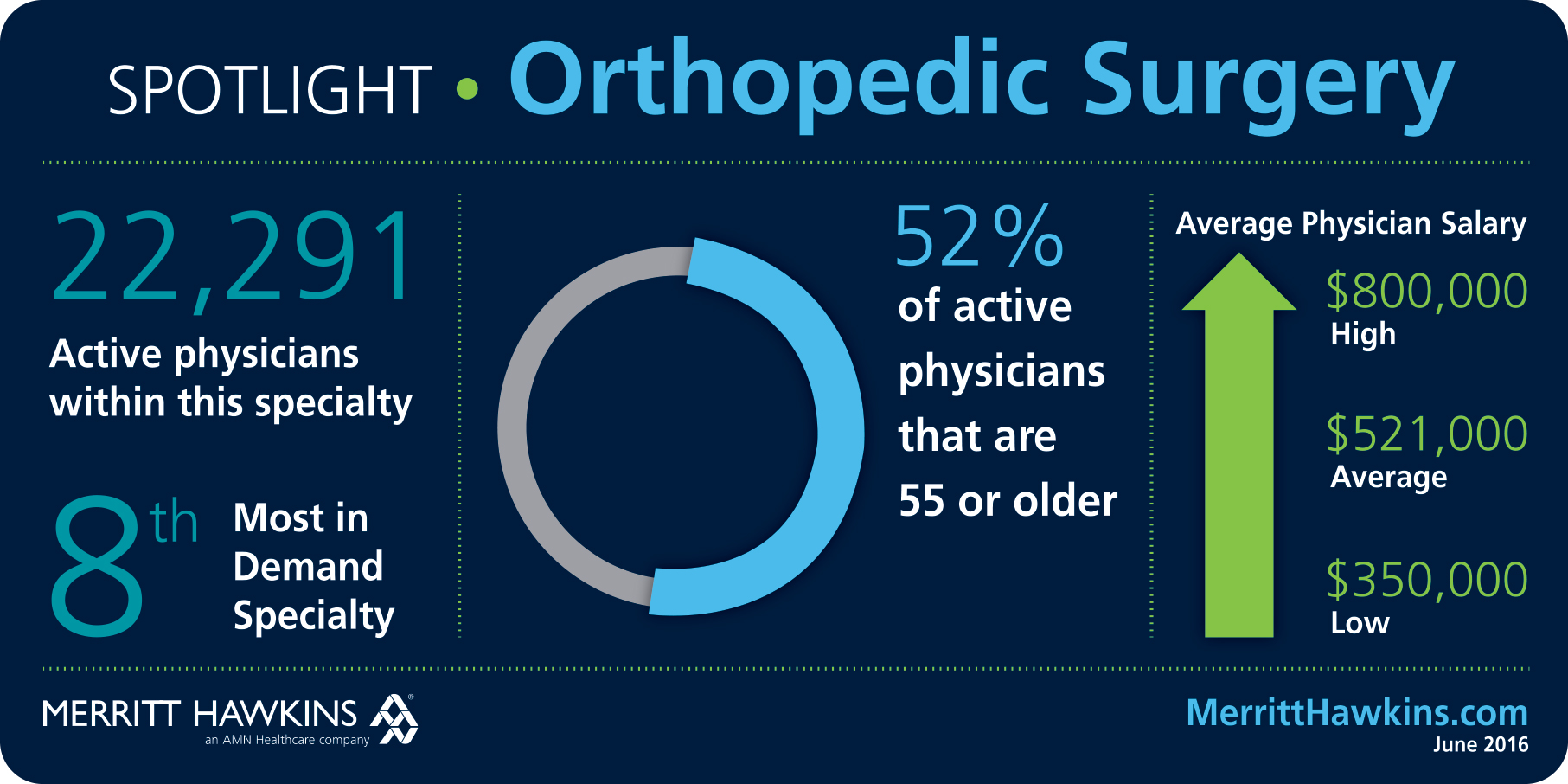
BOARD CERTIFICATION EXAM STUDY GUIDES Lower Extremity Trauma
[Click on Image to Enlarge]
ME-P Free Advertising Consultation
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
Medical & Surgical e-Consent Forms
ePodiatryConsentForms.com
iMBA Inc., OFFICES
Suite #5901 Wilbanks Drive, Norcross, Georgia, 30092 USA [1.678.779.8597]. Our location is real and we are now virtually enabled to assist new long distance clients and out-of-town colleagues.
ME-P Publishing
SEEKING INDUSTRY INFO PARTNERS?
If you want the opportunity to work with leading health care industry insiders, innovators and watchers, the “ME-P” may be right for you? We are unbiased and operate at the nexus of theoretical and applied R&D. Collaborate with us and you’ll put your brand in front of a smart & tightly focused demographic; one at the forefront of our emerging healthcare free marketplace of informed and professional “movers and shakers.” Our Ad Rate Card is available upon request [678-779-8597].
Hospitals saw a slight financial boost in November 2022, despite continued negative operating margins throughout the year, according to a new Kaufman Hall National Hospital Flash Report, as reported in Healthcare Brew.
Lower expenses and increased outpatient revenue help buoy their performance and increase margins by 12% month over month from October 2022. But Kaufman Hall, a management consulting firm, reported that its year-to-date operating margin index reflected an actual negative figure of -0.2% in November 2022.
The findings underscore the financial challenges hospitals continue to face as they recover from the Covid-19 pandemic.
And, Erik Swanson, senior vice president of data and analytics at Kaufman Hall, wrote that the “November data, while mildly improved compared to October, solidifies what has been a difficult year for hospitals amidst labor shortages, supply chain issues, and rising interest rates.”
The monthly report, which is based on data from more than 900 hospitals, partially attributed November’s lowered expenses to a decline in patient volume and slightly shorter lengths of stay. Decreased labor costs, likely due to a drop in a reliance on contract labor, also helped lower expenses, the Kaufman analysis found.
Hospitals further saw a 10% increase year over year in outpatient revenue in November 2022, despite inpatient revenue remaining flat, according to the report. Swanson said “[h]ospital leaders should continue to develop their outpatient care capabilities amid ongoing industry uncertainty and transformation.”
Posted on January 16, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
What is it and How Does it Work?
By Staff Reporters
***
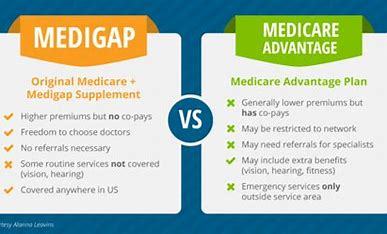
Did you know that Medicare Plan G is the most popular Medicare Supplement with Baby Boomer clients? Everyone has heard of Plan F, but what is Medicare Supplement Plan G? What does Plan G cover?
Medicare Plan G coverage is very similar to Plan F, which is no longer available for people new to Medicare on or after January 1st, 2020. Plan G offers great value for beneficiaries willing to pay a small annual deductible. After that, Plan G provides full coverage for all of the gaps in Medicare. It pays for your Medicare Part A hospital deductible, co-pays, and coinsurance. It also covers the 20% that Medicare Part B doesn’t cover. Doctors and other healthcare providers must accept a Medigap Plan G if they accept Original Medicare. Plan G policies can be used across the U.S. since they do not have network limitations, and the premium costs can be very reasonable for the coverage you receive.
As you can see below, Supplement Plan G covers almost everything that F does, except for the Part B deductible.
***
***
Medicare Plan G, also called Medigap Plan G, is an increasingly popular Supplement
Reasons:
First, Plan G covers each of the gaps in Medicare except for the annual Part B deductible. This deductible is only $226 in 2023. In fact, if you have a Plan F that has been in place for years, it can probably help you on premiums by looking at Plan G. When you shop for benefits, you can often find a Supplement Plan G that saves quite a bit in premiums over Plan F, usually substantially more than the $226 deductible that you’ll pay out.
Second, it has great coverage. For hospital stays, it covers all your hospital expenses. Most importantly, it pays the hospital deductible, which is over $1,600 in 2023. It also covers the expensive daily co-pays that you might encounter for a hospital stay that runs longer than 60 days. It provides an additional 365 days in the hospital after your Medicare benefits run out, and it covers your skilled nursing facility co-insurance, too.
What Other Medical Services Does Plan G Cover?
Medicare Supplement Plan G covers your percentage of any medical benefit that Original Medicare covers, except for the outpatient deductible. So, it helps to pay for inpatient hospital costs, such as the first three pints of blood, skilled nursing facility care, and hospice care. It also covers outpatient medical services such as doctor visits, lab work, diabetes supplies, cancer treatment, durable medical equipment, x-rays, ambulance, surgeries and much more. This means Plan G covers the coverage gaps with Original Medicare and all Plan G products must provide you with the exact same coverage.
Medicare pays first, then Plan G pays the remaining amount after you pay the once annual deductible. In addition, Plan G Medicare Supplements offer up to $50,000 in foreign travel emergency benefits (up to plan limits).
Posted on January 14, 2023 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
People living in the US are finding it increasingly difficult to afford needed health services—even with employer-sponsored health insurance, a new analysis suggests.
Researchers at the NYU School of Global Public Health (GPH) examined data from the National Health Interview Survey—an annual CDC survey—that was collected from 2000 to 2020 for 230,000+ adults who received health insurance through an employer or union. Both men and women found most healthcare services to be less affordable now compared to the early 2000s, according to the finding of the NYU analysis reported in a December 2022 JAMA abstract. Women, in particular, found all types of health services to be less affordable than men.
From a nationally representative survey which is conducted annually, researchers included data from 5,545 women and 5,353 men sampled in 2020, and found that about 6% of women reported they couldn’t afford needed medical care. This compares to just 3% of slightly larger sample groups from 2000, per the analysis. By contrast, about 3% of men gave that response in 2020, compared to 2% in 2000.
Avni Gupta, a doctoral student in the public health policy and management department at NYU GPH and the lead author of the analysis, offered that “lower incomes and higher healthcare needs among women could be driving these differences in reported affordability.”
And, José Pagán, the department chair and co-author of the JAMA analysis, said people with employer-sponsored coverage—the largest source of health insurance for people living in the US—“generally think they are protected.”
“[B]ut our findings show that health-related benefits have been eroding over time,” he said; according to Healthcare Brew
Posted on December 31, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
Centene Corporation showers politicians with millions as it courts contracts and settles over-billing allegationsby Samantha Young, Andy Miller, and Rebecca Grapevine (Kaiser Health News)
***
Somehow KHN made Medicaid over-billing sound sexy.
This deep dive into Centene, “the nation’s largest private managed-care provider for Medicaid,” shows how the company has maintained good relationships with politicians as it looked to keep its market share and settle over-billing allegations.
Posted on December 8, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Neutral-Site and Out-Patient Medical Payments
[By Staff Reporters]
The Medicare program currently pays significantly different rates for services provided in different settings, and site-neutral payments have been considered as one way of eliminating the payment gap.
However, that option has proven to be a contentious issue.
Here are 25 things to know about site-neutral payments
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
“Physicians who don’t understand modern risk management, insurance, business, and asset protection principles are sitting ducks waiting to be taken advantage of by unscrupulous insurance agents and financial advisors; and even their own prospective employers or partners. This comprehensive volume from Dr. David Marcinko and his co-authors will go a long way toward educating physicians on these critical subjects that were never taught in medical school or residency training.” —Dr. James M. Dahle, MD, FACEP, Editor of The White Coat Investor, Salt Lake City, Utah, USA
“With time at a premium, and so much vital information packed into one well organized resource, this comprehensive textbook should be on the desk of everyone serving in the healthcare ecosystem. The time you spend reading this frank and compelling book will be richly rewarded.” —Dr. J. Wesley Boyd, MD, PhD, MA, Harvard Medical School, Boston, Massachusetts, USA
Posted on December 2, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
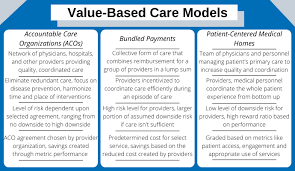
Paying paying doctors and medical providers for their services may seem simple on the surface, but it’s actually extremely complex. Enter two of the most commonly heard phrases in healthcare: “fee-for-service” and “value-based care,” two models insurers use to decide how much to pay providers. According to Healthcare Brew:
Under a fee-for-service model, providers are paid for each individual service they perform, like a blood test or an X-ray, according to Jennifer Clawson, partner and director of value-based health systems at Boston Consulting Group. A service is provided, and the doctor gets a fixed fee for providing it. Simple enough.
The value-based care model is a bit more complicated, as there are many types of value-based payments. What makes them “value-based” is that payers take patient outcomes into consideration, aka they consider the relative value. “The core of value-based care is ultimately, ‘How do I get a better outcome for less money?’” said Sam Hendler, managing director at private equity firm Thomas H. Lee Partners.
One type of value-based payment is called a bundled payment, Clawson said. Say you have a heart condition and need to get a stent put in. There are usually several providers involved in that process, e.g., a primary care doctor, cardiac surgeon, and anesthesiologist. An insurer gives the health system a set amount of money to cover everyone involved in the procedure, and the health system decides how to divvy it up.
Another type of value-based payment is called capitation, and there’s multiple types of capitation payments. It’s sort of like a bundled payment, but instead of insurers paying a set amount per procedure, they’re paying a set amount to cover an entire population of patients with a specific disease, like diabetes.
Posted on December 1, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Heath Capital Consultants, LLC
***
***
The launch of Amazon Clinic comes less than two months after the announcement that Amazon Care would be shut down. Amazon Clinic, the retail giant’s virtual and in-person medical care service, was rolled out in 2019 as a pilot employee benefit for their own employees and quickly expanded to servicing non-Amazon employers across the U.S. (including large companies such as Hilton, TrueBlue, and Silicon Labs) by 2021.
Posted on November 19, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
[Emergency Request]
By Staff Reporters
***
***
Children’s hospitals are asking the federal government to declare a public health emergency to help them deal with the surge of RSV cases. Infants are being hospitalized at seven times the rate of 2018.
DEFINITION: Respiratory syncytial virus, also called human respiratory syncytial virus and human orthopneumovirus, is a common, contagious airborne virus that causes infections of the respiratory tract. It is a negative-sense, single-stranded RNA virus.
DIGMAs (Drop-In Group Medical Appointments) are medical office appointments with a patient’s physician that take place in a supportive group setting. The model, developed in 1996 by Kaiser Permanente psychologist Dr. Ed Noffsinger, is a combination of an extended medical appointment with the patient’s own physician and effective group learning and support.
The group consists of the physician, a behavioral health professional, and patients from the physician’s panel. DIGMAs are best suited for routine appointments. Unfortunately, the nascent concept was met with mockery and great derision after the PP-ACA era.
Today, after the pandemic and with the rise of tel-health and tele-medicine, Shared Medical Appointments (SMAs), also known as Group Medical Visits [GMVs], are again a growing topic of discussion among providers and health economists, looking for ways to increase access to care and improve efficiency. The group visit format is also getting more attention in recent years as a strategy to add value for the patient. They typically involve up to a dozen patients or so and offer various efficiencies as well as benefits of shared discussion and experiences.
***
Behavioral Changes
Moreover, physicians and medical providers know that simply telling patients what to do often does not improve their health. The basic premise of DIGMAs, SMAs and GMVs is to build more patient engagement and inspire lasting behavior change by offering patients the opportunity to share their personal experiences not only with their provider but also with other patients dealing with similar issues.
Posted on November 8, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
“BIRTHING-FRIENDLY”
By Staff Reporters
***
***
The Centers for Medicare and Medicaid Services (CMS) added a new designation to identify which hospitals are “Birthing-Friendly”—a label it will begin adding to qualifying hospitals in fall 2023.
The designation aims to reduce maternal mortality and complications in the US; maternal mortality rose by 25% in 2020, and Black women die at nearly three times the rates of white women, according to a CDC report from February. The US ranked last in maternal mortality that year compared to 10 other high-income countries, according to the Commonwealth Fund.
To earn the designation, CMS said, hospitals must participate in a statewide or national collaborative program where medical teams and public health leaders work together to improve care quality for birthing parents and babies. Hospitals that opt in qualify for an operating payment rate increase of 4.3%, a much-needed boost for hospitals struggling with profitability in the wake of the Covid-19 pandemic and inflation.
But there’s no single set of metrics that hospitals will be required to follow to earn CMS’s new designation, and any changes they make may depend on what areas need improvement. For example, hospitals could focus on reducing pregnancy complications and early births, which happen before 39 weeks, according to the CDC.
CMS’s designation—at least in its initial form—isn’t tied to outcomes. However, medical professionals said there are a variety of measures and outcomes that have been shown to make a hospital truly birthing-friendly.
When it comes to measuring maternal-care quality, one metric comes up over and over again: a hospital’s C-section rate, said Holly Loudon, chair of obstetrics, gynecology, and reproductive science at Mount Sinai West and Mount Sinai Morningside in New York City.
Posted on November 6, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Health Capital Consultants, LLC
***
***
The American Hospital Association (AHA) is advocating for the creation of a new hospital designation for certain urban safety net hospitals.
In a report released in mid-October 2022, as well as in an accompanying fact sheet and letter sent to congressional leaders, the AHA defines these so-called Metropolitan Anchor Hospitals (MAHs), outlines their importance to the communities they serve, and explains why MAHs deserve supplemental financial support from the government.
Posted on November 2, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
CMS Cracks Down on Medicare Advantage TV Marketing
Dr. David Edward Marcinko MBA
***
***
CMS is cracking down on deceptive marketing practices and will no longer allow Medicare Advantage or Part D prescription drug plans to advertise on television without agency approval first. The new policy is effective Jan. 1st and was discussed in an Oct. 19th memo from CMS to MA and Part D providers. The agency said it issued the new policy after reviewing thousands of beneficiary complaints regarding confusing, misleading or inaccurate information from plans — plan sponsors are also responsible for all marketing activities from brokers and third-party agencies.
“CMS has conducted so-called ‘secret shopping’ by calling numbers associated with television advertisements, mailings, newspaper advertisements and internet searches to monitor the experience beneficiaries have engaging these entities,” the agency wrote.
“Our secret shopping activities have discovered that some agents were not complying with current regulation and unduly pressuring beneficiaries, as well as failing to provide accurate or enough information to assist a beneficiary in making an informed enrollment decision.”
Source: Jakob Emerson, Becker’s Payer Issues [10/27/22]
Posted on October 29, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
The future of healthcare will be defined by nurses. Giving them a platform where they can be seen, heard, and valued for what they contribute each and every day is healthcare innovation.
connectRN is an empowered community of nurses, helping them access the flexible work opportunities they want. Nurses use connectRN to find work, access resources, and get much-needed peer support. And healthcare facilities can get the staff they need to provide high-quality patient care.
From in-app shift scheduling to same-day pay to 24/7 support, connectRN offers nurses a modern, seamless, and stress-free experience. After all, thriving clinicians provide the best care.
Posted on October 28, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
“Behavioral Economic Strategies”
By Eric Bricker MD
***
As Published in the Annals of Internal Medicine by an All-Star Cast of Researchers:
1) Limitations of Information 2) Inertia/Status Quo Bias 3) Choice Overload 4) Immediacy 5) Loss Aversion 6) Relative Social Ranking 7) Threshold Effect 8) Limits of Willpower 9) Mental Accounting
Posted on October 27, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
Hospitals this year are seeing more red than black as growing financial challenges, like spiked labor costs and inflation on medical supplies, puts them on pace to have the worst financial performance into the pandemic thus far.
More than half of hospitals (53% of more than 900 sampled) are projected to have negative margins by the end of the year, compared to 39% in 2019, according to a September report from management consulting firm Kaufman Hall, on behalf of AHA. The firm put the median operating margin for hospitals at about -1%, which could mean service cuts, and for more vulnerable hospitals, including rural ones, closing their doors.
But why is the financial outlook so bleak for hospitals? A few factors are conspiring:
Labor costs: The top reasons hospitals are struggling financially in 2022 are “labor, labor, and labor,” said Kevin Holloran, senior director at Fitch Ratings. The healthcare labor shortage doesn’t just extend to nurses, but across the board.
Rising supply prices: Blame inflation. AHA reported that the “costs for energy, resins, cotton, and most metals surged in excess of 30%” between fall 2020 and early 2022.
Sicker patients, longer stays: Intensive care units across the country were overwhelmed with Covid-19 patients at the outset of the pandemic, but more recently hospitals have been caring for sicker non-Covid patients, said Aaron Wesolowski, AHA’s vice president for policy research and analytics
Posted on October 26, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
25% of Clinicians Want Out of Healthcare: Survey
***
***
One quarter of U.S. physicians, advanced practice providers, and nurses are considering switching careers and one third are considering switching employers, according to newly released results from a survey conducted by Bain & Company. Below are some key takeaways from the survey and brief, which was released October 11th and can be found in full here.
1. Of the 25 percent of clinicians who are thinking about exiting healthcare entirely, 89 percent cite burnout as the main driver.
2. The top three things clinicians care about most in their profession are compensation, quality of patient care, and workload, according to the survey. Of those three, they are least satisfied with compensation (59 percent expressed satisfaction) and workload (60 percent). Eighty percent said they are satisfied with the quality of patient care.
3. Burnout shows up throughout clinicians’ days, with 63 percent saying they feel worn out at the end of the workday, 51 percent saying they feel they don’t have time and energy for family and friends during leisure time, and 38 percent feeling exhausted in the morning at the thought of another workday.
Posted on October 15, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
***
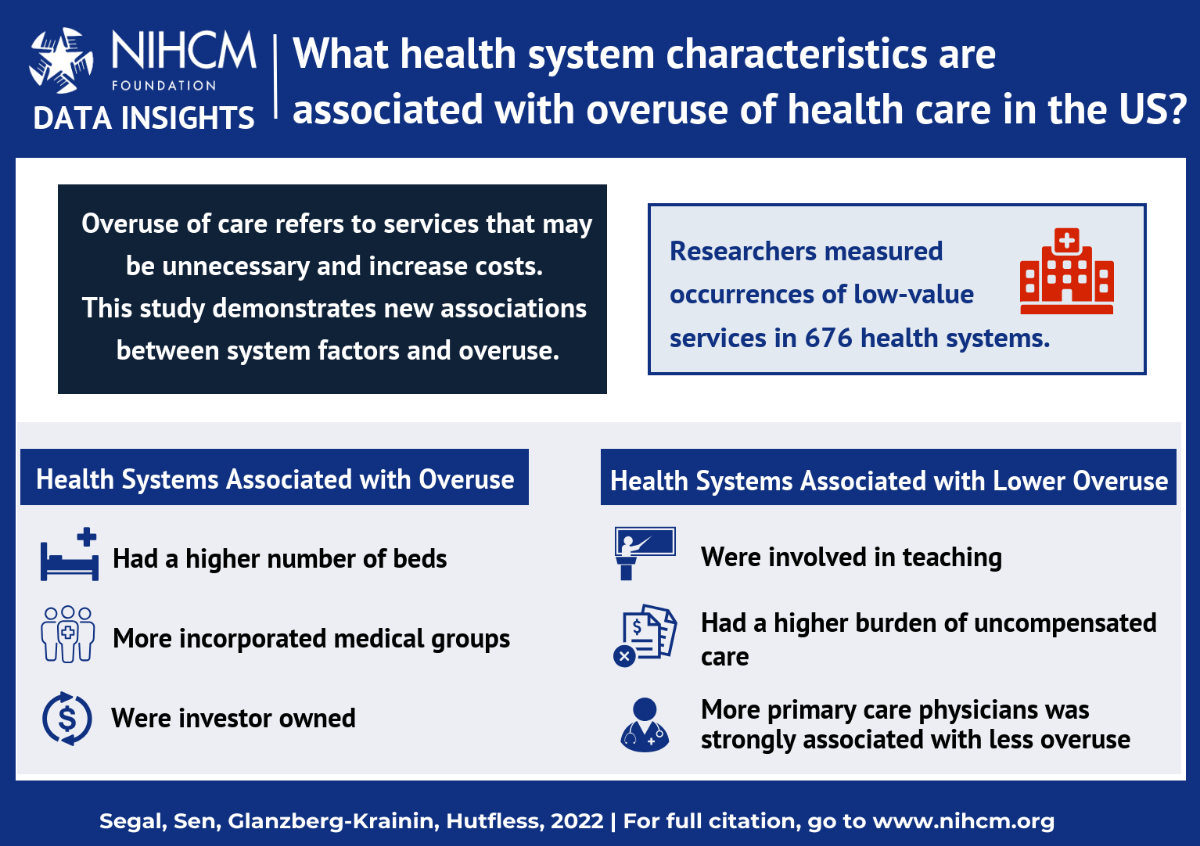
The high cost of health care in the United States is partially driven by an over-emphasis on low-value health care that is potentially harmful and offers little benefit to most patients.
New research by Jodi Segal, MD, and colleagues, advances efforts to solve the low-value care problem by placing a spotlight on health care system factors that likely contribute to an overuse of care. The work is analyzed in the latest NIHCM Research Insights. Key findings include:
Systems that are investor-owned, or have fewer primary care physicians, are more likely to be associated with the overuse of care.
Systems that have major teaching hospitals are less likely to overuse care.
To continue investigating, evaluating, and addressing the drivers of overuse, the research team updated their Overuse Index tool. This Index may be especially useful for health systems seeking to monitor care use performance over time. This study’s findings may support future research and interventions to increase the use of high-value care.
Posted on October 12, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Unknown and Under-Appreciated by Many
By Rick Kahler CFP®
I recently talked with an administrator of a private medical practice about some of the financial challenges she faces in dealing with the medical system, insurers, and patients.
Some of the insights she gave me into the realities that private physicians face in providing medical care were rather disturbing.
***
Here are a few of them.
Let’s start with the insurers who account for the bulk of their revenue. Many payments for procedures from insurance companies (including Medicare) are below the cost of providing the service. This forces physicians to make up the difference on other procedures or find other sources of income to sustain the profitability of the practice.
Conversely, in markets that have just one hospital, the insurance companies have no leverage. If the insurers won’t pay what the hospitals demand, the hospitals can threaten to drop out of the network, leaving the insurers with nowhere to send their insureds in those markets. The insurers end up agreeing to pay the hospitals more.
Charges for services provided in-house at the hospital can end up being substantially higher than those same services done by outside providers.
Example:
She gave me an example of a lab test that cost $1,500 to $2,000 at the hospital lab but $35 to $80 at an independent lab. Patients do have the option to direct the hospital to use an independent lab. But, how many people know that and will have the presence of mind to make the request? While it makes financial sense to price-shop if you have a high deductible HSA plan, there isn’t much incentive if your plan has low deductibles.
Collections
Another challenge is collecting from patients. She says a surprising percentage of Americans maintain checking accounts with no money or keep checks from accounts which have long been closed. While writing bad checks is a crime, those who game the system know they can probably get by with writing a low-dollar check because the cost of pursuing justice is much more than the check is worth.
Most companies would never do business with such a person again. Healthcare professionals tend to have a bias toward giving everyone services, so these same people do return requesting care. She said she and her physician employer have had huge internal arguments about this. Her position is that these people take advantage of the physician in a premeditated fashion and don’t deserve to be extended services. The physician argues that everyone, even deadbeats, deserves healthcare. Since the practice doesn’t provide life-and-death services, she was able to get the physician to agree that if someone has an outstanding bill they need to settle it upfront, in cash, before any new services are provided.
Then there are those who use credit cards and then fraudulently dispute the charges. Some providers let this go because of the difficulty of proving that the charge is legitimate. It requires photographs of customers during the transaction, copies of driver’s licenses, customers’ signatures on the paperwork, and notarized statements from the provider verifying that this was the person who received services and presented the credit card.
A final interesting point concerned patients’ Social Security numbers. She said the only time these are ever needed is when an outstanding bill is sent for collection. Otherwise, they are never accessed or used.
Assessment
Finally, she was quick to add that only a small fraction of their patients premeditate stealing from them. She also stressed that not all insurance companies or hospitals behave unethically, and some do wonderful, humane acts of kindness. Nevertheless, the lack of integrity that does occur on both sides is infuriating and adds to the cost of health services.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, urls and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Contact: MarcinkoAdvisors@msn.com
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, I.T, business and policy management ecosystem.
Posted on October 11, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
Book Marcinko for your Next Financial Planning Seminar, Meeting or Medical Business Event
By Ann Miller RN MHA
Professor and physician executive David Edward Marcinko MBBS DPM MBA MEd BSc CMP® is originally from Loyola University MD, Temple University in Philadelphia and the Milton S. Hershey Medical Center in PA; Oglethorpe University, and Atlanta Hospital & Medical Center in GA; and the Aachen City University Hospital, Koln-Germany. He is one of the most innovative global thought leaders in health care business and entrepreneurship today.
Dr. Marcinko is a multi-degreed educator, board certified physician, surgical fellow, hospital medical staff President, Chief Education Officer and philanthropist with more than 400 published papers; 5,150 op-ed pieces and over 125+ international presentations to his credit; including the top 10 biggest pharmaceutical companies and financial services firms in the nation. He is also a best-selling Amazon author with 30 published text books in four languages [National Institute of Health, Library of Congress and Library of Medicine].
Dr. Marcinko is past Editor-in-Chief of the prestigious “Journal of Health Care Finance”, and a former Certified Financial Planner®, who was named “Health Economist of the Year” in 2001. He is a Federal and State court approved expert witness featured in hundreds of peer reviewed medical, business, management and trade publications [AMA, ADA, APMA, AAOS, Physicians Practice, Investment Advisor, Physician’s Money Digest and MD News].
As a licensed insurance agent, RIA and SEC registered endowment fund manager, Dr. Marcinko is Founding Dean of the fiduciary focused CERTIFIED MEDICAL PLANNER® chartered designation education program; as well as Chief Editor of the HEALTH DICTIONARY SERIES® Wiki Project. His professional memberships include: ASHE, AHIMA, ACHE, ACME, ACPE, MGMA, FMMA and HIMSS.
Dr. Marcinko is a MSFT Beta tester, Google Scholar, “H” Index favorite and one of LinkedIn’s “Top Cited Voices”.
Posted on October 9, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Steve Febus
***
***
Hospital Finance 101: Understanding the Cost of Full-Service Healthcare in Pullman, WA Program by: Steve Febus, Pullman Regional Hospital Chief Financial Officer.
Navigating a course where sound organizational management is intertwined with financial acumen requires a strategy designed by subject-matter experts. Fortunately, Financial Management Strategies for Hospital and Healthcare Organizations: Tools, Techniques, Checklists and Case Studies provides that blueprint. ―David B. Nash, MD, MBA, Jefferson Medical College, Thomas Jefferson University
It is fitting that Dr. David Edward Marcinko, MBA, CMP™ and his fellow experts have laid out a plan of action in Financial Management Strategies for Hospital and Healthcare Organizations that physicians, nurse-executives, administrators, institutional CEOs, CFOs, MBAs, lawyers, and healthcare accountants can follow to help move healthcare financial fitness forward in these uncharted waters. ―Neil H. Baum, MD, Tulane Medical School
Posted on October 2, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Staff Reporters
***
Most likely to have an identity crisis: The Inflation Reduction Act
After a seemingly endless will-they-or-won’t-they make a deal dance, Democrats passed their signature piece of legislation, the Inflation Reduction Act, without Republican support.
The 755-page climate, tax, and healthcare package does a lot of things: It establishes a 15% minimum tax on megacorporations, boosts funding for the IRS, allows Medicare to negotiate prescription drug prices, offers $260 billion in tax credits for renewable energy projects, and more. One thing it likely won’t do: reduce inflation. Despite the name, the law’s impact on rising prices through 2023 is expected to be “negligible.”
Cityblock Health has raised $400 million in its latest funding round. This brings the value of the startup to a whopping $5.7 billion. The company focuses on delivering care to patients in marginalized groups, aiming to provide care for 10 million patients by the end of the decade. Two key parts of the company’s strategy is integrating community support into care plans and connecting members with resources and specialized providers.
According to a spokesperson for Cityblock Health, “We can confirm that Cityblock has raised a new round of capital as we continue to accelerate our plans to empower more people across the country more quickly. Millions of marginalized and lower-income people across the U.S., including those who receive their healthcare through Medicaid plans, continue to lack sufficient access to integrated, community-based health services. We are leveraging this investment to reach more people and have an even greater impact.”
Posted on September 10, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Jessie Hellmann
***
***
Doctors are again ramping up what has become a perennial lobbying campaign to urge Congress to increase Medicare payments in order to offset cuts scheduled to go into effect Jan. 1. The cuts, the result of a 2020 Centers for Medicare and Medicaid Services decision to increase payments for underpaid services like primary care and maternal health, are meant to offset the costs of increasing payments for those services.
Without action from Congress, the Medicare conversion factor, which is used to calculate billing codes into payment rates, would see a 4.5 percent cut, amounting to about $3 billion or $4 billion less for providers paid under the Medicare Physician Fee Schedule. As in past years, more expensive specialties like radiology, surgery, and podiatry are estimated to see the largest cuts, ranging from 4 to 7 percent.
Posted on September 5, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Robert King
***
***
The U.S. Court of Appeals for the District of Columbia just ruled that it did not have the power to overturn the Occupational Safety and Health Administration’s (OSHA’s) decision to scrap a temporary protection standard that outlined requirements for hospitals to keep front-line health workers safe from contracting COVID-19. The union National Nurses United decried the decision.
OSHA issued a temporary protection standard for COVID-19 back in June 2021. However, OSHA did not move to make a permanent standard before the temporary one expired last year, as the agency shifted resources toward a vaccine mandate, the appellate opinion said. OSHA had called for health systems to still impose the standard’s requirements voluntarily.
Posted on September 1, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Eric Bricker MD
***
As a result of SDOH problems, Johns Hopkins Hospital Trains Doctors That Have a Ton of Exposure to Diseases That Result from These Social Determinantsof Health: 1) Endocarditis, 2) Hepatitis C, 3) HIV, 4) Pancreatitis, 5) Liver Cirrhosis, 6) Diabetes, 7) Heart Attack, 8) Stroke, 9) Infections, 10) Cancer, 11) Spinal Injuries, 12) Dialysis, 13) Diabetic Ketoacidosis and 14) Hypertensive Emergencies.
Johns Hopkins Hospital Also Loses MoneyWhen Treating These Diseases Caused by Social Determinants of Health.
Posted on July 28, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Eric Bricker MD
Healthcare Stock and IPO Investing Can Be Confusing. The Story of Privia Health is a Good Case Study in Understanding the Underlying Economics in Healthcare Investing:
Posted on July 26, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By Dr. Keith L. Gurnick, DPM
[Los Angeles, CA via PM Online]
***
***
Paid spokespersons consisting exclusively of older celebrities, including William Shatner, George Forman, Joe Namath, and Jimmie “J.J.” Walker read similar, if not exact, scripts in an attempt to induce the elderly to phone and check their “zip code” to see if they are eligible. I can’t figure out what the zip code has to do with anything, but maybe someone can help me to understand this fish hook?
As of November 2021, 42% of all Medicare eligible patients are enrolled in Medicare Advantage plans. Does the viewing public not wonder why there is never any mention at all during these commercials that changing to a Medicare Advantage plan means switching their traditional Medicare over to an HMO, and that most likely they will lose their network of doctors and possibly hospitals as well?
Posted on July 21, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
Cigna, do you even have a clue that dentists don’t like you?
***
By Darrell K. Pruitt DDS
***
Hi Dr. Pruitt,
I’m truly sorry for any negative experience you’ve encountered with us. Is there a claim, benefit, or authorization concern I can help with? Please email me at LetUsHelpU@cigna.com. I’d like an opportunity to assist.
At a time when interest rates are surging, and just when I request an increase, CIGNA REDUCED MY REIMBURSEMENTS! Never again will I do business with you, and will discourage other dentists from falling into your trap …. And that is why dentists don’t like #TeamCigna.
What is your name, anyway. You know mine. Perhaps Linkedin’s transparency makes it a poor choice for marketing Cigna.
Asif things could get no worse between Cigna and dentists, you censored my response!
NOTE: Cigna representatives prefer to remain anonymous for reasons of accountability.
Posted on July 13, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
By MCOL.com
Dr. Seleem R. Choudhury
***
***
“Uberization” is a catchphrase that has quickly become part of common parlance in discussions about the pandemic-induced economy. Uberization is the movement by organizations to “replace fixed wage contracts with ‘dynamic pricing’ for labor” (Davis, & Sinha, 2021). It is transforming many elements of the economy and replacing employees employed by the organization with a type of self-employed or contract employee. In essence, it allows businesses to “recruit labour at a large scale in new ways” (Davis, & Sinha, 2021).
The global business community has had a range of responses to the trend of uberization (Babali, 2019), as has the healthcare industry in particular. Yet as health systems emerge from the pandemic, Bloomberg reports that “the ongoing elevated costs of [healthcare] workers are causing profit warnings” (KHN, 2022; Court, & Coleman-Lochner, 2022). Regardless of one’s resistance or acceptance of uberization, healthcare employment is in crisis. Change must occur to keep health systems from financial disaster.
It seems that the tide of uberization in the healthcare industry is already rising. An increasing number of employees are contracting with hospitals and health systems via a staffing agency. This trend is likely to evolve, with a portion of staff employed directly by the hospital, and the remaining employees self-contracting with hospitals or health systems with short-term or even daily contracts. In fact, hospitals are reporting that rather than temporary “travel nurses” coming from other states to work on a contract basis, nurses are taking short-term contract work at hospitals a short drive from their own homes rather than pursue permanent employment with these organizations. We are witnessing the uberization of nursing, which will eventually extend to other healthcare occupations.
Why uberization?
The healthcare workforce shouldered the heavy burden of fighting the COVID-19 pandemic. Yet a collaborative study from Indiana University, the nonprofit Rand Corp., and the University of Michigan that analyzed the changes in the U.S. healthcare workforce during the COVID-19 pandemic found that “the average wages for U.S. healthcare workers rose less than wages in other industries during 2020 and the first six months of 2021” (Toler, 2022; Cantor, Whaley, Kosali, & Nguyen, 2022). According to a February 2022 report by the U.S. Bureau of Labor Statistics, only about 35 percent of healthcare and social assistance organizations “increased wages and salaries, paid wage premiums, or provided bonuses because of the COVID-19 pandemic” (U.S. Bureau of Labor Statistics, 2022).
Due to the media attention the “Great Resignation” has received, it is common knowledge that workers across industries have been leaving their jobs at higher rates than before the pandemic (Parker, & Horowitz, 2022). Yet by October 2021, when the “quit rates” were at their highest recorded levels, healthcare and social assistance job resignations had increased to 35% higher than they had been before the pandemic, slightly higher than the increase of resignations among all workers in the same period (29%) (Wager, Amin, Cox, & Hughes-Cromwick, 2021).
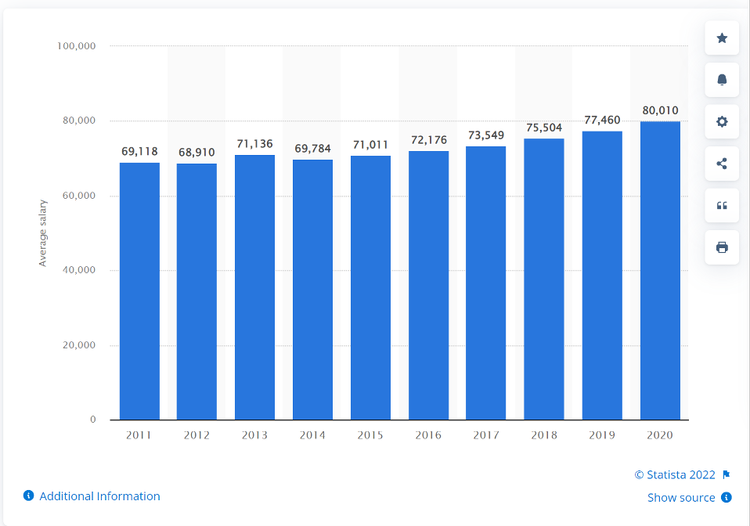
Over the last ten years, “the salary of registered nurses increased by 1.67 percent in the United States” (Michas, 2021). Whereas healthcare executives make on average eight times more than their hourly employees (Saini, Garber, & Brownlee, 2022). The pandemic has rebalanced the scales in favor of those underpaid for many years. The salary landscape has changed, and in response many hospital systems blindly grasp to the pre-pandemic state of agency staffing. This, combined with near flat salary increases, contribute to the uberization of healthcare.
For many healthcare professionals, the combination of work-related stress and incommensurate compensation was the final straw. However, in addition to fair salary, flexibility has become a top demand of employees—even in healthcare. “Gone are the days when job security or pay was everything. Workers now are giving more thought to how their jobs fit into their lives. Ambition for ambition’s sake is being reassessed” (Buckingham, & Richardson, 2022).
A recent survey articulated “higher pay and dissatisfaction with management were also key drivers of nurses changing work settings in 2020 or 2021,” with 28% of respondents saying they’ve changed work settings (Lagasse, 2022). The percentage of nurses considering changing employers increased by 6% from 2020 to 2021, with 17% saying they are contemplating making an employment change. The percentage of nurses who are “passive job seekers – not actively looking for a new job but open to new opportunities – also increased, from 38% in 2020 to 47% in the current survey” (Lagasse, 2022).
The moment: contractor or non-contractor
As the trend of uberization continues to spread beyond the transportation industry, the global business community should be watchful of challenges that the trendsetter Uber is facing to understand future implications of this movement in their own industry. For example, recent legal battles regarding the employment status of Uber drivers will likely impact the cost-benefit analysis of those considering traditional employment or independent contracting. While an independent contractor is free to offer services to anyone and doesn’t have the limits on their freedom that comes with being an employee of a single organization, the U.S. National Labor Relations Board decision that Uber drivers are independent contractors means that drivers have no federal right to unionize (HyreCar, 2021; Fishman, 2020). In Europe, however, Uber drivers are considered employees and not independent, which could mean that unionization could occur en masse.
The future
The future of healthcare employment could be via an app on smart phones. Imagine: daily staffing supplemented by workers employed and credentialed through the app. The healthcare worker could choose their rate and shifts, and the hospital could determine the desired experience, quality, and patient experience reviews for the open position. It could shift the future of employment healthcare significantly.
The rate of change in today’s workplace is accelerating whether it is through the uberization of healthcare workers or advancements in workers’ rights. A recent New York Times article entitled “The Revolt of the College-Educated Working Class” states: “The support for labor unions among college graduates has increased from 55 percent in the late 1990s to around 70 percent in the last few years, and is even higher among younger college graduates” (Scheiber, 2022).
This may have a ripple effect on the healthcare workforce. Years of stagnating salaries and organizations’ undefined workforce vision has primed the industry for action with record job-quits within healthcare. This has proven especially true in rural markets where recruitment of permanent and agency staff has posed numerous challenges. Our current climate potentially opens the door for workers to leverage themselves via the advocacy of a union.
Summary
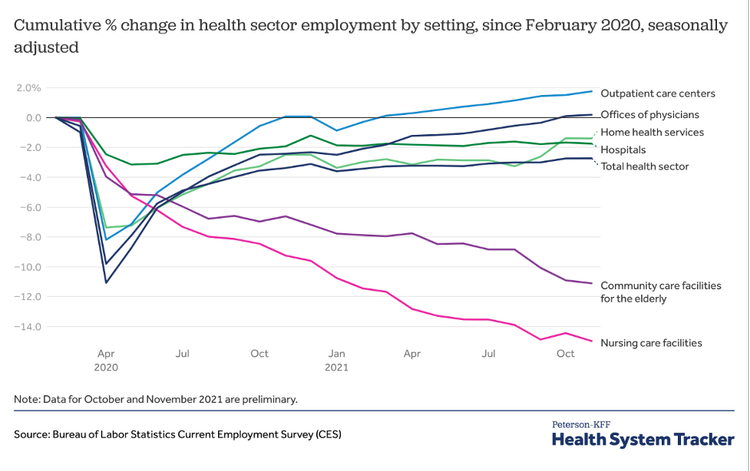
The labor supply and demand are out of balance. The long-term effects on the health sector labor market from the pandemic are unknown, but changes in healthcare delivery (such as the growth of telehealth) may lead to lasting shifts in the healthcare industry. Fierce competition for healthcare workers means that employers must go beyond good pay and benefits to attract the best candidates. Healthcare recruitment is a zero-sum game. There isn’t a pool of healthcare workers lying idle, and so recruitment is often at the cost of a competitor. The employee knows that this demand exists, and this could further drive the uberization of healthcare workers. However, there is potential for this new movement to benefit both parties. As limited number of employees equates to skill scarcity which drives salaries, hospitals could utilize their skilled workforce based on need and demand.
Posted on July 1, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
My Laundry Wish List for all US Healthcare Stakeholders
By Dr. David Edward Marcinko; MBA, CMP™
[Publisher-in-Chief]
As President Obama spoke, prodded and cajoled for Congress to pass HR 3200-3400 in 2008, I believe that for any healthcare reform effort to work successfully for the American people – for the long term – we need to consider the following in no particular prioritized order:
Insurance portability uncoupled from patient employment
Health insurance regional exchanges with inter-state purchase competition
Doctor, drug, DME and hospital pricing and payment transparency for HSAs, and all of us
Modifying or eliminating AMA owned CPT Codes®; a huge money maker for them
Abandoning ala’ carte medicine for values-based outcomes
Reduce JCAHO influence; encourage competition from Norwegian Det Norske Veritas [DNV]
Reduce big-pharma influence thru-out the entire medical education, career and care pipeline
End DTC advertising from big-pharma
Promote wholesale drug purchase competition, MC bidding and generic drugs
Encourage evidence-based medicine, not expert-based medicine
Less pay for medical specialists with a re-evaluation of the hospitalist concept
Advance the dying art of physical diagnosis, teach and embrace Paretto’s 80/20 rule for clinic issues
Reduce lab test, diagnostic imaging and testing
Encourage private 24/7/365 medical offices and clinics; and on-site and retail clinics
Abandon P4P, medical homes and disease management ideas
Give more economic skin-in-game to patients relative to health benchmarks
Concretize the “never-event” prohibitions and include a list of patient health responsibilities
More pay for primary care docs and internists
Adopt digital records and cloud computing for patients
Phase in true eHRs incrementally; and abandon CCHIT for open source SaaS
Promote Health 2.0 social media.
Augmented scope of practice, numbers and pay for NPs and DNPs, etc
Reduce pay for CRNAs and increase it for staff RNs
Develop step down triage and treatment units to reduce the number of full service ERs
Increase medical, osteopathic, dental, optometric and podiatric medical school classes
Increased practice scope for dentists, podiatrists and optometrists
Make some sort of catastrophic HI mandatory, much like auto insurance for all
End pre-existing conditon health insurance contract clauses
More choice and end of life control for the terminally ill patient
Increase marketplace competition with fewer political and financial “externalities”.
Teach basic healthcare topics in school and encourage physical exercise
Health and insurance education should be, but is not, the “answer” for Americans
Protect borders and discourage undocumented illegals
Adopt medical malpractice tort reform
Make all stakeholders fiduciaries
No public “option” unless you like food stamps, Section 8 housing, public transportation and schools
Budget deficit neutrality
Slow down!
Assessment
Recently, while in the Baltimore/Washing area, I was asked by several reporters to opine on the healthcare debate; which I did so freely having never been known as the shy type. And, regular readers will note that many of these items have been used as posts or comments on this ME-P. Unfortunately, my “laundry list” interview was pre-empted by two local but boisterous town-hall meetings with respective passionate politicians. It was redacted no doubt, but never broadcast. Thus, I missed the potential for my “five minutes” of fame. C’est la vive!
Conclusion
There you have it; direct and straight forward. And so, your thoughts and comments on this Medical Executive-Post are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Posted on June 30, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
By Darrell Pruitt DDS
***
***
“How Is The Market Feeling About Cigna?” Spoiler – According to Benzinga insights, the market is not optimistic about Cigna’s future. Neither am I. But then, I’m only their clients’ dentist.
Posted on June 9, 2022 by Dr. David Edward Marcinko MBA MEd CMP™
***
BY HEALTH CAPITAL CONSULTANTS, LLC.
DEFINITION: Vertical integration is an arrangement in which the supply chain of a company is integrated and owned by that company. Usually each member of the supply chain produces a different product or service, and the products combine to satisfy a common need.
A study released in the December 2021 issue of Health Affairs examined the correlation between hospital/health system ownership of physician practices and physician compensation. While a number of studies have analyzed the “rapidly growing trend” of vertical integration from the hospital/health system perspective, this is the first study to evaluate vertical integration from the physician practice perspective.
This Health Capital Topics article will discuss the study’s findings and potential implications. (Read more…)
























































































 Due to the media attention the “Great Resignation” has received, it is common knowledge that workers across industries have been leaving their jobs at higher rates than before the pandemic (Parker, & Horowitz, 2022). Yet by October 2021, when the “quit rates” were at their highest recorded levels, healthcare and social assistance job resignations had increased to 35% higher than they had been before the pandemic, slightly higher than the increase of resignations among all workers in the same period (29%) (Wager, Amin, Cox, & Hughes-Cromwick, 2021).
Due to the media attention the “Great Resignation” has received, it is common knowledge that workers across industries have been leaving their jobs at higher rates than before the pandemic (Parker, & Horowitz, 2022). Yet by October 2021, when the “quit rates” were at their highest recorded levels, healthcare and social assistance job resignations had increased to 35% higher than they had been before the pandemic, slightly higher than the increase of resignations among all workers in the same period (29%) (Wager, Amin, Cox, & Hughes-Cromwick, 2021).