BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Offering a blend of active and passive styles of management, a smart beta portfolio is low cost due to the systematic nature of its core philosophy – achieving efficiency by way of tracking an underlying index (e.g., MSCI World Ex US). Combining with optimization techniques traditionally used by active managers, the strategy aims at risk/return potentials that are more attractive than a plain vanilla active or passive product.
Originally theorized by Harry Markowitz in his work on Modern Portfolio Theory (MPT), smart beta is a response to a question that forms the basis of MPT – how to best construct the optimally diversified portfolio. Smart beta answers this by allowing a portfolio to expand on the efficient frontier (post-cost) of active and passive. As a typical investor owns both the active and index fund, most would benefit from adding smart beta exposure to their portfolio in addition to their existing allocations.
Assessment: The smart beta approach is an arguably perfect intersection between traditional value investing and the efficient market hypothesis. But, is it worth the cost?
According to the National Institute on Retirement Security, almost 40 million households have no retirement savings at all. The Employee Benefit Research Institute (EBRI) estimates in its 2019 Retirement Security Projection Model that America’s current retirement savings deficit is $3.8 trillion.
What does that mean? Well, the EBRI report aggregates the savings deficit of all U.S. households headed by someone between the ages of 35 and 64, inclusive. In total, those households have $3.8 trillion fewer dollars in savings than they should have for retirement.
For more recent data, Fidelity Investments reported that in the third quarter of 2022 the average account balance for an IRA was $101,900. Employees with a 401(k) averaged $97,200, while those with a 403(b) had $87,400.
Fidelity also estimated that “an average retired couple age 65 in 2022 may need approximately $315,000 saved (after tax) to cover health care expenses in retirement.” Keeping in mind that more Americans are also living longer than ever before, they will face more challenges to cover medical expenses in retirement.
Posted on October 17, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David E. Marcinko MBAMEd CMP
SWARM INTELLIGENCE IN MEDICINE
***
Warm Learning or Swarm Intelligence, is how swarms of bees or birds move in response to their environment.
When applied to data there is “more peer-to-peer communications, more peer-to-peer collaboration, more peer-to-peer learning and that’s the reason why swarm learning will become more and more important as … as the center of gravity shifts” from centralized to decentralized data.
Medicine Example:
Consider this example, “A hospital trains their machine learning models on chest X-rays and sees a lot of tuberculosis cases, but very little of lung collapsed cases. So therefore, this neural network model, when trained, will be very sensitive to what’s detecting tuberculosis and less sensitive towards detecting lung collapse.”
“However, we get the converse of it in another hospital. So what you really want is to have these two hospitals combine their data so that the resulting neural network model can predict both situations better. But since you can’t share that data, swarm learning comes in to help reduce that bias of both the hospitals.”
And this means, “each hospital is able to predict outcomes, with accuracy and with reduced bias, as though you have collected all the patient data globally in one place and learned from it.”
Moreover, it’s not just hospital and patient data that must be kept secure. What swarm learning does is to try to avoid or reduce the sharing of data, or totally prevent the sharing of data, to [a model] where you only share the insights, or you share the learnings.
The science of the modern medical practice valuation can be traced to the Estate of Edgar A. Berg v. Commissioner (T. C. Memo 1991-279). In this case, the Court criticized CPAs as not being qualified to perform business valuations, failing to provide analysis of an appropriate discount rates, and making only general references to justify their “Opinion of Value.”
In rejecting accountants, the Court accepted IRS economists because of background, education and training, as well as discount rate calculations and reproducible evidence applied to the assets being examined. This marked the beginning of the Tax Court leaning toward the side with the most comprehensive appraisal. Previously, it had a tendency to “split the difference.” Now, some feel the Berg case launched the valuation profession; especially for contemporaneous health economists.
But, it was not until after 1995 that the IRS issued guidelines for the valuation of physician practices. As a result, the Uniform Standards of Professional Appraisal Practice [USPAP] requires that a blended constellation of three recognized valuation approaches (income, market, and cost approaches) be considered when estimating fair market value.
Operative Valuation Definitions
When pursuing any discussion of medical practice worth, two key elements must be understood: (1) the valuation process, and (2) fair market value. According to the Dictionary of Health Economics and Finance
Practice valuation is the “the formal process of determining the worth of a healthcare or other medical business entity, at a specific point in time, and the act or process of determining fair market value.”
Fair market value [FMV] is “a legal term generally meaning the price at which a willing buyer will buy, and a willing seller will sell an asset in an open free market with full disclosure.” IRS Revenue Ruling 59-60 clearly states that FMV “is essentially a future prophesy and must be based on facts available at the required date of appraisal”
Unfortunately, the value of a medical practice cannot be directly observed by activity in thinly traded private markets. Perhaps this is why we continually observe the following valuation blunders? They are committed by both sellers and buyers who are pursuing opposite objectives; sale price maximization versus price minimization?
Top 10 Blunders:
Not Understanding What a Medical Practice Valuation Is and Is Not
Valuations are not source document fraud audits.
Valuations are material representations providing a range of transferable worth.
Valuations are reproducible estimates based on economic assumptions.
Valuations are not “back-of-the envelope multiples” using specious benchmarks.
Valuations are defensible and “signed-off” attesting to USPAP/IRS formats.
Financial accounting value [book-value] is not fair market value.
Professional valuators represent only one party at arm’s length; not both sides.
Engagement solicitor and/or valuation payer is the client.
Unbiased valuators do not provide financing or equity-participation schemes. Although not standardized, the Institute of Medical Business Advisors, Inc uses the following three levels that approximate engagement types for the industry.
2. A Limited Valuation lacks additional suggested USPAP procedures. It is considered an “agreed-upon-procedure”, used in circumstances where the client is the only user [i.e., updating a buy-sell agreement, or practice buy-in for a valued associate] and not for external purposes. No onsite visit is needed. A formal Opinion of Value is not rendered.
3. Not Observing Industry Standards, Rules and Regulations
Specifically, in USPAP transactions involving physician practices, the IRS implied:
Ad-Hoc Valuation is low level engagement that provides a gross and non-specific approximation of value based on limited meters by involved parties. Neither a written report, nor an Opinion of Value is rendered. It is often used periodically as an internal organic growth / decline gauge.
A Comprehensive Valuation is an extensive service designed to provide an unambiguous Opinion of Value range. It is supported by all procedures that valuators deem relevant with mandatory onsite review. This “gold-standard” is suitable for contentious situations like divorce, partnership dissolution, estate planning and gifting, etc. The written Opinion of Value is applicable for litigation support activities like depositions and trial. It is also useful for external reporting to bankers, investors, the public and IRS, etc.
4. Not Understanding Engagement Types and Levels
Discounted cash flow (DCF) analysis is the most relevant income approach and must be done on an “after-tax” basis.
Practice collections must be projected based on reasonable assumptions for the practice and market; etc.
Physician compensation must be based on market rates consistent with age, experience and productivity.
Majority premiums and minority discounts are to be considered.Goodwill represents the difference between practice purchase price and the value of the net assets. Personal goodwill results from the charisma, skills and reputation of a specific doctor. Its attributes accrue solely to the individual, are not transferable and can’t be sold. It has little or no economic value as it “goes to the grave” with the doctor. Transferable medical practice goodwill has value, may be transferred, and is defined as the unidentified residual attributes that contribute to the propensity of patients and managed care contracts (and their revenue streams) to return in the future (Schilbach v. Commissioner, T.C. Memo 1991-556). And so, one must also appreciate the: (i) impact of a changing environment; (ii) practice transfer in a local market which can augment or blunt goodwill value; and the (iii) determination of whether patients or HMOs return because of true goodwill, or are mandated by contractual obligations; among many other multi-variable determinants.
Even the Goodwill Registry however, a classic source used to determine the average percentage of revenue contributed to practice goodwill, may be dated for some specialties leading to abnormally high values.
5. Not Understanding the Value of Practice Goodwill: Unlimited life span.
6. Not Understanding the Value of Personal Goodwill: Limited life span.
Now, to further confuse the issue, how each kind of goodwill is allocated in situations like divorce depends on state law. For example, some courts include both kinds of goodwill to be apportioned – some exclude both – and others pursue a case-by-case approach.
7. Not Understanding “Excess Earnings Capitalization”
Another way to determine goodwill value is through “excess earnings capitalization.” This economic method looks at the difference between salary, and what you’d have to pay a comparable doctor replacement.
As an example, when you subtract the numbers, and divide the result by 20%, an important percentage referred to as the Capitalization Rate emerges. The final number gives a dollar value for practice goodwill. Courts seem to prefer this method in divorces because it tends to reflect a practice’s current value.
8. Not Understanding the Present Compensation versus Future Value Paradox
Regardless of practice business model, physician compensation is inversely related to practice value. In other words, the more a doctor takes home in above-average salary, the less the practice is generally worth, and vice versa; ceteris paribus
9. Substituting Benchmarks and Formulas for Practice Specificity
In the stable economic past, industry benchmarks might have been used as quick and inexpensive substitutes for professionally prepared valuations. Muck like preparing one’s own income tax return today – while legal – it is a fraught with peril if challenged. The Courts seem to frown on this simplistic and dated methodology.
Moreover, generic benchmark formulas assume a financial statement reporting standard that just does not exist in public accounting.
Therefore, most every competitive issue that impacts value should be addressed with each practice engagement. This includes, but is not limited to contemporary dislocations by third parties, Medicare and commercial payers; retail clinics and changes in supply/demand and specialty trends; rise of ambulatory surgery centers and specialty hospitals; outsourced care and medical tourism, alterations in resource based-relative value units, APCs, DRGs and newer MS-DRGs; the Medicare Modernization Act, HIPAA, OSHA, EEOC, Sarbanes-Oxley and US Patriot Acts, PP-CA, and ACOs; among other regulations.
Current employee trends to high-deductible health care plans [HD-HCPs] and private concierge medicine must also be considered, as well as demographic and employer shifts to defined contribution plans – from defined benefits plans – to name just a few more complicating issues.
10. Not Aggregating or “Normalizing” Financial Information
Employees may be interviewed and financial information must be gathered before a medical practice can be properly valued. The following data, for the most recent three year period, serves as a starting point:
Sample medical record chart review is increasingly being demanded.
It is especially important to eliminate one-time, non-recurring practice expenses. These are adjusted for excessive or below normal expenses on the profit and loss statement. Such “normalization” can produce a big surprise for benchmark proponents and formula-driven advocates when a selling doctor runs personal expenditures through the practice that a buyer [or Court] wouldn’t consider legitimate. Of course, such shenanigans are less noted using professional USPAP/IRS guidelines. Conversely, you may have to defend legitimate business expenses that an appraiser may seek to normalize. For example, doctors may pay for a vehicle through their practice, but if used to travel between multiple offices and hospitals, the expense may be legitimate. Of course, normalization is a sophisticated and time-intensive process. But, it is where the expert earns his/her professional fee, and defends the resulting valuation range when challenged.The most important credential to look for is fiduciary experience, specificity and independence. Some doctors mistakenly turn to those who may have never appraised a practice before. And, just because an appraiser has initials behind his name, doesn’t mean he understands the peculiarities of medical specialties, especially podiatry. We believe that only an independent health economist, who will be your advocate under Securities Exchange Commission [SEC] fiduciary [not lower “suitability”] guidelines, should be selected. Of course, it is almost impossible to answer concerns regarding fees without specific information. The cost of a valuation can range from $0 (benchmarks-rule of thumb) to $50,000 for an onsite team of experts for behemoth practices and ambulatory surgery centers. Keep in mind that in most cases you want to ensure the value determination will stand up to IRS scrutiny, so the $0 rule-of-thumb is not an optionExternal appraisals, or poorly aggregated financial information, onsite reviews and litigation support services incur additional costs; yet most doctors find the money well spent. Expect to pay a retainer and sign a formal professional engagement letter.
Assessment
Don’t be surprised if a sales-broker does not consider the above issues as the modern health era emerges. Most agent-appraisers are predominantly concerned with earning commissions by working both transaction parties, and may not represent your best interests. And, they are usually not obliged to disclose conflicts-of-interest and don’t provide legal testimony.
As a result, a good medical practice is no longer necessarily a good business; and retiring doctors can no longer automatically expect to extract premium sales prices. Moreover, uninformed young physicians should not be goaded to over-pay. Regardless of your dismay – or delight – in the changing healthcare milieu, always be foreword thinking and remember the admonition, Trust-but Verify, for any business transaction.
But, it is a fait accompli that medical practice worth is presently deteriorating. As the population ages and third-party reimbursements plummet, doctors are commoditized and traditional retail medicine is replaced by more efficient wholesale business models like workplace health clinics. The recent sub-prime mortgage de-fault fiasco, potential tax-reform law expiration and the political specter of a nationalized healthcare system, only adds fuel to the macro-economic fires of uncertainly.
Finally, once practice price is mutually agreed upon, sales contract terms and agreements present a plethora of financing challenges for both involved parties to consider [bank loan payment rates and length, personal promissory guarantees, down-payment offsets, earn-out arrangements, Uniform Commercial Codes-1 asset guarantees, etc] in their due-diligence efforts.
However, most reputable firms use a blended fee-schedule of fixed and hourly rates (plus expenses). So, doctors should expect to spend approximately $5,000-15,000 for an average sized – limited appraisal – that is completely suitable for most internal activities.
Moreover, look-out if the valuation not done at an-arm’s-length and independent manner; or worse still, if it is performed for both parties simultaneously.
Selecting the Wrong Valuator and Not Understanding Professional Fees
Realize too, that the appraiser may also add expenses that have not been incurred; like an office manager’s salary if your spouse is in that role for free. This produces a lower appraised value and is common in small medical practices. Honoraria are another example that does not figure into value calculations.
For example, we recall one doctor who painted his personal residence and wrote it-off as a valid business expense. Deleting other major expenses such as country club memberships, make a practice look more profitable—good news if you’re selling it, bad news if you’re getting a divorce.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Marcinko & Associates is financial guide. We help answer your questions in an empowering way. We educate and guide medical colleagues to understand their financial picture and to make better financial decisions. We strive to simplify everything, clear up confusion, and address specific needs and goals.
Simply put, we’re a financial services company on a mission to empower financial freedom for all healthcare professionals; only. We work with doctors, nurses, medical providers, individuals and all sizes of organizations to offer investment, wealth management and retirement solutions so everyone can have a clear and simple understanding of where their finances and career is today and where it is headed tomorrow.
Whatever your financial situation, we do not shame, criticize, or sell. We enrich, educate and empower. We work only with medical colleagues at every stage of their financial journey [students, interns, residents, practitioners, mid-career and mature physicians], through big life personal changes to annual employment reviews, in order to help them understand, invest, and protect their money and lifestyle.
Assess, develop, and align financial retirement and estate planning goals
Risk Management: Malpractice, home, life, medical, auto and personal indemnity
Life Insurance Need Reviews: whole, universal and term
Business, operations, HR, employment negotiations and medical practice management
Annuity Need Reviews: Indexed and Fixed [Pros and Cons].
***
***
At Marcinko & Associates we discuss specific needs and answer specific questions. We educate and make personalized recommendations that you are free to use, incorporate or disregard. Referrals to trusted specialists and strategic alliance partners then occur if – and as – needed [pro re nata].
Posted on October 13, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
AVERAGE REVENUE PER CASE
By Staff Reporters
***
Podiatry is 3rd in Average Revenue Per Case in ASCs
***
***
Orthopedic surgery topped the pack for ASC revenue per case, according to VMG Health’s “Multi-Specialty ASC Benchmarking Study” for 2022.
The specialty was only the fourth most-represented among ASC cases, however. Nationally, gastroenterology was the most-represented specialty among ASCs, with 32 percent of all cases, followed by ophthalmology, with 26 percent, and pain management and orthopedics, with 22 and 21 percent, respectively.
The following are some of the most common psychological biases. Some are learned while others are genetically determined (and often socially reinforced). While this essay focuses on the financial implications of these biases, they are prevalent in most areas in life.
[A] Incentives
It is broadly accepted that incenting someone to do something is effective, whether it be paying office staff a commissions to sell more healthcare products, or giving bonuses to office employees if they work efficiently to see more HMO patients. What is not well understood is that the incentives cause a sub-conscious distortion of decision-making ability in the incented person. This distortion causes the affected person – whether it is yourself or someone else – to truly believe in a certain decision, even if it is the wrong choice when viewed objectively. Service professionals, including financial advisors and lawyers, are affected by this bias, and it causes them to honestly offer recommendations that may be inappropriate, and that they would recognize as being inappropriate if they did not have this bias. The existence of this bias makes it important for each one of us to examine our incentive biases and take extra care when advising physician clients, or to make sure we are appropriately considering non-incented alternatives.
[B] Denial
Denial is a well known, but under-appreciated, psychological force. Physicians, clients and professionals (like everyone else) are prone to the mistake of ignoring a painful reality, like putting off an unpleasant call (thus prolonging a problematic situation and potentially making it worse) or not opening account statements because of the desire not to see quantitative proof of losses. Denial also manifests itself by causing human beings to ignore evidence that a mistake has been made. If you think of yourself as a smart person (and what professional doesn’t?), then evidence pointing to the conclusion that a mistake has been made will call into question that belief, causing cognitive dissonance. Our brains function to either avoid cognitive dissonance or to resolve it quickly, usually by discounting or rationalizing the disconfirming evidence. Not surprisingly, colleagues at Kansas State University and elsewhere, found that financial denial, including attempts to avoid thinking about or dealing with money, is associated with lower income, lower net worth, and higher levels of revolving credit.
[C] Consistency and Commitment Tendency
Human beings have evolved – probably both genetically and socially – to be consistent. It is easier and safer to deal with others if they honor their commitments and if they behave in a consistent and predictable manner over time. This allows people to work together and build trust that is needed for repeat dealings and to accomplish complex tasks. In the jungle, this trust was necessary to for humans to successfully work as a team to catch animals for dinner, or fight common threats. In business and life it is preferable to work with others who exhibit these tendencies. Unfortunately, the downside of these traits is that people make errors in judgment because of the strong desire not to change, or be different (“lemming effect” or “group-think”). So the result is that most people will seek out data that supports a prior stated belief or decision and ignore negative data, by not “thinking outside the box”. Additionally, future decisions will be unduly influenced by the desire to appear consistent with prior decisions, thus decreasing the ability to be rational and objective. The more people state their beliefs or decisions, the less likely they are to change even in the face of strong evidence that they should do so. This bias results in a strong force in most people causing them to avoid or quickly resolve the cognitive dissonance that occurs when a person who thinks of themselves as being consistent and committed to prior statements and actions encounters evidence that indicates that prior actions may have been a mistake. It is particularly important therefore for advisors to be aware that their communications with clients and the press clouds the advisor’s ability to seek out and process information that may prove current beliefs incorrect. Since this is obviously irrational, one must actively seek out negative information, and be very careful about what is said and written, being aware that the more you shout it out, the more you pound it in.
[D] Pattern Recognition
On a biological level, the human brain has evolved to seek out patterns and to work on stimuli-response patterns, both native and learned. What this means is that we all react to something based on our prior experiences that had shared characteristics with the current stimuli. Many situations have so many possible inputs that our brains need to take mental short cuts using pattern recognition we would not gain the benefit from having faced a certain type of problem in the past. This often-helpful mechanism of decision-making fails us when past correlations or patterns do not accurately represent the current reality, and thus the mental shortcuts impair our ability to analyze a new situation. This biologic and social need to seek out patterns that can be used to program stimuli-response mechanisms is especially harmful to rational decision-making when the pattern is not a good predictor of the desired outcome (like short term moves in the stock market not being predictive of long term equity portfolio performance), or when past correlations do not apply anymore.
[E] Social Proof
It is a subtle but powerful reality that having others agree with a decision one makes, gives that person more conviction in the decision, and having others disagree decreases one’s confidence in that decision. This bias is even more exaggerated when the other parties providing the validating/questioning opinions are perceived to be experts in a relevant field, or are authority figures, like people on television. In many ways, the short term moves in the stock market are the ultimate expression of social proof – the price of a stock one owns going up is proof that a lot of other people agree with the decision to buy, and a dropping stock price means a stock should be sold. When these stressors become extreme, it is of paramount importance that all participants in the financial planning process have a clear understanding of what the long-term goals are, and what processes are in place to monitor the progress towards these goals. Without these mechanisms it is very hard to resist the enormous pressure to follow the crowd; think social media.
[F] Contrast
Sensation, emotion and cognition work by contrast. Perception is not only on an absolute scale, it also functions relative to prior stimuli. This is why room temperature water feels hot when experienced after being exposed to the cold. It is also why the cessation of negative emotions “feels” so good. Cognitive functioning also works on this principle. So one’s ability to analyze information and draw conclusions is very much related to the context with in which the analysis takes place, and to what information was originally available. This is why it is so important to manage one’s own expectations as well as those of clients. A client is much more likely to be satisfied with a 10% portfolio return if they were expecting 7% than if they were hoping for 15%.
[G] Scarcity
Things that are scarce have more impact and perceived value than things present in abundance. Biologically, this bias is demonstrated by the decreasing response to constant stimuli (contrast bias) and socially it is widely believed that scarcity equals value. People who feel an opportunity may “pass them by” and thus be unavailable are much more likely to make a hasty, poorly reasoned decision than they otherwise would. Investment fads and rising security prices elicit this bias (along with social proof and others) and need to be resisted. Understanding that analysis in the face of perceived scarcity is often inadequate and biased may help professionals make more rational choices, and keep clients from chasing fads.
[H] Envy / Jealousy
This bias also relates to the contrast and social proof biases. Prudent financial and business planning and related decision-making are based on real needs followed by desires. People’s happiness and satisfaction is often based more on one’s position relative to perceived peers rather than an ability to meet absolute needs. The strong desire to “keep up with the Jones” can lead people to risk what they have and need for what they want. These actions can have a disastrous impact on important long-term financial goals. Clear communication and vivid examples of risks is often needed to keep people focused on important financial goals rather than spurious ones, or simply money alone, for its own sake.
[I] Fear
Financial fear is probably the most common emotion among physicians and all clients. The fear of being wrong – as well as the fear of being correct! It can be debilitating, as in the corollary expression on fear: the paralysis of analysis.
According to Paul Karasik, there are four common investor and physician fears, which can be addressed by financial advisors in the following manner:
Fear of making the wrong decision: ameliorated by being a teacher and educator.
Fear of change: ameliorated by providing an agenda, outline and/or plan.
Fear of giving up control: ameliorated by asking for permission and agreement.
Fear of losing self-esteem: ameliorated by serving the client first and communicating that sentiment in a positive manner.
Now, as human beings, our brains are booby-trapped with psychological barriers that stand between making smart financial decisions and making dumb ones. The good news is that once you realize your own mental weaknesses, it’s not impossible to overcome them.
In fact, Mandi Woodruff, a financial reporter whose work has appeared in Yahoo! Finance, Daily Finance, The Wall Street Journal, The Fiscal Times and the Financial Times among others; related the following mind-traps in a September 2013 essay for the finance vertical Business Insider; as these impediments are now entering the lay-public zeitgeist:
Anchoring happens when we place too much emphasis on the first piece of information we receive regarding a given subject. For instance, when shopping for a wedding ring a salesman might tell us to spend three months’ salary. After hearing this, we may feel like we are doing something wrong if we stray from this advice, even though the guideline provided may cause us to spend more than we can afford.
Myopia makes it hard for us to imagine what our lives might be like in the future. For example, because we are young, healthy, and in our prime earning years now, it may be hard for us to picture what life will be like when our health depletes and we know longer have the earnings necessary to support our standard of living. This short-sightedness makes it hard to save adequately when we are young, when saving does the most good.
Gambler’s fallacy occurs when we subconsciously believe we can use past events to predict the future. It is common for the hottest sector during one calendar year to attract the most investors the following year. Of course, just because an investment did well last year doesn’t mean it will continue to do well this year. In fact, it is more likely to lag the market.
Avoidance is simply procrastination. Even though you may only have the opportunity to adjust your health care plan through your employer once per year, researching alternative health plans is too much work and too boring for us to get around to it. Consequently, we stick with a plan that may not be best for us.
Loss aversion affected many investors during the stock market crash of 2008. During the crash, many people decided they couldn’t afford to lose more and sold their investments. Of course, this caused the investors to sell at market troughs and miss the quick, dramatic recovery.
Overconfident investing happens when we believe we can out-smart other investors via market timing or through quick, frequent trading. Data convincingly shows that people who trade most often under-perform the market by a significant margin over time.
Mental accounting takes place when we assign different values to money depending on where we get it from. For instance, even though we may have an aggressive saving goal for the year, it is likely easier for us to save money that we worked for than money that was given to us as a gift.
Herd mentality makes it very hard for humans to not take action when everyone around us does. For example, we may hear stories of people making significant profits buying, fixing up, and flipping homes and have the desire to get in on the action, even though we have no experience in real estate.
A class action lawsuit has been filed in Minnesota against UnitedHealth Group (NYSE:UNH) over allegations that the health insurer and its subsidiary, NaviHealth, used a faulty algorithm to deny rehabilitation care for Medicare Advantage beneficiaries. California-based Clarkson Law Firm filed the lawsuit in the U.S. District Court of Minnesota on Tuesday following an investigative report published by the health-focused news site Stat.
It alleges that UnitedHealth and its subsidiary, NaviHealth, used the computer algorithm named nH Predict to “systematically deny claims” of patients recovering from debilitating illnesses in nursing homes. According to the lawsuit, despite its 90% error rate, the company used the algorithm to deny claims, knowing that only 0.2% would appeal its decision. According to Stat, Humana (HUM), the nation’s second-largest player in the Medicare Advantage market behind UnitedHealth (UNH), also uses nH Predict. UnitedHealth (UNH) denied it used the NaviHealth predict tool to arrive at coverage decisions.
***
***
Ironically, UnitedHealth’s (NYSE:UNH) Optum Rx unit announced plans to move eight insulin products to “preferred” status on formularies to further expand the number of patients benefiting from $35 or less monthly out-of-pocket costs for the lifesaving therapy.
Optum Rx, UNH’s pharmacy benefit manager (PBM), said that effective January 1, 2024, all short- and rapid-acting insulins will move to Tier 1 in commercial formularies, a list of drugs the company maintains to indicate coverage for insured patients.
According to the Dupont Decomposition Equation – which involves the conglomeration of net operating income, revenues, expenses and average operating assets – ROI and economic profit is increased in three prioritized ways:
Cost and expense reductions.
Revenue increases [Rev]
Reduced average operating assets [AOO]
Note: ROI = NOI / Rev X Rev / AOO
Cost and expense reductions
Although many hospitals have reduced expenses, postponed projects and put clinical or information technology projects on hold because of the current healthcare conundrum, this may be unwise and quality may suffer. And, mental health care programs are almost always the first cost center to be reduced in tough times.
Upgrades today, especially with concurrent marketing and advertising promotions, may well be considered a strategic competitive advantage, and at bargain basement prices for those with cash or credit. This cost reduction is easy because it gives the biggest buck-bang in the ROI equation, and is the first line of ROI augmentation by savvy administrators and CEOs. It is also intuitive and wholly “wrung-out” in the marketplace, to date.
Revenue increases
On the other hand, revenues can usually be only incrementally increased by improving services like emergency care, urgent care, wellness, out-patient and/or surgical departments. This is the more difficult part of the equation and yields a positive, but lesser return in the ROI equation.
The following medical practice procedures will markedly increase upfront office collections:
Train staff to handle exceptions. What is your policy if the patient payment is significant? Will you allow 25% payments—one today and three over the next three months? Communicate your policy to all staff. What will you do if a patient shows up without an insurance card? There will be other exceptions. Train employees to call the appropriate practice-management contact when an exception does not fit in the categories you provide and make sure those managers are responsive.
Understand that not everyone will shine in collections. The value of this new front-desk function should be reflected in job descriptions and wages. Track staff performance and hold employees accountable for collection goals. The most successful practices collect in the 90% range.
Provide professional signage that states your basic policy. “Payments are due at time of service.” Avoid typewritten, lengthy explanations taped to walls or desks that look like clutter.
Reduced average operating assets
Finally, any delay in updating facilities – while easy and may reduce operating assets – there is little ROI advantage and profit potential. Of course, facility asset upgrades mean borrowing funds through tax-exempt bonds – the main source of debt for most hospitals – and is currently difficult or impossible in this climate. Loans from banks, private investors, angels, venture capitalists or other financial institutions are similarly difficult to obtain. Thus, this part of the equation may often be neglected; as is the case now.
“A reliable way to make people believe in falsehoods is frequent repetition, because familiarity is not easily distinguished from truth.” – Daniel Kahneman
As I was watching with interest more [fake] news such as stories surrounding evidence by citations of Russian involvement in US elections and fake prices leading to some violent market gyrations as in Bitcoin and the Corona Virus Pandemic, and societal musings around the thematic of hoaxes … we decided to offer this theme.
Enter the WOOZLE
And so, the Woozle effect, also known as evidence by citation, or a woozle, occurs when frequent citation of previous publications that lack evidence misleads individuals, groups and the public into thinking or believing there is evidence, and non-facts become urban myths and factoids.
Posted on October 2, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
The FTC said it would allow Chevron’s $53 billion purchase of Hess, but it barred Hess CEO John B. Hess from sitting on Chevron’s board over his communications with OPEC.
Soon, students may not need an extra year of college to attain CPA licensure. The AICPA and NASBA have proposed a “competency-based experience pathway” to licensure—with no post-bachelor’s coursework required.
Energy was the top-performing sector in the S&P 500 today thanks to rising fears of fighting between Iran and Israel. APA Corp. rose 4.91%, Halliburton climbed 3.10%, and Occidental Petroleum gained 3.33%.
Defensestocks rose for much the same reason, with Lockheed Martin up 3.66%, NorthropGrumman trading 3.04% higher, and L3Harris Technologies up 3.03%
Hess Corp. and Chevron rose after the FTC declared that, as long as John Hess isn’t allowed to sit on the board, the two companies might be allowed to merge. Shares of Hess gained 2.34%, while Chevron climbed 1.68%.
New Fortress Energy popped 6.49% on the news that it has priced a public offering of 46 million shares at $8.46 per share. That will go a long way to helping the struggling energy stock rake in some much-needed cash.
ArcosDorados, the world’s biggest McDonald’s franchisee, jumped 14.56% after it renewed its agreement with McDonald’s, locking down a flat royalty rate for the next decade.
What’s down
Signet Jewelers fell 7.91% on the news that CEO Virginia Drosos, who has led the company to strong success over the past seven years, will retire.
HP sank 3.09% after Citi analysts downgraded the company based on lower PC and printer demand in the years ahead.
Disney received a rare analyst downgrade today from Raymond James analysts, who think that theme park attendance will continue to slow in the next 12 to 18 months. Shares dropped 2.14%.
Amentum Holdings plummeted 20.16% only a day after the engineering services company debuted on the S&P 500.
Here’s where the major stock market benchmarks ended:
The S&P 500® index (SPX)fell 53.73 points (–0.93%) to 5,708.75; the Dow Jones Industrial Average® ($DJI) declined 173.18 points (–0.41%) to 42,156.97; the NASDAQ Composite® ($COMP) lost 278.81 points (–1.53%) to 17,910.36.
The 10-year Treasury note yield (TNX) fell six basis points to 3.74%.
The CBOE Volatility Index® (VIX) jumped to 19.28, the highest in nearly a month.
The American economy is seemingly fairing so well that UBS has signaled a potential return to the glory days. The European finance giant believes Uncle Sam is inching closer to a ‘Roaring 20s’ scenario, placing the likelihood of an incoming booming economic cycle at 50%. The phrase goes back to the same decade a century ago, when massive economic growth prompted a construction boom and rising prosperity for families.
Today, colleges and universities are beginning to identify students who are adept at learning online and reward top achievers and professors. Employers, graduate and business schools are beginning to troll MOOCs [massive open online courses] seeking viable job, and academic, candidates.
Definition
A massive open online course ( MOOC / m uː k / ) is an online course aimed at unlimited participation and open access via the web. In addition to traditional course materials such as filmed lectures, readings, and problem sets , many MOOCs provide interactive courses with user forums to support community interactions among students, professors, and teaching assistants (TAs) as well as immediate feedback to quick quizzes and assignments.
In fact, when I last checked, the nation’s graduate, B-school and MBA students were enrolled in more than 118 online MBA/MPH/MSH healthcare administration programs. MOOCs offer greater access for a larger number of students, at significantly lower costs than on-site programs.
By the same token, technology like Blackboard®, Cengage, eXplorance, BANNER and Kalture must be used to full potential. Smart phones, PCs and tablets, videos, interactive games, A.I. simulators and apps with Skype®-like virtual classrooms and cloud storage are obvious embellishments to online initiatives.
***
***
Definition
A Moodle is a free and open-source learning management system written in PHP and distributed under the GNU General Public License. Developed on pedagogical principles, Moodle is used for blended learning, distance education, flipped classroom and other e-learning projects in schools, universities, workplaces and other sectors.
Note: PHP is a popular general-purpose scripting language that is especially suited to web development. Fast, flexible and pragmatic, PHP powers everything from your blog to the most popular websites in the world.
Disposablecredit cards are the newest innovation to help reduce fraud and assumed identity scams on e-commerce based websites. As with traditional credit cards, these cards are numbered, but used only once. Then, electronically they are erased so that there is nothing left in the merchant’s database for hackers to steal.
But, in 2014, Congress began looking at new ways to keep personal credit card information safe after several high-profile security breaches at some of America’s top retailers.
WHY? Current credit cards use easy to hack magnetic strip technology from the 1960s. Many consumers want more secure “pin & chip” cards which have been in use in Europe for years. Even though micro-chip technology costs billions to implement, merchants are moving in that direction as they issue new cards to consumers. Most modern polls show nearly half of all people surveyed are extremely concerned about the safety of their personal credit card information.
Burner Cards: Similar to a burner phone or “throwaway” social media account, burner credit cards are temporary, virtual credit cards that are not your “main” credit card. The bank or burner card app will give you a temporary number that links back to your main credit card which you can use for online purchases.
An ANonymousCreditCard provides an extreme degree of privacy and prevents the tracking of your expenses by a spouse, people with bad intentions or government monitoring agencies. It is important to realize that there are plenty of legitimate reasons for wanting to buy something discreetly through an AnonymousCreditCard.
Credit Card Mistakes to Avoid
No number has as far-reaching an impact on your money as your credit scores.
Here are some obstacles, physicians and all of us, should dodge on the road to financial security:
If you are denied a credit card, you have the right to obtain a credit report free from the agency which denied you. Your request must be made in writing and within thirty-sixty days. Consumer credit is governed by the Fair Credit Reporting Act (FCRA). The regulations are issued by and enforced by the Federal Trade Commission. Certain states offer consumers additional rights. Credit reporting agencies are referred to as a “consumer reporting agency”.
The enterprise value [EV] tends to be thought of as a theoretical takeover price if a company were to be bought. It is calculated as market capitalization plus debt, minority interest and preferred shares, minus total cash and cash equivalents.
Enterprise value = common equity at market value (this line item is also known as “market cap”) + debt at market value (here debt refers to interest-bearing liabilities, both long-term and short-term) + minority interest at market value, if any + preferred equity at market value + unfunded pension liabilities and other debt-deemed provisions – value of associate companies – cash and cash equivalents.
In mathematics, the absolute value or modulus of a real number x, denoted |x|, is the non-negative value of x without regard to its sign. Namely, |x| = x if x is positive, and |x| = −x if x is negative (in which case −x is positive), and |0| = 0. For example, the absolute value of 3 is 3, and the absolute value of −3 is also 3. The absolute value of a number may be thought of as its distance from zero.
***
In finance, absolute value, also known as an intrinsic value, refers to a business valuation method that uses discounted cash flow (DCF) analysis to determine a company’s financial worth. The absolute value method differs from the relative value models that examine what a company is worth compared to its competitors. Absolute value models try to determine a company’s intrinsic worth based on its projected cash flows.
Absolute value refers to a business valuation method that uses discounted cash flow analysis to determine a company’s financial worth.
Investors can determine if a stock is currently under or overvalued by comparing what a company’s share price should be given its absolute value to the stock’s current price.
There are some challenges with using the absolute value analysis including forecasting cash flows, predicting accurate growth rates, and evaluating appropriate discount rates.
Absolute value, unlike relative value, does not call for the comparison of companies in the same industry or sector.
ACOs are groups of doctors, hospitals, and other health care providers, who come together voluntarily to give coordinated high-quality care to their Medicare patients. The goal of coordinated care is to ensure that patients get the right care at the right time, while avoiding unnecessary duplication of services and preventing medical errors.
When an ACO succeeds both in delivering high-quality care and spending health care dollars more wisely, the ACO will share in the savings it achieves for the Medicare program.
Now, suppose that in a new Accountable Care Organization [ACO] contract, a certain medical practice was awarded a new global payment or capitation styled contract that increased revenues by $100,000 for the next fiscal year. The practice had a gross margin of 35% that was not expected to change because of the new business. However, $10,000 was added to medical overhead expenses for another assistant and all Account’s Receivable (AR) are paid at the end of the year, upon completion of the contract.
Cost of Medical Services Provided (COMSP):
The Costs of Medical Services Provided (COMSP) for the ACO business contract represents the amount of money needed to service the patients provided by the contract. Since gross margin is 35% of revenues, the COMSP is 65% or $65,000. Adding the extra overhead results in $75,000 of new spending money (cash flow) needed to treat the patients. Therefore, divide the $75,000 total by the number of days the contract extends (one year) and realize the new contract requires about $ 205.50 per day of free cash flows.
Assumptions
Financial cash flow forecasting from operating activities allows a reasonable projection of future cash needs and enables the doctor to err on the side of fiscal prudence. It is an inexact science, by definition, and entails the following assumptions:
All income tax, salaries and Accounts Payable (AP) are paid at once.
Durable medical equipment inventory and pre-paid advertising remain constant.
Gains/losses on sale of equipment and depreciation expenses remain stable.
Gross margins remain constant.
The office is efficient so major new marginal costs will not be incurred.
Physician Reactions:
Since many physicians are still not entirely comfortable with global reimbursement, fixed payments, capitation or ACO reimbursement contracts; practices may be loath to turn away short-term business in the ACA era. Physician-executives must then determine other methods to generate the additional cash, which include the following general suggestions:
1. Extend Account’s Payable
Discuss your cash flow difficulties with vendors and emphasize their short-term nature. A doctor and her practice still has considerable cache’ value, especially in local communities, and many vendors are willing to work them to retain their business
2. Reduce Accounts Receivable
According to most cost surveys, about 30% of multi-specialty group’s accounts receivable (ARs) are unpaid at 120 days. In addition, multi-specialty groups are able to collect on only about 69% of charges. The rest was written off as bad debt expenses or as a result of discounted payments from Medicare and other managed care companies. In a study by Wisconsin based Zimmerman and Associates, the percentages of ARs unpaid at more than 90 days is now at an all time high of more than 40%. Therefore, multi-specialty groups should aim to keep the percentage of ARs unpaid for more than 120 days, down to less than 20% of the total practice. The safest place to be for a single specialty physician is probably in the 30-35% range as anything over that is just not affordable.
The slowest paid specialties (ARs greater than 120 days) are: multi-specialty group practices; family practices; cardiology groups; anesthesiology groups; and gastroenterologists, respectively. So work hard to get your money, faster. Factoring, or selling the ARs to a third party for an immediate discounted amount is not usually recommended.
3. Borrow with Short-Term Bridge Loans
Obtain a line of credit from your local bank, credit union or other private sources, if possible in an economically constrained environment. Beware the time value of money, personal loan guarantees, and onerous usury rates. Also, beware that lenders can reduce or eliminate credit lines to a medical practice, often at the most inopportune time.
4. Cut Expenses
While this is often possible, it has to be done without demoralizing the practice’s staff.
5. Reduce Supply Inventories
If prudently possible; remember things like minimal shipping fees, loss of revenue if you run short, etc.
6. Taxes
Do not stop paying withholding taxes in favor of cash flow because it is illegal.
Hyper-Growth Model:
Now, let us again suppose that the practice has attracted nine more similar medical contracts. If we multiple the above example tenfold, the serious nature of potential cash flow problem becomes apparent. In other words, the practice has increased revenues to one million dollars, with the same 35% margin, 65% COMSP and $100,000 increase in operating overhead expenses. Using identical mathematical calculations, we determine that $750,000 / 365days equals $2,055.00 per day of needed new free cash flows! Hence, indiscriminate growth without careful contract evaluation and cash flow analysis is a prescription for potential financial disaster.
Once the value of all personal assets and liabilities is known, net worth can be determined with the following formula: Net worth = assets minus liabilities. Obviously, higher is better.
In The Millionaire Next Door, Thomas H. Stanley, PhD, and William H. Danko give the following benchmark for net worth accumulation. Although conservative for physicians of a past generation, it may be more applicable in the future because of current managed care environment. Here is the guide: Multiple your age by your annual pre-tax income from all sources; except inheritances, and then divide by ten.
Example:
As an HMO pediatrician, Dr. Curtis earned $ 90,000 last year. So, if she is 35, her net worth should be at least $ 315,000.
How do you get to that point? In a word, consume less and save more. Stanley and Danko found that the typical millionaire set aside 15 percent of earned income annually and has enough invested to survive 10 years, at current income levels if he stopped working.
Question: If Dr. Curtis lost her job tomorrow, how long could she pay herself the same salary? Could you?
Posted on September 18, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Why Hospitals, Clinics and Medical Offices are Not Hotels, or Manufacturing Plants or Production Assembly Lines, etc!
By Dr. David E. Marcinko FACFAS, MBA, MEd, CMP™
[Editor-in-Chief]
The rising cost of health insurance remains a major concern for business; despite the Affordable Care Act [ACA] of March 2010. Local and national news publications have trumpeted that healthcare costs are not just rising but are growing in proportion to the cost of other goods and services.
Many of these publications have expressed the widely held view that because of the “inflation gap,” the cost of medical expenses needs curbing. Proponents of this viewpoint attribute the growth in the gross domestic product (GDP) devoted to personal medical services (from 5% in 1965 to approximately 14% in 2005 and 17% in 2012) to increases in both total national medical expenditures as well as prices for specific services, and then conclude that there is a need to rein in the growing costs of healthcare services for the average American, even if it be through a legislative mandate.
Healthcare Is the Economy
According to colleague Robert James Cimasi MHA, AVA, CMP™ of Health Capital Consultants LLC in St. Louis, MO, healthcare cannot be separated from the economy at large. Although economists have cited the aging population as the reason for the increase in healthcare’s share of the GDP, other voices assert that financial greed among HMOs, pharmaceutical companies, hospitals, and medical providers like doctors and nurses is responsible. In reality, the rise in healthcare expenditures is, at least in large part, the result of a much deeper economic force.
As economist William J. Baumol of New York University explained in a November 1993 New Republic article: “the relative increase in healthcare costs compared with the rest of the economy is inevitable and an ineradicable part of a developed economy. The attempt [to control relative costs] may be as foolhardy as it is impossible”.
Baumol’s observation is based on documented and significant differences in productivity growth between the healthcare sector of the economy and the economy as a whole.
Low Productivity Growth
Healthcare services have experienced significantly lower productivity growth rates than other industry sectors for three reasons, according to Cimasi:
1) Healthcare services are inherently resistant to automation. Innovation in the form of technological advancement has not made the same impact on healthcare productivity as it has in other industry sectors of the economy. The manufacturing process can be carried out on an assembly line where thousands of identical (or very similar) items can be produced under the supervision of a few humans utilizing robots and statistical sampling techniques (e.g., defects per 1,000 units). The robot increases assembly line productivity by accelerating the process and reducing labor input. In medicine, most technology is still applied in a patient-by-patient manner — a labor-intensive process. Patients are cared for one at a time. Hospitals and physician offices cannot (and, most would agree, should not) try to operate as factories because patients are each unique and disease is widely variable.
2) Healthcare is local. Unlike other labor-intensive industries (e.g., shoe making), healthcare services are essentially local in nature. They cannot regularly be delivered from Mexico, India or Malaysia. They must be provided locally by local labor. Healthcare organizations must compete within a local community with low or no unemployment among skilled workers for high quality and higher cost labor.
3) Healthcare quality is — or is believed to be — correlated with the amount of labor expended. For example, a 30-minute office visit with a physician is perceived to be of higher quality than a 10-minute office visit. In mass production, the number of work-hours per unit is not as important a predictor of product quality as the skills and talents of a small engineering team, which may quickly produce a single design element for thousands of products (e.g., a common car chassis).
Assessment
Healthcare suffers a number of serious consequences when its productivity grows at a slower rate than other industries, the most serious being higher relative costs for healthcare services. The situation is an inevitable and ineradicable part of a developed economy.
For example, as technological advancements increase productivity in the computer, and eHR, manufacturing industry, wages for computer industry labor likewise increase. However, the total cost per computer produced actually declines. But in healthcare (where technological advancements do not currently have the same impact on productivity), wage increases that would be consistent with other sectors of the economy yield a problem: the cost per unit of healthcare produced increases.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Marcinko & Associates is financial guide. We help answer your questions in an empowering way. We educate and guide medical colleagues to understand their financial picture and to make better financial decisions. We strive to simplify everything, clear up confusion, and address specific needs and goals.
Simply put, we’re a financial services company on a mission to empower financial freedom for all healthcare professionals; only. We work with doctors, nurses, medical providers, individuals and all sizes of organizations to offer investment, wealth management and retirement solutions so everyone can have a clear and simple understanding of where their finances and career is today and where it is headed tomorrow.
Whatever your financial situation, we do not shame, criticize, or sell. We enrich, educate and empower. We work only with medical colleagues at every stage of their financial journey [students, interns, residents, practitioners, mid-career and mature physicians], through big life personal changes to annual employment reviews, in order to help them understand, invest, and protect their money and lifestyle.
Assess, develop, and align financial retirement and estate planning goals
Risk Management: Malpractice, home, life, medical, auto and personal indemnity
Life Insurance Need Reviews: whole, universal and term
Business, operations, HR, employment negotiations and medical practice management
Annuity Need Reviews: Indexed and Fixed [Pros and Cons].
***
***
At Marcinko & Associates we discuss specific needs and answer specific questions. We educate and make personalized recommendations that you are free to use, incorporate or disregard. Referrals to trusted specialists and strategic alliance partners then occur if – and as – needed [pro re nata].
Experts estimate that it can cost more than $1 million to recruit and train a replacement for a doctor who leaves the profession because of burnout. But, as no broad calculation of burnout costs exists, Dr. Tait Shanafelt [Mayo Clinic researcher and Stanford Medicine’s first Chief Physician Wellness Officer] said Stanford, Harvard Business School, Mayo Clinic and the American Medical Association (AMA) are further cost estimating the issue. Nevertheless, Shanafelt and other researchers have shown that burnout erodes job performance, increases medical errors, and leads doctors to leave a profession they once loved.
Fortunately, we can help. From formal coaching to second career opinions, mentoring and advising, we can help with our remediation executive career programs. Regardless of what is happening in your life, it is wonderful to have a non-partial, confidential and informed career coach and sounding board on your side.
CITE: JAMA Internal Medicine [Effect of a Professional Coaching Intervention on the Well-Being and Distress of Physicians].
Did you know that at MARCINKO & Associates, all medical colleagues throughout the United States may contact us when they are considering the sale, purchase, strategic operating improvement, merger, acquisition and/or other financial business or related personal financial planning transaction?
Our difference is “hard” knowledge and insider financial guidance that helps medical colleagues, nurses, private practitioners, clinics, ambulatory surgery, radiology and outpatient wound care centers realize their ultimate economic goals. This typically includes managerial and cost accounting, financial ratio analysis, fair market valuation business appraisals, business plan creation and personal financial planning.
Our “expert witness” business litigation support service and divorce mediation, arbitration, asset division, settlement and second opinion offerings are always available, as well.
And, our “soft” skill professional career guidance and mentoring center includes executive coaching, consulting and mentoring advisory programs for stressed, conflicted or burned-out physicians and medical practitioners.
Most importantly, our professional fees are reasonable and always transparent.
MARCINKO & Associates also serves universities, medical, business, graduate and nursing schools; physicians, dentists, podiatrists, optometrists and legal societies. This includes accountants, financial service providers, wealth and hedge fund managers, emerging entities, hospitals, CEOs and their BODs, the press, media and related organizations.
According to the website, Engage with Grace, we make choices throughout our lives — where we want to live, what types of activities will fill our days, and with whom we spend our time, etc. These choices are often a balance between our desires and our means, but at the end of the day, they are decisions made with intent.
Somehow when we get close to death, however, we stop making decisions. We get frozen in our tracks and can’t talk about our preferences for end of life care.
Death Studies
Studies loom out there — 73% of Americans would prefer to die at home, but anywhere between 20-50% of Americans die in hospital settings. More than 80% of Californians say their loved ones “know exactly” or have a “good idea” of what their wishes would be if they were in a persistent coma, but only 50% say they’ve talked to them about their preferences.
But, end of life experience is about a lot more than statistics. It’s about all of us.
Genesis and Epiphany
In the summer of 2008, Matt Holt (Founder of Health2.0) and Alexandra Drane (President of Eliza) met with some friends for dinner. Over their second cocktail, they got deep into conversation about these very topics. Many of us live with such intent — why do we put the end of our lives in someone else’s control? Why isn’t this topic a conversation that people are having? How could we help start it? And it hit them — What if we could work together to start a viral movement — a movement focused on improving the end of life experience? What if we took responsibility for starting a national (even global) discussion that, until now, most of us haven’t had?
Engage With Grace
The One Slide Project was designed with one simple goal: to help get the conversation about end of life experience started. The idea is simple: Create a tool to help get people talking. One Slide, with just five questions on it. Five questions designed to help get us talking with each other, with our loved ones, about our preferences. And we’re asking people to share this One Slide — wherever and whenever they can… at a presentation, at dinner, at their book club. Just One Slide with five questions to help get all of us talking about death. Just One Slide that we as a community could collectively rally around sharing — in meetings, at a conference, or over a drink.
This is the link to the slide, and this is what we are asking you to do …
Share it any time you can — at the end of presentations, at dinner, or at your book club. Think of the slide as currency and donate just two minutes whenever you can. Commit to being able to answer these five questions about end of life experience for yourself and for your loved ones. Then commit to helping others do the same. Get this conversation started.
Assessment
Let’s start a viral movement driven by the change we as individuals can affect …and the incredibly positive impact we could have collectively. Donate just two minutes to adding just this One Slide to the end of your presentations. Get others involved. Help ensure that all of us — and the people we care for — can end our lives in the same purposeful way we live them.
Just One Slide, just one goal. Think of the enormous difference we can make together.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top
-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Financial advisors don’t ascribe to the Hippocratic Oath. People don’t go to work on “Wall Street” for the same reasons other people become firemen and teachers. There are no essays where they attempt to come up with a new way to say, “I just want to help people.”
Financial Advisor’s are Not Doctors
Some financial advisors and insurance agents like to compare themselves to CPAs, attorneys and physicians who spend years in training and pass difficult tests to get advanced degrees and certifications. We call these steps: barriers-to-entry. Most agents, financial product representatives and advisors, if they took a test at all, take one that requires little training and even less experience. There are few BTEs in the financial services industry.
For example, most insurance agent licensing tests are thirty minutes in length. The Series #7 exam for stock brokers is about 2 hours; and the formerly exalted CFP® test is about only about six [and now recently abbreviated]. All are multiple-choice [guess] and computerized. An aptitude for psychometric savvy is often as important as real knowledge; and the most rigorous of these examinations can best be compared to a college freshman biology or chemistry test in difficulty.
Yet, financial product salesman, advisors and stock-brokers still use lines such as; “You wouldn’t let just anyone operate on you, would you?” or “I’m like your family physician for your finances. I might send you to a specialist for a few things, but I’m the one coordinating it all.” These lines are designed to make us feel good about trusting them with our hard-earned dollars and, more importantly, to think of personal finance and investing as something that “only a professional can do.”
Unfortunately, believing those lines can cost you hundreds of thousands of dollars and years of retirement.
***
***
Suitability Rule
A National Association of Securities Dealers [NASD] / Financial Industry Regulatory Authority [FINRA] guideline that require stock-brokers, financial product salesman and brokerages to have reasonable grounds for believing a recommendation fits the investment needs of a client. This is a low standard of care for commissioned transactions without relationships; and for those “financial advisors” not interested in engaging clients with advice on a continuous and ongoing basis. It is governed by rules in as much as a Series #7 licensee is a Registered Representative [RR] of a broker-dealer. S/he represents best-interests of the firm; not the client.
And, a year or so ago there we two pieces of legislation for independent broker-dealers-Rule 2111 on suitability guidelines and Rule 408(b)2 on ERISA. These required a change in processes and procedures, as well as mindset change.
Note: ERISA = The Employee Retirement Income Security Act of 1974 (ERISA) codified in part a federal law that established minimum standards for pension plans in private industry and provides for extensive rules on the federal income tax effects of transactions associated with employee benefit plans. ERISA was enacted to protect the interests of employee benefit plan participants and their beneficiaries by:
Requiring the disclosure of financial and other information concerning the plan to beneficiaries;
Establishing standards of conduct for plan fiduciaries ;
Providing for appropriate remedies and access to the federal courts.
ERISA is sometimes used to refer to the full body of laws regulating employee benefit plans, which are found mainly in the Internal Revenue Code and ERISA itself. Responsibility for the interpretation and enforcement of ERISA is divided among the Department Labor, Treasury, IRS and the Pension Benefit Guarantee Corporation.
Yet, there is still room for commissioned based FAs. For example, some smaller physician clients might have limited funds [say under $100,000-$250,000], but still need some counsel, insight or advice.
Or, they may need some investing start up service from time to time; rather than ongoing advice on an annual basis. Thus, for new doctors, a commission based financial advisor may make some sense.
Prudent Man Rule
This is a federal and state regulation requiring trustees, financial advisors and portfolio managers to make decisions in the manner of a prudent man – that is – with intelligence and discretion. The prudent man rule requires care in the selection of investments but does not limit investment alternatives. This standard of care is a bit higher than mere suitability for one who wants to broaden and deepen client relationships.
***
***
Prudent Investor Rule
The Uniform Prudent Investor Act (UPIA), adopted in 1992 by the American Law Institute’s Third Restatement of the Law of Trusts, reflects a modern portfolio theory [MPT] and total investment return approach to the exercise of fiduciary investment discretion. This approach allows fiduciary advisors to utilize modern portfolio theory to guide investment decisions and requires risk versus return analysis. Therefore, a fiduciary’s performance is measured on the performance of the entire portfolio, rather than individual investments
Fiduciary Rule
The legal duty of a fiduciary is to act in the best interests of the client or beneficiary. A fiduciary is governed by regulations and is expected to judge wisely and objectively. This is true for Investment Advisors [IAs] and RIAs; but not necessarily stock-brokers, commission salesmen, agents or even most financial advisors. Doctors, lawyers, and the clergy are prototypical fiduciaries.
***
***
More formally, a financial advisor who is a fiduciary is legally bound and authorized to put the client’s interests above his or her own at all times. The Investment Advisors Act of 1940 and the laws of most states contain anti-fraud provisions that require financial advisors to act as fiduciaries in working with their clients. However, following the 2008 financial crisis, there has been substantial debate regarding the fiduciary standard and to which advisors it should apply. In July of 2010, The Dodd-Frank Wall Street Reform and Consumer Protection Act mandated increased consumer protection measures (including enhanced disclosures) and authorized the SEC to extend the fiduciary duty to include brokers rather than only advisors, as prescribed in the 1940 Act. However, as of 2014, the SEC has yet to extend a meaningful fiduciary duty to all brokers and advisors, regardless of their designation.
Ultimately, physician focused and holistic “financial lifestyle planning” is about helping some very smart people change their behavior for the better. But, one can’t help doctors choose which opportunities to take advantage of along the way unless there is a sound base of technical knowledge to apply the best skills, tools, and techniques to achieve goals in the first place.
Most of the harms inflicted on consumers by “financial advisors” or “financial planners” occur not due to malice or greed but ignorance; as a result, better consumer protections require not only a fiduciary standard for advice, but a higher standard for competency.
The CFP® practitioner fiduciary should be the minimum standard for financial planning for retail consumers, but there is room for post CFP® studies, certifications and designations; especially those that support real medical niches and deep healthcare specialization like the Certified Medical Planner™ course of study [Michael E. Kitces; MSFS, MTax, CLU, CFP®, personal communication].
Being a financial planner entails Life-Long-Learning [LLL]. One should not be allowed to hold themselves out as an advisor, consultant, or planner unless they are held to a fiduciary standard, period. Corollary – there’s nothing wrong with a suitability standard, but those in sales should be required to hold themselves out as a salesperson, not an advisor.
The real distinction is between advisors and salespeople. And, fiduciary standards can accommodate both fee and commission compensation mechanisms. However; there must be clear standards and a process to which advisors can be held accountable to affirm that a recommendation met the fiduciary obligation despite the compensation involved.
Ultimately, being a fiduciary is about process, not compensation.
As a medical practitioner, Dr. Marcinko is a fiduciary at all times. He earned Series #7 (general securities), Series #63 (uniform securities state law), and Series #65 (investment advisory) licenses from the National Association of Securities Dealers (NASD-FINRA), and the Securities Exchange Commission [SEC] with a life, health, disability, variable annuity, and property-casualty license from the State of Georgia.
Dr.Marcinko was a licensee of the CERTIFIED FINANCIAL PLANNER™ Board of Standards (Denver) for a decade; now reformed, and holds the Certified Medical Planner™ designation (CMP™). He is CEO of iMBA Inc and the Founding President of: http://www.CertifiedMedicalPlanner.org
[Two Newest Books by Marcinko annd the iMBA, Inc Team]
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
The decision to sell, buy or merge a medical practice, while often financially driven, and is inherently an emotional one for these impact investors who went into the profession largely because of a deep seated zeal to help others.
Still, beyond impact investing musings, there are other economic reasons for a practice valuation that include changes in ownership, determining insurance coverage for a practice buy-sell agreement or upon a physician-owner’s death, organic growth meter, establishing stock options, or bringing in a new partner; etc.
Practice appraisals are also used for legal reasons such as divorce, bankruptcy, breach of contract and minority shareholder complaints. In 2002, the Financial Accounting Standards Board (FASB) issued rules that required certain intangible assets to be valued, such as goodwill. This may be important for practices seeking start-up, service segmentation extensions, or operational funding. Some other reasons for a medical practice appraisal, and the considerations that go along with them, are discussed here.
Medical practice valuation may be required for estate planning purposes. For a decedent physician with a gross estate of more than current in-place tax limits, his or her assets must be reported at fair market value on an estate tax return. If lifetime gifts of a medial practice business interest are made, it is generally wise to obtain an appraisal and attach it to the gift tax return.
Note that when a “closely-held” level of value (in contrast to “freely traded,” “marketable,” or “publicly traded” level) is sought, the valuation consultant may need to make adjustments to the results. There are inherent risks relative to the liquidity of investments in closely held, non-public companies (e.g., medical group practice) that are not relevant to the investment in companies whose shares are publicly traded (freely-traded). Investors in closely-held companies do not have the ability to dispose of an invested interest quickly if the situation is called for, and this relative lack of liquidity of ownership in a closely held company is accompanied by risks and costs associated with the selling of an interest said company (i.e., locating a buyer, negotiation of terms, advisor/broker fees, risk of exposure to the market, etc.). Conversely, investors in the stock market are most often able to sell their interest in a publicly traded company within hours and receive cash proceeds in a few days. Accordingly, a discount may be applicable to the value of a closely held company due to the inherent illiquidity of the investment. Such a discount is commonly referred to as a “discount for lack of marketability.”
Discount for lack of marketability is typically discussed in three categories: (1) transactions involving restricted stock of publicly traded companies; (2) private transactions of companies prior to their initial public offering (IPO); and, (3) an analysis and comparison of the price to earnings (P/E) ratios of acquisitions of public and private companies respectively published in the “Mergerstat Review Study.”\
With a non-controlling interest, in which the holder cannot solely authorize and cannot solely prevent corporate actions (in contrast to a controlling interest), a “discount for lack of control,” (DLOC), may be appropriate. In contrast, a control premium may be applicable to a controlling interest. A control premium is an increase to the pro rata share of the value of the business that reflects the impact on value inherent in the management and financial power that can be exercised by the holders of a control interest of the business (usually the majority holders). Conversely, a discount for lack of control or minority discount is the reduction from the pro rata share of the value of the business as a whole that reflects the impact on value of the absence or diminution of control that can be exercised by the holders of a subject interest.
Several empirical studies have been done to attempt to quantify DLOC from its antithesis, control premiums. The studies include the Mergerstat Review, an annual series study of the premium paid by investors for controlling interest in publicly traded stock, and the Control Premium Study, a quarterly series study that compiles control premiums of publicly traded stocks by attempting to eliminate the possible distortion caused by speculation of a deal.
Buy-Sell Agreements
The ideal situation is for physician partners to put in place a buy-sell agreement when practice relationships are amicable. This establishes the terms for departure before they are required, and is akin to a prenuptial agreement in the marriage contract. Disagreements most often occur when a doctor leaves the group, often acrimoniously. Business operations of the practice decline, employee and partner morale suffers, feuding factions develop spilling over into the office, and the practice begins to implode creating a downward valuation spiral. And so, valuations should be done every 2-3 years, or as the economic circumstances of the practice change. Independence and credibility are provided, and emotional overtones are purged from the transaction.
Physician Partnership Disputes
Medical practice appraisals are often used in partnership disputes, such as breach-of-contract or departure issues. Obvious revenue declinations are not difficult to quantify. But, revenues may not immediately fall since certain Current Procedural Terminology [CPT®] code reimbursements may actually increase. Upon verification however, lost business may be camouflaged as the number of procedures performed, or number of patients decrease after partner departure.
Physicians getting divorced should get a practice appraisal, and either side may hire the appraiser, although occasionally the court will order an expert to provide a neutral valuation. Such valuations should be done in light of both court discovery rules and IRS requirements for closely held businesses. Generally, this requires the consideration of eight elements:
• Practice specialty and operating history
• Economic and healthcare industry condition
• Estimates of practice risks and future returns
• Book value and financial condition of the practice
• Practice future earning capacity
• Physician bonuses, dividends and distributions
• Intangible assets
• Comparable practice sales
Sometimes, the non-physician spouse may even desire a lifestyle analysis to evaluate the potential for under reported income, by a forensic accountant, or appraiser. A family law judge is often the final arbiter of different valuations, and because of varying state laws there may be 50 different nuances of what the practice is really worth.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, urls and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
When You May Need a Business, Management or Financial Planning Second Opinion?
The Marcinko & Associates second opinion service is a physician-to-advisor telephone or e-mail portal that connects independent financial and business management professionals and consultants, with doctors or healthcare executives desiring affordable and unbiased financial or business advice on an as-needed, or per-use basis.
***
Medical professionals and healthcare executives can now receive direct access to us in the areas of Practice Enhancement, Investing, Financial Planning, Asset Allocation, Portfolio Management, Insurance, Mortgage and Lending, Practice Management, Information Technology, Human Resources and Employee Benefits. To assist our doctor / healthcare executive members, we can be contracted with per-hour or per-project fees, and contacted by client phone, email or secure instant messaging.
This Marcinko & Associates service is designed to fill a growing need for medically focused financial or managerial advice that traditional consultants have not been able to serve.
Beside market, limit and stop orders, there are some other miscellaneous orders for the physician or guided investor, to know:
A stop limit order is a stop order that, once triggered or activated, becomes a limit order. Realize that it is possible for a stop limit to be triggered and not executed, as the limit price specified by the doctor may not be available.
In addition, there are all or none and fill or kill orders, and even though both require the entire order to be filled, there are distinct differences. An all or none (AON) is an order in which the broker is directed to fill the entire order or none of it.
A fill or kill (FOK) is an order either to buy or to sell a security in which the broker is directed to attempt to fill the entire’ amount of the order immediately and in full, or that it be canceled.
The difference between an all or none and a fill or kill order is that with an all or none order, immediate execution is not required, while immediate execution is a critical component of the fill or kill. Because of the immediacy requirement,
FOK orders are never found on the specialist’s book. Another difference is that AON orders are only permitted for bonds, not stocks, while FOK orders may be used for either.
Also, there exists an immediate or cancel order (IOC), which is an order to buy or sell a security in which the broker is directed to attempt to fill immediately as much of the order as possible and cancel any part remaining. This type of order differs from a fill-or-kill order which requires the entire order to be filled. An IOC order will permit a partial fill. Because of the immediacy requirement, IOC and FOK orders are never found on the specialist’s book.
Long and Short Positions
A long buy position means that shares are for sale from a market makers inventory or owned by the medical investor outright. Market makers take long positions when customers and other firms wish to sell, and they take short positions when customers and other firms want to buy in quantities larger than the market maker’s inventory. By always being ready, willing, and able to handle orders in this way, market makers assure the investing public of a ready market in the securities in which they are interested. When a security can be bought and sold at firm prices very quickly and easily the security is said to have a high degree of liquidity, also known as marketability.
A short position investor seeks to make a profit by participating in the decline in the market price of a security.
Now; let’s see how these terms, long and short, apply to transactions by medical investors [rather than market makers] in the securities markets.
When a doctor buys any security – he is said to be taking a long position in that security. This means the investor is an owner of the security. Why does a doctor take a long position in a security? Well, receiving dividend income to make a profit from an increase in the market price is one reason. Once the security has risen sufficiently in price to satisfy the investor’s profit needs, the investor will liquidate his long position, or sell his stock. This would officially be known as a long sale of stock, though few people in the securities business use the label “long sale”. This is the manner in which the above investor had made a profit is the traditional method used; buy low, sell high.
Let’s look at an actual investment in General Motors to investigate this principle further. A medical investor has taken a long position in 100 shares of General Motors stock at a price of $70 per share. This means that the manner in which he can do that is by placing a market order which will be executed at the best “available market price at the time, or by the placing of a buy limit order with a limit price of $70 per share. The investor firmly believes, on the basis of reports that he has read about the automobile industry and General Motors specifically, that at $70 a share, General Motors is a real bargain. He believes that based on its current level of performance, it should be selling for a price of between $80 and $85 per share. But, the doctor investor has a dilemma. He feels certain that the price is going to rise but he cannot watch his computer, or call his broker, every hour of every day. The reason he can’t watch is because patients have to be seen in the office. The only people who watch a computer screen all day are those in the offices of brokerage firms (stock broker registered representatives), and doctor day traders, among others.
In the above example, with a sell limit order, if the doctor investor was willing to settle for a profit of $12 per share, what order would he place at this time? If you said, “sell at $82 good ’til canceled”, you are correct. Why GTC rather than a day order? Because our doctor investor knows that General Motors is probably not going to rise from $70 to $82 in one day. If he had placed an order to sell at $82 without the GTC qualification, his order would have been canceled at the end of this trading day. He would have had to re-enter the order each morning until he got an execution at 82. Marking the order GTC (or open) relieves him of any need to replace the order every morning. Several weeks later, when General Motors has reached $82 per share in the market, his order to sell at 82 is executed. The medical investor has bought at 70 and sold at 82 and realized a $12 per share profit for his efforts.
Let’s suppose that the medical investor, who has just established a $12 per share profit, has evaluated the performance of General Motors common stock by looking at the market performance over a period of many years. Let’s further assume that the investor has found by evaluating the market price statistics of General Motors that the pattern of movement of General Motors is cyclical. By cyclical, we mean that it moves up and down according to a regular pattern of behavior.
Let’s say the investor has observed that in the past, General Motors had repeated a pattern of moving from prices in the $60 per share range as a low, to a high of approximately $90 per share. Further, our investor has observed that this pattern of performance takes approximately 10 to l2 months to do a full cycle; that is, it moves from about 60 to about 90 and back to about 60 within a period of roughly l2 months. If this pattern repeats itself continually, the investor would be well advised to buy the stock at prices in the low to mid 60’s hold onto it until it moves well into the 80’s, and then sell his long position at a profit. However, what this means is that our investor is going to be invested in General Motors only 6 months of each year. That is, he will invest when the price is low and, usually within half a year, it will reach its high before turning around and going back to its low again. How can the doctor-investor make a profit not only on the rise in price of General Motors in the first 6 months of the cycle, but on the fall in price of General Motors in the second half of the cycle? One technique that is available is the use of the short sale.
The Short Sale
If a doctor investor feels that GM is at its peak of $ 90 per share, he may borrow 100 shares from his brokerage firm and sell the 100 shares of borrowed GM at $ 90. This is selling stock that is not owned and is known as a short sale. The transaction ends when the doctor returns the borrowed securities at a lower price and pockets the difference as a profit. In this case, the doctor investor has sold high, and bought low.
Odd Lots
Most of the thousands of buy and sell orders executed on a typical day on the NYSE are in 100 share or multi-100 share lots. These are called round lots. Some of the inactive stocks traded at post 30, the non-horseshoe shaped post in the northwest corner of the exchange, are traded in 70 share round lots due to their inactivity. So, while a round lot is normally 700 shares, there are cases where it could be 10 shares. Any trade for less than a round lot is known as an odd lot. The execution of odd lot orders is somewhat different than round lots and needs explanation.
When a stock broker receives an odd lot order from one of his doctor customers, the order is processed in the same manner as any other order. However, when it gets to the floor, the commission broker knows that this is an order that will not be part of the regular auction market. He takes the order to the specialist in that stock and leaves the order with the specialist. One of the clerks assisting the specialist records the order and waits for the next auction to occur in that particular stock. As soon as a round lot trade occurs in that particular stock as a result of an auction at the post, which may occur seconds later, minutes later, or maybe not until the next day, the clerk makes a record of the trade price.
Every odd lot order that has been received since the last round lot trade, whether an order to buy or sell, is then executed at the just noted round lot price, the price at which the next round lot traded after receipt of the customer’s odd lot order, plus or minus the specialist’s “cut “. Just like everything else he does, the specialist doesn’t work for nothing. Generally, he will add 1/8 of a point to the price per share of every odd lot buy order and reduce the proceeds of each odd lot sale order by 1/8 per share. This is the compensation he earns for the effort of breaking round lots into odd lots. Remember, odd lots are never auctioned but, there can be no odd lot trade unless a round lot trades after receipt of the odd lot order.
Leveraged ETFs have received tremendous media attention and are proving to be extremely popular with both individual and institutional investors. There are hundreds of leveraged ETFs, covering virtually every asset class and industry sector. The majority are double-leveraged, but there’s a sizeable group of triple-leveraged ETFs.
For professional investors, leveraged ETFs are useful in statistical arbitrage, short-term tactical strategies, and for use as short-term hedges without the need to roll futures. For individual investors, leveraged ETFs are alluring because of the potential for higher returns.
Now, some physicians and Uninformed investors might assume that the leverage returns are generated on a continuous basis, so that if an underlying index is up 5% for a month, the double-leveraged ETF will be up 10% for the same month; if the index is up 10% for 6 months, the ETF will be up 20%, and so forth. That is absolutely not the case. The leverage is determined on a daily basis and the returns for any other period usually will not be double or triple the underlying index.
In order for the leveraged funds to achieve appropriate levels of assets so they can provide their implied leverage, they have to rebalance daily. In the case of an ETF providing long 2-times leveraged exposure, they would typically attain exposure to a notional set of assets equal to 2 times their NAV.
Example: An example would be an ETF that takes in 100 units in assets that does a swap with a counterparty to provide exposure to 200 units in performing assets. The rebalancing activity of these funds will almost always be in the same direction as the market.
In essence, a leveraged ETF is essentially marked to market every night. It starts with a clean slate the next day, almost as if the previous day had not existed. This process produces daily leverage results. However, over time, the compounding of this reset can potentially vary the performance of the fund versus its underlying benchmark. This can result in either greater or lesser degrees of final leverage over individual holding periods.
Incorporating a practice is something many doctors are unaware but at Marcinko Associates, Inc., we are here to help you in getting your medical practice or clinical business up and running. We believe this category is by far the most important when acquiring or starting a new practice as well as a continuing practice. Selecting a business entity that will be the most conducive to your overall clinic or medical practice objectives is vital.
For example, clinic or medical business entity selection would include: Sole Proprietorship, Limited Liability Company, S-Corporation, C-Corporation, Professional Association or Non-profit organization.
Financial ratio analysis typically involves the calculation of ratios that are financial and operational measures representative of the financial status of a clinic or medical practice enterprise. These ratios are evaluated in terms of their relative comparison to generally established industry norms, which may be expressed as positive or negative trends for that industry sector. The ratios selected may function as several different measures of operating performance or financial condition of the subject entity.
Common types of financial indicators that are measured by ratio analysis include:
Liquidity. Liquidity ratios measure the ability of an organization to meet cash obligations as they become due, i.e., to support operational goals. Ratios above the industry mean generally indicate that the organization is in an advantageous position to better support immediate goals. The current ratio, which quantifies the relationship between assets and liabilities, is an indicator of an organization’s ability to meet short-term obligations. Managers use this measure to determine how quickly assets are converted into cash.
Activity. Activity ratios, also called efficiency ratios, indicate how efficiently the organization utilizes its resources or assets, including cash, accounts receivable, salaries, inventory, property, plant, and equipment. Lower ratios may indicate an inefficient use of those assets.
Leverage.Leverage ratios, measured as the ratio of long-term debt to net fixed assets, are used to illustrate the proportion of funds, or capital, provided by shareholders (owners) and creditors to aid analysts in assessing the appropriateness of an organization’s current level of debt. When this ratio falls equal to or below the industry norm, the organization is typically not considered to be at significant risk.
Profitability. Indicates the overall net effect of managerial efficiency of the enterprise. To determine the profitability of the enterprise for bench marking purposes, the analyst should first review and make adjustments to the owner(s) compensation, if appropriate. Adjustments for the market value of the “replacement cost” of the professional services provided by the owner are particularly important in the valuation of professional medical practices for the purpose of arriving at an ”economic level” of profit.
The selection of financial ratios for analysis and comparison to the organization’s performance requires careful attention to the homogeneity of data. Bench marking of intra-organizational data (i.e., internal bench marking) typically proves to be less variable across several different measurement periods.
However, the use of data from external facilities for comparison may introduce variation in measurement methodology and procedure. In the latter case, use of a standard chart of accounts for the organization or recasting the organization’s data to a standard format can effectively facilitate an appropriate comparison of the organization’s operating performance and financial status data to survey results.
In Part 1, we discussed how to establish fair market value (FMV) for a medical practice in the article, “Establish Your Practice’s Fair Market Value.” This time, we’ll review important terms and conditions for the sale acquisition and transaction.
Unfortunately, as a general rule, medical practice worth is presently deteriorating. A good medical practice is no longer a good business necessarily, and selling doctors can no longer automatically expect to extract a premium sale price. Nevertheless, appraising your medical practice on a periodic basis can play a key role in obtaining maximum value for it.
Competent practice valuation specialists typically charge a retainer to cover out-of-pocket expenses. Fees should not be based on a percentage of practice value, and may take 30-45 days to complete. Flat fees should be the norm because a sliding scale or percentage fee may be biased toward over-valuation in a declining marketplace. Fees range from $7,500-$50,000 for the small to large medical practice or clinic.
Expect to pay a retainer and sign a formal, professional engagement letter. Seek an unbiased and independent viewpoint. Buyer and sellers should each have their own independent appraisal done, using similar statistics, accounting measures, and economic assumptions.
At the Institute of Medical Business Advisors, Inc www.MedicalBusinessAdvisors.com we use three engagement levels that vary in intensity, purpose, and cost:
1. A comprehensive valuation provides an unambiguous value range. It is supported by most all procedures that valuators deem relevant, with mandatory onsite review. This gold standard is suitable for contentious situations. A written “opinion of value” is applicable for litigation support activities like depositions and trial. It is also useful for external reporting to bankers, investors, the public, Internal Revenue Service (IRS), etc.
2. A limited valuation lacks additional suggested Uniform Standards of Professional Appraisal Practice (USPAP) procedures. It is considered to be an “agreed upon engagement,” when the client is the only user. For example, it may be used when updating a buy/sell agreement, or when putting together a practice buy-in for a valued associate. This limited valuation would not be for external purposes, so no onsite visit is necessary and a formal opinion of value is not rendered.
3. An ad-hoc valuation is a low level engagement that provides a gross non-specific approximation of value based on limited parameters or concerns involved parties. Neither a written report nor an opinion of value is rendered. It is often used periodically as an internal organic growth/decline gauge.
Structure Sales Transactions and Acquisitions
When the practice price has been determined and agreed on, the actual sales deal can be structured in a couple of ways:
(1) Stock Purchase v. Asset Purchase
In an asset transaction, the buyer will receive a tax amortization benefit associated with the intangible value of the business. This tax amortization represents a non-cash expense benefiting the buyer. In this case, the present value of those future tax benefits is added to the business enterprise value.
(2) Corporate Transactions
Typical private deals in the past involved some multiple (ratio) of earning before income taxes (EBIT)—usually a combination of cash, restricted stock, notes receivable, and possibly assumption of liabilities. For some physician hospital organizations, and public deals, the receipt of common stock can increase the practice price by as much as 40-50 percent (to accept the corresponding business risk, in lieu of cash).
Complete the Deal
The deal structure will vary depending on whether the likely buyer is a private practitioner, health system or a corporate partner. Some key issues to consider in the “art of the deal” include:
Working capital (in or out?): Including working capital in the transaction will increase the sale price.
Stock vs. asset transaction: Structuring the deal as an asset purchase will increase practice value due to the tax amortization benefits received by the buyer for intangible assets of the practice.
Common stock premium: The total sale price can be significantly higher than a cash equivalent price for accepting the risk and relative illiquidity of common stock as part of the payment.
Physician compensation: If your goal is to maximize practice value, take home a lower salary to increase practice sale price. The reverse is also true.
Understand Private Deal Structure
Assuming a practice sale is a private transaction, deal negotiations are based on the following pricing methodologies:
Seller financing: Many transactions involve an earn-out arrangement where the buyer puts money down and pays the balance under a formula based on future revenues, or gives the seller a promissory note under similar terms. Seller financing decreases a buyer’s risks (the longer the terms, the lower the risk). Longer terms demand premiums, while shorter terms demand discounts. Premiums that buyers pay for a typical seller-financed practice are usually more than what you would expect from a simple time value of money calculation, as a result of buyer risk reduction from paying over time, rather than up front with a bank loan or all cash. Remember to obtain a life insurance policy on the buyer.
Down payment: The greater the down payment for acquisition of a medical practice, the greater the risk is to the buyer. Consequently, sellers who will take less money up front can command a higher than average price for their practice, while sellers who want more down usually receive less in the end.
Taxation: Tax consequences can have a major impact on the price of a medical practice. For instance, a seller who obtains the majority of the sales price as capital gains can often afford to sell for a much lower price and still pocket as much or more than if the sales price were paid as ordinary income. Value attributed to the seller’s patient list, medical records, name brand, good will, and files qualifies for capital gains treatment. Value paid for the selling doctor’s continuing assistance after the sale and value attributed to a non-compete agreement are taxed at ordinary income. A buyer willing to allocate more for items with capital gains treatment, or a seller willing to take more in ordinary income, can frequently negotiate a better price. This is the essence of economically prudent practice transition planning.
Sidestep Common Buyer Blunders
Here are 10 blunders to avoid, as a buyer:
1. Believing the selling doctor’s attestations. Always verify data through an independent appraisal.
2. Wanting to change the culture of the practice. Be careful: Patients may not adjust quickly to change.
3. Using all available cash without keeping a reserve for potential contingencies.
4. Creating a conflict with the seller by recognizing a weakness and continually focusing on it for a bargain price.
5. Failing to realize that managed care plan contracts can be lost quickly or may not be always transferable.
6. Suffering from analysis paralysis. Money cannot be made by continually checking out a medical practice, only by actually running one.
7. Not appreciating the uniqueness of each practice, and using inaccurate “rules of thumb” from the golden age of medicine.
8. Not realizing that practice worth and goodwill value have plummeted lately and continue to decline in most parts of the country.
9. Not understanding that practice brokers may play both sides of the buy/sell equation for profit. Brokers usually are not obligated to disclose conflicts of interest, are not fiduciaries, and do not provide testimony as a court-approved expert witness.
10. Not hiring an appraisal professional who will testify in court, if need be, using the IRS-approved USPAP methods of valuation. Always assume that the appraisal will be contested (many times, it is).
After pricing and contracting due diligence has been performed, the next step in the medical practice sale process—as Donald Trump might say—is just good, old-fashioned negotiation.
Cimasi, R.J., A.P. Sharamitaro, T.A. Zigrang, L.A.Haynes. Valuation of Hospitals in a Changing Reimbursement and Regulatory Environment. Edited by David E. Marcinko. Healthcare Organizations: Financial Management Strategies. Specialty Technical Publishers, 2008.
Marcinko, D.E. “Getting it Right: How much is a plastic surgery practice really worth?” Plastic Surgery Practice, August 2006.
Marcinko, D.E., H.R. Hetico. The Business of Medical Practice (3rd ed). Springer Publishing,New York,N.Y., 2011.
Marcinko, D.E. and H.R. Hetico. Risk Management and Insurance Planning for Physicians and Advisors. Jones and Bartlett Publishers, Sudbury, Mass., 2007.
Marcinko, D.E. and H.R. Hetico. Financial Planning for Physicians and Advisors. Jones and Bartlett Publishers, Sudbury, Mass., 2007.
Marcinko, D.E. and H.R. Hetico. Dictionary of Health Insurance and Managed Care. Springer Publishers, New York, N.Y., 2007.
Marcinko, D.E. and H.R. Hetico. Dictionary of Health Economics and Finance. Springer Publishers,New York,N.Y., 2007.
There are a Myriad of Reasons for Obtaining a Medical Practice Valuation and Appraisal Engagement:
Outright selling-buying
Partnership and Associate buy-in / buy-out
Mergers and Acquisitions
Organic growth tracking
Hospital integrations
Private and public reporting
Financing and Venture Capital
Estate and tax planning
Our Capability
We have the ability to provide extensive analysis of value components in healthcare practices and provide appraisals based on business, economic, and market conditions. This involves detailed examination of financials and clinical data in the context of numerous factors including medical specialty, physician supply and demand, payer mix, regulatory environment, regional dynamics, and risk premium.
According to colleagues Jeffrey S. Coons PhD CFA, the Efficient Market Hypothesis (EMH) states that securities are fairly priced based on information about their underlying cash flows and that physician investors should not expect to consistently outperform the market over the long-term.
There are three distinct forms of EMH that vary by the type of information that is reflected in a security’s price:
Weak Form: This form holds that investors will not be able to use historical data to earn superior returns on a consistent basis. In other words, the financial markets price securities in a manner that fully reflects all information contained in past prices.
Semi-Strong Form: This form asserts that security prices fully reflect all publicly available information. Therefore, investors cannot consistently earn above normal returns based solely on publicly available information, such as earnings, dividend, and sales data.
Strong Form: This form states that the financial markets price securities such that, all information (public and non-public) is fully reflected in the securities price; investors should not expect to earn superior returns on a consistent basis, no matter what insight or research they may bring to the table.
While a rich literature has been established for doctors regarding to test whether EMH actually applies in any of its three forms in real world markets – probably the most difficult evidence to overcome for backers of EMH is the existence of a vibrant money management and mutual fund industry charging value-added fees for their services.
In fact, no less than Warren Buffett has suggested that the markets are decidedly not efficient.
A common stock is the least senior of securities issued by a company.
A preferred stock, in contrast, is slightly more senior to common stock, since dividends owed to the preferred stockholders should be paid before distributions are made to common stockholders.
However, distributions to preferred stockholders are limited to the level outlined in the preferred stock agreement (i.e., the stated dividend payments). Like a fixed income security, preferred stocks have a specific periodic payment that is either a fixed dollar amount or an amount adjusted based upon short-term market interest rates.
However, unlike fixed income securities, preferred stocks typically do not have a specific maturity date and preferred stock dividend payments are made from the corporation’s after tax income rather than its pre-tax income. Likewise, dividends paid to preferred stockholders are considered income distributions to the company’s equity owners rather than creditors, so the issuing corporation does not have the same requirement to make dividend distributions to preferred stockholders.
So, preferred stock is generally referred to as a “hybrid” security, since it has elements similar to both fixed income securities (i.e., a stated periodic payments) and equity securities (i.e., shareholders are considered owners of the issuing company rather than creditors).
Convertible preferred stocks (and convertible corporate bonds) are also considered hybrid securities since they have both equity and fixed income characteristics. A convertible security whether a preferred stock or a corporate bond, generally includes a provision that allow the security to be exchanged for a given number of common stock shares in the issuing corporation. The holder of a convertible security essentially owns both the preferred stock (or the corporate bond) and an option to exchange the preferred stock (or corporate bond) for shares of common stock in the company.
ASSESSMENT: Thus, at times the convertible security may behave more like the issuing company’s common stock than it does the issuing company’s preferred stock (or corporate bonds), depending upon how close the common stock’s market price is to the designated conversion price of the convertible security.
According to Rick Kahler MS CFP® ChFC CCIM [www.KahlerFinancial.com] real estate is one of the largest asset classes in the world. The family home is the largest asset many middle-class Americans own. And, real estate makes up a significant portion of the net worth of many wealth accumulators. Directly owning real estate is not an investment for the faint of heart, the armchair investor, or the uneducated. Most wealth accumulators would do well to leave direct ownership of real estate to the pros and invest in real estate investment trusts (REITs) instead [personal communication].
Still, as we have seen, the lure of investing in a tangible asset like real estate is enticing for high risk tolerant physician-investors who need a sense of control and interaction with their investments. If you are among them, here are a few guidelines that may keep you on a profitable path.
1. Don’t attempt to purchase investment real estate without the help of a commercial real estate specialist who is a fiduciary bound to look out for your best interest. Engage a Certified Commercial Investment Member (CCIM) with years of training and experience in analyzing and acquiring investment real estate. To find a CCIM near you, go to http://www.ccim.com.
2. You will sign a disclosure agreement that will tell you who the Realtor represents. Be sure the Realtor you engage represents you and not the seller, both parties, or neither party.
3. Never trust the income and expense data provided by the seller’s Realtor. While a seller represented by a CCIM will have a greater chance of supplying you with accurate data, most will significantly understate expenses and overstate the capitalization rate. Selling Realtors often understate the average annual cost of repairs and maintenance. I estimate this annual expense at 10%.
4. Another often understated expense is management. Many owners manage their own properties, so the selling broker doesn’t include an estimate for management expenses. They should. Real estate doesn’t manage itself, ever. You will either need to hire professional management or do your own management (always a scary proposition). Even if you do it yourself, you have an opportunity cost of your time, so you must include a management fee in the expenses. Most small residential apartments and single-family homes will pay 10% of their rents to a manager.
5. You must verify all the costs presented to you by the seller’s Realtor. Demand copies of at least the last three and preferably five years of tax returns. Research items like utility bills, property taxes, legal fees, insurance costs and repairs, maintenance costs, replacement reserves, tax preparation and all management fees. As a rule of thumb, expenses will average 40% of rental income on average-aged properties where the tenants pay all utilities except water. Newer properties may have expenses as low as 35%, while older properties can be as high as 50%.
6. By subtracting the vacancy rate and stabilized expenses from the rent, you will find the net operating income. This is the income you will put in your pocket—assuming the property is paid for. By dividing the net operating income by the purchase price, you will find the return you will receive on your investment, called the capitalization or “cap” rate. In Rapid City SD, for example, the cap rate tends to be 4% for single-family homes, 5% to 8% for duplexes to eight-plexes, and 8% to 12% for larger residential and commercial properties.
ASSESSMENT: Yes, physician-investors and all of us can build wealth with real estate. You just need to educate yourself, work hard, start conservatively, think long-term, and be prepared for lean years. This is not a quick or easy path to riches. Your comments are appreciated. Thank You.
Posted on August 16, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
PHYSICIAN RETIREMENT PLANNING
By Staff Reporters
***
***
The rule of 25 is just a different way to look at another popular retirement rule, the 4% rule. It flips the equation (100/4% = 25) to emphasize a different part of the retirement planning process — withdrawing vs. saving.
The 4% rule outlines a safe rate to withdraw funds for 30 years without running out of money. On the other hand, the rule of 25 is a savings-focused approach, providing a quick estimate of how much you need to accumulate before exiting the workforce.
Let’s consider a scenario to highlight the difference:
Rule of 25: After accounting for her Social Security and other sources of retirement income, Dr. Matie PhD plans to spend $40,000 a year in retirement. 40,000 x 25 = $1 million, so Matie would need $1 million invested to cover annual expenses of $40,000.
The 4% rule: Dr. Matie, now a retiree, has $1 million in retirement savings and follows the 4% rule. She can safely withdraw $40,000 annually (4% of $1 million).
Long-Short is an active portfolio construction discipline that balances long positions in high expected return securities and short positions in low expected return securities of approximately equal value and market sensitivity. This type of portfolio is “neutralized” or immunized against changes in value of the underlying market and, therefore, has zero systematic (beta) risk. If the selected securities perform as expected, the long-short positions will provide a positive return, whether the market rises or falls.
Misconceptions
While long-short portfolios are often perceived and portrayed as much costlier and much riskier than long-only, it is inherently neither. Much of the incremental cost and risk is either largely dependent on the amount of leverage employed or controllable via optimization. Those costs and risks that are not controllable—financial intermediation costs of borrowing shares to short, the trading costs incurred to meet long-short balancing, margin requirements, uptick rules, and the risks of unlimited losses on short positions—do not invalidate the viability of long-short strategies.
Long-Short Advantages
Compared with long-only portfolios, long-short portfolios offer enhanced flexibility not only in the control of risk and pursuit of return, but also in asset allocation. Basic market-neutral portfolios achieve a return consisting of three components: (1) interest on funds held as a liquidity buffer, (2) interest on the short sale proceeds maintained with the broker, and (3) the return spread between the aggregate long and aggregate short positions in the portfolios.
Disadvantages
Share borrow-ability and uptick rules make short-selling more difficult and costly than going long. Also, it may be legally or contractually restricted for some investors, such as mutual funds. Inefficiencies may be concentrated in overpriced stocks and, accordingly, short sales of the most overpriced stocks may offer higher positive returns than long purchases of underpriced stocks.
Assessment
Long-only portfolios are confined to altering the weighting of securities within an index in order to realize an excess return. Long-short portfolios are not constrained by index weights and, because they can short securities, they can “underweight” a security by as much as investment insights and risk considerations dictate. Long-short portfolios can be enhanced by “equitizing” them using stock index futures.
Note: “The Long and Short on Long-Short” by Bruce I. Jacobs and Kenneth N. Levy, The Journal of Investing, Spring 1997, pp. 73–86, Institutional Investor, Inc.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
The stock markets have been near all time highs, lately. Physician colleagues and clients are so excited that they are even checking the overnight status of favorite stocks and/or the domestic/overseas markets.
Some colleagues are even becoming a bit OCD by checking the implied open of various markets the night before. But, what exactly is the Implied Open? How is it calculated?
DEFINITION: The Implied Open attempts to predict the prices at which various stock indexes will open, at 9:30am New York time. It is frequently shown on various cable television channels prior to the start of the next business day.
EXAMPLE: Considering the DJIA as an example, the basis of calculating implied open is the price of a “DJX index option futures contract”. This is not the price of the DJIA itself but rather the current ticker price of an option issued by the Chicago Board Options Exchange.
CBOE: The Chicago Board Options Exchange, located at 400 South LaSalle Street in Chicago, is the largest U.S. options exchange with annual trading volume that hovered around 1.27 billion contracts at the end of 2014. CBOE offers options on over 2,200 companies, 22 stock indices, and 140 exchange-traded funds.
NOTE: We would like to remind you that new amendments adopted by the U.S. Securities Exchange Commission (SEC) have gone into effect as of September 28, 2021. These amendments restrict the ability of market makers to publish OTC quotations for those companies that have not made required current financial and company information available to regulators and investors.
Investment fees matter. They can make a big difference to your financial health in the long run. Before you put money into any investment, it’s vital to uncover the real costs.They typically include these six types of fees:
1. An up-front commission earned by the salesperson or their firm. Don’t rely on a vague assurance or a verbal answer: get a specific number in writing.If you have trouble getting a number, ask, “If I buy this investment today and want to get out tomorrow, how much do I get back?” If the answer is not “all your money,” the difference is probably the upfront fees and commissions.
I don’t recommend purchasing financial products with significant upfront commission or costs. I have seen investments where these fees run as high as 30% of the money invested. If you were to earn 5% a year on the investment, it would take 8 years just to break even.
2. Ongoing advisory fees. These are monthly, quarterly, or annual fees you pay advisors for their investment advice and oversight. This includes working with you to pick the asset classes, set the diversification, select the managers, tax optimization, rebalancing, and other periodic tasks.
This fee can have many names including wrap fee or investment advisory fee. The normal “rule of thumb” is 1% of the assets the advisor is managing, although fees can range from 0 to 7%. This fee can be charged to you even if the advisor receives an upfront commission. It can be easy to see or hidden away in the fine print of the investment.
3. Additional fees for services. Find out specifically what services are included in the advisor fee. Additional fees for financial planning or ancillary services are rarely disclosed or discussed.
Services can range from minimal hand-holding only focused on your investments to comprehensive, holistic financial planning. Amazingly, there is no correlation between price and the breadth of services. That’s illogical, but the financial services industry gets away with this, in part because consumers don’t do their homework.
4. Ongoing fees charged by the managers of the specific funds or investment products. These fees are referred to as the fund’s expense ratio. This comes out of the profits generated by the manager, and it is one of the hardest fees to find. Only the most transparent advisor or salesperson will disclose it. It is incredibly well hidden; you will never see it in your brokerage statements or your advisor’s invoices. The only way to know the amount of this fee is to read the prospectus or some other third party analysis of the investment, like Morningstar.
These fees can vary greatly for the same investment, depending on the class of share you buy. For example, American Fund’s New Perspective Fund’s expense ratio ranges from0.45% to 1.54%. The average expense ratio of a mutual fund that invests in stocks is 1.35%. Conversely, the average expense ratio of a Vanguard S&P 500 fund is 0.10%. The difference of 1.25% is staggering over time.
5. Miscellaneous fees. These are also rarely talked about and hard to find. Many advisors charge $50 to $100 a year per account, hundreds of dollars to open or close an account, and even fees to dollar cost average your funds into the market.
6. Transaction fees. Every time you buy or sell a fund, a fee is typically paid to a custodian. These can range from $5 to hundreds of dollars per transaction.
Assessment
Remember, it’s your job to persist until you find out the total costs of an investment. Next week I’ll suggest ways to ask the tough questions about fees.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
Posted on August 9, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Almost 40,000 seniors will be forced to change Medicare Advantage plans after yet another insurer decides to exit markets over cost concerns. Centene Corp announced it would be ending its Medicare Advantage plans in at least six states this year as the company faces cost pressures.
Hanesbrands surged 18.17% in spite of sales sagging faster than the waistband of your favorite old pair of undies. Shareholders liked that the company has become more lean and efficient after selling its Champions brand.
SolarEdge Technologies fell 3.05% despite beating revenue forecasts, but its bottom line was weaker than expected.
JFrog tanked 27.52% after beating profit estimates, missing revenue estimates, and guiding for a much worse third quarter and fiscal year than expected.
Here’s where the major stock market benchmarks ended:
The SPX rose 119.81 points (2.3%) to 5,319.31; the Dow Jones Industrial Average® ($DJI) climbed 683.04 points (1.76%) to 39,446,49; the NASDAQ Composite® ($COMP) rose 464.21 points (2.9%) to 16,660.02.
The 10-year Treasury note yield (TNX) rose to just under 4%.
Posted on August 8, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
You might be affected by one of the biggest data breaches ever and not even know it. A recent class action lawsuit filed against Jerico Pictures Inc., a background check company that does business under the name National Public Data, claims that the company was breached by hackers earlier this year.
The SPX dipped 40.5 points (0.8%) to 5,199.5; the Dow Jones Industrial Average® ($DJI) fell 234.2 points (0.6%) to 38,763.45 the NASDAQ Composite ($COMP) fell 171 points (1.1%) to 16,195.8.
The 10-year Treasury note yield (TNX) rose to 3.96%.
Fortinet skyrocketed 25.30% after the cybersecurity company posted strong second-quarter earnings that only served to underline its potential as a CrowdStrike alternative.
Lumen Technologies continued to power higher, rising another 32.90% today as the investors poured money into the telecom due to its AI business boom.
Shopify tore 17.80% higher after posting a beat-and-raise earnings report highlighted by strong demand despite weak consumer spending.
Lyft drove 17.23% lower in spite of strong ridership in the second quarter. Shareholders, however, did not like management’s dour financial forecast for the third quarter.
CVS Health sank 3.19% after it slashed its profit guidance for the full year, though it also announced a new cost-cutting program.
TripAdvisor took a trip south today, falling 16.61% due to a mixed earnings report and dire warnings of lower revenue in the coming quarter.
Novo Nordisk sales thinned on Ozempic earnings miss. Shares of Danish pharmaceutical giant Novo Nordisk sank 8.27% today after the company missed expectations on its sales of popular weight-loss drugs Ozempic and Wegovy. Novo reported $1.7 billion in Wegovy sales, below the $2 billion analysts expected, while Ozempic sales came in $0.2 billion lower than analyst estimates. Overall, the company reported a net profit of $1.86 billion in the second quarter.
Posted on August 7, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Stock Marketsseesawed up yesterday, making back some of the ground lost to Monday’s sell-off. Analysts say the market could remain volatile until September, when the Fed is widely expected to cut interest rates—barring an emergency cut before then. One of the day’s big winners was Uber, which revved up after smashing Q2 revenue expectations thanks to unexpectedly strong consumer demand.
***
One day after the S&P 500’s worst session since 2022, stocks partially rebounded, putting fears of a recession on hold. Tuesday started well, with Japan’s Nikkei—which had cratered on Monday—logging its best day since 2008, giving US investors some positive energy From there, US stocks, including Magnificent Seven stalwarts like Microsoft and Nvidia, and both major cryptocurrencies, moved up. “Get used to the volatility,” one Bank of America analyst told Bloomberg. The S&P 500 is still up over 10% this year despite this week’s turbulence.
Finally, DuckDuckGo might soon get its time to shine. A federal judge just ruled that Google has a monopoly over the search engine business, creating the potential for curbs to its power that could change how you look up people you just met online. Google said it will appeal the ruling, but that’s just on one front. It faces another lawsuit questioning whether it abused its monopoly on online advertising technology.
The relative strength index (RSI) is a technical indicator used in the analysis of financial markets. It is intended to chart the current and historical strength or weakness of a stock or market based on the closing prices of a recent trading period. The indicator should not be confused with relative strength.
The RSI is classified as a momentum oscillator, measuring the velocity and magnitude of price movements. Momentum is the rate of the rise or fall in price. The relative strength RS is given as the ratio of higher closes to lower closes. Concretely, one computes two averages of absolute values of closing price changes, i.e. two sums involving the sizes of candles in a candle chart. The RSI computes momentum as the ratio of higher closes to overall closes: stocks which have had more or stronger positive changes have a higher RSI than stocks which have had more or stronger negative changes.
The RSI is most typically used on a 14-day time frame, measured on a scale from 0 to 100, with high and low levels marked at 70 and 30, respectively. Short or longer time frames are used for alternately shorter or longer outlooks. High and low levels—80 and 20, or 90 and 10—occur less frequently but indicate stronger momentum.
The relative strength index was developed by J. Welles Wilder and published in a 1978 book, New Concepts in Technical Trading Systems, and in Commodities magazine (now Modern Trader magazine) in the June 1978 issue. It has become one of the most popular oscillator indices.
The RSI provides signals that tell investors to buy when the security or currency is oversold and to sell when it is overbought.
RSI with recommended parameters and its day-to-day optimization was tested and compared with other strategies in Marek and Šedivá (2017). The testing was randomized in time and companies and showed that RSI can still produce good results; however, in longer time it is usually overcome by the simple buy-and-hold strategy.
When it comes to purchasing a medical practice, there are a variety of factors that one must consider in evaluating the worth of the practice. Assessing the value of a practice is fraught with potential landmines if one does not go into the process with a strong understanding of some key principles to medical practice valuation.
According to the Dictionary of Health Economics and Finance, practice valuation is the “formal process of determining the worth of healthcare or other medical business entity at a specific point in time and the act or process of determining fair market value.” Fair market value is defined as “ … the price at which a willing buyer will buy and a willing seller will sell an asset in an open free market with full disclosure.”
The Internal Revenue Service (IRS) Revenue Ruling 59-60 clearly states that fair market value “is essentially a future prophecy and must be based on facts available at the required date of appraisal.”
Unfortunately, one cannot directly observe the value of a medical practice as there are a number of underlying issues. Obviously, the buyer and seller are pursuing opposite objectives, and this reality is not necessarily conducive to facilitating clarity on those issues.
Accordingly, let us consider a few mistakes that are commonly made by physicians who are considering the purchase of a medical practice.
A Guide To The Myths And Realities Of Medical Practice Valuation
• Valuations are material representations providing a range of transferable worth. • Valuations are reproducible estimates based on economic assumptions. • Valuations are not “back of the envelope multiples” using specious benchmarks. • Valuations are defensible and should be “signed off” by the completing firm attesting to origination guidelines and in accordance with the Uniform Standards of Professional Appraisal Practice (USPAP) and IRS formats as needed. • Financial accounting value (book value) is not fair market value. • Professional valuators represent only one party. The buyer or seller-owner is the client. • Unbiased valuators do not provide financing or equity participation schemes.
Knowing The Distinctions Among Engagement Types
The Institute of Medical Business Advisors uses three levels that approximate engagement types for the industry. These levels are comprehensive valuation, limited valuation and ad-hoc valuation.
A comprehensive valuation is an extensive service designed to provide an unambiguous opinion of the value range. It is supported by all procedures that valuators deem relevant with mandatory onsite review. This gold standard is suitable for contentious situations like divorce, partnership dissolution, estate planning and gifting, etc. The written opinion of value is applicable for litigation support activities like depositions and trial. It is also useful for external reporting to bankers, investors, the public and IRS, etc.
A limited valuation lacks additional suggested USPAP procedures. It is considered to be an “agreed upon procedure,” which is used in circumstances in which the client is the only user. For example, one may use the limited valuation when updating a buy-sell agreement or when putting together a practice buy-in for a valued associate. This limited valuation would not be for external purposes. No onsite visit is needed. A formal opinion of value is not rendered.
An ad-hoc valuation is a low level engagement that provides a gross and non-specific approximation of value based on limited limited parameters or concerns by involved parties. Neither a written report nor an opinion of value is rendered. The ad-hoc valuation is often used periodically as an internal organic growth/decline gauge.
Are You Following Industry Standards And Rules?
Specifically, when it comes to USPAP transactions involving physician practices, the following points are implied by the industry and the IRS.
• Discounted cash flow analysis is the most relevant income approach and must be done on an “after-tax” basis. It generally produces a higher value but is costly, detail-oriented and time consuming. • Project practice collections based on reasonable assumptions for the practice and market, etc. • Physician compensation is based on market rates consistent with age, experience and productivity. • Majority (control) premiums and minority (lack of control) discounts are also to be considered. A majority premium is the amount paid to gain enough ownership to set policies, direct operations and make decisions for the practice. A minority discount for partial ownership does not allow this power. Thus, majority ownership is valuated higher than minority ownership purchase.
What About Personal Goodwill And Practice Goodwill?
Goodwill represents the difference between practice purchase price and the value of the net assets. Personal goodwill results from the charisma, skills and reputation of a specific doctor. These attributes accrue solely to the individual, are not transferable and cannot be sold. Personal goodwill has little or no economic value.
Transferable medical practice goodwill has value, may be transferred and is defined as the unidentified residual attributes that contribute to the propensity of patients and managed care contracts (and their revenue streams) to return in the future.
However, bear in mind that the Goodwill Registry, an older source used to determine the average percentage of revenue contributed to practice goodwill, has sparse to no podiatry input, may be dated for some specialties and leads to abnormally high values.
In addition to various multiple factors, one must also appreciate the impact of a changing environment and practice transfer in a local market, which can augment or blunt goodwill value. It is also important to determine whether patients or HMOs return because of true goodwill or are mandated to do so by contractual obligations.
Now to further confuse the issue, how each kind of goodwill is allocated in situations like divorce depends on state law. For example, some courts weigh in on the apportionment of both kinds of goodwill, other courts exclude both kinds of goodwill and other courts pursue a case-by-case approach.
Understanding ‘Excess Earnings Capitalization’ And Compensation Issues
Another way to determine goodwill value is through “excess earnings capitalization.” This economic method looks at the difference between salary and what you would have to pay a comparable doctor replacement.
As an example, when you subtract the numbers and divide the result by 20 percent, an important percentage referred to as the capitalization rate emerges. The final number gives a dollar value for practice goodwill. Courts seem to prefer this method in divorce situations because it tends to reflect a practice’s current value.
Regardless of the practice business model, physician compensation is inversely related to practice value. In other words, the more a doctor takes home in above average salary, the less the practice is generally worth and vice versa.
Emphasize Practice Specifics Over Benchmarks And Formulas
In the stable economic past, physicians may have used industry benchmarks as quick and inexpensive substitutes for professionally prepared valuations. However, this practice can be fraught with peril if challenged. The courts seem to frown on this simplistic and dated methodology. Moreover, generic benchmark formulas assume a financial statement reporting standard that just does not exist with contemporary professional valuations.
Therefore, almost every competitive issue that impacts value should be addressed with each practice engagement. This includes but is not limited to:
• contemporary dislocations by third parties, Medicare and commercial payers; • retail clinics and changes in supply/ demand and specialty trends; • the rise of ambulatory surgery centers, walk-in clinics and specialty hospitals; • outsourced care and medical tourism; • alterations in resource based-relative value units, ambulatory payment classifications (APCs), diagnosis-related groups (DRGs) and newer Medicare-severity diagnosis-related groups (MS-DRGs); and • the Medicare Modernization Act, HIPAA, OSHA, the EEOC and other regulations.
One must also consider the impact of current employee trends to high-deductible health care plans and private concierge medicine. Another consideration is employer shifts away from defined benefits plans to defined contribution plans.
Aggregating Or ‘Normalizing’ Financial Information: What You Should Know
In addition to possibly conducting employee interviews, one must gather appropriate financial information in order to properly value a practice. As a starting point, interested physician buyers should be able to see the following information for the most recent three-year period.
It is especially important to eliminate one-time, non-recurring practice expenses. These are adjusted for excessive or below normal expenses on the profit and loss statement. Such “normalization” can produce a big surprise for benchmark proponents and formula-driven advocates when a selling doctor runs personal expenditures through the practice that a buyer or court would not consider legitimate. Of course, one is less likely to encounter such shenanigans when the valuation is conducted according to professional USPAP and IRS style guidelines.
For example, we recall one doctor who painted his home and wrote it off as a valid business expense. Deleting other major expenses such as country club memberships make a practice look more profitable. This is good news if you are selling it. It is bad news if you are getting a divorce.
Conversely, you may have to defend legitimate business expenses that an appraiser may seek to normalize. For example, doctors may pay for a vehicle through their practice. If they use the vehicle to travel between multiple offices and hospitals, the expense may be legitimate.
Also realize that the appraiser may also add expenses that have not been incurred. For example, the appraiser may add an office manager’s salary if your spouse is in that role for free. This produces a lower appraised value and is common in small podiatry practices. Honorarium is another example that does not figure into value calculations.
Of course, normalization is a sophisticated and time intensive process. However, the expert earns his or her professional fee, and defends the resulting valuation range when challenged.
Keys To Selecting The Right Valuator Professional
The most important credentials to look for are fiduciary level experience, specificity and independence. Some doctors mistakenly turn to those who may have never appraised a practice before. Just because an appraiser has initials behind his or her name, it does not mean he or she understands the peculiarities of medical specialties. Agents, brokers, solicitors and other intermediaries are not fiduciaries.
Physicians looking to assess a practice for possible sale/purchase should only select an independent health economist, who will be your advocate under Securities Exchange Commission (SEC), IRS or other relevant managerial accounting guidelines.
Moreover, be very wary if the valuation is not done in an independent manner or, worse, performed for both parties simultaneously.
Essential Insights On Professional Fees And What You Can Expect
Of course, it is almost impossible to answer concerns regarding fees without specific information. The cost of a valuation can range from $0 to $50,000 for an onsite team of experts for behemoth practices and ambulatory surgery centers. Keep in mind that in most cases you want to ensure the value determination will stand up to IRS scrutiny so the $0 rule of thumb approach is not an option.
However, most reputable firms use a blended fee schedule of fixed and hourly rates (plus expenses). Internists should expect to spend approximately $5,000 to $10,000 for an average sized practice and a limited appraisal that is completely suitable for most internal activities.
External appraisals or poorly aggregated financial information, onsite reviews and litigation support services incur additional costs. However, most doctors find the money well spent. Expect to pay a retainer and sign a formal professional engagement letter.
Finally, once the practice price is agreed upon, sales contract terms and agreements present a plethora of financing challenges for both parties to consider. For example, one must negotiate bank loans (if they are even available), payment rates and length, personal promissory guarantees, down payment offsets, earn-out arrangements and Uniform Commercial Codes.
Final Notes
Do not be surprised if a sales broker does not consider the aforementioned issues as the modern health era emerges. Most agent-appraisers are predominantly concerned with earning commissions by working both transaction parties and may not represent your best interests. Also be aware that they are usually not obliged to disclose conflicts of interest and do not provide testimony as a court approved expert witness.
However, it is a fait accompli that medical practice worth is presently deteriorating. As the population ages and third-party reimbursements plummet, doctors are commoditized and traditional retail medicine is replaced by more efficient wholesale business models like workplace health clinics. The subprime mortgage default fiasco, credit freeze, potential tax reform law expiration, the ACA, VBC, capitation payments and the political specter of a nationalized healthcare system only add fuel to the macroeconomic fires of uncertainty. Do not forget the corona pandemic.
As a result, a good medical practice is no longer good business necessarily and retiring doctors can no longer automatically expect to extract premium sales prices. Moreover, uninformed young physicians should not be goaded to overpay.
Posted on July 26, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Here’s where the major stock market benchmarks ended:
The S&P 500® index (SPX) fell about 28 points (0.5%) to 5,399.22; the Dow Jones Industrial Average® ($DJI) rose 81 points (0.2%) to 39,935.07; the NASDAQ Composite ended 161 points lower (0.9%) at 17,181.72.
The 10-year Treasury note yield (TNX) dropped four basis points to 4.255%.
The CBOE Volatility Index® (VIX)declined 0.6% to 17.94.
What’s up
IBM popped 4.36% after it crushed earnings expectations thanks to high AI bookings.
Tesla recovered 1.97% after yesterday’s terrible day as investors continue to digest a mixed earnings report.
ServiceNow soared 13.19% thanks to a strong earnings report that solidified the software company’s position as beneficiary of the AI trade.
Airline stocks flew higher today thanks to good news from two big players. Southwest Airlines ascended 5.64% on better-than-expected earnings, while American Airlines rose 4.23% in spite of issuing a profit warning for the coming quarter.
Ford plummeted 18.40% for the automaker’s worst day of trading since 2009 after it missed profit expectations and provided no positive forecast for the quarters ahead.
Royal Caribbean sank 7.61% after the company indicated that it’s facing a slowdown in demand.
Edwards Lifesciences crashed 31.27% thanks to a mixed earnings report, as well as management’s guidance that sales for its key heart valve replacement therapy will sink next quarter.
Thousands of seniors are losing coverage at local hospitals as problems plague Medicare Advantage. Lower payout rates for Medicare and Medicaid are sparking insurance companies to leave certain areas and change coverage options across the country.
Posted on July 22, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
MEDICAL EXECUTIVE-POST–TODAY’SNEWSLETTERBRIEFING
***
Essays, Opinions and Curated News in Health Economics, Investing, Business, Management and Financial Planning for Physician Entrepreneurs and their Savvy Advisors and Consultants
“Serving Almost One Million Doctors, Financial Advisors and Medical Management Consultants Daily“
A Partner of the Institute of Medical Business Advisors , Inc.
Shares of Charles Schwab (NYSE: SCHW) fell over 15% last week, according to data from S&P Global Market Intelligence. One of the largest brokerages posted slow growth and poor earnings as the company deals with low-yielding assets on its balance sheet. As of 1:31 p.m. ET on Friday, July 19th, Charles Schwab stock was down 17.5% this week.
Markets: The S&P 500 logged its worst week since April as investors pulled back from Big Tech stocks. CrowdStrike fell because causing a global IT outage is not good (more on that in a sec).
In a recent video, finance YouTuber Lena Petrova highlighted the troubling financial state of U.S. banks as they report significant losses and increase their reserves to cover a surge in loan delinquencies. With the second quarter results rolling in, it’s evident that the banking sector is under considerable strain.













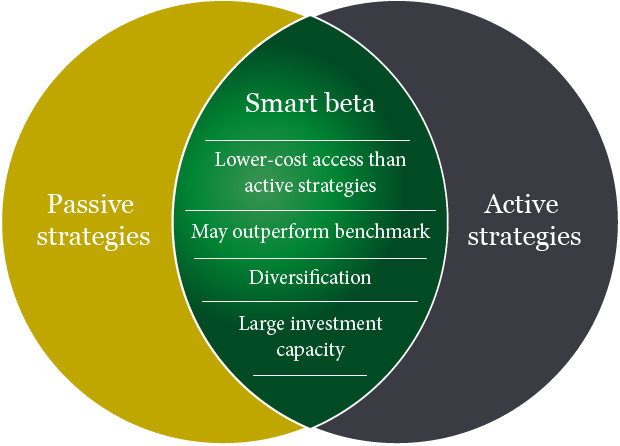

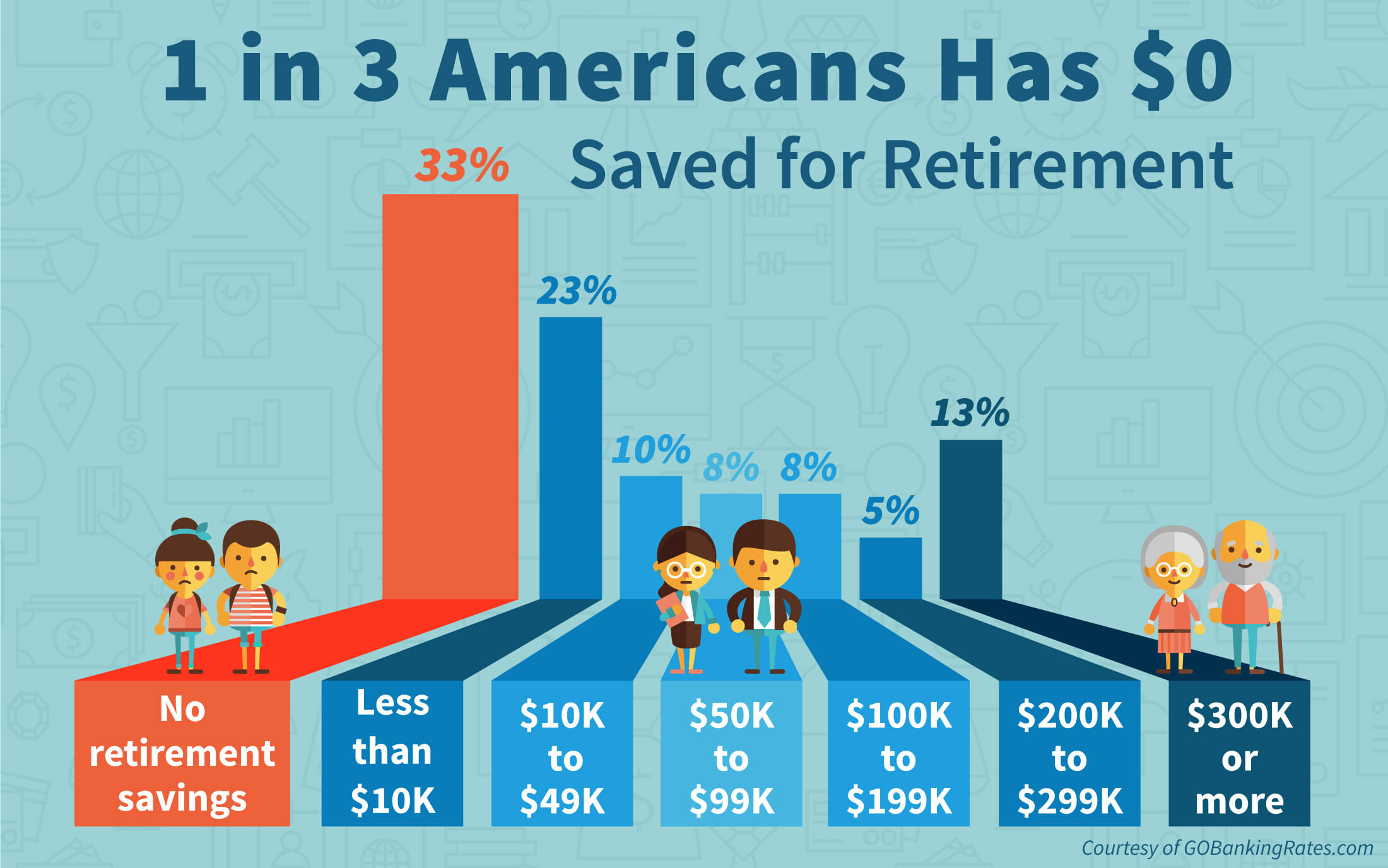
























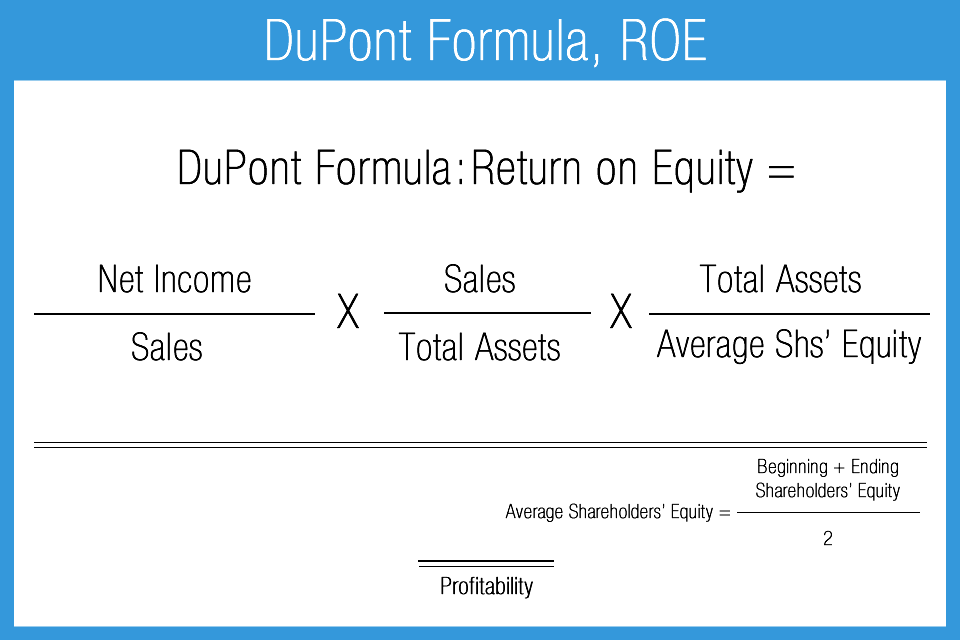














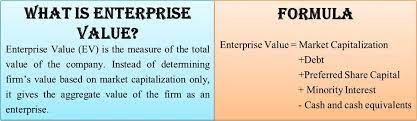
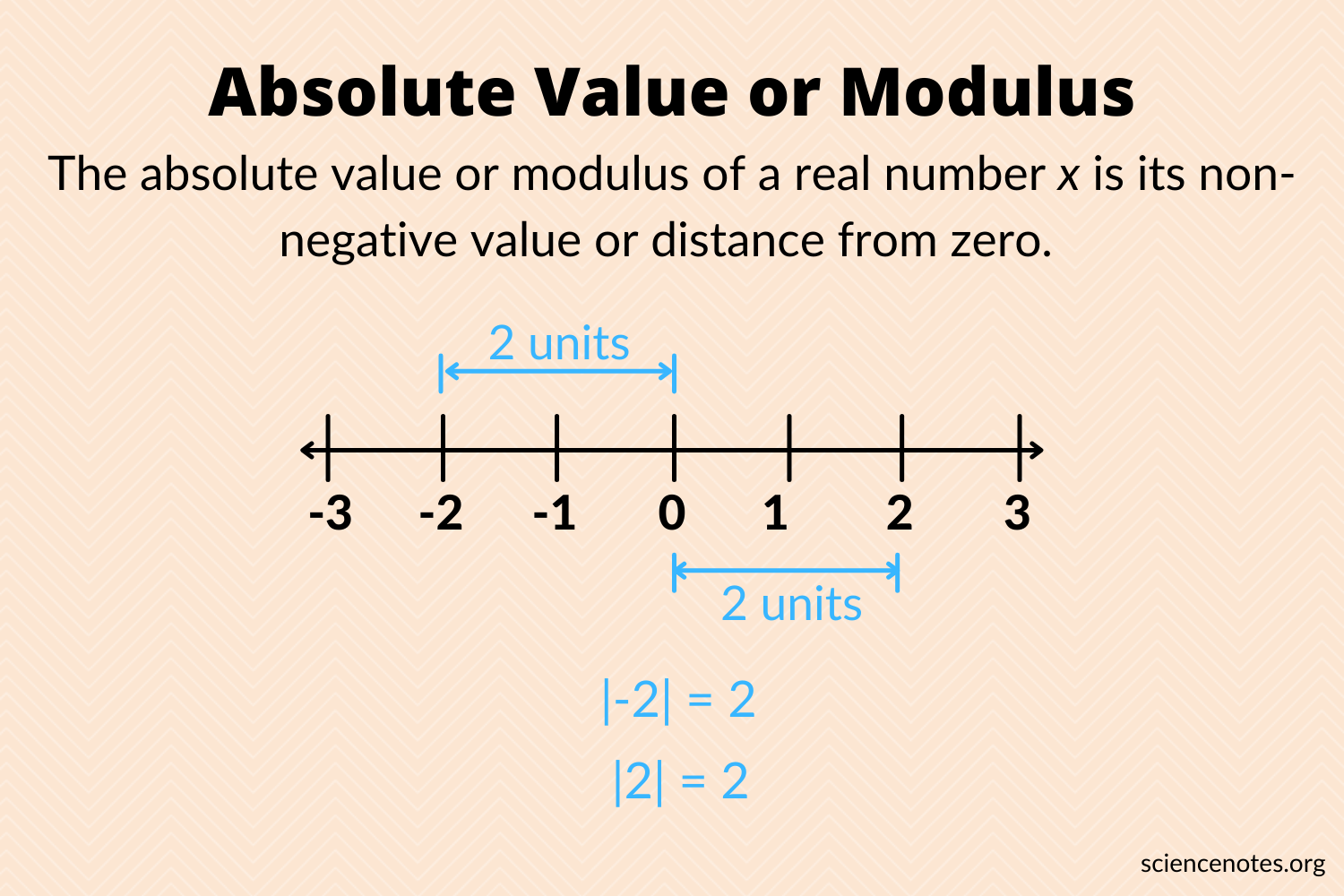

















































 DR. DAVID EDWARD MARCINKO MBA MEd CMP™
DR. DAVID EDWARD MARCINKO MBA MEd CMP™












