Dr. David Edward Marcinko; MBA MEd
SPONSOR: http://www.CertifiedMedicalPlanner.org
***

***
Redefining Access, Value and the Patient Experience
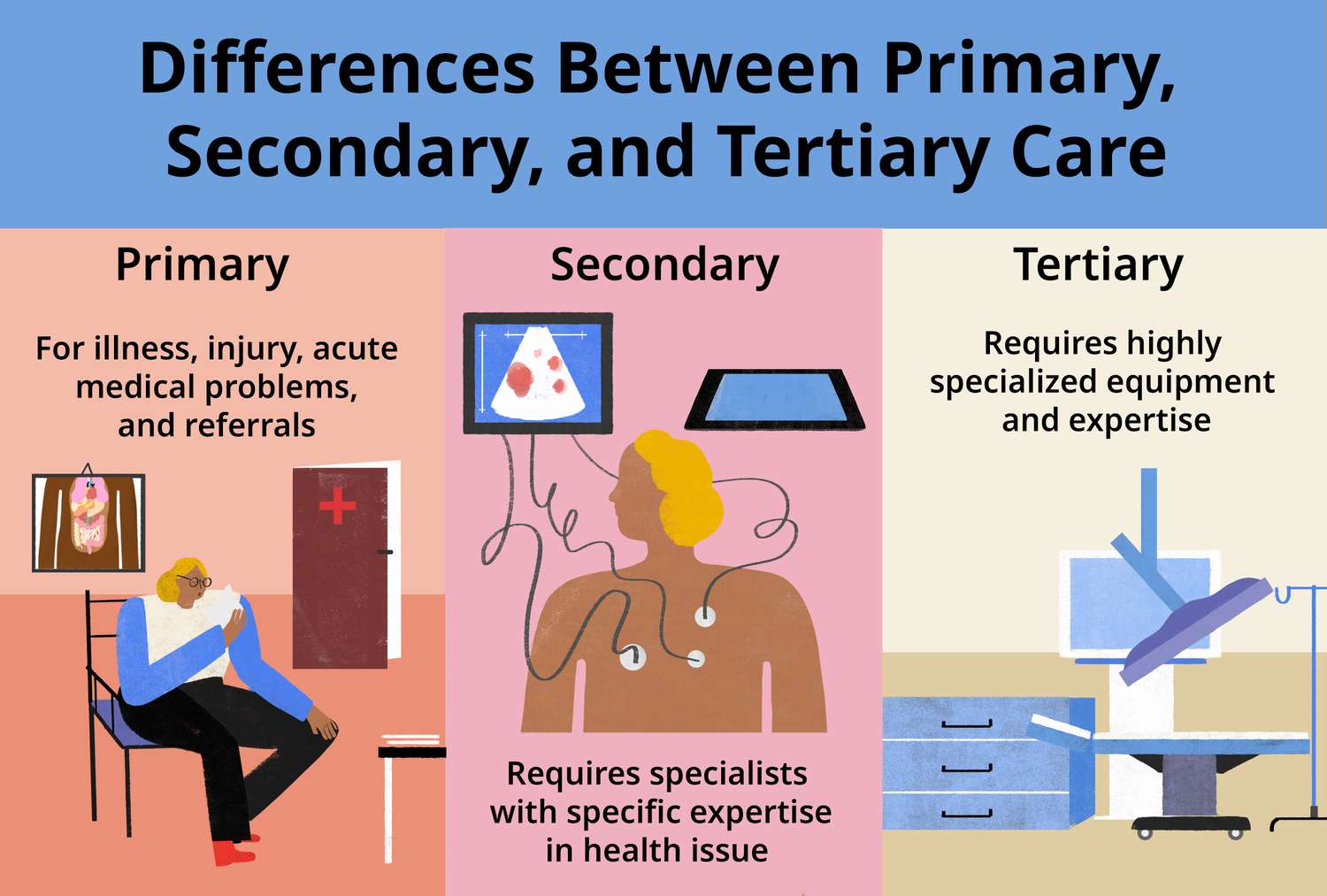
Concierge medicine has gained steady traction across many medical specialties, but its relevance to podiatry is especially compelling. Podiatrists sit at the intersection of primary care, chronic disease management, biomechanics, and minor surgical intervention. They often treat conditions that profoundly affect mobility, independence, and quality of life. Yet podiatry practices face the same pressures that challenge the broader healthcare system: shrinking reimbursements, rising administrative burdens, and patient panels that grow faster than the time available to serve them. Concierge medicine offers podiatrists a model that can restore time, autonomy, and depth to the patient relationship while elevating the standard of care.
At its core, concierge medicine replaces the high‑volume, insurance‑driven model with a membership‑based structure that allows clinicians to limit their patient load and provide more personalized, accessible care. For podiatrists, this shift can be transformative. Foot and ankle issues often require ongoing monitoring, detailed biomechanical assessments, and frequent follow‑ups. In a traditional practice, these needs can be difficult to meet when appointment slots are compressed into ten‑ or fifteen‑minute increments. Concierge podiatry, by contrast, allows for extended visits, same‑day access, and direct communication between patient and provider. This creates space for deeper evaluation, more thoughtful treatment planning, and a more collaborative approach to long‑term foot health.
One of the strongest arguments for concierge podiatry is the nature of the conditions podiatrists treat. Many patients struggle with chronic issues such as diabetic neuropathy, peripheral vascular disease, recurrent wounds, or structural deformities that require ongoing attention. These conditions do not resolve with a single visit; they evolve, fluctuate, and often require proactive management. In a concierge model, podiatrists can monitor these patients more closely, intervene earlier, and spend the time necessary to educate them about prevention and self‑care. This can reduce complications, improve outcomes, and foster a sense of partnership that is difficult to achieve in a high‑volume setting.
Concierge podiatry also aligns well with the growing emphasis on preventive care. Many foot and ankle problems—such as tendon injuries, stress fractures, or progressive deformities—develop gradually and can be mitigated with early intervention. A concierge structure allows podiatrists to conduct more comprehensive biomechanical evaluations, gait analyses, and footwear consultations. It also gives them the freedom to integrate services that are often squeezed out of traditional practice models, such as personalized orthotic management, fall‑risk assessments, or long‑term monitoring for athletes. Patients benefit from a more holistic approach that prioritizes prevention rather than simply reacting to acute problems.
***
***
Another advantage of concierge podiatry is accessibility. Foot pain can be debilitating, and delays in care often worsen the underlying condition. Concierge patients typically enjoy same‑day or next‑day appointments, direct messaging with their podiatrist, and the ability to address concerns quickly before they escalate. For individuals with diabetes, mobility limitations, or demanding schedules, this level of access can be invaluable. It also reduces reliance on urgent care centers or emergency departments, where foot issues may not receive specialized attention.
From the podiatrist’s perspective, concierge medicine offers a path to greater professional satisfaction. Many podiatrists enter the field because they enjoy building long‑term relationships and helping patients maintain mobility and independence. Yet the realities of insurance‑based practice—documentation requirements, declining reimbursements, and the pressure to see more patients in less time—can erode that sense of purpose. A concierge model restores control over scheduling, reduces administrative strain, and allows podiatrists to practice in a way that reflects their values. This can help prevent burnout and create a more sustainable career.
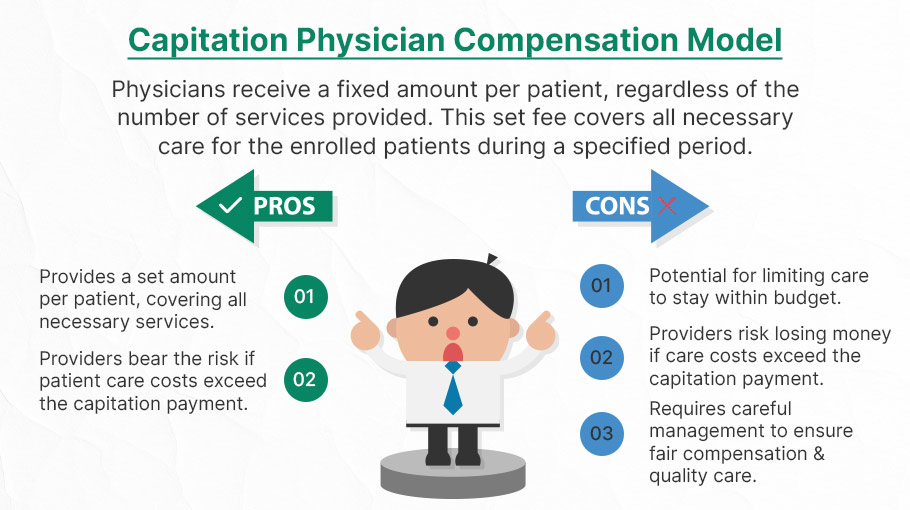
Of course, concierge podiatry is not without challenges. The most common criticism of concierge medicine in general is that it may limit access for patients who cannot afford membership fees. When a podiatrist transitions to a concierge model and reduces their patient panel, some individuals may need to seek care elsewhere. In communities with limited access to foot and ankle specialists, this can create gaps in care. Podiatrists considering this model must weigh the benefits of improved care for a smaller group of patients against the potential impact on the broader community.
Another challenge is determining which services are included in the membership fee and which remain billable through insurance. Podiatry encompasses a wide range of procedures—from routine nail care to surgical interventions—and patients may misunderstand what their membership covers. Clear communication is essential to avoid confusion and maintain trust. Some concierge podiatrists choose a hybrid model, where the membership fee covers enhanced access and preventive services, while procedures and surgeries are billed separately. Others opt for a fully cash‑based practice. Each approach has advantages, but all require transparency.
***

***
Despite these complexities, the potential for concierge medicine to elevate podiatric care is significant. As patients increasingly seek personalized, relationship‑driven healthcare, podiatrists are well positioned to offer a concierge experience that feels both meaningful and practical. Foot and ankle health is foundational to overall well‑being, and many patients are willing to invest in a model that prioritizes mobility, comfort, and long‑term function.
Looking ahead, concierge podiatry may continue to evolve in creative ways. Some practices may integrate wellness services such as physical therapy, nutrition counseling, or sports performance programs. Others may develop specialized concierge offerings for athletes, older adults, or individuals with diabetes. Technology may also play a role, enabling remote monitoring of gait, pressure distribution, or wound healing. The flexibility of the concierge model allows podiatrists to tailor their services to the unique needs of their patient population.
Ultimately, concierge medicine offers podiatrists an opportunity to reimagine how they deliver care. It provides a framework that values time, expertise, and human connection—elements that are often lost in traditional practice. While it may not be the right fit for every clinician or every community, it represents a powerful alternative for podiatrists who want to deepen their relationships with patients, enhance the quality of their care, and build a practice that reflects the true spirit of their profession.
COMMENTS APPRECIATED
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR- http://www.MarcinkoAssociates.com
Like, Refer and Subscribe
***
***
Share this:

Filed under: "Doctors Only", Ask a Doctor, Career Development, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Marcinko Associates, Touring with Marcinko | Tagged: bills, cash medicine, cash practice, concierge medicine, concierge podiatry, david marcinko, DPM, FEES, membership fees | Leave a comment »