

![]()
ME-P Special Report
Share this:

Filed under: Ethics, Experts Invited, Financial Planning | Tagged: Deception in the Financial Service Industry, fiduciary advisor, fiduciary oath, Financial Planning, Lon Jefferies MBA CFP® | Leave a comment »
ME-P SYNDICATIONS:
WSJ.com,
CNN.com,
Forbes.com,
WashingtonPost.com,
BusinessWeek.com,
USNews.com, Reuters.com,
TimeWarnerCable.com,
e-How.com,
News Alloy.com,
and Congress.org

![]()
![]()



BOARD CERTIFICATION EXAM STUDY GUIDES
Lower Extremity Trauma
[Click on Image to Enlarge]
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
![]()


 ePodiatryConsentForms.com
ePodiatryConsentForms.com
 “Providing Management, Financial and Business Solutions for Modernity”
“Providing Management, Financial and Business Solutions for Modernity”


![]()
Filed under: Ethics, Experts Invited, Financial Planning | Tagged: Deception in the Financial Service Industry, fiduciary advisor, fiduciary oath, Financial Planning, Lon Jefferies MBA CFP® | Leave a comment »
![]()
By Leanne Cole
***
***
Filed under: Experts Invited, LifeStyle | Tagged: Financial District New York, Leanne Cole, Wall Street | 1 Comment »
![]()
Be Ready for a Great 2016!

[By Patrick Bourbon CFA]
1. IRA – 401(k) / 403(b) retirement accounts – Are you on track for a comfortable retirement? You could increase the funding of your IRA and company retirement plan like a 401(k) or 403(b) accounts. 401(k) and 403(b) accounts allow individuals younger than 50 to contribute $18,000 each year, and individuals 50 and older to contribute $24,000. Some plans allow workers to make additional contributions of after-tax money.
For those under 50, the maximum is $53,000 for 2015. Doing so does not reduce your taxable income, but taxes are deferred on any earnings that the after-tax money makes. Later, some people roll these contributions into a Roth IRA, tax-free so the money would then grow tax-free. Traditional and Roth IRAs allow individuals younger than 50 to contribute $5,500 each year and individuals 50 and older to contribute $6,500. Even if you earn too much to contribute to a Roth IRA directly, you can open a traditional nondeductible IRA and convert it to a Roth; there is no income limit on traditional nondeductible IRAs or conversions. Returns generated in IRA and 401(k) / 403(b) accounts compound tax-free over their entire life.
2. Start tax planning! It’s not too early to think about taxes. Asset location & Tax efficiency Review your taxable and non-taxable accounts to ensure they are optimized for tax efficiency. If you have foreign bank accounts, make sure you comply with FATCA and FBAR (forms FinCEN 114, 8938, 8621…). If you have forgotten, you may look into the Offshore Voluntary Disclosure Program (OVDP) or Streamlined procedures.
3. Portfolio rebalancing Make sure you have rebalanced your portfolios to keep them in line with your goals, time horizon and risk tolerance. The market movements this summer may have thrown off your portfolio balance between stocks and bonds. David Swensen, the Chief Investment Officer at the Yale Endowment, performed an analysis that showed optimal rebalancing could add 0.4% to your annual return.
4. Harvest your capital losses Maybe it is time to sell some funds, ETF, stocks to generate some capital losses? Tax-loss harvesting is a method of reducing your taxes by selling an investment that is trading at a significant loss. Find out if you have any loss carryovers from prior years to be applied against capital gains (from sale of funds, ETF, stocks… in your taxable/brokerage accounts). If your current year’s capital losses exceed your capital gains, you have a net capital loss. You can use up to $3,000 of that loss ($1,500 if you are married filing separately) to offset other taxable income such as your salaries, wages, interest and dividends. If the capital loss is more than $3,000, you can carry over the excess and apply it against capital gains next year.
5. Emergency fund Don’t forget to establish or tune up your emergency fund. This is a good time to set aside money for next year’s cash needs. It is an account that is used to set aside funds to be used in an emergency, such as the loss of a job, an illness or a major expense.
6. Review your insurance policies Do you have a life, disability and long term care insurance? Make sure you and your loved ones are well protected if something happens to you. Your life may have changed (birth, marriage …). If you do have enough coverage it is also a good time simply to review the different types of coverage you have. Whole life or Variable Universal Life may help you reduce your taxes.
7. Health Spending Account Did you maximize your contribution to your healthcare HSA? The interest and earnings in this account are tax free! The maximum contribution for 2015 is $3,350 for an individual and $6,650 for a family ($1,000 catch-up over 55). The contributions are tax deductible and withdraws are non-taxable if they are used for medical expenses. Over the age of 65 you can withdraw funds at your ordinary tax rate (if the distribution is not used for unreimbursed medical expenses). Fidelity estimates that a 65-year-old couple retiring in 2014 will need $220,000 for health care costs in retirement, in addition to expenses covered by Medicare. The HSA can be a great source of tax-free money to pay those bills.
8. Required Minimum Distribution If you are age 70.5 or older, remember to take your required minimum distribution to avoid a potential 50% penalty.
9. 529 Plan Did you contribute to your 529 educational plan for your child/children? You can contribute $14,000 per year (annual limit) for each parent or you can pre-fund in a single instance up to five years’ worth of contributions, up to $70,000 (5 x $14,000). Together, that means a married couple can open a 529 plan with $140,000. Money saved in a 529 plan grows tax-free when used for eligible educational expenses, and some states have additional tax benefits for residents who contribute to a plan in that state.
10. Determine your net worth Add up what you own (home, car, savings, investments…) and subtract what you owe (mortgage, loans, credit cards, …). This will allow you to track your progress year to year. It may also give you some incentive to save more and create a better budget for next year.
11. Check your credit score Go to annualcreditreport.com and request a free credit report from each of the three nationwide credit reporting agencies. You’re entitled to one free report from each agency every 12 months.
12. Check your beneficiaries You can check the beneficiaries on your retirement accounts or insurance policies at any time, but it’s a good idea to do this at least annually.
13. Update your estate plan New baby? Newly married or divorced? Make sure your beneficiary designations reflect any changes. Don’t yet have an estate plan? Make that a new year’s resolution! Estate planning may include updating or establishing a “will” or trust that can help avoid public disclosure of assets in probate.
14. Spending and automated savings – You want to look ahead Did you review your budget and set up automated savings? You may have started the year with a clear budget, but did you to stick to it? Fall can be a good time of the year for your financial checkup and to reflect on your spending and develop a budget for next year. It is also a very good time to put whatever you can on automatic. Bills, recurring payments, even savings—the more you can put on auto pay now, the easier your financial life will be next year. With this year’s facts and figures in front of you, it will be easier to plan and prioritize your expenditures for next year.
Assessment

Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
***
Front Matter with Foreword by Jason Dyken MD MBA
![]()
“BY DOCTORS – FOR DOCTORS – PEER REVIEWED – FIDUCIARY FOCUSED”
***
Filed under: Experts Invited, Insurance Matters, Investing, Portfolio Management | Tagged: 2015 Year-End Financial Checklist, Financial Planning, Investing, Patrick Bourbon CFA | Leave a comment »
![]()
And … Business Owners
By Robert Whirley CPA
[Alpharetta, GA 30009]
As the end of the year approaches, it is a good time to think of planning moves that will help lower your tax bill for this year and possibly the next. Factors that compound the challenge include turbulence in the stock market, overall economic uncertainty, and Congress’s failure to act on a number of important tax breaks that expired at the end of 2014. Some of these tax breaks ultimately may be retroactively reinstated and extended, as they were last year, but Congress may not decide the fate of these tax breaks until the very end of 2015 (or later). These breaks include, for individuals: the option to deduct state and local sales and use taxes instead of state and local income taxes; the above-the-line-deduction for qualified higher education expenses; tax-free IRA distributions for charitable purposes by those age 70- 1/2 or older; and the exclusion for up-to-$2 million of mortgage debt forgiveness on a principal residence. For businesses, tax breaks that expired at the end of last year and may be retroactively reinstated and extended include: 50% bonus first-year depreciation for most new machinery, equipment and software; the $500,000 annual expensing limitation; the research tax credit; and the 15-year writeoff for qualified leasehold improvements, qualified restaurant buildings and improvements, and qualified retail improvements.
Higher-income earners have unique concerns to address when mapping out year-end plans. They must be wary of the 3.8% surtax on certain unearned income and the additional 0.9% Medicare (hospital insurance, or HI) tax. The latter tax applies to individuals for whom the sum of their wages received with respect to employment and their self-employment income is in excess of an unindexed threshold amount ($250,000 for joint filers, $125,000 for married couples filing separately, and $200,000 in any other case).
The surtax is 3.8% of the lesser of: (1) net investment income (NII), or (2) the excess of modified adjusted gross income (MAGI) over an unindexed threshold amount ($250,000 for joint filers or surviving spouses, $125,000 for a married individual filing a separate return, and $200,000 in any other case). As year-end nears, a taxpayer’s approach to minimizing or eliminating the 3.8% surtax will depend on his estimated MAGI and NII for the year. Some taxpayers should consider ways to minimize (e.g., through deferral) additional NII for the balance of the year, others should try to see if they can reduce MAGI other than NII, and other individuals will need to consider ways to minimize both NII and other types of MAGI.
The 0.9% additional Medicare tax also may require year-end actions. Employers must withhold the additional Medicare tax from wages in excess of $200,000 regardless of filing status or other income. Self-employed persons must take it into account in figuring estimated tax. There could be situations where an employee may need to have more withheld toward the end of the year to cover the tax. For example, if an individual earns $200,000 from one employer during the first half of the year and a like amount from another employer during the balance of the year, he would owe the additional Medicare tax, but there would be no withholding by either employer for the additional Medicare tax since wages from each employer don’t exceed $200,000. Also, in determining whether they may need to make adjustments to avoid a penalty for underpayment of estimated tax, individuals also should be mindful that the additional Medicare tax may be overwithheld. This could occur, for example, where only one of two married spouses works and reaches the threshold for the employer to withhold, but the couple’s combined income won’t be high enough to actually cause the tax to be owed.
We have compiled a checklist of additional actions based on current tax rules that may help you save tax dollars if you act before year-end. Not all actions will apply in your particular situation, but you (or a family member) will likely benefit from many of them. We can narrow down the specific actions that you can take once we meet with you to tailor a particular plan. In the meantime, please review the following list and contact us at your earliest convenience so that we can advise you on which tax-saving moves to make.
***

***
Year-End Tax Planning Moves for Individuals
***

***
Year-End Tax-Planning Moves for Medical Practices, & Business Owners
***

***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
***
Front Matter with Foreword by Jason Dyken MD MBA
![]()
“BY DOCTORS – FOR DOCTORS – PEER REVIEWED – FIDUCIARY FOCUSED”
***
Filed under: Accounting, Experts Invited, Taxation | Tagged: Robert Whirley CPA, Year End Tax Planning for Physicians | 5 Comments »
![]()

By Michael Lawrence Langan, M.D.
***
***

***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
[Foreword Dr. Phillips MD JD MBA LLM] *** [Foreword Dr. Nash MD MBA FACP]
***
Filed under: Ethics, Experts Invited, Risk Management | Tagged: physician health programs | 1 Comment »
![]()
 By Vitaliy Katsenelson CFA
By Vitaliy Katsenelson CFA
So many articles have been written recently about Apple — defending it or explaining why this glorious fruit will turn into a shriveling pumpkin by midnight (with Samsung’s help) — that I really haven’t felt the need to contribute to the unending debate.
But, when Apple’s stock crashed to $450 back in January 2013, we bought a little for our clients. After receiving an outraged e-mail from one of them calling the purchase “irresponsible” and proclaiming that everyone (including his neighbor) knows that Apple is going down to $300, I decided it was time to join the discourse. Clients rarely (almost never) contact us about stocks we own in their accounts. More important, this is far from the most “radioactive” stock we own or have owned.
So, here is a column on Apple, I wrote back then. I have no intention of defending or prosecuting the company, but I would like to share some thoughts about it that many pundits have either overlooked or ignored.
***

***
The Psychlogy
What makes Apple stock difficult to own is psychology. The company’s success since 2000 is a black swan. We tend to think of Nassim Nicholas Taleb’s black swans as significant random negative events, but Apple is a positive one. When co-founder Steve Jobs came back to the company in the late ’90s, Apple was about to take its last breath. Jobs pulled off a miracle. He revived the company’s computer product line, making Macs exciting again, and then came out with three revolutionary “i” products in a row: the iPod, iPhone and iPad. You could argue that the success of each “i” product in itself was a black swan, exceeding all rational expectations and revolutionizing, transforming and in some cases creating new categories of merchandise that had never existed before.
Revenue and Market Capitalization
Apple’s revenue and market capitalization deservedly surpassed those of almighty Microsoft Corp. — the hairy monster with stinky breath that performed CPR on dying Apple in the late ’90s by injecting liquidity into the company by buying its preferred stock. We have a hard time processing this highly improbable success and an even harder time imagining that there is another black swan about to take flight from the Apple labs, especially with no Steve Jobs around to sit on the egg.
Black swans come out of nowhere, unannounced, but their impact may be long-lasting. The wildly successful “i” gadgets dug a formidable moat around Apple. They created the most valuable and still most inspirational brand in the world, funded an enormous research and development effort, enabled huge buying power (Apple locks up supply and pays much lower prices than many of its competitors for parts), filled out a mature product ecosystem and stuffed Apple’s debt-free balance sheet with $137 billion — half the market capitalization of Microsoft. The moat is wide, deep and unlikely to be breached any time soon.
***

***
High Price
One reason the psychology of owning Apple stock is so difficult: it’s high price. (Note: I am talking not about its valuation but purely about its price.) Apple has had only one stock split since the late ’90s, when it was trading in double digits, and it now changes hands at about $450 (down from $700 just a few months ago). Stock splits create zero economic value in the long run — absolutely none. Apple could split its stock ten to one and you’d have ten $45 shares, and nothing about the company or its business would change. But, I’d argue that a 3 percent “slide” of $1.35 would grab fewer headlines than a $13.50 “drop” — there is a media magnification factor that is hard to ignore.
Hardware versus Software
Is Apple a hardware or a software company? This is a very important question because Apple’s net margins of 25 percent are dangerously higher than those of Microsoft, a software monopoly that, with the minor exception of the Xbox and its new venture into tablets, sells only software, which has a 100 percent incremental margin.
Apple is either a smart hardware company or a software maker dressed in hardware company clothes. Take a look at the PC businesses of traditional “dumb” hardware companies like Dell and Hewlett-Packard Co. (I am not insulting these companies, I am just highlighting their lack of PC-directed R&D.) They buy hard drives from Western Digital Corp., graphic cards from Nvidia Corp., processors from Intel Corp. and an operating system from Microsoft, then they have contract manufacturers put together these parts in Asia and ship PCs all over the world. Dell and HP engineers design the PCs but contribute minimal R&D to their boxes; most of the R&D is done by the suppliers. Dell and HP are really asset-lite marketing and logistics companies — this explains their razor-thin margins. (Side note: Because of a lack of fixed costs, Dell and HP can remain profitable despite the ongoing decline in PC sales.)
Same Surface
On the surface, Apple’s personal computer business is not that much different from Dell’s or HP’s: It uses the same highly commoditized hardware and it also outsources manufacturing, but Apple spends much more on the R&D of its own operating system and creates distinctive, innovative products. Apple gets to keep a slice of revenue that would otherwise go to Microsoft for the operating system. Also, Apple is able to charge a premium (usually a few hundred dollars per PC) for the aesthetic appeal and perceived ease of use of its products.
However, when it comes to the “i” devices, Apple is a much smarter hardware company; its value added goes further than just basic design and software. Though there is a lot of commoditized hardware that goes into an iPhone or iPad, Apple’s skill at fitting an ever-growing number of components into ever-shrinking devices constantly increases. Add world-class touch and feel, superior battery life and durability, and you have a package that turns what would otherwise be commodity items into highly differentiated, and undeniably sexy, products. Apple has even gone a step further and is designing its own microprocessors.
But — and this is a very important “but” — as phones and tablets mature, processor speed, battery life and weight will tend to become uniform across all devices. It is arguable that the competition has already caught up with Apple in the hardware race. As the hardware premium goes away, there will be only two premiums left: Apple’s brand and its ecosystem. (I will go into detail about the “i” ecosystem and what it means for Apple’s margins and profitability in my second essay posted below).
Note that I did not mention the software premium. Unlike Microsoft, which charges for the Windows operating system installed on PCs, Google gives away Android to anyone who dares to make a phone or a tablet. Unless Apple can maintain the operating system lead against Android, that premium will go away.
Assessment
Recently, I spent a few days playing with Nexus 7, Google’s Android-powered 7-inch tablet, which retails for $200 ($130 cheaper than Apple’s iPad mini). Nexus 7 is a good product, but I kept remembering that humans and monkeys share 98 percent of their DNA, and the Android operating system is missing the 2 percent that makes Apple iOS so special.
***
Apple’s ecosystem is an important and durable competitive advantage; it creates a tangible switching cost (or, an inconvenience) after Apple has locked you into the i-ecosystem. It takes time to build an ecosystem that consists of speakers and accessories that will connect only via Apple systems: Apple TV, which easily recreates an iPhone or iPad screen on a TV set; the music collection on iTunes (competition from Spotify and Google Play lessens this advantage); a multitude of great apps (in all honesty, gaming apps have a half-life of only a few weeks, but productivity apps and my $60 TomTom GPS have a much longer half-life); and, last, the underrated Photo Stream, a feature in iOS 6 that allows you to share photos with your close friends and relatives with incredible ease. My family and friends share pictures from our daily lives (kids growing up, ski trips, get-togethers), but that, of course, only works when we’re all on Apple products. (This is why Facebook bought Instagram for $1 billion. Photo Stream is a real competitive threat to Facebook, especially if you want to share pictures with a limited group of close friends.)
The i-ecosystem makes switching from the iPhone to a competitor’s device an unpleasant undertaking, something you won’t do unless you are really significantly dissatisfied with your i-device (or you are simply very bored). How much extra are you willing to pay for your Apple goodies? Brand is more than just prestige; it is the amalgamation of intangible things like perceptions and tangible things like getting incredible phone and e-mail customer service (I’ve been blown away by how great it is!) or having your problems resolved by a genius at the Apple store.
Of course, as the phone and tablet categories mature, Apple’s hardware premium will deflate and its margins will decline. The only question is, by how much?
Let me try to answer
From 2003 to 2012, Apple’s net margins rose from 1.1 percent to 25 percent. In 2003 they were too low; today they are too high. Let’s look at why the margins went up. Gross margins increased from 27.5 percent to 44 percent: Apple is making 16.5 cents more for every dollar of product sold today than it did in 2001. Looking back at Nokia Corp. in its heyday, in 2003 the Finnish cell phone maker was able to command a 41.5 percent margin, which has gradually drifted down to 28 percent.
Today, Nokia is Microsoft’s bitch, completely dependent on the success of the Windows operating system, which is far from certain. Nokia is a sorry shell of what used to be a great company, while Apple, despite its universal hatred by growth managers, is still, well, Apple. Its gross margins will decline, but they won’t approach those of 2003 or Nokia’s current level.
For Apple to conquer emerging markets and keep what it has already won there, it will need to lower prices. The company is not doing horribly in China — its sales are running at $25 billion a year and were up 67 percent in the past quarter.
However, a significant number of the iPhones sold in China (Apple doesn’t disclose the figure) are not $650 iPhone 5’s but the cheaper 4 and 4s models. (Also, on a recent conference call, Verizon Communications mentioned that half of the iPhones it has sold were the 4 and 4s models.) Apple’s price premium over its Android brethren is not as high as everyone thinks.
What is truly astonishing is that Apple’s spending on R&D and selling, general and administrative (SG&A) expenses has fallen from 7.6 percent and 19.5 percent, respectively, in 2003 to a meager 2.2 percent and 6.4 percent today. R&D and SG&A expenses actually increased almost eightfold, but they didn’t grow nearly as fast as sales. Apple spends $3.4 billion on R&D today, compared with $471 million in 2001. This is operational leverage at its best. As long as Apple can grow sales, and R&D and SG&A increase at the same rate as sales or slower, Apple should keep its 18.5 percentage points gain in net margins through operational leverage.
***

***
Growth of sales is an assumption in itself. Apple’s annual sales are approaching $180 billion, and it is only a question of when they will run into the wall of large numbers. At this point, 20 percent-a-year growth means Apple has to sell as many i-thingies as it sold last year plus an additional $36 billion worth. Of course, this argument could have been made $100 billion ago, and the company did report 18 percent revenue growth for the past quarter, but Apple is in the last few innings of this high-growth game; otherwise its sales will exceed the GDP of some large European countries.
If you treat Apple as a pure hardware company, you’ll miss a very important element of its business model: recurrence of revenues through planned obsolescence. Apple releases a new device and a new operating system version every year. Its operating system only supports the past three or four generations of devices and limits functionality on some older devices. If you own an iPhone 3G, iOS 6 will not run on it, and thus a lot of apps will not work on it, so you will most likely be buying a new iPhone soon. In addition — and not unlike in the PC world — newer software usually requires more powerful hardware; the new software just doesn’t run fast enough on old phones. My son got a hand-me-down iPhone 3G but gave it to his cousin a few days later — it could barely run the new software.
As I wrote above, Apple’s success over the past decade is a black swan, an improbable but significant event, thanks in large part to the genius of Steve Jobs. Today investors are worried because Jobs is not there to create another revolutionary product, and they are right to be concerned. Jobs was more important to Apple’s success than Warren Buffett is to Berkshire Hathaway’s today. (Berkshire doesn’t need to innovate; it is a collection of dozens of autonomous companies run by competent managers.) Apple will be dead without continued innovation.
Jobs was the ultimate benevolent dictator, and he was the definition of a micro-manager. In his book Steve Jobs, Walter Isaacson describes how Jobs picked shades of white for Apple Store bathroom tiles and worked on the design of the iPhone box. He had to sign off on every product Apple made, down to and including the iPhone charger. His employees feared, loved and worshiped him, and they followed him into the fire. Jobs could change the direction of the company on a dime — that was what it took to deliver black i-swans. Jobs is gone, so the probability of another product achieving the success of the iPhone or iPad has declined exponentially.
***
***
What is really amazing about Apple is how underwhelming its valuation is today — it doesn’t require new black swans.
In an analysis we tried very hard to kill the company. We tanked its gross margins to a Nokia-like 28 percent and still got $30 of earnings per share (the Street’s estimate for 2013 is $45), which puts its valuation, excluding $145 a share in cash, at 10 times earnings. We killed its sales growth to 2 percent a year for ten years, discounted its cash flows and still got a $500 stock.
There is a lot of value in Apple’s enormous ability to generate cash. The company is sitting on an ever-growing pile of it — $137 billion, about one third of its market cap. Over the past 12 months, despite spending $10 billion on capital expenditures, Apple still generated $46 billion of free cash flows. If it continues to generate free cash flows at a similar rate (I am assuming no growth), by the end of 2015 it will have stockpiled $300 of cash per share. At today’s price [2013] it will be commanding a price-earnings ratio (if you exclude cash) of 4.
Of course, the market is not giving Apple credit for its cash, but I think the market is wrong. Unlike Microsoft, which does something dumber than dumb with its cash every other year, Apple has a pristine capital allocation track record. It has not made any foolish acquisitions — or, indeed, any acquisitions of size. Other than buying an Eastern European country and renaming it i-Country, Apple will not be able to acquire a technologically related company of size, nor will it want or need to. The cash it accumulates will end up in shareholders’ hands, either through dividends or share buybacks.
What is Apple worth?
After the financial acrobatics I’ve done trying to murder the valuation of Apple, it is easier to say that it is worth more than $450 than to pinpoint a price target. When I use a significantly decelerating sales growth rate and normalize margins (reducing them, but not as low as Nokia’s current margins), I get a price of about $600 to $800 a share.
Growth managers don’t want Apple to pay a large dividend, as though that would somehow transform this growing teenager into a mature adult. But I have news for them: Apple already is a mature adult. Second, when your return on capital is pushing infinity (as Apple’s is), you don’t need to retain much cash to grow. Two thirds of Apple’s cash is offshore, but that doesn’t make it worthless; it just makes it worth less — only $65 billion, maybe, not $97 billion, once the company pays its tax bill to Uncle Sam.
***
***
Assessment
In the short term none of the things I am writing about here will matter. Remember, “Everyone knows Apple is going to $300,” as a client recently e-mailed me, as everyone knew it was going to a $1,000 a few months ago when Apple’s stock was trading at $700. The company’s stock will trade on emotion, fundamentals will not matter, and growth managers will likely rotate out of Apple, because once the stock declined from $700 to $450, the label on it changed from “growth” to “value.”
But ultimately, fundamentals will prevail. Like the laws of physics, they can only be suspended for so long. And so, do these retrospective thoughts on Apple hint of future prospects?
More: Should You Buy Apple Stock Ahead of Its September Event …
ABOUT
Vitaliy N. Katsenelson CFA is Chief Investment Officer at Investment Management Associates in Denver, Colo. He is the author of Active Value Investing (Wiley 2007) and The Little Book of Sideways Markets (Wiley, 2010). His books were translated into eight languages. Forbes Magazine called him “The new Benjamin Graham”.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Front Matter with Foreword by Jason Dyken MD MBA
![]()
***
Filed under: Experts Invited, Investing | Tagged: Android, Apple Inc, behavioral economics, behavioral finance, microsoft, Nexus 7, Nokia, psychology, Steve Jobs, Vitaliy Katsenelson CFA, Warren Buffett | 3 Comments »
![]()
An Encore Presentation
[By Steve Blank]
A team of 110 researchers and clinicians, in therapeutics, diagnostics, devices and digital health in 25 teams at UCSF, has just shown us the future of translational medicine. It’s Lean, it’s fast, it works and it’s unlike anything else ever done.
It’s going to get research from the lab to the bedside cheaper and faster.
Lean LaunchPad for Life Sciences and Healthcare
Welcome to the Lean LaunchPad for Life Sciences and Healthcare (part of the National Science Foundation I-Corps).
This post is part of our series on the Lean Startup in Life Science and Health Care.
***

***
The Class
Our class talked to 2,355 customers, tested 947 hypotheses and invalidated 423 of them. They had 1,145 engagements with instructors and mentors. (We kept track of all this data by instrumenting the teams with LaunchPad Central software.)
In a packed auditorium in Genentech Hall at UCSF, the teams summarized what they learned after 10 weeks of getting out of the building. This was our version of Demo Day – we call it “Lessons Learned” Day. Each team make two presentations:
Assessment
In the next few posts I’m going to share a few of the final “Lessons Learned” presentations and videos and then summarize lessons learned from the teaching team.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
“When a practicing physician thinks about their risk exposure resulting from providing patient care, medical malpractice risk immediately comes to mind. But; malpractice and liability risk is barely the tip of the iceberg, and likely not even the biggest risk in the daily practice of medicine. There are risks from having medical records to keep private, risks related to proper billing and collections, risks from patients tripping on your office steps, risks from medical board actions, risk arising from divorce, and the list goes on and on. These liabilities put a doctor’s hard earned assets and career in a very vulnerable position.
These new books from Dr. David Marcinko and Prof. Hope Hetico show doctors the multiple types of risk they face and provides examples of steps to take to minimize them. They are written clearly and to the point, and are a valuable reference for any well-managed practice. Every doctor who wants to take preventive action against the risks coming at them from all sides needs to read these books.”
Richard Berning MD FACC [New Haven, Connecticut, USA]
***
Filed under: Career Development, Experts Invited, Information Technology, Practice Management, Videos | Tagged: evidence based medicine, Future of Translational Medicine, Lean LaunchPad for Life Sciences and Healthcare, National Science Foundation I-Corps, Steve Blank, UCSF | Leave a comment »
![]()
More on Evidence-Based Translational Medicine
By Steve Blank
We have learned a remarkable process that allow us to be highly focused, and we have learned a tool of trade we can now repeat. This has been of tremendous value to us.
Andrew Norris
Principal Investigator BCN Biosciences
Over the last three years the National Science Foundation I-Corps has taught over 700 teams of scientists how to commercialize their technology and how to fail less, increasing their odds for commercial success.
To see if this same curriculum would work for therapeutics, diagnostics, medical devices and digital health, we taught 26 teams at UCSF a life science version of the NSF curriculum. 110 researchers and clinicians, and Principal Investigators got out of the lab and hospital, and talked to 2,355 customers. (Details here)
For the last 10 weeks 19 teams in therapeutics, diagnostics and medical devices from the National Institutes of Health (from four of the largest institutes; NCI, NHBLI, NINDS, and NCATS) have gone through the I-Corps at NIH.
87 researchers and clinicians spoke to 2,120 customers, tested 695 hypotheses and pivoted 215 times. Every team spoke to over 100 customers.
Three Big Questions
The NIH teams weren’t just teams with ideas, they were fully formed companies with CEO’s and Principal Investigators who already had received a $150,000 grant from the NIH. With that SBIR-Phase 1 funding the teams were trying to establish the technical merit, feasibility, and commercial potential of their technology. Many will apply for a Phase II grant of up to $1 million to continue their R&D efforts.
Going into the class we had three questions:

Evidence-based Translational Medicine
We’ve learned that information from 100 customers is just at the edge of having sufficient data to validate/invalidate a company’s business model hypotheses. As for whether you can/should push scientists past their comfort zone, the evidence is clear – there is no other program that gets teams anywhere close to talking to 100 customers. The reason? For entrepreneurs to get out of the building at this speed and scale is an unnatural act. It’s hard, there are lots of other demands on their time, etc. But we push and cajole hard, (our phrase is we’re relentlessly direct,) knowing that while they might find it uncomfortable the first three days of the class, they come out thanking us.
The experience is demanding but time and again we have seen I-Corps teams transform their business assumptions. This direct interaction with potential users and customers is essential to commercialize science (whether to license the technology or launch a startup.) This process can’t be outsourced. These teams saved years and millions of dollars for themselves, the NIH and the U.S. taxpayer. Evidence is now in-hand that with I-Corps@NIH the NIH has the most effective program for commercializing science.
Lessons Learned Day
Every week of this 10 week class, teams present a summary of what they learned from their customers interviews. For the final presentation each team created a two minute video about their 10-week journey and a 8-minute PowerPoint presentation to tell us where they started, what they learned, how they learned it, and where they’re going. This “Lessons Learned” presentation is much different than a traditional demo day. It gives us a sense of the learning, velocity and trajectory of the teams, rather than a demo day showing us how smart they are at a single point in time.
BCN Biosciences
This video from team BCN Biosciences describes what the intensity, urgency, velocity and trajectory of an I-Corps team felt like. Like a startup it’s relentless.
BCN is developing a drug that increases anti-cancer effect of radiation in lung cancer (and/or reduces normal tissue damage by at least 40%). They were certain their customers were Radiation Oncologists, that MOA data was needed, that they needed to have Phase 1 trial data to license their product, and needed >$5 million and 6 years. After 10 weeks and 100 interviews, they learned that these hypotheses were wrong.
If you can’t see the BCN Biosciences video click here
The I-Corps experience helped the BCN Bioscience team develop an entirely new set set of business model hypotheses – this time validated by customers and partners. The “money slides” for BCN Biosciences are slides 22 and 23.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
“When a practicing physician thinks about their risk exposure resulting from providing patient care, medical malpractice risk immediately comes to mind. But; malpractice and liability risk is barely the tip of the iceberg, and likely not even the biggest risk in the daily practice of medicine. There are risks from having medical records to keep private, risks related to proper billing and collections, risks from patients tripping on your office steps, risks from medical board actions, risk arising from divorce, and the list goes on and on. These liabilities put a doctor’s hard earned assets and career in a very vulnerable position.
These new books from Dr. David Marcinko and Prof. Hope Hetico show doctors the multiple types of risk they face and provides examples of steps to take to minimize them. They are written clearly and to the point, and are a valuable reference for any well-managed practice. Every doctor who wants to take preventive action against the risks coming at them from all sides needs to read these books.”
Richard Berning MD FACC [New Haven, Connecticut, USA]
Filed under: Career Development, Experts Invited, Information Technology, Practice Management, Videos | Tagged: evidence based medicine, Evidence-Based Translational Medicine, I-Corps at the NIH, Steve Blank, Translational Medicine | Leave a comment »
![]()
A ten-point plan for aspiring software entrepreneurs
By Lynne Strang – lbstrang@gmail.com
***

***
Channel Surfing
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
8
Filed under: Experts Invited, Research & Development | Tagged: medical startups, Starting a Software Business | Leave a comment »
![]()
Devastating?
 [By Austin Frakt PhD]
[By Austin Frakt PhD]
Noam Schieber’s NYT piece today is devastating.
About selecting papers to be most prominently featured at a top economics conference, David Card is quoted,
“‘I choose papers that are going to be written up’ in the mainstream press. […] ‘It’s what the people want.’”
via Non-financial conflicts of interest.
***
***
Channel Surfing
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Assessment
Has this philosophy seeped into medicine, the financial services industry and health economics; etc?
Dr. David Edward Marcinko MBA
More: Another report casts skeptical eye on patient satisfaction surveys
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
Sponsors Welcomed
And, credible sponsors and like-minded advertisers are always welcomed.
Support the “Medical Executive-Post”
***
UPDATE
Conflicts of interest, the NEJM, and where we go next
Posted: 04 Jun 2015 03:20 PM PDT
If you haven’t yet, take a look at Lisa Rosenbaum’s NEJM essays (here, here, and here) calling for new thinking about researchers and financial conflicts of interest. The essays are nuanced and go against the grain of much recent writing on research ethics.
Rosenbaum’s essays have generated many responses (the Lown Institute has collected some of them here). I examine Rosenbaum’s views in an essay in the New Republic. I’m sympathetic to many of her arguments, but I think we need more transparency in science, not less (see also here). Austin explores her views here, here, and here. Rosenbaum has elicited some exceptionally harsh rejoinders, including one from two former editors-in-chief of the NEJM.
This discussion has been intense because the stakes are very high. If manipulated research data allow bad drugs to enter the market, people can die. Conversely, if unjustified prejudice against industry slows the progress of research, that could kill people too.
Filed under: Ethics, Experts Invited, Health Economics | Tagged: Austin Frakt PhD, Noam Schieber's, Non-financial conflicts of interest | Leave a comment »
Competent, Ethical and Fair Legal Representation for Doctors
Wretched creatures are compelled by the severity of the torture to confess things they have never done and so by cruel butchery innocent lives are taken; and by new alchemy, gold and silver are coined from human blood.– Father Cornelius Loos (1592)
***

[“PHP-Approved Attorneys”]
***
Channel Surfing
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
8
Filed under: Experts Invited, Health Law & Policy, Professional Liability, Risk Management | Tagged: A New Niche area for [HealthLaw] Attorneys, Competent, Ethical and Fair Legal Representation for Doctors, Michael Lawrence Langan MD | 1 Comment »
![]()
Disruptive Technologies in Medicine
[By Dr. Bertalan Meskó]

Recently, I gave a talk to medical students about what kind of trends and technologies might shape the future and I was very curious what they think about these.
The Question
I asked them to give a score between 1 and 3 about how beneficial or advantageous those can be for society; and a score between 1 and 3 about how big threats they will pose to us.
They also gave a score between 1 and 10 about how much they look forward to using a technology in action. See the full size infographics here.
The Answer
So, I just wrote about how our Disruptive Technologies in Medicine university course prepares medical students for the coming waves of change. I also recently published an infographic related to new technologies in medicine.
***

***
Assessment
Preparing them for the future is a real challenge but I remain confident that we need to to that and it is still possible.
***
***
More:
***
FUTURISTIC MEDICAL INTERFACE
Our touch screen presentations bring the future directly to your exhibition stand, shop, museum, hospital or even your tv show or movie! No prerendered elements!
It’s realtime!
LINK: https://www.behance.net/gallery/14374555/FUTURISTIC-MEDICAL-INTERFACE
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
![]()
Filed under: Experts Invited, Information Technology | Tagged: Bertalan Meskó, Disruptive Technologies in Medicine, health information technology, How Do Medical Students View Future Technologies? | 3 Comments »
![]()
Seriously?
[By Vitaliy N. Katsenelson, CFA]
 I never thought I’d be giving writing advice. I was always the worst student in my literature class in Russia. I never received a grade higher than a C on any Russian essay I ever wrote. I have a theory that my teachers got sick of reading and grading my horrible essays, so they stopped and automatically gave me a passing grade out of pity. I don’t blame them.
I never thought I’d be giving writing advice. I was always the worst student in my literature class in Russia. I never received a grade higher than a C on any Russian essay I ever wrote. I have a theory that my teachers got sick of reading and grading my horrible essays, so they stopped and automatically gave me a passing grade out of pity. I don’t blame them.
When I came to the U.S., my grades in English class in college were not spectacular either; in fact, English was the only class I failed in college and actually had to retake my senior year.
My writing has improved slightly since then – and you, my loyal readers, get to be the judge of my scribbles. However, if the prequalification for giving writing advice was based solely on quantity – on how many words have blackened a perfectly fine white screen or besmirched innocent paper – then I am more than qualified. I have been at it for exactly a decade.
My writing “career” started in 2004 when I was hired as a writer by TheStreet.com. I was not hired because I was good – I wasn’t. But I had an investing background, and TheStreet.com was not very picky; it needed warm bodies (ideally with CFA next to their names) to comment on the markets and stocks. TheStreet.com paid almost nothing, and it was overpaying me.
I had zero experience, but I was ambitious. I took writing very seriously, and therefore my articles were serious. They were filled with big words, and, quite frankly, they were enormously boring. In addition, I was extremely self-conscious about grammar. Sentence structure and punctuation drove me nuts, and I was afraid of confusing words that were spelled similarly but had unrelated meanings (like comma and coma).
***

***
LESSONS LEARNED
This brings me to the first lesson that I want to impart about writing, and it’s one that will drive English teachers insane: Don’t worry about grammar.
Once I stopped worrying about grammar, I felt a huge weight lifted from my shoulders (as all those little punctuation marks emptied themselves from my brain). I completely gave up on a, an and the (my 12-year-old son, who was born here, does a great job fixing those for me), I stopped obsessing about commas (and comas), and I stopped trying to ferret out all the other marvelous secrets of English grammar. I let copy editors – who are very talented and oh so skilled at this – catch me out in all my little peccadilloes. Instead I channel my energy into making writing interesting and funny (if appropriate); this is Lesson No. 2.There are a lot of smart investors, and a lot of them write (just visit the web site Seeking Alpha), but only a small fraction manage to make their writing interesting (again, just visit Seeking Alpha) – and those are the ones who are read more than once.
As I mentioned, when I started writing, my articles were technical and boring. I still feel sorry for the people who read them and especially for my dear friends who felt an obligation to read them.
Then an accident happened. Six months into writing for TheStreet.com, I wrote about the digital video recorder company TiVo. In that article I dared to use a little bit of humor to describe a painful experience I had when I called TiVo’s automated telephone customer service, which did not seem to understand my “slight” Russian accent. To my embarrassment, I had to ask my three-year-old son, who by that time had already acquired a perfect “Disney” accent, to talk to the machine instead, and of course it understood him just fine.
That article was not brilliant – it contained as many or as few insights as my previous articles did – but it was not “proper,” and it was not boring. Suddenly, the feedback from readers was much different – I received a ton of e-mail. Then I understood the power of humor. But it was not just humor: I was able to deliver my otherwise boring message in an interesting way.
I realized that knowing what you want to say is not enough; you need to figure out how to say it.
To this day, I spend hours staring at the computer, trying to come up with an interesting analogy or a compelling angle on how to say something I already know. I often use analogies to tell a story, especially if the topic is complex. They help me relate complex ideas through simple examples.
Let me illustrate. I have a very smart investor friend of German ancestry. True to his roots, he is very efficient in everything he does. (I am stereotyping here, but why not?) He has written a very smart investment book. If you read the whole thing, you’d learn a lot. But that is a big if. His book is as efficient and properly structured as you would expect from a well-engineered German car or an instruction manual for that car. It doesn’t have an extra word or a superfluous sentence. But unfortunately, in the process of making it efficient, he sterilized his book. I was excited to read it but could not get past Chapter 3. I got terminally bored, and I do investments for a living.
Oh, and while we’re on the subject of boredom: Follow novelist Elmore Leonard’s advice when he said, “I try to leave out the parts that people skip.” Don’t try to be descriptive for the sake of being descriptive.
Andrew Blum in 2012 wrote a terrific book called Tubes: A Journey to the Center of the Internet . However, in his other life Andrew is a reporter who covers architecture. His job is to describe inanimate objects. In Tubes he often goes into “descriptive mode,” telling us all about things that do not need to be described. For example, at one point he falls into an exhaustive description of the hotel he stayed in near the Los Angeles International Airport. The hotel room had nothing to do with the story, but he went on and on, describing bars of soap, their colors, the plate they were on and how the sunlight bounced off each one of them.
After making it through the third chapter, I gave up and downloaded the audiobook of Tubes. So maybe Andrew succeeded after all, since I ended up buying two versions of his book. (And I do highly recommend listening to his book if you want to learn about the Internet.)
It took a while for my writing style to develop. A big part of its development came through reading great writers. The two people who had the most impact on me were John Mauldin and Cliff Asness.
John needs no introduction, as his economics newsletter (Mauldin Economics) is read by millions. He has a gift for explaining complex investment topics simply, but he also invites you into his life. He shares stories about the trips he takes and the people he meets; he talks about his kids and their travails, his lack of time for the gym and his penchant for cooking mushrooms. When you read him, you feel as if he’s writing for you – just you. This is different from fiction writing, in which the author’s fingerprints are hidden.
Cliff Asness has had a tremendous impact on me as well. Cliff is a hedge fund manager; he runs the large quant firm AQR Capital Management in Greenwich, Connecticut. Cliff has an incredible gift for being witty. Back in 2005 I read a paper by Cliff discussing the most boring topic on earth: the expensing of employee stock options. At the time, companies did not consider them an expense. Cliff argued that the companies were wrong and needed to show the options on their income statements, just like any other expense.
I had written on the same topic just a few months before, making a similar point. But after I read his paper, I sent Cliff an e-mail with the subject line “I am not worthy.” Cliff’s paper was published in the most boring finance magazine in the whole universe: Financial Analysts Journal (every article in it is full of geeky Greek symbols). To my astoundment, Cliff was able to inject humor where I thought it was not possible. I wrote a very boring, unmemorable article on stock options; Cliff wrote a great, funny article on the same topic that I still remember today.
John Mauldin showed me through his writing that it’s okay to be personal, and Cliff proved it is okay to be funny. No, Cliff proved that you must be funny when you discuss boring topics – this is how you make the reader stick with it. Lesson No. 3: Identify your favorite writers, the ones whose voices you can really relate to, and learn from them.
I could relate to John’s and Cliff’s writings because they fit my personality and my natural writing style. They liberated me from being sanitized, impersonal and boring.
A sublesson here is, Read to write. When you read, always have your writer’s hat on, and pay attention not just to content but to the quality of the writing as well. That is not something that comes automatically to most of us; we have to manually hit the “on” switch.
Lesson No. 4: Be respectful of your environment. This is not an ecological statement; I am talking about your writing environment. If you write long enough, you start to appreciate the importance of your external and internal environment. Stephen King, in his terrific book On Writing: A Memoir on the Craft , said that he listens to heavy metal band AC/DC when he writes; he feels it walls him off from the external world and helps him build his own worlds. I listen to classical music, and if I am really stuck, I start listening to opera.
And if that weren’t weird enough, I write only in italics. This little trick makes my letters look a bit friendlier to me. If you find that you like your font to be pink, go for it. We writers need any edge we can get, and you can always change back to a color and format that is acceptable to society when you are done.
The final lesson: Be prepared for pain – or maybe not. Writing is a very personal process. Some of us are great thinkers, able to puzzle through very complex ideas in our heads and lay them out logically on paper. I have tremendous respect for those lucky ones. For most of us, present company included, writing is usually a painful endeavor that involves staring at a blank screen for hours on end and writing and rewriting multiple times.
In fact, let me take it a step farther: I think through writing. A quote from George Bernard Shaw comes to mind: “Few people think more than two or three times a year; I have made an international reputation for myself by thinking once or twice a week.”
If you ask me a question about something I have not thought about before, even if you give me a minute to think about it, my answer will usually, well … suck. I have not written about that topic yet, and so I may not have thought it through, and the logical links may not have been made. That’s just how my mind operates.
Quite frankly, I am embarrassed for my brain. It’s like the dirty apartment of a confirmed bachelor, with unwashed clothes, empty pizza boxes and beer bottles all over the floor. For an idea to be developed to the point at which it can leave the room, I have to clean it up, organize it, put things in their rightful place. That is why I write – sorry, dear reader, it’s not about you; it’s about me, me and me again.
***

***
More:
ASSESSMENT
Writing is not a linear process, and when you sit down to write, your thoughts may not be quite ready to come out – it’s okay if they just haven’t come to a boil yet. Don’t blame it on writer’s block. Author Tom Clancy once said, “Writer’s block is just an official term for being lazy, and the way to get through it is work.” Just take some time off, do something fun and then get back on the writing horse.
ABOUT
Vitaliy N. Katsenelson, CFA, is Chief Investment Officer at Investment Management Associates in Denver, Colo. He is the author of The Little Book of Sideways Markets (Wiley, December 2010). To receive Vitaliy’s future articles by email or read his articles click here.
Investment Management Associates Inc. is a value investing firm based in Denver, Colorado. Its main focus is on growing and preserving wealth for private investors and institutions while adhering to a disciplined value investment process, as detailed in Vitaliy’s book Active Value Investing (Wiley, 2007).
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Filed under: Career Development, Experts Invited, iMBA, Investing, Op-Editorials | Tagged: Andrew Blum, AQR Capital Management, Elmore Leonard, TheStreet.com, Vitaliy N. Katsenelson, writing advice | 1 Comment »
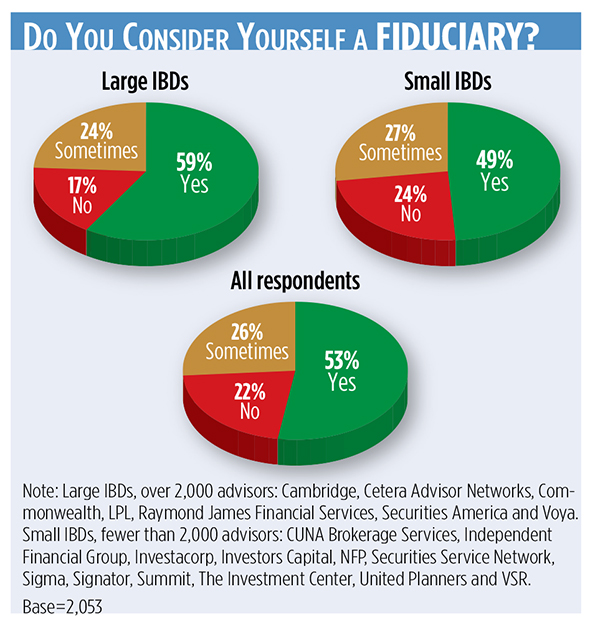
2015 IBD Report Card
By Diana Britton of WealthManagement
***
***
Link: http://wealthmanagement.com/ibd-report-card
How This Survey Was Conducted: Between Jan. 14 and Feb. 25, 2015, REP. magazine emailed invitations to participate in an online survey to print subscribers and advisors in the Meridian-IQ database at over 80 independent broker/dealers. By Feb. 25, a total of 2,069 completed responses were received. Brokers rated their current employers on several items related to their satisfaction. Ratings are based on a 1-to-10 scale, with 10 representing the highest satisfaction level.
Note: Large IBDs, over 2,000 advisors: Cambridge, Cetera Advisor Networks, Commonwealth, LPL, Raymond James Financial Services, Securities America and Voya. Small IBDs, fewer than 2,000 advisors: CUNA Brokerage Services, Independent Financial Group, Investacorp, Investors Capital, NFP, Securities Service Network, Sigma, Signator, Summit, The Investment Center, United Planners and VSR.
More:
Read even more:
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
***
***
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Filed under: Experts Invited | Tagged: "The Wall Street Casino", Diana Britton., fiduciary | Leave a comment »
![]()
Filed under: Experts Invited, iMBA, Practice Management | Tagged: experts invited, MEDICAL PRACTICE ADVERTISING, medical practice management, medical practice marketing, Practice Management | Leave a comment »
![]()

[By Edward Bukstel]
***
***

***
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
Filed under: Experts Invited, Information Technology | Tagged: Edward Bukstel, mHealth; mobile Health, Mobile-Health or Global Economy? | 4 Comments »
![]()
The Elephant in the Room
[By Michael Lawrence Langan MD]
***
***

[Courtesy SplitShire]
***
More:
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
* 8
Filed under: Ethics, Experts Invited | Tagged: Michael Lawrence Langan MD, physician suicide | 7 Comments »
![]()
***
***
***
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
More:
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
Filed under: Experts Invited, Health Economics, Practice Management, Research & Development, Risk Management | Tagged: Edward Bukstel, The Wharton School of Business, Why Healthcare is F@#Ked ! | Leave a comment »
![]()
Our Newest Text Book-in-Production
http://www.CertifiedMedicalPlanner.org
[By Ann Miller RN MHA]
![]()
***
***
***
Skills Needed
If you are a physician, nurse, accountant, attorney, medical risk manager or healthcare executive, we need you.
Form below or contact us for details to peer-review, etc. MarcinkoAdvisors@msn.com
Assessment
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
[Companion Text Book]
Filed under: CMP Program, Experts Invited, Insurance Matters, Professional Liability, Risk Management | Tagged: CMP Program, malpractice, malpractice insurance, medical liability, medical risk management, www.CertifiedfMedicalPlanner.org | 2 Comments »
![]()
Who needs it … What for?
[By Ann Miller RN MHA]

What’s the point of publishing your essays, thoughts, comments and articles on this ME-P?
Today, many physicians, FAs and health economic experts still don’t have the potential to express themselves to a large audience. By adding articles to their own blogs, with poor attendance, they deprive a wide audience of the opportunity to familiarize themselves with their works.
That’s why material from our ME-P website is available to all English-speaking inhabitants of the world. Some website owners even visit our web portal to pick up or re-post the best articles to place on their own websites.
Why publish with the ME-P?
All this is interesting, but what is the use of the website to an author? So, here is what you get by publishing with us:
• A unique method of promoting your website, self, financial advisory or medical practice; or ideas. If your essay is really interesting – many others will want to read our related books, white-papers and texts; so you will become well-known among our readers.
• The content of our website is automatically placed on other main web sources via RSS feeds. By this you can attract a wide range of readers – and with little effort. The readers will get acquainted with your thoughts, articles and the personal data you share in your included profile.
• Our website is a great launching pad for new doctors, starting academics, medical practitioners, FAs, CPAs, health economists and fledgling writers. By publishing your articles here, you will be able to raise your prestige among colleagues and ME-P readers.
• You may use any free articles from our website to fulfill your own web project (you must add a link to our original material) via RSS feeds. The probability that someone will be interested in you is increased many times.
• Everyday our website is visited by many people, and their numbers are growing constantly. By adding articles the number of your readers will grow in geometric sequence.
• Once placed on the ME-P, your essay will stay on our website [almost] forever. All published materials [probably] will not be deleted with the lapse of time. This means that many years later – your articles will be still available to everyone.
Assessment
The number of ME-P subscribers and regular visitors is growing rapidly. And, the traffic to our authors’ web sources are growing too. Join us – we welcome all authors who are willing to cooperate with our vision and mission!
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
![]()
![]()
* 8
Filed under: Experts Invited, iMBA, Inc. | Tagged: ME-P, medical executive post | 1 Comment »
![]()
By Eugene Schmuckler PhD MBA MEd CTS [Academic Provost]
About the Medical Executive-Post
We are an emerging online and onground community that connects medical professionals with financial advisors and management consultants.
We participate in a variety of insightful educational seminars, teaching conferences and national workshops. We produce journals, textbooks and handbooks, white-papers, CDs and award-winning dictionaries. And, our didactic heritage includes innovative R&D, litigation support, opinions for engaged private clients and media sourcing in the sectors we passionately serve.
Through the balanced collaboration of this rich-media sharing and ranking forum, we have become a leading network at the intersection of healthcare administration, practice management, medical economics, business strategy and financial planning for doctors and their consulting advisors. Even if not seeking our products or services, we hope this knowledge silo is useful to you.
In the Health 2.0 era of political reform, our goal is to: “bridge the gap between practice mission and financial solidarity for all medical professionals.”
More: Letterhead.iMBA_Inc.
***

***
Enter the Certified Medical Planners™
There is no certification program, course of study or professional designation for FAs who wish to enter the lucrative financial planning space serving physicians and healthcare professionals.
That’s why the R&D efforts of our governing board of physician-directors, accountants, financial advisors, academics and health economists identified the need for integrated personal financial planning and medical practice management as an effective first step in the survival and wealth building life-cycle for physicians, nurses, healthcare executives, administrators and all medical professionals.
Now – more than ever – desperate doctors of all ages are turning to knowledge able financial advisors and medical management consultants for help. Symbiotically too, generalist advisors are finding that the mutual need for extreme niche synergy is obvious.
But, there was no established curriculum or educational program; no corpus of knowledge or codifying terms-of-art; no academic gravitas or fiduciary accountability; and certainly no identifying professional designation that demonstrated integrated subject matter expertise for the increasingly unique healthcare focused financial advisory niche … Until Now!
Enter the Certified Medical Planner™ charter professional designation. And, CMPs™ are FIDUCIARIES, 24/7.
Video: http://vimeo.com/84247360
An Interview with Bennett Aikin AIF®
Physician-Investors and the “F” Word
More:
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Filed under: "Doctors Only", Career Development, CMP Program, Experts Invited, Health Economics, iMBA, Inc., Investing, Portfolio Management, Practice Management | Tagged: certified medical planner, fiduciary, Financial Planning, Institute Medical Business Advisors, medical practice management | 1 Comment »
![]()
The “Gift of Wonder” Flip Book
[Download and share your free copy]

Gosh. What a year it’s been!
2014 was a wild ride filled with the unexpected, unimaginable, and unusual. And you know what? I wouldn’t have had it any other way.
So what’s in store for 2015?
All the healthcare futurists and pundits are taking stabs at predictions with the odds of a poorly played roulette table. In reality your guess is as good as mine. So I decided to have some fun with it this year and opened up predictions to the community-at-large.
The results are finally in
So, to all those who have inspired me over the years to do the unimaginable, the impossible, and the unusual, I say thank you and offer you a small token of appreciation to stir your sense of wonder and curiosity into the New Year.
Please accept this “Gift of Wonder” – a crowdsourced flip book of the community’s wildest predictions for health in 2015.
I hope you enjoy it and I wish you all an unusual new year full of hope, wonder, and curiosity! Please pass-it-on and pay-it-forward!
With sincere admiration for all my readers and supporters who inspire me everyday.
***

Crowdsourced Health Predictions for 2015 (download and share your free copy)
***
About the Curator
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
More:
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
Filed under: Experts Invited, Research & Development | Tagged: "Gift of Wonder", Gautam Gulati MD, Health Predictions for 2015, healthcare futurists | 3 Comments »
CrowdMed Company Background
CrowdMed purports to harnesses the wisdom of crowds to collaboratively solve even the world’s most difficult medical cases quickly and accurately online.
The company offers individuals, insurance providers, and self-insured corporate customers the ability to more quickly diagnose medical conditions and reduce healthcare costs without compromising care.
***

***
The results speak for themselves?
Since launching publicly in April 2013, CrowdMed has helped solve hundreds of medical cases for patients around the world, and this number is quickly growing as word spreads of the new service. On average, these patients had been sick for 8 years, seen 8 doctors, and incurred more than $50,000 in medical expenses. Despite the difficulty of their cases, more than half of these patients tell us that the crowd successfully brought them closer to a correct diagnosis or cure.
Anyone can submit a case on the CrowdMed website for free (with a $50 refundable deposit), or along with a cash compensation offer to draw more attention to their case. They use incentives to increase participation, and the overall quality and confidence levels of suggested diagnoses. Thousands of people with diverse backgrounds in medicine, health care, education and research have already joined the crowd, and they are continually recruiting new medical and disease experts to help solve cases.
During early testing of the CrowdMed platform, the founder [Jared] submitted his own sister’s [Carly] anonymous case information to the crowd to test the system. More than 300 people participated, evaluating the same symptoms that had been provided to Carly’s original doctors. In just three days, the crowd gave Jared their answer: Fragile X-associated primary ovarian insufficiency
Founded by veteran technology entrepreneur Jared Heyman and based in San Francisco, CA, CrowdMed has received more than $2.4 million in funding from some of Silicon Valley’s top venture capital firms including NEA, Andreessen Horowitz, Greylock Partners, SV Angel, Khosla Ventures and Y Combinator. The company’s advisors have founded and run some the world’s most successful online healthcare companies including WebMD. CrowdMed graduated from Y Combinator’s Winter 2013 class, and was officially launched during the TEDMED 2013 conference in Washington DC.
You can read more about CrowdMed’s leadership team click here.
More:
Assessment
Check em’ out today: http://blog.crowdmed.com
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
![]()
![]()
Filed under: "Doctors Only", Ethics, Experts Invited, iMBA, Inc., Research & Development, Touring with Marcinko | Tagged: crowd-med, david marcinko, Wisdom of Crowds | 3 Comments »
![]()
By Michael Lawrence Langan MD
***
If you are ever asked to take a polygraph test–don’t do it. Those involved in the criminal justice system, including lawyers, are largely uneducated in the realm of scientific scrutiny and experimental methodology.
They may not separate science and pseudo-science, and erroneously believe that the polygraph is an accurate scientific instrument. Their interactions are with polygraph examiners who proselytize its use, and they have little or no interaction with scientists, psychologists, and physicians who refute its use.
Refuse to take the test and educate them. Cite the Frye Doctrine, go to the medical library, copy the scientific articles which belie its validity, and present them to whomever requested you to take the test. State that the principles and assumptions underlying polygraphy are not supported by our understanding of psychology, neurology, and physiology.
***  ***
***
Assessment
Then, put the burden of proof on their heads. Tell them to present you with scientific evidence that corroborates the validity of the test. There is simply no rational basis for a machine to detect liars.
More:
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.

About the Author
Dr. Langan graduated from Oregon Health Sciences University School Of Medicine, Portland Oregon with an MD 21 years ago. He had his residency training of Geriatric Medicine-Internal Medicine at Beth Israel Deaconess Medicine Center and Internal Medicine at St Vincent Hospital Medicine Center.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
![]()
![]()
Filed under: Ethics, Experts Invited, Risk Management | Tagged: evidence based medicine, Michael Lawrence Langan MD, On Junk-Science in the Medical Profession | 3 Comments »
![]()
What it is – How it works?
 By TIMOTHY J. McINTOSH; MBA, MPH, CFP®, CMP™ [Hon]
By TIMOTHY J. McINTOSH; MBA, MPH, CFP®, CMP™ [Hon]
Similar to private equity or venture capital, peer-to-peer lending [aka person-to-person lending, peer-to-peer investing and social lending] is the practice of lending money to unrelated individuals without the benefit a traditional financial intermediary like a bank or financial institution. P2P lending takes place online using various platforms and credit checking tools.
And, it has been in existence for about a decade.
Here are some important characteristics:

More:
Assessment
The Author
Timothy J. McIntosh is Chief Investment Officer and founder of SIPCO. As chairman of the firm’s investment committee, he oversees all aspects of major client accounts and serves as lead portfolio manager for the firm’s equity and bond portfolios. Mr. McIntosh was a Professor of Finance at Eckerd College from 1998 to 2008. He is the author of The Bear Market Survival Guide and the The Sector Strategist. He is featured in publications like the Wall Street Journal, New York Times, USA Today, Investment Advisor, Fortune, MD News, Tampa Doctor’s Life, and The St. Petersburg Times. He has been recognized as a Five Star Wealth Manager in Texas Monthly magazine; and continuously named as Medical Economics’ “Best Financial Advisors for Physicians since 2004. And, he is a contributor to SeekingAlpha.com., a premier website of investment opinion. Mr. McIntosh earned a Bachelor of Science Degree in Economics from Florida State University; Master of Business Administration (M.B.A) degree from the University of Sarasota; Master of Public Health Degree (M.P.H) from the University of South Florida and is a CERTIFIED FINANCIAL PLANNER® practitioner. His previous experience includes employment with Blue Cross/Blue Shield of Florida, Enterprise Leasing Company, and the United States Army Military Intelligence.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Filed under: CMP Program, Experts Invited, Investing, Risk Management | Tagged: certified medical planner, Lending Club, Peer-to-Peer Lending, Prosper, SIPCO, Timothy J. McIntosh | 1 Comment »
![]()
Why Physicians Need Financial Advisors Now!
[By Vicki Rackner MD]
http://www.CertifiedMedicalPlanner.org
 I recently attended a surgical meeting. Most conversations with my physician colleagues turned to the same singular topic: physicians’ new financial reality.
I recently attended a surgical meeting. Most conversations with my physician colleagues turned to the same singular topic: physicians’ new financial reality.
And the message is, “It hurts!”
Physicians’ Financial Plans
Financially savvy physicians execute thoughtful retirement plans. Yet, today about half of surveyed physicians are behind where they would like to be in retirement preparedness. Further, today only about half of physicians work with professional financial planners.
As a physician myself, I understand why smart physicians fail to take smart financial action. We physicians dedicate ourselves to the alleviation of pain and suffering of others. Retirement is a distant personal concern that does not cause immediate financial pain today. We put it off.
Lesson from My Dentist
Years ago my dentist recommended that I undergo a procedure to replace a filling. He explained that the filling material put in my mouth about 40 years ago tends to pull from the tooth over time and allow new cavities to form.
As much as I like my dentist, I actively avoid spending time in his dental chair. I put off the recommended filling replacement year after year. That is, of course, until I experienced vague throbbing from that tooth. I rearranged my schedule so I could tend to this small problem before it became a much bigger problem. Who wants a root canal!
For physicians retirement planning is like that proactive filling replacement. We understand that without action there will be problems down the road. However, the threat of a problem in the distant future does not propel many like myself to action today.
***
![]()
![]()
***
The ObamaCare [PP-ACA] Opportunity for Financial Advisors
ObamaCare is the source of acute financial pain for physicians. It’s the financial toothache. Practicing physicians are looking at:
Physicians’ Wants and Needs
As a financial advisor, you know that physicians NEED a retirement plan. Kids need to eat their broccoli, too. It’s good for them.
Physicians WANT a plan to help them achieve the personal, professional and financial goals that drew them to a career in medicine. Engaging physicians by address their ObamaCare plan is about as hard as getting kids to eat ice cream.
What This Means for You
Today physicians actively seek experts to help them create their ObamaCare plans.
Financial advisor are winning new physician clients. As Seattle Seahawks quarterback Russell Wilson asks, “Why not you?”
If you want to work with more physician clients, this is your moment! Seize it. You have a chance to join the high-performing financial advisors mining the treasures in the medical market.
Assessment
Should wish to learn more here’s a video that addresses 4 questions:
About the Author
Vicki Rackner MD is an author, speaker and consultant who offers a bridge between the world of medicine and the world of business. She helps businesses acquire physician clients.
VIDEO: https://www.youtube.com/watch?v=CeCyidc4JP8&feature=player_embedded
Enter the Certified Medical Planners™
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:

Filed under: Career Development, CMP Program, Experts Invited, Financial Planning, Retirement and Benefits | Tagged: ACA, certified medical planner, CMP™ Course, ObamaCare, Physicians' Financial Plans, PP-ACA, Vicki Rackner MD, Why Physicians Need Financial Advisors Now | 8 Comments »
![]()
More on the Fiduciary Problem
By Rick Kahler MS CFP® http://www.KahlerFinancial.com
 If you consult an attorney or a doctor, you don’t have to ask whether their advice is intended to serve your best interests.
If you consult an attorney or a doctor, you don’t have to ask whether their advice is intended to serve your best interests.
It’s understood they have a responsibility to put your welfare first.
The Financial Services Sector
There is no such understanding when it comes to financial services. Some financial advisors have a fiduciary duty requiring them to act in your best interest. Others do not. Even more confusing, the same professional can be held to a fiduciary standard at some times but not others. It’s hard for consumers to know the difference.
My Talk
Last week I promised a “five-minute” solution to clear up this confusion. Here it is: Before engaging any financial advisors, ask them to sign a written statement that they are fiduciaries, that you are a client, and that either the advisor receives no income from commissions or any commission income is trivial (with “trivial” clearly defined).
If advisors sign such statements, you can be assured they have a fiduciary duty to you as a client. If not, you then understand you are a customer and “caveat emptor” (buyer beware) applies.
The Conundrum
Now – a little background on the confusion. It exists largely because of the influence that large financial institutions (who earn revenue through the sale of financial products) have on legislators.
The IAA of 1940
For example, the Investment Advisors Act of 1940 requires that anyone giving investment advice must be acting in a fiduciary capacity. The intent was to separate the financial salespeople, who had significant conflicts of interest, from the investment advisors, who had few to none.
If you know very little about financial products, would you rather be educated as the customer of a commissioned salesperson or the client of a fee-for-service advisor? Hands down, you’d want the fee-for-service advisor.
***![]() ***
***
Financial Product Sales
Of course, the financial institutions selling products understood this. They were able to influence the drafting of the 1940 Investment Advisors Act, to exclude “any broker or dealer whose performance of such [advisory] services is solely incidental to the conduct of his business as a broker or dealer.” So if salespeople just happen to give some financial advice that is “incidental” to the sale of a product, they and their companies are not held to the fiduciary standard. Congress allows financial companies to advertise as if they are fiduciaries while their sales forces are not held to a fiduciary standard.
Certified Financial Planner® Designation Conflict
The same conflict arises in some professional designations, like the Certified Financial Planner® designation conferred by the CFP® Board. The designation initially certified the completion of training in financial planning. In 2008 the Board added a fiduciary requirement to the designation.
The Caveat
However, CFP®’s are only held to a fiduciary requirement when they are doing what the CFP® Board defines as financial planning. If a CFP® professional is giving advice to a client, the fiduciary standard applies. Yet the same professional can sell the same client an annuity with high fees and high commissions, even if the product may not be in the client’s best interest, as long as no “financial planning” is part of the transaction. The result is significant confusion for consumers.
My Suggestion
The bottom line is this: when you look for financial advice or financial products, don’t assume the advisor is looking out for you. It’s your responsibility to find out whether any financial professional owes you a fiduciary duty.
Assessment
So, I suggest you ask directly, “Am I a customer or a client?” The answer is almost always “a client,” as most financial services salespeople honestly don’t know the difference. After you explain that difference, ask them to verify their fiduciary duty in writing. That five-minute solution may have a lasting impact on your financial well-being.
Link: http://www.CertifiedMedicalPlanner.org
More:
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
TEXT BOOK
Filed under: Ethics, Experts Invited, Financial Planning | Tagged: Ben Aikin, Centre for Fiduciary Excellence, fiduciary accountability, Rick Kahler CFP® | 4 Comments »
![]()
###
 By Edwin P. Morrow III; JD LLM MBA CFP® RFC®
By Edwin P. Morrow III; JD LLM MBA CFP® RFC®
[©2007-12-14. All rights reserved. USA]
EDITOR’S NOTE:
Hi Ann,
A couple years ago you posted an earlier version of the attached Asset Protection Outline. I updated it to include quite a bit more discussion of different protection levels for various kinds of accounts, and included more discussion of states other than Ohio, including a 50 state chart with IRA/403b protections.
So please delete the old one and replace with this one which contains more topics, including some substantial discussion of issues regarding current class action litigation jeopardizing asset protection for Schwab and Merrill Lynch IRAs.
Regards
Ed
###
Asset Protection has become a ubiquitous buzz-word in the legal and financial community. It often means different things to different people. It may encompass anything from buying umbrella liability insurance to funding offshore trusts.
What is most likely to wipe out a client’s entire net worth? An investment scam, investment losses, a lawsuit, divorce or long-term health care expenses? “Asset Protection” may be construed to address all of these scenarios, but this outline will cover risk from non-spousal creditors as opposed to risk from bad investments, divorce, medical bills or excessive spending. Prudent business practice and limited liability entity use (LP, LLP, LLC, Corporation, etc) is the first line of defense against such risks. Similarly, good liability insurance and umbrella insurance coverage is paramount.
However, there is a palpable fear among many of frivolous lawsuits and rogue juries [especially among physicians and medical professionals]. Damages may exceed coverage limits. Moreover, insurance policies often have large gaps in coverage (e.g. intentional torts, “gross” negligence, asbestos or mold claims, sexual harassment).
As many doctors in Ohio know all too well, malpractice insurance companies can fail, too. Just as we advise clients regarding legal ways to legitimately avoid income and estate taxes or qualify for benefits, so we advise how to protect family assets from creditors. Ask your clients, “What level of asset protection do you want for yourself?
For the inheritance you leave to your family?” Do any clients answer “none” or “low”? Trusts that are mere beneficiary designation form or POD/TOD substitutes are going out of style in favor of “beneficiary-controlled trusts”, “inheritance trusts” and the like.
Table of Contents
While effort is made to ensure the material is accurate, this material is not intended as legal advice and no one may rely on it as such. Sections II(d), II(i), V, VI and XI were updated Feb 2012, but much of the material and citations have not been verified since 2010. Permission to reprint and share with fellow bar members is granted, but please contact author for updates if more than a year old.

T.O.C. [Page Number]
I. Importance of Asset Protection 2
II. State and Federal Protections Outside ERISA or Bankruptcy 4
a. Non-ERISA Qualified Plans: SEP, SIMPLE IRAs 5
b. Traditional and Roth IRAs, “Deemed IRAs” 7
c. Life Insurance 9
d. Long-Term Care, Accident/Disability Insurance 13
e. Non-Qualified Annuities 13
f. Education IRAs (now Coverdell ESAs) 16
g. 529 Plans 17
h. Miscellaneous State and Federal Benefits 18
i. HSAs, MSAs, FSAs, HRAs 18
III. Federal ERISA Protection Outside Bankruptcy 20
IV. Federal Bankruptcy Scheme of Creditor Protection 26
V. Non-Qualified Deferred Comp – Defying Easy Categorization 30
VI. Breaking the Plan – How Owners Can Lose Protection 32
(incl Prohibited Transactions and Schwab/Merrill Lynch IRA problems) 35
VII. Post-Mortem – Protections for a Decedent’s Estate 51
VIII. Post-Mortem – State Law Protections for Beneficiaries 52
IX. Post-Mortem – Bankruptcy Protections for Beneficiaries 54
X. Dangers and Advantages of Inheriting Through Trusts 56
XI. Piercing UTMA/UGMA and Other Third Party Created Trusts 59
XII. Exceptions for Spouses, Ex-Spouses and Dependents 61
XIII. Exceptions when the Federal Government (IRS) is Creditor 62
XIV. Fraudulent Transfer (UFTA) and Other Exceptions 68
XV. Disclaimer Issues – Why Ohio is Unique 69
XVI. Medicaid/Government Benefit Issues 71
XVII. Liability for Advisors 72
XVIII. Conflicts of Law – Multistate Issues 73
XIX. Conclusions 75
Appendices
A. Ohio exemptions – R.C. §2329.66 (excerpt), §3911.10, §3923.19 78
B. Bankruptcy exemptions – 11 U.S.C. § 522 excerpts 80
C. Florida IRA exemption – Fla Stat. § 222.21 (note-may be outdated) 85
D. Sal LaMendola’s Inherited IRA Win/Loss Case Chart 86
E. Multistate Statutory Debtor Exemption Chart 88

###
Assessment
This outline will discuss the sometimes substantial difference in legal treatment and protection for various investment vehicles and retirement accounts, with some further discussion of important issues to consider when trusts receive such assets.
Beware of general observations like: “retirement plans, insurance, IRAs and annuities are protected assets” – that may often be true, but Murphy’s law will make your client the exception to the general rules. The better part of this outline is pointing out those exceptions.
Creditor Protection for IRAs Annuities Insurance Nov 19 2010 WC CLE Feb 2012 update
***
Optimal Basis Increase Trust Aug 2014
***
ABOUT THE AUTHOR:
Mr. Edwin P. Morrow III, a friend of the Medical Executive-Post, is a Wealth Specialist and Manager, Wealth Strategies Communications Ohio State Bar Association Certified Specialist, Estate Planning, Probate and Trust Law Key Private Bank Wealth Advisory Services. 10 W. Second St., 27th Floor Dayton, OH 45402. He is an ME-P “thought leader”.
Constructive criticism or other comments welcome.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
![]()
Filed under: Estate Planning, Experts Invited, Financial Planning, Health Insurance, Insurance Matters, Portfolio Management, Risk Management | Tagged: 403(b) plans, 529 plans, Annuities and Insurance, anuities, asset protection, Creditor Protection Working White-Paper for IRAs, disability insurance, Education IRAs, Edwin P. Morrow III JD, Estate Planning, Financial Planning, HSA, insurance planning, IRAs, LTCI, MSA, Non-Qualified Retirement Plans, Qualified Retirement Plans, Risk Management, UTMA, Wealth Specialist | 5 Comments »
![]()

Ken is a hospital administrator and financial consultant for the Tseung Kwan O Hospital, in Hong Kong. He speaks English, Cantonese, Mandarin and Chinese.

Assessment

Link: http://www.CertifiedMedicalPlanner.org
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
OUR NEWEST BOOK:
Filed under: CMP Program, Experts Invited, Financial Planning | Tagged: certified medical planner, CMP Program, Ken Chi Yeung | 4 Comments »
![]()
What they Are – How they Work?
Money Scripts are unconscious beliefs about money that are typically only partially true, are developed in childhood, and drive adult financial behaviors.
Money Scripts may be the result of “financial flashpoints,” which are salient early experiences around money that have a lasting impact in adulthood. Money Scripts are often passed down through the generations; and social groups often share similar Money Scripts. The animal brain stores associations around money based on early experiences, which can result in rigid and often problematic money attitudes.
And so, we argue that Money Scripts are at the root of all illogical, ill-advised, self-destructive, or self-limiting financial behaviors.

The Research
In research at Kansas State University [KSU], researchers identified four distinct Money Script patterns, which are associated with financial health and predict financial behaviors
The 4 Money Scripts
When Money Scripts are identified, it is helpful to examine where they came from. What three lessons did you learn about money from your mother?
Examination
A simple technique involves reflecting on the following questions:
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Filed under: Ethics, Experts Invited | Tagged: “Money Scripts”, Brad Klontz PsyD CFP®, financial psychology, Ted Klontz PhD | 4 Comments »
![]()
Understanding the Nexus Between Fame and Quality
[By Rick Kahler CFP®] http://www.KahlerFinancial.com
The Case … For?
When a financial advisor, someone with a radio or television show, or an author of financial books becomes well-known, it’s easy to assume you can trust that person’s advice. This isn’t necessarily the case.
Recently I was selected by an Internet community site called moneytips.com as one of their top 50 “social influencers.” This is a list of professionals in the areas of wealth and personal finance who use social media and other Internet tools effectively.
Among the top three on this list are Dave Ramsey and Suze Orman, whose books and advice include a great deal of solid information to help people get out of debt, manage money well, and provide for the future. Many others in the top 50 are respected financial journalists and advisors.
The Case … Against?
However, the list also includes a few advocates for high-risk investment methods, proponents of dubious get-rich-quick schemes, and purveyors of poorly researched advice. Those who put together the list focused on how well people established a presence on the Internet and used technology to communicate. That’s an assessment completely unrelated to the question of whether the advice or information being communicated was worthwhile.
Financial Planning
Financial planning, just like any other field, has a solid core of practitioners who quietly and ethically serve their clients. It also has its gurus, its outstanding marketers, and its fringe practitioners with extreme ideas. The challenge for consumers is not to assume fame and quality always go together.
Linking Fame and Quality?
Here are a few suggestions for keeping a balanced perspective about famous or familiar financial faces:
1. Knowing about a professional isn’t the same as knowing a professional. Everyone you know may have heard of Noted Local Advisor. That’s not the same as being able to recommend him or her. Get recommendations first-hand, from people who actually are clients of a firm or have used someone’s plan or advice. Ask specific questions about what they’ve done and how it worked for them.
2. Yes, there are shortcuts to building wealth, but they come with very high risks. For most of us, the best ways to build wealth are gradual and even boring: saving part of every paycheck, living on less than we earn, and investing for the long term in a well-diversified portfolio of different asset classes. It’s natural to wish for an easier, faster way, but that desire can make you more vulnerable to high-risk schemes and even scams.
3. Even if a method of building wealth is perfectly legitimate and works for others, it still may not be a good fit for you. If you’re a reclusive introvert, for example, sales is probably not your best path to success.
4. Apply the same common sense and skepticism to financial products or wealth-building methods that you would use anywhere else. For example, you probably don’t assume that a car’s advertised gas mileage is what you’ll actually get under real-world conditions. In the same way, it’s a good idea to assume that your real-world results from a proposed investment or business will be lower than the advertised numbers.
5. Don’t assume every financial guru is a crook. Many reputable professionals can teach you a great deal about money. Your job is to learn the financial basics so you can evaluate them with some educated skepticism.

More:
Assessment
And always keep in mind that a product or idea is not the same thing as the selling of that product or idea. The true genius of some financial “experts,” after all, is marketing.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
![]()
Filed under: CMP Program, Ethics, Experts Invited, Financial Planning | Tagged: certified medical planner, CMP, Dave Ramsey, Enter the Financial Advisory Gurus, financial advice, financial planners, Mike Kitces, Rick Kahler CFP®, stock-brokers, Suze Orman | 1 Comment »
![]()
Who Will be Healthcare’s Amazon.com?
[By PwC Health Research Institute]
New entrants are already having an impact
Abundant opportunity in the expanding health sector is attracting new players from far afield, from Fortune 50 retailers and telecom companies to fledgling startups backed by venture capital.
These new entrants, like health, wellness and fitness, are moving fast with fresh ideas about how to satisfy consumers’ appetites for better health and more convenient, affordable, high-quality care.
***
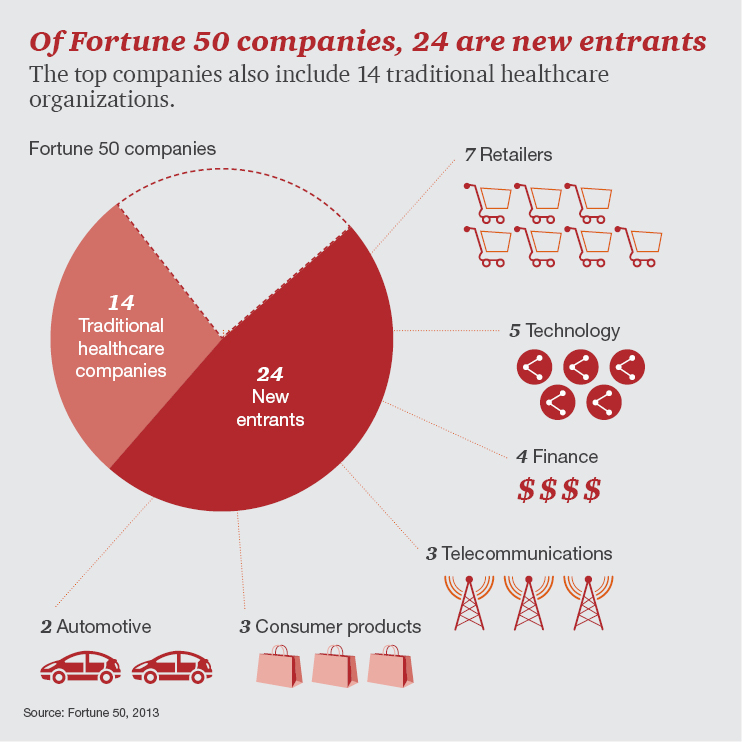
***
New Business Models
Consumers are ready to abandon traditional modes of care for new ones, suggesting billions in healthcare revenue are up for grabs now. Non-traditional players are creating these new modes of care – from home diagnostic kits that snap into smartphones to online services that can triage and prescribe treatments based on computer algorithms.
They are competing to be the Netflix, Amazon.com or Apple of the US health sector, all disruptors that transformed industries.
The Wellness and Fitness Sector
***

***
More: https://medicalexecutivepost.com/2015/06/28/why-i-love-amazon-com-but-wont-buy-its-stock/
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
Filed under: Experts Invited, Practice Management | Tagged: health sector, healthcare start-ups, PwC, US health sector, Venture Capital | 3 Comments »
![]()
[A SPECIAL R&D REPORT FOR THE ME-P]
By David K. Luke MIM, MS-PFP, CMP™ [Certified Medical Planner™]
Website: http://www.networthadvice.com
 There has been a lot of speculation since the words “Affordable Care Act” were first whispered years ago on how the various sectors in the Health Care Industry would fare under such legislation. I proposed that a good indicator would be to look at the performance of the individual health care sector stocks on the first trading day after the election.
There has been a lot of speculation since the words “Affordable Care Act” were first whispered years ago on how the various sectors in the Health Care Industry would fare under such legislation. I proposed that a good indicator would be to look at the performance of the individual health care sector stocks on the first trading day after the election.
(See With Obama Election Win, “Mr. Market” Weighs in on the ACA Equity Winners and Losers by David K. Luke on November 16, 2012).
Link: With Obama Election Win “Mr. Market” Weighs in on the ACA Equity Winners and Losers
The day after Pres. Obama’s reelection on Wednesday, November 7, 2012 the stock market was down over 2% as measured by the S&P 500 and the Dow Jones Industrial Average (DJIA). The common reason given was increased doubt that the impending “fiscal cliff” issue, which was splitting the House and the Senate, would be resolved. There was however, another big concern on investor’s mind: the future of the Affordable Care Act. While the election was close when measured by the popular vote with President Obama earning 51.06% versus Mitt Romney with 47.20%, the electoral vote showed a hands-down Obama victory with 332 versus 206 votes. Investors voted with their pocketbooks with that first trading session following the election showing certain healthcare sectors up in price, other healthcare sectors with moderate returns, and certain healthcare sectors down in price.
Disparate Health Care Sector Returns
It is interesting to look back now over a year and a half later and see how accurate those investor votes were on that first day of realization that health care reform was continuing forward at a much faster pace now that President Obama would be serving a second term. Keeping in mind that the day was a very negative day as a whole in the stock market, a number of healthcare sectors were up in price. This group includes Hospital Stocks and Medicaid HMOs. Note the phenomenal one-day returns (in a down 2% market!) on the sample stocks in these two groups:
Hospital Stocks
Medicaid HMOs
Such positive returns on a big down day in the market indicates investors assessing these healthcare sectors being good investments under an Obama presidency and a positive outlook for the implementation of the Affordable Care Act. The other up sector on that day was the Drug Wholesalers, up almost 1% on that negative day. (See “Selected Health Care Performance” Chart – below).
The market had a tepid response to the Pharmacy Benefit sector, as well as the Generic Pharmacy, Testing Labs, and Big Pharma. In my sample group, these sectors were down -.4%, -7%, -1.7%, and -1.4% respectively. It is important to note however that these sectors while slightly positive or barely negative still performed better than the general market that day.
Two Sectors
But, the two healthcare sectors that the stock market severely punished with the voting of substantially more sellers than buyers by investors on that first post-election day were the Medical Device Companies (down 2.5% in the sample group) and the Medicare Part D Companies (down 4.7% in the sample group). The thought at the time was that Medical Device Companies, facing an impending medical device excise tax of 2.3% on the sale of most medical devices in the United States, would be devastated, and that Medicare Part D Companies would face severe profit constraints with tighter-fisted government regulations imposed by the ACA.
***

***
The Retro-Specto-Scope
In hindsight, investors were correct on two out of the three predictions based on stock market prices on the various healthcare sectors. Hospital Stocks, Medicaid HMOs, and Drug Wholesalers, the leading sectors indicated to be winners with the impending implementation of the ACA, are up 69.8%, 63.6% and 76.5% respectively in the sample groups since November 7, 2012. This remarkable and closely parallel return for these three sectors seemed to prove that the stock market on November 7, 2012 correctly picked the three winning health care sectors! The S&P 500 index for the same time is up 32.02%, a nice return for 1 ½ years but about half the return of these apparently huge benefactors of the ACA. The healthcare sectors that investors felt less positive about (but more positive than the general stock market) on that first postelection day were Pharmacy Benefit Companies, Generic Pharmacy Companies, Testing Labs, and Big Pharma. These four health care sectors are up 43.8%, 40.5%, 6.4%, and 20.5% respectively. Again, in terms of ranking the sectors, these four sectors performed in line based on the comparative returns of the other healthcare sectors.
Wisdom of Crowds
Amazingly, it appears that the emotional Mr. Market predicated quite accurately on Wednesday, November 7, 2012, in one day of trading, not just which health sectors would be good investments for the near future, but the actually ranking of the future performance of the sectors! It seems as though the stock market, as one large voting machine, precisely dissected the over 20,000 pages + of resulting legislation created from the original 906 pages (pdf here) of the PPACA law and distilled it down to profits and losses with the resulting winners and losers in the health care industry in one trading session.
Two [2] Big Misses
Investors however were way off on their concerns about Medical Device Companies and Medicare Part D Companies. The two sample groups were up 71.3% and 66.4% in the time of November 7, 2012 to May 19, 2014 respectively, more than double the S&P 500 for the same period, and in line with the best performing sectors! This is spite of the fact that stock sample of these two groups were the two worst performers on post-election day trading. What happened?
***

***
The “Medical Device Excise Tax” Fable and the “Private Insurers Will Control Costs” Fairy Tale
Wall Street has sharpened their pencils in the last year and a half and realized they have gravely underestimated the profit potential of the Medical Device makers and the Managed Care Health Insurers, in spite of the ACA. Based on stock price performance of the sample group of major players in the past 18 months, fewer sectors look as profitable as the Medical Device Industry and the Medicare Part D Industry. What happened?
The Medical Device industry states that the tax will cost the US “tens of thousands of jobs” and that those jobs will be shipped overseas. A number of issues that are involved here however refute these claims (http://www.factcheck.org/2013/10/boehner-and-the-medical-device-tax/. It appears that any targeted reductions were not related to the implementation of the tax, which became effective January 1, 2013, in spite of heavy protest by the industry. Medical technology continues to have a bright future regardless of the tax.
The notion that the “Affordable” Care Act will help reign in the rampant cost increases of Medicare’s “Part D” program seem to be elusive. Private insurers have done a poor job of keeping drug prices down, especially when compared to the discounts the government gets for Medicaid. Medicare Part D companies wield significant influence on Capitol Hill, and impending steeper discounts look unlikely.
Everybody Wins, Except …
Before the ACA implementation, about 85% of Americans had health insurance. Currently with an additional 7 million Americans with health insurance thanks to Obamacare, an additional 2.2% of Americans now have coverage, or about 87% of all Americans. How can such a slight increase in new health care consumers be responsible for such large anticipated profits in the health care sector? It cannot. Wall Street is telling us that the new health law is not about new customers, but about increased profit margins for the health care industry. I can draw three conclusions:
THE CHART [Research and Development]
Selected Health Care Sector Stock Performance Random Sampling of Publically Traded Companies From President Obama Re-election Date to Present
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
![]()
![]()
![]()
![]()
Filed under: Breaking News, CMP Program, Drugs and Pharma, Experts Invited, Investing, Portfolio Management | Tagged: ACA, Affordable Care Act., CMP Program, david luke, Health Care Industry, Healthcare Sectors, hospital stocks, Investing, medicaid HMOs, Pharmacy Benefit sector, www.CertifiedfMedicalPlanner.org | 3 Comments »
![]()
And … Can it be Quantified?

[By Staff Reporters]
How much of a boost in net returns can financial advisors add to client portfolios? According to Vanguard Brokerage Services®; maybe as much as 3%?
The Study
In a recent paper from the Valley Forge, PA based mutual fund and ETF giant, Vanguard said financial advisors can generate returns through a framework focused on five wealth management principles:
• Being an effective behavioral coach: Helping clients maintain a long-term perspective and a disciplined approach is arguably one of the most important elements of financial advice. (Potential value added: up to 1.50%).
• Applying an asset location strategy: The allocation of assets between taxable and tax-advantaged accounts is one tool an advisor can employ that can add value each year. (Potential value added: from 0% to 0.75%).
• Employing cost-effective investments: This component of every advisor’s tool kit is based on simple math: Gross return less costs equals net return. (Potential value added: up to 0.45%).
• Maintaining the proper allocation through rebalancing: Over time, as investments produce various returns, a portfolio will likely drift from its target allocation. An advisor can add value by ensuring the portfolio’s risk/return characteristics stay consistent with a client’s preferences. (Potential value added: up to 0.35%).
• Implementing a spending strategy: As the retiree population grows, an advisor can help clients make important decisions about how to spend from their portfolios. (Potential value added: up to 0.70%).
Source: Financial Advisor Magazine, page 20, April 2014.
The Fine-Print
But, Vanguard notes that while it’s possible all of these principles could add up to 3% in net returns for clients, it’s more likely to be an intermittent number than an annual one because some of the best opportunities to add value happen during extreme market lows and highs when angst or giddiness [fear and greed] can cause investors to bail on their well-thought-out investment plans.
More: http://www.CertifiedMedicalPlanner.org
Assessment
Most retail financial services products are designed to enhance the well-being of the Financial Advisor and/or vendor at the expense of clients. The clients get only the leftovers. Of course, no one tells them that secret. They have to figure it out for themselves. As the old line goes, “Where are the customers’ boats?”
Source: Rowland, M: Planning Periscope [Where Advisors are the Clients]. Financial Advisors Magazine; page 36, April 2014
Conclusion
Are doctors different than the average investors noted in this essay?
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
![]()
8
***
Filed under: CMP Program, Experts Invited, Interviews, Portfolio Management | Tagged: financial advisors, How Much is a Financial Advisor Worth?, Investing, investment advisor, www.CertifiedMedicalPlanner.org | 4 Comments »
![]()
Watch These Channel Presentations
By Andrew Schwartz CPA
 Retirement Plan Basics for Practice Owners
Retirement Plan Basics for Practice Owners
Wondering which type of retirement plan makes the most sense for your practice? Here, you’ll also learn why it makes sense to set up and begin to max out your retirement plan savings as soon as possible.
Million Dollar Metrics for General Dentists
General dentists can learn which metrics to generate to gauge how their practice is doing, and compare those metrics with other practices, including a sample of practices that routinely collect one million dollars or more each year.
SIBS: Implementing a Simple Incentive Bonus System
Learn to increase revenues and profits at your practice by implementing a Simple Incentive Bonus System [SIBS]. We’ve seen a lot of clients implement a SIBS and experience immediate results within their practices.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
DICTIONARIES: http://www.springerpub.com/Search/marcinko
PHYSICIANS: www.MedicalBusinessAdvisors.com
PRACTICES: www.BusinessofMedicalPractice.com
HOSPITALS: http://www.crcpress.com/product/isbn/9781466558731
CLINICS: http://www.crcpress.com/product/isbn/9781439879900
BLOG: www.MedicalExecutivePost.com
FINANCE: Financial Planning for Physicians and Advisors
INSURANCE: Risk Management and Insurance Strategies for Physicians and Advisors
![]()
Filed under: Accounting, Experts Invited, Taxation, Videos | Tagged: Andrew D. Schwartz CPA | Leave a comment »
![]()
By Edwin P. Morrow III; JD LL.M, MBA CFP® RFC® CMP® [Hon]
Dave, Ann and ME-P Readers,
Many doctors are flummoxed with whether they need any “AB” trust in light of the new tax laws.
I’ve written quite a lot on this and have attached a short and a long version to review:
VIEW: Ohio Law
VIEW: Optimal Basis Increase Trust Sept 2013
You could delete the outdated ME-P sections on EGTTRA and replace them with some of this (although it may be too much for doctors and laypeople, so I’ve also toned-it-down similar to the shorter version above).
Assessment
Also, you should cover captive insurance companies if you have not already. Which physician/practice owners should consider it? How do you start? How do you choose a captive manager and attorney? What should you watch out for? I could do that too, I think I have some material.
More on Alternative Insurance Companies:
More on Asset Protection:
ABOUT THE AUTHOR:
Mr. Edwin P. Morrow III, a friend of the Medical Executive-Post, is a Wealth Specialist and Manager, Wealth Strategies Communications Ohio State Bar Association Certified Specialist, Estate Planning, Probate and Trust Law Key Private Bank Wealth Advisory Services. 10 W. Second St., 27th Floor Dayton, OH 45402. He is an ME-P “thought leader”.
This essay is based on presentation by the author at the Wealth Management Conference at Columbus on June 13, 2013.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
LEXICONS: http://www.springerpub.com/Search/marcinko
PHYSICIANS: www.MedicalBusinessAdvisors.com
PRACTICES: www.BusinessofMedicalPractice.com
HOSPITALS: http://www.crcpress.com/product/isbn/9781466558731
CLINICS: http://www.crcpress.com/product/isbn/9781439879900
ADVISORS: www.CertifiedMedicalPlanner.org
BLOG: www.MedicalExecutivePost.com
![]()
![]()
![]()
![]()
Filed under: Accounting, Estate Planning, Experts Invited, Risk Management, Taxation | Tagged: "AB" trust, ATRA, bypass trust, Captive Insurance Companies, Ed Morrow JD, EGTTRA, marital trust, Probate Law | 1 Comment »
![]()
Or … Just Delusional like the Rest of Us!
By Rick Kahler CFP® http://www.KahlerFinancial.com
According to Scarborough, a market research firm, only 9% of adults in the U.S. label themselves as spenders. This is the percentage that “mostly agrees” with the statement, “I am a spender rather than a saver.” On the opposite side, 29% “mostly disagree” with the statement and are considered savers. Presumably, the 62% in between consider themselves to have well-balanced financial habits that include both spending and saving.
Given these numbers, it would seem that most of the adults in this country ought to have healthy savings accounts. Unfortunately, that’s not the case.
Employee Benefit Research Institute
According to a report released in March 2013 by the Employee Benefit Research Institute, 57% of U.S. workers have less than $25,000 in total household investments and savings, not including the value of their homes. The Social Security Administration’s current figures show 34% of American workers have no savings set aside specifically for retirement.
Something doesn’t quite add up. Either a lot of Americans aren’t willing to admit that they are spenders, a lot of Americans are so poor that they can’t afford to save, or a lot of Americans are delusional.
Habits of Savors
Or maybe a lot of us just have different definitions of “saving.” Here are a few money habits that might encourage people to think of themselves as savers, but that don’t necessarily add up to being successful savers:
1. Buying things on sale. Waiting for discounts on items you need and want is a wise and standard practice for frugal shoppers. But you aren’t a saver if you buy bargains that you don’t need, might not even really want, or can’t afford. Maybe that $150 pair of shoes is half price. Yet if they will just sit in your closet, you haven’t saved $75. You’ve spent $75.
2. Having money in the bank. Yes, putting money into a savings account is the first place to start saving and a great habit to teach your kids. But once you have accumulated an emergency fund, keeping your money in the bank isn’t a good savings habit. Over time, savings accounts and CD’s don’t pay enough to keep pace with inflation. Money in the bank may be safe, but it isn’t really an investment because it isn’t growing. Mutual funds that include a well-diversified range of investments are far better places for your long-term retirement savings.
3. Not spending anything. There are times when choosing not to spend money now will only cost you more money later. Failing to maintain your car or do home repairs are two common non-spending habits that may seem like saving but actually turn into spending.
4. Saving for someone else. The time-tested advice to “pay yourself first” usually means taking money off the top for savings before you spend anything. Yet this has another application, as well. Make saving and investing for your own retirement your first priority. It needs to come ahead of saving for your kids’ college educations, weddings, or first homes. This may seem selfish or greedy, but in fact it’s the opposite. When you provide for your own financial well-being in retirement, your kids won’t end up having to help pay your bills.
###

Assessment
When we’re asked to label ourselves, it’s normal to tend to choose answers that fit the way we would like to think of ourselves. I’m sure most of us would prefer to think of ourselves as savers rather than spenders.
But, if we really want to become successful savers, we can’t settle for the money habits we wish we had. We need to look at the money habits we actually practice.
Psychologists and psychiatrists, please comment. Are doctors the same as the rest of us, or not?
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Health Dictionary Series: http://www.springerpub.com/Search/marcinko
Practice Management: http://www.springerpub.com/product/9780826105752
Physician Financial Planning: http://www.jbpub.com/catalog/0763745790
Medical Risk Management: http://www.jbpub.com/catalog/9780763733421
Hospitals: http://www.crcpress.com/product/isbn/9781439879900
Physician Advisors: www.CertifiedMedicalPlanner.org
![]()
![]()
Filed under: Experts Invited, Financial Planning | Leave a comment »
![]()
On Overhead and Practice Efficiency
By Neal Baum MD
 As I meet with doctors, other urologists and office managers throughout the country, I am frequently told, “Neil, we don’t need more patients. We need to increase our reimbursement, decrease our overhead, and improve the efficiency of care.”
As I meet with doctors, other urologists and office managers throughout the country, I am frequently told, “Neil, we don’t need more patients. We need to increase our reimbursement, decrease our overhead, and improve the efficiency of care.”
I will leave the reimbursements to the experts, but now I would like to focus on overhead and practice efficiency.
The Past
In the past we enjoyed the luxury of seeing a relatively few patients and enjoying very juicy, fat profit margins. Today, the situation is reversed. Many of us are seeing a lot more patients and we all know about those razor thin profit margins. As a result we are motivated to become more efficient.
The List
So, in this ME-P article, I will provide you with ten ideas to make your practice more efficient:

Assessment
There you have it; a few ideas that can help make you more efficient and allow you to see more patients and improve your bottom line. By the way if you have any other ideas that you have used successfully and would like to share with your colleagues, please let me hear from you.
More:
Out Recent Textbook Foreword by Dr. Baum
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
Filed under: Experts Invited, Practice Management | Tagged: Maximizing Medical Practice Income, Neal Baum MD | 3 Comments »
![]()
Greetings:
Please find attached the April 2013 edition of Plan Management Navigator. This month’s Navigator features three estimates of employment by U.S. private health plans:
***
1. The first estimate is of staffing as it exists at present, based on Sherlock Benchmarks.
Estimates
We estate that the combined effect of increased health plan enrollment and heightened efficiency to be a decline of 72,000 FTEs.

Webinar
On April 17th we held a brief conference call on this topic. You may still contact us to answer any methodological questions you may have.
Assessment
About
Sherlock Benchmarks help to identify whether your plan has high staffing ratios and which functional area’s staffing should be targeted for a closer look. We invite you to consider participation in the 2013 survey with the nearly 50 organizations that have already committed to this valuable analysis.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Health Dictionary Series: http://www.springerpub.com/Search/marcinko
Practice Management: http://www.springerpub.com/product/9780826105752
Physician Financial Planning: http://www.jbpub.com/catalog/0763745790
Medical Risk Management: http://www.jbpub.com/catalog/9780763733421
Hospitals: http://www.crcpress.com/product/isbn/9781439879900
Physician Advisors: www.CertifiedMedicalPlanner.org
Filed under: Experts Invited, Practice Management | Tagged: John Park, Plan Management Navigator, Sherlock Company, Staffing Level Effects of Health Care Reform | 2 Comments »
Our Newest ME-P “Thought-Leader”
By Ann Miller RN MHA
[Executive-Director]
Dr. Neil Baum is Associate Clinical Professor of Urology at Tulane Medical School and Louisiana State University Medical School, both in New Orleans, LA.
He is also on the medical staff at Touro Infirmary in New Orleans, and East Jefferson General Hospital in Metairie, LA.
Medical Background
Dr. Baum received his medical degree from Ohio State University Medical School in Columbus. He completed an internship at the University of California at Los Angeles, a residency in surgery at Harbor General Hospital, Torrance, California, followed by a second residency in surgery and a residency in urology, both at Baylor College of Medicine in Texas. Dr. Baum is certified by the American Board of Urology.
ME-P Relevance
Dr. Baum often shares his extensive experience from his urologic office and regularly speaks to medical practices, hospitals, and pharmaceutical and manufacturing companies on improving communications between physicians and patients, practice management, guerilla marketing, practice promotion and motivation.
He has also several books on efficient medical marketing. In fact, he is the author of Marketing Your Clinical Practice-Ethically, Effectively, and Economically, 4th Edition (Jones-Bartlett, 2010).
###
![]()
###
![]()
###
And so, we are pleased he accepted our invitation as ME-P “thought-leader.” All our readers and subscribers look forward to his essays, comments and insightful contributions.
Essential ME-P Reader Concerns
I recently caught up with Dr. Baum with these two readership questions.
Q: Why Market and Promote Your Practice in the Era of Managed Care?
A: “Often physicians will discuss the current health care situation in their community and believe that their days of practice promotion are over when they have joined all of the managed care plans in the vicinity. The reality is that noting could be farther from the truth. Now marketing and practice promotion is even more important than in the “good ol’ days” of fee-for-service”.
Q: What is the Most Common Medical Practice Disaster?
A: “Natural disasters are not the most common cause of practice failure; man-made disasters such as computer crashes, power outages, and loss of electronic data are more likely to impact a medical practice”.
Assessment
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:

[Available Now]
Filed under: Experts Invited, iMBA, Inc., Marketing & Advertising | Tagged: Neil Baum MD | Leave a comment »
[ProPublica, Feb. 28th 2013, 3:24 p.m]
There’s been a lot of talk of the looming budget cuts that, without a last-minute deal, must go into effect by 11:59 p.m. ET tomorrow night. President Obama will meet with congressional leaders on Friday to discuss how to avoid the worst consequences of the sequester.
Definition
But, what is the sequester anyway, and how big is it?
InfoGraphics
Here’s our quick graphic guide, from the budget terms you need to know, to how it could impact your home state.
###

A Graphic Guide to the Sequester
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Health Dictionary Series: http://www.springerpub.com/Search/marcinko
Practice Management: http://www.springerpub.com/product/9780826105752
Physician Financial Planning: http://www.jbpub.com/catalog/0763745790
Medical Risk Management: http://www.jbpub.com/catalog/9780763733421
Hospitals: http://www.crcpress.com/product/isbn/9781439879900
Physician Advisors: www.CertifiedMedicalPlanner.org
![]()
![]()
![]()
![]()
Filed under: Alerts Sign-Up, Breaking News, Experts Invited, Funding Basics, Glossary Terms | Tagged: Christie Thompson, ProPublica, Sequester | 2 Comments »
“Just because we have apps for smartphones doesn’t mean we have real mobility in healthcare“
By Ann Miller RN MHA
www.BusinessofMedicalPractice.com
App47 CEO and co-founder Chris Schroeder hosts a great podcast series called “What’s Happening!” in which he covers topics around enterprise-grade Mobile Application Management for securely deploying, managing, and analyzing business-critical mobile apps.
The Expert
Recently, Chris interviewed Shahid N. Shah MS, a ME-P “thought-leader” and The Healthcare IT Guy, for an episode in which they spoke at length about the management of enterprise healthcare apps, what mobility means in healthcare, and why technically-savvy clinicians are the only real salvation for the healthcare IT industry.
The Conversation
The audio version of the podcast is available on theApp47 site
More from the Expert
http://businessofmedicalpractice.com/chapter-13-2/
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
LEXICONS: http://www.springerpub.com/Search/marcinko
PHYSICIANS: www.MedicalBusinessAdvisors.com
PRACTICES: www.BusinessofMedicalPractice.com
HOSPITALS: http://www.crcpress.com/product/isbn/9781466558731
CLINICS: http://www.crcpress.com/product/isbn/9781439879900
ADVISORS: www.CertifiedMedicalPlanner.org
BLOG: www.MedicalExecutivePost.com

Filed under: Experts Invited, Information Technology, Videos | Tagged: App47, Chris Schroeder, healthcare apps, Mobile Application Management, Mobile Health | 7 Comments »
And … Will a Deal Fix It?
By Theodoric Meyer
ProPublica, Dec. 28, 2012, 12:34 p.m.
President Obama will meet with congressional leaders today [1] in another attempt to avert the fiscal cliff — the automatic tax increases and spending cuts set to take effect Jan. 1st unless Congress can strike a deal. The cuts and tax hikes, which total more than $500 billion, are so large and so sudden that many economists fear they would plunge the country back into recession.
As Washington tries to hash out a deal, we’ve taken a step back to break down the numbers behind our deficit — how it grew so big, why it is actually shrinking and whether a deal can bring it under control.
How much are we in debt?
The federal debt is just shy of $16.4 trillion [2] at the moment, which also happens to be the debt limit that Congress set in 2011. Treasury Secretary Timothy F. Geithner announced on Wednesday [3] that the nation would hit the limit on Dec. 31. The Treasury can take some “extraordinary measures” to keep paying its bills for a few weeks, but it’ll run out of cash by February or March unless Congress raises the limit again.
And that’s different from the deficit, right?
Yes. The debt is the total amount of the government’s outstanding obligations. The deficit is how much the government is in the red in a given year. In the 2012 fiscal year, which ended Sept. 30, the deficit amounted to $1.1 trillion [4].
That seems like a huge number. How did the deficit get so big?
The 2012 deficit was actually the smallest one since 2008. But it’s still a giant shortfall.
As Binyamin Appelbaum noted in The New York Times [5], the federal government has run a deficit in 45 of the last 50 years. (The exceptions were 1969 and 1998 through 2001.) The financial crisis in 2008, however, caused the deficit to skyrocket, as tax revenues fell because of the slump in incomes and production, and government spending on the stimulus and safety net measures such as unemployment insurance shot up. The deficit for the 2008 fiscal year was $455 billion. In 2009, it surged to more than $1.4 trillion.
Since then, the deficit has been falling, albeit very slowly. The government took in 6.4 percent more in taxes in 2012 than in 2011, as the economy improved a bit and several tax breaks expired. And it spent less on Medicaid, unemployment insurance and the continuing operations in Iraq and Afghanistan.
What about the total debt? How much of that is President Obama’s fault?
The debt has grown by nearly $6 trillion since Obama took office, from $10.5 trillion to $16.4 trillion.
Figuring out how much of that is due to Obama is tougher. The Washington Post’s Ezra Klein, working with the Center on Budget and Policy Priorities, calculated in January [6] that the legislation Obama had actually signed — as opposed to factors like the economy — had added about $983 billion to the debt.
Klein has also rounded up several charts [7] that break down exactly what’s caused our debt to grow so large. The biggest single factor has been the weak economy; President George W. Bush’s tax cuts and the wars in Iraq and Afghanistan also fueled the debt buildup, as did President Obama’s stimulus.
Have debt levels ever been this high before?
Yes, proportionally. Economists like talk about a country’s debt in relation to its gross domestic product (a measure of the economy’s total annual output). And instead of using a country’s total outstanding debt to calculate this debt-to-GDP ratio, economists typically use the amount of debt held by the public. (Somewhat confusingly, the federal government holds about $5 trillion in obligations to itself, most of which is money owed to the funds that support Social Security and other programs.)
Using this measurement, our debt was about 67.7 percent of GDP last year. As this chart compiled by Quartz’s Ritchie King shows [8], that’s the highest our debt-to-GDP ratio has been since the 1940s, when the need to finance World War II caused the debt to surge to 112.7 percent of GDP. But the economy grew fast enough after the war that the debt soon became a much smaller percentage of the country’s GDP.
It’s worth noting that a number of other developed countries have higher debt-to-GDP ratios [9] than the U.S. Germany’s public debt is 80.6 percent of GDP, and Canada’s is 87.4 percent. The euro zone’s most troubled countries fare even worse: Italy’s debt is 120.1 percent of GDP; Greece’s is 165.3 percent.

At least we’re not Greece. How much longer can we keep borrowing?
That’s a tough one. Some commentators — including Paul Krugman, the Nobel-winning economist and columnist for The New York Times — have argued that our current deficits are mostly a product of the sluggish economy. The deficit, Krugman wrote last week [10], “is a side-effect of an economic depression, and the first order of business should be to end that depression — which means, among other things, leaving the deficit alone for now.”
Other economists — including Carmen Reinhart and Kenneth Rogoff, who studied eight centuries’ worth of financial crises for their book “This Time Is Different” — argue that countries with debt-to-GDP ratios above a certain level tend to experience slower economic growth. Reinhart and Rogoff suggest the level is around 90 percent of GDP [11] — which the U.S. is rapidly approaching. A recent Congressional Research Service report [12] concluded that while the debt-to-GDP ratio can’t keep rising forever, “it can rise for a time.” The report continued:
It is hard to predict at what point bond holders would deem it to be unsustainable. A few other advanced economies have debt-to-GDP ratios higher than that of the United States. Some of those countries in Europe have recently seen their financing costs rise to the point that they are unable to finance their deficits solely through private markets. But Japan has the highest debt-to-GDP ratio of any advanced economy, and it has continued to be able to finance its debt at extremely low costs.
How does all this fit into the fiscal cliff? Would a deal to avert it fix our debt problem?
Actually, going over the fiscal cliff would almost singlehandedly erase the deficit. Tax rates would shoot up, and the fiscal cliff’s indiscriminate budget cuts would slash military and safety-net spending alike.
The problem is that all those tax increases and spending cuts would likely throw the economy back into a recession, causing the deficit to balloon again. “The economy will, I think, go off a cliff,” said Ben Bernanke [13], the Federal Reserve chairman.
(For more detail, see The Washington Post’s exhaustive fiscal cliff explainer [14].)
What the two sides are trying to do is identify cuts that are ultimately deep enough to bring down the deficit — and thus, eventually, the debt — without stalling the economy. But negotiations collapsed last week [15] after John Boehner, the Republican House speaker, tried and failed to pass a “Plan B” alternative to the president’s proposal in the House. Obama is set to meet with congressional leaders today to try to strike a deal to block at least some of the cliff’s impact by Monday night. But its prospects seem dim.
“I have to be very honest,” Sen. Harry Reid, the majority leader, said on Thursday. “I don’t know timewise how it can happen now.”
Assessment
Of course, some analysts have pointed out that people on both the Republican and the Democratic sides may actually want to move the cliff just slightly down the road into the next Congress, which convenes Thursday, Jan. 3. The advantages: Boehner can be safely re-elected as Speaker before he has to do serious twisting of arms of fellow GOP House members to get their votes for any compromise plan. And there will be a few more Democrats in the House and the Senate for the White House to rely on in enlisting the votes it needs to ratify any such deal. The disadvantage: Delay makes the risk of miscalculation greater for either or both sides — and for the public.
Link: http://www.propublica.org/article/how-bad-is-our-debt-problem-anyway-and-will-a-deal-fix-it
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
DICTIONARIES: http://www.springerpub.com/Search/marcinko
PHYSICIANS: www.MedicalBusinessAdvisors.com
PRACTICES: www.BusinessofMedicalPractice.com
HOSPITALS: http://www.crcpress.com/product/isbn/9781466558731
CLINICS: http://www.crcpress.com/product/isbn/9781439879900
BLOG: www.MedicalExecutivePost.com
FINANCE: Financial Planning for Physicians and Advisors
INSURANCE: Risk Management and Insurance Strategies for Physicians and Advisors
![]()
![]()
Filed under: Breaking News, Experts Invited, Funding Basics, Op-Editorials | Tagged: Ben Bernanke, Boehner, federal deficit, GDP, How Bad Is Our Debt Problem, Kenneth Rogoff, Paul Krugman, ProPublica, Theodoric Meyer, Timothy F. Geithner, US Debt Limit | 2 Comments »
Book Reviews
![]()
 By Peter Benedek PhD CFA www.RetirementAction.com
By Peter Benedek PhD CFA www.RetirementAction.com
Assessment
Link: http://retirementaction.com/category/books
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Health Dictionary Series: http://www.springerpub.com/Search/marcinko
Practice Management: http://www.springerpub.com/product/9780826105752
Physician Financial Planning: http://www.jbpub.com/catalog/0763745790
Medical Risk Management: http://www.jbpub.com/catalog/9780763733421
Hospitals: http://www.crcpress.com/product/isbn/9781439879900
Physician Advisors: www.CertifiedMedicalPlanner.org
![]()
![]()
Filed under: Book Reviews, Experts Invited, Retirement and Benefits | Tagged: Peter Benedek, www.RetirementAction.com | 1 Comment »
![]()
A Remarkable Plunge in Economic Freedom
By Rick Kahler MS CFP® ChFC CCIM www.KahlerFinancial.com
The United States has experienced a “remarkable plunge in economic freedom” over the past ten years. This is the conclusion of the 2012 Economic Freedom of the World Annual Report, by Gwartney, Lawson, and Hall.
The GLH Report
The report measures the degree to which a country supports the cornerstones of economic freedom, defined as personal choice, voluntary exchange, freedom to compete, and the security of privately owned property. It surveys forty-two variables used to construct an index that measures 144 countries in five areas of economic freedom: the size of government, property rights, sound money, freedom to trade, and regulation.
Historical Review
For 20 years, from 1980 to 2000, the U.S. usually ranked as the third freest economy in the world behind Hong Kong and Singapore. By 2005 the U.S. fell to eighth, and by 2010 it was ranked 18th. In addition to Hong Kong and Singapore, the US is now less economically free than New Zealand, Switzerland, Australia, Canada, Bahrain, Mauritius, Finland, Chile, UAE, Ireland, United Kingdom, Estonia, Taiwan, Denmark, and Qatar. Right on our heels within .08 of a point are Kuwait, Cyprus, Japan, Oman, Jordan, and Peru.
Size of Government
The size of government measures the degree to which a country relies on personal choice and free markets rather than government control of markets and politics. Countries with low levels of government spending, a smaller government sector, and lower tax rates did best in this measure. The U.S. ranks 78th in this category and has seen the size of its government and control over markets significantly expand in the past 10 years.
The security of property rights and a legal system that protects them is the foundation of economic freedom and free markets. If businesses and individuals don’t have confidence that contracts will be enforced and their investments protected, it sabotages their incentive to produce. And production is at the heart of any strong economy. The U.S. ranks 28th among nations in property rights and a strong legal system. This decline is one of the more surprising to me.

Reasons for Low US Ratings
The report suggests several reasons for the low rating. One is the U.S. expansion of eminent domain powers that now allows cities to condemn private property for resale to private developers, something that was once unthinkable. Another example is the violation of the property rights of bondholders in the government bailout of GM. Finally, the ramifications of the wars on drugs and terrorism, with laws allowing the government to invade and seize property, have contributed to the sharp decline of property rights.
Sound money is the oil that keeps an economy running. While sovereign governments cannot involuntarily go bankrupt because they can create money, they are constrained by inflation. To earn a high rating in this category a country must have a low and stable rate of inflation. This is where the US scored highest, ranking seventh.
Most Free Countries
The countries with the most freedom to trade internationally have low tariffs, easy clearance and efficient administration of customs, and few controls on the movement of capital. The US ranks 57th in free trade!
Finally, a free economy avoids regulations that restrict entry into markets and restrict exchange. It allows markets to determine prices and avoids regulations that increase costs and restrict people’s ability to get into business. Here, the U.S. ranks 31st.
Report Executive Summary
Link: http://www.cato.org/pubs/efw/efw2012/efw-2012-executive-summary.pdf
Assessment
Clearly, there can be no doubt that the U.S. is in economic decline. The economic freedoms we once took for granted are slowly slipping away. Only time will tell if we will rally and turn back toward the economic principles that once made American the envy of the world, or whether we will continue our slow fall to mediocrity.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Filed under: Breaking News, Experts Invited, Financial Planning, Funding Basics, Investing | Tagged: 2012 Economic Freedom of the World Annual Report, and Hall, Gwartney, Lawson, On the Decline of US Economic Freedom, Rick Kahler CFP® | 2 Comments »
![]()
Expert Voices Essay – NIHCM Foundation
By Ann Miller RN MHA
The PP-ACA has introduced sweeping market changes that bring new uncertainty to the task of developing premiums for products to be offered in the health insurance exchanges beginning in 2014. The added complexity greatly increases the chances that these premiums will be off the mark.
In this essay, Alice Rosenblatt explains how actuaries set premiums, shows how key provisions of the ACA will affect their pricing for the October 2013 open enrollment period and describes what’s at stake if they don’t get it right.

Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
DICTIONARIES: http://www.springerpub.com/Search/marcinko
PHYSICIANS: www.MedicalBusinessAdvisors.com
PRACTICES: www.BusinessofMedicalPractice.com
HOSPITALS: http://www.crcpress.com/product/isbn/9781466558731
CLINICS: http://www.crcpress.com/product/isbn/9781439879900
BLOG: www.MedicalExecutivePost.com
FINANCE: Financial Planning for Physicians and Advisors
INSURANCE: Risk Management and Insurance Strategies for Physicians and Advisors
Filed under: Experts Invited, Health Insurance, Information Technology | Tagged: ACA, Alice F. Rosenblatt, Health Insurance Exchanges, HIE's | 3 Comments »
![]()
By Ann Miller RN MHA
[Executive-Director]
Contributors
The Medical Executive-Post is written by contributors that represent a range of professional expertise. From PhDs, MDs, DDSs, FAs, CPAs, MBAs, CFPs and CMPs, RNs etc; becasue managing a medical practice, clinic or healthcare business, and tracking one’s personal financial career is a complex and difficult task.
So, we have asked physicians, practice managers, CXOs and financial services industry participants and leaders to provide advice, experience and insight.
Link: ME-P MAST HEAD

Want to Join Us?
Have something important to add – join us.
Link: Why Post Your e-Content or Print Publish with Us?
We welcome your comments and if you would like to become a featured author just complete the reply form below and we will contact you.
Crowd-Sourced Print Examples of Our Text Books
![]()
![]()
![]()
![]()


Filed under: Career Development, Experts Invited, MAST-HEAD, Research & Development | Tagged: Write for the Medical Executive-Post | Leave a comment »
![]()
Just Think Like an Entrepreneur
By Rick Kahler MS CFP® ChFC CCIM
This Monday [9/24] morning I got up at 6:30 am. I took a hot shower, turned on the sprinkler to water the lawn, cooked an omelet for breakfast, put the dishes in the dishwasher, read The Wall Street Journal on my iPad while I enjoyed a cup of espresso, and answered five questions from my staff and clients via email. Then I got into my car and drove five miles to arrive at work at 7:45 am.
Technology
The point here isn’t that there’s anything exciting about my morning routine. It’s to emphasize how much our current technology allows one person to do in 75 ordinary minutes. Some of what I do every day, like getting to work in ten minutes or reading an East Coast newspaper the same day it’s published, would have taken hours or days to accomplish 100 years ago.
Time
One of the greatest benefits we all receive from new inventions, discoveries, technology, and tools is time. The most valuable commodity a dollar can buy is time. Time to do what we want, when we want to do it … Time that allows us to easily provide for our day-to-day needs and frees us to develop and use our own particular skills.
Thanks
Who do we have to thank for that gift of time? The entrepreneurs [medical, healthcare and others]. Through their inventions and services, successful entrepreneurs don’t just make it possible for us to live more comfortably and have easy access to more goods and services. They create more time for all of us.
Politicians
According to many politicians, the real problem with America is its entrepreneurs. If all those business people just paid more taxes, focused less on profitability, hired more people, and spent more money, all our problems would be solved.
I would suggest the opposite is true. Entrepreneurs are actually what is right with America. Instead of demonizing them, our politicians should support them in every manner possible. Entrepreneurs are the reason for our nation’s relatively high standard of living.
Disdain of entrepreneurs shows an ignorance of how a successful economy works. Production drives an economy. Show me a nation where the government produces most of the goods and services, and I will show you a nation in poverty. Cuba comes to mind.

Government
Certainly, governments do have an important role to play. They provide services and infrastructure that support and encourage entrepreneurship. To do so, governments must take a portion of the production of their citizens by requiring them to pay taxes. Therefore, citizens must sell their labor, goods, and services to acquire the country’s currency with which to pay their tax obligations.
A government must strike a fine balance in the amount of productivity it takes from its citizens and what it leaves them. Taking too much risk killing the golden goose of productivity. If entrepreneurs decide that what is left after paying taxes is not worth their capital, time, and risk, they will expend less effort and become less productive. Some will even move to countries that encourage productivity.
Assessment
According to Adam Smith, “The real price of everything, what everything really costs to the man who wants to acquire it, is the toil and trouble of acquiring it.”
The work of entrepreneurs like Alexander Graham Bell, Thomas Edison, and Bill Gates continually reduces the toil and trouble it takes us to acquire goods and services. The enormous improvements in our standard of living over the past 100 years have come from the creativity and risk-taking of entrepreneurs. It is they who provide us with the most important form of wealth—more time to do what matters to us in our own pursuit of happiness.
Link: On Disruptive Healthcare Innovators and Financial Industry Change Agents
Conclusion
But … Who and where are the medical and healthcare entrepreneurs?
Link: About HealthSpottr.com
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Health Dictionary Series: http://www.springerpub.com/Search/marcinko
Practice Management: http://www.springerpub.com/product/9780826105752
Physician Financial Planning: http://www.jbpub.com/catalog/0763745790
Medical Risk Management: http://www.jbpub.com/catalog/9780763733421
Hospitals: http://www.crcpress.com/product/isbn/9781439879900
Physician Advisors: www.CertifiedMedicalPlanner.org
![]()
![]()
![]()
![]()
Filed under: Experts Invited, Research & Development | Tagged: biomedical innovation., healthcare entrepreneurs, medical innovation, Rick Kahler CFP® | Leave a comment »
The Importance of Rules
By Jacqueline Mitus, MD, Senior Vice President, Product Strategy; Steve Silverstein, MD, FACEP, Vice President, Chief Clinical Architect; and Matthew Zubiller, Vice President, Decision Management, McKesson Health Solutions
![]()
Clear, consistent and reproducible rules logic is at the core of translating information into actionable content. In other words, rules make content more intelligent by tying disparate pieces of information together — for example, heart failure codes and care guidelines — so that a conclusion can be drawn, a recommendation can be made or an action can occur. In so doing, the content becomes meaningful and can drive the right, timely intervention or behavior.
Value Driven
Rules do not have to be complex to drive value. A very simple rule can be very actionable: for example, an automated reminder to both member and physician about annual mammograms.
Simple or complex, transforming clinical content into reproducible, actionable rules is a highly precise endeavor. Consider how nuance and meaning can be lost in any translation and the time and effort that can be spent debating an author’s original intent. In healthcare, the stakes are significantly higher in “getting it right,” and shades of gray in meaning can affect the intended outcome.
For example, concepts such as “worsening,” “severe” and “over time” are common parameters that need specific definition to become actionable and measurable.

“Rules” for a good rule:
Assessment
To learn more, download the full white paper on Actionable Content: A Framework for Better Decision-Making.
###
Learn more about McKesson Health Solutions at:http://www.mckesson.com/en_us/McKesson.com/Our+Businesses/McKesson+Health+Solutions/McKesson+Health+Solutions.html.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Health Dictionary Series: http://www.springerpub.com/Search/marcinko
Practice Management: http://www.springerpub.com/product/9780826105752
Physician Financial Planning: http://www.jbpub.com/catalog/0763745790
Medical Risk Management: http://www.jbpub.com/catalog/9780763733421
Hospitals: http://www.crcpress.com/product/isbn/9781439879900
Physician Advisors: www.CertifiedMedicalPlanner.org
Filed under: Experts Invited, Practice Management | Tagged: Jacqueline Mitus MD, Making Medical Content Actionable, Matthew Zubiller, McKesson Health Solutions, Steve Silverstein MD | Leave a comment »
![]()
An Encore Presentation from a ME-P Thought-Leader
By Ann Miller RN MHA [Executive-Director]
 In this ME-P, Shahid N. Shah MS shares his best advice for information technology workers looking to get started in the healthcare industry.
In this ME-P, Shahid N. Shah MS shares his best advice for information technology workers looking to get started in the healthcare industry.
Mr. Shah is also known as the Healthcare IT Guy [http://www.healthcareguy.com] informing us about technology issues in the healthcare field.
Link: http://www.physbiztech.com/video/shahid-shah-how-get-started-healthcare-it
###
More Expert Advice from Leaders in Healthcare Management
And, sourced below are related interviews with these experts:

Link: Health Administration Degrees http://www.healthadministrationdegrees.com
Assessment
Shahid also authored Chapter 13 on eMRs, HIT and Clinical GroupWare [INTEROPERABLE e-MRs FOR THE SMALL-MEDIUM SIZED MEDICAL PRACTICE] in our best-selling book, the “Business of Medical Practice” http://businessofmedicalpractice.com/chapter-13-2/
So, the text and videos are worth a look www.BusinessofMedicalPractice.com Our colleague, and uber hospitalist Robert Wachter MD, is also mentioned in the book.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Health Dictionary Series: http://www.springerpub.com/Search/marcinko
Practice Management: http://www.springerpub.com/product/9780826105752
Physician Financial Planning: http://www.jbpub.com/catalog/0763745790
Medical Risk Management: http://www.jbpub.com/catalog/9780763733421
Hospitals: http://www.crcpress.com/product/isbn/9781439879900
Physician Advisors: www.CertifiedMedicalPlanner.org
Filed under: Career Development, Experts Invited, Information Technology, Videos | Tagged: EHRs, EMRs, Healthcare IT Guy, HIT, How to Get Started in Healthcare IT, IT, Shahid Shah MS | 1 Comment »


















































