BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Most of the thousands of buy and sell orders executed on a typical day on the NYSE are in 100 share or multi-100 share lots. These are called round lots. Some of the inactive stocks traded at post 30, the non-horseshoe shaped post in the northwest corner of the exchange, are traded in 70 share round lots due to their inactivity. So, while a round lot is normally 700 shares, there are cases where it could be 10 shares. Any trade for less than a round lot is known as an odd lot. The execution of odd lot orders is somewhat different than round lots and needs explanation.
When a stock broker receives an odd lot order from one of his doctor customers, the order is processed in the same manner as any other order. However, when it gets to the floor, the commission broker knows that this is an order that will not be part of the regular auction market. He takes the order to the specialist in that stock and leaves the order with the specialist. One of the clerks assisting the specialist records the order and waits for the next auction to occur in that particular stock. As soon as a round lot trade occurs in that particular stock as a result of an auction at the post, which may occur seconds later, minutes later, or maybe not until the next day, the clerk makes a record of the trade price.
Every odd lot order that has been received since the last round lot trade, whether an order to buy or sell, is then executed at the just noted round lot price, the price at which the next round lot traded after receipt of the customer’s odd lot order, plus or minus the specialist’s “cut “. Just like everything else he does, the specialist doesn’t work for nothing. Generally, he will add 1/8 of a point to the price per share of every odd lot buy order and reduce the proceeds of each odd lot sale order by 1/8 per share. This is the compensation he earns for the effort of breaking round lots into odd lots. Remember, odd lots are never auctioned but, there can be no odd lot trade unless a round lot trades after receipt of the odd lot order.
Posted on December 30, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Ann Miller RN MHA CMP®
***
About the Institute of Medical Business Advisors, Inc
The Institute of Medical Business Advisors, Inc provides a team of experienced, senior level consultants led by iMBA Chief Executive Officer Dr. David Edward Marcinko MBA CMP™ MBBS [Hon] and Ann Miller RN MHA CMP™ to provide ongoing contact with our clients throughout all phases of each project, with most of the communications between iMBA and the key client participants flowing through this Senior Team. iMBA Inc., and its skilled staff of certified professionals have many years of significant experience, enjoy a national reputation in the healthcare consulting field, and are supported by an unsurpassed research and support staff of CPAs, MBAs, MPHs, PhDs, CMPs™, CFPs® and JDs to maintain a thorough and extensive knowledge of the healthcare environment. The iMBA team approach emphasizes providing superior service in a timely, cost-effective manner to our clients by working together to focus on identifying and presenting solutions for our clients’ unique, individual needs.
***
The iMBA Inc project team’s exclusive focus on the healthcare industry provides a unique advantage for our clients. Over the years, our industry specialization has allowed iMBA to maintain instantaneous access to a comprehensive collection of healthcare industry-focused data comprised of both historically-significant resources as well as the most recent information available. iMBA Inc’s specific, in-depth knowledge and understanding of the “value drivers” in various healthcare markets, in addition to the transaction marketplace for healthcare entities, will provide you with a level of confidence unsurpassed in the public health, health economics, management, administration, and financial planning and consulting fields. iMBA Inc’s information resources and network of healthcare industry textbook resources enhanced by our professional consultants and research staff, ensure that the iMBA project team will maintain the highest level of knowledge regarding the current and future trends of the specific specialty market related to the project, as well as the healthcare industry overall, which serves as the “foundation” for each of our client engagements.
The bargain-hunting value style is looking for shares that are under priced in relation to the company’s future potential. A value investor will invest in a company in the expectation that its shares will increase in value over time. Value investing is based essentially on quantitative criteria; asset values, cash flow, and discounted future earnings. The key properties of value shares are low Price/Earnings, Price/Sales ratios, and normally higher dividend yields.
So, on observing a company’s earnings growth, a value manager will decide whether to buy shares based on the company’s consistency or recovery prospects. The key research questions are: 1) Does the current P/E ratio warrant an investment in a slow growth company or, 2) Is the company a higher growth candidate that has dropped in price due to a temporary problem. If this is the case, will the company’s earnings growth recover, and if so, when? The key to value investing is to find bargain shares (priced low historically or for temporary and/or irrational reasons), avoiding shares that are merely cheap (priced low because the company is failing).
The buying opportunity is identified when a company undergoing some immediate problems is perceived to have good chances of recovery in the medium to long term. If there is a loss in market confidence in the company, the share price may fall, and the value investor can step in. Once the share price has achieved a suitable value, reflecting the predicted turnaround in company performance, the shareholding is sold, realizing a capital gain. A potential risk in value investing is that the company may not turn around, in which case the share price may stay static or fall.
Happy Holidays from the Institute of Medical Business Advisors, Inc
At this special time of year, we give thanks for our clients and our employees, as well as all essential workers in hospitals, health centers and medical practices across the country.
May the holiday spirit be with you and your family throughout the season and everyday We look forward to serving you in 2024.
Frequently, we hear the axiom that asset allocation is the most important investment decision, explaining 93.6% of portfolio returns. The presumption has been that once the risk tolerance and time horizon have been established, investing is simply a matter of implementing a fixed mix of stocks, bonds, and cash using mutual funds selected for this purpose. This axiom is based on a famous study by Brinson, Hood, and Beebower (BHB) published in the Financial Analysts Journal in July/August 1986. It is the stuff of most modern business school and graduate students in economics and finance.
Enter the Critics
One critic claims that BHB’s conclusions and the interpretation of their conclusions are wrong, stating that because of several methodological problems, BHB needed to make certain assumptions for their analysis to go forward. They assumed that the average asset-class weights for the 10-year period studied are the same as the actual normal policy weights; that investments in foreign stocks, real estate, private placements, and venture capital can be proxied by a mix of stocks, bonds, and cash; and that the benchmarks for stocks, bonds, and cash against which fund performance was measured are appropriate. The author believes that each of these assumptions can lead to a faulty measurement of success or failure at market timing and stock selection.
The Jahnke Study
William Jahnke claims that BHB erred in their focus on explaining the variation of quarterly portfolio returns rather than portfolio returns over the 10-year period studied. According to the study, asset allocation policy explains only a small fraction of the range of 10-year portfolio returns earned by the pension funds reported in the study. The author concluded that this discrepancy is caused by the effect of compounding returns. He adds that BHB were wrong to use variance of quarterly returns rather than the standard deviation. Use of standard deviation would reduce the often cited 93.6% to about 79%. Moreover, BHB did not consider the cost of investing, such as operating expenses, management fees, brokerage commissions, and other trading costs, which are more significant for individual investors than for the pension plans studied. Jahnke claims that excessive costs can reduce wealth accumulation by 50%.
Note: (“The Asset Allocation Hoax,” William W. Jahnke, Journal of Financial Planning, February 1997, Institute of Certified Financial Planners [303] 759-4900).
Assessment
Finally, the author takes issue with establishing long-term fixed asset class weights. Asset allocation should be a dynamic process. Higher equity return expectations should in turn produce larger equity allocations, other things being equal.
Conclusion
Are doctors different than the average investor noted in this essay?
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Did you know that most experts recommend against naming a practice with your own name because it limits future growth and you may lose the benefits that a more descriptive name would bring?
Your business name will likely be incorporated using your practice’s name, although larger (multi-specialty group) practices may use a more general name for the entire enterprise; and then having multiple “dba’s” (”Doing Business As”) for the individual practices under the umbrella. It is important to discuss these options with an attorney if you believe this arrangement has advantage; others find it confusing.
Usually, your medical specialty can be used as a base-name, and then some descriptor to differentiate it from local competing practices. Selecting a name like “The Allegiance Partners” does not indicate that medicine is your service. On the other hand, naming your practice “Podiatry Associates of Your Town” won’t be helpful to patients looking for you in the yellow pages, health insurance provider network list, or internet search engines, and finding your practice listed just before “Your Town Podiatry Partners”. It is therefore good to be cognizant of your competitors’ names when choosing your own. And, you should select a name that will hopefully grow with you into a larger enterprise.
For example, are you a solo doctor, but are pretty sure you’ll take on one or more partners in the future? Then besides not naming your practice after yourself, you may choose to add “Group” or “Partners” to your name initially even if you’re the only doctor. Is there any possibility you’ll open a second office in another town? Naming your medical practice something like the ”Apple Street Internal Medicine Group” may not make sense when your second office is opened on Main Street in a nearby city, in a few years.
Order Forms and Practice Stationary
Orders forms, invoices, purchase and estimate forms, business cards, envelopes, stationary and specialty labels can all be personalized for your medical practice name, script, colors and logo. Often, local or regional printers are the most cost effective and you support another entrepreneur, as well.
“Physicians who don’t understand modern risk management, insurance, business, and asset protection principles are sitting ducks waiting to be taken advantage of by unscrupulous insurance agents and financial advisors; and even their own prospective employers or partners. This comprehensive volume from Dr. David Marcinko and his co-authors will go a long way toward educating physicians on these critical subjects that were never taught in medical school or residency training.” —Dr. James M. Dahle, MD, FACEP, Editor of The White Coat Investor, Salt Lake City, Utah, USA
“With time at a premium, and so much vital information packed into one well organized resource, this comprehensive textbook should be on the desk of everyone serving in the healthcare ecosystem. The time you spend reading this frank and compelling book will be richly rewarded.” —Dr. J. Wesley Boyd, MD, PhD, MA, Harvard Medical School, Boston, Massachusetts, USA
Posted on November 27, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Of Healthcare Claims [What it is – How it works]
Dr. David Edward Marcinko MBA
[Editor-in-Chief]
Typically, denied and rejected healthcare claims quickly surface as a source of multi-millions in revenue leakage and unnecessary expense for doctors, clinics and hospitals, etc.
Why?
Payers have been struggling with increased costs. They thoroughly inspect claims for errors and have become adept at using their rules to deny and delay claims.
For example, Zimmerman reported the denied percentage of gross charges climbed from 4% in 2000 to 11% in 2011. In contrast, providers typically lack the tools to aggressively manage current denied claims and prevent future ones.
Financial Recognition
Without denial tracking, an organization may not recognize the heavy financial impact of denied claims.
A HARA [Hospital Accounts Receivable Analysis] report indicates that bad debt and gross days are declining. However, a majority of providers write off denials as contractual allowance, distorting the numbers but not the resulting lower margins and reduced cash.
H*Works reported that the typical 350-bed hospital loses between $4 million and $9 million each year in earned revenue from denials and underpayments (assume $103 million annual gross revenue and 40% contractual allowance). Recouping lost revenue from denials and underpayments will, according to H*Works, increase an organization’s operating margin by 2.6%.
Industry estimates report that at least 50% of denials are recoverable and 90% are preventable with the appropriate workflow processes, management commitment, strong change leadership, and the correct technology. H*Works estimates that for a revenue capture of $3 million from denials and underpayments, the recovery infrastructure costs are only about 3%.
Assessment
With all this in mind, better management of rejections and denials, as well as the information necessary to resolve and prevent them, surfaces as probably the best strategy to improving financials. By streamlining the revenue cycle, managing rejections and denials proves to be less expensive and to provide faster returns than initiating new services.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on November 24, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA
[Editor-in-Chief]
***
***
I first met my esteemed colleague Tony Fauci MD more than 30 years ago as a young surgical resident in Atlanta. My esteem for him has grown immensely since then. After all, he is an American physician-scientist and immunologist serving as the director of the National Institute of Allergy and Infectious Diseases and the Chief Medical Advisor to the President
And so, upon his retirement, Dr. Anthony Fauci urged Americans to get their reformulated Covid boosters in his final White House press briefing yesterday. Fauci, the nation’s top infectious disease official and the leader of the NIAID since 1984, announced recently that he’d be stepping down to “pursue the next chapter” of his career in December, 2022.
Dr. Fauci’s final plea comes as public health officials warn that a “viral jumbalaya” of respiratory infections threatens to push hospitals to the brink this coming winter.
Quote: “My final message—maybe the final message I give you from this podium—is that, please, for your own safety, for that of your family, get your updated Covid-19 shot as soon as you’re eligible, to protect yourself, your family, and your community.”
DEFINITION: Eisoptrophobia is the fear of mirrors or, more specifically, of seeing your own reflection in a mirror. Looking into a mirror can cause people with eisoptrophobia shame or distress.
The term is derived from the Greek “eis” and “optikos”. Even though the sufferers know their fear is irrational, they experience excessive anxiety when they look into the mirror.
Posted on November 23, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
It is NOT the Boyer Model
[By Dr. David E. Marcinko MBA]
The Boyer Model of Education and Scholarship
OK – I may subscribe to the Boyer Model but with several specific personal variations which I will keep propriety and not disclose here. But, I will discuss my teaching pragmatism, below.
Definition
Boyer’s Model of scholarship and education is an academic model advocating expansion of the traditional definition of scholarship and research into four types of scholarship. It was introduced in 1990 by Ernest Boyer.
According to Boyer, traditional research, or the scholarship of discovery, had been the center of academic life and crucial to an institution’s advancement but it needed to be broadened and made more flexible to include not only the new social and environmental challenges beyond the campus but also the reality of contemporary life.
His vision was to change the research mission of universities by introducing the idea that scholarship needed to be redefined.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
One of my favorite patients told me this anecdote as he recalled the story of the old man who spent a day watching his physician son treating HMO patients in the office.
The doctor had been working at his usual feverish pace all morning, and although he was working hard, bitterly complained to his dad that he was not making as much money as he used to.
Finally, the old man interrupted him and said,
“Son, why don’t you just treat the sick patients?”
The doctor-son looked annoyed at his father, and responded,
“Dad, can’t you see, I don’t have time to treat just the sick ones.”
Originally, a Potemkin Village was any construction whose sole purpose was to provide an external façade making people believe a failing country was prosperous.
The term comes from a fake portable village built to impress Empress Catherine II by her lover Grigory Potemkin, during her journey to Crimea, in 1787.
Posted on November 15, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
MEDIA / INTERVIEW REQUESTS
We like to talk: MarcinkoAdvisors@msn.com
BLOGGING / VLOGGING / CROSS AND RE-POSTS
Yes. We’re looking for writers & cross-posts.
Send them to us: MarcinkoAdvisors@msn.com
WHAT WE’RE LOOKING FOR
Op-eds. Cross and Re-Posts, Links and Columns. Great ideas for improving physician focused financial planning, health insurance, economics and the financial ecosystem; etc. Pitches for healthcare-focused startups and business. Write-ups of original research. Reviews of new health care products, DME and AI. Data driven analysis of health care trends. Policy proposals; etc.
DIGMAs (Drop-In Group Medical Appointments) are medical office appointments with a patient’s physician that take place in a supportive group setting. The model, developed in 1996 by Kaiser Permanente psychologist Dr. Ed Noffsinger, is a combination of an extended medical appointment with the patient’s own physician and effective group learning and support.
The group consists of the physician, a behavioral health professional, and patients from the physician’s panel. DIGMAs are best suited for routine appointments. Unfortunately, the nascent concept was met with mockery and great derision after the PP-ACA era.
Today, after the pandemic and with the rise of tel-health and tele-medicine, Shared Medical Appointments (SMAs), also known as Group Medical Visits [GMVs], are again a growing topic of discussion among providers and health economists, looking for ways to increase access to care and improve efficiency. The group visit format is also getting more attention in recent years as a strategy to add value for the patient. They typically involve up to a dozen patients or so and offer various efficiencies as well as benefits of shared discussion and experiences.
***
Behavioral Changes
Moreover, physicians and medical providers know that simply telling patients what to do often does not improve their health. The basic premise of DIGMAs, SMAs and GMVs is to build more patient engagement and inspire lasting behavior change by offering patients the opportunity to share their personal experiences not only with their provider but also with other patients dealing with similar issues.
The lowering of the book or market value of the shares of a company’s stock as a result of more shares outstanding. A company’s initial registration may include more shares than are initially issued when the company goes public for the first time.
Later, an issue of more stock by a company (called a “primary offering,” distinguished from the “initial public offering”) dilutes the existing shares outstanding.
Also, earnings-per-share calculations are said to be “fully diluted” when all common stock equivalents (convertible securities, rights, and warrants) are included. “Fully diluted” numbers are used in analysis when there is a likelihood of conversion or exercise of rights and warrants.
Posted on November 2, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
CMS Cracks Down on Medicare Advantage TV Marketing
Dr. David Edward Marcinko MBA
***
***
CMS is cracking down on deceptive marketing practices and will no longer allow Medicare Advantage or Part D prescription drug plans to advertise on television without agency approval first. The new policy is effective Jan. 1st and was discussed in an Oct. 19th memo from CMS to MA and Part D providers. The agency said it issued the new policy after reviewing thousands of beneficiary complaints regarding confusing, misleading or inaccurate information from plans — plan sponsors are also responsible for all marketing activities from brokers and third-party agencies.
“CMS has conducted so-called ‘secret shopping’ by calling numbers associated with television advertisements, mailings, newspaper advertisements and internet searches to monitor the experience beneficiaries have engaging these entities,” the agency wrote.
“Our secret shopping activities have discovered that some agents were not complying with current regulation and unduly pressuring beneficiaries, as well as failing to provide accurate or enough information to assist a beneficiary in making an informed enrollment decision.”
Source: Jakob Emerson, Becker’s Payer Issues [10/27/22]
Posted on October 22, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Turning Data into Information
By Dr. David Edward Marcinko MBA
***
As reported on this ME-P and elsewhere, I was recently in Philadelphia for a number of reasons and had the opportunity to stop by Drexel University to get some information on their nursing program. There, I learned that it is one of the nation’s top nursing schools.
In fact, Drexel University is ranked one of “America’s BEST Colleges 2011” by U.S.News & World Report. I also learned the following about breast cancer:
***
Assessment
Understanding the facts about breast cancer is of vital importance, because it may save your life or the life of someone you love.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Insider transactions shouldn’t be used primarily to make an investing decision, however an insider transaction can be an important factor in the investing decision.
In legal terms, an “insider” refers to any shareholder who owns at least 10% of a company. This can include executives in the c-suite and large hedge funds. These insiders are required to let the public know of their transactions via a Form 4 filing, which must be filed within two business days of the transaction.
Mark Zuckerberg, CEO at Facebook (NASDAQ:FB), just made a large buy and sell of company shares on November 3, according to a new SEC filing. A Form 4 filing from the U.S. Securities and Exchange Commission states that Mark Zuckerberg exercised options to purchase 62,300 Facebook shares for $0 on November 3. They then sold their shares on the same day in the open market. They sold at prices ranging from $324.04 to $332.02 to raise a total of $25,463,482 from the stock sale.
Zuckerberg still owns a total of 232,400 shares of Facebook worth, $78,226,142.
Posted on October 18, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA
***
DEFINITION: A Colonoscopy and/or sigmoidoscopy are procedures that let your doctor look inside your large intestine. They use instruments called scopes. Scopes have a tiny camera attached to a long, thin tube. The procedures let your doctor see things such as inflamed tissue, abnormal growths, and ulcers.
EDITOR’S NOTE: The ME-P does not normally discuss medical or clinical matters. But, this report is noteworthy to all.
***
***
About 15 million colonoscopies are performed in the US yearly as part of standard preventive care for adults over 45, but a new study has called into question whether all the footage from those tiny cameras is really necessary.
Over a 10-year period, people who had the screenings were 18% less likely to develop colon cancer than people who didn’t, according to the study in the New England Journal of Medicine. However, the risk of death from the cancer for both the screened and un-screened was about the same, hovering around 0.3%.
Posted on October 17, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Try (or learn about) Entrepreneurship
BY DR. DAVID EDWARD MARCINKO MBAMEdCMP®
One of the greatest things about the virtual economy is the expanded opportunity for people to branch out on their own and create something using their own expertise. Related to this is the growing societal desire to have more free time and a more balanced, efficient life overall.
In fact, years ago when I was in business school, I learned that during a recession when jobs were sparse – folks would either go back to school to re-engineer and re-educate OR start their own business.
Today – If the pandemic taught us anything, it’s that we need to be able to pivot when circumstances call for it. In the years ahead, there will be a premium on flexibility, portability, and improvisation; knowing how to earn income outside the traditional employer-employee relationship will continue to be an especially valuable skill.
ASSESSMENT: So, if you are a physician, nurse, medical professional or financial advisor in the healthcare space, think about what you’re naturally good at (or at least interested in), and determine if there’s an opportunity to monetize it in some way on your own. Your career might thank you for it!
Posted on October 16, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Dear Pharmaceutical Company, Financial Services Firm or Corporate Medical Vendor
We often serve as Medical Science Liaison [MSL] for pharmaceutical companies, at medical seminars and/or financial services organization meetings. Based on our education, experience and skills, we are confident that we would be a great addition to your team.
My Record
For example, I have a proven record in collaborative leadership with functional healthcare executive management experience to develop and implement coordinated strategies designed to deliver top line growth; drive organizational change and enhance competitive positioning within multiple key markets; enhance relationships and influence physicians; analyze financial, economics, operational and quality measures and ensure health practices are operating within goals and standards.
In this role, I can identify external experts (KOLs), and engage, enhance, and build relationships by listening and understanding the views of these experts.
An Independent Conduit Link
More importantly, I can bring value to external experts through excellent communication of scientific dialogue. I see this position as a non-promotional conduit link between you and this community. It is one where I fuse scientific knowledge with business acumen to accelerate commercialization success. As a fully independent MSL, I can:
Serve as MC, key or end-note speaker
Integrate quickly within any existing internal MSL structure or culture
Train, develop and team build career path management processes
Offer modern and flexible health 2.0 solutions.
CV and Related Information
And, a formal CV with evidence of national notoriety and gravitas is available with related information online:
Travel is non-problematic from Atlanta. Teaching, speaking, writing and mentoring are areas of expertise. Thank you in advance for your time. Please do not hesitate to contact me if you have any questions.
Cordially,
Dave
Dr. David Edward Marcinko; FACFAS, MBA, CMP™
Forner, Certified Financial Planner™
Former, Certified Physician in Healthcare Quality
Former, American Society of Health Economists (ASHE) member
Former, American Health Information Management Association (AHIMA) member
Former, Healthcare Information and Management Systems Society (HIMSS) member
According to Wikipedia, selling away in the U.S. securities brokerage industry is the inappropriate practice of an investment professional who sells, or solicits the sale of, securities not held or offered by the brokerage firm with which he is associated.
An example of the term expressed in a sentence is, “The broker was selling investments away from the firm.” Brokers marketing securities must have obtained the appropriate securities licenses for various types of investments. Brokers in the U.S. may be “associated” with one or more Brokerage firms and must obtain licenses by passing standardized Financial Industry Regulatory Authority exams such as the Series 6 or Series 7 exam.
***
In the past I’ve held these as well as a Series 63 and 65 license [SEC].
Posted on October 11, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Book Marcinko for your Next Financial Planning Seminar, Meeting or Medical Business Event
By Ann Miller RN MHA
Professor and physician executive David Edward Marcinko MBBS DPM MBA MEd BSc CMP® is originally from Loyola University MD, Temple University in Philadelphia and the Milton S. Hershey Medical Center in PA; Oglethorpe University, and Atlanta Hospital & Medical Center in GA; and the Aachen City University Hospital, Koln-Germany. He is one of the most innovative global thought leaders in health care business and entrepreneurship today.
Dr. Marcinko is a multi-degreed educator, board certified physician, surgical fellow, hospital medical staff President, Chief Education Officer and philanthropist with more than 400 published papers; 5,150 op-ed pieces and over 125+ international presentations to his credit; including the top 10 biggest pharmaceutical companies and financial services firms in the nation. He is also a best-selling Amazon author with 30 published text books in four languages [National Institute of Health, Library of Congress and Library of Medicine].
Dr. Marcinko is past Editor-in-Chief of the prestigious “Journal of Health Care Finance”, and a former Certified Financial Planner®, who was named “Health Economist of the Year” in 2001. He is a Federal and State court approved expert witness featured in hundreds of peer reviewed medical, business, management and trade publications [AMA, ADA, APMA, AAOS, Physicians Practice, Investment Advisor, Physician’s Money Digest and MD News].
As a licensed insurance agent, RIA and SEC registered endowment fund manager, Dr. Marcinko is Founding Dean of the fiduciary focused CERTIFIED MEDICAL PLANNER® chartered designation education program; as well as Chief Editor of the HEALTH DICTIONARY SERIES® Wiki Project. His professional memberships include: ASHE, AHIMA, ACHE, ACME, ACPE, MGMA, FMMA and HIMSS.
Dr. Marcinko is a MSFT Beta tester, Google Scholar, “H” Index favorite and one of LinkedIn’s “Top Cited Voices”.
A Dividend Aristocrat is a stock that has exhibited a remarkable level of consistency, measured by the fact that only those S&P 500 companies that have increased their annual dividend for 25 straight years — or more — can be called one. The name was coined by cable TV personality and investor Jim Cramer
These companies have raised their dividends through good times and bad, including recessions, crashes, and pandemics. Being able to continue doing so is a tribute to their stability and strength. Now, the past 18 months have been a particularly difficult economic environment to operate in, and some companies were forced to slash or hold the line on their dividends as a result.
But others are just fine, like investment manager T. Rowe Price (NASDAQ: TROW), which increased its dividend for the 35th straight year in 2022. It is located in Baltimore Maryland not far from where I grew up. In fact, I used to play stick ball, as a kid, in the parking lot.
Navigating a course where sound organizational management is intertwined with financial acumen requires a strategy designed by subject-matter experts. Fortunately, Financial Management Strategies for Hospital and Healthcare Organizations: Tools, Techniques, Checklists and Case Studies provides that blueprint. ―David B. Nash, MD, MBA, Jefferson Medical College, Thomas Jefferson University
It is fitting that Dr. David Edward Marcinko, MBA, CMP™ and his fellow experts have laid out a plan of action in Financial Management Strategies for Hospital and Healthcare Organizations that physicians, nurse-executives, administrators, institutional CEOs, CFOs, MBAs, lawyers, and healthcare accountants can follow to help move healthcare financial fitness forward in these uncharted waters. ―Neil H. Baum, MD, Tulane Medical School
Posted on September 28, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Everyone wants to be a doctor – or get paid like one!
[By Dr. David Edward Marcinko MBA CMP™]
Most regular ME-P readers and subscribers know that I am a Jaguar automobile fan. Except perhaps for a Bentley or Rolls Royce, I think that Jags are the finest mass produced luxury vehicles on the planet.
Backstory
My regular car guy, Jimmie the mechanic, was removing a cylinder head from a late model Jaguar sedan when he spotted a world-famous heart surgeon in his garage; we have many such dignitaries on this side of town.
In fact, it is called “pill-hill” around here, for the many hospitals, medical clinics and physician offices. The heart surgeon was waiting for the service manager to come and take a look at his car.
The Query
Jimmie shouted across the garage, ‘Hey Doc can I ask you a question?’
The famous surgeon, a bit surprised, walked over to him. Jimmie straightened up, wiped his hands on a rag and asked, ‘So Doc, look at this engine. I also can open hearts, take valves out, fix’em, put in new parts and when I finish this Jaguar will work just like a new one.’
Salary Comparisons
“So how come I work for a pittance and you get the really big money, when you and I are doing basically the same work?”
The MD’s Answer
The surgeon paused, smiled and leaned over and whispered into Jimmie’s ear: ‘Try doing it with the engine running.’
***
***
Assessment
Of course this story is a classic; oft repeated ad nauseam.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Universal Precautions refer to the medical practice of avoiding contact with patients’ bodily fluids, by means of the wearing of nonporous articles such as medical gloves, goggles, and face shields.
The infection control techniques were essentially good hygiene habits, such as hand washing and the use of gloves and other barriers, the correct handling of hypodermic needles, scalpels, and aseptic techniques.
Following the AIDS outbreak in the 1980s the US CDC formally introduced them in 1985–88. Every patient was treated as if infected and therefore precautions were taken to minimize risk.
There are more than 950,000 physicians in the United States. Yet, the brutal supply and demand, and demographic calculus of the matter is that there are just too many aging patients chasing too few doctors. Compensation and reimbursement is plummeting as Uncle Sam becomes the payer-of-choice for more than 52% of us. More so, going forward with the PP-ACA OR, perhaps not so much after the Trump election.
Furthermore, many large health care corporations, hospitals, and clinical and medical practices have not been market responsive to this change. Some physicians with top-down business models did not recognize the changing health care ecosystem or participatory medicine climate. Change is not inherent in the DNA of traditionalists. These entities and practitioners represented a rigid or “used-to-be” mentality, not a flexible or “want-to-be” mindset.
Yet today’s physicians and emerging Health 2.0 initiatives must possess a market nimbleness that cannot be recreated in a command-controlled or collectivist environment. Going forward, it is not difficult to imagine the following rules for the new virtual medical culture, and young physicians of the modern era.
A. Rule 1
Forget about large office suites, surgery centers, fancy equipment, larger hospitals, and the bricks and mortar that comprised traditional medical practices. One doctor with a great idea, good bedside manners, or competitive advantage can outfox a slew of insurance companies, Certified Public Accountants, or the Associate Management Accountant, while still serving patients and making money. It is now a unit-of-one economy where “ME Inc.,” is the standard. Physicians must maneuver for advantages that boost their standing and credibility among patients, peers, and payers.
Examples include patient satisfaction surveys, outcomes research analysis, evidence-based-medicine, direct reimbursement compensation, physician economic credentialing, and true patient-centric medicine. Physicians should realize the power of networking, vertical integration, and the establishment of virtual offices that come together to treat a patient and then disband when a successful outcome is achieved. Job security is earned with more successful outcomes; not a magnificent office suite or onsite presence.
B. Rule 2
Challenge conventional wisdom, think outside the traditional box, recapture your dreams and ambitions, disregard conventional gurus, and work harder than you have ever worked before. Remember the old saying, “if everyone is thinking alike, then nobody is thinking.” Do traditionalists or collective health care reform advocates react rationally or irrationally?
For example, some health care competition and career thought-leaders, such as Shirley Svorny, PhD, a professor of economics and chair of the Department of Economics at California State University, Northridge, wonder if a medical degree is a barrier—rather than enabler—of affordable health care. An expert on the regulation of health care professionals, including medical professional licensing, she has participated in health policy summits organized by Cato and the Texas Public Policy Foundation. She argues that licensure not only fails to protect consumers from incompetent physicians, but, by raising barriers to entry, makes health care more expensive and less accessible.
Institutional oversight and a sophisticated network of private accrediting and certification organizations, all motivated by the need to protect reputations and avoid legal liability, offer whatever consumer protections exist today.
C. Rule 3
Differentiate yourself among your health care peers. Do or learn something new and unknown by your competitors. Market your accomplishments and let the world know. Be a non-conformist. Conformity is an operational standard and a straitjacket on creativity. Doctors must create and innovate, not blindly follow entrenched medical societies into oblivion.
For example, the establishment of virtual medical schools and hospitals, where students, nurses, and doctors learn and practice their art on cyber entities that look and feel like real patients, can be generated electronically through the wonders of virtual reality units.
D. Rule 4
Realize that the present situation is not necessarily the future. Attempt to see the future and discern your place in it. Master the art of quick change with fast, but informed decision making. Do what you love, disregard what you do not, and let the fates have their way with you.
Assessment
I receive a couple of phone calls each month from young doctors on this topic. I ask them to decide if they are of the philosophical ilk to adhere to the above rules; or become another conformist and go along … to get along? In other words, get fly!
Or, become an employed, or government doctor. Just remember … the entity that gives you a job, can also take it away.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on August 5, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Including Public Relations, Risk, Change and Crisis Management
By Dr. David Edward Marcinko MBA
Marketing is the business process of identifying, anticipating and satisfying customers’ needs and wants. It is your unique value proposition or strategic competitive advantage. Marketers can direct product to other businesses or directly to consumers.
Advertising is a marketing communication that employs an openly sponsored, non-personal message to promote or sell a product, service or idea. Sponsors of advertising are typically businesses wishing to promote their products or services. Advertising is communicated through various mass media, including traditional media such as newspapers, magazines, television, radio, outdoor advertising or direct mail; and new media such as search results, blogs, social media, websites or text messages. The actual presentation of the message in a medium is referred to as an advertisement, or “ad” or advert for short.
Advertising is differentiated from public relations in that an advertiser pays for and has control over the message. It differs from personal selling in that the message is non-personal, i.e., not directed to a particular individual. We pay for advertising but pray for public relations.
Sales are activities related to selling or the number of goods or services sold in a given targeted time period. The seller, or the provider of the goods or services, completes a sale in response to an acquisition, appropriation, requisition, or a direct interaction with the buyer at the point of sale. There is a passing of title (property or ownership) of the item, and the settlement of a price, in which agreement is reached on a price for which transfer of ownership of the item will occur. The seller, not the purchaser, typically executes the sale and it may be completed prior to the obligation of payment. In the case of indirect interaction, a person who sells goods or service on behalf of the owner is known as a salesman or saleswoman or salesperson, but this often refers to someone selling goods in a store/shop, in which case other terms are also common, including salesclerk, shop assistant, and retail clerk.
Change management is the discipline that guides how we prepare, equip and support individuals to successfully adopt change in order to drive organizational success and outcomes.
Crisis management is the identification of threats to an organization and its stakeholders, and the methods used by the organization to deal with these threats.
***
***
Risk management is the identification, evaluation, and prioritization of risks (defined in ISO 31000 as the effect of uncertainty on objectives) followed by coordinated and economical application of resources to minimize, monitor, and control the probability or impact of unfortunate events or to maximize the realization of opportunities.
Assessment: Your thoughts are appreciated from a healthcare perspective.
QUESTION: We are in near bear market correction territory – especially for tech stocks – so what are the 2 major types of valuation approaches for common stock?
ANSWER: There are basically two different approaches for common stock valuation; top-down and bottom-up. Under either of the two fundamental approaches, a physician investor will have to work with individual company data. In reality, each of these approaches is used by investors and security analysts when doing fundamental analysis.
With the bottom-up approach, investors focus directly on a company’s prospects. Analysis of such information as the company’s products, its competitive position, and its financial status leads to an estimate of the company’s earnings potential, and, ultimately, its value in the market. Considerable time and effort are required to produce the type of detailed financial analysis needed to understand a firm’s standing. The emphasis in this approach is on finding companies with good long-term growth prospects, and making accurate earnings estimates.
The top-down approach is the opposite of the bottom-up approach. Investors begin with the economy and the overall market, considering such important factors as interest rates and inflation. They next consider likely industry prospects, or sectors of the economy that are likely to do particularly well (or particularly poorly). Finally, having decided that factors are favorable for investing, and having determined which parts of the overall economy are likely to perform well, individual companies are analyzed.
The concept of a self-taught and student motivated, but automated outcomes driven classroom may seem like a nightmare scenario for those who are not comfortable with computers. Now everyone can breathe a sigh of relief, because the Institute of Medical Business Advisors just launched an “automated” final examination review protocol that requires no programming skill whatsoever.
In fact, everything is designed to be very simple and easy to use. Once a student’s examination “blue-book” is received, computerized “robotic reviewers” correct student assignments and quarterly test answers. This automated examination model lets the robots correct tests and exams, while the students concentrate on guided self-learning.
According to Eugene Schmuckler PhD MBA MEd, Academic Provost of the CERTIFIED MEDICAL PLANNER® professional designation and certification program,
“This option allows the modern adult-learner save both time and money as s/he progresses toward the ultimate goal of board certification as a CMP® mark holder.”
The trend is growing and iMBA, Inc., is leading the way.
Posted on June 19, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
REALLY?
By Dr. David Edward Marcinko MBA
***
The business cycle is also known as the economic cycle and reflects the expansion or contraction in economic activity. Understanding the business cycle and the indicators used to determine its phases may influence investment or economic business decisions and financial or medical planning expectations.
Although often depicted as the regular rising and falling of an episodic curve, the business cycle is very irregular in terms of amplitude and duration. Moreover, many elements move together during the cycle and individual elements seldom carry enough momentum to cause the cycle to move.
However, elements may have a domino effect on one another, and this is ultimately drives the cycle, too. We can also have a large positive cycle, coincident with a smaller but still negative cycle, as may be seen in the current healthcare climate of today.
First Phase: Trough to Recovery (service and production driven)
Scenario: A depressed GNP leads to declining industrial production and capacity utilization. Decreased workloads result in improved labor productivity and reduced labor (unit) costs until actual producer (wholesale) prices decline.
Second Phase: Recovery to Expansion (patient and consumer driven)
Scenario: CPI declines (due to reduced wholesale prices) and consumer real income rises, improving consumer sentiment and actual demand for consumer goods.
Third Phase: Expansion to Peak (service and production driven)
Scenario: GNP raises leading to increased industrial production and capacity utilization. But, labor productivity declines and unit labor costs and producer (wholesale) prices rise.
Fourth Phase: Peak to Contraction (patient and consumer driven)
Scenario: CPI rises making consumer real income and sentiment erode until consumer demand, and ultimately purchases, shrink dramatically. Recessions may occur and economists have an alphabet used to describe them.
For example, with a “V” graph shape, the drop and recovery is quick. For a “U” shaped graph, the economy moves up more sluggishly from the bottom. A “W” is what you would expect: repeated recoveries and declines. An “L” shaped recession describes a prolonged dry economic spell or even depression.
Posted on June 16, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
About the SoPE
***
***
By Dr. David Edward Marcinko MBA
The Society of Physician Entrepreneurs (SoPE) was established as a community of interest in 2008 by several members of the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS), including Dr. Arlen Meyers, the President & CEO. SoPE became a separate and independent legal entity; incorporating in Washington, D.C. in January 2011.
It is a 501 (c) 6 member organization with the stated purpose of providing support; idea stage through funding, for physician entrepreneurs with ideas on how to improve healthcare. Currently there are over 1,000 members included in their LinkedIn site.
Vision
SoPE’s vision is to accelerate physician originated biomedical innovation.
Mission
The mission of SoPE is to foster scholarship in biomedical entrepreneurship and provide education, training and support; idea stage through funding, to primarily community-based physician entrepreneurs in the interest of better healthcare.
Membership
SoPE membership is open to all physicians and also accepts individuals as associate members; representatives of medical device, legal, venture capital, and other firms with an interest in serving and/or supporting physician entrepreneurs.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on May 19, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
As part of its Mental Health initiative, MTV’s second-annual Mental Health Action Day – an open-source movement of brands, organizations, government agencies, and cultural leaders to drive culture of mental health from awareness to action – will bring together more than 1,600 organizations in cities across the country to encourage and empower people to take action for mental health on Thursday, May 19, 2022.
Posted on May 10, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Altered and Poorly Written Rx for Vicodin
By Dr. David Edward Marcinko MBA
***
***
Poorly-written Rx for vicodin
Drug: Rx Vicodin
Disp: # 10
Sig: Take I, as needed for pain.
Refills: 1 2 3 4 or 5
AM2685591
David Edward Marcinko, MBBS DPMMBA
The patient abuser may change drug quantity numbers, copy or remember the doctors’ DEA number, or take extra Rx pads. For this reason, a physician’s Rx pad should contain his/her name, address and telephone number. The doctor’s DEA number should not be pre-printed on the pad, for fear of mis-use.
Example:
Increase the quantity 10, to 100, by adding a zero, so that the additional capsules can be used, sold or bartered with on the street.
Change the directions to take 2 capsules, rather than 1 in order to produce greater euphoria.
Increase the Rx refills, from one to two, by extending the underline, or checking an additional quantity box.
Pre-printed DEA number can be stolen, sold or reused.
Pre-printed (not original) physician signature can be reproduced and widely distributed for more prescriptions.
Altered Rx for vicodin
Drug: Rx Vicodin
Disp: # 100
Sig: Take II, as needed for pain.
Refills: 1 2 3 4 or 5
AM2675591
David Edward Marcinko, MDBBS DPM MBA
The doctor drug addict, or a doc in need of funds, may write for more narcotic agent than needed, and receive the additional pills back from the patient-shill for personal consumption, sell them on the street himself for money, or receive a monetary kickback from the patient-shill.
A pharmacist may also indirectly alter a prescription using the above methods, or simply short-change the patient with fewer narcotic capsules than the prescription intends. This is more difficult to do with pills or tablets in the out patient setting, but easy to do in the in-patient setting when liquid IV drugs are used, by dilution and placing less than the full amount in IV bottles or bags. The harm to patients, of course, may be fatal.
Well-written Rx for vicodin
Drug: Rx Vicodin
Disp: # 10 (ten) capsules
Sig: Take one or two capsules, po, prn pain.
Refills: 1 2 3 4 or 5
AM2685591
David Edward Marcinko, MBBS DPM MBA
Example:
Drug quantity can-not be changed.
Directions can-not be changed. Route of administration (by mouth) indicated.
Rx refills clearly indicated.
Handwritten, not pre-printed, DEA number.
Original physician signature, only.
Doctor Rx prescription abuse foibles are legendary in the DEA and include a Maryland podiatrist who wrote prescriptions for more than 1,235 Mepergan Fortis capsules ostensibly for his wife following minor foot surgery. Or, the Florida physician who prescribed more than 2,150 Vicodin capsules for a patient with whom he was having an extra-marital affair in order that his consort not disclose the fling to his wife. Or, the osteopath from New Jersey who wrote more than 100 narcotic prescriptions every 8 hour day, for more than a year, to any patient standing in a line in front of his office. And, finally the California dentist whose excuse for writing more than 1,845 narcotic tablet prescriptions in a six month period for the same patient was that they would be needed in his next reincarnation. Yes, all of these incidents are laughable if not for their serious consequences to the involved individuals, and society, alike. The bastards!
Fortunately, unlike drug local domestic drug kingpins or international narco-traffickers who ply their trade virtually undetected, these naive white-collared nerds, always get caught by the Drug Enforcement Agency. Their Rx abuse tactics are so amateurish!
Posted on May 9, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Dr. David Edwarrd Marcinko MBA
Rx DRUG ABUSE
Traditional medicinal agents come in a variety of ways, known as dispensing vehicles. Drugs may be in liquid, pill or inject able form, they may be compounded in capsules, caplets, gelatin tablets, powders or suppositories, or they may come in creams or ointments for the eye, anus and vagina. They may be ingested into the stomach, placed and dissolved under the tongue, put into the eyes, popped, injected or smeared and transported through the human skin from patches.
A valid drug prescription is a written order, by a doctor, to a pharmacist. In this country, prescriptions are written by physicians, podiatrists, osteopaths, dentists. and some optometrists, physician assistants and nurse practitioners. In addition to the name of the patient and that of the medical prescriber, the prescription contains the name of the drug (not necessarily a narcotic), its quantity, instructions to the pharmacist, and directions to the patient. Narcotic prescriptions may not be prescribed to a drug addict to prevent withdrawal symptoms, as there must be some other therapeutic purpose for such an order.
The art of medicinal prescription writing, and pharmaceutical compounding, has declined in modern medicine for several reasons. Most drugs are made by pharmaceutical companies, and the role of the pharmacist, in most cases, consists only of compounding and error prevention. Many drugs are even automatically dispensed, and tracked, in the hospital setting with bar coding technology and modern inventory tracking mechanisms. Also, the practice of writing long and complicated prescriptions, containing many active ingredients, adjuvants, correctives, and elegant vehicles, has been abandoned in favor of using pure compounds.
Drugs may be prescribed by their official names, which were first given by the United States Pharmacopeia (USP), in 1920, or by the National Formulary (NF), since 1906. Unofficial or generic names may be used, known as New and Non-Official Drugs (NND) or by the United States Adopted Names (USAN), or by the manufactures trade name. For example, the generic narcotic meperidine or pithidine, is also known by the trade named, demerol. The designation USAN does not imply endorsement by the American Medical Association (AMA) Council on Drugs (CODs), or by the USP.
Of course, there is an advantage and disadvantages to prescribing drugs by their trade name, or generic names. Advantages of generics include economies of scale for both the patient and pharmacist, and although the active ingredient in generics are identical to trade drugs, they are often less expensive since research and development costs are absent, and various binders, colorizing agents, preservatives or dispersing agents are of an inferior quality, and hence cheaper for the patient. Appearance, size and taste issues are common. For the pharmacist, generics are cheaper since a multiplicity of very similar drugs need not be shelved.
***
***
For example, the tablet or capsular form of many drugs contains inactive ingredients, such as: ammonio methacrylate copolymer, hydroxypropyl methylcellulose, lactose, magnesium stearate, povidone, redironoxide, stearyl alcohol, talc, titanium dioxide, triacetin, yellowironoxide, yellowironoxide with FD&C blue No.2 (80 mgstrengthtablet only), FD&C blue No.2 and other ingredients. And yes, I’ve seen an addict do into shock, or die from acute anaphylaxis, after taking drugs containing ingredient he was highly allergic to.
Shock is a life-threatening condition where blood pressure falls too low to sustain life. It occurs when low blood volume (due to severe bleeding, excessive fluid loss or inadequate fluid uptake), inadequate pumping action of the heart or excessive dilation of the blood vessel walls (vasodilation) causes low blood pressure. This in turn results in inadequate blood supply to body cells, which can quickly die or be irreversibly damaged.
Anaphylactic shock is the severest form of allergy that is a medical emergency. It is a Type I reaction according to the Gell and Coombs medical classification, and is often severe and sometimes fatal systemic reaction in a susceptible individual upon exposure to a specific antigen (such as wasp venom or penicillin) following previous sensitization, or drug use. Characterized especially by respiratory symptoms, fainting, itching, itching and swelling of the throat or other mucous membranes and a sudden decline in blood pressure! The victim literally cannot breathe and drowns in its own congested and fluid filled lungs
So, patients in need of routine drugs for acute or chronic conditions like arthritis, high blood pressure, asthma, acne, hay fever, performance enhancing steroids or, so called life style drugs, like Viagra for a limp woody, or hair growth stimulator Rogaine, may get a good deal by going to Canada or Mexico for generics. But for important drugs, like nitroglycerine fro your heart, blood thinner coumadin, birth control pills or various anti-cancer agents, stick with brand names.
The main disadvantage of trade drugs is increased cost, due to R & D, patents, trademarks, marketing and company advertising expenses. Of course, trade drug are first to market, and hence may be beneficial as a new treatment modality, or injurious if significant side affects or other complications arise.
Today, the prime source for drug information is probably the well known, Physicians Desk Reference (PDR). Now, in its 58th edition, the PDR® provides the latest information on prescription, but not illegal street drugs. It is considered the standard reference that can be found in virtually every physician’s office, hospital and pharmacy in the United States. The current edition is over 3,000 pages long, and is where you can find data on more than 4,000 drugs, by brand and generic name, manufacturer and product categories. The PDR also provides usage information and warnings, drug interactions, plus full-size, full-color photos cross-referenced to specific drugs. For the layman, it also includes: phonetic spelling for each listing, a key to controlled substances, adverse reactions and contraindications, pregnancy ratings, dosages and all other FDA-required information. Of course, on the street, or in Mexico, none of this information matters.
Latin abbreviations, sometimes still used by doctors on prescription blanks include:
Rx = take thou (receipe)
po = by mouth (para orbis)
prn = as needed (pro re’nata)
hs = at bed time (hora somnae)
BID = twice daily
TID = three times daily
QID = four times daily
M = Mix
Traditionally, a medical prescription is written in a certain order, well known to drug abusers, and DEA agents, and consist of six basic parts:
Superscription: This is the Rx, or recipe. In Latin it means take thou.
Inscription: Represents the ingredients and amounts.
Subscription: Represent the description for drug dispensing, and may be represented by the letter M, for mix.
Signature: Often abbreviated as Sig, and contains the directions for patient use.
Refill Status: Indicates the number of refills allowed.
DEA Number: This is nine-character alpha-numeric sequence, used by all licensed physicians who prescribe narcotic agents. An example is AM2685591. The second letter is the first letter of the doctor’s last name, (ie, Marcinko) and the first two digits add up to the third (ie, 2+6=8).
Finally, in addition to the basic parts of a prescription, it should have the patient’s name, and physician signature written in ink, followed by degree designation, such as MD, DPM, DO or DDS, etc.
***
***
Perhaps the most egregious narcotic prescribing habits recently encountered by DEA agents have been by doctors of all degrees and medical designations. Reasons are generally two-fold. First, the doctor may become a drug addict himself, either by accident or through initial legitimate therapeutic use, and over-prescribe the narcotics. Or, increasing office costs, and decreased reimbursement fee reductions of many managed medical care have so economically destabilized the medical community, that economically impoverished doctors desperately sell prescriptions to finance their personal lifestyles, automobiles, clothes, fancy vacations or own addictions.
For example, a staggering medical student loan debt burden of $100,000-$250,000 is not unusual for new practitioners. In fact, the federal Health Education Assistance Loan (HEAL) program reported that for the Year 2001, it squeezed significant repayment settlements from its Top 5 list of deadbeat doctor debtors. This included a $303,000 settlement from a New York dentist, $186,000 from a Florida osteopath, $158,000 from a New Jersey podiatrist, $128,000 from a Virginia podiatrist, and $120 from a Virginia dentist. The agency also excluded 303 practitioners from Medicare, Medicaid and other federal healthcare programs and had their cases referred for non-payment of debt.
These facts indicate that the current healthcare reimbursement climate has caused more pain and tumult to doctors than the pubic realizes. Older medical practitioners are retiring prematurely, mature providers are frustrated and in despair, and young physicians have no concept of the economic servitude to which they are about to be subjected. Frustration is high and physician suicides have been documented. Many doctors get divorced at the start of their careers. Even the U.S. Inspector General has declared healthcare providers to be public enemy #2,behind international narco-traffickers, for their federal drug, fraud and abuse initiatives. Still, the statistic above lends itself to narcotic drug prescription abuse, either on the part of the doctor or patient, since only these two parties that can directly alter a prescription for illicit drug use, as illustrated by this poorly written prescription for a narcotic pain killer, vicodin.
Posted on May 6, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
May 2nd to May 6th
DEALS AND FREEBIES
By Dr. David Edward Marcinko MBA
***
In 1984, the National Parents Teachers Association designated the first week of May as Teacher Appreciation Week as a special time to honor the individuals who educated our children. It has become a tradition for restaurants and businesses to offer special deals during that week.
Posted on April 23, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
“Now and Then”
By Dr. David Edward Marcinko MBA
[Editor-in-Chief]
I was recently at a car show and could not help but snap a photo of the beautiful black 1955 vehicle; below.
Ambulance Defined [Wikipedia]
An ambulance is a vehicle for transportation of sick or injured people to, from or between places of treatment for an illness or injury, and in some instances will also provide out of hospital medical care to the patient. The word is often associated with road going emergency ambulances which form part of an emergency medical service, administering emergency care to those with acute medical problems.
The term ambulance does, however, extend to a wider range of vehicles other than those with flashing warning lights and sirens. The term also includes a large number of non-urgent ambulances which are for transport of patients without an urgent acute condition (see functional types, below) and a wide range of urgent and non-urgent vehicles including trucks, vans, bicycles, motorbikes, station wagons, buses, helicopters, fixed-wing aircraft, boats, and even hospital ships (see vehicle types, also below).
The term ambulance comes from the Latin word ambulare, meaning to walk or move about which is a reference to early medical care where patients were moved by lifting or wheeling. The word originally meant a moving hospital, which follows an army in its movements. During the American Civil War vehicles for conveying the wounded off the field of battle were called ambulance wagons. Field hospitals were still called ambulances during the Franco-Prussian War of 1870 and in the Serbo-Turkish war of 1876 even though the wagons were first referred to as ambulances about 1854 during the Crimean War.
There are other types of ambulance, with the most common being the patient transport ambulance (sometimes called an ambulette). These vehicles are not usually (although there are exceptions) equipped with life-support equipment, and are usually crewed by staff with fewer qualifications than the crew of emergency ambulances. Their purpose is simply to transport patients to, from or between places of treatment. In most countries, these are not equipped with flashing lights or sirens. In some jurisdictions there is a modified form of the ambulance used, that only carries one member of ambulance crew to the scene to provide care, but is not used to transport the patient. Such vehicles are called fly-cars. In these cases a patient who requires transportation to hospital will require a patient-carrying ambulance to attend in addition to the fast responder.
###
[The Editor in Marquette, MI]
Hearse Defined [Wikipedia]
Originally, a hearse was an elaborate framework that was erected over a coffin or tomb to which memorial verses or epitaphs were attached. It was then put on the top of horse-drawn carriages, looking much like a luggage rack. Today, the original hearse remains acknowledged by the bit of scroll work or stretched-out “S” on the side of a funeral coach, called Landau bars.
Hearses were originally horse-drawn, but silent electric motorized carts were introduced as horses began to be phased out as transportation. Examples that were used in Paris were reported in the pages of Scientific American May 1907 and petrol-driven hearses began to be produced from 1909 in the United States. Motorized hearses became more widely accepted in the 1920s.
The vast majority of hearses since then have been based on larger, more powerful car chassis, generally retaining the front end up to and possibly including the front doors but with custom bodywork to the rear to contain the coffin. Some early hearses also served as ambulances, owing to the large cargo capacity in the rear of the vehicle. A few cities experimented with funeral trolley cars and/or subway cars to carry both the casket and mourners to cemeteries, but these were not popular.
The only exception was Chicago, IL which operated 3 different funeral trolley cars over the elevated tracks in downtown Chicago to outlying cemeteries in the western suburbs. A special funeral bureau handled the funeral trains which sometimes operated 3-4 funeral trains a week over the ‘L’.
Back in 1955, this Cadillac performed double-duty for a small town in North East Georgia. Both as ambulance for the still living, as well as hearse for the newly deceased. Notice the dual red [“cherry”] light and siren on the roof A very utilitarian approach to both functions, don’t you think?
History [Wikipedia]
A combination car was a vehicle built upon a (usually Cadillac) “professional car” chassis which could be employed either as a hearse or as an ambulance, and had the capability of being swapped between those roles without much difficulty. These vehicles were upgraded by coachbuilders such as Superior, Miller-Meteor, and Cotner-Bevington, and were typical of the era when funeral homes offered emergency ambulance service in addition to their primary trade.
Even if a “combo” has no flashing lights (mounted or concealed), siren, or two-way radio installed, an experienced vehicle collector can recognize it as such by it having systems to carry either a gurney or a casket, one or more foldable seats on one side in the rear compartment where a first-aid person can sit while looking after a patient on their way to the hospital, and a cabinet where first-aid supplies can be stored.
Also, the presence of ambulance technology made combos useful in the first call role, as a gurney is also used in that function.
Some combos were equipped with rotating roof beacons that could flash either yellow lights in processional mode, or both red and yellow lights in emergency response mode. Alternately, a hole on the roof was often supplied where a beacon could be bolted on an intermittent basis, a wire passing through to the driver’s compartment where it could be plugged in when needed.
Combos employed more often or exclusively as ambulances were often fitted with ambulance markings and additional lighting. However, usage of passenger car or station wagon derived vehicles as ambulances became impractical in the US after c. 1980 due to upgraded equipment and interior measurement requirements imposed by US government regulators. Many such vehicles were donated or otherwise found their way to developing nations.
The Cadillac combination unit was made famous in Ghostbusters as the Ecto-1, a modified 1959 Miller-Meteor coach.
Note: The Hess & Eisenhardt company also produced luxury Jaguar automobiles; my favorites.
###
[My vintage 2000 Jaguar XJ-V8L Touring Sedan]
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
DEFINITION: A centenarian is a person who has reached the age of 100 years. Because life expectancy worldwide are below 100 years, the term is invariably associated with longevity. In 2012, the United Nations estimated that there were 316,600 living centenarians worldwide.
Sto Lat (One Hundred Years) is a traditional Polish song that is sung to express good wishes, good health and long life to a person. It is also a common way of wishing someone a happy birthday in Polish. Sto lat is used in the Spring, many birthdays and on international days of language.
***
***
What Percentage of the Population Lives to 100?
According to the Social Security Administration, the overall chances of living to 100 aren’t actually that great. And, according to the World Economic Forum, there are over 500,000 centenarians among the 7.9 billion people worldwide. That means that only a 0.006% of the population is 100 or more.
Here are a few additional facts from the most recently available information from the Society of Actuaries and the Social Security Administration:
One out of three males and one out of two females who are in their mid-50s today will live to be 90.
For a couple who is 65 today, there is a 50% chance that one person will be alive at 92.
If you have lived to be 65, you will likely live another 20 years, on average.
If you live to be 75, the average life expectancy is 88.
If you live to be 85, the average life expectancy is 92.
And, if you live to be 95, the average life expectancy is 98.
Hospitals, a local family practice office, a pharmaceutical company, all likely have one thing in common. Somewhere within these companies or partnerships, there are key employees or profit makers. Due to their expertise, management skills, knowledge, or “history of why,” they have become indispensable to their employers.
If this key employee were to die prematurely, what would potentially happen to the company? In many cases, especially in smaller companies, it would have a devastating effect on the bottom line, or even precipitate a bankruptcy. In these circumstances, a form of business insurance, called key person coverage, is recommended in order to alleviate the potential financial problems resulting from the death of that employee.
The business would purchase and own a life insurance policy on the key person. Upon the death of the employee, the life insurance proceeds could be used to:
Pay off bank loans.
Replace the lost profits of the company.
Establish a reserve for the search, hiring and training of a replacement.
[B] Business Continuation Funding
See the chapters on buy-sell agreements and asset protection planning.
[C] Executive Bonus Plan
An executive bonus plan (or § 162 plan) is an effective way for a company to provide valued, select employees an additional employment benefit. One of the main advantages to an executive bonus plan, when compared to other benefits, is its simplicity. In a typical executive bonus plan, an agreement is made between the employer and employee, whereby the employer agrees to pay for the cost of a life insurance policy, in the form of a bonus, on the life of the employee.
The major benefits of such a plan to the employee are that he or she is the immediate owner of the cash values and the death benefit provided. The only cost to the employee is the payment of income tax on any bonus received. The employer receives a tax deduction for providing the benefit, improves the morale of its selected employees, and can use the plan as a tool to attract additional talent.
[D] Non-Qualified Salary Continuation
Commonly referred to as deferred compensation, this is a legally binding promise by an employer to pay a salary continuation benefit at a specific point in the future, in exchange for the current and continued performance of its employee. These plans are normally used to supplement existing retirement plans.
Although there are different variations of deferred compensation, in a typical deferred compensation agreement, the employer will purchase and own a life insurance policy on the life of the employee. The cash value of the policy grows tax deferred during the employee’s working years. After retirement, these cash values can be withdrawn from the policy to reimburse the company for its after-tax retirement payments to the employee.
Upon the death of the employee, any remaining death benefit would likely be received income tax free by the employer (Alternative Minimum Taxes could apply to any benefit received by certain larger C corporations). The death benefit could then be used to pay any required survivor benefits to the employee’s spouse, or provide partial or total cost recovery to the employer.
In a typical plan, the terms of the agreement are negotiated as to the amount of benefit received by the employee, when retirement benefits can begin, how long retirement benefits will be paid, and if benefits will be provided for death or disability. The business has established what is commonly referred to as “golden handcuffs” for the employee. As a result, the benefit will only be received if the employee continues to work for the company until retirement. If the employee is terminated or quits prior to retirement, the plan would end and no benefits would be payed.
[E] Split Dollar Plans
Split dollar arrangements can be a complicated and confusing concept for even the most experienced insurance professional or financial advisor. This concept is, in its simplest terms, a way for a business to share the cost and benefit of a life insurance policy with a valued employee. In a normal split dollar arrangement, the employee will receive valuable life insurance coverage at little cost to them. The business pays the majority of the premium, but is usually able to recover the entire cost of providing this benefit at termination of employment, death or surrender of the policy.
Following the publication of IRS Notices 2002-8 and 2002-59, there are currently two general approaches to the ownership of business split-dollar life insurance: Employer-owned or Employee-owned.
***
[1] Employer-Owned Method
In the employer-owned method the employer is the sole owner of the policy. A written split-dollar agreement usually permits the employee to name the beneficiary for most of the death proceeds. The employer owns all the cash value and has the unfettered right to borrow or withdraw it as necessary. At the end of the formal agreement, the business can generally (1) continue the policy as key person insurance, (2) transfer ownership to the insured and report the cash values as additional income to the insured, (3) sell the policy to the insured, or (4) use a combination of these methods. This is commonly referred to as “rollout.”
Practitioners should be careful not to include rollout language in the split-dollar agreement. The reason the rollout should not be included is that if the parties formally agree that after a specified number of years—or following a specific event—related only to the circumstances surrounding the policy, that the policy will be turned over to the insured, the IRS could declare that the entire transaction was a sham and that its sole purpose was to avoid taxation of the premiums to the employee, generating substantial interest and penalties in addition to the additional taxes due.
The death proceeds available to the insured employee’s beneficiary is considered a current and reportable economic benefit (REB), and it is an annually taxable event to the employee. If an individual policy is involved, the REB is calculated by multiplying the face amount times the government’s Table 2004 rates or the insurance company’s alternative term rates, using the insured’s age. If a second-to-die policy is involved, the government’s PS38 rates or the company’s alternative PS38 rates will be used. Any part of the premium actually paid by the employee is used to offset any REB dollar-for-dollar.
[2] Employee-Owned Method
With the employee-owned method, the insured-employee is generally the applicant and owner of the policy. Any premiums paid by the business are deemed to be loans to the employee and the employee reports as income an imputed interest rate on the cumulative amount of loan based on Code § 7872. A collateral assignment is made for the benefit of the business to cover the cumulative loan amount. In some cases, the assignment may allow the assignee to have access to the cash values of the policy by way of a policy loan. This method is unavailable for officers and executives of publicly- held corporations because of the current restrictions on corporate loans (the Sarbanes-Oxley Act of 2002).
The employee-owned method is somewhat similar to the older collateral assignment form of split-dollar. The benefits for the employee are both the ability to control large amounts of death proceeds as well as developing equity in the policy. Whether or not this new method catches on will depend greatly on the imputed interest rate published by the IRS every July. If set low enough, this may be an excellent opportunity for the employee to use inexpensive business dollars to pay for life insurance.
Posted on April 8, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. David Edward Marcinko MBA
***
***
National Public Health Week is observed during the first week of April every year. That’s seven days to champion the health of all Americans. It’s a week to recognize that everyone should lead healthier lives, irrespective of where they live, work, or come from. Since its founding in 1955, the initiative has become an important movement to highlight issues that can improve the health and happiness of a nation. You could choose to crush a workout or any workout challenge today. It’s a great week to start eating healthy and stick to it. Whatever you do, remember to involve your friends, family, and the larger community. It’s also a week when we campaign for health policies that are fair, inclusive, and accessible to all communities in the United States.
The first National Public Health Week took place in April 1955 and was organized by the American Public Health Association (A.P.H.A.). Since then, the initiative has received tremendous support from civil societies and administrations across the United States. The day recognizes the long history and achievements in public health. It also serves to highlight critical issues to help people lead healthier and happier lives.
In attempting to reach these goals, National Public Health Week seeks to address the root causes of poor health, disease, and lifestyles. It starts with recognizing that healthcare is still a privilege many cannot afford. Where people are born, their neighborhoods, places of work, different lives, and backgrounds determine the quality of healthcare access.
For example, a child who goes to school hungry will not be an engaged student. People working for minimum wages sacrifice health for the sake of an income. It’s thousands of families who have no access to nutritious food in their communities. Or those without the means to travel to access quality healthcare, often located far away.
National Public Health Week is committed to making health inclusive and equitable. It hopes to foster decision-making that considers the health of all communities — irrespective of income, race, or gender. Each year, the first full week in April celebrates the power of the community in realizing this vision. The A.P.H.A. usually announces different themes for each day of the week. From fitness challenges and discussions to sharing healthy recipes — it’s seven days of committing to health as a country.
So, no matter where you are, APHA invites you to join us as we celebrate National Public Health Week! This year’s theme, Public Health Is Where You Are, celebrates what we know is true: The places where we are, physically, mentally and societally, affect our health and our lives.
Celebrate and promote health in your community by hosting your own NPHW event!
***
… Here are a few ideas:
Host virtual health panels and discussions. …
Team up to reach new audiences and build community. …











































































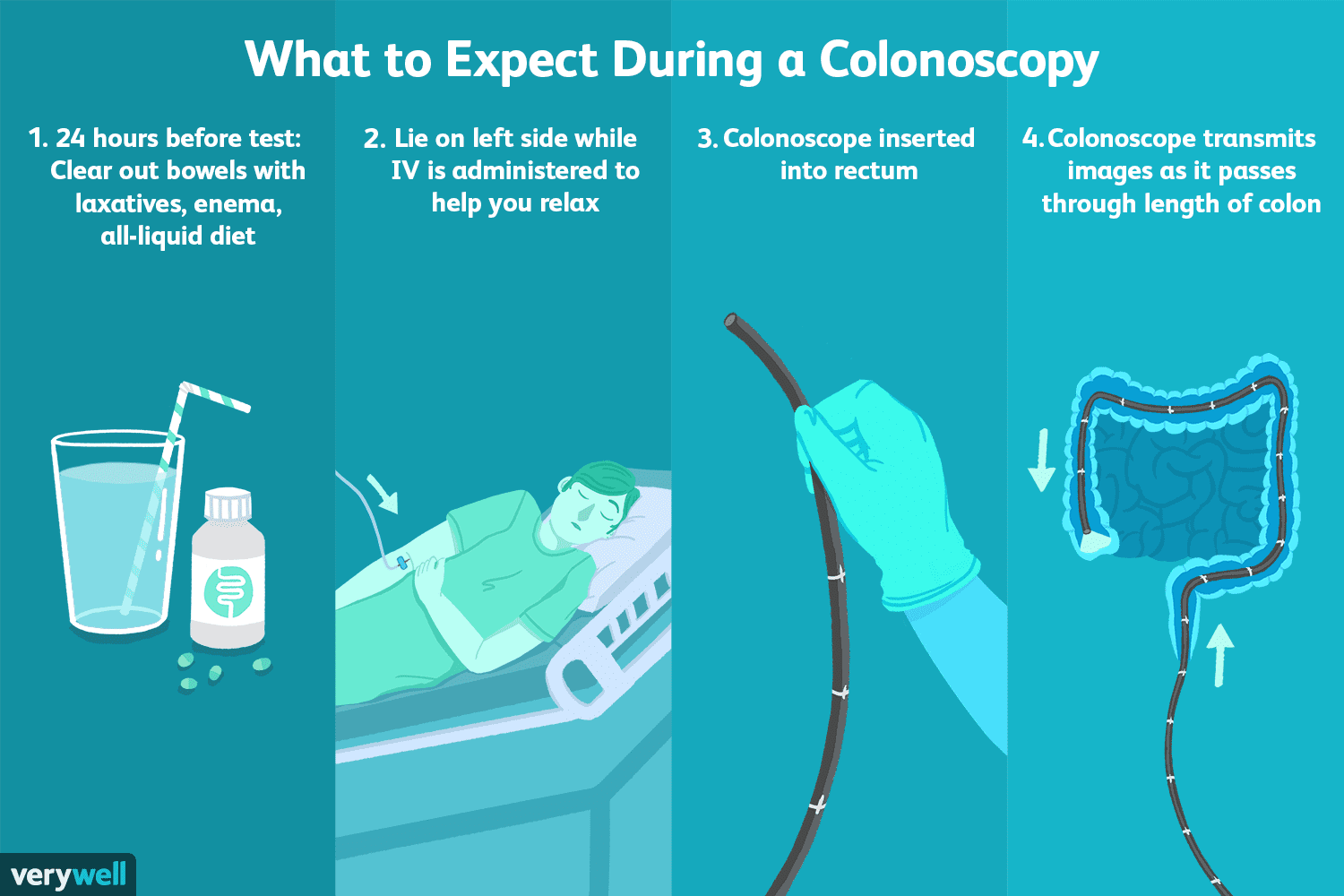

















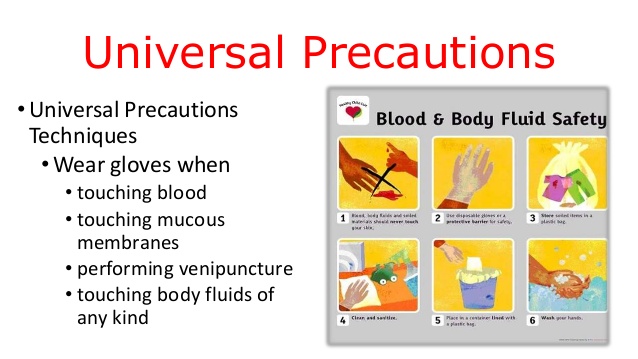
























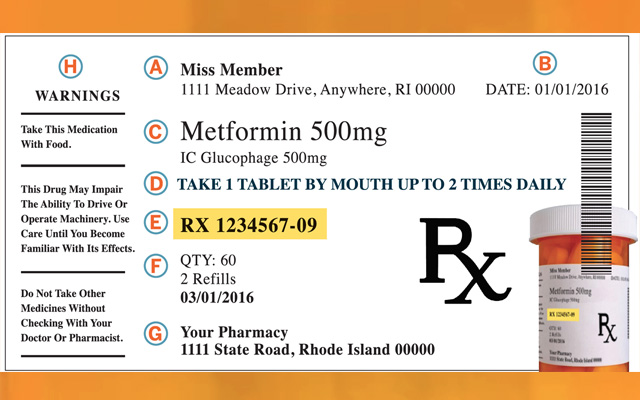














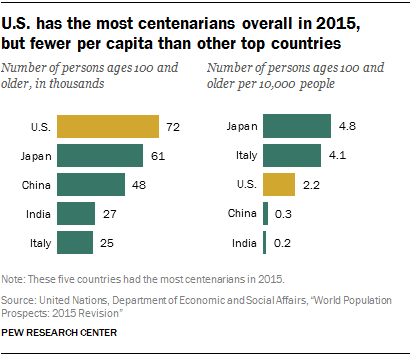






{kind=link}