BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on October 2, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
LESSONS FROM THE RETAIL SECTOR
***
Discover how ProMedica uses customer feedback and a digital-first approach to consumers to achieve stellar results across more than 400 facilities in 28 states.
How much will it cost you to start a dental practice – with Business Plan?
There are many costs to consider to set up a successful dental practice. Note that the following values are not the exact amount but an average of setting up a dental practice:
Purchase price – this includes valuation fees of between $1,000-4,500, solicitor fees of between $4,000 – 17,000, accountancy and bank fees of around $3,000, and bank solicitors, which can be up to $3,500. Many of these can be reduced or obliterated.
Materials – $40,000
Lab fees – $36,000
Staff costs – $82,000
Other costs (associates fees) – [$245,000 – $295,000]
Other Factors
“Big” Tech – Many startup doctors want to include CBCT or CAD/CAM or 3D printing in their startup, any of which can add $25,000-$175,000. In other situations, waiting is the best option.
Cabinetry Preferences – Costs for cabinetry can range from $5,000 to $175,000.
Practice Management Software (PMS) – Pricing will range from a few thousand dollars to $25,000; OR none at all.
Mechanical Delivery – Typically referred to as chairs, lights, and units, this category of dental equipment costs will range between $5,000 and $100,000 based on your startup plans.
Vision – Ignore the so-called “experts” who will try to create a cookie-cutter model for your equipment costs. That is the thinking of corporate dentistry. You want a customized private practice vision that allows you to create a model matching your standards. Prioritize your vision, so your values and philosophy will lead your dental equipment budget and purchasing decisions. Your equipment budget will be—and should be—customized.
Posted on September 28, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
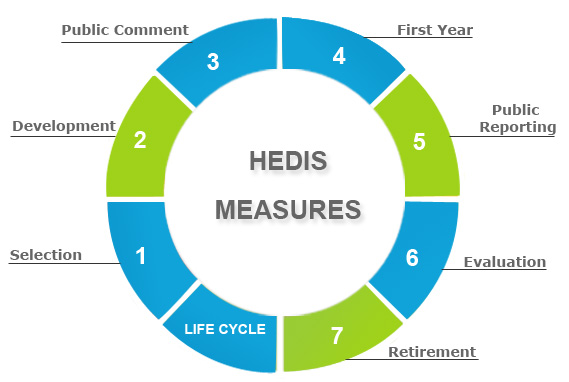
90 NCQI MEASUREMENTS
BY ERIC BRICKER MD
The Healthcare Effectiveness Data and Information Set (HEDIS) is a tool used by more than 90 percent of U.S. health plans to measure performance on important dimensions of care and service. More than 190 million people are enrolled in health plans that report quality results using HEDIS.
The National Committee for Quality Assurance is an independent 501 nonprofit organization in the United States that works to improve health care quality through the administration of evidence-based standards, measures, programs, and accreditation.
Posted on September 26, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
BY ENTREPRENUER MD AND ROBERT PEARL MD
In this episode the Entrepreneur MD is joined by Dr Robert Pearl, MD, to talk about his latest book Uncaring and the need to stand up against the current healthcare model.
Posted on September 7, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
The boom and bust of private equity-owned dental practices in the U.K …. Lessons to be learned?
By Darrell Kellus Pruitt DDS
“Why the dental business became more and more like pulling teeth,” by Harry Wilson, City Editor of The Times (U.K.)
Describes problems caused by agreements made between investor-owned dental groups and the government. Neither the investors nor government officials – the stakeholders – will suffer the inevitable permanent harm. The losers are dentists and patients – the principals.
If you are an NHS dental patient, there is a better than one in ten chance that you are a customer of Integrated Dental Holdings, better known as Mydentist.
The private equity-owned dental practice owner has grown nationwide in a dozen years of debt-fuelled buying that has made it the biggest dental services company not merely in Britain but Europe. In the past seven years alone, Mydentist has acquired 237 dental practices, increasing its network to more than 600.
Yet having grown so rapidly in the recent past, questions now are being asked about its future. Results last month showed why, as revenues fell for the third straight year, while pre-tax losses nearly doubled to £144 million. With more than £1 billion of debt, including hundreds of millions in shareholder loans to The Carlyle Group and Palamon Capital Partners, its private equity owners, Mydentist said that it would not be buying any more dentist surgeries for the time being. (more).
———————
Bringing it home:
Rumors of “Medicare for all” are in the air, making your support of Texas Dentists for Medicaid Reform very worthwhile, Doc.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
Posted on September 3, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
A QUARTET OFREASONS!
It’s going to be a good idea to do everything you can to help your company succeed. One good thing that you can do for your company is to create a clear mission statement.
Why is a mission statement so important for your company, though? Read on to learn exactly why your company needs a clear mission statement so much.
Posted on August 29, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
EMR OVERVIEW
BY ERIC BRICKER MD
Electronic Medical Records (EMRs) are Used by 80-90% of Hospitals and Physician Practices. One Study Found that EMRs Have Lowered Patient Mortality by 0.09%.
Posted on August 4, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
***
TEXTBOOKREVIEW
Drawing on the expertise of decision-making professionals, leaders, and managers in health care organizations, Hospitals & Health Care Organizations: Management Strategies, Operational Techniques, Tools, Templates, and Case Studies addresses decreasing revenues, increasing costs, and growing consumer expectations in today’s increasingly competitive health care market.
Offering practical experience and applied operating vision, the authors integrate Lean managerial applications, and regulatory perspectives with real-world case studies, models, reports, charts, tables, diagrams, and sample contracts. The result is an integration of post PP-ACA market competition insight with Lean management and operational strategies vital to all health care administrators, comptrollers, and physician executives. The text is divided into three sections:
Managerial Fundamentals
Policy and Procedures
Strategies and Execution
Using an engaging style, the book is filled with authoritative guidance, practical health care–centered discussions, templates, checklists, and clinical examples to provide you with the tools to build a clinically efficient system. Its wide-ranging coverage includes hard-to-find topics such as hospital inventory management, capital formation, and revenue cycle enhancement. Health care leadership, governance, and compliance practices like OSHA, HIPAA, Sarbanes–Oxley, and emerging ACO model policies are included. Health 2.0 information technologies, EMRs, CPOEs, and social media collaboration are also covered, as are 5S, Six Sigma, and other logistical enhancing flow-through principles. The result is a must-have, “how-to” book for all industry participants.
There is Copay for Each Office Visit and Visits are Unlimited.
Direct Primary Care Doctors Are Most Frequently Family Practice Physicians, but Internal Medicine and Pediatricians Can Also Have Direct Primary Care Practices.
The Average Direct Primary Care Practice Has a Panel of 345 Patients, with a Goal of About 600 Patients at Full Capacity.
For Comparison, the Typical Fee-for-Service Primary Care Doctor Has a Patient Panel of 2,500.
57% of Direct Primary Care Practices Contract with Employers That Pay the Monthly Membership on the Employee’s Behalf.
Direct Primary Care is a Strategy to Increase the Quality of Care and Decrease Healthcare Costs for an Employee Health Plan.
Disclaimer: Dr. Bricker is the Chief Medical Officer of Virtual Care Company First Stop Health.
Posted on July 21, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
TEXTBOOK RELEASE AND REVIEW
Reviews
Navigating a course where sound organizational management is intertwined with financial acumen requires a strategy designed by subject-matter experts. Fortunately, Financial Management Strategies for Hospital and Healthcare Organizations: Tools, Techniques, Checklists and Case Studiesprovides that blueprint. ―David B. Nash, MD, MBA,Jefferson Medical College, Thomas Jefferson University
It is fitting that Dr. David Edward Marcinko, MBA, CMP™ and his fellow experts have laid out a plan of action in Financial Management Strategies for Hospital and Healthcare Organizationsthat physicians, nurse-executives, administrators, institutional CEOs, CFOs, MBAs, lawyers, and healthcare accountants can follow to help move healthcare financial fitness forward in these uncharted waters. ―Neil H. Baum, MD, Tulane Medical School
Recruitment has become a refined art in recent years as practices and physicians themselves grow increasingly savvy about the finer points of marketing positions and securing employment. It’s more competitive than ever, too. Many organizations are going after the same physicians. Add to that a shortage of doctors in key specialties and certain geographical areas and the pressure becomes that much more intense. Moreover, the aging of the physician workforce, their increased dissatisfaction with managed care, and changes in doctors’ work expectations (they want more free time) have affected the demand and supply.
Additionally, both practicing physicians and residents fresh out of training have become more discerning and skillful in managing the search process. Candidates have learned to be selective based on how they’re treated on the phone, how they’re treated in person during site visits, or how smoothly the negotiations go. One small bump in the road and they could choose to go elsewhere. In truth, they look to rule organizations out, not in.
Even the smallest of practices must have an effective recruitment plan because they compete directly with the big guys — larger practices and hospitals that have polished their efforts and perfected their processes.
Facts about Physician Recruiters and Executive Search Firms
1) If you are job hunting, you should send your resume to recruiters
Different recruiters know about different positions. They do not usually know about the same ones. This is particularly true with retained firms. By sending your resume out widely, you will be placed in many different confidential databases and be alerted of many different positions. If you send your resume to only a few, it may be that none you send to will be working with positions which are suited for you. Throw your net widely.
If you change jobs, it is also wise to send follow-up letters to the recruiters and alert them of your new career move. Many search firms follow people throughout their careers and enjoy being kept up-to-date. It is a good idea to have your resume formatted in plain text so you can copy and paste it into email messages when requested to do so. Then, follow up with a nicely formatted copy on paper by postal mail.
Some estimate that only 1% to 3% of all resumes sent will result in actual job interviews. So, if you only send 50 resumes, you may only have less than 2 interviews, if that many. Send your resume to as many recruiters as you can. It is worth the postage or email time. Generally, recruiters will not share your resume with any employer or give your name to anyone else without obtaining your specific permission to do so. The recruiter will call first, talk to you about a particular position and then ask your permission to share your resume with that employer.
2) Your resume will be kept strictly confidential by the executive search firm.
It is safe to submit your resume to a search firm and not worry that the search firm will let it leak out that you are job hunting. Recruiters will call you each and every time they wish to present you to an employer in order to gain your permission. Only after they have gained your permission will they submit your name or resume to the identified employer. The wonderful aspect of working with search firms is that you can manage your career and your job search in confidence and privacy.
3) Fees are always paid by the employer, not the job candidate.
Recruiters and search firms work for the employer or hiring entity. The employer pays them a fee for locating the right physician for the job opening. This is important to remember, in that when you interact with executive recruiters, you are essentially interacting with an agent or representative of the employer. Recruiters are more loyal to employers than they are to job candidates because they work for the employer. This should not present a problem, but, should cause you to develop your relationship with the recruiter with the same integrity and professionalism that you would with the employer.
Recruiters are paid fees in one of two ways – retainer fees or contingency fees. This is an important distinction and will affect your process with both the employer and the recruiter. Some employers prefer working with contingency firms and some with retained firms. Both are respected by employers and useful in your job search, but, the two types of firms will not be handling the same positions with the same employers simultaneously.
A “retained” recruiter has entered an exclusive contract with an employer to fill a particular position. The retained recruiter, then, is likely to advertise a position, sharing the specifics of the position, location and employer openly. The retained firm feels a great obligation to fulfill the contract by finding the best person for the job.
A “contingency recruiter” on the other hand, usually does not have an exclusive relationship with the employer, and is only paid a fee if the job search is successful. Often, if the employer uses contingency firms, there will be more than one contingency firm competing to fill a certain position. As a job hunter, if you are sent to an interview by a contingency firm, you may find that you are competing with a larger number of applicants for a position. Generally, retained firms only send in from 3 to 5 candidates for a position.
Recruiters will be paid fees equal to about 25% to 35% of the resulting salary of the successful candidate plus expenses. This does not come out of the job candidate’s salary. This is paid to the recruiter through a separate relationship between the employer and the search firm. This may seem like a large fee, but, keep in mind that recruiters incur a great many expenses when searching for successful job candidates. They spend enormous amounts of money on computer systems, long distance calls, mail-outs, travel and interviews. Recruiters work very hard for these fees. Employers recognize the value of using recruiters and are more than willing to pay recruiters the fees. All you have to do is contact the recruiter to get the process moving.
4) Not all medical recruiters work only with physicians.
Some search firms work exclusively with physicians or in healthcare, while others may work in several fields at once. Some of the larger generalist firms will have one or more search consultants that specialize in healthcare. It is important for you, as a job hunter, to assess the recruiters’ knowledge of your field. If you use industry or medical specialty buzz words in describing your skills, experience or career aspirations, you may or may not be talking a language the recruiter understands fully. It is wise to explore fully with the recruiter his understanding of your field and area of specialization.
5) Recruiters and search consultants move around.
Recruiters, like many professionals, move to new firms during their careers. Often you will find that recruiters will work at several firms during their careers. Since it is much more effective to address your letters to a person rather than “to whom it may concern”, it is smart for job hunters to have accurate and up-to-date information about who is who and where, since this can change frequently. Search firms also move their offices, sometimes to another suite, street or state. If you have a list of recruiters that is over one year old, you will certainly waste some postage in mailing your resumes and cover letters. Many of your mail-outs will be returned to you stamped “non-deliverable”, unless you obtain an up-to-date list. A resource, like the Directory of Healthcare Recruiters is updated very frequently, usually monthly [www.pohly.com/dir3.html].
6) Most search firms work with positions all over the country.
If you are from a particular state, and want to remain in that state, don’t make the mistake of only sending your resume to recruiters in your state. Often the recruiters in your state are working on positions in other states, and recruiters in other states are working on positions in your state. This is usually the case. Very few recruiters work only in their local area, most work all around the US and some internationally. Regardless of your geographic preference, you should still send your resume to all the healthcare recruiters. If you really only want to remain in your area, you can specify that preference in your cover letter.
7) Recruiters primarily work with hard to fill positions or executive positions.
Some recruiters specialize in clinical positions for physicians, managed care executive positions, healthcare financial positions or health administration positions. Others may specialize in finding doctors, nurses or physical therapists. Generally, an employer does not engage a recruiter’s assistance in filling a position unless it is hard to fill. Sometimes employers will engage search firms to save them the valuable time of advertising or combing through dozens of resumes.
Contingency recruiters tend to work with more mid-level management and professional positions, but, this is not always the case. Retained firms generally work with the higher level clinical or administrative positions.
One thing you will be assured of is that if a recruiter is working on a position that means that the employer is willing to pay a fee. That usually means that the position is a valued position and one worth closer inspection on your part. Even in healthcare, with certain exceptions, our economy is an “employer’s market”. This means that employers receive a deluge of resumes for their open positions. Increasingly, employers are using recruitment firms to handle their openings and schedule the interviews because employers simply do not have the manpower or time to handle the many resumes they receive. Therefore, if a job hunter is submitted by a recruiter, that job hunter has a great advantage over all other applicants.
Managed care is a prospective payment method where medical care is delivered regardless of the quantity or frequency of service, for a fixed payment, in the aggregate. It is not traditional fee-for-service medicine or the individual personal care of the past, but is essentially utilitarian in nature and collective in intent. Will new-age healthcare reform be even more draconian?
Unhappy Physicians
There are many reasons why doctors are professionally and financially unhappy, some might even say desperate, because of managed care; not to mention the specter of healthcare reform from the Obama administration. For example:
A staggering medical student loan debt burden of $100,000-250,000 is not unusual for new practitioners. The federal Health Education Assistance Loan (HEAL) program reported that for the Year 2000, it squeezed significant repayment settlements from its Top 5 list of deadbeat doctor debtors. This included a $303,000 settlement from a New York dentist, $186,000 from a Florida osteopath, $158,000 from a New Jersey podiatrist, $128,000 from a Virginia podiatrist, and $120,000 from a Virginia dentist. The agency also excluded 303 practitioners from Medicare, Medicaid, and other federal healthcare programs and had their cases referred for nonpayment of debt.
Because of the flagging economy, medical school applications nationwide have risen. “Previously, there were a lot of different opportunities out there for young bright people”; according to Rachel Pentin-Maki; RN, MHA”; not so today. In fact, Physicians Practice Digest recently stated, “Medicine is fast becoming a job in which you work like a slave, eke out a middle class existence, and have patients, malpractice insurers, and payers questioning your motives.” Remarkably, the Cornell University School of Continuing Education has designed a program to give prospective medical school students a real-world peek, both good and bad.
The Ripple Effects of Managed Care and Reform
“Many people who are currently making a great effort and investment to become doctors may be heading for a role and a way of life that are fundamentally different from what they expect and desire,” according to Stephen Scheidt, MD, director of the $1,000 Cornell fee program; why?
Fewer fee-for-service patients and more discounted patients.
More paperwork and scrutiny of decisions with lost independence and morale.
Reputation equivalency (i.e., all doctors in the plan must be good), or commoditization (i.e., a doctor is a doctor is a doctor).
The provider is at risk for (a) utilization and acuity, (b) actuarial accuracy, (c) cost of delivering medical care, and (d) adverse patient selection.
Practice costs are increasing beyond the core rate of inflation.
Medicare reimbursements are continually cut.
Early Opinions
Richard Corlin MD, opined back in 2002 that “these are circumstances that cannot continue because we are going to see medical groups disappearing.” Furthermore, he stated, “This is an emergency that lawmakers have to address.” Such cuts also stand to hurt physicians with private payers since commercial insurers often tie their reimbursement schedules to Medicare’s resources. “That’s the ripple effect here,” says Anders Gilberg, the Washington lobbyist for the Medical Group Management Associations (MGMA).
Assessment
And so, some desperate doctors are pursing these sources of relief, among many others:
A growing number of doctors are abandoning traditional medicine to start “boutique” practices that are restricted to patients who pay an annual retainer of $1,500 and up for preferred services and special attention. Franchises for the model are also available.
Regardless of location, the profession of medicine is no longer ego-enhancing or satisfying; some MDs retire early or leave the profession all together. Few recommend it, as a career anymore.
Assessment
To compound the situation, it is well known that doctors are notoriously poor investors and do not attend to their own personal financial well being, as they expertly minister to their patients’ physical illnesses.
Conclusion
And so, your thoughts and comments on this Medical Executive-Post are appreciated. Tell us what you think? Are you a desperate doctor? Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe to the ME-P. It is fast, free and secure.
Posted on July 12, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
MANAGEMENT STRATEGIES, OPERATIONAL TECHNIQUES, TOOLS, TEMPLATES AND CASE STUDIES
TEXTBOOKREVIEWS:
Hospitals and Health Care Organizationsis a must-read for any physician and other health care provider to understand the multiple, and increasingly complex, interlocking components of the U.S. health care delivery system, whether they are employed by a hospital system, or manage their own private practices.
The operational principles, methods, and examples in this book provide a framework applicable on both the large organizational and smaller private practice levels and will result in better patient care. Physicians today know they need to better understand business principles and this book by Dr. David E. Marcinko and Professor Hope Rachel Hetico provides an excellent framework and foundation to learn important principles all doctors need to know. ―Richard Berning, MD, Pediatric Cardiology
… Dr. David Edward Marcinko and Professor Hope Rachel Hetico bring their vast health care experience along with additional national experts to provide a health care model-based framework to allow health care professionals to utilize the checklists and templates to evaluate their own systems, recognize where the weak links in the system are, and, by applying the well-illustrated principles, improve the efficiency of the system without sacrificing quality patient care. … The health care delivery system is not an assembly line, but with persistence and time following the guidelines offered in this book, quality patient care can be delivered efficiently and affordably while maintaining the financial viability of institutions and practices. ―James Winston Phillips, MD, MBA, JD, LLM
Posted on July 5, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
At Least in PartACCORDING TO THESE BOOKS
BY ERIC BRICKER MD
Understandably, Many Doctors Take Issue with This Accusation and Say They Treat Their Patients with Integrity and Accountability. Both Statements May Be TRUE … How is That Possible?
Because of ‘Bad Apples.’
While the Majority of Physicians May Put Their Patients First, There Are a Minority of Physicians that Put Money, Power, Prestige and Promotions Ahead of Patients. It’s These Bad Apples That Ruin Physician Culture.
Problem: Fee-for-Service Rewards Bad Apple Physicians, While Paying the High-Integrity Doctors as Well.
Assessment: If Doctors Want to Keep Fee-for-Service, Then the Bad Apples Must Be Reduced Through 1) Increased Transparency, 2) Greater Doctor Self-Regulation, 3) More Federal Oversight and 4) Increased Employer Investigation.
However, That 5% of High-Cost Claimants is a Heterogenous Population
2.5 Percentage Points of the 5% Are Claimants That Were Either High-Cost Claimants the Previous Year with On-Going Complex Medical Situations or Generated Claims Related to Chronic Diseases Such as Diabetes or Multiple Sclerosis.
HOWEVER, the Other 2.5 Percentage Points of the 5% Are Claimants That Generated Zero or Almost-Zero Claims in the Previous 12-Months.
They Essentially ‘Blow Up’ Out of Nowhere.
This Video Describes the 4 Categories of These High-Cost Claimants:
1) Previously Known and Prolonged High Costs
2) Previously Known and Episodic High Costs (that no longer continue)
3) Previously Unknown and Prolonged High Costs
4) Previously Unknown and Episodic High Costs (that no longer continue)
Learn the Clinical Diagnoses That Make Up Each Category and the Secret of Which Groups to Target and Why.
Nurses on General Medical and Surgical Floors Typically Have a 4:1 Patient to Nurse Ratio During the Day and an 8:1 Patient to Nurse Ratio Overnight.
Nurses in the ICU Typically Have a 2:1 or 1:1 Patient to Nurse Ratio.
Nurses on a Floor or Unit Have a ‘Charge Nurse‘ Who is the Head Nurse for the Floor for That Specific Shift.
Those Charge Nurses Then Collaborate with the Shift Coordinator Who is a Very Senior and Experience Nurse Who Coordinates All the Patient Beds for a Particular Division at a Large Hospital (e.g. All Medicine Patients vs. All Surgical Patients) or for the Entire Hospital If It Is a Smaller Hospital.
Medical Techs Provide Support Roles in Patient Rooms Such as Checking Vitals, Blood Glucose Finger-Sticks, Etc.
The Clerk Sits at the Nurses Station for the Floor and Typically Answers the Call-Button for Each of the Patient Rooms During the Day in Addition To Their Administrative Responsibilities.
Posted on June 20, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Management Strategies, Operational Techniques, Tools, Templates and Case Studies
Tex Book Review
Drawing on the expertise of decision-making professionals, leaders, and managers in health care organizations, Hospitals & Health Care Organizations: Management Strategies, Operational Techniques, Tools, Templates, and Case Studies addresses decreasing revenues, increasing costs, and growing consumer expectations in today’s increasingly competitive health care market.
Offering practical experience and applied operating vision, the authors integrate Lean managerial applications, and regulatory perspectives with real-world case studies, models, reports, charts, tables, diagrams, and sample contracts. The result is an integration of post PP-ACA market competition insight with Lean management and operational strategies vital to all health care administrators, comptrollers, and physician executives. The text is divided into three sections:
Managerial Fundamentals
Policy and Procedures
Strategies and Execution
Using an engaging style, the book is filled with authoritative guidance, practical health care–centered discussions, templates, checklists, and clinical examples to provide you with the tools to build a clinically efficient system. Its wide-ranging coverage includes hard-to-find topics such as hospital inventory management, capital formation, and revenue cycle enhancement. Health care leadership, governance, and compliance practices like OSHA, HIPAA, Sarbanes–Oxley, and emerging ACO model policies are included. Health 2.0 information technologies, EMRs, CPOEs, and social media collaboration are also covered, as are 5S, Six Sigma, and other logistical enhancing flow-through principles. The result is a must-have, “how-to” book for all industry participants.
Posted on June 17, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Dr. David E. Marcinko is at your Service
Dr. David Edward Marcinko MBA CMP® enjoys personal coaching and public speaking and gives as many talks each year as possible, at a variety of medical society and financial services conferences around the country and world.
These have included lectures and visiting professorships at major academic centers, keynote lectures for hospitals, economic seminars and health systems, keynote lectures at city and statewide financial coalitions, and annual keynote lectures for a variety of internal yearly meetings.
His talks tend to be engaging, iconoclastic, and humorous. His most popular presentations include a diverse variety of topics and typically include those in all iMBA, Inc’s textbooks, handbooks, white-papers and most topics covered on this blog.
Posted on June 16, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
DEFINITION:Telehealth is the distribution of health-related services and information via electronic information and telecommunication technologies. It allows long-distance patient and clinician contact, care, advice, reminders, education, intervention, monitoring, and remote admissions.
Telehealth could include two clinicians discussing a case over video conference; a robotic surgery occurring through remote access; physical therapy done via digital monitoring instruments, live feed and application combinations; tests being forwarded between facilities for interpretation by a higher specialist; home monitoring through continuous sending of patient health data; client to practitioner online conference; or even videophone interpretation during a consult.
Rich talks with veteran Telehealth executive, C.J. Mark about the growth of Telehealth in the last decade. They discuss the issues surrounding Telehealth, and how Covid has accelerated the importance of remote medical care.
Each generation of doctors and medical professionals is extraordinarily complex, bringing various skills, expertise and expectations to the modern medical work environment. Determining the best method to unite such diverse thinking is one of the many challenges faced by physician executives and healthcare leaders today.
And, as linguistic evolution occurs, the nomenclature of hospitalist was followed by that of intensivist, proceduralist and nocturnalist, etc [www.MedInnovationBlog.com and Personal communication Richard L. Reece MD].
Is it any wonder that many medical leaders and executive in the Baby Boomer generation find themselves at a loss? The days of functional leadership are gone and suddenly, no one cares about the expertise of the Baby Boomers or how they climbed the corporate ladder, in medicine or elsewhere. Leadership in the new era is no longer about command-control or dictating with intense focus on the bottom line; it is about collaboration, empowerment and communication. And, it is not about titles and nomenclature; it is about lifestyle choice.
What else drives these new-wave specialists?
The answer, of course, is the next-generation of physicians and their emerging new medical business and practice models, which include:
“Ambulists” are doctors that travel locally, have no, or only a sparse physical office presence of their own. They sporadically provide services that are additive to traditional practice models [i.e., endocrinologist in a large family medical office with many diabetics].
“In-Situ” physicians regularly provide services that are complimentary to existing traditional practice models [i.e., dentists or podiatrists in a medical practice].
“Laborists” are obstetricians that do not wish to be on-call. First begun in Cape Cod and other Massachusetts hospitals, such obstetricians work regular shifts for the sole purpose of delivering babies.
“Locum Tenens” doctors travel around the country as itinerants [i.e., cruise ships] as temporary substitutes for another the same specialty.
“Officists” remain in their own physical practice, and rarely see patients in the hospital, nursing home, patient home, out-patient facility, etc.
Finally, “dayhawk physicians” mimic the “nighthawk physician” model where radiologists in remote locations read films in the middle of the night as cash-strapped hospitals often find it cheaper to outsource with better services and more timely interpretations in many cases.
Posted on June 13, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
See the Future of Healthcare By Looking to Medicare’s Past
***
BY DR. ERIC BRICKER MD
***
Desire for a Healthcare ‘Safety Net’ Goes Back Almost 100 years to President F.D.R. and His “New Deal“
FDR Was Able to Pass Social Security, but He Also Wanted a Healthcare Safety Net Too.
Presidents Truman and Kennedy Also Wanted a Federally-Funded Healthcare Safety Net.
LBJ Carried the Torch of the Healthcare Safety Net. He Was Able to Have Medicare Legislation Passed in 1965 by Combining 3 Separate Proposals and Acts:
1) Hospital Insurance
2) Doctor Insurance That Was Voluntary
3) the State-Administered Kerr-Mills Act
Hospital Insurance Became Medicare Part A. Doctor Insurance Became Medicare Part B. The Kerr-Mills Act Became Medicaid.
Presidents Carter and Clinton Also Wanted to Expand the Healthcare Safety Net. President Obama Expanded the Healthcare Safety Net with Passage of Obamacare. President Biden is Seeking to Expand the Healthcare Safety Net Too.
The Arc of Government-Funded Healthcare Stretches Back Almost 100 Years and Will Inevitably Result in the Full Government Payment for Healthcare in America.
It’s Not a Question of If, But When.
Implication:United Health Group is Making Many Acquisitions to Become a Vertically Integrated Healthcare Company to Position Itself as a Major Government Contractor for the Eventual Federal Takeover.
Posted on June 11, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Bhagwan Satiani, MD, MBA, DFSVS, FACHE, FACS
Todd A. Zigrang, MBA, MHA, FACHE, CVA, ASA
Jessica L. Bailey-Wheaton, JD
ABSTRACT
The appropriate focus in managing the COVID-19 pandemic in the United States has been addressing access and delivery of care to the population affected by the outbreak. All sectors of the U.S. economy have been significantly affected,including physicians. Physician groups of all specialties and sizes have experienced the financial effects of the pandemic.Hospitals have received billions of dollars to support and enable them to manage emergencies and cover the costs of the disruption.
However, many vascular surgeons are under great financial pressure because of the postponement of all non-emergency procedures. The federal government has announced a myriad of programs in the form of grants and loans to reimburse physicians for some of their expenses and loss of revenue. It is more than likely that unless the public health emergency subsides significantly, many practices will experience dire consequences without additional financial assistance.
The authors have attempted to provide a concise listing of such programs and resources available to assist vascular surgeons who are small businesses in accessing these opportunities.
Posted on June 9, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
A Hardening Market Arrives Just in Time TO GREET the GLOBAL Pandemic
The year 2019 marked a turning point for the medical professional liability (MPL) insurance industry. Reserve releases declined to less than 5% of premium. Insurers projected a combined ratio over 120% on 2019 earned business. Frequency increased for many writers and the trend in indemnity severity was above inflation. In response, insurers began to take rate action, manifesting in growth in direct written premium that exceeded inflation for the first time since 2005.
Despite significant underwriting losses, the MPL industry returned double its net income for the year as dividends to policyholders. Policyholder dividends show little sign of declining as the MPL industry remains well-capitalized and able to fund policyholder dividends with investment income.
Just as it is an acceptable and reasonable practice to screen incoming patients, it is acceptable and reasonable to know when to end relationships. Termination criteria are numerous and varied. Although not exhaustive, the following are situations in which termination may be appropriate and acceptable:
Treatment noncompliance—The patient does not or will not follow the treatment plan.
Follow-up noncompliance—The patient repeatedly cancels follow-up visits or is a no-show.
Office policy noncompliance—The patient uses weekend on-call physicians or multiple health care practitioners to obtain refill prescriptions when office policy specifies a certain number of refills between visits.
Verbal abuse—The patient or a family member is rude and uses improper language with office personnel, exhibits violent behavior, makes threats of physical harm, or uses anger to jeopardize the safety and well-being of office personnel with threats of violent actions.
Nonpayment—The patient owes a backlog of bills and has made no effort to arrange a payment plan.
It is an acceptable practice to end a patient relationship under most conditions. There are a few situations, however, that may require additional steps or a delay of the termination. According to The Doctors Company, Laura A. Dixon JD RN,the following circumstances fall into this category:
If the patient is in an acute phase of treatment, termination must be delayed until the acute phase has passed. For example, if the patient is in the immediate postoperative stage or is in the process of medical workup for diagnosis, it is not advisable to end the relationship.
If the practitioner is the only source of medical or dental care within a reasonable driving distance, he or she may need to continue care until other arrangements can be made.
When the practitioner is the only source of a particular type of specialized medical or dental care, he or she is obliged to continue this care until the patient can be safely transferred to another practitioner who is able to provide treatment and follow up.
If the patient is a member of a prepaid health plan, the patient cannot be discharged until the practitioner has communicated with the third-party payer to request a transfer of the patient to another practitioner.
A patient may not be terminated solely because he or she is diagnosed with AIDS/HIV.
When the situation with the patient is such that terminating the relationship is appropriate and acceptable and none of the restrictions mentioned above are present, termination of the patient relationship should be completed formally. The patient should be put on written notice that he or she must find another health care practitioner. The written notice should be mailed to the patient by regular and certified mail, return receipt requested. Keep copies of the letter, the original certified mail receipt, and the original certified mail return receipt (even if the patient refuses to sign for the certified letter) in the patient’s medical record.
Many folks feels that private preventative medical contracts may be one possible solution for those Americans going without healthcare; especially the young and healthy. Generally, and generically, they have a moniker like the “No Health Insurance Club”; or similar
Why?
Some pundits are leaning toward universal healthcare, or Medicare-4-All, which seems too socialized for others. Yet, private insurers continue to increase premiums, which prices healthcare out of reach for the average American. Employers can no longer float the cost of insurance so they pass it on to their employees. Patients aren’t the only ones being affected by the current state of healthcare. More and more doctors are going out of business and hospitals are cutting back due to escalating costs and payment defaults.
So, current remedies to this dilemma include major medical insurance policies for catastrophic events with high-deductibles to keep monthly premiums down, Medicaid, mini retail-clinics at grocery stores/pharmacies, and emergency room visits for common illnesses; as well as the PP-ACA.
Medical Maintenance
But, preventative healthcare and medical maintenance is not typically addressed. More than 90 percent of health related issues can be taken care of with preventative care and maintenance but only a small percentage of Americans currently enjoy the benefit of preventative healthcare. Healthcare economists are rethinking healthcare by offering an affordable alternative to traditional insurance options. NHICs, connect patients with participating board certified physicians that will treat and care for preventative healthcare needs for a one-time prepaid annual membership fee.
In this NHIC model:
Patients make a one-time annual payment that is typically less than a one-month premium with traditional insurance.
Patients receive up to 12 office visits per year that also include immunizations, $10 or less in-office prescriptions, and additional services including blood tests.
No deductible, no co-pays, no premiums.
No surprise bills to patients.
Viable alternative to COBRA for employees disengaged from work.
Low cost option for the self-employed.
The Doctors
What’s in it for the doctors? How about no insurance clerks, no need to snail mail medical insurance claims or use expensive electronic claims submission clearinghouse services, no bad debts or bad expense write-offs, no ARs; and fast cash.
ASSESSMENT: Your thoughts are comments are appreciated.
Posted on June 3, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Dr. Robert Pearl’s Book from Moral Injury to Fee-for-Service … and More
By Eric Bricker MD
Dr. Robert Pearl Was the CEO of the Permanente Medical Group from 1999 to 2017. Permanente is the Physician Group for all of Kaiser Permanente. It is the Largest Physician Group in America with 10,000 Doctors, 38,000 Staff and 5 Million Members.
EDITOR’S NOTE: Normally, book reviews are boring but this presentation from colleague Eric Bricker MD is well worth a watch.
Posted on June 2, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Here are the major issues facing healthcare according to PwC
Will a health system battered by the pandemic emerge stronger in the year ahead? The annual report predicts challenges such as profitably merging virtual and in-person care, and capitalizing on new consumer- and clinician-facing digital health tools.
Posted on June 1, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
By HEALTH CAPITAL CONSULTANTS, LLC
On May 4, 2021, the National Academies for Sciences, Engineering and Medicine (NASEM) released a major report expressing a dire need to improve primary care in the U.S.
Since January 2020, an extensive committee within NASEM has worked to develop an implementation plan that will reopen the discussion of improving primary care as a means to improving overall health and achieving health equity.
Congress bypassed an opportunity in recently enacted COVID-19 relief bills to significantly increase the number of Medicare-funded residency positions at hospitals.
In the last package, which amounted to $1.4 trillion in government spending and was signed by President Trump on December 31, lawmakers set aside $120 million for 1,000 new physician training slots over the next five years. There was a more ambitious bill on the table that would have added 15,000 residencies over the next five years, but it failed to make it into the giant year-end coronavirus relief package.
“The increase of 1,000 slots is a good first step but a far cry from what is needed,” said David Balat, director of the Right on Health initiative at the Texas Public Policy Foundation.
I wish to make one clarification and one prediction regarding employed physicians.
The clarification is this: There is a common misconception that if healthcare operated under free market conditions, it would primarily be a cottage industry of solo practices and of small physician-owned hospitals. Such operations would not develop the capabilities of large healthcare entities that we commonly associate with central planning.
ASSESSMENT: In reality, however, the opposite would be the case.
Emerging fintech apps are looking to apply this lending model to sectors, from health care to travel to rent. Sure, people are growing acclimated to dividing their purchases into four easy payments, even applauding the option to do so.
But no matter how you frame it, the pitfalls of these plans seem to be, unfortunately, just more debt.
Buy now, pay later providers Klarna, Afterpay, and Quadpay spent years slowly infiltrating the retail market. The pandemic has accelerated their popularity among all sorts of online brands
1) If you are job hunting, you should send your resume to recruiters
Different recruiters know about different positions. They do not usually know about the same ones. This is particularly true with retained firms. By sending your resume out widely, you will be placed in many different confidential databases and be alerted of many different positions. If you send your resume to only a few, it may be that none you send to will be working with positions which are suited for you. Throw your net widely.
If you change jobs, it is also wise to send follow-up letters to the recruiters and alert them of your new career move. Many search firms follow people throughout their careers and enjoy being kept up-to-date. It is a good idea to have your resume formatted in plain text so you can copy and paste it into email messages when requested to do so. Then, follow up with a nicely formatted copy on paper by postal mail.
Some estimate that only 1% to 3% of all resumes sent will result in actual job interviews. So, if you only send 50 resumes, you may only have less than 2 interviews, if that many. Send your resume to as many recruiters as you can. It is worth the postage or email time. Generally, recruiters will not share your resume with any employer or give your name to anyone else without obtaining your specific permission to do so. The recruiter will call first, talk to you about a particular position and then ask your permission to share your resume with that employer.
2) Your resume will be kept strictly confidential by the executive search firm.
It is safe to submit your resume to a search firm and not worry that the search firm will let it leak out that you are job hunting. Recruiters will call you each and every time they wish to present you to an employer in order to gain your permission. Only after they have gained your permission will they submit your name or resume to the identified employer. The wonderful aspect of working with search firms is that you can manage your career and your job search in confidence and privacy.
3) Fees are always paid by the employer, not the job candidate.
Recruiters and search firms work for the employer or hiring entity. The employer pays them a fee for locating the right physician for the job opening. This is important to remember, in that when you interact with executive recruiters, you are essentially interacting with an agent or representative of the employer. Recruiters are more loyal to employers than they are to job candidates because they work for the employer. This should not present a problem, but, should cause you to develop your relationship with the recruiter with the same integrity and professionalism that you would with the employer.
Recruiters are paid fees in one of two ways – retainer fees or contingency fees. This is an important distinction and will affect your process with both the employer and the recruiter. Some employers prefer working with contingency firms and some with retained firms. Both are respected by employers and useful in your job search, but, the two types of firms will not be handling the same positions with the same employers simultaneously.
A “retained recruiter” has entered an exclusive contract with an employer to fill a particular position. The retained recruiter, then, is likely to advertise a position, sharing the specifics of the position, location and employer openly. The retained firm feels a great obligation to fulfill the contract by finding the best person for the job.
A “contingency recruiter” on the other hand, usually does not have an exclusive relationship with the employer, and is only paid a fee if the job search is successful. Often, if the employer uses contingency firms, there will be more than one contingency firm competing to fill a certain position. As a job hunter, if you are sent to an interview by a contingency firm, you may find that you are competing with a larger number of applicants for a position. Generally, retained firms only send in from 3 to 5 candidates for a position.
Recruiters will be paid fees equal to about 25% to 35% of the resulting salary of the successful candidate plus expenses. This does not come out of the job candidate’s salary. This is paid to the recruiter through a separate relationship between the employer and the search firm. This may seem like a large fee, but, keep in mind that recruiters incur a great many expenses when searching for successful job candidates. They spend enormous amounts of money on computer systems, long distance calls, mail-outs, travel and interviews. Recruiters work very hard for these fees. Employers recognize the value of using recruiters and are more than willing to pay recruiters the fees. All you have to do is contact the recruiter to get the process moving.
4) Not all medical recruiters work only with physicians.
Some search firms work exclusively with physicians or in healthcare, while others may work in several fields at once. Some of the larger generalist firms will have one or more search consultants that specialize in healthcare. It is important for you, as a job hunter, to assess the recruiters’ knowledge of your field. If you use industry or medical specialty buzz words in describing your skills, experience or career aspirations, you may or may not be talking a language the recruiter understands fully. It is wise to explore fully with the recruiter his understanding of your field and area of specialization.
5) Recruiters and search consultants move around.
Recruiters, like many professionals, move to new firms during their careers. Often you will find that recruiters will work at several firms during their careers. Since it is much more effective to address your letters to a person rather than “to whom it may concern”, it is smart for job hunters to have accurate and up-to-date information about who is who and where, since this can change frequently. Search firms also move their offices, sometimes to another suite, street or state. If you have a list of recruiters that is over one year old, you will certainly waste some postage in mailing your resumes and cover letters. Many of your mail-outs will be returned to you stamped “non-deliverable”, unless you obtain an up-to-date list. A resource, like the Directory of Healthcare Recruiters is updated very frequently, usually monthly [www.pohly.com/dir3.html].
6) Most search firms work with positions all over the country.
If you are from a particular state, and want to remain in that state, don’t make the mistake of only sending your resume to recruiters in your state. Often the recruiters in your state are working on positions in other states, and recruiters in other states are working on positions in your state. This is usually the case. Very few recruiters work only in their local area, most work all around the US and some internationally. Regardless of your geographic preference, you should still send your resume to all the healthcare recruiters. If you really only want to remain in your area, you can specify that preference in your cover letter.
7) Recruiters primarily work with hard to fill positions or executive positions.
Some recruiters specialize in clinical positions for physicians, managed care executive positions, healthcare financial positions or health administration positions. Others may specialize in finding doctors, nurses or physical therapists. Generally, an employer does not engage a recruiter’s assistance in filling a position unless it is hard to fill. Sometimes employers will engage search firms to save them the valuable time of advertising or combing through dozens of resumes.
ASSESSMENT
Contingency recruiters tend to work with more mid-level management and professional positions, but, this is not always the case. Retained firms generally work with the higher level clinical or administrative positions.
One thing you will be assured of is that if a recruiter is working on a position that means that the employer is willing to pay a fee. That usually means that the position is a valued position and one worth closer inspection on your part. Even in healthcare, with certain exceptions, our economy is an “employer’s market”. This means that employers receive a deluge of resumes for their open positions. Increasingly, employers are using recruitment firms to handle their openings and schedule the interviews because employers simply do not have the manpower or time to handle the many resumes they receive.
Therefore, if a job hunter is submitted by a recruiter, that job hunter has a great advantage over all other applicants.
Value-based payment (VBP) structures have the potential to reduce health disparities and, during the pandemic, health care organizations with VBP models have had greater flexibility to effectively pivot their care delivery.
This Health Affairs Blog post outlines three strategies for payers and providers to embrace health equity in VBP design and implementation.
Posted on May 10, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Essentia Health, Ochsner Accountable Care Network, and Primaria Health win NAACOS Leaders in Quality Excellence Awards
[By David Raths]
At its Spring 2021 Conference, the National Association of Accountable Care Organizations (NAACOS) recognized three ACOs for their outstanding work to improve patient care in their communities.
NAACOS said the three inaugural winners exemplify how ACOs across the country are improving care by addressing food insecurity, making house calls to reduce preventable emergency department visits, and engaging patients in preventive services.
The Federal Trade Commission (FTC) recently announced plans to examine the consequences of physician group consolidation with healthcare facilities.
The agency said it had sent orders for 6 years’ worth of patient claims data to six insurers to inform this review: Cigna, United Healthcare, Anthem, Florida Blue, Aetna, and Health Care Service Corporation.
Posted on April 25, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Private? Public? With a Payer?
[By staff reporters]
Reporter Jessica DaMassa, the emerging ‘It girl’ of health tech interviewing, chats it up with a ‘who’s who’ of the health care business scene. Today, it is Scott Shreeve MD of Crossover Health.
Looking past the virtual-first primary care company’s $168M Series D offering, CEO Shreeve gets grilled on the long-game.