![]()
Consequences of the Accountable Care Act [PP-ACA]
By Dr. David Edward Marcinko MBA CMP™
[Editor-in-Chief]
 There is a fair amount of activity that will take place in the next 24 months in response to ICD-10 transition, healthcare reform, Accountable Care Act (ACA), meaningful use compliance and its financial incentives, and other regulatory issues that will require system or software upgrades to support the new efforts.
There is a fair amount of activity that will take place in the next 24 months in response to ICD-10 transition, healthcare reform, Accountable Care Act (ACA), meaningful use compliance and its financial incentives, and other regulatory issues that will require system or software upgrades to support the new efforts.
Some ACA Examples
As an example, The Affordable Care Act is sure to significantly alter reimbursement structures and delivery of care.
Below are several areas that will be affected:
- With the projected increase in patient volumes, the associated cost of about 62% will emanate from Medicare cuts: $162 Billion through reducing fee-for-service Medicare payments; $136 Billion from setting Medicare Advantage rates based on Fee-for-Service payments; and $36 Billion from cutting hospital Medicare/Medicaid disproportionate share.
- Compliance reviews will be increased through the Recovery Audit Contractors (RACs) where Centers for Medicare and Medicaid Services (CMS) expect to obtain $2.9 Billion in additional savings. With the RAC in place, hospitals and providers need to increase their focus and attention in improving documentation quality and validating medical necessity to substantiate their reviews.
- Reduced payments for readmissions and Medicare penalties for poor outcomes can and will affect the bottom line for both hospitals and providers in the future.
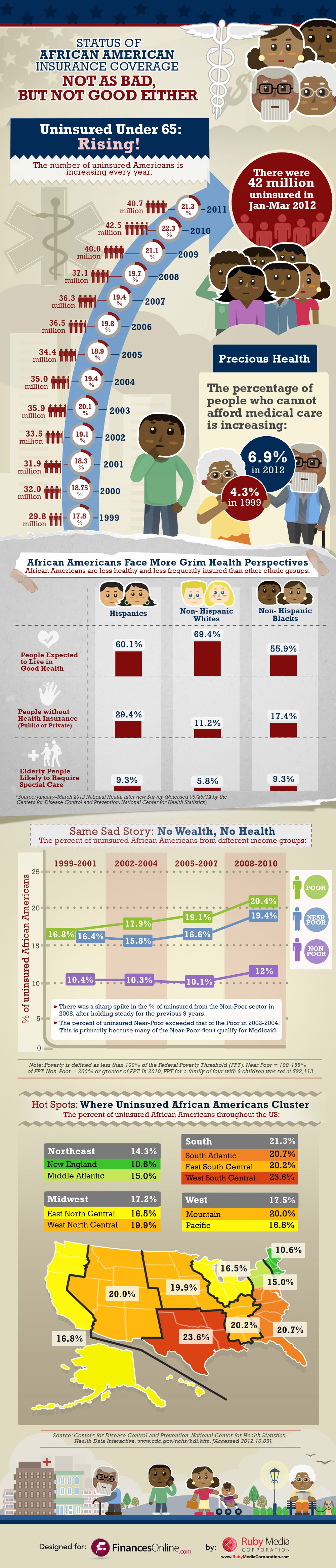
- By 2015, more than 19 million uninsured will receive coverage and in 2016, another 11 Million uninsured will be insured. This will create more patients per hospital/provider and will require more full-time equivalents to support the revenue cycle process of registration, documentation, billing and collection.
- With the ICD-10 conversion will create a more complex requirement for documenting diagnoses and will require software modifications for hospitals and providers as well as significant training.
###

[Our Forthcoming Book]
More:
- Healthcare Promises [aka ACA]
- With Obama Election Win “Mr. Market” Weighs in on the ACA Equity Winners and Losers
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
- PRACTICES: www.BusinessofMedicalPractice.com
- HOSPITALS: http://www.crcpress.com/product/isbn/9781466558731
- CLINICS: http://www.crcpress.com/product/isbn/9781439879900
- ADVISORS: www.CertifiedMedicalPlanner.org
- FINANCE: Financial Planning for Physicians and Advisors
- INSURANCE: Risk Management and Insurance Strategies for Physicians and Advisors
- Dictionary of Health Economics and Finance
- Dictionary of Health Information Technology and Security
- Dictionary of Health Insurance and Managed Care
![]()
![]()

Share this:

Filed under: Book Reviews, Health Insurance, Health Law & Policy | 2 Comments »