BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] E-mail: MarcinkoAdvisors1738@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on March 7, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
LAUGHTER
By staff reporters
Laughter is a physical reaction in humans consisting usually of rhythmical, often audible contractions of the diaphragm and other parts of the respiratory system resulting most commonly in forms of “hee-hee” or “ha-ha”.
Posted on March 3, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
WHAT IS PHYSICIAN BOARD CERTIFICATION AND BOARD ELIGIBILITY?
Courtesy: https://lnkd.in/drrYKeT
BOARD CERTIFICATION (Boarded, Diplomate): A doctor who is board certified has pursued advanced training in his or her specialty and has passed a qualifying examination; a doctor who is board eligible has received the training but has not taken or passed the exam. DHIMC: https://lnkd.in/e9AmEhd
BOARD ELIGIBLE: Describes a physician who is eligible to take the specialty board examination by virtue of being graduated from an approved medical school, completing a specific type and length of training, and practicing for a specified amount of time. Some HMOs and other health facilities accept board eligibility as equivalent to board certification, significant in that many managed care companies restrict referrals to physicians without certification. FOREWORD:https://lnkd.in/gywd_Ad
Posted on March 1, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Rare Disease Day 2021
[By staff reporters]
February 28th 2021 was the fourteenth international Rare Disease Day coordinated by EURORDIS. On and around this day hundreds of patient organizations from countries and regions all over the world held awareness-raising activities.
Posted on February 27, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
FINANCIAL OPINIONS OF MEDICAL PRACTICE FAIR MARKET VALUE [FMV]
Courtesy: https://lnkd.in/eBf-4vY Plastic Surgery-Medical Practice Worth, Valuation, Sales & Succession Planning
For doctor-colleagues, buying or selling a practice may be the biggest financial transaction of their lives. Reasons for appraising practice worth include: sales, merger, succession, retirement and estate planning; partnership disputes and divorce; or as an important tool for organic growth and strategic planning.
However, the transaction is fraught with many pitfalls to avoid and no medical specialty seems immune; especially when it comes to contentious fair market value [FMV] appraisals.
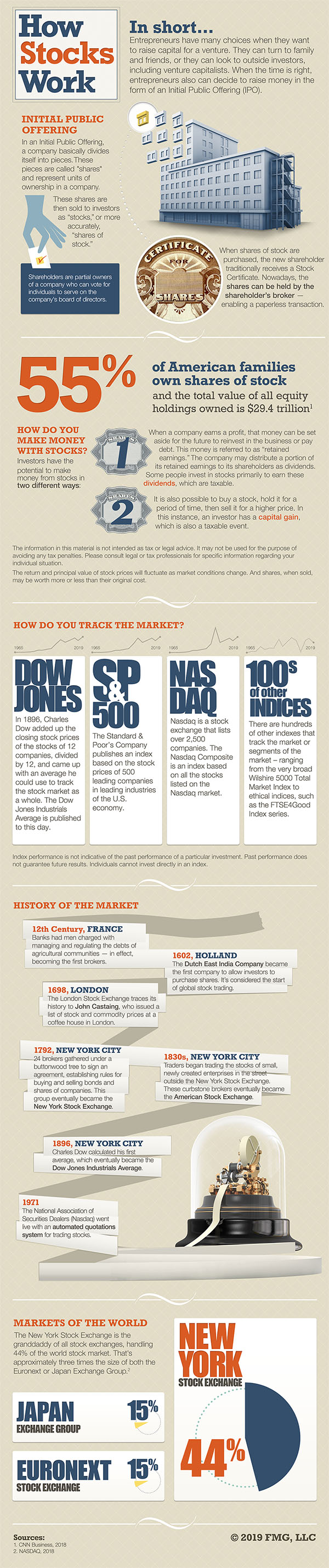
DEFINITION: A member of a securities exchange with the essential function of maintaining a fair and orderly market, insofar as reasonably practicable, in the stocks in which he is registered as a specialist. To do this, s/he must buy and sell for his own account and risk, to a reasonable degree, when there is a temporary disparity between supply and demand. In order to equalize trends, he must buy or sell counter to the direction of the market. DHEF:https://lnkd.in/dqdbWM9 FOREWORD: https://lnkd.in/ecwZWxu
At all times the specialist must put his customer’s interest before his own. All specialists are registered with the exchange, but are not employees of that exchange. Your thoughts are appreciated.
Posted on February 17, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
RED CROSS DAY
On this day in 1863, Henry Dunant founded the Red Cross, which would go onto receive the Nobel Peace Prize three times.
During the Battle of Solferino in the Franco-Austrian war, Swiss businessman Dunant was shocked to witness tens of thousands dead or wounded left on the field after just one day of fighting.
After this experience, on 17 February 1863, he decided to form the International Committee of the Red Cross in Geneva Switzerland with four other Swiss businessmen to take care of casualties and prisoners of war. In the following year, the first Geneva Convention was adopted, “for the Amelioration of the Condition of the Wounded and Sick in Armed Forces in the Field.”
The First World War was an enormous challenge for the organisation. At the outbreak of the war in 1914 medical staff from all over the world gathered to take care of the many wounded. One of them was the young Ernest Hemingway (awarded the Nobel Prize in Literature 1954), employed as an ambulance driver on the Austrian-Italian front. The experience later inspired him to write the novel ‘Farewell to Arms’.
***
Henry Dunant was awarded the first ever Nobel Peace Prize in 1901 for his humanitarian work.
The organization he founded received the prize three times.
Posted on February 9, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
FINANCIAL OPINIONS OF MEDICAL PRACTICE FAIR MARKET VALUE [FMV] Courtesy: https://lnkd.in/eBf-4vY Medical Practice Worth, Valuation, Sales and Succession Planning
Posted on February 5, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
NATIONAL WEAR RED DAY 2021
National Wear Red Day for the year 2021 is celebrated / observed on Friday, February 5th.
Every year the first Friday of February has been dedicated to National Wear Red Day as an awareness day for American women to understand their number one health threat – heart disease.
Posted on February 1, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
DISCLOSURE OF CASH PRICE
SECTION 1.
(a) In this section, “hospital” means a hospital: (1) licensed under Chapter 241; or (2) owned or operated by this state or an agency of this state. (b) A hospital shall disclose the hospital’s cash price for each health care service regularly provided by the hospital. The required disclosure must be made: (1) by posting the prices on the Internet website of the hospital; or (2) if the hospital does not have an Internet website, by providing the prices in writing on request to any person.
SECTION 2. This Act takes effect September 1, 2021.
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, urls and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Posted on January 3, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
HAPPY FIRST NEW YEAR SUNDAY 2021
PATTERSON PARK
[East Baltimore City, Maryland]
Patterson Park is an urban park in Southeast Baltimore, Maryland, United States, adjacent to the neighborhoods of Canton, Highlandtown, Patterson Park, and Butchers Hill. It is bordered by East Baltimore Street, Eastern Avenue, South Patterson Park Avenue, and South Linwood Avenue.
The Patterson Park extension lies to the east of the main park, and is bordered by East Pratt Street, South Ellwood Avenue, and Eastern Avenue.
The Biden Administration has put forth their healthcare plan, which seeks to expand access to affordable healthcare with the following:
***
***
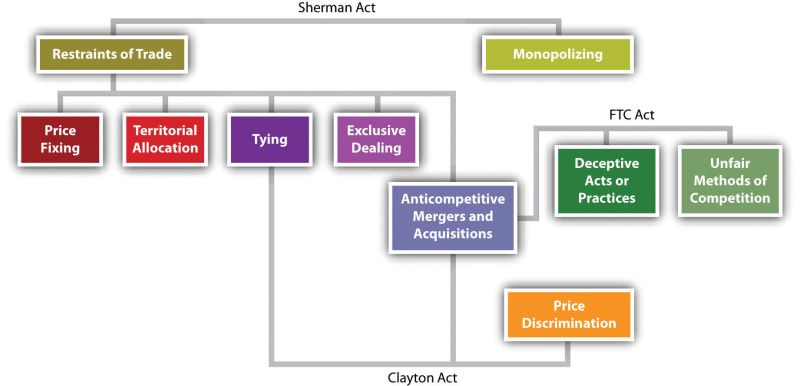
(1) upholding and expanding the Patient Protection and Affordable Care Act (ACA), to reduce the amount that consumers pay for health insurance on the individual marketplace; (2) offering a new, public insurance option similar to Medicare; (3) prohibiting the practice of “surprise billing”; (4) leveraging the Department of Justice’s (DOJ’s) and Federal Trade Commission’s (FTC’s) antitrust authority to target market concentration within the healthcare system; and, (5) driving down prescription drug prices by increasing competition for, and regulation, of pharmaceutical companies.
DEFINITION: The PPI is a group of indexes that measure the change, over time, in the prices received by domestic producers of goods and services. It measures price changes from the perspective of the seller rather than the consumer, as with the CPI. The CPI would include imported goods, while the PPI is relevant to U.S. producers, and therefore would not include imports.
The PPI measures over 10,000 products and services. It reports the price changes prior to the retail level. This information is useful to the government in formulating fiscal and monetary policies. The data gathered from the PPI is often used in escalating purchase and sales contracts. That is the dollar amount to be paid at some time in the future.
NOTE: Long-term managed medical care contracts of the future will seek escalation clauses for increases in prices. DHEF: https://lnkd.in/dqdbWM9
Posted on November 29, 2020 by Dr. David Edward Marcinko MBA MEd CMP™
Healthcare Transparency
By Health Capital Consultants, LLC
On October 29, 2020, the Centers for Medicare & Medicaid Services (CMS) released the Transparency in Coverage final rule. This long-anticipated final rule stems from President Donald Trump’s June 2019 executive order on “Improving Price and Quality Transparency” and builds upon the hospital Outpatient Prospective Payment System (OPPS) price transparency requirements released in November 2019.
These requirements came under fire in a lawsuit filed by the American Hospital Association (AHA), Association of American Medical Colleges (AAMC), Children’s Hospital Association (CHA), and Federation of American Hospitals (FAH), against the Department of Health and Human Services (HHS); the requirements were upheld by the courts in June 2020 and the lawsuit is being appealed by the plaintiffs. (Read more…)
The second installment in this five-part Health Capital Topics series on the valuation of telemedicine will focus on the reimbursement environment for telemedicine.
***
Telemedicine is reimbursed based on the services provided through this medium and includes many restrictions on where, how, and by whom services can be conducted. The first installment in this series introduced telemedicine and its increasing importance to, and popularity among, providers and patients. It also discussed the current and future challenges related to telemedicine, many of which hinge upon reimbursement restrictions and regulations. (Read more…)
Posted on November 13, 2020 by Dr. David Edward Marcinko MBA MEd CMP™
About iMBA, Inc
By Staff Reporters
iMBA Inc., is a healthcare consulting and financial planning analytics firm specializing in medical practice management and physician alignment.
Our mission is to empower physician colleagues and healthcare organizations to drive clarity, improve performance, and create accountability.
Our team combines a cross-section of skill-sets including public and population health, financial operations, business intelligence, and data science.
And, our diverse background of experience includes advanced academic training, economic and financial research, global marketing, management consulting, and entrepreneurial spirit.
SCHEDULE A MEDICAL PRACTICE & FINANCIAL PLANNING CONSULTATION TODAY!
Courtesy: https://lnkd.in/eBf-4vY
For Doctors – By Doctors – Confidential – Video Conference WEB: https://lnkd.in/eVGcji5
Posted on November 9, 2020 by Dr. David Edward Marcinko MBA MEd CMP™
The McCarran–Ferguson Act
By Howard Green MD
***
The McCarran–Ferguson Act, 15 U.S.C. §§ 1011-1015, is a United States federal law that exempts the business of insurance from most federal regulation, including federal antitrust laws to a limited extent.
***
The McCarran–Ferguson Act was passed by the 79th Congress in 1945 after the Supreme Court ruled in United States v. South-Eastern Underwriters Association that the federal government could regulate insurance companies under the authority of the Commerce Clause in the U.S. Constitution and that the federal antitrust laws applied to the insurance industry.
-United States Federal Law
***
Health Insurance industry redistributing unlimited cash from patient premiums into the Georgia US Senate run off election to prevent a Democrat Senate Majority from removing the health insurance exemption to Federal antitrust, monopoly, price fixing and collusion McCarran Ferguson laws.
Posted on October 25, 2020 by Dr. David Edward Marcinko MBA MEd CMP™
ProPublica
The thousands of “Trumpcare” ads Facebook and Google have published show that the shadowy “lead generation” economy has a happy home on the platforms — and even big names like UnitedHealthcare take part.
Posted on October 9, 2020 by Dr. David Edward Marcinko MBA MEd CMP™
The CDC has finally acknowledged that the coronavirus can be airborne
The news: The US Centers for Disease Control and Prevention has updated its guidelines to acknowledge that the coronavirus can be spread by tiny particles that linger in the air. The agency said it took the decision due to the mounting evidence that people with covid-19 can infect people even if they are more than six feet away, or shortly after the infected person left the area. These cases all occurred in poorly ventilated and enclosed spaces, and often involved activities that cause heavier breathing, like singing or exercise.
The significance: Evidence that airborne transmission is occurring has been mounting for months. The WHO still has not recognized airborne transmission as a significant factor in the pandemic and the CDC’s slowness to acknowledge it has caused frustration among aerosol researchers, some of whom say it is the main route for infections. The CDC maintains it only occurs in “limited, uncommon” circumstances. Airborne transmission has become a topic of fierce contention, partly due to the fact it makes it far riskier to reopen spaces like restaurants, gyms, bars, schools, and offices.
What do we do now? The CDC advises that people stay at least six feet away from others, wear a mask that covers their nose and mouth, frequently wash their hands, clean high-touch surfaces often, and stay home when they are feeling sick. However, the implications of airborne transmission mean the CDC perhaps ought to shift its emphasis and go further, advising people to properly ventilate buildings, limit the number of people indoors at any given time while encouraging them to stay further apart and masked, and try to socialize outdoors where possible. Read the full story.
Posted on October 3, 2020 by Dr. David Edward Marcinko MBA MEd CMP™
By Chad Mulvany
President Trump has signed into law the HR 8337, Short Term Continuing Resolution (CR) to fund the government through December 11.
The president’s action was expected after the Senate passed the bill earlier this week. Both sides of the aisle are eager to avoid a government shutdown prior to the election Nov. 3 and in the middle of a public health emergency.
The legislation includes provisions that relax the terms of the Medicare Advanced and Accelerated Payment Program (AAP) loans.
Now that the CR is signed into law, the AAP loan terms increased the repayment period to 29 months before a demand letter is submitted. During the 29-month period, there would be no claims offset for the first 12 months, a 25% payment offset for the next 11 months, and 50% offset for the final six months. The legislation would also reduce the interest rate applied to any funds outstanding after the initial 29-month period to 4%.
Source: Chad Mulvany
Healthcare Financial Management Association [10/1/20]
Posted on September 13, 2020 by Dr. David Edward Marcinko MBA MEd CMP™
Waived Co-Pays for United Healthcare Medicare Advantage Plans
By Jessica M. Wade, MHA, Practice Manager
Just to clarify, the UHC copay waiver info is listed clearly on the UHC website as follows: “Members will have a $0 copay for covered primary care provider (PCP) and specialist physician services, as well as other covered services (listed below) between May 11, 2020 until September 30, 2020″. By lowering our PCP and specialist copays to $0, along with our telehealth cost-share waiver, we hope to help make it easier for you to access care”
Services included
The following services, if covered by your plan, are eligible for a $0 copay under the cost-share waiver, but do not include diagnostic tests and certain other services.
• Primary care provider (PCP) office visits
• Specialist physician office visits
• Physician assistant or nurse practitioner office visits
• Medicare-covered chiropractic and acupuncture services
• Medical and Podiatry services and routine eye and hearing exams
• Physical therapy, occupational therapy and speech therapy
• Cardiac and pulmonary rehabilitation services
• Outpatient mental health and substance abuse visits
• Opioid treatment services
The $0 copay applies to services from a network provider and out-of-network services covered by the plan. Member cost-share is not waived for the
following services, unless they are related to COVID-19 testing or treatments:
• Lab and Diagnostic tests (radiological and non-radiological)
• Part B and Part D drugs
• Durable Medical Equipment, Prosthetics, Orthotics and Supplies
• Renal Dialysis
• Other services not covered by your plan
Co-pays, co-insurance and deductibles for services in the following settings are not waived. Members will be responsible for their share of the cost under their benefit:• Inpatient hospital and Outpatient surgery or observation services.
• Skilled Nursing Facilities
• Emergency, Urgent and Ambulance services
Furthermore, reimbursement is based on the Medicare fee schedule as these plans waiving copay are Medicare Advantage plans and subject
to Medicare guidelines and reimbursement models.
On August 4, 2020, CMS released the latest in a series of recently-published proposed rules, the Outpatient Prospective Payment System (OPPS) and Ambulatory Surgical Center (ASC) proposed rule for fiscal year (FY) 2021.
This proposed rule builds upon executive orders such as “Protecting and Improving Medicare for Our Nation’s Seniors,” signed by President Trump in October 2019 and Trump Administration initiatives such as “Patients Over Paperwork.” In a press release, CMS highlighted the proposed rule’s focus on increasing competition among providers to give patients more choice, lowering out-of-pocket surgery costs, increasing provider flexibility, and allowing patients to make more informed decisions about their care. (Read more…)













 ***
***
















































 ***
***




 ***
***