Are Doctors Responsible?

By Dr. Pankaj Kumar
Namaste!
The following features have led to increasing dependence on investors in the medical field which then has to run along the lines of an industry to ensure its financial viability.
For example:
1. Newer technology and rapid advances in newer innovations in medical fields for improvement in diagnostic and newer treatment modalities: If a hospital or doctor does not upgrade, it will be regarded as having obsolete technology. Most of these medical technologies are extremely expensive and owned and marketed by big multinational companies who sell them. Since cost involved is very high, there can be various types of deals involved between middlemen involved in selling and buying the equipment and technologies. Doctors are the end users of these technologies, but not part of business process. They are actually the consumers and users for these technologies.
2. Expensive real estate: A self made doctor at the start or even during his life time, does not have the kind of finances to build a hospital which needs a large parcel of land with commercial location. Therefore there is a need for big investment or investor to pitch in and invest funds. And if they invest, obviously they would look for some returns.
3. Equipping the Hospital: Building of hospital with the infrastructure and equipping it well needs lot of money and investment which only an investor can provide. Same is true for maintenance of equipment, bills, insurances, AMC etc.
4. Staffing of Hospital: A hospital needs lot of skilled human resources, health care being a highly labour intensive industry. Doctors , nurses, technicians, para medical, administrative and clerical staff is required. Employment of non medical in hospital industry too has been increasing because of various regulatory requirements and complex processes other than just treating patients.
5. High regulatory requirements: globally the requirements of regulatory authorities have been sky rocketing and it requires a lot of manpower to maintain such data. Getting accreditation etc are processes which requires manpower, time, and a legal team. All these legal requirements are expensive.
6. Consumer protection act: This single important factor can increase the cost of healthcare for the patient. As doctors are increasingly scared of being dragged to court, they are always on backfoot and are forced to do defensive practice. Investigations are required for documentation. Patient and courts will ask for proof and goes by documentation. Medical problems are very complex and sometimes it is difficult to judge the future course of disease or decisions for surgery, or how patient will behave before or after surgery. A doctor, thus, will always try to play safe legally in present scenarios. Because everything he does will be scrutinized later, with retrospective wisdom, by courts. And since doctors manage so many patients everyday, they never know which one will harass and deceive them later. Mistrust has increased to such an extent that patient relatives do not understand even if things are told in good faith and in patient’s interest. Summarily doctors have to safeguard themselves from treatment as well as legal and documentation hassles.
7. Expensive legal services: Every case that goes to court involves lawyers and their expensive fees. Most of the time even though the doctors may be right, he has to defend himself with the help of lawyers. Law industry has been benefitted enormously because of consumer protection act at the cost of doctors. Increasing mistrust and unhappiness in patient’s mind definitely does not help patients and doctors. Strangely doctor’s fee are quite low but lawyers charges them astronomical amounts, which are beyond any logic.
8. Increased expectation of patients: People want exceptional care, best in the world with best technology, that also at a price less than even a meal in restaurant, and then they want a quick relief!! This is an expectation almost impossible to fulfil. Even government hospitals, which are funded by taxayer’s money find it difficult to provide free treatment with quality.
9. Large claims given by courts: in a country where people fight with their parents, brothers and sisters for money and property, it will be naive to think that idea of making money from doctor does not exist. With court compensations going into crores, doctors can sense many times that some patient relatives try to use the opportunity. They have nothing at stake so they try to make some noise on social media and harass the doctor in court or on social platforms. Even for patients, who had poor prognosis at the very onset of treatment, relatives can create problems. Doctors have no protection from these nuisanse. All these factors further enhance insecurity in doctor’s mind.
10. Expensive and time consuming medical education, on sale: Although an open secret , as reported routinely in news, medical seats are big business. Each private medical college seat sells for huge money. Such doctors, who have purchased seats have already behaved as investors. Once these doctors are in practice, they will try to recover the investment. This can obviously push up the health care costs not to mention vitiation of the medical fraternity.
11. Requirement for maintaining huge data and audits: to maintain standards, to have accreditations, for medicolegal issues , large data storage, audits and surveillance is required. These systems also need new systems and manpower.
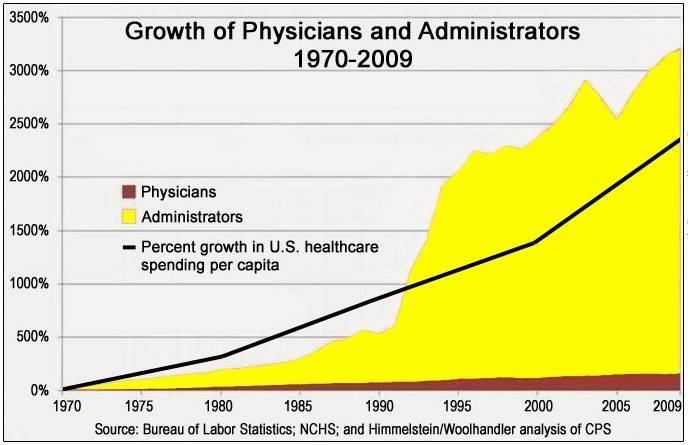
12. Employment of large numbers of non-medical personnel: earlier management work was handled by doctors. All senior doctors were given small and differnet departments of administrative work at very little or no extra cost. But now for all these works separate administrators are appointed. Now a days ratio of doctors to nondoctors is higher as compared to previous years. Increased regulatory and and insurance system needs more non- medical staff. But productivity of hospital still remains by doctor-patient interaction. This change in arrangement in Hospitals has caused increase in costs and hence pushed the health care expenses. Advantages and disadvangages of these changes in arrangement will be known with time in future.
13. Non regulation of businesses associated with large health care industry: for example pharma industry, suppliers , biomedical, equipments, consumables. Such individuals, although play important part in medicine, cost, sale and purchase, but are largely unregulated. Unlike doctors, who are regulated by multiple governing bodies. But doctors are often perceived as culprits for these costs escalation.
14. Increasing extinction of Single doctor and small setups: for them it will be difficult to keep pace with newer technology and buying expansive equipments. It will be difficult for them to manage requirements of new medical system, legal problems . At the most they will continue to provide cheap medical services, but for only common and simple ailments. It will be difficult to manage serious patients and sick and complex patients in view of high public expectations . These set ups are under severe security threat and pressure because of non – acceptance of even genuinine complications of treatment. As legal requirements increase, these systems will become unviable and option of common public for cheaper, friendly services may become extinct. So it will decrease the easy and sometimes last option of doctors to settle with a small set up. Chances of them to work for investors and insurance companies will increase, and they will be cheap labour for industry.
15. Medical and health Insurance becoming indispensible: Insurance companies are every where. They sell policies to patients , as well as doctors. In fact, they are positioned between doctor and patients. They make money from both sides. Obviously more expensive the treatment, more dependence on insurance. Therefore a cycle has been set up. Increase in insurance cost will push health care more expensive and a vicious cycle is set up. One should not be surprised, if in future treatment to a large extent will be dictated by insurance companies.
16. Conversion to a industry: Because of above reasons Medical and health care has become an industry and needs investors. So as it is business proposition. Funded by investors and run on commercial principles, the doctors are being slowly reduced to skilled labour, alienated from the core.
17. Aging, multiple diseases: as life expectancy is increasing, it is leading to multiple diseases and more complex diseases and new expensive treatments. In this changed scenario and all people want to prolong life as much as possible. Cost of prolonging life with multiple problems is quite high. It consumes more medication and resouces and hence consequently pushes up the cost of medical treatment.
18. Evolution of complex infections: Advent of antibiotics and germ theory was thought to be game changer in medical history. But because bacteria proved to be smarter than humans and acquired resistant. New and expensive antibiotics have been gradually being rendered useless. Need for more antibiotics is causing treatment to be costlier.
19. Evolution of advanced treatment: Invention of Expensive and new diagnostic techniques along with highly technical treatments by industry is not without added cost. Although it may be useful in certain patients, but how much it will help overall in masses, for general treatment, as it increases the cost of overall treatment.
20. Increasing need for heightened security: It is not uncommon to have mobs causing physical harms to medical workers and damaging hospital properties. These incidents have caused increased need for security for the premises and adding to the cost.
21. Complex interplay of various industries eg pharma industry and consumable industry: large number of consumables pharmaceuticals, sutures, surgical instruments, IT industry, drugs, implants, medical supplies are required. These industries supply their items on a price commanded by them and there is complex interplay of various industries.
22. Non uniform and variable care and cost: each city has multiple hospitals. Care and cost varies in every set up. Even all government set ups are not uniform in facilities and cost. Private setups vary in cost and care, to the extent of maximum possible variations. All this non-uniformity has created confusion in the mind of patients and variation in financial issues.
23. Poor public health care facilities: due to less expenditure on health care, government health care facilities have been under developed. Less investment by government has given way to private health care to flourish.
24: Conversion to a industry model and entry of investors: all the above investments are very expensive. Doctors usually do not have that much money to invest. Therefore Investors and financers have become indispensible part of health. once investor invests money, it will be driven on business principles.
25. Future course: I do not see in future that this arrangement is going to change , rather it will be strengthened more and more and quality care will become more costly. Doctors will be totally alienated from financial and business aspect, because industry will not be sustainable without an investor.

Assessment
As we look at reasons above, doctors are no where in the financial picture and to be blamed for increase in overall health cost. But, since only doctors are visible part of industry, who treat and interact with patients, often they are blamed for the cost. They have actually being alienated from financial aspect, barring small percentage of doctors, who are financially literate. Consequently, the doctors who will be unable to entrench themselves in the business milieu will be unfit in future and hence extinct.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
Contact: MarcinkoAdvisors@msn.com
https://www.crcpress.com/Comprehensive-Financial-Planning-Strategies-for-Doctors-and-Advisors-Best/Marcinko-Hetico/p/book/9781482240283
***
 8
8
Filed under: Health Economics, Health Insurance, iMBA, Inc. | Tagged: Dr. Pankaj Kumar, healthcare costs, Rising Healthcare Costs | 4 Comments »









































 ***
***




















 ***
***