

International Day of Women and Girls in Science
***

***
Share this:

Filed under: Breaking News, Career Development, iMBA, Inc., LifeStyle | Tagged: International Day of Women and Girls in Science | Leave a comment »
ME-P SYNDICATIONS:
WSJ.com,
CNN.com,
Forbes.com,
WashingtonPost.com,
BusinessWeek.com,
USNews.com, Reuters.com,
TimeWarnerCable.com,
e-How.com,
News Alloy.com,
and Congress.org

![]()
![]()



BOARD CERTIFICATION EXAM STUDY GUIDES
Lower Extremity Trauma
[Click on Image to Enlarge]
The “Medical Executive-Post” is about connecting doctors, health care executives and modern consulting advisors. It’s about free-enterprise, business, practice, policy, personal financial planning and wealth building capitalism. We have an attitude that’s independent, outspoken, intelligent and so Next-Gen; often edgy, usually controversial. And, our consultants “got fly”, just like U. Read it! Write it! Post it! “Medical Executive-Post”. Call or email us for your FREE advertising and sales consultation TODAY [678.779.8597] Email: MarcinkoAdvisors@outlook.com
![]()


 ePodiatryConsentForms.com
ePodiatryConsentForms.com
 “Providing Management, Financial and Business Solutions for Modernity”
“Providing Management, Financial and Business Solutions for Modernity”


***
***
Filed under: Breaking News, Career Development, iMBA, Inc., LifeStyle | Tagged: International Day of Women and Girls in Science | Leave a comment »
By Pro Publica
LINK:
https://www.propublica.org/article/inside-the-fall-of-the-cdc?utm_source=pocket-newtab
***

***
Filed under: Breaking News, Career Development, Quality Initiatives | Tagged: CDC, Fall of the CDC | Leave a comment »


http://www.CertifiedMedicalPlanner.org
We are able to connect and communicate in more ways than ever before, and yet we seem more disconnected, divided, and confused than ever before. Yet, if we get caught in the trap of watching the same news channels and getting our data from the same source, then it is ineventible that our views and perspectives start to be swayed in that particular direction. Almost everyone is on a social media platform of some sort if they aren’t on all of them. Once you share or like posts, the algorithms go to work to show you things they know you will like and engage in even if that puts you inside an echo chamber of ideas and thoughts that prevent us from having any meaningful dialogue around complex issues.
When it comes to investing and financial planning in 2020 there is an abundance of information and resources. There are discount brokerage firms that allow you to trade stocks for free. Firms are offering world class educational materials, webinars, seminars, etc. It seems everyone who can fog a window has articles on the internet about investment strategies and ideas – from pot stocks, to crypto-currency, to Roth conversions, etc. It can be daunting trying to figure out where to go and who you can trust.
The truth is there is no one best way to use these tools, resources, and the vast amount of technology at all of our fingertips. But there is just one rule – As the novelist E.M. Forster said, “Only connect.” I’ve been asked a million times if I have a ‘stock tip’ or ‘hot idea’ by friends, family, and clients.
My recommendation as it relates to investing and financial health is always to develop a financial plan and stay the course. Just as there is no perfect solution for connecting and communicating, there is no perfect investment for everyone.
Now, regarding communication – you can take your pick: You can communicate via blogs, tweets, chat rooms, Facebook, and other social networks.
Or, when investing you can take your pick as well: you can do it yourself and utilize stocks, bonds, funds, ETFs, options, etc. Or, you can have someone do it for you to help keep the emotions out of investing and help keep your plans on track.
CONCLUSION: And so, whether we are talking about connecting and communicating online – or whether we are talking about financial planning or investing my main point is to get started. There are tons of benefits between social connection and good health. There is a ton of correlation between financial piece of mind and good health. So, take an inventory of the tools at your disposal, and let’s discuss some plans and goals for you, and let’s get to work.
***

***
Filed under: Career Development, CMP Program | Tagged: About the Certified Medical Planner™ Program, CMP Program, cross-discipline healthcare communication teams, Joe Prokup, Relationships | Leave a comment »
ENTER A HEALTHCARE ENTREPRENEURIAL BUSINESS “DISRUPTOR” FOR 2020
Courtesy: https://lnkd.in/eBf-4vY
A New Initial Public Offering [I.P.O.]
On January 30, 2020, 1Life Healthcare, Inc. (One Medical) went public, opening at $14 per share, and closing at $22.07 per share. The innovative San Francisco-based direct primary care organization more closely resembles a technology start-up than a traditional healthcare organization.
LINK: https://lnkd.in/eZxrhtp
Their membership model service provides “seamless access” to primary medical care services at “calming offices,” 24/7 virtual care, and 21st century technology (e.g., a mobile application that allows patients to schedule appointments and message their providers).
 And so, here is a report from colleagues over at Health Capital Consultants, LLC.
And so, here is a report from colleagues over at Health Capital Consultants, LLC.
ESSAY: https://lnkd.in/gVqDVR4
Your thoughts and comments are appreciated.
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
1 – https://lnkd.in/ebWtzGg
2 – https://lnkd.in/ezkQMfR
3 – https://lnkd.in/ewJPTJs
THANK YOU
****
Filed under: Career Development, Quality Initiatives | Tagged: ENTER A HEALTHCARE ENTREPRENEURIAL BUSINESS “DISRUPTOR” FOR 2020 | Leave a comment »
THE FUTURE VALUE IS IN “WHO” WE CONNECT !

By Dr. David E. Marcinko MBA
Forget amassing “likes”, “smiles”, “winks” or cultivating your online persona. Micro-Networks are all about being your true authentic self with just a select and carefully curated few people; and that’s it! No social influencers, marketers or viral posts. Just micro-segmentation!
THINK: Family members, professional colleagues, neighbors and close friends; sport or class-mates, and co-workers or faculty members in small distinct groups. There is no “network” as you occupy the space with just these people. The total number of participants is pre-determined; 25, 50, 100, 175, 250; etc. And, when reached, the only way to add new members is for existing members to drop out.
“The Vital Few … Not the Trivial Many.”
QUERY: Would you join a micro-network? What cohort of members?
Please comment.
QUERY: Would you pay a small membership surcharge? How much?
Please comment.
ASSESSMENT: Your thoughts and comments are appreciated.

THANK YOU
***
Filed under: Career Development, Touring with Marcinko | Tagged: Micro-Networks | Leave a comment »
![]()
[By staff reporters]
Tell us about the issues affecting your medical practice, clinic, hospital, wellness center, or healthcare organization in 2020.
We are conducting a brief survey to learn more about the key issues affecting your healthcare entity, and how they impact your outlook for the coming year.
Just send in your thoughts on the survey form below.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com

![]()
***
Filed under: "Doctors Only", Career Development, Practice Management, Quality Initiatives | Tagged: Issues Affecting your Clinic, Issues Affecting your Hospital, Issues Affecting your Medical Practice | Leave a comment »
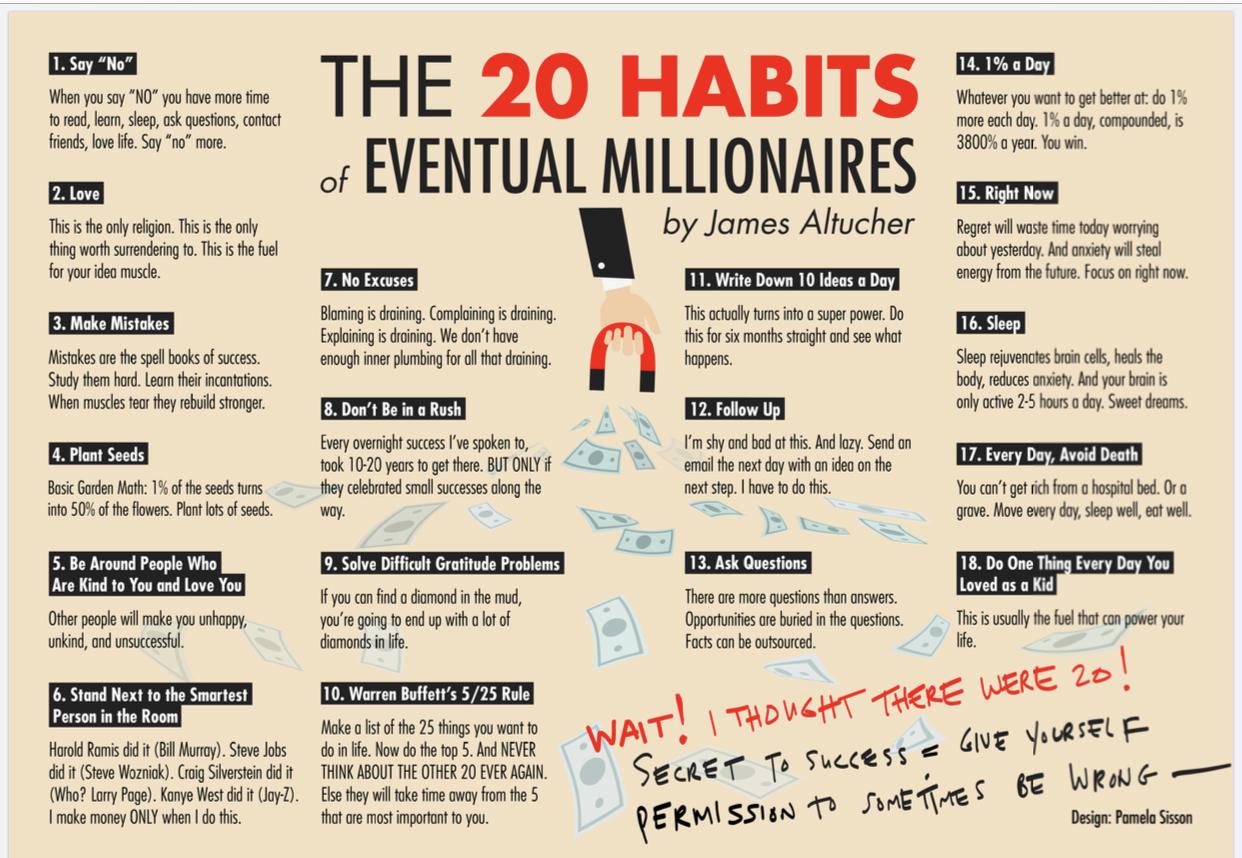
But, Maybe NOT … Doctors!
By staff reporters
***
***
 8
8
***
Filed under: Career Development, Investing | Tagged: Habits of "Eventual" Millionaires, Millionaires | Leave a comment »
What it is – How it works!
[By staff reporters]
Bonini’s paradox, named after Stanford business professor Charles Bonini, explains the difficulty in constructing models or simulations that fully capture the workings of complex systems (such as the human brain
***
***
MORE: https://en.wikipedia.org/wiki/Bonini%27s_paradox
Your thoughts are appreciated.
BUSINESS, FINANCE, INVESTING AND INSURANCE TEXTS FOR DOCTORS:
***
![]()
![]()

THANK YOU
Filed under: Career Development, Glossary Terms | Tagged: Bonini's paradox | Leave a comment »
DECISION-MAKING AND THE “ANALYSIS OF PARALYSIS”
Courtesy: www.CertifiedMedicalPlanner.org
Analysis paralysis or paralysis by analysis is an anti-pattern, the state of over-analyzing (or over-thinking) a situation so that a decision or action is never taken, in effect paralyzing the outcome. A decision can be treated as over-complicated, with too many detailed options, so that a choice is not made.
ESSAY: https://medicalexecutivepost.com/2019/09/18/the-buridans-ass-paradox/
VIDEO: https://www.youtube.com/watch?v=9PhnHQQYprA
Your thoughts and comments are appreciated.
BUSINESS, FINANCE AND INSURANCE TEXTS FOR DOCTORS:
THANK YOU
***
Filed under: Career Development, Ethics | Tagged: Analysis of Paralysis, decision-making | Leave a comment »
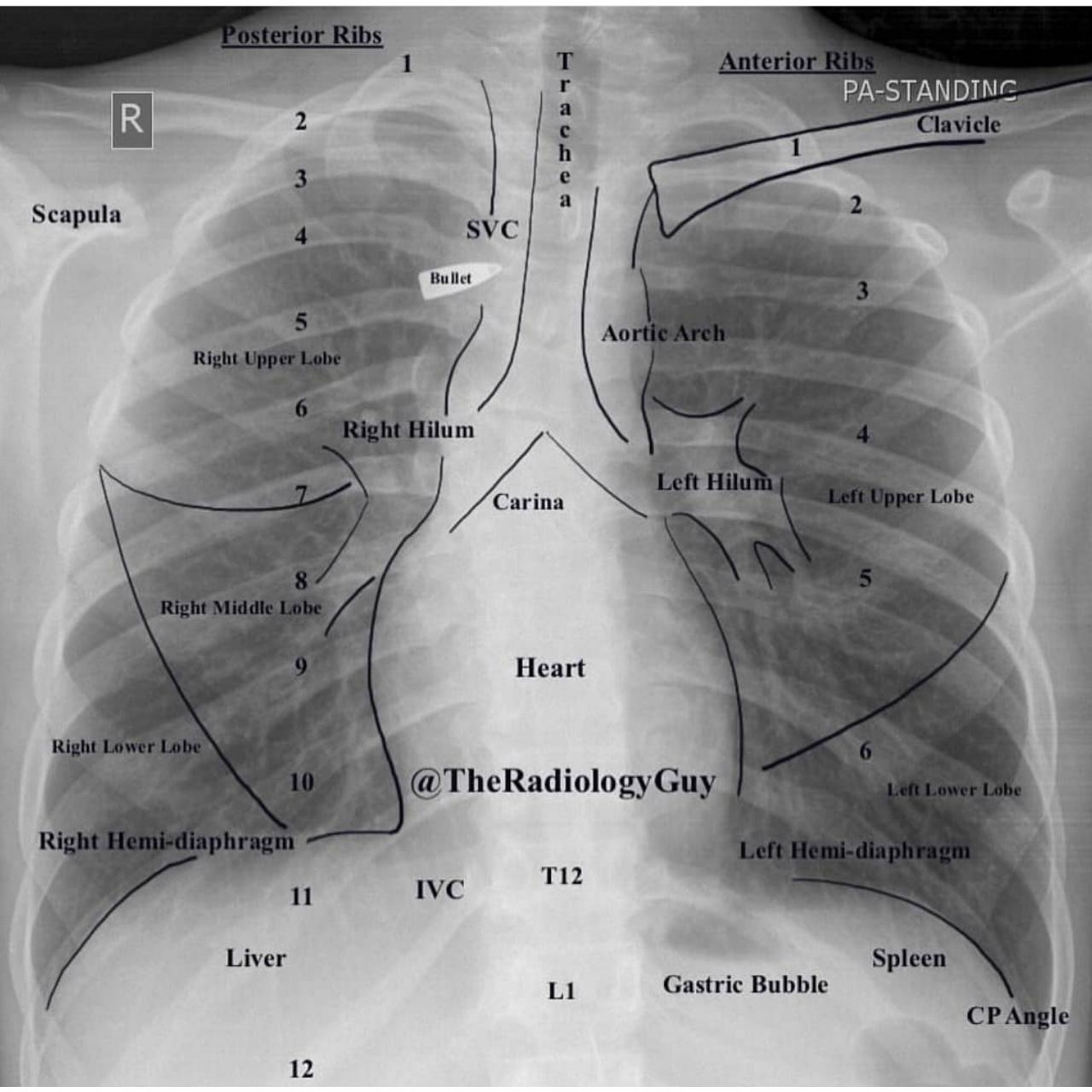
Please – Do Not Do This!
By Francisco Gutiérrez, MD., Lucio Leon, M.D. at: nejm.org
***
Submitted for your consideration. Just In case you ever wondered what injecting 10 ml of elemental mercury would do to you?
Case report: A 21 yo woman attempted suicide by injecting 10 ml (135 g) of elemental mercury (quicksilver) intravenously.
Normal AP Chest X-Ray
***
***
Case: She presented to the emergency room with tachypnea, a dry cough, and bloody sputum. While breathing room air, she had a partial pressure of oxygen of 86 mm Hg.
***
Assessment
The patient was discharged after one week, with improvement in her pulmonary symptoms. Oral chelation therapy with dimercaprol was given for nine months. At follow-up at 10 months she was healthy, with no serious consequences. The abnormalities on the chest radiograph were still apparent.
Your thoughts are appreciated.
***
![]()
![]()
***
Filed under: Career Development, Experts Invited, Risk Management | Tagged: mercury poisoning | Leave a comment »
***
Filed under: Career Development, iMBA, Inc. | Tagged: nurses week, RN | 1 Comment »
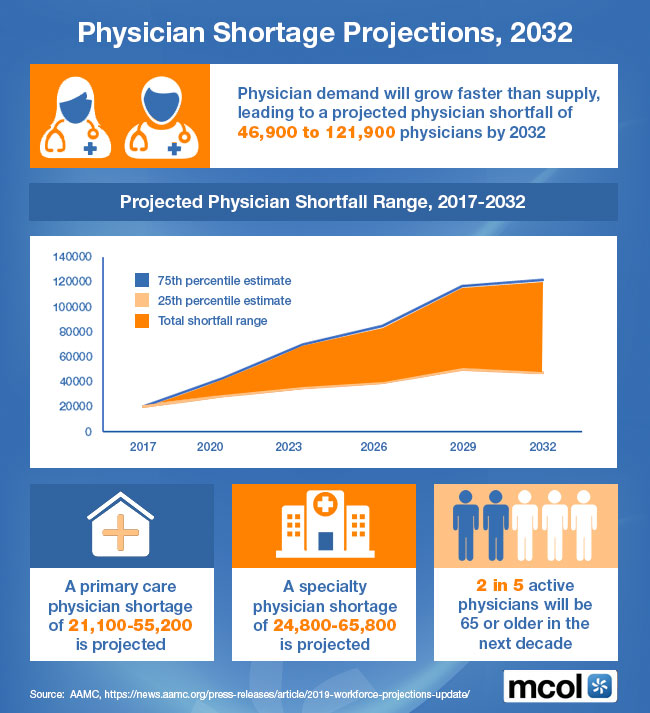
FY 2032
***
***
 8
8
***
***
Filed under: Career Development | Tagged: Physician Shortage Projections | Leave a comment »
VISITING WORLD FAMOUS TUSKEGEE UNIVERSITY

Dr. David E. Marcinko MBA
Just a quick announcement that I will be at Tuskegee University on Friday April 12th to keynote a niche seminar on biological sciences, medical education and contemporary healthcare career trends.
Link: https://www.tuskegee.edu/programs-courses/colleges-schools/cas/office-of-the-dean-cas
The gracious invitation was extended by College of Arts & Sciences Dean Channa Prakash PhD and Assistant Dean Dr. Joe Jimmeh; with renowned faculty and basic science researchers Dr. Marcia Martinez, Dr. Richard Whittington, Dr. Albert Russell, Dr. Clayton Yates; and Professor of Mathematics Dr. Mohammad Qazi to attend.
Link: https://www.tuskegee.edu/programs-courses/colleges-schools/cas/cas-faculty-and-staff
I am especially eager to tour the historic TU campus, and meet two-time graduate Dr. Roberta Troy who is Founding Director of the Health Disparities Institute for Research and Education (HDIRE). As a native of Baltimore, Maryland, this is an important issue to me. And, Dr. Troy was just appointed new University Provost. I understand she is a true academic dynamo and congratulate her, collegially.
Of course, I will be sure to order a slice of Dorothy Restaurant’s specialty key-lime pie at the Kellogg Conference Center during the post-reception dinner. Yummy!
HOPE TO SEE YOU, THERE!

***
***
Filed under: Career Development, Touring with Marcinko | Tagged: david marcinko speaking, tuskegee university | 3 Comments »
OR – Why W.A.I.T.?
By Dr. David E. Marcinko MBA
***

***
Assessment
Seek to learn!
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Book Marcinko: https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
HOSPITALS:
“Financial Management Strategies for Hospitals” https://tinyurl.com/yagu567d
“Operational Strategies for Clinics and Hospitals” https://tinyurl.com/y9avbrq5
![]()
Filed under: Career Development | Tagged: Why Am I Talking? | Leave a comment »
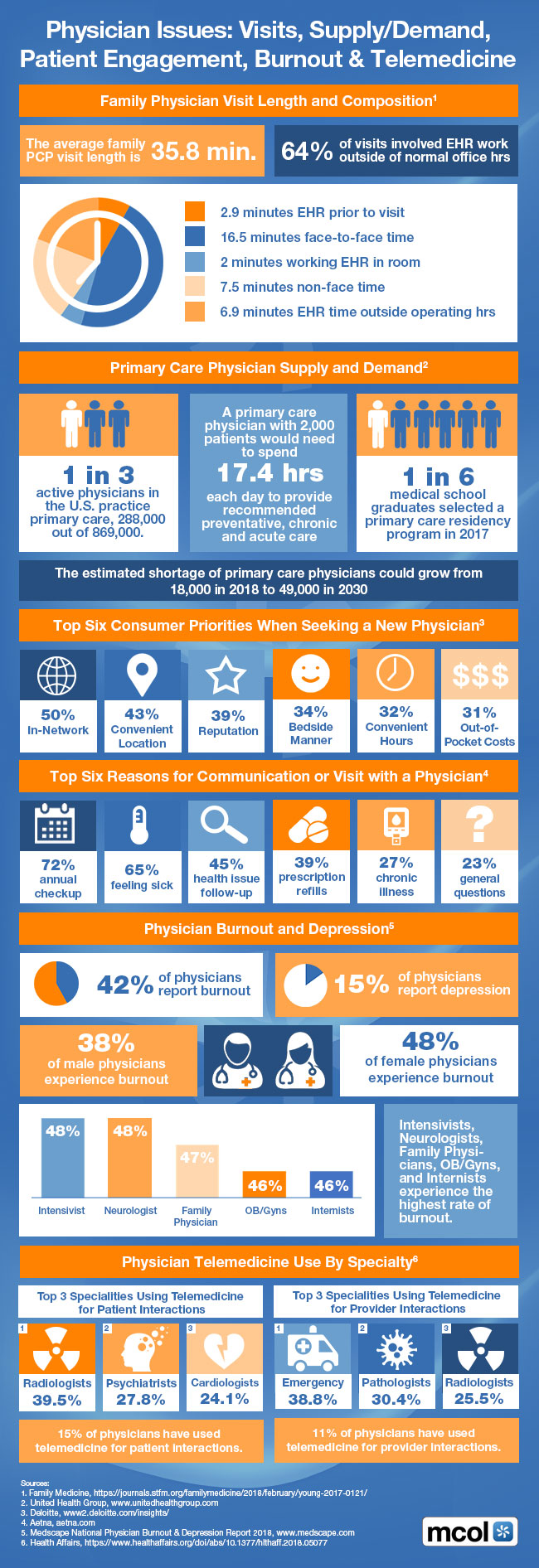
A Growing Concern
[By MCOL.com]
***
***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Book Marcinko: https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
HOSPITALS:
“Financial Management Strategies for Hospitals” https://tinyurl.com/yagu567d
“Operational Strategies for Clinics and Hospitals” https://tinyurl.com/y9avbrq5
***
Filed under: Career Development, Practice Management | Tagged: Patient engagement, Physician burnout, Physician issues, tele-medicine | Leave a comment »
That a NON-CFP® Certificant … CAN-NOT?
[By Dr. David Edward Marcinko MBA CMP®]
http://www.CertifiedMedicalPlanner.org
OK – I was a Certified Financial Planner® before my academic team launched the Certified Medical Planner™ online and on-ground chartered education and board certification designation program a few years ago. I am now reformed and in remission.
Enter the Certified Medical Planner™ Chartered Designation
Today, we are gratified that Certified Medical Planner™ mark notoriety is growing organically in the healthcare, as well as financial services, industry.
In fact, even uber-blogger Mike Kitces MSFS, MTAX, CFP, CLU, ChFC, RHU, REBC, CASL has taken note of us in his musings on the Nerd’s Eye View website.
And, the reality is that there are a growing number of CFP educational programs at the post-CFP niche market level. But, none for healthcare industrial complex: for doctors … by doctors!

QUERY
Nevertheless, I was a bit flummoxed when a physician college recently asked me this simple question:
Q: What can a CFP® mark holder do for me that a non-CFP® certificant can not?
Assessment
Now, much like a good interrogating attorney, I think I already know the answer to this question. Nevertheless, it is important to determine and understand what our ME-P readers believe; and why they believe it!
So, please opine and tell us what you think.

Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Book Marcinko: https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
DOCTORS:
“Insurance & Risk Management Strategies for Doctors” https://tinyurl.com/ydx9kd93
“Fiduciary Financial Planning for Physicians” https://tinyurl.com/y7f5pnox
“Business of Medical Practice 2.0” https://tinyurl.com/yb3x6wr8
8

HOSPITALS:
“Financial Management Strategies for Hospitals” https://tinyurl.com/yagu567d
“Operational Strategies for Clinics and Hospitals” https://tinyurl.com/y9avbrq5
![]()
ADULT LEARNERS AND STUDENTS:
![]()
![]()
***
Filed under: Career Development, CMP Program, Financial Planning, Glossary Terms, Health Economics, Health Insurance, Healthcare Finance | Tagged: certified financial planner, certified medical planner | 1 Comment »
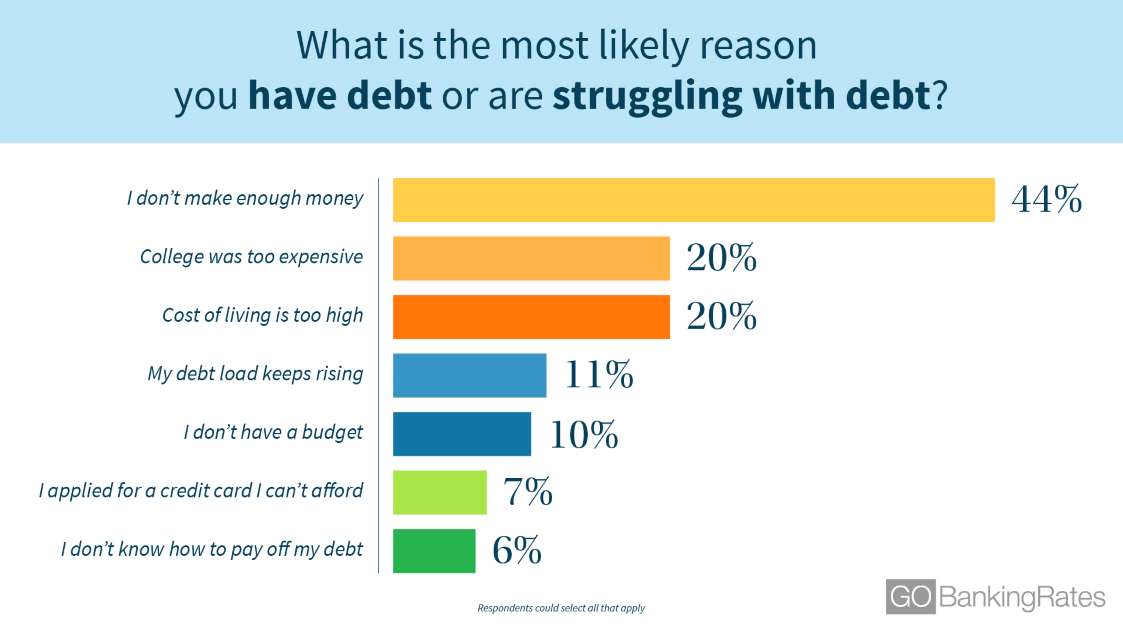
Causes and Reasons
[By staff reporters]
A valid post Black Friday and Cyber Monday Concern!
***
***
Assessment
Your thoughts are appreciated. How and Why do you struggle with debt?
MORE BUSINESS AND INVESTING FOR DOCTORS:
“Insurance & Risk Management Strategies for Doctors” https://tinyurl.com/ydx9kd93
“Fiduciary Financial Planning for Physicians” https://tinyurl.com/y7f5pnox
“Business of Medical Practice 2.0” https://tinyurl.com/yb3x6wr8
THANK YOU
8
Filed under: Career Development | Tagged: Debt Struggles?, What are Your Debt Struggles? | 1 Comment »
By MedScape
Geisinger Health System offers free genetic screenings and money-back guarantees to all of its patients, not to mention free rides and healthy food for those who need them.
CEO David Feinberg tells Eric Topol MD how it all works.
***
***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Book Marcinko: https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
DOCTORS:
“Insurance & Risk Management Strategies for Doctors” https://tinyurl.com/ydx9kd93
“Fiduciary Financial Planning for Physicians” https://tinyurl.com/y7f5pnox
“Business of Medical Practice 2.0” https://tinyurl.com/yb3x6wr8
HOSPITALS:
“Financial Management Strategies for Hospitals” https://tinyurl.com/yagu567d
“Operational Strategies for Clinics and Hospitals” https://tinyurl.com/y9avbrq5
***
![]()
Filed under: "Doctors Only", Career Development | Tagged: David Feinberg, Eric Topol MD, Geisinger | Leave a comment »
Researchers should embrace negative results instead of accentuating the positive, which is one of several biases that can lead to bad science.
MORE: https://bohatala.com/parts-of-a-research-paper/
Assessment
Your thoughts are appreciated.
***

***
MORE FOR DOCTORS:
“Insurance & Risk Management Strategies for MDs” https://tinyurl.com/ydx9kd93
“Fiduciary Financial Planning for Physicians” https://tinyurl.com/y7f5pnox
“Business of Medical Practice 2.0” https://tinyurl.com/yb3x6wr8
THANK YOU
![]()
***
Filed under: Career Development, Ethics | Leave a comment »
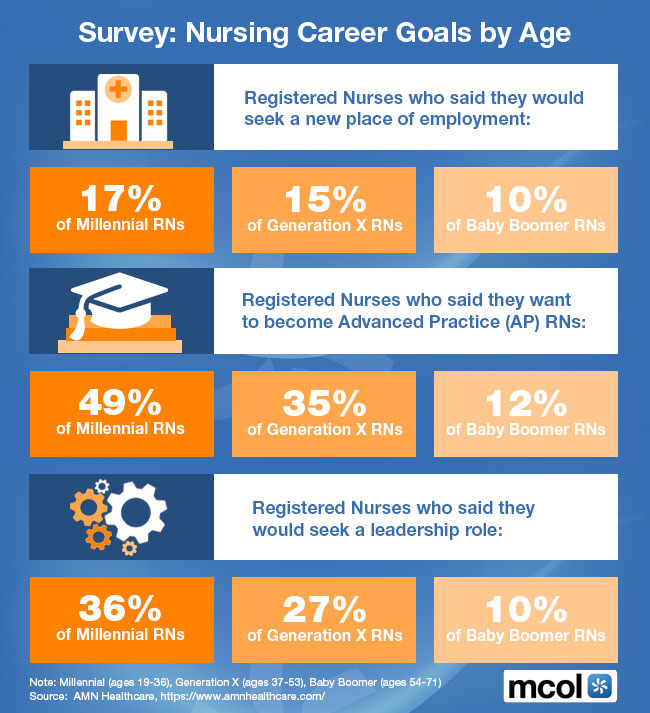
A Survey
***
***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Book Marcinko: https://medicalexecutivepost.com/dr-david-marcinkos-bookings/
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
MORE FOR DOCTORS AND NURES:
“Insurance & Risk Management Strategies for Doctors” https://tinyurl.com/ydx9kd93
“Financial Management Strategies for Hospitals” https://tinyurl.com/yagu567d
“Operational Strategies for Clinics and Hospitals” https://tinyurl.com/y9avbrq5
***
![]()
Filed under: Career Development, iMBA, Inc. | Tagged: Nursing Career Goals by Age, www.MCOL.com | Leave a comment »
***

Chief Executive / Education Officer * Speaker * Author * Researcher and Professor of Health Economics, Finance & Policy Management
![]()
8
![]()
![]()
***
Filed under: Career Development, CMP Program, Experts Invited, Touring with Marcinko | Tagged: CMP™ Course, David Marcinko; Dr. Marcinko | Leave a comment »
![]()
About Our Professional User-Generated Ratings Interface
From the Contributing Editors
How We Work
The Medical Executive-Post is a professional ranking and educational rating system for the integrated industries, readers and contributors we serve.
We function as an open social utility that allows readers and users to submit and collectively evaluate the quality of blog posts, opinions and essays on any of more than 50 specific topics and related subject matters of collective interest.

Assessment
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Our Other Print Books and Related Information Sources:
Health Dictionary Series: http://www.springerpub.com/Search/marcinko
Practice Management: http://www.springerpub.com/product/9780826105752
Physician Financial Planning: http://www.jbpub.com/catalog/0763745790
Medical Risk Management: http://www.jbpub.com/catalog/9780763733421
Hospitals: http://www.crcpress.com/product/isbn/9781439879900
Physician Advisors: www.CertifiedMedicalPlanner.org
![]()
![]()
![]()
![]()
Filed under: Career Development, Experts Invited, iMBA, Inc., Marketing & Advertising | Tagged: ME-P, ranking services, rating services, www.MedicalExecutivePost.com | Leave a comment »
Financial Experts Share Tips on Obtaining Loans to Start or Expand a Medical Practice
By Michael Gibbons
Editor: ADVANCE Newsmagazines
Maybe you’re a young dermatologist or plastic surgeon who dreams of starting your own practice. Or maybe you’re an established professional but want to expand your palette of anti-aging services. Either way, you’ve probably made an unpleasant discovery: Banks are leery about lending today. Global recessions with seemingly no end in sight tend to give loan officers sticky fingers.
Dermatologists and Plastic Surgeons
We have it on good authority that dermatologists and plastic surgeons as a group are less affected by this problem than physicians in some other branches of medicine. Still, there’s no better time than now to absorb some sound advice on how to approach banks for loans—whether you’re a fresh-faced newcomer to the fresh-face business or a wrinkled veteran at eliminating wrinkles.
Start Small
There’s no soft-soaping it: Starting a healthy aging practice is much harder than expanding an existing practice, even in the flushest of times.
“For young dermatologists starting out, I recommend you start small,” advises Jerome Potozkin, MD, who offers facial rejuvenation, liposuction, body contouring and dermatological care through his practice in Walnut Creek, CA. “You can always expand. Keep your overhead low. Know what your credit score is and do everything you can to improve it. Pay your bills on time.”
Lasers aren’t cheap. Besides the initial acquisition costs, a service contract can cost $7,000 to $12,000 a year, according to Dr. Potozkin. “Don’t feel you have to buy every new laser under the sun,” he says. “In fact, renting rather than purchasing is an option many companies offer. When your volume is low you can rent and schedule laser days—although the pitfall there is you don’t have lasers available whenever patients come in.”
Also, young dermatologists “will probably have an easier time getting a loan if they go to a relatively underserved area, as opposed to an area that has a large number of dermatologists per capita,” says Dr. Potozkin, who began practicing 10 years ago. “There are two schools of thought on this: Go where you want to live to start a practice or go to where there’s a need and be instantly successful. I chose the former. It took me longer to get started but I’m very happy where I am.”
Patience, Prudence and Passion
Be patient, prudent, passionate—and start with a spare office and as little debt as possible, advises Dr. David E. Marcinko MBA, a financial advisor and Certified Medical Planner™. Marcinko, a health economist, is CEO of the Institute of Medical Business Advisors Inc., a national physician and medical practice consulting firm based in Norcross, GA www.MedicalBusinessAdvisors.com
“Patients are looking for passion from you, not lavish trappings,” Dr. Marcinko says. “When a banker or a loan officer sees $175,000 or more of debt they are loath to give a loan—and it’s hard to blame them. Purchase a home after you become a private practitioner. You need to be as close to debt-free as you can be.
Exit Strategy
“Another thing bankers want to know is, ‘If we give you a loan and you start a practice and it fails, how will we be paid back?’ They want an exit strategy.”
The good news is dermatology “remains a very lucrative specialty, and in most parts of the country they are in a shortage position, particularly with the aging population,” says Sandra McGraw, JD, MBA, principal and CEO of the Health Care Group, a financial and legal consulting firm based in Plymouth Meeting, PA., that advises the American Academy of Dermatology, among other groups.
“I would start with a realistic business plan for why you think this practice can succeed, in the specific location,” McGraw says. “How many patients do you expect to see? How will they know you are there and available? Remember that banks lend to all kinds of people, so keep your numbers realistic. Overestimating expenses is as bad as underestimating them. Then determine how you want the money—usually a fixed loan for a period of time and then a line of credit as you get your practice going and sometimes need the cash flow.”
Expanding a Practice
Established dermatologists should have an easier time getting loans to expand their practices. They have, one hopes, a track record of success and assets to put up as collateral.
Mid-career physicians “have cash flow, physician assets and equity to some degree in a house and personal assets,” Dr. Marcinko observes. “Banks can attach loans to personal assets and savings accounts. Ninety-nine percent of times you must sign a personal asset guarantee. Mid-lifers have assets young ones don’t, so mid-lifers aren’t quite the risk. They have businesses that have value and cash flow. Banks like cash flow.”
However, even veterans must do some homework before approaching a bank. “You still want to establish why you want the money and how the expansion will increase your income,” McGraw says.
Another tip: If the bank has loans out with reputable vendors, you might ask the loan officer to recommend them to you as potential contractors. “Sometimes keeping it local and supporting others with loans at the bank can be helpful,” she says.
Assessment
Dr. Marcinko adds, “Bankers today want you to come in with a well-reasoned, well-thought-out and well-written business plan. Give bankers a 30-second elevator speech on why you are different. It’s really important to ask yourself, ‘What can I offer the community as a doctor in my specialty that nobody else can?’ If you bill yourself as the first dermatologist to do laser surgery, that’s a perceived advantage. You purchased the equipment and learned to use it. But anyone can do that. If you can come up with something that nobody else has or can do, that’s how you’re successful in anything.”
Link: Dr. Marcinko Interview
Link: https://medicalexecutivepost.com/wp-content/uploads/2009/08/dr-marcinko-interview.pdf
Conclusion
And so, your thoughts and comments on this Medical Executive-Post are appreciated. Tell us what you think. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, be sure to subscribe to the ME-P. It is fast, free and secure.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Sponsors Welcomed
And, credible sponsors and like-minded advertisers are always welcomed.
Link: https://healthcarefinancials.wordpress.com/2007/11/11/advertise
Filed under: "Doctors Only", Book Reviews, Career Development, CMP Program, Experts Invited, iMBA, Inc., Interviews, Managed Care, Practice Management, Practice Worth, Recommended Books, Research & Development | Tagged: ADVANCE Newsmagazines, bankers, business plan, certified medical planner, CMP, credit, credit crunch, david marcinko, dermatologists, Health Care Group, Jerome Potozkin, loans, MD, Michael Gibbons, plastic surgeons, Sandra McGraw, www.certifiedmedicalplanner.com, www.medicalbusinessadvisors.com | 2 Comments »
History of National Doctors’ Day

By Dr. David E. Marcinko MBA CMP™
http://www.CertifiedMedicalPlanner.org
National Doctors’ Day is held every year on March 30th – April 1st – in the United States. It is a day to celebrate the contribution of physicians who serve our country by caring for its’ citizens.
The first Doctor’s Day observance was March 30, 1933 in Winder, Georgia. Eudora Brown Almond, wife of Dr. Charles B. Almond, decided to set aside a day to honor physicians. This first observance included the mailing greeting cards and placing flowers on graves of deceased doctors.
Following overwhelming approval by the United States Senate and the House of Representatives, on October 30, 1990, President George Bush signed S.J. RES. #366 (which became Public Law 101-473) designating March 30th as “National Doctor’s Day.”

***
Filed under: Career Development, CMP Program, Touring with Marcinko | Tagged: CMP™ Course, National Doctors' Day | 1 Comment »
![]()
Happy World Oral Health Day
[By Staff Reporters]
Today is March 20th – World Oral Health Day (WOHD), a day in which dentists and organizations worldwide are promoting oral health.
***

***
According to the FDI WOHD website, 90% of the world’s population will suffer from oral diseases in their lifetime, and many of them can be avoided with increased governmental, health association and society support and funding for prevention, detection and treatment programs.

Filed under: Breaking News, Career Development, iMBA, Pruitt's Platform | Tagged: DDS, dental care, World Oral Health Day | Leave a comment »
And … Depression
***

***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Book Marcinko: https://medicalexecutivepost.com/dr-david-marcinkos-bookings
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, IT, business and policy management ecosystem.
***
Filed under: Career Development, Ethics | Tagged: Physician Burn-Out, Physician Depression | 4 Comments »
A Brief History

By Eric A. Dover MD
The first medical board was established in Connecticut in 1792 by the state legislature. It consisted of a group of physicians who evaluated the competency of physicians wishing to practice in the State. Medical Boards eventually evolved and became very powerful with the addition of Medical Practice Acts containing a plethora of administrative rules. The Medical Boards stated mission was, and still is, the protection, health and safety of the public. State Boards formed a national group, the Federation of State Medical Boards (FSMB), in 1912. The FSMB was the first institution to publically list names of disciplined physicians in a monthly bulletin.
In the 1980’s and 1990’s there were a number of high profile cases involving physicians and public safety. One such case, international in scope, concerned surgeon Dr. Jayant Patel. Significant news coverage regarding his surgical outcomes and knowledge resulted in the heightened questioning of Medical Boards and whether they were actually fulfilling their mission of protecting public health and safety. The Oregon Medical Board (OMB) was scrutinized for allegedly “ignoring” 79 complaints, and at least three deaths, attributed to Dr. Patel’s surgical care from 1989 to 1998. The OMB abdicated all responsibility for the situation with a myriad of excuses for why they had no control over this physician or the HMO he worked for.
OMB
The OMB then came to the state legislature with a “fix” to supposedly prevent any further such incidents. The OMB advocated for greater authority over physicians and greater independence from government oversight. With the din of the press and public, the Oregon Legislature gladly granted the OMB their wish. Other states followed Oregon’s example. Not a single individual associated with the OMB, whether administrative or board member was investigated in any meaningful way for their horrendous dereliction of duty. Not one of them had their license restricted, suspended or revoked for such serious offenses. None of them were ordered to pay out of pocket to go to “programs” for competency evaluations, psychological examinations or “courses” to help them become better board members. No one resigned, nor was anyone dismissed, from their position of power. The OMB’s inaction led to a number of deaths and numerous patients with chronic post-surgical medical disorders, yet all individuals involved with the OMB were protected from malpractice lawsuits
Case examples
With cases such as Dr. Patel’s featured prominently in the mainstream media, Medical Boards nationwide came under intense public pressure and scrutiny as it became clear they were not fulfilling their mission of protecting the public’s health and safety. The public saw physicians as a privileged class, protected by their colleagues and Medical Boards. They were correct to a degree. Public safety groups like Public Citizen, who had been taking Medical Boards, hospitals and large clinics to task for years regarding what they felt was a lack of physician oversight and discipline, began ranking state medical boards based on how many disciplinary actions they handed out each year. In their 2011 report, Public Citizen’s Health Research Group Ranking of the Rate of State Medical Boards’ Serious Disciplinary Actions, 2009-2011, the authors made the erroneous assumption that the greater the number of physician “disciplines” (actions) per 1000 physicians, the better job that State’s Medical Board was doing. Therefore, at 6.79 actions per 1000 physicians, Wyoming was doing the “best” job and at 1.33 actions per 1000 physicians, South Carolina was doing the “worst” job.
Medical boards vary state -2- state
Medical Boards vary remarkably from state to state. There are only two constants among them. First, each state has a Medical Board. Second, the Board makes all final decisions concerning licensees. Otherwise, there’s no consistency when it comes to what’s sandwiched in between. The Medical Board’s authority is grounded in the States Medical Practice Act, which gives them the authority to enforce laws for licensing, monitoring and disciplining physicians in the state. Every state has its own unique laws and processes, but every medical practice act covers the basics regarding oversight of physicians practicing medicine in the State.
Assessment
The U.S. Federation of State Medical Boards (FSMB) periodically issues guidelines on the essential elements of a medical practice act.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, urls and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements.
Contact: MarcinkoAdvisors@msn.com
Subscribe: MEDICAL EXECUTIVE POST for curated news, essays, opinions and analysis from the public health, economics, finance, marketing, I.T, business and policy management ecosystem.
***
Filed under: Career Development, Ethics, Risk Management | Tagged: A Brief History of Medical Boards, Eric A. Dover MD | Leave a comment »
NON-CONSENSUAL AMOROUS RELATIONSHIPS DEFINED
By Vicki L. Buba JD
By Dr. David Edward Marcinko MBA CMP™
http://www.CertifiedMedicalPlanner.org
An “Amorous Relationship” is defined as a consensual romantic, sexual or dating relationship. This definition excludes marital unions. The term also encompasses those relationships in which amorous or romantic feelings exist without physical intimacy and which, when acted upon by the faculty or staff member, exceed the reasonable boundaries of what a person of ordinary sensibilities would believe to be a collegial or professional relationship. The faculty/student and supervisor/employee relationship should not be jeopardized by question of favoritism or fairness in professional judgment.
Furthermore, whether the consent by a student or employee in such relationship is indeed voluntary is suspect due to the imbalance of power and authority between the parties. All members of the healthcare entity should be aware that initial consent to a romantic relationship does not preclude the potential for charges of conflict of interest, or for charges of sexual harassment arising from the conflict of interest, particularly when students and employees not involved in the relationship claim they have been disadvantaged by the relationship. A faculty, staff member or graduate assistant who enters into an “Amorous Relationship” with a student under his or her supervision, or a supervisor who enters into an “Amorous Relationship” with an employee under his or her supervision, must realize that if a charge of sexual harassment is subsequently lodged, it will be exceedingly difficult to prove blamelessness on grounds of mutual consent. This policy is superseded by the laws governing inability to consent based on age.
HANDLING ROMANTIC PATIENT ADVANCES
While physicians vary in their approaches to managing flirtatious patients, many agree that nipping the behavior in the bud is critical to maintaining professionalism and upholding ethical standards. “It’s flattering to have a flirtatious patient,” said Dr. William P. Scherer MS, Professor of Radiology at the Barry University School of Medicine, Boca Raton, Florida. “But, we have an obligation to protect the integrity of our medical profession, and to our marital contracts and spousal relationships and family, and to act professionally at all times” [personal communication].
Dr. Scherer finds it helpful to put some professional distance between himself and a flirtatious patient. “I have no problem saying to a patient: I appreciate what interests you may have, but I have to draw the line to take proper professional care of you, instead.”
And a good way to derails flirtatious behavior from patients is by deflecting their unwelcome comments. “And, you can’t act sheepish about it.” When a patient’s remark crosses the line from complimentary to something uncomfortable, the doctor may either curtly laugh it off or ignore it. “I don’t acknowledge the statement and immediately move the conversation into something clinical in order to put the rest of the visit in a serious tone.”
On the other hand, Dr. Barbara S. Schlefman MS, a fitness trainer and retired podiatrist, instructed her nurses to have another staffer accompany them into an examination room when a patient is known for being flirtatious was waiting to be seen; and to leave the door open [personal communication].
Likewise, other physicians use a “more is merrier” approach for themselves and their staff as a defense against flirtatious behavior. This is a problem that can be avoided by having physicians never see patients alone. So, as Dr. Schlefman advised, be sure to always a nurse or medical assistant in the room with the physician, even if you have to see somebody in the office on call after hours. And, be sure to have a call schedule for the nursing and medical assistant staff that includes patients of both genders, regardless of physician gender, since flirtatious behavior can be same-sex flirtatious behavior. Fortunately, adjunct or visiting clinical professors, or doctors on a medical school clinical teaching staff, rarely have patient encounters without a medical student, intern, resident fellow or nurse in the room during examinations.
Recognize the Signs
While it’s important that physicians don’t act on a flirtatious patient’s advances, it’s equally critical to recognize subtle flirtatious signs from a patient; according to Donna Petrozzello MD, an otolaryngologist at the California Sinus Centers.
A patient that maintains unusually long eye contact with their doctor, or engages in talk not related to their visit, or makes a habit of touching the physicians when not medically necessary may be flirting. Additionally, doctors can protect themselves when performing some common procedures that put the physician in close proximity to a patient’s face, breasts, genitals, legs and even feet. That closeness could turn a clinical exam into a flirtatious event. Wearing a mask to perform each of these local or regional examinations is not only for the purposes of infection control but gives the added benefit of establishing some personal space and protection, to avoid any potential misunderstanding. For example, auscultating lungs through a shirt, not underneath, is a good idea with this type of exam on a young woman patient.
[Two icons of romantic relationships]
Filed under: Career Development, Ethics, iMBA, Inc. | Tagged: CMP™ Course, CONSENSUAL AMOROUS RELATIONSHIPS IN MEDICINE, David E. Marcinko, HANDLING ROMANTIC PATIENT ADVANCES | 6 Comments »
|

|
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
8
***
Filed under: Career Development | Tagged: Investor's Guide to Better Writing, Vitaliy Katsenelson CFA | 1 Comment »
Experimenting in Business
By Dan Ariely PhD
***
Part of the CAH Startup Lab Experimenting in Business Series
By Rachael Meleney and Aline Holzwarth
Missteps in business are costly—they drain time, energy, and money.
Of course, business leaders never start a project with the intention to fail—whether it’s implementing a new program, launching a new technology, or trying a new marketing campaign.
Yet, new…
***
Filed under: Career Development, Experts Invited, Interviews, Op-Editorials, Retirement and Benefits, Videos | Tagged: Aline Holzwarth, Backward Market Research, CAH Startup Lab, Dan Ariely PhD, Rachael Meleney | Leave a comment »
A New HBR Report on Job Satisfaction

By Rick Kahler CFP®
According to a new global survey on work and happiness, a significant number of us aren’t very happy about our workplace. That’s especially unfortunate, since working is how most of us spend the majority of our waking hours.
World Happiness Report
The results of the survey, the World Happiness Report, were summarized in the Harvard Business Review by Jan-Emmanuel De Neve and George Ward on March 20th, 2017. When asked a yes/no question (maybe was not an option) if they were satisfied or dissatisfied with their jobs, most workers around the world said they were satisfied with their jobs. Austria has the highest job satisfaction with 95%, followed closely by Norway and Iceland.
Since I recently visited Iceland, this immediately grabbed my attention. While I acknowledge that my interactions with the workforce of Iceland were limited, I did not get the impression that most were happy. Most seemed to be relatively unhappy. And therein lies the difference: being satisfied with one’s work does not equate to being happy with it.
When asked if they were happy, people’s responses varied greatly depending whether they were blue-collar workers, white-collar workers, or small business owners. About 60% of those who were managers, executives, or professionals (white-collar) reported being happy, while just 45% of those working at more labor-intensive jobs (blue-collar) said they were happy. The number of happy workers was higher—65% to 75%—for workers living in North America, Australia, New Zealand, Western Europe, and Central and Eastern Europe. Regions like South Asia and Africa reported lower happiness levels, from 40% to 55%.
Business Owners
One fact I found especially interesting is that business owners [like doctors] had lower levels of happiness than full-time employees and generally ranked in the middle of the happiness range in most regions. This probably comes as no surprise to a small business owner. My 35 years of experience doing financial planning for business owners finds that many work harder, take greater financial risks, and make less than if they did the same job for a larger company.
Maybe there is an opportunity for a country western song here:
***

“You can take this business and shove it.”
No matter how unhappy you may be working, you would be even unhappier unemployed. De Neve and Ward note that “unemployment is destructive to people’s wellbeing.” Those employed rate their happiness higher in every region in the world. The study also found that repeated incidences of unemployment permanently decreases a person’s happiness, which doesn’t rise to previous levels after they have found a new job.
While most workers are satisfied with their jobs, only about 50% are happy with their jobs. But how happy is happy? The surveyors wondered how many workers were really fulfilled, engaged, and excited about their jobs. To find this out, they asked the respondents if they felt “actively engaged,” “not engaged,” or “actively disengaged.”
The Shocker
Here is the shocker to me: globally less than 20% of workers say they are engaged with their jobs. In Western Europe that number is 10% and in East Asia it’s around 5%. The Caribbean, at 28%, had the highest level of active engagement. About 65% of workers say they are “not engaged” at work, while 15% to 20% of workers are actually “actively disengaged.”
Clearly, the planet has an epidemic of people not being excited to go to work in the morning. Most people are not finding fulfillment, connection, happiness, growth, or challenge in their workplace.Assessment
Assessment
If you are one of them, it may be worthwhile to evaluate your job choices. Since work requires so much of our time, being engaged and happy with it has a significant impact on our well-being.
More: Physician “Burnout” Rates
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
8
***
Filed under: Career Development | Tagged: George Ward, Jan-Emmanuel De Neve, job satisfaction, Rick Kahler CFP®, World Happiness Report | 1 Comment »
Publishing and Peer-Review Opportunities Always Available
By Ann Miller; RN, MHA![]()
If you have academic credentials and experience like those of our contributing authors, subject matter experts and “thought-leaders – and would like to contribute to our blog or become a peer reviewer – please contact us today!
CV Required
We’d be happy to review your CV, submission and/or a copy of you previously published works. OR, just point us to your own blog, wiki, or website; etc. You may also use the contact form, below.
Phone: 770-448-0769
Email: MarcinkoAdvisors@msn.com
Channel Surfing
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these 50 topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register.
Link: http://feeds.feedburner.com/HealthcareFinancialsthePostForcxos
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
Sponsors Welcomed
And, credible sponsors and like-minded advertisers are always welcomed.
Link: https://healthcarefinancials.wordpress.com/2007/11/11/advertise
Filed under: "Advisors Only", "Doctors Only", Career Development, Experts Invited, Quality Initiatives | Tagged: CFA, CFP, CMP, david marcinko, financial advisors, Health Economics, health journalist, healthcare administration, Healthcare Finance, healthcare thought leaders, medical practice management, www.CertifiedMedicalPlanner | Leave a comment »
![]()
By staff reporters
Tell us about the issues affecting your physician-focused financial advisory or financial planning practice in 2020.
We are conducting a brief survey to learn more about the key issues affecting your practice, and how they impact your outlook for the coming year.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
8
***
Filed under: "Advisors Only", "Ask-an-Advisor", Career Development, Practice Management | Tagged: Physician Focused Financial Advice, Tell us About your Financial Advisory Practice | Leave a comment »
![]()
Crowd Sourcing My Job Search – An Academic Social Media Experiment?

Dr. David Edward Marcinko MBBS DPM MBA MEd BSc CMP®
Any New Year typically brings to mind the passage of Father Time.
And, as a former endowed chairman and distinguished Business School professor of capitalism, health economics, policy and management; it’s hard to believe that I’ll be finishing up my current visiting scholar-on-sabbatical tenure after this Spring semester.
So, I am crowd-sourcing my next university job search as an emerging trend. It’s the career development equivalent of my just launched WIKI health dictionary project.

***
Filed under: Breaking News, Career Development, iMBA, Inc., Touring with Marcinko | Tagged: David Edward Marcinko, health dictionary series | 1 Comment »
![]()
A Framework to Identify the influence of Special Interest Groups and “Bent” Science
***
Channel Surfing the ME-P
Have you visited our other topic channels? Established to facilitate idea exchange and link our community together, the value of these topics is dependent upon your input. Please take a minute to visit. And, to prevent that annoying spam, we ask that you register. It is fast, free and secure.
More:
In Bending Science: How Special Interests Corrupt Public Health Research 1 Thomas McGarity and Wendy Wagner describe how special interest groups scheme to advance their own economic or ideological goals by using distorted or “bent” science to influence legal, regulatory and public health policy.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
* 8
Filed under: Book Reviews, Career Development, Health Law & Policy | Tagged: Bending Science:, Policy and Regulatory Decision Making in the Medical Profession, Thomas McGarity, Wendy Wagner | 2 Comments »
![]()
By Rick Kahler MSFS CFP®
Not long ago, one of Americans’ top fears was public speaking. Apparently Toastmasters is working; this fear didn’t even make this year’s Top 10 list.
Survey of American Fears
Chapman University recently completed its third Survey of American Fears, as reported in an October 12 article in Science Daily. Based on responses to questions about 65 potential fears from more than 1,500 adult participants, here are the top 10 things Americans fear:
Four of these top fears (numbers 3, 7, 8, and 10) relate directly to financial health
The survey additionally identified four attitudes essential to motivating ourselves to protect against a fear:
Let’s apply these attitudes to just one of the top fears: not having enough money for the future.
There’s a good reason this fear made the top ten. Around 70% of all Americans live paycheck to paycheck. Faced with a sudden need for $1,000, 75% would need to sell something or borrow to come up with the money. Around 48% would need to sell something or borrow just to come up with $400. Clearly, many Americans are not saving for emergencies and retirement.
***

***
Motivation
Let’s look at the first motivator, This can happen to me. We are a nation of optimists. Many have money scripts like “The money will always be there,” and “Social Security and future government programs will provide for me.” We don’t consider realities such as the meager living Social Security would provide or whether taxpayers can or will support expanding aid programs. Thinking happy thoughts won’t create emergency reserves or retirement investments.
Which brings us to This is serious. If you are not investing enough money from each paycheck to continue your standard of living into retirement, it is really serious. If you retire unprepared and underfunded, it will be too late to save. And continuing to work won’t be an option for 8 out of 10 because of health reasons or inability to find a job. This is serious.
I can actually do something to help myself. Today, while you have a job and your health, you can make changes. You can get creative to reduce your standard of living and begin to save and invest. You can change your diet and take better care of your health so you can work longer. You can go back to school and reeducate yourself so you stay relevant in the workforce. You can make double and triple payments on your debts and become debt free. You can relocate to an area with a lower cost of living. You can even focus on rebuilding great relationships with your kids so they may let you move in with them in your last years.
Taking action will make a difference. Indeed it will—and starting now is key. Someday is today. Search online for printed materials, online courses, local classes, or professionals that can help you create spending plans that work, get out of debt, creatively cut expenses, increase your income, and maximize your investment growth.
Assessment
There is a lot you can do to help yourself, and your most important action is to take a first step.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
8
***
Filed under: Breaking News, Career Development, Experts Invited, Research & Development | Tagged: Rick Kahler CFP®, Survey of American Fears | 1 Comment »


[Chief Executive and Education Officer]
David E. Marcinko MBBS DPM FACFAS MBA MEd BSc
***
Filed under: Breaking News, Career Development, iMBA, Inc. | Tagged: David Edward Marcinko, Dr. David Marcinko, Linked-In | Leave a comment »
![]()
Choose Science, Technology, Engineering and Mathematics
By Bert Mesko MD
***

It is as simple as the ABC: if you are thinking about your future now, please choose Science, Technology, Engineering and Mathematics (STEM). If you are way in your career, please send this to those who are still considering their options. Read more.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
![]()
![]()
***
Filed under: Career Development | Tagged: Bert Mesko, Engineering and Mathematics, Science, STEM, Technology | Leave a comment »
![]()
Practical Psychology

By Gus
A gentleman is one who puts more into the world than he takes out.
-George Bernard Shaw
According to a recent article in Salon, the “radical” act of paying attention to each other.…
***

***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
***
Filed under: Career Development, Ethics, Videos | Tagged: 50 Things Every Gentleman Should Know | 1 Comment »
![]()
Finding satisfaction in medical practice
By DR RNJB MD
Every day I read many letters and posts from undergraduate students who view a career in medicine as the ultimate prize for academic achievement.
While this view may keep many pre-med students on the road to high academic achievement, a more realistic view of this profession and it’s practice is a better choice for […]

Is medicine the “holy grail”(finding satisfaction in practice)? — Medicine From The Trenches
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
***
Filed under: Career Development | Leave a comment »
![]()
A CMS … Proposal
[By Andy Salmen]
The Centers for Medicaid and Medicare Services (CMS) have finally released the much anticipated unveiling of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) rule proposal.
The goal of this rule is to establish key parameters for the new Quality Payment Program, a framework that includes the Merit-based Incentive Payment System (MIPS) and Alternative Payment Models (APMs). These two paths for compliance allow doctors more flexibility in achieving compliance.
MIPS
MIPS scores clinicians based measures and activities chosen by physicians and is based on their specialty. MIPS would basically streamline and combine three of the different programs that currently exist under Medicare. These programs are Physician Quality Reporting System, the Value-Based Modifier Program, and the ‘Meaningful Use’ of electronic health records.
There will be four performance categories for clinicians (clinicians include physicians, physician assistants, nurse practitioners, clinical nurse specialists, certified registered nurse anesthetists, etc.) to be scored on. These performance categories are:
APMs
CMS proposed implementing an Advanced Payment Models (APM) pathway, allowing eligible clinicians to become “qualified participants”. This means that eligible clinicians will be able to earn statutorily specified incentives for participation.
CMS predicts most providers to initially opt for MIPS. It is expected that participation in APMs, both number of physicians and number of payment models, will grow over time, as this program will qualify clinicians for financial bonuses in exchange for taking the risks associated with providing “coordinated, high-quality care”, according to CMS.
***
***
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
***
Filed under: Career Development, Practice Management | Tagged: Advanced Payment Models, APMs, By Andy Salmen, CMS Reveals MACRA Rule, meaningful use, MIPS, Value-Based Modifier Program | 5 Comments »
MAYBE NOT?
[By Rick Kahler MSFS CFP®]
How do you know when the cost of a college education is really worth it? A lot of factors—both financial and emotional—go into making that decision. Weighing the pros and cons can be daunting.
Example:
Let’s consider a couple of examples that will help conceptualize the process of determining if a college education makes financial sense.
First, here are some numbers for traditional students. The cost of an average four-year education at Yale is around $240,000, and the average starting salary for its graduates is $55,000. The monthly payment on a student loan for that amount would be $2,420, or $29,159 a year. That equals 53% of the starting salary. There are a lot of other variables to consider, like potential scholarships that would lower the tuition, or lowering the loan payment by stretching out the amortization period (which actually increases the overall cost). But given these facts the answer to whether this education makes financial sense is a no-brainer. No; find another school.
At the South Dakota School of Mines, by contrast, the cost of an average four-year education is around $65,000 and the average starting salary is $68,000. The monthly payment on a student loan for that amount would be $648, or $7,897 a year. That equals 12% of the starting salary. The cost of this education makes complete sense.
For traditional students, my personal rule of thumb is this: don’t pay more than one and a half times the average starting salary of a job for the education to obtain it.
For non-traditional students who are looking to switch careers, the calculation is a little more involved. You must weigh the salary you earn in your current career with the cost and net increase in the career you are considering.
Example:
Recently a reader emailed me this question: “I have a bachelor’s degree in my chosen career and am unable to find a full-time, benefitted, permanent job. When is it no longer a good financial decision to not go back to college? I can pick up a degree in a different field for $8,000. If I am 12-13 years from retirement, is it worth it?”
The average salary for a job in her career field is $20 an hour, or $42,000 a year. The problem is that she has not been able to find employment in her career field. She has only been able to find temporary jobs with earnings of $9.77 to $12.75 per hour.
So far her four-year degree has netted her around $12,500 a year. Her research shows that if she went back to school for two years she could switch to a career field more in demand in her area and earn $45,000 a year. That’s $32,500 more per year. If she invests two years and $8,000 in education, then works in her new career for 10 years, she can earn an additional $325,000 before retirement.
If she were to borrow the funds needed for her education and repay the loan at 4% for 10 years, her monthly payment would be $81, or $972 a year. That equals about 2% of her salary. Given these facts, going back to school makes clear financial sense.

Assessment
Of course, financial factors are not the only ones to consider in deciding whether to invest in education. Looking at the numbers is essential, but it’s equally important to find a career field that suits your talents and interests. It makes no sense to spend time and money preparing for a career you don’t want. The most rewarding college investment is one that provides worthwhile returns in emotional satisfaction as well as financial success.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
***
Filed under: "Ask-an-Advisor", Career Development | Tagged: college costs, Rick Kahler CFP® | 4 Comments »
![]()
Find out with this income calculator
[By Staff reporters]
***

Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
8
***
Filed under: Career Development, LifeStyle, Voting Polls | Tagged: American middle class?, income calculator | 6 Comments »
![]()
Florence Nightingale’s Birthday
[By Staff Reporters]
National Nurses Week
[May 6-12, 2016]
International Nurses Day is celebrated around the world every May 12th, the anniversary of Florence Nightingale’s birth.

The Florence Nightingale International Foundation
According to their website, the FNIF is the International Council of Nurses (ICN) premier foundation. It supports and complements the work and objectives of the ICN. Its history dates back to 1912 when a memorial to Florence Nightingale was first proposed by Mrs. Ethel Bedford Fenwick at an ICN Congress in Cologne. The vision was of an educational foundation for nurses. As the First World War intervened, it was not until 1929 that the memorial was finally activated by the ICN Grand Council in Montreal. Mrs. Bedford Fenwick, the first president of ICN was elected the first chair of the Florence Nightingale Memorial Committee.
History
From 1931, national Florence Nightingale committees were established in countries where ICN had member associations. In 1932 discussions were held between ICN and the League of Red Cross Societies to use their Red Cross international post-graduate courses as an international memorial to Florence Nightingale.
The ICN Grand Council agreed to take over the international courses, and in 1934, established the Florence Nightingale International Foundation (FNIF) as a living memorial to Florence Nightingale. FNIF became an autonomous organization under British law with its own governing body and a mandate to develop and promote nursing education world wide.
Charitable Intent
FNIF is a registered Charity in the United Kingdom and maintains its original purpose; to support the advancement of nursing education, research and services for the public good. Though UK registered, the day-to-day administration is carried out in Geneva through the International Council of Nurses, a federation of 133 national nurses’ associations working to ensure quality care for all and sound health policies globally.
FNIF is a new foundation for a new day! They have a new board, a new program and a new look. The focus is global – as the needs of nurses everywhere are similar but the resources to meet those needs differ around the world.
Link: http://www.fnif.org/aboutfnif.htm
Assessment
As you know, Florence Nightingale is considered to be the founder of modern nursing. She was devoted to health, education and research, and worked tirelessly to raise health care standards.
At the M-P, we are honored to promote her legacy. You can find information about Florence Nightingale on the Florence Nightingale International Foundation (FNIF) web site and the Girl Child Education Fund. On this page you will also find items for purchase and links that will help you plan and celebrate the nursing profession making your special event a success.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Filed under: Alerts Sign-Up, Breaking News, Career Development | Tagged: Ethel Bedford Fenwick, Florence Nightingale, Florence Nightingale International Foundation, Florence Nightingale Memorial Committee, FNIF, ICN, International Council of Nurses, International Nurses Day, League of Red Cross Societies, nurse, Nurses Day, nursing, RN | 4 Comments »
By Dr. David Edward Marcinko MBA CMP®
http://www.CertifiedMedicalPlanner.org
The health care provider should not alter the medical record under any circumstances.
The office, clinic or hospital must zealously guard its medical records from alterations by physicians or members of the nursing staff.
Even an inconsequential alteration will throw the validity of the entire record into question. If an entry must be changed, a single line should be drawn through the entry, taking particular care to make sure that the original entry is clearly legible. The new entry should be written above or next to the old entry, and the date of the new entry, as well as the name of the person making the entry, should be recorded. The entry must also be signed by that person.
Juries are very intolerant of altered medical records; and even innocent mistakes, such as the loss of a few pages of a record, will be construed as an intentional cover-up. Under no circumstances should materials such as liquid paper or other opaque liquids be applied to the record in order to correct any entry.
Assessment
The health care provider should not alter the medical record under any circumstances.
Conclusion
Is there an emerging migration back to paper medical records?
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
Harvard Medical School
Boston Children’s Hospital – Psychiatrist
Yale University
Filed under: Career Development, iMBA, Inc., Practice Management, Risk Management | Tagged: Altered Medical Records, Dr. David Marcinko, medical records | 1 Comment »
Know the territory and solve a problem
![]()
 |
By Jonah Comstock |
Health tech investors are looking for entrepreneurs that really understand the healthcare space and are solving the real problems doctors are facing. That may sound like an obvious statement, but according to Dr. Ricky Bloomfield, director of mobile technology strategy at Duke University and Claire Celeste Carnes, partner at Providence Ventures, plenty of entrepreneurs fail that test.
Bloomfield and Carnes were one half of a panel at HIMSS16 in Las Vegas that aimed to answer the question ‘What are investors looking for in a health tech company?’ HealthLoop CEO Todd Johnson and Health Expense CEO Vineet Gulati rounded out the panel, moderated by Andrew Colbert, managing director of Ziegler. “One of the things when we meet with individuals is making sure that they’ve started with the problem in mind,” Bloomfield said. “We’ll see people who see the latest technology, whether it’s a wearable or a sensor, whatever it might be, and they’re going all around trying to look for a way to apply that technology.
One of the best examples is Google Glass, where they released the technology and said, ‘Now look for good ways to use this.’ And now where is Google Glass?” Gulati said that his healthcare payment startup found that a deep understanding of the industry was a big differentiator for them when they went up against other startups. “If you don’t understand the complexity, that’s not going to result in either a valuation or a successful business in the end,” he said. “Whoever comes to the table has to understand that complexity and be willing to work through it. The benefits market is like an elephant, everybody understands a part of it, everybody has their unique point of view and everybody tries to attack a single point of value. Understanding the entire value chain is absolutely critical.”
***

***
Even when entrepreneurs make an effort to be knowledgable, the healthcare space is complex enough that they’ll sometimes fall short. Bloomfield says the easiest way to build that understanding is to enlist the help of actual physicians. “I’ve worked with folks who showed me a product and they hadn’t engaged any physicians yet in the design or strategy of their solution, and I could immediately see several different holes in their product,” he said. “If they had engaged with any physician they would have pointed them out to them.” Similarly, Carnes said, the best investments will be companies that have both knowledge and humility. “Management team is very important to us,” she said. “Do they have both the maturity, experience in this space, and are they coachable and willing to learn about the intricacies of healthcare? No one’s going to get things right 100 percent of the time out of the gate, so there’s going to need to be some adjustments as we go to market.
A management team that is confident and leading but can adjust to the market and is coachable is really one of the primary things we look for.” The final thing that will help a startup get noticed is, of course, evidence that its technology works. As Bloomfield pointed out, this one can be a real challenge. “There’s a huge Catch-22 there,” he admitted. “It takes a lot of investment to get to the point where your product can even show value, much less have a randomized control trial. This is why drugs cost billions of dollars to make, because they can invest that. I think it’s really hard. It’s a really hard position to be in.
***
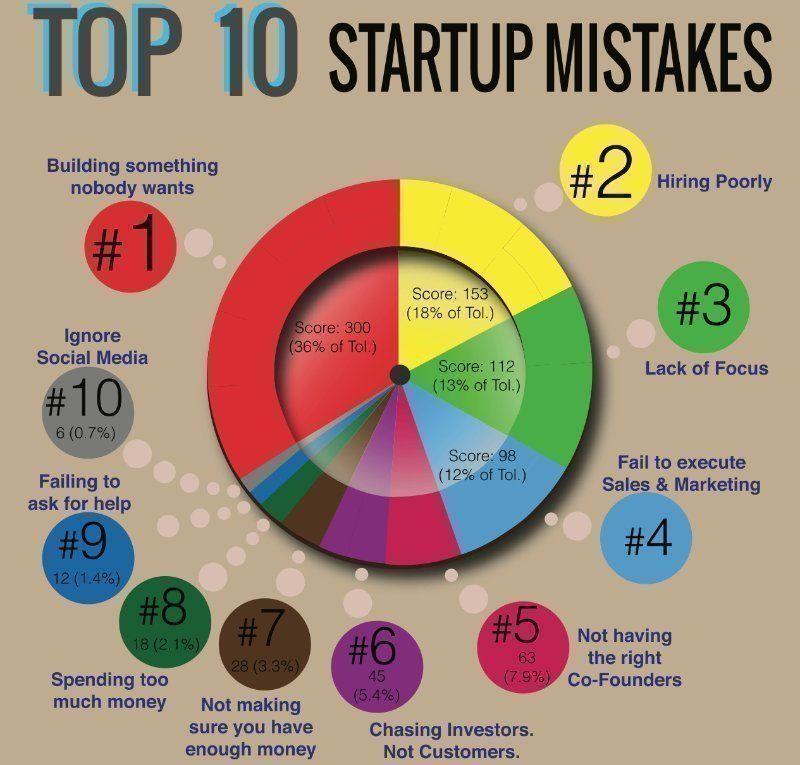
***
Assessment
So sometimes anecdotal evidence is the best you get until you can partner with a large health system and get a lot more information.”
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
***
Filed under: Career Development, Research & Development | Tagged: Dr. Ricky Bloomfield, health tech startup, HealthLoop, Jonah Comstock, Venture Capital, Vineet Gulati | 3 Comments »
![]()
A Passionate Discussion
By Rick Kahler MS CFP®
Income inequality is a topic of passionate discussion today in many of the circles I move in. The discussion typically starts with a foregone conclusion that income inequality is a huge problem in the US. Some solutions I hear include increasing the top income tax bracket to 90%, initiating an annual wealth tax, or increasing the estate tax to 100%.
While leveling the playing field will certainly solve income inequality, it won’t solve the real problem. When I say that, I often get stares of bewilderment and disdain. It isn’t unusual for people to slowly distance themselves as if I had shapeshifted into Donald Trump.
How bad is it?
First, how bad is income inequality in the US? It’s certainly no worse today than it’s been in the last 80 years. The CIA World Factbook 2015 Gini Index, a rating where 0 is equal income and 100 is completely unequal income, finds the US rates a 45.0, exactly what it was in 1929. That puts us in 38th place, slightly above the global median, which is 39.4. The worst 30 countries have ratings of 46.8 to 63.2.
Regardless of the fact that it has not increased over the last 80 years, what is the real problem with income inequality? A common assumption is that it has created an America where most people don’t have enough to afford a minimal quality of life.
But is that true?
In a column from October 2015, George Will cites a new book, On Equality, by Harry G. Frankfurt, a Princeton emeritus professor of philosophy. Frankfurt drives home a main contention that economic inequality is not inherently morally objectionable and that “doing worse than others does not entail doing badly.” His alternative to economic egalitarianism is the “doctrine of sufficiency,” which is that the moral imperative should be that everyone have enough.
Now, consider this
If you are a US citizen with an income of over $32,400, you are in the world’s top 1%. Globally, you are considered “rich.” Indeed, the poorest 1% of US citizens have more wealth than two-thirds of the world’s people. Clearly, income inequality in the US doesn’t inherently mean everyone in society doesn’t have enough. This would suggest that complaints about US income inequality may be in response to something other than having enough.
***

***
Perhaps the real problem is more of a “discontent of those who are comfortable but envious,” as George Will suggests. Consider this: to be in the top 1% in income in the US you need to earn over $380,000 a year. Someone earning $32,400 a year, even though they are in the global top 1%, may easily lose that perspective when viewing someone earning over $380,000. The comparison could foster discontent by stirring up feelings of envy, jealousy, unworthiness, shame, and guilt. Rather than taking responsibility for and exploring these difficult emotions, instead we often shove them deep within and demonize others.
Will suggests that the biggest underlying producer of income inequality is freedom. Freedom includes the power to choose careers, such as opting to be a teacher rather than an engineer with full knowledge that teachers generally earn substantially less than engineers. The economic and non-economic benefits of each profession are dictated by market forces, rather than those in government deciding the winners and losers.
Assessment
Envy of the rich is almost timeless and universal. Properly reframed, it also can be motivating. Contrary to common perception, 85% of the top 1% did not inherit wealth but are first-generation millionaires or billionaires. Perhaps envy didn’t drive them to try to tear down what others had achieved. Instead, it motivated them to build their own success.
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:

***
Filed under: Career Development, Ethics, Funding Basics | Tagged: Harry G. Frankfurt, Income Inequality, On Equality, Rich envy, Rick Kahler CFP® | 1 Comment »
![]()
Dear Dr. David Marcinko,
#GivingTuesday is the global movement dedicated to giving back. It kicks off the holiday giving season and I hope you will join me by making a contribution to APHA.
Please consider making a donation in two areas where we need your help the most:
Your donation makes you part of Generation Public Health, APHA’s movement to create the healthiest nation in one generation. With your generous contribution we can continue to support the groundbreaking work of public health professionals and help turn today’s students into tomorrow’s leaders.
After you make your donation, please share on Facebook, Twitter, Instagram and other social media that you donated on #GivingTuesday and joined #GenerationPublicHealth.
Thank you for all that you do to support APHA!
Sincerely,

Georges C. Benjamin, MD
[Executive Director]

Filed under: Career Development, Ethics | Tagged: APHA - Giving Tuesday, Generation Public Health, Georges C. Benjamin, MD | Leave a comment »

![]()
By Ann Miller RN MHA
[Executive-Director]
If you are not reading our subscriber “comments”, you are not getting all you can from each Medical Executive-Post. And, if you are not reading the links in each post, you are not getting all you can from the ME-P.
Industry Specificity
Then, purchase our textbooks, white-papers, handbooks, dictionaries and CDs for deeper integrated and peer-reviewed industry specificity.
Consulting Too!
And, we are now scheduling private consultations, events and corporate engagements, too. Online and on-ground seminars and private appointments are also available! But for now, read and learn from the “comments“ tab. It’s fast, free and secure!
Conclusion
So, there are several ways to interact with the ME-P, and more are scheduled in the future.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
***
![]()
![]()
![]()
8
***
Filed under: Career Development, Estate Planning, Financial Planning, Information Technology, Managed Care, Marketing & Advertising, Professional Liability, Recommended Books, Risk Management | Tagged: CMP, Dr. David Marcinko, Medical Executve-Post, www.certifiedmedicalplanner.com | 1 Comment »
![]()
Call for Applications
 By David B. Nash, MD, MBA
By David B. Nash, MD, MBA
[Dean, Jefferson College of Population Health]
Dear Colleagues:
We are excited to announce that we are now accepting applications for the Hearst Health Prize for Excellence in Population Health. The winner will receive a $100,000 cash prize in recognition of outstanding achievement in managing or improving population health.
Hearst Health Prize
The Hearst Health Prize, in partnership with the Jefferson College of Population Health (JCPH), was created to help identify and promote promising new ideas in the field that will help to improve health outcomes. Our goal is to discover, support and showcase the work of an individual, group, or institution that has successfully implemented a population health program or intervention that has made a measurable difference. image The competition is open to individuals, groups, organizations or institutions, except those employed JCPH, Hearst Corporation, or their respective affiliates.
For more details, click here. Finalists will be invited to present their project at a special poster session at the Population Health Colloquium in Philadelphia on March 7, 2016. The winner of the prize will be announced during the opening session of the Population Health Colloquium on March 8, 2016.
***

***
Assessment
Click here to apply or learn more about the Hearst Health Prize. The deadline to apply is October 23, 2015. If you have questions, please email HearstHealthPrize@jefferson.edu. We hope that you share this amazing opportunity with your colleagues!
More:
We are pleased that Dr. Nash wrote the Foreword to our newest book. Read it here: [Foreword Dr. Nash MD MBA FACP
Conclusion
Your thoughts and comments on this ME-P are appreciated. Feel free to review our top-left column, and top-right sidebar materials, links, URLs and related websites, too. Then, subscribe to the ME-P. It is fast, free and secure.
Speaker: If you need a moderator or speaker for an upcoming event, Dr. David E. Marcinko; MBA – Publisher-in-Chief of the Medical Executive-Post – is available for seminar or speaking engagements. Contact: MarcinkoAdvisors@msn.com
OUR OTHER PRINT BOOKS AND RELATED INFORMATION SOURCES:
[Foreword Dr. Phillips MD JD MBA LLM]
![]()
[Foreword Dr. Nash MD MBA FACP]
***
Filed under: Career Development, Research & Development | Tagged: David B. Nash, Hearst Health Prize, MBA, MD, Population Health | 1 Comment »










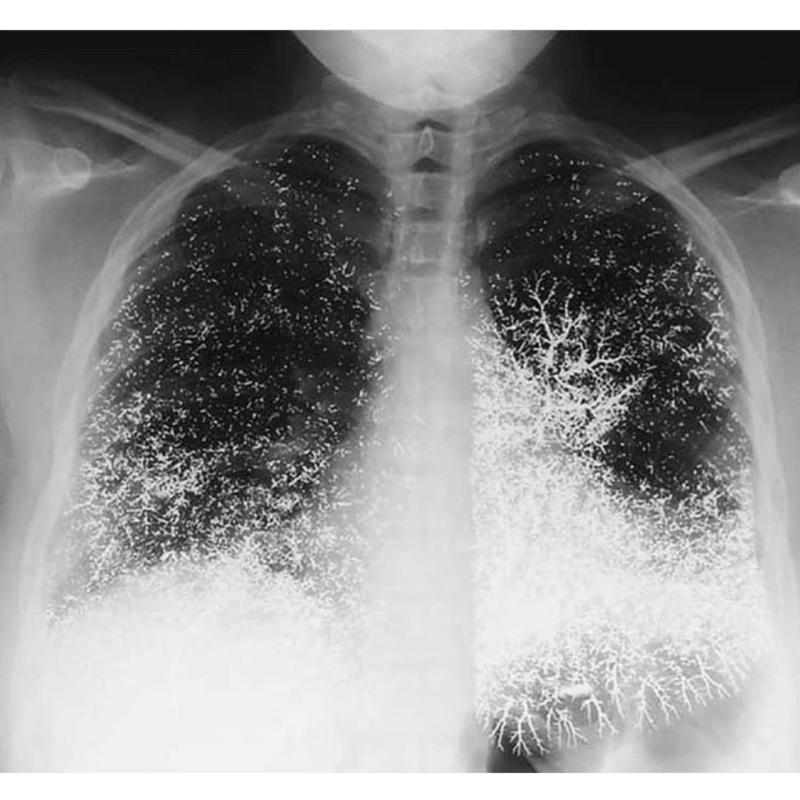 A chest radiograph showed that the mercury was distributed in the lungs in a vascular pattern that was more pronounced at the bases.
A chest radiograph showed that the mercury was distributed in the lungs in a vascular pattern that was more pronounced at the bases.







































