BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on October 2, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
LESSONS FROM THE RETAIL SECTOR
***
Discover how ProMedica uses customer feedback and a digital-first approach to consumers to achieve stellar results across more than 400 facilities in 28 states.
How much will it cost you to start a dental practice – with Business Plan?
There are many costs to consider to set up a successful dental practice. Note that the following values are not the exact amount but an average of setting up a dental practice:
Purchase price – this includes valuation fees of between $1,000-4,500, solicitor fees of between $4,000 – 17,000, accountancy and bank fees of around $3,000, and bank solicitors, which can be up to $3,500. Many of these can be reduced or obliterated.
Materials – $40,000
Lab fees – $36,000
Staff costs – $82,000
Other costs (associates fees) – [$245,000 – $295,000]
Other Factors
“Big” Tech – Many startup doctors want to include CBCT or CAD/CAM or 3D printing in their startup, any of which can add $25,000-$175,000. In other situations, waiting is the best option.
Cabinetry Preferences – Costs for cabinetry can range from $5,000 to $175,000.
Practice Management Software (PMS) – Pricing will range from a few thousand dollars to $25,000; OR none at all.
Mechanical Delivery – Typically referred to as chairs, lights, and units, this category of dental equipment costs will range between $5,000 and $100,000 based on your startup plans.
Vision – Ignore the so-called “experts” who will try to create a cookie-cutter model for your equipment costs. That is the thinking of corporate dentistry. You want a customized private practice vision that allows you to create a model matching your standards. Prioritize your vision, so your values and philosophy will lead your dental equipment budget and purchasing decisions. Your equipment budget will be—and should be—customized.
It has been well documented that the COVID-19 pandemic resulted in unprecedented increases in telemedicine utilization across the U.S. However, rural providers and patients, as evidenced by their lower rates of telemedicine usage during this time, have not been able to take advantage of the opportunities provided by telemedicine to the same extent as urban providers.
On August 18, 2021, the Health Resources and Services Administration (HRSA) of the Department of Health and Human Services (HHS) announced the latest attempt to ameliorate this issue – the distribution of nearly $20 million to 36 recipients for the purpose of strengthening telehealth services in rural and underserved communities and expanding innovation and quality. (Read more…)
Posted on September 28, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
90 NCQI MEASUREMENTS
BY ERIC BRICKER MD
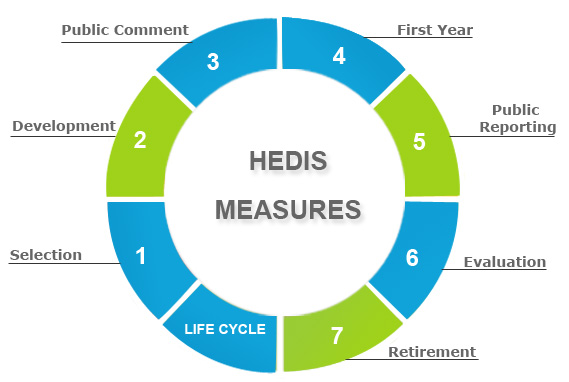
The Healthcare Effectiveness Data and Information Set (HEDIS) is a tool used by more than 90 percent of U.S. health plans to measure performance on important dimensions of care and service. More than 190 million people are enrolled in health plans that report quality results using HEDIS.
The National Committee for Quality Assurance is an independent 501 nonprofit organization in the United States that works to improve health care quality through the administration of evidence-based standards, measures, programs, and accreditation.
Posted on September 26, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
BY ENTREPRENUER MD AND ROBERT PEARL MD
In this episode the Entrepreneur MD is joined by Dr Robert Pearl, MD, to talk about his latest book Uncaring and the need to stand up against the current healthcare model.
Posted on September 24, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
HEALTHCARE ECONOMIST
By Eric Bricker MD
Uwe Reinhardt PhD was a Princeton Healthcare Economist Who Passed Away in 2017. He Was Possibly the Most Well Known Healthcare Economist in America and Even the World.
Posted on September 15, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
CONFLICTS OF INTEREST?
The New York Times Had an Excellent Article on the FDA on September 2, 2021.
The Article Described How the FDA Began Receiving Funding from the Pharmaceutical Industry Itself to Pay for FDA Employee Salaries in 1992–a Potential Conflict-of-Interest. Subsequently, a Study Found that 1/3 of Drugs Approved by the FDA Were Found to Have Safety Problems from 2000 -2010. Another Potential Conflict-of-Interest is Number of FDA Regulators Who Leave Their Positions to Take High-Paying Jobs at Pharmaceutical Companies.
There’s an aspect to retirement that many physicians do not plan for … the transition from work and practice to retirement. Your work has been an important part of your life. That’s why the emotional adjustments of retirement may be some of the most difficult ones.
For example, what would you like to do in retirement? Your retirement vision will be unique to you. You are retiring to something not from something that you envisioned. When you have more time, you would like to do more traveling, play golf or visit more often, family and friends. Would you relocate closer to your kids? Learn a new art or take a new class? Fund your grandchildren’s education? Do you have philanthropic goals? Perhaps you would like to help your church, school or favorite charity? If your net worth is above certain limits, it would be wise to take a serious look at these goals. With proper planning, there might be some tax benefits too. Then you have to figure how much each goal is going to cost you.
If have a list of retirement goals, you need to prioritize which goal is most important. You can rate them on a scale of 1 to 10; 10 being the most important. Then, you can differentiate between wants and needs. Needs are things that are absolutely necessary for you to retire; while wants are things that still allow retirement but would just be nice to have.
Recent studies indicate there are three phases in retirement, each with a different spending pattern [Richard Greenberg CFP®, Gardena CA, personal communication]. The three phases are:
The Early Retirement Years. There is a pent-up demand to take advantage of all the free time retirement affords. You can travel to exotic places, buy an RV and explore forty-nine states, go on month-long sailing vacations. It’s possible during these years that after-tax expenses increase during these initial years, especially if the mortgage hasn’t been paid off yet. Usually the early years last about ten years until most retirees are in their 70’s.
Middle Years. People decide to slow down on the exploration. This is when people start simplifying their life. They may sell their house and downsize to a condo or townhouse. They may relocate to an area they discovered during their travels, or to an area close to family and friends, to an area with a warm climate or to an area with low or no state taxes. People also do their most important estate planning during these years. They are concerned about leaving a legacy, taking care of their children and grandchildren and fulfilling charitable intent. This a time when people spend more time in the local area. They may start taking extension or college classes. They spend more time volunteering at various non-profits and helping out older and less healthy retirees. People often spend less during these years. This period starts when a retiree is in his or her mid to late 70’s and can last up to 20 years, usually to mid to late-80’s.
Late Years. This is when you may need assistance in our daily activities. You may receive care at home, in a nursing home or an assisted care facility. Most of the care options are very expensive. It’s possible that these years might be more expensive than your pre-retirement expenses. This is especially true if both spouses need some sort of assisted care. This period usually starts when the retiree is their 80’s; however they can sometimes start in the mid to late 70’s.
If early retirement is a major objective, start thinking about activities that will fill up your time during retirement. Maintaining your health is more critical, since your health habits at this time will often dictate how healthy you will be in retirement.
Planning Issues – Mid Career
If early retirement is a major objective, start thinking about activities that will fill up your time during retirement. Maintaining your health is more critical, since your health habits at this time will often dictate how healthy you will be in retirement
Planning Issues – Late Career
Three to five years before you retire, start making the transition from work to retirement.
Try out different hobbies;
Find activities that will give you a purpose in retirement;
Establish friendships outside of the office or hospital;
Discuss retirement plans with your spouse.
If you plan to relocate to a new place, it is important to rent a place in that area and stay for few months and see if you like it. Making a drastic change like relocating and then finding you don’t like the new town or state might be very costly mistake. The key is to gradually make the transition.
Current reimbursement structures involve the submission and payment of medical CPT® coded claims. But, some doctors feel they need to “up-code” to maximize revenue or “down-code” for fear of having a claim denied. Contradictory business goals bastardize the system into a payer versus provider tug-of-war, with patient care as a potential bargaining chip. Instituting quality metrics should be included in this equation and, a hybrid reimbursement model may be a viable option while integrating quality care metrics and reducing costs for all stakeholders.
This hybrid reimbursement system might use a two-payment structure.
For the first payment, claims would be paid at hypothetical rate of 60% within one week of submission.
The second payment, consisting of the remaining zero to 40% of some total maximum allowable fee, be paid quarterly. It would be based on scores like patient satisfaction and stewardship of healthcare resources by analyzing a statistically valid sample of patient encounters taken from the electronic health record.
Such a hybrid system would remove unnecessary steps, like re-submitting claims, and would lower the operational and administrative costs of claims processing. These changes would decrease operational cost and drive quality stewardship of the healthcare dollar.
Physicians Beware … the Medical Management Consultants?
Are you a doctor desperate for practice enhancement solutions, but don’t know where to turn for help? Or, maybe you’ve already had a bad experience with a non-fiduciary business consultant, or management guru, more interested in his bottom line than your success?
Posted on August 28, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
ANTI-KICKBACK STATUTEOverview and Impact
Do you want to learn more about the Stark Law and Anti-Kickback Statute Final Rules and how they impact your practice? Join us for a one-hour webinar, presented with Hancock Daniel.
Historically, Medicare has offered value-based payment models to healthcare organizations on both a voluntary and a mandatory participation basis. Because voluntary participants could self-select into programs to reduce spending, it was assumed that they achieved greater savings than mandated participants, but until recently, no data had tested this.
However, a June 2021 study in the Journal of the American Medical Association (JAMA) found no difference in risk-adjusted episodic spending between voluntary and mandatory payment model participants. (Read more…)
Use National Financial Awareness Day to your Advantage
Aug. 14th is National Financial Awareness Day. Financial awareness is about more than just understanding the basics on how money works. It’s also about evaluating your own budget, savings and investments to make sure your finances are working for your needs.
So if it’s been a while since your last financial “check up,” National Financial Awareness Day can be the extra push you’ve needed to finally take a look under the hood.
On July 13, 2021, the Centers for Medicare & Medicaid Services (CMS) released its proposed Medicare Physician Fee Schedule (MPFS) for calendar year (CY) 2022.
In addition to numerous payment updates in the MPFS, such as significant updates to the Merit-based Incentive Payment System (MIPS), new policies may preserve expanded telemedicine services through 2023 and clinicians may incur more difficulty earning bonuses under the Quality Payment Program (QPP) eligibility threshold. CMS also includes in the proposed rule a request for information to address COVID-19 vaccine reimbursement proposals. (Read more...)
Posted on August 4, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
***
TEXTBOOKREVIEW
Drawing on the expertise of decision-making professionals, leaders, and managers in health care organizations, Hospitals & Health Care Organizations: Management Strategies, Operational Techniques, Tools, Templates, and Case Studies addresses decreasing revenues, increasing costs, and growing consumer expectations in today’s increasingly competitive health care market.
Offering practical experience and applied operating vision, the authors integrate Lean managerial applications, and regulatory perspectives with real-world case studies, models, reports, charts, tables, diagrams, and sample contracts. The result is an integration of post PP-ACA market competition insight with Lean management and operational strategies vital to all health care administrators, comptrollers, and physician executives. The text is divided into three sections:
Managerial Fundamentals
Policy and Procedures
Strategies and Execution
Using an engaging style, the book is filled with authoritative guidance, practical health care–centered discussions, templates, checklists, and clinical examples to provide you with the tools to build a clinically efficient system. Its wide-ranging coverage includes hard-to-find topics such as hospital inventory management, capital formation, and revenue cycle enhancement. Health care leadership, governance, and compliance practices like OSHA, HIPAA, Sarbanes–Oxley, and emerging ACO model policies are included. Health 2.0 information technologies, EMRs, CPOEs, and social media collaboration are also covered, as are 5S, Six Sigma, and other logistical enhancing flow-through principles. The result is a must-have, “how-to” book for all industry participants.
In 2020, at the request of the U.S. House Committee on Ways and Means (the Committee), the Medicare Payment Advisory Commission (MedPAC) began investigating the role that private equity (PE) plays in healthcare provided to Medicare beneficiaries.
In its June 2021 “Report to the Congress on Medicare and the Health Care Delivery System,” MedPAC included for the first time a chapter on PE’s effect on Medicare, wherein it discussed the findings and observations from its investigation and answered a number of questions posed by the Committee. This Health Capital Topics article will analyze MedPAC’s answers to those questions, review its investigation of PE’s role in healthcare, and summarize reactions from stakeholders.(Read more…)
On July 19, 2021, CMS released the proposed rule for the Outpatient Prospective Payment System (OPPS) and Ambulatory Surgery Centers (ASCs) for calendar year (CY) 2022. The proposed rule builds on President Joe Biden’s July 9, 2021 executive order on “Promoting Competition in the American Economy,” as it relates to increasing access and price transparency in the healthcare industry.
In a press release regarding the proposed rule, CMS stated their commitment to addressing the persistent health inequities in the U.S. and finding opportunities to improve data collection that will lead to policy changes to help meet the health needs of patients. (Read more…)
Posted on July 30, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
15 Self-Funded Employers Analyzed Their Pharmacy Claims Data in Conjunction with the Commonwealth Fund and Discovered the Following Regarding their PBM FormularIES
There is Copay for Each Office Visit and Visits are Unlimited.
Direct Primary Care Doctors Are Most Frequently Family Practice Physicians, but Internal Medicine and Pediatricians Can Also Have Direct Primary Care Practices.
The Average Direct Primary Care Practice Has a Panel of 345 Patients, with a Goal of About 600 Patients at Full Capacity.
For Comparison, the Typical Fee-for-Service Primary Care Doctor Has a Patient Panel of 2,500.
57% of Direct Primary Care Practices Contract with Employers That Pay the Monthly Membership on the Employee’s Behalf.
Direct Primary Care is a Strategy to Increase the Quality of Care and Decrease Healthcare Costs for an Employee Health Plan.
Disclaimer: Dr. Bricker is the Chief Medical Officer of Virtual Care Company First Stop Health.
Health Insurance Carriers Are Misaligned by Owning PBMs That Make More Money in Rebate Kick-Backs When the Employee Health Plan Spends More Money on Expensive Prescription Drugs.
Doctors Are Misaligned When They *Are Employed by Hospitals That Tie Test and Procedure Ordering Volume to Doctor Compensation.
Hospitals are Misaligned When They Buy Physician Practices and Raise the Prices for In-Office Testing and Procedures by 300%… Even Though NOTHING Has Changed Other Than the Sign on the Door.
Accordingly, True Employee Health Plan Innovation is ALIGNMENT Innovation That Provides Care Outside the of the Status Quo Fee-for-Service System.
Onsite Clinics, Near Site Clinics, Direct Primary Care and Capitated Virtual Care All Provide Real Alignment Innovation for Employee Health Plans.
Recruitment has become a refined art in recent years as practices and physicians themselves grow increasingly savvy about the finer points of marketing positions and securing employment. It’s more competitive than ever, too. Many organizations are going after the same physicians. Add to that a shortage of doctors in key specialties and certain geographical areas and the pressure becomes that much more intense. Moreover, the aging of the physician workforce, their increased dissatisfaction with managed care, and changes in doctors’ work expectations (they want more free time) have affected the demand and supply.
Additionally, both practicing physicians and residents fresh out of training have become more discerning and skillful in managing the search process. Candidates have learned to be selective based on how they’re treated on the phone, how they’re treated in person during site visits, or how smoothly the negotiations go. One small bump in the road and they could choose to go elsewhere. In truth, they look to rule organizations out, not in.
Even the smallest of practices must have an effective recruitment plan because they compete directly with the big guys — larger practices and hospitals that have polished their efforts and perfected their processes.
Facts about Physician Recruiters and Executive Search Firms
1) If you are job hunting, you should send your resume to recruiters
Different recruiters know about different positions. They do not usually know about the same ones. This is particularly true with retained firms. By sending your resume out widely, you will be placed in many different confidential databases and be alerted of many different positions. If you send your resume to only a few, it may be that none you send to will be working with positions which are suited for you. Throw your net widely.
If you change jobs, it is also wise to send follow-up letters to the recruiters and alert them of your new career move. Many search firms follow people throughout their careers and enjoy being kept up-to-date. It is a good idea to have your resume formatted in plain text so you can copy and paste it into email messages when requested to do so. Then, follow up with a nicely formatted copy on paper by postal mail.
Some estimate that only 1% to 3% of all resumes sent will result in actual job interviews. So, if you only send 50 resumes, you may only have less than 2 interviews, if that many. Send your resume to as many recruiters as you can. It is worth the postage or email time. Generally, recruiters will not share your resume with any employer or give your name to anyone else without obtaining your specific permission to do so. The recruiter will call first, talk to you about a particular position and then ask your permission to share your resume with that employer.
2) Your resume will be kept strictly confidential by the executive search firm.
It is safe to submit your resume to a search firm and not worry that the search firm will let it leak out that you are job hunting. Recruiters will call you each and every time they wish to present you to an employer in order to gain your permission. Only after they have gained your permission will they submit your name or resume to the identified employer. The wonderful aspect of working with search firms is that you can manage your career and your job search in confidence and privacy.
3) Fees are always paid by the employer, not the job candidate.
Recruiters and search firms work for the employer or hiring entity. The employer pays them a fee for locating the right physician for the job opening. This is important to remember, in that when you interact with executive recruiters, you are essentially interacting with an agent or representative of the employer. Recruiters are more loyal to employers than they are to job candidates because they work for the employer. This should not present a problem, but, should cause you to develop your relationship with the recruiter with the same integrity and professionalism that you would with the employer.
Recruiters are paid fees in one of two ways – retainer fees or contingency fees. This is an important distinction and will affect your process with both the employer and the recruiter. Some employers prefer working with contingency firms and some with retained firms. Both are respected by employers and useful in your job search, but, the two types of firms will not be handling the same positions with the same employers simultaneously.
A “retained” recruiter has entered an exclusive contract with an employer to fill a particular position. The retained recruiter, then, is likely to advertise a position, sharing the specifics of the position, location and employer openly. The retained firm feels a great obligation to fulfill the contract by finding the best person for the job.
A “contingency recruiter” on the other hand, usually does not have an exclusive relationship with the employer, and is only paid a fee if the job search is successful. Often, if the employer uses contingency firms, there will be more than one contingency firm competing to fill a certain position. As a job hunter, if you are sent to an interview by a contingency firm, you may find that you are competing with a larger number of applicants for a position. Generally, retained firms only send in from 3 to 5 candidates for a position.
Recruiters will be paid fees equal to about 25% to 35% of the resulting salary of the successful candidate plus expenses. This does not come out of the job candidate’s salary. This is paid to the recruiter through a separate relationship between the employer and the search firm. This may seem like a large fee, but, keep in mind that recruiters incur a great many expenses when searching for successful job candidates. They spend enormous amounts of money on computer systems, long distance calls, mail-outs, travel and interviews. Recruiters work very hard for these fees. Employers recognize the value of using recruiters and are more than willing to pay recruiters the fees. All you have to do is contact the recruiter to get the process moving.
4) Not all medical recruiters work only with physicians.
Some search firms work exclusively with physicians or in healthcare, while others may work in several fields at once. Some of the larger generalist firms will have one or more search consultants that specialize in healthcare. It is important for you, as a job hunter, to assess the recruiters’ knowledge of your field. If you use industry or medical specialty buzz words in describing your skills, experience or career aspirations, you may or may not be talking a language the recruiter understands fully. It is wise to explore fully with the recruiter his understanding of your field and area of specialization.
5) Recruiters and search consultants move around.
Recruiters, like many professionals, move to new firms during their careers. Often you will find that recruiters will work at several firms during their careers. Since it is much more effective to address your letters to a person rather than “to whom it may concern”, it is smart for job hunters to have accurate and up-to-date information about who is who and where, since this can change frequently. Search firms also move their offices, sometimes to another suite, street or state. If you have a list of recruiters that is over one year old, you will certainly waste some postage in mailing your resumes and cover letters. Many of your mail-outs will be returned to you stamped “non-deliverable”, unless you obtain an up-to-date list. A resource, like the Directory of Healthcare Recruiters is updated very frequently, usually monthly [www.pohly.com/dir3.html].
6) Most search firms work with positions all over the country.
If you are from a particular state, and want to remain in that state, don’t make the mistake of only sending your resume to recruiters in your state. Often the recruiters in your state are working on positions in other states, and recruiters in other states are working on positions in your state. This is usually the case. Very few recruiters work only in their local area, most work all around the US and some internationally. Regardless of your geographic preference, you should still send your resume to all the healthcare recruiters. If you really only want to remain in your area, you can specify that preference in your cover letter.
7) Recruiters primarily work with hard to fill positions or executive positions.
Some recruiters specialize in clinical positions for physicians, managed care executive positions, healthcare financial positions or health administration positions. Others may specialize in finding doctors, nurses or physical therapists. Generally, an employer does not engage a recruiter’s assistance in filling a position unless it is hard to fill. Sometimes employers will engage search firms to save them the valuable time of advertising or combing through dozens of resumes.
Contingency recruiters tend to work with more mid-level management and professional positions, but, this is not always the case. Retained firms generally work with the higher level clinical or administrative positions.
One thing you will be assured of is that if a recruiter is working on a position that means that the employer is willing to pay a fee. That usually means that the position is a valued position and one worth closer inspection on your part. Even in healthcare, with certain exceptions, our economy is an “employer’s market”. This means that employers receive a deluge of resumes for their open positions. Increasingly, employers are using recruitment firms to handle their openings and schedule the interviews because employers simply do not have the manpower or time to handle the many resumes they receive. Therefore, if a job hunter is submitted by a recruiter, that job hunter has a great advantage over all other applicants.
–The Private Equity Firm Offers an Up Front Lump Sum of Money and Administrative Services Such as Billing and Collections for the Practice.
–In Return, the Doctors in the Practice Agree to Have 30-40% of All Future Revenue Go to the Private Equity Firm.
The Up Front Lump Sum Can Be Equal to as Much as 10 – 20 Years of Income for a Physician.
The Older Doctors in the Practice Who Are Usually the Partners Frequently Take This Deal, Resulting in the Younger Partners Making Less Take-Home Pay.
Implication for Employers:
Private Equity Firms Create Larger Group Practices to Have Better Negotiating Leverage with Commercial Insurance Carriers and Obtain Higher Fee-for-Service Reimbursement.
Overall Healthcare Costs for Physician Services Go Up, While the Take-Home Pay for Doctors Goes Down… and the Private Equity Firm Keeps the Difference.
NOTE: The Older Doctors Who Are Paid the Lump Sum Are Still Required to Stay at the Practice for a Certain Number of Years After the Transaction.
Posted on July 7, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
BOOK REVIEW
BY ERIC BRICKER MD
Our Brains Have a Reward Chemical Called Dopamine That Causes a Brief Pleasurable Feeling Followed by a Worsening of our Mood.
However, Our Brains Also Have a Contentment Chemical Called Serotonin That Causes Peace and a Calming of our Mood.
Substances and Behaviors That Stimulate Dopamine Include: Sugar, Caffeine, Alcohol, Nicotine, Illicit Drugs, Prescription Narcotics, Social Media Apps, Gambling and Sex.
Substances and Behaviors That Stimulate Serotonin Include: The Amino Acid Tryptophane, Positive Relationships with Others, Service to Others, Prayer and Meditation.
Corporations Tailor Their Products with Dopamine Stimulating Strategies to Increase Sales.
Facebook’s Chamath Palihapitiya Even Admitted on CNBC that Facebook Intentionally Designed its Social Media Platform to Stimulate Dopamine in the User’s Brain To Make Them Use the App More.
Unfortunately, the Constant Stimulation of Dopamine in Our Brains Has Increased Obesity, Metabolic Syndrome, Cancer, Cardiovascular Disease, Diabetes and Depression.
Lustig Estimates That 75% of the $4 Trillion Spent on US Healthcare is for These Diseases That Can Be Traced to Our ‘Hacked Minds.’
Posted on July 2, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
ELECTRIC HEALTH RECORDS
By White Hat Anonymous
Epic Systems, the country’s leading e-health record company, says an algorithm it developed can accurately flag sepsis in patients 76% of the time. The life-threatening disease, which arises from infections, is a major concern for hospitals: One-third of patients who die in hospitals have sepsis, per the CDC.
Generally, the earlier sepsis is diagnosed and treated, the better a patient’s chances of survival—and hundreds of hospitals use Epic Systems’s sepsis prediction model, The Verge reports.
The problem: According to a study published this week in JAMA Internal Medicine, Epic Systems may have gotten the success rate wrong: The model is only correct 63% of the time—“substantially worse than the performance reported by its developer,” the researchers wrote.
Part of the issue can be traced to the algorithm’s development, Stat News reports. It was trained to flag when doctors would submit bills for sepsis treatment—which doesn’t always line up with patients’ first signs of symptoms.
“It’s essentially trying to predict what physicians are already doing,” Dr. Karandeep Singh, study author.
When reached for comment, Epic Systems told us the researchers’ hypothetical scenario lacked “the required validation, analysis, and tuning that organizations need to do before deployment,” adding that the JAMA study’s findings differed from other research.
Posted on June 23, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
OVER HEARD IN THE DOCTOR’S LOUNGE
The financial planner is a like juggler, trying to keep a variety of balls simultaneously in the air. Each aspect of practice becomes critical, just as action is needed.
Some of the activities of operating a successful financial planning practice generally attract more attention than others, such as marketing and advertising, closing engagements, and office administration. Because product review, selection and implementation are often related to advisor compensation, they attract a great deal of the financial juggler’s concentration.
But, the heart of financial planning, niche advice, often receives little attention. Not because it is unimportant, it just doesn’t seem immediately and predictably urgent. Here, that ball does not seem to be dropping so rapidly.
However, retaining clients and receiving referrals from other professionals is very dependent on the quality of the advice delivered. And, the first line of protection from practitioner liability exposure is to not deliver incorrect or incomplete advice.
But, where does the financial advisor turn for ideas and organized research in the healthcare sector?
Posted on June 18, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Important Economic Concepts to UNDERSTAND
BY ERIC BRICKER MD
One of Their Applications Pertains to the Impact on Time Spent Working Vs. Time Spend on Leisure if a Healthcare Worker’s Pay is Changed.
DEFINITION: The INCOME EFFECT States That If a Worker’s Pay is Decreased, They Will Work More Hours to Maintain the Same Income. Conversely, If a Worker’s Pay is Increased, They Will Work Fewer Hours and Still Maintain the Same Income.
A Real-World Example of the Income Effect is When Medicare Decreased Reimbursement for Echocardiograms and as a Result, Decreased Cardiologists’ Pay. Accordingly, Cardiology Practices Increased the Number of Patients They Saw Per Day to Make Up for the Lost Pay and Maintain Their Income.
The SUBSTITUTION EFFECT States That Work and Leisure Time Have OPPORTUNITY COSTS for Each Other.
If a Worker’s Pay Goes Up, then the Opportunity Cost for Leisure (i.e. Not Working) Also Goes Up and the Worker Will Work MORE, Not LESS. Conversely, If a Worker’s Pay Goes Down, then the Opportunity Cost for Leisure Goes Down and the Worker Will Work LESS, Not MORE.
Whether the Income or Substitution Effect Dominates Depends on the Person and the Situation.
THE POINT: In the World of Fee-for-Service Reimbursement, a Decrease in Doctor Pay Per Service May Result in Doctors Providing More Services In Order to Maintain Their Income… Nullifying Any Cost-Savings.
Example 1: Dr. Kurt purchases an automobile for $15,000.
His hospital business use is 80% and he drives 20,000 total miles per year. Operating costs for the year, including gasoline, oil, insurance, maintenance, repairs, and license fees, are $4,000. If Kurt owns the car for five years, ownership will cost $35,000 ($4,000 x 5 = $20,000, $20,000 + $15,000 = $35,000), or $7,000 per year. For, each personal use mile costs $1.75 (100% -80% = 20%, 20% x 20,000 miles = 4,000 miles, $7,000/4,000 miles = $1.75). Kurt’s employer reimburses him 34.5 cents per mile for the business-related miles. As a result, the business use of the car is only partially reimbursed (16,000 business miles x 34.5 cents = $5,520).
However, the business usage costs Kurt $5,600(80% of $7,000). Kurt subsidizes the employer 9.25 cents per mile ($7,000 – $5,520 = $1,480, $1,480 /16,000 = 9.25 cents). Kurt’s total cost of ownership is $1.84 per mile, or $36,850 ($1.88 x 20,000 personal miles over the five-year life).
Example 2: Dr. Ben uses a hospital employer-provided vehicle 4,000 miles per year in 2003.
He reimburses the employer 34.5 cents per mile. His cost for five years is $6,900 (5y x 4,000 = 20,000 miles, 20,000 miles x 34.5 = $6,900).
Beginning on January 1st 2013, the standard mileage rates for the use of a car (also vans, pickups or panel trucks) were:
56.5 cents per mile for business miles driven
24 cents per mile driven for medical or moving purposes
14 cents per mile driven in service of charitable organizations
Note the dramatic contrast, from the employee’s perspective, between the above two examples, of the company reimbursing the employee for business use of his personal car, versus the employee reimbursing the company for personal use of the vehicle.
The business, medical, and moving expense rates decrease one-half cent from the 2013 rates. The charitable rate is based on statute.
Posted on June 15, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
BY ERIC BRICKER MD
[Book Review]
***
The Technology Adoption Lifecycle Was Explained in Geoffrey Moore’s Famous Book ‘Crossing the Chasm.‘
If You Are a Healthcare Entrepreneur or Innovator Your MUST Understand and Apply the Technology Adoption Lifecycle.
It States that Disruptive Innovation (i.e. Innovations that Require Behavior Change) Is Not Evenly Adopted Across a Population.
Rather, People Segment Themselves into Sub-Groups That Adopt the New Innovation Differently. To Whit:
**************
Early AdoptersLove Tinker and Like New Innovations Just Because They Are New. Early Adopters Tend to Not Be Price-Sensitive.
PragmatistsHave a Specific Problem that the New Innovation Will Solve and If They See Other People Using It, They Will Use It Too. Pragmatists Are Somewhat Price-Sensitive.
Conservatives Would Rather Not Adopt the New Innovation, but if it is Already Built-in to Something They Already Buy, Then They Will Be More Likely to Use It. Conservatives are Very Price Sensitive.
Skeptics Will Never Adopt the New Innovation.
**************
To Spread a New Innovation, One Must Cross the Chasm Between the Early Adopters and Pragmatists With a ‘Niche‘ and ‘Bowling Pin‘ Strategy.
Each generation of doctors and medical professionals is extraordinarily complex, bringing various skills, expertise and expectations to the modern medical work environment. Determining the best method to unite such diverse thinking is one of the many challenges faced by physician executives and healthcare leaders today.
And, as linguistic evolution occurs, the nomenclature of hospitalist was followed by that of intensivist, proceduralist and nocturnalist, etc [www.MedInnovationBlog.com and Personal communication Richard L. Reece MD].
Is it any wonder that many medical leaders and executive in the Baby Boomer generation find themselves at a loss? The days of functional leadership are gone and suddenly, no one cares about the expertise of the Baby Boomers or how they climbed the corporate ladder, in medicine or elsewhere. Leadership in the new era is no longer about command-control or dictating with intense focus on the bottom line; it is about collaboration, empowerment and communication. And, it is not about titles and nomenclature; it is about lifestyle choice.
What else drives these new-wave specialists?
The answer, of course, is the next-generation of physicians and their emerging new medical business and practice models, which include:
“Ambulists” are doctors that travel locally, have no, or only a sparse physical office presence of their own. They sporadically provide services that are additive to traditional practice models [i.e., endocrinologist in a large family medical office with many diabetics].
“In-Situ” physicians regularly provide services that are complimentary to existing traditional practice models [i.e., dentists or podiatrists in a medical practice].
“Laborists” are obstetricians that do not wish to be on-call. First begun in Cape Cod and other Massachusetts hospitals, such obstetricians work regular shifts for the sole purpose of delivering babies.
“Locum Tenens” doctors travel around the country as itinerants [i.e., cruise ships] as temporary substitutes for another the same specialty.
“Officists” remain in their own physical practice, and rarely see patients in the hospital, nursing home, patient home, out-patient facility, etc.
Finally, “dayhawk physicians” mimic the “nighthawk physician” model where radiologists in remote locations read films in the middle of the night as cash-strapped hospitals often find it cheaper to outsource with better services and more timely interpretations in many cases.
To start, let us all recall the Canadian physician Sir William Osler MD, one of the founders of Johns Hopkins Hospital in my hometown of Baltimore Maryland, and where I played stickball in the parking lot as a kid. He left a sizeable body of wisdom that has guided many physicians in the practice of medicine. So, allow me to share with you some of that accumulated wisdom and the quotes that have served me well over the years.
From Dr. Osler, I learned the art of putting myself in the patient’s shoes. “The motto of each of you as you undertake the examination and treatment of a case should be ‘put yourself in his place.’ Realize, so far as you can, the mental state of the patient, enter into his feelings.” Osler further stresses that we should “scan gently (the patient’s) faults” and offer the “kindly word, the cheerful greeting, the sympathetic look.”1
“In some of us, the ceaseless panorama of suffering tends to dull that fine edge of sympathy with which we started,” writes Osler in his famous essay “Aequanimitas.”2 “Against this benumbing influence, we physicians and nurses, the immediate agents of the Trust, have but one enduring corrective — the practice towards patients of the Golden Rule of Humanity as announced by Confucius: ‘What you do not like when done to yourself, do not do to others.’”
Medicine can be both art and science as many physicians have discovered. As Osler tells us, “Errors in judgment must occur in the practice of an art which consists largely of balancing probabilities.”2 Osler notes that “Medicine is a science of uncertainty and an art of probability” and also weighs in with the idea that “The practice of medicine is an art, based on science.”3,4
Osler emphasized that excellence in medicine is not an inheritance and is more fully realized with the seasoning of experience. “The art of the practice of medicine is to be learned only by experience,” says Osler. “Learn to see, learn to hear, learn to feel, learn to smell, and know that by practice alone can you become expert.”5
Finally, some timeless wisdom on patient care came from Osler in an address to St. Mary’s Hospital Medical School in London in 1907: “Gain the confidence of a patient and inspire him with hope, and the battle is half won.”6
***
***
Osler has also imparted plenty of advice on the business of medicine. In “Aequanimitas,” Osler says there are only two types of doctors: “those who practice with their brains, and those who practice with their tongues.”7
In a valedictory address to medical school graduates at McGill University, Osler suggested treating money as a side consideration in a medical career.8 “You have of course entered the profession of medicine with a view of obtaining a livelihood; but in dealing with your patients let this always be a secondary consideration.”
“You are in this profession as a calling, not as a business: as a calling which exacts from you at every turn self-sacrifice, devotion, love and tenderness to your fellow man,” explains Osler in the address to St. Mary’s Hospital Medical School.6 “Once you get down to a purely business level, your influence is gone and the true light of your life is dimmed. You must work in the missionary spirit, with a breadth of charity that raises you far above the petty jealousies of life.”
It is not easy for doctors to combine a passion for patient care, a knowledge of science and the maintenance of business, according to Osler in the British Medical Journal.9 “In the three great professions, the lawyer has to consider only his head and pocket, the parson the head and heart, while with us the head, heart, and pocket are all engaged.”
While some aspects of practice may fall short or be devoid of appropriate financial remuneration, the giving of one’s time, expertise and experience in improving patient outcomes and the quality of their lives may be the greatest gift. “The ‘good debts’ of practice, as I prefer to call them … amount to a generous sum by the end of each year,” says Osler.9
And so, as you practice medicine and reflect on your career, always remember the words and wisdom of Dr. William Osler, and keep patient welfare as your first priority.
References
1. Penfield W. Neurology in Canada and the Osler centennial. Can Med Assoc J. 1949; 61(1): 69-73
2. Osler W. Aequanimitas. Chapter 9, P. Blakiston’s Son and Co., Philadelphia, 1925, p. 159
3. Bean WB. William Osler: Aphorisms, CC Thomas, Springfield, IL, p. 129.
4. Osler W. Aequanimitas. Chapter 3, P. Blakiston’s Son and Co., Philadelphia, 1925, p. 34
5. Thayer WS. Osler the teacher. In: Osler and Other Papers. Johns Hopkins Press, Baltimore, 1931, p. 1.
6. Osler W. The reserves of life. St. Mary’s Hosp Gaz. 1907;13 (1):95-8.
7. Osler W. Aequanimitas. Chapter 7, P. Blakiston’s Son and Co., Philadelphia, 1925, p. 124
8. Osler W. Valedictory address to the graduates in medicine and surgery, McGill University. Can Med Surg J. 1874; 3:433-42.
9. Osler W. Remarks on organization in the profession. Brit Med J. 1911; 1(2614):237-9.