By Dr. David Edward Marcinko MBA MEd
BASIC DEFINITIONS
***
***
The Direct Reimbursement Payment Model allows physicians to receive payment directly from patients or employers, bypassing traditional insurance systems. This model emphasizes transparency, autonomy, and personalized care, offering an alternative to fee-for-service and managed care structures.
The Direct Reimbursement Payment Model is a healthcare financing approach in which physicians are paid directly by patients or sponsoring entities—such as employers—rather than through insurance companies or government programs. This model is gaining traction as a response to the administrative burdens, opaque billing practices, and fragmented care often associated with traditional insurance-based systems.
One prominent example of direct reimbursement is Direct Primary Care (DPC). In DPC, patients pay a recurring fee—monthly, quarterly, or annually—that covers a broad range of primary care services. These include routine checkups, preventive screenings, chronic disease management, and basic lab work. By eliminating third-party billing, DPC practices reduce overhead costs and administrative complexity, allowing physicians to spend more time with patients and focus on quality care.
***
***
Employers have also embraced direct reimbursement models to manage healthcare costs and improve employee wellness. In such arrangements, employers reimburse physicians or clinics directly for services rendered to their employees, often through a defined benefit structure. This can be part of a self-funded health plan or a supplemental offering alongside high-deductible insurance policies. The goal is to provide accessible, cost-effective care while avoiding the inefficiencies of traditional insurance networks.
Key advantages of the direct reimbursement model include:
- Price transparency: Patients know upfront what services cost, reducing surprise billing and financial stress.
- Improved access: Physicians often offer same-day or next-day appointments, extended visits, and direct communication via phone or email.
- Lower administrative burden: Without insurance paperwork, practices can operate more efficiently and focus on patient care.
- Stronger patient-physician relationships: More time per visit fosters trust, continuity, and better health outcomes.
However, the model is not without limitations. Direct reimbursement may not cover specialist care, hospitalization, or emergency services, requiring patients to maintain supplemental insurance. Additionally, the model may be less accessible to low-income populations who cannot afford recurring fees or out-of-pocket payments. Critics also argue that widespread adoption could fragment care and reduce risk pooling, undermining the broader goals of universal coverage.
Despite these concerns, the direct reimbursement model aligns with broader trends in healthcare reform, including value-based care, consumer empowerment, and decentralized service delivery. It offers a viable path for physicians seeking autonomy and for patients desiring personalized, transparent care. As healthcare continues to evolve, hybrid models that combine direct reimbursement with traditional insurance may emerge, offering flexibility and choice across diverse patient populations.
In conclusion, the Direct Reimbursement Payment Model represents a meaningful shift in how healthcare services are financed and delivered.
By prioritizing simplicity, transparency, and patient-centered care, it challenges the status quo and opens new possibilities for sustainable, high-quality medical practice.
COMMENTS APPRECIATED
SPEAKING: Dr. Marcinko will be speaking and lecturing, signing and opining, teaching and preaching, storming and performing at many locations throughout the USA this year! His tour of witty and serious pontifications may be scheduled on a planned or ad-hoc basis; for public or private meetings and gatherings; formally, informally, or over lunch or dinner. All medical societies, financial advisory firms or Broker-Dealers are encouraged to submit an RFP for speaking engagements: CONTACT: Ann Miller RN MHA at MarcinkoAdvisors@outlook.com -OR- http://www.MarcinkoAssociates.com
Like, Refer and Subscribe
***
***
Share this:

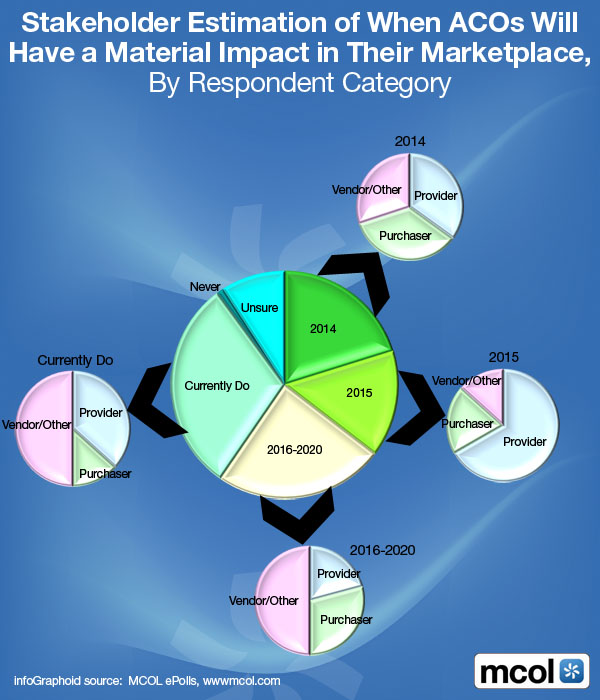
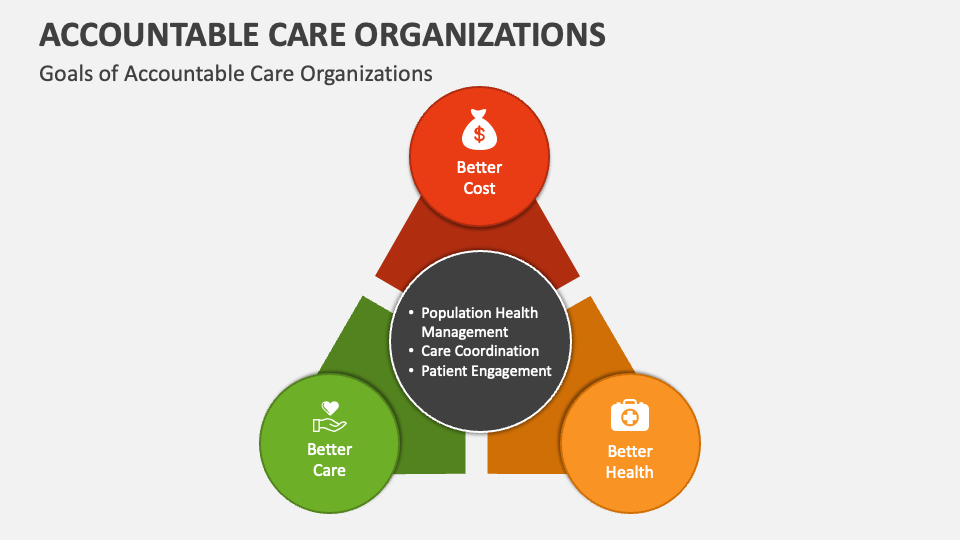
Filed under: "Doctors Only", Ask a Doctor, Career Development, Funding Basics, Glossary Terms, Health Economics, Health Insurance, Health Law & Policy, Healthcare Finance, Insurance Matters, Managed Care, Marketing & Advertising | Tagged: ACOs, david marcinko, direct primary are, direct reimbursement payment, DO, doctors, DPC, DPM, health, healthcare, MD, mental health, physicians, value based csare, VBC | Leave a comment »












































 ***
***