

Stages of COVID-19 Vaccine Development in Humans
By staff reporters
***

***
Share this:

Filed under: iMBA, Inc. | Tagged: COVID-19 Vaccine Development | Leave a comment »
ME-P SYNDICATIONS:
WSJ.com,
CNN.com,
Forbes.com,
WashingtonPost.com,
BusinessWeek.com,
USNews.com, Reuters.com,
TimeWarnerCable.com,
e-How.com,
News Alloy.com,
and Congress.org

![]()
![]()



BOARD CERTIFICATION EXAM STUDY GUIDES
Lower Extremity Trauma
[Click on Image to Enlarge]
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] E-mail: MarcinkoAdvisors1738@outlook.com
![]()


 ePodiatryConsentForms.com
ePodiatryConsentForms.com
 “Providing Management, Financial and Business Solutions for Modernity”
“Providing Management, Financial and Business Solutions for Modernity”


Stages of COVID-19 Vaccine Development in Humans
By staff reporters
***
***
Filed under: iMBA, Inc. | Tagged: COVID-19 Vaccine Development | Leave a comment »
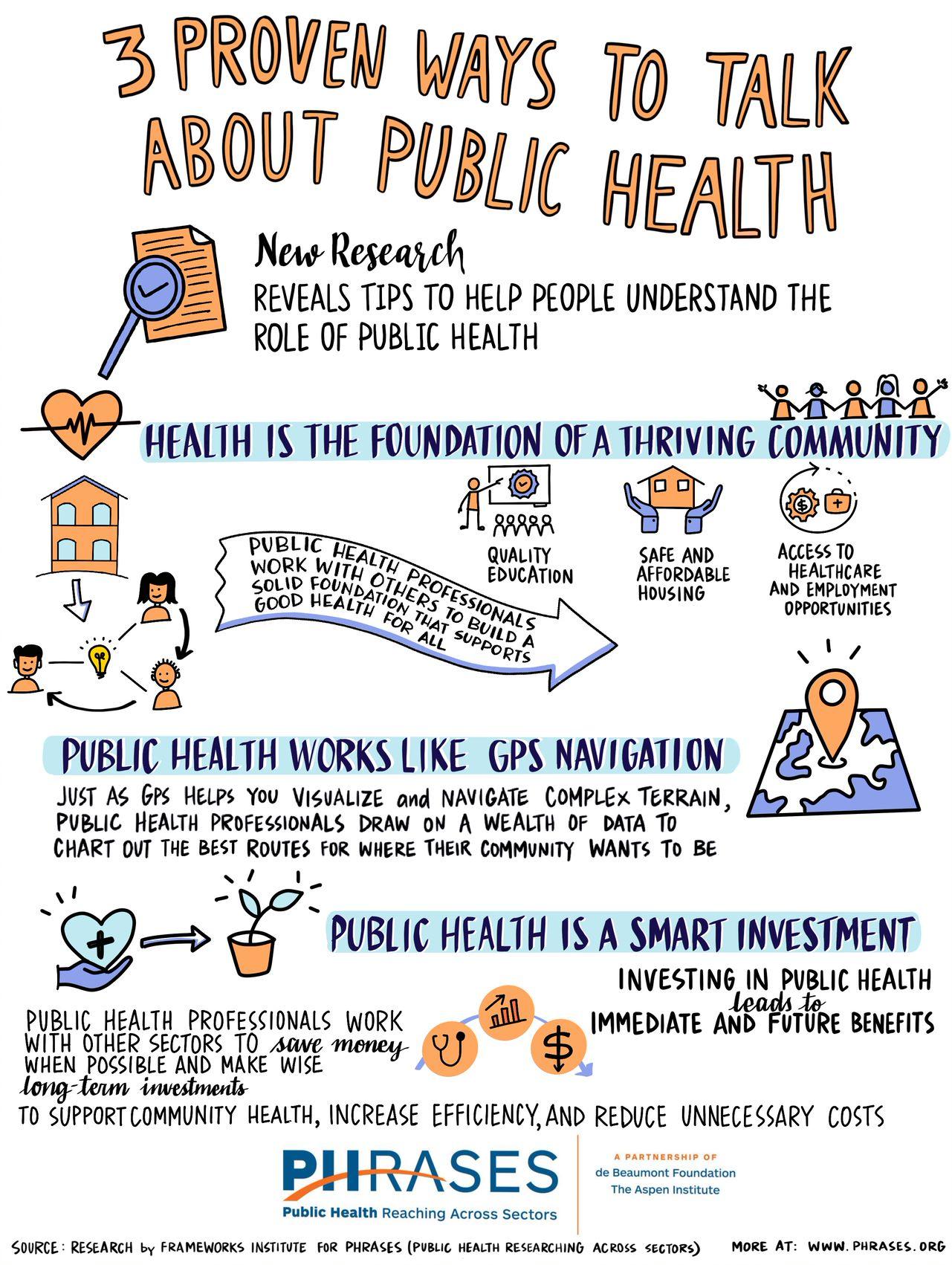
Three Ways to Discuss
By staff reporters
***
THANK YOU
***
Filed under: Health Insurance, Health Law & Policy, iMBA, Inc. | Tagged: public health | Leave a comment »
By staff reporters
***
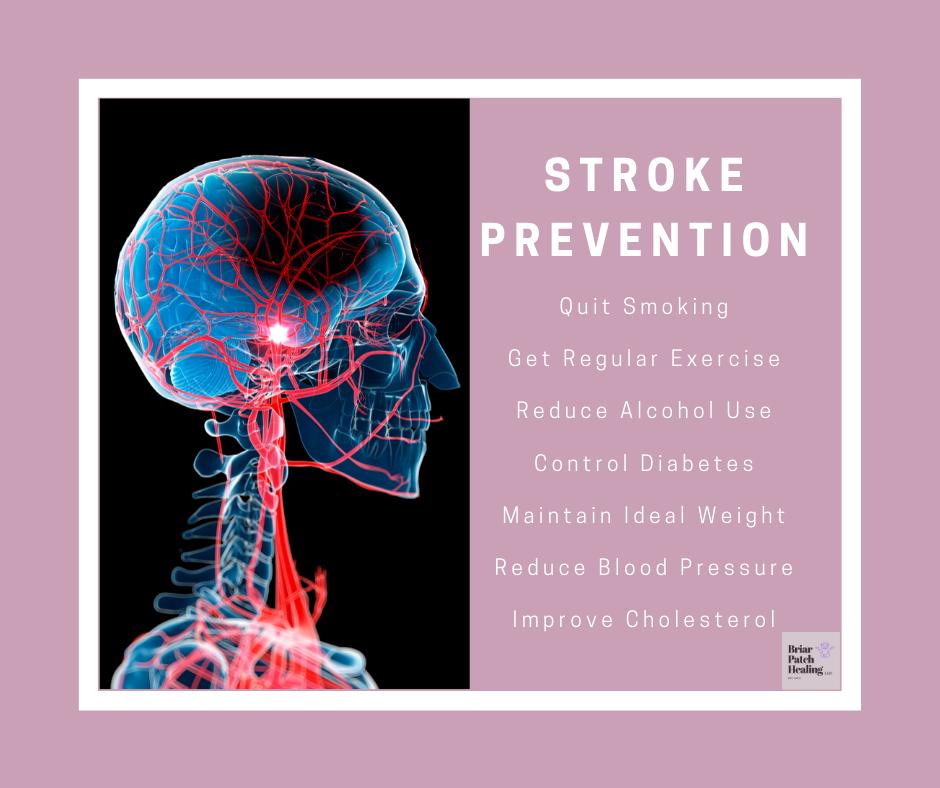
MORE: https://medicalexecutivepost.com/2020/04/13/stroke-cva/
***
“Medical Management and Health Economics Education for Financial Advisors”
CMP® CURRICULUM: https://lnkd.in/eDTRHex
CMP® WEB SITE: https://lnkd.in/guWSApq
Your thoughts and comments are appreciated.
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
THANK YOU
***
Filed under: iMBA, Inc., LifeStyle | Tagged: CVA, stroke | Leave a comment »
WHAT IS “ANOSMIA”

By Darrell Pruitt DDS and David E. Marcinko MBBS, MBA
Anosmia, also known as smell blindness, is the loss of the ability to detect one or more smells. Anosmia may be temporary or permanent. It differs from Hyposmia which is a decreased sensitivity to some or all smells.
According to Wikipedia, Anosmia can be due to a number of factors, including an inflammation of the nasal mucosa, blockage of nasal passages or a destruction of one temporal lobe. Inflammation is due to chronic mucosa changes in the lining of the paranasal sinus and in the middle and superior turbinates. When anosmia is caused by inflammatory changes in the nasal passageways, it is treated simply by reducing inflammation. It can be caused by chronic meningitis and neurosyphilis that would increase intracranial pressure over a long period of time, and in some cases by ciliopathy, including ciliopathy due to primary ciliary dyskinesia. The term derives from the New Latin anosmia, based on Ancient Greek ἀν- (an-) + ὀσμή (osmḗ, “smell”; another related term, hyperosmia, refers to an increased ability to smell). Some people may be anosmic for one particular odor, a condition known as “specific anosmia”. The absence of the sense of smell from birth is known as congenital anosmia.
Ageusia is the loss of taste functions of the tongue, particularly the inability to detect sweetness, sourness, bitterness, saltiness, and umami. It is sometimes confused with anosmia – a loss of the sense of smell. Because the tongue can only indicate texture and differentiate between sweet, sour, bitter, salty, and umami, most of what is perceived as the sense of taste is actually derived from smell. True Ageusia is relatively rare compared to Hypogeusia – a partial loss of taste – and Dysgeusia – a distortion or alteration of taste.
ASSESSMENT:
If you should suddenly lose your sense of smell (anosmia), you might want to get tested for COVID-19 – even without the presence of other symptoms.
“A majority of COVID-19 patients experience some level of anosmia, most often temporary. Analyses of electronic health records indicate that COVID-19 patients are 27 times more likely to have smell loss but are only around 2.2 to 2.6 times more likely to have fever, cough or respiratory difficulty, compared to patients without COVID-19.”
See: “How COVID-19 Causes Loss of Smell – Olfactory support cells, not neurons, are vulnerable to novel coronavirus infection.” By Kevin Jiang for Harvard Medical School, July 24, 2020.
https://hms.harvard.edu/news/how-covid-19-causes-loss-smell

Your thoughts and comments are appreciated.
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
THANK YOU
***
Filed under: Glossary Terms, Health Insurance, iMBA, Inc., Pruitt's Platform, Touring with Marcinko | Tagged: AGEUSIA, ANOSMIA, corona, Corvid-19, D. Kellus Pruitt DDS, David Edward Marcinko, DYSGEUSIA, HYPERSOMIA, HYPOGEUSIA, pandemic | Leave a comment »
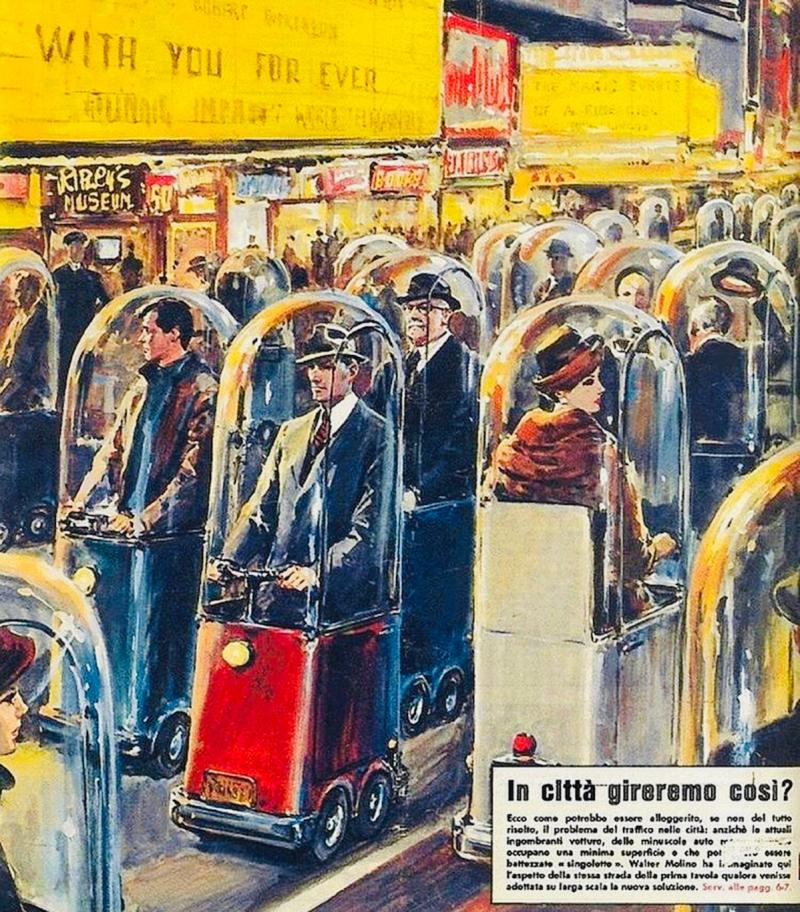
BACK TO THE FUTURE
By Anonymous
***
***
Filed under: iMBA, Inc., LifeStyle | Tagged: Corona Virus Human Bubbles, Covid-19, pandemic | Leave a comment »
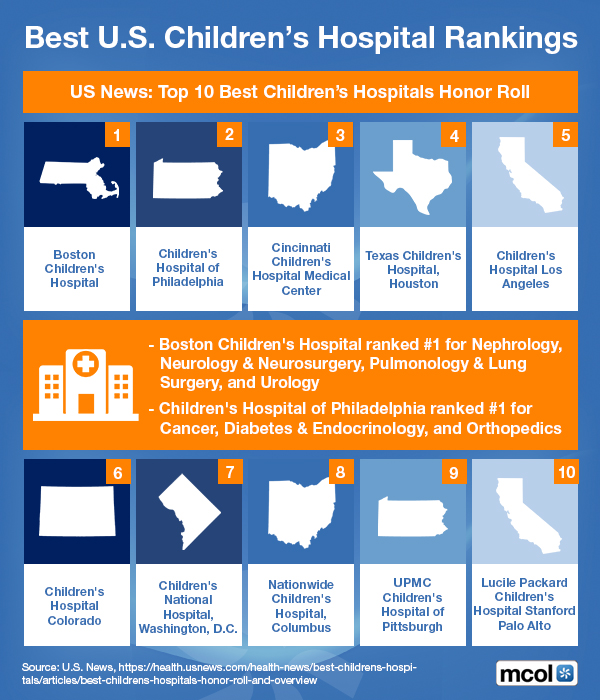
Top 10 [Ten] Rankings
***
***
Filed under: iMBA, Inc. | Tagged: U.S Children's Hospitals | Leave a comment »
RE-EMERGING PANDEMIC INDUCED MENTAL DISORDERS?
Courtesy: www.CertifiedMedicalPlanner.org
More than a decade ago, our firm commenced studying and crafting an exclusive report on medical professionals and their investing compulsions. It was headed by one of the nation’s leading psychologists, gambling addiction and trauma specialists; and personal friend.
Colleague Eugene Schmuckler; PhD, MBA, M.Ed CTS® is from Georgia State University.
***
***
“Medical Management and Health Economics Education for Financial Advisors”
CMP® CURRICULUM: https://lnkd.in/eDTRHex
CMP® WEB SITE: https://lnkd.in/guWSApq
Assessment: Your thoughts and comments on the Working-White-Paper are appreciated.
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
THANK YOU
***
Filed under: CMP Program, iMBA, Inc., Investing | Tagged: Eugene Schmuckler PhD, Internet addiction | 1 Comment »
| AJPH | |||||||||
|
Filed under: Health Economics, Health Insurance, iMBA, Inc., Practice Management, Quality Initiatives | Tagged: AJPH, American Journal Public Health | Leave a comment »
Courtesy: www.CertifiedMedicalPlanner.org
![]()
[On Finding Physician-Focused Financial Advice]
“The financial planner is a like juggler, trying to keep a variety of balls simultaneously in the air. Each aspect of practice becomes critical, just as action is needed.
Some of the activities of operating a successful financial planning practice generally attract more attention than others, such as marketing and advertising, closing engagements, and office administration. Because product review, selection and implementation are often related to advisor compensation, they attract a great deal of the financial juggler’s concentration.
But, the heart of financial planning, niche advice, often receives little attention. Not because it is unimportant, it just doesn’t seem immediately and predictably urgent. Here, that ball does not seem to be dropping so rapidly.
However, retaining clients and receiving referrals from other professionals is very dependent on the quality of the advice delivered. And, the first line of protection from practitioner liability exposure is to not deliver incorrect or incomplete advice.
But, where does the financial advisor turn for ideas and organized research in the healthcare sector?”
Edwin P. Morrow; CFPTM, CLU, ChFC, RFC
[Middletown, Ohio, USA]
Your thoughts are appreciated.
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
THANK YOU
 8
8
***
Filed under: Book Reviews, Experts Invited, iMBA, Inc., Investing | Tagged: Edwin P. Morrow; CFPT, Financial Planning | Leave a comment »
FOR DOCTORS AND PATIENTS, ALIKE

By Dr. David E. Marcinko MBA
Doctor Scheduling Issues
Nothing creates more distress for a new medical practice administrator than “holes”, or empty slots, in a physician’s appointment schedule. While doctors may complain about too much work and not enough time with patients, a corollary is the lack of production that accompanies such downtime.
This scenario is common in January-February [patient insurance deductibles not paid] and August-September [new doctors join existing practices]. An increase in new doctor days, and marginal native practice growth, usually mean space in the daily schedule.
Now, the natural tendency is to try and fill the day. And, it is best if the day is filled by increasing patient services acuity levels. However, a common, but ill-advised approach is to add time to existing patient appointments. So, when a practice accepts a new medical provider, creation of a checklist similar to the one below may be helpful.
LIST:
The danger of open appointment slots is adding inefficiencies to a schedule by the pressure to fill time. Instead, look at organic practice growth [5-8% annually for a mature practice], the change in provider time and have realistic expectations for open time-slots in the first few years of new practitioner availability [see http://waittimes.blogspot.com, Wait Time & Delayed Care; a blog devoted to helping healthcare providers shorten wait times and improve patient flow].
Patuient Scheduling Issues
Most mature doctors follow a linear (series-singular) time allocation strategy for scheduling patients (i.e., every 15 or 20 minutes). This can create bottlenecks because of emergencies, late patients, traffic jams, absent office personal, paperwork delays, etc. Therefore, as proposed by Dr. Neal Baum, a practicing urologist in New Orleans, one of these three newer scheduling approaches might prove more useful.
1. Customized Scheduling
The bottleneck problem may be reduced by trying to customize, estimate or project the time needed for the patient’s next office visit. For example: CPT #99211 (5 minutes), #99212 (10 minutes), #99213 (15 minutes), #99214 (25 minutes), or #99215 (40 minutes). Occasionally, extra time is need, and can be accommodated, if the allocated times are not too tightly scheduled.
Some patient populations do not mind a brief 20-30 minute wait prior to seeing the doctor. Wave scheduling assumes that no patient will wait longer than this time period, and that for every three patients; two will be on time and one will be late. This model begins by scheduling the three patients on the hour; and works like this. The first patient is seen on schedule, while the second and third wait for a few minutes. The later two patients are booked at 20 minutes past the hour and one or both may wait a brief time. One patient is scheduled for 40 minutes past the hour. The doctor then has 20 minutes to finish with the last three patients and may then get back on schedule before the end of the hour.
3. Bundle Scheduling
Bundling involves scheduling like-patient activities in blocks of time to increase efficiency. For example, schedule minor surgical checkups on Monday morning, immunizations on Tuesday afternoon, and routine physical examinations on Wednesday evening, or make Thursday kid’s day and Friday senior citizens day. Do not be too rigid, but by scheduling similar activities together, assembly-line efficiency is achieved without assembly line mentality, and allows you to develop the most economically profitable operational flow process possible for the office.
***

Patient Self Scheduling (Internet Based Access Management)
The traditional linear patient scheduling system is slowly being abandoned by modern medical practitioners; an all venues (medical practices, clinics, hospitals and various other healthcare entireties). New software programs, and internet cloud applications, allow patients to schedule their own appointments over the internet. The software allows solo or individual group physicians with a practice to set their own parameters of time, availability and even insurance plans. Through a series of interrogatories, the program confirms each appointment. When the patient arrives, a software tracker communicates with office staff and follows the patients from check-in, to procedures, to checkout. Today, many hospitals have even abandoned the check-in or admissions, department. It has been replaced by access management systems.
Automated Medical Office Access Management Systems [Patient Check-In Kiosks]
According to a McLean report published in InfoTech,
“Today’s patients demand the same level of self-service convenience in healthcare that they do in other industries. Medical kiosks save money, reduce wait times, and significantly enhance the patient experience. The payback period for medical kiosks is often as short as 180 days”
Automated medical office access management [AM] or patient self check-in solutions provide a wide range of functionality including patient registration, insurance verification, and demographic-validation, electronically consent form completion, back-end scheduling, financial systems integration, real-time appointment re-scheduling, direction text mapping and way finding; and more. Often, solutions can be individualized and integrated with HIT systems using HL7, XML, web and other standard data exchange protocols.
Open Access Patient Scheduling
A sub variant of the above is open-access patient self-scheduling, either in full or part. Benefits include reduced patient appointment wait times, matching and scheduling patients with physician, improved continuity of care, increased productivity per patient visits, higher physician compensation and higher net gains for medical offices and clinics.
Real Time Claim Adjudication
Real Time Claim Adjudication [RTCA] or expecting payment at the time of service is becoming the rule, not the exception, in the modern AM era. RTCA makes a medical practice more like other businesses.
Benefit of Automated Medical Office Access Management
Vendors for the above AM processes include: Phreesia.com, KioHealth.com, MediSolve.Ca; VecnaMedical.com; MeridianKiosks.com; AppointmentDesk.com; and KioskMarketPlace.com; etc.
***

Five people are sitting in the waiting room of a doctor’s office. Some of the people look tense or upset, and others look completely relaxed.
More: Simple Steps to a Patient Registry: Ticket to Care Coordination, Quality Reporting and Pay for Performance
Assessment: Your thoughts are appreciated.
***

***
Filed under: iMBA, Inc., Practice Management, Touring with Marcinko | Tagged: patient scheduling, Patient Scheduling Issues, physician scheduling | Leave a comment »
Advertisement
![]()
PodiatryPrep.org is an education-based physician engagement company that provides innovative medical, orthopedic and surgical education and personalized learning management solutions to podiatrists, orthopedic foot surgeons and all physicians, residents and students performing lower extremity reconstructive and trauma surgery; or foot and ankle medicine, wound care and/or orthopedics.
***

***
Through our customized, data driven and ever fluid analytical testing tools and comprehensive educational libraries, we are transforming the way doctors and practitioners [students and institutional residency directors] monitor and prepare for all State licensure tests and Board Certification or Qualification examinations.
TEST TAKING TIPS: PodiatryPrep.ORG
MORE: Pass Points
HAV: GEN.SX.PRINCIPLES
Our secure PodiatryPrep.org email delivery platform makes learning an engaging science, measures doctor & institutional comprehension, improves clinical literacy, and empowers all foot and ankle care providers to take greater control of their testing and examination needs.
VISIT US TODAY!
***

***
Filed under: iMBA, Inc. | Tagged: ABFAS, ABPS, Podiatry Board Exams, PodiatryPrep | 5 Comments »
Courtesy: https://lnkd.in/eBf-4vY
“Of the 125 medical schools in the USA, only one of them to my knowledge offers a class related to saving or investing money.”
– William C. Roberts, MD
Private Banker Jorge Russe; MBA CMP™ explains in this PPT Presentation on Net Worth; NOT Income.
ESSAY: https://lnkd.in/eGArJR2
CMP® CURRICULUM: https://lnkd.in/eDTRHex
Assessment: Your comments are appreciated.
***
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
1 – https://lnkd.in/ebWtzGg
2 – https://lnkd.in/ezkQMfR
3 – https://lnkd.in/ewJPTJs
THANK YOU
***
Filed under: Health Economics, Healthcare Finance, iMBA, Inc. | Tagged: physician net worth, physician salary | 1 Comment »
Courtesy: https://lnkd.in/eBf-4vY
The VM is a measure of the number of times that the average unit of currency is used to purchase goods and services within a given time period. The concept relates the size of economic activity to a given money supply. This speed of money exchange is one of the variables that determine inflation.
VM is the ratio of gross national product (GNP) to a country’s money supply. The more often money changes hands, the greater the level of commerce. The VM is determined by money supply, interest rates, inflation, commerce and the Federal Reserve.
LINK: https://lnkd.in/eZxrhtp
Physicians, like most consumers, tend to hold less money as interest rates and inflation increase, and therefore the velocity of money increases.
ESSAY: https://lnkd.in/e6TvuVM
VM is reduced when people increase money holdings in periods of low interest rates and low inflation; the opposite when rates and inflation are high.
CMP® CURRICULUM: https://lnkd.in/eDTRHex
Assessment: Comments appreciated.
***
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
1 – https://lnkd.in/ebWtzGg
2 – https://lnkd.in/ewJPTJs
THANK YOU
***
Filed under: Financial Planning, Glossary Terms, iMBA, Inc. | Tagged: Velocity Money | Leave a comment »
CIRCA: 202-2016
By staff reporters
***
 ***
***
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
THANK YOU
***
Filed under: Health Economics, Health Insurance, Healthcare Finance, iMBA, Inc. | Tagged: Medical Expenditure Distribution | Leave a comment »
THREE MEDICAL VIDEO MESSAGES FOR THE POST- PANDEMIC WORLD
Courtesy: https://lnkd.in/eBf-4vY
On Population Health
Colleague David Nash MD MBA, Founding Dean Emeritus and Professor of Health Policy, Jefferson College of Population Health, provides the top three things hospitals and health system leaders must do to move forward after the pandemic from a population health perspective.
PODCAST: https://lnkd.in/d2WqvNr
David also wrote the Foreword to our text book: “Financial Management Strategies for Hospitals and Healthcare Organizations” [Tools, Techniques, Checklists and Case Studies].

FOREWORD: https://lnkd.in/eea7PTb
BOOK: https://lnkd.in/eEf-xEH
Your thoughts and comments are appreciated.
***
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
1 – https://lnkd.in/ebWtzGg
2 – https://lnkd.in/ezkQMfR
3 – https://lnkd.in/ewJPTJs
THANK YOU
***
Filed under: iMBA, Inc. | Leave a comment »
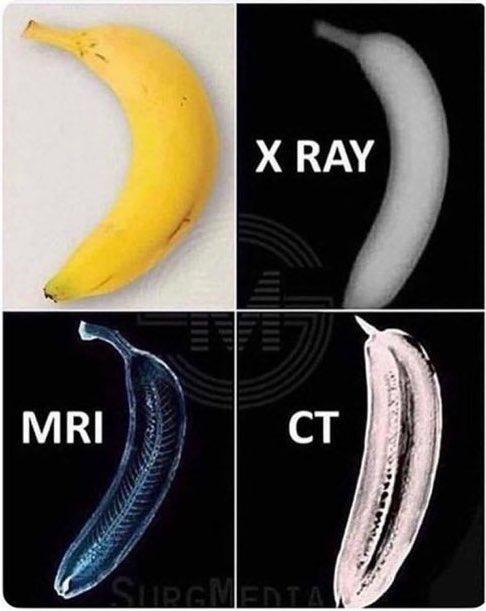
VERSUS A BANANA
By staff reporters
***
 ***
***
Assessment: Your thoughts are appreciated.
***
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS
THANK YOU
***
Filed under: iMBA, Inc. | Tagged: MRIs, x rays; CT scans | Leave a comment »
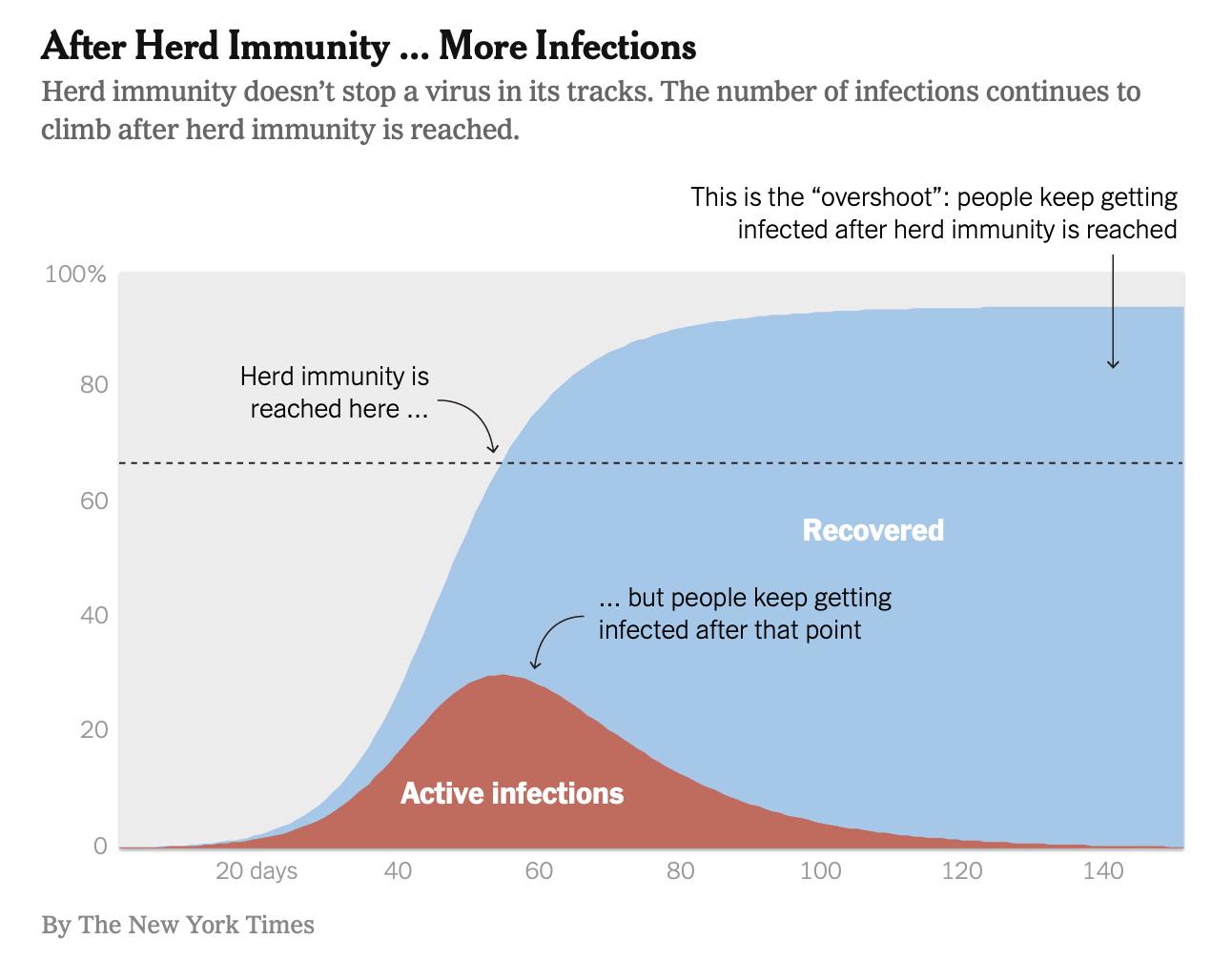
More Infections?
[By staff reporters]
***
***
LINK: https://thehealthcareblog.com/blog/2020/05/05/the-problem-with-herd-immunity-as-a-covid-19-strategy/
***
Assessment: Your thoughts are appreciated

![]()
***
Filed under: iMBA, Inc. | 1 Comment »
Impact Assessment Survey
Dear David, and ME-P Readers

We are pleased to share with you the release of Research2Guidance’s “Impact Assessment Survey: How Corona Impacts the Global Digital Health Industry” whitepaper.
513 digital health experts representing a broad range of healthcare companies shared their views in our global study. Discover their opinions and 10 key takeaways.
Below are just some of the insights from the study and the first special story.
If you have any questions, please let me know. Thank you for your time.
Stay safe and healthy.
Ralf Jahns, MD
Filed under: iMBA, Inc. | 5 Comments »
WHAT IS “CONTACT TRACING” IN PUBLIC HEALTH?
Courtesy: www.CertifiedMedicalPlanner.org
When a patient tests positive, you make a list of everyone they came in close contact with. Then, you find those people and make sure they self-isolate before infecting others.
That sounds straightforward, but contact tracing a new patient typically takes three days, which is “an insurmountable hurdle in the U.S., with its low numbers of public health workers and tens of thousands of new cases every day.”
ELSEWHERE: South Korea used high-tech contact tracing to tame its outbreak. The government compiled GPS data, credit card swipes, and other info into a public log showing where COVID-19 patients had traveled.
Some countries (including the U.S.) are trying other methods, including looking at smart-phone location data and developing Bluetooth systems that provide warnings if you’ve crossed paths with an infected person.
PROBLEMS: Despite its widespread use in places like Singapore, contact tracing has raised concerns about privacy and governments following citizens’ whereabouts.
***

***

***

PODCAST: https://www.youtube.com/watch?v=hlHCLXv2HQs
PODCAST: https://www.youtube.com/watch?v=CQBO_DHBtzw
And so, Contact Tracing is a term you’ll be hearing a lot more of in the coming weeks.
Assessment: Your thoughts and comments are appreciated.
BUSINESS TEXTS FOR PHYSICIAN-EXECUTIVES AND MEDICAL CXO
THANK YOU

***
Filed under: Glossary Terms, Health Insurance, iMBA, Inc. | Tagged: contact tracing, corona virus, Covid-19, public health | 6 Comments »
Courtesy: https://lnkd.in/eVGcji5
By Ann Miller RN MHA CMP®
[Executive Director]
After an overwhelming initial response, the Institute of Medical Business Advisors [iMBA, Inc] is again offering free 60 minute phone or video consultations and second opinions to doctors, nurses and medical colleagues on a limited scheduling and time basis, during the current Corona Virus outbreak 24/7.
REGULAR SERVICE: https://lnkd.in/dw7FHyP Professional fees are waved during this time of crisis. According to Professor and CEO Dr. David Edward Marcinko MBA CMP, “this is our small way to help give back to colleagues who are vital to the US public health system and wellness of the country.” Topics include a plethora of personal financial planning and / or medical practice management and entrepreneurial business issues.
TOPIC LIST: https://lnkd.in/e7WrDj9
TO SCHEDULE: MarcinkoAdvisors@msn.com B
***

***
BUSINESS, FINANCE, INVESTING & INSURANCE TEXTS FOR DOCTORS
PHYSICIAN-EXECUTIVES AND MEDICAL CXOs:
THANK YOU
***
Filed under: CMP Program, Financial Planning, iMBA, Inc., Investing | 2 Comments »
Front Line First Medical Covid-19 Responders
[By staff reporters]
***

***
Assessment: Your thoughts are appreciated.
***
BUSINESS TEXTS FOR PHYSICIAN-EXECUTIVES AND MEDICAL CXOs:
THANK YOU
***
Filed under: iMBA, Inc. | Tagged: Corona first responders, Covid-19 | Leave a comment »
National Doctors’ Day is Global
[By staff reporters]
National Doctors’ Day is a day celebrated to recognize the contributions of physicians to individual lives and communities. The date may vary from nation to nation depending on the event of commemoration used to mark the day.
In some nations the day is marked as a holiday. Although supposed to be celebrated by patients in and benefactors of the healthcare industry it is usually celebrated by health care organizations. Staff may organize a lunch for doctors to present the physicians with tokens of recognition. Historically, a card or red carnation may be sent to physicians and their spouses, along with a flower being placed on the graves of deceased physicians.
***

***
LINK: https://nationaltoday.com/doctors-day/
Assessment: Your thoughts are appreciated.
***
BUSINESS, FINANCE AND INSURANCE TEXTS FOR DOCTORS
THANK YOU
***
Filed under: iMBA, Inc. | Tagged: National Doctors' Day | 1 Comment »
 ***
***
Filed under: Financial Planning, iMBA, Inc., Investing, Portfolio Management | Tagged: Daivd Marcinko, Free consultations, iMBA, Inc., second opinions | Leave a comment »
What it is – How it works?
Courtesy: http://www.CertifiedMedicalPlanner.org
In public health epidemiology, while numerators are measures of health events, the denominator is the population from which events are drawn.
For example, if we are measuring the incidence of Covid-19 among teens, who might comprise your denominator?
ANSWER: Any denominators used should be reflective of the population who could have been included in the numerator had they developed the condition of interest. This is the population at risk, and is often taken as the number of people who are disease-free at the start of data collection. If individuals who could not develop the condition of interest were included in the denominator, this would result in an underestimation of calculated rates.
*****
***
PODCAST: https://www.coursera.org/lecture/epidemiology-tools/denominators-jnpaa
Assessment: Your thoughts and comments are appreciated.
***
BUSINESS, FINANCE AND INSURANCE TEXTS FOR DOCTORS
THANK YOU
***
Filed under: iMBA, Inc. | Tagged: Epidemiology, public health denominator, public health numerator | Leave a comment »
Human Health Behavior and COVID-19 Thoughts
Courtesy: www.CertifiedMedicalPlanner.org
Here are 3 theories and 1 “rule” for the healthcare industrial complex that may help explain how the sector may not work correctly; from trauma, to epidemiology and to Corona; all the time.
1 – Berkson’s Paradox: Strong correlations can fall apart when combined with a larger population.
For example, among motorcycle crash victims wearing helmets are more likely to be seriously injured than those not wearing helmets. But, that’s because most crash victims saved by helmets did not need to become hospital patients, and those without helmets are more likely to die before becoming a hospital patient.
2 – Group Attribution Error: Incorrectly assuming that the views of a group member, like a physician, reflect those of the whole group in a different discipline.
3 – Baader-Meinhof Phenomenon: Noticing an idea or word every where you look as soon as it’s brought to your attention in a way that makes you overestimate its prevalence.
***
LINK:
The 90-9-1 Rule: In social media networks, 90% of users just read content, 9% of users contribute a little content, and 1% of users contribute almost all the content.
QUERY: Does Social Media really give a false impression of what ideas are popular or “average.”
THINK: Corona Virus?
ASSESSMENT: Your thoughts and comments are appreciated.
***
TEXTS FOR PHYSICIAN EXECUTIVES:
THANK YOU
***
Filed under: Health Economics, Health Insurance, Healthcare Finance, iMBA, Inc., Quality Initiatives | Tagged: Baader-Meinhof Phenomenon, Berkson’s Paradox:, corona virus, Group Attribution Error, The 90-9-1 Rule | 2 Comments »
Office Fire Drills

By Dr. David E. Marcinko MBA
Fire Drills should be performed at least annually and documented.
When first opening an office or when a new employee is brought onboard, staff need to be trained on the use of a fire extinguisher, location of the nearest fire extinguisher and location of alarm pull station (if any) on the first day. Training should be documented and placed in the employee file.
Generally speaking, a fire extinguisher is required every 75 feet in office space and be the appropriate type for the nature of business and equipment in use. Most offices use a multi-purpose ABC extinguisher that can be used on most types of fires.
The types of fires are listed below:
EXTINGUISHERS
Carbon Dioxide (CO2) extinguishers can be used for class B and C fires. These extinguishers are highly pressurized and are best suited for electrical or computer equipment. They have an advantage over dry chemical extinguishers for this use since they do not leave damaging residue. However, they are not effective for Class A fires.
It is important to know which type of extinguisher is best for the office and equipment since using the wrong type can be critical in an emergency.
***

***
THE EMERGENCY LIST:
At a minimum, a physician office should have a safety program that addresses the following in the event of an emergency:
If you are in an area susceptible to weather emergencies such as tornadoes, the emergency plan should address these as well.
Assessment: Your thoughts are appreciated
***
***
Filed under: iMBA, Inc., Insurance Matters, Practice Management | Tagged: David Marciniko, Medical Office Fire Drills | Leave a comment »

|
Filed under: iMBA, Inc. | Tagged: corona virus, Covid-19, Vitaliy Katsenelson CFA | 1 Comment »
R.I.P Jack Welch and Freeman Dyson
By Dr. David E. Marcinko MBA
I studied both these management icons in business and graduate school. Then, I modified their ideas for my own medical practice and related corporate business entities.
Later, I ported their styles into the healthcare industrial complex and continue to stream line them into my academic professional university endeavors. Many thanks to you both!
Freeman Dyson in his Own Words
Jack Welch, Legendary CEO of General Electric, Dies at Age 84
LINK: https://www.wsj.com/articles/jack-welch-legendary-ceo-of-general-electric-dies-at-age-84-11583158270
Assessment: Your thoughts are appreciated
***
![]()
***
Filed under: iMBA, Inc. | Tagged: Jack Welch | 2 Comments »
Modern Corono Virus Thoughts?
By: http://www.CertifiedMedicalPlanner.org
Here are a few theories of human behavior for the healthcare industrial complex that might help explain how sector thoughts may not work correctly; all the time.
WHY: Perhaps they might be considered in light of the CorVid-19epidemic?
****
Erkson’s Paradox: Strong correlations can fall apart when combined with a larger population. For example, among motorcycle crash victims wearing helmets are more likely to be seriously injured than those not wearing helmets. But, that’s because most crash victims saved by helmets did not need to become hospital patients, and those without helmets are more likely to die before becoming a hospital patient.
Group Attribution Error: Incorrectly assuming that the views of a group member, like a physician, reflect those of the whole group in a different discipline.
***

***
Baader-Meinhof Phenomenon: Noticing an idea or word everywhere you look as soon as it’s brought to your attention in a way that makes you overestimate its prevalence.
The 90-9-1 Rule: In social media networks, 90% of users just read content, 9% of users contribute a little content, and 1% of users contribute almost all the content.
QUERY: Does Social Media give a false impression of what ideas are popular or “average.”
ASSESSMENT: Your thoughts and comments are appreciated.
TEXTS FOR PHYSICIAN EXECUTIVES:
THANK YOU
***
![]()
![]()
***
Filed under: Ethics, Glossary Terms, iMBA, Inc. | Tagged: 90-9-1 Rule, Baader-Meinhof Phenomenon, Erkson’s Paradox, Group Attribution Error | Leave a comment »
FEBRUARY 2020 AJPHBy Alfredo Morabia, MD, PhD Editor-in-chief, AJPH Dear Dr. David Marcinko, |
***
| This month, AJPH has a collection of articles on ending the HIV epidemic, population health and telemedicine services.
New! Enjoy the current issue of AJPH on your mobile device. Download the e-Reader or Kindle version today. Here are a few of the many articles in the February 2020 issue: |
***
***
| Also, don’t miss our just released supplement on Documenting and Addressing the Health Impacts of Carceral Systems. It’s full of timely and insightful articles on mass incarceration and related topics.
The mission of AJPH is to advance public health research, policy, practice and education. Toward that goal, the journal also produces monthly podcasts available in English, Spanish and Chinese at ajph.org. The monthly podcasts also are on iTunes and Google Play. Be on the lookout for more timely research from AJPH, and consider subscribing or becoming an APHA member for full access. Thank you and Happy New Year 2020 |

| Alfredo Morabia, MD, PhD
Editor-in-chief, AJPH |
Filed under: Experts Invited, Health Law & Policy, iMBA, Inc. | Tagged: Alfredo Morabia, MD, PhD, Role of Pleasure in Public Health | Leave a comment »
Of STOCKMARKET Bear Markets
Update Courtesy: http://www.CertifiedMedicalPlanner.org
28,992.41 ▼ -227.57
A Bull market is one of rising stock prices, while a Bear market is the opposite. More specifically, a Bear market is defined as a drop of 20% or more from its high, and can vary in duration and severity. While a Bull market has no such threshold.
Whither the Bear?
Typically, bear markets are associated with declines in an overall market or index like the S&P 500, but individual securities or commodities can be considered to be in a bear market over a sustained period of time – typically two months or more.
ESSAY: https://medicalexecutivepost.com/2018/12/22/stocks-and-sectors-in-bear-territory/
Now, a Minsky moment is a sudden major collapse of asset values which is part of the credit cycle or business cycle. Such moments occur because long periods of prosperity and increasing value of investments lead to increasing speculation using borrowed money
ESSAY: https://medicalexecutivepost.com/2018/11/16/what-is-a-minsky-moment/
And so, what is a physician-investor to do in a bear market?
9,576.59 ▼ -174.38 -1.79%
ESSAY: https://medicalexecutivepost.com/2016/03/18/doctors-and-bull-and-bear-markets/
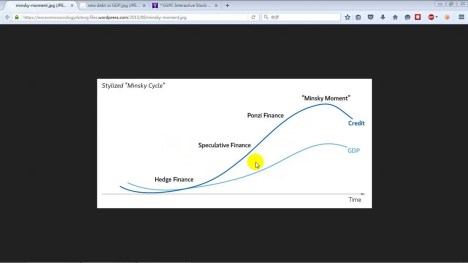
MORE: https://realinvestmentadvice.com/the-return-of-the-minsky-moment/
Your thoughts and comments are appreciated.
BUSINESS, FINANCE AND INSURANCE TEXTS FOR DOCTORS:
THANK YOU
![]()
![]()
***
Filed under: iMBA, Inc. | Leave a comment »
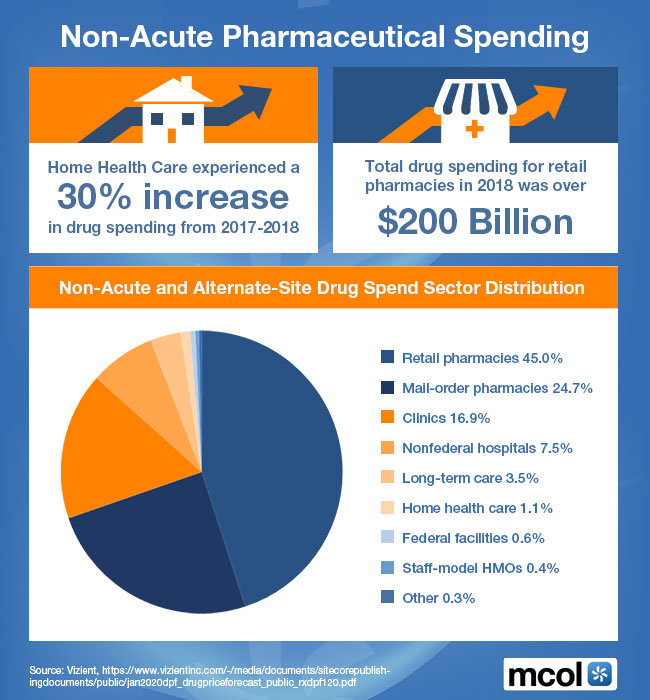
Alternate Site Drug Spend Sector Distribution
[By staff reporters]
***
***
![]()
***
Filed under: iMBA, Inc. | Tagged: Alternate Drug Site Spend Sector Distribution, Non-Acute Pharmaceutical Spending | Leave a comment »
More on Epidemiology and Health Economics
Courtesy: www.CertifiedMedicalPlanner.org
By Dr. David E. Marcinko MBA
We’ve talked about the “Number Needed to Treat”, before.
QUERY: But, what is the “Number Needed to Harm”?
ANSWER: The number needed to harm (NNH) is an epidemiological measure that indicates how many persons on average need to be exposed to a risk factor over a specific period to cause harm in an average of one person who would not otherwise have been harmed.
Colleague Aaron Carroll MD explains even more.
PODCAST: https://www.youtube.com/watch?v=e_ytF2-4NkI
***

***
MORE: https://www.youtube.com/watch?v=90CWXT5zxjw
Conclusion: Your thoughts are appreciated.
TEXTS FOR PHYSICIAN EXECUTIVES AND HOSPITAL CXOs:
THANK YOU
![]()
![]()
***
Filed under: Glossary Terms, iMBA, Inc., Research & Development | Tagged: NNTH, Number Needed TO Harm | Leave a comment »
On “WHAT’S-WHAT” and more!
By Dr. David E. Marcinko MBA
Is there a Difference? – Know the Difference!
DEDUCTIVE reasoning and logic is the process of reasoning from one or more statements (premises) to reach a logically certain conclusion. Deductive reasoning goes in the same direction as the conditionals, and links premises with conclusions. If all premises are true, the terms are clear, and the rules of deductive logic are followed, then the conclusion reached is necessarily true.
INDUCTIVE reasoning is a method in which the premises are viewed as supplying some evidence for the truth of the conclusion. While the conclusion of a deductive argument is certain, the truth of the conclusion of an inductive argument may be probable, based upon the evidence given. Many dictionaries define inductive reasoning as the derivation of general principles from specific observations, though there are many inductive arguments that do not have that form.
***
***
SEMANTICALLY NULL doesn’t mean anything but is grammatically sound. A sentence as a whole can be semantically null because its internal inconsistencies prevent it from developing a meaning; ie., “I know what’s what?
An EXPLETIVE is a word or phrase inserted into a sentence that is not needed to express the basic meaning of the sentence. It is regarded as semantically null or a place holder.
A SYLLOGISM is a form of reasoning in which a conclusion is drawn (whether validly or not) from two given or assumed propositions (premises), each of which shares a term with the conclusion, and shares a common or middle term not present in the conclusion (e.g., all dogs are animals; all animals have four legs; therefore all dogs have four legs). This school of epistemology is highly advanced in syllogism and logical reasoning.
MORE: https://medicalexecutivepost.com/2019/05/14/what-is-epistemic-ambivalence/
MORE: https://medicalexecutivepost.com/2019/12/23/rationalism-versus-empiricism/
Conclusion: Your thoughts are appreciated.
***
![]()
![]()
***
Filed under: Glossary Terms, iMBA, Inc. | Tagged: Epistemic ambivalence, expletive, inductive and deductive reasoning, logic, semantically null | Leave a comment »
FOR ALL … ALL!
[By staff reporters]
***
***
![]()
***
Filed under: iMBA, Inc. | Tagged: medical quality, medical quality improvement | Leave a comment »
A SYNOPSIS OF MY ADVISORY FEES & CONSULTING BUSINESS MODEL
Courtesy: https://lnkd.in/eVGcji5
[Authentic Consulting for Physicians & Medical Colleagues]
My fee is $250 per hour prorated, so you only pay for the time used. This fee covers almost any medical practice management, insurance and risk management, personal financial planning or investment related topic, including document review, phone or Skype® consultation, research and/or written investment strategies.
MODEL: https://lnkd.in/eVWcyaq
IOW: No high water marks, no claw-back fees, sales or commissions, front or back end loads, 12[b]-1 fees or Assets Under Management [AUM] charges; etc. “Pay-as-you-Go”; period! Client Centricity.
TOPICS: https://lnkd.in/e7WrDj9
2nd OPINIONS: https://lnkd.in/dw7FHyP
INVITE: https://lnkd.in/e3-SFmb Your thoughts are appreciated.
CONTACT: Ann Miller RN MHA CMP® PHONE: 770-448-0769
EMAIL: MarcinkoAdvisors@msn.com
BUSINESS, FINANCE, INVESTING & INSURANCE TEXTS FOR DOCTORS:
THANK YOU
![]()
***
Filed under: iMBA, Inc., Touring with Marcinko | Tagged: David Marcinko MBA, Marcinko | Leave a comment »
DOCTOR COLLEAGUES BEWARE = HARD “SELLING” FINANCIAL ADVICE
Courtesy: https://lnkd.in/eBf-4vY
Please Know – It’s all about Sales, Sales and Sales!
Steve Forbes, editor of the well-respected financial publication Forbes Magazine, once said:
“You make more selling advice than following it. It’s one of the things we count on in the magazine business, along with the short memory of our readers.”
ESSAY: https://lnkd.in/ebGmB7W
MORE: https://lnkd.in/er8tQ8y
Assessment: Your thoughts are appreciated.
BUSINESS, FINANCE, INVESTING & INSURANCE TEXTS FOR DOCTORS:
THANK YOU
8
***
Filed under: iMBA, Inc. | Leave a comment »
U.S.A BUSINESS CYCLE REPORT 2019
Courtesy: www.CertifiedMedicalPlanner.org
[Pictographic Presentation for December 2019]
Constructed and presented by Nick Reece CFA of MERK Investments LLC., and Research.
GRAPHIC CHART BOOK: MR
Your thoughts are appreciated.
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
THANK YOU
8
Filed under: Experts Invited, iMBA, Inc. | Tagged: U.S.A BUSINESS CYCLE REPORT 2019 | Leave a comment »
A Picto-Graphic Presentation
Courtesy: www.CertifiedMedicalPlanner.org
Constructed and presented by Nick Reece CFA of MERK Investments LLC., and Research.
CHART BOOK: 2019-12-18-merk-business-cycle-chart-book
Your thoughts are appreciated.
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:

THANK YOU
Filed under: iMBA, Inc. | Tagged: business cycle. investing cycle | Leave a comment »
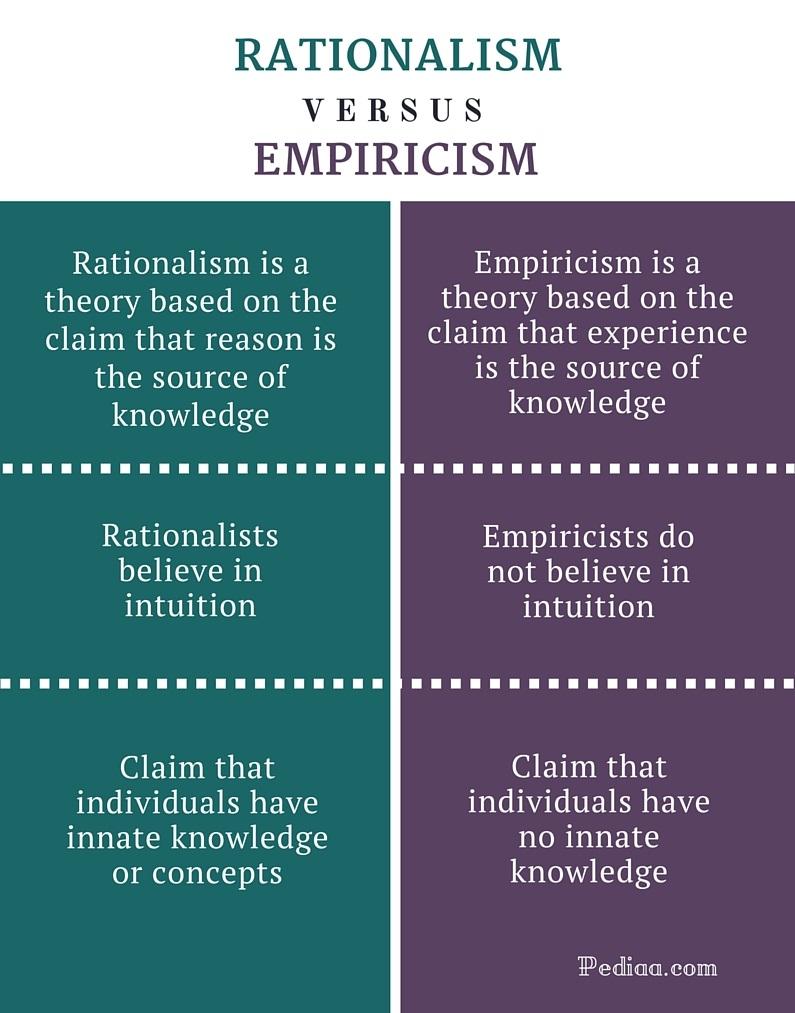
PHILOSOPHY – What is Knowledge?
***
***
***
MORE: https://medicalexecutivepost.com/2019/05/14/what-is-epistemic-ambivalence/
![]()
![]()
***
Filed under: iMBA, Inc., LifeStyle | Tagged: Empiricism, epistemology, Rationalism | Leave a comment »
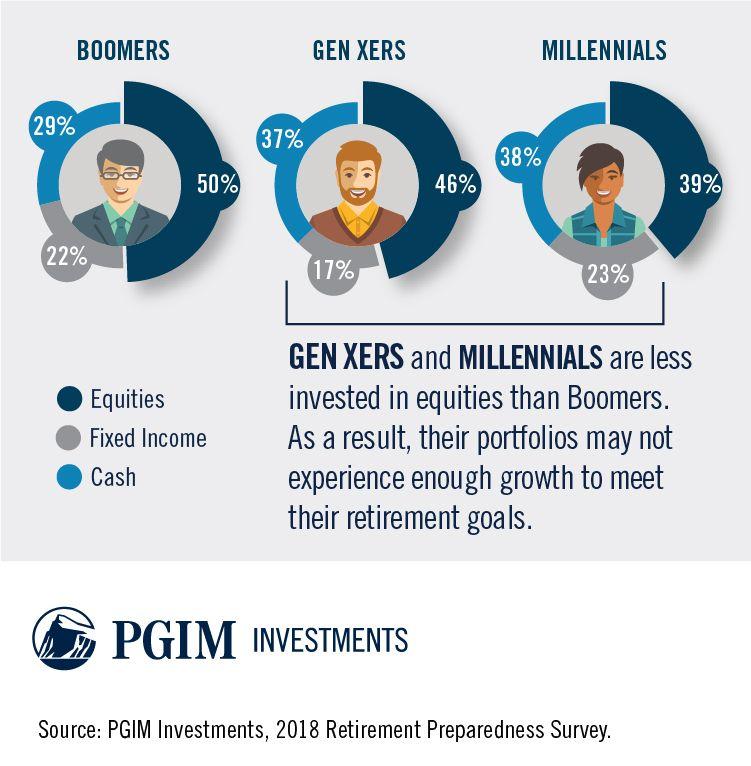
Portfolio Asset Allocations
By PGIM Investments
***
***
Assessment: Your thoughts are appreciated.
BUSINESS, FINANCE, INVESTING & INSURANCE TEXTS FOR DOCTORS:
***
8
THANK YOU
Filed under: iMBA, Inc. | Tagged: baby boomers, Gen X, Millennials | Leave a comment »
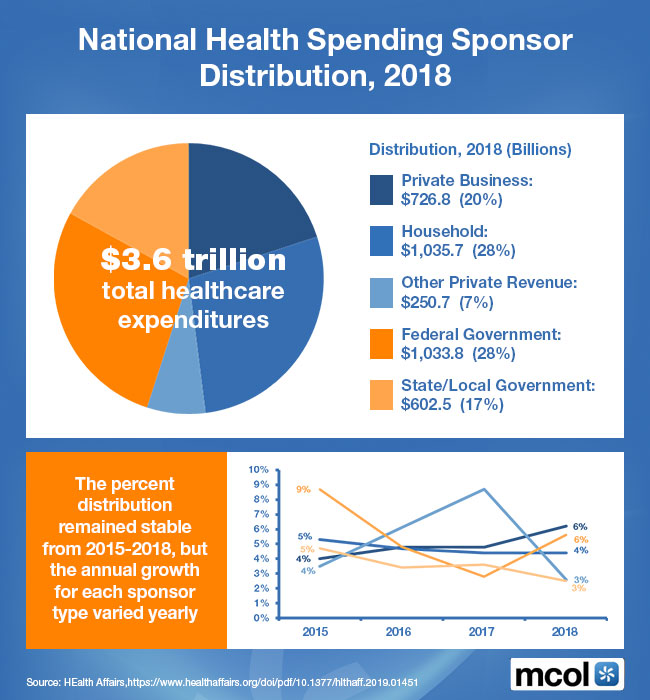
Sponsor Distribution for 2018
***
***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
![]()
***
Filed under: Health Economics, Health Insurance, iMBA, Inc. | Tagged: National Health Care Spending, www.MCOL.com | Leave a comment »
Medicare Part C
***

***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
***
Filed under: iMBA, Inc. | 3 Comments »
Where Will Your Money Come From?
 By Rick Kahler CFP®
By Rick Kahler CFP®
The list is fairly short: Social Security, a pension, working, your assets, children, or public assistance.
According to an April 22, 2019 Bloomberg article by Suzanne Woolley, entitled “America’s Elderly Are Twice as Likely to Work Now Than in 1985“, only twenty percent of those age 65 or older are working. The rest either can’t work physically, can’t find work, or don’t want to work. According to the ADA National Network, over 30 percent of people over 65 are disabled in some manner.
According to the Center on Budget and Policy Priorities, Social Security provides the majority of income for most elderly Americans. It provides at least 50% of income for about half of seniors and at least 90% of income for about one-fourth of seniors. The average Social Security retirement benefit isn’t as high as many people think. In June 2019 it was about $1,470 a month, or about $17,640 a year.
And, as per the Pension Rights Center, around 35% of Americans receive a pension or VA benefits. The greatest percentage of pensions are government. This would include retired state and federal workers like teachers, police, firefighters, military, and civil service workers. In 2017 the median state or local government pension benefit was $17,894 a year, the median federal pension was $28,868, and the median military pension was $21,441.
Working provides the highest source of retirement income for the 20 percent of those who are over 65 and are still working. According to SmartAsset.com, Americans aged 65 and older earn an average of $48,685 per year. However, in a NewRetirement.com article dated February 26, 2019, “Average Retirement Income 2019, How Do You Compare“, Kathleen Coxwell cites a figure from AARP that the median retirement income earned from employment is $25,000 a year.
About 3% of retirees receive public assistance.
This leaves around 20% of those over 65 who depend partially or fully for their retirement income on money they set aside during their working years. According to TheStreet.com, “What Is the Average Retirement Savings in 2019“, by Eric Reed, updated on Mar 3, 2019, the average retirement account for those age 65 to 74 totals $358,000. That amount will safely provide around $15,000 a year for most retirees’ lifetime. The median savings is $120,000, which will produce only about $5,000 a year. In order to retire at age 65 with an annual investment income of $30,000 to $40,000, someone would need a retirement nest egg of over $1 million.
***

***
My conclusion from this data is that most Americans are woefully underprepared to live a comfortable lifestyle when they can no longer work. Between Social Security, pensions, and retirement savings, a retiree can expect a median income of $18,000 to a maximum of $52,000 a year. According to data I compiled from NewRetirement.com, the average median retirement income of those over age 65 is around $40,000.
What are some things you can do to increase your chances of enjoying a comfortable retirement income?
If you are under age 50, begin setting aside 15% to 25% of your income for retirement.
If you are over 60, keep working as long as you can. If you retire early, your monthly Social Security benefit is lower for the rest of your life.
Consider ways to stretch your retirement income by downsizing, sharing housing, or relocating to an area of the US or even outside the country with a lower cost of living.
Research what you can reasonably expect from Social Security and other sources of retirement income. Base your retirement expectations on informed planning, not on vaguely optimistic expectations.
Assessment: Your thoughts are appreciated.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
***
 8
8
***
Filed under: iMBA, Inc., Retirement and Benefits | Tagged: retirement, retirement planning, Rick Kahler CFP | Leave a comment »
Projections 2020

***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Your thoughts are appreciated.
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
THANK YOU
Filed under: iMBA, Inc. | Tagged: Health Plan Premium Increases | Leave a comment »
Over Heard in the Doctor’s Lounge
Courtesy: www.CertifiedMedicalPlanner.org
On the PPMCs of Yester Year and Today
PPMC = Physician Practice Management Corporation
Reflect on medical colleagues willing to securitize their practices a few years later, and cash out to Wall Street servitude for riches not rightly deserved. Where are firms such as MedPartners, Phycor, FPA, Coastal Healthcare, and a host of others, now?
ESSAY: https://medicalexecutivepost.com/2007/11/27/ppmc-redux/
A survey of the Cain Brothers Physician Practice Management Corporation Index of publicly traded PPMCs revealed a market capital loss of more than 99%, since inception.
QUERY: Would niche educated and physician-focused financial advisors [The Certified Medical Planner™ professional designation did not yet exist] have been able to avoid this calamity?

TODAY: https://medicalexecutivepost.com/wp-content/uploads/2007/11/ppmc.pdf
Your thoughts are appreciated.
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
THANK YOU
Filed under: iMBA, Inc. | Leave a comment »
By RICK KAHLER, CFP
You have probably never seen an ad like this, because entrepreneurs are not hired. They hire themselves. Merriam-Webster defines an entrepreneur as “a person who starts a business and is willing to risk loss in order to make money” or “one who organizes, manages, and assumes the risks of a business or enterprise.”
God bless entrepreneurs. Without them our world would look much different. We would probably still be living in caves, hunting with clubs, and eating raw meat. They create companies from scratch. In so doing, they create jobs and take significant monetary risks of a business failure.
They also stand to gain substantial rewards for success, but that success is far from guaranteed. Few people realize that most entrepreneurs fail in their attempts in business. According to Investopedia, 50% of all new businesses fail in 5 years, 66% in 10 years, and 75% in 15 years.
Given those statistics, the entrepreneurs who succeed must be rich, right? A study by Career Explorer found that the average full-time salary of an entrepreneur is $43,240 a year. To put this into perspective, the average starting salary for a graduating four-year degree student at the South Dakota School of Mines and Technology is $63,354. Maybe there should be a song, “Mamas, don’t let your babies grow up to be entrepreneurs.”
My experience, however, is that it really doesn’t matter what Mama says. The entrepreneurial mindset is somewhat inextinguishable. While there have been some attempts at teaching entrepreneurial skills, it’s hard to teach grit, determination, and perseverance, coupled with a good dose of fantasy thinking and denial. It’s really hard to “tell” an entrepreneur anything.
Fittingly, entrepreneurs love to invest in their own companies. Investment advisors call such holdings “tangible” investments, ones you can see and touch. Tangible investments include start-up businesses, family-owned businesses, and all types of directly owned real estate. They are inherently non-diversified and illiquid. Typically, entrepreneurs have the vast portion of their net worth tied up in their businesses. It’s incredibly rare to find one with a stash of cash or any type of liquid portfolio or retirement plan.
Why? The entrepreneurial mindset. First, entrepreneurs don’t believe in traditional diversification. Why settle for earning an average of 5% a year when you can earn ten times that in your business? Never mind that the chance of losing it all is three to one. Most entrepreneurs firmly believe they are the one guaranteed to succeed even though the deck is stacked against them.
Second is that since 75% of businesses ultimately fail, most entrepreneurs are losing, not making, money. They are perennially cash-poor and need every dollar they can find to fund their negative cash flows. Even those who are making money rarely have any liquid investments because entrepreneurs are always looking for new ventures, which of course, need funding.
One of the most difficult tasks I face is persuading a successful entrepreneur to take some hard-earned “chips” off the table and sock away a low-risk, diversified nest egg to assure a comfortable retirement. The only ones I’ve convinced to do that were older entrepreneurs who had owned their companies for well over 15 years and were under five years from retirement. All the younger entrepreneurs to whom I have given that advice have refused the notion. All have eventually lost 75% to 90% of their net worth and, sadly, the opportunity to secure their future.
The entrepreneurial mindset of determination and perseverance can bring significant financial rewards. Expanding that mindset to include a broader, more diversified view of investing for the future can turn those rewards into long-term financial independence.
Assessment: Your thoughts are appreciated.

BUSINESS, FINANCE, INVESTING & INSURANCE TEXTS FOR DOCTORS:
THANK YOU
***
Filed under: Experts Invited, Financial Planning, iMBA, Inc. | Tagged: Entrepreneurs | Leave a comment »
INVITE A PHYSICIAN & TRUSTED FINANCIAL ADVISOR COLLEAGUE TO YOUR NEXT SEMINAR, MEETING OR EVENT
Courtesy: https://lnkd.in/eBf-4vY
Your Audience Deserves a Nationally Known Speaker and Colleague.
[Professor Dr. David E. Marcinko MBA CMP® is Now at Your Service]
CONTACT: Ann Miller RN MHA
THANK YOU
![]()
***
Filed under: iMBA, Inc., Touring with Marcinko | Tagged: CMP Program, David E. Marcinko | Leave a comment »
Nothing Typical
By Rick Kahler CFP
As a fan of our local ECHL hockey team, the Rapid City Rush, I was sorry to learn recently that the team’s new owners had uncovered evidence of some $500,000 worth of embezzlement over the past several years.
Other embezzlement arrests or convictions in our area in 2019 have included a priest, an accountant for a nonprofit, a former chief of a volunteer fire department, and a former secretary of a tribal office. Amounts stolen ranged from $9,100 to $250,000.
Few things strike more fear and disbelief into the heart of an employer than learning a trusted employee has embezzled thousands of dollars. Employers that have gone through this tell me their feelings range from disbelief, violation, anger both at the employee and at themselves, sadness, and fear over the loss of capital and ensuing financial problems the embezzlement often causes.
The study
According to the 2018 Hiscox Embezzlement Study, most instances of embezzlement are serious, long-term crimes. The average case lasted over two years, and the average loss was $357,650. The vast majority of cases involved more than one person. Nearly a third of employee theft cases persisted for more than five years. The average loss for cases that continued for five years or more was $2.2 million and for cases lasting 10 years or more was $5.4 million.
The study found that there is no “typical” embezzler. However, it did find that the median age of embezzlers is 48, slightly more women than men commit this type of crime, and embezzlers’ most common job functions are finance and accounting.
Embezzlers may target organizations of all sizes and types. Four of the five local cases I cited were non-profits. Large organizations experience fewer instances of embezzlement than small and mid-sized organizations. According to the study, financial services continues to account for the highest number of cases of employee theft of any industry examined.
Many business owners, executive directors, and board members blame themselves for allowing theft to happen under their watch, but in all fairness the warning signs are often subtle.
Hiscox has identified five common characteristics to watch for:
• Intelligence and curiosity: Embezzlers are often eager to know how everything in the office works. Once they learn the processes, they manipulate them for their own gain.
• Extravagance: Watch for employees who are living a lifestyle that is out of proportion to their salary.
• Egotistical risk-taking. Embezzlers often break rules, from traffic laws to company policies to social norms, both at work and in their personal lives.
• Diligence and ambition. Embezzlers may work long hours or refuse to take time off—not out of dedication to the job but in an attempt to avoid being caught.
• Disgruntlement. Employees who feel they are being treated unfairly may be tempted to get even by stealing.
In my experience, most people are honest and trustworthy. But there are some whose past trauma contributes to a pattern of poor financial decisions and behaviors. Embezzlement, which to some degree can be a crime of opportunity, might even seem to be a way to avoid the consequences of previous poor money choices.
The study noted that more than half of the organizations recovered less than a third of what was taken. It also pointed out that embezzlement costs companies far more than money. Business partners may be lost. The damage to an organization’s reputation results in lost customers or donors and difficulty attracting new ones. It can take years to recover. Yet three-quarters of respondents said their current employers did not have insurance to cover embezzlement losses.
Assessment: Embezzlement is a serious crime with serious consequences.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
8
***
Filed under: iMBA, Inc. | Tagged: embezzlemen | 1 Comment »
NALOXONE SPRAY!
By Anonymous DEA Agent
Naloxone, sold under the brandname Narcan among others, is a medication used to block the effects of opioids, especially decreased breathing in overdose. Naloxone may be combined with an opioid (in the same pill) to decrease the risk of opioid misuse. When given intravenously, naloxone works within two minutes, and when injected into a muscle, it works within five minutes; it may also be sprayed into the nose. The effects of naloxone last about half an hour to an hour. Multiple doses may be required, as the duration of action of most opioids is greater than that of naloxone.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
***
![]()
***
Filed under: iMBA, Inc. | Tagged: naloxone, narcan | Leave a comment »



















































iMBA IS NOW OFFERING FREE FINANCIAL & BUSINESS ADVISORY CONSULTATIONS
***