjoy the MedicalExecutive-Post and our monthly Events-Planner with our compliments.
A Look Ahead this Month
March 1: Print Edition Healthcare Journalism: If you would like to “step-up-your-game” and be considered as a peer-reviewed contributor to the third print edition of: The Business of Medical Practice [Health 2.0 Profit Maximizing Techniques for Savvy Doctors]; contact Ann at: MarcinkoAdvisors@msn.com. There are several chapter topics still available. Now, the important dates:
March 1-4: HIMSS-10 Conference, Atlanta, GA
March 4-5: Medicare RAC Summit, Washington, DC
March 6-9: BISA Annual Convention, Westin Diplomat, Hollywood, FLA
March 7-9: ABA Wealth Management and Trust Conference, Biltmore, AZ
March 11: Health Plan Innovations Conference, Orlando, FLA
March 13: AORN Congress, Denver, CO
March 14: Health Facility Planning, San Diego, CA
March 25: World Healthcare Congress on HI-TECH, Washington, DC
March 29: HIT and the Future of Managed Care Industry Forum, NY
Please send in your meetings and dates for listing in the next issue of our ME-P Events-Planner: MarcinkoAdvisors@msn.com
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest E-Ps delivered to your email box each morning? Just subscribe using the link below. It’s free. You can unsubscribe at any time. Security is assured.
Posted on December 31, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
How Doctors Get Paid
By Dr. David Edward Marcinko; MBA, CMP™
[Publisher-in-Chief]
Just before the Christmas Holidays, I flew up to Boston at the invitation of a pharmaceutical company to lead a managerial workshop entitled: “How Doctors Get Paid” [Treatment is only the beginning in the Changing Billing and Medical Reimbursement Climate].
Our goal was to inform drug representatives, and their regional managers, what value added information physician offices might expect from the pharmaceutical industry of the future.
Topics of Discussion
The two hour interactive workshop included team projects, flip chart exercises, a mock role-playing session and the customary [hopefully energetic] ppt presentation. Other topics of discussion included:
Health insurance payment evolution
Collapse of Medicare
Rise of managed care
Medical records documentation
ICD-9 and 10, HCPCS, DRGs and CPT® coding
ABNs, super-bills and HCFA 150 forms
Billing methodologies
Healthcare fraud, abuse and related policies
Capitation, HSAs, concierge medicine and RACs
Futuristic health 2.0 payment mechanisms, and more.
Assessment
Rest assured; these folks were a very knowledgeable and aggressive group; not like your father’s “detail men” of yore! They seek to … talk the talk, and walk the walk, of the Health 2.0 era.
Many thanks again to Helen, and Jon D, for the invite.
Channel Surfing
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on September 14, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
Illustrative Case Model – Are You CMP™ Worthy?
By Staff Reporters
The Hope Outreach Medical Clinic (HOMC) is a private, for-profit, single specialty medical clinic in a south-eastern state. It submitted its bi-annual Request for Proposal (RFP) to continue its current managed care fixed-rate contract. Upon review of the RFP, however, Sunshine Indemnity Insurance Company, the managed care organization (MCO), denied the contract request for the upcoming year.
Seeing Economic Estimates
In shock, the clinic’s CEO asked the clinic’s administrator to work with its legal team to develop a defensible estimate of economic damages that would occur as a result of the lost contract. The clinic intended to bring suit against the MCO for breach-of-contract. However, the administrator is not an attorney and is loathe to-enter the fray. After consideration however, he decided to assist in filing the Statement of Claim (SOC) because he realized that changes in patient services (unit) volume would be a valid economic surrogate. He then requested the following information from his controller, in order to develop a change in economic profit [damages] estimate.
Change in patient visits (unit) volume
Fees (price) per patient (unit)
Marginal (incremental) cost per patient (unit)
Change in current fees (prices)
Patient volume (units) affected
Key Issues:
Fee (price) per patient (units) may be obtained from the fee schedule used by the MCO to pay HOMC.
Marginal (incremental) costs per patient (unit) are approximated using variable costs.
Higher cost payors exist because lower patient volumes raise the average cost per patient (unit) due to existing fixed costs.
Assessment
Medical management consultants, are you up to answering this challenge? We dare you to respond!
And so, your thoughts and comments on this Medical Executive-Post are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Posted on September 14, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
It’s the Government – Silly
By Ann Miller; RN, MHA
[Executive Director]
By far, our federal government is the largest purchaser of healthcare services, according to Robert James Cimasi MHA, AVA, CMP™ of Health Capital Consultants, in St. Louis, MO; and many others.
Obama Care
Although the government faces immense pressure to control healthcare costs, especially during the current HR 3200-3400 debates, it also faces pressure to expend additional funds in order to achieve its ostensible primary mission in its involvement in healthcare, i.e., to expand and improve public health.
Federal Payment Schemes
In many ways the government has led the way for cost control through its development of resource-based reimbursement, prospective payment systems, budget limitations and other payment schemes. However, its conflicting goals have led it to approach these controls in a hesitant and piecemeal manner rather than effecting bold, comprehensive reforms.
Consider, for example, the lack of government intervention in the face of mounting pressure to remove some of the barriers preventing a reduction in US pharmaceutical costs.
Assessment
Today, most experts agree that Uncle Sam pays for at least 51% of domestic healthcare when Medicare, Medicaid, SHIPS, the VA, Indian and Prison Healthcare Systems are considered. In fact, according to our Publisher-in-Chief, Dr. David Edward Marcinko; MBA:
‘We already have a single payer health system in this country, but most folks just don’t realize it.”
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on August 8, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
ADVERTISEMENT
Whither the Dictionary of Health Insurance and Managed Care?
A simple query that demands a cogent answer!
Why do we need the Dictionary of Health Insurance and Managed Care, and, why do payers, providers, benefits managers, consultants, and consumers need a credible and unbiased source of explanations for their health insurance needs and managed care products?
The Answer is Clear!
Health care is the most rapidly changing domestic industry. The revolution occurring in health insurance and managed care delivery is particularly fast. Some might even suggest these machinations were malignant, as many industry segments, professionals, and patients suffer because of them. And so, because knowledge is power in times of great flux, codified information protects all people from physical, as well as economic harm.
We appreciate the support of our sponsors. So, click-on on the links and review all dictionary products.
Subscribe Now: Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
The changes in reimbursement for Medicare services through the introduction of prospective payment systems and physician reimbursement cuts for professional services, as well as the increased focus on patient quality and transparency initiatives and health 2.0 collaboration have forced healthcare providers to look for more efficient ways to provide services, as well as additional sources of revenue and margin-producing business.
Additionally, with the rise of corporate healthcare provider networks and health systems, together with rising healthcare costs, competition among providers has become prevalent in the healthcare industry.
Assessment
Strict control of reimbursement costs from payers and consistent decreases in physician professional component fee reimbursement yields; reduction in traditional hospital inpatient use; and higher costs of capital have all contributed to the trend of physician investment in outpatient (and inpatient) specialty provider enterprises [ASCs, specialty hospitals and clinics, etc] , which often compete with general acute care community hospital providers.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on April 24, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
ADVERTISEMENT
Plan Management Navigator
By Marco Georeno
Ph: 215-628-2289
Please find attached the April 2009 edition of Plan Management Navigator. In it we provide an update on the timing of the Blue Cross Blue Shield universe and the Independent / Provider-Sponsored editions of the Sherlock Expense Evaluation Report (SEER). In addition, we expect to circulate the benchmarking surveys for the Medicaid and Medicare universes on or about June 1st, for completion by July 20th, 2009.
Benchmarking Studies
If you are interested in participating in our benchmarking studies please contact us as soon as possible. Additional information about SEER is available at www.sherlockco.com/seer.shtml or by contacting Doug Sherlock (sherlock@sherlockco.com).
Best Practices for the Healthcare Enterprise
We also endeavor to provide an enterprise view of best practice. Best practice is typically considered to be the most efficient way of achieving a desired outcome. We believe that the best way of determining the best practice in its most practical application is to start with an overall objective and weigh all particular practices in light of how they contribute to that overall objective.
In that vein, over the next several months, Sherlock Company will be offering web conferences focused on best practices. The first conference will address activities within Customer Services, as well as activities or effects in other functional areas. This web conference will be held on Wednesday May 20th at 2:30 PM, Eastern Time. The costs will be $225. Participation is free of charge to health plans participating in our 2009 benchmarking studies. If you are interested in participating, please email Erin Sawchuk (erinsawchuk@sherlockco.com) or call at 215-628-2289.
Assessment
This edition of Navigator also discusses the latest private health plan Dashboard results for the trailing three months ended January 31, 2009.
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.comor Bio: www.stpub.com/pubs/authors/MARCINKO.htm
Subscribe Now:Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
An HMO is a legal corporation that offers health insurance and medical care. It is a health care delivery system that provides comprehensive services for subscribing members in a particular geographic area. Most HMO care is provided through a managed network made up of MD/DOs, hospitals, and other allopathic/osteopathic professionals selected by the HMO. HMO enrollees are required to obtain care from this network of providers in order for their care to be covered, except in cases of emergency. All the care the members may need is paid for by the single monthly fee, plus nominal co-payments. HMOs typically offer a range of health care services at a fixed price (capitation).
Different Types
The types of HMOs are:
1. STAFF MODEL: Organization owns its clinics and employs its doctors.
2. GROUP MODEL: Contract with medical groups for services.
3. INDEPENDENT PHYSICIAN ASSOCIATION (IPA) MODEL: IPA contract that in turn contracts with individual physicians.
4. DIRECT CONTRACT or NETWORK MODEL: Contracts directly with individual physicians.
5. MIXED MODEL: Members get options ranging from staff to IPA models.
6. OPEN-PANEL MODEL: A managed care plan or HMO where members can see any provider for an extra premium cost.
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.comor Bio: www.stpub.com/pubs/authors/MARCINKO.htm
Subscribe Now:Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on April 13, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
An Emerging Health Economics Issue
By Staff Reporters
Comparative Medical Effectiveness [CME] is not a new healthcare term or health economics concept. Federal initiatives specifically promoting CME were authorized under the Medicare Modernization Act of 2003, but the genesis took root decades before.
Finally … a Hot Topic
Comparative Medical Effectiveness has recently become a hot topic again throughout the arena of health care stakeholders, due to funding and initiatives advanced by the Obama administration, and the positive and negative reactions drawn by different sectors of stakeholders.
Related to Evidence Based Outcomes
For stakeholders including numerous health care policy organizations, the health plan industry, and various health care provider organizations: public and private promotion of Comparative Medical Effectiveness reviews and processes offer the potential for more evidence-based, outcome-benefit or even cost-benefit driven information to improve the health care decision making for all parties. And, for stakeholders concerned about limiting the role of government and third parties in their level of regulation and control over the direct delivery of specific patient care, Comparative Medical Effectiveness may become a lightening rod due to perceived potential as to how the process and information could ultimately be applied.
Definition of the CBO Report
The Congressional Budget Office Report “Comparative Effectiveness: Issues and Options for an Expanded Federal Role” offers the definition that follows:
“As applied in the health care sector, an analysis of comparative medical effectiveness is simply a rigorous evaluation of the impact of different options that are available for treating a given medical condition for a particular set of patients. Such a study may compare similar treatments, such as competing drugs, or it may analyze very different approaches, such as surgery and drug therapy. The analysis may focus only on the relative medical benefits and risks of each option, or it may also weigh both the costs and the benefits of those options. In some cases, a given treatment may prove to be more effective clinically or more cost-effective for a broad range of patients, but frequently a key issue is determining which specific types of patients would benefit most from it. Related terms include cost–benefit analysis, technology assessment, and evidence-based medicine, although the latter concepts do not ordinarily take costs into account.”
Assessment
For related financial, economics, managed-care, insurance, health information technology and security, and health administrative terms and definitions of modernity, visit: http://www.springerpub.com/Search/marcinko
Conclusion
And so, your thoughts and comments on this Medical Executive-Post are appreciated. How do you define this term, and is its’ very definition evolving?
Posted on April 3, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
Delta Dental Sends More Easy Prey My Way
By Darrell K. Pruitt; DDS
When it comes to blindsiding witless PR departments, what good is Schadenfreude if it can’t be shared for the entertainment of my large collection of quirky, unshaven sports fans – a special class of readers who would stick around to watch the sequelae of an ignited paper bag on a front porch … even if from a safe distance.
Devoted and Abandoned Employees
The rumor is, watching PR professionals silently vanish from the Internet is becoming a popular spectator sport – especially when it’s the more expensive hacks for sleazy discount dental companies like Delta Dental. I intend to show you that when someone writes really nasty things about their most devoted employees – employees who publicly donate their name and reputation to Internet branding for the interests of Delta Dental – Delta Dental will still not come to their defense (No wagering, please). The devoted and abandoned, whose objectives in life are to take hits for some team, make easy prey.
Thinking of Ari Adler
Remember Ari Adler? He heads Delta’s Corporate and Public Affairs division, and was quoted in DrBicuspid Assistant Editor Rabia Mughal’s article, “Dentists or patients: Who should get the insurance check?”
It was on DrBicuspid that Adler broke the news to the nation that Delta Dental now guarantees the fillings done by their preferred providers. When confronted by a special bastard to explain Delta’s unprecedented sales pitch, Adler immediately sat his butt down and shut up. (See “I will hurt you Delta Dental”)
That was two months ago, and Adler still hasn’t uttered another peep on behalf of Delta Dental. Now doesn’t that make the air in the land of the free just a little more pleasant? And yesterday, Rabia Mughal posted another article illustrating managed care dentistry’s level of ethics titled “Study: Insurers’ market power lowers dentists’ income.”
Mughal describes the findings of a study titled “The effects of insurance carrier market power on dentists and patients” that appeared in the January edition of the JADA. Here is the abstract of the study:
The effects of insurance carrier market power on dentists and patients
By L. Jackson Brown; DDS, PhD
By Albert H. Guay; DMD
By Donald R. House; PhD
Background
Market power among dental insurance carriers is a carrier’s ability to reimburse dentists at rates below what would exist in more competitive areas. Competition among carriers for dentists’ participation in their networks protects dentists from highly discounted fees. The authors examined the extent to which dental insurance carriers facing less competition increase fee discounts.
Methods
The authors selected a sample of dentists from listings of general practitioners. They identified 219 metropolitan areas and contacted 11,542 dentists in those areas by mail, telephone or both. A total of 8,017 dentists completed surveys (a response rate of 69.46 percent). The authors’ key focus was the possible relationship between carrier market power and the size of the fee discount. The authors compared discounts across metropolitan areas with their differing levels of insurance coverage and carrier market shares.
Results
Carrier market power was directly related to the sizes of fee discounts. The larger discounts were found where there was significant dental insurance coverage and few carriers providing this coverage. Dentists’ net incomes were significantly less in areas with larger fee discounts.
Conclusions and Practice Implications
Dental insurance carrier market power leads to increased fee discounts. These higher discounts reduce dentists’ earnings. Although the larger discounts may result in lower overall patient costs, this patient benefit is temporary. Ultimately, the number of practicing dentists in these communities will decrease as dentists seek improved practicing conditions elsewhere. This reduction will lead to overall fee increases until the earning potential of dentists is restored.
Abbreviations: IPAs: Independent practice associations. • PPO: Preferred provider organization. • UCR: Usual, customary and reasonable.
####################
As one can imagine, Delta Dental, the largest dental discount service in America, did not like what both the ADA study and Mughal had to say about discount dentistry brokers. This time though, instead of sending Ari Adler into the wide open spaces once more, Delta sacrificed a new, unsuspecting traditional-type of PR executive whose feelings have never been hurt. Her name is Janis Oshensky, and she is the vice president of professional relations for Delta Dental Plans Association.
Enter Again Ms. Janis Oshensky
Ms. Oshensky confidently said that it is her opinion that the study is flawed. Here is what Ms. Oshensky told Mughal:
“The study speculates that dentists will leave markets dominated by a few large carriers, which would lead to higher fees for uninsured patients and reduced access to care. In fact, the miniscule effect of concentration on the fees paid to dentists — as they are reported in the study — is unlikely to trigger a mass exodus of dentists from concentrated areas.”
Ms. Oshensky further states – on dentists’ behalf – that we actually realize that discounts do not necessarily mean less pay, and that network participation increases dental visits (for the same pay). Now that woman deserves a company wristwatch!
Devoted to Delta
To show you how devoted Oshensky is to Delta Dental, her act almost fooled me into believing that she believes the NPI number makes sense. That’s no joke. Look at what she posted on the Delta Dental Website celebrating Delta’s success, and you will see what I mean:
“Thanks to all of the dentists and health professionals who have applied for NPIs and who have notified us of their new identifiers. While we’re not ready to completely replace the current identifiers with NPIs, we’re making great progress and will work to keep dentists and their office staff informed about our NPI readiness.”
Now that’s talent. I would imagine that she probably charges more than Adler ever will. Her name is all over the Internet on behalf of Delta Dental, and she sounds even more enthusiastic about the NPI number than Patrick Cannady of the ADA Department of Dental Informatics did a couple of years ago when his department was still telling ADA members to quickly volunteer for the ten digit identifier. You know, come to think of it, Delta Dental’s Website closely resembles the ADA’s. How do you think that happened?
Re-Enter Rabia Mughal
My hat goes off to author Rabia Mughal. How he can successfully lure another Delta Dental slow-mover into the open following the ambush of Ari Adler is pure genius in a mis-match of wits.
Assessment
So here we go again, sports fans. Come on out, Janis Oshensky, I can make you famous. Please bring everything you know about the NPI number with you as well because I have a few questions to ask … or not. Schadenfreude macht Freude.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on April 1, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
ADVERTISEMENT
Events-Planner: APRIL 2009
Staff Writers
“Keeping track of important health economics and financial industry meetings, conferences and summits”
Welcome to this issue of the Medical Executive-Post and our Events-Planner. It contains the latest information on conferences, news, and relevant resources in healthcare finance, economics, research and development, business management, pharmaceutical pricing, and physician/entity reimbursement! Watch for a new Events-Planner each month.
First, a little about us! The Executive-Post is still a newcomer. But today, we have almost 15,000 visitors and readers each month from all over the country, in addition to our growing subscriber base. We have been a successful collaborative effort, thanks to your contributions. As a result, we are adding new resources daily. And, we hope the website continues to provide the best place to go for journals, books, conferences, educational resources, tools, and other things you need to establish the value your healthcare consulting and financial advisory intervention. And so, enjoy the Executive-Post and our monthly Events-Planner with our compliments.
A Look Ahead this Month
April 1: Print Edition Healthcare Journalism: If you would like to “step-up-your-game” and be considered as a peer-reviewed contributor to the third print edition of: The Business of Medical Practice [Advanced Profit Maximizing Techniques for Savvy Doctors]; contact Ann at: MarcinkoAdvisors@msn.com. There are several chapter topics still available. Now, the important dates:
April 21-23: Introduction to Applied Health Economics: Methods for analysis of healthcare utilization and expenditure, University of York. April 23-25: AIP Conference on Philanthropy, Rosemont, Ill.
April 25-29:Society for Pain Practice Management Meeting, Phoenix, AZ.
April 26-29:Wound Healing Society Symposium, Dallas, TX.
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.comor Bio: www.stpub.com/pubs/authors/MARCINKO.htm
Subscribe Now:Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest E-Ps delivered to your email box each morning? Just subscribe using the link below. It’s free. You can unsubscribe at any time. Security is assured.
Posted on March 2, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
Introducing our Newest Thought-Leader
[By Ann Miller RN MHA]
The Medical Executive-Post is proud to introduce Dr. Gary L. Bode as our newest thought-leader for healthcare financial modernity. Dr. Bode was the Chief Financial Officer [CFO] for a private mental healthcare facility, and previously the Chief Executive Officer [CEO] of Comprehensive Practice Accounting, Inc, in Wilmington, NC. The firm specialized in providing tax solution to medical professionals. Dr. Bode was a board certified practitioner and managing partner of a multi-office medical group practice for a decade before earning his Master’s of Science degree in Accounting [MSA] from the University of North Carolina. He is a nationally known forensic health accountant, financial author, educator and speaker.
A Multi-Faceted Healthcare Financial Expert
Areas of expertise include producing customized managerial accounting reports, practice appraisals and valuations, restructurings and innovative financial accounting, as well as proactive tax positioning and tax return preparation for healthcare facilities. Currently, Dr. Bode is Chief Accounting and Valuation Officer (CAVO) for the Institute of Medical Business Advisors, Inc. He is also a Certified Medical Planner™ http://www.CertifiedMedicalPlanner.org He provides litigation support in his areas of expertise and has been previously accepted as a legal expert witness www.MedicalBusinessAdvisors.com
Assessment
Gary has promised to publish his most exciting ideas and innovative work on our blog. He is also available for private consulting engagements and related professional work on an ad-hoc, or interim basis. So, let’s give a warm ME-P “shout-out” to Dr. Gary L Bode; our newest thought-leader.
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
All hospitals, healthcare systems and organizations use a variety of teaching, educational and didactic techniques to bring value to patients, payers, providers, governments and third-party intermediaries.
Intellectual Capital
This intellectual capital is the sum total of all knowledge and expertise used to serve the healthcare industrial complex and its’ stakeholders. Leaders, CXOs, CEOs, CFO, managers, administrators and employees provide most all of this current cognitive capital.
Print Journal Guide
We believe that Healthcare Organizations:[Financial Management Strategies] adds to this intellectual capital by guiding you, empowering your organization, and creating value for your patients, employees, investors and clients by bridging the intersection of medical mission and profit margin.
Assessment
www.HealthcareFinancials.comseeks to “Bridge the Intersection of Medical Mission and Profit Margin”; using the aggregated free-labor knowledge of those in the industry. There is just no better method available.
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.comor Bio: www.stpub.com/pubs/authors/MARCINKO.htm
Subscribe Now:Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest E-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on February 9, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
The Most Important Medical Executive-Post Asset
By Hope Rachel Hetico; RN, MHA
Managing Editor
The Medical Executive-Post is a knowledge aggregator of user-generated content. It is a network where users share, recommend, rank and comment on professional submissions by experts and thought-leaders. We believe that better submissions, lead to better actionable knowledge and professional lives.
Great information can also help us do, become and experience the professional goals and accomplishments that make us happy and more successful. Our mission is to help people discover and use this deeply gratifying electronic and/or print content.
Content Broadcasting
Every Medical Executive-Post is submitted by members of our community. You send-in content and comments, and we rate the clicks as recommendations on this blog. We call this ranking process “content-broadcasting.” It increases your exposure and helps to establish and disseminate your uniquely professional brand-image. Your submit content, and we do the rest.
A Niche Industry
When you make a submission, click-on a post or make a comment, you are in-effect saying that you think the content is worth reading and spending time to review. You are answering the question, “What do I need to know and where can I find the answer“, for people who share your interests and passion in the healthcare industrial complex and related health economics and nice practice management space.
Built by Free-Labor Entrepreneurs
The Medical Executive-Post is a privately-funded Web 2.0 company. We are committed to improving the overall quality of deeply specific Internet content search experiences by offering this utility platform for professional user-generated content and recommendations. The Medical Executive-Post was initially built by a team of seasoned Internet entrepreneurs, editors, and bloggers. But you, our free-labor entrepreneurs and contributing authors are now our most important long-term survival asset. Thank you.
Assessment
To see what else we are up to; please visit our related websites, links, books and products on each side-bar. Learn how your bottom-up efforts – become valuable real-world print content.
Conclusion
And so, your thoughts and comments on this Medical Executive-Post are appreciated.
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.comor Bio: www.stpub.com/pubs/authors/MARCINKO.htm
Our Other Print Books and Related Information Sources:
Subscribe Now:Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest E-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on February 7, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
Transforming Home Health Care Services
Staff Reporters
According to its website, ENURGI is a revolutionary web-based healthcare services company that connects families and patients in need, with local clinical caregivers across the country.
Online Empowerment
ENURGI allows patients, family members and caregivers to independently manage the care process through on-line scheduling, messaging, referral and direct payment transactions.
A Caregiver Database
ENURGI’s goal is to transform the delivery of home health care services across the country. It is the first web-based company to aggregate and create a clinical caregiver database for families and patients in need of home health care to access and connect with.
Assessment
By harnessing the power of technology, ENURGI has accumulated over 1,000,000 clinicians within its caregiver database for families/patients in need to access when seeking a licensed clinician, certified nurses aide or home health aide.
And so, your thoughts and comments on this Medical Executive-Post are appreciated. Is this not the perfect post to conclude our four part series on: At Home or Nursing Home Care for Long Term Care? Opinions from physicians, medical case and geriatric care managers, and LTC insurance agents are especially valued.
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.comor Bio: www.stpub.com/pubs/authors/MARCINKO.htm
Our Other Print Books and Related Information Sources:
Subscribe Now:Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest E-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on February 2, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
A Coalition from the New America Foundation
Staff Reporters
Many pundits posit that real health reform will entail quality, affordable coverage for all Americans and a restructured health care delivery system. And, a growing number of health industry leaders understand they must reorganize their business models to realize these goals.
Health CEOs for Reform
Recognizing that business as usual is no longer a sustainable model in health care, a diverse coalition of six CEOs from across the health care sector have come together to form Health CEOs for Health Reform [HC4HR]. The coalition, facilitated by the New America Foundation, brings together health industry leaders with a unique willingness to transform their business models to create a more sustainable health system.
Guiding Principles
According the its website, the group’s members are committed to moving past broad policy concepts toward detailed blueprints that reconcile the legislative goals and principles of lawmakers with the operational realities of our health care system. The coalition is built on the following three principles:
Health reform is an urgent priority for our nation and should not be postponed.
Meaningful health reform entails quality, affordable health coverage for all and delivery system reform. This will require all stakeholders to move away from “business as usual.”
A more sustainable health system will require all health care stakeholders to offer and accept changes to their business models as part of a catalytic package that will better serve everyone.
Assessment
The CEOs announced the formation of HC4HR in an event at the National Press Club. Senator Sheldon Whitehouse [D-RI] provided a Congressional keynote for the event, stressing the importance of health reform in our national agenda and applauding the leadership shown by HC4HR.
And so, your thoughts and comments on this Medical Executive-Post are appreciated. Do we really need another group to discuss healthcare reform? We all know the problems of divergent stakeholder interest. Is this the time for solutions, or another group reframing the problem?
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com or Bio: www.stpub.com/pubs/authors/MARCINKO.htm
Subscribe Now:Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest ME-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.
Posted on January 13, 2009 by Dr. David Edward Marcinko MBA MEd CMP™
Understanding Disproportional Influence
By Dr. David Edward Marcinko; MBA,
Most domestic health care is paid for by some type of insurance, whether private or governmental. Most private health insurance is purchased through employers who, to a great degree, make most of the buying decisions. Employer coalitions have emerged but, in general, most command leverage on price rather than quality or value. This often leaves healthcare providers as the only advocates for the quality, choice and access concerns of consumers.
Business Impact
According to Robert James Cimasi, writing and opining in the print journal: Healthcare Organizations [Financial Management Strateges] www.HealthCareFinancials.com, despite the fact that businesses bear less of the total U.S. healthcare premium dollar (approximately 25%) than government or individuals; corporate buyers and their coalitions and associations have asserted substantial, if disproportionate, influence over healthcare companies.
Best Community Interest Debate
Whether or not this is necessarily always in the best interests of consumers or the community at large is a matter of heated debate. What is generally acknowledged is that the relative bargaining position of buyers and providers in a given market has a dramatic impact on healthcare provider financial performance.
Healthcare is Different
Much like F. Scott Fitzgerald’s different-rich; keep in mind that healthcare differs in several respects from other industry sectors, in that:
There is more than one class of buyers: there are patients, families (proxies), insurance companies, and employers, each with different objectives.
The single largest payer, the government, both dictates a large portion of the healthcare pricing structure and strongly influences the rest.
There is a crucial divide or (“disconnect”) between consumer and payer.
A lack of information regarding consumer needs and quality of providers impedes the purchasers of health insurance from selecting the optimal plan.
Assessment
Of course, the impact of the Obama administration on this topic has yet to be seen.
Conclusion
And so, your thoughts and comments on this Medical Executive-Post are appreciated. Is this commercial influence on health insurance good or bad; please share your experiences with us.
Speaker:If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.comor Bio: www.stpub.com/pubs/authors/MARCINKO.htm
Our Other Print Books and Related Information Sources:
Subscribe Now:Did you like this Medical Executive-Post, or find it helpful, interesting and informative? Want to get the latest E-Ps delivered to your email box each morning? Just subscribe using the link below. You can unsubscribe at any time. Security is assured.