BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on April 11, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
On Differences and Similarities
By David K. Luke; MIM CMP
The difference between internal marketing and external marketing for physicians is that internal marketing is the management strategy of improving satisfaction by making patients aware of the positive differences in the physician’s practice –versus- other modern or traditional alternatives that the doctor might externally use [yellow pages, coupons, TV, radio, internet, blogs, etc].
Now, compare marketing with advertising, which attempts to draw patients to the medical practice or clinic using more expensive channel distribution means and/or media messaging.
The “X” Factor
Internal marketing gives the patient “something extra” during the visit that tends to make them pleased, satisfied – or better yet – delighted!
In show business, Simon Cowell calls this something extra the “X” factor.
Whether it is a “Patient Bill of Rights” or just making sure that patients are treated fairly, and with respect throughout the process, turns the patient into a practice advocate instead of a patient from hell.
Improved listening/communication can come in the form of an attentive and caring human ear, enhanced bedside manner, or technology like P[C]RM (Patient {Client} Relationship Management) tools and/or eMRs, for example.
Sloppy Medical Office Procedures
Having office staff involved, by noticing improvements, can also help with the implementation of a successful internal marketing strategy. Sloppy office procedures can be cleaned up, scheduling access management can be revamped, and any administrative mix-ups can be avoided.
Negative practices such as “we enforce a minimum $50 office visit fee” should be stopped, as this casts a negative attitude on all patients, not just future deadbeats.
An effective P[C] RM strategy can increase patient satisfaction and be inexpensive to implement and maintain, especially in light of modern advertising tools for medical practices.
Financial Advisor Comparisons
A physician’s internal marketing program is comparative to an FA’s internal marketing program, in that both methods are much more cost effective and yield better results than traditional external marketing or advertising.
For an FA, the practice of encouraging referrals can be done discreetly without making the existing clients uncomfortable.
An FA practice that is “referable” is one in which there are consistent standards and procedures in place. This creates a comfort factor with existing clients and assures them that when they refer their friends and family they will also receive consistent quality treatment.
Assessment
An FA can implement procedures similar to a medical practice by training staff to point out and recognize office procedures that might be improved. Letting clients know they are appreciated and that referrals are accepted sounds like obvious advice, but is often ignored by too many Financial Advisors, and even doctors.
Editor’s Note: David K. Luke is currently enrolled in the online www.CertifiedMedicalPlanner.org chartered professional designation program.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on April 10, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Is Business Finally Embracing Medical Values?
[By Render S. Davis MHA CHE]
[By David Edward Marcinko MBA MEd]
In the evolutionary shifts in models for medical care, physicians have been asked to embrace business values of efficiency and cost effectiveness, sometimes at the expense of their professional judgment and personal values.
While some of these changes have been inevitable as our society sought to rein in out-of-control costs, it is not unreasonable for physicians to call on payers, regulators and other business parties to the health care delivery system to raise their ethical bar.
Tit-for-Tat
Harvard University physician-ethicist Linda Emmanuel noted that “health professionals are now accountable to business values (such as efficiency and cost effectiveness), so business persons should be accountable to professional values including kindness and compassion.”
***
[Medicine versus Business]
***
Assessment
Within the framework of ethical principles, John La Puma, M.D., wrote in Managed Care Ethics, that “business’s ethical obligations are integrity and honesty.
Medicine’s are those plus altruism, beneficence, non-maleficence, respect, and fairness.”
About the Author
Render Davis was a Certified Healthcare Executive, now retired from Crawford Long Hospital at Emory University, in Atlanta, GA He served as Assistant Administrator for General Services, Policy Development, and Regulatory Affairs from 1977-95. He is a founding board member of the Health Care Ethics Consortium of Georgia and served on the consortium’s Executive Committee, Advisory Board, Futility Task Force, Strategic Planning Committee, and chaired the Annual Conference Planning Committee, for many years.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on April 10, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Medical Ethics – Ever on Guard
***
ByAaron Carroll MD, MS
***
I’m a doctor. My father is a doctor. My colleagues are doctors, the people I train are doctors, lots and lots of my friends are doctors.
***
But, that doesn’t meant that doctors sometimes aren’t blind to certain issues like their own financial conflicts of interest. Sometimes we have to poke doctors with a stick. That’s how we show our love.
***
Conflicts of interest are the topic of this Healthcare Triage video.
Dr. Carroll has published some of the seminal work on various types of health care reform, and continues to be a sought after speaker on cost, quality and access-and the Affordable Care Act and its implications for our future. Considered one of the leading pediatric informaticists in the U.S. he has received millions of dollars in grants to explore the use of information technology in health care. Dr. Carroll was the Primary Investigator on a grant from the Agency for Healthcare Research and Quality to study the true impact of malpractice claims on the practice of medicine.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on April 10, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Physicians Received $12 Billion from Drug & Device Makers in Less Than 10 Years
A review of the federal Open Payments database found that the pharmaceutical and medical device industry paid physicians $12.1 billion over nearly a decade. Almost two thirds of eligible physicians — 826,313 doctors — received a payment from a drug or device maker from 2013 to 2022, according to a study published online in JAMA on March 28th. Overall, the median payment was $48 per physician.
Orthopedists received the largest amount of payments in aggregate, $1.3 billion, followed by neurologists and psychiatrists at $1.2 billion, and cardiologists at $1.29 billion. To find out what any physician was paid, click here.
On August 14, 2023, the Centers for Medicare and Medicaid Services (CMS) announced updates to their Accountable Care Organization Realizing Equity, Access, and Community Health (ACO REACH) model.
In response to feedback from stakeholders, starting in performance year (PY) 2024, the agency expects to increase the predictability for the model and further advance health equity. Only in its first PY, ACO REACH is a revision and replacement of the Global and Professional Direct Contracting (GPDC) model and the Geographic Direct Contracting (Geo Model) model, a subset of the GPDC model. This Health Capital Topics article will discuss the updates to the ACO REACH model and its implications for existing accountable care organizations (ACOs). (Read more…)
In a recent survey by Edelman Financial Engines, 57% of respondents said they’d feel wealthy if they had $1 million in the bank. But for many people, like doctors, that may not be enough.
Among those with $500,000 and $3 million in assets, 53% said it would take over $3 million in the bank for them to feel wealthy, and 33% said it would take over $5 million. Given that these are amounts some people will never even come close to amassing in their lifetimes, it may be hard to wrap your head around these answers.
Posted on April 7, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
Since 2013 – Americans believe they now need $1.46 million to retire in style
***
***
The new magic number for retirement, found in a study by Northwestern Mutual, is 15% higher than what people thought they needed last year—and 53% higher than the amount people in 2020 pictured themselves needing to feel comfortable leaving the workforce to sit on a beach in Florida.
In fact, it’s also more than most people have socked away: On average, US adults have $88,400 saved for retirement.
Written by doctors and healthcare professionals, this textbook should be mandatory reading for all medical school students—highly recommended for both young and veteran physicians—and an eliminating factor for any financial advisor who has not read it. The book uses jargon like ‘innovative,’ ‘transformational,’ and ‘disruptive’—all rightly so! It is the type of definitive financial lifestyle planning book we often seek, but seldom find. —LeRoy Howard MA CMPTM,Candidate and Financial Advisor, Fayetteville, North Carolina I taught diagnostic radiology for over a decade. The physician-focused niche information, balanced perspectives, and insider industry transparency in this book may help save your financial life. —Dr. William P. Scherer MS, Barry University, Ft. Lauderdale, Florida This book was crafted in response to the frustration felt by doctors who dealt with top financial, brokerage, and accounting firms. These non-fiduciary behemoths often prescribed costly wholesale solutions that were applicable to all, but customized for few, despite ever-changing needs. It is a must-read to learn why brokerage sales pitches or Internet resources will never replace the knowledge and deep advice of a physician-focused financial advisor, medical consultant, or collegial Certified Medical Planner™ financial professional. —Parin Khotari MBA,Whitman School of Management, Syracuse University, New York In today’s healthcare environment, in order for providers to survive, they need to understand their current and future market trends, finances, operations, and impact of federal and state regulations. As a healthcare consulting professional for over 30 years supporting both the private and public sector, I recommend that providers understand and utilize the wealth of knowledge that is being conveyed in these chapters. Without this guidance providers will have a hard time navigating the supporting system which may impact their future revenue stream. I strongly endorse the contents of this book.—Carol S. Miller BSN MBA PMP,President, Miller Consulting Group, ACT IAC Executive Committee Vice-Chair at-Large, HIMSS NCA Board Member This is an excellent book on financial planning for physicians and health professionals. It is all inclusive yet very easy to read with much valuable information. And, I have been expanding my business knowledge with all of Dr. Marcinko’s prior books. I highly recommend this one, too. It is a fine educational tool for all doctors.—Dr. David B. Lumsden MD MS MA,Orthopedic Surgeon, Baltimore, Maryland There is no other comprehensive book like it to help doctors, nurses, and other medical providers accumulate and preserve the wealth that their years of education and hard work have earned them. —Dr. Jason Dyken MD MBA,Dyken Wealth Strategies, Gulf Shores, Alabama I plan to give a copy of this book written ‘by doctors and for doctors’ to all my prospects, physician, and nurse clients. It may be the definitive text on this important topic. —Alexander Naruska CPA,Orlando, Florida
Health professionals are small business owners who need to apply their self-discipline tactics in establishing and operating successful practices. Talented trainees are leaving the medical profession because they fail to balance the cost of attendance against a realistic business and financial plan. Principles like budgeting, saving, and living below one’s means, in order to make future investments for future growth, asset protection, and retirement possible are often lacking. This textbook guides the medical professional in his/her financial planning life journey from start to finish. It ranks a place in all medical school libraries and on each of our bookshelves. —Dr. Thomas M. DeLauro DPM,Professor and Chairman – Division of Medical Sciences, New York College of Podiatric Medicine
Physicians are notoriously excellent at diagnosing and treating medical conditions. However, they are also notoriously deficient in managing the business aspects of their medical practices. Most will earn $20-30 million in their medical lifetime, but few know how to create wealth for themselves and their families. This book will help fill the void in physicians’ financial education. I have two recommendations: 1) every physician, young and old, should read this book; and 2) read it a second time! —Dr. Neil Baum MD,Clinical Associate Professor of Urology, Tulane Medical School, New Orleans, Louisiana
I worked with a Certified Medical Planner™ on several occasions in the past, and will do so again in the future. This book codified the vast body of knowledge that helped in all facets of my financial life and professional medical practice. —Dr. James E. Williams DABPS, Foot and Ankle Surgeon, Conyers, Georgia
This is a constantly changing field for rules, regulations, taxes, insurance, compliance, and investments. This book assists readers, and their financial advisors, in keeping up with what’s going on in the healthcare field that all doctors need to know. —Patricia Raskob CFP® EA ATA, Raskob Kambourian Financial Advisors, Tucson, Arizona I particularly enjoyed reading the specific examples in this book which pointed out the perils of risk … something with which I am too familiar and have learned (the hard way) to avoid like the Black Death. It is a pleasure to come across this kind of wisdom, in print, that other colleagues may learn before it’s too late— many, many years down the road. —Dr. Robert S. Park MD, Robert Park and Associates Insurance, Seattle, Washington
Although this book targets physicians, I was pleased to see that it also addressed the financial planning and employment benefit needs of nurses; physical, respiratory, and occupational therapists; CRNAs, hospitalists, and other members of the health care team….highly readable, practical, and understandable. —Nurse Cecelia T. Perez RN, Hospital Operating Room Manager, Ellicott City, Maryland
Personal financial success in the PP-ACA era will be more difficult to achieve than ever before. It requires the next generation of doctors to rethink frugality, delay gratification, and redefine the very definition of success and work–life balance. And, they will surely need the subject matter medical specificity and new-wave professional guidance offered in this book. This book is a ‘must-read’ for all health care professionals, and their financial advisors, who wish to take an active role in creating a new subset of informed and pioneering professionals known as Certified Medical Planners™. —Dr. Mark D. Dollard FACFAS, Private Practice, Tyson Corner, Virginia As healthcare professionals, it is our Hippocratic duty to avoid preventable harm by paying attention. On the other hand, some of us are guilty of being reckless with our own financial health—delaying serious consideration of investments, taxation, retirement income, estate planning, and inheritances until the worry keeps one awake at night. So, if you have avoided planning for the future for far too long, perhaps it is time to take that first step toward preparedness. This in-depth textbook is an excellent starting point—not only because of its readability, but because of his team’s expertise and thoroughness in addressing the intricacies of modern investments—and from the point of view of not only gifted financial experts, but as healthcare providers, as well … a rare combination. —Dr. Darrell K. Pruitt DDS, Private Practice Dentist, Fort Worth, Texas This text should be on the bookshelf of all contemporary physicians. The book is physician-focused with unique topics applicable to all medical professionals. But, it also offers helpful insights into the new tax and estate laws, fiduciary accountability for advisors and insurance agents, with investing, asset protection and risk management, and retirement planning strategies with updates for the brave new world of global payments of the Patient Protection and Affordable Care Act. Starting out by encouraging readers to examine their personal ‘money blueprint’ beliefs and habits, the book is divided into four sections offering holistic life cycle financial information and economic education directed to new, mid-career, and mature physicians.
This structure permits one to dip into the book based on personal need to find relief, rather than to overwhelm. Given the complexity of modern domestic healthcare, and the daunting challenges faced by physicians who try to stay abreast of clinical medicine and the ever-evolving laws of personal finance, this textbook could not have come at a better time. —Dr. Philippa Kennealy MD MPH, The Entrepreneurial MD, Los Angeles, California Physicians have economic concerns unmatched by any other profession, arriving ten years late to the start of their earning years. This textbook goes to the core of how to level the playing field quickly, and efficaciously, by a new breed of dedicated Certified Medical Planners™. With physician-focused financial advice, each chapter is a building block to your financial fortress. —Thomas McKeon, MBA, Pharmaceutical Representative, Philadelphia, Pennsylvania An excellent resource … this textbook is written in a manner that provides physician practice owners with a comprehensive guide to financial planning and related topics for their professional practice in a way that is easily comprehended. The style in which it breaks down the intricacies of the current physician practice landscape makes it a ‘must-read’ for those physicians (and their advisors) practicing in the volatile era of healthcare reform. —Robert James Cimasi, MHA ASA FRICS MCBA CVA CM&AA CMP™, CEO-Health Capital Consultants, LLC, St. Louis, Missouri Rarely can one find a full compendium of information within a single source or text, but this book communicates the new financial realities we are forced to confront; it is full of opportunities for minimizing tax liability and maximizing income potential. We’re recommending it to all our medical practice management clients across the entire healthcare spectrum. —Alan Guinn, The Guinn Consultancy Group, Inc., Cookeville, Tennessee Dr. David Edward Marcinko MBA CMP™ and his team take a seemingly endless stream of disparate concepts and integrate them into a simple, straightforward, and understandable path to success. And, he codifies them all into a step-by-step algorithm to more efficient investing, risk management, taxation, and enhanced retirement planning for doctors and nurses. His text is a vital read—and must execute—book for all healthcare professionals and physician-focused financial advisors. —Dr. O. Kent Mercado, JD, Private Practitioner and Attorney, Naperville, Illinois
Kudos. The editors and contributing authors have compiled the most comprehensive reference book for the medical community that has ever been attempted. As you review the chapters of interest and hone in on the most important concerns you may have, realize that the best minds have been harvested for you to plan well… Live well. —Martha J. Schilling; AAMS® CRPC® ETSC CSA, Shilling Group Advisors, LLC, Philadelphia, Pennsylvania I recommend this book to any physician or medical professional that desires an honest no-sales approach to understanding the financial planning and investing world. It is worthwhile to any financial advisor interested in this space, as well. —David K. Luke, MIM MS-PFP CMP™, Net Worth Advisory Group, Sandy, Utah Although not a substitute for a formal business education, this book will help physicians navigate effectively through the hurdles of day-to-day financial decisions with the help of an accountant, financial and legal advisor. I highly recommend it and commend Dr. Marcinko and the Institute of Medical Business Advisors, Inc. on a job well done. —Ken Yeung MBA CMP™, Tseung Kwan O Hospital, Hong Kong I’ve seen many ghost-written handbooks, paperbacks, and vanity-published manuals on this topic throughout my career in mental healthcare. Most were poorly written, opinionated, and cheaply produced self-aggrandizing marketing drivel for those agents selling commission-based financial products and expensive advisory services. So, I was pleasantly surprised with this comprehensive peer-reviewed academic textbook, complete with citations, case examples, and real-life integrated strategies by and for medical professionals. Although a bit late for my career, I recommend it highly to all my younger colleagues … It’s credibility and specificity stand alone. —Dr. Clarice Montgomery PhD MA,Retired Clinical Psychologist In an industry known for one-size-fits-all templates and massively customized books, products, advice, and services, the extreme healthcare specificity of this text is both refreshing and comprehensive. —Dr. James Joseph Bartley, Columbus, Georgia
My brother was my office administrator and accountant. We both feel this is the most comprehensive textbook available on financial planning for healthcare providers. —Dr. Anthony Robert Naruska DC,Winter Park, Florida
Posted on April 6, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
THE AMA A.U.I. REPORT
***
By Staff Reporters
Doctors are excited—yet cautious—about the role augmented intelligence (AUI) could play in the future of healthcare. That’s the takeaway from an American Medical Association (AMA) survey released last month.
About two-thirds (65%) of 1,000+ physicians that the AMA surveyed in August 2023 agreed that there was at least some advantage to using AUI-powered tools, particularly when it comes to diagnostic ability (72%), work efficiency (69%), and clinical outcomes (61%). More than half (56%) of doctors said AUI tools could best help address administrative burdens.
Posted on April 5, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
On March 5th, 2024, the Department of Justice’s (DOJ’s) Antitrust Division, the Federal Trade Commission (FTC), and the Department of Health and Human Services (HHS), announced the launch of a multi-agency inquiry – in the form of a request for information (RFI) and public workshop – focusing on the increasing control of private equity (PE) and other corporations over the healthcare industry.
This Health Capital Topics article discusses the agencies recent actions and how it appears to be in line with the government’s recent moves to crack down on anti-competitive actions in healthcare. (Read more…)
The Institute of Medical Business Advisors Inc identified several reasons based on observations working with medical professional and physician clients over the years.
A late start
By the time doctors finish medical school and residency they’re typically in their middle or late thirties. Many have families to feed, and substantial student loans to pay off. It will be years before they can even start accumulating wealth. Consider that physicians typically enter careers at later ages, often with larger debts from training. Some specialties may not lead a case until 10 years of practice, and many specialties have limited longevity. Peak earning years may also be shorter for health care providers than other professionals. Financial survival skills are paramount for converting the limited earnings time period to personal financial security.
Challenging socio-political environment
It is increasingly challenging to practice medicine. With the Medicare Trust Fund slated to go bust in 2019, the Center for Medicare and Medicare Service (CMS) is increasingly resorting to cutting physician reimbursements and implementing capitation and bundled value based medical payments models. The medical reimbursement effects of the PP-ACA are not yet fully discerned; but appear to continue the decline in compensation. And to illustrate this potential governmental control, in what other industry can participants debate the simple question, “who is the customer?”
Lifestyle expectations
Society expects a doctor to live like a doctor, dress like a doctor, and drive like a doctor. Meeting social expectations can be quite expensive.
Time and energy
A doctor can’t be just a doctor any more. S/he also has to deal with ever increasing regulatory mandates, paperwork requirements by state and federal agencies and capricious insurance companies. It is estimated that for every hour spent on patient care, and additional half-hour is spent on paperwork. To-date, the use of electronic medical records has exacerbated; not ameliorated this problem. The demand on their time is mind-boggling. A typical doctor works a ten- to twelve-hour day. After work and family, they simply don’t have time and energy left to do comprehensive financial planning.
Financially naïve
Doctors are smart. They’re highly trained in their area of expertise. But, that doesn’t translate into understanding about finance or economics. Because they are smart, it’s easy for them to think they can easily master and execute concepts of personal financial planning, as well. Often, they don’t.
Lack of trust and delegation
Many doctors don’t trust financial advisors working for major Wall Street banks. They have the good instinct to realize that their interests are not aligned. Not knowing there are independent advisors out there who observe a strict fiduciary standard, they tend to do everything by themselves.
In fact, Paul Larson CFP®, President-CEO of the firm LARSON Financial Group LLC, noted a disquieting trend among physician client in his firm [personal communication]. Almost 90% of them fail to take care of their own family finances in a comprehensive manner; while only 10% are succeeding. The strategies in this chapter and book are common to their success.
Too Trusting
Another aspect of naivety, many physicians do not realize that the financial advisory industry lacks the same discipline and regulation that the average physician operates in. A primary care doctor would never even attempt a complicated surgery on a patient, but is trained to refer such patients to a specialist in the field with the proper training and experience. Financial Advisors often come from a sales background and are trained to keep a client in house even if the advisor is lacking in expertise. Also, many physicians are not trained to discern a qualified financial advisor from a sales person dressed up like a financial advisor. It is illegal to call yourself a physician in the United States unless you have the credentials to back it up; yet, anyone in the US can legally call themselves a financial advisor or a financial planner.
Posted on April 3, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
PATIENT COMPLICATION RATES
By Staff Reporters
***
***
Hospitals under private equity (PE) ownership reported higher rates of patient complications when compared to other facilities, according to a recent JAMA study—raising questions about how the business model might affect staffing and subsequent quality of care.
The surveyed Medicare beneficiaries saw a 25.4% increase in “hospital-acquired conditions,” which the Centers for Medicare and Medicaid Services defines as falls, infections, and other adverse events, when they received treatment at a PE-acquired hospital compared to those run under other forms of ownership.
On the whole, the study found that Medicare enrollees at hospitals under PE control were not only younger and less likely to additionally qualify for Medicaid but also more likely to experience complications.
Posted on April 2, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
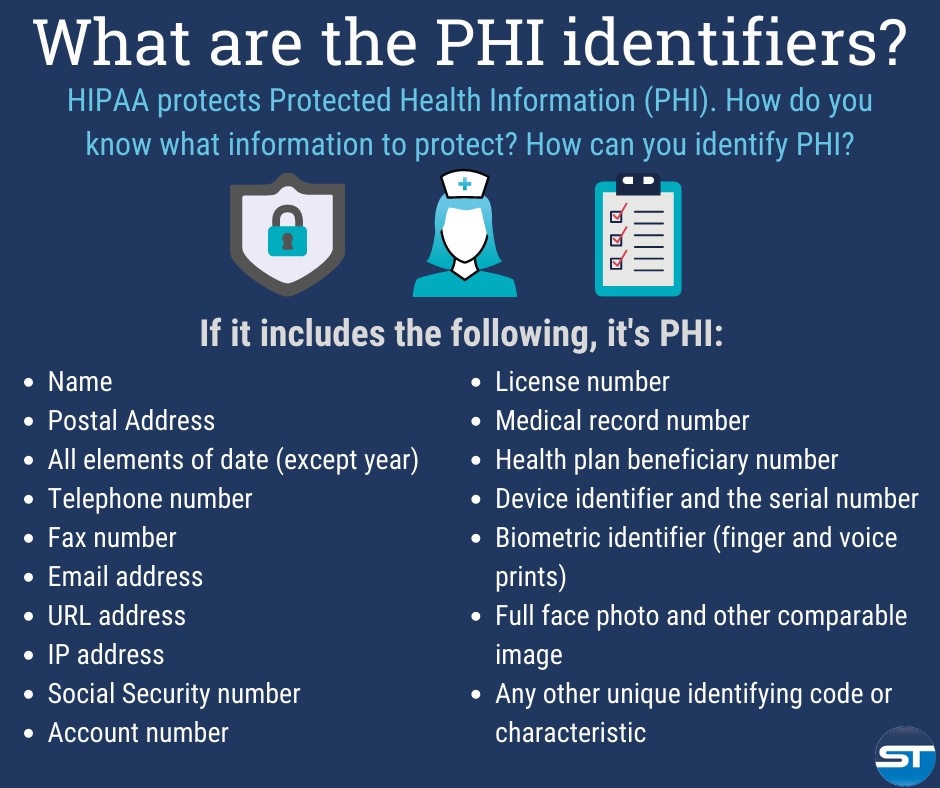
The Designated Medical Record Set [DMRS]: Contains medical and billing records and any other records that a physician, hospital, clinic and/or medical practice utilizes for making decisions about a patient; a hospital, emerging healthcare organization, or other healthcare organization. It serves to define which set of information comprises “protected health information” and which set does not; or contains medical or mixed billing records, and any other information that a physician and/or medical practice utilizes for making decisions about a patient.
It is up to the hospital or healthcare organization to define which set of information comprises “protected health information” and which does not though logically this should not differ from locale to locale. The patient has the right to know who in the lengthy data chain has seen their Protected Health Information. This sets up an audit challenge for the medical organization, especially if the accountability is programmed, and other examiners view the document without cause.
Posted on April 2, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
What’s Your Back-up Plan – Doctor?
As per a recent study, 32% of data is lost by human errors. However hardware, software, hacks and smack-downs are responsible for remaining 68% data loss.
Data protection gains major importance in data loss. It can be achieved by implementing data management successfully.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on April 2, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Federal health officials said they would offer emergency funding to physicians, physical therapists, and other professionals that provide outpatient healthcare, following a cyberattack that crippled the nation’s largest processor of medical claims and left many organizations in financial distress. The Centers for Medicare and Medicaid Services also announced that it would make advance payments available to suppliers that bill through Medicare Part B, which serves a wide array of healthcare organizations.
***
***
Officials had previously announced a similar program to make emergency payments available for hospitals that had been ensnared by the February 21st hack of Change Healthcare, a unit of UnitedHealth Group, and have struggled to get paid for more than two weeks. The emergency funds represent upfront payments made to healthcare providers and suppliers based on their expected future claims.
Posted on April 1, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
On March 9th, 2024, President Biden signed into law a $460 billion spending package to continue funding the federal government for the remainder of the 2024 fiscal year. Contained within the spending package was legislation to cut in half the 2024 Medicare physician payment update of approximately -3.4%.
This Health Capital Topics article discusses the payment update, other healthcare provisions contained in the bipartisan spending bills, and responses from stakeholders. (Read more…)
It’s never a source of pride stepping out of a dirty car or truck, especially for image conscious doctors. But, keeping your vehicle looking like new, for the doctor’s parking lot, is tough work. Sure, you may take it through the drive-thru car wash every now and then, but that isn’t the deep cleaning that your car deserves.
All in the Details
Detailing, on the other hand, is promised to give your beloved vehicle that ‘new-car’ feeling all over again. It isn’t easy work, but the results are amazing. While you could detail your car at home, is it really worth it? Let’s take a look at why letting the pros detail your vehicle is the way to go – or – not!
Working at the Car Wash
When you wash your vehicle at a drive-thru car wash, you may be doing more harm than good. If the car wash has brushes or pieces of cloth that scrub your vehicle as it goes through, these components can easily scratch your car’s finish. All of the bits of dirt from cars before can be trapped in the cloth and brushes, and as they scrub your vehicle, they act as sandpaper, permanently marring your paint.
One step better is hand washing your car at home, but even then, you must be careful to not just become a humanized version of the car wash. Using two buckets is a good start, with one bucket being a rinse bucket to remove the dirt from your sponge, and the other containing the soap.
SOAP Suds – Not SOAP Notes
Also, be careful of the type of soaps and car care products being used. The interior and exterior cleaners found at the local parts store are often of decent quality, but they aren’t always the best, and they must be used properly. Even then, for a normal car owner, detailing a car can become an all-day task, sometimes with less than perfect results.
Don’t forget to use a clay bar or brick followed by your favorite Carnuba wax, too.
The Pros
So, why should you let the pros handle your detailing needs? They should know exactly what specialty products are right for your vehicle to get the perfect results every time. And, they know the techniques that will yield showroom-finish results while you don’t have to even touch your car.
And, while you won’t want to clean out all the dried soda, coffee stains, or leftover cheeseburger wrappers from under your seat, they will gladly do it for you – for a price.
Imagine
Just picture getting into a blindingly shiny, clean vehicle with an interior that looks equally as pristine. No more purchasing all kinds of car care products that don’t deliver results. No more spending hours in the driveway getting soaked and frustrated. No more wasted time. Pros know what it takes to detail your vehicle to concourse standards.
But then, it is just a job for them. It is a labor of love for me. Am I neurotic or compulsive?
My near showroom and mint conditioned 2000 Jaguar XJ-V8-L is a full-size luxury sedan, offers sporting drive characteristics, mixed with a classic style and interior comfort. It was available in multiple trims which all came very well equipped with upscale amenities.
And, this extended wheelbase version offers much more rear seat leg room for long and winding Georgia road trips. The standard steel engine [not nikasil] in this XJ is a 4.0L V8 which produces 290 hp. The upper and lower timing chain tensioners are original, second generation metal, not plastic.
There is also a supercharged version of this vehicle which bumps output to an impressive 370 hp. Even with all of its power and weight, my XJ-8-L is still rated at over 20 mpg on the highway. Ammenities and upgrades include a mobile phone, Magellan GPS, LoJack theft recovery system, CD and MP-3 players, with internal and external cable antenna for satellite radio.
What a Cat? She is my third favorite female after my intelligent and beautiful wife, and smart and lovely daughter.
Conclusion
Are you a DIYer, like me? Nothing says you care more than doing it yourself.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Managerial and medical cost accounting is not governed by generally accepted accounting principles (GAAP) as promoted by the Financial Accounting Standards Board (FASB) for CPAs. Rather, a healthcare organization costing expert may be a Certified Cost Accountant (CCA) or Certified Managerial Accountant (CMA) designated by the Cost Accounting Standards Board (CASB), an independent board within the Office of Management and Budget’s (OMB) Office of Federal Procurement Policy (OFPP).
The Cost Accounting Standards Board
CASB consists of five members, including the OFPP Administrator who serves as chairman and four members with experience in government contract cost accounting (two from the federal government, one from industry, and one from the accounting profession). The Board has the exclusive authority to make, promulgate, and amend cost accounting standards and interpretations designed to achieve uniformity and consistency in the cost accounting practices governing the measurement, assignment, and allocation of costs to contracts with the United States.
Codified at 48 CFR
CASB’s regulations are codified at 48 CFR, Chapter 99. The standards are mandatory for use by all executive agencies and by contractors and subcontractors in estimating, accumulating, and reporting costs in connection with pricing and administration of, and settlement of disputes concerning, all negotiated prime contract and subcontract procurement with the United States in excess of $500,000. The rules and regulations of the CASB appear in the federal acquisition regulations.
North American Industry Classification System (NAICS) codes are used to categorize data for the federal government. In acquisition they are particularly critical for size standards. The NAICS codes are revised every five years by the Census Bureau. As of October 1, 2007, the federal acquisition community began using the 2007 version of the NAICS codes at www.census.gov/epcd/www/naics.html
Cost Accounting Standards
Healthcare organizations and consultants are obligated to comply with the following cost accounting standards (CAS) promulgated by federal agencies:
CAS 501 requires consistency in estimating, accumulating, and reporting costs.
CAS 502 requires consistency in allocating costs incurred for the same purpose.
CAS 505 requires proper treatment of unallowable costs.
CAS 506 requires consistency in the periods used for cost accounting.
The requirements of these standards are different from those of traditional financial accounting, which are concerned with providing static historical information to creditors, shareholders, and those outside the public or private healthcare organization.
Assessment
Functionally, most healthcare organizations also contain cost centers, which have no revenue budgets or mission to earn revenues for the organization. Examples include human resources, administration, housekeeping, nursing, and the like. These are known as responsibility centers with budgeting constraints but no earnings. Furthermore, shadow cost centers include certain non-cash or cash expenses, such as amortization, depreciation and utilities, and rent. These non-centralized shadow centers are cost allocated for budgeting purposes and must be treated as costs http://www.CertifiedMedicalPlanner.org
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
A young concierge medical practice is a business with challenges in these Customer [Patient] Relationship Management’s [CRM] areas that are critical for success.
Areas of Most Challenge
Maturity of Processes:
Processes are often associated with bureaucracy or stuffy hierarchical healthcare systems that are anathema to emerging concierge medical practices. At small practices, doctors are often owners who fiercely pride themselves on flat structures, autonomy and flexibility. However, processes are imperative to conduct a streamlined practice that can be woven around a CM culture that still ensures practice business is conducted in a systematic manner.
Organization Structure:
Young concierge medical practices have challenges managing growth while grappling to incorporate an organization structure that promotes the elite private practice culture.
Multi-tasking, rapidly growing work places:
Young CM practices are often characterized by employees who multi-task and assume several roles to make their resources stretch farther. Especially in the current healthcare reform climate, young practice employees take up a broader set of responsibilities. In addition, as young private CM practices grow, they may become anguished with a growing office workplace that may not be equipped with an evolving infrastructure to cope. They have a fierce need to carefully control growth with tightly managed resources.
Changing business needs and strategy:
In an era after the golden age of traditional medicine, profitability is critical for emerging concierge practices. It is imperative to be nimble and change marketing strategies as socio-political and competitive climates dictate. A good C[P] RM system is tightly integrated, but loosely coupled, to allow CM practices to communicate appropriately with patients.
Little room for Slack:
Small concierge medical practices do not have as much established name-brand equity as larger, established practices of any model type, and patients are less willing to tolerate mistakes. Concierge practices have to run a much tighter ship and build impeccable patient experiences.
Fierce Competition:
The cash or retainer medicine landscape today looks very different from just five years ago. Competition is becoming fierce and practices are fighting for mindshare and patients. Young practices are competing with older concierge practices – large traditional practices, micro-practices, behemoth healthcare systems, enterprise-wide medical corporations and every other practice model in-between – to attract and retain patients with private resources.
Assessment
The above characteristics form the basis of a compelling strategy to embrace C[P]RM and streamline patient relationships and cash revenue opportunities. Concierge practices still need to build scalable marketing programs that can easily ramp up and down effortlessly as needs and economic environments demand. But, they do need to establish marketing metrics and processes that can demonstrate the Return on Investment (ROI) on their CRM, and marketing programs, and for getting critical cash-paying patient buy-in.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
The fact that every physician in private medical practice, without a business education, leaves approximately a million dollars on the table and is unaware of it is well known to business experts who work with medical doctors experiencing financial difficulties.
Business experts such as Dan S. Kennedy, Peter Drucker, Michael Gerber, Maxwell Maltz, Neil Baum, William Hanson,Huss and Coleman, Steven Hacker, Thomas Stanley, Chris Hurn, Napoleon Hill, and Dave Ramsey, among others, understand the financial problems faced by medical practices and how to solve them.
Posted on March 25, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Colin Hung
***
Small- and medium-sized medical practices are struggling. The uncertain economic environment, staffing challenges, and the increasing complexity of providing care is putting practice owners under tremendous stress. EverHealth, providers of end-to-end solutions for healthcare providers, believes that these practices need support from partners that can take on some of the administrative, operational, and financial tasks so they can continue to deliver care to patients.
Healthcare IT Today sat down with Adam Laskey, General Manager of EverHealth at EverCommerce, to find out more about the company’s work, their vision for medical practices, and how the acquisitions of DrChrono and Updox is progressing.
Posted on March 24, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Financial hardship has led dozens of operators of senior facilities to file for bankruptcy over the past three years, with 13 companies filing petitions in 2021, 12 debtors filing in 2022 and 15 more in 2023, according to Gibbins Advisors.
***
***
Notable Chapter 11 filings over the past year have included Evangelical Retirement Homes of Greater Chicago, which filed Chapter 11 in the U.S. Bankruptcy Court for the Northern District of Illinois in June 2023 to sell its assets at auction. Also, Windsor Terrace Health, an operator of 32 nursing homes in California and three in Arizona, filed its petition in the U.S. Bankruptcy Court for the Central District of California in August 2023 listing $1 million to $10 million in assets and liabilities and unable to pay its debts.
More recently, Magnolia Senior Living, an operator of four facilities in Georgia, filed for Chapter 11 protection on March. 19 in the U.S. Bankruptcy Court for the Northern District of Georgia.
***
The Great Recession of 2008 had a lot of downsides: People lost homes, jobs, and retirement savings, had their careers derailed, and were forced to learn what the heck synthetic collateralized debt obligations are. But according to recent research, it also made people in the US live longer.
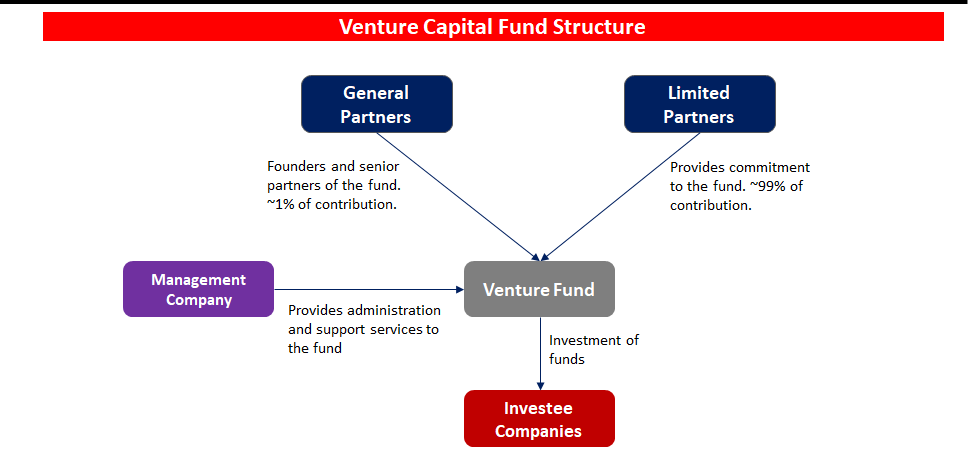
Venture capital funding in the digital health space cooled a bit in 2022 following a red-hot 2021. Overall, digital health companies raised $15.3 billion last year, down from the $29.1 billion raised in 2021—but still above the $14.1 billion raised in 2020, according to Rock Health a seed fund that supports digital health startups.
Nevertheless, analysts predict VC investors and bankers will still put a good amount of money into digital health in 2024 and 2025, especially in alternative care, drug development, health information technology technology, EMRs and software that reduces physician workload.
Of course. an essential first part of attracting VC interest and money is the crafting and presentation of your formal business plan [“elevator pitch”]; as well as the needed technical and managerial experience. This is crucial for success and exactly where we can assist.
(“Informed Voice of a New Generation of Fiduciary Advisors for Healthcare”)
For most lay folks, personal financial planning typically involves creating a personal budget, planning for taxes, setting up a savings account and developing a debt management, retirement and insurance recovery plan. Medicare, Social Security and Required Minimal Distribution [RMD] analysis is typical for lay retirement. Of course, we can assist in all of these activities, but lay individuals can also create and establish their own financial plan to reach short and long-term savings and investment goals.
But, as fellow doctors, we understand better than most the more complex financial challenges doctors can face when it comes to their financial planning. Of course, most physicians ultimately make a good income, but it is the saving, asset and risk management tolerance and investing part that many of our colleagues’ struggle with. Far too often physicians receive terrible guidance, have no time to properly manage their own investments and set goals for that day when they no longer wish to practice medicine.
For the average doctor or healthcare professional, the feelings of pride and achievement at finally graduating are typically paired with the heavy burden of hundreds of thousands of dollars in student loan debt.
You dedicated countless hours to learning, studying, and training in your field. You missed birthdays and holidays, time with your families, and sacrificed vacations to provide compassionate and excellent care for your patients. Amidst all of that, there was no time to give your finances even a second thought.
Between undergraduate, medical school, and then internship and residency, most young physicians do not begin saving for retirement until late into their 20s, if not their 30s. You’ve missed an entire decade or more of allowing your money and investments to compound and work for you. When it comes to addressing your financial health and security, there’s no time to waste.
Almost every medical profession has its fair share of grossness and unbelievable moments. But, when it comes to podiatrists, you could argue that they have it extra bad for the simple reason that they specialize in feet. Most people would probably agree feet can be one of the human body’s most disgusting parts. People often neglect or ignore their feet, which can suffer badly from some common diseases and become a hotbed for unsanitary practices.
But, is a podiatrist really a physician?
You bet! Now, while the American Podiatric Medical Association [APMA] defines Doctor of Podiatric Medicine, or podiatrist, as “a physician and surgeon of the foot and ankle,” the The Social Security Administration’s Program Operations Manual System (POMS) legally defines a podiatrist as the following:
A podiatrist is a “physician” with respect to those functions which the podiatrist is legally authorized to perform in the State in which the individual performs them. Furthermore, the POMS states: A podiatrist is considered a “physician” for any of the following purposes: 1. for making the required physician certification and re-certifications of the medical necessity for Part A and Part B provider services. 2. for the purpose of establishing and periodically reviewing a home health plan of treatment; and for purposes of constituting a member of a Utilization Review (UR) committee but only if: a. the performance of these functions is consistent with the policy of the institution or agency with respect to which the podiatrist performs them; b. the podiatrist is legally authorized by the State to perform such functions; and c. at least two of the physicians on the Utilization Review committee are doctors of medicine or osteopathy.
In the United States, podiatrists are educated and licensed as Doctors of Podiatric Medicine (DPM). After a 4-year bachelor’s degree, the preparatory education of most podiatric physicians — similar to the paths of traditional physicians (MD or DO) — includes four years of undergraduate work, followed by four years in an accredited podiatric medical school, followed by a three or four year hospital-based residency program.
Optional one to two-year fellowships in foot and ankle reconstruction, surgical limb salvage, sports medicine, plastic surgery, pediatric foot and ankle surgery, and wound care is also available. Podiatric medical residencies and/ or fellowships are accredited by the Council on Podiatric Medical Education (CPME). The overall scope of podiatric practice varies from state to state with a common focus on foot and ankle surgery. Podiatrists work in hospitals, private practices and clinics, university medical centers and/or specialized practices.
Generally podiatrists can:
Perform physical examinations and study medical histories
Order and interpret X-rays and also other imaging studies like MRIs, and CAT scans.
Giving podiatric advice, second opinions and diagnosis
Administer drugs, narcotics, anesthetics and also sedation
Perform surgery related to the foot, ankle and legs
Perform plastic, macro and micro-surgeries and reconstructive bone surgeries
Prescribe medications such as narcotic pain killers, sleep aides and antibiotics
Perform certain physical and occupational therapies
Be on hospital staffs and take Emergency Room hospital call
Be on health insurance plans for covered physicians and medical providers
Prescribe, order, and fit prosthetics, casts, insoles, and orthotic devices
Attest to physical disability, write a doctor’s medical, treatment or absentee note, etc
In fact, the American Board of Podiatric Medicine [ABPM] offers a comprehensive qualification and certification process in podiatric medicine and orthopedics. Sub-specialties of podiatry include:
Posted on March 15, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
On December 26, 2023, a study published in the Journal of the American Medical Association (JAMA) found concerning changes in patient outcomes and hospital adverse events associated with private equity (PE) acquisition and ownership of hospitals. Over the past ten years, PE firms have set their sights on hospitals as a lucrative investment opportunity, spending nearly $1 trillion to finance healthcare acquisitions, and purchasing more than 200 hospitals from non-PE owners.
Did you know that the American Medical Association is calling on medical schools and residency programs to include specific information about healthcare economics and financing in their curricula.
But, is health economics heterodoxic, or not? And; what about demand-derived economics in medicine?
Posted on March 12, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
On January 29, 2024, the Centers for Medicare and Medicaid Services (CMS) announced that Performance Year 2024 participation increased in their various accountable care organization (ACO) initiatives. Specifically, 50 new ACOs joined the Medicare Shared Savings Program (MSSP), and 71 ACOs renewed their contracts, bringing the total participation in the MSSP to 480 ACOs.
Additionally, 245 organizations chose to continue participation in two other CMS models – the ACO Realizing Equity, Access, and Community Health (REACH) Model and the Kidney Care Choice (KCC) Model.
Posted on March 11, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Indications for 2024
By Health Capital Consultants, LLC
***
***
After healthcare mergers and acquisitions (M&A) activity began to regain momentum in 2022, following the slowing of deals in the wake of the COVID-19 pandemic, transactional activity continued to accelerate in 2023. While the healthcare sector continued to be impacted by factors such as valuation gaps, higher-for-longer interest rates, general macroeconomic risks, and increased state and federal regulatory concerns in 2023, the outlook for 2024 remains cautiously optimistic.
This Health Capital Topics article reviews the U.S. healthcare industry’s 2023 M&A activity and discusses what these trends may mean for 2024. (Read more…)
Posted on March 10, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Stat: According to HIPPA, and the cyberattack on Change Healthcare, there were 725 “large” reported healthcare security breaches in the US last year. Experts say health organizations suffer from a lack of basic security measures, and are being targeted by “increasingly sophisticated cyberattacks.” (The HIPAA Journal)
Quote: “Having a [doctor] who can coordinate your healthcare and is willing to do so on a personal basis was very important to me. And I really feel like that is completely gone, and I feel like it happened overnight.”—Deborah Wood, an older adult patient at primary care provider Iora Health, where some patients say care quality has worsened after Amazon acquired its parent company One Medical in 2022 (the Washington Post)
Posted on March 8, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
TO FIX THE FDA APPROVAL’S FLAW
By Staff Reporters
***
***
DEFINITION: Right-to-try laws are United States state laws and a federal law that were created with the intent of allowing terminally ill patients access to experimental therapies (drugs, biologics, devices) that have completed Phase I testing but have not been approved by the Food and Drug Administration (FDA).
This law would allow patients suffering from rare and genetic diseases to try personalized treatments not yet approved by the FDA, as long as they have the support of their physician and have exhausted other treatment options. This policy would have an outsized impact on patients with rare diseases. Although rare diseases have small patient pools by definition, collectively, about 30 million Americans are estimated to have a rare disease.
Posted on March 4, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Spiked in 2023
By Staff Reporters
***
***
Healthcare company bankruptcies spiked in 2023 amid high interest rates, rising labor and supply costs, and an uptick in denials from payers, according to a January report from healthcare restructuring firm Gibbins Advisors.
For example, Seventy-nine healthcare companies filed for bankruptcy in 2023—the highest number since 2019, which saw 51 bankruptcies, according to the report. The volume of bankruptcies last year was nearly 2x as high as 2022 and over 3x the level seen in 2021.
“We saw a dramatic increase in healthcare bankruptcy filings in 2023, continuing the trend which began in mid-2022,” Clare Moylan, co-founder and principal at Gibbins Advisors, said in a statement. “Key observations from 2023 are the return of large bankruptcy cases with over $100 million in liabilities, and a spike in hospital filings, both of which appear to primarily be a result of Covid-19 pandemic-related protections ending.”
Our virtual consulting model at DE MARCINKO & ASSOCIATES offer services to their clients primarily or entirely online, by phone or video-conference.
This means that no matter where you are or choose to live, you’re always just an email, telephone call or Zoom® conference away from a face-to-face meeting.
THE CONSULTATION IS VIRTUAL – THE INFORMATIONAL ADVICE IS REAL !
Posted on March 1, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Cyber villains have struck again, and they’re going after the US health system. Pharmacies and hospitals nationwide are coping with a debilitating cyberattack against the prescription processor Change Healthcare, owned by America’s biggest health insurer, UnitedHealth.
The health tech company noticed the breach last week and rushed to disconnect its systems, throwing a wrench into pharmacies’ ability to dispense pills. Change Healthcare said some of its services were still on pause, and it’s unclear if any patient info was stolen.
Posted on February 28, 2024 by Dr. David Edward Marcinko MBA MEd CMP™
Pay for Performance Initiatives
[By Staff Writers]
Of course, consumer directed healthcare trends and fee transparency increasingly mandate physician economic accountability, such as in the P4P initiatives, but CMS may also begin profiling physicians and targeting those it deems inefficient sometime next year, as well.
In May 2007, Herbert Kuhn, acting deputy administrator of CMS, told a House subcommittee that the agency will have the data and computer capacity available to do tracking as soon as mid-2008.
To monitor efficiency, CMS would compare levels of tests physicians order for certain types of patients to tests ordered by other doctors who achieve similar outcomes. The agency would then contact the physicians whose testing patterns seem to be out of line. No doubt, the effects on private pay-for-performance [P4P] initiatives is obvious. Kuhn told the subcommittee that his largest concern was figuring out how to use the data to help physicians grow more efficient.
Assessment
To date, the agency hasn’t established plans to link efficiency measures with reimbursement changes. If it wants to do so, Congress would probably have to enact new legislation, according to several policymakers.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
In a January 24th letter, AHA and other national hospital organizations voiced support for the Safety from Violence for Healthcare Employees (SAVE) Act (H.R. 2584/S. 2768), bipartisan legislation that would provide federal protections for health care workers similar to those that apply to aircraft and airport workers.
“Although our members have for many years had protocols in place designed to protect their employees and promote a safe environment for patient care, the number of violent attacks against health care workers has increased markedly in recent years,” the letters to House and Senate sponsors note. “Recent studies indicate that 44% of nurses have reported being subjected to physical violence and 68% have reported verbal abuse. These experiences affect the individual provider, who may suffer from both physical and psychological trauma, and they can also interfere with care delivery when providers fear for their personal safety, are distracted by disruptive patients or family members, or are traumatized from prior violent interactions. These types of incidents also consume scarce hospital and health system resources, which in turn could impact the care available for other patients.”
Managed care insurers have profited handsomely from Medicare Advantage plans, scoring billions in annual profits. They credit this financial wizardry to their use of sophisticated data analytics, preventative care, cost optimization, provider networks, evidence and value-based care and risk mitigation strategies. However, doctors, hospitals, and medical providers assert something else.
In fact, Medicare Advantage plans have been making headlines in 2024, but not in a positive light, at least for health insurance companies. Medicare is a government-sponsored health insurance benefit; generally for retired people aged 65 and older.
For most, the money for Medicare Part B medical insurance or Part C Medicare Advantage plans is withdrawn directly from Social Security benefits monthly, coupled with a relatively small monthly payment from the patient. Nearly half of the Medicare population is enrolled in Part C Medicare Advantage plans.
***
***
However, there have been rumblings in the medical sector between medical providers and medical insurers coming to a head. So, where do you stand?