Establishing the Way-Forward
[By Dr. David Edward Marcinko MBA CMP™]
 Medical practices today are operating in a new or next-generation practice management environment. There are significant pressures on physicians to increase, or at least maintain revenues and bottom line profits. These pressures are coming from many sources.
Medical practices today are operating in a new or next-generation practice management environment. There are significant pressures on physicians to increase, or at least maintain revenues and bottom line profits. These pressures are coming from many sources.
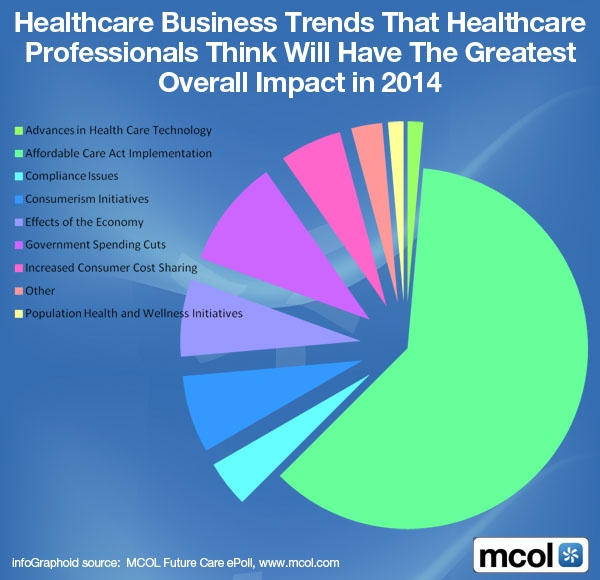
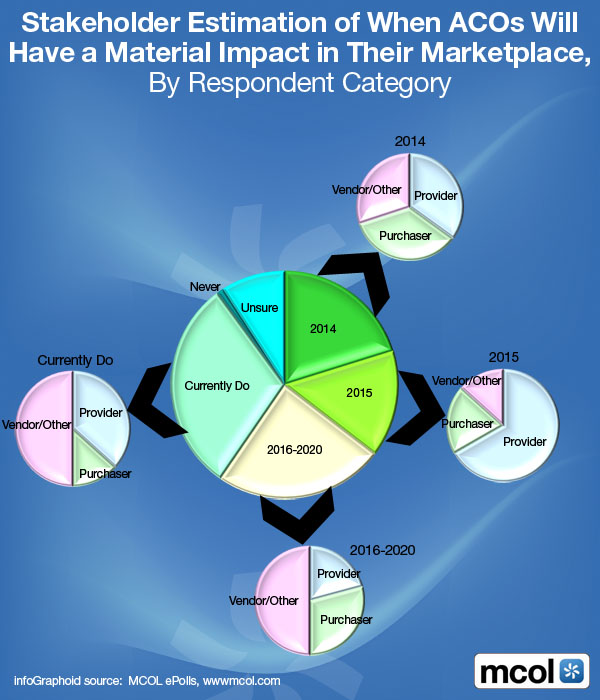
First, there is the increase in managed care penetration. As managed care grows, and the ACA implements via ACOs, doctors are forced to sign up with these health plans in order to maintain their patient base. They perform the same services but get paid less for them. Reimbursement is undergoing a paradigm shift, progressing from retail, to a wholesale, mentality. Capitation is changing reimbursement patterns. When capitation becomes the payment system, most doctors lose revenue simply because they do not know how to practice in this type of payment environment.
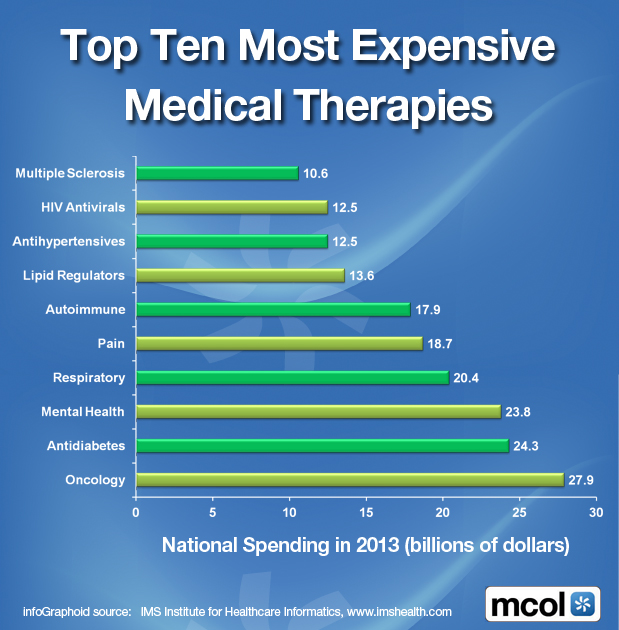
Second, payers’ have a continuous desire to reduce costs, including federal government programs such as Medicare and Medicaid. Many are bundling services together into single payments. More importantly, many payers are simply reducing what they pay doctors. Government intervention, such as HIPAA and eHRs, is also putting pressures on practice revenues. Increased scrutiny by the Government with regard to fraud and abuse issues, along with the Stark rules and regulations, have both impacted practice revenues. Some practices have found they cannot create the revenues they used to since Stark became law. As a result of government scrutiny, physicians coding practices have become much more conservative, thus impairing revenue.
Finally, these pressures have created a significant increase in competition within the healthcare marketplace. To increase revenues, physicians are becoming more aggressive in the marketplace. Many are spending more money on marketing activities in order to increase patient volume. Others are forming affiliations or alliances to go out and obtain exclusive contracting relationships, which is another way to increase patient volume.
In aggregate, physicians are now forced to take initiatives to increase practice revenues. Practices that do not place emphasis on this strategic strategy find themselves with declining revenues as well as declining profits. This means less money available for physician compensation. However, some practices have been successful in growing their revenues with the following practical strategies, which vary for each practice and each practice locale.
***

***
Competing for Managed Care Related Contracts
The objective here is to go out and obtain exclusive contracting arrangements that will add profitability, not necessarily volume, to the practice. This usually means entering into an arrangement with a third party payer. To do this, the practice must do two things. First, it must make sure it is positioned so that a payer will want to award a contract to the practice. In other words, it must have something to sell to the payer. For example, primary care practices are attractive to those payers who want to award global risk contracting arrangements. Second, the practice must market itself to these payers. This means going out and meeting with payer representatives about potential contracting arrangements. The meeting should solicit from the payer what kind of exclusive contracting relationships it is looking for and more importantly, what it thinks about the practice itself. In other words, find out if the payer would even consider awarding a contract to the practice.
Ancillary services
A practice should analyze the services that it is now referring out, so that it can bring them in house to generate revenue. This conflicts with hospital-owned practices since the employed physicians refer most ancillaries to the hospital. In other words, because of government rules, the physicians cannot look to these revenues for additional compensation. However, still look for these opportunities – there might be ancillary services the hospital does not render or does not want to render that could be provided by the practice itself.
Examples of ancillary services that most medical practices could implement include lab, radiology (ie, X-Ray, mammography, echo testing, bone density testing, etc.).
Physician Extenders
As a result of declining reimbursement, physicians are spending less time on patient treatments that do not pay well. In other words, they are not spending time on care that could be rendered by someone else (i.e. by a lower cost provider). Adding a physician extender to a practice can increase revenues simply by freeing up physician time to do other, better paying clinical activities.
For example, an extender could conduct certain post-operative visits, which usually are not paid if treatment is within a designated global surgical period. Extenders could also be used to add patient volume, especially in primary care practices. Many busy practices hire extenders in order to allow patients quick, convenient access to a healthcare provider for simple medical conditions. This way, patients do not have to wait for an appointment. As a result, this leverages the volume of patients a practice can treat on a daily basis.
Added Venue Value
In some service areas, a medical practice can branch out to increase revenue. Practices may be successful adding satellite locations in areas that are either underserved or need a more qualified physician. For example, some practices in urban areas have set up satellite offices in other parts of their county, which are usually geographically outside the urban area itself. Since a significant amount of capital will normally be required to start up the office from scratch, it may be more practical to acquire or merge with an existing practice. The emphasis would then be on increasing the efficiency and profitability of that practice site.
Improving Operations and Productivity
In most cases, revenues can be increased for a medical practice simply by improving operations and physician productivity. For example, many practices have problems with their billing and collection activities, including receivables management. Charges do not get billed on a timely basis, collections at the time of service are inadequate, there is a failure to detect incorrect payer reimbursement, and receivable follow up is unstructured or non-existent. All of this can lead to high receivables and low collections – in other words, lower revenues. The entire billing and collection process should be analyzed and evaluated to see if there are any improvements that can be made that could increase practice revenues.
Next, physicians should look closely at CPT® coding patterns. This is critical for those practices operating in a fixed fee environment because fee schedules cannot be increased to generate additional revenues. First, look at your coding for evaluation and management services. Many doctors under code these services and many do not know how to bill for consultative visits. Look at all other coding issues related to your specific medical specialty. Are modifiers being applied correctly? Are surgical complications identified and billed correctly? Are all available CPT® codes being billed? These are just a few examples.
Make sure the practice fee schedule is maximized. There should not be any billing of a service where the billed charge is approved 100% for payment by the payer. This is especially true for managed care payers. To identify these situations, you must have a system in place to review the Explanation of Benefits (EOBs) that are received from the payers with each reimbursement. Look for those charges that were approved 100% for payment. When identified, the related service fee on the practice charge master should be increased immediately.
Finally, for hospital-owned medical practices, increasing physician productivity can result in an immediate increase in revenues. History has shown that physician productivity often declines after a physician practice is acquired. This is usually because the incentives in the employment contract are misplaced. In these situations, the incentive should be placed on the doctor’s base salary and not any bonus possibilities. A doctor will often maintain productivity if he or she knows that his or her base salary could decline if productivity targets are not met.
***
***
The Template Textbook for Success
For comprehensive practice management information on how to increase office efficiency, operations, revenue and profit, an excellent textbook is: The Business of Medical Practice, 3rd edition.
Assessment
Regardless, the keystone of integrated financial planning for all physicians is consistent income. The following practice benchmarking methodology will assist in proactively monitoring this all-important parameter of your financial life, before it is too late.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:



Filed under: Managed Care, Practice Management | Tagged: Dr. Marcinko, medical practice management | 2 Comments »