BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
The concept of a self-taught and student motivated, but automated outcomes driven classroom may seem like a nightmare scenario for those who are not comfortable with computers. Now everyone can breathe a sigh of relief, because the Institute of Medical Business Advisors just launched an “automated” final examination review protocol that requires no programming skill whatsoever.
In fact, everything is designed to be very simple and easy to use. Once a student’s examination “blue-book” is received, computerized “robotic reviewers” correct student assignments and quarterly test answers. This automated examination model lets the robots correct tests and exams, while the students concentrate on guided self-learning.
Posted on July 22, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
BOOK REVIEW
“The Dictionary of Health Insurance and Managed Care lifts the fog of confusion surrounding the most contentious topic in the health care industrial complex today. My suggestion therefore is to ‘read it, refer to it, recommend it, and reap’.”
—Michael J. Stahl, PhD, Physician Executive MBA Program [William B. Stokely Distinguished Professor of Business]
The University of Tennessee, College of Business Administration
Posted on July 21, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
TEXTBOOK RELEASE AND REVIEW
Reviews
Navigating a course where sound organizational management is intertwined with financial acumen requires a strategy designed by subject-matter experts. Fortunately, Financial Management Strategies for Hospital and Healthcare Organizations: Tools, Techniques, Checklists and Case Studiesprovides that blueprint. ―David B. Nash, MD, MBA,Jefferson Medical College, Thomas Jefferson University
It is fitting that Dr. David Edward Marcinko, MBA, CMP™ and his fellow experts have laid out a plan of action in Financial Management Strategies for Hospital and Healthcare Organizationsthat physicians, nurse-executives, administrators, institutional CEOs, CFOs, MBAs, lawyers, and healthcare accountants can follow to help move healthcare financial fitness forward in these uncharted waters. ―Neil H. Baum, MD, Tulane Medical School
The U.S. individual tax return is based around the concepts of Adjusted Gross Income (AGI) and Taxable Income (TI). AGI is the amount that shows up at the bottom of page one of Form 1040, individual income tax return. It is the sum of all of the taxpayer’s income less certain allowed adjustments (like alimony, one-half of self-employment taxes, a percentage of self-employed health insurance, retirement plan contributions and IRAs, moving expenses, early withdrawal penalties and interest on student loans). This amount is important because it is used to calculate various limitations within the area of itemized deductions (e.g., medical deductions: 10 percent of AGI; miscellaneous itemized deductions: 2 percent of AGI).
When a healthcare professional taxpayer hears the phrase “an above the line deduction”, the line being referenced is the AGI line on the tax return. Generally, it is better for a deduction to be an above the line deduction, because that number helps a taxpayer in two ways. First, it reduces AGI, and second, since it reduces AGI, it is also reducing the amounts of limitations placed on other deductions as noted above.
Obviously, if there is an above the line there is also a “below the line” deduction. These below the line deductions are itemized deductions (or the standard deduction if itemizing is not used) plus any personal exemptions allowed. AGI less these deductions provides the taxable income on which income tax is actually calculated. All of that being said, it is better for a deduction to be an above the line deduction. Although this is a bit dry, it helps to understand the concepts in order to know where items provide the most benefit to the medical professional taxpayer.
PERSONAL TAXATION CALCULATIONS
Gross Income (all income, from whatever source derived, including illegal activities, cash, indirect for the benefit of, debt forgiveness, barter, dividends, interest, rents, royalties, annuities, trusts, and alimony payments-no more)
Less non-taxable exclusions (municipal bonds, scholarships, inheritance, insurance
proceeds, social security and unemployment income [full or
partial exclusion], etc.).
Total Income
Less Deductions for AGI (alimony, IRA contributions, capital gains, 1/2 SE tax,
moving, personal, business and investment expenses, and
penalties, etc.).
Adjusted Gross Income (bottom Form 1040)
Less Itemized Deductions from AGI, (medical, charitable giving, casualty,
involuntary conversions, theft, job and miscellaneous expenses, etc.), or
Less Standard Deduction (based on filing status)
Less Personal Exemptions (per dependents, subject to phase outs)
Taxable Income
Calculate Regular Tax
Plus Additional Taxes (AMT, etc.)
Minus Credits (child care, foreign tax credit, earned income housing, etc.)
Recruitment has become a refined art in recent years as practices and physicians themselves grow increasingly savvy about the finer points of marketing positions and securing employment. It’s more competitive than ever, too. Many organizations are going after the same physicians. Add to that a shortage of doctors in key specialties and certain geographical areas and the pressure becomes that much more intense. Moreover, the aging of the physician workforce, their increased dissatisfaction with managed care, and changes in doctors’ work expectations (they want more free time) have affected the demand and supply.
Additionally, both practicing physicians and residents fresh out of training have become more discerning and skillful in managing the search process. Candidates have learned to be selective based on how they’re treated on the phone, how they’re treated in person during site visits, or how smoothly the negotiations go. One small bump in the road and they could choose to go elsewhere. In truth, they look to rule organizations out, not in.
Even the smallest of practices must have an effective recruitment plan because they compete directly with the big guys — larger practices and hospitals that have polished their efforts and perfected their processes.
Facts about Physician Recruiters and Executive Search Firms
1) If you are job hunting, you should send your resume to recruiters
Different recruiters know about different positions. They do not usually know about the same ones. This is particularly true with retained firms. By sending your resume out widely, you will be placed in many different confidential databases and be alerted of many different positions. If you send your resume to only a few, it may be that none you send to will be working with positions which are suited for you. Throw your net widely.
If you change jobs, it is also wise to send follow-up letters to the recruiters and alert them of your new career move. Many search firms follow people throughout their careers and enjoy being kept up-to-date. It is a good idea to have your resume formatted in plain text so you can copy and paste it into email messages when requested to do so. Then, follow up with a nicely formatted copy on paper by postal mail.
Some estimate that only 1% to 3% of all resumes sent will result in actual job interviews. So, if you only send 50 resumes, you may only have less than 2 interviews, if that many. Send your resume to as many recruiters as you can. It is worth the postage or email time. Generally, recruiters will not share your resume with any employer or give your name to anyone else without obtaining your specific permission to do so. The recruiter will call first, talk to you about a particular position and then ask your permission to share your resume with that employer.
2) Your resume will be kept strictly confidential by the executive search firm.
It is safe to submit your resume to a search firm and not worry that the search firm will let it leak out that you are job hunting. Recruiters will call you each and every time they wish to present you to an employer in order to gain your permission. Only after they have gained your permission will they submit your name or resume to the identified employer. The wonderful aspect of working with search firms is that you can manage your career and your job search in confidence and privacy.
3) Fees are always paid by the employer, not the job candidate.
Recruiters and search firms work for the employer or hiring entity. The employer pays them a fee for locating the right physician for the job opening. This is important to remember, in that when you interact with executive recruiters, you are essentially interacting with an agent or representative of the employer. Recruiters are more loyal to employers than they are to job candidates because they work for the employer. This should not present a problem, but, should cause you to develop your relationship with the recruiter with the same integrity and professionalism that you would with the employer.
Recruiters are paid fees in one of two ways – retainer fees or contingency fees. This is an important distinction and will affect your process with both the employer and the recruiter. Some employers prefer working with contingency firms and some with retained firms. Both are respected by employers and useful in your job search, but, the two types of firms will not be handling the same positions with the same employers simultaneously.
A “retained” recruiter has entered an exclusive contract with an employer to fill a particular position. The retained recruiter, then, is likely to advertise a position, sharing the specifics of the position, location and employer openly. The retained firm feels a great obligation to fulfill the contract by finding the best person for the job.
A “contingency recruiter” on the other hand, usually does not have an exclusive relationship with the employer, and is only paid a fee if the job search is successful. Often, if the employer uses contingency firms, there will be more than one contingency firm competing to fill a certain position. As a job hunter, if you are sent to an interview by a contingency firm, you may find that you are competing with a larger number of applicants for a position. Generally, retained firms only send in from 3 to 5 candidates for a position.
Recruiters will be paid fees equal to about 25% to 35% of the resulting salary of the successful candidate plus expenses. This does not come out of the job candidate’s salary. This is paid to the recruiter through a separate relationship between the employer and the search firm. This may seem like a large fee, but, keep in mind that recruiters incur a great many expenses when searching for successful job candidates. They spend enormous amounts of money on computer systems, long distance calls, mail-outs, travel and interviews. Recruiters work very hard for these fees. Employers recognize the value of using recruiters and are more than willing to pay recruiters the fees. All you have to do is contact the recruiter to get the process moving.
4) Not all medical recruiters work only with physicians.
Some search firms work exclusively with physicians or in healthcare, while others may work in several fields at once. Some of the larger generalist firms will have one or more search consultants that specialize in healthcare. It is important for you, as a job hunter, to assess the recruiters’ knowledge of your field. If you use industry or medical specialty buzz words in describing your skills, experience or career aspirations, you may or may not be talking a language the recruiter understands fully. It is wise to explore fully with the recruiter his understanding of your field and area of specialization.
5) Recruiters and search consultants move around.
Recruiters, like many professionals, move to new firms during their careers. Often you will find that recruiters will work at several firms during their careers. Since it is much more effective to address your letters to a person rather than “to whom it may concern”, it is smart for job hunters to have accurate and up-to-date information about who is who and where, since this can change frequently. Search firms also move their offices, sometimes to another suite, street or state. If you have a list of recruiters that is over one year old, you will certainly waste some postage in mailing your resumes and cover letters. Many of your mail-outs will be returned to you stamped “non-deliverable”, unless you obtain an up-to-date list. A resource, like the Directory of Healthcare Recruiters is updated very frequently, usually monthly [www.pohly.com/dir3.html].
6) Most search firms work with positions all over the country.
If you are from a particular state, and want to remain in that state, don’t make the mistake of only sending your resume to recruiters in your state. Often the recruiters in your state are working on positions in other states, and recruiters in other states are working on positions in your state. This is usually the case. Very few recruiters work only in their local area, most work all around the US and some internationally. Regardless of your geographic preference, you should still send your resume to all the healthcare recruiters. If you really only want to remain in your area, you can specify that preference in your cover letter.
7) Recruiters primarily work with hard to fill positions or executive positions.
Some recruiters specialize in clinical positions for physicians, managed care executive positions, healthcare financial positions or health administration positions. Others may specialize in finding doctors, nurses or physical therapists. Generally, an employer does not engage a recruiter’s assistance in filling a position unless it is hard to fill. Sometimes employers will engage search firms to save them the valuable time of advertising or combing through dozens of resumes.
Contingency recruiters tend to work with more mid-level management and professional positions, but, this is not always the case. Retained firms generally work with the higher level clinical or administrative positions.
One thing you will be assured of is that if a recruiter is working on a position that means that the employer is willing to pay a fee. That usually means that the position is a valued position and one worth closer inspection on your part. Even in healthcare, with certain exceptions, our economy is an “employer’s market”. This means that employers receive a deluge of resumes for their open positions. Increasingly, employers are using recruitment firms to handle their openings and schedule the interviews because employers simply do not have the manpower or time to handle the many resumes they receive. Therefore, if a job hunter is submitted by a recruiter, that job hunter has a great advantage over all other applicants.
Posted on July 16, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
HSA Update 2021
By Michael Thompson
High-deductible health plans have been popular, but it’s becoming clear they are not right for all employees, said Michael Thompson, president and chief executive officer of the National Alliance of Healthcare Purchaser Coalitions.
Posted on July 12, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
MANAGEMENT STRATEGIES, OPERATIONAL TECHNIQUES, TOOLS, TEMPLATES AND CASE STUDIES
TEXTBOOKREVIEWS:
Hospitals and Health Care Organizationsis a must-read for any physician and other health care provider to understand the multiple, and increasingly complex, interlocking components of the U.S. health care delivery system, whether they are employed by a hospital system, or manage their own private practices.
The operational principles, methods, and examples in this book provide a framework applicable on both the large organizational and smaller private practice levels and will result in better patient care. Physicians today know they need to better understand business principles and this book by Dr. David E. Marcinko and Professor Hope Rachel Hetico provides an excellent framework and foundation to learn important principles all doctors need to know. ―Richard Berning, MD, Pediatric Cardiology
… Dr. David Edward Marcinko and Professor Hope Rachel Hetico bring their vast health care experience along with additional national experts to provide a health care model-based framework to allow health care professionals to utilize the checklists and templates to evaluate their own systems, recognize where the weak links in the system are, and, by applying the well-illustrated principles, improve the efficiency of the system without sacrificing quality patient care. … The health care delivery system is not an assembly line, but with persistence and time following the guidelines offered in this book, quality patient care can be delivered efficiently and affordably while maintaining the financial viability of institutions and practices. ―James Winston Phillips, MD, MBA, JD, LLM
Depression is Highest Among 18-25 Year Olds at 11%.
19% of US Adults Have Anxiety and 56% of Those with Anxiety Are Impaired By Their Condition.
12% of People with Diabetes Have Associated Depression… Resulting in Missed Appointments, Poorer Diet, Decreased Medication Adherence and Increased Complications.
To Address This Problem, The Intermountain Health System Incorporated a Mental Health Provider in Their Primary Care Clinics.
Results: Improved in Diabetes Care, Decreased Hospitalizations and Decreased ER Utilization.
Treating Mental Health Not Only Improves Mental Wellbeing, But Also Lowers Overall Healthcare Costs as Well.
Disclaimer: Dr. Bricker is the Chief Medical Officer of Virtual Care Company First Stop Health.
NOTE: If you or someone you know is considering suicide, please contact the National Suicide Prevention Lifeline at 1800-273-TALK (8255), text “help” to the Crisis Text Line at 741-741 or go to suicidepreventionlifeline.org.
Posted on July 10, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Dr. David Edward Marcinko is Speaking Up
Dr. David Edward Marcinko MBA CMP® enjoys personal coaching and public speaking and gives as many talks each year as possible, at a variety of medical society and financial services conferences around the country and world.
These have included lectures and visiting professorships at major academic centers, keynote lectures for hospitals, economic seminars and health systems, keynote lectures at city and statewide financial coalitions, and annual keynote lectures for a variety of internal yearly meetings.
His talks tend to be engaging, iconoclastic, and humorous. His most popular presentations include a diverse variety of topics and typically include those in all iMBA, Inc’s textbooks, handbooks, white-papers and most topics covered on this blog.
Posted on July 10, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
It’s official, Dr. David Marcinko, your advocacy is making a big impact!
Just Nominated
Congratulations on your 10th annual WEGO Health Awards nomination. Whether you’re a patient advocate, influencer or collaborator, we’re honored to recognize your contributions to the online health community.
We created the WEGO Health Awards as a way to celebrate and thank the patients and caregivers who support, educate, and inspire others. It’s now our 10th season and the patient leader community is stronger than ever. We could not be more proud to include you as a nominee.
You can expect to hear from us each week with updates and important announcements.
I recently learned from Bloomberg editor David Shipley that the American citizenship test wasn’t standardized until the 1950s, and before that aspiring citizens were quizzed on their understanding of American history by a judge. It was … pretty hard.
Here are several questions you might’ve been asked to become an American citizen in 1944. How would you do? Answers at the bottom of this post.
Which of the following states seceded during the Civil War? Florida, Maryland, Delaware, Kentucky*
Which of these cities has not been a capital of the US? NYC, Boston, Princeton, Philadelphia
Where must all bills intended to raise revenue originate? Popular referendum, the House, the Senate, the president
Which was not one of the original 13 colonies? South Carolina, Massachusetts, Georgia, Maine.
HAVE A GREAT MONDAY OFF
And, thank you if working today.
Citizenship test: 1) Florida seceded 2) Boston wasn’t a capital 3) Bills to raise revenue must originate in the House 4) Maine wasn’t an original colony
A “MEME” stock isn’t as easily defined as a growth or value stock, so to give it a definitive categorization would be inappropriate. Nor would actually categorizing it alongside growth and value stocks. They won’t be found in textbooks anytime soon, but to overlook their impact could potentially be an expensive oversight.
There are varying opinions on how much of your total income should go toward savings and retirement goals each month. Moreover, the answer is likely to vary, depending on your full financial profile.
But if you’re looking for some basic KISS guidelines, consider applying the 50-30-20 rule, a budgeting method that allocates 50% of your income to essentials, like rent and bills, 30% to discretionary spending and 20% to savings.
The housing market is HOT right now. Lumbar and wood is expensive. Inflation is emerging. So, owning a home can be very lucrative. Seriously, owning a home can not only give you a cheaper monthly payment than renting but in many cases, the tax benefits make the decision a no-brainer.
Here are a few of the larger deductions that you need to be sure to take:
Interest you pay on your mortgage: If you own a home and don’t have a mortgage greater than $750,000, you can deduct the interest you pay on the loan. This is one of the biggest benefits to owning a home versus renting–as you could get massive deductions at tax time. The limit used to be $1 million, but the Tax Cuts and Jobs Act of 2017 (TCJA) reduced the limit and made some clarifications on deducting interest from a home equity line of credit.
Property taxes: Another awesome benefit to owning a home is the ability to deduct your property taxes. Before TCJA, the rules were a little more flexible and you were able to deduct the entirety of your property taxes. Now things have a changed a bit. Under the new law, you can deduct up to $10,000. The deduction for state and local income taxes was combined with the deduction for state and local property taxes, too.
Tax incentives for energy-efficient upgrades: While most of the tax incentives for making energy-efficient upgrades to your home have gone away, there are still a couple worth noting. You can still claim tax deductions on solar energy–both for electric and water heating equipment, through 2021. The longer you wait, though, the less money you’ll get back. Here’s the percentage of equipment you can deduct, based on time of installation:
Between January 1, 2017, and December 31, 2019 – 30% of the expenditures are eligible for the credit Between January 1, 2020, and December 31, 2020 – 26% Between January 1, 2021, and December 31, 2021 – 22%
ASSESSMENT: But, is now the best time to buy a home? Your thoughts are appreciated.
Posted on June 20, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Management Strategies, Operational Techniques, Tools, Templates and Case Studies
Tex Book Review
Drawing on the expertise of decision-making professionals, leaders, and managers in health care organizations, Hospitals & Health Care Organizations: Management Strategies, Operational Techniques, Tools, Templates, and Case Studies addresses decreasing revenues, increasing costs, and growing consumer expectations in today’s increasingly competitive health care market.
Offering practical experience and applied operating vision, the authors integrate Lean managerial applications, and regulatory perspectives with real-world case studies, models, reports, charts, tables, diagrams, and sample contracts. The result is an integration of post PP-ACA market competition insight with Lean management and operational strategies vital to all health care administrators, comptrollers, and physician executives. The text is divided into three sections:
Managerial Fundamentals
Policy and Procedures
Strategies and Execution
Using an engaging style, the book is filled with authoritative guidance, practical health care–centered discussions, templates, checklists, and clinical examples to provide you with the tools to build a clinically efficient system. Its wide-ranging coverage includes hard-to-find topics such as hospital inventory management, capital formation, and revenue cycle enhancement. Health care leadership, governance, and compliance practices like OSHA, HIPAA, Sarbanes–Oxley, and emerging ACO model policies are included. Health 2.0 information technologies, EMRs, CPOEs, and social media collaboration are also covered, as are 5S, Six Sigma, and other logistical enhancing flow-through principles. The result is a must-have, “how-to” book for all industry participants.
Posted on June 18, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Medicare “Safe Harbor” Regulations
The Medicare Safe Harbor rules were passed in an effort to identify areas of practice that would not lead to a conviction under the anti-fraud statute. The Safe Harbor regulations provide for eleven areas where providers may practice without violating the anti-fraud statute.
Areas of safe practice under these regulations are briefly highlighted below:
Large Entity Investments – Investment in entities with assets over $50 million. The entity must be registered and traded on national exchanges.
Small Entity Investments – Small entity investment entities must abide by the 40-40 rule. No more than 40% of the investment interests may be held by investors in a position to make referrals. Additionally, no more than 40% of revenues can come through referrals by these investors.
Space and Equipment Rentals – Such lease agreements must be in writing and must be for at least a one year term. Furthermore, the terms must be at fair market value.
Personal Services and Management Contracts – These contracts are allowable as long as certain rules are followed. Like lease agreements, these personal service and management contracts must be in writing for at least a one-year term, and the services must be valued at fair market value.
Sale of a medical practice – There are restrictions if the selling practitioner is in a position to refer patients to the purchasing practitioner.
Referral services– Referral services (such as hospital referral services) are allowed. However, such referral services may not discriminate between practitioners who do or do not refer patients.
Warranties – There is certain requirements if any item of value is received under a warranty.
Discounts – Certain requirements must be met if a buyer receives a discount on the purchase of goods or services that are to be paid for by Medicare or Medicaid.
Payments to Bona Fide Employees – Payments made to bona fide employees do not constitute fraud under the Safe Harbor Regulations.
Group Purchasing Organizations – Organizations that purchase goods and services for a group of entities or individuals are allowed; provided certain requirements are met.
Waiver of Beneficiary Co-Insurance and Deductible – Routine waiver would not come under the safe harbor.
A physician’s actions that come under the Safe Harbor Regulations will not violate the Medicare Fraud and Abuse Statutes. However, the provider must still abide by the Stark amendments and must also abide by applicable state law.
Posted on June 17, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Dr. David E. Marcinko is at your Service
Dr. David Edward Marcinko MBA CMP® enjoys personal coaching and public speaking and gives as many talks each year as possible, at a variety of medical society and financial services conferences around the country and world.
These have included lectures and visiting professorships at major academic centers, keynote lectures for hospitals, economic seminars and health systems, keynote lectures at city and statewide financial coalitions, and annual keynote lectures for a variety of internal yearly meetings.
His talks tend to be engaging, iconoclastic, and humorous. His most popular presentations include a diverse variety of topics and typically include those in all iMBA, Inc’s textbooks, handbooks, white-papers and most topics covered on this blog.
Example 1: Dr. Kurt purchases an automobile for $15,000.
His hospital business use is 80% and he drives 20,000 total miles per year. Operating costs for the year, including gasoline, oil, insurance, maintenance, repairs, and license fees, are $4,000. If Kurt owns the car for five years, ownership will cost $35,000 ($4,000 x 5 = $20,000, $20,000 + $15,000 = $35,000), or $7,000 per year. For, each personal use mile costs $1.75 (100% -80% = 20%, 20% x 20,000 miles = 4,000 miles, $7,000/4,000 miles = $1.75). Kurt’s employer reimburses him 34.5 cents per mile for the business-related miles. As a result, the business use of the car is only partially reimbursed (16,000 business miles x 34.5 cents = $5,520).
However, the business usage costs Kurt $5,600(80% of $7,000). Kurt subsidizes the employer 9.25 cents per mile ($7,000 – $5,520 = $1,480, $1,480 /16,000 = 9.25 cents). Kurt’s total cost of ownership is $1.84 per mile, or $36,850 ($1.88 x 20,000 personal miles over the five-year life).
Example 2: Dr. Ben uses a hospital employer-provided vehicle 4,000 miles per year in 2003.
He reimburses the employer 34.5 cents per mile. His cost for five years is $6,900 (5y x 4,000 = 20,000 miles, 20,000 miles x 34.5 = $6,900).
Beginning on January 1st 2013, the standard mileage rates for the use of a car (also vans, pickups or panel trucks) were:
56.5 cents per mile for business miles driven
24 cents per mile driven for medical or moving purposes
14 cents per mile driven in service of charitable organizations
Note the dramatic contrast, from the employee’s perspective, between the above two examples, of the company reimbursing the employee for business use of his personal car, versus the employee reimbursing the company for personal use of the vehicle.
The business, medical, and moving expense rates decrease one-half cent from the 2013 rates. The charitable rate is based on statute.
Each generation of doctors and medical professionals is extraordinarily complex, bringing various skills, expertise and expectations to the modern medical work environment. Determining the best method to unite such diverse thinking is one of the many challenges faced by physician executives and healthcare leaders today.
And, as linguistic evolution occurs, the nomenclature of hospitalist was followed by that of intensivist, proceduralist and nocturnalist, etc [www.MedInnovationBlog.com and Personal communication Richard L. Reece MD].
Is it any wonder that many medical leaders and executive in the Baby Boomer generation find themselves at a loss? The days of functional leadership are gone and suddenly, no one cares about the expertise of the Baby Boomers or how they climbed the corporate ladder, in medicine or elsewhere. Leadership in the new era is no longer about command-control or dictating with intense focus on the bottom line; it is about collaboration, empowerment and communication. And, it is not about titles and nomenclature; it is about lifestyle choice.
What else drives these new-wave specialists?
The answer, of course, is the next-generation of physicians and their emerging new medical business and practice models, which include:
“Ambulists” are doctors that travel locally, have no, or only a sparse physical office presence of their own. They sporadically provide services that are additive to traditional practice models [i.e., endocrinologist in a large family medical office with many diabetics].
“In-Situ” physicians regularly provide services that are complimentary to existing traditional practice models [i.e., dentists or podiatrists in a medical practice].
“Laborists” are obstetricians that do not wish to be on-call. First begun in Cape Cod and other Massachusetts hospitals, such obstetricians work regular shifts for the sole purpose of delivering babies.
“Locum Tenens” doctors travel around the country as itinerants [i.e., cruise ships] as temporary substitutes for another the same specialty.
“Officists” remain in their own physical practice, and rarely see patients in the hospital, nursing home, patient home, out-patient facility, etc.
Finally, “dayhawk physicians” mimic the “nighthawk physician” model where radiologists in remote locations read films in the middle of the night as cash-strapped hospitals often find it cheaper to outsource with better services and more timely interpretations in many cases.
To start, let us all recall the Canadian physician Sir William Osler MD, one of the founders of Johns Hopkins Hospital in my hometown of Baltimore Maryland, and where I played stickball in the parking lot as a kid. He left a sizeable body of wisdom that has guided many physicians in the practice of medicine. So, allow me to share with you some of that accumulated wisdom and the quotes that have served me well over the years.
From Dr. Osler, I learned the art of putting myself in the patient’s shoes. “The motto of each of you as you undertake the examination and treatment of a case should be ‘put yourself in his place.’ Realize, so far as you can, the mental state of the patient, enter into his feelings.” Osler further stresses that we should “scan gently (the patient’s) faults” and offer the “kindly word, the cheerful greeting, the sympathetic look.”1
“In some of us, the ceaseless panorama of suffering tends to dull that fine edge of sympathy with which we started,” writes Osler in his famous essay “Aequanimitas.”2 “Against this benumbing influence, we physicians and nurses, the immediate agents of the Trust, have but one enduring corrective — the practice towards patients of the Golden Rule of Humanity as announced by Confucius: ‘What you do not like when done to yourself, do not do to others.’”
Medicine can be both art and science as many physicians have discovered. As Osler tells us, “Errors in judgment must occur in the practice of an art which consists largely of balancing probabilities.”2 Osler notes that “Medicine is a science of uncertainty and an art of probability” and also weighs in with the idea that “The practice of medicine is an art, based on science.”3,4
Osler emphasized that excellence in medicine is not an inheritance and is more fully realized with the seasoning of experience. “The art of the practice of medicine is to be learned only by experience,” says Osler. “Learn to see, learn to hear, learn to feel, learn to smell, and know that by practice alone can you become expert.”5
Finally, some timeless wisdom on patient care came from Osler in an address to St. Mary’s Hospital Medical School in London in 1907: “Gain the confidence of a patient and inspire him with hope, and the battle is half won.”6
***
***
Osler has also imparted plenty of advice on the business of medicine. In “Aequanimitas,” Osler says there are only two types of doctors: “those who practice with their brains, and those who practice with their tongues.”7
In a valedictory address to medical school graduates at McGill University, Osler suggested treating money as a side consideration in a medical career.8 “You have of course entered the profession of medicine with a view of obtaining a livelihood; but in dealing with your patients let this always be a secondary consideration.”
“You are in this profession as a calling, not as a business: as a calling which exacts from you at every turn self-sacrifice, devotion, love and tenderness to your fellow man,” explains Osler in the address to St. Mary’s Hospital Medical School.6 “Once you get down to a purely business level, your influence is gone and the true light of your life is dimmed. You must work in the missionary spirit, with a breadth of charity that raises you far above the petty jealousies of life.”
It is not easy for doctors to combine a passion for patient care, a knowledge of science and the maintenance of business, according to Osler in the British Medical Journal.9 “In the three great professions, the lawyer has to consider only his head and pocket, the parson the head and heart, while with us the head, heart, and pocket are all engaged.”
While some aspects of practice may fall short or be devoid of appropriate financial remuneration, the giving of one’s time, expertise and experience in improving patient outcomes and the quality of their lives may be the greatest gift. “The ‘good debts’ of practice, as I prefer to call them … amount to a generous sum by the end of each year,” says Osler.9
And so, as you practice medicine and reflect on your career, always remember the words and wisdom of Dr. William Osler, and keep patient welfare as your first priority.
References
1. Penfield W. Neurology in Canada and the Osler centennial. Can Med Assoc J. 1949; 61(1): 69-73
2. Osler W. Aequanimitas. Chapter 9, P. Blakiston’s Son and Co., Philadelphia, 1925, p. 159
3. Bean WB. William Osler: Aphorisms, CC Thomas, Springfield, IL, p. 129.
4. Osler W. Aequanimitas. Chapter 3, P. Blakiston’s Son and Co., Philadelphia, 1925, p. 34
5. Thayer WS. Osler the teacher. In: Osler and Other Papers. Johns Hopkins Press, Baltimore, 1931, p. 1.
6. Osler W. The reserves of life. St. Mary’s Hosp Gaz. 1907;13 (1):95-8.
7. Osler W. Aequanimitas. Chapter 7, P. Blakiston’s Son and Co., Philadelphia, 1925, p. 124
8. Osler W. Valedictory address to the graduates in medicine and surgery, McGill University. Can Med Surg J. 1874; 3:433-42.
9. Osler W. Remarks on organization in the profession. Brit Med J. 1911; 1(2614):237-9.
Posted on June 11, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
OVER HEARD IN THE DOCTOR’S LOUNGE
I currently have no fewer than 10 separate insurance policies associated with my plastic surgery practice. I understand very little about the policies other than that somebody at some point told me I needed each and every one of them, and each made sense when I bought it. But, I often wonder:
Am I over-insured and thus wasting money?
Am I under-insured and thus at risk for a liability disaster?
I never really had the means of answering these questions …. Until Now!
BOOK-VALUE: Cost of capital assets minus accumulated depreciation for a healthcare [corporation], or other organization.
The net asset value of a [healthcare] companies common stock. This is calculated by dividing the net tangible assets of the company (minus the par value of any preferred stock the company has) by the number of common shares outstanding.
****
PAR VALUE: For common stock, the value on the books of the corporation. It has little to do with market value or even the original price of shares at first issuance.
The difference between par and the price at first issuance is carried on the books of a corporation as “paid-in capital” or “capital surplus.”
Many folks feels that private preventative medical contracts may be one possible solution for those Americans going without healthcare; especially the young and healthy. Generally, and generically, they have a moniker like the “No Health Insurance Club”; or similar
Why?
Some pundits are leaning toward universal healthcare, or Medicare-4-All, which seems too socialized for others. Yet, private insurers continue to increase premiums, which prices healthcare out of reach for the average American. Employers can no longer float the cost of insurance so they pass it on to their employees. Patients aren’t the only ones being affected by the current state of healthcare. More and more doctors are going out of business and hospitals are cutting back due to escalating costs and payment defaults.
So, current remedies to this dilemma include major medical insurance policies for catastrophic events with high-deductibles to keep monthly premiums down, Medicaid, mini retail-clinics at grocery stores/pharmacies, and emergency room visits for common illnesses; as well as the PP-ACA.
Medical Maintenance
But, preventative healthcare and medical maintenance is not typically addressed. More than 90 percent of health related issues can be taken care of with preventative care and maintenance but only a small percentage of Americans currently enjoy the benefit of preventative healthcare. Healthcare economists are rethinking healthcare by offering an affordable alternative to traditional insurance options. NHICs, connect patients with participating board certified physicians that will treat and care for preventative healthcare needs for a one-time prepaid annual membership fee.
In this NHIC model:
Patients make a one-time annual payment that is typically less than a one-month premium with traditional insurance.
Patients receive up to 12 office visits per year that also include immunizations, $10 or less in-office prescriptions, and additional services including blood tests.
No deductible, no co-pays, no premiums.
No surprise bills to patients.
Viable alternative to COBRA for employees disengaged from work.
Low cost option for the self-employed.
The Doctors
What’s in it for the doctors? How about no insurance clerks, no need to snail mail medical insurance claims or use expensive electronic claims submission clearinghouse services, no bad debts or bad expense write-offs, no ARs; and fast cash.
ASSESSMENT: Your thoughts are comments are appreciated.
In 1987 the magazine Fast Company published an article authored by Tom Peters entitled “The Brand Called You.” Although some individuals may shy away from the concept of self-branding in actuality, many of the online social network sites such as Facebook become media by which we in fact brand ourselves.
In his article, Peter’s stated. “Regardless of position, regardless of the business we happen to be in, all of us need to understand the importance of branding. We are CEOs of their own companies: Me Inc. to be in business today, our most important job is to be head marketer for the brand called you.”
As a medical practitioner how do you differentiate yourself from others in your specialty and why should a new patient choose your practice above those of the others in the field?
Branding is about finding your big idea and building your identity and game plan around it. The bottom line: if you can’t explain who you are, and the value you bring to your practice in a short sentence or two, you have work to do.
According to Catherine Kaputa, a personal coach she suggests that there are the objective things: your credentials, the schools you went to, your years of experience, and your skill set, which represent what she refers to as hard power. Then there’s soft power: your image and reputation, your visibility in the community, your network of contacts, supporters and mentors. In today’s competitive marketplace, soft power plays a vital role in attracting people to you and your practice.
Standing Out
Peters suggests that everyone has a chance to stand out. Everyone has a chance to learn, improve, and build up their skills. Everyone has a chance to be a brand worthy of remark. Corporations spend millions of dollars creating and maintaining their distinct brand.
The Olympic Rings are representative of a brand which the International Olympic Committee guards zealously. Professional services firms such as McKinsey, foster self-branding among their employees. Major corporations have as employees those individuals who are smart, motivated and talented. Self-branding allows the employees to differentiate themselves from their peers. For one to engage in self-branding is first necessary to ask the question,
“What is it that my practice does that makes it different?”
You can begin by identifying the qualities or characteristics that make you distinctive from your competitors-or your colleagues.
What have you done lately-this week-to make yourself stand out? What would your colleagues say is your greatest and clearest strength?
What would they say is your most noteworthy personal trait? As a practitioner does your customer get dependable, reliable service that meets his or her strategic needs?
In addition, ask yourself: “what do I do that adds remarkable, measurable, distinguished distinctive value.”
Business Cards
While we are on the topic of mass media look at your business card and check to see if it has a distinctive logo on it. Keep in mind that packaging counts.
Getting and using power, intelligently, responsibly, and powerfully are essential skills for growing your brand. One of the things that attract us to certain brands is the power they project. Power, is largely a matter of perception. If you want people to see you as a powerful brand, act like a credible leader.
Another technique advocated by Peters is developing loyalty among your patients. In addition, you yourself need to be loyal to your colleagues, your staff, patients and to yourself.
Another way in which you can begin to promote yourself is, with a personal visibility campaign; getting yourself on a panel discussion with signing up to make a presentation at a workshop. If you are a medical writer, try writing about the corona pandemic, or contributing a column on a regular basis to your local newspaper. Community newspapers and professional newsletters are always seeking articles to fill the space. Not only does it give you the opportunity to express yourself it also is an excellent means to expose your practice and your capabilities to a mass audience.
ASSESSMENT: Your thoughts are comments are appreciated.
Charges of money laundering may seem foreign to the practice of medicine. The term “money laundering” evokes visions of a suitcase of drug cash being brought into a legitimate business and being transformed into that business’s receipts and later tunneled through legal channels.
In medicine the route beings with receipt of a claim payment check (i.e., a check as opposed to the drug dealer’s cash). The check is then deposited into the professional corporation’s checking account. The funds are then paid to the physician in the form of wages. Those wages are then deposited into the physician’s personal checking account.
Those funds and other similarly situated funds are then accumulated until a check is written to pay for a new automobile. The money received from the alleged fraudulent insurance claim has successful been “laundered” into a hard asset (e.g., Jaguar XJL-V8 4 door luxury sedan).
I am not a neurologist, psychologist, or psychiatrist. But, it is well known that emotional and behavioral change involves the human nervous system. And, there are two parts of the nervous system that are especially significant for holistic financial advisor; the first is the limbic system and the second is the autonomic nervous system.
According to Dr. C. George Boerre of Shippensburg University of Pennsylvania, this is known as the emotional nervous system.
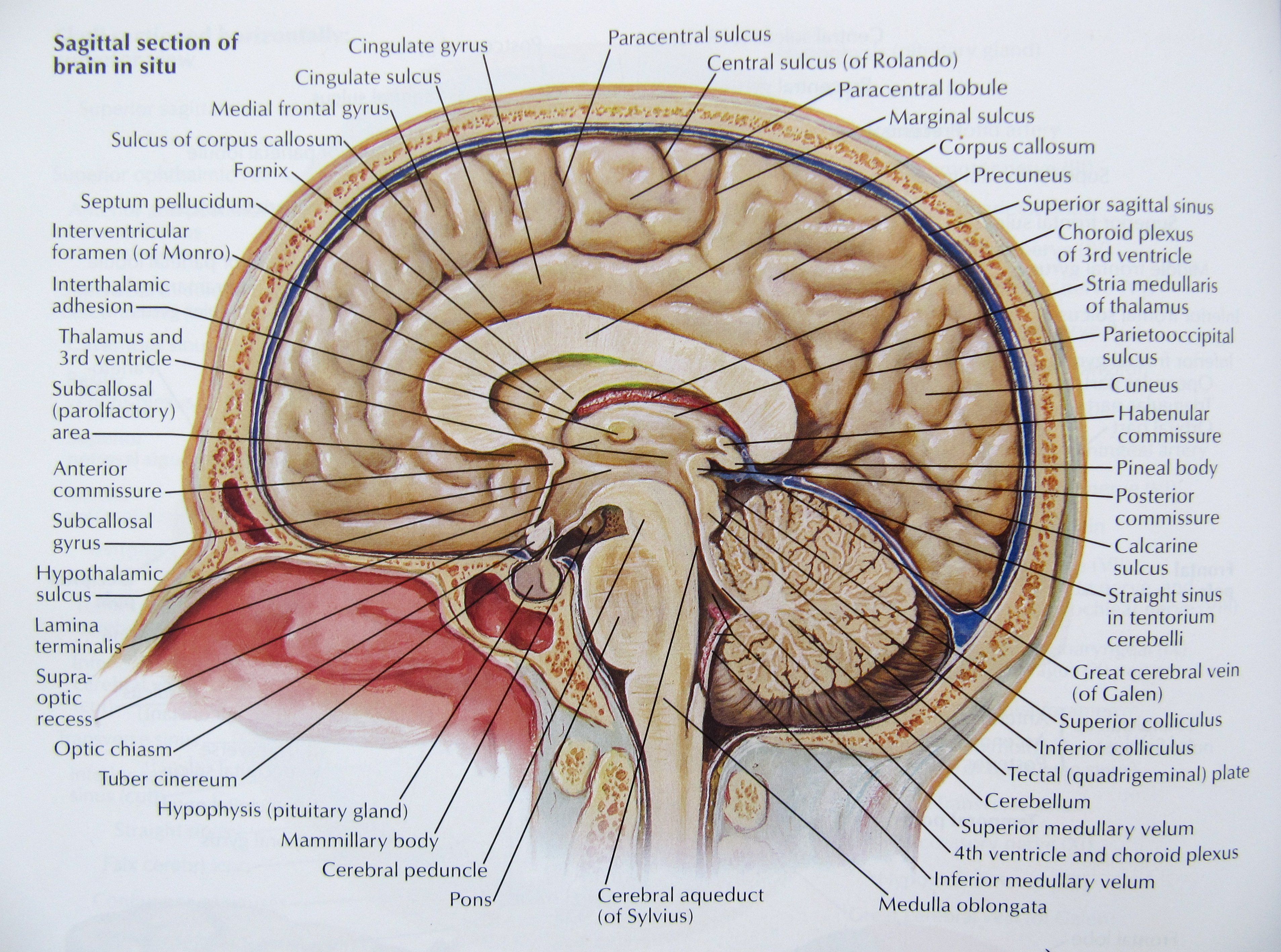
1. The Limbic System
The limbic system is a set of structures that lies on both sides of the thalamus, just under the cerebrum. It includes the hypothalamus, the hippocampus, the amygdala, and nearby areas. It is primarily responsible for emotions, memories and recollection.
Hypothalamus
The small hypothalamus is located just below the thalamus on both sides of the third ventricle (areas within the cerebrum filled with cerebrospinal fluid that connect to spinal fluid). It sits inside both tracts of the optic nerve, and just above the pituitary gland.
The hypothalamus is mainly concerned with homeostasis or the process of returning to some “set point.” It works like a thermostat: When the room gets too cold, the thermostat conveys that information to the furnace and turns it on. As the room warms up and the temperature rises, it sends turns off the furnace. The hypothalamus is responsible for regulating hunger, thirst, response to pain, levels of pleasure, sexual satisfaction, anger and aggressive behavior, and more. It also regulates the functioning of the autonomic nervous system, which means it regulates functions like pulse, blood pressure, breathing, and arousal in response to emotional circumstances. In a recent discovery, the protein leptin is released by fat cells with over-eating. The hypothalamus senses leptin levels in the bloodstream and responds by decreasing appetite. So, it seems that some people might have a gene mutation which produces leptin, and can’t tell the hypothalamus that it is satiated. The hypothalamus sends instructions to the rest of the body in two ways. The first is to the autonomic nervous system. This allows the hypothalamus to have ultimate control of things like blood pressure, heart rate, breathing, digestion, sweating, and all the sympathetic and parasympathetic functions.
The second way the hypothalamus controls things is via the pituitary gland. It is neurally and chemically connected to the pituitary, which in turn pumps hormones called releasing factors into the bloodstream. The pituitary is the so-called “master gland” as these hormones are vitally important in regulating growth and metabolism.
Hippocampus
The hippocampus consists of two “horns” that curve back from the amygdala. It is important in converting things “in your mind” at the moment (short-term memory) into things that are remembered for the long run (long-term memory). If the hippocampus is damaged, a patient cannot build new memories and lives in a strange world where everything they experience just fades away; even while older memories from the time before the damage are untouched! Most patients who suffer from this kind of brain damage are eventually institutionalized.
Amygdala
The amygdalas are two almond-shaped masses of neurons on either side of the thalamus at the lower end of the hippocampus. When it is stimulated electrically, animals respond with aggression. And, if the amygdala is removed, animals get very tame and no longer respond to anger that would have caused rage before. The animals also become indifferent to stimuli that would have otherwise have caused fear and sexual responses.
Related Anatomic Areas
Besides the hypothalamus, hippocampus, and amygdala, there are other areas in the structures near to the limbic system that are intimately connected to it:
The cingulate gyrus is the part of the cerebrum that lies closest to the limbic system, just above the corpus collosum. It provides a pathway from the thalamus to the hippocampus, is responsible for focusing attention on emotionally significant events, and for associating memories to smells and to pain.
The ventral tegmental area of the brain stem (just below the thalamus) consists of dopamine pathways responsible for pleasure. People with damage here tend to have difficulty getting pleasure in life, and often turn to alcohol, drugs, sweets, and gambling.
The basal ganglia (including the caudate nucleus, the putamen, the globus pallidus, and the substantia nigra) lie over to the sides of the limbic system, and are connected with the cortex above them. They are responsible for repetitive behaviors, reward experiences, and focusing attention.
The prefrontal cortex, which is the part of the frontal lobe which lies in front of the motor area, is also closely linked to the limbic system. Besides apparently being involved in thinking about the future, making plans, and taking action, it also appears to be involved in the same dopamine pathways as the ventral tegmental area, and plays a part in pleasure and addiction.
2. The Autonomic Nervous System
The second part of the nervous system to have a particularly powerful part to play in our emotional life is the autonomic nervous system.
The autonomic nervous system is composed of two parts, which function primarily in opposition to each other. The first is the sympathetic nervous system, which starts in the spinal cord and travels to a variety of areas of the body. Its function appears to be preparing the body for the kinds of vigorous activities associated with “fight or flight,” that is, with running from danger or with preparing for violence. Activation of the sympathetic nervous system has the following effects:
dilates the pupils and opens the eyelids,
stimulates the sweat glands and dilates the blood vessels in large muscles,
constricts the blood vessels in the rest of the body,
increases the heart rate and opens up the bronchial tubes of the lungs, and
inhibits the secretions in the digestive system.
One of its most important effects is causing the adrenal glands (which sit on top of the kidneys) to release epinephrine (adrenalin) into the blood stream. Epinephrine is a powerful hormone that causes various parts of the body to respond in much the same way as the sympathetic nervous system. Being in the blood stream, it takes a bit longer to stop its effects, and may take some time to calm down again
The sympathetic nervous system also takes in information, mostly concerning pain from internal organs. Because the nerves that carry information about organ pain often travel along the same paths that carry information about pain from more surface areas of the body, the information sometimes get confused. This is called referred pain, and the best known example is the pain in the left shoulder and arm when having a heart attack.
The other part of the autonomic nervous system is called the parasympathetic nervoussystem. It has its roots in the brainstem and in the spinal cord of the lower back. Its function is to bring the body back from the emergency status that the sympathetic nervous system puts it into.
Some of the details of parasympathetic arousal include some of the following:.
pupil constriction and activation of the salivary glands,
stimulating the secretions of the stomach and activity of the intestines,
stimulating secretions in the lungs and constricting the bronchial tubes, and;
decreases heart rate.
The parasympathetic nervous system also has some sensory abilities: It receives information about blood pressure, levels of carbon dioxide in the blood, etc.
There is actually another part of the autonomic nervous system that is not mentioned too often: the enteric nervous system. It is a complex of nerves that regulate the activity of the stomach.
For example, if you get sick to your stomach with a new financial advisory client – or feel nervous butterflies with your first patient encounter as a doctor- you can blame the enteric nervous system.
Today, whether independent or employed, physicians can pursue several creative compensation models, other than fee-for service reimbursement based on Current Procedural Terminology [CPT®] codes, not popular a few decade ago:
Pay-for-Performance Initiatives [P4P]: According to Mark Fendrick, MD and Michael E. Chernew, PhD, instead of the one size fits all approach of traditional health insurance, a “clinically-sensitive” cost-sharing system that supports co-payments related to evidence-based value for targeted patients is emerging. In 2014, for example, there were a number of changes to Medicare’s pay-for-performance programs [personal communication]. These value-based payment modifiers will show up in physicians’ paychecks in few years, and will be expanded to practices with 10 or more eligible professionals. The program, mandated by the Affordable Care Act, assesses a provider’s quality of care and costs, and increases Medicare payments for good performers and decreases them for bad ones. And, doctor performance will be reflected in adjustments to 2016 payments. As much as 2% of Medicare payments will be at risk in 2021 based on physician performance in 2019. It was only 1% for 2015, which was based on doctors’ 2013 performance.
Physician Quality Reporting Initiative Model. The Centers for Medicare and Medicaid Services [CMS] paid out more than $40 million in monetary incentives to medical providers who reported data on quality of care delivered between July 2020 and December 2020; as part of its PQRI. Under the PQRI, healthcare providers who participated received bonuses of 1.5 percent of their total CMS payments during the reporting period.
Direct Reimbursement Payment Model: A Health Reimbursement Arrangement (HRA) is a tool which is used to provide direct reimbursement by an employer for qualified medical expenses. The HRA is an employer-established benefit plan, and contributions to the plan may only be made by the employer. The HRA can be used in conjunction with any insurance plan, including a high-deductible plan. Qualified reimbursements made under the HRA are tax-deductible for the employer, and the payments are not counted as income for the employee. Any balance in an HRA can generally be carried over to the next year. This plan allows for flexibility and tailored to meet the particular needs of both employers and employees in a tax-advantaged manner. From the physician’s perspective, increasing use of HRAs poses new challenges. Payment for services in the medical office may be required of the patient/employee before reimbursement from the employer occurs. These extra steps can easily result in delayed payment or non-payment to medical providers who are not prepared to work with this model of reimbursement. The provisions for this model are outlined in IRS publication 969, http://www.irs.gov/pub/irs-pdf/p969.pdf.
Concierge Practice Model: The concept of concierge medicine (CM), also known as retainer medicine, first emerged in Seattle, Washington in the 1990’s. With CM, the physician charges an annual retainer fee to patients. The fee usually ranges from $1,000 to $20,000 per year, and the number of patients in a practice is usually limited to a few hundred. In return, patients receive increased levels of access and personalized care. This often includes same day appointments, extended visit times, house calls, and 24/7 access to the physician by pager and cell phone. An annual executive physical is often included, as well as an increased emphasis on preventive care. Many physicians choosing this type of practice model do so for lifestyle and control reasons, although the average income for a successful CM primary care physician is higher than that of a typical primary care physician. .
Global Healthcare Model: American businesses are extending their cost-cutting initiatives to include offshore employee medical benefits, and facilities like the Bumrungrad Hospital in Bangkok, Thailand (cosmetic surgery), the Apollo Hospital in New Delhi, India (cardiac and orthopedic surgery) are premier examples for surgical care. Both are internationally recognized institutions that resemble five-star hotels equipped with the latest medical technology. Countries such as Finland, England and Canada are also catering to the English-speaking crowd, while dentistry is especially popular in Mexico and Costa Rica. Although this is still considered “medical tourism,” Mercer Health and Benefits was recently retained by three Fortune 500 companies interested in contracting with offshore hospitals and The Joint Commission [TJC] has accredited 88 foreign hospitals through a joint international commission. To be sure, when India can discount costs up to 80%, the effects on domestic hospital reimbursement and physician compensation may be assumed to increase downward compensation pressures.
Locum Tenens Practitioner Model: Locum Tenens (LT) as an alternative to full-time employment is enjoying a comeback for most specialties. Some younger physicians enjoy the travel, while mature physicians like to practice at their leisure. Employment factors to consider include: firm reputation, malpractice insurance, credentialing, travel and relocation expenses (which are negotiable). However, a LT firm typically will not cover taxes [NALTO.org and http://www.studentdoc.com/locum-tenens.html%5D
1) If you are job hunting, you should send your resume to recruiters
Different recruiters know about different positions. They do not usually know about the same ones. This is particularly true with retained firms. By sending your resume out widely, you will be placed in many different confidential databases and be alerted of many different positions. If you send your resume to only a few, it may be that none you send to will be working with positions which are suited for you. Throw your net widely.
If you change jobs, it is also wise to send follow-up letters to the recruiters and alert them of your new career move. Many search firms follow people throughout their careers and enjoy being kept up-to-date. It is a good idea to have your resume formatted in plain text so you can copy and paste it into email messages when requested to do so. Then, follow up with a nicely formatted copy on paper by postal mail.
Some estimate that only 1% to 3% of all resumes sent will result in actual job interviews. So, if you only send 50 resumes, you may only have less than 2 interviews, if that many. Send your resume to as many recruiters as you can. It is worth the postage or email time. Generally, recruiters will not share your resume with any employer or give your name to anyone else without obtaining your specific permission to do so. The recruiter will call first, talk to you about a particular position and then ask your permission to share your resume with that employer.
2) Your resume will be kept strictly confidential by the executive search firm.
It is safe to submit your resume to a search firm and not worry that the search firm will let it leak out that you are job hunting. Recruiters will call you each and every time they wish to present you to an employer in order to gain your permission. Only after they have gained your permission will they submit your name or resume to the identified employer. The wonderful aspect of working with search firms is that you can manage your career and your job search in confidence and privacy.
3) Fees are always paid by the employer, not the job candidate.
Recruiters and search firms work for the employer or hiring entity. The employer pays them a fee for locating the right physician for the job opening. This is important to remember, in that when you interact with executive recruiters, you are essentially interacting with an agent or representative of the employer. Recruiters are more loyal to employers than they are to job candidates because they work for the employer. This should not present a problem, but, should cause you to develop your relationship with the recruiter with the same integrity and professionalism that you would with the employer.
Recruiters are paid fees in one of two ways – retainer fees or contingency fees. This is an important distinction and will affect your process with both the employer and the recruiter. Some employers prefer working with contingency firms and some with retained firms. Both are respected by employers and useful in your job search, but, the two types of firms will not be handling the same positions with the same employers simultaneously.
A “retained recruiter” has entered an exclusive contract with an employer to fill a particular position. The retained recruiter, then, is likely to advertise a position, sharing the specifics of the position, location and employer openly. The retained firm feels a great obligation to fulfill the contract by finding the best person for the job.
A “contingency recruiter” on the other hand, usually does not have an exclusive relationship with the employer, and is only paid a fee if the job search is successful. Often, if the employer uses contingency firms, there will be more than one contingency firm competing to fill a certain position. As a job hunter, if you are sent to an interview by a contingency firm, you may find that you are competing with a larger number of applicants for a position. Generally, retained firms only send in from 3 to 5 candidates for a position.
Recruiters will be paid fees equal to about 25% to 35% of the resulting salary of the successful candidate plus expenses. This does not come out of the job candidate’s salary. This is paid to the recruiter through a separate relationship between the employer and the search firm. This may seem like a large fee, but, keep in mind that recruiters incur a great many expenses when searching for successful job candidates. They spend enormous amounts of money on computer systems, long distance calls, mail-outs, travel and interviews. Recruiters work very hard for these fees. Employers recognize the value of using recruiters and are more than willing to pay recruiters the fees. All you have to do is contact the recruiter to get the process moving.
4) Not all medical recruiters work only with physicians.
Some search firms work exclusively with physicians or in healthcare, while others may work in several fields at once. Some of the larger generalist firms will have one or more search consultants that specialize in healthcare. It is important for you, as a job hunter, to assess the recruiters’ knowledge of your field. If you use industry or medical specialty buzz words in describing your skills, experience or career aspirations, you may or may not be talking a language the recruiter understands fully. It is wise to explore fully with the recruiter his understanding of your field and area of specialization.
5) Recruiters and search consultants move around.
Recruiters, like many professionals, move to new firms during their careers. Often you will find that recruiters will work at several firms during their careers. Since it is much more effective to address your letters to a person rather than “to whom it may concern”, it is smart for job hunters to have accurate and up-to-date information about who is who and where, since this can change frequently. Search firms also move their offices, sometimes to another suite, street or state. If you have a list of recruiters that is over one year old, you will certainly waste some postage in mailing your resumes and cover letters. Many of your mail-outs will be returned to you stamped “non-deliverable”, unless you obtain an up-to-date list. A resource, like the Directory of Healthcare Recruiters is updated very frequently, usually monthly [www.pohly.com/dir3.html].
6) Most search firms work with positions all over the country.
If you are from a particular state, and want to remain in that state, don’t make the mistake of only sending your resume to recruiters in your state. Often the recruiters in your state are working on positions in other states, and recruiters in other states are working on positions in your state. This is usually the case. Very few recruiters work only in their local area, most work all around the US and some internationally. Regardless of your geographic preference, you should still send your resume to all the healthcare recruiters. If you really only want to remain in your area, you can specify that preference in your cover letter.
7) Recruiters primarily work with hard to fill positions or executive positions.
Some recruiters specialize in clinical positions for physicians, managed care executive positions, healthcare financial positions or health administration positions. Others may specialize in finding doctors, nurses or physical therapists. Generally, an employer does not engage a recruiter’s assistance in filling a position unless it is hard to fill. Sometimes employers will engage search firms to save them the valuable time of advertising or combing through dozens of resumes.
ASSESSMENT
Contingency recruiters tend to work with more mid-level management and professional positions, but, this is not always the case. Retained firms generally work with the higher level clinical or administrative positions.
One thing you will be assured of is that if a recruiter is working on a position that means that the employer is willing to pay a fee. That usually means that the position is a valued position and one worth closer inspection on your part. Even in healthcare, with certain exceptions, our economy is an “employer’s market”. This means that employers receive a deluge of resumes for their open positions. Increasingly, employers are using recruitment firms to handle their openings and schedule the interviews because employers simply do not have the manpower or time to handle the many resumes they receive.
Therefore, if a job hunter is submitted by a recruiter, that job hunter has a great advantage over all other applicants.
Posted on May 16, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
EDITOR’S POINT OF PRIVILEGE
This week, for the first time in a year, I took a walk without wearing a mask. It was all going great until I saw a woman walking her dog approach me. She was wearing a mask, and my body instinctively moved to cross the street to give her space. It made me realize that we’ve been living in fear of other humans, which is pretty sad.
Pandemic-era habits die hard, but I’m confident we can once again re-wire our brains to view other people not as biological vectors for disease, but as … people, just with germs.
So, here’s to hoping this summer, we’ll learn to come together as quickly as we learned to distance.
Posted on May 11, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
DOCTOR OF OSTEOPATHIC MEDICINE
By Dr. David Edward Marcinko MBA CMP®
[Editor-in-Chief]
OK; I admit it. I have a formal educational background in allopathic, podiatric and osteopathic medicine. I also have both earned and conferred medical degrees from the States as well as Europe. I even dropped out of dental and law school back in the day … Such the protean dilettante!
Now, today there are about 950,000 allopathic physicians, 20,000 podiatrists, 150,000 dentists and 50,000 osteopaths. And, from this cohort of medical professionals, the Doctor of Osteopathic Medicine [DO] seems to be the least well understood practitioner.
And so, I thought this essay from Very Well Health might be helpful to all our Medical Executive-Post readers and subscribers [Differences Between a DO Physician and an MD – Comparing Osteopathic and Allopathic Medical Training].
Book Speaker Dr. David E. Marcinko CMP® MBA for your Next Medical, Pharma, Hospital, University or Financial Services Seminar or Personal and Corporate Coaching Sessions
Dr. David Edward Marcinko, editor-in-chief, is a next-generation apostle of Nobel Laureate Kenneth Joseph Arrow PhD, as a health-care economist, insurance advisor, financial advisor, risk manager, and board-certified surgeon from Temple University in Philadelphia.
In the past, he edited eight practice-management books, three medical textbooks and manuals in four languages, five financial planning yearbooks, dozens of interactive CD-ROMs, and three comprehensive health-care administration dictionaries.
Internationally recognized for his clinical work, he is a past endowed chair; professor of health economics, finance and public health policy management; and distinguished visiting professor of surgery as a Bachelor of Medicine–Bachelor of Surgery (MBBS) degree recipient from Marien Hospital in Aachen, Germany.
He provides litigation support and expert witness testimony in state and federal court, with medical publications archived in the Library of Congress and the Library of Medicine at the National Institutes of Health.
Posted on July 26, 2020 by Dr. David Edward Marcinko MBA MEd CMP™
WHAT IS “ANOSMIA”
By Darrell Pruitt DDS and David E. Marcinko MBBS, MBA
Anosmia, also known as smell blindness, is the loss of the ability to detect one or more smells. Anosmia may be temporary or permanent. It differs from Hyposmia which is a decreased sensitivity to some or all smells.
According to Wikipedia, Anosmia can be due to a number of factors, including an inflammation of the nasal mucosa, blockage of nasal passages or a destruction of one temporal lobe. Inflammation is due to chronic mucosa changes in the lining of the paranasal sinus and in the middle and superior turbinates. When anosmia is caused by inflammatory changes in the nasal passageways, it is treated simply by reducing inflammation. It can be caused by chronic meningitis and neurosyphilis that would increase intracranial pressure over a long period of time, and in some cases by ciliopathy, including ciliopathy due to primary ciliary dyskinesia. The term derives from the New Latin anosmia, based on Ancient Greek ἀν- (an-) + ὀσμή (osmḗ, “smell”; another related term, hyperosmia, refers to an increased ability to smell). Some people may be anosmic for one particular odor, a condition known as “specific anosmia”. The absence of the sense of smell from birth is known as congenital anosmia.
Ageusia is the loss of taste functions of the tongue, particularly the inability to detect sweetness, sourness, bitterness, saltiness, and umami. It is sometimes confused with anosmia – a loss of the sense of smell. Because the tongue can only indicate texture and differentiate between sweet, sour, bitter, salty, and umami, most of what is perceived as the sense of taste is actually derived from smell. True Ageusia is relatively rare compared to Hypogeusia – a partial loss of taste – and Dysgeusia – a distortion or alteration of taste.
ASSESSMENT:
If you should suddenly lose your sense of smell (anosmia), you might want to get tested for COVID-19 – even without the presence of other symptoms.
“A majority of COVID-19 patients experience some level of anosmia, most often temporary. Analyses of electronic health records indicate that COVID-19 patients are 27 times more likely to have smell loss but are only around 2.2 to 2.6 times more likely to have fever, cough or respiratory difficulty, compared to patients without COVID-19.”
See: “How COVID-19 Causes Loss of Smell – Olfactory support cells, not neurons, are vulnerable to novel coronavirus infection.” By Kevin Jiang for Harvard Medical School, July 24, 2020.











































:max_bytes(150000):strip_icc():format(webp)/the-50-30-20-rule-of-thumb-453922-final-5b61ec23c9e77c007be919e1-5ecfc51b09864e289b0ee3fa0d52422f.png)