The RLH – From Concept to Action
[By Staff Reporters]
According to Greene, Reid and Larson, clinicians and health systems are facing widespread challenges, including changes in care delivery, escalating health care costs, and the need to keep up with rapid scientific discovery.
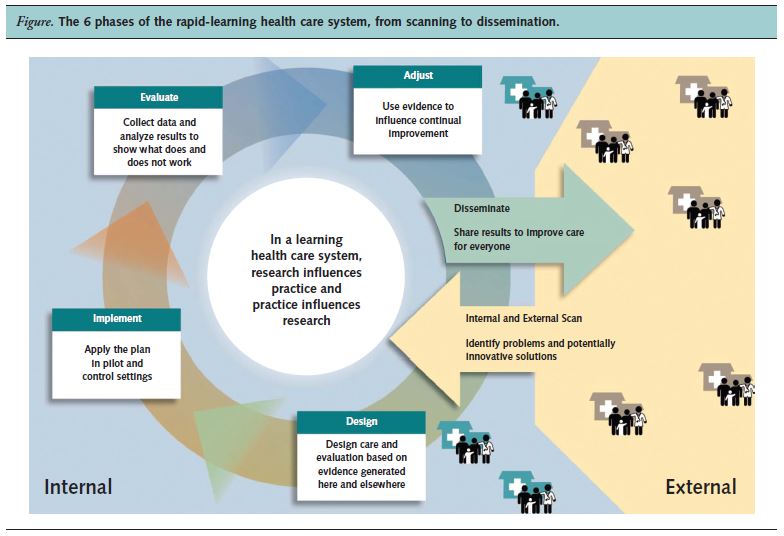
Re-organizing U.S. health care and changing its practices to render better, more affordable care requires transformation in how health systems generate and apply knowledge. The “rapid-learning health system” is posited as a conceptual strategy to spur such transformation – leverages and recent developments in health information technology and a growing health data infrastructure to access and apply evidence in real time, while simultaneously drawing knowledge from real-world care-delivery processes to promote innovation and health system change on the basis of rigorous research.
***
[A Rapid Learning Health System]
***
The Essay
This article describes an evolving learning health system at Group Health Cooperative, the 6 phases characterizing its approach, and examples of organization-wide applications.
Link: http://www.ncbi.nlm.nih.gov/pubmed/22868839
It is a practical model that promotes bidirectional discovery and an open mind at the system level, resulting in willingness to make changes on the basis of evidence that is both scientifically sound and practice-based.
Assessment
Rapid learning must be valued as a health system property to realize its full potential for knowledge generation and application.
Citation
Implementing the learning health system: from concept to action. Greene SM1, Reid RJ, Larson EB. Author information: Group Health Cooperative, 320 Westlake Avenue North, GHQ E2N, Seattle, WA 98109, USA. greene.sm@ghc.org
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
More:
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
More: http://onlinelibrary.wiley.com/doi/10.1002/hast.134/abstract
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
- PRACTICES: www.BusinessofMedicalPractice.com
- HOSPITALS: http://www.crcpress.com/product/isbn/9781466558731
- CLINICS: http://www.crcpress.com/product/isbn/9781439879900
- ADVISORS: www.CertifiedMedicalPlanner.org
- FINANCE: Financial Planning for Physicians and Advisors
- INSURANCE: Risk Management and Insurance Strategies for Physicians and Advisors
- Dictionary of Health Economics and Finance
- Dictionary of Health Information Technology and Security
- Dictionary of Health Insurance and Managed Care

![]()
Share this:

Filed under: Career Development, Experts Invited, Glossary Terms, iMBA, Information Technology | Tagged: . Greene SM1, Group Health Cooperative, Larson EB, rapid-learning health system, Reid RJ | 3 Comments »