BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Posted on August 28, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
ANTI-KICKBACK STATUTEOverview and Impact
Do you want to learn more about the Stark Law and Anti-Kickback Statute Final Rules and how they impact your practice? Join us for a one-hour webinar, presented with Hancock Daniel.
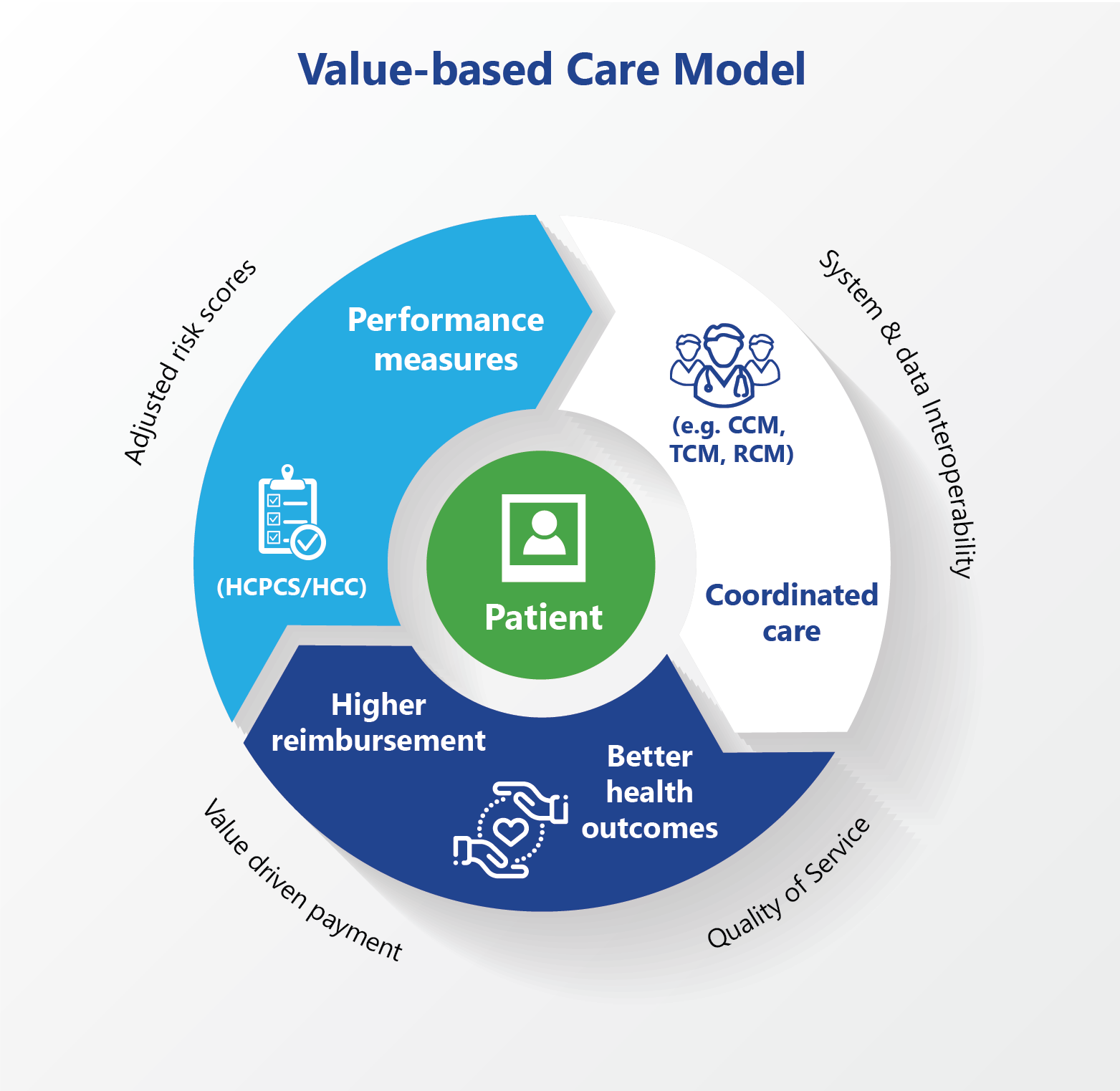
Historically, Medicare has offered value-based payment models to healthcare organizations on both a voluntary and a mandatory participation basis. Because voluntary participants could self-select into programs to reduce spending, it was assumed that they achieved greater savings than mandated participants, but until recently, no data had tested this.
However, a June 2021 study in the Journal of the American Medical Association (JAMA) found no difference in risk-adjusted episodic spending between voluntary and mandatory payment model participants. (Read more…)
Posted on August 25, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
In this episode, DWealthMuse host, Dara Albright, and guest Jeff Ross, CIO of Vailshire Capital Management, discuss why bitcoin may just be that once-in-a-species asset class that saves the planet from economic and, yes, even environmental ruin.
Thisepisode is loaded with so many great insights including:
Why Jeff believes bitcoin’s investment risk has evaporated;
How bitcoin fits into Warren Buffet’s investment thesis;
Two characteristics bitcoin skeptics share: a lack of understanding and deep ties to the traditional banking system;
Why bitcoin is a dishonest politician’s worst nightmare;
Why every modern retirement portfolio should have bitcoin exposure;
Why regulatory scrutiny may be turning away from bitcoin and heading straight towards ethereum and altcoins;
How bitcoin could solve the world’s energy problems;
Why we may be nearing the end of the Keynesian economic experiment;
How bitcoin forces an honest unit of accounting by governments;
Why fiat is destined to self-destruct while bitcoin is designed to appreciate in time;
Whether bitcoin can reach a new all-time high by Jeff’s August 29th birthday and cross 100,000 by Dara’s December 24th birthday?
Posted on August 17, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
BY NIHCM
****
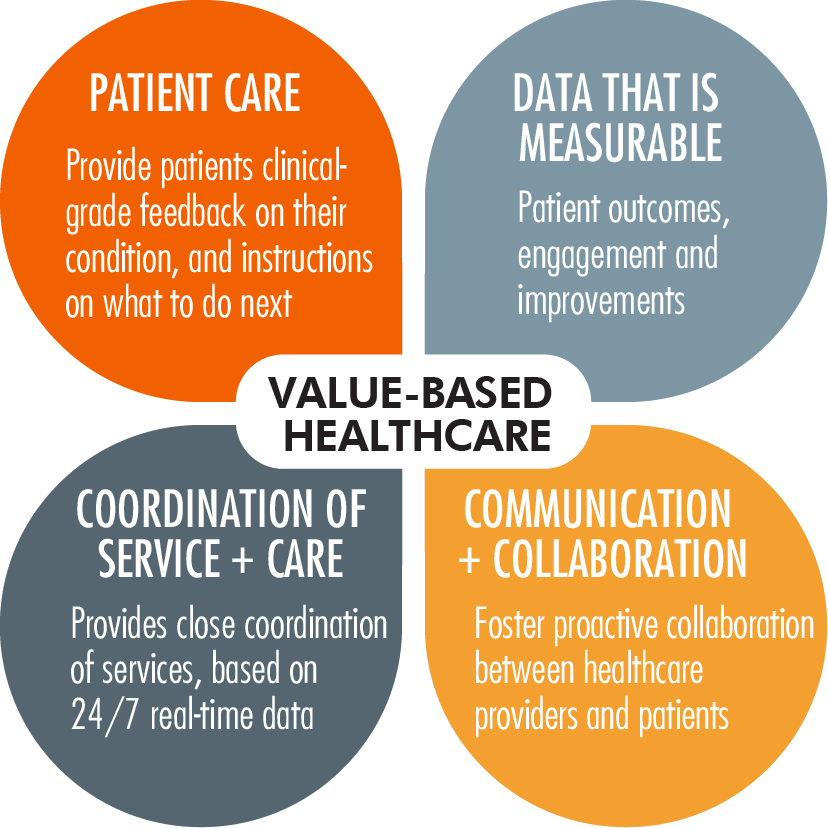
Value-based care has the potential to transform health care, improving quality and access for millions of people, while addressing COVID-19 related disparities. As a result of the pandemic, many rural communities and communities of color face significant reductions in access to health care.
More than 8% of practicing physicians nationwide closed during COVID-19 despite 82 million Americans living in “health professional shortage areas.” The financial strain and burnout experienced by providers has fueled interest in accelerating the adoption of value-based care. As of 2017, only 34% of health care dollars were the result of value-based care payments. This low rate of adoption exists despite evidence tying payments to patient health outcomes and rewarding higher quality care leads to reduced costs.
This webinar brought together experts who are driving innovative initiatives, achieving excellence in health outcomes, and uncovering more effective ways to implement value-based care.
Posted on August 15, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
BY DARRELL K. PRUITT DDS
Do you really need digital records, Doc?
Why?
“Ransomware criminals’ demands rise as aggressive tactics pay off – Average ransomware demands and payments are up as criminal enterprises pour money into the profitable operations.”
Crothers: “The ransomware crisis just keeps getting worse as criminal enterprises pour money into highly profitable ransomware operations, according to a report from Palo Alto Networks’ Unit 42 security consulting group. The average ransomware payment climbed 82% to a record $570,000 in the first half of 2021 from $312,000 in 2020.”
I am asking Dr. Roger P. Levin, DDS, founder and CEO of Levin Group, why he and his international consultant group still promote electronic dental records.
How about it, Dr. Levin? Can you describe how practice management software benefits dental patients? The software doesn’t make dentistry safer or less expensive than paper records – even if digital is more convenient for dentists and staff (most of the time).
On July 13, 2021, the Centers for Medicare & Medicaid Services (CMS) released its proposed Medicare Physician Fee Schedule (MPFS) for calendar year (CY) 2022.
In addition to numerous payment updates in the MPFS, such as significant updates to the Merit-based Incentive Payment System (MIPS), new policies may preserve expanded telemedicine services through 2023 and clinicians may incur more difficulty earning bonuses under the Quality Payment Program (QPP) eligibility threshold. CMS also includes in the proposed rule a request for information to address COVID-19 vaccine reimbursement proposals. (Read more...)
In 2020, at the request of the U.S. House Committee on Ways and Means (the Committee), the Medicare Payment Advisory Commission (MedPAC) began investigating the role that private equity (PE) plays in healthcare provided to Medicare beneficiaries.
In its June 2021 “Report to the Congress on Medicare and the Health Care Delivery System,” MedPAC included for the first time a chapter on PE’s effect on Medicare, wherein it discussed the findings and observations from its investigation and answered a number of questions posed by the Committee. This Health Capital Topics article will analyze MedPAC’s answers to those questions, review its investigation of PE’s role in healthcare, and summarize reactions from stakeholders.(Read more…)
On July 19, 2021, CMS released the proposed rule for the Outpatient Prospective Payment System (OPPS) and Ambulatory Surgery Centers (ASCs) for calendar year (CY) 2022. The proposed rule builds on President Joe Biden’s July 9, 2021 executive order on “Promoting Competition in the American Economy,” as it relates to increasing access and price transparency in the healthcare industry.
In a press release regarding the proposed rule, CMS stated their commitment to addressing the persistent health inequities in the U.S. and finding opportunities to improve data collection that will lead to policy changes to help meet the health needs of patients. (Read more…)
Posted on July 30, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
15 Self-Funded Employers Analyzed Their Pharmacy Claims Data in Conjunction with the Commonwealth Fund and Discovered the Following Regarding their PBM FormularIES
–Just Seeing the Cost of the Lab Test DECREASED the Number of Labs Ordered Per Patient by 9%.
–Doctors Also SUBSTITUTED a Lower Cost Lab Test for a Higher Cost Lab Test 10,000 Times.
The Doctors Were NOT Clinically Directed to Change Their Behavior.
The Doctors’ Pay Was NOT Affected by Their Lab Ordering Either Way.
This Study Illustrates How Giving Doctors Cost Information in a Setting of Clinical and Financial Independence AUTOMATICALLY Decreases Healthcare Waste.
Doctors Can Be Much Better Stewards of Healthcare Dollars … and the Technological Innovation Needed is Minimal.
Disclosure: Dr. Bricker is the Chief Medical Officer of Virtual Care Company First Stop Health.
Posted on July 24, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Residents disproportionately affected by COVID-19
***
BY JAMES BLUMENSTOCK MA
Residents of nursing homes have been disproportionately affected by COVID-19. The nature of this coronavirus—which is particularly harmful to older adults and people with multiple chronic conditions—has left residents vulnerable.
Additionally, the pandemic has exacerbated existing challenges in our fragmented long-term care system, which is financed, regulated, and administered by states, the federal government, and private care facilities.
During this webinar, panelists discussed policy options to support high quality care for nursing home residents during the COVID-19 pandemic.
NOTE: This webinar is a project of the Alliance for Health Policy and NIHCM Foundation, in collaboration with The Commonwealth Fund.
There is Copay for Each Office Visit and Visits are Unlimited.
Direct Primary Care Doctors Are Most Frequently Family Practice Physicians, but Internal Medicine and Pediatricians Can Also Have Direct Primary Care Practices.
The Average Direct Primary Care Practice Has a Panel of 345 Patients, with a Goal of About 600 Patients at Full Capacity.
For Comparison, the Typical Fee-for-Service Primary Care Doctor Has a Patient Panel of 2,500.
57% of Direct Primary Care Practices Contract with Employers That Pay the Monthly Membership on the Employee’s Behalf.
Direct Primary Care is a Strategy to Increase the Quality of Care and Decrease Healthcare Costs for an Employee Health Plan.
Disclaimer: Dr. Bricker is the Chief Medical Officer of Virtual Care Company First Stop Health.
Posted on July 22, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
BOOK REVIEW
“The Dictionary of Health Insurance and Managed Care lifts the fog of confusion surrounding the most contentious topic in the health care industrial complex today. My suggestion therefore is to ‘read it, refer to it, recommend it, and reap’.”
—Michael J. Stahl, PhD, Physician Executive MBA Program [William B. Stokely Distinguished Professor of Business]
The University of Tennessee, College of Business Administration
The U.S. individual tax return is based around the concepts of Adjusted Gross Income (AGI) and Taxable Income (TI). AGI is the amount that shows up at the bottom of page one of Form 1040, individual income tax return. It is the sum of all of the taxpayer’s income less certain allowed adjustments (like alimony, one-half of self-employment taxes, a percentage of self-employed health insurance, retirement plan contributions and IRAs, moving expenses, early withdrawal penalties and interest on student loans). This amount is important because it is used to calculate various limitations within the area of itemized deductions (e.g., medical deductions: 10 percent of AGI; miscellaneous itemized deductions: 2 percent of AGI).
When a healthcare professional taxpayer hears the phrase “an above the line deduction”, the line being referenced is the AGI line on the tax return. Generally, it is better for a deduction to be an above the line deduction, because that number helps a taxpayer in two ways. First, it reduces AGI, and second, since it reduces AGI, it is also reducing the amounts of limitations placed on other deductions as noted above.
Obviously, if there is an above the line there is also a “below the line” deduction. These below the line deductions are itemized deductions (or the standard deduction if itemizing is not used) plus any personal exemptions allowed. AGI less these deductions provides the taxable income on which income tax is actually calculated. All of that being said, it is better for a deduction to be an above the line deduction. Although this is a bit dry, it helps to understand the concepts in order to know where items provide the most benefit to the medical professional taxpayer.
PERSONAL TAXATION CALCULATIONS
Gross Income (all income, from whatever source derived, including illegal activities, cash, indirect for the benefit of, debt forgiveness, barter, dividends, interest, rents, royalties, annuities, trusts, and alimony payments-no more)
Less non-taxable exclusions (municipal bonds, scholarships, inheritance, insurance
proceeds, social security and unemployment income [full or
partial exclusion], etc.).
Total Income
Less Deductions for AGI (alimony, IRA contributions, capital gains, 1/2 SE tax,
moving, personal, business and investment expenses, and
penalties, etc.).
Adjusted Gross Income (bottom Form 1040)
Less Itemized Deductions from AGI, (medical, charitable giving, casualty,
involuntary conversions, theft, job and miscellaneous expenses, etc.), or
Less Standard Deduction (based on filing status)
Less Personal Exemptions (per dependents, subject to phase outs)
Taxable Income
Calculate Regular Tax
Plus Additional Taxes (AMT, etc.)
Minus Credits (child care, foreign tax credit, earned income housing, etc.)
Posted on July 18, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
THE SHERLOCK COMPANY
This podcast features a brief discussion by colleague Doug B. Sherlock CFA, Senior Health Care Analyst and President, Sherlock Company http://www.sherlockco.com featuring his insights into the quarterly financial reports of health plans, for the first quarter 2021.
The Charges Were Regarding Illegal Payments and Kickbacks to Doctors that Were Thinly-Veiled as ‘Speaker Fees’ and Fancy Dinners.
Why Where the Doctors Not Held Accountable and What Does This Say About a Doctor’s Mentality on Money?
Learn the Psychology of Doctors and Money.
Understand How It Leads to Counterproductive Relationships Between Physicians and Drug Companies, Which Can Compromise the #1 Rule in Medicine: The Patient Comes First, Always.
Disclaimer: Dr. Bricker is the Chief Medical Officer of Virtual Care Company First Stop Health
Posted on July 16, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
HSA Update 2021
By Michael Thompson
High-deductible health plans have been popular, but it’s becoming clear they are not right for all employees, said Michael Thompson, president and chief executive officer of the National Alliance of Healthcare Purchaser Coalitions.
Specifically, Forrester Research Says That Customer Service is ‘Poor’ at Blue Cross of Texas and Illinois, Blue Shield of California, CareFirst Blue Cross, Anthem, United Healthcare, Cigna and Aetna.
Hospital Billing Customer Services Is Bad Too.
Hospital Billing Complexity is So Troublesome to Patients, that 40% Say They Avoid Preventive Care and Screening Tests Just to Avoid the Billing Headache.
Healthcare Customer Service is Terrible Because Health Insurance Companies and Hospitals Do Not Need Good Billing Customer Service to Be Successful, As Demonstrated by High and Rising Health Insurance Stock Prices and Large and Growing Hospital System Revenue.
For Health Insurance Companies and Hospitals, Not Fixing Their Poor Customer Service May Be a Calculated Business Decision.
Implications:To Help Make Their Employees’ Lives Better, Employers May Need to 1) Hire a Healthcare Navigation Company or 2) Deliver More Care to Their Plan Members Outside of the Traditional Health Insurance and Hospital Systems… and Avoid the Terrible Customer Service All Together.
Disclaimer: Dr. Bricker is the Chief Medical Officer of Virtual Care Company First Stop Health and is the Former Co-Founder of Compass Professional Health Services.
–The Private Equity Firm Offers an Up Front Lump Sum of Money and Administrative Services Such as Billing and Collections for the Practice.
–In Return, the Doctors in the Practice Agree to Have 30-40% of All Future Revenue Go to the Private Equity Firm.
The Up Front Lump Sum Can Be Equal to as Much as 10 – 20 Years of Income for a Physician.
The Older Doctors in the Practice Who Are Usually the Partners Frequently Take This Deal, Resulting in the Younger Partners Making Less Take-Home Pay.
Implication for Employers:
Private Equity Firms Create Larger Group Practices to Have Better Negotiating Leverage with Commercial Insurance Carriers and Obtain Higher Fee-for-Service Reimbursement.
Overall Healthcare Costs for Physician Services Go Up, While the Take-Home Pay for Doctors Goes Down… and the Private Equity Firm Keeps the Difference.
NOTE: The Older Doctors Who Are Paid the Lump Sum Are Still Required to Stay at the Practice for a Certain Number of Years After the Transaction.
Depression is Highest Among 18-25 Year Olds at 11%.
19% of US Adults Have Anxiety and 56% of Those with Anxiety Are Impaired By Their Condition.
12% of People with Diabetes Have Associated Depression… Resulting in Missed Appointments, Poorer Diet, Decreased Medication Adherence and Increased Complications.
To Address This Problem, The Intermountain Health System Incorporated a Mental Health Provider in Their Primary Care Clinics.
Results: Improved in Diabetes Care, Decreased Hospitalizations and Decreased ER Utilization.
Treating Mental Health Not Only Improves Mental Wellbeing, But Also Lowers Overall Healthcare Costs as Well.
Disclaimer: Dr. Bricker is the Chief Medical Officer of Virtual Care Company First Stop Health.
NOTE: If you or someone you know is considering suicide, please contact the National Suicide Prevention Lifeline at 1800-273-TALK (8255), text “help” to the Crisis Text Line at 741-741 or go to suicidepreventionlifeline.org.
Posted on July 10, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
Dr. David Edward Marcinko is Speaking Up
Dr. David Edward Marcinko MBA CMP® enjoys personal coaching and public speaking and gives as many talks each year as possible, at a variety of medical society and financial services conferences around the country and world.
These have included lectures and visiting professorships at major academic centers, keynote lectures for hospitals, economic seminars and health systems, keynote lectures at city and statewide financial coalitions, and annual keynote lectures for a variety of internal yearly meetings.
His talks tend to be engaging, iconoclastic, and humorous. His most popular presentations include a diverse variety of topics and typically include those in all iMBA, Inc’s textbooks, handbooks, white-papers and most topics covered on this blog.
1) The 90s HMOs: Lower Premiums, Lower Out-of-Pocket Costs, Many Many Rules Restricting Care.
2) The 2000s PPOs: High and Even Higher Premiums, Lower Out-of-Pocket Costs, Fewer Rules Restricting Care.
3) The 2010s CDHPs: Lower Premiums, HIGH Out-of-Pocket Costs, Fewer Rules Restricting Care.
The Last 30 Years Have Taught Us that Employer-Sponsored Health Plans CANNOT Have All 3–Low Premiums, Low Out-of-Pocket Costs and Few Care Restrictions.
In the 2020s, Employers Are Moving More of Their Employee Healthcare OUTSIDE of the Traditional Healthcare and Health Insurance System with On-Site Clinics, Near-Site Clinics, Virtual Urgent Care, Virtual Primary Care and Bundled-Payment Centers-of-Excellence.
Posted on July 7, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
BOOK REVIEW
BY ERIC BRICKER MD
Our Brains Have a Reward Chemical Called Dopamine That Causes a Brief Pleasurable Feeling Followed by a Worsening of our Mood.
However, Our Brains Also Have a Contentment Chemical Called Serotonin That Causes Peace and a Calming of our Mood.
Substances and Behaviors That Stimulate Dopamine Include: Sugar, Caffeine, Alcohol, Nicotine, Illicit Drugs, Prescription Narcotics, Social Media Apps, Gambling and Sex.
Substances and Behaviors That Stimulate Serotonin Include: The Amino Acid Tryptophane, Positive Relationships with Others, Service to Others, Prayer and Meditation.
Corporations Tailor Their Products with Dopamine Stimulating Strategies to Increase Sales.
Facebook’s Chamath Palihapitiya Even Admitted on CNBC that Facebook Intentionally Designed its Social Media Platform to Stimulate Dopamine in the User’s Brain To Make Them Use the App More.
Unfortunately, the Constant Stimulation of Dopamine in Our Brains Has Increased Obesity, Metabolic Syndrome, Cancer, Cardiovascular Disease, Diabetes and Depression.
Lustig Estimates That 75% of the $4 Trillion Spent on US Healthcare is for These Diseases That Can Be Traced to Our ‘Hacked Minds.’
Posted on July 7, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
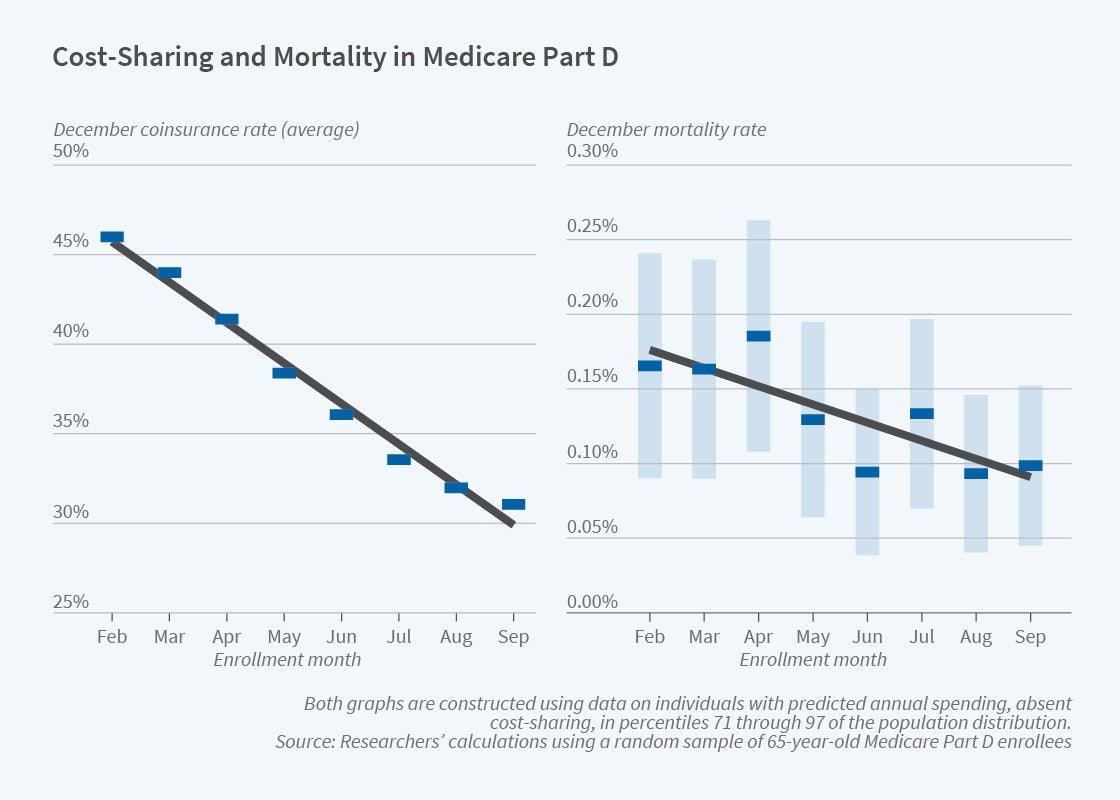
Raises Mortality among Medicare PART D Beneficiaries
QUERY: What are the health consequences when patients reduce their use of prescribed medications in response to higher out-of-pocket costs?
In The Health Costs of Cost-Sharing (NBER Working Paper 28439), researchers Amitabh Chandra, Evan Flack and Ziad Obermeyer use the distinctive out-of-pocket cost-sharing features of Medicare Part D to demonstrate that such reductions can increase mortality.
1) Prospecting: The Strategy of Aaron Ross in Dividing Prospecting into Seeds, Nets and Spears Was Effective in Generating Leads at Compass Professional Health Services.
2) Pitching: The Miller-Heiman Strategy of Identifying Economic, Outcome and Technical Buyers Allows for Effective Pitching to a Buying Team.
3) Closing: The Model of ‘Fit-Risk-Price’ is Essential To Understanding How and When to Close a Sale.
Posted on July 5, 2021 by Dr. David Edward Marcinko MBA MEd CMP™
At Least in PartACCORDING TO THESE BOOKS
BY ERIC BRICKER MD
Understandably, Many Doctors Take Issue with This Accusation and Say They Treat Their Patients with Integrity and Accountability. Both Statements May Be TRUE … How is That Possible?
Because of ‘Bad Apples.’
While the Majority of Physicians May Put Their Patients First, There Are a Minority of Physicians that Put Money, Power, Prestige and Promotions Ahead of Patients. It’s These Bad Apples That Ruin Physician Culture.
Problem: Fee-for-Service Rewards Bad Apple Physicians, While Paying the High-Integrity Doctors as Well.
Assessment: If Doctors Want to Keep Fee-for-Service, Then the Bad Apples Must Be Reduced Through 1) Increased Transparency, 2) Greater Doctor Self-Regulation, 3) More Federal Oversight and 4) Increased Employer Investigation.
1) Some Individual Doctors Were Paid Upwards of $5.8 Million Dollars by Medicare in Just a Single Year!
2) The Specialists That Charged Medicare the Most Tended to Be Vascular Surgeons, Ophthalmologists, Oncologists and Cardiologists.
Implications for Employer-Sponsored Health Plans:
1) Medicare Data Can Be Used to Identify High Volume Physicians and Surgeons.
2) The Highest-Costing Doctors Are Concentrated in a Relatively Small Number of Specialties That Can Be Targeted for Detailed Review, Feedback and Possible Exclusion/Steerage Away.
ASSESSMENT: Your thoughts and comments are appreciated.
Many accountable care organizations (ACOs) received disappointing news on May 21, 2021, when the Centers for Medicare & Medicare Services (CMS) announced that it would not be extending the Next Generation ACO (NGACO) model for 2022.
After five years and a dwindling number of participating ACOs, experts were split on whether or not CMS should keep the model in place for another year. On one hand, stakeholders have argued for the NGACO model’s extension until it can be replaced with or integrated into another program; howowever, others asserted that resources could not be properly invested with only one more year left in the program. (Read more…)