

Medicare cuts by specialty 1/1/2021
***

***

Share this:

Filed under: Health Economics, Health Insurance, Health Law & Policy | Tagged: medicare, Medicare cuts by specialty | Leave a comment »
ME-P SYNDICATIONS:
WSJ.com,
CNN.com,
Forbes.com,
WashingtonPost.com,
BusinessWeek.com,
USNews.com, Reuters.com,
TimeWarnerCable.com,
e-How.com,
News Alloy.com,
and Congress.org

![]()
![]()



BOARD CERTIFICATION EXAM STUDY GUIDES
Lower Extremity Trauma
[Click on Image to Enlarge]
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
![]()


 ePodiatryConsentForms.com
ePodiatryConsentForms.com
 “Providing Management, Financial and Business Solutions for Modernity”
“Providing Management, Financial and Business Solutions for Modernity”


Medicare cuts by specialty 1/1/2021
***
***
Filed under: Health Economics, Health Insurance, Health Law & Policy | Tagged: medicare, Medicare cuts by specialty | Leave a comment »
By Staff Reporters
***

***
The World Health Organization declared the outbreak of monkeypox to be a public health emergency of international concern. “The global monkeypox outbreak represents a public health emergency of international concern,” WHO Director-General Dr. Tedros Adhanom Ghebreyesus said during a briefing in Geneva. At the virtual press conference, Ghebreyesus also said that the outbreak has spread around the world “rapidly” and that officials understand “too little” about the disease.
And, the U.S. Dollar had an incredible run throughout 2022, appreciating against most major currencies as the world’s central banks continue to combat rising inflation. This year alone, the dollar is up 15% against the Japanese yen, 10% against the British pound, and 5% compared to China’s Renminbi. The Wall Street Journal’s Dollar Index, which measures the dollar against 16 other major currencies, has also had its best first half performance since 2010 this year, rising more than 10% year-to-date. And for the lucky Americans who could find cheap airfare to Europe (and made it through with all their luggage), the dollar even reached equal standing with the euro for the first time in two decades earlier this month.
***
CITE: https://www.r2library.com/Resource/Title/082610254
COMMENTS APPRECIATED
Thank You
***
Filed under: Accounting, Glossary Terms, Health Insurance, Health Law & Policy, Investing, Taxation | Tagged: dollar, Ghebreyesus, renminbi, US Dollar, WHO, Yen | Leave a comment »
***
Cigna, do you even have a clue that dentists don’t like you?
***

By Darrell K. Pruitt DDS
***
Hi Dr. Pruitt,
I’m truly sorry for any negative experience you’ve encountered with us. Is there a claim, benefit, or authorization concern I can help with? Please email me at LetUsHelpU@cigna.com. I’d like an opportunity to assist.
At a time when interest rates are surging, and just when I request an increase, CIGNA REDUCED MY REIMBURSEMENTS! Never again will I do business with you, and will discourage other dentists from falling into your trap …. And that is why dentists don’t like #TeamCigna.
What is your name, anyway. You know mine. Perhaps Linkedin’s transparency makes it a poor choice for marketing Cigna.
As if things could get no worse between Cigna and dentists, you censored my response!
NOTE: Cigna representatives prefer to remain anonymous for reasons of accountability.
***
COMMENTS APPRECIATED
Thank You
***
BUSINESS MEDICINE: https://www.amazon.com/Business-Medical-Practice-Transformational-Doctors/dp/0826105750/ref=sr_1_9?ie=UTF8&qid=1448163039&sr=8-9&keywords=david+marcinko
Health Insurance: https://www.amazon.com/Dictionary-Health-Insurance-Managed-Care/dp/0826149944/ref=sr_1_4?ie=UTF8&s=books&qid=1275315485&sr=1-4
***
Filed under: "Doctors Only", Career Development, Ethics, Health Insurance, Health Law & Policy, Industry Indignation Index, Managed Care, Op-Editorials, Pruitt's Platform | Tagged: Cigna, Darrell Pruitt, Pruitt | Leave a comment »
***
By Health Capital Consultants, LLC
***

***
Biden Administration to Overhaul Vertical Merger Guidelines
The U.S. healthcare industry has seen a rise in vertical integration transactions since the passage of the ACA, especially among physician groups integrating with health systems or insurers, as providers seek to fill gaps in their continuum of care. In response to these trends and resulting market imbalances, the Biden Administration is aggressively pursuing antitrust enforcement by updating and revising U.S. antitrust law guidance.
This Health Capital Topics article will discuss the vertical integration movement and the proposed changes to antitrust laws that may affect the future of healthcare. (Read more…)
***
CITE: https://www.r2library.com/Resource/Title/0826102549
***
COMMENTS APPRECIATED
Thank You
***
Filed under: Experts Invited, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, iMBA, Inc., Investing, Professional Liability, Research & Development | Tagged: ACA, Biden, Biden Administration to Overhaul Vertical Merger Guidelines, Health Capital Consultants LLC, Vertical Integration, Vertical Merger Guidelines | Leave a comment »
![]()
Emerging Problems
By Dr. David Edward Marcinko; MBA, CMP™
[Publisher-in-Chief]
According to the Dictionary of Health Insurance and Managed Care, informed consent is the oral and written communication process between a patient and physician that results in the agreement to undergo a particular procedure, surgical intervention or medical treatment.
Unfortunately, a lack of standardization surrounding this process represents a major risk for patients and surgeons, and may lead to inaccurate patient expectations, lost or incomplete consent forms, missing encounter documentation and delays in critical surgeries and procedures.
History: Render S. Davis of Emory University [2008 recipient of the Health Care Ethics Consortium’s Heroes in Healthcare Ethics Award] writes for us in the Business of Medical Practice www.MedicalBusinessAdvisors.com that the concept of informed consent is rooted in medical ethics and codified as a legal principle. It is based on the assertion that a competent person has the right to determine what is done to him or her [self-regulated autonomy].
Rationale: The American Medical Association recommends that its members disclose and discuss the following with their patients:
The requirements for informed consent are spelled out in statutes and case law in all 50 states. It is a necessary protocol for all hospitals, medical clinics, podiatry practices and ASCs.
Inadequacy of Traditional Consent Forms-to-Date
The typical informed consent process, particularly one that relies solely on traditional generic consent forms, is often inadequate, incomplete or offers the potential for not fully explaining and documenting a particular procedure to a given patient.
Traditional consent forms are subject to errors and omissions, such as missing signatures (patient, provider or witness), missing procedure(s), and missing dates that place the validity of consent at risk. Lost or misplaced forms may result in delayed or postponed procedures often at the expensive of costly operating room time. Moreover, far too many forms are generic in nature and wholly unsuited for a specific patient or increasingly sophisticated medical procedure.
Patient Safety Background
According to the Institute of Medicine’s [IOM] repot, To Err is Human, more than 1 million injuries and nearly 100,000 deaths occur annually in the United States due to mistakes in medical care. Wrong patient, wrong-side, wrong-procedure and wrong-toe surgery are particularly egregious. In fact, these are among several other “never-events” that Medicare, and an increasing number of private insurance companies are refusing to reimburse.
Based on the need to make healthcare safer, the Agency for Healthcare Research and Quality (AHRQ) undertook a study to identify patient safety issues and develop recommendations for “best practices”.
AHRQ Evidence Report
The AHRQ report identified the challenge of addressing shortcomings such as missed, incomplete or not fully comprehended informed consent, as a significant patient safety opportunity for improvement.
The authors of the AHRQ report hypothesized that better informed patients “are less likely to experience errors by acting as another layer of protection.” And, the AHRQ study ranked a more interactive informed consent process among the top 11 practices supporting more widespread implementation.
General Accounting Office report found that malpractice insurance premiums were relatively flat for most of the 1990’s, but projections began to increase dramatically to 2010.
Results of Improper Informed Consent
Failure to obtain adequate informed consent, depending on state law, may place surgeons, resident, fellows, ambulatory and office surgery centers, medical clinics and hospitals at risk for litigation ranging from medical negligence to assault and battery.
Proceedings Involving Informed Consent
Informed consent is often a factor in medical malpractice litigation. Some attorneys note that physicians are liable, and that plaintiffs may be able to recover damages, in cases involving improper informed consent, even if the procedure is successful. Inadequate informed consent is often cited as a secondary cause in malpractice complaints and anecdotal evidence suggests this strategy may be especially pursued in podiatric malpractices cases.
Avoiding Litigation
The AMA advises its membership of the following regarding informed consent:
“To protect yourself in litigation, in addition to carrying adequate liability insurance, it is important that the communications process itself be documented. Good documentation can serve as evidence in a court of the law that the process indeed took place. A timely and thorough documentation in the patient’s chart by the physician providing the treatment and/or performing the procedure can be a strong piece of evidence that the physician engaged the patient in an appropriate discussion.”
Impact of Comprehensive Informed Consent Forms
Another study found that providing informed consent information to patients in written form increased comprehension of the procedure. It was also hypothesized that:
Medical Ethics
The ethical foundation of informed consent is based on the creation of an environment that supports respect for patients and protects their right to autonomous, informed participation in all collaborative Healthcare 2.0 decisions.
Assessment
Thus, the essence of the informed consent problems of modern medicine today!
More: http://www.ePodiatryConsentForms.com
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
![]()
Filed under: Health Insurance, Health Law & Policy, Insurance Matters, Practice Management, Quality Initiatives, Research & Development, Risk Management, Uncategorized | Tagged: AHRQ, informed consent, medical consent, medical consent forms | 6 Comments »

BY DR. DAVID E. MARCINKO MBA CMP®
SPONSOR: http://www.CertifiedMedicalPlanner.org
REFERENCES
https://mises.org/library/mayo-clinic-and-free-market
http://www.kevinmd.com/blog/2017/08/problem-free-market-health-care.html
http://www.healthsharetv.com/content/dr-zeke-emanuel-history-healthcare-reform-us
https://www.pointnurse.com/blog/do-you-have-a-healthcare-blockchain-strategy/
Not Really Insurance: The Pre-Existing Condition Debate
Learn More about Concierge Medicine
http://www.kevinmd.com/blog/2017/04/health-care-right-privilege-cant-answer.html
http://www.healthissocial.com/
https://www.pointnurse.com/blog/do-you-have-a-healthcare-blockchain-strategy/
http://www.kevinmd.com/blog/2017/06/golden-era-medicine-never-coming-back.html
http://mdwhistleblower.blogspot.com/2016/02/concierge-medicine-is-it-ethical-or.html
https://studymatescom.wordpress.com/
Is Healthcare a Right? A Privilege? Something Entirely Different?
http://www.kevinmd.com/blog/2017/07/moral-assassination-physicians-must-stop.html
http://www.kevinmd.com/blog/2017/01/emphasize-public-health-medical-education.html
Hobson’s Wrong Answer
Is Health Privacy a Human Right?
http://www.kevinmd.com/blog/2016/12/must-temper-unregulated-free-market-philosophy-health-care.html
http://www.kevinmd.com/blog/2017/06/slow-death-private-practices.html
A Primer For Conservatives: Health Insurance is not Really Insurance
http://www.kevinmd.com/blog/2017/06/doctors-pr-problem.html
http://www.kevinmd.com/blog/2017/06/doctors-cops-can-fight-mistrust-way.html
http://www.sheknows.com/health-and-wellness/articles/1030383/crowdsourcing-health-care
DIY Textbooks: https://medicalexecutivepost.com/2021/04/29/why-are-certified-medical-planner-textbooks-so-darn-popular/
INVITE DR. MARCINKO: https://medicalexecutivepost.com/dr-david-marcinkos-
CONTACT: Ann Miller RN MH
[Executive Director]
MarcinkoAdvisors@msn.com
***
Filed under: Book Reviews, Career Development, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance | Tagged: Health Economics, health law, Healthcare Finance, healthcare management, healthcare policy | Leave a comment »
By Staff Reporters
***

***
The Justice Department’s (JD) efforts returned almost $1.9 billion to the federal government or paid it out to private individuals. Of that money, about $1.2 billion went to the Medicare trust fund. About $98.7 million in federal Medicaid money was transferred to CMS. The JD opened 831 criminal healthcare fraud cases last year. Federal prosecutors filed criminal charges in 462 cases involving 741 defendants. A total of 312 defendants were convicted of healthcare fraud during the year. The JD opened 805 civil healthcare fraud investigations and had 1,432 civil healthcare fraud matters pending at the end of last year.
HHS Office of the Inspector General (OIG) investigations resulted in 504 criminal actions against individuals or entities accused of Medicare- and Medicaid-related crimes. The OIG filed 669 civil actions, which included false claims and unjust-enrichment lawsuits filed in federal district courts, and civil monetary penalties. The OIG excluded 1,689 individuals and entities from participating in federal healthcare programs, including Medicare and Medicaid.
Source: Andrew Cass, Becker’s Hospital Review
***
COMMENTS APPRECIATED
Thank You
***
***
Filed under: Accounting, Ethics, Health Economics, Health Insurance, Health Law & Policy | Tagged: healthcare fraud, Justice Recovers $5B from Healthcare Fraud Cases, Justice Recovers $5B from Healthcare Fraud Cases in 2021 | Leave a comment »
***

***
By Health Capital Consultants, LLC
FTC Scrutiny Results in Several Scrapped Hospital Deals
A series of Federal Trade Commission (FTC) challenges to hospital mergers and acquisitions in 2022 indicates heightened regulatory scrutiny of hospital deals. Perhaps emboldened by the July 2021 executive order that focused attention on antitrust enforcement of hospital consolidation, the agency has voted to challenge a number of transactions, which has lead hospitals to call off the deals rather than challenge the government.

This Health Capital Topics article reviews three of the largest transactions called off this year, two of which were announced in June. (Read more…)
***
COMMENTS APPRECIATED
Thank You
***
***
Filed under: Breaking News, Career Development, Ethics, Experts Invited, Health Insurance, Health Law & Policy, Healthcare Finance | Tagged: Federal Trade Commission, FTC, Health Capital Consultants LLC, Scrapped Hospital Deals | Leave a comment »
My Laundry Wish List for all US Healthcare Stakeholders
By Dr. David Edward Marcinko; MBA, CMP™
[Publisher-in-Chief]
As President Obama spoke, prodded and cajoled for Congress to pass HR 3200-3400 in 2008, I believe that for any healthcare reform effort to work successfully for the American people – for the long term – we need to consider the following in no particular prioritized order:
Assessment
Recently, while in the Baltimore/Washing area, I was asked by several reporters to opine on the healthcare debate; which I did so freely having never been known as the shy type. And, regular readers will note that many of these items have been used as posts or comments on this ME-P. Unfortunately, my “laundry list” interview was pre-empted by two local but boisterous town-hall meetings with respective passionate politicians. It was redacted no doubt, but never broadcast. Thus, I missed the potential for my “five minutes” of fame. C’est la vive!
Conclusion
There you have it; direct and straight forward. And so, your thoughts and comments on this Medical Executive-Post are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Practice Management: http://www.springerpub.com/prod.aspx?prod_id=23759
Physician Financial Planning: http://www.jbpub.com/catalog/0763745790
Medical Risk Management: http://www.jbpub.com/catalog/9780763733421
Healthcare Organizations: www.HealthcareFinancials.com
Health Administration Terms: www.HealthDictionarySeries.com
Physician Advisors: www.CertifiedMedicalPlanner.com
THANK YOU
Filed under: Career Development, Drugs and Pharma, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Information Technology, Interviews, Managed Care, Op-Editorials | Tagged: ADA, AMA, CCHIT, CPT codes, CRNAs, david marcinko, dentists, DNPs, DNV, ER, evidence based medicine, expert based medicine, Fox news, Health Insurance, healthcare reform, hospitalists, HR 3200, HR 3400, HSAs, JCAHO, malpractice reform, medicare, never-events, NPs, nurses, obama, osteopaths, P4P, podiatrists, politics, retail medical clinics, RNs, tort reform, townhall meetings | 6 Comments »
By Professor Jon
***
***
PODCAST: https://www.youtube.com/watch?v=fwYYae_U1OI
PODCAST: https://medicalexecutivepost.com/2022/05/30/ama-to-teach-medical-students-about-health-economics/
***
***
***
***
COMMENTS APPRECIATED
Thank You
***
Filed under: Career Development, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Videos | Tagged: AMA, AMA economics, Health Economics, Health Insurance, healthcare economics, Healthcare Finance, Professor Jon | Leave a comment »
By Staff Reporters and MCOL
***

***
• Ambulatory encounters decreased by 1.0% and the number of in-person encounters per enrollee decreased by 17.0% from 2019 to 2020.
• For members with an initial telehealth encounter for a new acute condition, the adjusted odds ratio was 1.44 for all follow-ups combined and 1.11 for an emergency department encounter.
• For members with an initial telehealth encounter for a new chronic condition, the adjusted odds ratios were 0.94 for all follow-ups combined and 0.94 for in-patient admissions.
Source: JAMA Network, April 26, 2022
***
***
****
Filed under: Career Development, Ethics, Experts Invited, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Quality Initiatives | Tagged: Amwell, in-person doctor visits, In-Person medicine, JAMA Network, MCOL, online care, online medical care, OUTCOMES: In-Person and Tele-Health Encounters During COVID-19, Tele-Health, tele-health doctor visits | Leave a comment »
A HISTORICAL REVIEW WITH UPDATE

By Dr. David E. Marcinko MBA CMP®
SPONSOR: http://www.CertifiedMedicalPlanner.org
The Great Moderation is the name given to the period of decreased macroeconomic volatility experienced in the United States starting in the 1980s.
CITE: https://www.r2library.com/Resource/Title/0826102549
During this period, the standard deviation of quarterly real gross domestic product (GDP) declined by half and the standard deviation of inflation declined by two-thirds, according to figures reported by former U.S. Federal Reserve Chair Ben Bernanke. The Great Moderation can be summed up as a multi-decade period of low inflation and positive economic growth.
But, what about health economics, writ large? And, the actual practice of medicine by physicians in the trenches. Consider this historical review.
GOLDEN AGE OF MEDICINE
The ‘golden age of medicine’ – the first half of the 20th century, reaching its zenith with Jonas Salk’s 1955 polio vaccine – was a time of profound advances in surgical techniques, immunization, drug discovery, and the control of infectious disease; however, when the burden of disease shifted to lifestyle-driven, chronic, non-communicable diseases, the golden era slipped away. Although modifiable lifestyle practices now account for some 80% of premature mortality, medicine remains loathe to embrace lifestyle interventions as medicine Here, we argue that a 21st century golden age of medicine can be realized; the path to this era requires a transformation of medical school recruitment and training in ways that prioritize a broad view of lifestyle medicine. Moving beyond the basic principles of modifiable lifestyle practices as therapeutic interventions, each person/community should be viewed as a biological manifestation of accumulated experiences (and choices) made within the dynamic social, political, economic and cultural ecosystems that comprise their total life history. This requires an understanding that powerful forces operate within these ecosystems; marketing and neoliberal forces push an exclusive ‘personal responsibility’ view of health – blaming the individual, and deflecting from the large-scale influences that maintain health inequalities and threaten planetary health. The latter term denotes the interconnections between the sustainable vitality of person and place at all scales. We emphasize that barriers to planetary health and the clinical application of lifestyle medicine – including authoritarianism and social dominance orientation – are maintaining an unhealthy status quo.
NOTE: https://pubmed.ncbi.nlm.nih.gov/31828026/
GOLDEN AGE OF MEDICAL PRACTICE
To listen to all those desperate to reform health care, you get the impression that physicians are pretty horrible people. We are all sexist, greedy, money grubbing tyrants who will perform unnecessary tests and procedures just to make money. We don’t care about quality or cost. We are killing off 250,000 patients every year with our ignored “errors.”
We purposely keep our patients in pain, or we addict them to narcotics just to shut them up. We are constantly told by lawyers that lawsuits are necessary to protect patients from doctors. We provide unsafe drugs just because the drug reps give us free pens and coffee cups. The government must step in to clean up the mess.
PODCAST: https://www.kevinmd.com/blog/2017/08/9-reasons-golden-age-medicine-golden.html
GOLDEN AGE OF PATIENT TRUST
****
***
THE GREAT PHYSICIAN RETIREMENT AND RESIGNATION: https://medicalexecutivepost.com/2021/11/09/healthcare-industry-hit-with-the-great-resignation-retirement/
YOUR COMMENTS ARE APPRECIATED.
Thank You
***

RETIREMENT PLANNING: https://www.routledge.com/Risk-Management-Liability-Insurance-and-Asset-Protection-Strategies-for/Marcinko-Hetico/p/book/9781498725989
***

***
Filed under: Ethics, Experts Invited, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, iMBA, Inc., LifeStyle, Quality Initiatives, Research & Development, Retirement and Benefits, Videos | Tagged: David Edward Marcinko, doctor trust, Eric Bricker MD, golden age medical practice, golden age medicine, nurse trust, patient trust trust, Physician retirement, physician trust | 4 Comments »
***
By Health Capital Consultants, LLC
***

***
Valuation of Home Health Agencies: Reimbursement Environment
The U.S. government is the largest payor of medical costs, through Medicare and Medicaid, and has a strong influence on reimbursement for home healthcare services. In 2020, Medicare and Medicaid accounted for an estimated $829.5 billion and $671.2 billion in healthcare spending, respectively. The outsized prevalence of these public payors in the healthcare marketplace often results in their acting as a price setter, and being used as a benchmark for private reimbursement rates. This effect may be even stronger in the home health industry.
The third installment of this home health valuation series will discuss the reimbursement environment in which these organizations operate. (Read more…)
***
CITE: https://www.r2library.com/Resource/Title/0826102549
COMMENTS APPRECIATED
Thank You
***
***
***
Filed under: "Doctors Only", Ethics, Experts Invited, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance | Tagged: Health Capital Consultants LLC, home health, home health agencies, Medicaid, medicare | Leave a comment »
***

By Eric Bricker MD
***
| According to One Survey, only 4% of People Understand the Basic Insurance Terms of Deductible, Co-Insurance, Copay and Out-of-Pocket Maximum. In Another Survey by United Healthcare Itself, Only 9% Understood the Terms Premium, Deductible, Co-Insurance and Out-of-Pocket Max. This Lack of Understanding is Not the Fault of the Employee Benefits Professionals or the Employees… Rather, the Health Insurance Plan Designs Are Just Too Complicated. CITE: https://www.r2library.com/Resource/Title/082610254 |
***
***
Comments Appreciated
THANK YOU
***
***
****
Filed under: "Ask-an-Advisor", Ethics, Experts Invited, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Videos | Tagged: co-insurance, complicated health insurance, deductibles, Eric Bricker MD, Health Insurance, UHC, UnitedHealth Group | Leave a comment »
![]()
About Four-Twenty Day
[By Anonymous DEA Agent]
Today is … 420, 4:20, or 4/20 (pronounced four-twenty)
And, it refers to consumption of cannabis and, by extension, a way to identify oneself with cannabis subculture. Observances based on the number include the time (4:20 p.m.) as well as the date (April 20).
Again … that’s today as this ME-P was published @ 4:20 p.m., EST!








PHOTOS:
© iMBA Inc. All rights reserved.
Assessment
Link: http://en.wikipedia.org/wiki/420_(cannabis_culture)
In 2019: Carl’s Jr. was become the first major fast-food chain to debut a cannabis-infused burger.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
![]()
Filed under: Breaking News, Drugs and Pharma, Glossary Terms, Health Law & Policy | Tagged: cannabis, DEA, ganga, marijuana, mary jane, medicinal marijuana, pot, pot farm, The 4/20 Cannabis Culture, weed | 13 Comments »
****
By Dr. David E. Marcinko MBA CMP®
INVITE DR. MARCINKO: https://medicalexecutivepost.com/dr-david-marcinkos-
SPONSOR: http://www.CertifiedMedicalPlanner.org
[A] Key Person Insurance
Hospitals, a local family practice office, a pharmaceutical company, all likely have one thing in common. Somewhere within these companies or partnerships, there are key employees or profit makers. Due to their expertise, management skills, knowledge, or “history of why,” they have become indispensable to their employers.
If this key employee were to die prematurely, what would potentially happen to the company? In many cases, especially in smaller companies, it would have a devastating effect on the bottom line, or even precipitate a bankruptcy. In these circumstances, a form of business insurance, called key person coverage, is recommended in order to alleviate the potential financial problems resulting from the death of that employee.
The business would purchase and own a life insurance policy on the key person. Upon the death of the employee, the life insurance proceeds could be used to:
[B] Business Continuation Funding
See the chapters on buy-sell agreements and asset protection planning.
[C] Executive Bonus Plan
An executive bonus plan (or § 162 plan) is an effective way for a company to provide valued, select employees an additional employment benefit. One of the main advantages to an executive bonus plan, when compared to other benefits, is its simplicity. In a typical executive bonus plan, an agreement is made between the employer and employee, whereby the employer agrees to pay for the cost of a life insurance policy, in the form of a bonus, on the life of the employee.
The major benefits of such a plan to the employee are that he or she is the immediate owner of the cash values and the death benefit provided. The only cost to the employee is the payment of income tax on any bonus received. The employer receives a tax deduction for providing the benefit, improves the morale of its selected employees, and can use the plan as a tool to attract additional talent.
[D] Non-Qualified Salary Continuation
Commonly referred to as deferred compensation, this is a legally binding promise by an employer to pay a salary continuation benefit at a specific point in the future, in exchange for the current and continued performance of its employee. These plans are normally used to supplement existing retirement plans.
Although there are different variations of deferred compensation, in a typical deferred compensation agreement, the employer will purchase and own a life insurance policy on the life of the employee. The cash value of the policy grows tax deferred during the employee’s working years. After retirement, these cash values can be withdrawn from the policy to reimburse the company for its after-tax retirement payments to the employee.
Upon the death of the employee, any remaining death benefit would likely be received income tax free by the employer (Alternative Minimum Taxes could apply to any benefit received by certain larger C corporations). The death benefit could then be used to pay any required survivor benefits to the employee’s spouse, or provide partial or total cost recovery to the employer.
In a typical plan, the terms of the agreement are negotiated as to the amount of benefit received by the employee, when retirement benefits can begin, how long retirement benefits will be paid, and if benefits will be provided for death or disability. The business has established what is commonly referred to as “golden handcuffs” for the employee. As a result, the benefit will only be received if the employee continues to work for the company until retirement. If the employee is terminated or quits prior to retirement, the plan would end and no benefits would be payed.
[E] Split Dollar Plans
Split dollar arrangements can be a complicated and confusing concept for even the most experienced insurance professional or financial advisor. This concept is, in its simplest terms, a way for a business to share the cost and benefit of a life insurance policy with a valued employee. In a normal split dollar arrangement, the employee will receive valuable life insurance coverage at little cost to them. The business pays the majority of the premium, but is usually able to recover the entire cost of providing this benefit at termination of employment, death or surrender of the policy.
Following the publication of IRS Notices 2002-8 and 2002-59, there are currently two general approaches to the ownership of business split-dollar life insurance: Employer-owned or Employee-owned.
***
[1] Employer-Owned Method
In the employer-owned method the employer is the sole owner of the policy. A written split-dollar agreement usually permits the employee to name the beneficiary for most of the death proceeds. The employer owns all the cash value and has the unfettered right to borrow or withdraw it as necessary. At the end of the formal agreement, the business can generally (1) continue the policy as key person insurance, (2) transfer ownership to the insured and report the cash values as additional income to the insured, (3) sell the policy to the insured, or (4) use a combination of these methods. This is commonly referred to as “rollout.”
Practitioners should be careful not to include rollout language in the split-dollar agreement. The reason the rollout should not be included is that if the parties formally agree that after a specified number of years—or following a specific event—related only to the circumstances surrounding the policy, that the policy will be turned over to the insured, the IRS could declare that the entire transaction was a sham and that its sole purpose was to avoid taxation of the premiums to the employee, generating substantial interest and penalties in addition to the additional taxes due.
The death proceeds available to the insured employee’s beneficiary is considered a current and reportable economic benefit (REB), and it is an annually taxable event to the employee. If an individual policy is involved, the REB is calculated by multiplying the face amount times the government’s Table 2004 rates or the insurance company’s alternative term rates, using the insured’s age. If a second-to-die policy is involved, the government’s PS38 rates or the company’s alternative PS38 rates will be used. Any part of the premium actually paid by the employee is used to offset any REB dollar-for-dollar.
[2] Employee-Owned Method
With the employee-owned method, the insured-employee is generally the applicant and owner of the policy. Any premiums paid by the business are deemed to be loans to the employee and the employee reports as income an imputed interest rate on the cumulative amount of loan based on Code § 7872. A collateral assignment is made for the benefit of the business to cover the cumulative loan amount. In some cases, the assignment may allow the assignee to have access to the cash values of the policy by way of a policy loan. This method is unavailable for officers and executives of publicly- held corporations because of the current restrictions on corporate loans (the Sarbanes-Oxley Act of 2002).
The employee-owned method is somewhat similar to the older collateral assignment form of split-dollar. The benefits for the employee are both the ability to control large amounts of death proceeds as well as developing equity in the policy. Whether or not this new method catches on will depend greatly on the imputed interest rate published by the IRS every July. If set low enough, this may be an excellent opportunity for the employee to use inexpensive business dollars to pay for life insurance.
***
CITE: https://www.r2library.com/Resource/Title/0826102549
***
Your Comments are appreciated.

Risk Management Textbook: https://www.routledge.com/Risk-Management-Liability-Insurance-and-Asset-Protection-Strategies-for/Marcinko-Hetico/p/book/9781498725989
THANK YOU
***
Filed under: "Doctors Only", Health Law & Policy, Insurance Matters, Touring with Marcinko | Tagged: Business Insurance Doctors, David E. Marcinko, insurance doctors, key person insurance, life insurance, risk management physicians | Leave a comment »
MANAGEMENT STRATEGIES, TOOLS TEMPLATES AND CASE STUDIES
***
Hospitals and Health Care Organizations is a must-read for any physician and other health care provider to understand the multiple, and increasingly complex, interlocking components of the U.S. health care delivery system, whether they are employed by a hospital system, or manage their own private practices.
The operational principles, methods, and examples in this book provide a framework applicable on both the large organizational and smaller private practice levels and will result in better patient care. Physicians today know they need to better understand business principles and this book by Dr. David E. Marcinko and Professor Hope Rachel Hetico provides an excellent framework and foundation to learn important principles all doctors need to know.
―Richard Berning, MD, Pediatric Cardiology
… Dr. David Edward Marcinko and Professor Hope Rachel Hetico bring their vast health care experience along with additional national experts to provide a health care model-based framework to allow health care professionals to utilize the checklists and templates to evaluate their own systems, recognize where the weak links in the system are, and, by applying the well-illustrated principles, improve the efficiency of the system without sacrificing quality patient care. … The health care delivery system is not an assembly line, but with persistence and time following the guidelines offered in this book, quality patient care can be delivered efficiently and affordably while maintaining the financial viability of institutions and practices.
―James Winston Phillips, MD, MBA, JD, LLM
***
***
***
PURCHASE: https://www.amazon.com/dp/B00BC9IIUM?ref_=k4w_oembed_faGUzLlJ9ojLIx&tag=kpembed-20&linkCode=kpd
***
Filed under: "Doctors Only", Accounting, Book Reviews, Career Development, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Information Technology, Professional Liability, Recommended Books, Research & Development, Risk Management | Tagged: David E. Marcinko, Healthcare CEOs, Hospitals and Healthcare Organizations, Industrial Organizations, Medical COOs, Medical CXOs | 1 Comment »
By American Journal of Public Health
***

***
DEFINITION: Public health is “the science and art of preventing disease, prolonging life and promoting health through the organized efforts and informed choices of society, organizations, public and private, communities and individuals”.
CITE: https://www.r2library.com/Resource/Title/082610254
CDC: https://www.cdcfoundation.org/what-public-health
PODCASTS: https://www.apha.org/what-is-public-health
***
READ HERE: https://ajph.aphapublications.org/doi/10.2105/AJPH.2022.306756
***
COMMENTS APPRECIATED
Thank You
***
***
***
Filed under: "Ask-an-Advisor", Ethics, Glossary Terms, Health Economics, Health Law & Policy, Videos | Tagged: AJPH, CDC, next generation public health, public health, public health professionals, public health training | Leave a comment »
By Eric Bricker MD
***
1) Traditional Medicare: Health Insurance for Seniors 65 and older. Medicare Part A is coverage for hospital services. Medicare Part B is coverage for doctor, physical therapist and other provider services and for outpatient services such as labs and imaging.
2) Medicare Advantage: Health Insurance for Seniors 65 and older administered through a private health insurance company. It is sometimes referred to as Medicare Part C. It can be chosen instead of Traditional Medicare and often includes Dental Insurance, Vision Insurance, Hearing Aid Insurance and Prescription Drug Coverage.
3) Medicare Part D Prescription Coverage: Additional insurance for people on Traditional Medicare to cover their prescription medications as well. Medicare Part D is administered by private insurance companies.
4) Medicare Supplement Plans: Insurance that can be purchased in addition to Traditional Medicare to cover the expenses that Traditional Medicare does not cover, such as hospitalization deductibles and Medicare Part B co-insurance.
5) Medicaid: The health insurance program administered by each state for it’s economically disadvantaged residents. It is funded in part by the Federal Government and in part by each state. It is administered by private health insurance companies.
6) Affordable Care Act (ACA) Exchange Plans: Health insurance for people under 65 who make too much money to qualify for Medicaid, but do not received health insurance through their employer. ACA Exchange Plans are subsidized by the Federal Government and administered by private insurance companies.
***
***
COMMENTS APPRECIATED.
Thank You
Subscribe to the Medical Executive-Post
***
***
***
****
Filed under: Experts Invited, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Insurance Matters, Videos | Tagged: ACA, Affordable Care Act., Eric Bricker MD, Health Insurance, Medicaid, medicare, Medicare Advantage, Medicare Part C, Medicare Part D, medigap, Prescription Insurance Coverage | Leave a comment »
BY HEALTH CAPITAL CONSULTANTS, LLC.
DEFINITION: The False Claims Act, also called the “Lincoln Law”, is an American federal law that imposes liability on persons and companies who defraud governmental programs. It is the federal Government’s primary litigation tool in combating fraud against the Government. The law includes a provision that allows people who are not affiliated with the government, called “relators” under the law, to file actions on behalf of the government. Persons filing under the Act stand to receive a portion of any recovered damages.
CITE: https://www.r2library.com/Resource/Title/0826102549
***
DOJ Recoveries for False Claims Act Cases Doubled in 2021
On February 1, 2022, the U.S. Department of Justice (DOJ) announced their recovery of $5.6 billion in settlements and judgments from civil cases involving fraud and false claims for fiscal year (FY) 2021. Over $5 billion was recouped from the healthcare industry for federal losses alone, and included recoveries from drug and medical device manufacturers, managed care providers, hospitals, pharmacies, hospice organizations, laboratories, and physicians.
***
This figure is more than double the amount of healthcare-related recoveries secured in FY 2020, which totaled $1.8 billion. (Read more…)
***
***
***
COMMENTS APPRECIATED
Thank You
Subscribe to the Medical Executive-Post
***
Filed under: "Doctors Only", Accounting, Career Development, Ethics, Experts Invited, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance | Tagged: DOJ, false claims act, Health Capital Consultants LLC, health fraud, Lincoln Law, qui tam, relators | 1 Comment »
By Eric Bricker MD
C.O.N. Legislation is Not New!
Certificate of need laws are state-level regulations that require healthcare institutions to obtain approval from state officials before moving forward on large capital expenditure projects, such as the construction of a new facility or the purchase of expensive new equipment.
CITE: https://www.r2library.com/Resource/Title/082610254
***
***
COMMENTS APPRECIATED
Thank You
Subscribe to the Medical Executive-Post
***
***
***
***
Filed under: Career Development, Experts Invited, Health Economics, Health Insurance, Health Law & Policy, Videos | Tagged: Certificate of Need, certificate of need laws, CON laws, Eric Bricker MD | Leave a comment »
By Eric Bricker MD
An accumulator is a running total of money you’ve paid towards your out-of-pocket max for covered services. This includes any copayments, coinsurance, and other health care costs, but not your monthly premium payments.
CITE: https://www.r2library.com/Resource/Title/082610254
***
***
COMMENTS APPRECIATED
Thank You
Subscribe to the Medical Executive-Post
***
***
***
****
Filed under: Accounting, Alerts Sign-Up, Ethics, Experts Invited, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Managed Care, Videos | Tagged: accumulator, doctor payments, Eric Bricker MD, Health Insurance, healthcare costs, hospital payments, out pocker costs | 1 Comment »
| A Professional and Personal look at Health Insurance, with Karl Albrecht |
| Rich talks with the president of Action Benefits, Karl Albrecht about the state of Health Insurance. Albrecht also gives a candid insight to his personal fight with pancreatic cancer and how being a Health Insurance executive as well as a patient, has given him a unique perspective on how things work, and how they could improve. |

BY RICHARD HELPPIE
PODCAST: https://richardhelppie.com/karl_albrecht/
YOUR COMMENTS ARE APPRECIATED.
Thank You
***
***
***
Filed under: Experts Invited, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Videos | Tagged: Health Insurance, HSAs, Karl Albrecht, Richard Helppie | Leave a comment »
Balance Medical Billing
By Dr. David E. Marcinko MBA CMP®
The No Surprises Act is looking to make the practice of out of network balance billing a thing of the past.
CITE: https://www.r2library.com/Resource/Title/0826102549
***

***
Beginning in 2022, there will be few situations in which a patient can receive a bill for out-of-network care they believed would be covered by their insurance company. This new rule should especially benefit patients in emergency situations who don’t have the time or luxury to dig up the details on every provider they encounter.
CONGRESS: https://www.congress.gov/bill/116th-congress/house-bill/3630/
The No Surprises Act also requires insurance companies to provide patients with at least 90 days of coverage if an in-network provider moves out of network. That way, patients aren’t forced to switch providers immediately if such a move happens while they’re in the middle of a treatment plan.
DOCTORS: https://www.elixirehr.com/what-the-no-surprises-act-means-for-healthcare-providers/
Now, the No Surprises Act does have its limitations. Patients can still get a bill for out-of-network care if they visit an urgent care clinic for non-emergency purposes. Also, if consumers are informed that the care they’re about to receive is out of network and they give written consent to move forward, then they may get billed for that care even once the new rule takes effect.
CMS: https://www.cms.gov/nosurprises
YOUR COMMENTS ARE APPRECIATED.
***
***
Thank You
***
***
Filed under: "Doctors Only", Accounting, Breaking News, Career Development, CMP Program, Estate Planning, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Managed Care | Tagged: Balance billing, Certified Medical Planner™, CMP, David Edward Marcinko, medical balance billing, No Surprise Act, Surprise billing | 2 Comments »
IS PRIVATE EQUITY BUYING DOCTORS ILLEGAL?
By Eric Bricker MD
***
***
YOUR COMMENTS APPRECIATED
Thank You
***
***
Filed under: Accounting, Career Development, Ethics, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, iMBA, Inc., Investing, Videos | Tagged: Blackstone, corporate practice medicine, KKR, PPMC, Private Equity, Private Equity Medicare, VCs, Venture Capital | Leave a comment »
Surprise Medical Bills Outlawed?
By Eric Bricker MD
****
***
https://medicalexecutivepost.com/2021/11/03/balance-billing-the-emerging-no-surprise-act/
QPA DEFINITION: The qualifying payment amount is generally the median of contracted rates for a specific service in the same geographic region within the same insurance market as of January 31, 2019. The rate will be adjusted per the Consumer Price Index for All Urban Consumers (CPI-U).
CITE: https://www.r2library.com/Resource/Title/0826102549
***
COMMENTS APPRECIATED
Thank You
Subscribe to the Medical Executive-Post
***
BUSINESS MEDICINE: https://www.amazon.com/Business-Medical-Practice-Transformational-Doctors/dp/0826105750/ref=sr_1_9?ie=UTF8&qid=1448163039&sr=8-9&keywords=david+marcinko
***
***
Filed under: "Ask-an-Advisor", Accounting, Events-Planner, Experts Invited, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Managed Care | Tagged: Eric Bricker MD, in-network, network billing, out-network, QPA, qualifying payment amount, Surprise billing, surprise medical billing | 1 Comment »
Indications for 2022
BY HEALTH CAPITAL CONSULTANTS, LLC
***
2021 M&A in Review: Indications for 2022
After an understandable slowdown in 2020, due to the onset of the COVID-19 pandemic, merger & acquisition (M&A) activity in the healthcare industry accelerated in 2021, and the industry is expected to continue the high number of deals and high deal volume in 2022.
***

***
This Health Capital Topics article will review the U.S. healthcare industry’s M&A activity in 2021, and discuss what these trends may mean for 2022. (Read more…)
***
CITE: https://www.r2library.com/Resource/Title/0826102549
COMMENTS APPRECIATED
Thank You
Subscribe to the Medical Executive-Post
***
***
***
Filed under: "Ask-an-Advisor", Accounting, Ethics, Experts Invited, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, iMBA, Inc., Managed Care | Tagged: Covid-19, Health Capital Consultants LLC, healthcare mergers acquisitions, HEALTHCARE: 2021 M&A in Review, M&As | Leave a comment »
By Staff Reporters
***
***
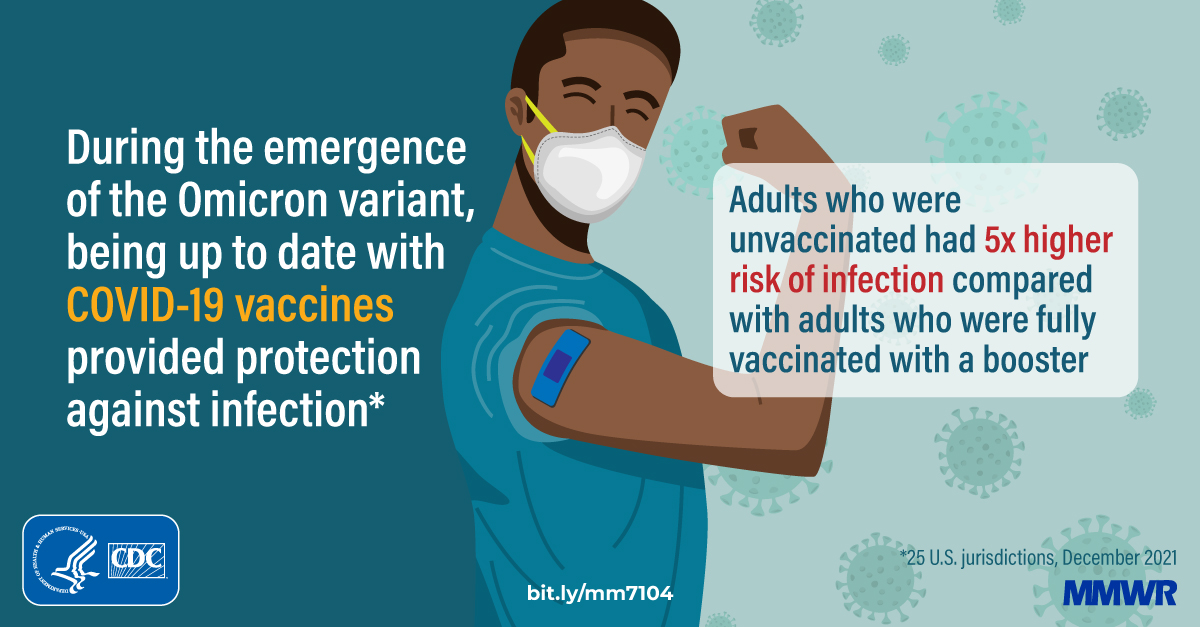
According to a recent CDC study. Among 422,966 reported SARS-CoV-2 infections in LAC residents aged ≥18 years during November 7, 2021–January 8, 2022:
• 33.6% were in unvaccinated persons
• 13.3% were in fully vaccinated persons with a booster
• 53.2% were in fully vaccinated persons without a booster
• Unvaccinated persons were most likely to be hospitalized, representing 2.8% of COVID infections
• Unvaccinated persons were most likely to be admitted to an ICU, or 0.5% of COVID infections
• Unvaccinated persons were most likely to be require intubation for mechanical ventilation, or 0.2% of COVID infections.
Source: CDC, Morbidity and Mortality Weekly Report, February 1, 2022
Lost Vaccine Card: https://portal.ct.gov/vaccine-portal/Vaccine-Knowledge-Base/Articles/Lost-Vaccine-Card?language=en_US
CITE: https://www.r2library.com/Resource/Title/0826102549
***
***
COMMENTS APPRECIATED
Thank You
Subscribe to the Medical Executive-Post
***
Filed under: Breaking News, Drugs and Pharma, Ethics, Health Economics, Health Law & Policy, LifeStyle, Quality Initiatives | Tagged: booster, CDC, corona, corona pandemic, covid, covid infections, LAC, lost vaccine card, MMWR, Morbidity Mortality Weekly Report, SARS-CoV-2, unvaccinated covid infections, Unvaccinated Persons, vaccinations, vaccine, vaccine booster | Leave a comment »
By Staff Reporters
***
A recent AKASA survey of 514 chief financial officers and revenue cycle leaders at hospitals and health systems in the U.S. found:
• Entry-level revenue cycle talent (0-5 years): On average, costs $2,167 for recruitment and takes 84 days to fill vacant roles.
• Mid-level revenue cycle talent (6-10 years): On average, costs $3,581 for recruitment and takes 153 days to fill vacant roles.
• Senior-level revenue cycle talent (10+ years): On average, costs $5,699 for recruitment and takes 207 days to fill vacant roles.
Source: AKASA via PR Newswire, “Survey: Recruitment Costs, Long Hiring Timelines Negatively Impact Healthcare Finance Teams”, January 26, 2022
***
***
***
Filed under: Experts Invited, Health Law & Policy, Healthcare Finance, Managed Care | Tagged: AKASA, Hospital Revenue Cycle Recruitment, hospitals, MCOL, RCR, revenue recruitment | Leave a comment »
Medicare Payment Advisory Commission
By Health Capital Consultants, LLC

***
MedPAC Recommends Payment Updates for 2023
DEFINITION: The Medicare Payment Advisory Commission is an independent, non-partisan legislative branch agency headquartered in Washington, D.C. MedPAC was established by the Balanced Budget Act of 1997.
CITE: https://www.r2library.com/Resource/Title/082610254
***
In a January 2022 meeting of MedPAC, commissioners reviewed various recommendations related to the Medicare fee schedule for various health sectors, and unanimously agreed to update Medicare payments to hospitals and keep physician payment rates the same for 2023. This Health Capital Topics article will review the recommendations made by MedPAC for each of the health sectors and their respective payment systems. (Read more…)
***
***
***
***
Filed under: Accounting, Career Development, Experts Invited, Glossary Terms, Health Law & Policy | Tagged: Health Capital Consultants LLC, Medicare Payment Advisory Commission, MedPAC, MedPAC 2023 | Leave a comment »
By Eric Bricker MD
The Centers for Medicare and Medicaid Services (CMS) Announce Changes to Doctor and Healthcare Provider Payments
CITE: https://www.r2library.com/Resource/Title/082610254
****
***
PODCAST Related Medical Payments: https://medicalexecutivepost.com/2021/10/01/podcast-on-medicare-payments-to-doctors/
***
COMMENTS APPRECIATED
Thank You
Subscribe to the Medical Executive-Post
***
***
****
Filed under: "Doctors Only", Career Development, Experts Invited, Health Economics, Health Insurance, Health Law & Policy, Videos | Tagged: CMS, doctor charges, Eric Bricker MD, fee for service, FFS, medicare, medicare payments, physician payments | Leave a comment »
By Staff Reporters
***
• United States: $11,946
• Switzerland: $7,138
• Germany: $6,731
• Netherlands: $6,299
• Austria: $5,899
• Sweden: $5,754
• France: $5,564
• Belgium: $5,458
• Canada: $5,370
• United Kingdom: $5,268
• Australia: $4,919
• Japan: $4,691
Notes: U.S. value obtained from National Health Expenditure data. Data from Australia, Belgium, Canada, Japan and Switzerland are from 2019. Data for Australia, France, and Japan are estimated. Data for Austria, Canada, Germany, Netherlands, and Sweden are provisional. Health consumption does not include investments in structures, equipment, or research. Data for 2020 except as noted.
Source: KFF analysis of National Health Expenditure (NHE) and OECD data, January 21, 2022
CITE: https://www.r2library.com/Resource/Title/0826102549
***
COMMENTS APPRECIATED
Thank You
Subscribe to the Medical Executive-Post
***
***
Filed under: Funding Basics, Health Economics, Health Insurance, Health Law & Policy | Tagged: domestic health costs, Health Consumption Expenditures Per Capita, healthcare costs, KFF | Leave a comment »
***
By Eric Bricker MD
***
Health Insurance Cost Has Risen 55% in the last 10 Years. The Annual Health Insurance Cost for Family Coverage is Now $21,000 Per Year
***
Dysfunctional Employee Benefits Article in Journal of the American Medical Association
***
***
COMMENTS APPRECIATED
Thank You
Subscribe to the Medical Executive-Post
***
***
***
CITE: https://www.r2library.com/Resource/Title/082610254
***
Filed under: Accounting, Book Reviews, Ethics, Experts Invited, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Insurance Matters, Risk Management, Videos | Tagged: AMA, Annual Health Insurance Cost, Dysfunctional Employee Benefits, Eric Bricker MD, Health Insurance, Health Insurance Costs | 1 Comment »
By Staff Reporters
***

***
According to reporter Neal Freyman, Tech giant Oracle said it’s paying $28.3 billion to buy electronic medical records company Cerner, because anything that makes paperwork less excruciating seems like a savvy business play.
Oracle is known for being aggressive with acquisitions (it even rallied a group to try and buy TikTok last year), but Cerner is Oracle’s biggest purchase in its history. The deal is further evidence that health care is “on par with banking in terms of the importance to our future,” as cofounder Larry Ellison told analysts earlier this month.
Bottom line: Big tech companies see a golden opportunity in bringing the health care industry to the cloud, given its size (health care spending accounts for almost 20% of US GDP), and its old-school record-keeping process. A Mayo Clinic study cited by Oracle showed that doctors and nurses spend an average of 1–2 hours on desk work for every hour they take to see patients.
***
EMR PODCAST: https://medicalexecutivepost.com/2021/08/29/podcast-on-electronic-medical-records/
***
COMMENTS APPRECIATED.
Thank You
Subscribe to the Medical Executive-Post
***
BUSINESS MEDICINE: https://www.amazon.com/Business-Medical-Practice-Transformational-Doctors/dp/0826105750/ref=sr_1_9?ie=UTF8&qid=1448163039&sr=8-9&keywords=david+marcinko
***
***
THANK YOU
***
Filed under: Breaking News, Career Development, Experts Invited, Health Economics, Health Law & Policy, Information Technology, Videos | Tagged: Cerner, EMRs, Epic, health information technology, HIT, IT, Klay Thompson, Larry Ellison, Mayo clinic, Neal Freyman, oracle | 1 Comment »
By Staff Reporters
***
The 2022 Global Medical Trends Survey shows variation in healthcare cost increases. Increases across different regions next year are expected to range from:
• 14.2% in Latin America
• 10.6% in the Middle East
• 10.6% in Africa
• 7.6% in Asia Pacific
• 6.7% in Europe
• 7.6% in the U.S.
Source: Willis Towers Watson, November 15, 2021
***
COMMENTS APPRECIATED.
Thank You
Subscribe to the Medical Executive-Post
***
***
Filed under: Alerts Sign-Up, Glossary Terms, Health Economics, Health Law & Policy | Tagged: global healthcare cost trends, healthcare cost increases., medical cost trends, Willis Towers Watson | Leave a comment »
By Staff Reporters
Medical education in the U.S. and Canada has changed considerably in the last several decades.
***
According to the AMA, the major changes are the following:
***
COMMENTS APPRECIATED.
Thank You
Subscribe to the Medical Executive-Post.com
***
***
***
Filed under: "Doctors Only", Career Development, Health Law & Policy, iMBA, Op-Editorials | Tagged: AMA, medical education, objective structured clinical examinations, OSCE, PBL, problem based learning | Leave a comment »
PANDEMIC “versus” EPIDEMIC
 Dr. David E. Marcinko MBA
Dr. David E. Marcinko MBA
Courtesy: www.CertifiedMedicalPlanner.org
Is there a Difference? – Know the Difference!
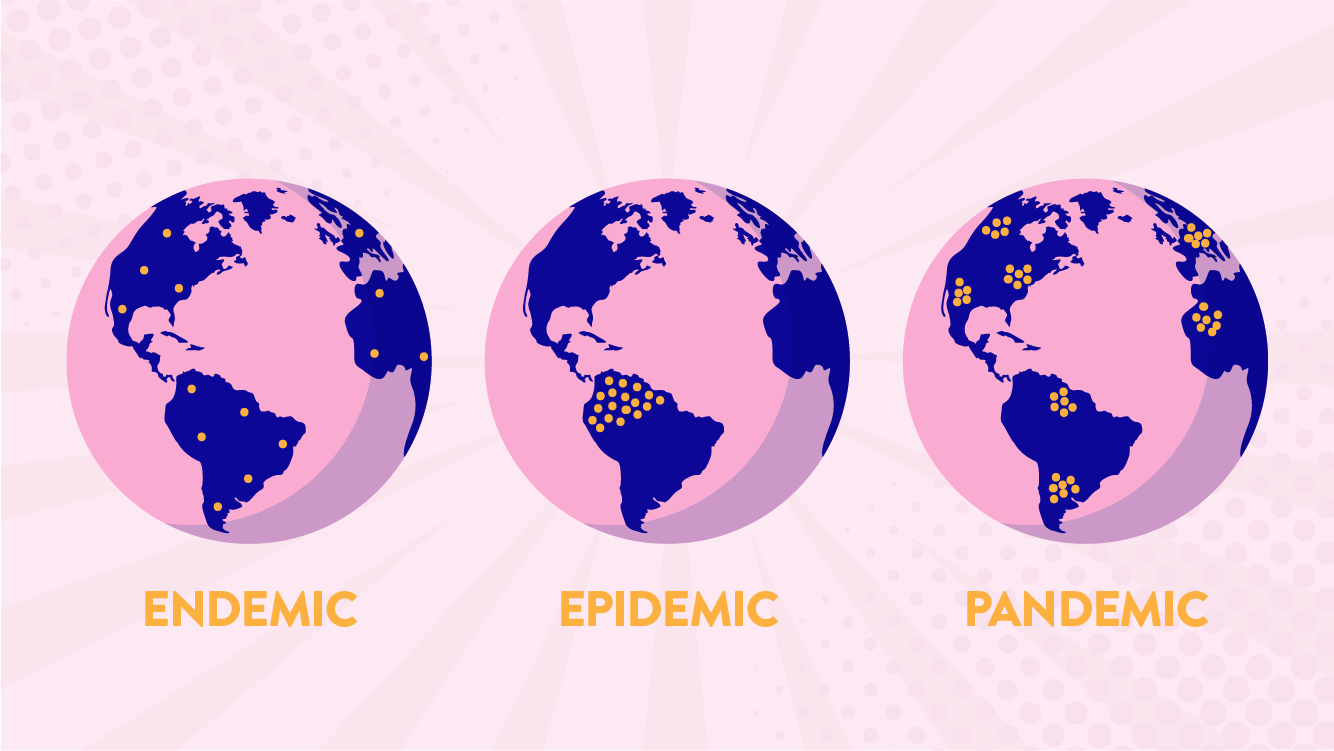
A Pandemic (from Greek πᾶν pan “all” and δῆμος demos “people”) is an epidemic of disease that has spread across a large region; for instance multiple continents, or even worldwide. A widespread endemic disease that is stable in terms of how many people are getting sick from it is not a pandemic.
Further, flu pandemics generally exclude recurrences of seasonal flu. Throughout history, there have been a number of pandemics, such as smallpox and tuberculosis. One of the most devastating pandemics was the Black Death, which killed an estimated 100 million people in the 14th century. Some recent pandemics include: HIV, Spanish flu, 2009 flu pandemic and H1N1.
An Epidemic is the rapid spread of infectious disease to a large number of people in a given population within a short period of time, usually two weeks or less.
For example, in meningococcal infections, an attack rate in excess of 15 cases per 100,000 people for two consecutive weeks is considered an epidemic.
***
***
Key Differences
MORE: https://www.verywellhealth.com/difference-between-epidemic-and-pandemic-2615168
ENDEMIC: If you translate it literally, endemic means “in the population.” It derives from the Greek endēmos, which joins en, meaning “in,” and dēmos, meaning “population.” “Endemic” is often used to characterize diseases that are generally found in a particular area; malaria, for example, is said to be endemic to tropical and subtropical regions. This use differs from that of the related word epidemic in that it indicates a more or less constant presence in a particular population or area rather than a sudden, severe outbreak within that region or group.
Conclusion: Your thoughts are appreciated.
***
![]()
![]()

THANK YOU
Filed under: Glossary Terms, Health Law & Policy, Risk Management, Touring with Marcinko | Tagged: corona virus, epidemics, pandemics | Leave a comment »
SPONSOR: http://www.CertifiedMedicalPlanner.org
SECOND OPINIONS: https://medicalexecutivepost.com/schedule-a-consultation/
INVITE DR. MARCINKO: https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
THANK YOU
***
Filed under: "Doctors Only", Accounting, Book Reviews, Career Development, CMP Program, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, iMBA, Inc., Managed Care, Practice Management, Recommended Books, Sponsors, Touring with Marcinko | Tagged: Certified Medical Planner™, CMP™ Course, david marcinko, Dr. David Edward Marcinko MBA CMP™, Financial Management Healthcare, Financial Management Hospitals | 1 Comment »
BY ERIC BRICKER MD
***
YOUR COMMENTS ARE APPRECIATED.
CITE: https://www.r2library.com/Resource/Title/082610254
Subscribe to the Medical Executive-Post
***
***
***
***
Filed under: Accounting, Ethics, Experts Invited, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Videos | Tagged: charity care, Eric Bricker MD, FAP, hospital charity care | Leave a comment »
Economy Works’ Applied to Healthcare … Credit Cycles and Healthcare Policy
By Eric Bricker MD
***
***
COMMENTS APPRECIATED
Subscribe to the ME-P
Thank You
HEALTH ECONOMICS CITE: https://www.r2library.com/Resource/Title/0826102549
RICARDIAN DEMAND HEALTH ECONOMICS: https://medicalexecutivepost.com/2021/12/14/ricardian-derived-demand-economics-in-medicine/
RISING HEALTH CARE COSTS: https://medicalexecutivepost.com/2018/03/11/medical-treatment-costs-becoming-expensive-25-factors/
***
***
Filed under: "Ask-an-Advisor", "Doctors Only", Experts Invited, Funding Basics, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Interviews, Videos | Tagged: credit, credit cycles, Eric Bricker MD, health accountihng, Health Economics, Health Insurance, healthcare credit, Ray Dalio, supply-demand | Leave a comment »
New Study Compares Medicare-Commercial Payment Gaps by Specialty
BY HEALTH CAPITAL CONSULTANTS
Utilizing data from FAIR Health, the Urban Institute conducted an October 2021 study which reviewed commercial insurance claims across the U.S. (for approximately 60 insurers and third-party administrators covering over 150 million Americans under age 65) from March 2019 through February 2020.
CITE: https://www.r2library.com/Resource/Title/0826102549
This study assessed the gap between commercial insurance payments and Medicare payments for professional physician services to determine whether the payment gap between Medicare and commercial insurance differs by specialty. (Read more…)
YOUR COMMENTS ARE APPRECIATED.
***
Thank You
***
Filed under: Breaking News, Career Development, Experts Invited, Health Insurance, Health Law & Policy, Healthcare Finance | Tagged: CMS, Health Capital Consultants LLC, medical payment gaps specialty, medicare, medicare commercial payments | 1 Comment »
BY HEALTH CAPITAL CONSULTANTS, LLC
CMS Innovation Center Launches “Bold New” Strategy
When President Joe Biden was elected in 2020, there was much anticipation and speculation regarding what his election would mean for the U.S. healthcare industry in the coming years.
CITE: https://www.r2library.com/Resource/Title/0826102549

As an ardent supporter of the Patient Protection and Affordable Care Act (ACA) who campaigned on offering a public insurance option similar to Medicare, many in the healthcare industry assumed that the Biden Administration would be a strong proponent of continuing the shift to value-based care, which shift was largely spurred by his predecessor and former boss, Barack Obama, with the passage of the ACA. (Read more…)
YOUR COMMENTS ARE APPRECIATED.
***
Thank You
***
Filed under: "Advisors Only", "Doctors Only", Accounting, Breaking News, Career Development, Experts Invited, Health Insurance, Health Law & Policy, Healthcare Finance, Practice Management, Research & Development | Tagged: ACA, CMS, CMS Innovation, value based care, VBC | Leave a comment »
BY ERIC BRICKER MD
YOUR COMMENTS ARE APPRECIATED.
MORE: https://medicalexecutivepost.com/2021/05/27/activity-based-medical-cost-accounting-and-management/
***
Filed under: Ethics, Events-Planner, Health Economics, Health Insurance, Health Law & Policy, Research & Development, Videos | Tagged: capitation, Fee For Servioce, FFS, value based care, VBC | Leave a comment »

By Dr. David Edward Marcinko MBA CMP©
SPONSOR: http://www.CertifiedMedicalPlanner.org
A Medical Practice Misrepresentation Case Model
Let’s say a physician decided to sell his practice and move to another state. The value of the sale was based, in part, on the yearly gross of the practice. The physician accepted installment payment terms from the buyer and moved to the new state. The buyer began to practice medicine at his new office. Although he was busy, his gross never approached the gross of the prior physician.
Eventually the buyer defaulted on the loan. The selling physician sued for the deficit. The defaulting physician and his forensic consultants then performed an in-depth evaluation of the seller’s practice. The buyer and his team noticed some discrepancies in the billing patterns and practices of the seller. Considering these discrepancies to constitute Medicare and insurance billing fraud, the seller counter-sued the buyer on the grounds of misrepresentation, alleging the gross receipts of the practice purchase price, was grossly inflated.
Citation: https://www.r2library.com/Resource/Title/0826102549
ASSESSMENT: Therefore, the buyer determined that the seller had fraudulently misrepresented the potential of the practice. He also notified state and federal authorities and filed complaints of insurance fraud against the seller.
The seller thought that he would move to the good life in the new state, but his old practice kept him in constant legal trouble.
YOUR THOUGHTS ARE APPRECIATED
Order Textbook: https://www.routledge.com/Risk-Management-Liability-Insurance-and-Asset-Protection-Strategies-for/Marcinko-Hetico/p/book/9781498725989
SECOND OPINIONS: https://medicalexecutivepost.com/schedule-a-consultation/
INVITE DR. MARCINKO: https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
THANK YOU
***
Filed under: Accounting, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Practice Management, Recommended Books, Risk Management | Tagged: David Edward Marcinko, Medical Practice Misrepresentation, Medical Practice Misrepresentation Risks, practice appraisal, practice fraud, practice value | Leave a comment »
ALIGNMENT / MISALIGNMENT INNOVATION?
By Dr. Eric Bricker MD
****
***
YOUR COMMENTS ARE APPRECIATED.
Thank You
***
***
***
Filed under: "Doctors Only", Career Development, Experts Invited, Health Economics, Health Law & Policy, Healthcare Finance, Videos | Tagged: Eric Bricker MD, fee for service medicine, FFS, health plan alignment, health plan misalignment, HMO, network, PPO | Leave a comment »
Hospitals Must Treat All Patients
BY ERIC BRICKER MD
***
The Emergency Medical Treatment and Active Labor Act is an act of the United States Congress, passed in 1986 as part of the Consolidated Omnibus Budget Reconciliation Act
CITE: https://www.r2library.com/Resource/Title/0826102549
***
***
***
YOUR COMMENTS ARE APPRECIATED.
****
***
Thank You
***
***
Filed under: "Ask-an-Advisor", Ethics, Experts Invited, Health Economics, Health Insurance, Health Law & Policy, Videos | Tagged: COBRA, EMTALA, Eric Bricker MD | Leave a comment »
MEDICAID AND A.C.A. the GIANT
By Eric Bricker MD
****
***
YOUR COMMENTS ARE APPRECIATED.
***
Thank You
***
Filed under: "Advisors Only", "Doctors Only", Accounting, Career Development, Experts Invited, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Op-Editorials, Videos | Tagged: ACA, Centene, centene medicaid hmo, Eric Bricker MD, HMO, MCO, Medicaid, Medicaid HMO | Leave a comment »
But Also That It Varies from 150% to 400%.

BY ERIC BRICKER MD
Health Insurance Companies Paid for Hospital Outpatient Services at an Even Higher Average Rate of 293% of Medicare.
A Detailed Look at the RAND Analysis Reveals that the ‘Basket’ of Services at Each Hospital Had Very Little Data.
For Example, the RAND Study’s Data for the Baylor Scott & White Hospital System in Dallas – Fort Worth Represented Only 0.4% of the Hospital’s Total Revenue.
For the Texas Health Hospital System Also in Dallas – Fort Worth, the RAND Study’s Data Only Represented 0.96% of the Hospital’s Total Revenue.
That Sample Size Is Likely Too Small to Make Accurate Comparisons from One Hospital System to Another Regarding their Commercial Insurance Prices Relative to Medicare.
ASSESSMENT: Your thoughts and comments are appreciated.
THANK YOU
***
Filed under: Ethics, Experts Invited, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Insurance Matters, Managed Care, Quality Initiatives, Videos | Tagged: Commercial health insurance, Eric Bricker MD, hospital reimbursement, medicare, Part C, Rand | 1 Comment »
Healthcare Costs Projected to Grow in 2022
A June 2021 PricewaterhouseCoopers (PwC) report found that healthcare costs have been on a steady decline for the past decade, but trailing effects from the COVID-19 pandemic could cause increases above anticipated rates over the next several years.
In 2007, the annual cost growth for healthcare spending was 11.9% and declined steadily until 2017, where it floated between 5.5% and 6.0% until 2020. However, projected healthcare cost growth for 2022 is expected to reach 6.5% due to factors such as deferred or forgone care, increased mental health issues, preparation for future pandemics, and investment in digital tools. (Read more...)
ASSESSMENT: Your thoughts are appreciated.
Citation: https://www.r2library.com/Resource/Title/0826102549
THANK YOU
***
***
Filed under: Experts Invited, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance | Tagged: Health Capital Consultants LLC, health care costs, Healthcare Costs Grow in 2022, PwC | 1 Comment »
36 Blue Cross Health Insurance Companies Explained

BY ERIC BRICKER MD
***
***
PODCAST: https://www.ahealthcarez.com/blue-cross-explained
***
***
***
Filed under: Career Development, Experts Invited, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Insurance Matters, Videos | Tagged: BC/BS, Blue Cross, Blue Cross Shield, Blue Shield, Eric Bricker MD, Health Insurance Companies Explained | Leave a comment »















































